
Submitted:
24 February 2026
Posted:
25 February 2026
You are already at the latest version
Abstract
Purpose: To investigate the short-term impact of scleral lens wear on intraocular pressure (IOP) and retinal nerve fiber layer thickness (RNFL).
Methods: This prospective study included 31 healthy participants aged 26 ± 3 years who were randomly fitted with a 16.5 mm scleral lens over one eye and a soft contact lens on the other eye. IOP and RNFL thickness were examined at baseline in the morning and following 8 hours of scleral and soft contact lens wear in the evening. Two tonometers (a transpalpebral Diaton and a non-contact tonometer) were used to measure IOP. Measurements of IOP and RNFL were taken under four different conditions: pre- and post-lens application, and pre- and post-lens removal.
Results: Eyes fitted with a scleral lens exhibited a significant increase in IOP (pre-application: 11± 3 mmHg vs. post-application: 16 ± 4 mmHg, P < 0.001) immediately after scleral lens application, and the increase in pressure was sustained throughout the 8 hours of lens wear (pre-removal IOP: 16 ± 4 mmHg). IOP returned to baseline after scleral lens removal (11 ± 3 mmHg). Eyes fitted with soft contact lenses did not show significant IOP changes under any condition (P >0.05). Eyes with a scleral lens also showed a small but significant thinning of peripapillary RNFL (pre-application: 110 ± 11 µm vs. post-application: 107 ± 11 µm, P < 0.001) after 8 hours of lens wear, which was not significant with soft contact lens wear (P > 0.05). IOP data obtained from Diaton showed poor
within-participant variation and poor agreement compared to IOP data from the non-contact tonometer.
Conclusion: This study suggests that short-term scleral lens wear may significantly raise IOP and cause transient peripapillary RNFL thinning, which returns to baseline immediately following lens removal. Monitoring IOP and RNFL is recommended for scleral lens wearers, with future research needed to assess the long-term effects.
Keywords:
scleral lens
; intraocular pressure
; retinal fiber thickness
; contact lens
1. Introduction
Scleral contact lenses have gained significant popularity over the last two decades due to their advantages in enhancing visual outcomes and comfort across a range of ocular conditions.[1] These lenses have demonstrated therapeutic potential by successfully fitting most patients with distorted corneas who are intolerant to other forms of vision correction, such as piggyback, hybrid, or corneal gas-permeable lenses.[2] Scleral lenses are essential optimizing visual outcomes, protecting the ocular surface, improving ocular aesthetics, and supporting performance in athletic activities.[3] Corneal ectasia remains the primary indication for scleral lens fitting, followed by post-penetrating keratoplasty patients.[2,4] Scleral lenses have been shown to reduce higher order aberrations, including coma and spherical aberrations, in corneal ectasias and surfaceirregularities.[5] Furthermore, severe ocular surface disease has long been an indication for large scleral lens use.[6] Patients suffering from exposure keratitis and ocular surface disease may particularly benefit from scleral lenses due to the fluid reservoir maintained behind the lens.[7] Scleral lenses have also proven useful in managing various eyelid conditions such as ptosis, eyelid coloboma, entropion, and ectropion.[8] Studies have documented a marked reduction in photophobia in 75% of patients treated with scleral lenses.[9] Despite the successes of scleral lenses, adverse events, such as an associated increase in intraocular pressure (IOP), have raised concerns.[10] The fitting of scleral lenses differs substantially from that of soft contact lenses. Scleral lenses typically vault over the cornea and rest on the adjacent bulbar conjunctiva. Mechanical pressure from eyelid blinking is hypothesized to displace scleral lenses deeper into the conjunctiva, generating a suction effect that may impact ocular structures such as the episcleral veins, trabecular meshwork, and associated drainage pathways.[11] The amount of posterior-directed force may contribute to resistance in aqueous humor outflow from the eye.[12] All current clinical methods for measuring IOP require direct contact with the cornea, such as with a Goldmann tonometer or using a non-contact tonometer on a bare cornea. Both methods present challenges when measuring IOP with scleral lenses in place.[13] Researchers have developed strategies to address this issue by either measuring IOP immediately after lens removal, using devices on the conjunctiva, or obtaining measurements through the eyelid while the scleral lens is still being worn using a transpalpebral tonometer.[14] Several recent studies have examined the changes in lens settling time, fluid reservoir thickness and IOP associated with scleral lens wear.[6,14,15,16] The majority of these studies reported an increase in IOP with scleral lens use. Some studies have reported no change in IOP after 2 hours of scleral lens wear compared to fellow non-contact lens wearing eyes.[17,18] Similarly, some studies have even observed decreases in IOP following lens wear, consistent with a normal diurnal fluctuation in IOP.[19]
However, there are variations in the types of scleral lenses used, sizes, and IOP measurement techniques across studies. Retinal nerve fiber layer (RNFL) defects are a structural manifestation of the damage caused by elevated IOP, such as in glaucoma, and typically precede the development of glaucomatous vision loss.[20,21] Therefore, elevated IOP raises concerns about potential damage to the RNFL. Although studies have shown that for glaucoma progressing eyes, each 1 mmHg higher average IOP during follow-up was associated with an additional average loss of 0.20 µm/year and higher levels of IOP were associated with faster rates of RNFL loss over time measured by SD OCT.[22]Studies also have looked at the effect of scleral lens wear on Bruch’s membrane opening, minimum rim width and reported insignificant impact on optic nerve head morphology.[23] However, the impact of scleral lens-associated increases in IOP on the RNFL has not been thoroughly investigated. This study aims to examine the short-term impact of scleral lens wear on IOP, using two IOP measurement techniques (Diaton and non-contact tonometer), and the impact of scleral lens wear on RNFL compared with soft contact lens wear.
2. Methods
This randomized cross-over study complied with the tenets of the Declaration of Helsinki and received approval from the Institutional Review Board at Pacific University College of Optometry. Randomization was carried out using an online randomization tool, and participants were assigned sequential study identification number in the order of enrollment. The subjects were recruited based on voluntary sign up in response to the email that was sent out as a list-served provided by the school for optometry and vision science students studying in various years. Written informed consent was obtained from all participants before the study commenced.
