
Submitted:
23 February 2026
Posted:
26 February 2026
You are already at the latest version
Abstract
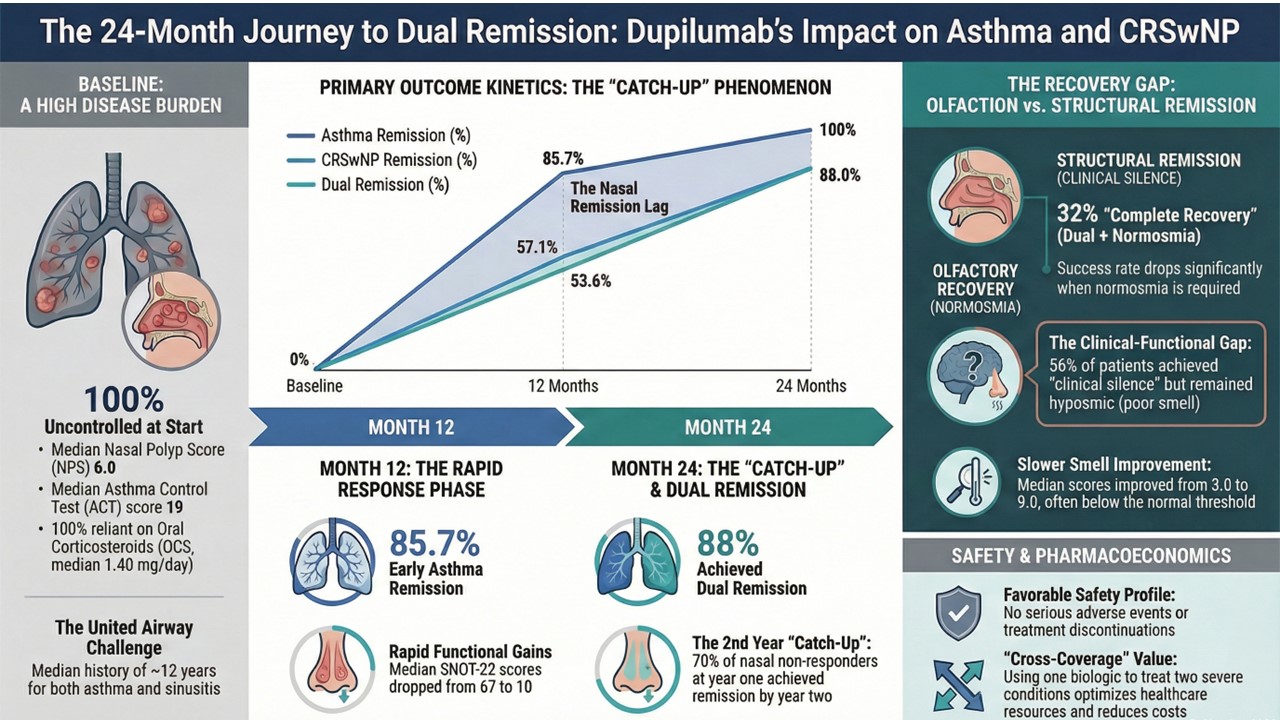
Background: "Remission" is a primary therapeutic goal in severe asthma and chronic rhinosinusitis with nasal polyps (CRSwNP), though definitions vary regarding olfactory function. We evaluated "Dual Remission" kinetics in patients treated with dupilumab over 24 months. Methods: This single-center retrospective study analyzed 28 patients with comorbid severe asthma and CRSwNP. Dual Remission was defined as simultaneous asthma remission (ACT ≥ 20, no exacerbations, no OCS) and CRSwNP remission (SNOT-22 < 40, NPS ≤ 1). We additionally analyzed "Complete Recovery" by applying a stricter composite definition requiring the restoration of normosmia (Sniffin’ Sticks score ≥ 12). Results: At baseline, patients exhibited uncontrolled disease (median ACT 19, NPS 6). Treatment led to rapid asthma remission (85.7% at 12 months, 100% at 24 months). CRSwNP remission was slower but progressive, rising from 57% at 12 months to 88% at 24 months, demonstrating a significant "catch-up" phenomenon. Consequently, Dual Remission rates increased from 54% to 88% by month 24. However, when requiring normosmia for "Complete Recovery," only 32% met the criteria, revealing that 56% achieved clinical silence yet remained hyposmic. Conclusion: Dupilumab is highly effective, enabling 88% of patients to achieve Dual Remission after 24 months. However, full olfactory restitution is distinct from structural polyp regression and harder to achieve, likely due to persistent neuroepithelial damage.
Keywords:
asthma
; chronic rhinosinusitis with nasal Polyps
; dupilumab
; dual remission
; real-world evidence
; type 2 inflammation
1. Introduction
Asthma and Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) are frequently comorbid conditions, linked by a shared pathogenic mechanism known as Type 2 (T2) inflammation [1]. This inflammatory pathway is driven by key cytokines, particularly interleukin-4 (IL-4), IL-13 and IL-5, which recruit eosinophils and drive tissue remodeling in both the upper and lower airways [1,2]. Dupilumab, a fully human monoclonal antibody, targets the IL-4 receptor alpha subunit (IL-4/13 R α), effectively blocking the signaling of both IL-4 and IL-13 [3].
In long-term clinical studies of dupilumab, approximately 11% of patients with CRSwNP and comorbid asthma achieved clinical remission of nasal polyposis after 12 months of treatment, rising to 31% at 24 months based on comprehensive remission definitions. In Type 2 asthma clinical trials (QUEST and TRAVERSE), around 37% of patients on dupilumab met asthma remission criteria at 12 months and ~43% at 24 months, significantly higher than multicomponent clinical placebo, demonstrating meaningful dual disease control with this biologic therapy [4,5].
While these clinical trials have demonstrated its efficacy in reducing exacerbations and polyp size individually, there is a scarcity of real-world data assessing simultaneous clinical remission, i.e., dual remission. This concept—reaching strict treat-to-target goals in both nose and lungs concurrently—represents a higher standard of care than merely controlling symptoms.
This study aims to fill this gap by evaluating the effectiveness of dupilumab on asthma and nasal polyps over a 24-month period in a retrospective monocentric cohort of comorbid severe Type 2 asthma and CRSwNP, specifically tracking the kinetics of this dual remission.
