Submitted:
09 February 2026
Posted:
11 February 2026
You are already at the latest version
Abstract
Background: Documentation in oncologist Electronic Health Records (EHRs) plays a critical role in communication, shared decision-making, and the detection of adverse effects all of which influence treatment concordance and adherence. However, narrative content is often incomplete, delayed, or written in formal styles that obscure patient priorities. Methods: Following PRISMA-ScR guidelines, we conducted a scoping review of studies published between 2013 and early 2024 that used natural language processing (NLP) or text mining on oncologist notes, or qualitatively examined EHR use in oncology. Data were charted by topic (e.g., adverse effects, note style, stigma, workflow burden) and synthesized using discourse analysis. Results: Twenty-three studies met inclusion criteria. Four clinician-side themes emerged: (1) compliance-oriented EHR design; (2) incomplete or delayed documentation of adverse effects, pain, and social determinants of health (SDOH); (3) formal or stigmatizing language; and (4) time and cognitive burden limiting person-centred narratives. These factors hinder concordance documentation and communication transparency. Conclusions: Improvements in EHR design, including person-centred prompts, plain-language templates, and audit-log-informed workflow changes, may enhance adherence by supporting better documentation and communication. Nursing and service leaders can implement these changes to promote trust, engagement, and continuity of care. Registration: Not registered.
Keywords:
adverse effects
; documentation quality
; electronic health records
; nursing informatics
; oncologist notes
; person-centred care
; stigma in notes
; text mining
; treatment concordance
1. Introduction
Electronic Health Records (EHRs) are central to oncology care, yet much of their clinically relevant content is captured in unstructured text progress notes, pathology/radiology reports, and other narrative fields [1,2]. Narrative documentation is the locus where adverse effects, symptom trajectories, psychosocial issues, patients’ goals and values, and shared decision making should be recorded. However, multiple studies suggest that such information is inconsistently captured, delayed, or written in formal styles that obscure patient priorities [3,4]. Access and data sharing constraints, privacy concerns, and limited availability of shared de-identified corpora have also slowed oncology specific Natural Language Processing (NLP) [5,6]. Recent reviews note that extracting oncology concepts from clinical notes remains an active methodological frontier [7,8].
Documentation gaps have implications for treatment concordance and adherence. Adverse effects and pain may be incompletely recorded, and social determinants of health (SDOH) under documented, hindering timely recognition of barriers to ongoing therapy [1,9,10,11]. Language choices in notes can transmit bias, with stigmatizing terms linked to alienation and trust erosion [12]. At the same time, clinicians face time pressure and cognitive burden: template driven and compliance oriented EHRs demand substantial navigation and coding effort, which can crowd out person-centred narratives, encourage copy paste practices, and limit explicit recording of concordance conversations [13,14,15,16,17,18]. The result is a documentation ecosystem optimized for billing and standardized data capture, but not always for the transparency, inclusivity, and specificity that shared decision making requires [19,20].
NLP and text mining make it possible to analyze clinician notes at scale, revealing patterns in documentation density, topic emphasis, language tone, and reporting delays. Studies have used such methods to classify serious illness communication and to compare recorded notes with the substance of clinical encounters, highlighting discrepancies and missed opportunities to codify patient goals and agreements [21,22]. Similar research on patient access to notes underscores the communicative function of documentation itself. Clinical notes are often in plain language and person-centred phrasing can strengthen understanding, trust, and engagement [4,23,24].
Aim and research questions. This scoping review synthesizes evidence from NLP and text mining studies of oncologist EHR narratives. Qualitative reports on EHR use in oncology were also included because they can also identify documentation patterns that may impede or enable treatment concordance and adherence. Using discourse analysis, we ask:
- 1.
- 2.
2. Method
2.1. Design and Reporting
We conducted a scoping review compliant with PRISMA-ScR [25] to map NLP and text mining evidence from oncologist EHR narratives and qualitative EHR studies in oncology. The goal was to identify documentation patterns linked to concordance and adherence, and to derive nursing service design implications.
2.2. Eligibility Criteria
Inclusion. Studies were eligible if they: (i) mined oncologist or clinician notes or oncology clinical documentation using NLP or text mining; or (ii) investigated oncologist EHR use qualitatively with implications for documentation and communication; (iii) reported on constructs relevant to concordance and adherence; (iv) were peer reviewed and published in English between 2013 and early 2024 [4,7,8,21].
Exclusion. We excluded non oncology note mining, non English publications, economic analyses, and grey literature except World Health Organisation (WHO) and Australian Commission on Safety and Quality in Health Care (ACSQHC) policy statements used for definitional clarity.
2.3. Information Sources and Search Strategy
We searched PubMed, CINAHL, and Scopus (2013–early 2024) using combinations of oncology and EHR terms and documentation constructs (e.g., “oncology” AND “electronic health records” AND “clinical notes”; “text mining” AND “adverse effects” AND “oncology”; “stigma” AND “clinical documentation”). The strategy was iteratively refined to include design and workflow terms (e.g., audit logs, template burden, copy–paste) and language and style concepts (plain language, person-centred phrasing, stigmatizing lexicon) [12,13,14,20]. We noted barriers to corpus access and de-identification highlighted in informatics studies [5,6] and the infancy of oncology specific NLP [7].
2.4. Study Selection
2.5. Data Charting
We charted author, year, and country, cancer domain, EHR system context, corpus properties (size, note types), NLP and text mining methods, targeted documentation topics (e.g., adverse effects, pain, SDOH, concordance cues, note style), and key findings. We also captured feasibility indicators (time and cognitive burden, reuse or copy–paste, template constraints), and language considerations (plain language phrasing, stigma markers, person-centred content) [12,15,20].
2.6. Critical Appraisal
We used the Critical Appraisal Toolkit (CAT) to describe the methodological rigor of heterogeneous sources (NLP pipelines; qualitative studies; mixed-methods) with ratings (low/medium/high) and strength of evidence descriptors [26]. Appraisal results informed interpretation; consistent with scoping review methodology, studies were not excluded solely on appraisal scores [27,28].
2.7. Synthesis Approach
Discourse analysis guided a narrative synthesis of clinician side themes: (i) EHR barriers or compliance-oriented design; (ii) incomplete or late documentation (adverse effects, pain, SDOH); (iii) formal note style and stigmatizing language; and (iv) time and cognitive burden limiting Patient Centred Care (PCC) narratives [12,13,14,20]. We used sentinel exemplars to illustrate misalignment between recorded notes and serious illness communication or patient goals [21,22], and integrated evidence on patient access portals to emphasize documentation’s communicative function [4,23,24]. A thematic barrier map (Figure 2) summarizes the relationships between documentation features and concordance and adherence outcomes.
3. Results
3.1. Overview
A total of twenty–three studies met the inclusion criteria for this scoping review and were synthesized to characterize documentation patterns in oncology EHR narratives and their implications for treatment concordance and adherence. Reasons for exclusion at full text stage comprised non oncology note mining, non English publications, economic analyses, and grey literature beyond WHO and ACSQHC definitional sources. The overall selection process is summarized in the PRISMA–ScR flow diagram (Figure 1) [25].
