Submitted:
30 January 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Background: Lipedema is a chronic, progressive adipose tissue disorder that affects almost exclusively women and is characterized by disproportionate limb fat accumulation, pain, edema, and resistance to conventional weight-loss strategies. Although traditionally approached as a disorder of adipose tissue expansion, emerging evidence suggests that functional impairment in advanced lipedema cannot be fully explained by fat pathology alone. Methods: This hypothesis-driven review proposes a novel conceptual framework in which advanced lipedema is accompanied by a parallel failure of skeletal muscle function, characterized by dynapenia despite preserved or increased limb volume. Results: Our findings indicate a phenotype characterized by reduced muscle strength and quality in advanced lipedema, which we term lipedemata dynapenic myosteatosis. We synthesize clinical, imaging, and mechanistic data indicating that inflammatory myosteatosis, mitochondrial dysfunction, and impaired lipid oxidation contribute to reduced muscle quality and exercise intolerance in late-stage lipedema, particularly Stage 3, while emphasizing that functional decline should be proactively investigated from Stage 2 onward. Within this context, conventional resistance exercise, while physiologically required to prevent dynapenia, may be poorly tolerated due to inflammation, edema, and pain, creating a therapeutic deadlock. To address this paradox, we present a hypothesis-generating dual-target framework that integrates metabolic modulation aimed at restoring mitochondrial fatty-acid oxidation with anabolic signaling directed toward contractile tissue, drawing mechanistic analogies from established catabolic states. Conclusions: Importantly, this model is presented as a conceptual and translational framework rather than a clinical recommendation. By shifting the focus from adipose volume to muscle quality and function, this work reframes advanced lipedema as a disorder of coupled adipose–muscle bioenergetic failure. Future clinical studies are required to validate this framework, with outcomes centered on strength, mobility, pain, and functional independence rather than weight loss alone.
Keywords:
lipedema
; dynapenia
; myosteatosis
; skeletal muscle dysfunction
; mitochondrial diseases
; tirzepatide
; adipose tissue
; skeletal muscle
1. Introduction
Lipedema is a chronic, progressive, and frequently underdiagnosed disorder of adipose tissue that affects almost exclusively women, with prevalence estimates ranging from 6% to 11% of the female population [1,2,3]. First described Allen and Hines in 1940 at the Mayo Clinic, the condition is characterized by a symmetrical, bilateral accumulation of subcutaneous adipose tissue (SAT) predominantly affecting the lower extremities and frequently the arms, while typically sparing the hands and feet [1,2]. Unlike common obesity, lipedema is characterized by orthostatic edema, capillary fragility with easy bruising, and, most notably, spontaneous pain and tenderness of the affected tissues [4,5].
Despite its distinctive clinical phenotype, lipedema remains poorly recognized in general medical practice and is frequently misclassified as lymphoedema, gynoid obesity, or simple physical deconditioning [4]. Lipedema has long been recognized as one of several rare adipose disorders that masquerade as simple obesity, a misconception that contributes to diagnostic delay, inappropriate weight-centered counseling, and persistent patient stigmatization [4]. This diagnostic ambiguity imposes a substantial psychosocial burden. Observational studies and patient-reported surveys describe an average diagnostic delay approaching two decades, during which many women experience persistent invalidation of symptoms, often described by patients as ‘medical gaslighting’ [6]. During this period, individuals are frequently advised that their disproportionate limb volume reflects lifestyle choices alone, leading to repeated cycles of aggressive caloric restriction and excessive physical activity with limited clinical benefit [7,8]. This prolonged mismatch between effort and outcome is associated with significant psychological distress, including elevated rates of depression, anxiety, and disordered eating behaviors [9,10,11].
A defining clinical feature of lipedema is its apparent resistance to interventions based solely on negative energy balance. While bariatric surgery and intensive lifestyle modification reliably reduce visceral adiposity and systemic inflammatory markers, lipedematous tissue in the extremities often remains largely unaffected [12,13]. Emerging clinical observations further suggest that even first-generation glucagon-like peptide-1 (GLP-1) receptor agonists, such as semaglutide, despite their effectiveness in treating general obesity, frequently fail to meaningfully improve the fibrotic architecture and pain-related symptoms characteristic of lipedema [14]. Collectively, these findings suggest that lipedema may involve tissue-specific mechanisms of metabolic inflexibility that extend beyond central energy regulation pathways targeted by conventional anti-obesity pharmacotherapies.
Importantly, this apparent therapeutic resistance may not be confined to adipose tissue alone. Increasing evidence points toward concurrent impairment within the skeletal muscle compartment. Whereas classical obesity is often accompanied by a compensatory increase in muscle mass to support greater mechanical load, individuals with lipedema frequently exhibit a disproportionate reduction in functional muscle strength relative to limb volume a phenomenon consistent with dynapenia [15,16]. We hypothesize that this functional decline may be driven by inflammatory myosteatosis, characterized by inter- and intramuscular lipid infiltration, mitochondrial dysfunction, and chronic low-grade inflammation [17,18].
In this article, we propose a novel pathophysiological framework termed “Lipedematous Dynapenic Myosteatosis.” Within this model, progression from early-stage lipedema to functional limitation and reduced mobility is conceptualized as a self-reinforcing cycle involving pain, inflammation, and skeletal muscle bioenergetic failure. This cycle may render conventional behavioral recommendations such as caloric restriction and increased physical activity, progressively less feasible at a physiological level, rather than reflecting lack of adherence or motivation [19]. On this basis, we explore a hypothesis-generating mechanistic rationale in which metabolic interventions capable of improving mitochondrial substrate utilization, such as dual glucose-dependent insulinotropic polypeptide (GIP)/GLP-1 receptor agonism (e.g., tirzepatide) [20], may theoretically complement strategies aimed at restoring muscle contractile capacity in advanced dynapenia. The discussion of anabolic androgenic steroids (AAS) is therefore presented strictly within a, pathophysiological and rehabilitative framework, as a conceptual extrapolation from established models of catabolic and muscle-wasting conditions, rather than as a clinical recommendation.
2. The Clinical Paradox: Lipedematous Dynapenia
2.1. The Illusion of Mass: Pseudo-Hypertrophy versus Functional Reality
In classical obesity, the relationship between body mass and muscle strength is often approximately linear, as increased gravitational load requires compensatory hypertrophy of antigravity muscles to preserve locomotion. This adaptation is largely physiological and functionally meaningful. Lipedema, however, represents a marked deviation from this allometric pattern. Clinical examination of patients in Stages 2 and 3 frequently reveals lower limbs with substantial volume which, under superficial assessment or bioelectrical impedance analysis (BIA), may be interpreted as reflecting increased fat-free mass (FFM).
