
Submitted:
03 February 2026
Posted:
05 February 2026
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Objectives: The study aimed to analyze diphtheria-tetanus-pertussis (DTP) vaccination coverage and anti-pertussis herd immunity levels globally and in World Health Organization (WHO) regions in 2024, as well as their variation from 2019 to 2024. Methods: Mean percentages of vaccination coverage with three, two, one and zero doses of DTP vaccine in WHO regions in 2024 were calculated using data from the WHO/UNICEF global and regional immunization information system. Results: Global DTP vaccination coverage in 2024 for three, two, one, and zero doses of vaccine were 72.8%, 21.1%, 5.3%, and 0.8%, respectively. Three-dose DTP coverage was below 90% in all WHO regions, with only 12.3% of countries achieving a three-dose coverage of ≥95%. Anti-pertussis herd immunity levels were insufficient in preventing Bordetella pertussis transmission in WHO regions. From 2019 to 2024, three-dose DTP coverage decreased by 5.5%, while zero-dose coverage increased by 14.3%. Conclusion: In 2024, global and regional DTP vaccination coverage and anti-pertussis herd immunity indicators in 2024 did not recover to pre-COVID-19 levels, making it difficult to achieve the Immunization Agenda 2030 objective.
Keywords:
health indicators
; vaccine coverage
; pertussis vaccines
; zero-dose
; three-dose coverage
; herd immunity
; pertussis prevention
; COVID impact
; WHO regions
; immunization agenda 2030
1. Introduction
Pertussis or whooping cough is an endemic infectious disease caused by Bordetella pertussis. Pertussis infections can generate outbreaks and epidemics affecting individuals of all ages. However, the incidence of pertussis is greater among unvaccinated or partially vaccinated children aged less than 1 year and adolescents between 10 and 18 years than among adults, and the risk of pertussis complications is greater in infants and children than in adults [1,2].
Despite the availability of pertussis vaccines since 1960, pertussis cases and outbreaks have occurred every year worldwide and pertussis resurgence has been reported in different countries in the past two decades [3,4]. The number of pertussis cases reported worldwide ranged from I49,000 to 174,000 prior to the COVID-19 pandemic (2015−2020) and decreased to less than 70,000 during the pandemic [5] (Figure 1). However, pertussis resurged in 2024, as 941,565 cases were reported worldwide, with 591,193 in the Western Pacific region and 298,595 in the European region [5] (Figure 1).
In 2024, the number of pertussis cases reported was 476% greater than that registered in 2023. The global incidence of pertussis, which ranged from 4,9 to 9 per million population during 2020−2022, increased to 137 per million population in 2024 [5]. In 2024, pertussis incidence was 324 and 307 per million population in the European and Western Pacific regions, respectively [5].
Several factors have been proposed to explain pertussis resurgence, including insufficient vaccination coverage, insufficient anti-pertussis herd immunity, waning of vaccine-induced immunity over time, and lower vaccine effectiveness due to Bordetella pertussis changes after widespread vaccination [6,7,8,9].
Routine pertussis vaccination is the key intervention to achieve prevention and control [10]. The Immunization Agenda 2030 (IA2030) agenda endorsed by the 73rd World Health Assembly proposed an ambitious strategy for vaccines and immunization for the 2021-2030 decade [11]. Routine pertussis vaccination includes three doses of diphtheria-−tetanus−pertussis-containing (DTP) vaccines at 2, 4, and 6−12 months of age, and two booster doses are recommended between the ages of 12 months and 16 years to maintain protection [12]. Vaccination programs can use pertussis-containing vaccines including acellular or whole-cell pertussis antigens. Acellular pertussis-containing vaccines (DTaP for children aged <7 years, Tdap for adolescents and adults) are used in developed countries, while whole-cell pertussis-containing vaccines (wP) are used in low-income countries [12].
The pertussis prevention strategy based on routine vaccination requires achieving high percentages of coverage and high levels of pertussis vaccination effectiveness to prevent community transmission [9]. The Immunization Agenda 2030 proposed to achieve 90% vaccination coverage for the first and third doses of DTP-containing vaccines by 2030 at the national and regional level [13].
A prior study found global mean vaccination coverages with three, two, one and zero doses of DTP vaccine in 2019 of 77%, 18%, 4.3% and 0.7%, respectively [9]. In addition, the three-dose DTP vaccination coverage was greater than 90% in only 34% of countries worldwide [9]. The objectives of this study were: 1) to assess the vaccination coverage for three, two, one and zero doses of DTP vaccine in all countries: 2) to assess the mean vaccination coverage for DTP1 and DTP3 vaccines, and three, two, one and zero doses of DTP vaccine in different WHO regions in 2024; 3) to assess the prevalence of vaccine-induced pertussis protection in all counties and WHO region in 2024; 4) to assess variations from 2019 to 2024 in DTP vaccination coverage and anti-pertussis herd immunity indicators in different WHO regions; and 5) to assess whether zero-dose vaccination coverage indicators and the number of zero-dose children were on track to achieve the Immunization Agenda 2030 objective.
2. Methods
2.1. Mean Vaccination Coverage with Zero, One, Two and Three DTP Vaccine Doses in the WHO Regions in 2024
Mean percentages of vaccination coverage with three, two, one and zero doses of DTP-containing vaccines in children aged one year (target population) were determined in each WHO region using the vaccination coverage reported by different countries for the first (DTP1) and third (DTP3) vaccine doses, as well as the estimated vaccination coverage for the second DTP dose (DTP2) [9]. WHO and UNICEF produce country-specific estimates for routine DTP1 and DTP3 vaccination coverage by individually reviewing each country’s data about annual administrative-based official coverage and survey reports [14,15,16]. Administrative DTP1 and DTP3 vaccination coverage is defined as the number of DTP1 and DTP3 doses administered to targeted children by the estimated target population [17]. Survey-based DTP1 and DTP3 vaccination coverage is defined as the proportion of children in the target age group who received the DTP1 and DTP3 vaccines, respectively [17].
The percentages of vaccination coverage with zero, one, two, and three doses of DTP vaccine were determined in each country using a conservative approach [9]. In this analysis, it was assumed that children could have received any of the DTP doses independently of receiving other DTP doses. Children unvaccinated with the DTP1 dose could have received the DTP2 and DTP3 doses; children vaccinated with the DTP2 could have not received the DTP1 vaccine; and children could have received the DTP3 vaccine independently of receiving the DTP1 and DTP2 doses. By contrast, the WHO and UNICEF assumed that children unvaccinated with the DTP1 vaccine did not receive the DTP2 and/or DTP3 vaccines, and that children vaccinated with the DTP3 vaccine received the DTP1 and DTP2 vaccines [16,17].
The zero-dose DTP coverage in children aged one year was determined in each country from the vaccination coverage with one, two, and three doses of DTP vaccine, and the mean zero-dose vaccination in each WHO region was determined from country values [9].
The three-dose and zero-dose DTP coverages in children aged one year are good indicators of vaccination program performance in different countries and WHO regions, as they show the percentage of children who have completed the three-dose DTP vaccination and the percentage of those who have not received any DTP dose, respectively. The WHO and UNICEF have used the DTP1 and DTP3 vaccination coverage as indicators of vaccination program performance [16].
2.2. Anti-Pertussis Herd Immunity Levels in the Target Vaccination Population in WHO Regions in 2024
Anti-pertussis herd immunity levels in different WHO regions were determined using the country-based mean prevalence of vaccine-induced pertussis protection in children aged one year. This prevalence was determined in each country from the DTP1, DTP2 and DTP3 vaccination coverage and vaccine effectiveness in preventing pertussis cases of 84%, 77%, 59%, respectively [9,18,19].
Herd immunity against Bordetella pertussis was considered to be established in each country and WHO region when the prevalence of pertussis protection was higher than 90%, 90.9%, 91.7%, 92.3%, 92.9%, 93.3%, 93.8%, 94.1% and 94.4% for transmissibility (Ro) values of 10, 11, 12, 13, 14, 15, 16, 17 and 18, respectively [9]. The percentage of countries with sufficient herd immunity against Bordetella pertussis with Ro values of 10, 12, 15 and 18 was determined in each WHO region.
2.3. Assessment of Whether Zero-Dose DTP Vaccination Indicators in 2024 Were on Track to Achieve the Immunization Agenda 2030 Objective
The tracks required to achieve a worldwide and regional 50% reduction from 2019 to 2030 were assessed for the following vaccination performance indicators: (1) number of zero-dose children [15,16]; (2) mean zero-dose coverage (100 − DTP1); and (3) mean zero-dose coverage derived from the covefrage with one, two and three doses of DTP vaccine (conservative approach) [9].
For the number of zero-dose children, the 2019−2030 track was determined taking into account the zero-dose children in 2019 (12.86 million) [15,16] and its 50% reduction in 2030 (9.0 million). The estimated number of zero-dose children in 2024 was compared with the number required to achieve the IA2030 objective.
For the mean zero-dose coverage (DTP1-based), the 2019−2030 track was determined taking into account the mean zero-dose coverage in 2019 (7.4%) [9] and its 50% reduction in 2030 (3.7%). The mean zero-dose coverage in 2024 was compared with the coverage required to achieve the IA2030 objective.
For the mean zero-dose DTP coverage derived from one-, two- and three-doses coverage, the 2019−2030 track was determined taking into account the mean zero-dose coverage in 2019 (0.7%) [9] and its 50% reduction in 2030 (0.35%). The mean zero-dose coverage in 2024 was compared with the coverage required to achieve the IA2030 objective.
2.4. High-Priority Countries for Routine DTP Vaccination Coverage Increase
In this study, high prioirty countries for DTP vaccination coverage incrresae were identified in each WHO region using the following criteria:
- Very-high-priority: Countries with zero-dose DTP coverage greater than the regional mean.
- High-priority: Countries with three-dose DTP coverage lower than 80% and lower than their regional mean coverage.
- High-priority: Countries with DTP1 coverage lower than 90%.
- High-priority: Countries with DTP3 coverage lower than 90%.
2.5. Statistical Analysis
Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was used to calculate: (1) the vaccination coverage with three, two, one and zero DTP doses in each country and mean regional coverages in 2024; (2) the prevalence of pertussis protection in each country and mean regional prevalences in 2024; and (3) the variation from 2019 to 2024 for vaccination coverage and anti-pertussis herd immunity indicators in WHO regions.
Microsoft Excel (Microsoft Corporation, Redmond, WA, USA) was used to assess the establishment of anti-pertussis herd immunity in different countries and WHO regions in 2024; and to assess whether zero-dose vaccination coverage indicators were on track to achieve the Immunization Agenda 2030 objective.
