
Submitted:
01 February 2026
Posted:
02 February 2026
You are already at the latest version
Abstract
The quality of trabecular and cortical bone is significant for preventing fractures and ensuring implant success, particularly given the rising prevalence of osteoporosis associated with population ageing. However, consensus on the clinical application of bone quality assessments remains elusive. This narrative review examines available methods for assessing bone quality prior to skeletal and maxillofacial surgeries, and explores their impact on prosthesis selection and implant outcomes. A comprehensive literature search was conducted in MEDLINE database to synthesize clinical data on Dual-energy X-ray Absorptiometry (DXA), Computed Tomography (CT), Cone Beam CT (CBCT), Magnetic Resonance Imaging (MRI), and Quantitative Ultrasound (QUS). Current literature reveals that while DXA and MRI are increasingly utilized for orthopedic assessment, CBCT remains the standard in dentistry. The findings emphasize that bone quality, encompassing microarchitecture and turnover, is as critical as mineral density for initial stability and osseointegration. Furthermore, a significant correlation exists between systemic and local bone density, suggesting that maxillary assessments may reflect overall bone health. Integrating these viewpoints enhances preoperative planning and highlights the potential for opportunistic osteoporosis screening in dental settings.
Keywords:
bone density [MeSH]
; osteoporosis [MeSH]
; dental implants [MeSH]
; osseointegration [MeSH]
; bone quality
; opportunistic screening
; preoperative assessment
1. Introduction
Currently, the most significant global health issue related to bone health is osteoporosis. This skeletal disorder is characterized by compromised bone strength, is associated with aging, and has a rising prevalence due to the rapid aging of the population. The global prevalence of osteoporosis was estimated at 18.3%, with a 95% confidence interval ranging from 16.2% to 20.7% [1]. The clinical importance of this disease lies in its severe health consequences, including a high risk of falls and fractures, hospitalizations, disability, and mortality [2].
Bone assessment reflects primarily the integration of bone mineral density (BMD) and bone quality (BQ) [3]. These are fundamental concepts in the study of both skeletal and dental systems, particularly for fracture prevention and the success of prosthetic and implant surgeries. BMD refers to the amount of bone mass per unit volume, typically measured by Dual-energy X-ray Absorptiometry (DXA) [4]. DXA, also known as DEXA, is a widely used noninvasive method for assessing BMD. It operates by transmitting two X-ray beams at different energies through the bone; by evaluating the absorption of each beam, it determines bone density and enables discrimination between bone and soft tissue [5]. This technique is rapid and entails minimal radiation exposure, making it a safe method for evaluating bone health [6]. On the other hand, BQ describes aspects of bone composition and structure that contribute to bone strength independently of BMD [7]. BQ encompasses a variety of factors, including bone microarchitecture, bone turnover, accumulated damage, and mineralization [8].
BMD is a crucial indicator for assessing the risk of osteoporotic fractures, particularly in older adults [9]. Evaluation of BMD enables the identification of individuals at risk and early intervention to prevent fractures [10]. In addition to BMD, BQ is equally important, particularly in the context of dental implant surgery, where it affects initial stability, osseointegration, and long-term longevity [11]. Understanding BQ prior to surgery enables surgeons to plan the procedure more effectively, select appropriate materials, and anticipate potential complications [12].
In orthopedic procedures such as hip and knee replacements, understanding both BMD and BQ aids in selecting the appropriate surgical approach and prosthetic materials [3]. A practical preoperative evaluation can prevent implant failure and enhance the functionality of prosthetic devices [13]. However, preoperative assessment of BQ is especially critical in dental implantology [14]. Studies have shown that poor BQ, particularly in the maxilla, is associated with lower survival rates of dental implants than in the mandible [15].
Standard methods for assessing bone include the use of T-scores and Z-scores defined by the World Health Organization (WHO), where osteoporosis is diagnosed when the BMD is 2.5 standard deviations (SD) or more below the mean for healthy young women [16]. In dentistry, bone quality and density vary significantly by location; for example, the anterior maxilla typically has denser trabecular bone [17], while the mandible is generally thicker than the maxilla, with density decreasing in the posterior region [18]. These variations require specific evaluations for proper implant planning [19].
Routine dental assessments typically involve Cone Beam Computed Tomography (CBCT) for detailed evaluation of bone characteristics. The Lekholm and Zarb classification, along with the Misch classification, are commonly used to analyze these images [17,19].
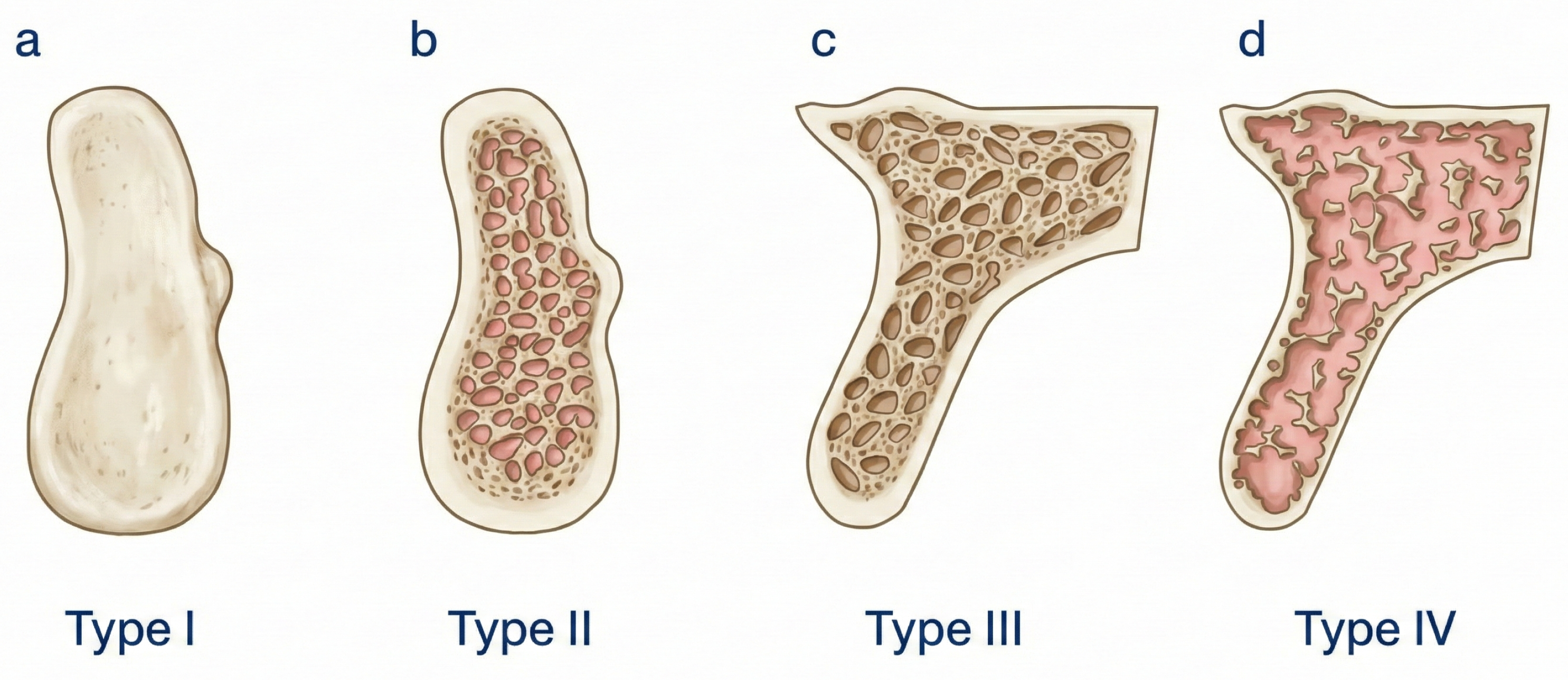
The Lekholm and Zarb system classifies bone into four types based on clinical observations and used to characterise the implant site in order to predict primary stability and surgical success [20].
Similarly, Misch’s classification focuses on bone density measured in Hounsfield units (HU) from Computed Tomography (CT) scans is applied to quantitatively measure local bone density to guide implant design, insertion torque, and loading protocols [21].
Finally, DXA considers four categories based on T-score, defined as the normalized distance in standard deviations, with respect to the reference BMD values of a healthy population [16]. This parameter allows to compared the different available devices and to assess systemic bone mineralisation to stratify fracture risk and to diagnose osteoporosis (Table 1).