This apparent increase in “mass,” however, may be misleading. Characterizations by Al-Ghadban et al. (2025) demonstrate that although skeletal muscle mass (SMM) appears to increase across lipedema stages, this increase does not translate into proportional functional capacity [5]. In contrast, van Esch-Smeenge et al. (2017) reported that women with lipedema exhibit markedly reduced quadriceps strength (~260–270 N) compared with BMI-matched obese controls (~400 N) [15]. This dissociation defines lipedematous dynapenia: impaired muscle strength despite preserved or increased tissue volume.
We hypothesize that a substantial portion of this limb volume represents a form of pseudo-hypertrophy, composed not of functional myofibrillar expansion but of a disorganized matrix including intracellular edema, extracellular fibrosis, and ectopic lipid deposition. Support for this concept comes from sodium-MRI studies by Crescenzi et al., which revealed elevated sodium content in the skin and skeletal muscle of patients with lipedema, consistent with chronic low-grade inflammatory edema that expands tissue volume while compromising contractile efficiency [16]. In parallel, Shiose et al. demonstrated that muscle inflammation and injury significantly distort bioimpedance measurements, leading to systematic overestimation of muscle mass due to the conductive properties of interstitial fluid [21].
2.2. The Failure of Standard Metrics: Why BMI Is Blind
Failure to recognize this paradox is partly attributable to continued reliance on body mass index (BMI). As emphasized by Borga et al. (2018), BMI is inherently insensitive to body-composition quality and cannot differentiate functional myofibrillar tissue from pathological infiltration or edema [22]. In the context of lipedema, Taylor et al. (2022) employed chemical-shift–encoded MRI (Dixon technique) to demonstrate that muscle quality, assessed by fat fraction and radiodensity, is significantly compromised despite preserved limb size [23].
Accordingly, apparent preservation of limb circumference may mask a progressive degradation of muscle quality. Limbs often described clinically as “strong” are, in fact, disproportionately heavy, metabolically inefficient, and burdened by non-contractile tissue, representing a critical but underrecognized contributor to disability in advanced lipedema.
2.3. Inflammatory Myosteatosis as a Metabolic Bottleneck
A central mechanism underlying this functional impairment is myosteatosis, defined as pathological accumulation of lipid within and between skeletal muscle fibers. In metabolic diseases such as obesity, insulin resistance, and type 2 diabetes, intramuscular lipid content correlates more strongly with functional limitation and metabolic dysfunction than muscle mass alone [18]. Experimental work by Gumucio et al. demonstrates that impaired mitochondrial lipid oxidation precedes intramyocellular fat accumulation following muscle injury or atrophy [17].
By analogy, we hypothesize that in lipedema, skeletal muscle mitochondria are exposed to excess free fatty acids but exhibit reduced metabolic flexibility and oxidative capacity. This mismatch may promote intramyocellular lipid accumulation, lipotoxic stress, and impaired contractile performance [18]. Within this framework, myosteatosis is positioned not as a passive consequence of inactivity, but as an active metabolic bottleneck that amplifies functional decline.
2.4. The Vicious Cycle of Pain, Inactivity, and Functional Decline
These metabolic and structural abnormalities have direct clinical and psychosocial consequences. Intramuscular lipid accumulation and chronic inflammatory signaling may sensitize nociceptors, contributing to the deep, aching pain reported by patients with lipedema. Observational data from Erbacher and Bertsch (2020) suggest that pain in lipedema extends beyond purely mechanical factors and is influenced by persistent inflammation and chronic disease-related distress [24]. Population-level data from Czech women with lipedema further demonstrate substantial impairments in physical and mental quality of life, underscoring the pervasive functional and psychosocial burden of the disease [25].
Pain-driven avoidance of movement promotes disuse atrophy and further mitochondrial deconditioning. Reduced oxidative capacity exacerbates myosteatosis, reinforcing a self-perpetuating cycle of pain, inactivity, and functional deterioration—a trajectory described by Aitzetmüller-Klietz et al. (2023) as a progressive loop of decline in advanced disease stages [19,26]. Within this framework, immobility emerges not as a behavioral failure, but as a predictable physiological consequence of intersecting inflammatory, metabolic, and neuromuscular dysfunction.
Taken together, the mechanisms described above indicate that functional impairment in advanced lipedema arises from a self-reinforcing interaction between metabolic inflexibility, inflammation, and declining muscle quality, limiting the effectiveness of conventional lifestyle-based interventions.The following section introduces a hypothesis-driven conceptual framework exploring how modulation of the metabolic milieu may alter the biological context in which functional recovery becomes feasible, without implying therapeutic efficacy.
3. The Therapeutic Deadlock and a Translational, Hypothesis-Driven Pharmacological Bypass
Building on the mechanisms described above, this section introduces a hypothesis-driven conceptual framework integrating metabolic inflexibility and skeletal muscle dysfunction in advanced lipedema. The aim is not to propose therapeutic interventions, but to clarify how tissue environment conditions the feasibility of exercise adaptation and functional recovery, without implying clinical efficacy.
3.1. The Exercise Paradox: Why Mechanical Loading May Fail
Resistance exercise is conventionally regarded as the cornerstone intervention for dynapenia and sarcopenia in healthy and metabolically stable populations. However, in lipedema, the physiological context in which mechanical loading occurs appears fundamentally altered. Emerging consensus statements from the Italian Society of Motor and Sports Sciences (SISMES) and the Italian Society of Phlebology (SIF) caution that high-intensity exercise may exacerbate inflammation, increase capillary filtration, and worsen edema in patients with lipedema, particularly in Stage 3 and severe func-tional phenotypes [27]. These effects are attributed to lactate accumulation, tissue hy-poxia, and microvascular fragility within an already inflamed adipose–muscle inter-face.
This clinical scenario gives rise to what we conceptualize as a therapeutic deadlock (Figure 1). On one hand, reversal of established dynapenia requires a sufficient ana-bolic stimulus. On the other, the mechanical stress typically required to induce such adaptation may trigger disproportionate inflammatory and edematous responses. As reported by Aitzetmüller-Klietz et al. [19] and Annunziata et al. [27], high-intensity loading in lipedema frequently aggravates pain and swelling, leading to exercise intol-erance and subsequent avoidance. The patient thus becomes biologically constrained: metabolically limited by impaired lipid oxidation and mechanically limited by in-flammatory hypersensitivity, rendering conventional “train harder” strategies physi-ologically impractical rather than behaviorally deficient.
