
Submitted:
16 April 2025
Posted:
18 April 2025
You are already at the latest version
Abstract
Clinician notes are a rich source of patient information but often contain inconsistencies due to varied writing styles, abbreviations, medical jargon, grammatical errors, and non-standard formatting. These inconsistencies hinder the meaningful extraction of data from electronic health records, limiting their utility for quality improvement, population health, precision medicine, decision support, and research. We present a large language model approach to standardizing a corpus of 1,618 clinical notes. Standardization corrected grammatical and spelling errors, converted non-standard terms to standardized terminology, and expanded abbreviations and acronyms. Notes were also restructured using consistent section headings. Expert review of randomly sampled notes found no significant information loss. The F1 score for Human Phenotype Ontology concept extraction increased from 0.40 to 0.61 following standardization, indicating improved accuracy without sacrificing clinical content. We conclude that standardizing physician notes enhances their usability for downstream applications such as clinical care, concept extraction, exploratory data analysis, and data exchange.
Keywords:
electronic health records
; physician notes
; standardization
; human phenotype ontology
; doc2hpo
; large language models
; data interoperability
; concept extraction
1. Introduction
Electronic Health Records (EHRs) have transformed healthcare documentation by improving the legibility and availability of patient data [1]. They solved the “availability problem”—where paper charts were often inaccessible—and the “legibility problem” of handwritten notes [2,3,4]. Yet, physician dissatisfaction with EHRs remains high, driven by poor interface design, excessive documentation burden, clerical overload, and limited perceived benefit for patient care [5,6,7,8,9,10,11,12].
Since the release of ChatGPT in late 2022, interest in large language models (LLMs) has surged in healthcare [13,14,15,16,17]. LLMs are now being explored for a range of clinical applications: decision support, diagnosis explanation, summarization, concept extraction, ontology mapping, and transforming documents into interoperable formats [18,19,20,21,22,23]. Among these, LLM-based clinical note standardization holds special promise for improving note quality and downstream reusability. Some recent surveys show increasing physician satisfaction with EHRs due to improvements referable to AI [24]/
We define standardization as the process of improving the structural and linguistic integrity of a clinical note without altering its clinical meaning. This includes correcting spelling and grammar, replacing colloquialisms with standardized terms (e.g., upgoing toe →Babinski sign), expanding abbreviations (e.g., OU→ both eyes), and enforcing consistent formatting and section headers.
Clinical notes are typically written through direct entry, dictation, copy-paste, or auto-insertion of structured fields. As a result, they often suffer from inconsistent structure, misspellings, excessive abbreviations, slang, and ambiguous terminology [25,26,27,28,29,30]. Up to 20% of note content may be abbreviations or acronyms [31,32,33,34,35,36,37,38]. Moreover, many notes lack machine-readable codes (e.g., ICD-11, SNOMED CT, LOINC, RxNorm) and are poorly formatted or excessively verbose [39,40,41,42].
LLMs can help address these limitations by:
- Expanding abbreviations based on context (e.g., MS” → multiple sclerosis’’ or mental status”).
- Correcting typographical and grammatical errors to improve clarity [43].
- Replacing colloquialisms and dictation artifacts with standardized terminology (e.g., heart attack’’ → “myocardial infarction’’) [44].
- Structuring notes into canonical sections (e.g., History, Examination, Impression, Plan) to enhance navigability.
These improvements (Figure 1) can:
- Enhance the readability and clinical utility of notes.
- Improve the accuracy of pipelines that extract and normalize medical concepts to standard ontologies.
2. Methods
This study evaluates the effectiveness of GPT-4 in standardizing 1,618 de-identified clinical notes from a Neurology Clinic. We hypothesize that standardization will improve structural consistency, linguistic clarity, and the extractability of clinical concepts, thereby enhancing downstream applications such as ontology-based normalization, natural language processing (NLP), and data interoperability.
The evaluation framework (Figure 2) compares concept extraction accuracy under three conditions: from raw notes, from GPT-4-standardized notes, and from ground truth phrases. We define concept extraction as identifying relevant clinical terms or phrases in free text. Concept normalizationrefers to mapping each extracted term to a standardized ontology concept with its corresponding identifier. Notably, correct identification of a term does not guarantee accurate normalization, as models may capture semantic meaning without retrieving the correct machine-readable code [49,50,51,52,53,54,55].
Data Acquisition: Institutional Review Board (IRB) approval was obtained from the University of Illinois to use de-identified clinical notes from the Neurology Clinic. All notes were de-identified using REDCap [56]. We selected notes containing neuroimmunological diagnoses, including multiple sclerosis, myasthenia gravis, neuromyelitis optica, and Guillain–Barré syndrome. From an initial pool of 21,028 notes (2016–2022), a subset meeting the following inclusion criteria was selected: (1) outpatient visits, (2) authored in the Neurology Clinic, (3) written by physicians (residents or attendings), and (4) minimum note length of 2,000 characters. The final dataset comprised 1,618 typed notes exported as ASCII text and stored in a JSON-compatible format (Figure 3).
Note Standardization: GPT-4o (Open AI) was prompted to standardize neurology notes (Appendix A) into a standard format (Appendix B). GPT-4 produced a detailed list of all modifications for each note (Appendix C). Character count, word count, sentence count, spelling and grammar corrections, abbreviation expansion, and word substitutions were calculated for each note (Figure 4). To evaluate fidelity, 100 randomly selected note pairs were manually reviewed to ensure no clinically significant information was omitted and to screen for any spurious additions, such as hallucinations or confabulations.
Concept Extraction Using doc2hpo: We used the open-source Python implementation of doc2hpo [57], executed locally with the Aho-Corasick string-matching algorithm and a custom negation detection module (`NegationDetector`) that applies a windowed keyword search within sentence boundaries. We used the HPO release dated 2025-03-03. No modifications were made to the doc2hpo source code. doc2hpo was applied under three conditions:
- Raw notes (unmodified exports from REDCap),
- Standardized notes (post-GPT-4 processing),
- Ground truth phrases (GPT-4 extracted candidate HPO terms).
For the ground truth, GPT-4 was prompted to identify all candidate HPO-eligible phrases in each note (Appendix D). These phrases were combined into a single synthetic sentence for doc2hpo input (e.g., “The patient has ataxia, weakness, aphasia, and hyperreflexia.”). doc2hpo returned a list of matched terms and corresponding HPO IDs. For each of the 1,618 notes, we compiled three term sets:
- Ground truth terms: GPT-4 extracted phrases successfully matched by doc2hpo.
- Raw-note terms: doc2hpo output from raw notes.
- Standardized-note terms: doc2hpo output from standardized notes.
Metric Computation: For each extracted term, we classified its match status as follows:
- True Positive (TP): Term present in both the extracted set and the ground truth set.
- False Negative (FN): Ground truth term not captured in extraction set.
- False Positive (FP): Term extracted but not part of ground truth set.
- True Negative (TN): Term present in the note but not successfully mapped to HPO by doc2hpo.
Performance metrics (precision, recall, accuracy, and F1 score) were calculated by the method of Powers [58].