2.1. Subjects
A total of thirty-one healthy participants were aged 18 to 40 years were recruited from the pool of optometry and vision science program at Pacific University. All participants had a best-corrected visual acuity of 0.3 logMAR or better and blood pressure within the range of 90/60 to 135/90 mmHg in a normal resting position. Participants with any ocular pathologies, elevated intraocular pressure (IOP) greater than 20 mmHg at the screening visit, a history of glaucoma, or previous refractive surgery were excluded from the study. Subjects were instructed to refrain from hard physical activities and/or or caffeine, marijuana, and/or alcohol consumption 6 hours before all visits in the study, as these behaviors may influence the IOP.

Table 1.
Specifications of Scleral and Soft Contact Lenses.
| Scleral lens | Soft lens | |
|---|---|---|
| Contact lens brand | Comfort Optimum Extra | Acuvue Oasys 1 Day |
| Material | Roflufocon D | Senofilcon A |
| Refractive index | 1.43 | 1.40 |
| Dk value (Barrer) | 100 | 103 |
| Diameter (mm) | 16.5 | 14.3 |
2.2. Measurements and Data Collection Procedures
This study required a total of 5 visits over 3 days (Figure 1). The Baseline day’s visits include scleral contact lens determination and soft contact lens fitting, and the baseline measurements of refractive errors, IOP and the anterior segment and retinal imaging. Refractive error and K readings were measured objectively using an auto-refractor/keratometer (Nidek ARK-510A, Tokyo, Japan) and Medmont E300 Corneal Topography was used to choose the initial contact lens from the diagnostic set for each eye. A slit-lamp screening was performed to confirm their eligibility for the study based on our inclusion and exclusion criteria using a slit lamp biomicroscope (Carl Zeiss Meditec AG, Jena, Germany). During the screening visit, participants’ eligibility was determined, and baseline measurements, including subjective refraction, IOP (measured with non-contact tonometer and Diaton tonometers), retinal nerve fiber layer (RNFL) thickness, and blood pressure, were collected.
Contact lenses were selected randomly based on the randomization generator and sign-up order of the participants. The experiment was conducted on two separate days, ensuring a minimum washout period of 24 hours between sessions to minimize carryover effects.
IOP and RNFL measurements were taken four times daily: 1) pre-lens application, 2)post-lens application, 3) pre-lens removal, and 4) post-lens removal. All pre- and post-lens application measurements were obtained in the morning, while pre- and post-lens removal measurements were taken in the evening. Each participant wore both lenses for 8 hours. Figure 1 illustrates the data collection procedures.
IOP measurements were obtained using a non-contact tonometer (Canon Full Auto Tonometer TX-F, Japan) for pre-lens application and post-lens removal. The Diaton tonometer (BICOM Inc., Long Beach, NY, USA) was used to measure IOP under all four conditions, with participants in a supine position, gazing at a target placed approximately 45 degrees downward. The probe was positioned vertically over the tarsus, just above the lens margin on the upper eyelid. At least three measurements were taken and averaged for the final IOP value at each time point. Any IOP readings falling outside ±2 mmHg of the first measurements was disregarded and the average of three measurements was recorded as a single reading. IOP measurements were consistently obtained within 2–3 minutes after lens removal, a timeframe selected based on prior evidence indicating that post-lens IOP fluctuations occur rapidly within the first few minutes. Measurement consistency was enhanced by standardizing Diaton probe placement relative to the superior limbus, controlling upper eyelid positioning, utilizing a single experienced examiner for all measurements, and avoiding contact over the scleral lens landing zone. Although minor micro-variations in probe placement cannot be entirely eliminated, intersession variability remained low (standard deviation < 2 mmHg across repeated trials), supporting acceptable reproducibility.
Optovue optical coherence tomography (Optovue Inc., Fremont, CA) was used to measure the RNFL with a scanning speed of 70,000 A-scans/second, optical axial resolution of 5 μm, and transverse resolution of 15 μm. RNFL measurements were taken at baseline and under all four conditions. Three scans were obtained and averaged to derive the final value. Peripapillary, overall average, superior, and inferior RNFL were analyzed. The optic nerve head scan method consisted of four circular scans with a 3.45-mm diameter centered on the optic disc, each containing 1,024 A-scans. The "average RNFL thickness" was determined as the automated average of superior and inferior RNFL thickness and the overall RNFL thickness from the optic nerve head scan that was examined using Optovue optical coherence tomography (Optovue Inc., Fremont, CA). All the measurements were conducted around the same time of the day for each participants to avoid the influence from the diurnal variation.
2.3. Randomization and Crossover Protocol
A prospective, randomized, contralateral-eye crossover design was employed. After eligibility was confirmed during the screening visit, subjects were randomized using a computer-generated allocation sequence to determine which eye would receive the SL and which would receive the SCL at the first study visit.
At Visit 1, one eye was fitted with a scleral lens and the fellow eye with a soft contact lens according to the randomization assignment. Following a washout period of at least 24 hours without lens wear, participants returned for Visit 2, during which the lens assignments were reversed between eyes. For example, if the right eye received the SL and the left eye received the SCL at Visit 1, the right eye received the SCL and the left eye received the SL at Visit 2.
Both lens types were fitted with full refractive correction to achieve best-corrected visual acuity in each eye. This contralateral crossover design allowed each eye to serve as its own control while minimizing inter-subject variability.
Contact lens fitting was performed using a standardized diagnostic fitting set. An initial scleral contact lens from the diagnostic set and targeting 200 µm to 300µm of the apical corneal clearance after the lens settling. All SL fitting utilized 16.5 mm Ampleye Scleral Lenses (Boston MA, USA) manufactured in Contamac Extra (Contamac Ltd., UK). Soft contact lens (SCL) of 14.00mm diameter were used. Lens selection was based on the horizontal visible iris diameter (HVID) and the refractive error of the participant to ensure the optimal vision, centration and movement. Both SL and SCL fits were evaluated using slit-lamp biomicroscopy to confirm adequate centration, movement (for SCL), absence of conjunctival blanching or impingement (for SL), and overall ocular surface compatibility.
To minimize procedural variability and potential confounding effects on intraocular pressure (IOP), a single experienced investigator performed all lens applications and removals for every participant. This approach was implemented to reduce inter-operator variability and to control for differences in application force, which may influence conjunctival compression and subsequently affect IOP measurements, particularly in inexperienced contact lens wearers.