3.2. The Dual-Target Hypothesis: Breaking the Pathophysiological Cycle
To address the therapeutic deadlock observed in advanced lipedema, we propose a dual-target, hypothesis-driven framework that considers metabolic inflexibility and contractile dysfunction as interdependent, but hierarchically organized, components of functional decline. Rather than implying a direct pharmacological shortcut or linear intervention–response sequence, this framework seeks to interrupt the self-reinforcing biological loops that sustain inflammatory myosteatosis, exercise intolerance, and progressive loss of mobility in lipedema.
Within this model, metabolic dysregulation is positioned as the primary and enabling constraint, shaping the tissue environment in which mechanical loading and muscle adaptation occur. Contractile dysfunction is therefore conceptualized not as an isolated muscular defect, but as a downstream consequence of chronic inflammation, ectopic lipid accumulation, and impaired mitochondrial substrate handling. This distinction is critical, as it implies that restoration of muscle function cannot be achieved through mechanical or anabolic stimuli alone unless the underlying metabolic milieu is first reconditioned.
3.2.1. Metabolic Modulation: Tirzepatide and Mitochondrial Flexibility
Restoration of mitochondrial lipid handling and oxidative flexibility represents a biological prerequisite for mitigating inflammatory myosteatosis and improving muscle quality in lipedema. As discussed in detail in our previous narrative review on tirzepatide in lipedema, mitochondrial dysfunction, impaired fatty acid oxidation, chronic inflammation, and extracellular matrix fibrosis constitute interrelated pathogenic nodes that sustain metabolic rigidity in lipedematous adipose depots and adjacent tissues [6,21,24,27,28,29,30].
Dual GIP/GLP-1 receptor agonism offers mechanistic advantages over GLP-1–only therapies by modulating lipid metabolism, immune signaling, and stromal remodeling beyond appetite suppression alone [22,23,24]. Experimental and translational evidence indicates that co-activation of GIP and GLP-1 receptors enhances mitochondrial efficiency, improves substrate utilization, and promotes adipose tissue remodeling, including increased thermogenic signaling and beige adipocyte differentiation [24,29,30]. Importantly, these effects are consistent with a global restoration of metabolic flexibility, rather than activation or inhibition of any single molecular pathway.
These mechanisms are particularly relevant to lipedema, where adipose tissue fibrosis, microvascular dysfunction, and mitochondrial inflexibility contribute to resistance to lipid mobilization and perpetuate ectopic lipid deposition in skeletal muscle [6,27,28]. In this context, tirzepatide may indirectly recondition the metabolic and inflammatory microenvironment surrounding myocytes by attenuating inflammatory signaling, reducing profibrotic pathways, and improving insulin sensitivity, thereby lowering lipid spillover into muscle fibers [21,24,29]. Tirzepatide is therefore conceptualized here as a metabolic enabler, restoring the oxidative capacity required to safely process mobilized substrates rather than acting directly on contractile tissue.
Lipolysis–Oxidation Mismatch
Isolated stimulation of lipolysis in the absence of adequate mitochondrial oxidative capacity is insufficient and may be metabolically maladaptive. Fatty acids mobilized without parallel enhancement of mitochondrial oxidation are prone to re-esterification or conversion into lipotoxic intermediates, exacerbating oxidative stress, mitochondrial dysfunction, and intramyocellular lipid accumulation [6,24,29]. This lipolysis–oxidation mismatch has been identified as a key contributor to myosteatosis and impaired muscle performance in chronic metabolic and inflammatory states.
Within this framework, signaling pathways that promote lipid mobilization or nitrogen retention may increase substrate availability but do not, in isolation, resolve ectopic lipid overload. Without concurrent restoration of mitochondrial flexibility, such mechanisms risk amplifying lipid overflow rather than alleviating it [24,27,28]. Consequently, mitochondrial reactivation through metabolic modulation is foundational, providing the oxidative capacity necessary to dissipate mobilized substrates and prevent further ectopic lipid deposition. This hierarchy underscores why metabolic modulation must precede, or at least accompany, any strategy aimed at restoring muscle contractile function.
Once the metabolic and inflammatory milieu is partially reconditioned, the biological context in which mechanical loading occurs is fundamentally altered. In the absence of such reconditioning, higher-intensity resistance exercise applied to a rigid, inflamed, and metabolically inflexible tissue environment is more likely to propagate oxidative stress, pain, and edema rather than induce adaptive hypertrophy.
This helps explain why conventional training strategies may fail or even exacerbate symptoms in advanced lipedema, not because mechanical loading is intrinsically ineffective, but because it is introduced in a biologically unfavorable phase of the disease. Within this framework, restoration of metabolic flexibility is expected to reduce inflammatory amplification during exercise, thereby lowering the physiological cost of movement and permitting re-engagement with mechanical stimuli under more tolerable conditions.
Only in this reconditioned context does it become conceptually appropriate to discuss functional support mechanisms aimed at restoring strength and contractile capacity, which are addressed below as a secondary and dependent component of the proposed framework.
3.2.2. Anabolic Signaling as a Functional Rescue Analogy
In this reconditioned metabolic context, where inflammatory burden and mitochondrial inflexibility are at least partially attenuated, limitations in skeletal muscle function become more clearly interpretable as a downstream consequence of prior chronic catabolic stress rather than as an immutable structural defect. In advanced stages of lipedema (Stage 3), skeletal muscle may exhibit features consistent with localized, sustained catabolism, including reduced strength, impaired mobility, and diminished tolerance to mechanical loading. Earlier stages (Stage 2 and transitional phenotypes) should therefore be regarded as a critical window for proactive functional assessment, as overt disability is most consistently recognized only once Stage 3 is established.
Within this framework, it is informative to draw a mechanistic analogy with established catabolic conditions—such as HIV-associated wasting, severe burns, trauma, and chronic inflammatory disease—in which augmentation of anabolic signaling has historically been explored as a means of preserving or restoring muscle function. Importantly, this analogy is used here to contextualize functional recovery, not to propose therapeutic transfer across disease states.
The discussion of anabolic androgenic steroids (AAS) in this manuscript is strictly confined to a functional and rehabilitative framework. The objective is the preservation or recovery of contractile capacity and mobility under conditions of documented catabolic stress, not aesthetic modification, performance enhancement, or therapeutic recommendation. Accordingly, AAS are referenced as a pharmacological class, serving as an illustrative model for how anabolic signaling may influence muscle function when biological prerequisites for adaptation are met.