2. Materials and Methods
2.1. Study Design and Population
This single-center, observational, retrospective study was conducted at the Multidisciplinary Pulmonology and Otolaryngology Unit of the S. Valentino Hospital in Montebelluna (TV) in a real-life setting involving consecutive patients (>18 years old) suffering from moderate-to-severe asthma and CRSwNP. All patients were treated with dupilumab (initial dose of 600 mg followed by 300 mg every 2 weeks) as an add-on therapy. Inclusion criteria were a diagnosis of severe asthma according to GINA guidelines and concomitant CRSwNP eligible for biological treatment [6]. Data were collected at baseline (T0) and after 6 (T6), 12 (T12), and 24 (T24) months of treatment.
2.2. Clinical and Functional Assessment
At each visit, patients underwent a multidisciplinary assessment. Asthma control was evaluated using the Asthma Control Test (ACT) [7], number of exacerbations, and use of oral corticosteroids (OCS). Lung function was assessed by measuring Forced Expiratory Volume in 1 second (FEV1) according to ERS/ATS technical standards [8]. Nasal outcomes were evaluated using the Sino-Nasal Outcome Test-22 (SNOT-22) for Quality of Life [9] and the Nasal Polyp Score (NPS) via nasal endoscopy (scored 0–4 per nostril, total 0–8) [10,11]. Olfactory function was assessed using the Sniffin’ Sticks Identification test (SS-I), where a score < 12 indicates hyposmia/anosmia and ≥ 12 indicates normosmia. Type 2 inflammation biomarkers (blood eosinophils, total IgE, and FeNO) were also recorded.
2.3. Definition of Clinical Outcomes
The primary outcome was the achievement of “Dual Remission. “Asthma Remission was defined according to the Severe Asthma Network Italy (SANI) criteria as the simultaneous presence of: (1) no use of OCS, (2) no asthma exacerbations, and (3) an ACT score ≥ 20 [12]. CRSwNP Remission was defined according to EPOS/EUFOREA guidelines as: (1) an NPS ≤1 and (2) a SNOT-22 score < 40 [13]. Dual remission was defined as meeting the criteria for both asthma remission and CRSwNP remission simultaneously. To evaluate the full restoration of sensory function, we additionally calculated a composite endpoint termed “Complete Recovery” (Dual Remission + normosmia). This stricter definition required patients to meet all criteria for Dual Remission and additionally achieve normosmia, defined as a SS-I test score of ≥ 12 [14].
2.4. Statistical Analysis
Continuous variables are reported as medians and interquartile ranges (IQR) or means ± standard deviation, as appropriate. Categorical variables are reported as counts and percentages. Comparisons between time points were performed using the Wilcoxon signed-rank test for paired data. A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Baseline Patient Features
Twenty-eight patients (mean age 54.2 ± 12.8, 43% females) were enrolled and included in the baseline and 12-month analyses. At the 24-month follow-up, data were available for 25 patients; the difference in sample size (N=25) resulted solely from three patients having not yet reached the 24-month observation window at the time of data lock. No discontinuations due to adverse events or lack of efficacy were recorded during the study period. The median history of asthma was almost 12 years, and the median history of sinusitis was approximately 12.5 years. Analysis of the baseline asthma severity (Table 1) revealed that 8 patients (29%) were affected by severe asthma, characterized by high-dose Inhaled Corticosteroids (ICS) and Long-Acting Beta-Agonists (LABA) often combined with Long-Acting Muscarinic Antagonists (LAMA) or OCS dependence. The remaining 20 patients (71%) presented with moderate asthma, where the primary indication for biologic therapy was the uncontrolled severe CRSwNP burden. All patients had uncontrolled disease at inclusion, with a mean SNOT-22 score of 65.7 and a median NPS of 6.0. Asthma was poorly controlled (median ACT 19) and patients were reliant on OCS (median 1.40 mg/day).
3.2. Clinical Evolution
Treatment resulted in dramatic improvements across all clinical parameters over the 24-month period (Table 2, Figure 1). Asthma control improved strongly at 12 months (median ACT increasing from 19 to 25) and remained stable at 24 months. Sino-nasal symptoms ameliorated, with median SNOT-22 scores dropping from 67 at baseline to 10 at 12 months, and 5 at 24 months. Nasal polyps significantly reduced from a median NPS of 6.0 to 0.5 at 12 months and 0.0 at 24 months.
Graphs illustrate the rapid and sustained improvement in clinical parameters during dupilumab treatment. (A) Asthma Control Test (ACT) scores improved significantly by month 12 and remained stable at month 24. (B) Sino-Nasal Outcome Test-22 (SNOT-22) scores showed a dramatic reduction by month 12, maintained at month 24. (C) Nasal Polyp Score (NPS) demonstrated a progressive decline, with significant additional reduction observed between month 12 and month 24, indicating continued tissue remodeling. Data are presented as means/medians. Significant improvements (p<0.05) were observed for all parameters compared to baseline.
Assessment of olfactory function using the SS-I test revealed a marked recovery in olfactory capacity among treated patients. The median olfactory identification score increased significantly from a baseline value of 3.0 (IQR 3.0–3.0) to 7.0 (IQR 5.25–9.75) after 12 months of treatment (p < 0.001) (Table 2). This improvement proved to be stable and durable over time, with a median score reaching 9.0 (IQR 5.0–11.0) at the 24-month follow-up (p < 0.001 vs baseline). The comparison between the 12- and 24-month timepoints showed no statistically significant differences (p = 0.75), confirming the maintenance of the clinical benefit in the long term.
OCS usage dropped to 0 mg/day by month 12 and was maintained through month 24 (p<0.001) (Table 2). Notably, asthma metrics (ACT, FEV1) showed no significant difference between 12 and 24 months, indicating maximum benefit is reached early. In contrast, nasal polyps progressively shrank through follow-up (Figure 1), with NPS showing statistically significant reduction between month 12 and month 24 (p < 0.05).
3.3. Safety
No serious adverse events were recorded, and there were no discontinuations due to adverse events. Transient asymptomatic blood hypereosinophilia (≥1,500 cells/µL) was observed in 3 patients (11%) at 12 months and 1 patient (6%) at 24 months, with no high-grade hypereosinophilia (>3,000 cells/µL) (Table 3).