2.4. Statistical Analysis
With the effect size of 0.5 and correlation of 0.7,sample size estimates were calculated for a power of 80% and a p-value of 0.05.The normality of the data was assessed using the Kolmogorov- Smirnov test. For each variable of interest (IOP, RNFL thickness etc.), repeated measures analysis of variance (ANOVA) was used. This statistical approach considers both factors; lens type (2 levels) and time point (4 levels) as well as their interaction (lens type × time point). The repeated measures ANOVA sphericity assumption was met and verified in the analysis. Paired t- tests were also utilized for specific comparisons, with Bonferroni corrections applied to adjust for multiple comparisons where applicable. Bland-Altman analysis, linear regression, and the
Pearson correlation coefficient was used to evaluate the performance of the two tonometers (Diaton and non-contact tonometer) in measuring IOP. All statistical analyses were performed using SPSS Statistics, version 28 (SPSS Inc., Chicago, IL, USA).
3. Results
3.1. Demographics and Clinical Characteristics
A total of thirty-one healthy participants (20 females, 64.5%), aged between 20 and 31 years (mean age 26 ± 3 years), were recruited and completed the study. The mean spherical equivalent was -3.25 ± 3.25 D, with a range of -9.25 to -0.50 D. All participants had normal baseline intraocular pressure (IOP), which ranged from 8 to 20 mmHg, with a mean IOP of 14.0 ± 3.0 mmHg. The demographic and clinical data of the participants are summarized in Table 2.
3.2. Intraocular Pressure (IOP)
To control for diurnal variation, all measurements for both IOP and RNFL thickness were taken at the same time of day for each participant during their experimental visits. The mean baseline IOP (pre-lens application) measured on the morning of the first experimental visit using the non-contact tonometer (NCT) and Diaton tonometer was 11.3 mmHg (95% CI, 11 to 12 mmHg). In contrast, the baseline IOP measured simultaneously with the NCT tonometer was 14.17 mmHg (95% CI, 14 to 15 mmHg). There was no significant difference in baseline IOP between the right and left eyes with either tonometer (all P > 0.05). The assumption of sphericity was tested using Mauchly’s test for IOP. The results indicated that the assumption of sphericity was met, with Mauchly's test yielding a non-significant result, P = 0.48. The repeated measures ANOVA revealed a significant main effect of lens type, F(1,685) =102, P < 0.001, and a significant main effect of time point, F(3, 685) = 13.3, P < 0.001. In addition, there was a significant interaction between lens type and time point, F(3, 685) =31.7, P < 0.001.
After lens application, IOP was measured using the Diaton tonometer within 5 minutes of lens wear. In eyes fitted with scleral lenses, the mean IOP increased to 15.8 mmHg (95% CI, 15 to 17 mmHg), representing a significant rise of 4.5 mmHg from baseline (P < 0.0001). In contrast, the mean IOP in eyes with soft contact lenses was 11.7 mmHg (95% CI, 11 to 12 mmHg), with no significant difference from baseline 11.63 mmHg (P = 0.48) (Figure 2).
During the 8 hours of contact lens wear, the average IOP in control eyes (soft contact lenses) remained stable at approximately 12 mmHg (95% CI, 11 to 12 mmHg) between post-lens application and pre-removal, with no significant change from application to removal (P = 0.63). There was no significant difference in IOP during the 8-hour lens wear period (post-lens application and pre-removal) in the scleral lens group (P = 0.37) (Figure 2).
After lens removal, the soft contact lens group had a mean IOP (Diaton) of 10.68 mmHg (95% CI, 10 to 11 mmHg), which was a small but statistically significant reduction of 1 mmHg from baseline (Diaton, 11.63 mmHg [95% CI, -1 to -1 mmHg]; P = 0.02). In the scleral lens group, mean IOP after removal returned to baseline (Diaton, 11.2 mmHg [95% CI, 11 to 12 mmHg]; P = 0.71) (Figure 2).
Comparing Diaton and NCT for IOP measurements at bassline, there was a significant difference (Diaton, 11.35 ± 3 mmHg [95% CI, 11 to 12 mmHg]; NCT, 14.17 ± 3 mmHg [95% CI, 14 to 15 mmHg]; P < 0.001). Bland-Altman analysis revealed poor agreement between the two instruments (regression slope = 22, R² = 0.024, and Y-intercept = 9.5). An ANOVA summary for IOP showing both main effects and interactions is provided in Table 3.
3.3. Retinal Nerve Fiber Layer (RNFL) Thickness
The mean overall RNFL thickness at baseline, measured in the morning, was 98.9 ± 7 μm (95% CI, 97 to 101 μm) in eyes fitted with scleral lenses and 98.6 ± 8 μm (95% CI, 97 to 101 μm) in eyes fitted with soft contact lenses (P = 0.23). The assumption of sphericity was tested using Mauchly’s test for RNFL. The results indicated that the assumption of sphericity was met, with Mauchly's test yielding a non-significant result, P = 0.62. For the overall RNFL, the repeated measures ANOVA showed a significant main effect of lens type, F(1, 701) = 18, P < 0.001, and a significant main effect of time point, F(3,701) = 47, P < 0.001. In addition, there was a significant interaction between contact lens type and time point, F(3, 701) = 13.5, P < 0.001.
After lens application, eyes fitted with scleral lenses showed a reduction in overall RNFL thickness, reaching a mean of 96 ± 8 μm (95% CI, 95 to 98 μm) (P < 0.001). In contrast, eyes fitted with soft lenses showed unchanged mean thickness of 98 μm (95% CI, 97 to 100 μm) (P < 0.30). Prior to lens removal, eyes fitted with scleral lenses showed a reduction in overall RNFL thickness, reaching a mean of 96 ± 8 μm (95% CI, 95 to 98; P < 0.001). Eyes fitted with soft lenses did not exhibit a statistically significant reduction, with a mean thickness of 98 ± 8 μm (95% CI, 97 to 100 μm; P < 0.11). suggesting that the initial thinning observed with scleral lenses occurred shortly after lens application and was maintained throughout the wear period.
Following lens removal, the overall RNFL thickness returned toward baseline in both the scleral lens group (97.8 ± 8 μm [95% CI, 96 to 100 μm]; P = 0.07) and the soft lens group (97.6 ± 8 μm [95% CI, 96 to 100 μm]; P = 0.10). Over the 8-hour lens wear period, overall RNFL thickness remained stable in both the scleral and soft lens groups (P = 0.27 and 0.1, respectively). Following lens removal, the overall RNFL thickness returned to baseline in both the scleral lens group (97.8 μm [95% CI, 96 to 100 μm]; P = 0.07) and the soft lens group (97.6 μm [95% CI, 96 to 100 μm]; P = 0.1). An ANOVA summary for RNFL showing both main effects and interactions is provided in Table 4.