3. Results
3.1. Mean DTP Vaccination Coverage Percentages in 2024
This study found a global mean vaccination coverage of 90.7% and 86.6% for the DTP1 and DTP3 vaccines, respectively (Table 1). Mean percentages of vaccination coverage were greater than 90% in the European, South-East Asia and Western Pacific regions for the DTP1 vaccine, and in the European and South-East Asia regions for the DTP3 vaccine (Table 1). The global means DTP1 and DTP3 vaccination coverage were slightly greater than the population-based values estimated by WHO-UNICEF: 89% for DTP1 coverage and 85% for DTP3 coverage [16].
3.2. Mean Percentages of Vaccination Coverage with Three, Two, One and Zero Doses of DTP Vaccine in 2024
This study found global mean percentages of vaccination coverage with three, two, one and zero doses of DTP vaccine of 72.8%, 21.1%, 5.3% and 0.8%, respectively (Table 1). The three-dose coverage ranged from 82.5% in the European region to 59.5% in the African region; the two-dose DTP vaccination coverage ranged from 30.4% in the African region to 15.3% in the European region; the one-dose DTP vaccination coverage from 8.9% in the African region to 2% in the European region; and the zero-dose DTP vaccination coverage ranged from 1.2% in the African region to 0.2% in the European region (Table 1).
The three-dose DTP coverage was ≥95% and ≥90% only in 12.3% and 21% of the countries worldwide, respectively (Table 1). The percentage of countries with a three-dose DTP coverage ≥90% was 18−37% in the Americas, European, South-East Asia and Western Pacific regions, while it was lower than 10% in the African and Eastern Mediterranean regions (Table 1).
This study found that all children aged one year could have received at least one dose of DTP vaccine (1, 2 or 3 doses) in 53.3% of the countries worldwide (Table 1). The percentage of countries where all children aged one year could have received at least one dose of DTP vaccine ranged from 82.3% in the European region to 27.7% in the African region (Table 1).
The mean three-dose DTP coverage obtained in this study (72.8%) was lower than the percentage of children that had received the first three doses of DTP vaccine (85%) estimated by WHO-UNICEF from DTP3 coverage [15,16]. The three-dose coverage obtained in this study can be considered the lowest percentage of children that could have received the first three DTP doses (conservative estimation), while the WHO-UNICEF value can be considered the highest percentage.
The mean zero-dose DTP coverage obtained in this study (0.8%) was lower than the percentage of zero-dose children (11%) estimated from 100 – DTP1 coverage by WHO-UNICEF [15,16]. The zero-dose coverage obtained in this study can be considered the lowest possible percentage of zero-dose children (conservative estimation), while the WHO-UNICEF value can be considered the highest.
Supplementary Table S1 presents the three- and zero-dose DTP vaccination coverages among one-year-old children in different countries in 2024.
3.3. Anti-Pertussis Herd Immunity Levels in 2024
This study found a global mean prevalence of vaccine-induced pertussis protection in the target vaccination population (children aged 1 year) of 53.3% (Table 1). The mean prevalence of pertussis protection ranged from 72.7% in the South-East Asia region to 22.7% in the African region (Table 1).
Supplementary Table S1 presents the prevalence of vaccine-induced protected one-year-old children in different countries in 2024. Pertussis protection levels were not sufficient to establish herd immunity against Bordetella pertussis with transmissibility values (Ro) equal to or greater than 10 in any WHO region, as the prevalence of pertussis protection was lower than 90% in all regions (Table 1).
3.4. Variation in DTP Vaccination Coverage and Anti-pertussis Herd Immunity Indicators from 2019 to 2024
The following DTP vaccination program indicators worsened worldwide from 2019 to 2024: mean DTP1 coverage (−2%), mean DTP3 coverage (−1.8%), mean three-dose coverage (−5.3%), mean zero-dose coverage (14.3%), percentage of countries with three-dose coverage ≥95% (−31.7%), percentage of countries with three-dose coverage ≥90% (−38.2%), percentage of countries where all children aged one year had received at least one dose of DTP vaccine (−17.2%), and mean prevalence of children aged one year with vaccine-induced pertussis protection (−5.6%) (Table 2). By contrast, the two-dose and one-dose coverage improved by 17.2% and 23.3%, respectively, from 2019 to 2024 (Table 2). The percentage of countries with sufficient anti-pertussis herd immunity did not vary from 2019 to 2024 (Table 2).
The highest three-dose and zero-dose coverage increases from 2019 to 2024 were found in the African (7.2%) and Western Pacific (33%) regions, respectively (Table 2).
The mean DTP1 vaccination coverage decreased in all WHO regions from 2019 to 2024, except in the Western Pacific region (Table 2, Figure 2, Figure 2). The mean DTP3 vaccination coverage decreased in all WHO regions from 2019 to 2024 (Table 2, Figure 2, Figure 3).
The COVID-19 pandemic was associated with a significant negative effect on DTP1 and DTP3 vaccination coverage in the South-East Asia region, and fewer negative effects in the other WHO regions (Figure 2, Figure 3). In 2021, the mean zero-dose DTP coverage dropped to 20.4% in the South-East Asia region (Figure 4) due to a mean DTP1 coverage of 45%, (Figure 2), mean DTP3 coverage of 37% and three-, two- and one-dose coverages of 6.8%, 29.8% and 42.9%, respectively. However, since 2021, mean DTP1, DTP3 and zero-dose DTP coverages have recovered in the Western Pacific region and other affected WHO regions (Figure 2, Figure 3, Figure 4). In 2024, the regional mean DTP1 and DTP3 coverages were only 1−3% lower than those found in 2019 (pre-pandemic period), and the regional three-dose coverages were 3−7% lower than those found in 2019 (Table 2, Figure 2, Figure 3).
The study found that the global mean three-dose DTP vaccination coverage decreased by 5.5%, while the mean two-dose and mean one-dose coverages increased by 17.2% and 23.3%, respectively, from 2019 to 2024 (Table 2). In addition, the percentage of countries with three-dose DTP coverage ≥95% and ≥90% decreased by 31.7% and 38.2%, respectively (Table 2).
The mean zero-dose coverage increased by 14.3%, and the percentage of countries where all children aged one year could have received one, two or three DTP doses and had not zero-dose children decreased by 17.2% from 2019 to 2024 (Table 2).
The prevalence of one-year-old children with vaccine-induced pertussis protection decreased by 8.6% from 2019 to 2024 (Table 2). However, anti-pertussis herd immunity levels did not vary from 2019 to 2024, as the prevalence of pertussis protection was not sufficient to block the community transmission of Bordetella pertussis with transmissibility values ≥Ro 10 worldwide and in any WHO region in 2019 and 2024 (Table 2).
Six DTP vaccination program indicators worsened in the African region, seven in the Americas region, eight in the Eastern Mediterranean region, eight in the European region, six in the South-East Asia region, and seven in the Western Pacific region. By contrast, four DTP vaccination program indicators improved in the African region, three in the Americas region, and two in the Eastern Mediterranean, European region, South-East Asia region Western Pacific region. (Table 2).
The mean DTP1 coverage decreased from 2019 to 2024 in African region, three in the Americas region, and two in the Eastern Mediterranean, European region and South-East Asia region regions and improved in the Western Pacific region (Table 2, Figure 2).
The mean DTP3 coverage and the mean three-dose coverage decreased from 2019 to 2023 in all WHO regions (Table 2, Figure 3). The mean two-dose coverage improved from 2019 to 2024 in all WHO regions except in the Eastern Mediterranean region (Table 2). The mean one-dose coverage improved from 2019 to 2024 in all WHO regions (Table 2).
The mean zero-dose coverage worsened (increased) from 2019 to 2024 in the Americas, Eastern Mediterranean, European region, and South-East Asia regions (Table 2, Figure 4). This indicator increased from 0% in 2019 to 0.2% in 2024 in the European region, and from 0% in 2019 to 0.3% in 2024 in the Western Pacific region (Figure 4). By contrast, the mean zero-dose coverage improved from 2019 to 2024 in the African region and Western Pacific regions (Table 2, Figure 4)
The percentage of countries with three-dose DTP coverage ≥95% decreased from 2019 to 2024 in the African, Eastern Mediterranean, European and Western Pacific regions, and improved in the Americas region (Table 2). The percentage of countries with three-dose DTP coverage ≥90% decreased from 2019 to 2024 in all WHO regions (Table 2).
The percentage of countries where all children aged one year could have received one, two or three DTP doses and had not zero-dose children decreased in all WHO regions, except in the South-East Asia region (Table 2).
The mean prevalence of one-year-old children with vaccine-induced pertussis protection decreased in all WHO regions, except in the African region (Table 2). Herd immunity levels generated by routine DTP vaccination programs in different WHO regions were not sufficient to prevent pertussis transmission in 2019 and 2024 (Table 2).
3.5. Assessment of Whether Zero-Dose DTP Vaccination Indicators in 2024 Were on Track to Achieve the IA2030 Objective by 2030
The three zero-dose DTP coverage indicators assessed in this study were not on track to achieve the IA2030 objective of reducing the 2019 levels by 50% in 2030. In 2024, the number of zero-dose children, mean DTP1-based zero-dose coverage and mean zero-dose coverage were 43.9%, 62.2% and 48.1% greater, respectively, than the values required in 2024 to achieve the IA2030 objective.
The number of zero-dose children in 2024 (14.3 million) [16] was not on track to achieve 6.43 million by 2030 (Figure 5). The number of zero-dose children required in 2024 was 9.94 million (Figure 5).
The mean zero-dose DTP1-based coverage in 2024 (9.28%) was not on track to achieve a coverage of 3.7% by 2030 (Figure 6). The zero-dose DTP1-based coverage required in 2024 was 5.72% (Figure 6). The mean zero-dose coverage in 2024 (0.8%) was not on track to achieve a coverage of 0.35% by 2030 (Figure 7). The zero-dose coverage required in 2024 was 0.54% (Figure 7).
3.6. High-Priority Countries for Routine DTP Vaccination Coverage Increase
This study found 37 (19%) very-high-priority countries for routine DTP vaccination coverage increase because the zero-dose coverage was greater than the regional mean (Table 3). Seventy-eight (40%) countries were high-priority for DTP vaccination coverage increase because the three-dose coverage was lower than 80%, in countries with three- and zero-dose coverage lower than the regional means (Table 3). Fifty-eight (29.7%) were high-priority for DTP vaccination coverage increase because the DTP1 coverage was lower than 90%, and 85 (43.6%) countries because the DTP3 coverage was lower than 90% (Table 3).
