Submitted:
30 January 2026
Posted:
03 February 2026
You are already at the latest version
Abstract
Seismic resilience of healthcare facilities in earthquake-prone regions is often con-strained by spatial inefficiencies, complex evacuation behaviors, and limited accessi-bility for vulnerable populations. This study develops an AI-enhanced framework to evaluate and improve the seismic evacuation performance of hospital campus by in-tegrating field surveys, GIS spatial data, and hospital BIM layouts. Using a hospital redevelopment project in the Liangshan Yi Autonomous Prefecture of China as a case study, a high-fidelity hospital digital twin is constructed and coupled with an agent-based model to simulate heterogeneous evacuation behaviors under earth-quake-induced emergency scenarios. A Q-learning-based evacuation strategy is benchmarked against a random walk baseline. The results demonstrate statistically significant improvements, with mean evacuation time reduced by 40.9% and the 90th-percentile evacuation time reduced by 58.6%. In addition, the AI-driven strategy reduces performance disparities between medical staff and vulnerable patients, indi-cating improved evacuation equity. The proposed digital twin framework further en-ables scenario-based evaluation of spatial layouts and operational strategies prior to implementation. Overall, this study provides a performance-based approach for en-hancing evacuation safety and functional seismic resilience of healthcare facilities in underserved regions.
Keywords:
seismic resilience
; hospital evacuation
; healthcare facilities
; digital twin
; agent-based modeling
; earthquake-prone regions
; underserved regions
1. Introduction
1.1. Research Background and Motivation
Health is widely recognized as a the cornerstone of human development and socioeconomic progress. Reflecting this imperative, the Chinese government issued the Healthy China 2030 Planning Outline [1],, reaffirming its commitment to global health governance and alignment with the United Nations Sustainable Development Goals (SDGs) [2]. Achieving these objectives requires not only expanded healthcare provision but also systemic improvements in the safety, resilience, and functional reliability of healthcare infrastructure. In disaster-prone contexts, particularly in seismically active regions, the capacity of healthcare facilities to maintain operational continuity and protect vulnerable populations under extreme events has become a critical determinant of public health outcomes. Consequently, advancing seismic-resilient, inclusive, and human-centered hospital design has emerged as a pressing priority at the intersection of health policy, building performance, and risk governance.
Within this evolving landscape, two complementary paradigms have emerged as critical to next-generation hospital design in earthquake-prone regions. First, evidence-based therapeutic landscape design has demonstrated measurable benefits for mental well-being and physiological recovery through exposure to natural environments [3]. While traditionally associated with healing and patient experience, such spatial qualities also influence movement patterns, wayfinding clarity, and crowd behavior under emergency conditions.Second, recognizing hospitals as critical lifeline infrastructure necessitates the adoption of high-resilience design principles to ensure functional continuity during and after extreme events [4,5]. In seismically active contexts, the capacity for rapid emergency evacuation and effective patient dispersal becomes a decisive determinant of survival outcomes. Post-event investigations following the 1994 Northridge earthquake revealed that even moderate seismic damage—particularly to non-structural components—can force full-scale hospital evacuation, with timely and well-organized evacuation proving essential to minimizing secondary injuries and prolonged service disruption [6,7].Despite their shared relevance to hospital performance under seismic stress, these paradigms have largely evolved in parallel. Effectively integrating therapeutic spatial design with resilience-oriented evacuation planning, especially in resource-constrained and culturally diverse settings, remains an underexplored challenge. Southwest China, characterized by high seismic risk alongside pronounced ethnic and linguistic heterogeneity, represents a critical context in which AI-driven spatial simulation and intelligent digital systems can enhance both emergency preparedness and equitable healthcare delivery. This study therefore addresses the following research question: How can AI-based spatial simulation and multilingual metaverse platforms be synergistically integrated into hospital campus design in earthquake-prone regions to strengthen seismic evacuation preparedness while supporting human-centered spatial quality in underserved, multi-ethnic contexts?
1.2. Research Gaps
1.2.1. Therapeutic Landscapes in Multicultural Contexts
A substantial body of empirical research corroborates the efficacy of therapeutic landscapes in accelerating patient convalescence and mitigating staff burnout [8]. However, empirical research and theoretical synthesis regarding therapeutic landscape development within the multicultural context of Southwest China remain remarkably limited. Investigating how to organically integrate high-quality healing environments into healthcare institutions serving ethnically diverse populations, while concurrently leveraging emerging digital technologies to narrow regional disparities, represents a topic of considerable research value and practical urgency.
1.2.2. AI-Driven Evacuation Modeling and Agent-Based Simulation
Recent advances in AI and ABM have demonstrated significant potential for hospital design optimization. Agent-based frameworks effectively model real-time crowd behaviors during emergencies, enabling designers to identify congestion hotspots and optimize evacuation routes in complex healthcare settings [9]. AI-driven digital twins, integrating reinforcement learning algorithms such as Q-learning, facilitate the iterative evolution of virtual hospital environments, combining immersive simulations with data-informed infrastructure adaptation [10].
Despite recent advances, several critical gaps remain in the literature:
(1) Behavioral Heterogeneity: Current evacuation models often assume homogeneous agent populations, neglecting role-specific behaviors (e.g., patients with mobility limitations vs. medical staff under time-critical tasks) and their emergent interactions during crises [11,12].
(2) Algorithmic Transparency and Comparison: While RL-based methods show potential, empirical comparisons between advanced algorithms (e.g., Q-learning) and baseline models (e.g., stochastic random walk) in hospital-specific contexts remain insufficient, limiting evidence-based adoption [13,14].
(3) Spatial Contextualization: Most existing studies focus on generic building typologies, often overlooking the unique spatial complexities inherent to healthcare facilities. In particular, limited systematic attention has been given to exterior evacuation spaces in hospital settings, such as outdoor plazas, entrances, and circulation areas, despite their critical role in organizing crowd dispersion, reducing congestion, and ensuring operational efficiency during emergency evacuations [15,16].
1.2.3. Multilingual Metaverse for Inclusive Healthcare
Metaverse platforms enhanced by multimodal Large Language Models (LLMs) can theoretically overcome linguistic barriers through real time translation, which fosters equitable care delivery and improved patient provider interaction [17]. However, the actual implementation of these technologies in underrepresented and linguistically diverse regions remains embryonic. Current systems rarely address the dual challenges of culturally adaptive content representation and real time emergency communication in multilingual contexts [18], which consequently exacerbates health inequities in minority communities.
These limitations collectively underscore the need for an integrated and evidence- based framework that bridges therapeutic landscape theory, intelligent evacuation modeling, and inclusive digital service design specifically tailored to the socio spatial realities of underserved hospital settings.
1.3. Research Objectives and Contributions
To address the aforementioned gaps, this study investigates Puge County People's Hospital (普格县人民医院) in Sichuan Province as a representative case study. Situated in the Liangshan Yi Autonomous Prefecture of Southwest China, this facility serves an ethnically diverse population, predominantly comprising the Yi minority, within a region characterized by limited healthcare resources, geographic isolation, and constrained digital infrastructure [19]. Consequently, the hospital embodies the critical need for resilient, intelligent, and culturally adaptive healthcare environments in underserved areas facing significant resource and digital access disparities.
This research aims to:
- Develop and validate an AI driven agent based evacuation simulation framework that accounts for role based behavioral heterogeneity among doctors, nurses, and patients, and systematically compares the performance of a Q learning based strategy with a knowledge biased stochastic walk baseline under earthquake induced emergency scenarios.
- Design and prototype a multilingual Medical Metaverse interface that supports inclusive and barrier free interaction for linguistically diverse users across both virtual and physical healthcare environments, with a particular focus on accessibility for elderly and ethnic minority populations.