Although both lens types were associated with transient RNFL thinning, only the scleral lens group demonstrated concurrent IOP elevation, suggesting that different mechanisms such as mechanical deformation, fluid dynamics, or measurement artifact may underlie these changes This distinction warrants further investigation and is discussed in more detail below.
Further analysis of the peripapillary, superior, and inferior RNFL thickness revealed no significant differences in peripapillary RNFL (P = 0.41), superior RNFL (P = 0.20), or inferior RNFL (P = 0.74) before lens application between the scleral and soft lens groups. However, consistent with the observed overall RNFL thickness reduction after scleral lens application, significant thinning was observed in peripapillary (P < 0.001), superior (P < 0.001), and inferior RNFL thickness (P < 0.001). The most pronounced thinning occurred in the peripapillary region (mean difference from baseline = -2.9 μm), followed by superior RNFL (-2.2 μm), average RNFL (-1.9 μm), and inferior RNFL (-1.8 μm) thickness. There were no significant differences in RNFL thickness between pre-lens application and post-lens removal (Figure 3 A-D).
4. Discussion
This study investigated the short-term effects of scleral lens wear on IOP and RNFL thickness in healthy young adults with a wide range of refractive errors. A significant increase in IOP, exceeding 4 mmHg on average, was observed during scleral lens wear and persisted until lens removal. Simultaneously, a statistically significant thinning of the RNFL was detected, suggesting a potential association between the observed RNFL changes and increased IOP.
Following scleral lens removal, IOP in the test eye dropped significantly to baseline levels, with less than a 1 mmHg difference between test and control eyes using the Diaton tonometer. These findings align with previous studies reporting transient increases in IOP during scleral lens wear.[16] The potential causes of this IOP elevation include compression of the bulbar conjunctiva, leading to altered aqueous humor dynamics, increased red cell content, and local cyanosis in the scleral lens-covered region.[24] Additionally, post-lens fluid forces and eyelid tension may contribute to altered lens fit and compression of conjunctival and scleral tissues, further exacerbating IOP elevation.[19] A previous study revealed an average IOP increase of 5 mmHg with a 16.5 mm diameter scleral lens, consistent with prior research reporting similar IOP elevations regardless of lens diameter.[16] However, due to the lack of a standardized device for measuring IOP during scleral lens wear, the clinical significance of these findings remains inconclusive. The poor agreement between Diaton tonometer and NCT measurements highlights the variability and limitations of current methods for assessing IOP in the presence of scleral lenses.[25,26] While the NCT showed better agreement with GAT, the inconsistency of Diaton measurements underscores the need for improved measurement techniques in such scenarios.[18] Changes in RNFL thickness during scleral lens wear were also explored, marking this study as the first to examine this parameter. The RNFL thinning observed immediately after scleral lens application may be linked to the IOP increase; however, the small magnitude of change is likely not clinically significant in healthy individuals. This result aligns with previous studies suggesting that RNFL thickness is correlated with other structural metrics, such as minimum rim width.[27] Additionally, RNFL thinning throughout the day is well-documented, as diurnal variations lead to greater thinning in the afternoon and evening compared to morning measurements.[28] However, the RNFL thinning detected in this study occurred shortly after lens application, which may reflect a more immediate response to mechanical or pressure-related factors. The natural homeostasis of IOP involves complex regulatory mechanisms that help mitigate transient IOP spikes, such as those observed during scleral lens wear. Factors like trabecular meshwork adaptation, enhanced pulsatile flow, or upstream resistance reduction play a critical role in maintaining stable IOP.[29] In healthy individuals, these mechanisms are generally sufficient to prevent prolonged stress on the optic nerve head. However, glaucomatous eyes, which lack robust autoregulatory mechanisms, may be more vulnerable to the effects of IOP elevation.[30,31] Future studies should replicate similar experiments in glaucoma patients to assess whether scleral lens wear poses additional risks in this population. While scleral lenses are traditionally used to manage corneal ectasias and surface irregularities, their growing adoption among individuals with high myopia highlights the importance of understanding their potential impacts on IOP and ocular health. Elevated IOP may pose a higher risk of glaucoma-like damage to the posterior structures in highly myopic eyes due to the unique biomechanical and structural changes associated with high myopia.[32] Axial elongation, a hallmark of high myopia, leads to stretching and thinning of the sclera, particularly in the posterior pole.[33] This thinning reduces the sclera’s ability to provide structural support to the ONH and surrounding tissues, making them more vulnerable to IOP- related stress.[34] Additionally, scleral thinning is often accompanied by changes in scleral stiffness; the sclera becomes more compliant and less able to resist deformation under elevated IOP. This increased biomechanical susceptibility can exacerbate stress and strain transmission to the ONH, leading to deformation of the lamina cribrosa and potential disruption of axonal pathways.[35] Furthermore, in highly myopic eyes, the elongated geometry creates a steeper translaminar pressure gradient, further amplifying the mechanical impact of elevated IOP on the ONH. These combined factors axial elongation, scleral thinning, and altered stiffness render highly myopic eyes less capable of withstanding IOP fluctuations, increasing the risk of glaucomatous damage even at IOP levels that may be considered normal in non-myopic eyes.[36] This underscores the need for cautious monitoring of IOP and posterior segment changes in patients with high myopia, particularly during interventions such as scleral lens wear that may transiently elevate IOP. For future studies, vascular landmarks should be integrated into the analysis to better quantify potential variations in transverse magnification and to realign images, ensuring direct comparison of RNFL thickness at the exact same location.
5. Conclusions
This study is the first to evaluate peripapillary retinal nerve fiber layer (RNFL) thickness as an indirect structural marker of intraocular pressure (IOP) changes during scleral lens wear. The findings demonstrate a statistically significant increase in IOP in healthy eyes during scleral lens use, accompanied by modest peripapillary RNFL thinning. Although small variations were observed, the magnitude of change did not suggest a clinically significant impact on the optic nerve in this cohort of healthy participants. These findings support the hypothesis that short-term scleral lens wear can induce measurable alterations in ocular physiology; however, the observed effects were subtle and may not reach a clinically meaningful threshold in the short term.
