
Submitted:
19 February 2026
Posted:
24 February 2026
You are already at the latest version
Abstract
Background/Objectives: Peristomal skin complications are common among individuals with a stoma and are associated with decreased quality of life, increased healthcare costs, social isolation, and various other challenges. However, these complications can often be prevented through appropriate care, patient education, counseling, and follow-up. This quasi-experimental study aimed to evaluate the effectiveness of education based on Orem’s Self-Care Deficit Nursing Theory (SCDNT) in preventing peristomal skin complications. Methods: The study sample included 45 patients with newly formed stomas, divided into an experimental group (n=24) and a control group (n=21). Data were collected using the Patient Characteristics Form, Self-Care Agency Scale (SCAS), Stoma Quality of Life Scale (SQOL), Patient Outcomes Evaluation Form, and Patient Opinions Questionnaire. The experimental group received education and counseling structured according to the components of SCDNT. Patient care, education, and follow-up were carried out in alignment with this framework. Results: Among the participants, 73.3% had undergone stoma surgery due to cancer, and 53.3% had an ileostomy. Peristomal skin complications were observed in 54.2% of patients in the experimental group and 95.2% in the control group (p<0.05). The most frequently reported complications were irritant dermatitis (71.4%) and hyperplasia (22.7%). The average complication recovery time was significantly shorter in the experimental group (21 ± 12.95 days) compared to the control group (44.65 ± 23.56 days) (p<0.05). Conclusions: Education, counseling, and follow-up based on SCDNT were effective in reducing both the incidence and duration of peristomal skin complications and enhancing patient engagement in self-care.
Keywords:
peristomal skin complications
; Self‐Care Deficit Nursing Theory
; patient education
; nursing care
; tele‐nursing
1. Introduction
Stoma formation is a common surgical procedure that helps manage fecal or urinary diversion, often due to conditions like colorectal cancer, inflammatory diseases, or trauma. While stomas can be life-saving and play a crucial role in maintaining essential bodily functions, they often come with a host of complications that can significantly impact a patient's quality of life. Some of the typical issues include excessive gas, unpleasant odors, leakage, irritation of the skin around the stoma, indigestion, loss of appetite, nausea, diarrhea, constipation, and pain. These physical challenges can lead to psychological distress and social difficulties, such as anxiety, lowered self-esteem, and feelings of isolation [1,2,3,4,5].
The literature shows varying frequencies of stomal and peristomal skin complications [1,4,5]. Even with advancements in surgical techniques, medical technology, and the design of ostomy products, these complications still occur at a notable rate, with peristomal skin irritation being the most commonly reported issue. In Türkiye, research on this subject is somewhat limited. However, Karadağ [6] retrospectively analyzed 128 patients with stomas who were regularly monitored in a stomatherapy unit and found a complication rate of 32.8%, with peristomal skin irritation making up 17.9% of those cases. Other national studies [2,7,8,9] have reported rates of peristomal complications ranging from 5.8% to 48.7%.
It's important to note that nearly all patients with a stoma will likely face complications at some point. Numerous studies [5,9,10,11,12] have consistently indicated that peristomal skin complications are the most prevalent. Educating patients has emerged as a vital strategy for preventing these issues. Evidence suggests that providing education during the preoperative or postoperative phases can shorten hospital stays, reduce the likelihood of rehospitalization, lower healthcare costs, and ultimately improve patients' quality of life [11,13,14]. These strategies have also been shown to decrease anxiety and increase patient compliance regarding stoma care [11,12,13].
Nurses play a vital role in the prevention and management of stoma-related complications. As members of a professional discipline dedicated to promoting health and providing holistic care, it is essential that nurses base their interventions on theoretical frameworks. Nursing theories offer structured guidance for clinical practice, enhance decision-making, and ensure consistency in care delivery. One such model is the Self-Care Deficit Nursing Theory (SCDNT), developed by Dorothea Orem. Originally introduced in 1956 as the Self-Care Theory and later expanded into SCDNT between 1971 and 2001, the theory emphasizes the importance of supporting individuals who are unable to meet their self-care needs. Orem posits that individuals can develop the necessary intellectual and practical skills to manage their own care if properly motivated and educated [15].
The principles of SCDNT align closely with the needs of individuals living with a stoma. During periods when patients experience self-care deficits, particularly in the early postoperative phase, support from nurses is critical. As patients adapt and gain confidence, they gradually assume responsibility for their own care [15]. Educational interventions informed by Orem’s theory may thus facilitate the transition from dependence to independence, contributing to continuity of care and improved outcomes in individuals with stomas.
Aims and Research Questions
This quasi-experimental study aimed to evaluate the effectiveness of education based on the SCDNT in preventing peristomal skin complications among patients with newly created stomas.
The research questions were as follows;
- Is the training provided in accordance with the SCDNT effective in reducing peristomal skin complications?
- Is the training provided in accordance with the SCDNT effective in reducing healing time of developing peristomal skin complications?
- Is training provided in accordance with SCDNT effective in increasing patients' level of participation in stoma care?
2. Materials and Methods
2.1. Research Design
This quasi-experimental study was conducted in the General Surgery Clinic and Stomatherapy Unit of a University Health Research and Application Center, where approximately 100 stoma surgeries are performed annually. The study was carried out over 8 months.
2.2. Sample and Power Analysis
The study population included all patients with a newly created stoma treated at the center during the study period. A total of 45 patients (experimental= 24, control= 21) meeting the inclusion criteria formed the study sample. Inclusion criteria were: being over 18 years old, having a newly created stoma, ability to read and write in Turkish, access to the internet, no physical or psychiatric condition preventing self-care, and voluntary participation. Power analysis using PASS 2023 indicated that a minimum of 42 participants (21 per group) were needed to achieve 80% power at α=0.05 with a moderate effect size (0.5). A total of 69 patients were assessed, but 24 were excluded due to refusal to participate (n=5), dropout (n=4), lack of internet (n=5), illiteracy (n=4), or clinical deterioration (n=6).
2.3. Group Assignment
Participants were assigned to either the experimental or control group in alternating two-week periods to prevent contamination. Randomization was not feasible due to the study's clinical conditions.
2.4. Ethical Considerations
Ethical approval was obtained from the hospital (13.02.2017–E-22427) and Ethics Committee (21.04.2017–E.59760). Written informed consent was obtained from all participants.