The African region included 46% of the very-high-priority countries for DTP vaccination coverage increase (Table 3). In addition, the African region includes 28%, 43% and 36% of the high-priority countries based on criteria 2, 3 and 4, respectively (Table 3).
Supplementary Table S1 presents the DTP1 and DTP3 vaccination coverage and the three-dose and zero-dose DTP vaccination coverage among one-year-old children in different countries in 2024.
Supplementary Table S2 presents the list of high-priority countries in each WHO region for routine DTP vaccination coverage increase based on the four considered criteria. Using the zero-dose DTP criteria, the number of countries was 52.6%, 36.2% and 56.5% lower than using criteria 2 (three-dose), 3 (DTP1) and 4 (DTP3), respectively. Using the three-dose criteria, the number of countries was 34.5% higher than using the DTP1 criteria and 8.2% lower than using the DTP3 criteria.
Eighty-eight (45%) countries (31 from the African region) were high-priority for DTP vaccination coverage increase based on their DTP1 and DTP3 coverage levels lower than 90%. Using DTP1 vaccination coverage criteria, the number of countries was 31.8% lower than with the DTP3 criteria. Using the DTP1 criteria, Lesotho, Tanzania, Sao Tome and Principe, and Burundi in the African region were high-priority for DTP1 coverage increase despite their coverage being greater than the regional mean (Supplementary Table S2).
Using the DTP3 vaccination coverage criteria, Gambia, Mali, Tanzania, Liberia, Eswatini, Lesotho, Mauritania, Niger, Sao Tome and Principe, and Burundi in the African region; Dominican Republic, Belize, Colombia, and Nicaragua in the Americas regio; and Libya, Pakistan and Palestine in the Eastern Mediterranean region were high-priority for DTP3 coverage increase despite their coverage being greater than the regional mean (Supplementary Table S2).
4. Discussion
This study found that three-dose DTP vaccination coverage lower than 90% worldwide and in all WHO regions. Furthermore, vaccine-induced anti-pertussis herd immunity levels in children aged one year were lower than those necessary to block Bordetella pertussis transmission worldwide and in all WHO regions in 2024.
Routine DTP vaccination programs could not generate sufficient herd immunity to block Bordetella pertussis transmission worldwide, as the estimated prevalence of one-year-old children with vaccine induced pertussis protection was lower than lower than 90% worldwide and in all WHO regions.
The global mean percentages of DTP vaccination coverage for three, two, one and zero doses of vaccine were 72.8%, 21.1%, 5.3% and 0.8%, respectively. The mean three-dose coverage decreased by 5.5% worldwide from 2019 to 2024, and it decreased in all WHO regions. The mean zero-dose coverage increased by 14.3% worldwide from 2019 to 2024, and it increased in all WHO regions except in the Western Pacific region.
In 2024, The African region has the worst DTP coverage profile, with less than 60% DTP3 coverage, while Europe and the Western Pacific have the best profile, with DTP1 coverage over 90% and DTP3 coverage between 77% and 82%. The mean three-dose DTP coverage was 59.5% in the African region and from 77% to 82% in the European, South-East Asia and Western Pacific regions. The zero-dose coverage was 1.2% in the African region and lower than 0.6% in the European, South-East Asia and Western Pacific regions.
The DTP vaccination coverage profile in the Americas and Eastern Mediterranean regions was better than in the Africa region and worse than in European, South-East Asia and Western Pacific regions, as the DTP1, DTP3 and three-dose DTP vaccination coverages were lower than in the European, South-East Asia and Western Pacific regions and greater than in the African region.
This study found that eight of the routine DTP vaccination coverage and anti-pertussis herd immunity indicators assessed in this study worsened from 2029 to 2024 worldwide, including the mean DTP1 coverage, mean DTP3 coverage, three-dose coverage, zero-dose coverage, percentage of countries with three-dose coverage ≥95%, percentage of countries with three-dose coverage ≥90%, percentage of countries where all children aged one year had received at least one dose of DTP vaccine, and mean prevalence of children aged one year with vaccine-induced pertussis protection.
The insufficient levels for routine DTP vaccination coverage and anti-pertussis herd immunity are two factors explaining pertussis resurgence. Other explanatory factors include the type of vaccine, waning pertussis immunity, lower effectiveness of DTP-containing vaccines due to Bordetella pertussis mutations, and a lack of or insufficient vaccination coverage with booster doses among adolescents and adults [6–9,20-24]. Recent studies have found that Bordetella pertussis without the pertactin and pertussis toxin vaccine antigens could also favor pertussis resurgence in 2024. Several studies have found that emergent Bordetella pertussis strains with non-vaccine antigens could be associated with lower levels of acellular pertussis vaccine effectiveness [7,8,20,22,23]. A study carried out in the United States found an association between the switch from whole-cell to acellular pertussis vaccines and pertussis incidence registered from 1992 to 2024, one that was statistically significant after adjusting for vaccination coverage [20]. However, a direct comparison between pertussis incidence in countries using acellular (aP) vaccines and countries using whole-cell (wP) vaccines is difficult due to differences in pertussis surveillance activities, pertussis case management, the definition of pertussis, and laboratory detection methods [25,26,27,28,29]. In fact, the worldwide impact of emerging Bordetella pertussis without vaccine antigens on the effectiveness of DTP-containing vaccines and herd immunity levels has not been assessed.
Several factors can be proposed to explain the DTP vaccination coverage decrease from 2019 to 2024, including COVID-19 pandemic disruptions, vaccine hesitancy, and insufficient resources for routine vaccination programs. The COVID-19 pandemic disrupted routine DTP vaccination programs due to lockdowns, logistical problems, and the reallocation of health and economic resources to COVID-19 vaccination, detection and management [30,31]. The WHO-UNICEF and studies focused on countries and WHO regions found that DTP vaccine coverage dropped during the pandemic period and that COVID-19-associated vaccination disruptions varied across countries and WHO regions [30,31,32,33,34,35]. The results of the study showing that routine DTP vaccination programs had not completely recovered from COVID-19 pandemic disruptions in 2024, can be explained by the following factors: (1) sustained COVID-19 pandemic effects on routine vaccination programs, (2) vaccine hesitancy, and (3) insufficient health and economic resources for routine vaccination programs.
The COVID-19 pandemic’s impact on routine DTP vaccination could still have been in effect in many countries in 2024 if the health and economic resources necessary to implement routine DTP vaccination activities did not recover their pre-COVID levels. Parent’s hesitancy to vaccinate their children with DTP-containing vaccines could be other factor contributing to the lower DTP vaccination performance. Parental vaccine hesitancy has been associated with 25% lower vaccination coverage among children aged 19-35 months [36]. Such hesitancy includes concerns for vaccine safety and effectiveness [37], a lack of information [38], and low trust in vaccines and health services [39]. A study comparing parental attitudes and behaviors towards childhood vaccination with DTP-containing vaccines in the United Kingdom and Israel before and after the COVID-19 pandemic, found that 5.1% and 6.6% of parents reported a shift towards not-vaccinating their child after the pandemic vaccines in their countries, respectively [40]. The study found that after the COVID-19 pandemic, concerns regarding potential side effects were greater and trust in vaccines was lower than before the pandemic [40].
The results found in this study showed that it is necessary to develop a more ambitious pertussis vaccination strategy than that based only on routine vaccination of children, one with the objective of ensuring individual protection among one-year-old children and generating sufficient anti-pertussis herd immunity to prevent Bordetella pertussis transmission in the population [9,41]. This strategy must include the following components: (1) ≥90% routine three-dose DTP vaccination coverage in children aged one year; (2) vaccination of adolescents and adults every 10 years with booster doses of pertussis vaccine [41,42]; and (3) vaccination of pregnant women with a single dose of Tdap or Tdap-IPV vaccines between 27 and 36 weeks of gestation and of unvaccinated women who have recently given birth [43,44]. In the European region, pertussis vaccination in adolescents and adults differs from country to country, with all countries recommending booster doses in adolescents and 12 countries recommending adult vaccination with 1−2 booster doses or booster doses every 10 years after the last dose [42]. Supplementary DTP vaccination activities can be developed to increase pertussis immunity in countries with very low vaccination coverage, especially in the African region [16]. However, intensive supplementary vaccination activities should not be undergone during a long period of time, because they demand significant resources and can disrupt routine vaccination activities [45,46].
Different criteria can be used to decide which countries in each WHO region must be high-priority for routine DTP vaccination coverage increase. This study found that 37 countries (15 from the African region) were very-high-priority for DTP vaccination coverage, based on the zero-dose coverage determined from the one−, two− and three−dose coverage, and another 41 countries were high-priority based on their <80% three-dose coverage (Supplementary Table S2). In addition, 88 countries were high-priority for DTP vaccination coverage increase based on the <90% DTP1 and DTP3 vaccination coverage (Supplementary Table S2). The WHO and UNICEF gave high priority to increase the DTP coverage to (1) the 10 countries with the highest number of unvaccinated one-year-old children (Nigeria, India, Sudan, Democratic Republic of Congo, Ethiopia, Indonesia, Yemen, Angola and Pakistan); and (2) the 10 countries with the lowest DTP1 coverage (Sudan, Angola, Afghanistan, Azerbaijan, Bolivia, Gabon, Papua New Guinea, and Democratic Republic of Congo) [16]. The results obtained in this study showed that a significant number of countries should increase their routine DTP vaccination coverage, and that countries with low DTP vaccination performance must be high-priority for DTP vaccination coverage increase in all WHO regions (Supplementary Table S2). In each WHO region, all countries should reach the regional mean DTP vaccination performance.
The analysis carried out in this study has four limitations. Firstly, the analysis was carried out using the information provided by different countries on DTP1 and DTP3 vaccines distributed and administered to the target population to the WHO-UNICEF immunization information system. However, the routine DTP1 and DTP3 vaccination coverage reported by the WHO-UNICEF immunization information system is periodically validated by the WHO [16,17,47]. Secondly, the vaccination coverage for three-, two- and one-doses of DTP vaccine were determined by estimating the DTP2 vaccination coverage from the mean DTP1 and DTP3 coverage. However, this method can be considered adequate because the WHO-UNICEF immunization information system does not provide data for the DTP2 vaccine. Thirdly, anti-pertussis herd immunity levels in different countries and WHO regions were assessed by assuming vaccine effectiveness levels of 84%, 77%, and 59% for three, two and one vaccine doses, respectively. Greater or lower effectiveness values would result in greater or lower levels of anti-pertussis herd immunity, respectively. However, the vaccination effectiveness assumed in this study was based on evaluative studies [18,19]. Fourthly, anti-pertussis herd immunity levels were assessed against Bordetella pertussis with Ro values ranging from 10 to 18. Ro values lower than 10 would result in s greater than those found in this study in different countries and WHO regions. However, this range derived from studies assessing Bordetella pertussis transmissibility [9,48].