3.2. Study Selection Narrative (PRISMA–ScR)
Across database searches (PubMed, CINAHL, Scopus) and iterative query refinement, records were screened on title and abstract for EHR narrative mining or oncology EHR relevance, followed by full text assessment against predefined inclusion/exclusion criteria. Disagreements between reviewers were resolved by consensus. While exact counts at each PRISMA node are depicted in Figure 1, the final corpus comprises 23 included studies spanning NLP/text mining of oncologist notes and qualitative examinations of oncology EHR use [4,7,8,9,10,12,13,14,20,21,22,23].
3.3. Characteristics of Included Studies
Table 1 summarizes the most salient features of the included sources: cancer domain, corpus type and size, EHR context, analytic method (e.g., rule based extraction, machine learning, linguistic analysis), and concordance and adherence relevant indicators derived from narrative documentation. Across studies, corpora and pipelines were heterogeneous ranging from progress notes and discharge letters to audit logs and portal view data yet converged on documentation constructs central to concordance (adverse effects, pain, SDOH, note style, timing, reuse) [1,4,9,10,12,13,14,15,20].

Table 1.
Summary of oncologist studies (Part 1 of 3)
| Author & Title | Method | Data Sources | Sample | Results | NLP Technique | Nonadherence/Inference |
|---|---|---|---|---|---|---|
| Masukawa et al., 2022 [1] . Machine Learning Models to Detect Social Distress and severe physical/psychological symptoms in terminally ill patients with cancer from unstructured EHR text data | Quantitative study | Retrospective cancer patient records | 808 cancer patients.CAT: Strength=Moderate; Quality = Medium | ML detected social distress and symptoms (pain, dyspnea, nausea, insomnia, anxiety). | Supervised machine learning | Text data can identify social distress; areas like anxiety receive scant attention compared to physical pain (∼40% of narratives), affecting adherence risks. |
| Alpert et al., 2019 [4] . Patient access to clinical notes in oncology: A mixed method analysis of oncologists’ and linguistic attitudes towards notes | Mixed methods | National Cancer Institute, Virginia | 13 interviews; 500 clinical notes; 22 oncologists.CAT: Strength=Moderate; Quality = Medium | Oncologists acknowledged that changing note content could improve patient communication but may hinder interdisciplinary communication. | Linguistic Inquiry and Word Count (LIWC); random effects modelling | Tension between patient-centred language and clinical interaction; challenges in non-clinical communication may affect adherence. |
| Che-Chen Kuo et al., 2022 [9] . Using data mining technology to predict medication-taking behaviour in women with breast cancer: A retrospective study | Quantitative (structured EHR data) | Breast cancer patient records | 385 records.CAT: Strength = Weak; Quality = Low | Highest polarity of reviews related to patient–doctor experience and pain. | Multiple logistic regression, decision tree, artificial neural network | Structured medical records may not capture adverse effects; missing factors can influence adherence. |
| Tamang et al., 2015 [10] . Detecting Unplanned Care from Clinician Notes in Electronic Health Records | Quantitative study | Cancer patient EHRs | 308,096 free-text machine-readable notes.CAT: Strength=Moderate; Quality = Medium | Including free-text notes increased identification of ED visits; textual analysis identified most reported symptoms. | Clinical text mining | Combining structured & unstructured data improved detection; pain was the most common reason for ED visits — cancer pain management suboptimal. |
| Himmelstein et al., 2023 [12] . Examination of Stigmatising Language in the Electronic Health Record | Quantitative | Longitudinal retrospective | National Danish Patient Registry; 4,418 pancreatic cancer patients.CAT: Strength=Moderate; Quality = Medium | Text-based approach identified 132 unique symptoms in clinical notes. | Text mining comparisons to registry data | Stigmatizing language appears in admission notes and varies by condition; stigmatization may alienate patients and lead to treatment discordance. |
| Patel et al., 2023 [13] . Clinician Perspectives on Electronic Health Records, Communication, and Patient Safety Across Diverse Medical Oncology Practices | Mixed-methods | Michigan Oncology Quality Collaborative (MOQC) | 29 oncology practices; 297 clinicians.CAT: Strength=Moderate; Quality = Medium | More seamless EHR integration into routine care is needed. | Sociotechnical framework; surveys | EHRs disrupt communication and increase workloads; patient communication may be compromised, risking unintentional nonadherence. |
| Huilgol et al., 2022 [14] . Opportunities to use electronic health record audit logs to improve cancer care | Qualitative | Report (article) | Summary on interpreting metadata from oncologist audit logs.CAT: Strength=Moderate; Quality = Medium | Audit logs can show how oncologists access information and collaborate. | Non-NLP (audit log analytics) | Understanding audit logs may clarify barriers to communication from EHR dissatisfaction (time/data entry/navigation), with adherence implications. |
| Rahimian et al., 2019 [15] . Significant and Distinctive n-grams in Oncology Notes: A Text-Mining Method to Analyse the Effect of OpenNotes on Clinical Documentation | Quantitative (n-gram analysis) | Oncology provider notes | 102,135 notes by 36 clinicians.CAT: Strength=Moderate; Quality = Medium | Significant differences before/after patient access to notes; longer explanatory notes observed. | Text mining (n-grams) | Oncologists may be less prolific note-takers; subtle empathetic changes with patient access may reflect communication skills relevant to adherence. |
Table 2.