Importantly, these initial results warrant further investigation in larger and more diverse populations, with extended wear durations, to determine whether cumulative or long-term exposure may produce clinically significant structural or functional consequences. This is particularly relevant for individuals at higher risk of optic nerve vulnerability, such as those with high myopia or other predisposing conditions. A more comprehensive understanding of these physiological responses will be essential for refining evidence-based clinical guidelines and ensuring the safe use of scleral lenses across diverse patient populations.
6. Limitation
This study was limited by its short-term evaluation of SCL wear (eight hours) in healthy young adults, which may not reflect the long-term effects on IOP and RNFL thickness. Healthy eyes may temporarily regulate IOP increases, but the duration and extent of this compensation remain unclear. Additionally, glaucomatous eyes and individuals with collagen disorders like keratoconus may respond differently due to impaired IOP regulation, underscoring the need for further research in these populations. Moreover, the use of the Diaton tonometer may present limitations, as several studies have questioned its accuracy and reliability in measuring true intraocular pressure.
Disclosure: This research was conducted as partial fulfillment of the requirements for the Master of Science in Vision Science degree at Pacific University School of Optometry. The manuscript/abstract was previously submitted as a thesis and deposited in the Pacific University Library repository.
References
- Pearson, RM. Karl Otto Himmler, manufacturer of the first contact lens. Contact Lens and Anterior Eye 2007, 30(1), 11–16. [Google Scholar] [CrossRef]
- Pecego, M; Barnett, M; Mannis, MJ; Durbin-Johnson, B. Jupiter Scleral Lenses: The UC Davis Eye Center Experience. Eye & Contact Lens: Science & Clinical Practice 2012, 38(3), 179–182. [Google Scholar] [CrossRef]
- Harthan, JS; Shorter, E. Therapeutic uses of scleral contact lenses for ocular surface disease: patient selection and special considerations. OPTO 2018, Volume 10, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Pullum, KW; Whiting, MA; Buckley, RJ. Scleral Contact Lenses: The Expanding Role. Cornea 2005, 24(3), 269–277. [Google Scholar] [CrossRef]
- Visser, ES; Visser, R; van Lier, HJJ; Otten, HM. Modern Scleral Lenses Part II: Patient Satisfaction. Eye & Contact Lens: Science & Clinical Practice 2007, 33(1), 21–25. [Google Scholar] [CrossRef]
- Gumus, K; Gire, A; Pflugfelder, SC. The Impact of the Boston Ocular Surface Prosthesis on Wavefront Higher-Order Aberrations. American Journal of Ophthalmology 2011, 151(4), 682–690.e2. [Google Scholar] [CrossRef]
- Fadel, D. The influence of limbal and scleral shape on scleral lens design. Contact Lens and Anterior Eye 2018, 41(4), 321–328. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, P; Croteau, A. Fluid-Ventilated, Gas-Permeable Scleral Contact Lens Is an Effective Option for Managing Severe Ocular Surface Disease and Many Corneal Disorders That Would Otherwise Require Penetrating Keratoplasty. Eye & Contact Lens: Science & Clinical Practice 2005, 31(3), 130–134. [Google Scholar] [CrossRef]
- Van Der Worp, E; Bornman, D; Ferreira, DL; Faria-Ribeiro, M; Garcia-Porta, N; González-Meijome, JM. Modern scleral contact lenses: A review. Contact Lens and Anterior Eye 2014, 37(4), 240–250. [Google Scholar] [CrossRef]
- Michaud, L; Balourdet, S; Samaha, D. Variation of Bruch’s membrane opening in response to intraocular pressure change during scleral lens wear, in a population with keratoconus. Ophthalmic Physiologic Optic 2025, 45(2), 405–415. [Google Scholar] [CrossRef]
- Schornack, MM; Brown, WL; Siemsen, DW. The use of tinted contact lenses in the management of achromatopsia. Optometry - Journal of the American Optometric Association 2007, 78(1), 17–22. [Google Scholar] [CrossRef] [PubMed]
- Walker, MK; Bergmanson, JP; Miller, WL; Marsack, JD; Johnson, LA. Complications and fitting challenges associated with scleral contact lenses: A review. Contact Lens and Anterior Eye 2016, 39(2), 88–96. [Google Scholar] [CrossRef]
- Thoft, RA; Friend, J. Biochemical Aspects of Contact Lens Wear. American Journal of Ophthalmology 1975, 80(1), 139–145. [Google Scholar] [CrossRef]
- Kauffman, MJ; Gilmartin, CA; Bennett, ES; Bassi, CJ. A Comparison of the Short-Term Settling of Three Scleral Lens Designs. Optometry and Vision Science 2014, 91(12), 1462–1466. [Google Scholar] [CrossRef]
- Nau, CB; Schornack, MM; McLaren, JW; Sit, AJ. Intraocular Pressure After 2 Hours of Small-Diameter Scleral Lens Wear. Eye & Contact Lens: Science & Clinical Practice 2016, 42(6), 350–353. [Google Scholar] [CrossRef] [PubMed]