3. Results and Discussion
3.1. Note Standardization Improves Structure and Readability
We used GPT-4 to standardize 1,618 de-identified clinical notes from a neurology clinic. Each note was converted from plaintext to a structured JSON format with high-level section headers (e.g., History, Examination, Impression, Plan). GPT-4 was prompted to standardize each note by correcting spelling and grammatical errors, expanding acronyms and abbreviations, and replacing non-standard phrasing (Appendix E). GPT-4 corrected and average of 4.9 ± 1.8 grammatical errors, 3.3 ± 5.2 spelling errors, and expanded 12.6 ± 8.1 abbreviations or acronyms per note. Additionally, it substituted standardized clinical terminology for 3.1 ± 3.0 instances of jargon or non-standard language. A manual review of 100 randomly selected notes confirmed the preservation of clinical content, with improvements in clarity, structure, and overall readability. No hallucinations or spurious additions were identified during human expert review.
3.2. Standardization Improves HPO Term Extraction by doc2hpo
To evaluate whether GPT-4-based standardization improves phenotype term extraction, we compared three parallel data flows:
- Raw Notes → doc2hpo → Raw Terms
- Standardized Notes → doc2hpo → Standardized Terms
- GPT-4 Extracted Phrases → doc2hpo → Ground Truth Terms
All extracted terms were mapped to the HPO using doc2hpo. The ground truth was defined as HPO terms extracted by doc2hpo from GPT-4-supplied candidate phrases. For each note, term sets from the raw and standardized notes were evaluated against the corresponding ground truth set using standard classification metrics: precision, recall, accuracy, and F1 score.
GPT-4-standardized notes yielded higher precision and accuracy compared to raw notes. Recall also improved, rising from 0.61 to 0.68. Although modest in absolute terms, this gain was statistically significant due to the large sample size (n = 1,618) and contributed to a measurable improvement in F1 score (Figure 3). The combined improvements suggest that GPT-4 preprocessing enhances overall extraction performance without sacrificing sensitivity. The simultaneous increase in both precision and recall indicates that GPT-4 did not introduce spurious terms or omit clinically relevant information. These results support the hypothesis that physician note standardization by LLMs improves the performance of NLP pipelines performing ontology-term normalization.
3.3. Downstream Use Cases After Note Standardization
Once physician notes are standardized by a large language model, several downstream applications become feasible (Figure 1):
- Standardized notes can be integrated in real time into the EHR to enhance note quality, readability, and clinical interpretability.
- Extracted terms can be passed into NLP pipelines that map these terms to ontology concepts, making clinical data computable for exploratory analysis, machine learning, population health, and quality improvement.
3.4. Addressing Systemic Challenges in EHR Documentation
While large language models improve note structure and readability, systemic challenges in EHR documentation remain. Copy-and-paste practices, unverified carry-forward data, and documentation that omits or exaggerates care are beyond the scope of current AI tools [62,63,64]. Standardization alone does not reduce documentation burden, which is more fundamentally tied to EHR design, clinician workflows, and organizational practices [10,65,66,67]. Promising technologies like ambient AI may help, but broader reforms are needed to address who documents, what is documented, and how. Encouragingly, recent surveys suggest that the introduction of AI tools is already improving physician satisfaction with the EHR [24].
3.5. Limitations
This study analyzed 1,618 de-identified neurology notes, primarily from patients with multiple sclerosis. Broader validation across diverse diagnoses, note types, and clinical settings is needed. Ground truth medical concepts were identified using GPT-4 with human expert review. While this approach enabled scalable evaluation, future work should incorporate fully manual annotation for comparison. We did not assess the processing time or computational costs of standardization. Although deploying LLMs in production may incur costs, many institutions are actively exploring this path [61,68]. De-identification ensured HIPAA compliance, but explicit consent from clinicians and patients was not obtained. In active clinical environments, reconfiguration of notes may require additional safeguards or institutional approval. Nevertheless, our results support the growing interest in note reconfiguration, template engineering, and documentation quality. Once digitized, clinical text can be adapted to multiple formats, enhancing interoperability and downstream utility [61,69,70,71,72].
4. Conclusions
Standardizing physician notes with large language models improves their readability, consistency, and interoperability without loss of clinical content. In this study, GPT-4 enhanced note structure, corrected errors, and expanded abbreviations, facilitating more accurate extraction and normalization of medical concepts by doc2hpo. These findings suggest that LLMs can augment both clinical and research workflows by making unstructured text more usable for downstream NLP and ontology-based analysis. As adoption grows, early evidence indicates that such tools may also contribute to improved physician satisfaction with electronic health records [24].
Author Contributions
Conceptualization, All authors; Methodology, D.B.H. and T.O.; Software, D.B.H.; Validation, all authors; Formal analysis, D.B.H. and T.O.; Investigation and data acquisition, M.A.C.; Data curation, D.B.H. and M.A.C.; Writing—original draft preparation, D.B.H.; Writing—review and editing, all authors; Visualization, D.B.H. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported in part by the National Science Foundation under Award Number 2423235.
Institutional Review Board Statement
The use of EHR clinical notes for research was approved by the IRB of the University of Illinois (Protocol 2017-0520Z).
Informed Consent Statement
Informed consent was obtained from all participants as part of enrollment in the UIC Neuroimmunology Biobank.
Data Availability Statement
Data and code supporting this study are available from the corresponding author on request.
Acknowledgments
We thank the UIC Neuroimmunology BioBank Team for their support.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Prompt to GPT-4 to Standardize a Physician Note
You are a highly skilled medical terminologist
specializing in clinical note standardization.
Your task is to standardize the note using the following rules:
1. Expand abbreviations (e.g., BP blood pressure),
retaining common abbreviations in parentheses.
2. Correct spelling and grammar while preserving meaning.
3. Reorganize content under the following headings:
History, Vital Signs, Examination, Labs, Radiology,
Impression, and Plan.
4. Replace non-standard terms with standard clinical terminology.
Appendix B. Note Format Used by GPT-4 for Standardized Notes
{
"HISTORY": {
"Chief Complaint": "...",
"Interim History": "..."
},
"VITAL SIGNS": {
"Blood Pressure": "...",
"Pulse": "...",
"Temperature": "...",
"Weight": "..."
},
"EXAMINATION": {
"Mental Status": "...",
"Cranial Nerves": "...",
"Motor": "...",
"Sensory": "...",
"Reflexes": "...",
"Coordination": "...",
"Gait and Station": "..."
},
"LABS": "...",
"RADIOLOGY": "...",
"IMPRESSION": {
"Assessment": "..."
},
"PLAN": {
"Testing": "...",
"Education Provided": {
"Instructions": "...",
"Barriers to Learning": "...",
"Content": "...",
"Outcome": "..."
},
"Return Visit": "..."
},
"Metrics": {
"Grammatical Errors": n,
"Abbreviations and Acronyms Expanded": ["..."],
"Spelling Errors": ["..."],
"Non-Standard Terms Corrected": ["..."]
}
}
Appendix C. Example of Corrections Made by GPT-4
"Abbreviations Expanded": [
"BP", "IVIG", "MRI", "EMG", "PT", "OTC", "OT", "CSF",
"WBC", "RBC", "HSV", "PCR", "CIDP", "INCAT", "BPD",
"CBD", "BSA", "FPL", "EHL", "FN", "PA"
],
"Spelling Errors Corrected": [
"wreight", "materal", "unknwon", "schizphernia", "tjhan"
],
"Non-Standard Terms Mapped": [
"heart attack -> myocardial infarction"
]
Appendix D. Prompt to GPT-4 to Identify Ground Truth Terms
You are an expert medical coder with expertise in medical
terminologies such as the Human Phenotype Ontology (HPO).