Oxandrolone is cited as a representative example within this class, given its extensive documentation in the literature as an adjunct therapy in conditions characterized by severe catabolic imbalance, sarcopenia, and dynapenia. In HIV-associated wasting, oxandrolone has been shown to improve lean body mass, nitrogen balance, and functional parameters, including in women, under controlled clinical conditions [31,32]. When combined with structured exercise interventions, anabolic strategies in HIV populations further demonstrated improvements in muscle performance and functional outcomes, reinforcing the concept that anabolic signaling requires adequate mechanical and nutritional support to translate into benefit [33].
In pediatric populations exposed to profound catabolic stress, including malnourished children with HIV and severe burn injury, oxandrolone has likewise been investigated as a rehabilitative adjunct. Clinical studies and systematic reviews report improvements in lean mass accretion, growth parameters, and functional recovery when oxandrolone is used within carefully monitored protocols [34,35]. These data underscore that the primary rationale for oxandrolone use in such contexts is functional recovery, rather than cosmetic or performance-related outcomes.
Importantly, contemporary systematic reviews evaluating oxandrolone across catabolic and chronic disease states conclude that its effects on muscle mass and function are context-dependent, modest in magnitude, and contingent upon appropriate nutritional intake, metabolic support, and clinical monitoring [36]. These analyses further emphasize that anabolic signaling alone does not override energetic constraints and should not be interpreted as a standalone solution for muscle dysfunction.
From a mechanistic perspective, anabolic signaling may favor nutrient partitioning toward skeletal muscle by enhancing protein synthesis efficiency and limiting excessive proteolysis. However, effective muscle protein synthesis requires sufficient caloric intake, adequate protein availability, and an intact oxidative environment. Severe caloric restriction or persistent metabolic inflexibility would be expected to blunt anabolic responsiveness regardless of signaling intensity.
Within the proposed hypothesis-driven framework, metabolic modulation remains foundational, establishing the energetic and oxidative conditions necessary for anabolic signaling to translate into functional benefit. In this sequence, anabolic signaling—illustrated here by oxandrolone and related agents—should be interpreted as secondary and dependent, potentially facilitating recovery of strength and tolerance to mechanical loading once the metabolic–inflammatory milieu has been favorably modified. This hierarchy reinforces that restoration of muscle function in complex metabolic diseases such as lipedema cannot be achieved through isolated anabolic stimulation, but rather through coordinated modulation of metabolic environment, nutritional adequacy, and mechanical exposure.
In summary, this hypothesis-driven framework positions dynapenia in advanced lipedema as a context-dependent outcome of metabolic and inflammatory constraints rather than an isolated muscular defect. The model is non-prescriptive and does not infer clinical efficacy, but serves to generate mechanistically informed hypotheses to be tested in future translational and clinical studies.
4. Discussion: Translational Implications and Safety Considerations
4.1. Identifying the Functional Inflection Point
The pharmacological framework proposed in this manuscript is not intended for early-stage lipedema, in which conservative strategies such as compression therapy, lymphatic management, and low-impact physical activity remain appropriate. Rather, this hypothesis is specifically oriented toward a functional inflection point, at which progressive tissue volume begins to compromise biomechanics, muscle quality, and mobility.
This perspective is consistent with recent disease re-characterization by Al-Ghadban et al. (2025), who demonstrated that skeletal muscle mass, interstitial fluid accumulation, and functional performance represent partially independent dimensions of disease severity that do not correlate linearly with BMI [5]. Within this framework, overt functional impairment is most consistently recognized in Stage 3. However, the transition from Stage 2 toward Stage 3 may represent a window in which early functional signals emerge and therefore warrants proactive assessment, even before disability becomes clinically explicit. Figure 2 illustrates the established morphological progression from Stage 2 to Stage 3, contextualizing the point at which functional impairment becomes clinically evident, while Figures 3 and 4 provide representative examples of advanced phenotypes.
Rather than serving as diagnostic categories, these images are intended to contextualize a spectrum in which mechanical restriction, inflammatory burden, and muscle dysfunction progressively converge. At this stage, pharmacological strategies are discussed solely as a conceptual research consideration in individuals who demonstrate objective evidence of functional loss, inflammatory mechanical intolerance, and refractoriness to conservative management. Table 1 therefore represents a hypothesis-generating clinical phenotype, not a treatment algorithm. Importantly, the domains outlined below are intended for research stratification and hypothesis generation only, and should not be interpreted as criteria for clinical decision-making.
4.2. Contextualizing the Anabolic Rationale Within Evidence-Based Medicine
Oxandrolone occupies a distinct position among AAS due to its relatively low androgenicity and extensive historical use in catabolic conditions. Seminal work by Orr and Fiatarone Singh [28] and others has documented its use in severe burn injury, trauma, and chronic wasting states, where preservation of lean mass and bone density was achieved with acceptable long-term safety profiles. These populations represent extreme models of sustained catabolism rather than aesthetic or performance contexts.
Importantly, data from these settings are not invoked here to justify direct clinical transfer, but rather to support mechanistic plausibility: namely, that lipedematous skeletal muscle in advanced disease may share features with chronically catabolic tissue. From this perspective, anabolic signaling may theoretically function as a contractile rescue mechanism, rather than as a driver of hypertrophy per se.
4.3. Safety Considerations in a Hypothesis-Driven Framework
Any translational consideration of anabolic signaling in lipedema must be accompanied by explicit safety acknowledgment. Oxandrolone, as a 17-α-alkylated steroid, carries a recognized hepatic signal, necessitating careful contextualization. In therapeutic catabolic models, transient aminotransferase elevations were common but typically reversible, with clinically significant hepatotoxicity remaining rare under controlled conditions [28,37].
Beyond hepatic considerations, oral AAS are associated with reductions in HDL cholesterol, raising theoretical cardiovascular concerns in long-term use. In the conceptual framework proposed here, concurrent metabolic modulation via incretin-based therapy introduces a potential counterbalance. Dual GLP-1/GIP receptor agonists have consistently demonstrated favorable effects on triglycerides, LDL-cholesterol, and systemic inflammation [38], suggesting a theoretical interaction that warrants cautious evaluation, rather than presuming additive cardiometabolic risk.
Fluid handling represents an additional consideration. Androgen-mediated sodium retention could theoretically exacerbate edema in lipedema; however, GLP-1 receptor signaling has been associated with natriuresis and improved endothelial function. While such interactions remain speculative, they underscore the necessity of integrated metabolic-hormonal reasoning rather than isolated pharmacological thinking. While biologically plausible, this framework should be viewed as a conceptual scaffold intended to stimulate mechanistically informed clinical investigation rather than to anticipate clinical efficacy.