2.5. Data Collection Tools
The following instruments were used: Patient Characteristics Form (PCF), Self-Care Agency Scale (SCAS) [16], Stoma Quality of Life Scale (SQOL) [17], Peristomal Skin Complications Management Training Booklet (PSCMTB), Patient Outcomes Evaluation Form (POEF), and Patient Opinions Questionnaire (POQ). Patients also submitted peristomal photographs taken with mobile devices throughout follow-up. The content validity of researcher-developed tools (PCF, PSCMTB, POEF, POQ) was assessed by 11 experts, yielding a content validity index of 1.0.
2.5.1. Patient Characteristics Form (PCF)
The PCF comprises 33 items across two sections: sociodemographic data (13 items, e.g., age, sex, education, comorbidities) and stoma-related information (20 items, e.g., diagnosis, surgery type, stoma site marking, early complications).
2.5.2. Self-Care Agency Scale (SCAS)
Originally developed by Kearney and Fleischer (1979) and adapted by Nahcivan (1994) for Turkish populations, the SCAS contains 35 items measuring self-care ability. Responses range from 0 (“does not define me at all”) to 4 (“defines me a lot”), with reverse scoring applied to eight (3, 6, 9, 13, 19, 22, 26 and 31) negatively worded items. The scale’s Cronbach’s alpha reliability coefficient is 0.92 [16].
2.5.3. Stoma Quality of Life Scale (SQOL)
Developed by Baxter et al. [18] and validated in Turkey by Karadağ et al. [17], the SQOL has 21 items divided into four subdimensions: work/social life, sexuality/body image, stoma function, plus two standalone items assessing overall life satisfaction and economic status. Items use a 5-point Likert scale, and subdimensions are scored from 0 to 100, with higher scores indicating better quality of life.
2.5.4. Peristomal Skin Complications Management Training Booklet (PSCMTB)
The PSCMTB, developed based on relevant literatüre [4,9,10,19], addresses eight common peristomal skin complications with sample images, symptom descriptions, care interventions, and prevention guidelines. The booklet is divided into three parts: assessment algorithms (Figure 1, Figure 2.) for peristomal skin, routine stoma care instructions, and management strategies for complications. It also includes guidance on photography techniques, photo submission schedules, and researcher contact details (Figure 3).
2.5.5. Patient Outcomes Evaluation Form (POEF)
This nine-item form records data collected during the three-month follow-up, including caregiver involvement, patient participation in stoma care, patient's goals of participation in care, presence of complications, counseling provided, care recommendations, hospitalizations, and recovery status.
2.5.6. Patient Opinions Questionnaire (POQ)
Designed to evaluate patient feedback on the PSCMTB, the POQ uses an 11-item, 5-point Likert scale (1 = strongly disagree to 5 = strongly agree) assessing the booklet’s clarity, content adequacy, visual appropriateness, usability, and its role in promoting patient engagement. It also contains an open-ended question for additional comments.
2.6. Implementation
Preoperative stoma education and site marking were provided by a stomatherapy nurse using a standardized booklet. After surgery, patients were informed about the study and initial assessments (PCF, SCAS) were completed. Patients received care according to group assignment: SCDNT-based care for the experimental group, routine hospital care for the control group. All participants were trained in stoma self-care and discharged with educational materials.
According to the literature [1,2,5,8], early complications occur within the first month, and late complications typically appear 6–10 weeks after surgery. Therefore, a 3-month (90-day) follow-up period was selected to observe both early and late peristomal skin complications in patients with permanent and temporary stomas.
2.6.1. Experimental Group Protocol
In addition to standard care, experimental group patients received PSCMTB-based education aligned with SCDNT framework. SCAS and SQOL were administered pre- and post-intervention. Patients submitted photographs of the peristomal area weekly during the first month, biweekly in the second month, and monthly in the third month. Remote support and follow-up were provided via the booklet and telephone. Interventions focused on correcting incorrect care, promoting self-care behavior, setting progressive goals, and providing support through the stomatherapy unit when needed. After 90 days, SCAS, SQOL, and POQ were re-administered.
2.6.2. Control Group Protocol
Control group patients received standard care and education and completed the same pre- and post-discharge assessments (PCF, SCAS, SQOL). They followed the same photo submission schedule and were evaluated similarly via POEF. Care support was limited to routine follow-up and consultation when needed.
2.6.3. Pilot Study
A preliminary implementation was conducted with 10 patients (5 per group). As no issues were encountered, these participants were included in the main study.
2.6.4. Data Collection Standardization
A structured "Interview Steps Checklist for the Researcher" was used throughout the study to ensure consistency across both groups.
2.7. Statistical Analysis
All data were analyzed using SPSS for Windows, version 22.0. Descriptive statistics (mean, standard deviation, frequency, and percentage) were used to summarize patient characteristics and outcome measures. A significance level of p<0.05 was considered statistically significant.
To examine associations between categorical variables and complication development, Fisher’s exact test, likelihood ratio test, or Pearson’s chi-square test were applied as appropriate. Changes in patient participation in care over time were assessed using Fisher’s exact test, Pearson’s chi-square test, and Cochran’s Q test.
The Mann–Whitney U test was used to compare SCAS and SQOL scores between groups, as data were non-normally distributed and group sizes were less than 30 (experimental = 24, control = 21). Within-group comparisons were conducted using the Wilcoxon signed-rank test due to non-normal distribution and repeated measurements.
3. Results
There were no statistically significant differences between the experimental and control groups in terms of sociodemographic or stoma-related characteristics (p>0.05), indicating group homogeneity. Most stomas were created due to colorectal cancer, and nearly all patients underwent planned surgery. Stoma site marking was performed preoperatively in 75% of the experimental group and 71.4% of the control group. More than half had temporary stomas, and ileostomy was the most common type (Table 1, Table 2).
Within the first 24 hours postoperatively, 15.6% of patients developed complications, predominantly irritant contact dermatitis (71.4%). By the end of the three-month follow-up, complications were observed in 54.2% of the experimental group and 95.2% of the control group (p<0.05). Statistically significant differences in complication rates between groups were found at the 2nd, 3rd, and 4th follow-ups, with fewer complications in the experimental group (p<0.05). No new complications were observed in the experimental group by the 4th follow-up.
