Submitted:
02 February 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
This article examines how sustainability is understood and enacted within South Africa’s private healthcare sector, a setting marked by high resource intensity, concentrated ownership, and uneven regulatory guidance. The study investigates which sustainability practices matter most and how they can be systematically integrated into organisational routines. A qualitative interpretivist methodology was used, drawing on phenomenological interviews with seventeen professionals across clinical, managerial, and operational roles. Data were analysed using thematic analysis to identify patterns in the implementation of environmental, operational, and governance practices. The analysis revealed that sustainability is shaped by the interaction of leadership commitment, coordinated governance structures, resource optimisation in high consumption areas, and integrated performance feedback. These dynamics coalesced into the Sustainability Integration and Performance Model (SIPM), which advances existing scholarship by demonstrating how sustainability becomes a coherent organisational capability rather than a set of isolated initiatives. The findings provide novel insights into how private healthcare organisations navigate institutional ambiguity while aligning stakeholder expectations and developing internal capabilities. The study also highlights the distinct contextual pressures shaping sustainability in South Africa, including infrastructure constraints and varying organisational maturity. While the qualitative scope limits broader generalisation, the research provides a grounded foundation for future comparative studies and the development of measurable indicators for the integration of sustainability.
Keywords:
private healthcare sustainability
; organisational capabilities
; governance integration
; resource optimisation
; systems thinking in healthcare
; sustainability performance
; South Africa healthcare sector
1. Introduction
Sustainability has moved from a peripheral concern to a strategic imperative in healthcare globally. Health systems are high-intensity users of energy, water, materials, and single-use products, generating substantial waste and contributing materially to greenhouse gas emissions. Recent syntheses estimate the sector’s climate footprint at roughly 6–8% of global emissions, with operating rooms and energy-hungry diagnostics among the most carbon-intensive hotspots [1,2,3]. Within this context, sustainability is increasingly framed as congruent with clinical excellence rather than in competition with it, as environmental stewardship, resource efficiency and care quality can be mutually reinforcing when embedded into everyday practice and governance.
South Africa exemplifies both the urgency and opportunity for sustainable transformation in private healthcare. Hospitals are the dominant operational units and account for an estimated 50–80% of sectoral resource consumption and around 35% of emissions, underscoring the need for targeted interventions in facilities management, anaesthesia, waste streams and procurement [3,4]Private provision plays an outsized role in the national system: while roughly 84% of the population relies on the public sector, the private sector serves about 16% through medical schemes and out-of-pocket payments and is highly consolidated—approximately 178 private hospitals operate nationally, with a few groups controlling ~80% of private beds [5,6]. Professional interest in environmental sustainability is growing—regional studies report positive attitudes yet variable knowledge, especially in areas such as theatre emissions and waste management [7,8]. These system features collectively make South African private healthcare an important and timely context for empirical inquiry into how sustainability can be systematically integrated into organisational practice.
Despite global and local momentum, the sustainability trajectory in South African private healthcare remains uneven. Evidence indicates that many initiatives are fragmented and unsystematic—often pursued as isolated projects rather than as part of an integrated operating model—owing to skills gaps, limited guidance, and ambiguous or piecemeal regulatory expectations [9,10]. Performance measurement and reporting also lag. Although triple-bottom-line perspectives are widely endorsed, tools for assessing and governing sustainable performance in healthcare remain in the early stages of design and uptake [11]. The cumulative effect is a patchwork of practices that do not consistently translate into operational efficiency, clinical value, or strategic learning across facilities and groups. This study is positioned to address that gap by examining what constitutes “critical” sustainability business practices in the South African private context and how they can be embedded coherently rather than ad hoc.
The article aims to explore the critical sustainability business practices adopted by South Africa’s private healthcare organisations, identify best practices and success factors, and examine mechanisms for their systematic implementation to enhance sustainable performance alongside clinical excellence and economic viability. Guided by this aim, the research addresses the following question: (RQ1) What critical sustainability business practices are adopted in private healthcare, and what success factors enable their uptake? and (RQ2) How can these practices be implemented systematically to improve sustainable performance while maintaining clinical and economic outcomes? These questions deliberately foreground both the “what” and the “how” of sustainability, recognising that design and execution must be considered together to move from aspiration to impact.
A qualitative, interpretivist design was adopted to elicit the lived meanings, rationales, and context-specific trade-offs that underpin sustainability decisions in practice. Interpretivism is well-suited to complex, evolving organisational phenomena such as sustainability, in which stakeholders’ sense-making, values, and experiences shape what is considered feasible and legitimate [12,13]. We conducted semi-structured online interviews (30–60 minutes) with 17 purposively selected professionals across clinical, managerial, and administrative roles in Gauteng and KwaZulu-Natal, enabling variation in vantage points while remaining focused on actors directly involved in implementing sustainability practices. Data were analysed inductively using reflexive thematic analysis supported by ATLAS.ti, following a six-phase process (familiarisation, coding, theme development, review, naming, reporting) and incorporating strategies to ensure trustworthiness (triangulation, audit trail, participant verification, reflexivity [14,15].
Internationally, emerging work highlights pragmatic pathways for greener theatres, energy optimisation, supply chain stewardship, and the digital enablement of low-carbon care [16,17]. In South Africa, however, structural fragmentation between public and private subsystems and variability in governance maturity impede the diffusion of good practice across facilities and groups [5,10]. Furthermore, managerial guidance on configuring leadership, governance, and performance routines to integrate environmental, social, economic, and clinical objectives remains under-specified—a lacuna noted in assessments of sustainability reporting and governance in the South African context [11,18]. Addressing this gap requires context-specific evidence that articulates which practices matter most, which organisational conditions enable them, and how they can be routinised and measured in ways that support, rather than distract from, patient care.
Empirically, the study offers a granular account of sustainability as enacted by private-sector clinicians and managers in South Africa, providing practice-proximal insights that complement top-down frameworks. Conceptually, it advances the SIPM—an integrative lens that links four empirically derived themes: (i) leadership, innovation and engagement as drivers of transformation; (ii) integrated governance and systematic implementation; (iii) resource optimisation and environmental stewardship for operational excellence; and (iv) performance integration and continuous improvement. Collectively, these dimensions explain how private healthcare organisations can treat environmental responsibility, clinical quality and economic performance as mutually reinforcing capabilities rather than competing priorities. For scholars, SIPM synthesises Stakeholder, Resource-Based, Institutional and Systems perspectives into a contextually grounded framework for studying healthcare sustainability. For executives and clinical leaders, it offers actionable guidance on sequencing and aligning initiatives—leadership commitment and staff engagement, governance mechanisms and partnerships, resource-efficiency programmes, and performance routines—to move from fragmented “projects” to coherent, value-creating systems of practice.
In sum, sustainability in private healthcare is both an ethical obligation and a strategic pathway to resilient, high-quality care. Yet without systematic integration, efforts risk remaining episodic and ineffectual. By articulating critical practices and the organisational conditions that sustain them, this article contributes an empirically grounded, theoretically integrated account of how private healthcare in South Africa can embed sustainability to create durable value for patients, professionals, organisations, and society.
2. Literature Review and Theoretical Framing
2.1. Sustainability Practices in Private Healthcare
Across international and South African scholarship, the private hospital is identified as the epicentre of healthcare’s environmental burden, with energy-intensive theatres, diagnostics, sterilisation, and diverse waste streams creating concentrated hotspots that invite managerial intervention and learning [2,3]. Environmental measures that show consistent traction include anaesthetic gas reduction, energy optimisation, greener procurement, and rigorous waste segregation, increasingly organised under holistic facility frameworks rather than single-issue fixes [19,20]. The literature converges on a practical insight. Environmental stewardship that cuts emissions and waste frequently aligns with operational efficiency, which is essential for margin-sensitive private providers seeking reliability in theatre throughput and asset utilisation. These patterns matter for South Africa, where hospitals account for a large share of resource use and emissions, and where facility-level programmes can deliver quick wins that support strategic adoption at the group level.