5. Conclusions
Lipedema has long been framed primarily as a disorder of disproportionate adipose tissue accumulation, frequently interpreted through cosmetic or lifestyle-oriented paradigms. This narrow perspective has shaped a standard of care largely centered on fat reduction, often overlooking functional outcomes. The synthesis presented in this hypothesis-driven review suggests that such an approach is incomplete. In advanced stages, lipedema may be more accurately conceptualized as a disorder involving systemic impairment of musculoskeletal bioenergetics, a pathological state we describe as lipedematous dynapenic myosteatosis.
A central implication of this framework is recognition of an exercise paradox in Stage 3, where functional impairment becomes clinically evident. Importantly, this paradox may begin to develop earlier, and therefore should be investigated from Stage 2 onward, before overt disability is established. While resistance training represents the physiological cornerstone for preventing dynapenia in most populations, the inflammatory and fibrotic milieu characteristic of advanced lipedema appears to render high-intensity mechanical loading poorly tolerated. This mismatch between physiological need and biological feasibility may help explain the high rates of exercise intolerance, treatment attrition, and psychological distress observed in conventional management strategies. Within this context, immobility should be understood not as behavioral non-adherence, but as a predictable consequence of intersecting metabolic, inflammatory, and mechanical constraints.
The dual-target strategy discussed in this manuscript combining metabolic modulation aimed at restoring mitochondrial fatty acid oxidation with anabolic signaling directed toward contractile tissue, is presented strictly as a conceptual and hypothesis-generating framework. Rather than replacing lifestyle-based interventions, this approach is intended to explore whether temporary pharmacological modulation could theoretically function as a physiological bridge, reducing metabolic and mechanical barriers that currently limit participation in rehabilitative exercise. Importantly, this model does not redefine the goal of therapy, but reframes the sequence by which functional recovery might be achieved.
Beyond its therapeutic implications, this work calls for a broader shift in clinical assessment. Evaluation of lipedema should extend beyond adipose tissue volume to include objective measures of muscle quality, strength, and functional performance. Preservation of contractile capacity and mobility may represent more meaningful clinical endpoints than weight loss alone. Future clinical studies are therefore warranted to test this framework prospectively, with outcomes centered on strength, mobility, pain, and independence rather than purely anthropometric change. No pharmacological class discussed herein should be interpreted as endorsed, recommended, or clinically transferable to lipedema outside formal research settings. By redirecting attention from visible fat to invisible muscle dysfunction, this paradigm has the potential to reshape both research priorities and clinical decision-making in advanced lipedema.
Author Contributions
Conceptualization; writing—original draft preparation; writing—review and editing; supervision, D.P.C.V. The author has read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
The author thanks the Federal University of São Paulo (UNIFESP) for providing academic and scientific support.
Conflicts of Interest
The author declares no conflicts of interest.
Abbreviations
| AAS | Anabolic Androgenic Steroids |
| BIA | Bioelectrical Impedance Analysis |
| BMI | Body Mass Index |
| CPT-1 | Carnitine Palmitoyltransferase 1 |
| ECM | Extracellular Matrix |
| ERα | Estrogen Receptor Alpha |
| ERβ | Estrogen Receptor Beta |
| FFM | Fat-Free Mass |
| GIP | Glucose-Dependent Insulinotropic Polypeptide |
| GLP-1 | Glucagon-Like Peptide-1 |
| HDL | High-Density Lipoprotein |
| HFpEF | Heart Failure with Preserved Ejection Fraction |
| IL-6 | Interleukin-6 |
| MRI | Magnetic Resonance Imaging |
| ROS | Reactive Oxygen Species |
| RQ | Respiratory Quotient |
| SAT | Subcutaneous Adipose Tissue |
| SIF | Italian Society of Phlebology |
| SISMES | Italian Society of Motor and Sports Sciences |
| SMM | Skeletal Muscle Mass |
| STS | Sit-to-Stand Test |
| TNF-α | Tumor Necrosis Factor Alpha |
| TUG | Timed Up and Go Test |
| UCP1 | Uncoupling Protein 1 |
References
- Allen, E.; Hines, E.; Hines, E. Lipedema of the Legs: A Syndrome Characterized by Fat Legs and Orthostatic Edema. Proc. Staff Meet. Mayo Clin 1940, 15, 184–187. [Google Scholar] [CrossRef]
- Wold, L.E.; Hines, E.A.; Allen, E.V. Lipedema of the Legs: A Syndrome Characterized by Fat Legs and Edema. Ann Intern Med 1951, 34, 1243–1250. [Google Scholar] [CrossRef]
- Földi, E.; Földi; Lipedema, M. Földi’s Textbook of Lymphology: For Physicians and Lymphedema Therapists; Elsevier, 2006. [Google Scholar]
- Herbst, K.L. Rare Adipose Disorders (RADs) Masquerading as Obesity. Acta Pharmacol Sin 2012, 33, 155–172. [Google Scholar] [CrossRef]