5. Conclusion
This study found that global and regional DTP vaccination coverage and anti-pertussis herd immunity indicators in 2024 did not recover completely to pre-COVID levels. The mean DTP1 coverage, mean DTP3 coverage, mean three-dose DTP coverage, mean zero-dose DTP coverage, percentage of countries with three-dose coverage ≥95% and ≥90, percentage of countries where one-year-old children had received at least one dose of DTP vaccine, and mean prevalence of one-year-old children with vaccine-induced pertussis protection worsened worldwide from 2019 to 2024. In addition, the zero-dose DTP vaccination coverage and the number of zero-dose DTP children were not on track to achieve the Immunization Agency 2030 objective. Interventions to increase routine DTP vaccination coverage among children aged less than one year should be developed in all WHO regions to improve routine DTP vaccination programs.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Vaccination coverage for first (DTP1) and third (DTP3) dose of DTP vaccine, three-dose DTP vaccination coverage, zero-dose DTP vaccination coverage, and prevalence of vaccine-induced pertussis protection among one-year-old children in different countries in 2024; Table S2: High-priority countries for DTP vaccination coverage increase in different WHO regions, based on four indicators: 1) zero-dose DTP coverage lower than the regional mean (very high priority); three-dose DTP coverage <80% and lower than the regional mean; 3) DTP1 vaccination coverage <90%; and 4) DTP3 vaccination coverage <90%.
Funding
This research received no external funding.
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Acknowledgments
Mean percentages of measles routine vaccination coverage in regions of the WHO were calculated using the information of the WHO and UNICEF on “WHO/UNICEF estimates of routine vaccines”:.
Conflicts of Interest
The author declares no conflicts of interest.
References
- Decker, M.D.; Edwards, K.M. Pertussis (whooping cough). J. Infect. Dis. 2021, 224, S310–S320. [Google Scholar] [CrossRef]
- Mi, Y.M.; Deng, J.K.; Zhang, T.; Cao, Q.; Wang, C.Q.; Ye, S.; Chen, Y.H.; He, H.Q.; Wu, B.B.; Liu, Y.; Zeng, M.; Li, W.; Wu, F.; Xu, H.M.; Zhao, S.Y.; Liu, G.; Hua, W.; Xu, D.; Bai, G.N.; Yang, Y.; Huang, L.S.; Chen, Y.P.; Yao, K.H.; Shao, Z.J.; Hua, C.Z. Expert consensus for pertussis in children: new concepts in diagnosis and treatment. World J. Pediatr. 2024, 20, 1209−1222. [Google Scholar] [CrossRef] [PubMed]
- Bricks, L.F.; Vargas-Zambrano, J.C.; Macina, D. Epidemiology of Pertussis After the COVID-19 Pandemic: Analysis of the Factors Involved in the Resurgence of the Disease in High-, Middle-, and Low-Income Countries. Vaccines 2024, 12, 1346. [Google Scholar] [CrossRef] [PubMed]
- Mengyang, G.; Yahong, H.; Qinghong, M.; Wei, S.; Kaihu, Y. Resurgence and atypical patterns of pertussis in China. J. Infect. 2024, 88, 106140. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Pertussis reported cases and incidence. Pertussis reported cases and incidence (accessed on 12 October 2025).
- Nian, X.; Liu, H.; Cai, M.; Duan, K.; Yang, X. Coping Strategies for Pertussis Resurgence. Vaccines 2023, 11, 889. [Google Scholar] [CrossRef]
- Gambhir, M.; Clark, T.A.; Cauchemez, S.; Tartof, S.Y.; Swerdlow, D.L.; Ferguson, N.M. A change in vaccine efficacy and duration of protection explains recent rises in pertussis incidence in the United States. PLoS Comput. Biol. 2015, 11, e1004138. [Google Scholar] [CrossRef]
- Fu, P.; Wang, C.; Tian, H.; Kang, Z.; Zeng, M. Bordetella pertussis Infection in Infants and Young Children in Shanghai, China, 2016-2017: Clinical Features, Genotype Variations of Antigenic Genes and Macrolides Resistance. Pediatr. Infect. Dis. J. 2019, 38, 370−376. [Google Scholar] [CrossRef]
- Plans-Rubió, P. Vaccination Coverage for Routine Vaccines and Herd Immunity Levels against Measles and Pertussis in the World in 2019. Vaccines 2021, 9, 256. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Global Vaccine Action Plan; WHO: Geneve, Switzerland, 2020; Available online: https://www.who.int/publications/i/item/global-vaccine-action-plan-2011-2020 (accessed on 15 October 2025).
- WHO-UNICEF. Immunization Agenda 2030. A Global Strategy to Leave No One Behind. Available online: https://cdn.who.int/media/docs/default-source/immunization/strategy/ia2030/ia2030-draft-4-wha_b8850379-1fce-4847-bfd1-5d2c9d9e32f8.pdf?sfvrsn=5389656e_69&download=true (accessed on 15 October 2025).
- World Health Organization (WHO). Vaccination schedule for pertussis. Vaccination schedule for Pertussis (accessed on 15 October 2025).
- WHO-UNICEF. Implementing the Immunization Agenda 2030: A framework for action. Implementing the Immunization Agenda 2030 (acc4esed on 10 October 2025).
- World Health Organization (WHO). Diphtheria tetanus toxoid and pertussis (DTP) vaccination coverage. Available on line: Diphtheria tetanus toxoid and pertussis (DTP) vaccination coverage. (accessed on 5 December 2025).
- UNICEF. Immunization. Available on line: Vaccination and Immunization Statistics - UNICEF DATA (accessed on 5 December 2025).
- WHO-UNICEF. Progress and Challenges with Achieving Universal Immunization Coverage. 2024 Estimates of National Immunization Coverage (Released 15 July 2025). Geneve: WHO/UNICEF, 2025. Available online: Progress and challenges with Achieving Universal Immunization Coverage.
- Burton, A.; Monasch, R.; Lautenbach, B.; Gacic-Dobo, M.; Neill, M.; Karimov, R.; Wolfson, I.; Jones, G.; Birmingham, M. WHO and UNICEF estimates of national infant immunization coverage: methods and processes. Bull. World Health Organ. 2009, 87, 535−541. [Google Scholar] [CrossRef]
- Greco, D.; Salmaso, S.; Mastrantonio, P.; Giuliano, M.; Tozzi, A.E.; Anemona, A.; Ciofi Deggli Atti, M.L.; Giammanco, A.; Panei, P.; Blackwelder, W.C.; et al. A controlled trial of two acellular vaccines and one whole-cell vaccine against pertussis. N. Engl. J. Med. 1996, 334, 341–348. [Google Scholar] [CrossRef]
- Zhang, L.; Prietsch, S.O.M.; Axelsson, I; Halperin, S.A. Acellular vaccines for preventing whooping cough in children. Cochrane Database of Systematic Reviews 2014, Issue 9. Art. No., CD001478. [Google Scholar] [CrossRef] [PubMed]
- Parikh, J.; Hoare, I.; Izurieta, R. Evaluating the Relationship Between the Introduction of the Acellular Pertussis Vaccine and Whooping Cough Resurgence in the United States. Vaccines 2025, 13, 841. [Google Scholar] [CrossRef] [PubMed]
- Wendelboe, AM; Van Rie, A; Salmaso, S; Englund, JA. Duration of immunity against pertussis after natural infection or vaccination. Pediatr. Infect. Dis. J. 2005, 24, S58–61. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Caulfield, A.; Dewan, K.K.; Harvill, E.T. Pertactin-Deficient Bordetella pertussis, Vaccine-Driven Evolution, and Reemergence of Pertussis. Emerg. Infect. Dis. 2021, 27, 1561–1566. [Google Scholar] [CrossRef]
- Barkoff, A.M.; Mertsola, J.; Guillot, S.; Guiso, N.; Berbers, G.; He, Q. Appearance of Bordetella pertussis Strains not Expressing the Vaccine Antigen Pertactin in Finland. Clin. Vaccine Immunol. CVI 2012, 19, 1703–1704. [Google Scholar] [CrossRef]
- Nian, X.; Liu, H.; Cai, M.; Duan, K.; Yang, X. Coping Strategies for Pertussis Resurgence. Vaccines 2023, 11, 889. [Google Scholar] [CrossRef]
- Bricks, L.F.; Vargas-Zambrano, J.C.; Macina, D. Epidemiology of Pertussis After the COVID-19 Pandemic: Analysis of the Factors Involved in the Resurgence of the Disease in High-, Middle-, and Low-Income Countries. Vaccines 2024, 12, 1346. [Google Scholar] [CrossRef]
- Risti’c, M.; Radosavljevi’c, B.; Stojanovi’c, V.D.; Dilas, M.; Petrovi’c, V. Performance of the new clinical case definitions of pertussis in pertussis suspected infection and other diagnoses similar to pertussis. PLoS ONE 2018, 13, e0204103. [Google Scholar]
- Cherry, J.D.; Tan, T.; von-Konig, C.H.W.; Forsyth, K.D.; Thisyakorn, U.; Greenberg, D.; Johnson, D.; Marchant, C.; Plotkin, S. Clinical definitions of pertussis: Summary of a Global Pertussis Initiative roundtable meeting. Clin. Infect. Dis. 2012, 54, 1756–1764. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Laboratory Manual for the Diagnosis of Whooping Cough Caused by Bordetella Pertussis/Bordetella Parapertussis; WHO: Geneva, Switzerland, 2014; Available online: http://apps.who.int/iris/bitstream/10665/127891/1/WHO_IVB_14.03_eng.pdf (accessed on 16 July 2025).
- Centers for Disease Control and Prevention (CDC). Laboratory Testing for Pertussis|Pertussis (Whooping Cough). CDC. Available online: https://www.cdc.gov/pertussis/php/laboratories/index.html (accessed on 15 December 2025).
- World Health Organization (WHO). Varied Impact of COVID-19 on Routine Immunization in the European Region. Available online: https://www.who.int/europe/news/item/16-07-2021-varied-impact-of-covid-19-on-routine-immunization-in-the-european-region.