Beyond facilities, supply chain choices and digital modalities shape sustainability performance. Work on greener healthcare logistics highlights the leverage in supplier standards, circular approaches for devices, and real-time data to curb stockouts and waste, while digitalisation enables process visibility across purchasing, storage, and disposal [17,21]. Telemedicine is noted for its benefits in access and reduced travel, yet it raises governance challenges related to privacy, interoperability, and consistent power supply that are salient in Southern Africa [22,23]. South African studies report positive clinician attitudes toward environmental sustainability, but knowledge gaps remain in operational practices, such as theatre gases and water stewardship, underscoring the need for structured training and measurement routines within private groups [7,8,24]. Together, these streams portray sustainability not as a single programme but as a portfolio of mutually reinforcing practices that require organisational integration to scale.
2.2. Stakeholder Orientation
Stakeholder Theory clarifies why sustainability advances when private providers frame it as value for patients, staff, suppliers, communities, investors, and regulators rather than as a compliance afterthought. Studies show that patient expectations for safe and responsible care, employee participation in improvement work, and supplier collaboration for greener inputs underpin durable adoption in provider organisations [25,26]. In South Africa, concentrated ownership and purchasing power within large private groups can enable or constrain sustainability within hospital supply chains, making internal governance and external engagement decisive levers for implementation and accountability [5]. Reporting research indicates that disclosure and integrated thinking build legitimacy, yet the quality of information and line of sight from board to ward remain uneven, which limits learning across facilities [18]. These insights justify this study’s focus on leadership, engagement, and governance as core conditions for practice uptake in private hospitals where stakeholder demands intersect with competitive and regulatory pressures.
Stakeholder alignment also matters for cross-sector collaboration. Reviews of governance for public-private partnerships in health emphasise that structured agreements, transparent metrics, and shared routines are needed to move from ad hoc pilots to reliable system improvement, a finding that travels to private group collaborations with suppliers and community providers in South Africa [26,27]. These patterns inform the article’s analytical attention to integrated governance mechanisms and to routines that translate stakeholder expectations into everyday practice, which underpin the study’s model.
2.3. Capabilities for Sustainability
The Resource-Based View explains why sustainability sticks where organisations build capabilities that are valuable, rare, and hard to imitate, such as data-driven energy management, advanced waste analytics, green human resource practices, and innovation-friendly cultures. Evidence indicates that green HR and employee environmental citizenship support operational gains in hospitals, whereas leadership-anchored learning routines sustain improvement beyond project cycles [28,29]. Digital and analytics capabilities are pivotal. Studies link sensor-enabled maintenance, real-time dashboards, and decision tools to reductions in waste and energy use, thereby aligning environmental goals with performance routines that are cost- and quality-sensitive [30,31]. These capabilities, combined with process innovations in procurement and logistics, strengthen resilience and reduce losses across the care pathway [17,32]. In South African private healthcare, RBV directly addresses findings that highlight leadership commitment, staff engagement, and operational expertise as drivers of sustainable performance. The logic is straightforward. When group leadership invests in learning systems, digital infrastructure, and targeted training for theatre teams, estates, and procurement, sustainability becomes a source of operational reliability and reputational value rather than a peripheral cost. These insights are built into the model’s emphasis on leadership and innovation as enabling conditions and on resource optimisation as a performance domain.
2.4. Institutional and Systems Dynamics
Institutional pressures create both opportunity and ambiguity in South African private healthcare. Normative expectations from clinicians and professional bodies, investor and community scrutiny of environmental footprints, and regulatory frameworks for quality and disclosure shape adoption, yet guidance on how to operationalise sustainability in hospital routines remains uneven [18,33]. Work on performance assessment notes that health systems still lack mature tools for triple-bottom-line measurement in care settings, which constrains organisational learning and external accountability [11]. This is the backdrop for the study’s emphasis on pragmatic metrics that integrate clinical outcomes with environmental and cost indicators, enabling sustainability to be managed as any other core process.
Systems thinking explains why isolated projects underperform. Healthcare is a complex service system with tight couplings between clinical workflows, estates, procurement, and information systems. Reviews show that sustainability gains are larger where organisations identify leverage points, coordinate across subsystems, and use structured methods to evaluate trade-offs and stakeholder values in decision-making [34,35]. Supply chain studies reinforce the need for coordination with vendors and distributors to reduce waste and environmental impact across the value stream, especially in resource-constrained contexts [21,36]. These perspectives directly shape the Sustainability Integration and Performance Model proposed in this article. The model links four dynamics observed in the data and theorised in the literature. Leadership and engagement develop capabilities, integrated governance aligns stakeholders, resource optimisation advances operational excellence, and performance integration provides the feedback loops that embed sustainability as a system property rather than a standalone initiative.
3. Materials and Methods
This study was guided by an interpretivist paradigm that positions reality as socially constructed and accessible through the meanings individuals attribute to their experiences. Interpretivism is well-suited to inquiries that seek to understand how organisational actors make sense of complex and evolving phenomena. Sustainability work in private healthcare involves situated judgments, tacit knowledge, and locally negotiated practices, which makes interpretive inquiry appropriate for revealing the contextual logics that shape adoption and implementation. The study’s orientation aligns with qualitative traditions that privilege depth, nuance, and attention to insider perspectives [13].
A phenomenological design was employed to explore how private healthcare professionals understand and enact sustainability within their organisational settings. Phenomenology was selected because sustainability practices are embedded in daily routines, professional norms, and operational constraints. The design supports an examination of lived experience rather than surface descriptions. This approach enabled the study to capture how participants interpret sustainability demands, navigate competing priorities, and articulate the organisational conditions that support or hinder implementation. It also allowed for attention to the emotional, ethical, and practical dimensions of sustainability work that may not be evident through quantitative or survey-based methods. The emphasis on lived experience is supported in the literature on phenomenological healthcare research and interpretive inquiry [12].
Purposive sampling was used to identify information-rich participants with direct responsibility for sustainability practices in private healthcare. The sample included 17 professionals representing clinical, managerial, quality, training, and administrative domains within private hospital groups and primary care settings. Participants were selected based on their involvement in implementing, coordinating, or overseeing sustainability initiatives, which ensured that insights reflected practical engagement rather than abstract opinions. This approach prioritised depth over representativeness, consistent with qualitative sampling logic that seeks varied yet relevant perspectives. Sampling focused on Gauteng and KwaZulu-Natal, the two provinces with the highest concentration of private healthcare activity. The purposive strategy aligns with recommended approaches for qualitative health systems research [13,37].
Data were collected through semi-structured interviews conducted via Microsoft Teams. This mode of interviewing provided flexibility for participants working in demanding healthcare environments and enabled the inclusion of geographically dispersed professionals. Interviews lasted between 30 and 60 minutes and followed an interview guide that covered definitions of sustainability, existing practices, organisational enablers and barriers, performance expectations, regulatory considerations, and perceived future directions. The semi-structured format allowed the researcher to probe emergent issues while ensuring comparability across interviews. All interviews were audio recorded with participant consent and transcribed verbatim. Electronic communication prior to the interviews ensured informed consent and clarified the study’s purpose and expectations for participants.