Variables such as stoma type, output level, and stoma positioning showed significance in specific follow-ups. More complications occurred in patients with ileostomy (2nd follow-up), excessive output (4th follow-up), and stomas at or below skin level (1st follow-up) (p<0.05). The most common complication was irritant contact dermatitis (71.4%), followed by hyperplasia (22.7%) (Table 3).

Table 3.
Distribution of Peristomal Skin Complications During The Follow-Up Period (n=45*).
| Complication | 1. Monitoring (15th day) |
2. Monitoring (1st month) |
3. Monitoring (2nd month) |
4. Monitoring (3rd month) | GENERAL | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Experiment | Control | Total | Experiment | Control | Total | Experiment | Control | Total | Experiment | Control | Total | Experiment n (%) |
Control n (%) |
Total n (%) |
|
| Allergic Contact Dermatitis | 1 | - | 1 | - | 1 | 1 | - | 2 | 2 | - | - | - | 1 (3.23) |
3 (3.40) |
4 (3.36) |
| Irritant Contact Dermatitis | 7 | 16 | 23 | 15 | 25 | 40 | 5 | 14 | 19 | 3 | 3 | 27 (87.09) |
58 (65.90) |
85 (71.42) |
|
| Peristomal Trauma | - | - | - | - | - | - | - | 1 | 1 | - | - | - | - | 1 (1.14) |
1 (0.84) |
| Hyperplasia | 2 | 2 | 4 | - | 5 | 5 | 1 | 15 | 16 | - | 4 | 4 | 3 (9.68) |
24 (27.28) |
27 (22.68) |
| Uric Acid Crystals | - | - | - | - | 1 | 1 | - | 1 | 1 | - | 2 (2.28) |
2 (1.68) |
|||
| Total | 1 | 2 | 3 | 1 | 5 | 6 | 8 | 11 | 19 | 7 | 15 | 22 | 31 (100.0) |
88 (100.0) | 119 (100.0) |
* n folded. The average complication recovery time was significantly shorter in the experimental group (21±12.95 days) than in the control group (44.65±23.56 days) (p<0.05) (Table 4, Figure 4). These results support the hypotheses that SCDNT-based training reduces both the incidence and recovery time of peristomal skin complications.
Figure 4.
Histogram of recovery times associated with peristomal skin complications.
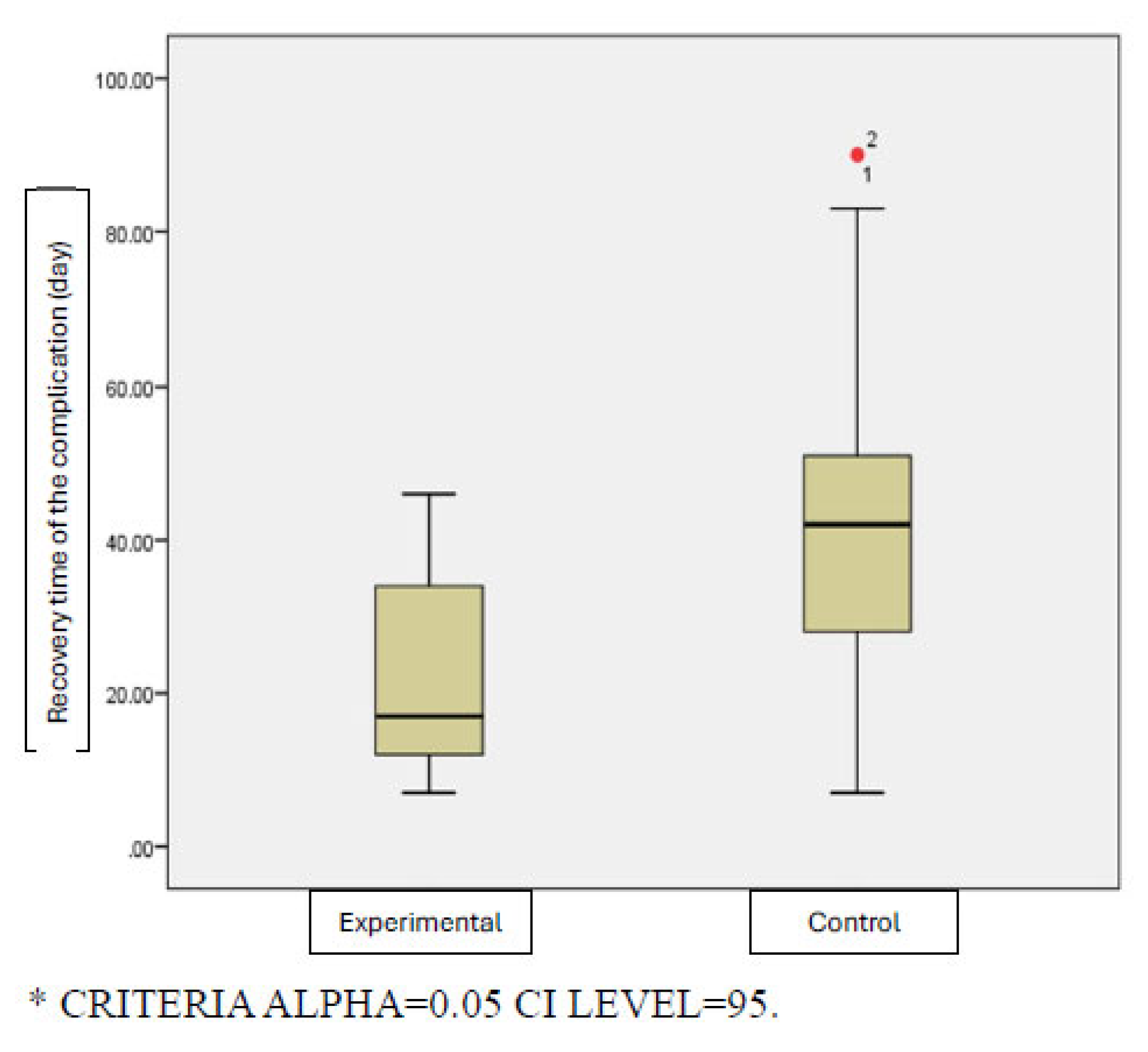
Table 4.