While existing classification systems are essential for predicting surgical outcomes, there remains limited integration between the methods used to assess bone quality in maxillofacial surgery, orthopedics, and osteoporosis diagnosis. Although the biological principles underlying bone healing and osseointegration are largely shared across these clinical domains, their assessment protocols, measurement strategies, and interpretative frameworks have evolved in relative isolation. As a result, key methodological advances and clinical findings are not consistently translated or shared across disciplines.
Figure 1.
Schematic representation of the Lekholm and Zarb bone quality classification system based on clinical observations. Bone is categorized into four types according to cortical thickness and trabecular density: (a) Type I, dense cortical bone; (b) Type II, dense cortical bone with trabecular bone; (c) Type III, dense trabecular bone with a thin cortical layer; and (d) Type IV, sparse trabecular bone with a thin cortical layer [20].
Figure 1.
Schematic representation of the Lekholm and Zarb bone quality classification system based on clinical observations. Bone is categorized into four types according to cortical thickness and trabecular density: (a) Type I, dense cortical bone; (b) Type II, dense cortical bone with trabecular bone; (c) Type III, dense trabecular bone with a thin cortical layer; and (d) Type IV, sparse trabecular bone with a thin cortical layer [20].
Against this background, this narrative review aims to provide an integrative synthesis of the main methods and empirical findings related to BQ assessment across two interconnected clinical domains: maxillofacial and skeletal disciplines. Specifically, the review addresses two overarching questions: (i) which methods and parameters are currently used to characterize bone quality in the context of pre-implant and prosthetic planning, and (ii) to what extent these parameters reflect related or complementary aspects of bone quality across systemic and local anatomical sites.
To address these questions, this paper is structured in two complementary parts. First, it synthesizes current evidence on how different approaches to bone quality assessment influence prosthetic and implant-related decision-making. Second, it examines the relationship between systemic and local bone density measures as a basis for cross-disciplinary clinical interpretation. Within this structure, the review adopts a clinically oriented and integrative perspective, using osteoporosis as a reference framework to explore broader challenges in bone quality assessment and to analyze how heterogeneous measurement methodologies inform prosthetic decision-making across orthopedic and maxillofacial disciplines.
2. Materials and Methods
To provide a broad and comprehensive overview of the current landscape of bone assessment, a literature search was conducted in the MEDLINE bibliographic database (via PubMed) for articles published between 2008 and 2024. This review synthesizes clinical evidence on preoperative assessment of BMD and BQ in both skeletal and maxillofacial applications. Given its nature as a narrative review designed to provide a qualitative synthesis of the literature, it does not follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol [22].
The search strategy was designed to identify studies focusing on the intersection of bone health and surgical outcomes. Key terms included “bone mineral density”, “bone quality”, “preoperative assessment”, “hip prosthetic”, and “dental implants”. The inclusion focused on clinical studies involving human subjects that utilized diagnostic modalities such as DXA, CT, CBCT, Magnetic Resonance Imaging (MRI), and Quantitative Ultrasound (QUS).
During the selection process, studies were prioritized based on their relevance to preoperative planning, implant stability, and prosthetic success. To ensure a focused narrative, the review primarily considered full-text articles that addressed the clinical implications of bone assessment or the relationship between skeletal and maxillary bone densities. Studies focusing exclusively on osteoporosis treatment without a surgical context or those with limited clinical relevance were excluded.
Data synthesis was organized by grouping studies into three thematic areas: skeletal bone assessment in orthopedics, maxillary bone assessment in dentistry, and the correlation between these two regions. For each included study, key variables were analyzed, including study design, sample size, population characteristics, assessment methods, and primary clinical outcomes.
This study was approved by the Institutional Committee of Bioethics of Research in Human Beings of the University of Valparaíso (CEC-UV) with resolution code: ’CEC-UV 299-4’.
3. Results
3.1. Skeletal Bone Assessment: Orthopedic Applications and Clinical Outcomes
Preoperative planning in orthopedic surgeries, such as total hip arthroplasty (THA) and periacetabular osteotomy (PAO), relies heavily on the accurate characterization of bone status to ensure long-term implant stability [12,13]. A summary of the primary clinical studies, methodologies, and findings related to skeletal bone assessment is provided in Table 1.
3.1.1. Conventional Radiography and Morphometric Indices
Radiographic assessment remains a fundamental tool for evaluating hip anatomy and selecting appropriate implants [23]. Parameters such as the canal-to-calcar isthmus ratio and the cortical index are frequently used to forecast outcomes in THA. For instance, a significant correlation has been established between the cortical index and the intraoperative femoral neck diameter, aiding the selection of appropriate prosthetic dimensions [23]. As noted in Table 1, these traditional indices provide essential baseline data, although their predictive power for mechanical complications may be limited relative to newer modalities.
However, the predictive power of these indices varies. Research has shown that while morphometric parameters provide valuable insights, they may not be as precise as densitometry in assessing BMD [23]. This suggests that combining traditional radiographic evaluation with densitometry could provide a more comprehensive assessment of bone quality prior to THA. Regarding mechanical stability, research by Ries et al. (2019) demonstrated that while subsidence was significantly higher in collarless stems compared to collared designs, traditional anatomical parameters like the canal flare index (CFI) or canal fill ratio (CFR) were not identified as definitive risk factors [24]. Beyond mechanical stability, the radiographic severity of osteoarthritis serves as a strong predictor of patient-reported outcomes, including satisfaction and the Oxford Hip Score [25]. In the context of PAO, preoperative incipient osteoarthritis is the most important predictor of poor hip joint survival, leading to an increased risk of conversion to THA [26].
3.1.2. The Role of DXA
DXA is the most widely utilized method for evaluating systemic BMD prior to surgery [5,6]. While men generally exhibit higher BMD values across all anatomical regions, women often experience a decrease in hip BMD with age, while lumbar spine values remain relatively stable [27].
The relationship between systemic BMD and local implant stability remains complex. Recent studies found no significant association between preoperative BMD and femoral stem subsidence in patients younger than 75 years with a T-score above -2.5, suggesting that in younger populations with adequate press-fit, BMD may not be the primary predictor of early migration [28,29]. Conversely, other findings suggest that women with normal total hip BMD experience less stem rotation and subsidence [30]. Furthermore, longitudinal DXA scans have shown significant periprosthetic bone loss within the first six months post-THA, particularly in the femoral calcar region (Gruen zone 7), suggesting that preoperative assessments could identify patients who might benefit from osteoinductive therapies [31].
3.1.3. Advanced Imaging: CT and MRI-Based Quality Scores
Beyond densitometry, advanced imaging provides insights into bone microarchitecture. Preoperative BMD measurement using CT can reveal bone mechanical properties, which are essential for planning THA. There is a significant correlation between cortical BMD measured on CT and micro-CT scans, suggesting that preoperative CT can provide critical information on bone porosity [19]. These advanced quantitative techniques, along with MRI-derived scores such as Vertebral Bone Quality (VBQ) and Endplate Bone Quality (EBQ), represent a shift toward site-specific assessment (Table 2). In unicompartmental knee replacement (UKR), micro-CT evaluations showed that tibial component migration was not necessarily associated with baseline density or turnover, suggesting the influence of other mechanical factors [32]. However, calibrated CT scans have been shown to predict patient-reported outcomes (PROMs) after cementless THA, with higher preoperative BMD at the planned stem site associated with better short-term outcomes [33].
MRI is emerging as a critical tool, particularly in spine surgery. The VBQ score, derived from T1-weighted MRI, enables differentiation between healthy and osteoporotic bone and predicts complications such as loss of lumbar lordosis [34,35]. More recently, the EBQ score has demonstrated superior predictive value for cage subsidence following lateral lumbar interbody fusion (LLIF) and anterior cervical discectomy and fusion (ACDF) [36,37,38]. These MRI-based scores are radiation-free and can be obtained opportunistically from standard preoperative scans [35,38].
3.1.4. QUS
Non-invasive, radiation-free ultrasound methods are gaining interest for assessing peripheral and local bone [14]. The Azalée guided-wave Ultrasound (US) device (an axial-transmission device) has been investigated for its ability to estimate the thickness and porosity of cortical bone, showing good correlation with micro-CT. Specifically, pulse-echo ultrasonometry used to measure cortical thickness in the distal radius has been linked to an increased risk of femoral stem subsidence in postmenopausal women [39].