Thematic analysis was used to analyse the data. The analysis followed an iterative, interpretive process informed by Braun and Clarke’s principles of thematic development, adapted to the study's interpretivist orientation. Transcripts were read repeatedly to build familiarity and generate initial codes grounded in the data. Coding focused on both semantic content and underlying patterns that captured organisational, operational, and experiential aspects of sustainability. ATLAS.ti software supported code organisation, retrieval, and comparison, which assisted in identifying relationships among codes and clustering them into broader thematic structures. Themes were refined through constant comparison and examined in relation to theoretical constructs from Stakeholder Theory, RBV, Institutional Theory, and Systems Theory. This analytic approach allowed empirical patterns to be placed in conversation with theoretical explanations while remaining grounded in participant accounts.
Trustworthiness was addressed through multiple strategies. Credibility was enhanced through prolonged engagement with the data, iterative coding, and analytic memoing that documented interpretive decisions. Reflexivity was maintained throughout the research process, supported by a reflexive journal in which the researcher critically examined assumptions, positionality, and potential biases. This reflexive stance was essential given the researcher’s professional experience within the private healthcare sector. Dependability was supported through an audit trail that documented sampling decisions, data collection procedures, coding processes, and theme development. Transferability was strengthened by a thick description of the context, enabling readers to assess its relevance to comparable settings. Confirmability was pursued by grounding all interpretations in participant statements and maintaining transparency about the analytic process. These procedures align with established qualitative criteria for trustworthiness, including those articulated by Guba (1981) and later refinements within qualitative health research.
The methodology thus provides a coherent interpretive framework for understanding sustainability practices in private healthcare. The combination of phenomenological inquiry, purposive sampling, semi-structured interviewing, and rigorous thematic analysis offers a robust foundation for examining how sustainability is enacted within complex healthcare organisations. This approach supports the study’s objective of generating conceptually rich and context-sensitive insights that inform the development of the Sustainability Integration and Performance Model.
4. Findings
The findings are organised into four meta-themes that directly address the research questions. RQ1 focused on identifying critical sustainability practices and success factors in private healthcare. RQ2 examined how these practices can be implemented systematically without compromising clinical or economic performance. Figure 1 summarises the thematic structure that informed subsequent analysis and the development of the SIPM.
4.1. Theme 1: Leadership and Engagement as Primary Drivers (RQ1)
Participants consistently highlighted leadership commitment as the foundational driver of sustainability adoption. Executive attention legitimised sustainability work and shaped how staff interpreted organisational priorities. Managers who encouraged experimentation enabled teams to trial and refine new practices. This produced a cascading effect in which senior direction aligned operational activities and created psychological readiness for change.
As one senior participant explained, “Sustainability must begin with leadership vision. When executives prioritise it, staff follow naturally” (P6). Another elaborated, “Innovation thrives where leaders support experimentation and reward engagement” (P12). These accounts illustrate that leadership, employee engagement, and local innovation reinforce one another, rather than acting as isolated drivers.
This theme clarifies the core success factors that address RQ1. Where sponsorship, consistent communication, and targeted support were present, facilities advanced in areas such as waste segregation, energy monitoring, and greener procurement. Conversely, facilities without these enabling conditions reported stalled or short-lived initiatives. Leadership, engagement, and innovation reinforce one another. Where these conditions were aligned, units demonstrated rapid improvement in waste reduction, energy awareness, procurement changes, and daily sustainability routines. Table 1 highlights that leadership visibility, team engagement, and an enabling climate for innovation emerged as interrelated drivers of sustainability adoption, as evidenced by consistent empirical indicators and participant narratives from the interview data.
4.2. Theme 2: Integrated Governance and Coordinated Implementation (RQ2)
Respondents described coordinated governance as essential for transforming sustainability from site-specific initiatives into organisation-wide practice. Structures such as sustainability committees, cross-functional task teams, standard procedures, and compliance dashboards allowed teams to navigate interdependencies between estates, clinical units, suppliers, and regulatory requirements.
One participant noted, “Sustainability efforts work when departments, suppliers, and regulators share data and goals” (P10). Another emphasised the institutionalisation of oversight, stating, “Formal governance committees that monitor compliance and ensure continuous improvement keep initiatives on track” (P3).
This theme identifies the organisational mechanisms that answer RQ2. Effective implementation required the alignment of procurement contracts, standardised reporting formats, collaborative problem-solving with waste vendors, and structured communication flows across facilities. The evidence shows that sustainability accelerated when coordination replaced fragmented decision-making. Governance mechanisms reduce fragmentation and create organisational coherence. Sustainability advanced when procurement, clinical units, facility management, and external vendors operated through unified procedures. Figure 2 illustrates the multi-level governance architecture within private healthcare, demonstrating how executive leadership cascades through sustainability and quality structures to operational and external actors, with shared reporting mechanisms enabling coordination, accountability, and system-wide learning.
4.3. Theme 3: Resource Optimisation and Environmental Stewardship as Operational Excellence (RQ1)
Participants described environmental sustainability and operational efficiency as mutually reinforcing. Improved waste segregation reduced disposal costs and contamination. Energy-aware behaviours and investments, such as solar systems, improved reliability in high-demand units such as theatres. Stewardship was therefore conceptualised not as an environmental add-on but as a contributor to operational performance.
A clinical leader highlighted this synergy. “Switching to solar and proper waste segregation cut costs and improved morale” (P9). Another noted the operational logic, stating, “Energy efficient devices reduce the footprint and running expenses” (P14).
Practices viewed as “critical” included clear visual cues for waste sorting, energy dashboards, reprocessing where clinically appropriate, and strengthened collaboration between clinical and estates teams. These results respond to RQ1 by illustrating the sustainability practices that most consistently delivered operational value in private healthcare settings. Environmental stewardship was treated as an operational competency rather than as an external environmental obligation. Teams that embedded sustainable behaviours into everyday workflow experienced greater efficiencies, fewer disruptions, and improved staff morale. Table 2 summarises high-leverage operational practices identified by participants, illustrating how waste, energy, and equipment optimisation translate into measurable cost, efficiency, and reliability benefits within private healthcare operations.
4.4. Theme 4: Performance Integration and Continuous Improvement (RQ2)
Participants emphasised that sustainability gained longevity when integrated into existing performance management routines. Organisations progressed when environmental indicators such as waste volumes and energy consumption were reviewed alongside patient safety, cost, and experience metrics.
A general practitioner summarised this interdependence. “Quality care and cost management are inseparable. Sustainability depends on balancing both” (P2). A quality manager added, “Tracking patient outcomes alongside environmental metrics helps us identify where we add most value” (P17).
The theme responds to RQ2 by demonstrating how integrated reporting, routine review meetings, internal benchmarking, and simple visualisation tools supported continuous improvement. Units that engaged with real-time or near-real-time data demonstrated greater adaptability and stronger ownership of sustainability outcomes.
Synthesis across the four themes produced the Sustainability Integration and Performance Model. The SIPM depicts sustainability as the cumulative effect of four interacting components. Leadership and engagement operate as enabling conditions. Governance integration provides structured pathways for implementation. Resource optimisation defines the domain of operational practice. Performance integration creates feedback loops that refine, stabilise, and scale improvements.
The model emerged inductively from participant accounts and cross-case convergence rather than from a prescriptive template. It represents how private healthcare organisations in this study moved from fragmented sustainability efforts to cohesive systems of practice grounded in everyday operational realities. Meaningful metrics anchored sustainability in real organisational routines. Units that used clear visualisations, simple run charts, and cross-hospital comparisons demonstrated higher engagement and continuous learning. Figure 3 illustrates the iterative feedback loop in which performance measurement informs learning, adjustment, and continuous improvement, thereby reinforcing the integration of sustainability over time.