- Al-Ghadban, S.; Evancio, J.V.; Alfiscar, P.E.F.; Herbst, K.L. New Characterization of Lipedema Stages: Focus on Pain, Water, Fat and Skeletal Muscle. Life 2025, 15, 1397. [Google Scholar] [CrossRef]
- Christoffersen, V.; Tennfjord, M.K. Younger Women with Lipedema, Their Experiences with Healthcare Providers, and the Importance of Social Support and Belonging: A Qualitative Study. Int J Environ Res Public Health 2023, 20, 1925. [Google Scholar] [CrossRef]
- Falck, J.; Rolander, B.; Nygårdh, A.; Jonasson, L.-L.; Mårtensson, J. Women with Lipoedema: A National Survey on Their Health, Health-Related Quality of Life, and Sense of Coherence. BMC Women’s Health 2022, 22, 457. [Google Scholar] [CrossRef]
- Romeijn, J.R.M.; De Rooij, M.J.M.; Janssen, L.; Martens, H. Exploration of Patient Characteristics and Quality of Life in Patients with Lipoedema Using a Survey. Dermatol Ther (Heidelb) 2018, 8, 303–311. [Google Scholar] [CrossRef] [PubMed]
- Dudek, J.E.; Białaszek, W.; Gabriel, M. Quality of Life, Its Factors, and Sociodemographic Characteristics of Polish Women with Lipedema. BMC Women’s Health 2021, 21, 27. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, J. Lipedema, Body-Related Emotional and Disordered Eating to Cope. Surg Obes Relat Dis 2023, 19, 667–668. [Google Scholar] [CrossRef]
- Clarke, C.; Kirby, J.N.; Best, T. Beyond the Physical: The Interplay of Experienced Weight Stigma, Internalised Weight Bias and Depression in Lipoedema. Clin Obes 2025, 15, e12727. [Google Scholar] [CrossRef] [PubMed]
- Torre, Y.S.-D.L.; Wadeea, R.; Rosas, V.; Herbst, K.L. Lipedema: Friend and Foe. Horm Mol Biol Clin Investig 2018, 33, 20170076. [Google Scholar] [CrossRef] [PubMed]
- Bertsch, T.; Erbacher, G.; Elwell, R.; Partsch, H. Lipoedema: A Paradigm Shift and Consensus. J Wound Care 2020, 29, 1–51. [Google Scholar] [CrossRef]
- Viana, D.P.C.; Invitti, A.L.; Schor, E. Tirzepatide as a Potential Disease-Modifying Therapy in Lipedema: A Narrative Review on Bridging Metabolism, Inflammation, and Fibrosis. Int J Mol Sci 2025, 26, 10741. [Google Scholar] [CrossRef]
- van Esch-Smeenge, J.; Damstra, R.J.; Hendrickx, A.A. Muscle Strength and Functional Exercise Capacity in Patients with Lipoedema and Obesity: A Comparative Study. J Lymphoedema 2017, 12. [Google Scholar]
- Crescenzi, R.; Marton, A.; Donahue, P.M.C.; Mahany, H.B.; Lants, S.K.; Wang, P.; Beckman, J.A.; Donahue, M.J.; Titze, J. Tissue Sodium Content Is Elevated in the Skin and Subcutaneous Adipose Tissue in Women with Lipedema. Obesity 2018, 26, 310–317. [Google Scholar] [CrossRef]
- Gumucio, J.P.; Qasawa, A.H.; Ferrara, P.J.; Malik, A.N.; Funai, K.; Mcdonagh, B.; Mendias, C.L. Reduced Mitochondrial Lipid Oxidation Leads to Fat Accumulation in Myosteatosis. FASEB J 2019, 33, 7863–7881. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Wolf, D. Skeletal Muscle Lipid Accumulation in Obesity, Insulin Resistance, and Type 2 Diabetes. Pediatr Diabetes 2004, 5, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Aitzetmüller-Klietz, M.-L.; Busch, L.; Hamatschek, M.; Paul, M.; Schriek, C.; Wiebringhaus, P.; Aitzetmüller-Klietz, M.; Kückelhaus, M.; Hirsch, T. Understanding the Vicious Circle of Pain, Physical Activity, and Mental Health in Lipedema Patients—A Response Surface Analysis. J Clin Med. 2023, 12, 5319. [Google Scholar] [CrossRef] [PubMed]
- Viana, D. C. P.; Caseri Câmara, L.; Borges Palau, R. Menopause as a Critical Turning Point in Lipedema: The Estrogen Receptor Imbalance, Intracrine Estrogen, and Adipose Tissue Dysfunction Model. Int J Mol Sci 2025, 26, 7074. [Google Scholar] [CrossRef]
- Shiose, K.; Tanabe, Y.; Ohnishi, T.; Takahashi, H. Effect of Regional Muscle Damage and Inflammation Following Eccentric Exercise on Electrical Resistance and the Body Composition Assessment Using Bioimpedance Spectroscopy. J Physiol Sci 2019, 69, 895–901. [Google Scholar] [CrossRef]
- Borga, M.; West, J.; Bell, J.D.; Harvey, N.C.; Romu, T.; Heymsfield, S.B.; Dahlqvist Leinhard, O. Advanced Body Composition Assessment: From Body Mass Index to Body Composition Profiling. J Investig Med 2018, 66, 1–9. [Google Scholar] [CrossRef]
- Taylor, S.L.; Donahue, P.M.C.; Pridmore, M.D.; Garza, M.E.; Patel, N.J.; Custer, C.A.; Luo, Y.; Aday, A.W.; Beckman, J.A.; Donahue, M.J.; et al. Semiautomated Segmentation of Lower Extremity MRI Reveals Distinctive Subcutaneous Adipose Tissue in Lipedema: A Pilot Study. J. Med. Imag. 2023, 10. [Google Scholar] [CrossRef]
- Erbacher, G.; Bertsch, T. Lipoedema and Pain: What is the role of the psyche? – Results of a pilot study with 150 patients with Lipoedema. Phlebologie 2020, 49, 305–316. [Google Scholar] [CrossRef]
- Kunzová, M.; Lagová, E.; Keith, L. Mental and Physical Health Burden and Quality of Life in Czech Women with Lipedema. Front Glob Womens Health 2025, 6, 1629077. [Google Scholar] [CrossRef] [PubMed]
- Janota, B.; Michalska, P.; Janota, K. Lipedema: The Intersection of Physical and Mental Health. Arch Psych Psych 2025, 27, 59–66. [Google Scholar] [CrossRef]
- Annunziata, G.; Paoli, A.; Manzi, V.; Camajani, E.; Laterza, F.; Verde, L.; Capó, X.; Padua, E.; Bianco, A.; Carraro, A.; et al. The Role of Physical Exercise as a Therapeutic Tool to Improve Lipedema: A Consensus Statement from the Italian Society of Motor and Sports Sciences (Società Italiana Di Scienze Motorie e Sportive, SISMeS) and the Italian Society of Phlebology (Società Italiana Di Flebologia, SIF). Curr Obes Rep 2024, 13, 667–679. [Google Scholar] [CrossRef] [PubMed]