3.4. Dual Remission and Complete Recovery
Asthma remission was achieved rapidly and maintained at high rates: 85.7% (24/28) of patients achieved remission at 12 months, rising to 100% (25/25 of the remaining patients) by 24 months in the observed population. In contrast, CRSwNP remission showed a higher initial response rate than previously estimated, followed by continued improvement. At 12 months, 57% (16/28) of patients met the criteria for CRSwNP remission. This rate increased substantially to 88% (22/25) at 24 months, confirming that tissue remodeling continues well into the second year of therapy.
Consequently, the rate of “Dual Remission” (simultaneous achievement of both asthma and CRSwNP remission) rose from 54% (15/28) at year 1 to 88% (22/25) at year 2. Notably, 70% of patients who had not achieved CRSwNP remission at year 1 (due to residual polyp scores > 1) successfully achieved it by year 2 (Table 4 and Figure 2). When adding normosmia to the remission criteria, the rate of “Complete Recovery” was 32% (8/25), revealing that 56% of patients achieved clinical silence but remained hyposmic (not shown).
4. Discussion
This study confirms that dupilumab is a transformative therapy for patients with severe T2 respiratory comorbidities, capable of inducing a state of “clinical silence”. Our main findings showed that dual remission increased substantially from 53.6% at 12 months to 88.0% at 24 months (Figure 2). The most critical insight is the temporal dissociation between asthma and CRSwNP remission. While 100% of patients achieved asthma remission within the observed period, endoscopic normalization required a longer duration (Table 4). This “lag” suggests fundamental differences in tissue responsiveness: bronchial smooth muscle dysfunction resolves rapidly, whereas nasal polyps represent substantial tissue remodeling that requires a longer duration to regress. Clinical control often aligns with polyp regression in the majority of patients (57%) by year 1. However, the significant leap to 88% remission at year 2 validates the “catch-up” phenomenon.
Our cohort achieved substantially higher asthma remission rates (100% at 24 months) compared to the 37–43% reported in the QUEST and TRAVERSE trials [3,4]. This result must be interpreted in light of the specific composition of our population. As detailed in Table 1, 71% of our cohort suffered from mild-to-moderate asthma, while only 28.6% had severe asthma. This prevalence of mild-to-moderate asthma phenotypes, driven primarily by the severe CRSwNP indication, likely contributed to the high ceiling of asthma remission observed.
Achieving “remission” (no exacerbations, stable lung function) is inherently more attainable in mild-to-moderate disease once the upper airway trigger is controlled, compared to refractory severe asthma [15]. However, the fact that remission was achieved in the entire cohort, including the 8 patients with severe disease, underscores the biologic’s efficacy across the severity spectrum.
Furthermore, viewing our results through the lens of the VESTIGE trial reinforces the concept of “united airway remodeling.” In VESTIGE, clinical improvements in lung function were mechanistically linked to the reduction in airway mucus volume and inflammation (FeNO) [16]. Similarly, in our study, the eventual achievement of dual remission likely relies on the same IL-4/13 blockade reducing fluid extravasation and fibrin deposition in both the lungs and sinuses. The contrast we observed—rapid asthma control versus delayed polyp regression—mirrors the kinetic difference often seen between functional biomarkers and structural imaging endpoints. This reinforces the hypothesis that while “clinical control” (symptoms) can be achieved early, “structural remission” (tissue normalization) is a prolonged event that accrues well beyond the first year of therapy.
Our findings resonate with the real-life data presented by De Corso et al. in their consecutive multicentric analyses. In their 2022 study, De Corso et al. observed that while patient-reported outcomes (SNOT-22) improve dramatically and rapidly, the reduction of the polypoid burden (NPS) follows a more gradual slope [17]. Furthermore, in the large-scale DUPIREAL study, De Corso et al. reported that while 96.9% of patients were classified as moderate/excellent responders at 12 months, the achievement of full clinical remission requires sustained therapy [18]. Both our single-center data and their multicentric findings convergently support the conclusion that patient-reported “response” often precedes objective “remission,” and that dupilumab requires prolonged administration to fully reverse structural remodeling.
This dissociation is also evident in olfactory recovery. In our cohort, we observed a progressive restoration of smell, with median SS-I scores tripling from 3 at baseline to 9 at 24 months (p < 0.001). However, distinct from the structural improvement (NPS) which continued significantly into the second year, olfactory function stabilized after the first 12 months (p = 0.75 for T12 vs T24), suggesting that functional recovery may plateau earlier than anatomical normalization. This objective improvement aligns with the dramatic reduction in SNOT-22 scores, yet it highlights a crucial area of divergence in the literature regarding remission definitions. Our observed dual remission rate of 88% at 24 months is notably higher than the 31% reported by Tajiri et al. [19].
This difference likely reflects our definition of remission, which accepts “clinical silence” and minor mucosal thickening, whereas other studies may demand absolute olfactory restitution and total polyp disappearance [20]. While our study demonstrates that dupilumab significantly improves olfactory performance (SS-I score 9.00 at 24 months [p < 0.001 vs baseline]), requiring “complete” restitution—which may be limited by long-standing neuroepithelial damage—sets a much higher bar than the EPOS/EUFOREA criteria used in our analysis [13]. Thus, while smell improves substantially, the definition of “remission” heavily influences reported success rates in real-world studies. In this regard, while 88% of our cohort achieved Dual Remission at 24 months, indicating effective control of type 2 inflammation in both the upper and lower airways, the restoration of olfactory function followed a distinct and less complete trajectory. When we applied a stricter composite definition requiring Dual Remission plus normosmia (SS-I score ≥ 12), the success rate dropped to 32% (8/25 patients), overlapping with the data from the study by Tajiri et al. [19]. This observation reveals a significant ‘clinical-functional gap’ affecting approximately 56% of our patients (14/25), who achieved clinical silence (no asthma exacerbations, OCS independence, and reduced polyp burden) but remained hyposmic. This discrepancy strongly supports the hypothesis that long-standing CRSwNP may cause irreversible neuroepithelial damage or remodeling that persists even after the inflammatory burden is resolved. Consequently, while Dupilumab proves highly effective at inducing clinical remission, ‘complete’ recovery including full olfactory restitution may require longer treatment duration or may not be achievable for all patients with severe, chronic disease.