The four meta-themes converged into the SIPM. The model represents sustainability as a system formed by interaction among enabling conditions, operational practices, governance structures, and performance loops. The SIPM visualises sustainability as a coherent system rather than a collection of isolated initiatives. It is grounded entirely in empirical patterns that emerged across the 17 participants’ accounts. Figure 4 presents the SIPM, illustrating how external environmental pressures, organisational enablers, and sustainability practices interact through systemic implementation and feedback mechanisms to shape performance outcomes.
5. Discussion
This study examines the integration of sustainability in South African private healthcare through four complementary lenses. Together, they explain why adoption depends on aligning stakeholder expectations, building distinctive organisational capabilities, navigating institutional ambiguity, and coordinating interdependent subsystems. The SIPM translate these theoretical insights into an empirically grounded architecture that links enabling conditions with implementation, operational practice, and performance feedback.
Stakeholder orientation and actionable legitimacy. Stakeholder theory clarifies why leadership visibility and genuine engagement proved decisive. Private hospital groups operate at the convergence of patient expectations, workforce values, supplier obligations, investor scrutiny, and regulatory oversight. Prior work shows that sustainability endures when organisations frame it as value creation for these constituencies rather than as compliance alone [25,26]. Our evidence extends this literature by showing that stakeholder alignment must be operationalised as accountable forums, shared targets, and cross-boundary routines that connect procurement, clinical units, and estates. In South Africa’s concentrated private market, internal governance choices of a few groups can shift practices at the system level, underscoring the importance of credible reporting and a line of sight from board to ward [5,18]. The findings, therefore, specify how legitimacy is produced in practice through visible sponsorship, collaborative problem-solving with vendors, and transparent performance reviews, rather than through disclosure alone.
RBV and the capability logic of sustainability. The resource-based view accounts for the observed shift from project activity to embedded routines. Studies link green human resource practices, environmental citizenship, and data-driven operations with durable performance in hospitals[28,29]. Our results show that capability bundles matter more than individual tools. Sensor-enabled energy management, waste analytics, and life-cycle costing had no effect on outcomes when used in isolation; however, when combined with learning systems, middle-management stewardship, and targeted upskilling for theatres, estates, and procurement, they had a significant impact. This extends prior work on digital and analytics capability by identifying the micro sequence through which organisations move from visibility of consumption to local problem solving and then to standardised practice across sites [17,30,31]. Sustainability becomes a source of operational reliability and reputational value when these bundles are built deliberately and reinforced by leadership attention to experimentation and recognition.
Institutional pressures and governance work operate in an environment of ambiguity. Institutional theory helps to interpret why governance depth emerged as a differentiator. South African guidance on how to operationalise sustainability in hospital routines remains uneven, with voluntary codes and fragmented mandates that produce varied interpretations across organisations [10,18]. Measurement systems for triple-bottom-line performance in clinical settings remain underdeveloped, which limits organisational learning and external accountability [11]. The study shows how organisations compensate for this ambiguity by institutionalising internal committees, standard operating procedures, and vendor clauses that embed expectations into everyday work. Normative pressures from professional communities and growing clinician interest in environmental responsibility add momentum, yet require structured training to convert attitudes into practice, a pattern echoed in regional studies of knowledge and capability gaps in theatres and water stewardship[7,8]. The contribution is to show governance as active work that substitutes for weak external coordination and that translates diffuse institutional signals into concrete organisational routines.
Systems thinking and the choreography of integration. Systems perspectives argue that meaningful improvement depends on coordination across tightly coupled subsystems in healthcare. Reviews document stronger sustainability outcomes when organisations identify leverage points, synchronise across care, estates, and supply, and evaluate trade-offs through structured decision methods [34,35]. Our analysis corroborates this and advances it by showing the choreography through which integration took hold in private hospitals. Performance integration was effective when environmental and cost indicators were reviewed at the same cadence as safety and throughput, and when cross-facility benchmarking facilitated peer learning. Supply chain research stresses collaboration with vendors and distributors in resource-constrained contexts, which aligns with our observation that waste and device flows improved when hospitals and suppliers used shared data and routine audits [21,36]. The systems lens, therefore, explains why isolated projects stalled and why performance feedback loops stabilised new practices.
What is contextually new about South African private healthcare? The South African setting introduces features that reshape theory. The private sector is relatively small by population coverage but large by resource intensity and is highly consolidated, with a limited number of groups controlling most private beds. This amplifies the systemic effects of internal governance and procurement choices, as changes in one group quickly affect suppliers and professional norms across the market [5,6]. Digital innovations such as telemedicine and electronic systems promise sustainability benefits, yet reliability challenges in connectivity and power supply create unique governance and capability demands for private providers that aim to scale these models responsibly in Southern Africa [22,23]. Clinician attitudes toward environmental stewardship are increasingly positive, which generates normative pressure that can be converted into practice once training and simple metrics are in place [7,8,38]. These contextual conditions make South Africa a revealing case of how stakeholder alignment, capability building, governance work, and systems coordination interact when formal policy direction is partial, and market power is concentrated.
Advancing sustainability integration through SIPM. Existing reviews offer lists of practices or call for holistic frameworks, yet many fall short of specifying the connective tissue linking leadership intent, governance, practice change, and measurement in hospital operations [19,39]. The Sustainability Integration and Performance Model advance these debates in three ways. First, it demonstrates that enabling conditions are not generic culture statements but are observable routines that legitimate experimentation and mobilise engagement across professional groups. Second, it shows that governance integration is the mechanism that turns diffuse stakeholder and institutional signals into shared procedures and supplier relationships that travel across facilities. Third, it locates the core of sustainability in resource-optimisation practices monitored through a single performance view, thereby anchoring environmental work within the same improvement cycles that private hospitals already use for safety and flow. In doing so, SIPM converts systems thinking into a pragmatic sequence of linked activities that can be audited, learned from, and scaled.
Overall, the theoretical integration developed here reframes sustainability in private healthcare as coordinated capability rather than programmatic activity. Stakeholder legitimacy, distinctive capabilities, institutional navigation, and systems coordination are mutually reinforcing rather than substitutable. The South African case makes these relations especially visible, and the SIPM shows how they can be enacted through specific organisational routines.
5.1. Implications
5.1.1. Theoretical Implications
This study advances conceptual understanding of sustainability integration in healthcare by demonstrating that sustainable performance emerges not from isolated initiatives but from the interaction of stakeholder alignment, organisational capabilities, institutional navigation, and systems coordination. The SIPM provides a structured explanation of how these dimensions function together within private healthcare organisations. It extends Stakeholder Theory by showing that legitimacy must be operationalised through governance routines that bind clinical, operational, and supplier relationships rather than through high-level messaging alone. The findings also deepen the Resource-Based View by demonstrating that sustainability capability is not a single competence but rather a bundle of capabilities, including analytical tools, staff engagement, and leadership, anchored in learning cultures. Institutional Theory is advanced by identifying governance work as a response to incomplete regulation in South Africa. Systems Theory is extended through empirical mapping of the feedback loops that support coherent implementation across subsystems. Together, these contributions offer a theoretical account of sustainability as the coordinated formation of capabilities in a resource-intensive service environment.
5.1.2. Managerial Implications
Leaders in private healthcare should approach sustainability as a strategic integration task rather than an environmental add-on. The findings show that leadership visibility must be coupled with accountability structures that coordinate estates, clinical units, procurement, and vendors. Senior managers should institutionalise cross-functional committees with clear decision-making authority and establish shared reporting systems that integrate environmental indicators into routine performance reviews. Investment in capability building is essential. Managers should prioritise targeted upskilling for staff who influence high consumption areas such as theatres, sterilisation, and estates. The evidence also shows that change accelerates when frontline staff can experiment and adapt practices within a clear strategic frame. Leaders should therefore cultivate an innovation climate that rewards local solutions and facilitates peer learning across facilities. Integrated dashboards and simple visual tools should be used to support unit-level reflection and continuous improvement. Overall, sustainability must be embedded into the same operational rhythms that govern safety, flow, and cost management.