- Integrate evacuation modeling and digital interface design within a holistic evidence based framework that connects therapeutic landscape principles, emergency preparedness, and digital health innovation, thereby informing resilient hospital planning and improving building level seismic resilience.
Principal Contributions:
- Methodological innovation in evacuation simulation.This study develops a comparative agent based evacuation modeling framework that employs a Q learning based strategy and a knowledge biased stochastic walk baseline to simulate heterogeneous crowd behaviors during hospital evacuation scenarios. Through quantitative analysis of evacuation trajectories, flow patterns, and performance indicators including distance time relationships and T50 and T90 metrics, the framework provides empirical evidence on how algorithm supported strategies can improve evacuation efficiency and consistency in healthcare specific spatial environments under emergency conditions.
- Prototype development of a multilingual digital interface for healthcare accessibility.A proof of concept Medical Metaverse platform is introduced to support multilingual interaction and inclusive access to healthcare information. By integrating a bilingual digital human interface that supports Mandarin Chinese, the Yi language, and English, the system demonstrates the technical feasibility of reducing linguistic and cognitive barriers in minority serving hospitals. The prototype highlights the potential role of culturally adaptive digital interfaces in improving communication, wayfinding, and preparedness in both routine and emergency contexts.
- Holistic integration into evidence based hospital design.The study synthesizes therapeutic landscape principles, AI driven spatial evaluation, and inclusive digital service design into a unified framework for hospital planning in resource constrained and culturally diverse regions. By bridging architectural design, computational modeling, and healthcare operations, the proposed framework supports building level seismic resilience and emergency preparedness while offering practical insights for policy and practice in underserved regions.
2. Theoretical Background
2.1. Therapeutic Landscapes and Evidence-Based Design
The concept of therapeutic landscapes, first articulated by Gesler (1992), frames healing not merely as a medical outcome but as a dynamic process emerging from the complex interplay of physical settings, social relations, and symbolic meanings [20]. These theoretical underpinnings, including the Biophilia Hypothesis and Stress Reduction Theory, have evolved into spatial imperatives defined by sense of control, social support, and positive distractions [21]. In contemporary healthcare architecture, these theoretical underpinnings have evolved into Evidence-Based Design (EBD) protocols. These protocols advocate for the rigorous use of credible data to influence design decisions [22]. Historically, EBD relied on post-occupancy evaluations, but recent advancements in the post-pandemic era have fundamentally shifted this paradigm.
Central to this evolution is the increasing use of objective biometric data to quantify human responses to environmental design. Recent meta-analyses across diverse natural settings have demonstrated that such interventions are associated with measurable improvements in autonomic nervous system indicators (e.g., RMSSD and SDNN) and EEG patterns, providing robust empirical evidence for the psycho-physiological benefits of nature [23]. Seminal research in hospital settings has demonstrated that biophilic-informed environmental interventions, particularly access to natural views, are associated with reduced analgesic consumption and shorter lengths of stay [24]. These findings have been further validated by recent systematic reviews that correlate green views and natural daylight with reduced pain medication use, shorter hospitalization, and improved patient-reported outcomes [8].
However, a critical implementation gap persists. Despite this wealth of data, traditional design processes remain predominantly manual and static. Architects often apply these findings as broad, qualitative guidelines, failing to address the intricate functional trade-offs inherent in modern healthcare facilities. In these high-stakes environments, the conflict between strict clinical requirements (such as sterility and operational efficiency) and the integration of restorative nature is acute. Recent scholarship suggests that without computational optimization and AI-driven simulation, it is nearly impossible to balance these multi-objective constraints effectively [25,26]. This necessitates a transition from intuitive design to algorithmic precision.
2.2. Medical Metaverse and Digital Twins
Healthcare is undergoing a revolutionary transformation through the emergence of the medical metaverse, which functions as an immersive digital ecosystem that transcends the physical-virtual divide [17]. Underpinned by the convergence of extended reality, artificial intelligence, and digital twins, this realm enables providers and patients to interact seamlessly in real time [27]. At the core of this transformation are digital twins, which serve as dynamic virtual counterparts of physical systems that are continually synchronized with real-world data to provide predictive insights [28,29]. Functioning across multiple scales from individual organs to entire hospital operational flows, these systems integrate real-time streams from IoT sensors, wearable devices, and electronic health records. Within this framework, AI algorithms leverage extensive multi-modal datasets to simulate disease trajectories, forecast therapeutic responses, and generate predictive insights with high precision. This bidirectional data exchange allows continuous refinement, enabling the digital model to evolve in lockstep with the patient’s changing physiological state [30,31]. This synergy between DTs and AI unlocks a broad spectrum of opportunities. At the clinical level, key applications include in silico clinical trial design, drug discovery, patient-specific therapies, and precision surgical planning [32]. At the organizational level, DTs are increasingly utilized for the holistic management of hospital infrastructure, including capacity planning, resource allocation, and the optimization of indoor and outdoor environmental quality [33].
However, a critical disparity persists because digital twins are primarily applied to clinical workflows, which leaves their integration into therapeutic landscape planning largely unexplored [34,35]. There is an urgent need to expand the digital twin paradigm into a versatile platform that orchestrates the restorative potential of hospital gardens through simulations powered by artificial intelligence.
2.3. Agent-Based Modeling for Human Behavior Simulation
Human behavior is inherently heterogeneous and nonlinear, which creates challenges for aggregate, top-down modeling approaches. Agent-Based Modeling (ABM) addresses these limitations by simulating autonomous agents that interact through local decision rules to generate complex macro-level patterns through emergence [36]. While traditionally applied in sociology, ABM is now particularly valuable in spatial research for simulating evacuation procedures and crowd dynamics [37]. A transformative development in this field is the integration of Large Language Models (LLMs) into agent architectures. Unlike traditional agents driven by rigid heuristic rules, LLM-empowered agents possess cognitive capabilities such as memory retention and nuanced responses to environmental stimuli, which significantly enhances the ecological validity of simulations for sensitive healthcare scenarios [38]. Nevertheless, ABMs primarily function as evaluative tools rather than generative ones, which necessitates rigorous validation protocols and points to the need for integrating simulation with optimization algorithms like Reinforcement Learning to bridge the gap between behavioral analysis and spatial generation [39].
Nevertheless, ABMs face persistent challenges, including high data requirements for calibration, computational costs, and the difficulty of empirically grounding stochastic agent behaviors [40,41]. Furthermore, in design-oriented applications, ABM primarily functions as evaluative rather than optimization-oriented tools [42,43]. While it can effectively predict how a given hospital layout may perform in terms of patient flow or infection risk, it cannot inherently generate improved design alternatives. This limitation necessitates rigorous validation protocols and points to the need for integrating ABM with learning-based optimization methods, such as Reinforcement Learning, to close the loop between behavioral simulation and spatial optimization.
2.4. Reinforcement Learning and Spatial Optimization
Reinforcement Learning (RL) has emerged as a powerful computational paradigm for addressing complex spatial optimization problems, particularly those involving sequential decision-making within dynamic urban or built environments [44,45,46]. Due to the computational complexity of exact algorithms and the uncertain solution quality of heuristic methods, which often struggle with the high dimensionality and combinatorial structure of real-world spatial planning, RL offers a learning-based alternative that automates the discovery of adaptive strategies through iterative interaction [47,48,49]. By framing spatial tasks as a Markov Decision Process (MDP), an autonomous agent learns to map environmental states, such as facility distribution and network connectivity, to optimal actions, including resource allocation and layout modification, by maximizing a cumulative reward signal [47,50,51].This learning-based approach represents a paradigm shift in tackling intractable resource-allocation dilemmas. Recent integrations of Deep Reinforcement Learning (DRL) with Graph Neural Networks (GNNs) have substantially enhanced the capacity to model complex spatial dependencies, scaling effectively to solve Vehicle Routing Problems (VRP) and Facility Location Problems (FLP) [52,53,54,55]. Empirical evidence demonstrates that DRL methods frequently outperform commercial solvers in both computational speed and solution quality, laying a robust foundation for intelligent, adaptive urban planning [56,57,58]. Furthermore, while advanced DRL tackles high-dimensional environments, classical model-free methods like Q-learning remain highly effective for specific real-time allocation tasks, such as adaptive traffic signal control, emergency logistics and fire evacuation [59,60,61,62,63].