Summary of oncologist studies (Part 2 of 3)
| Author & Title | Method | Data Sources | Sample | Results | NLP Technique | Nonadherence/Inference |
|---|---|---|---|---|---|---|
| Asan et al., 2023 [17] . Oncologists’ views regarding the role of Electronic Health Records in Care Coordination | Qualitative report | Semi-structured interviews | 60 oncologists.CAT: Strength=Moderate; Quality = Medium | Perceptions of oncologist EHR use during care coordination. | Traditional qualitative (non-NLP) | Oncologists report EHRs often not updated during encounters, potentially impacting communication and adherence. |
| Geskey et al., 2023 [19] . National Documentation and Coding Practices of Noncompliance: The Importance of Social Determinants of Health and the Stigma of African American Bias | Quantitative | Z codes (social determinants) in U.S. patient records | ∼9 million adult patients.CAT: Strength = Medium; Quality = Medium | Two or three comorbidities doubled the ratio of noncompliance. | Analysis of ICD-10 diagnosis codes in EHRs | Clinician bias in noncompliance coding (e.g., financial circumstances) may misclassify nonadherence from a multifactorial perspective. |
| Davoudi et al., 2022 [21] . Using Natural Language Processing to Classify Serious Illness Communication with Oncology Patients | Quantitative study | University of Pennsylvania Abramson Cancer Center | 3,563 patients; 5,145 notes; 8,695 distinct responses.CAT: Strength=Moderate; Quality = Medium | Validated SIC classifier enabling quality metrics (communication quality, goal-concordance). | Machine learning (domain/subdomain classification) | NLP can identify treatment concordance, a potential factor in nonadherence. |
| Simoulin et al., 2023. [36] From free-text electronic health records to structured cohorts: Onconum, an innovative methodology for real-world data mining in breast cancer | Quantitative study | Hospital patients with breast cancer at Strasbourg University Hospital | 9,599 patients.CAT: Strength = Weak; Quality = Low | Successfully extracted and structured information from EHRs in breast cancer without pre-existing dictionaries or manually annotated corpora. | Hybrid NLP (machine learning + rule-based lexical methods) | Multiple sources improved extraction rates and quality; structured information can be recovered from text. May enable comparison of codified adherence against notes. |
| Xin et al., 2023.[37] Pancreatic cancer symptom trajectories from Danish registry data and free text in electronic health records | Quantitative | Longitudinal retrospective | National Danish Patient Registry; 4,418 pancreatic cancer patients.CAT: Strength=Moderate; Quality = Medium | Text-based approach identified 132 unique symptoms in clinical notes. | Text mining comparisons to registry data (technique not stated) | Text mining identified more symptoms than coded registries alone, potentially improving detection of issues related to adherence. |
| Elbers et al., 2023.[38] Sentiment analysis of medical record notes for lung cancer patients at the Department of Veterans Affairs | Quantitative study | Department of Veterans Affairs (U.S.) lung cancer patients | 10,000 patients; 3,500,000+ notes.CAT: Strength=Moderate; Quality = Medium | Recalibration of a general-purpose sentiment lexicon for oncology. | Hedonometer sentiment scoring adapted to clinical oncology | Detected higher adverse effects in final days of treatment/chemotherapy, suggesting increased risk of nonadherence toward end of cycles. |
| Leis et al., 2022.[39] Exploring the association of cancer and depression in Electronic Health Records: Combining Encoded Diagnosis and Mining Free-Text Clinical Notes | Quantitative | EHR database in a general hospital | 4,238 cancer patients.CAT: Strength=Moderate; Quality = Medium | Mining free-text identified more patients with depression than encoded data alone. | Open-source language analysis framework; text analysis | Depression often absent from structured data but detectable in notes; unintentional nonadherence may be influenced. |
| Mashima et al., 2022.[40] Using Natural Language Processing Techniques to Detect Adverse Events from Progress Notes Due to Chemotherapy | Quantitative | Kagawa University Hospital | 200 cancer patients receiving chemotherapy.CAT: Strength=Moderate; Quality = Medium | Significant increase in adverse effect detection via progress notes analysis. | Dictionary/corpus + proprietary NLP system | Adverse effects (a factor in nonadherence) may be missed in coded data; text mining of developmental progress needed. |
| Jensen et al., 2017.[41] Analysis of free text in electronic health records for identification of cancer patient trajectories | Quantitative | University Hospital of North Norway | 1,133,223 unstructured EHR text documents; 7,741 patients.CAT: Strength=Moderate; Quality = Medium | Free-text methods to identify trajectories may support decisions, decrease adverse events/readmissions, and improve cancer care quality. | Machine learning; text analyses using NOR-MeSH for automated capture | Time constraints for free-text entries are severe; patient access to notes may impact relationships and influence nonadherence/discordance. |
Table 3.
Summary of oncologist studies (Part 3 of 3)
| Author & Title | Method | Data Sources | Sample | Results | NLP Technique | Nonadherence/Inference |
|---|---|---|---|---|---|---|
| Feldman et al., 2016.[42] Mining the Clinical Narrative: All Text are not Equal | Quantitative | Publicly available electronic medical records | 45,000 patient records.CAT: Strength = Weak; Quality = Medium | Deep understanding of clinical text required; coding cannot fully describe clinician diagnosis; nuanced language is critical. | Natural Language Toolkit (NLTK) & Python | Nuanced language complicates NLP on clinical text; notes seldom record patient feedback in non-clinical terms, limiting adherence insights. |
| Ganesan et al., 2016.[43] Discovering Related Clinical Concepts Using Large Amounts of Clinical Notes | Quantitative study | MIMIC database | 10,000 clinical notes.CAT: Strength=Moderate; Quality = Medium | Related concepts can be used for query expansion, hypothesis generation, incident investigation, sentence completion, etc. | Mining related clinical concepts with graph data structures | Related concepts in notes may be keystones for inferring treatment nonadherence. |
| Falotico et al., 2015.[44] Identifying Oncological Patient Information Needs to Improve e-Health Communication: a preliminary text-mining analysis | Mixed methods (quantitative text → qualitative interviews) | Semi-structured interviews; text mining | 12 rare cancer patients; 20,400 words; >3,000 distinct terms.CAT: Strength=Moderate; Quality =Medium | Online communication should be supervised. | Text mining (interview transcripts) | Information needs become more treatment-specific and sophisticated over the trajectory; physician relationship quality may modulate adherence. |
| Hamid et al., 2020.[45] Text Parsing Based Identification of Patients with Poor Glaucoma Medication Adherence in the Electronic Health Record | Quantitative study | University of Michigan | 736 glaucoma patients.CAT: Strength = Weak; Quality = Low | Identified a larger proportion of patients with poor adherence than automated EHR pull alone. | Text parsing of physician notes | Medication adherence identifiable only in progress notes, emphasizing unstructured text value. |
| Zhu et al., 2019.[46] Automatically identifying social isolation from clinical narratives for patients with prostate cancer | Quantitative study | Medical University of South Carolina | 3,138 patients.CAT: Strength=Moderate; Quality = Medium | Highly accurate identification of social isolation when noted in clinical narratives. | NLP algorithm + lexicon for social isolation | Poor documentation of social factors in notes can lead to nonadherence; both physician and shared factors involved. |
| Datta et al., 2019.[47] A frame semantic overview of NLP-based information extraction for cancer-related EHR notes | Quantitative study (overview) | NLP literature | 78 articles.CAT: Strength = Weak; Quality = Low | Guidance for general-purpose cancer frame resources and NLP systems to extract diverse cancer information types. | Frame construction; scoping review of NLP techniques | Treatment adherence not specifically framed despite importance; gap for future work. |
3.4. Main Findings at a Glance
Synthesis of the 23 studies reveals four clinician-side themes that recur across oncology documentation and workflow research (prevalence summarized in Table 4):
These themes and their interrelations are depicted in the conceptual map (Figure 2), highlighting pathways by which documentation features affect concordance/adherence outcomes [1,4,9,10,12,13,14,16,20].
Table 4.
Key clinician side themes and prevalence.
| Theme | % of P2 sources |
|---|---|
| EHR barriers and compliance oriented design (templates, coding, immature UX) [13,14,19] | 47% |
| Incomplete/late documentation (adverse effects, pain, SDOH) [1,9,10,11] | 35% |
| Formal note style / stigmatizing language [4,12,20] | 12% |
| Time/cognitive burden limiting PCC narratives [14,16,18] | (frequent; overlaps with barrier theme) |
Note: Percentages reflect proportions reported in the EHR subset (Table 3). Time/cognitive burden is integral to barrier design and often co-occurs; a single percentage is therefore not reported independently.