Despite its potential in predicting implant stability and complications, certain limitations must be noted. Research has shown that US measurements at peripheral sites, such as the radius and tibia, are unreliable predictors of the mechanical properties of the femoral neck. This emphasizes the critical need for site-specific measurements rather than relying on peripheral proxies for central bone assessment.
3.2. Maxillofacial Bone Assessment and Its Clinical Implications
The preoperative evaluation of bone status in the maxillofacial region is not merely a diagnostic step but a fundamental determinant of successful dental implant outcomes [11,12]. Table 1 summarizes clinical studies investigating the efficacy and application of various maxillofacial bone assessment modalities. Anatomical variability plays a decisive role; while the maxilla presents specific challenges due to varying bone density and its proximity to the maxillary sinus [40], the anterior mandible typically offers superior mechanical properties, including significantly higher density, elastic modulus, and ultimate compressive strength compared to posterior regions [11].
3.2.1. Anatomical Considerations and Site-Specific Selection
Understanding these site-specific characteristics is essential for optimizing implant dimensions and surgical planning [40]. For instance, the posterior maxilla, characterized by less dense cancellous bone, often requires longer or wider implants to achieve adequate primary stability. In contrast, the denser cortical bone found in the anterior maxilla may accommodate shorter implant designs without compromising success rates [40]. This precision in selection is vital for minimizing both early and late complications, thereby ensuring long-term prosthetic longevity.
3.2.2. The Digital Evolution: From 2D Imaging to Artificial Intelligence
Radiographic imaging remains the cornerstone of pre-surgical evaluation. Traditionally, two-dimensional (2D) modalities, such as panoramic and periapical views, were the standard for assessing bone availability and anatomical features. However, the integration of Artificial Intelligence (AI) has significantly enhanced the utility of these 2D views. Current deep learning models, trained on extensive radiographic and CBCT datasets, can now categorize bone quality from panoramic images with high precision, showing strong correlations with both three-dimensional (3D) evaluations and surgical assessments [41]. This advancement provides clinicians with objective, quantitative data to support clinical decision-making.
In addition, postoperative care must include diligent radiographic follow-up. Studies have demonstrated that tracking bone density changes around titanium implants in the posterior mandible is effective for evaluating osseointegration and identifying early signs of failure [42].
3.2.3. The Paradigm Shift to 3D: CT and CBCT Protocols
Despite the utility of 2D imaging, the inherent limitations in representing 3D architecture led to the adoption of CT and CBCT. CT provides quantitative data in HU, enabling precise determination of the appropriate implant type and placement technique [43,44]. Clinical research has shown a significant correlation between CT-derived bone density and the surgeon’s tactile sense during placement, effectively confirming clinical judgment with objective data [43].
Dynamic assessment of bone healing is also possible through CT; research indicates a characteristic decrease in density during the first month of bone regeneration, followed by a gradual increase until prosthetic loading [45]. To optimize early loading protocols, a minimum bone density threshold of 528 HU has been suggested as a prerequisite for success [44]. Additionally, significant correlations have been established between CT-derived density and primary stability measured via resonance frequency analysis (RFA) [46].
Since its introduction in the late 1990s, CBCT has become the gold standard for preoperative bone evaluation [47,48,49]. CBCT provides highly accurate assessments of bone dimensions and quality while identifying vital structures such as nerves and sinuses [49]. Recent sensitivity analyses emphasize that bone mass density influences stress distribution, particularly in cases of alveolar resorption, thereby directly guiding implant selection [50]. A robust association exists between CBCT-derived density and initial implant stability, a critical factor for long-term survival [51]. In immediate implant scenarios, CBCT outperforms traditional radiographs in assessing crestal bone levels and in monitoring healing and loading protocols [52].
3.2.4. The DXA Paradox in Dental Implantology
While DXA remains the global standard for diagnosing systemic osteoporosis, its role in dental implant planning is controversial. Studies have failed to demonstrate a direct, consistent correlation between systemic BMD (measured by DXA) and local jawbone quality required for implant success [53]. Notably, retrospective data on postmenopausal women show no significant association between a systemic osteoporosis diagnosis and dental implant failure rates [54]. This suggests that while DXA is invaluable for identifying systemic conditions, it may not reliably predict local surgical outcomes, and its results should be interpreted with caution in a dental context.
3.3. The Interplay Between Skeletal and Maxillofacial Bone Health
The relationship between skeletal BMD and jaw bone density is a critical area of research with profound clinical implications for both diagnosis and treatment planning [57]. Evidence suggests that bone conditions observed in the mandible and maxilla can reflect a patient’s overall skeletal health, providing a comprehensive view of systemic bone status [57]. A summary of studies examining these correlations across various imaging modalities and anatomical sites is provided in Table 3.
3.3.1. Correlations via Conventional Imaging and DXA
Initial studies using DXA have demonstrated a positive correlation between the BMD of the femur and lumbar vertebrae and various regions within the jaws [57]. Specifically, a significant link exists between mandibular cortical bone height and lumbar spine BMD [58]. Research indicates that a reduced cortical bone height at the mental foramen and gonion can serve as a predictor for decreased BMD in the lumbar spine, suggesting that panoramic radiographs are useful preliminary tools for identifying osteoporosis risk [58].
However, this association is not uniform across all anatomical sites. Some investigations have found that although mandibular BMD varies significantly by region, it does not always correlate strongly with femoral neck BMD, highlighting the influence of regional biomechanical factors on jaw bone density measurements [59].
3.3.2. Advanced Modalities and Opportunistic Screening
The integration of sophisticated imaging technologies has further clarified the link between systemic and mandibular BMD [60]. Mandibular radiomorphometric indices and CT values derived from CBCT images have shown strong positive correlations with spine BMD measurements [60]. Furthermore, CBCT gray values and fractal dimension (FD) analysis have emerged as reliable, non-invasive indicators of systemic bone health [61,62].
CBCT indices effectively differentiate between normal and osteoporotic groups, particularly in postmenopausal women, advocating for its use in opportunistic osteoporosis risk assessment [63,64]. Although the trabecular bone structure of the jaws may appear less affected in some osteoporotic models, dense trabecular bone analysis via CBCT remains a promising avenue for early screening [65]. Using CBCT in conjunction with DXA facilitates a thorough evaluation of bone health, aiding early detection and cross-disciplinary management of systemic skeletal conditions [65].
Figure 2.