However, despite these methodological advancements [64,65,66,67,68], a critical research gap persists. Existing literature is predominantly confined to optimizing operational efficiency and logistics, which rely on metrics that are easily quantifiable, such as travel time, throughput, or coverage [64,69]. In contrast, the potential of RL to address complex spatial configuration and therapeutic design, tasks that require balancing ecological sustainability, psychological restoration, and accessibility, remains largely unexplored. Current frameworks often struggle to encode the nuanced and human-centric qualities of a healing environment into a computable reward function. Consequently, there is an urgent need to develop novel RL architectures that can bridge the divide between algorithmic precision and the qualitative demands of restorative environments.
3. Materials and Methods
3.1. Research Framework and Process
The research establishes a robust and systematic methodological framework for designing resilient and intelligent landscapes for healthcare facilities (Figure 1).
(1) Geospatial and Architectural Data Acquisition. This phase includes high-precision topographical mapping, administrative boundary delineation, and detailed site documentation.
(2) Spatial and Behavioral Analysis. This stage integrates GIS/BIM-based spatial analytics with Agent-Based Modeling (ABM) to quantitatively evaluate human behavioral patterns and evacuation dynamics.
(3) Integrated Implementation. In the final phase, digital-twin environments are developed for advanced spatial simulation, through which the physical built environment is optimized to enhance wayfinding, safety, and overall environmental resilience.
The data preprocessing workflow, encompassing visualization, georeferencing, and conversion into GeoJSON and TIFF formats, was executed within the Arcgis Pro 3.2. To ensure spatial consistency and preserve metric accuracy, all datasets were standardized to the WGS 84 / UTM Zone 48N (EPSG:32648) coordinate reference system (CRS). Human behavior simulation, algorithm testing, and result visualization were subsequently carried out in MATLAB R2024b. High-precision architectural and topographical CAD survey data provided by the hospital were used to build a detailed 3D model in Autodesk 3ds Max 2020, the final interactive simulation environment was deployed in Unity (version 2022.3.44f1c1, LTS), enabling real-time rendering and user interaction.
As illustrated in Figure 1, the framework comprises three phases: (1) Geospatial and Architectural Data Ac-quisition as well as site survey; (2) Analytical Core, utilizing GIS/BIM, Agent-based Models, (3) Integrated Unity for spatial analysis and simulation, developing digital twin hospitals to inform physical environment improvements. Evacuation simulations were performed using Q-learning and random walk. Q-learning, an iterative reinforcement learning technique, optimized exit selection by learning from simulated experiences, while the random walk algorithm simulated non-directed movement, serving as a comparative baseline.
To our knowledge, this study represents one of the earliest systematic applications of digital twin modeling in conjunction with ML-based behavioral prediction in therapeutic landscape planning. The proposed framework offers a replicable and data-informed pathway for designing resilient, culturally embedded, and health-supportive therapeutic environments.
3.2. Site Selection, Context and Date Source
3.2.1. Site Selection
As shown in Figure 2, The People’s Hospital of Puge County is located in the Liangshan Yi Autonomous Prefecture of Sichuan Province, Southwest China. Established in 1952, it has undergone continuous expansion and modernization, and was accredited as a Grade II, Class A general hospital in 2017 [70]. The hospital sits at an elevation of approximately 1,430 meters in Puji Town, south of the county’s urban center, on a gently sloping mid-mountain site. The terrain includes an internal elevation difference of about 3.5 meters, which offers open scenic views but also presents challenges for construction design, drainage organization, and emergency accessibility. The hospital campus occupies approximately 13,800 m², and its green coverage of about 6% adds to the challenges of spatial planning and ecological restoration.
The hospital specializes in obstetrics and gynecology, pediatrics, and traditional Chinese medicine rehabilitation, providing comprehensive services for common, critical, and complex conditions. In 2024, it treated 85,066 patients, an increase of 3.78% from the previous year, and currently serves approximately 218,800 residents, 85.6% of whom are Yi ethnic minority. This demographic profile underscores the necessity of inclusive, multilingual, and culturally responsive healthcare provision (Figure 2).
3.2.2. Cultural Context
The Yi people adhere to an animistic worldview in which all elements of nature are regarded as living entities that are closely intertwined with human existence in a relationship of mutual dependence and shared vitality [71,72]. Within Liangshan Yi cosmology, red, yellow, and black are regarded as the primordial colors of the cosmos, encoding the Yi people’s understanding of origin, vitality, and ancestral homeland [73,74]. The red derives from reverence for fire and symbolizes warmth and life force; yellow represents the sun as the generative source of all things; and black signifies the fertile earth and surrounding mountains, reflecting ancestral homeland and survival. These color meanings are embodied across clothing, artifacts, festivals, and spatial forms, where they articulate a worldview that values harmony among nature, community, and living beings.
Grounded in this animistic cosmology and tri-color symbolism, Yi cultural expressions flow naturally from visual aesthetics to spatial and embodied practices, most vividly manifested in communal dance rituals. As illustrated in Figure 3, The cultural–spatial logic of the Yi Duoluohe circular dance is not merely decorative, but functions as a behavioral and psychosocial mechanism supported by empirical evidence (Figure 3). Contemporary research demonstrates that synchronized collective movement strengthens social bonding, emotional attunement, and psychological resilience [75,76]. Drawing on Durkheim’s notion of collective effervescence [77] and Collins’s interaction ritual theory [78], these shared rhythmic practices generate collective emotional energy and a sense of belonging. In this context, designing therapeutic landscapes that facilitate communal gathering and reflect local cultural meanings can further promote place attachment, social cohesion, and psychological resilience.
3.2.3. Data Selection
The process begins with comprehensive data preparation, including on-site field surveys, UAV photogrammetry, and the integration of multi-source geospatial and institutional datasets obtained from official repositories and the Puge County People’s Hospital. Regional topographic data was derived from the ASTER GDEM v3 dataset [79], and administrative boundary data was sourced from the Alibaba Cloud DataV Atlas platform [80]. The virtual environment was then populated with 3D elements such as human avatars, vegetation, and contextual objects from professional model libraries [81,82]. The dataset was further enriched with UAV imagery, door access control logs, ward surveillance footage, and on-site photographic documentation to support validation of behavioral interactions among doctors, nurses, and patients. These heterogeneous spatial and behavioral datasets collectively enabled the construction of a multimodal digital environment for simulation and decision analysis. Administrative boundary and basemap data were downloaded from the Alibaba Cloud DataV Geo Atlas platform. The original geospatial data are provided by Amap (AutoNavi), with a dataset release date of May 2021 [83].