- Jones, C.E.; Danovaro-Holliday, M.C.; Mwinnyaa, G.; Gacic-Dobo, M.; Francis, L.; Grevendonk, J.; Nedelec, Y.; Wallace, A.; Sodha, S.V.; Sugerman, C. Routine Vaccination Coverage — Worldwide, 2023. MMWR Morb. Mortal. Wkly. Rep. 2024, 73, 978–984. [Google Scholar] [CrossRef]
- Santoli, J.M.; Lindley, M.C.; De Silva, M.B.; Kharbanda, E.O.; Daley, M.F.; Galloway, L.; Gee, J.; Glover, M.; Herring, B.; Kang, Y.; et al. Effects of the COVID-19 Pandemic on Routine Pediatric Vaccine Ordering and Administration—United States, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 591–593. [Google Scholar] [CrossRef]
- Aguinaga-Ontoso, I.; Guillen-Aguinaga, S.; Guillen-Aguinaga, L.; Alas-Brun, R.; Guillen-Aguinaga, M.; Onambele, L.; Aguinaga-Ontoso, E.; Rayón-Valpuesta, E.; Guillen-Grima, F. The Impact of COVID-19 on DTP3 Vaccination Coverage in Europe (2012–2023). Vaccines 2025, 13, 6. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Barchitta, M.; Cappuccio, G.; Favara, G.; Magnano San Lio, R.; Agodi, A. Trends of Diphtheria–Tetanus–Pertussis and Measles Vaccine Coverage Preceding and during the COVID-19 Pandemic: An Analysis of the WHO European Region from 2000 to 2022. Vaccines 2024, 12, 1145. [Google Scholar] [CrossRef] [PubMed]
- Aguinaga-Ontoso, I.; Guillén-Aguinaga, S.; Guillén-Aguinaga, L.; Alas-Brun, R.; Aguinaga-Ontoso, E.; Rayón-Valpuesta, E.; Guillén-Grima, F. Has COVID-19 Affected DTP3 Vaccination in the Americas? Vaccines 2024, 12, 238. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.H.; Srivastav, A.; Lindley, M.C.; Fisher, A.; Kim, D.; Greby, S.M.; Lee, J.; Singleton, J.A. Parental Vaccine Hesitancy and Association With Childhood Diphtheria, Tetanus Toxoid, and Acellular Pertussis; Measles, Mumps, and Rubella; Rotavirus; and Combined 7-Series Vaccination. Am J Prev Med. 2022, 62, 367−376. [Google Scholar] [CrossRef]
- Sharif-Nia, H.; She, L.; Allen, KA.; et al. Parental hesitancy toward children vaccination: a multi-country psychometric and predictive study. BMC Public Health 2024, 24, 1348. [Google Scholar] [CrossRef]
- Loomba, S.; de Figueiredo, A.; Piatek, S.J.; de Graaf, K.; Larson, H.J. Measuring the impact of COVID-19 vaccine misinformation on vaccination intent in the UK and USA. Nat. Hum. Behav. 2021, 5, 337–348. [Google Scholar] [CrossRef]
- Trent, M.; Seale, H.; Chughtai, A.A.; Salmon, D.; Mac Intyre, C.R. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: a comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine 2022, 40, 2498–505. [Google Scholar] [CrossRef]
- Omar, M.; Shibli, H.; Edelstein, M. Comparative impact of the COVID-19 pandemic on parental behaviour towards childhood vaccination in Israel and the United Kingdom: A self-controlled matched cross-sectional study. Vaccine 2025, 61, 127385. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Summary of the Pertussis Vaccines: WHO Position Paper-September. 2015. Available online: https://cdn.who.int/media/docs/default-source/immunization/position_paper_documents/pertussis/pertussis-pp-2015-summary.pdf (accessed on 10 November 2025).
- European Centre for Disease Prevention and Control (ECDC). Vaccine scheduler. Pertussis: Recommended vaccinations. Available online: https://vaccine-schedule.ecdc.europa.eu/Scheduler/ByDisease?SelectedDiseaseId=3&SelectedCountryIdByDisease=-1 (accessed on 15 January 2026).
- Leontari, K.; Lianou, A.; Tsantes, A.G.; Filippatos, F.; Iliodromiti, Z.; Boutsikou, T.; Paliatsou, S.; Chaldoupis, A.E.; Ioannou, P.; Mpakosi, A.; et al. Pertussis in Early Infancy: Diagnostic Challenges, Disease Burden, and Public Health Implications Amidst the 2024 Resurgence, with Emphasis on Maternal Vaccination Strategies. Vaccines 2025, 13, 276. [Google Scholar] [CrossRef]
- Merdrignac, L.; Acosta, L.; Habington, A.; Garc.a-Cenoz, M.; Pandolfi, E.; Fabianova, K.; Jordan, I.; O’Sullivan, N.; Navasues, A.; Tozzi, A.E.; et al. Effectiveness of pertussis vaccination in pregnancy to prevent hospitalisation in infants aged <2 months and effectiveness of both primary vaccination and mother’s vaccination in pregnancy in infants aged 2–11 months. Vaccine 2022, 40, 6374–6382. [Google Scholar] [CrossRef]
- Chakrabarti, A.; Grépin, K.A.; Helleringer, S. The impact of supplementary immunization activities on routine vaccination coverage: An instrumental variable analysis in five low-income countries. PLoS One 2019, 14, e0212049. [Google Scholar] [CrossRef]
- Arevshatian, L.; Clements, C.; Lwanga, S.; Misore, A.; Ndumbe, P.; Seward, J.; Taylor, P. An evaluation of infant immunization in Africa: is a transformation in progress? Bull. World Health Organ. 2007, 85, 449−457. [Google Scholar] [CrossRef]
- Burton, A.; Kowalski, R.; Gacic-Dobo, M.; Karimov, R.; Brown, D. A Formal Representation of the WHO and UNICEF Estimates of National Immunization Coverage: A Computational Logic Approach. PLoS ONE 2012, 7, e47806. [Google Scholar] [CrossRef]
- Anderson, R. M.; May, R. M. Infectious Diseases of Humans: Dynamics and Control; Oxford University Press: Oxford, 1991. [Google Scholar]
Figure 1.
Number of pertussis cases reported worldwide from 2000 to 2024. .
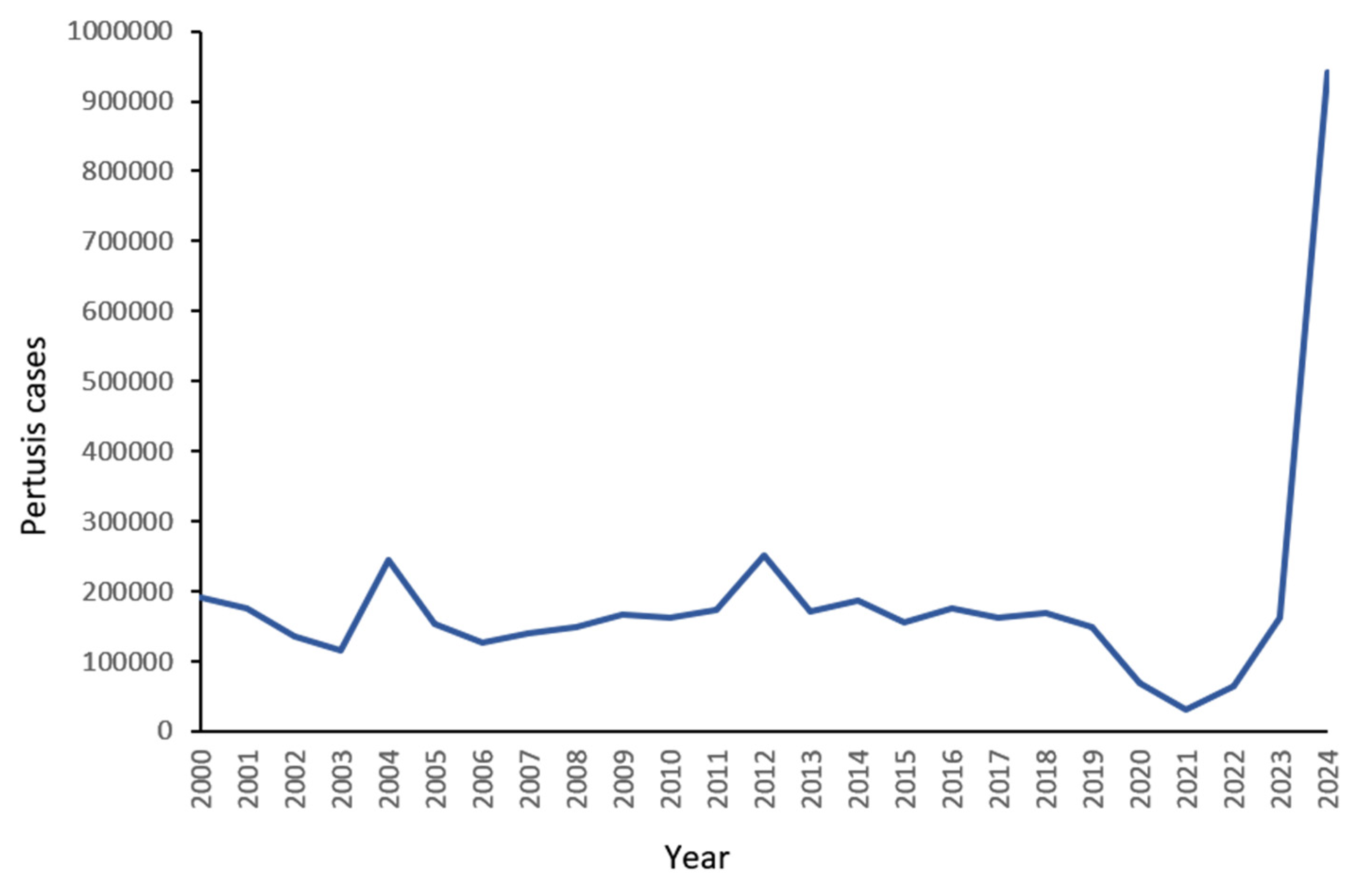
Figure 2.
Variation from 2019 to 2024 for mean DTP1 vaccination coverage worldwide and in WHO regions.
Figure 2.
Variation from 2019 to 2024 for mean DTP1 vaccination coverage worldwide and in WHO regions.