Healing Time of Peristomal Skin Complications (days).
| Group | Average | Std. Deviation | Minimum | Maximum | p |
|---|---|---|---|---|---|
| Experiment | 21.00 | 12.95505 | 7.00 | 46.00 | 0.002* |
| Control | 44.65 | 23.56240 | 7.00 | 90.00 |
*Mann-Whitney U Test was used.
At the 1st follow-up, significantly more patients in the experimental group participated in stoma care (p<0.05). Participation increased over time in both groups (p<0.05), with earlier improvement in the experimental group. By the 4th follow-up, 33.3% of the experimental group and 19.0% of the control group could independently manage care, though this difference was not significant (p>0.05).
The control group received more counseling overall, mostly by phone, and experienced a sharp increase in complications at the 2nd follow-up—likely due to transitioning to home care. The most frequent advice given was to properly size the appliance and protect exposed skin. The control group also had more hospital admissions due to complications. These findings partially support the hypothesis that SCDNT-based training increases self-care participation.
No significant differences were found in pretest–posttest SCAS or SQOL scores between the groups (p>0.05). Improvements in SQOL subdimensions were also not significant, except for work/social life (all patients) and sexuality (control group) (p<0.05). These findings do not support the hypotheses that SCDNT-based training improves self-care agency or quality of life scores.
Most patients found the booklet (PSCMTB) beneficial for self-care, informative, easy to understand, and useful in managing skin issues. They reported that it helped reduce hospital admissions and was easy to use. Common responses included: “It was very useful” (70.8%), “I think it is necessary” (79.2%), and “It was nice to have someone to consult.”
4. Discussion
The findings of this study demonstrate that education and counseling based on SCDNT significantly reduced the incidence and recovery time of peristomal skin complications and promoted earlier and more active patient engagement in self-care. The complication rate in the experimental group was significantly lower compared to the control group, especially after discharge. These outcomes align with previous literature, which highlights the importance of structured patient education in reducing postoperative complications and improving care outcomes [2,8,14].
In this study, 15.6% of patients developed early complications within the first 24 hours postoperatively, with irritant contact dermatitis being the most common diagnosis—consistent with earlier reports [1,7,8,13]. During the 3-month follow-up, the cumulative complication rate was significantly lower in the experimental group than in the control group. Notably, no new complications were observed in the experimental group at the final follow-up, underscoring the effectiveness of the SCDNT-guided intervention.
The most prevalent complications—irritant contact dermatitis (71.4%) and hyperplasia (22.6%)—mirror those reported in prior studies [1,4,9]. The observed increase in complications during the immediate post-discharge period (second follow-up) likely reflects the transition from supervised hospital care to independent home care. However, this trend was less pronounced in the experimental group, likely due to continued structured follow-up and guidance based on the PSCMTB. This supports previous findings that highlight the importance of continuity of care and targeted education in the early postoperative period [4,5,13].
Importantly, the mean recovery time for complications was significantly shorter in the experimental group (21±12.95 days) compared to the control group (44.65±23.56 days). Although literature lacks robust data on recovery duration, this finding suggests that theory-based education can accelerate healing through timely identification and appropriate management of complications.
Another important finding was the increased and earlier participation in stoma care observed in the experimental group. Previous studies have shown that early patient involvement in self-care leads to improved confidence, reduced dependency, and better overall adjustment [5,11,20]. The educational approach used in this study emphasized collaborative goal setting, motivational interviewing, and reinforcement—all of which have been identified as effective strategies in promoting self-care among patients with chronic health conditions (de la Quintana Jiménez et al., 2020; Ko et al., 2023).
Regarding self-care engagement, patients in the experimental group began participating in stoma care earlier and more consistently. While both groups showed increased participation over time, the experimental group demonstrated a statistically significant earlier transition to independent care. This aligns with the conceptual framework of SCDNT, which emphasizes guided support during periods of self-care deficit and gradual restoration of autonomy [15]. Previous studies have shown that enhanced education improves care participation and adaptation [14,20]. In addition, Ko et al. [14] reported that multimedia training given to patients with stoma significantly increased patients' self-care skills and QoL scores. Encouraging and supporting patients to participate in care is very effective in increasing adaptation [20].
Although improvements in SCAS and overall SQOL scores were observed, these changes were not statistically significant. However, subdimension analysis of the SQOL revealed significant improvements in the work/social life domain across both groups, and in sexuality/body image for the control group. The absence of significant improvement in the experimental group may reflect heightened awareness of potential complications resulting from increased education, as well as ongoing psychosocial distress related to cancer diagnoses and adjuvant therapies. Similar to prior findings [1,11,19], patients experienced multifaceted challenges—physical, psychological, and social—that may have negatively affected QoL outcomes despite reduced complication rates. These observations support the notion that a longer follow-up period may be necessary to capture the full benefits of educational interventions on self-care capacity and QoL. It is also possible that ongoing cancer treatments and psychological distress related to stoma adjustment diminished the impact of the educational intervention on broader QoL indicators.
Nevertheless, patient feedback on the PSCMT booklet was overwhelmingly positive. The majority found it useful, easy to understand, and supportive in daily self-care, suggesting that theory-based, structured educational materials can enhance patient experience and promote engagement. The booklet's emphasis on self-care goals, complication recognition, and problem-solving likely contributed to reduced hospital admissions and complication severity. Educational materials developed using a theoretical framework and tailored to patient needs have been found to enhance knowledge retention and improve care behaviors [11,14,20].
In summary, this study demonstrates that incorporating nursing theory into patient education—specifically SCDNT—can lead to meaningful improvements in clinical outcomes and care participation among individuals with new stomas. While long-term psychosocial adaptation remains a challenge, especially in oncology populations, early structured support appears essential to promote effective self-care and reduce complications.
4.1. Research Limitations
Although initially planned as a randomized controlled trial, the study was conducted as a quasi-experimental design due to group imbalances and attrition in the control group. Additionally, while patients were instructed to send peristomal photos based on a fixed schedule, many chose to send photos during appliance changes to receive immediate expert feedback. This increased interaction, particularly in the experimental group, may have influenced outcomes. Continuous reminders were required to ensure the use of the educational booklet (PSCMTB), and some participants relied more on direct support than self-guided resources.
Despite these challenges, the study's strength lies in its three-month follow-up and its novel application of the Self-Care Deficit Nursing Theory (SCDNT) in a relatively large stoma patient population.