5.1.3. Policy Implications
The South African regulatory environment for healthcare sustainability remains fragmented, which places disproportionate responsibility on private organisations to interpret and implement sustainability expectations. Policymakers should provide clearer operational guidance on environmental and social performance standards to reduce variability across facilities. Strengthening requirements for integrated reporting would support transparency and shared learning, particularly in a sector where a small number of groups influence national patterns of procurement and resource use. Regulators could also encourage the adoption of standardised environmental performance metrics that are compatible with clinical reporting systems. Incentives for coordinated waste management, energy efficiency, and greener procurement in private hospitals may accelerate system-wide improvement. Given the role of vendors and distributors, policy frameworks should promote collaborative procurement models that align supplier practices with national sustainability goals. Support for digital infrastructure and reliable connectivity would further enable private facilities to expand telemedicine and other technology-supported sustainability interventions. A more coherent regulatory architecture would help translate organisational efforts into sector-level progress.
6. Conclusions
This study examined how sustainability becomes embedded within the operational and strategic fabric of South Africa’s private healthcare sector. The analysis demonstrated that sustainable performance is not the product of isolated environmental interventions but arises from the interaction of leadership commitment, integrated governance, resource optimisation, and performance-driven learning. Taken together, these dynamics reveal sustainability as a coordinated organisational capability rather than a set of discrete projects. The proposed SIPM synthesise these insights by showing how enabling conditions, systemic implementation, operational practices, and feedback mechanisms shape sustainability outcomes in complex healthcare environments. The study offers a conceptual contribution by connecting four major theoretical traditions to an empirical understanding of healthcare sustainability. Stakeholder Theory illuminated how legitimacy is actively produced through structured engagement and transparent reporting. The Resource-Based View clarified why sustainability gains depend on capability bundles that combine analytical infrastructure, staff participation, and innovation-supporting leadership. Institutional Theory explains organisational responses to regulatory ambiguity in contexts in which private organisations bear a significant interpretive burden. Systems Theory revealed the coordinated nature of sustainability integration, highlighting the importance of cross-functional processes and feedback loops. The SIPM model extends current debates by offering an empirically grounded template that illustrates how these theoretical strands interact in practice. The study also highlights contextual features that shape sustainability in South African private healthcare. The concentration of private hospital ownership amplifies the system-wide influence of governance and procurement choices. Regulatory ambiguity necessitates that private groups develop their own internal guidance and oversight structures. Operational pressures, particularly in energy and waste-intensive facilities, create strong incentives for resource optimisation that align environmental stewardship with financial resilience. These conditions offer valuable lessons for healthcare systems operating under similar resource constraints. The research is not without limitations. As a qualitative study involving 17 participants across two provinces, the findings cannot be generalised to all private healthcare contexts. Self-reported experiences may also reflect organisational cultures or personal orientations that differ from other settings. Despite these boundaries, the depth of lived experience captured provides a robust foundation for analytical insight. Future research should test and refine the SIPM in other healthcare environments to assess its transferability and identify additional mechanisms that affect the integration of sustainability. There is value in conducting comparative studies between public and private healthcare to examine how different governance arrangements shape the capacity for sustainability. Quantitative work could also strengthen the evidence base by linking specific sustainability practices to measurable performance outcomes. Further inquiry into vendor relationships, digital infrastructure, and patient-facing sustainability expectations would deepen understanding of the broader system forces that accelerate or constrain progress. Overall, this research provides a theoretically informed and empirically grounded account of how private healthcare organisations can move from fragmented sustainability efforts to coherent, value-creating systems of practice. It underscores the strategic importance of coordinated leadership, governance, operational capability, and performance learning in advancing sustainable healthcare in South Africa.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used Conceptualization, N.N. and B.T.; methodology, N.N. and B.T.; software, N.N. and B.Y.; validation, N.N. and B.T.; formal analysis, N.N. and B.T.; investigation, N.N. and B.T.; resources, N.N. and B.T.; data curation, N.N. and B.T.; writing—original draft preparation, N.N. and B.T.; writing—review and editing, N.N. and B.T.; visualization, N.N. and B.T.; supervision, B.T.; project administration, B.T.; funding acquisition, B.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Department of Business Management Research Ethics Committee at the University of Johannesburg, Ethical clearance code: 25SOM/BM64 and 01 August 2025.
Data Availability Statement
Data will be made available upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Afjal, M.; Trivedi, J. Greening healthcare: exploring economic and ecological synergies in the pursuit of net-zero carbon futures. Sustain. Futur. 2024, 8. [Google Scholar] [CrossRef]
- Johnson, S.M.; Marconi, S.; Sanchez-Casalongue, M.; Francis, N.; Huo, B.; Alseidi, A.; Alimi, Y.R.; Pietrabissa, A.; Arezzo, A.; Frountzas, M.; et al. Sustainability in surgical practice: a collaborative call toward environmental sustainability in operating rooms. Surg. Endosc. 2024, 38, 4127–4137. [Google Scholar] [CrossRef]
- Keller, R.L.; Muir, K.; Roth, F.; Jattke, M.; Stucki, M. From bandages to buildings: Identifying the environmental hotspots of hospitals. J. Clean. Prod. 2021, 319. [Google Scholar] [CrossRef]
- van Schie, V. Governance related factors influencing the implementation of sustainability in hospitals: A systematic literature review. Health Policy. 2024, 146, 105115. [Google Scholar] [CrossRef] [PubMed]
- Schutte, C.; Niemann, W.; Kotzé, T. EXPLORING RELATIONSHIP POWER IN SUPPLY CHAIN SUSTAINABILITY PRACTICES: A CASE STUDY OF A SOUTH AFRICAN HOSPITAL GROUP. South Afr. J. Ind. Eng. 2022, 33, 154–176. [Google Scholar] [CrossRef]
- Carstens, P; Pearmain, D. The Regulatory Framework of the South African Health System. Med & L 2009, 28, 91. [Google Scholar]