- Michaud, L; Samaha, D; Giasson, CJ. Intra-ocular pressure variation associated with the wear of scleral lenses of different diameters. Contact Lens and Anterior Eye 2019, 42(1), 104–110. [Google Scholar] [CrossRef]
- Nau, CB; Schornack, MM; McLaren, JW; Sit, AJ. Intraocular Pressure After 2 Hours of Small-Diameter Scleral Lens Wear. Eye & Contact Lens: Science & Clinical Practice 2016, 42(6), 350–353. [Google Scholar] [CrossRef] [PubMed]
- Walker, MK; Pardon, LP; Redfern, R; Patel, N. IOP and Optic Nerve Head Morphology during Scleral Lens Wear. Optom Vis Sci. 2020, 97(9), 661–668. [Google Scholar] [CrossRef]
- Vincent, SJ; Alonso-caneiro, D; Collins, MJ. Evidence on scleral contact lenses and intraocular pressure. Clinical and Experimental Optometry 2017, 100(1), 87–88. [Google Scholar] [CrossRef]
- Jung, EH; Lee, EJ; Kim, TW. Topographic Relationship with a Retinal Nerve Fiber Layer Defect Differs between β -Zone and γ -Zone Parapapillary Atrophy. Journal of Ophthalmology 2020, 2020, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, K; Bowd, C; Weinreb, RN; Medeiros, FA; Sample, PA; Zangwill, LM. Retinal nerve fiber layer thickness measurements with scanning laser polarimetry predict glaucomatous visual field loss. American Journal of Ophthalmology 2004, 138(4), 592–601. [Google Scholar] [CrossRef]
- Diniz-Filho, A; Abe, RY; Zangwill, LM; et al. Association between Intraocular Pressure and Rates of Retinal Nerve Fiber Layer Loss Measured by Optical Coherence Tomography. Ophthalmology 2016, 123(10), 2058–2065. [Google Scholar] [CrossRef]
- Walker, MK; Pardon, LP; Redfern, R; Patel, N. IOP and Optic Nerve Head Morphology during Scleral Lens Wear. Optom Vis Sci. 2020, 97(9), 661–668. [Google Scholar] [CrossRef] [PubMed]
- Mcmonnies, CW. A hypothesis that scleral contact lenses could elevate intraocular pressure. Clinical and Experimental Optometry 2016, 99(6), 594–596. [Google Scholar] [CrossRef] [PubMed]
- Li, Y; Shi, J; Duan, X; Fan, F. Transpalpebral measurement of intraocular pressure using the Diaton tonometer versus standard Goldmann applanation tonometry. Graefe’s Archive for Clinical and Experimental Ophthalmology 2010, 248(12), 1765–1770. [Google Scholar] [CrossRef]
- Doherty, MD; Carrim, ZI; O’Neill, DP. Diaton tonometry: an assessment of validity and preference against Goldmann tonometry. Clinical Exper Ophthalmology 2012, 40(4). [Google Scholar] [CrossRef] [PubMed]
- Chauhan, BC; Danthurebandara, VM; Sharpe, GP; et al. Bruch’s Membrane Opening Minimum Rim Width and Retinal Nerve Fiber Layer Thickness in a Normal White Population: A Multicenter Study. Ophthalmology 2015, 122(9), 1786–1794. [Google Scholar] [CrossRef]
- The Trabecular Meshwork: A Basic Review of Form and Function. J Ocul Biol. 2014, 2(1). [CrossRef]
- Johnstone, M; Jamil, A; Martin, E. Aqueous Veins and Open Angle Glaucoma. In The Glaucoma Book; Schacknow, PN, Samples, JR, Eds.; Springer New York, 2010; pp. 65–78. [Google Scholar] [CrossRef]
- Acott, TS; Kelley, MJ; Keller, KE; et al. Intraocular Pressure Homeostasis: Maintaining Balance in a High-Pressure Environment. Journal of Ocular Pharmacology and Therapeutics 2014, 30(2-3), 94–101. [Google Scholar] [CrossRef]
- Johnstone, M; Jamil, A; Martin, E. Aqueous Veins and Open Angle Glaucoma. In The Glaucoma Book; Schacknow, PN, Samples, JR, Eds.; Springer New York, 2010; pp. 65–78. [Google Scholar] [CrossRef]
- Chuangsuwanich, T; Tun, TA; Braeu, FA; et al. How Myopia and Glaucoma Influence the Biomechanical Susceptibility of the Optic Nerve Head. Invest Ophthalmol Vis Sci. 2023, 64(11), 12. [Google Scholar] [CrossRef]
- Ohno-Matsui, K; Wu, PC; Yamashiro, K; et al. IMI Pathologic Myopia. Invest Ophthalmol Vis Sci. 2021, 62(5), 5. [Google Scholar] [CrossRef]
- Jia, X; Yu, J; Liao, SH; Duan, XC. Biomechanics of the sclera and effects on intraocular pressure. Int J Ophthalmol. 2016, 9(12), 1824–1831. [Google Scholar] [CrossRef]
- Boote, C; Sigal, IA; Grytz, R; Hua, Y; Nguyen, TD; Girard, MJA. Scleral structure and biomechanics. Prog Retin Eye Res. 2020, 74, 100773. [Google Scholar] [CrossRef]
- Jiang, J; Lin, T; Lin, F; et al. Effect of intraocular pressure reduction on progressive high myopia (PHM study): study protocol of a randomised controlled trial. BMJ Open. 2024, 14(6), e084068. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart illustrating the study data collection procedures in screening and experimental visits.
Figure 1.
Flowchart illustrating the study data collection procedures in screening and experimental visits.
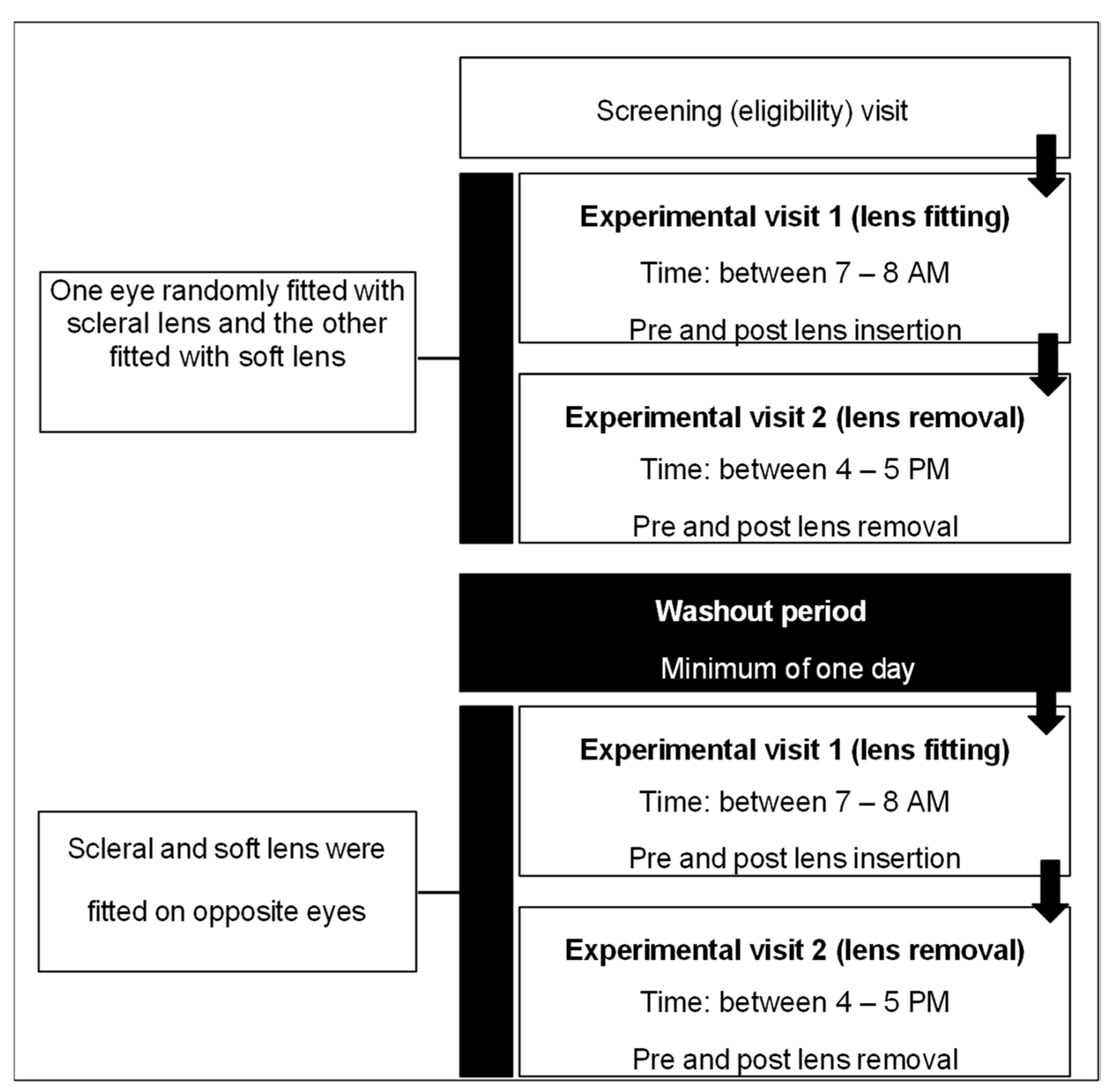
Figure 2.