5. Conclusions
This study provides evidence that SCDNT-based education and counseling reduce the incidence of peristomal skin complications, shorten the recovery time of complications, promote patient participation in stoma care, and decrease the need for additional counseling and hospital admissions related to complications. However, the intervention did not significantly improve self-care agency or quality of life scores within the three-month period.
Patients with newly created stomas should be closely monitored in the early postoperative period to enable timely detection and management of complications. The PSCMTB should be adopted as a standard educational tool to ensure consistent, evidence-based stoma care. Structured education and counseling on complication management can enhance patients’ knowledge, confidence, and self-care abilities. Healthcare professionals should actively promote patient participation in stoma management, guided by frameworks such as the SCDNT. Further randomized controlled trials with larger samples and longer follow-up are needed to confirm and extend these findings, ultimately improving clinical outcomes and quality of life for individuals with stomas.
Author Contributions
Conceptualization, A.A. and H.B.; methodology, A.A. and H.B.; investigation, A.A.; formal analysis, A.A. and H.B.; data curation, A.A..; writing—original draft preparation, A.A.; writing—review and editing, H.B..; visualization, A.A..; validation, A.A. and H.B.; supervision, H.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of GAZI UNIVERSITY (21.04.2017-E.59760).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to (The institution where the study was conducted does not permit the sharing of records with other individuals, institutions, or organizations).
Acknowledgments
Authors are grateful to all the participants who voluntarily offered their time, conscientiously provided honest and thoughtful responses. “During the preparation of this manuscript/study, the author(s) used [SPSS for Windows, version 22.0] for the purposes of [statistical analysis]. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Public Involvement Statement
Patients were informed about the study, and their consent was obtained. It was explained that participation was voluntary and that they could withdraw from the study at any time without providing a reason. They were assured that the collected information would remain confidential and would not be used for any other purpose. Following this information, written informed consent was obtained from the patients who agreed to participate. All stages of the study were completed in accordance with the principles of the Declaration of Helsinki.
Guidelines and Standards Statement
No reporting guideline were used when drafting the report.
Use of Artificial Intelligence
AI or AI-assisted tools were used in the preparation of the manuscript for language translation, language editing and grammar.
Abbreviations
The following abbreviations are used in this manuscript:
| SCDNT | Self-Care Deficit Nursing Theory |
| SCAS | Self-Care Agency Scale |
| SQOL | Stoma Quality of Life Scale |
| PCF | Patient Characteristics Form |
| PSCMTB | Peristomal Skin Complications Management Training Booklet |
| POEF | Patient Outcomes Evaluation Form |
| POQ | Patient Opinions Questionnaire |
References
- D’Ambrosio, F; Pappalardo, C; Scardigno, A; Maida, A; Ricciardi, R; Calabrò, GE. Peristomal Skin Complications in Ileostomy and Colostomy Patients: What We Need to Know from a Public Health Perspective. Int J Environ Res Public Health 2023, 20. [Google Scholar] [CrossRef] [PubMed]
- Ay, A; Bulut, H. Assessing the Validity and Reliability of the Peristomal Skin Lesion Assessment Instrument Adapted for Use in Turkey. Ostomy Wound Manag 2015, 61, 26–34. [Google Scholar]
- Guerra, E; Denti, FC; Di Pasquale, C; Caroppo, F; Angileri, L; Cioni, M; et al. Peristomal Skin Complications: Detailed Analysis of a Web-Based Survey and Predictive Risk Factors. Healthc 2023, 11, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Karadağ, A. Peristomal Cilt Komplikasyonları: Tanılama, Önleme, Tedavi The Peristomal Skin Complications: Diagnosis, Prevention, Treatment. In Hacettepe Üniversitesi Hemşirelik Fakültesi Derg; 2016; p. 3. [Google Scholar]
- Salvadalena, G; Colwell, JC; Skountrianos, G; Pittman, J. Lessons Learned about Peristomal Skin Complications: Secondary Analysis of the ADVOCATE Trial. J Wound, Ostomy Cont Nurs 2020, 47, 357–63. [Google Scholar] [CrossRef] [PubMed]
- Karadag, A. Frequency of stomal complications. World Counc Enteros Ther J 2004, 24, 41–3. [Google Scholar]
- Ayik, C; Özden, D; Cenan, D. Ostomy Complications, Risk Factors, and Applied Nursing Care: A Retrospective, Descriptive Study. Wound Manag Prev 2020, 66, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Ayik, C; Bişgin, T; Cenan, D; Manoğlu, B; Özden, D; Sökmen, S. Risk factors for early ostomy complications in emergency and elective colorectal surgery: A single-center retrospective cohort study. Scand J Surg 2024, 113, 50–9. [Google Scholar] [CrossRef] [PubMed]
- Harputlu, D; Özsoy, SA. A tool to diagnose of peristomal skin complication: ostomy skin tool [Stoma çevresi cilt komplikasyonlarının tanılanmasında bir araç : peristomal cilt aracı]. Florence Nightingale J Nurs 2016, 24, 38–48. [Google Scholar]
- Ceylan, H; Vural, F. Living with stoma - A phenomenological study. J Nurs Res Pract 2017, 1, 6–12. [Google Scholar]
- Doucette, JE; Mawn, BE; Beitz, JM; Koren, A. Factors Affecting Psychosocial Adjustment in Persons with a Recent Ostomy. J Wound, Ostomy Cont Nurs 2023, 50, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Vural, F; Harputlu, D; Karayurt, O; Suler, G; Edeer, AD; Ucer, C; et al. The impact of an ostomy on the sexual lives of persons with stomas. J Wound, Ostomy Cont Nurs 2016, 43, 381–4. [Google Scholar] [CrossRef] [PubMed]
- Kittscha, J; Fairbrother, G; Bliokas, V; Wilson, V. Adjustment to an Ostomy: An Integrative Literature Review. J Wound, Ostomy Cont Nurs 2022, 49, 439–48. [Google Scholar] [CrossRef] [PubMed]
- Ko, HF; Wu, MF; Lu, JZ. A randomized control study: The effectiveness of multimedia education on self-care and quality of life in patients with enterostomy. Int Wound J 2023, 20, 4244–52. [Google Scholar] [CrossRef] [PubMed]
- Smith, MC; Parker, ME. Nursing theories & nursing practice; 2015. [Google Scholar]
- Nahcivan, NÖ. Geçerlilik ve Güvenilirlik Çalışması: Öz-bakım Gücü Ölçeğinin Türkçe’ye Uyarlaması. Hemşirelik Bülteni 1994, 7, 109–19. [Google Scholar]
- Karadaǧ, A; Öztürk, D; Çelik, B. Ostomili Bireylere Yönelik Yaşam Kalitesi Ölçeğinin Türkçeye Uyarlanması. Kolon ve Rektum Hast Dergisi/Journal Dis Colon Rectum 2011, 21, 173–81. [Google Scholar]
- Baxter, NN; Novotny, PJ; Jacobson, T; Maidl, LJ; Sloan, J; Young-Fadok, TM. A stoma quality of life scale. Dis Colon Rectum 2006, 49, 205–12. [Google Scholar] [CrossRef] [PubMed]
- Collado-Boira, EJ; Machancoses, FH; Folch-Ayora, A; Salas-Medina, P; Bernat-Adell, MD; Bernalte-Martí, V; et al. Self-Care and Health-Related Quality of Life in Patients with Drainage Enterostomy: A Multicenter, Cross Sectional Study. Int J Environ Res Public Heal 2021, Vol 18 18, 2443 2021 2443. [Google Scholar] [CrossRef] [PubMed]
- Martín-Muñoz, B; Montesinos-Gálvez, AC; Crespillo-Díaz, AY; Jódar-Sánchez, F. Efficacy of a Social Interaction Intervention in Early Postoperative Period to Improve Coping in Persons with an Ostomy: A Randomized Controlled Trial. J Wound, Ostomy Cont Nurs 2022, 49, 352–7. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The first stage of determining the type of complication.