Our data integrates also the recently published “Two-Year Turning Point” study, the largest real-life investigation to date involving 926 patients up to 1 year [20]. These authors demonstrated that patients who had not yet achieved optimal control targets at 12 months showed continued significant improvement during the second year of therapy. This confirms our observation of a “catch-up” phenomenon on a much larger scale, validating the concept that 12 months is often an insufficient horizon to judge the full potential of biologic therapy in tissue remodeling. Furthermore, they found that tapering the dosage to every 4 weeks was feasible in nearly 19% of patients without loss of control, suggesting that once the “turning point” of deep remission is reached, the therapeutic burden can be reduced. The novelty of our findings lies in the “catch-up” phenomenon: approximately 67% who had not achieved CRSwNP remission at 1 year achieved it by year 2 (6 out of 9 evaluated non-responders) (Figure 1). This argues strongly against switching therapies prematurely if a patient has excellent asthma control but “sub-optimal” polyp reduction at 12 months.
These real-world observations regarding the kinetics of remission offer a complementary long-term perspective to the recently published EVEREST trial [21]. While this head-to-head trial validated the early superiority of dupilumab over omalizumab at 24 weeks, our 24-month data suggest that the full extent of structural remodeling—particularly in the upper airways—accrues well beyond the timeframe of substantial clinical trials. Furthermore, the high consistency of dual remission observed in our cohort contrasts with recent transcriptomic findings by Estravís et al., who identified specific biomarkers (e.g., RGS1) as necessary predictors for a “dual super-response” to mepolizumab [22]. This distinction reinforces the hypothesis that the broad upstream blockade of IL-4 and IL-13 may induce “clinical silence” across a wider phenotypic spectrum compared to the more biomarker-dependent efficacy observed with distal cytokine inhibition.
Our findings of high “dual remission” rates (88% at 24 months) also warrant a critical comparison with the recent data reported by Tajiri et al. [19]. While both studies reinforce the necessity of prolonged dupilumab treatment to achieve maximum benefit, a marked divergence exists in the absolute rates of remission reported. Tajiri et al. reported a CRSwNP remission rate of 31% at 24 months, significantly lower than the 81.3% observed in our cohort. This discrepancy is likely attributable to the stringency of the remission definitions applied; whereas Tajiri et al. utilized a rigorous definition requiring complete recovery of olfactory function and endoscopic silence, our study applied the EPOS/EUFOREA criteria, which allows for a state of “controlled” low-grade disease rather than demanding absolute clearance [13]. Furthermore, regarding asthma, the difference between our 100% remission rate and the lower rates in comparable severe asthma cohorts reinforces that “dual remission” is most attainable in “united airway” phenotypes where the upper airway burden is the primary driver (mild-to-moderate asthma), while “complete biological clearance” in refractory severe disease remains a more elusive target.
Beyond the clinical benefits, the achievement of dual remission has significant pharmacoeconomic implications. The high acquisition cost of monoclonal antibodies is a frequent subject of debate; however, the concept of “cross-coverage”—treating two severe, resource-intensive comorbidities with a single agent—substantially improves the therapy’s value proposition [23]. Jommi et al. analyzed this “crowding-out” effect in the Italian National Health Service (NHS) perspective, estimating that the use of dupilumab for cross-coverage (treating CRSwNP in patients with severe asthma and vice-versa) generates significant savings by displacing the costs of alternative treatments, surgeries, and comorbidity management. Their model estimated total potential annual savings ranging from €0.95 to €8.36 million, depending on market penetration [23].
These findings are supported by a specific cost-utility analysis for Italy conducted by De Corso et al., which demonstrated that dupilumab as an add-on treatment for severe uncontrolled CRSwNP is cost-effective. They reported an incremental cost-utility ratio (ICUR) of €21,817 per quality-adjusted life year (QALY) gained, a figure well below the commonly accepted willingness-to-pay thresholds in the Italian healthcare system (€25,000–€40,000/QALY) [24]. International data further contextualizes this: in South Korea, Oh et al. found that add-on dupilumab was cost-effective for severe asthma (ICER 20,325/QALY), driven largely by the reduction in severe exacerbations and improvements in quality of life [25]. However, cost-effectiveness is sensitive to local pricing and comparators; a Canadian study by Yong et al. noted that while dupilumab demonstrated superior efficacy in SNOT-22 improvement compared to omalizumab and mepolizumab, its relative cost-effectiveness was heavily dependent on drug acquisition costs and dosing frequency [26]. Therefore, the “dual remission” observed in our real-world cohort—where 100% of asthma patients and 81.3% of CRSwNP patients achieved remission at 24 months—likely represents the scenario of maximum economic efficiency, where the single biologic cost is offset by the simultaneous cessation of resource utilization in both the upper and lower airways.
5. Conclusion
Dupilumab demonstrates substantial effectiveness in achieving simultaneous clinical remission in severe asthma and CRSwNP. The path to “dual remission” is asynchronous, with asthma improving rapidly and nasal polyps requiring prolonged treatment. The significant increase in dual remission rates at 24 months confirms that “clinical silence” is a realistic target that accrues well beyond the first year of treatment. Furthermore, achieving dual remission supports the pharmacoeconomic sustainability of this therapy; leveraging the cross-coverage potential of dupilumab to simultaneously resolve both upper and lower airway burdens optimizes healthcare resource allocation compared to treating each condition in isolation.
Author Contributions
Study conception and design were performed by FM, AB and EDC. Data collection and interpretation were carried out by all authors. The manuscript was drafted by FM and critically revised by all authors. All authors approved the final version of the manuscript and its submission.
Funding
There was no funding associated with the preparation of this article.
Informed Consent Statement
All patients provided signed informed consent to participate in this study.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of interest
Dr Menzella has received fees from AstraZeneca, Chiesi, GlaxoSmithKline, and Sanofi, as well as research grants from AstraZeneca, GlaxoSmithKline, and Sanofi. Prof Berti has received advisory board honoraria, consultancy fees and/or speaker fees from GSK. Dr Cottini reports personal fees for lectures from Chiesi, Menarini, and GSK, and support for attending scientific meetings from Chiesi. Prof De Corso reports lecture fees and participations in experts board meeting of GSK, Novartis, Sanofi, Astrazeneca. The remaining authors have no conflicts of interest to declare.