3.5. Theme Wise Results
Theme A: Compliance Oriented Design Constrains Person Centred Narratives
Across multi site interviews and workflow studies, clinicians describe template heavy, coding centered interfaces that privilege billing and standardized capture over nuanced narrative documenting of goals, preferences, and teach back confirmations [13,14]. Evidence suggests that limited or fragmented fields for concordance cues (e.g., goals of care rationales) make such information implicit or absent in notes, complicating retrieval and continuity across teams [21,22].
Theme B: Incomplete/Late Documentation of Adverse Effects, Pain, and SDOH
Rule based extraction and data mining analyses show pain as a frequent driver of unplanned care; however, symptom trajectories and supportive care triggers are often inconsistently recorded or delayed in the narrative, risking missed opportunities for early mitigation [9,10]. Palliative oncology notes reveal social distress and spiritual pain detectable in free text but absent in structured data, indicating hidden barriers to adherence when narrative signals are not systematically captured [1].
Theme C: Formal Tone and Stigmatizing Lexicon Undermine Trust and Comprehension
Lexicon driven studies identify stigmatizing language patterns in notes, with potential to transmit bias and alienate patients [12]. Mixed methods analyses in oncology point to benefits of plain language, person centred phrasing for understanding and anxiety reduction, while surveys of portal users indicate that documentation style functions as communication and shapes satisfaction and engagement [4,20,23].
Theme D: Time/Cognitive Burden Reduces Specificity and Explicit Concordance Recording
Audit log reviews document high navigation time, haphazard chart review patterns, and documentation fatigue that favor copy–paste over tailored narratives [14,16]. These pressures contribute to implicit recording of goals/values and fragmented adverse effect capture, reinforcing Theme A’s design constraints and Theme B’s coverage gaps [10,13].
3.6. Linkage to Research Questions
RQ1 (documentation patterns hindering concordance): Themes B and C show that under capture of adverse effects, pain, SDOH and formal orstigmatizing language systematically hinder retrieval of concordance relevant information and erode trust, respectively [1,4,9,10,12,20]. Theme A indicates that compliance driven designs reduce explicit documentation of goals, preferences, and decision rationales [13,14].
RQ2 (optimizing language and workflow): Evidence supports person centred prompts/fields, plain language templates, stigma flagging, and audit log informed workflow redesign to expand narrative space, improve coverage/timing of key constructs, and enhance readability for patients accessing notes [13,14,20,21,23,24].
3.7. Guidance to Figures and Tables
Figure 1 provides the selection flow; Table details corpus characteristics and methods; Table 4 summarizes theme prevalence across the EHR subset; and Figure 2 visualizes how design, coverage/timing, language/style, and workflow burden interact to shape concordance/adherence outcomes [1,4,9,10,12,13,14,16,20,21,22,23,24].
4. Discussion
4.1. Summary of Principal Findings
Across 23 studies of oncology documentation and EHR use, we identified four clinician-side themes tied to concordance and adherence: (1) EHR barriers and compliance-oriented design (template burden, coding-centric workflows), (2)incomplete/late documentation of adverse effects, pain, and social determinants of health, (3) formal note style and occasional stigmatizing language, and (4) time/cognitive burden limiting person-centred narratives [1,4,9,10,12,13,14,16,18,20]. These patterns align with informatics constraints (de-identification, corpus access) that have slowed oncology-specific NLP and sustained reliance on heterogeneous local corpora [5,6,7,8].
4.2. Interpretation in Relation to Communication, Trust, and Concordance
When adverse effects, pain, and SDOH are under-documented, teams miss timely opportunities to mitigate barriers to ongoing therapy [1,9,10]. Note style matters: formal, jargon-heavy, or stigmatizing phrasing can alienate patients, especially where portals expose notes directly [4,12,23]. Conversely, plain-language, stigma-free, and person-centred documentation supports understanding, trust, and participation—determinants consistently linked to adherence [29,30]. Studies classifying serious-illness communication show that goal-concordance cues are detectable in notes yet often remain implicit or absent, risking misalignment between care plans and patient priorities [21,22]. Overall, documentation quality is not merely archival; it is a communication act that shapes concordance.
4.3. Theoretical Framing: Communication, Trust, and Concordance
The findings of this review align with established theories of clinical communication and shared decision-making. According to relational communication theory, the quality of clinician–patient interactions including language tone, transparency, and responsiveness directly influences trust and engagement. When EHR documentation reflects formal, stigmatizing, or impersonal language, it may undermine these relational dynamics, particularly in oncology where patients often face complex, emotionally charged decisions.
Shared decision-making (SDM) frameworks emphasize the co-construction of care plans based on patient values, preferences, and goals. However, our synthesis shows that EHRs often lack structured fields or narrative space to document these elements explicitly. This gap risks misalignment between recorded care plans and actual patient priorities.
In this context, we define treatment concordance as the documented alignment between a patient’s expressed goals, values, and preferences and the treatment plan recorded in the EHR. Concordance is not merely agreement on a clinical decision but includes the rationale, context, and shared understanding that underpin it. Effective concordance documentation requires both structured fields (e.g., goals-of-care checkboxes) and narrative entries that capture nuance, emotion, and evolving preferences.
Improving concordance documentation requires both technical solutions (e.g., NLP-ready templates) and a cultural shift toward communication-enhancing practices.
4.4. Implications for Nursing Practice, Documentation, and Service Design
Based on our findings, we recommend the following practical changes:
4.5. Practical Toolkit and Policy Alignment
To translate the findings of this review into actionable strategies, we propose a practical toolkit for improving EHR documentation in oncology. These recommendations align with the Australian Charter of Healthcare Rights and ACSQHC standards, especially in person-centred care, communication, and partnership.
Table 5.
Toolkit for Enhancing Concordance-Focused EHR Documentation
| Recommendation | Rationale and Policy Alignment |
|---|---|
| Add person-centred prompts and fields (e.g., goals, values, decision rationale) | Supports shared decision-making and aligns with the Charter’s principles of partnership and respect. |
| Use plain-language templates and examples | Enhances patient understanding and trust; aligns with ACSQHC communication standards. |
| Implement stigma-flagging tools (e.g., NLP-based detection of stigmatizing language) | Reduces bias and promotes dignity and respect in documentation. |
| Capture adverse effects, pain, and SDOH using structured and narrative fields | Improves early identification of barriers to adherence; supports safety and access principles. |
| Leverage audit-log data to streamline workflows | Reduces cognitive burden and documentation fatigue; aligns with safety and accountability standards. |
Note: Recommendations are mapped to the Australian Charter of Healthcare Rights (2020) and ACSQHC documentation and communication standards.