3.3. Evidence-Based Design
Weaving Culture, Health, and Land, this study proposes a digital twin–integrated evidence-based design (EBD) framework that connects empirically observed challenges in therapeutic landscape environments with practical spatial and operational interventions. Evidence-Based Design (EBD) is a systematic approach that applies the best available research and practice-based evidence, in collaboration with clients, to guide critical design decisions throughout a project’s lifecycle [84,85]. EBD enhances the scientific rigor of healthcare facility planning while upholding the Hippocratic ethical principle of benefiting patients and avoiding harm [86]. As illustrated in Figure 4, the EBD framework is conceptualized as a multi-layered systemic model. The Sankey diagram visualizes the complex many-to-many relationships among five core components. The flow begins with Problem Domains (the 'why'), which are linked to corresponding Impact Pathways (the 'how'). These pathways are subsequently connected to Enabling Technologies (the 'tools') that support the formulation of specific Intervention Strategies (the 'actions'). The framework ultimately converges on a set of desired Outcomes (the 'goals'), providing a coherent visual logic for translating empirical problem diagnosis into targeted, evidence-based design solutions.
3.4. Behavioral Simulation Framework
The simulation environment is constructed based on real-world geospatial data to ensure the fidelity of the evacuation scenarios. We utilized a GeoTIFF basemap representing a complex urban layout and a GeoJSON file (walkable.geojson) to define the specific walkable boundaries and obstacle zones. The environment features multiple architectural barriers and narrow passages, creating a challenging setting for evacuation. This geospatial foundation allows for a precise mapping of the physical constraints that influence agent behaviors.
3.4.1. Spatial Dynamics and Role Heterogeneity
The simulation initializes a population of agents, categorized into three distinct roles: Doctors (), Nurses (), and Patients ().This classification reflects the social hierarchy typical of a healthcare environment. Each agent i is defined by a state vector:
where:
denotes the position vector of agent in the continuous 2D space;
represents the instantaneous velocity vector.
in [0,1] is the scalar Exit Knowledge Parameter, reflecting the agent's cognitive awareness of evacuation routes.
denotes the discrete behavioral state (e.g., Normal, Panic, Helping).
To capture the stochastic nature of human psychology during emergencies, the model incorporates a set of dynamic behavioral rules. The behavioral state of agent at the next time step is determined by the following conditional transition logic, with threshold parameters calibrated based on pedestrian dynamics literature [37,87]:
where:
is the local crowd density around agent . The critical threshold is set to . This critical threshold corresponds to the onset of severe congestion and turbulence.
is a uniform random variable representing uncertainty.
is the Panic Probability, determining the susceptibility of an agent to enter a disorganized state under high density.
is the Helping Probability, reflecting the high deontological commitment of doctors to stabilize panicked neighbors ().
represents the set of neighboring agents within the interaction radius ( units).
Helping State: When encountering a panicked patient within the interaction range, they transition to this state with a probability of , a value derived from the observed ratio of active responders in emergency drills [9,88].
Guiding State: Nurses actively influence the trajectory of nearby patients, creating a cohesive "flocking" behavior that mitigates entropy.
3.4.2. Baseline Model: Knowledge-Biased Stochastic Walk
As a baseline for comparison, we formulated a Knowledge-Biased Stochastic Walk algorithm. Unlike a pure random walk (Brownian motion), this model assumes that agents possess varying degrees of spatial cognition regarding exit locations. The movement direction for agent at time is modeled as:
where:
is the normalized unit vector pointing from the agent's current position towards the nearest exit centroid, representing the conscious intention to evacuate.
is a Gaussian random vector representing environmental uncertainty or panic-induced erratic movement.
is the weighting coefficient derived from the agent's role (Table 1) and dynamically updated through social interactions (e.g., nurse guidance). This parameter creates a spectrum of behaviors: Patients (low ) exhibit high-entropy search patterns, while Doctors (high ) follow near-deterministic paths.
denotes the vector normalization operation.
3.4.3. Advanced Model: Q-Learning Enhanced Navigation
To overcome the limitations of the heuristic baseline, we implemented a Reinforcement Learning (RL) model using the Q-learning algorithm. This approach allows agents to autonomously learn optimal evacuation strategies through trial-and-error, without relying on hard-coded knowledge parameters ().
State Space and Action Space. The continuous hospital environment is discretized into a state space , defined as:
Here, represents the agent's grid coordinates, denotes the discretized distance to the nearest exit, and encodes local obstacle configurations. The agent selects actions from 8 cardinal directions (Moore neighborhood). The Q-value is iteratively updated via the Bellman equation:
where is the learning rate and is the discount factor, balancing immediate and future rewards.
Area-Weighted Reward Function. To simulate the realistic preference for main entrances, we designed a novel reward function that incorporates exit capacity:
where is the completion reward, is the weighting factor, and is the normalized area of the reached exit. This incentivizes agents to learn paths towards larger, more visible exits (e.g., Exit #1) rather than merely the closest ones, thereby optimizing global evacuation flow.
Training and Testing Protocols. The model underwent training for 500 episodes, a duration sufficient to achieve stable convergence as validated in Figure 5. During the training phase, we employed an -greedy strategy, where the exploration probability was initialized at 1.0 and exponentially decayed to a minimum of 0.05. This schedule facilitated a smooth transition from stochastic exploration to a near-deterministic policy. As illustrated in the dual-axis training plot (Figure 5), this strategy proved effective: the agent demonstrated rapid learning, with the average evacuation steps (blue curve) decreasing sharply and the success rate (green curve) reaching near 100% by approximately Episode 100. Furthermore, the narrow standard deviation bands (shaded regions) across 20 independent runs indicate that the learned policy is highly stable and robust. In the subsequent testing phase, the optimal learned policy was applied to heterogeneous agent groups (Doctors, Nurses, and Patients). To ensure a rigorous comparison with the baseline model, the simulation utilized the identical role-specific speed multipliers defined in Section 3.4.1.
4. Results
4.1. Construction of the Medical Metaverse Architecture
4.1.1. Digital Twin Integration
Building upon this multi-source data foundation, the Digital Twin and Intelligence Core performs multimodal fusion by integrating BIM-based spatial models with real-time IoT telemetry. As illustrated in Figure 6, this layer maintains high-fidelity digital replicas of the physical and clinical environment, encompassing spatial geometries and clinical workflow mapping. A key feature of this digital twin is its multilingual semantic mapping (Yi-Chinese), which bridges cultural gaps in healthcare delivery. These high-fidelity representations serve as the primary input for the Analytics and Intelligence Engine, the system’s computational nerve center. By coupling Agent-Based Modeling (ABM) with Reinforcement Learning (RL) for complex evacuation simulations, alongside spatial optimization and predictive maintenance algorithms, the engine translates raw data into actionable decision-optimization insights.
The final stage of the architecture facilitates Interaction and Closed-Loop Control via a Metaverse Interface. As shown in Figure 7, users can engage with the hospital’s digital twin through XR-based immersive visualization and head-mounted displays (HMD), enabling real-time spatial exploration and navigation. Within the Command & Control Cabin (Figure 6), the interface empowers clinicians with AI-assisted diagnostics and personalized medicine insights. For emergency management, the Emergency Decision Support module delivers dynamic triage protocols and intelligent resource dispatching based on a historical knowledge base and real-time conditions.
Crucially, the architecture is underpinned by an iterative optimization feedback loop, indicated by the numbered flows (1 through 7) in the system diagram. These loops, which extend from initial IoT stream data (Flow 1) and Kafka/Flink processing (Flow 2 & 3) all the way to decision support (Flow 4 & 6) and final optimization feedback/control (Flow 7), ensure that both the digital twin and physical operations are continuously synchronized. This closed-loop mechanism ensures the framework remains adaptive and resilient, providing evidence-based governance for both routine clinical operations and extreme emergency scenarios.