Abbreviations
| ACT | Asthma Control Test |
| OCS | Oral Corticosteroids |
| SNOT-22 | Sino-Nasal Outcome Test-22 |
| NPS | Nasal Polyp Score |
| BMI | Body Mass Index |
| CRSwNP | Chronic Rhinosinusitis with Nasal Polyps |
| FEF25-75 | Forced Expiratory Flow at 25-75% of FVC |
| FeNO | Fractional exhaled Nitric Oxide |
| FEV1 | Forced Expiratory Volume in 1 second |
| FVC | Forced Vital Capacity |
| GERD | Gastroesophageal Reflux Disease |
| ICS | Inhaled Corticosteroids |
| ICUR | Incremental Cost-Utility Ratio |
| IgE | Immunoglobulin E |
| IL-4 | Interleukin-4 |
| IL-5 | Interleukin-5 |
| IL-13 | Interleukin-13 |
| IQR | Interquartile Ranges |
| LABA | Long-Acting Beta-Agonists |
| LAMA | Long-Acting Muscarinic Antagonists |
| NHS | National Health Service |
| NSAID-ERD | Non-Steroidal Anti-Inflammatory Drug-Exacerbated Respiratory Disease |
| QALY | Quality-Adjusted Life Year |
| RV | Residual Volume |
| SANI | Severe Asthma Network Italy |
| SS-I | Sniffin’ Sticks Identification test |
| T2 | Type 2 (inflammation) |
| TLC | Total Lung Capacity |
References
- Pelaia, C.; Pelaia, G.; Maglio, A.; et al. Pathobiology of Type 2 Inflammation in Asthma and Nasal Polyposis. J Clin Med. 2023, 12, 3371. [Google Scholar] [CrossRef]
- Sahnoon, L.; Bajbouj, K.; Mahboub, B.; et al. Targeting IL-13 and IL-4 in Asthma: Therapeutic Implications on Airway Remodeling in Severe Asthma. Clin Rev Allergy Immunol. 2025, 68, 44. [Google Scholar] [CrossRef]
- Le Floc’h, A.; Allinne, J.; Nagashima, K.; et al. Dual blockade of IL-4 and IL-13 with dupilumab, an IL-4Rα antibody, is required to broadly inhibit type 2 inflammation. Allergy 2020, 75, 1188–1204. [Google Scholar] [CrossRef]
- Castro, M.; Corren, J.; Pavord, I.D.; et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. 2018, 378, 2486–2496. [Google Scholar] [CrossRef]
- Wechsler, M.E.; Ford, L.B.; Maspero, J.F.; et al. Long-term safety and efficacy of dupilumab in patients with moderate-to-severe asthma (TRAVERSE): an open-label extension study. Lancet Respir Med. 2022, 10, 11–25. [Google Scholar] [CrossRef]
- Gelardi, M.; Bocciolini, C.; Notargiacomo, M.; et al. Chronic rhinosinusitis with nasal polyps: how to identify eligible patients for biologics in clinical practice. Acta Otorhinolaryngol Ital. 2022, 42, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Nathan, R.A.; Sorkness, C.A.; Kosinski, M.; et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004, 113, 59–65. [Google Scholar] [CrossRef]
- Stanojevic, S.; Kaminsky, D.A.; Miller, M.R.; et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. 2022, 60, 2101499. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, C.; Gillett, S.; Slack, R.; et al. Psychometric validity of the 22-item Sinonasal Outcome Test. Clin Otolaryngol. 2009, 34, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Lund, V.J.; Kennedy, D.W. Staging for rhinosinusitis. Otolaryngol Head Neck Surg. 1997, 117, S35–40. [Google Scholar] [CrossRef]
- Mauthe, T.; Ryser, F.S.; Brühlmann, C.; et al. Correlation of sino-nasal outcome test and nasal polyp score in dupilumab-treated chronic rhinosinusitis with nasal polyps. Eur Arch Otorhinolaryngol. 2025, 282, 207–218. [Google Scholar] [CrossRef]
- Canonica, G.W.; Blasi, F.; Carpagnano, G.E.; et al. Severe Asthma Network Italy Definition of Clinical Remission in Severe Asthma: A Delphi Consensus. J Allergy Clin Immunol Pract. 2023, 11, 3629–3637. [Google Scholar] [CrossRef]