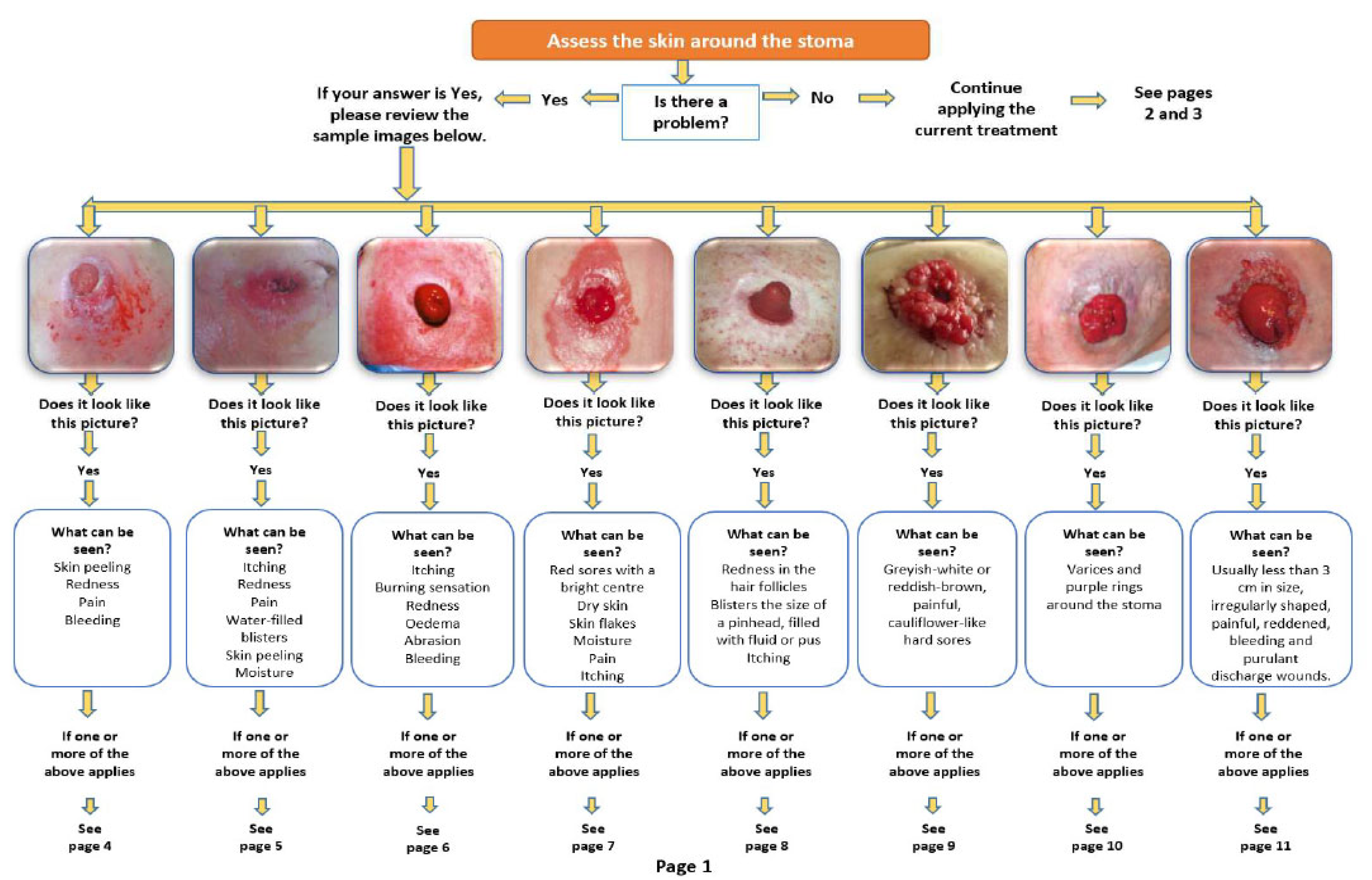
Figure 2.
Verification of the type of complication with different sample pictures and causes.