4.1.2. Multilingual Interface and Inclusive Interaction
Based on the proposed framework, we instantiated the Medical Metaverse platform. As illustrated in Figure 8, the architecture centers on an Integrated Service Orchestration Layer. This FHIR-compliant, cloud-native infrastructure ensures secure interoperability across heterogeneous subsystems via federated health information exchange [89,90,91]. Supported by this central digital fabric, the Yi-Chinese bilingual medical metaverse was implemented to specifically address the linguistic accessibility gap in minority ethnic regions.
The user journey begins at the Virtual Hospital Entrance (Figure 8a). Here, Yi cultural design elements, such as traditional patterns and symbolic decorations, are integrated to create a culturally familiar environment that reduces psychological barriers for Yi-speaking patients. Upon entering the platform, users utilize the Bilingual Patient Registration System (Figure 8b), which presents department options and time slots in both Yi script and Mandarin Chinese, enabling users to seamlessly complete the appointment booking process.
The platform extends bilingual support beyond registration to encompass comprehensive healthcare services. The Interactive Health Education Module (Figure 8c) provides anatomical visualizations with synchronized Yi-Chinese annotations, facilitating patient understanding of medical conditions and treatment plans. Multilingual Information Boards (Figure 8d), located throughout the virtual environment, display hospital announcements, health guidelines, and emergency protocols in both languages to ensure critical information reaches all populations. Additionally, a Virtual Healthcare Assistant (Figure 8e) enables real-time consultation through natural language processing, accepting voice or text input in the Yi language and responding with culturally appropriate medical guidance. Technically, this inclusive interaction is realized within the Unity environment by integrating the iFLYTEK Machine Translation API for real-time Yi-Chinese linguistic bridging [92], alongside the Baichuan Medical Large Language Model (LLM) [93], which functions as the cognitive backend to generate evidence-based clinical consultation responses.
Beyond daily healthcare services, the platform integrates Emergency Evacuation Simulation capabilities (Figure 8f). This allows hospital administrators and emergency response teams to visualize crowd dynamics, test evacuation routes, and optimize emergency protocols within a risk-free digital twin environment. This functionality bridges the platform's dual role as both a comprehensive healthcare service interface and a decision-support tool, setting the stage for the rigorous evaluation of spatial patterns and algorithmic performance in Section 4.2.
4.2. Spatial Patterns and Evacuation Dynamics
This section presents the simulation results within the digital twin of Puge County People's Hospital. By comparing the spatial trajectories of heterogeneous agents (Doctors, Nurses, and Patients), we evaluate how the proposed Q-learning algorithm enhances evacuation efficiency and safety compared to the baseline Knowledge-Biased Stochastic Walk. The analysis focuses on spatial distribution patterns, emergent social behaviors, and the quantitative improvement of evacuation metrics.
4.2.1. Role-Based Spatial Distribution and Behavioral Heterogeneity
The generated heatmaps and trajectory visualizations (Figure 9) illustrate a fundamental divergence in movement patterns driven by agent heterogeneity. Medical staff (Doctors and Nurses), leveraging their higher spatial memory parameters () and mobility, exhibited streamlined, high-density trajectories along optimal paths toward exits. This pattern reflects efficient wayfinding behavior characteristic of personnel familiar with the facility layout. In sharp contrast, Patient agents (Figure 6c,f), constrained by limited exit knowledge (), displayed high-entropy dispersion patterns across the building perimeters and the entrance plaza. This visualizes a "high-risk" operational scenario where disorientation leads to frequent backtracking in open spaces and critical delays.
Furthermore, the visualization of flow dynamics confirms that congestion naturally emerges at intersection nodes where these conflicting agent flows converge. To quantify specific spatial vulnerabilities, we analyzed the movement density under the evacuation scenario (Figure 10). The comparative heatmaps reveal a distinct "density hierarchy" correlated with agent capability. Specifically, Doctors maintain near-free-flow conditions, visualized as continuous blue trails with low peak density (), while Nurses exhibit moderate clustering, indicated by yellow/orange zones (). Conversely, Patient agents generate severe congestion "hotspots"—characterized by deep red zones with peak densities exceeding 6.0 agents/m²—at central intersections. This specific localization of bottlenecks provides empirical evidence necessitating architectural interventions, such as widened circulation paths at key intersections or the installation of clearer, high-visibility signage to guide vulnerable populations.
4.2.2. Emergent Social Behaviors
The simulation results validated the effectiveness of the dynamic behavioral rules, revealing emergent social dynamics essential for institutional resilience. A notable "Guiding Effect" was observed in the interaction between different agent roles, specifically where the high-entropy movements of Patient agents were regulated by the deterministic paths of Medical Staff.
To understand this phenomenon, we analyzed the underlying force dynamics. As illustrated in Figure 11, Nurse agents function as mobile attractors within the digital twin environment. When a Patient agent, characterized by low exit knowledge (), detects a Nurse within the interaction radius (), the algorithm triggers a "Flocking State" transition. Visually, this is represented by the convergence of Patient trajectories (Green lines) with Nurse trajectories (Red lines), creating dynamic "safety platoons" that navigate through bottlenecks with reduced friction.
This emergent behavior significantly reduced the randomness of the evacuation process compared to the unassisted baseline. In the random walk scenario, vulnerable agents frequently exhibited "oscillation" behaviors at corridor intersections due to a lack of directional cues. In contrast, the intervention of active guiding roles effectively smoothed these oscillations. Quantitatively, this mechanism demonstrates that social cohesion—specifically the active scaffolding provided by nursing staff—is as critical as physical infrastructure in maintaining orderly flow, preventing the chaotic scattering of vulnerable individuals in complex hospital layouts.
4.2.3. Algorithmic Performance and Evacuation Efficiency
The quantitative evaluation confirms that the proposed Q-learning strategy substantially outperforms the stochastic Random Walk baseline in terms of evacuation efficiency, stability, and spatial logic.
First, regarding overall temporal efficiency, the probability density distribution of evacuation time (Figure 12a) exhibits a pronounced leftward shift under the Q-learning policy. The mean evacuation time was reduced from 49.2 steps for the Random Walk baseline to 29.1 steps with Q-learning, representing a 40.9% improvement in average performance. Crucially, this efficiency gain is accompanied by a significant reduction in variance: the standard deviation decreased from 49.1 to 19.1, indicating that the AI-driven strategy offers far greater predictability—a vital factor for emergency management. A Wilcoxon rank-sum test confirmed that these performance differences are statistically significant (), validating that the improvements are attributable to the learned policy rather than stochastic fluctuations.
Second, the cumulative evacuation curves (Figure 12b) demonstrate a critical enhancement in safety margins. The Q-learning strategy produced a significantly steeper cumulative profile, reflecting a faster and more concentrated evacuation process. Most notably, the 90th percentile evacuation time (), a key indicator of safety for the most vulnerable occupants, was reduced from 145 steps (Random Walk) to 60 steps (Q-learning). This 58.6% reduction in worst-case duration suggests that the algorithm effectively eliminates the "long-tail" effect of lingering evacuees, which is often the primary cause of casualties in real-world scenarios.
Finally, the spatial analysis of exit utilization (Figure 13) reveals the underlying mechanism of this efficiency. As shown in the bar chart, the baseline Random Walk model resulted in a stochastic dispersion of evacuees, failing to account for the varying capacities of different exits. In stark contrast, the Q-Learning agents demonstrated an emergent capacity for capacity-aware navigation. Driven by the area-weighted reward function defined in Equation (6), the agents successfully identified and prioritized the primary evacuation route (Exit 1). By funneling the majority of the flow through this high-capacity exit rather than evenly distributing them to less efficient bottlenecks, the AI strategy significantly optimized the aggregate throughput of the facility. Additional quantitative analyses of evacuation time distributions, role-specific performance, and trajectory patterns are provided in Appendix A (Figure A1, Figure A2, Figure A3 and Figure A4).
of 60 steps compared to 145 steps for the baseline, demonstrating a significantly improved safety margin.