From the note text {note_text}, extract all potential HPO terms
the patient may have. Return a JSON object with a list of
extracted terms under the key "hpo_terms".
Use this exact format:
{
"hpo_terms": ["term1", "term2", "term3"]
}
Appendix E. Sample Neurological Examinations: Before and After Standardization
Neurological Examination Prior to Standardization. Expanded terms are highlighted in blue.
Neurologic:
Mental status : awake , alert , oriented to person ,
place , and time. Follows commands briskly ,
including 2 step commands. Naming and repetition intact.
Fluent speech with no dysarthria.
Cranial nerves : \textcolor[rgb]{0,0,1}{PERRL} , no \textcolor[rgb]{0,0,1}{rAPD} ,
unable to perform full \textcolor[rgb]{0,0,1}{L}
lateral gaze but otherwise \textcolor[rgb]{0,0,1}{EOMI} , facial sensation full
and symmetric , smile full and symmetric , palate and
uvula elevate symmetrically , shoulder shrug intact ,
tongue midline
...continues....
Neurological Examination After Standardization by GPT-4.
EXAMINATION:
Mental Status: Awake, alert, oriented to person, place,
and time. Follows commands briskly, including
two-step commands. Naming and repetition intact.
Fluent speech with no dysarthria.
Cranial Nerves: Pupils equal, round, and reactive
to light, no relative afferent pupillary
defect, unable to perform full left lateral gaze but
otherwise extraocular movements are intact,
facial sensation full and symmetric,
smile full and symmetric, palate and uvula elevate
symmetrically, shoulder shrug intact, tongue midline
...continues....
Appendix F. Abbreviations
The following abbreviations are used in this manuscript:
| API | Application Programming Interface |
| ASCII | American Standard Code for Information Interchange |
| EHR | Electronic Health Record |
| FHIR | Fast Healthcare Interoperability Resources |
| HIPAA | Health Insurance Portability and Accountability Act |
| HPO | Human Phenotype Ontology |
| ICD | International Classification of Diseases |
| IRB | Institutional Review Board |
| JSON | JavaScript Object Notation |
| LLM | Large Language Model |
| LOINC | Logical Observation Identifiers Names and Codes |
| NLP | Natural Language Processing |
| REDCap | Research Electronic Data Capture |
| RxNorm | Standardized Nomenclature for Clinical Drugs |
| TP/FN/FP/TN | True Positive / False Negative / False Positive / True Negative |
References
- Menachemi, N.; Collum, T.H. Benefits and drawbacks of electronic health record systems. Risk Management and Healthcare Policy 2011, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Bruner, A.; Kasdan, M.L. Handwriting errors: harmful, wasteful and preventable. Journal-Kentucky Medical Association 2001, 99, 189–192. [Google Scholar]
- Kozak, E.A.; Dittus, R.S.; Smith, W.R.; Fitzgerald, J.F.; Langfeld, C.D. Deciphering the physician note. Journal of General Internal Medicine 1994, 9, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Vera, F.J.; Marin, Y.; Sanchez, A.; Borrachero, C.; Pujol, E. Illegible handwriting in medical records. Journal of the Royal Society of Medicine 2002, 95, 545–546. [Google Scholar] [CrossRef]
- Holmgren, A.J.; Hendrix, N.; Maisel, N.; Everson, J.; Bazemore, A.; Rotenstein, L.; Phillips, R.L.; Adler-Milstein, J. Electronic health record usability, satisfaction, and burnout for family physicians. JAMA Network Open 2024, 7, e2426956–e2426956. [Google Scholar] [CrossRef]
- Muhiyaddin, R.; Elfadl, A.; Mohamed, E.; Shah, Z.; Alam, T.; Abd-Alrazaq, A.; Househ, M. Electronic health records and physician burnout: a scoping review. Informatics and Technology in Clinical Care and Public Health 2022, 481–484. [Google Scholar]
- Downing, N.L.; Bates, D.W.; Longhurst, C.A. Physician burnout in the electronic health record era: are we ignoring the real cause? Annals of Internal Medicine 2018, 169, 50–51. [Google Scholar] [CrossRef]
- Elliott, M.; Padua, M.; Schwenk, T.L. Electronic health records, medical practice problems, and physician distress. International Journal of Behavioral Medicine 2022, 1–6. [Google Scholar] [CrossRef]
- Carroll, A.E. How health information technology is failing to achieve its full potential. JAMA Pediatrics 2015, 169, 201–202. [Google Scholar] [CrossRef]
- Rodríguez-Fernández, J.M.; Loeb, J.A.; Hier, D.B. It’s time to change our documentation philosophy: writing better neurology notes without the burnout. Frontiers in Digital Health 2022, 4, 1063141. [Google Scholar] [CrossRef]
- Koopman, R.J.; Steege, L.M.B.; Moore, J.L.; Clarke, M.A.; Canfield, S.M.; Kim, M.S.; Belden, J.L. Physician information needs and electronic health records (EHRs): time to reengineer the clinic note. The Journal of the American Board of Family Medicine 2015, 28, 316–323. [Google Scholar] [CrossRef]
- Budd, J. Burnout related to electronic health record use in primary care. Journal of primary care & community health 2023, 14, 21501319231166921. [Google Scholar]
- Sahoo, S.S.; Plasek, J.M.; Xu, H.; Uzuner, Ö.; Cohen, T.; Yetisgen, M.; Liu, H.; Meystre, S.; Wang, Y. Large language models for biomedicine: foundations, opportunities, challenges, and best practices. Journal of the American Medical Informatics Association 2024, ocae074. [Google Scholar] [CrossRef]
- Yan, C.; Ong, H.H.; Grabowska, M.E.; Krantz, M.S.; Su, W.C.; Dickson, A.L.; Peterson, J.F.; Feng, Q.; Roden, D.M.; Stein, C.M.; et al. Large language models facilitate the generation of electronic health record phenotyping algorithms. Journal of the American Medical Informatics Association 2024, ocae072. [Google Scholar] [CrossRef] [PubMed]
- Munzir, S.I.; Hier, D.B.; Carrithers, M.D. High Throughput Phenotyping of Physician Notes with Large Language and Hybrid NLP Models. arXiv, 2024; arXiv:2403.05920. [Google Scholar] [CrossRef]
- Omiye, J.A.; Gui, H.; Rezaei, S.J.; Zou, J.; Daneshjou, R. Large language models in medicine: the potentials and pitfalls. arXiv 2023, arXiv:2309.00087. [Google Scholar] [CrossRef] [PubMed]
- Clusmann, J.; Kolbinger, F.R.; Muti, H.S.; Carrero, Z.I.; Eckardt, J.N.; Laleh, N.G.; Löffler, C.M.L.; Schwarzkopf, S.C.; Unger, M.; Veldhuizen, G.P.; et al. The future landscape of large language models in medicine. Communications Medicine 2023, 3, 141. [Google Scholar] [CrossRef]
- Li, Y.; Wang, H.; Yerebakan, H.; Shinagawa, Y.; Luo, Y. Enhancing Health Data Interoperability with Large Language Models: A FHIR Study. arXiv 2023, arXiv:2310.12989. [Google Scholar]