- Fokkens, W.J.; De Corso, E.; Backer, V.; et al. EPOS2020/EUFOREA expert opinion on defining disease states and therapeutic goals in CRSwNP. Rhinology 2024, 62, 287–298. [Google Scholar] [CrossRef] [PubMed]
- Masala, C.; Cavazzana, A.; Sanna, F.; et al. Correlation between olfactory function, age, sex, and cognitive reserve index in the Italian population. Eur Arch Otorhinolaryngol. 2022, 279, 4943–4952. [Google Scholar] [CrossRef]
- Bosi, A.; Lombardi, C.; Caruso, C.; et al. Clinical remission and control in severe asthma: agreements and disagreements. Drugs Context 2024, 13, 2024-7-2. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.; Papi, A.; Porsbjerg, C.; et al. Effect of dupilumab on exhaled nitric oxide, mucus plugs, and functional respiratory imaging in patients with type 2 asthma (VESTIGE): a randomised, double-blind, placebo-controlled, phase 4 trial. Lancet Respir Med. 2025, 13, 208–220. [Google Scholar] [CrossRef]
- De Corso, E.; Settimi, S.; Montuori, C.; et al. Effectiveness of dupilumab in the treatment of severe uncontrolled chronic rhinosinusitis with nasal polyps (CRSwNP): A multicentric real-life study. Int Forum Allergy Rhinol. 2022, 12, 1266–1275. [Google Scholar]
- De Corso, E.; Pasquini, E.; Trimarchi, M.; et al. Dupilumab in the treatment of severe uncontrolled chronic rhinosinusitis with nasal polyps (CRSwNP): A multicentric observational Phase IV real-life study (DUPIREAL). Allergy 2023, 78, 2683–2693. [Google Scholar] [CrossRef]
- Tajiri, T.; Suzuki, M.; Nishiyama, H.; et al. Dupilumab-induced remission in chronic rhinosinusitis with nasal polyps and comorbid asthma: a 24-month study. J Clin Med. 2025, 14, 3654. [Google Scholar] [CrossRef]
- De Corso, E.; Montuori, C.; Pipolo, C.; et al. Two-Year Turning Point With Dupilumab in CRSwNP: Control, Remission, and Tapering Dosage. Allergy 2025. [Google Scholar] [CrossRef]
- De Corso, E.; Canonica, G.W.; Heffler, E.; et al. Dupilumab versus omalizumab in patients with chronic rhinosinusitis with nasal polyps and coexisting asthma (EVEREST): a multicentre, randomised, double-blind, head-to-head phase 4 trial. Lancet Respir Med. 2025, 13, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Estravís, M.; Carreiras-Quintas, D.; Triviño, J.C.; et al. Identification of Dual Super-Response in Patients With Asthma and CRSwNP Treated With Mepolizumab. J Investig Allergol Clin Immunol. 2025. [Google Scholar] [CrossRef]
- Jommi, C.; Cipriani, F.; Fanelli, F.; et al. The effects of disease cross-coverage by dupilumab on the costs sustained by the Italian National Health Service. Glob Reg Health Technol Assess. 2020, 7, 33–39. [Google Scholar] [CrossRef] [PubMed]
- De Corso, E.; Furneri, G.; Salsi, D.; et al. Cost-Utility Analysis of Dupilumab for the Treatment of Chronic Rhinosinusitis with Nasal Polyps (CRSwNP) in Italy. J Pers Med. 2022, 12, 951. [Google Scholar] [CrossRef]
- Oh, S.H.; Rhee, C.K.; Bae, E.J.; et al. Cost-effectiveness analysis of dupilumab among patients with uncontrolled severe asthma using LIBERTY ASTHMA QUEST Korean data. Health Econ Rev. 2024, 14, 67. [Google Scholar] [CrossRef]
- Yong, M.; Kirubalingam, K.; Desrosiers, M.Y.; et al. Cost-effectiveness analysis of biologics for the treatment of chronic rhinosinusitis with nasal polyps in Canada. Allergy Asthma Clin Immunol. 2023, 19, 90. [Google Scholar] [CrossRef]
Figure 1.
Longitudinal trajectories of asthma and sinonasal disease activity over 24 months.
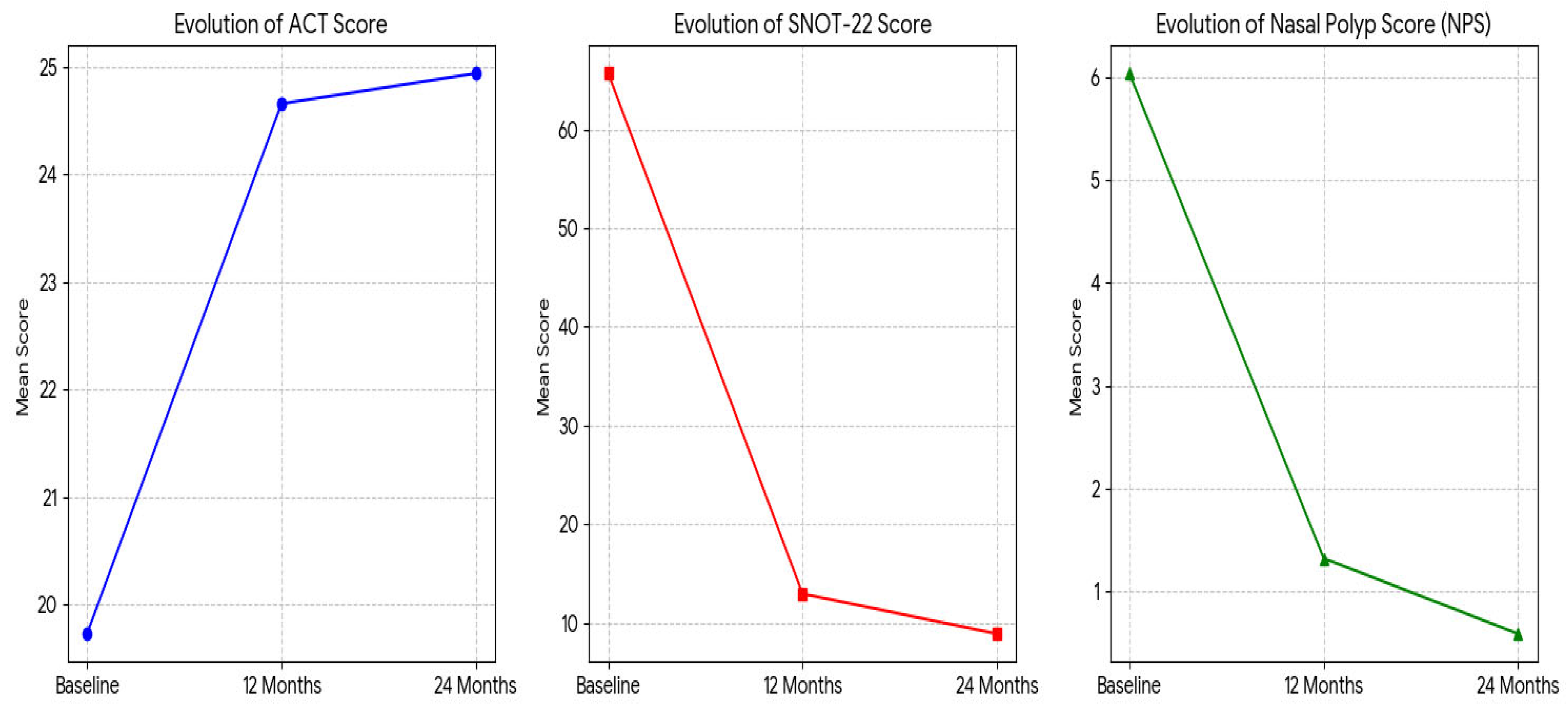
Figure 2.