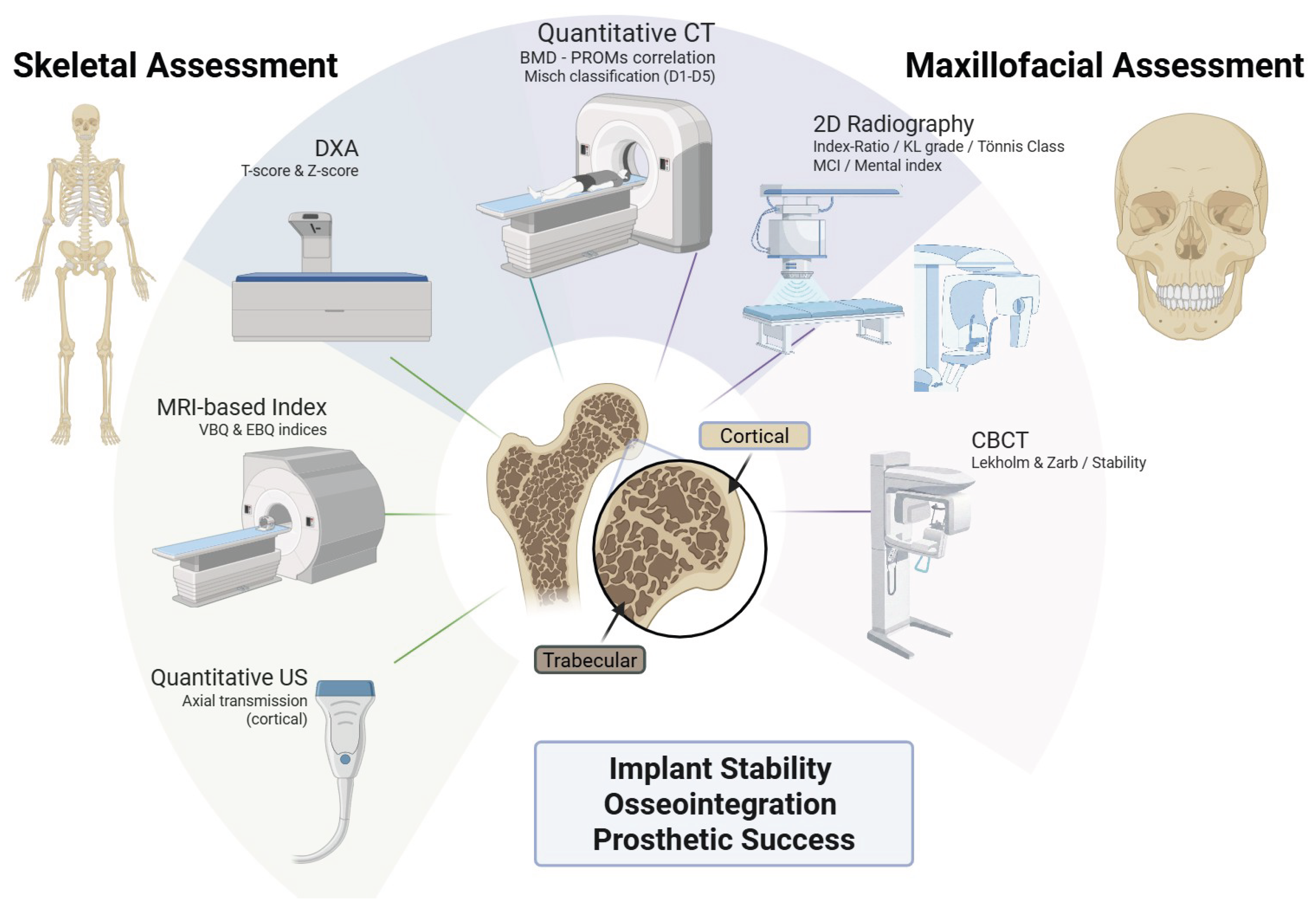
Multi-modal diagnostic landscape for bone quality characterization. Comparison between skeletal (DXA, CT, MRI, QUS) and maxillofacial (CBCT, CT, 2D X-ray) assessment tools. The integration of these modalities aims to optimize preoperative planning for achieving primary stability and successful osseointegration in both orthopedic and dental applications.
Figure 2.
Multi-modal diagnostic landscape for bone quality characterization. Comparison between skeletal (DXA, CT, MRI, QUS) and maxillofacial (CBCT, CT, 2D X-ray) assessment tools. The integration of these modalities aims to optimize preoperative planning for achieving primary stability and successful osseointegration in both orthopedic and dental applications.
4. Discussion
The findings of this review underscore a pivotal transition in bone assessment, moving from traditional structural observations toward a multi-modal, site-specific characterization of bone quality. Between 2008 and 2024, the literature reveals an accelerated adoption of specialized modalities such as CT and MRI [34,60]. While conventional radiography remains the baseline for orthopedic and dental planning, as established by the historical work of Noble et al. (1988), it is no longer sufficient to address the complexities of modern implantology and prosthetic stability [23,55]. This narrative synthesis suggests that the challenge lies not in the lack of technology but in the need for an integrated clinical framework that bridges the gap between systemic health and local surgical outcomes.
A significant theme emerging from this synthesis is the clinical reliability of local bone quality over systemic metrics in predicting surgical success. This leads to what might be termed the “DXA Paradox”: while DXA is the gold standard for diagnosing systemic osteoporosis, its predictive value for local dental implant stability is surprisingly limited [53,54]. This discrepancy likely stems from the fundamental difference between systemic bone metabolism—captured by DXA as a measure of overall skeletal health—and the local mechanical response of the alveolar bone when subjected to functional loading during and after implant placement. Regarding dental implant therapy, evidence suggests that osteoporosis is not an absolute contraindication, as implant survival rates in osteoporotic patients are statistically comparable to those in healthy individuals [15,69]. However, systemic low bone mass does appear to influence peri-implant tissue stability; systematic reviews indicate significant, albeit clinically manageable, increases in marginal bone loss around implants in osteoporotic patients compared to controls [15,69].
This phenomenon is closely linked to compromised local bone quality; specifically, implants placed in low-density bone (Type IV) exhibit lower survival rates and primary stability than those placed in denser bone types (Types I, II, and III) [70,71]. Consequently, accurate preoperative assessment remains critical. New classification systems that quantitatively analyze cortical thickness and cancellous density separately via CBCT may offer superior guidance for surgical planning than traditional subjective models, helping clinicians predict primary stability and mitigate risks in patients with compromised microarchitecture [72,73]. This localized focus is mirrored in orthopedics, where advanced MRI-based scores such as the VBQ and EBQ are now preferred over systemic T-scores to predict complications, including cage subsidence, in spine surgery [34,37].
The interdisciplinary link between skeletal and maxillofacial bone health represents a promising frontier for opportunistic screening. While DXA remains the standard for diagnosis, its limited accessibility for routine population screening underscores the potential of dental imaging as a valuable adjunctive tool. The indisputable correlation between mandibular indices, such as the Mandibular Cortical Index (MCI), and spinal BMD positions the dental professional as a critical actor in the early detection of systemic bone fragility [56,66]. Recent investigations into CBCT have validated the use of radiomorphometric indices, such as the three-dimensional mandibular osteoporosis index (3D MOI), to distinguish postmenopausal women with osteoporosis with high specificity [74]. This supports findings that qualitative and quantitative indices on standard panoramic radiographs—including mandibular cortical width and the Klemetti index—can effectively identify patients with low BMD [58,61,75]. Furthermore, establishing a significant positive correlation between the BMD of the mandible and that of the lumbar spine and femur reinforces the viability of using regional jawbone density as a prognostic parameter for systemic health [57,73].
Looking ahead, technologies such as high-resolution peripheral quantitative computed tomography (HR-pQCT) and opportunistic Quantitative CT (QCT) are fundamentally redefining the assessment of bone fragility [76,77]. By analyzing the “void space” within trabecular networks, these tools can identify patients at high fracture risk even when DXA T-scores appear normal [76,77]. Such advancements emphasize that bone “quality” is a multi-dimensional construct—integrating density, microstructure, and turnover—that demands a personalized diagnostic approach over a generalized metric [78]. Complementing these high-resolution methods, the integration of cortical thickness and porosity reference values with anthropometric data (height, weight, and body surface area) provides a robust framework for enhancing fracture risk detection via portable and non-invasive ultrasonic devices [79].
Despite the wealth of evidence, several limitations persist in the current body of research. The geographic concentration of studies—with a notable scarcity of data from regions such as Latin America—limits the generalizability of findings across diverse ethnic and environmental contexts. Furthermore, a persistent clinical silo exists; despite sharing the same biological principles of osseointegration and bone healing, orthopedic and maxillofacial surgeons rarely utilize unified assessment protocols. Moving forward, the goal should be to harmonize these fields, using the dentist’s accessibility for screening and the orthopedic surgeon’s advanced diagnostic tools to create a comprehensive roadmap for bone health management.
5. Conclusions
The inherent disparity between assessment methods in the skeletal and maxillofacial realms underscores a persistent clinical silo between medical and dental specialties. Despite this separation, foundational imaging modalities such as DXA and CBCT remain universally essential for the precision planning of both orthopedic and dental implants. This review highlights that bone quality—a multidimensional construct encompassing microarchitecture and turnover—is as critical as mineral density for achieving surgical success and preventing future fractures.
Preoperative evaluation of these parameters is not merely a diagnostic formality; it is the cornerstone for tailoring surgical techniques, selecting appropriate materials, and anticipating potential complications. In both orthopedic and dental contexts, the quality of the underlying bone substrate directly dictates the initial stability and long-term osseointegration of the implant, ultimately determining the longevity of the prosthetic rehabilitation.
Furthermore, the established relationship between systemic and local bone density measurements—while not yet definitive—opens a significant window for interdisciplinary synergy. The potential to use maxillofacial imaging for the early detection of systemic osteoporosis presents a transformative opportunity for public health. By adopting advanced technological methods that bridge these two "worlds," clinicians can move toward a model of opportunistic screening that improves post-surgical results and systemic patient outcomes based on their specific bone status.
Finally, it is imperative to acknowledge that bone health does not exist in isolation. Surgical success and fracture risk are moderated by a complex interplay of factors, including the patient’s systemic health, body mass index, and detrimental habits such as smoking. Future research should aim to integrate these variables into unified predictive models, fostering a genuinely holistic approach to bone health that transcends traditional disciplinary boundaries.