- Orr, R.; Fiatarone Singh, M. The Anabolic Androgenic Steroid Oxandrolone in the Treatment of Wasting and Catabolic Disorders: Review of Efficacy and Safety. Drugs 2004, 64, 725–750. [Google Scholar] [CrossRef]
- Ring, J.; Heinelt, M.; Sharma, S.; Letourneau, S.; Jeschke, M.G. Oxandrolone in the Treatment of Burn Injuries: A Systematic Review and Meta-Analysis. J Burn Care Res 2020, 41, 190–199. [Google Scholar] [CrossRef]
- Jeschke, M.G.; Finnerty, C.C.; Suman, O.E.; Kulp, G.; Mlcak, R.P.; Herndon, D.N. The Effect of Oxandrolone on the Endocrinologic, Inflammatory, and Hypermetabolic Responses During the Acute Phase Postburn. Ann Surg 2007, 246, 351–362. [Google Scholar] [CrossRef]
- Grunfeld, C.; Kotler, D.P.; Dobs, A.; Glesby, M.; Bhasin, S. Oxandrolone in the Treatment of HIV-Associated Weight Loss in Men: A Randomized, Double-Blind, Placebo-Controlled Study. J Acquir Immune Defic Syndr 2006, 41, 304–314. [Google Scholar] [CrossRef]
- Pharo, A.; Salvato, P.; Vergel, N.; Carroll, E.; Sauer, L.; Mooney, M. Oxandrolone: Anabolic Steroid Use in HIV Positive Women. Nutrition 1997, 13, 268. [Google Scholar] [CrossRef]
- Fontanarosa, P.B.; Romeyn, M.; Gunn, N., Iii. Resistance Exercise and Oxandrolone for Men With HIV-Related Weight Loss. JAMA 2000, 284, 176. [Google Scholar] [CrossRef]
- Fox-Wheeler, S.; Heller, L.; Salata, C.M.; Kaufman, F.; Loro, M.L.; Gilsanz, V.; Haight, M.; Umman, G.C.; Barton, N.; Church, J.A. Evaluation of the Effects of Oxandrolone on Malnourished HIV-Positive Pediatric Patients. Pediatrics 1999, 104, e73–e73. [Google Scholar] [CrossRef] [PubMed]
- Reeves, P.T.; Herndon, D.N.; Tanksley, J.D.; Jennings, K.; Klein, G.L.; Mlcak, R.P.; Clayton, R.P.; Crites, N.N.; Hays, J.P.; Andersen, C.; et al. Five-Year Outcomes after Long-Term Oxandrolone Administration in Severely Burned Children: A Randomized Clinical Trial. Shock 2016, 45, 367–374. [Google Scholar] [CrossRef] [PubMed]
- de Mello Gindri, I.; Almeida, G.; Saraiva, C.; Ferrari, G.; Dallacosta, D.; Roesler, C.R. The Safety and Effectiveness of Oxandrolone on Different Clinical Conditions: A Systematic Review. Endocr. Metab. Sci. 2025, 18. [Google Scholar] [CrossRef]
- Li, H.; Guo, Y.; Yang, Z.; Roy, M.; Guo, Q. The Efficacy and Safety of Oxandrolone Treatment for Patients with Severe Burns: A Systematic Review and Meta-Analysis. Burns 2016, 42, 717–727. [Google Scholar] [CrossRef]
- Jastreboff, A.M.; Aronne, L.J.; Ahmad, N.N.; Wharton, S.; Connery, L.; Alves, B.; Kiyosue, A.; Zhang, S.; Liu, B.; Bunck, M.C.; et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med 2022, 387, 205–216. [Google Scholar] [CrossRef]
Figure 1.
Conceptual model of lipedematous dynapenic myosteatosis and a hypothesis-driven pharmacological bypass. (A) Lipedematous blockade. In the untreated state, intramyocellular lipid accumulation (myosteatosis) is shown in association with mitochondrial inflexibility, illustrated as impaired CPT-1–mediated fatty acid transport. High-intensity mechanical loading may further amplify reactive oxygen species (ROS) production and pro-inflammatory cytokine signaling (e.g., TNF-α, IL-6), favoring muscle dysfunction and atrophy rather than adaptive hypertrophy. (B) Hypothesis-driven pharmacological bypass. A dual-target conceptual framework is illustrated. Metabolic modulation through dual GIP/GLP-1 receptor agonism (e.g., tirzepatide) may enhance mitochondrial substrate oxidation and reduce ectopic lipid accumulation. In parallel, anabolic signaling—shown using oxandrolone as an illustrative example—may theoretically promote contractile protein synthesis via nuclear androgen receptor pathways, partially reducing dependence on high mechanical loading. This schematic is intended solely for conceptual visualization and should not be interpreted as a therapeutic sequence, algorithm, or clinical pathway.
Figure 1.
Conceptual model of lipedematous dynapenic myosteatosis and a hypothesis-driven pharmacological bypass. (A) Lipedematous blockade. In the untreated state, intramyocellular lipid accumulation (myosteatosis) is shown in association with mitochondrial inflexibility, illustrated as impaired CPT-1–mediated fatty acid transport. High-intensity mechanical loading may further amplify reactive oxygen species (ROS) production and pro-inflammatory cytokine signaling (e.g., TNF-α, IL-6), favoring muscle dysfunction and atrophy rather than adaptive hypertrophy. (B) Hypothesis-driven pharmacological bypass. A dual-target conceptual framework is illustrated. Metabolic modulation through dual GIP/GLP-1 receptor agonism (e.g., tirzepatide) may enhance mitochondrial substrate oxidation and reduce ectopic lipid accumulation. In parallel, anabolic signaling—shown using oxandrolone as an illustrative example—may theoretically promote contractile protein synthesis via nuclear androgen receptor pathways, partially reducing dependence on high mechanical loading. This schematic is intended solely for conceptual visualization and should not be interpreted as a therapeutic sequence, algorithm, or clinical pathway.