- Van Veen, D.; Van Uden, C.; Blankemeier, L.; Delbrouck, J.B.; Aali, A.; Bluethgen, C.; Pareek, A.; Polacin, M.; Reis, E.P.; Seehofnerova, A.; et al. Clinical text summarization: adapting large language models can outperform human experts. Research Square 2023. [Google Scholar]
- Tang, L.; Sun, Z.; Idnay, B.; Nestor, J.G.; Soroush, A.; Elias, P.A.; Xu, Z.; Ding, Y.; Durrett, G.; Rousseau, J.F.; et al. Evaluating large language models on medical evidence summarization. NPJ digital medicine 2023, 6, 158. [Google Scholar] [CrossRef]
- Zhou, W.; Bitterman, D.; Afshar, M.; Miller, T.A. Considerations for health care institutions training large language models on electronic health records. arXiv 2023, arXiv:2309.12339. [Google Scholar]
- Qiu, J.; Li, L.; Sun, J.; Peng, J.; Shi, P.; Zhang, R.; Dong, Y.; Lam, K.; Lo, F.P.W.; Xiao, B.; et al. Large ai models in health informatics: Applications, challenges, and the future. IEEE Journal of Biomedical and Health Informatics 2023. [Google Scholar] [CrossRef]
- Wang, Y.; Zhao, Y.; Petzold, L. Are Large Language Models Ready for Healthcare. A Comparative Study on Clinical Language Understanding. ArXiv 2023, arXiv:/2304.05368. [Google Scholar]
- Henderson, J. Fewer Physicians Consider Leaving Medicine, Survey Finds. MedPage Today, 29 March 2025. [Google Scholar]
- Kugic, A.; Schulz, S.; Kreuzthaler, M. Disambiguation of acronyms in clinical narratives with large language models. Journal of the American Medical Informatics Association 2024, 31, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Aronson, J.K. When I use a word... Medical slang: a taxonomy. bmj 2023, 382. [Google Scholar] [CrossRef]
- Lee, E.H.; Patel, J.P.; VI, A.H.F. Patient-centric medical notes: Identifying areas for improvement in the age of open medical records. Patient Education and Counseling 2017, 100, 1608–1611. [Google Scholar] [CrossRef] [PubMed]
- Castro, C.M.; Wilson, C.; Wang, F.; Schillinger, D. Babel babble: physicians’ use of unclarified medical jargon with patients. American Journal of Health Behavior 2007, 31, S85–S95. [Google Scholar] [CrossRef]
- Pitt, M.B.; Hendrickson, M.A. Eradicating jargon-oblivion—a proposed classification system of medical jargon. Journal of General Internal Medicine 2020, 35, 1861–1864. [Google Scholar] [CrossRef]
- Workman, T.E.; Shao, Y.; Divita, G.; Zeng-Treitler, Q. An efficient prototype method to identify and correct misspellings in clinical text. BMC Research Notes 2019, 12, 1–5. [Google Scholar] [CrossRef]
- Hamiel, U.; Hecht, I.; Nemet, A.; Pe’er, L.; Man, V.; Hilely, A.; Achiron, A. Frequency, comprehension and attitudes of physicians towards abbreviations in the medical record. Postgraduate Medical Journal 2018, 94, 254–258. [Google Scholar] [CrossRef]
- Myers, J.S.; Gojraty, S.; Yang, W.; Linsky, A.; Airan-Javia, S.; Polomano, R.C. A randomized-controlled trial of computerized alerts to reduce unapproved medication abbreviation use. Journal of the American Medical Informatics Association 2011, 18, 17–23. [Google Scholar] [CrossRef]
- Horon, K.; Hayek, K.; Montgomery, C. Prohibited abbreviations: seeking to educate, not enforce. The Canadian Journal of Hospital Pharmacy 2012, 65, 294. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.; Hoi, S.; Fernandes, O.; Huh, J.; Kynicos, S.; Murphy, L.; Lowe, D. Audit on the use of dangerous abbreviations, symbols, and dose designations in paper compared to electronic medication orders: A multicenter study. Annals of Pharmacotherapy 2018, 52, 332–337. [Google Scholar] [CrossRef]
- Shultz, J.; Strosher, L.; Nathoo, S.N.; Manley, J. Avoiding potential medication errors associated with non-intuitive medication abbreviations. The Canadian journal of hospital pharmacy 2011, 64, 246. [Google Scholar] [CrossRef]
- Baker, D.E. Campaign to Eliminate Use of Error-Prone Abbreviations. Hospital Pharmacy 2006, 41, 809–810. [Google Scholar] [CrossRef]
- Association, A.H.; of Health-System Pharmacists, A.S.; et al. Medication safety issue brief. Eliminating dangerous abbreviations, acronyms and symbols. Hospitals & Health Networks 2005, 79, 41–42. [Google Scholar]
- Hultman, G.M.; Marquard, J.L.; Lindemann, E.; Arsoniadis, E.; Pakhomov, S.; Melton, G.B. Challenges and opportunities to improve the clinician experience reviewing electronic progress notes. Applied Clinical Informatics 2019, 10, 446–453. [Google Scholar] [CrossRef]
- McDonald, C.J.; Huff, S.M.; Suico, J.G.; Hill, G.; Leavelle, D.; Aller, R.; Forrey, A.; Mercer, K.; DeMoor, G.; Hook, J.; et al. LOINC, a universal standard for identifying laboratory observations: a 5-year update. Clinical Chemistry 2003, 49, 624–633. [Google Scholar] [CrossRef]
- Hanna, J.; Joseph, E.; Brochhausen, M.; Hogan, W.R. Building a drug ontology based on RxNorm and other sources. Journal of Biomedical Semantics 2013, 4, 1–9. [Google Scholar] [CrossRef]
- Zarei, J.; Golpira, R.; Hashemi, N.; Azadmanjir, Z.; Meidani, Z.; Vahedi, A.; Bakhshandeh, H.; Fakharian, E.; Sheikhtaheri, A. Comparison of the accuracy of inpatient morbidity coding with ICD-11 and ICD-10. Health Information Management Journal 2025, 54, 14–24. [Google Scholar] [CrossRef]
- Lee, D.; de Keizer, N.; Lau, F.; Cornet, R. Literature review of SNOMED CT use. Journal of the American Medical Informatics Association 2014, 21, e11–e19. [Google Scholar] [CrossRef]
- Ficarra, B.J. Grammar and Medicine. Archives of Surgery 1981, 116, 251–252. [Google Scholar] [CrossRef]
- Goss, F.R.; Zhou, L.; Weiner, S.G. Incidence of speech recognition errors in the emergency department. International Journal of Medical Informatics 2016, 93, 70–73. [Google Scholar] [CrossRef]
- Bender, D.; Sartipi, K. HL7 FHIR: An Agile and RESTful approach to healthcare information exchange. In Proceedings of the Proceedings of the 26th IEEE international symposium on computer-based medical systems.
- Vorisek, C.N.; Lehne, M.; Klopfenstein, S.A.I.; Mayer, P.J.; Bartschke, A.; Haese, T.; Thun, S. Fast healthcare interoperability resources (FHIR) for interoperability in health research: systematic review. JMIR medical informatics 2022, 10, e35724. [Google Scholar] [CrossRef]
- Braunstein, M.L. Health Informatics on FHIR: How HL7’s New API is Transforming Healthcare; Springer, 2018.