- Frewen, L.; Grossman, E.; Basson, C. Mostly harmless? A survey of South African anaesthetists’ knowledge and attitudes regarding environmental sustainability in the operating theatre. South. Afr. J. Anaesth. Analg. 2022, 28, 35–40. [Google Scholar] [CrossRef]
- Lister, HE; Mostert, K; Botha, T; Field, E; Knock, D; Mubi, N; et al. Development and validation of a Knowledge, Attitudes and Practices (KAP) questionnaire for healthcare professionals on environmental sustainability in healthcare in Southern Africa. F1000Research 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Bradstreet, R.S.; Stoop, H. Finding Space for the B CorporationWithin the South African Legal Landscape; The International Handbook of Social Enterprise Law: Benefit Corporations and Other Purpose-Driven Companies, 2022; pp. 759–76. [Google Scholar]
- Chuma, K.; Sibiya, P. Digital Health Ecosystem Framework to Address Fragmentation of the Health System in South Africa. Afr. J. Nurs. Midwifery 2022, 24, 28 pages–28 pages. [Google Scholar] [CrossRef] [PubMed]
- Cavicchi, C. Sustainable Development and Performance Measurement in Healthcare Organizations. Int. J. Sustain. Policy Pr. 2016, 12. [Google Scholar] [CrossRef]
- Brinkmann, S; Kvale, S. Doing interviews. 2018. [Google Scholar]
- Creswell, JW; Poth, CN. Qualitative inquiry and research design: Choosing among five approaches; Sage publications, 2016. [Google Scholar]
- Guba, E.G. Criteria for assessing the trustworthiness of naturalistic inquiries. Educ. Commun. Technol. J. 1981, 29, 75–91. [Google Scholar] [CrossRef]
- Nowell, LS; Norris, JM; White, DE; Moules, NJ. Thematic analysis: Striving to meet the trustworthiness criteria. International journal of qualitative methods 2017, 16(1), 1609406917733847. [Google Scholar] [CrossRef]
- Engler, I.D.; Curley, A.J. Environmental Sustainability in Orthopaedic Surgery – Where We Are and Where We Are Going. Oper. Tech. Orthop. 2022, 32. [Google Scholar] [CrossRef]
- Man, L.C.; Lin, Y.; Pang, G.; Sanderson, J.; Duan, K. Digitalization to achieve greener healthcare supply chain. J. Clean. Prod. 2024, 463. [Google Scholar] [CrossRef]
- Corvino, A.; Doni, F.; Martini, S.B. Corporate Governance, Integrated Reporting and Environmental Disclosure: Evidence from the South African Context. Sustainability 2020, 12, 4820. [Google Scholar] [CrossRef]
- Asperti, F.; Cannavacciuolo, L.; Foglia, E.; Garagiola, E.; Gheduzzi, E.; Manetti, S. Seventy-two shades of environmental sustainability in healthcare: A holistic framework proposal. J. Clean. Prod. 2025, 493. [Google Scholar] [CrossRef]
- Mostepaniuk, A.; Akalin, T.; Parish, M.R. Practices Pursuing the Sustainability of A Healthcare Organization: A Systematic Review. Sustainability 2023, 15, 2353. [Google Scholar] [CrossRef]
- Jia, F.; Aboagye, S.; Shahzadi, G.; Chen, L. Sustainable practices in healthcare supply chains: a review of strategies, challenges, and impacts. Int. J. Logist. Res. Appl. 2025, 1–25. [Google Scholar] [CrossRef]
- Agbeyangi, A.O.; Lukose, J.M. Telemedicine Adoption and Prospects in Sub-Sahara Africa: A Systematic Review with a Focus on South Africa, Kenya, and Nigeria. Healthcare 2025, 13, 762. [Google Scholar] [CrossRef]
- Prinsen, L. Challenges to and Regulation of Telemedicine in South Africa. Afr. J. Int. Comp. Law 2023, 31, 204–227. [Google Scholar] [CrossRef]
- Lister, H.E.; Mostert, K.; Botha, T.; van der Linde, S.; van Wyk, E.; Rocher, S.-A.; Laing, R.; Wu, L.; Müller, S.; Tombe, A.D.; et al. South African Healthcare Professionals’ Knowledge, Attitudes, and Practices Regarding Environmental Sustainability in Healthcare: A Mixed-Methods Study. Int. J. Environ. Res. Public Heal. 2022, 19, 10121. [Google Scholar] [CrossRef]
- Parmar, BL; Freeman, RE; Harrison, JS; Wicks, AC; Purnell, L; De Colle, S. Stakeholder theory: The state of the art. Academy of Management Annals 2010, 4(1), 403–45. [Google Scholar] [CrossRef]
- Rodriguez, R.; Svensson, G.; Eriksson, D. Priorities Determining Future Directions of Sustainable Development in Business Models of the Healthcare Industry—Findings and Framework. Sustainability 2021, 13, 6507. [Google Scholar] [CrossRef]
- Dove, G; Craig, A; Harris-Roxas, B; Kelly-Hanku, A. Governance of Public-Private Partnerships for Primary Healthcare in Low-and Lower-Middle-Income Countries, 2000-2023: A Systematic Review. International Journal of Health Policy and Management 2025, 14. [Google Scholar] [CrossRef]
- Allam, NM; Mansour, MM. Do Green Human Resource Management Practices Improve Sustainable Performance? Empirical Evidence From Egyptian Private Hospitals. International Journal of Customer Relationship Marketing and Management 2024, 15(1). [Google Scholar] [CrossRef]
- Nasim, I.; Cheema, S.M.; Imtiaz, S.; Naeem, K. The role of green human resource management practices towards the health sector: with mediating role of organisational citizenship behaviour towards environment and psychological green climate. Int. J. Manag. Pr. 2024, 17, 170–199. [Google Scholar] [CrossRef]
- Chaudhuri, R.; Chatterjee, S.; Mariani, M.M.; Wamba, S.F. Assessing the influence of emerging technologies on organizational data driven culture and innovation capabilities: A sustainability performance perspective. Technol. Forecast. Soc. Chang. 2023, 200. [Google Scholar] [CrossRef]
- Alighardashi, M.; Mousavi, S.A.; Almasi, A.; Mohammadi, P. Development of a decision support tool for choosing the optimal medical waste management scenario using waste flow analysis and life cycle cost. Results Eng. 2024, 22. [Google Scholar] [CrossRef]
- Saihi, A.; Ben-Daya, M.; As'AD, R. Underpinning success factors of maintenance digital transformation: A hybrid reactive Delphi approach. Int. J. Prod. Econ. 2022, 255. [Google Scholar] [CrossRef]
- Irlam, J.H.; Scheerens, C.; Mash, B. Planetary health and environmental sustainability in African health professions education. Afr. J. Prim. Heal. Care Fam. Med. 2023, 15, e1–e3. [Google Scholar] [CrossRef]
- A SYSTEMS THINKING PERSPECTIVE FOR SUSTAINABLE HEALTHCARE. In Proceedings of the 2024 International Annual Conference and 45th Annual Meeting: Engineering Management Riding the Waves of Smart Systems; ASEM 2024, Katina, PF, Miller, T, Flanigan, D, Omolo, B, Eds.; 2024. [Google Scholar]
- Khosravi, M.; Izadi, R.; Shojaei, P.; Delavari, S. Strategies to promote patient-centeredness within the healthcare industry: A grey-based multicriteria decision making methods. J. Evaluation Clin. Pr. 2024, 30, 1585–1593. [Google Scholar] [CrossRef]
- Nsikan, J.; Affiah, E.A.; Briggs, I.; Koko, N. Sustainable supplier selection factors and supply chain performance in the Nigerian healthcare industry. J. Transp. Supply Chain Manag. 2022, 16. [Google Scholar] [CrossRef]
- Suri, H. Purposeful Sampling in Qualitative Research Synthesis. Qual. Res. J. 2011, 11, 63–75. [Google Scholar] [CrossRef]
- Lister, H.E.; Mostert, K.; Ramkilawon, G.; Oelschig, C.; Ntiyane, O.; Richardt, E.; Rocha, D.P.D.S.; Sheerin, S.; Phaahla, T.; Ashipala, D.; et al. Namibian Healthcare Professionals’ Knowledge, Attitudes and Practices Regarding Environmental Sustainability in Healthcare. Int. J. Environ. Res. Public Heal. 2025, 22, 751. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Pronovost, P.; Al-Kindi, S. Implementing a Sustainability Framework in Healthcare: A Three-Lens Framework. Healthcare 2023, 11, 1867. [Google Scholar] [CrossRef]
Figure 1.
Overview of the four meta-themes.