4.6. Methodological Reflections and Limitations
EHR corpora vary widely by setting, EHR vendor, and policy; access is constrained by privacy and de-identification, complicating replication and external validity [5,6]. Text-mining pipelines differ in preprocessing, section segmentation, and lexicons; oncology-specific vocabularies for concordance and SDOH remain emergent [7,8]. Our discourse is an analytic synthesis is interpretive and cannot infer causality; observed documentation features may correlate with but not necessarily cause adherence outcomes. Finally, English language restriction and heterogeneity of clinical services may limit generalisability.
While this scoping review identifies key documentation patterns associated with treatment concordance and adherence, it does not establish causality. The generalizability of findings is further constrained by the heterogeneity of EHR systems, institutional practices, and the limited availability of oncology specific, de-identified corpora. Many included studies rely on local datasets or proprietary systems, which may not reflect broader clinical contexts. Additionally, NLP methods varied widely in preprocessing, lexicon use, and classification strategies, with some pipelines lacking transparency or validation across settings. Such inconsistencies hinder cross study comparability and weaken the reliability of synthesized themes. Future research should prioritize standardized ontologies, shared corpora, and reproducible NLP workflows to enhance external validity and translational impact.
4.6.1. Gaps in the Literature and Future Directions
This review highlights several underexplored areas in the current literature. First, many included studies lacked detailed reporting on patient demographics, limiting insights into how documentation practices may differentially affect diverse populations. Few studies broke down findings by age, gender, ethnicity, or cancer type, despite known disparities in communication and adherence. Future research should prioritize inclusion of underrepresented groups and stratified analyses to ensure that documentation improvements benefit all patients equitably.
Second, there is a pressing need for standardized ontologies and shared vocabularies specific to oncology. Current NLP pipelines rely on heterogeneous lexicons, often adapted from general clinical contexts, which may not adequately capture oncology-specific constructs such as treatment concordance, adverse effect trajectories, or social determinants of health (SDOH). The development and adoption of open, validated ontologies for these domains would enhance the comparability, reproducibility, and clinical utility of NLP driven documentation analysis.
Closing these gaps is vital to developing equitable, scalable, and context sensitive documentation practices for person-centred oncology care.
NLP Techniques and Variability.
The included studies employed a range of NLP methods, including rule based extraction [10], machine learning classifiers [1], and n-gram or lexicon-based sentiment analysis [12,15]. However, few studies reported external validation or reproducibility metrics, and preprocessing steps (e.g., section segmentation, negation handling) were inconsistently described. This variability reduces comparability and may introduce bias.
Corpus Characteristics.
Table 6 summarizes corpus features across studies, including note types, corpus size, and language characteristics. Most studies relied on datasets from a single institution that are often with limited diversity in cancer types or patient demographics. The lack of standardized corpora and oncology specific annotation guidelines further constrains generalizability.
Bias and Validation.
Several studies lacked transparency regarding model training data, annotation protocols, or inter-rater reliability. This raises concerns about potential bias, particularly in detecting stigmatizing language or adverse effects, and limits confidence in generalizing findings. Future NLP research in oncology should focus on open-source corpora, multi-site validation, and standardized evaluation metrics to strengthen methodological rigor.
4.7. Future Research
We highlight four priorities:
- 1.
- 2.
- 3.
- 4.
5. Conclusions
Documentation quality in oncology is a modifiable determinant of communication, concordance, and adherence. This review identified four clinician-side barriers design constraints, incomplete documentation, formal or stigmatizing language, and workflow burden that limit the recording and retrieval of person-centred information.
By addressing these barriers through person-centred prompts, stigma-free language, improved capture of adverse effects and SDOH, and workflow redesign, nursing and service leaders can enhance trust, engagement, and continuity of care. These strategies directly support the principles of shared decision-making and align with national safety and quality standards.
Our findings respond to both research questions: they identify documentation patterns that hinder concordance and propose actionable design and language interventions to improve adherence outcomes. Future research should focus on scalable implementation, equity in documentation practices, and co-design with patients.
Author Contributions
Conceptualization, L.W.; methodology, L.W., R.G. and X.Z; formal analysis, L.W.; investigation, L.W; writing—original draft preparation, L.W; writing—review and editing, L.W., R.G. and X.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any funding.
Institutional Review Board Statement
Ethical review was not needed for this study.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Public Involvement Statement
There was no public involvement in any aspect of this research.
Guidelines and Standards Statement
This manuscript was drafted against the PRISMA-ScR checklist for reporting of scoping reviews.
Use of Artificial Intelligence
Generative AI tools were not used in drafting this manuscript. However, the study relies on AI-based analytical methods such as Natural Language Processing (NLP) and sentiment analysis to examine patient-generated narratives. Existing AI tools were employed strictly for data analysis, not for content creation.
References
- Masukawa, K.; Aoyama, M.; Yokota, S.; Nakamura, J.; Ishida, R.; Nakayama, M.; Miyashita, M. Machine learning models to detect social distress, spiritual pain, and severe physical psychological symptoms in terminally ill patients with cancer from unstructured text data in electronic medical records. Palliative Medicine 2022, 36(8), 1207–1216. [Google Scholar] [CrossRef] [PubMed]
- Percha, B. Modern Clinical Text Mining: A Guide and Review. Annual Review of Biomedical Data Science 2021, 4(1), 165–187. [Google Scholar] [CrossRef]