Evolution of single and dual remission rates. Bar chart displaying the percentage of patients achieving remission criteria at 12 months (blue bars) and 24 months (orange bars). Abbreviations: CRSwNP: Chronic Rhinosinusitis with nasal Polyps.
Figure 2.
Evolution of single and dual remission rates. Bar chart displaying the percentage of patients achieving remission criteria at 12 months (blue bars) and 24 months (orange bars). Abbreviations: CRSwNP: Chronic Rhinosinusitis with nasal Polyps.
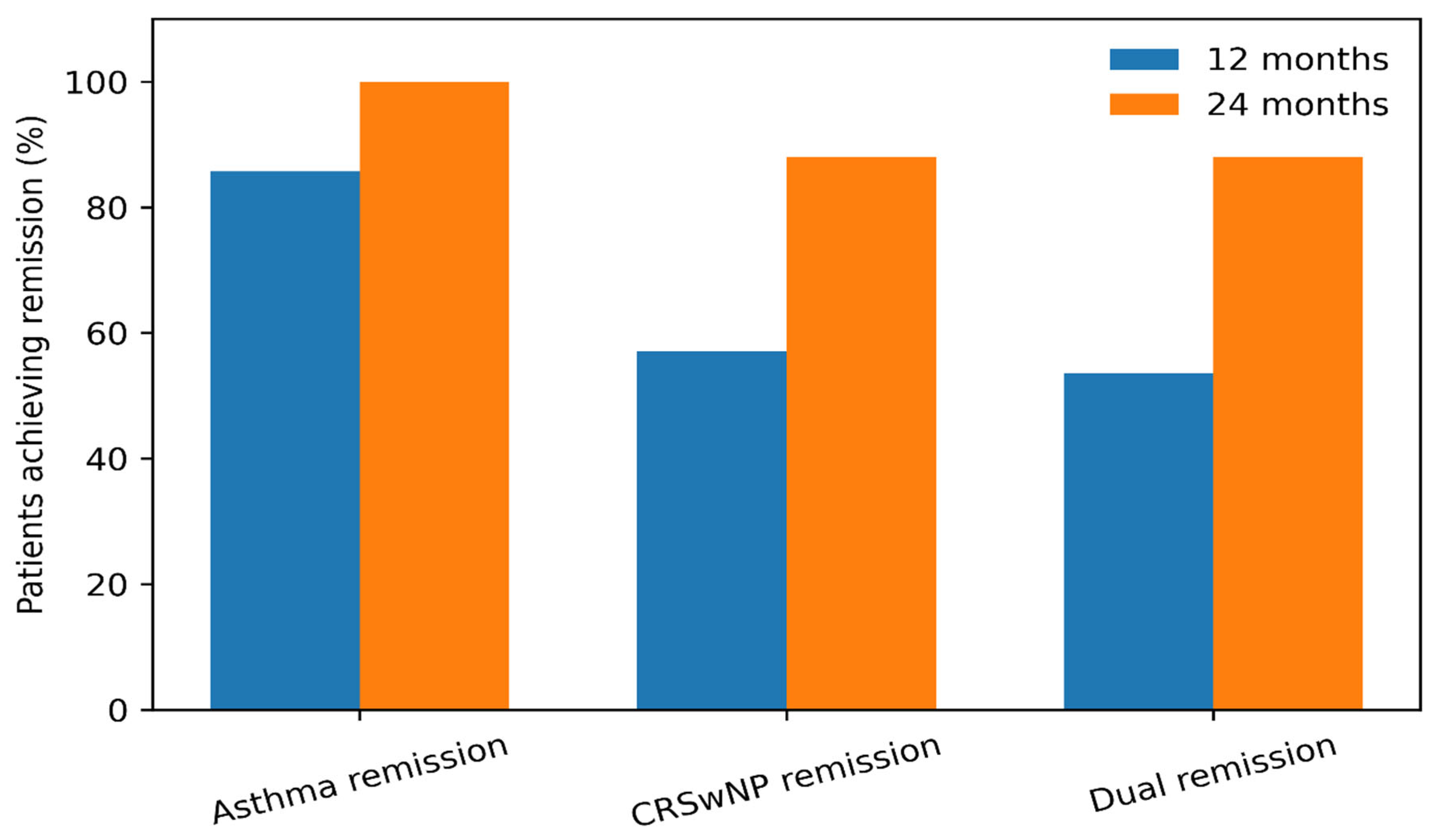

Table 1.
Baseline demographic and clinical characteristics of the 28 patients included in this study.
Table 1.
Baseline demographic and clinical characteristics of the 28 patients included in this study.
| Variable | Value (N=28) |
| Demographics | |
| Age, years | 53.50 (48.75 – 61.25) |
| Sex, n (%) | Male: 17 (61%) / Female: 11 (39%) |
| BMI, kg/m2 | 24.75 (22.75 – 28.00) |
| Disease history & severity | |
| Asthma severity, n (%) | |
| Severe asthma | 8 (29%) |
| Mild-Moderate asthma | 20 (71%) |
| Asthma duration, years | 12.00 (2.00 – 21.75) |
| CRSwNP duration, years | 12.50 (8.00 – 20.50) |
| Comorbidities (NSAID-ERD), n (%) | 12 (42.9%) |
| Baseline clinical metrics | |
| Blood eosinophils, cells/µL | 525.00 (400.00 – 652.50) |
| Total IgE, IU/mL | 164.50 (101.75 – 324.25) |
| FEV1, L | 3.12 (2.56 – 3.61) |
| ACT score | 19.00 (16.50 – 24.00) |
| SNOT-22 score | 67.00 (54.50 – 80.00) |
| Nasal Polyp Score (NPS) (0-8) | 6.00 (6.00 – 6.00) |
| Daily OCS, mg/day | 1.40 (0.00 – 2.90) |
Data are presented as Median (IQR 25th–75th percentile) for continuous variables and n (%) for categorical variables. N=28 unless otherwise specified. Abbreviations: BMI, Body Mass Index; CRSwNP, Chronic Rhinosinusitis with Nasal Polyps; NSAID-ERD, Non-Steroidal Anti-Inflammatory Drug-Exacerbated Respiratory Disease; GERD, Gastroesophageal Reflux Disease; IgE, Immunoglobulin E; FeNO, Fractional exhaled Nitric Oxide; FEV1, Forced Expiratory Volume in 1 second; FVC, Forced Vital Capacity; ACT, Asthma Control Test; SNOT-22, Sino-Nasal Outcome Test-22; NPS, Nasal Polyp Score; OCS, Oral Corticosteroids.