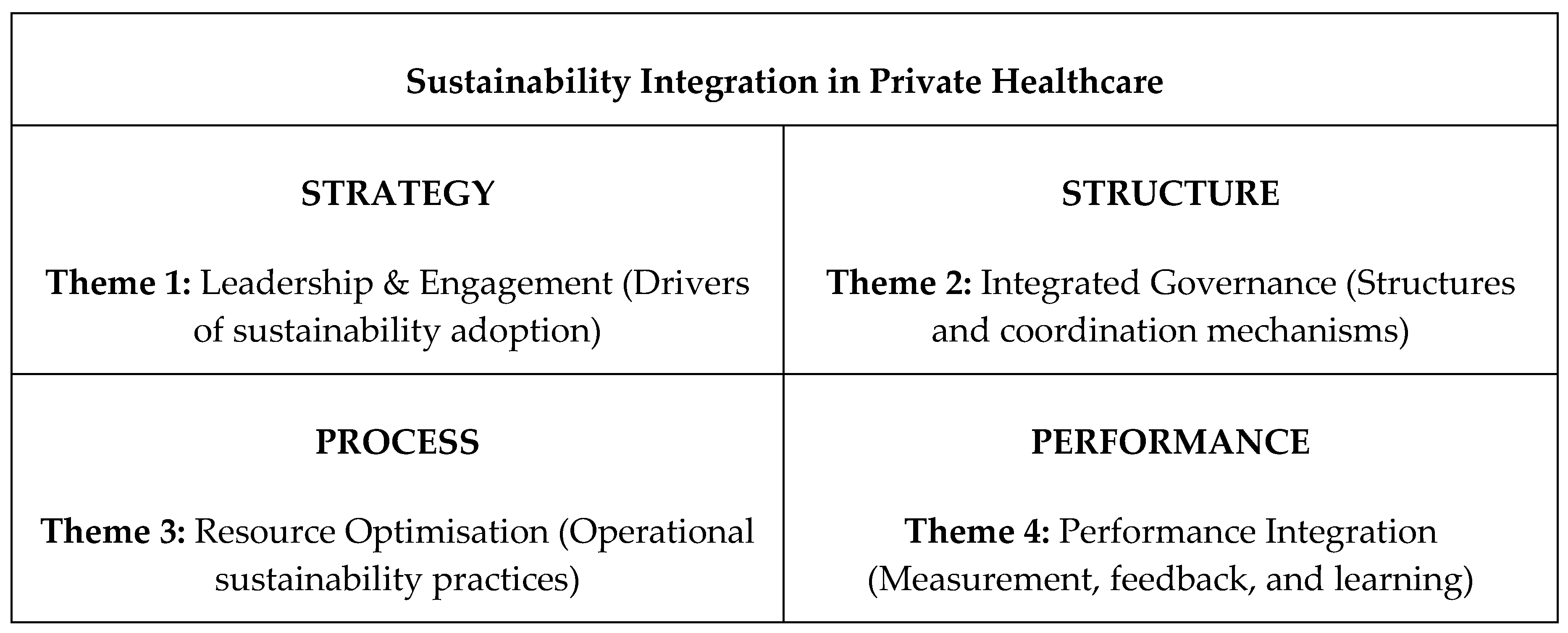
Figure 2.
Governance Links Across the Private Healthcare System.
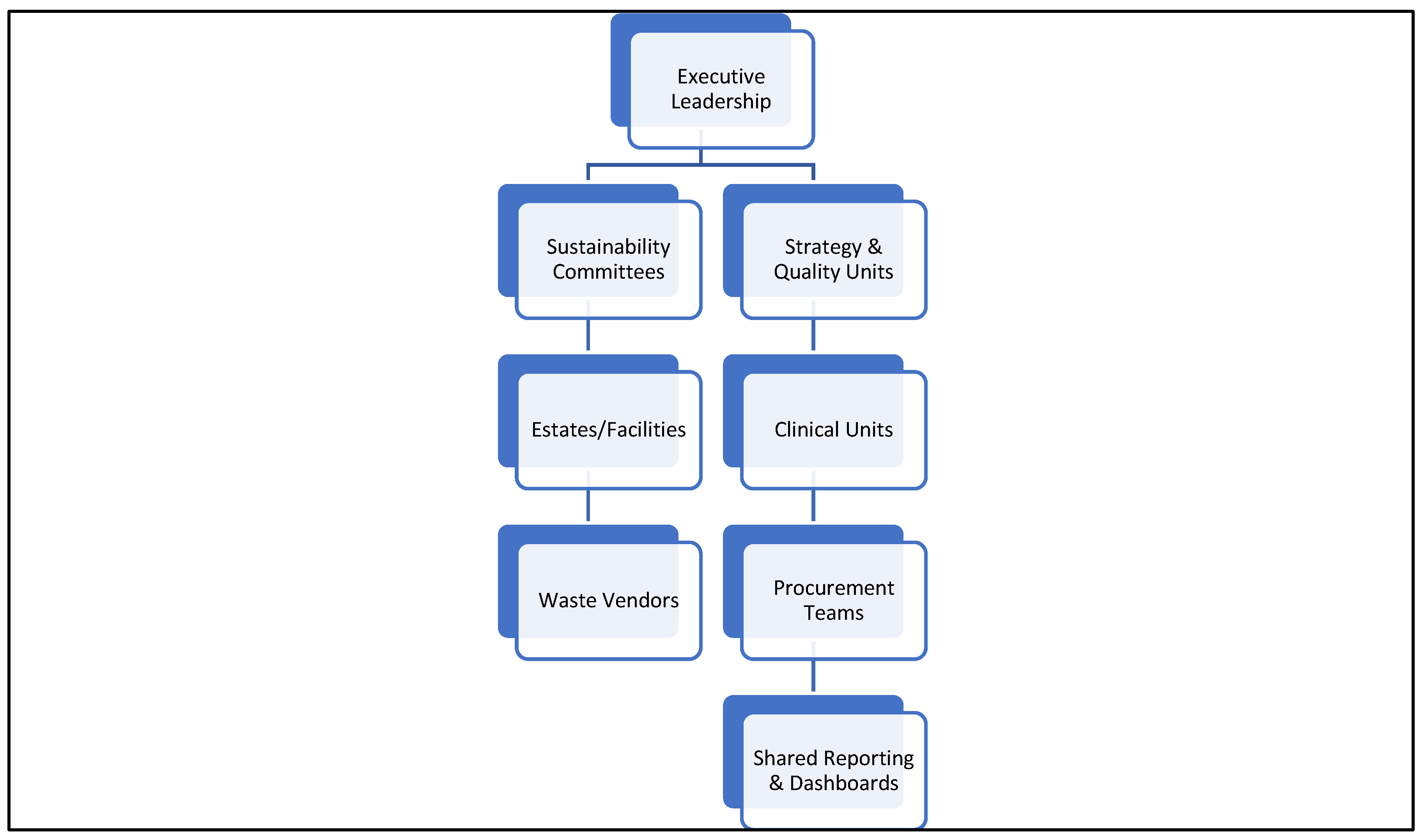
Figure 3.
Feedback loop of integrated performance.