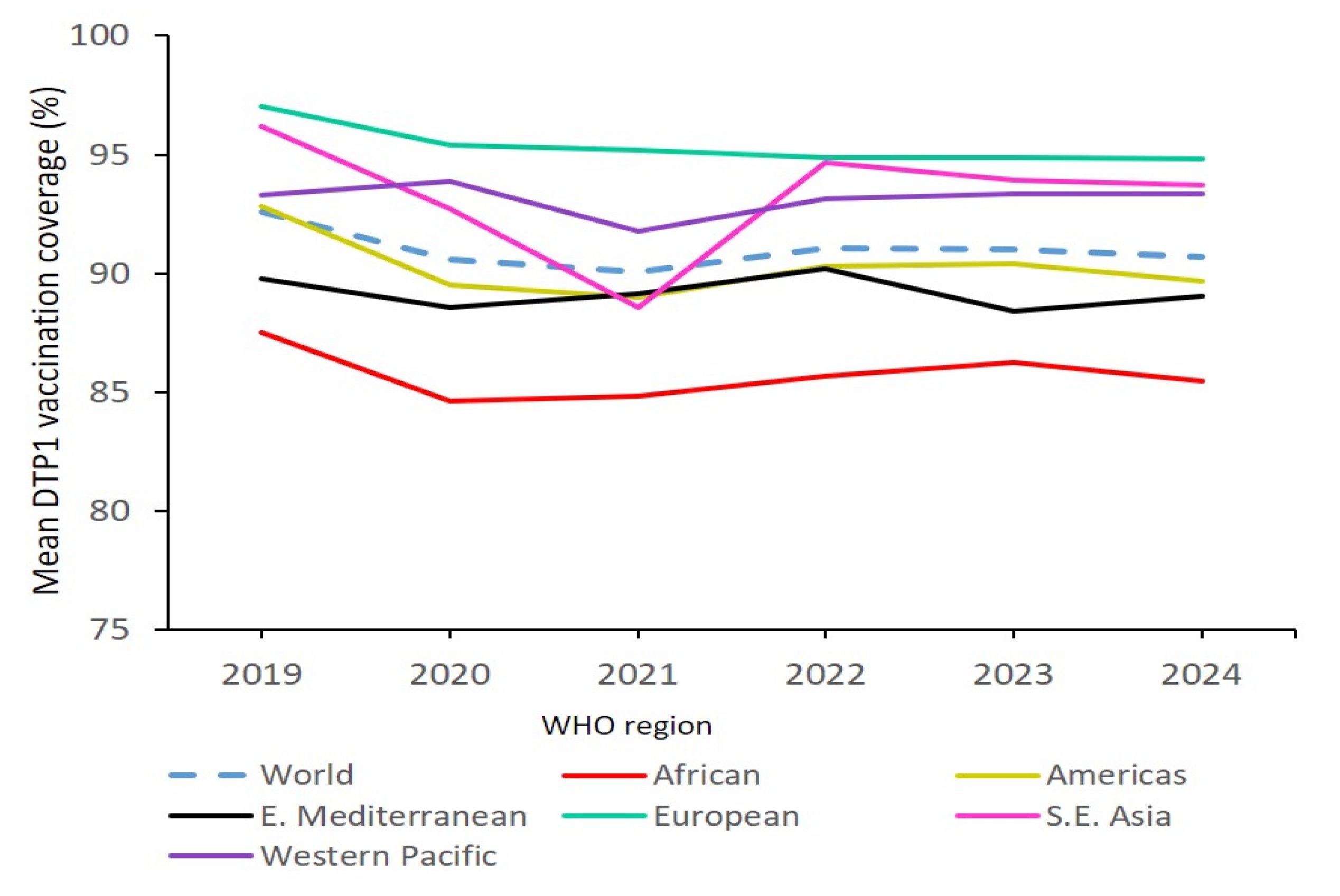
Figure 3.
Variation from 2019 to 2024 for mean DTP3 vaccination coverage worldwide and in WHO regions.
Figure 3.
Variation from 2019 to 2024 for mean DTP3 vaccination coverage worldwide and in WHO regions.
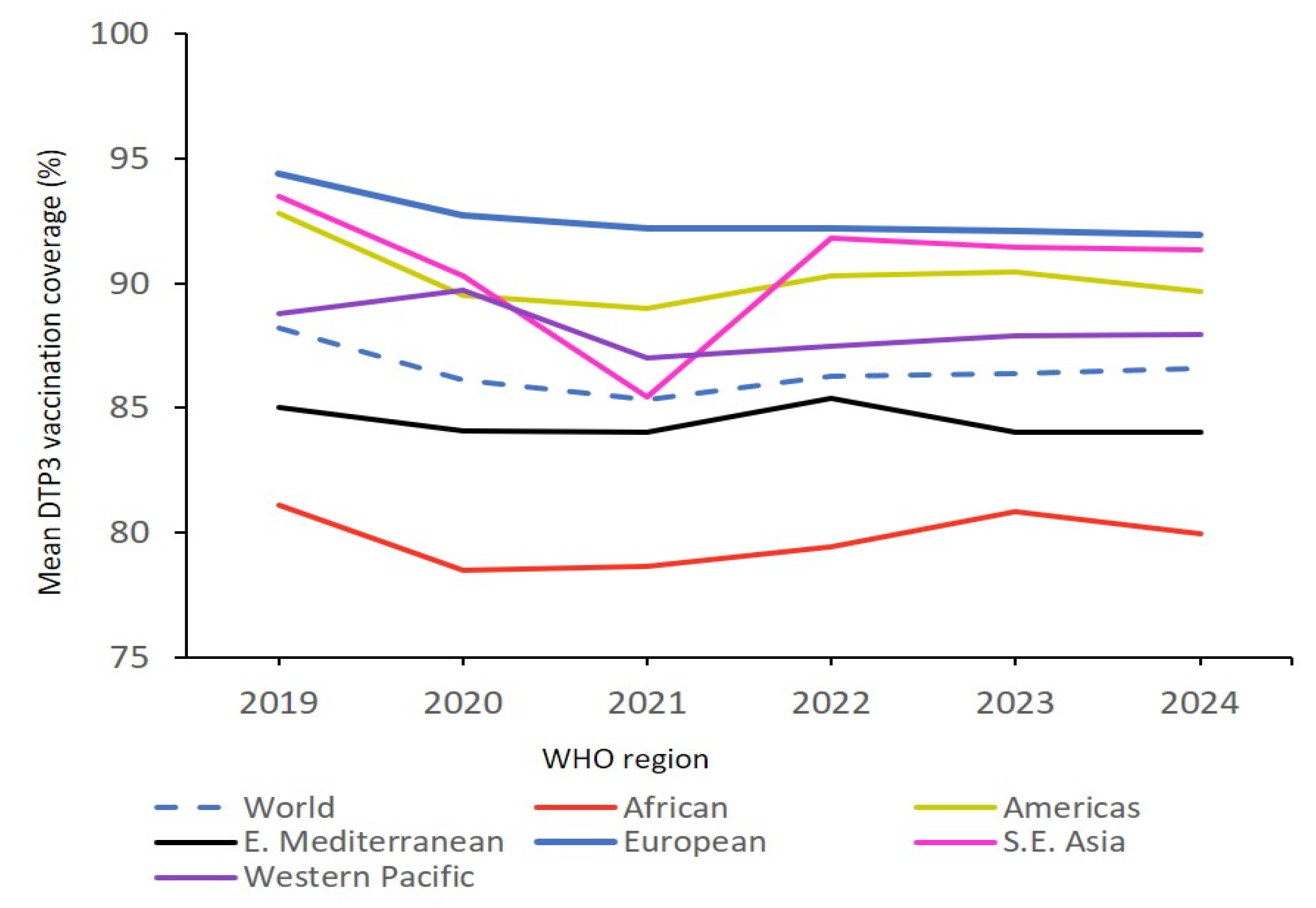
Figure 4.
Zero-dose DTP vaccination coverage in WHO regions from 2019 to 2024.
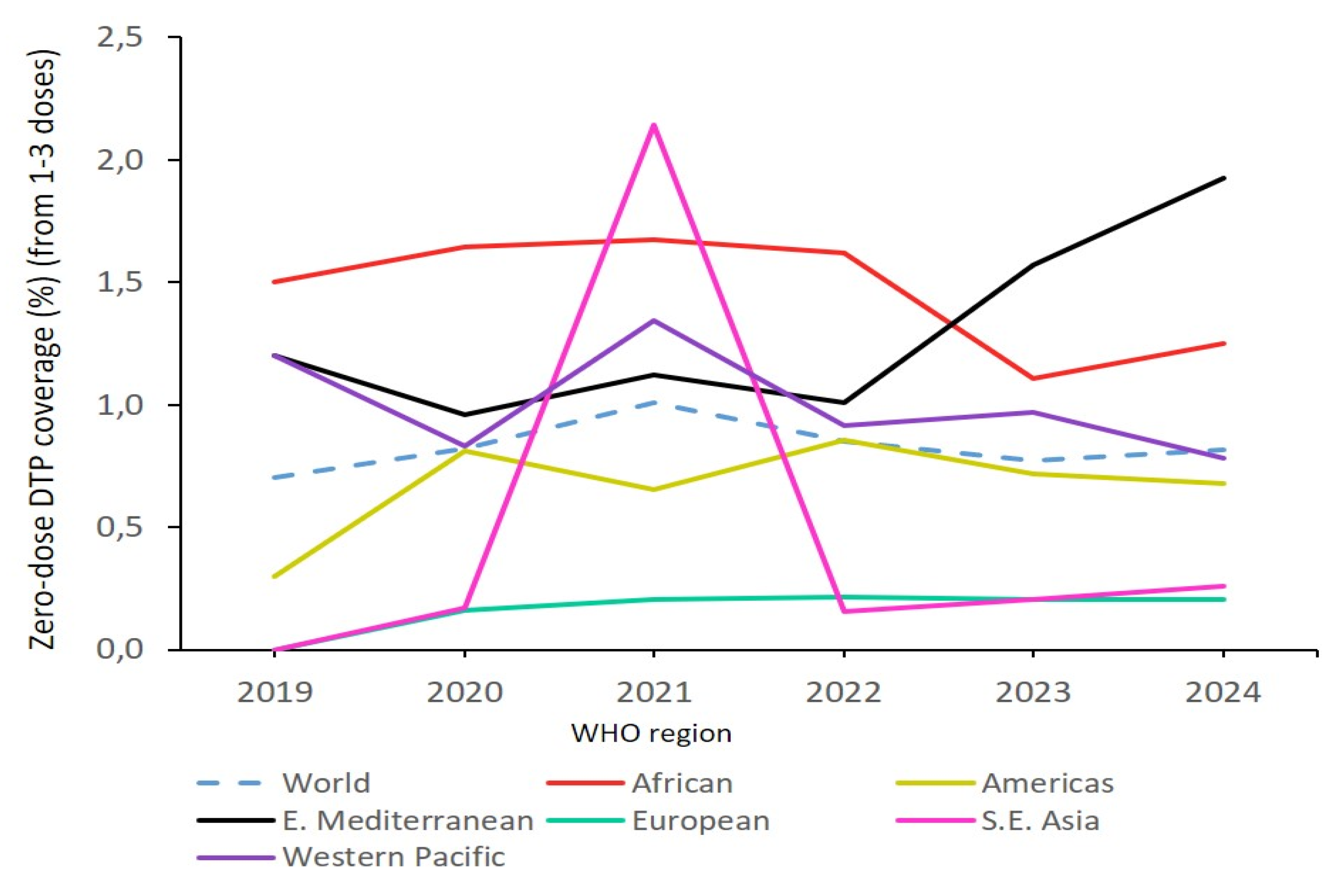
Figure 5.