5. Discussion
5.1. Promoting Resilience through AI-Driven Design
This study exposes the limitations of traditional hospital design paradigms, which predominantly rely on static capacity metrics and often fail to capture the emergent complexity of emergency scenarios. By contrasting baseline behaviors with AI-optimized navigation, our simulation demonstrates that resilience is not merely a product of static geometry, but of dynamic flow management. The Q-Learning simulation proves that optimizing exit strategies via the Area-Weighted Reward mechanism can yield substantial gains in evacuation efficiency. Our results indicate that the Q-learning model achieves 90% evacuation completion () in just 60 steps, representing a 58.6% reduction compared to the 145 steps required by the Random Walk strategy. This significant improvement highlights the system’s enhanced robustness, particularly in worst-case scenarios, demonstrating that operational safety can be dramatically improved without requiring costly structural retrofitting. Consequently, this validates AI simulation as a vital, pre-emptive instrument for architectural stress evaluation, allowing designers to resolve latent bottlenecks pre-construction.
Furthermore, the resilience of the system is amplified by the heterogeneous behavioral dynamics captured in our model. Complementary analysis of role-specific performance indicates that the Q-learning algorithm provides disproportionate benefits to vulnerable populations. While medical staff, including doctors and nurses, inherently possess higher movement speeds and greater spatial familiarity, patients, who are modeled with lower velocities and higher uncertainty, experience the most pronounced reductions in evacuation time. This suggests that a form of 'collective intelligence' emerges not solely from individual pathfinding, but from the implicit guidance embedded in the AI-optimized flow of high-knowledge agents. By mitigating congestion at critical bottlenecks, the algorithm generates a 'slipstream effect', analogous to the self-organized lane formation observed in social force models [94,95], in which the efficient movement of capable agents facilitates the progression of slower, mobility-impaired individuals. Importantly, this finding demonstrates that the proposed framework does not merely optimize for the 'average' user, but actively safeguards the 'slowest' users, thereby aligning technical efficiency with the ethical imperative of inclusive healthcare safety.
5.2. Bridging the Digital Divide for Social Sustainability
Within the resource constrained context of the Liangshan Yi Autonomous Prefecture, the digital divide remains a critical barrier to equitable access to healthcare services and effective emergency response. In earthquake prone regions, cognitive overload, linguistic mismatch, and unfamiliar digital interfaces can directly undermine evacuation efficiency and amplify disparities among vulnerable populations. The proposed Medical Metaverse framework, illustrated in Figure 6, addresses these challenges by reorienting the mode of user system interaction. Instead of requiring users to adapt to complex digital environments, the system shifts the cognitive burden toward algorithm supported assistance, thereby lowering participation thresholds for elderly and Yi speaking patients. Through a Yi Chinese bilingual digital human interface, users are able to navigate healthcare services and emergency guidance via natural language interaction rather than text based hierarchical menus.
From a seismic resilience perspective, reducing cognitive and linguistic barriers is not merely a social objective but a functional prerequisite for reliable evacuation performance. During earthquake induced emergencies, delayed comprehension or misinterpretation of instructions can translate directly into slower response times and uneven evacuation outcomes. By improving situational understanding and wayfinding confidence among vulnerable users, the proposed bilingual interface indirectly enhances the consistency and equity of building level evacuation behavior under seismic stress.
Importantly, this design philosophy is conceptually aligned with the behavioral insights derived from the evacuation simulations presented in Section 5.1. In the physical domain, high knowledge agents generated a flow facilitation effect that supported the movement of slower individuals during evacuation. At the cognitive level, the Medical Metaverse functions as a form of digital scaffolding that translates this physical guidance mechanism into structured informational support. The virtual companion acts as an assistive interface that helps alleviate psychological stress and information overload, challenges that are known to disproportionately affect vulnerable populations during emergency situations [96,97].
Rather than merely delivering static information, the culturally responsive interface provides context aware guidance, adaptive pacing, and linguistic familiarity, which together enhance user confidence and situational comprehension [98,99]. By embedding cultural and linguistic intelligence into the digital layer of healthcare environments, the proposed approach contributes to social sustainability while reinforcing functional seismic resilience. In this way, the framework demonstrates how inclusive digital design can support safer, more equitable, and more resilient evacuation outcomes in healthcare facilities located in underserved regions.
5.3. Limitations and Future Directions
Notwithstanding the contributions of this framework, certain limitations remain. First, the behavioral model currently abstracts human panic into a binary state, whereas actual panic involves a complex continuum driven by emotional contagion [100,101]. Future work will integrate granular psychometric parameters, such as the OCEAN personality model [102], and leverage Large Language Models (LLMs) to function as the cognitive control layer for agents. This will enable more realistic simulations of inter-agent communication and dynamic decision-making under stress. Second, as the metaverse prototype currently utilizes simulated data for specific modules, empirical validation through large-scale deployment at Puge County Hospital is essential to confirm the longitudinal efficacy of VR interventions. Finally, extending the simulation to account for vertical evacuation dynamics across multiple floors represents a pivotal direction for holistic hospital safety planning.
6. Conclusions
This study develops an integrated framework for enhancing the seismic resilience and evacuation performance of healthcare facilities in resource constrained ethnic minority regions. By combining high fidelity digital twins, agent-based evacuation modeling, and reinforcement learning, the proposed approach provides a scalable and data driven pathway for evaluating spatial and operational strategies in underserved healthcare environments.
The results demonstrate that spatial resilience is not solely determined by architectural geometry, but emerges from the dynamic interaction between spatial configuration and evacuation flow management. When evaluated against a random walk baseline, the Q learning based strategy achieved substantial efficiency gains, reducing the mean evacuation time by 40.9 percent and the 90th percentile evacuation time by 58.6 percent. These findings confirm that algorithm supported evacuation strategies can significantly enhance life safety and functional performance in high density healthcare settings, particularly in outdoor plazas and external circulation areas, without requiring costly structural retrofitting. From an operational perspective, the results further highlight the importance of integrating intelligent evacuation strategies into emergency preparedness through coordinated physical and digital drills.
In addition, the incorporation of a Yi Chinese bilingual digital interface extends the framework beyond purely spatial optimization by addressing accessibility and inclusivity in healthcare environments. Rather than functioning as a standalone technological feature, this interface supports clearer wayfinding and reduces cognitive barriers for minority patients, contributing to more equitable evacuation outcomes under emergency conditions.
Beyond the specific case study, this research offers a replicable paradigm for integrating artificial intelligence, spatial simulation, and human-centered design in the assessment of seismic resilience of complex healthcare building systems. The findings suggest that AI assisted digital twin approaches can play a critical role in supporting safer, more inclusive, and operationally resilient healthcare facilities under increasing pressures from urbanization and seismic risk.
Author Contributions
Conceptualization, Gang Meng and Chunlin Bian; methodology, Chunlin Bian; software, Xiaofeng Cai; validation, Hua Chen and Liuyang Li; formal analysis, Chunlin Bian; investigation, Fuhong Lv; resources, Liuyang Li; data curation, Yonghao Guo; writing—original draft preparation, Chunlin Bian; writing—review and editing, Gang Meng and Chunlin Bian; funding acquisition, Liuyang Li. All authors have read and agreed to the published version of the manuscript.
Data Availability Statement
The data associated with this research may be accessed by contacting the corresponding author under reasonable conditions.
Acknowledgments
The authors would like to express their sincere appreciation to the Xichang Branch of Chengdu Meisha Architectural Design Co., Ltd., and The People’s Hospital of Puge County, Liangshan Yi Autonomous Prefecture, for their generous support throughout the research and writing of this work. We would also like to thank the editors and reviewers for their valuable comments.