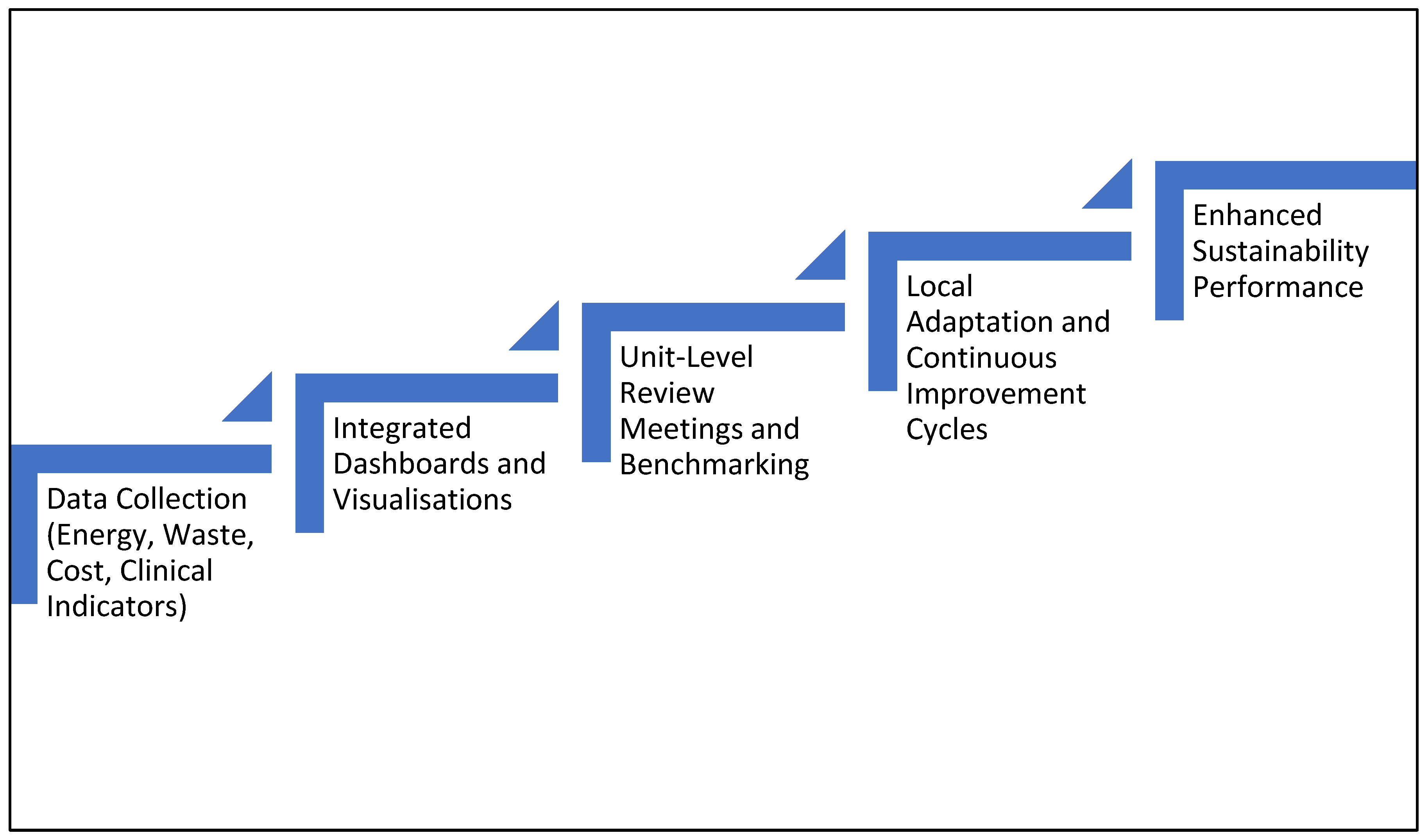
Figure 4.
Sustainability Integration and Performance Model (SIPM).
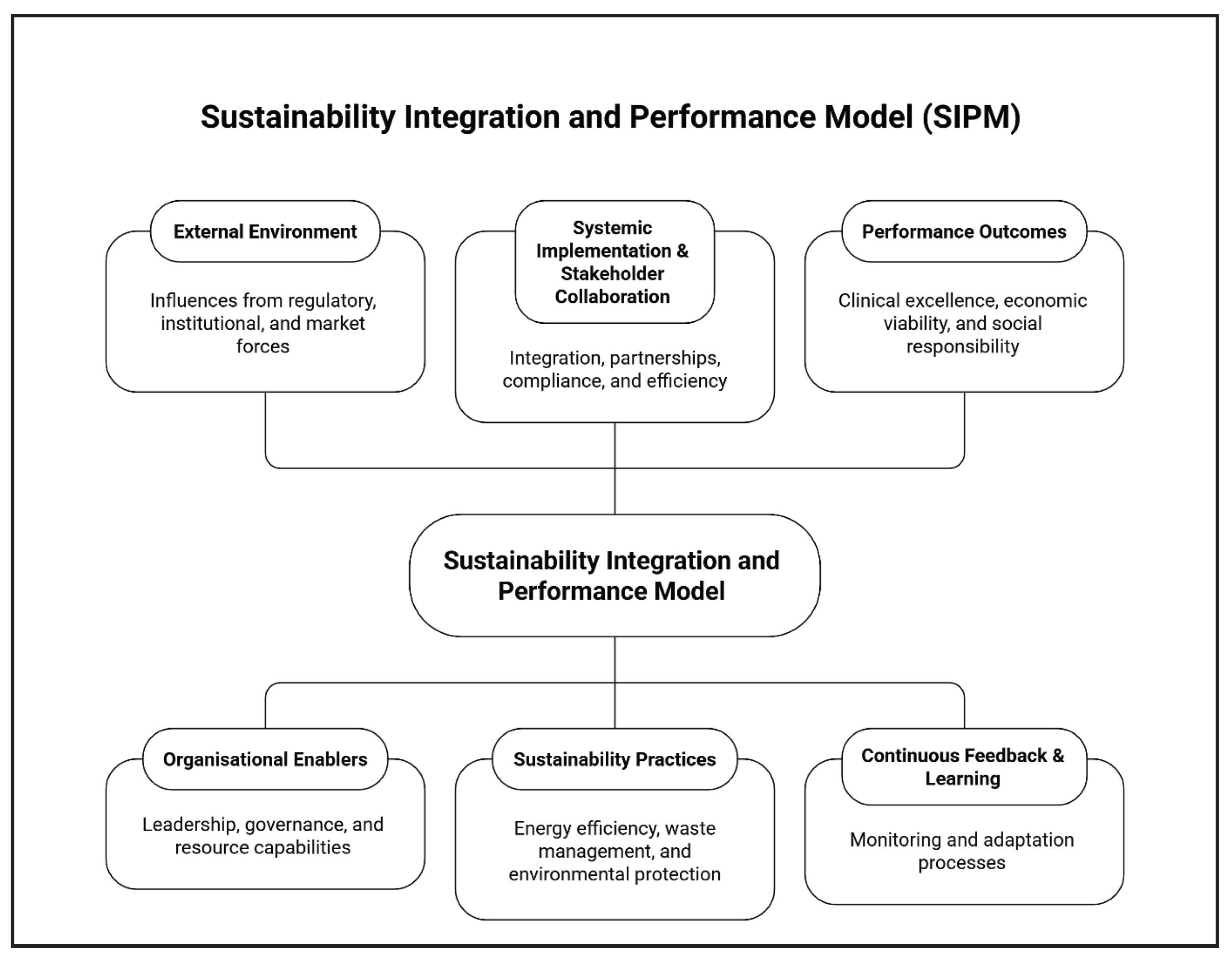

Table 1.
Theme 1 Core drivers identified by participants.
| Driver Identified | Empirical Indicators from Interviews | Example Participant Voice |
|---|---|---|
| Leadership visibility | Formal directives, strategy alignment, and sustainability messaging | “Leadership vision sets the tone” (P6) |
| Engagement of teams | Staff willingness, empowerment, and initiative-taking | “When leaders back us, we try new things” (P12) |
| Innovation climate | Permission to pilot, adapt, and refine ideas | “We test and improve as we go” (P3) |
Table 2.
High-Leverage Operational Practices.
| Practice Area | Examples of Actions Mentioned by Participants | Operational Benefits |
|---|---|---|
| Waste optimisation | Segregation at source, vendor coordination | Lower costs, fewer contamination incidents |
| Energy optimisation | Solar introduction, switching off idle loads | Cost savings, greater reliability |
| Equipment efficiency | Reprocessing where appropriate, device management | Reduced waste generation, smoother workflow |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