Number of zero-dose DTP children (based on DTP1 coverage) estimated by WHO-UNICEF and number required from 2019 to 2030 to achieve the IA 2030 objective (6.43 million).
Figure 5.
Number of zero-dose DTP children (based on DTP1 coverage) estimated by WHO-UNICEF and number required from 2019 to 2030 to achieve the IA 2030 objective (6.43 million).
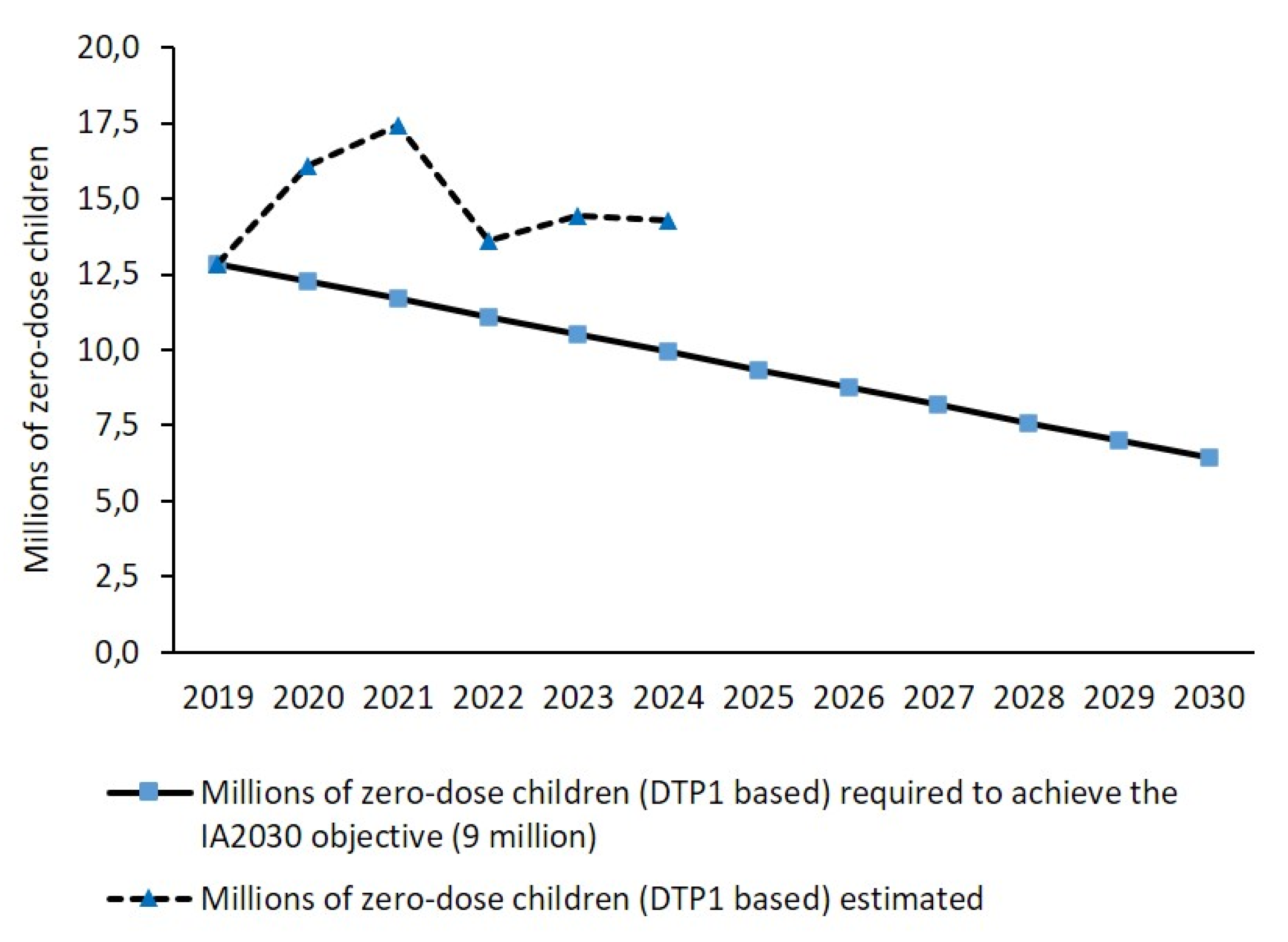
Figure 6.
Zero-dose DTP vaccination coverage (determined from 100 – DTP1) observed from 2019 to 2024, and zero-dose coverage required from 2019 to 2030 to achieve the IA 2030 objective (3.7%).
Figure 6.
Zero-dose DTP vaccination coverage (determined from 100 – DTP1) observed from 2019 to 2024, and zero-dose coverage required from 2019 to 2030 to achieve the IA 2030 objective (3.7%).
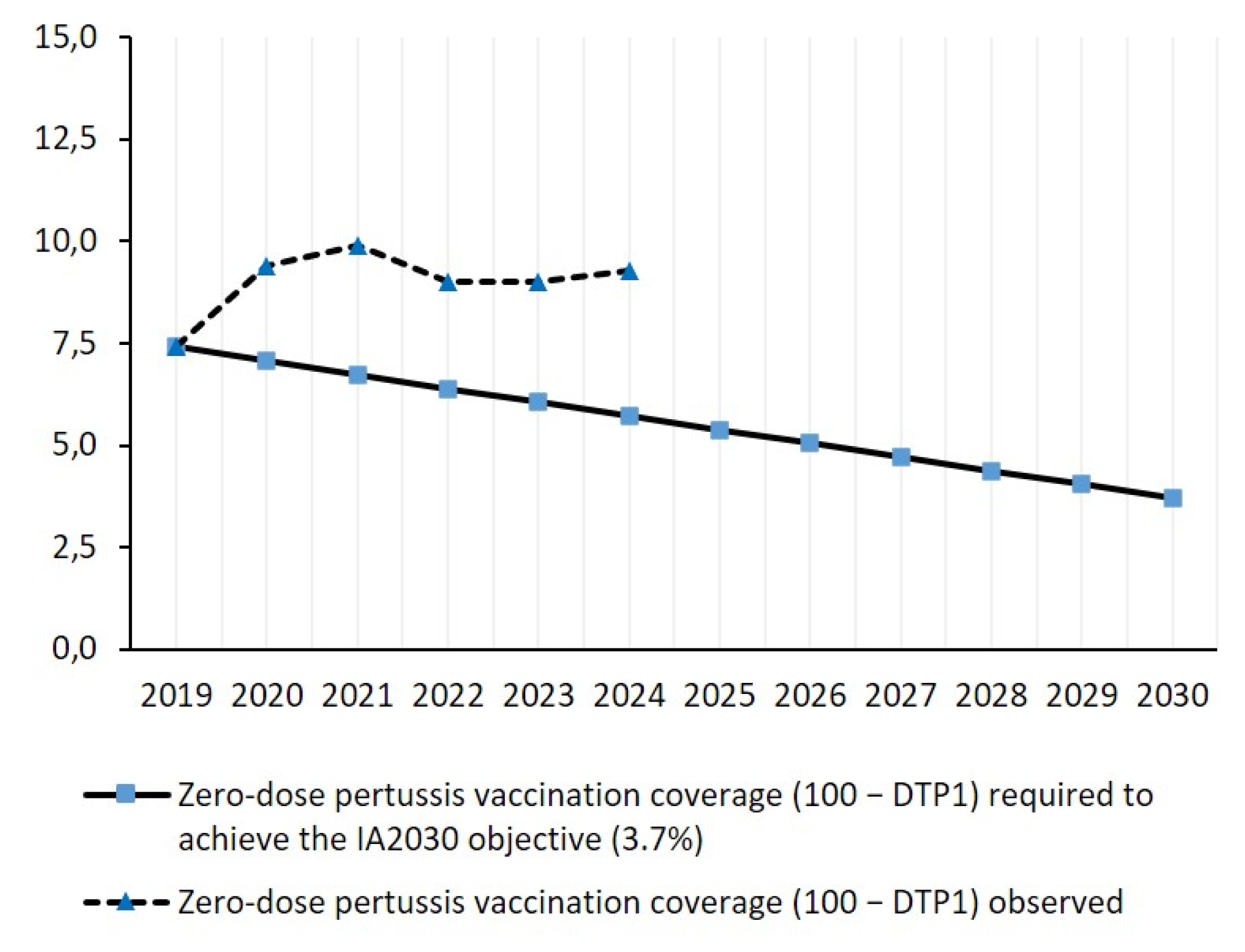
Figure 7.
Zero-dose DTP vaccination coverage observed from 2019 to 2024, and zero-dose coverage required from 2019 to 2030 to achieve the IA 2030 objective (0.35%).
Figure 7.
Zero-dose DTP vaccination coverage observed from 2019 to 2024, and zero-dose coverage required from 2019 to 2030 to achieve the IA 2030 objective (0.35%).