Conflicts of Interest
authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ABM | Agent-Based Modeling |
| AI | Artificial Intelligence |
| AWR | Area-Weighted Reward |
| DT | Digital Twin |
| GIS | Geographic Information System |
| PCPH | Puge County People's Hospital |
| RL | Reinforcement Learning |
| RW | Random Walk |
| Time to 90% Evacuation Completion |
Appendix A
Appendix A.1. Additional Quantitative Analyses of Evacuation Performance
Figure A1.
Statistical distribution of evacuation times represented by boxplots. This figure provides supplementary quantitative evidence for the algorithmic stability discussed in Section 4.2.3. The Random Walk baseline exhibits a substantially wider interquartile range (IQR) and numerous extreme outliers exceeding 140 steps, indicating pronounced stochastic volatility and long-tail latency. In contrast, the Q-learning strategy demonstrates a compact distribution with minimal outliers, statistically confirming (p < 0.05) its effectiveness in suppressing extreme evacuation delays.
Figure A1.
Statistical distribution of evacuation times represented by boxplots. This figure provides supplementary quantitative evidence for the algorithmic stability discussed in Section 4.2.3. The Random Walk baseline exhibits a substantially wider interquartile range (IQR) and numerous extreme outliers exceeding 140 steps, indicating pronounced stochastic volatility and long-tail latency. In contrast, the Q-learning strategy demonstrates a compact distribution with minimal outliers, statistically confirming (p < 0.05) its effectiveness in suppressing extreme evacuation delays.
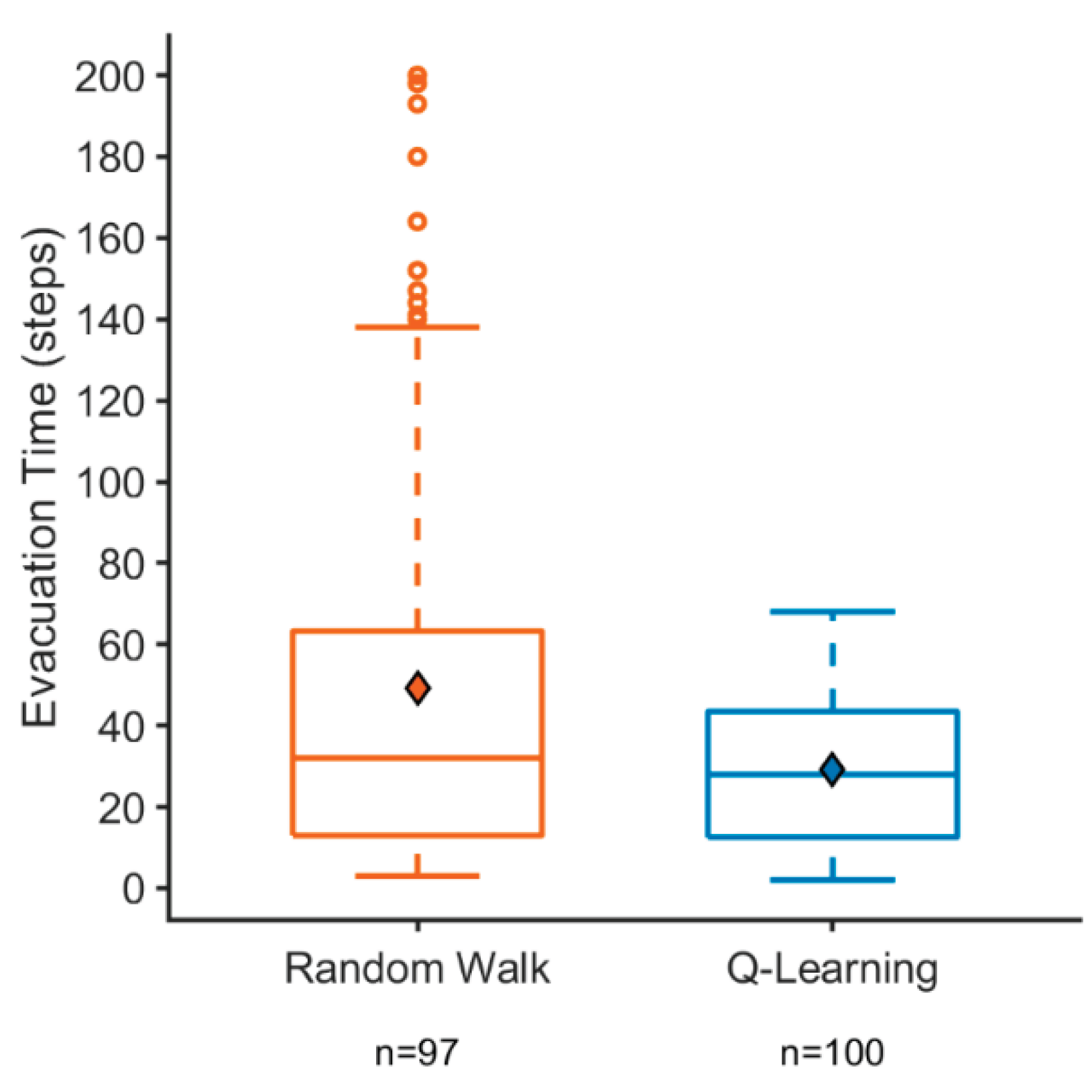
Figure A2.
Role-specific evacuation performance as a function of initial distance to exits. (a) Random Walk baseline: regression analysis reveals a pronounced performance disparity, with Patients exhibiting a steep slope, indicating that increased distance disproportionately penalizes vulnerable agents due to lower speed and spatial uncertainty. (b) Q-learning strategy: the proposed algorithm significantly flattens the regression slope for Patients, aligning their performance trajectory more closely with that of Doctors and Nurses. This supplementary analysis provides quantitative support for the ‘slipstream effect’ discussed in Section 5.1.
Figure A2.
Role-specific evacuation performance as a function of initial distance to exits. (a) Random Walk baseline: regression analysis reveals a pronounced performance disparity, with Patients exhibiting a steep slope, indicating that increased distance disproportionately penalizes vulnerable agents due to lower speed and spatial uncertainty. (b) Q-learning strategy: the proposed algorithm significantly flattens the regression slope for Patients, aligning their performance trajectory more closely with that of Doctors and Nurses. This supplementary analysis provides quantitative support for the ‘slipstream effect’ discussed in Section 5.1.