- Sikorskii, A.; Wyatt, G.; Tamkus, D.; Victorson, D.; Rahbar, M. H.; Ahn, S. Concordance between patient reports of cancer-related symptoms and medical records documentation. J Pain Symptom Manage 2012, 44(3), 362–372. [Google Scholar] [CrossRef]
- Alpert, J. M.; Morris, B. B.; Thomson, M. D.; Matin, K.; Sabo, R. T.; Brown, R. F. Patient access to clinical notes in oncology: A mixed method analysis of oncologists’ attitudes and linguistic characteristics towards notes. Patient Educ Couns 2019, 102(10), 1917–1924. [Google Scholar] [CrossRef]
- Chapman, W.; Nadkarni, P.; Hirschman, L.; D’Avolio, L.; Savova, G.; Uzuner, O. Overcoming barriers to NLP for clinical text: the role of shared tasks and the need for additional creative solutions; Journal of the American Medical Informatics Association: JAMIA, 2011; pp. 540–543. [Google Scholar] [CrossRef]
- Johnson, A.; Pollard, T.; Horng, S.; Anthony, L.; Mark, R. MIMIC-IV-Note: Deidentified free-text clinical notes. PhysioNet 2023, Version 2.2. [Google Scholar] [CrossRef]
- Zeng, J.; Banerjee, I.; Henry, A. S.; Wood, D. J. Natural Language Processing to Identify Cancer Treatments With Electronic Medical Records. JCO: Clinical Cancer Informatics 2021, 5. [Google Scholar] [CrossRef]
- Gholipour, M.; Khajouei, R.; Amiri, P.; Hajesmaeel Gohari, S.; Ahmadian, L. Extracting cancer concepts from clinical notes using natural language processing: a systematic review. BMC Bioinformatics 2023, 24. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C. C.; Wang, H. H.; Tseng, L. P. Using data mining technology to predict medication-taking behaviour in women with breast cancer: A retrospective study. Nurs Open 2022, 9(6), 2646–2656. [Google Scholar] [CrossRef]
- Tamang, S.; Patel, M.; Blayney, D.; Kuznetsov, J.; Finlayson, S.; Vetteth, Y. Detecting unplanned care from clinician notes in electronic health records. J Oncol Pract 2015, 11, e313–e319. [Google Scholar] [CrossRef] [PubMed]
- Cho, J. E.; Tang, N.; Pitaro, N.; Bai, H.; Cooke, P. V.; Arvind, V. Sentiment Analysis of Online Patient-Written Reviews of Vascular Surgeons. Ann Vasc Surg 2023, 88, 249–255. [Google Scholar] [CrossRef]
- Himmelstein, G.; Bates, D.; Zhou, L. Examination of Stigmatizing Language in the Electronic Health Record. JAMA Network Open 2022, 5(1), e2144967. [Google Scholar] [CrossRef]
- Patel, M. R.; Friese, C. R.; Mendelsohn-Victor, K.; Fauer, A. J.; Ghosh, B.; Bedard, L.; Griggs, J. J.; Manojlovich, M. Clinician Perspectives on Electronic Health Records, Communication, and Patient Safety Across Diverse Medical Oncology Practices. Journal of Oncology Practice 2019, 15(6), e529–e536. [Google Scholar] [CrossRef]
- Huilgol, Y. S.; Adler-Milstein, J.; Ivey, S. L.; Hong, J. C. Opportunities to use electronic health record audit logs to improve cancer care. Cancer Medicine 2022, 11(17), 3296–3303. [Google Scholar] [CrossRef]
- Rahimian, M.; Warner, J.; Jain, S.; Davis, R.; Zerillo, J.; Joyce, R. Significant and Distinctive n-Grams in Oncology Notes: A Text-Mining Method to Analyze the Effect of OpenNotes on Clinical Documentation. JCO Clin Cancer Inform 2019, 3, 1–9. [Google Scholar] [CrossRef]
- Warner, J.; Hochberg, E. Where is the EHR in oncology? J Natl Compr Canc Netw 2012, 10(5), 584–588. [Google Scholar] [CrossRef]
- Asan, O.; Nattinger, A. B.; Gurses, A. P.; Tyszka, J. T.; Yen, T. W. F. Oncologists’ Views Regarding the Role of Electronic Health Records in Care Coordination. JCO Clinical Cancer Informatics 2018, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Burke, H. B. Standardized Documentation Is Not the Solution to Reduce Physician Time in the Electronic Health Record. JAMA Oncology 2023, 9(8), 1151–1152. [Google Scholar] [CrossRef]
- Geskey, J. M.; Kodish-Wachs, J.; Blonsky, H.; Hohman, S. F.; Meurer, S. National Documentation and Coding Practices of Noncompliance: The Importance of Social Determinants of Health and the Stigma of African-American Bias. Am J Med Qual 2023, 38(2), 87–92. [Google Scholar] [CrossRef] [PubMed]
- Heckemann, B.; Chaaya, M.; Jakobsson Ung, E.; Olsson, D. S.; Jakobsson, S. Finding the Person in Electronic Health Records. A Mixed-Methods Analysis of Person-Centered Content and Language. Health Communication 2022, 37(4), 418–424. [Google Scholar] [CrossRef] [PubMed]
- Davoudi, A.; Tissot, H.; Doucette, A.; et al. Using Natural Language Processing to Classify Serious Illness Communication with Oncology Patients. AMIA Jt Summits Transl Sci Proc 2022, 168–177. [Google Scholar] [PubMed Central]
- Geerse, O. P.; Lamas, D. J.; Bernacki, R. E.; Sanders, J. J.; Paladino, J.; Berendsen, A. J.; Hiltermann, T. J. N.; Lindvall, C.; Fromme, E. K.; Block, S. D. Adherence and Concordance between Serious Illness Care Planning Conversations and Oncology Clinician Documentation among Patients with Advanced Cancer. J Palliat Med 2021, 24(1), 53–62. [Google Scholar] [CrossRef]
- Rexhepi, H.; Moll, J.; Huvila, I. Online electronic healthcare records: Comparing the views of cancer patients and others. Health Informatics Journal 2020, 26(4), 2915–2929. [Google Scholar] [CrossRef]
- Griffin, J. M.; Kroner, B. L.; Wong, S. L.; Preiss, L.; Wilder Smith, A.; Cheville, A. L.; Mitchell, S. A.; Lancki, N.; Hassett, M. J.; Schrag, D.; Osarogiagbon, R. U.; Ridgeway, J. L.; Cella, D.; Jensen, R. E.; Flores, A. M.; Austin, J. D.; Yanez, B. Disparities in electronic health record portal access and use among patients with cancer. J Natl Cancer Inst 2024, 116(3), 476–484. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Moralejo, D.; Ogunremi, T.; Dunn, K. Critical Appraisal Toolkit (CAT) for assessing multiple types of evidence. Can Commun Dis Rep 2017, 43(9), 176–181. [Google Scholar] [CrossRef]
- Skeat, J.; Roddam, H. The qual-CAT:Applying a rapid review approach to qualitative research to support clinical decision-making in speech-language pathology practice. Evidence-Based Communication Assessment and Intervention 2019, 13(1-2), 3–14. [Google Scholar] [CrossRef]
- CASP. Critical Appraisal Skills Programme. In CASP UK - OAP Ltd; 2023; Available online: https://casp-uk.net/casp-tools-checklists/.
- Hillen, M. A.; de Haes, H. C. J. M.; Stalpers, L. J. A.; Klinkenbijl, J. H. G.; Eddes, E. H.; Butow, P. N.; van der Vloodt, J.; van Laarhoven, H. W. M.; Smets, E. M. A. How can communication by oncologists enhance patients’ trust? An experimental study. Annals of Oncology 2014, 25(4), 896–901. [Google Scholar] [CrossRef] [PubMed]
- Zolnierek, K. B.; Dimatteo, M. R. Physician communication and patient adherence to treatment: a meta-analysis. Med Care 2009, 47(8), 826–834. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care. Australian Charter of Healthcare Rights (Second Edition). ACSQHC . 2020. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/australian-charter-healthcare-rights-second-edition-a4-accessible.