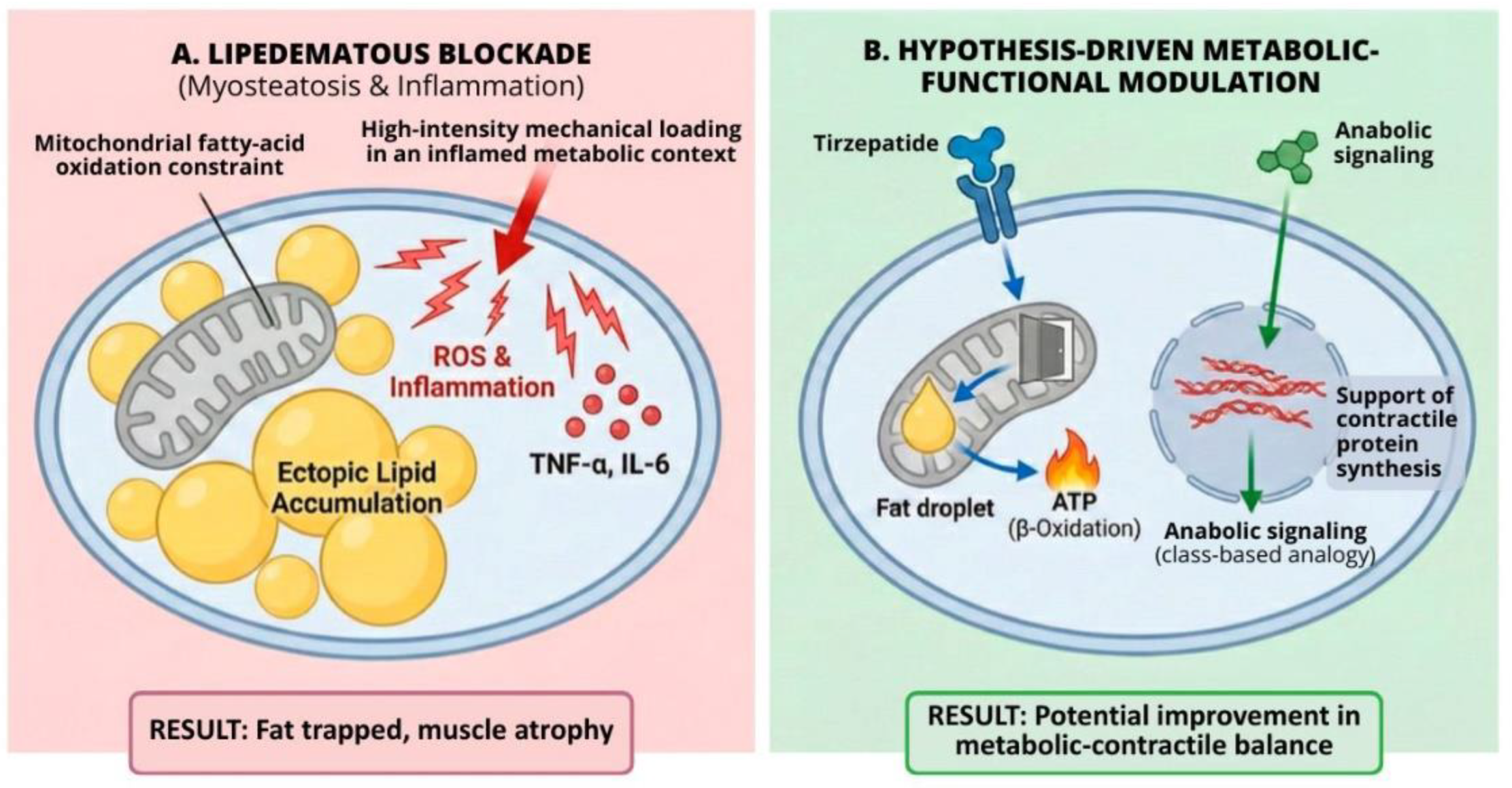
Figure 2.
Morphological progression of lipedema from Stage 2 to Stage 3 and its relationship with functional impairment. Representative schematic illustration of lipedema Stages 2, 2.5, and 3, highlighting progressive morphological changes in skin and subcutaneous tissue. Stage 2 shows diffuse thigh indentations with grainy to pearl-to-walnut-sized nodules; Stage 2.5 represents a transitional phenotype with early lobule formation around the hips and knees; Stage 3 is characterized by pronounced skin folds, large deforming lobules, and clinically evident functional impairment, including reduced mobility, pain, and mechanical limitation. The figure preserves established morphological staging and emphasizes that functional impairment is most consistently recognized at Stage 3, while earlier stages may warrant proactive functional assessment. The illustration is intended for conceptual clarification and does not redefine diagnostic or staging criteria.
Figure 2.
Morphological progression of lipedema from Stage 2 to Stage 3 and its relationship with functional impairment. Representative schematic illustration of lipedema Stages 2, 2.5, and 3, highlighting progressive morphological changes in skin and subcutaneous tissue. Stage 2 shows diffuse thigh indentations with grainy to pearl-to-walnut-sized nodules; Stage 2.5 represents a transitional phenotype with early lobule formation around the hips and knees; Stage 3 is characterized by pronounced skin folds, large deforming lobules, and clinically evident functional impairment, including reduced mobility, pain, and mechanical limitation. The figure preserves established morphological staging and emphasizes that functional impairment is most consistently recognized at Stage 3, while earlier stages may warrant proactive functional assessment. The illustration is intended for conceptual clarification and does not redefine diagnostic or staging criteria.


Table 1.
Hypothesis-Generating Functional Phenotype for Research Stratification in Advanced Lipedematous Dynapenia.
Table 1.
Hypothesis-Generating Functional Phenotype for Research Stratification in Advanced Lipedematous Dynapenia.
| Domain | Operational definition & assessment (examples) | Pathophysiological significance | Suggested objective endpoints |
|---|---|---|---|
| 1. Objective dynapenia (function) | Timed Up and Go (TUG) >10 s; Sit-to-Stand (5×STS or 30 s STS) below age/sex norms; handgrip or quadriceps strength below normative values (specify dynamometer and units). | Dissociation between limb volume and contractile performance, indicating failure of muscle quality rather than simple mass loss. | TUG, STS, handgrip, isokinetic quadriceps torque, gait speed, mobility-related patient-reported outcomes. |
| 2. Mechanical intolerance and refractoriness to loading | Post-exertional pain persisting >24 h; measurable limb volume increase within 24–48 h after activity; persistence of symptoms despite ≥6 months of documented conservative therapy (compression, physiotherapy, diet). | Captures the “exercise paradox,” in which inflammatory and edematous responses limit tolerance to mechanical loading and promote disuse atrophy. | Pain NRS/VAS, post-exertional symptom diary, limb volume change, pressure pain thresholds, accelerometry-based activity metrics. |
| 3. Myosteatosis and impaired muscle quality (structure) | MRI Dixon fat fraction or muscle radiodensity; ultrasound echo-intensity where advanced imaging is unavailable; sodium-MRI markers when feasible. | Links dynapenia to ectopic lipid deposition, inflammatory muscle remodeling, and reduced contractile efficiency. | Muscle fat fraction, radiodensity/echo-intensity, correlation with strength and mobility, longitudinal structural change. |
| 4. Metabolic–inflammatory milieu consistent with oxidative mismatch | Optional enrichment markers: insulin resistance indices, inflammatory cytokines, adipokines, and fibrosis/ECM-related biomarkers. | Tests the proposed lipolysis–oxidation mismatch and immunometabolic drivers sustaining myosteatosis and functional decline. | Metabolic flexibility (RQ/indirect calorimetry), insulin sensitivity, inflammatory and fibrosis-related panels, association with imaging and function. |
This table defines a hypothesis-generating phenotype intended to operationalize the proposed pathophysiological framework and inform future study design. It does not establish diagnostic criteria, therapeutic eligibility, or clinical recommendations.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