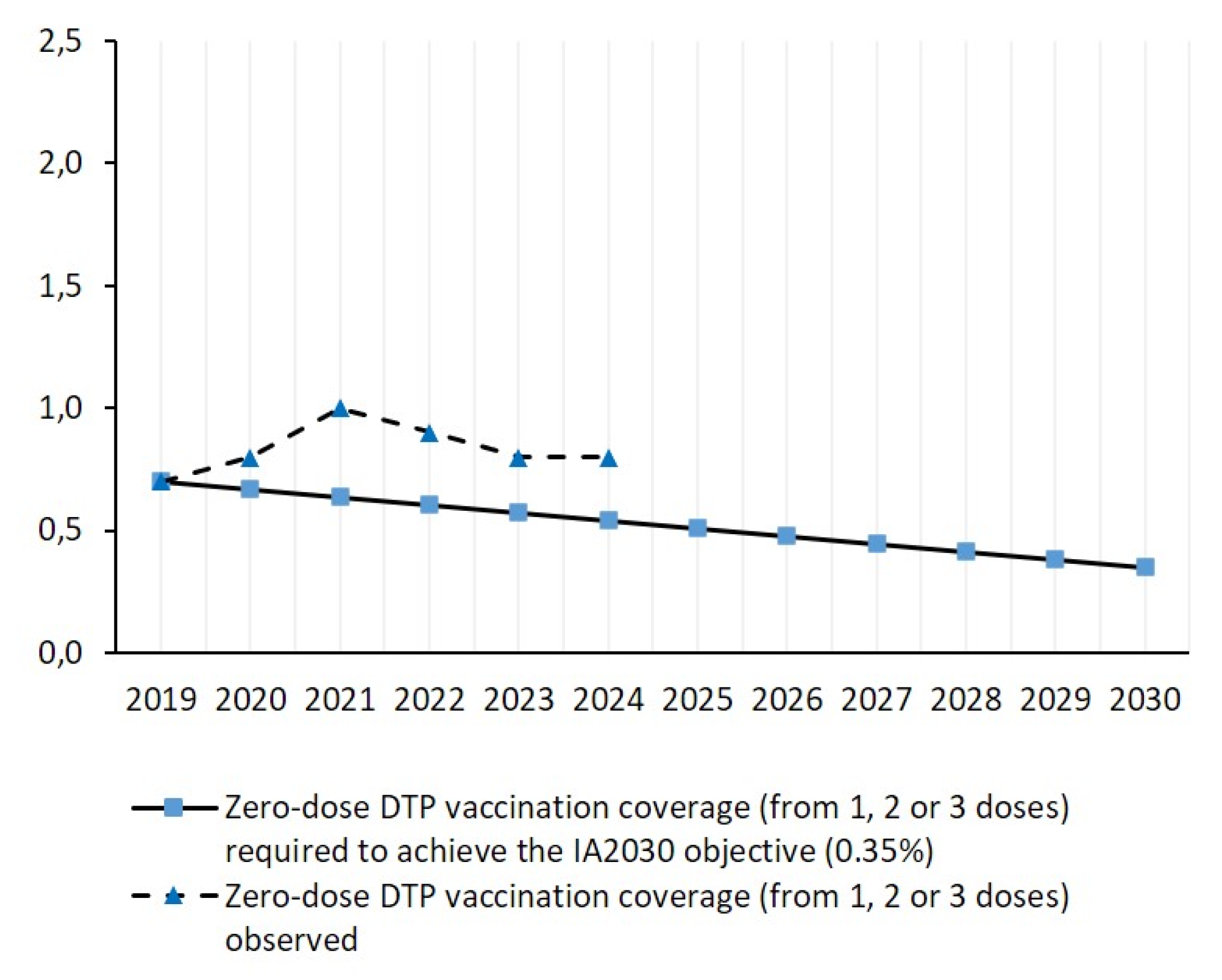

Table 1.
DTP vaccination coverage and anti-pertussis herd immunity indicators worldwide and in WHO regions in 2024. Mean vaccination coverage with DTP1 and DTP3 vaccines; mean vaccination coverage with zero, one, two and three doses of DTP vaccine; percentage of countries with three-dose coverage ≥95 and ≥90; percentage of countries where all children aged one year could have received at least one dose of DTP vaccine (0% zero-dose children); prevalence of children aged one year with vaccine-induced pertussis protection; and percentage of countries with herd immunity in the target population with vaccination against Bordetella pertussis (Ro from 10 to 18).
Table 1.
DTP vaccination coverage and anti-pertussis herd immunity indicators worldwide and in WHO regions in 2024. Mean vaccination coverage with DTP1 and DTP3 vaccines; mean vaccination coverage with zero, one, two and three doses of DTP vaccine; percentage of countries with three-dose coverage ≥95 and ≥90; percentage of countries where all children aged one year could have received at least one dose of DTP vaccine (0% zero-dose children); prevalence of children aged one year with vaccine-induced pertussis protection; and percentage of countries with herd immunity in the target population with vaccination against Bordetella pertussis (Ro from 10 to 18).
| World | African Region | Americas Region | Eastern Mediterranean Region |
European Region | South-East Asia Region | Western Pacific Region |
|
|---|---|---|---|---|---|---|---|
| No. of countries | 195 | 47 | 35 | 22 | 53 | 11 | 27 |
| DTP vaccination coverage indicators | |||||||
| Mean vaccination coverage (%) with DTP1 and DTP3 vaccines | |||||||
| DTP1 | 90.7 | 85.5 | 89.7 | 89.0 | 94.8 | 93.7 | 93.3 |
| DTP3 | 86.6 | 79.9 | 86.4 | 84.0 | 91.9 | 91.4 | 88.0 |
| Mean vaccination coverage (%) with three, two, one and zero doses of DTP vaccine | |||||||
| 3 doses | 72.8 | 59.5 | 71.0 | 71.0 | 82.5 | 81.1 | 77.5 |
| 2 doses | 21.1 | 30.4 | 22.7 | 19.6 | 15.3 | 15.8 | 17.7 |
| 1 dose | 5.3 | 8.9 | 5.6 | 7.5 | 2.0 | 2.9 | 4.0 |
| 0 doses | 0.8 | 1.2 | 0.7 | 1.9 | 0.2 | 0.3 | 0.5 |
| Percentage of countries with three-dose DTP vaccination coverage ≥ 95% and ≥90% | |||||||
| ≥95% | 12.3 | 2.1 | 17.1 | 9.1 | 15.1 | 18.2 | 18.5 |
| ≥90% | 21.0 | 4.2 | 20.0 | 9.1 | 34.0 | 18.2 | 37.0 |
| Percentage of countries where all children aged one year could have received at least one dose of DTP vaccine (without zero-dose children) | |||||||
| 80.5 | 78.6 | 80.4 | 79.1 | 82.3 | 82.0 | 81.1 | |
| Anti-pertussis herd immunity indicators | |||||||
| Mean prevalence (%) of vaccine-induced pertussis protection pertussis protection in children aged one year | |||||||
| Pertussis immunity | 53.3 | 27.7 | 45.7 | 59.1 | 67.9 | 72.7 | 66.7 |
| Percentage of countries with sufficient herd immunity against Bordetella pertussis with Ro from 10 to 18 | |||||||
| Ro ≤ 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ro ≤ 12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ro ≤ 15 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ro ≤ 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Table 2.
Variation from 2019 to 2024 for DTP vaccination coverage and anti-pertussis herd immunity indicators worldwide and in WHO regions.
Table 2.
Variation from 2019 to 2024 for DTP vaccination coverage and anti-pertussis herd immunity indicators worldwide and in WHO regions.
| World | African Region | Americas Region | Eastern Mediterranean Region | European Region | South-East Asia Region | Western Pacific Region | |
|---|---|---|---|---|---|---|---|
| No. of countries | 195 | 47 | 35 | 22 | 53 | 11 | 27 |
| DTP vaccination coverage indicators | |||||||
| Mean vaccination coverage (%) with DTP1 and DTP3 vaccines | |||||||
| DTP1 | −2.0 | −2.3 | −3.4 | −0.8 | −2.3 | −2.6 | 0.0 |
| DTP3 | −1.8 | −1.4 | −2.2 | −1.1 | −2.6 | −2.3 | −0.9 |
| Mean vaccination coverage (%) with three, two, one and zero doses of DTP vaccine | |||||||
| 3 doses | -5.5 | -7.2 | -6.5 | -0.4 | -6.4 | -5.6 | -2.9 |
| 2 doses | 17.2 | 16.5 | 12.9 | -6.2 | 37.8 | 22.5 | 20.4 |
| 1 dose | 23.3 | 7.2 | 51.4 | 13.6 | 150.0 | 141.7 | -7.0 |
| 0 doses | 14.3 | -20.0 | 133.3 | 58.3 | - | - | -33.3 |
| Percentage of countries with three-dose DTP vaccination coverage ≥ 95% and ≥90% | |||||||
| ≥95% | -31.7 | -50.0 | 19.6 | -61.8 | -33.2 | 0.0 | -44.4 |
| ≥90% | -38.2 | -34.4 | -22.2 | -68.2 | -35.6 | -66.6 | -28.6 |
| Percentage of countries where all children aged one year could have received at least one dose of DTP vaccine (without zero-dose children) | |||||||
| −17.2 | −34.8 | −20.0 | 12.8 | -24.0 | 0.0 | -14.3 | |
| Anti-pertussis herd immunity indicators | |||||||
| Mean prevalence (%) of vaccine-induced pertussis protection pertussis protection in children aged one year | |||||||
| Pertussis immunity | -8.6 | 1.3 | -12.4 | -10.3 | -12.2 | -12.0 | -8.7 |
| Percentage of countries with sufficient herd immunity against Bordetella pertussis with Ro from 10 to 18 | |||||||
| Ro ≤ 10 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ro ≤ 12 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ro ≤ 15 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Ro ≤ 18 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
Table 3.
No. (%) of high-priority countries worldwide and in different WHO region for routine DTP vaccination coverage increase based on four criteria: 1) zero-dose DTP coverage greater than the regional mean coverage (very high priority); 2) three-dose DTP coverage lower than 80% and lower than the regional mean; 3) DTP1 coverage lower than 90%; 4) DTP3 coverage lower than 90%.
Table 3.
No. (%) of high-priority countries worldwide and in different WHO region for routine DTP vaccination coverage increase based on four criteria: 1) zero-dose DTP coverage greater than the regional mean coverage (very high priority); 2) three-dose DTP coverage lower than 80% and lower than the regional mean; 3) DTP1 coverage lower than 90%; 4) DTP3 coverage lower than 90%.
|
Criteria |
No. (%) of high-priority countries for routine DTP vaccination coverage increase based on four criteria | ||||||
| World | African region |
Americas region |
Eastern Mediterranean region |
European region |
South-East Asia region | Western Pacific region |
|
| 0-dose DTP coverage < regional mean |
37 (19.0) | 15 (31.9) | 7 (20.0) | 5 (22.7) | 4 (7.5) | 2 (18.2) | 4 (14.8) |
| 3-dose DTP vaccination coverage <80% and <regional mean |
78 (40.0) | 22 (46.8) | 15 (42.9) | 8 (36.4) | 18 (34.0) | 4 (36.4) | 11 (40.7) |
| DTP1 vaccination coverage <90% |
58 (29.7) | 25 (53.2) | 14 (40.0) | 7 (31.8) | 5 (9.4) | 3 (27.3) | 4 (14.8) |
| DTP3 vaccination coverage <90% |
85 (43.6) | 31 (66.0) | 16 (45.7) | 9 (40.9) | 15 (28.3) | 3 (27.3) | 11 (40.7) |
| No. of countries | 195 | 47 | 35 | 22 | 53 | 11 | 27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