Author Contributions
Conceptualization, methodology, validation, formal analysis, investigation, resources, data curation, writing—original draft preparation, writing—review and editing, visualization, supervision, project administration, and funding acquisition, J.-G.M., P.M.R. and J.J.R. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Agencia Nacional de Investigación y Desarrollo (ANID), Chile, through the “Doctorado en Chile Scholarship Program, Academic Year 2025 (Grant No. 1340/2025)”, “Doctorado en Chile Scholarship Program, Academic Year 2024 (Grant No. 1202/2024)” and by the Chilean projects ANID Fondecyt Regular 1241091 and ANID NAM 23|0059.
Institutional Review Board Statement
The study was approved by the Institutional Committee of Bioethics of Research in Human Beings of the University of Valparaíso (CEC-UV) with resolution code: ’CEC-UV 299-4’
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no financial or non-financial conflicts of interest that could be perceived as influencing the work reported in this manuscript.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| BMD | Bone Mineral Density |
| BQ | Bone Quality |
| DXA | Dual Energy X-Ray Absorptiometry |
| WHO | World Health Organization |
| SD | Standard Deviation |
| CBCT | Cone Beam Computed Tomography |
| HU | Hounsfield Unit |
| MRI | Magnetic Resonance Image |
| QUS | Quantitative Ultrasound |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| CEC-UV | Committee of Bioethics of Research in Human Beings of the University of Valparaíso |
| THA | Total Hip Arthroplasty |
| PAO | Periacetabular osteotomy |
| CFI | Canal Flare Index |
| CFR | Canal Fill Ratio |
| VBQ | Vertebral Bone Quality |
| EBQ | Endplate Bone Quality |
| UKR | Unicompartmental Knee Replacement |
| PROMs | Patient Reported Outcomes |
| LLIF | Lateral Lumbar Interbody Fusion |
| ACDF | Anterior Cervical Discectomy and Fusion |
| US | Ultrasound |
| 2D | Two-dimensional |
| AI | Artificial Intelligence |
| 3D | Three-dimensional |
| RFA | Resonance Frequency Analysis |
| FD | Fractal Dimensions |
| MCI | Mandibular Cortical Index |
| HR-pQCT | High Resolution Peripherical Quantitative Computed Tomography |
| QCT | Quantitative Computed Tomography |
| 3D MOI | three-dimensional mandibular osteoporosis index |
References
- Salari, N.; Ghasemi, H.; Mohammadi, L.; Behzadi, M.H.; Rabieenia, E.; Shohaimi, S.; Mohammadi, M. The global prevalence of osteoporosis in the world: a comprehensive systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research 2021, 16, 609. [Google Scholar] [CrossRef]
- Lewis, S.R.; Macey, R.; Parker, M.J.; Cook, J.A.; Griffin, X.L. Arthroplasties for hip fracture in adults. Cochrane Database of Systematic Reviews 2022, 2, CD013410. [Google Scholar] [CrossRef]
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis Prevention, Diagnosis, and Therapy. JAMA 2001, 285, 785–795. [CrossRef]
- Kanis, J.A.; Cooper, C.; Rizzoli, R.; Reginster, J.Y.; of the European Society for Clinical, S.A.B.; of Osteoporosis (ESCEO), E.A.; the Committees of Scientific Advisors.; of the International Osteoporosis Foundation (IOF), N.S. European guidance for the diagnosis and management of osteoporosis in postmenopausal women. Osteoporosis International 2019, 30, 3–44. [CrossRef]
- Blake, G.M.; Fogelman, I. An update on dual-energy x-ray absorptiometry. Seminars in Nuclear Medicine 2010, 40, 62–73. [Google Scholar] [CrossRef]
- Shepherd, J.A.; Ng, B.K.; Sommer, M.J.; Heymsfield, S.B. Body composition by DXA. Bone 2017, 104, 101–105. [Google Scholar] [CrossRef]
- Compston, J. Bone quality: what is it and how is it measured? Arquivos brasileiros de endocrinologia e metabologia 2006, 50, 579–585. [Google Scholar] [CrossRef]
- Bouxsein, M.L. Bone quality: where do we go from here? Osteoporosis International 2003, 14 Suppl 5, S118–S127. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporosis International 2006, 17, 1726–1733. [Google Scholar] [CrossRef] [PubMed]
- Cummings, S.R.; Melton, L.J. Epidemiology and outcomes of osteoporotic fractures. Lancet 2002, 359, 1761–1767. [Google Scholar] [CrossRef] [PubMed]
- Misch, C.E.; Qu, Z.; Bidez, M.W. Mechanical properties of trabecular bone in the human mandible: implications for dental implant treatment planning and surgical placement. Journal of Oral and Maxillofacial Surgery 1999, 57, 700–708. [Google Scholar] [CrossRef]
- Alsaadi, G.; Quirynen, M.; Komárek, A.; van Steenberghe, D. Impact of local and systemic factors on the incidence of late oral implant loss. Clinical Oral Implants Research 2008, 19, 670–676. [Google Scholar] [CrossRef]
- Dervis, E. Oral implications of osteoporosis. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 2005, 100, 349–356. [Google Scholar] [CrossRef]
- Okada, S.; Kawano, A.; Oue, H.; Takeda, Y.; Yokoi, M.; Koretake, K.; Tsuga, K. Preoperative evaluation of bone quality for dental implantation using an ultrasound axial transmission device in an ex vivo model. Clinical and Experimental Dental Research 2017, 3, 81–86. [Google Scholar] [CrossRef]
- Lemos, C.A.A.; de Oliveira, A.S.; Faé, D.S.; Oliveira, H.F.F.E.; Del Rei Daltro Rosa, C.D.; Bento, V.A.A.; Verri, F.R.; Pellizzer, E.P. Do dental implants placed in patients with osteoporosis have higher risks of failure and marginal bone loss compared to those in healthy patients? A systematic review with meta-analysis. Clinical Oral Investigations 2023, 27, 2483–2493. [Google Scholar] [CrossRef]
- Kanis, J.A. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: synopsis of a WHO report. WHO Study Group. Osteoporosis International 1994, 4, 368–381. A journal established as result of cooperation between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. [CrossRef]
- Wakimoto, M.; Matsumura, T.; Ueno, T.; Mizukawa, N.; Yanagi, Y.; Iida, S. Bone quality and quantity of the anterior maxillary trabecular bone in dental implant sites. Clinical Oral Implants Research 2012, 23, 1314–1319. [Google Scholar] [CrossRef]
- Hao, Y.; Zhao, W.; Wang, Y.; Yu, J.; Zou, D. Assessments of jaw bone density at implant sites using 3D cone-beam computed tomography. European Review for Medical and Pharmacological Sciences 2014, 18, 1398–1403. [Google Scholar]
- Parsa, A.; Ibrahim, N.; Hassan, B.; van der Stelt, P.; Wismeijer, D. Bone quality evaluation at dental implant site using multislice CT, micro-CT, and cone beam CT. Clinical Oral Implants Research 2015, 26, e1–e7. [Google Scholar] [CrossRef]
- Lekholm, U.; Zarb, G. Patient selection and preparation. In Tissue-integrated prostheses: osseointegration in clinical dentistry; P.-I. Branemark, G. A., Zarb, T.A., Eds.; Quintessence Publishing Co.: Chicago, 1985; pp. 199–209. [Google Scholar]
- Misch, C.E. Density of bone: effect on treatment plans, surgical approach, healing, and progressive bone loading. International Journal of Oral Implantology 1990, 6, 23–31. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Żarnowska, I.; Wilk, B.; Chilińska, M.; Kołodziejczyk, K.; Garlewicz, R.; Zlotorowicz, M. Bone Quality Assessment Before Total Hip Arthroplasty: The Role of Densitometry. Cureus 2024, 16, e55480. [Google Scholar] [CrossRef] [PubMed]
- Ries, C.; Boese, C.K.; Dietrich, F.; et al. Femoral stem subsidence in cementless total hip arthroplasty: a retrospective single-centre study. International Orthopaedics (SICOT) 2019, 43, 307–314. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Naylor, J.M.; Adie, S.; Liu, V.K.; Harris, I.A. Preoperative Factors and Patient-Reported Outcomes After Total Hip Arthroplasty: Multivariable Prediction Modeling. The Journal of Arthroplasty 2022, 37, 714–720.e4. [Google Scholar] [CrossRef]