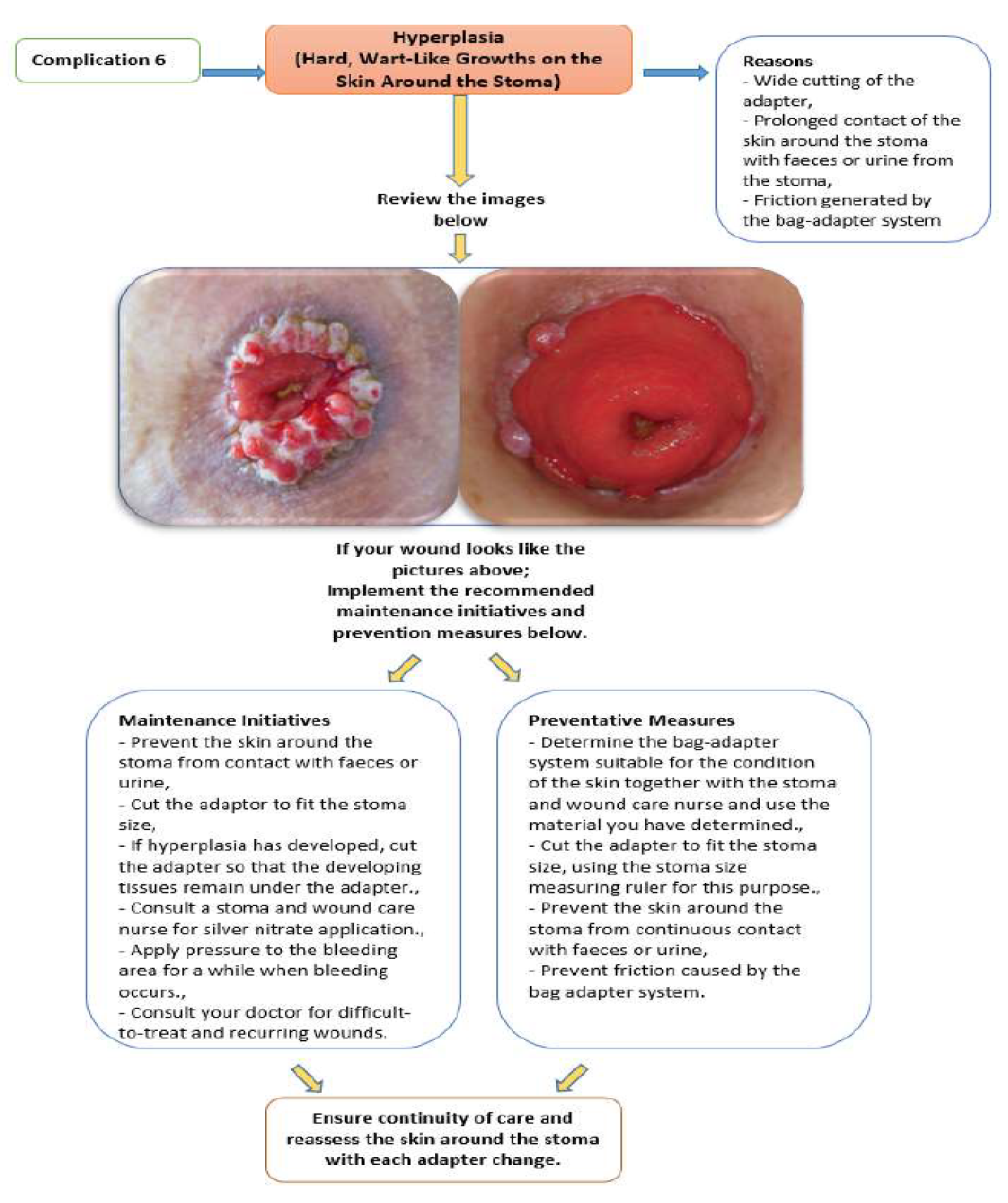
Figure 3.
Instructions for taking and sending photos.
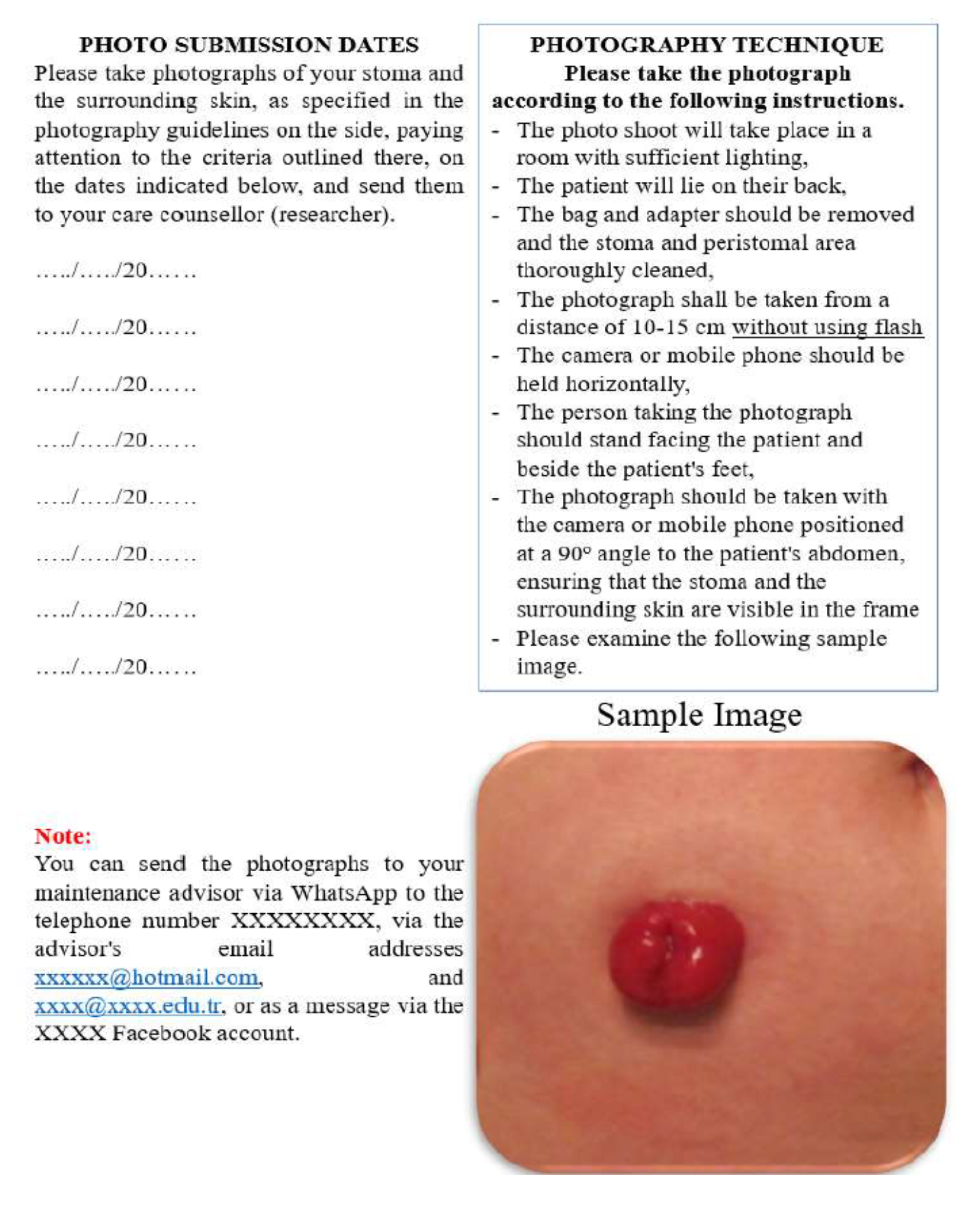
Table 1.