- Benson, T.; Grieve, G. Principles of health interoperability. Springer International.
- Groza, T.; Köhler, S.; Doelken, S.; Collier, N.; Oellrich, A.; Smedley, D.; Couto, F.M.; Baynam, G.; Zankl, A.; Robinson, P.N. Automatic concept recognition using the human phenotype ontology reference and test suite corpora. Database 2015, 2015. [Google Scholar] [CrossRef]
- Hu, J.; Bao, R.; Lin, Y.; Zhang, H.; Xiang, Y. Accurate medical named entity recognition through specialized NLP models. arXiv 2024, arXiv:2412.08255. [Google Scholar]
- Luo, Y.F.; Henry, S.; Wang, Y.; Shen, F.; Uzuner, O.; Rumshisky, A. The 2019 n2c2/UMass Lowell shared task on clinical concept normalization. Journal of the American Medical Informatics Association 2020, 27, 1529–e1. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, M.; O’Connell, C.; Fatemi, Y.; Levy, A.; Sontag, D. Robust benchmarking for machine learning of clinical entity extraction. In Proceedings of the Machine Learning for Healthcare Conference. PMLR; 2020; pp. 928–949. [Google Scholar]
- Fu, S.; Chen, D.; He, H.; Liu, S.; Moon, S.; Peterson, K.J.; Shen, F.; Wang, L.; Wang, Y.; Wen, A.; et al. Clinical concept extraction: a methodology review. Journal of Biomedical Informatics 2020, 103526. [Google Scholar] [CrossRef] [PubMed]
- Funk, C.; Baumgartner, W.; Garcia, B.; Roeder, C.; Bada, M.; Cohen, K.B.; Hunter, L.E.; Verspoor, K. Large-scale biomedical concept recognition: an evaluation of current automatic annotators and their parameters. BMC bioinformatics 2014, 15, 1–29. [Google Scholar] [CrossRef]
- Zheng, J.G.; Howsmon, D.; Zhang, B.; Hahn, J.; McGuinness, D.; Hendler, J.; Ji, H. Entity linking for biomedical literature. BMC Medical Informatics and Decision Making 2015, 15, 1–9. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Liu, C.; Peres Kury, F.S.; Li, Z.; Ta, C.; Wang, K.; Weng, C. Doc2Hpo: a web application for efficient and accurate HPO concept curation. Nucleic Acids Research 2019, 47, W566–W570. [Google Scholar] [CrossRef] [PubMed]
- Powers, D.M. Evaluation: from precision, recall and F-measure to ROC, informedness, markedness and correlation. arXiv 2020, arXiv:2010.16061. [Google Scholar]
- Tayefi, M.; Ngo, P.; Chomutare, T.; Dalianis, H.; Salvi, E.; Budrionis, A.; Godtliebsen, F. Challenges and opportunities beyond structured data in analysis of electronic health records. Wiley Interdisciplinary Reviews: Computational Statistics 2021, 13, e1549. [Google Scholar] [CrossRef]
- Jiang, L.Y.; Liu, X.C.; Nejatian, N.P.; Nasir-Moin, M.; Wang, D.; Abidin, A.; Eaton, K.; Riina, H.A.; Laufer, I.; Punjabi, P.; et al. Health system-scale language models are all-purpose prediction engines. Nature 2023, 619, 357–362. [Google Scholar] [CrossRef]
- Feldman, J.; Hochman, K.A.; Guzman, B.V.; Goodman, A.; Weisstuch, J.; Testa, P. Scaling note quality assessment across an academic medical center with AI and GPT-4. NEJM Catalyst Innovations in Care Delivery 2024, 5, CAT–23. [Google Scholar] [CrossRef]
- Siegler, E.L.; Adelman, R. Copy and paste: a remediable hazard of electronic health records. The American Journal of Medicine 2009, 122, 495–496. [Google Scholar] [CrossRef]
- Weiner, S.J.; Wang, S.; Kelly, B.; Sharma, G.; Schwartz, A. How accurate is the medical record? A comparison of the physician’s note with a concealed audio recording in unannounced standardized patient encounters. Journal of the American Medical Informatics Association 2020, 27, 770–775. [Google Scholar] [CrossRef]
- Sharma, R.; Kostis, W.J.; Wilson, A.C.; Cosgrove, N.M.; Hassett, A.L.; Moreyra, A.E.; Delnevo, C.D.; Kostis, J.B. Questionable hospital chart documentation practices by physicians. Journal of General Internal Medicine 2008, 23, 1865–1870. [Google Scholar] [CrossRef]
- Bakken, S. Can informatics innovation help mitigate clinician burnout? Journal of the American Medical Informatics Association 2019, 26, 93–94. [Google Scholar] [CrossRef]
- Kapoor, M. Physician burnout in the electronic health record era. Annals of Internal Medicine 2019, 170, 216. [Google Scholar] [CrossRef]
- Kang, C.; Sarkar, N. Interventions to reduce electronic health record-related burnout: a systematic review. Applied Clinical Informatics 2023. [Google Scholar] [CrossRef] [PubMed]
- Ji, Z.; Wei, Q.; Xu, H. Bert-based ranking for biomedical entity normalization. AMIA Summits on Translational Science Proceedings 2020, 2020, 269. [Google Scholar]
- Epstein, J.A.; Cofrancesco, J.; Beach, M.C.; Bertram, A.; Hedian, H.F.; Mixter, S.; Yeh, H.C.; Berkenblit, G. Effect of outpatient note templates on note quality: NOTE (Notation Optimization through Template Engineering) randomized clinical trial. Journal of General Internal Medicine 2021, 36, 580–584. [Google Scholar] [CrossRef] [PubMed]
- Savoy, A.; Frankel, R.; Weiner, M. Clinical thinking via electronic note templates: who benefits? Journal of General Internal Medicine 2021, 36, 577–579. [Google Scholar] [CrossRef]
- Ebbers, T.; Kool, R.B.; Smeele, L.E.; Dirven, R.; den Besten, C.A.; Karssemakers, L.H.; Verhoeven, T.; Herruer, J.M.; van den Broek, G.B.; Takes, R.P. The impact of structured and standardized documentation on documentation quality; a multicenter, retrospective study. Journal of Medical Systems 2022, 46, 46. [Google Scholar] [CrossRef]
- Burke, H.B.; Hoang, A.; Becher, D.; Fontelo, P.; Liu, F.; Stephens, M.; Pangaro, L.N.; Sessums, L.L.; O’Malley, P.; Baxi, N.S.; et al. QNOTE: an instrument for measuring the quality of EHR clinical notes. Journal of the American Medical Informatics Association 2014, 21, 910–916. [Google Scholar] [CrossRef]
Figure 1.
Potential Downstream Use Cases for Standardized Notes. Standardized notes offer opportunties for improved clinical documentation. Thes notes can be mined for medical concepts and then normalized to an appropriate ontology to support exploratory data analysis and machine learning and conversion to Fast Interoperability Healthare Resources for data exchange.
Figure 1.
Potential Downstream Use Cases for Standardized Notes. Standardized notes offer opportunties for improved clinical documentation. Thes notes can be mined for medical concepts and then normalized to an appropriate ontology to support exploratory data analysis and machine learning and conversion to Fast Interoperability Healthare Resources for data exchange.