- Isaksen, K.F.; Roscher, E.K.; Iversen, K.S.; Eitzen, I.; Clarke-Jenssen, J.; Nordsletten, L.; Madsen, J.E. Preoperative incipient osteoarthritis predicts failure after periacetabular osteotomy: 69 hips operated through the anterior intrapelvic approach. Hip International 2019, 29, 516–526. [Google Scholar] [CrossRef]
- Ishii, Y.; Noguchi, H.; Sato, J.; Takahashi, I.; Ishii, H.; Ishii, R.; Ishii, K.; Toyabe, S.I. Preoperative bone assessment by bone mineral density and bone turnover in patients undergoing total knee arthroplasty. Journal of Orthopaedics 2021, 28, 121–125. [Google Scholar] [CrossRef]
- Dyreborg, K.; Sørensen, M.S.; Flivik, G.; Solgaard, S.; Petersen, M.M. Preoperative BMD does not influence femoral stem subsidence of uncemented THA when the femoral T-score is > -2.5. Acta Orthopaedica 2021, 92, 538–543. [Google Scholar] [CrossRef]
- Rolvien, T.; Thiessen, M.L.; Boese, C.K.; Bechler, U.; Strahl, A.; Beil, F.T.; Ries, C. Areal bone mineral density is not associated with femoral stem subsidence in patients younger than 70 years undergoing total hip arthroplasty. Archives of Orthopaedic and Trauma Surgery 2024, 144, 1415–1422. [Google Scholar] [CrossRef]
- Nazari-Farsani, S.; Vuopio, M.; Löyttyniemi, E.; Aro, H.T. Contributing factors to the initial femoral stem migration in cementless total hip arthroplasty of postmenopausal women. Journal of Biomechanics 2021, 117, 110262. [Google Scholar] [CrossRef]
- Mohanty, S.S.; Vasavda, A.N.; Rai, A.K.; Rathod, T.N.; Kamble, P.; Keny, S. Short-Term Analysis of the Changes in the Bone Mineral Density of the Proximal Femur After Uncemented Total Hip Arthroplasty: A Prospective Study of 110 Patients. Cureus 2022, 14, e23257. [Google Scholar] [CrossRef] [PubMed]
- Bendtsen, M.A.F.; Odgaard, A.; Madsen, F.; Mosegaard, S.B.; Thomsen, J.S.; Hauge, E.M.; Søballe, K.; Stilling, M. Preoperative proximal tibial bone density, bone microarchitecture, and bone turnover are not associated with postoperative tibial component migration in cemented and cementless medial unicompartmental knee replacements: secondary analyses from a randomized controlled trial. Acta orthopaedica 2024, 95, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Sariali, E.; Gaujac, N.; Grimal, Q.; Klouche, S. Pre-operative bone mineral density is a predictive factor for excellent early patient-reported outcome measures in cementless total hip arthroplasty using a proximally fixed anatomic stem. A prospective study at two year minimum follow-up. International Orthopaedics 2020, 44, 2253–2259. [Google Scholar] [CrossRef]
- Ehresman, J.; Pennington, Z.; Schilling, A.; Lubelski, D.; Ahmed, A.K.; Cottrill, E.; Khan, M.; Sciubba, D.M. Novel MRI-based score for assessment of bone density in operative spine patients. The spine journal: official journal of the North American Spine Society 2020, 20, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Gong, Z.; Zheng, C.; Chen, Y.; Ma, X.; Wang, H.; Jiang, J. Preoperative Assessment of Bone Density Using MRI-Based Vertebral Bone Quality Score Modified for Patients Undergoing Cervical Spine Surgery. In Global Spine Journal; Advance online publication, 2022. [Google Scholar] [CrossRef]
- Jones, C.; Okano, I.; Arzani, A.; Dodo, Y.; Moser, M.; Reisener, M.J.; Chiapparelli, E.; Adl Amini, D.; Shue, J.; Sama, A.A.; et al. The predictive value of a novel site-specific MRI-based bone quality assessment, endplate bone quality (EBQ), for severe cage subsidence among patients undergoing standalone lateral lumbar interbody fusion. The spine journal: official journal of the North American Spine Society 2022, 22, 1875–1883. [Google Scholar] [CrossRef]
- Ran, L.; Xie, T.; Zhao, L.; Wang, C.; Luo, C.; Wu, D.; You, X.; Huang, S.; Zeng, J. MRI-based endplate bone quality score predicts cage subsidence following oblique lumbar interbody fusion. In The spine journal: official journal of the North American Spine Society; Advance online publication, 2024. [Google Scholar] [CrossRef]
- Tuo, Y.; Lin, K.; Yang, J.; Wang, S.; Abudouaini, H. Preoperative MRI-based endplate quality: a novel tool for predicting cage subsidence after anterior cervical spine surgery. Journal of Orthopaedic Surgery and Research 2024, 19, 245. [Google Scholar] [CrossRef]
- Nazari-Farsani, S.; Vuopio, M.E.; Aro, H.T. Bone Mineral Density and Cortical-Bone Thickness of the Distal Radius Predict Femoral Stem Subsidence in Postmenopausal Women. The Journal of Arthroplasty 2020, 35, 1877–1884.e1. [Google Scholar] [CrossRef]
- Staedt, H.; Rossa, M.; Lehmann, K.M.; Al-Nawas, B.; Kämmerer, P.W.; Heimes, D. Potential risk factors for early and late dental implant failure: a retrospective clinical study on 9080 implants. International Journal of Implant Dentistry 2020, 6, 81. [Google Scholar] [CrossRef]
- Lee, J.H.; Yun, J.H.; Kim, Y.T. Deep learning to assess bone quality from panoramic radiographs: the feasibility of clinical application through comparison with an implant surgeon and cone-beam computed tomography. Journal of Periodontal & Implant Science Advance online publication. 2024. [Google Scholar] [CrossRef]
- Issa, N.S.H.; Othman, T.A.; Sleman, B.M. A comparative radiographic study of bone density changes around titanium implants in the posterior mandible, preoperative, and postoperative. Annals of Medicine and Surgery 2024, 86, 3216–3221. [Google Scholar] [CrossRef]
- Rokn, A.; Rasouli Ghahroudi, A.A.; Daneshmonfared, M.; Menasheof, R.; Shamshiri, A.R. Tactile sense of the surgeon in determining bone density when placing dental implant. Implant Dentistry 2014, 23, 697–703. [Google Scholar] [CrossRef]
- Turkyilmaz, I.; McGlumphy, E.A. Is there a lower threshold value of bone density for early loading protocols of dental implants? Journal of Oral Rehabilitation 2008, 35, 775–781. [Google Scholar] [CrossRef]
- Takekawa, T.; Moroi, A.; Gomi, K.; Takayama, A.; Yoshizawa, K.; Ueki, K. Correlation Between Acquisition of Dental Implant Stability and Hounsfield Units at Dental Implant Placement. The Journal of oral implantology 2024, 50, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Coutant, J.C.; Seguela, V.; Hauret, L.; Caix, P.; Ella, B. Assessment of the correlation between implant stability and bone density by computed tomography and resonance frequency analysis in fresh cadavers. The International journal of oral maxillofacial implants 2014, 29, 1264–1270. [Google Scholar] [CrossRef] [PubMed]
- Arai, Y.; Tammisalo, E.; Iwai, K.; Hashimoto, K.; Shinoda, K. Development of a compact computed tomographic apparatus for dental use. Dento maxillo facial radiology 1999, 28, 245–248. [Google Scholar] [CrossRef]
- Mozzo, P.; Procacci, C.; Tacconi, A.; Martini, P.T.; Andreis, I.A. A new volumetric CT machine for dental imaging based on the cone-beam technique: preliminary results. European Radiology 1998, 8, 1558–1564. [Google Scholar] [CrossRef]
- Handelsman, M. Surgical guidelines for dental implant placement. British Dental Journal 2006, 201, 139–152. [Google Scholar] [CrossRef]
- Ye, Z.; Ye, H.; Wu, Y.; Jiang, Z.; Yao, H.; Xu, X.; Zhang, Y.; Du, W.; Li, W.; Zheng, Y.; et al. Effect of bone mass density and alveolar bone resorption on stress in implant restoration of free-end edentulous posterior mandible: Finite element analysis of double-factor sensitivity. Annals of Anatomy - Anatomischer Anzeiger 2024, 253, 152210. [Google Scholar] [CrossRef] [PubMed]