Mean IOP and changes during 8 hours of soft and scleral lens wear, measured using Diaton tonometer. Error bars represent the 95% confidence intervals of each time.
Figure 2.
Mean IOP and changes during 8 hours of soft and scleral lens wear, measured using Diaton tonometer. Error bars represent the 95% confidence intervals of each time.
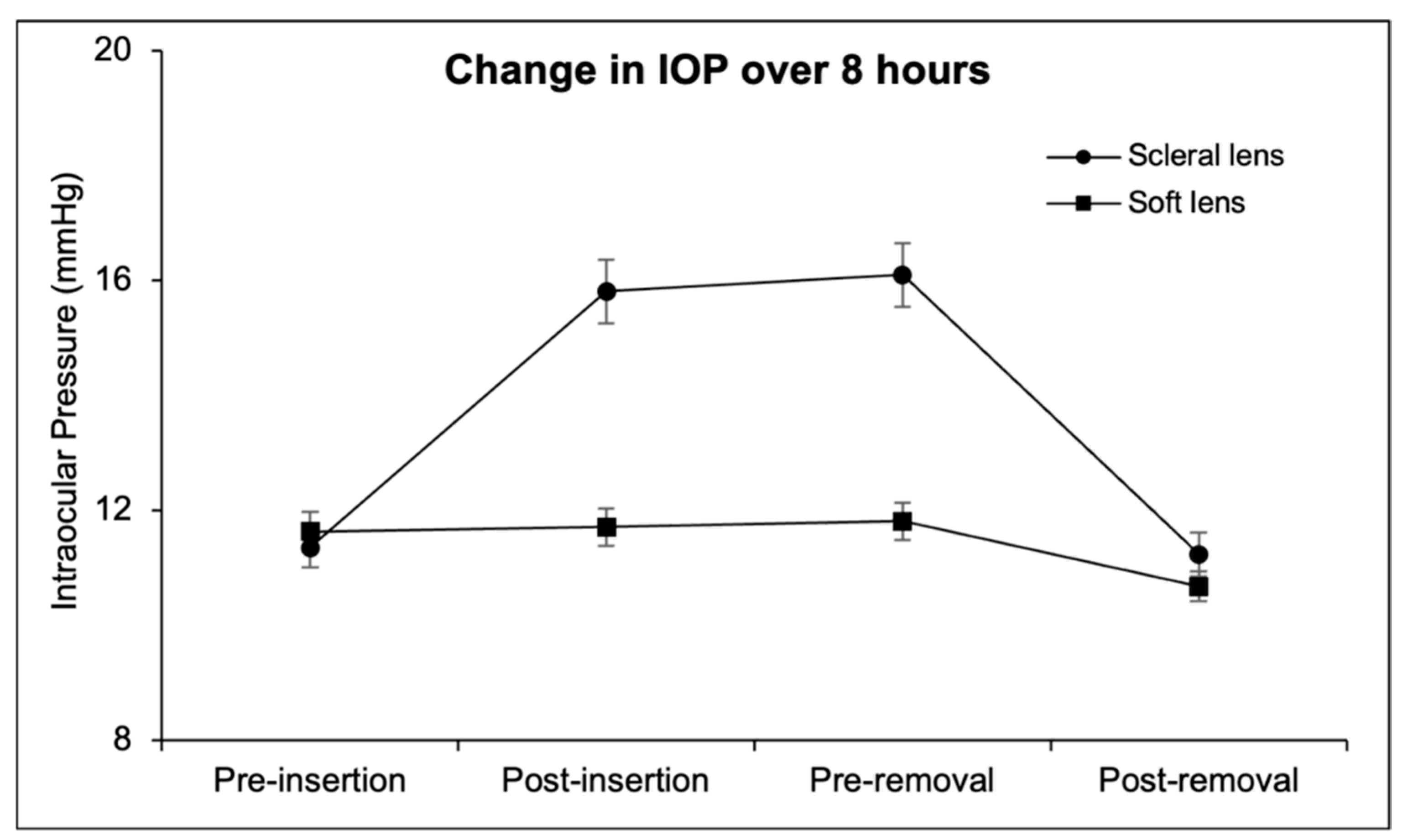
Figure 3.
Mean RNFL [average (A), peripapillary (B), superior (C) and inferior (D)] and changes during 8 hours of soft and scleral lens wear. Error bars represent the 95% confidence intervals of each time.
Figure 3.
Mean RNFL [average (A), peripapillary (B), superior (C) and inferior (D)] and changes during 8 hours of soft and scleral lens wear. Error bars represent the 95% confidence intervals of each time.