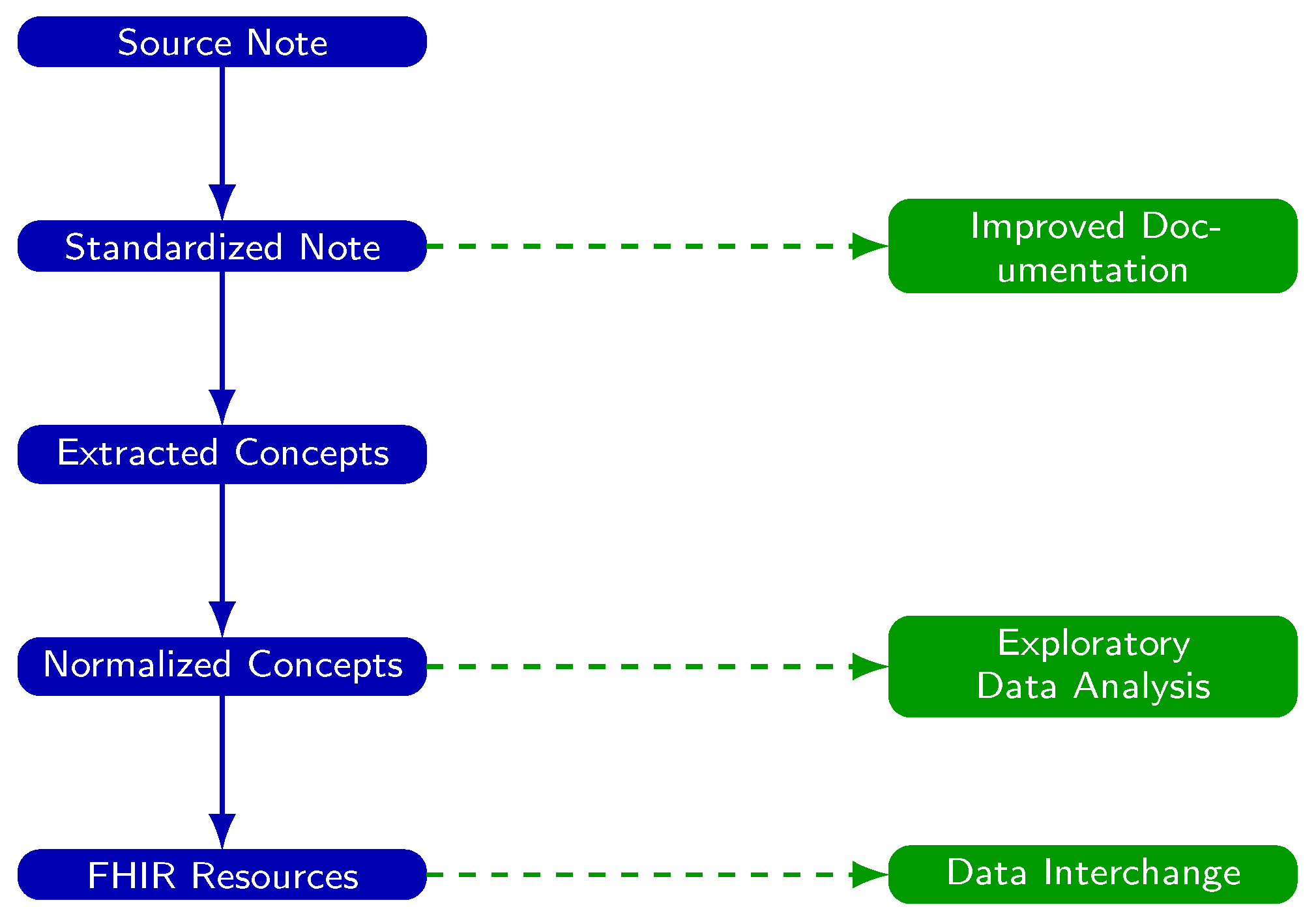
Figure 2.
Experimental Setup for Evaluating the Accuracy of Note Standardization. Each clinical note is processed along three parallel paths: (1) raw notes are analyzed directly, (2) standardized notes are analyzed after GPT-4-based processing, and (3) ground truth phrases are analyzed after identification by GPT-4. In all paths, text is mapped to Human Phenotype Ontology (HPO) terms using doc2hpo, producing a set of terms from each path. Term sets from the raw and standardized notes are then compared to the ground truth set to compute accuracy, precision, recall, and F1 score.
Figure 2.
Experimental Setup for Evaluating the Accuracy of Note Standardization. Each clinical note is processed along three parallel paths: (1) raw notes are analyzed directly, (2) standardized notes are analyzed after GPT-4-based processing, and (3) ground truth phrases are analyzed after identification by GPT-4. In all paths, text is mapped to Human Phenotype Ontology (HPO) terms using doc2hpo, producing a set of terms from each path. Term sets from the raw and standardized notes are then compared to the ground truth set to compute accuracy, precision, recall, and F1 score.
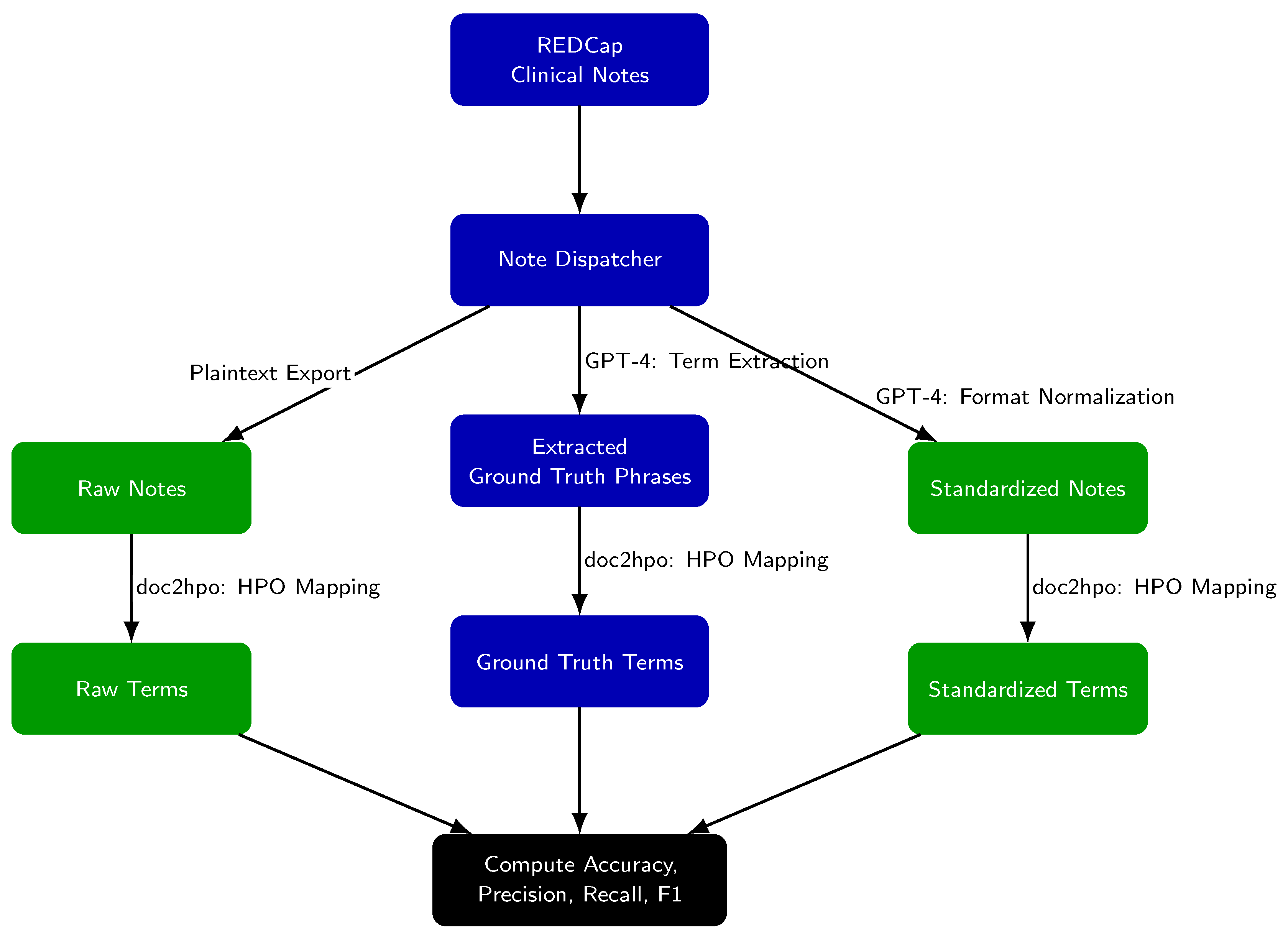
Figure 3.