- Ahmad, B.; Jun, S. Sentiment Analysis of Cancer Patients About Their Treatment During the Peak Time of Pandemic COVID-19. 2021 4th International Conference on Computing and Information Sciences (ICCIS), 2021; pp. 29–30 Nov. [Google Scholar] [CrossRef]
- Amossy, R. Argumentation in Discourse: A Socio-discursive Approach to Arguments. Informal Logic 2009, 29, 252–267. [Google Scholar] [CrossRef]
- An, Y.; Fang, Q.; Wang, L. Enhancing patient education in cancer care: Intelligent cancer patient education model for effective communication. Computers in Biology and Medicine 2024, 169, 107874. [Google Scholar] [CrossRef]
- Arditi, D.; Gilles, I.; Lesage, S.; Griesser, A.-C.; Bienvenu, C.; et al. Computer-assisted textual analysis of free-text comments in the Swiss Cancer Patient Experiences (SCAPE) survey. BMC Health Serv Res 2020, 20, 1029. [Google Scholar] [CrossRef] [PubMed]
- Simoulin, A.; Thiebaut, N.; Neuberger, K.; Ibnouhsein, I.; Brunel, N.; Viné, R.; Bousquet, N.; Latapy, J.; Reix, N.; Molière, S.; Lodi, M.; Mathelin, C. From free-text electronic health records to structured cohorts: Onconum, an innovative methodology for real-world data mining in breast cancer. Computer Methods and Programs in Biomedicine 2023, 240, 107693. [Google Scholar] [CrossRef]
- Xin, J.; Hjaltelin, J.X.; Novitski, S.I.; Jørgensen, I.F.; Siggaard, T.; Vulpius, S.A.; Westergaard, D.; Johansen, J.S.; Chen, I.M.; Jensen, L.J.; Brunak, S. Pancreatic cancer symptom trajectories from Danish registry data and free text in electronic health records. eLife 2023, 12, e84919. [Google Scholar] [CrossRef] [PubMed]
- Elbers, D.C.; La, J.; Minot, J.R.; Gramling, R.; Brophy, M.T.; Do, N.V.; Fillmore, N.R.; Dodds, P.S.; Danforth, C.M. Sentiment analysis of medical record notes for lung cancer patients at the Department of Veterans Affairs. PLOS ONE 2023, 18(1), e0280931. [Google Scholar] [CrossRef] [PubMed]
- Leis, A.; Casadevall, D.; Albanell, J.; Posso, M.; Macià, F.; Castells, X.; Ramírez-Anguita, J.M.; Martínez Roldán, J.; Furlong, L.I.; Sanz, F.; Ronzano, F.; Mayer, M.A. Exploring the Association of Cancer and Depression in Electronic Health Records: Combining Encoded Diagnosis and Mining Free-Text Clinical Notes. JMIR Cancer 2022, 8(3), e39003. [Google Scholar] [CrossRef]
- Mashima, Y.; Tamura, T.; Kunikata, J.; Tada, S.; Yamada, A.; Tanigawa, M.; Hayakawa, A.; Tanabe, H.; Yokoi, H. Using Natural Language Processing Techniques to Detect Adverse Events From Progress Notes Due to Chemotherapy. Cancer Informatics 2022, 21, 11769351221085064. [Google Scholar] [CrossRef]
- Jensen, K.; Soguero-Ruiz, C.; Mikalsen, K.Ø.; Lindsetmo, R.-O.; Kouskoumvekaki, I.; Girolami, M.; Skrovseth, S.O.; Augestad, K.M. Analysis of free text in electronic health records for identification of cancer patient trajectories. Scientific Reports 2017, 7, 46226. [Google Scholar] [CrossRef]
- Feldman, K.; Hazekamp, N.; Chawla, N.V. Mining the Clinical Narrative: All Text Are Not Equal. 2016 IEEE International Conference on Healthcare Informatics (ICHI), 2016; pp. 306–314. [Google Scholar] [CrossRef]
- Ganesan, K.; Lloyd, S.; Sarkar, V. Discovering Related Clinical Concepts Using Large Amounts of Clinical Notes. Biomedical Engineering and Computational Biology 2016, 7 (Suppl 2), 27–33. [Google Scholar] [CrossRef]
- Falotico, R.; Liberati, C.; Zappa, P. Identifying Oncological Patient Information Needs to Improve e-Health Communication: a preliminary text-mining analysis. Quality and Reliability Engineering International 2015, 31(7), 1115–1126. [Google Scholar] [CrossRef]
- Hamid, M.S.; Valicevic, A.; Brenneman, B.; Niziol, L.M.; Stein, J.D.; Newman-Casey, P.A. Text Parsing-Based Identification of Patients with Poor Glaucoma Medication Adherence in the Electronic Health Record. American Journal of Ophthalmology 2020, 222, 54–59. [Google Scholar] [CrossRef]
- Zhu, V.J.; Lenert, L.A.; Bunnell, B.E.; Obeid, J.S.; Jefferson, M.; Hughes Halbert, C. Automatically identifying social isolation from clinical narratives for patients with prostate cancer. BMC Medical Informatics and Decision Making 2019, 19, 43. [Google Scholar] [CrossRef] [PubMed]
- Datta, S.; Bernstam, E.V.; Roberts, K. A frame semantic overview of NLP-based information extraction for cancer-related EHR notes. Journal of Biomedical Informatics 2019, 100, 103301. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA Flow Diagram [25].
Figure 1.
PRISMA Flow Diagram [25].