Table 2.
Evolution of clinical, functional, and biological parameters during Dupilumab treatment.
| Parameter | Baseline | 12 Months | 24 Months | p-value(12m vs baseline) | p-value(24m vs baseline) |
| Clinical control | |||||
| ACT score | 19 (16.5 – 24) | 25 (25 – 25) | 25 (25 – 25) | <0.001 | 0.007 |
| SNOT-22 score | 67 (54.5 – 80) | 10 (5– 15) | 5 (3 – 13.25) | <0.001 | <0.001 |
| NPS (0-8) | 6 (6 – 6) | 0.5 (0 – 2) | 0 (0 – 0) | <0.001 | <0.001 |
| Sniffin’ Stick score | 3 (3 – 3) | 7 (5.25 – 9.75) | 9 (5 – 11) | <0.001 | <0.001 |
| OCS (mg/day) | 1.4 (0.0 – 2.9) | 0.0 (0.0 – 0.0) | 0.0 (0.0 – 0.0) | <0.001 | <0.001 |
| Lung function | |||||
| FEV1 (L) | 3.12 (2.56 – 3.61) | 3.50 (3.05 – 3.83) | 3.50 (3.11 – 3.91) | 0.064 | 0.018 |
| FEV1 (% predicted) | 94.00 (84.00 – 111.8) | 102.50 (90.25 – 111.3) | 109.00 (101.5 – 117.8) | 0.127 | 0.017 |
| FVC (L) | 4.53 (3.87 – 5.21) | 4.42 (4.37 – 5.99) | 4.57 (4.13 – 5.40) | 0.433 | 0.330 |
| FVC (% predicted) | 112.00 (102.5 – 120.5) | 116.50 (109.3 – 121.5) | 117.50 (108.5 – 123.0) | 0.426 | 0.469 |
| FEF25-75 (L/s) | 1.76 (1.27 – 2.88) | 2.34 (1.45 – 2.83) | 2.74 (1.74 – 2.95) | 0.231 | 0.635 |
| FEF25-75 (% pred) | 54.00 (41.00 – 92.50) | 70.00 (51.50 – 88.75) | 88.00 (66.50 – 114.5) | 0.071 | 0.569 |
| Lung volumes | |||||
| RV (L) | 1.86 (1.35 – 2.56) | 1.79 (1.47 – 2.07) | 1.87 (1.46 – 2.17) | 0.022 | 1.000 |
| TLC (L) | 5.92 (4.84 – 6.73) | 6.15 (5.77 – 6.93) | 6.19 (5.85 – 7.38) | 0.241 | 0.042 |
| Biomarkers | |||||
| Blood eosinophils (/µL) | 525 (400 – 653) | 535 (405 – 1195) | 660 (140 – 1033) | 0.053 | 0.229 |
| FeNO (ppb) | 23.00 (22.00 – 90.00) | 37.00 (28.00 – 48.00) | 25.00 (19.00 – 30.00) | 0.500 | 1.000 |
Data are presented as Median (IQR 25th–75th). P-values calculated using Wilcoxon signed-rank test. Abbreviations: ACT, Asthma Control Test; SNOT-22, Sino-Nasal Outcome Test-22; NPS, Nasal Polyp Score; OCS, Oral Corticosteroids; FEV1, Forced Expiratory Volume in 1s; FVC, Forced Vital Capacity; FEF25-75, Forced Expiratory Flow at 25-75% of FVC; RV, Residual Volume; TLC, Total Lung Capacity; FeNO, Fractional exhaled Nitric Oxide.
Table 3.
Safety profile and blood eosinophils evolution.
| Parameter | Baseline (N=28) | 12 Months (N=28) | 24 Months (N=25) |
| Hypereosinophilia | |||
| Eosinophils ≥ 1,500 cells/µL, n (%) | 0 (0%) | 3 (11%) | 1 (6%) |
| Eosinophils > 3,000 cells/µL, n (%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Adverse events, n (%) | |||
| Serious infections* | 0 (0%) | 0 (0%) | 0 (0%) |
| Discontinuation due to AE | — | 0 (0%) | 0 (0%) |
Data are presented as number (percentage) of patients. Eosinophil counts refer to absolute blood eosinophil levels. *No severe infections or injection site reactions requiring treatment discontinuation were reported during the 24-month observation period.
Table 4.
Comprehensive clinical & olfactory outcomes.
| Outcome measure | Baseline (N=28) | T12 (12 months) (N=28) | T24 (24 months) (N=25) | p-value (T12 vs baseline) | p-value (T24 vs baseline) |
| 1. Clinical remission outcomes | |||||
|
Asthma remission (ACT ≥ 20 + No OCS + No Exacerbations) |
0% | 24/28 (85.7%) | 25/25 (100%) | < 0.001 | < 0.001 |
|
CRSwNP remission (NPS ≤ 1 + SNOT-22 < 40) |
0% | 16/28 (57.1%) | 22/25 (88.0%) | < 0.001 | < 0.001 |
|
Dual Remission (Achieved both above) |
0% | 15/28 (53.6%) | 22/25 (88.0%) | < 0.001 | < 0.001 |
| 2. Olfactory outcomes | |||||
| Sniffin’ sticks score (Median) | 3.0 | 7.0 | 9.0 | < 0.001* | < 0.001* |
|
Olfactory recovery (Normosmia: Score ≥ 12) |
0% | < 10% (Est.) | 8 (32.0%) | ns | < 0.01 |
| 3. Combined “Complete” recovery | |||||
| Dual remission + normosmia | 0% | -- | 8 (32.0%) | -- | < 0.01 |
Values expressed as n/N (%). N varies due to data availability at each timepoint. Abbreviations: ACT: Asthma Control Test; OCS: Oral Corticosteroids; CRSwNP: Chronic Rhinosinusitis with Nasal Polyps; NPS: Nasal Polyp Score; SNOT-22: Sino-Nasal Outcome Test-22; SS-I: Sniffin’ Sticks-Identification test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