- Yuvashree, C.S.; Rajasekar, A. Prevalence and Association between Primary Stability and Bone Quality in Implants Placed in Edentulous Dental Arches: A Retrospective Analysis. Journal of Long-Term Effects of Medical Implants 2024, 34, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Wakankar, J.; Mangalekar, S.B.; Kamble, P.; Gorwade, N.; Vijapure, S.; Vhanmane, P. Comparative Evaluation of the Crestal Bone Level Around Pre- and Post-loaded Immediate Endoosseous Implants Using Cone-Beam Computed Tomography: A Clinico-Radiographic Study. Cureus 2023, 15, e34674. [Google Scholar] [CrossRef]
- Holahan, C.M.; Wiens, J.L.; Weaver, A.; Assad, D.; Koka, S. Relationship between systemic bone mineral density and local bone quality as effectors of dental implant survival. Clinical Implant Dentistry and Related Research 2011, 13, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Holahan, C.M.; Koka, S.; Kennel, K.A.; Weaver, A.L.; Assad, D.A.; Regennitter, F.J.; Kademani, D. Effect of osteoporotic status on the survival of titanium dental implants. The International Journal of Oral Maxillofacial Implants 2008, 23, 905–910. [Google Scholar]
- Noble, P.C.; Alexander, J.W.; Lindahl, L.J.; Yew, D.T.; Granberry, W.M.; Tullos, H.S. The anatomic basis of femoral component design. Clinical Orthopaedics and Related Research 1988, 148–165. [Google Scholar] [CrossRef]
- Aggarwal, D.A.; Goyal, D.R.; Gupta, D.J.; Khwaja, D.K.J. Comparative Analysis of Mandibular Cortical Index in Orthopantomogram and Bone Mineral Density in Dual Energy X-Ray Absorptiometry in Postmenopausal Females – A Radiological Study in North Indian Population; 2015. [Google Scholar]
- Esfahanizadeh, N.; Davaie, S.; Rokn, A.R.; Daneshparvar, H.R.; Bayat, N.; Khondi, N.; Ajvadi, S.; Ghandi, M. Correlation between bone mineral density of jaws and skeletal sites in an Iranian population using dual X-ray energy absorptiometry. Dental Research Journal 2013, 10, 460–466. [Google Scholar]
- Miliuniene, E.; Alekna, V.; Peciuliene, V.; Tamulaitiene, M.; Maneliene, R. Relationship between mandibular cortical bone height and bone mineral density of lumbar spine. Stomatologija 2008, 10, 72–75. [Google Scholar] [PubMed]
- Gulsahi, A.; Paksoy, C.S.; Ozden, S.; Kucuk, N.O.; Cebeci, A.R.I.; Genc, Y. Assessment of bone mineral density in the jaws and its relationship to radiomorphometric indices. Dentomaxillofacial Radiology 2010, 39, 284–289. [Google Scholar] [CrossRef]
- Güngör, E.; Yildirim, D.; Çevik, R. Evaluation of osteoporosis in jaw bones using cone beam CT and dual-energy X-ray absorptiometry. Journal of Oral Science 2016, 58, 185–194. [Google Scholar] [CrossRef]
- Shokri, A.; Ghanbari, M.; Hafez Maleki, F.; Ramezani, L.; Amini, P.; Tapak, L. Relationship of gray values in cone beam computed tomography and bone mineral density obtained by dual energy X-ray absorptiometry. Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology 2019. [Google Scholar] [CrossRef]
- Mostafa, R.A.; Arnout, E.A.; Abo El-Fotouh, M.M. Feasibility of cone beam computed tomography radiomorphometric analysis and fractal dimension in assessment of postmenopausal osteoporosis in correlation with dual X-ray absorptiometry. Dento maxillo facial radiology 2016, 45, 20160212. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.J.; Kim, K.A. Utility of the computed tomography indices on cone beam computed tomography images in the diagnosis of osteoporosis in women. Imaging Science in Dentistry 2011, 41, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Brasileiro, C.B.; Chalub, L.L.F.H.; Abreu, M.H.N.G.; Barreiros, I.D.; Amaral, T.M.P.; Kakehasi, A.M.; Mesquita, R.A. Use of cone beam computed tomography in identifying postmenopausal women with osteoporosis. Archives of Osteoporosis 2017, 12, 26. [Google Scholar] [CrossRef]
- Barngkgei, I.; Al Haffar, I.; Shaarani, E.; Khattab, R.; Mashlah, A. Assessment of jawbone trabecular bone structure amongst osteoporotic women by cone-beam computed tomography: the OSTEOSYR project. Journal of Investigative and Clinical Dentistry 2016, 7, 332–340. [Google Scholar] [CrossRef]
- Horner, K.; Devlin, H.; Alsop, C.W.; Hodgkinson, I.M.; Adams, J.E. Mandibular bone mineral density as a predictor of skeletal osteoporosis. The British Journal of Radiology 1996, 69, 1019–1025. [Google Scholar] [CrossRef]
- Drage, N.A.; Palmer, R.M.; Blake, G.; Wilson, R.; Crane, F.; Fogelman, I. A comparison of bone mineral density in the spine, hip and jaws of edentulous subjects. Clinical Oral Implants Research 2007, 18, 496–500. [Google Scholar] [CrossRef] [PubMed]
- Lindh, C.; Obrant, K.; Petersson, A. Maxillary bone mineral density and its relationship to the bone mineral density of the lumbar spine and hip. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 2004, 98, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Grisa, A.; Veitz-Keenan, A. Is osteoporosis a risk factor for implant survival or failure? Evidence-Based Dentistry 2018, 19, 51–52. [Google Scholar] [CrossRef]
- Becker, W.; Becker, B.E.; Alsuwyed, A.; Al-Mubarak, S. Long-term evaluation of 282 implants in maxillary and mandibular molar positions: a prospective study. Journal of periodontology 1999, 70, 896–901. [Google Scholar] [CrossRef] [PubMed]
- Rosa, C.; Bento, V.; Duarte, N.; Sayeg, J.; Santos, T.; Pellizzer, E. Do dental implants installed in different types of bone (I, II, III, IV) have different success rates? A systematic review and meta-analysis. The Saudi Dental Journal 2024, 36, 428–442. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.H.; Hsu, J.T.; Fuh, L.J.; Peng, S.L.; Huang, H.L.; Tsai, M.T. New classification for bone type at dental implant sites: a dental computed tomography study. BMC Oral Health 2023, 23, 324. [Google Scholar] [CrossRef]
- Pisulkar, S.G.; Mistry, R.A.; Nimonkar, S.; Dahihandekar, C.; Pisulkar, G.; Belkhode, V. The Correlation of Mineral Density of Jaws With Skeletal Bone and Its Effect on Implant Stability in Osteoporotic Patients: A Review of Patient-Based Studies. Cureus 2022, 14, e27481. [Google Scholar] [CrossRef]
- Castro, J.G.K.d.; Carvalho, B.F.; Melo, N.S.d.; Figueiredo, P.T.d.S.; Moreira-Mesquita, C.R.; Vasconcelos, K.d.F.; Jacobs, R.; Leite, A.F. A new cone-beam computed tomography-driven index for osteoporosis prediction. Clinical Oral Investigations 2020, 24, 3193–3202. [Google Scholar] [CrossRef]
- Selvakumar, R.; Chandran, A.; Patil, A.; Harini, T.C.; Dandekeri, S.; Verma, D.; Babu J, S.; Swarnalatha, C.; Nayyar, A.S. Osteoporosis risk group: Screening for osteoporosis in dental clinics using panoramic radiographs. Journal of Education and Health Promotion 2022, 11. [Google Scholar] [CrossRef]
- Whittier, D.E.; Burt, L.A.; Boyd, S.K. A new approach for quantifying localized bone loss by measuring void spaces. Bone 2021, 143, 115785. [Google Scholar] [CrossRef]
- Samelson, E.J.; Broe, K.E.; Xu, H.; Yang, L.; Boyd, S.; Biver, E.; Szulc, P.; Adachi, J.; Amin, S.; Atkinson, E.; et al. Cortical and trabecular bone microarchitecture as an independent predictor of incident fracture risk in older women and men in the Bone Microarchitecture International Consortium (BoMIC): a prospective study. The Lancet. Diabetes & Endocrinology 2019, 7, 34–43. [Google Scholar] [CrossRef]
- Löffler, M.T.; Jacob, A.; Valentinitsch, A.; Rienmüller, A.; Zimmer, C.; Ryang, Y.M.; Baum, T.; Kirschke, J.S. Improved prediction of incident vertebral fractures using opportunistic QCT compared to DXA. European radiology 2019, 29, 4980–4989. [Google Scholar] [CrossRef] [PubMed]
- Minonzio, J.G.; Ramiandrisoa, D.; Fernandez, S.; Chappard, C.; Cohen-Solal, M. Cortical bone parameters measured at the one-third distal radius obtained with axial transmission and HR-pQCT compared with anthropometric data in a representative population. Ultrasonics 2026, 159, 107829. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Comparative bone quality and density classification systems.