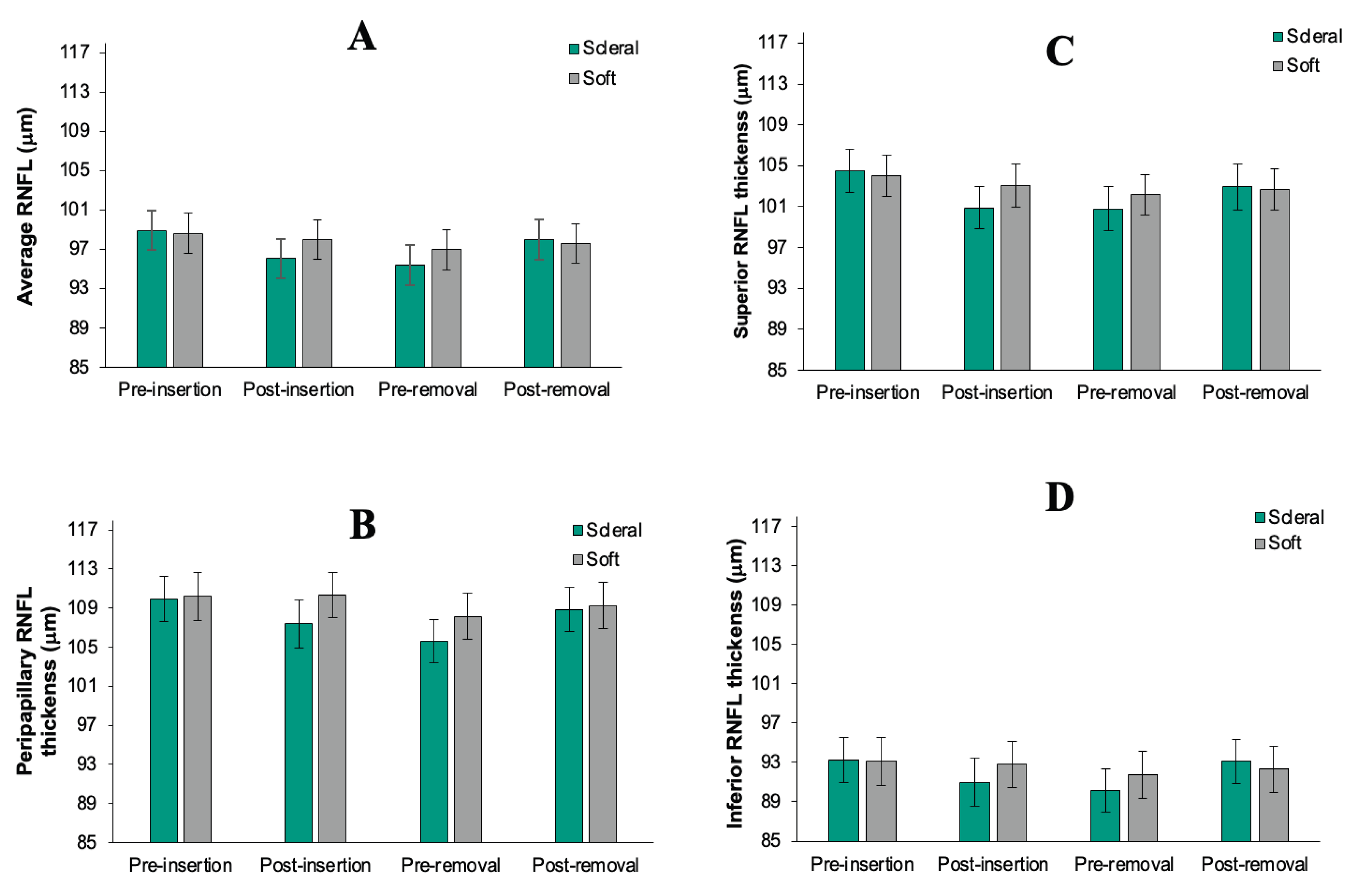
Table 2.
Demographics and clinical characteristics of Participants.
| N (%) | Mean ± SD | Range | |
|---|---|---|---|
| Age(years) | 26 ± 3 | 20 - 31 | |
| Sex, male/female: n (%) | 20/11 (64.5%/35.5%) |
||
| Race: n (%) | |||
| · White | 18 (58.1%) | ||
| · Asian | 3 (9.7%) | ||
| · Asian/Indian | 3 (9.7%) | ||
| · Other | 7 (22.6%) | ||
| Refractive error (Spherical equivalent) (D) | -3.25 ± 3.25 | -9.25-+0.50 | |
| Average corneal curvature (D) | 43 ± 2.25 | 40.25 - 46.5 | |
| Baseline IOP (mmHg) | 14.3 ± 3 | 8 - 20 | |
| Pulse (BPM) | 72 ± 13 | 46 - 97 | |
| Systolic BP (mmHg) | 105 ± 13 | 84 - 140 | |
| Diastolic BP (mmHg) | 62 ± 8 | 43 - 86 | |
| OPP (mmHg) | 38 ± 7 | 18 - 63 |
Table 3.
ANOVA summary table for IOP showing both main effects and interactions.
| Source | Numerator df | Denominator df | F | Sig. |
|---|---|---|---|---|
| Intercept | 1 | 30.933 | 1826.294 | <.001 |
| Eye | 1 | 685.211 | 0.4 | 0.527 |
| LensType | 1 | 685.211 | 102.13 | <.001 |
| Conditions | 3 | 685.545 | 13.34 | <.001 |
| Eye * LensType | 1 | 685.211 | 0.06 | 0.806 |
| Eye * Conditions | 3 | 685.211 | 0.915 | 0.433 |
| LensType * Conditions a Dependent Variable: IOP. |
3 | 685.211 | 31.741 | <.001 |
Table 4.
ANOVA summary table for RNFL showing both main effects and interactions.
| Source | Numerator df | Denominator df | F | Sig. |
|---|---|---|---|---|
| Intercept | 1 | 30.023 | 4891.669 | <.001 |
| Eye | 1 | 701 | 3.738 | 0.054 |
| LensType | 1 | 701 | 17.925 | <.001 |
| Conditions | 3 | 701 | 47.057 | <.001 |
| Eye * LensType | 1 | 701 | 0.172 | 0.678 |
| Eye * Conditions | 3 | 701 | 2.62 | 0.052 |
| LensType * Conditions | 3 | 701 | 13.552 | <.001 |
a Dependent Variable: average RNFL.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