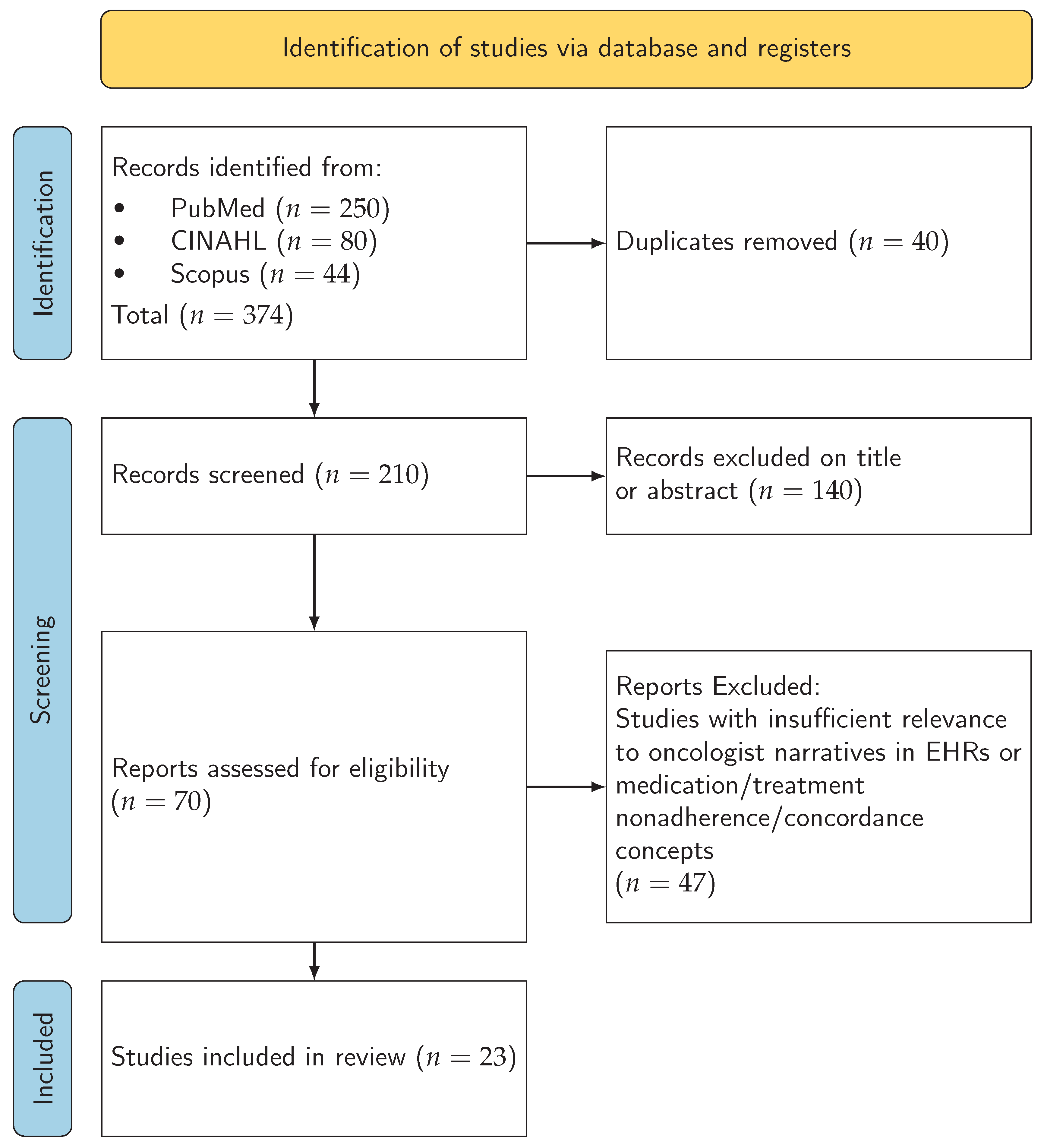
Figure 2.
Conceptual links between EHR determinants and clinician-side themes (barriers, coverage/timing, language/style, workflow burden) and their effects on concordance/adherence outcomes [1,4,9,10,12,13,14,16,20]; bridging constructs: [21,22,23,24]).
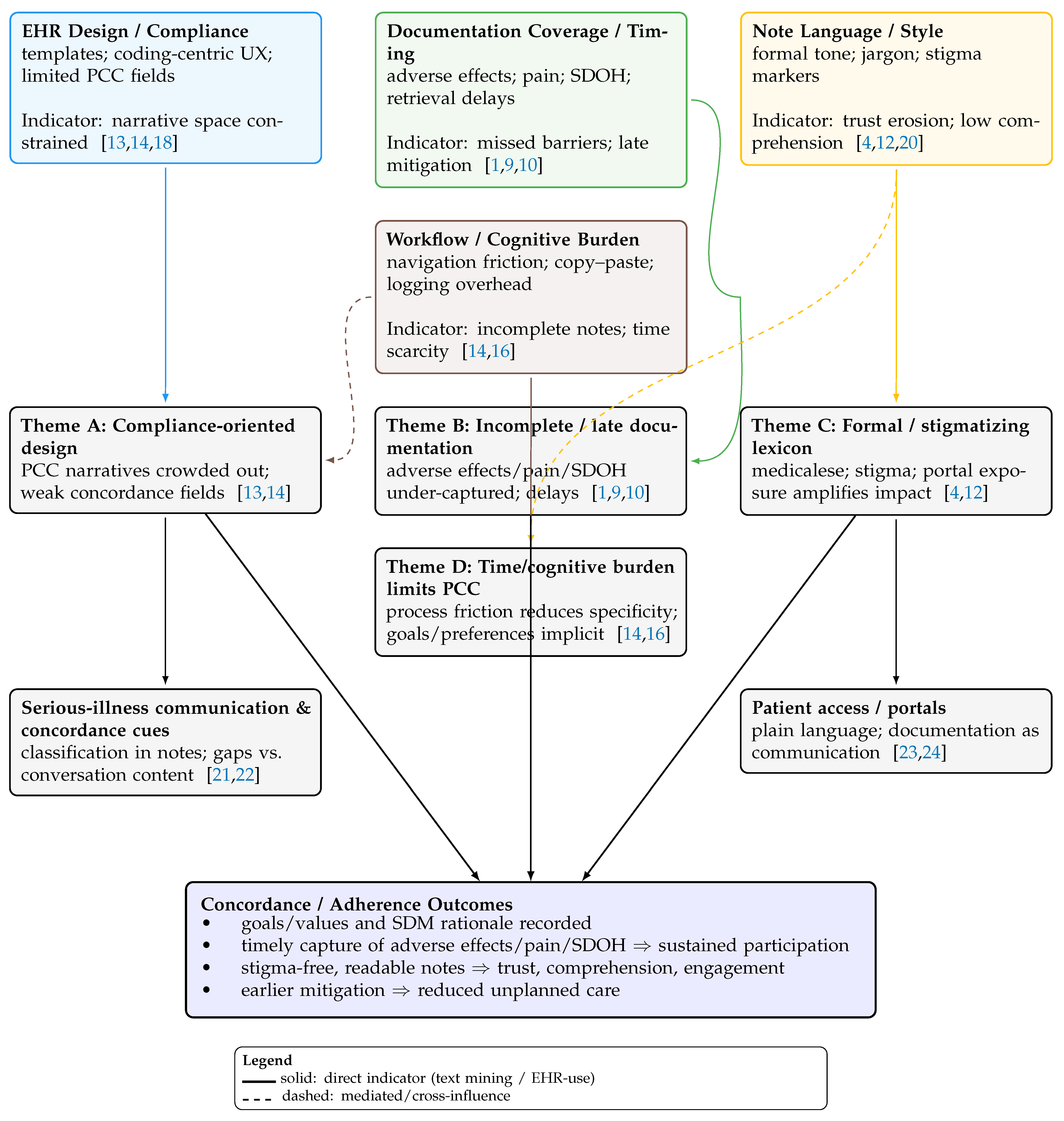
Table 6.
Summary of corpus characteristics in included studies.
| Study | Corpus Size | Note Types | Language Features |
|---|---|---|---|
| Masukawa et al. (2022) [1] | 1,200 | Palliative care notes | Japanese; spiritual pain terms |
| Tamang et al. (2015) [10] | 5,000+ | Progress notes | Pain-related expressions |
| Himmelstein et al. (2022) [12] | 10,000+ | Admission notes | Stigma lexicon, U.S. English |
| Rahimian et al. (2019) [15] | 3,000 | Oncology notes (OpenNotes) | n-gram frequency, formal tone |
| Heckemann et al. (2022) [20] | 500 | Discharge letters | Person-centred phrasing |
Note: Corpus sizes and note types vary widely across studies. Language features reflect the primary focus of each study’s NLP or linguistic analysis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