Example neurology note converted to JSON format. Note has been truncated for brevity.
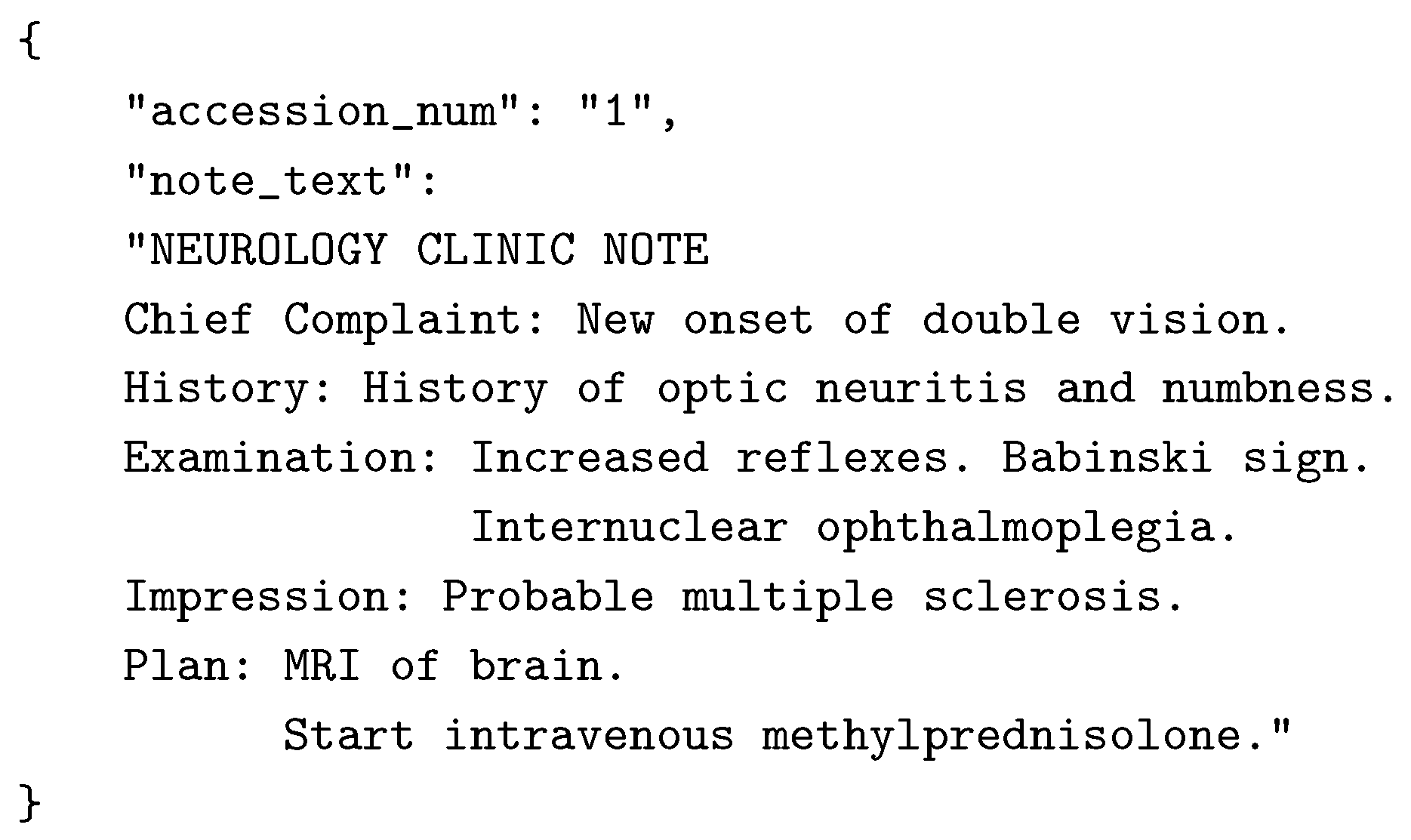
Figure 4.
Performance metrics for doc2hpo on normalizing extracted terms from raw and standardized to their correct HPO term and HPO ID. Accuracy, precision, and recall improve after GPT-4-based note standardization (, n = 1592, two-way t-test.)
Figure 4.
Performance metrics for doc2hpo on normalizing extracted terms from raw and standardized to their correct HPO term and HPO ID. Accuracy, precision, and recall improve after GPT-4-based note standardization (, n = 1592, two-way t-test.)