| Lekholm & Zarb (1985) - CBCT | Misch (1990) – CT | WHO (1994) - DXA |
|---|---|---|
| Type I: dense cortical bone | D1: ≥ 1250 HU | High BMD: T-score |
| Type II: dense cortical and trabecular bone | D2: 850–1250 HU | Normal: T-score |
| Type III: dense trabecular bone with a thin cortical layer | D3: 350–850 HU | Osteopenia: T-score |
| Type IV: sparse trabecular bone with a thin cortical layer | D4: 150–350 HU | Osteoporosis: T-score |
| – | D5: ≤ 150 HU | – |
Table 2.
Summary of preoperative bone assessment methods and clinical implications.
| Author (Year) | Site | Parameters | Key Clinical Findings |
|---|---|---|---|
| Skeletal Applications (Orthopedics & Spine) | |||
| 2D Radiographs | |||
| Żarnowska (2024) [23] | Hip | CI, CC ratio | Indices correlate with femoral neck diameter and cortical thickness. |
| Noble (1988) [55] | Hip | Canal Flare Index | CFI decreases with age; requires specific proximally wider stems. |
| Aggarwal (2022) [56] | Hip | KL Grade (OA) | Lower radiographic OA severity predicts worse post-THA outcomes. |
| Isaksen (2019) [26] | Hip (PAO) | Tönnis Classif. | Incipient OA is the main predictor for poor joint survival after PAO. |
| Ries (2019) [24] | Hip | CFI, CFR | Collarless stems show higher subsidence; morphometry is not primary risk. |
| DXA | |||
| Dyreborg (2021) [28] | Hip | T-score () | Pre-op BMD does not predict migration in patients ≤ 75y. |
| Rolvien (2024) [29] | Hip | aBMD by DXA | No significant association between BMD and subsidence in young patients. |
| Mohanty (2022) [31] | Hip | Periprosthet. BMD | Low pre-op BMD increases post-op loss in Gruen zone 7. |
| Ishii (2021) [27] | Knee | T-score, Turnover | High occult osteoporosis in TKA; screening is mandatory. |
| QCT | |||
| Sariali (2020) [33] | Hip | CT-derived BMD | Cancellous BMD predicts early PROMs in cementless THA. |
| MRI | |||
| Ehresman (2020) [34] | Spine | VBQ (MRI) | Novel score differentiates bone quality; correlates with T-score. |
| Ran (2024) [37] | Spine | EBQ (MRI) | High EBQ scores indicate increased risk of cage subsidence post-OLIF. |
| QUS | |||
| Nazari-Farsani (2020) [39] | Hip/Radius | Cortical thickness | QUS of distal radius predicts femoral stem subsidence risk. |
| Maxillofacial Applications (Dentistry) | |||
| 2D Radiographs | |||
| Lee (2024) [41] | Maxilla/Mand. | AI / Panoramic | DL matches CBCT accuracy for bone quality categorization. |
| Issa (2024) [42] | Mandible | 2D Density | Normal healing shows density drop at 1mo, then steady increase. |
| CT | |||
| Takekawa (2024) [45] | Maxilla/Mand. | HU at site | CT-HU values correlate with RFA stability and healing. |
| Rokn (2014) [43] | Maxilla/Mand. | HU vs. Tactile | Strong correlation (0.61) between HU and surgeon’s tactile sense. |
| Turkyilmaz (2008) [44] | Maxilla/Mand. | HU threshold | Threshold of HU proposed for safe early loading. |
| CBCT | |||
| Yuvashree (2024) [51] | Maxilla/Mand. | CBCT / Stability | D2 density significantly associated with stability of 30–40 Ncm. |
| Wakankar (2023) [52] | Maxilla/Mand. | Crestal bone | CBCT is superior to 2D RX for monitoring immediate implant healing. |
| DXA | |||
| Holahan (2008) [54] | Maxilla/Mand. | DXA T-score | Osteoporosis/osteopenia is not a contraindication for implants. |
Note: Comparison indicates the skeletal and maxillofacial sites correlated; Parameters refers to the diagnostic tools used. Abbreviations: BMD: bone mineral density; CBCT: cone beam computed tomography; CTCI: CT cortical index; CTI: CT index; CTMI: CT mental index; DXA: dual-energy X-ray absorptiometry; FD: fractal dimension; GV: gray values; MCI: mandibular cortical index; SPA: single-photon absorptiometry.
Table 3.
Summary of studies correlating skeletal and maxillofacial bone mineral density.
| Author (Year) | Comparison | Parameters | Key Correlation Findings |
|---|---|---|---|
| Horner (1996) [66] | Mandible vs. Spine/Femur | DXA (Mandible, Spine, Femur) | Mandible body BMD is an appropriate predictor of general bone mass. |
| Drage (2007) [67] | Jaws vs. Spine/Hip | DXA (L-spine, Hip, Jaws) | Hip/Spine BMD cannot predict maxillary density; good correlation with ramus. |
| Esfahanizadeh (2013) [57] | Jaws vs. Spine/Femur | DXA T-scores | Significant correlation between skeletal and jaw bone densities. |
| Lindh (2004) [68] | Maxilla vs. Spine/Hip | DXA (Skeletal), CT HU (Maxilla) | Anterior maxilla BMD significantly correlates with lumbar spine BMD. |
| Gulsahi (2010) [59] | Jaws vs. Femur | DXA (Femur, Jaws), Pan. indices | No significant correlation found between jaw BMD and femoral BMD or indices. |
| Miliuniene (2008) [58] | Mandible vs. Spine | DXA (L2-L4), Pan. indices (CI, GI) | Mandibular cortical height correlates with lumbar BMD; predictive of osteoporosis. |
| Aggarwal (2015) [56] | Mandible vs. Spine | Pan. MCI, DXA BMD (Lumbar) | Significant MCI-lumbar BMD correlation; panoramic RX is a viable screening tool. |
| Shokri (2019) [61] | Jaws vs. Neck/Spine | CBCT Gray Values, DXA BMD | Maxilla Gray Values correlate with BMD; GV < 298 screens for osteoporosis. |
| Gungor (2016) [60] | Jaws vs. Neck/Spine | CBCT indices (CTMI, CTI), DXA | Spine BMD correlates with mandibular CT and histogram analysis values. |
| Mostafa (2016) [62] | Mandible vs. Spine | CBCT indices (CTMI, CTI, FD), DXA | CBCT radiomorphometric indices serve as useful adjuvant screening tools. |
| Brasileiro (2017) [64] | Mandible vs. Neck/Spine | CBCT indices (CTMI, CTI), DXA | Quantitative CBCT indices identify postmenopausal women with low BMD. |
| Koh (2011) [63] | Mandible vs. Neck/Spine | CBCT indices (CTI, CTCI), DXA | CBCT indices (CTI, CTCI) differentiate normal vs. osteoporotic women. |
| Barngkgei (2016) [65] | Mandible vs. Neck/Spine | CBCT histomorpho., DXA | Specific trabecular analysis via CBCT may aid in opportunistic screening. |
Note: Comparison indicates the skeletal and maxillofacial sites correlated; Parameters refers to the diagnostic tools used. Abbreviations: BMD: bone mineral density; CBCT: cone beam computed tomography; CTCI: CT cortical index; CTI: CT index; CTMI: CT mental index; DXA: dual-energy X-ray absorptiometry; FD: fractal dimension; GV: gray values; MCI: mandibular cortical index; SPA: single-photon absorptiometry.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