Sociodemographic Characteristics of The Patients (n=45).
| Experiment (n=24) n(%) |
Control (n=21) n(%) |
Statistical Analysis | |
|---|---|---|---|
| Age | |||
| X±SD(min-max) | 57.04±11.07(34-75) | 53.66±13.11(18-72) | U=213.000 p=0.374*** |
| Gender | |||
| Female | 12 (50.0) | 9 (42.9) | X2=0.632 |
| Male | 12 (50.0) | 12 (57.1) | p=0.767**** |
| Clinic | |||
| General Surgery | 18(75.0) | 19(90.5) | X2=0.176 |
| Urology | 6(25.0) | 2(9.5) | p=0.252**** |
| Chronic Disease | |||
| Yes | 10(41.7) | 9(42.9) | X2=0.936 |
| No | 14(58.3) | 12(57.1) | p=1.000**** |
| Receiving Additional Treatment (CT, RT, CAM) | |||
| Yes | 10 (41.7) | 14 (66.7) | X2=0.094 |
| No | 14 (58.3) | 7 (33.3) | p=0.136**** |
| Marital Status | |||
| Married | 22 (91.7) | 20 (95.2) | X2=0.632 |
| Single | 2 (8.3) | 1 (4.8) | p=1.000**** |
| Education Status | |||
| Primary school or below** | 14 (58.3) | 12 (57.1) | X2=0.926 |
| Middle School | 3 (12.5) | 2 (9.5) | |
| High school and above | 7 (29.2) | 7 (33.3) | |
| Job | |||
| Retired | 12 (50.0) | 8 (38.1) | X2=0.891 |
| Housewife | 10 (41.7) | 5 (23.8) | p=0.555**** |
| Officer | 2 (8.3) | 3 (14.3) | |
| Tradesmen | 0 (0.0) | 1 (4.8) | |
| Student | 0 (0.0) | 1 (4.8) | |
| Other *** | 0 (0.0) | 3 (14.3) | |
| Lifestyle | |||
| Active | 9 (37.5) | 10 (47.6) | X2=0.493 |
| Sedanter | 15 (62.5) | 11 (52.4) | |
| Social Life | |||
| Going out | 15 (62.5) | 9 (37.5) | X2=0.967 |
| Spending time at home | 13 (61.9) | 8 (38.1) | p=1.000**** |
| Place of Residence | |||
| City | 19 (79.2) | 15 (71.4) | X2=0.547 |
| District/ Town/ Village | 5 (20.8) | 6 (28.6) | p=0.730**** |
CT: Chemotherapy, RT: Radiotherapy, CAM: Complementary and Alternative Medicine. ** Primary school graduate or literate. *** Not working, Self-employed. *** Mann-Whitney U Test was used. **** Fisher's Exact Test was used.
Table 2.
Patients' Characteristics Related to The Stoma (n=45).
| Experiment (n=24) n(%) |
Control (n=21) n(%) |
Statistical Analysis | |
|---|---|---|---|
| Medical diagnosis | |||
| Cancer | 17 (70.8) | 16 (76.2) | X2=0.891 |
| Inflammatory Bowel Disease | 1 (4.2) | 1 (4.8) | |
| Other* | 6 (25.0) | 4 (19.0) | |
| Type of Surgery | |||
| Elective | 19 (79.2) | 20 (95.2) | X2=0.114 |
| Urgent | 5 (20.8) | 1 (4.8) | p=0.193** |
| Stoma Area Marking | |||
| Yes | 18 (75.0) | 15 (71.4) | X2=0.787 |
| No | 6 (25.0) | 6 (28.6) | p=0.1000** |
| Duration of the stoma | |||
| Permanent | 8 (33.3) | 5 (23.8) | X2=0.482 |
| Temporary | 16 (66.7) | 16 (76.2) | p=0.528** |
| Type of stoma | |||
| Colostomy | 8 (33.3) | 5 (23.8) | X2=0.205 |
| Ileostomy | 10 (41.7) | 14 (66.7) | |
| Urostomy | 6 (25.0) | 2 (9.5) | |
| Shape of the stoma | |||
| Round | 9 (37.5) | 11 (52.4) | X2=0.316 |
| Oval or shapeless | 14 (58.3) | 8 (38.1) | p=0.377** |
| Soma Height | |||
| Bud | 19 (79.2) | 13 (61.9) | X2=0.202 |
| Same level with the skin or retracted | 5 (20.8) | 8 (38.1) | p=0.323** |
| Output Type | |||
| Liquid | 22 (91.7) | 20 (95.2) | X2=0.632 |
| Solid | 2 (8.3) | 1 (4.8) | p=1.000** |
| Output Quantity | |||
| Too much (>2000ml/24h) | 0 (0.0) | 3 (14.3) | X2=0.109 |
| Normal(400-800ml/24h) | 23 (95.8) | 18 (85.7) | |
| Very little (<400ml/24h) | 1 (4.2) | 0 (0.0) | |
| Presence of folds in the peristomal area | |||
| Yes | 8 (33.3) | 8 (38.1) | X2=0.739 |
| No | 16 (66.7) | 13 (61.9) | p=0.765** |
| Bag-Adapter System Used | |||
| One-piece-flat adapter | 2 (8.3) | 0 (0.0) | X2=0.193 |
| Two-piece-flat adapter | 19 (79.2) | 15 (71.4) | |
| Two-piece convex adapter | 3 (12.5) | 6 (28.6) |
* Intestinal obstruction, Intestinal perforation, Mucocutaneous Fistula. **Fisher’s Exact Test was used.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