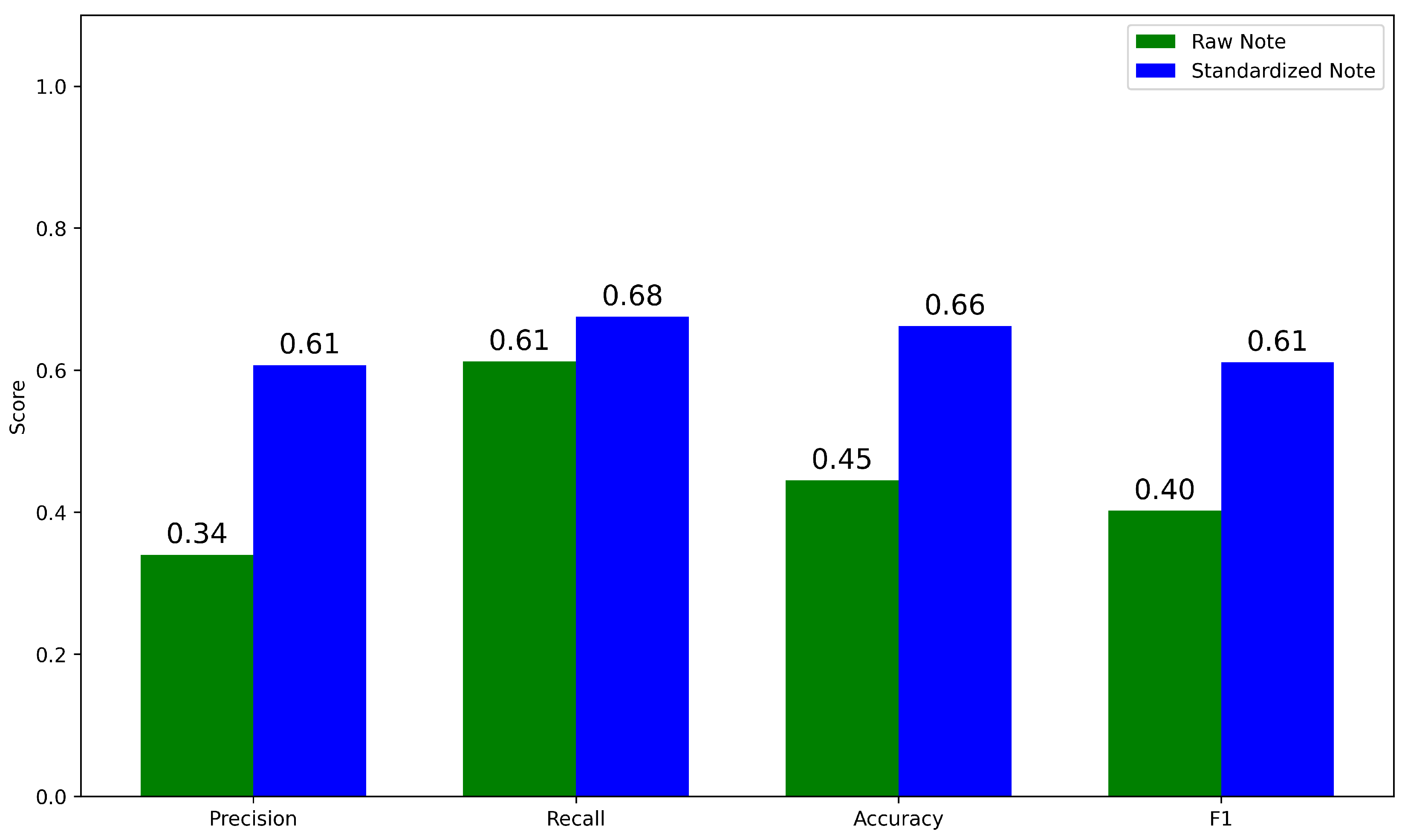
Figure 5.
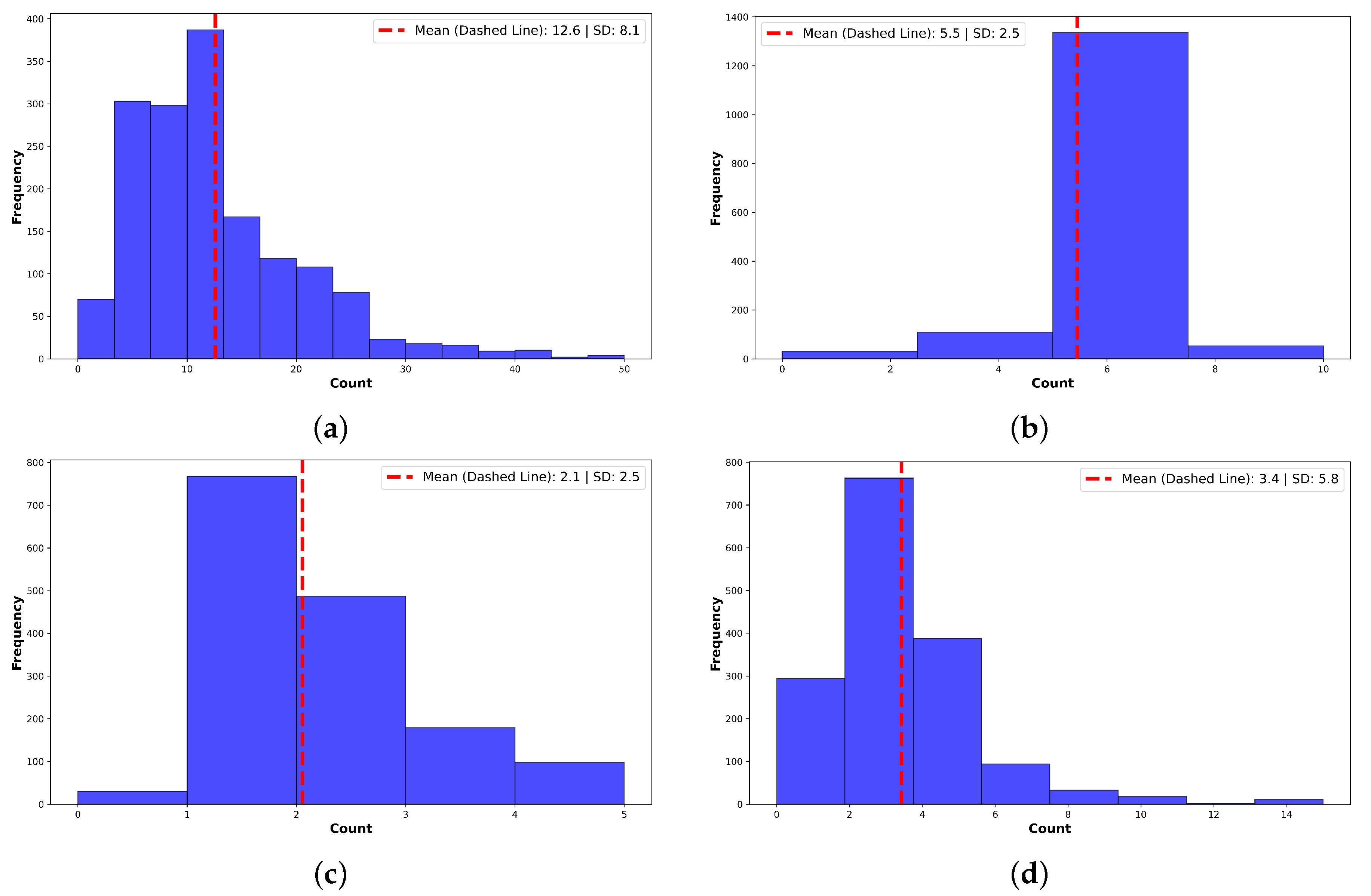
Summary of Corrections made by GPT-4o. (a) Acronyms and Abbreviations. Normalization expanded a mean of per note. (b) Grammatical Errors. Normalization corrected a mean of grammatical errors per note. (c) Slang, Jargon, and Non-Standard Terms. GPT-4 corrected non-standard terms per note. Example: “feeling blue” → “symptoms of depression”. (d) Spelling Errors. GPT-4 corrected a mean of errors per note. High variance reflects many outlier notes.
Figure 5.
Summary of Corrections made by GPT-4o. (a) Acronyms and Abbreviations. Normalization expanded a mean of per note. (b) Grammatical Errors. Normalization corrected a mean of grammatical errors per note. (c) Slang, Jargon, and Non-Standard Terms. GPT-4 corrected non-standard terms per note. Example: “feeling blue” → “symptoms of depression”. (d) Spelling Errors. GPT-4 corrected a mean of errors per note. High variance reflects many outlier notes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