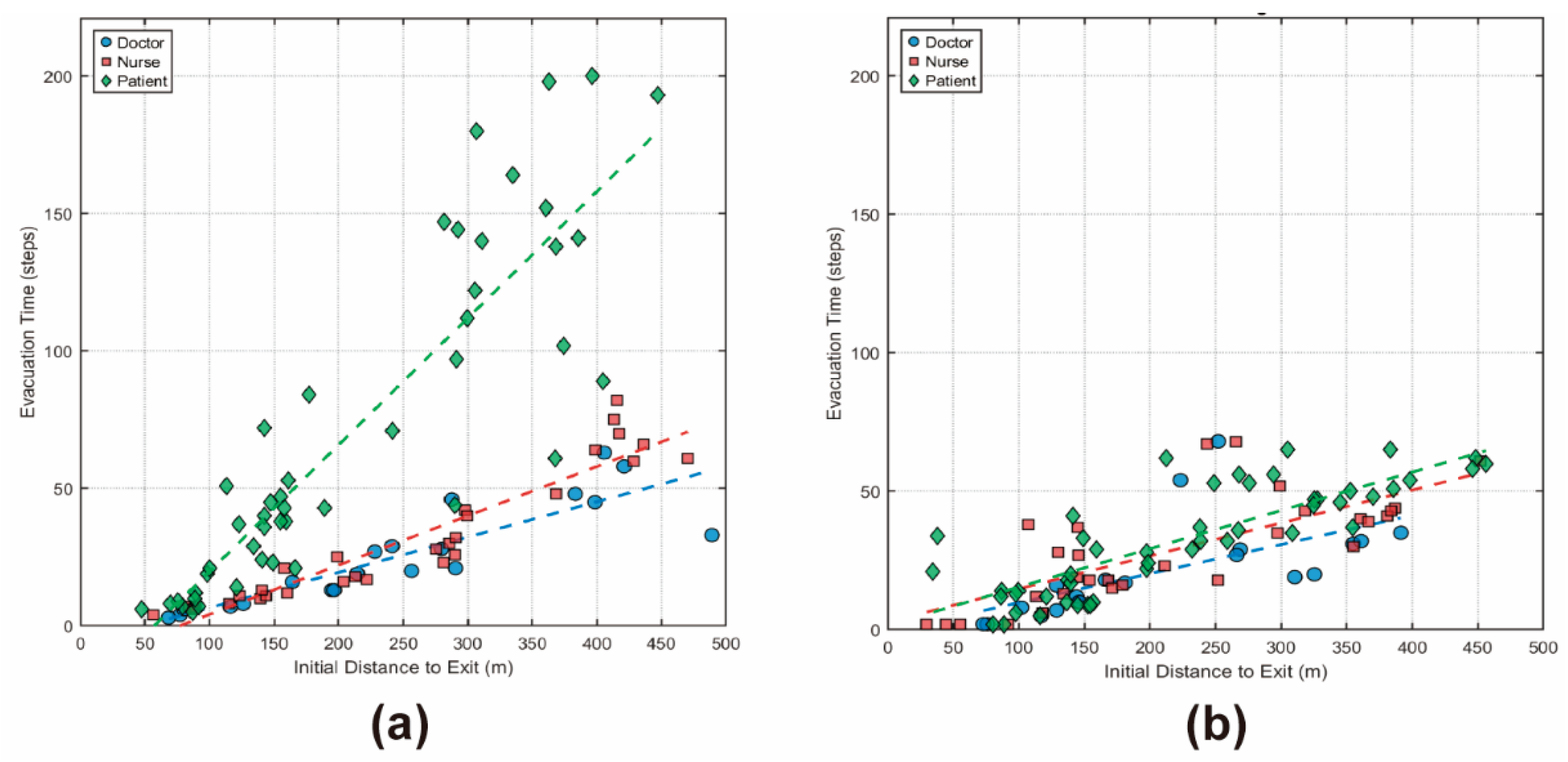
Figure A3.
Comparison of role-specific evacuation time distributions under different strategies. (a) Random Walk baseline: a clear hierarchy of vulnerability emerges, with Patients experiencing severe delays and high variance, indicating systematic disadvantage. (b) Q-learning strategy: the algorithm substantially reduces the mean evacuation time for Patients by 54.1% (from 71.0 to 32.6 steps) and compresses the distribution variance. The performance gap between the fastest and slowest roles is markedly reduced, quantitatively demonstrating the equity-enhancing effect of the proposed approach.
Figure A3.
Comparison of role-specific evacuation time distributions under different strategies. (a) Random Walk baseline: a clear hierarchy of vulnerability emerges, with Patients experiencing severe delays and high variance, indicating systematic disadvantage. (b) Q-learning strategy: the algorithm substantially reduces the mean evacuation time for Patients by 54.1% (from 71.0 to 32.6 steps) and compresses the distribution variance. The performance gap between the fastest and slowest roles is markedly reduced, quantitatively demonstrating the equity-enhancing effect of the proposed approach.
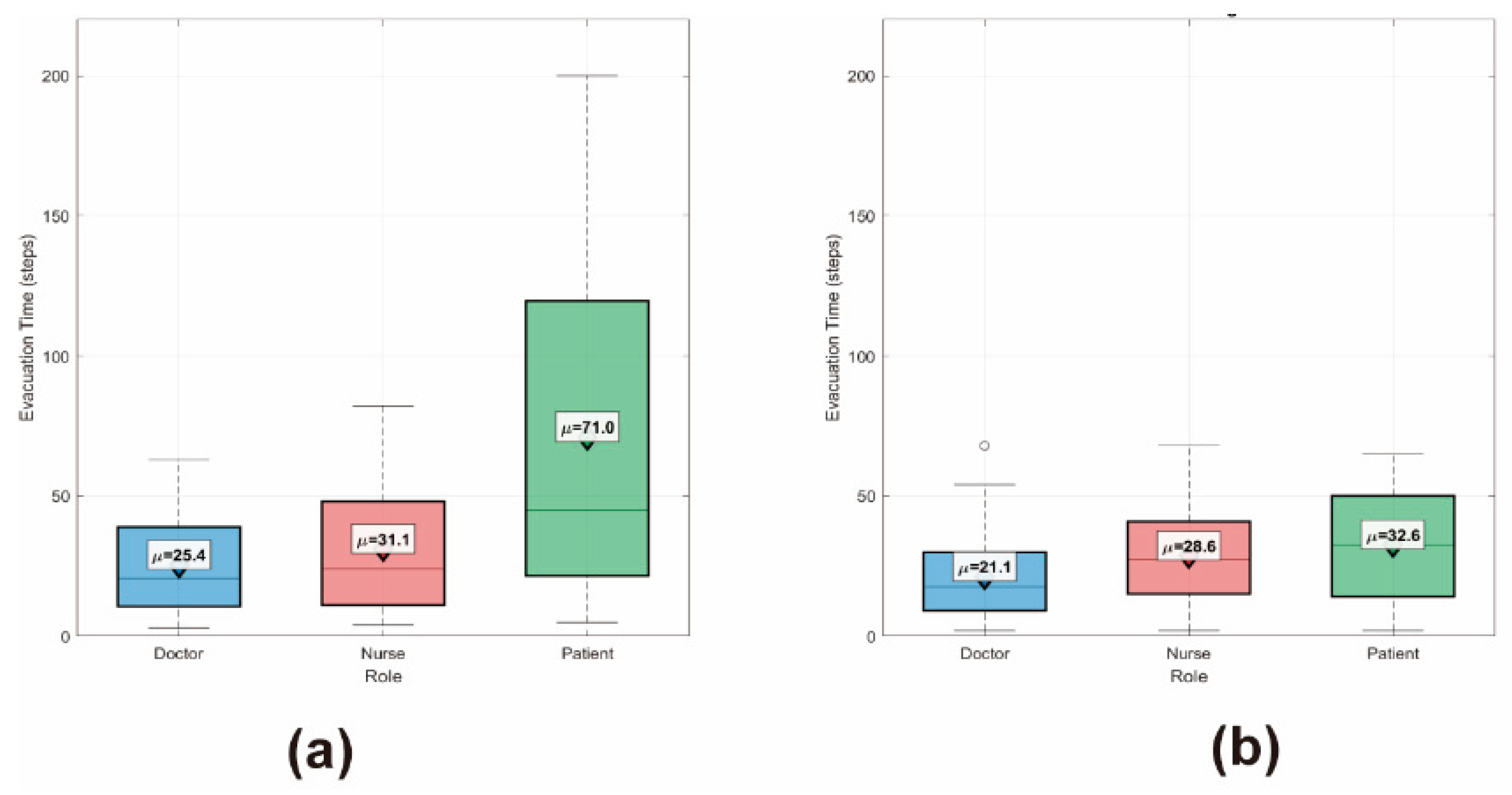
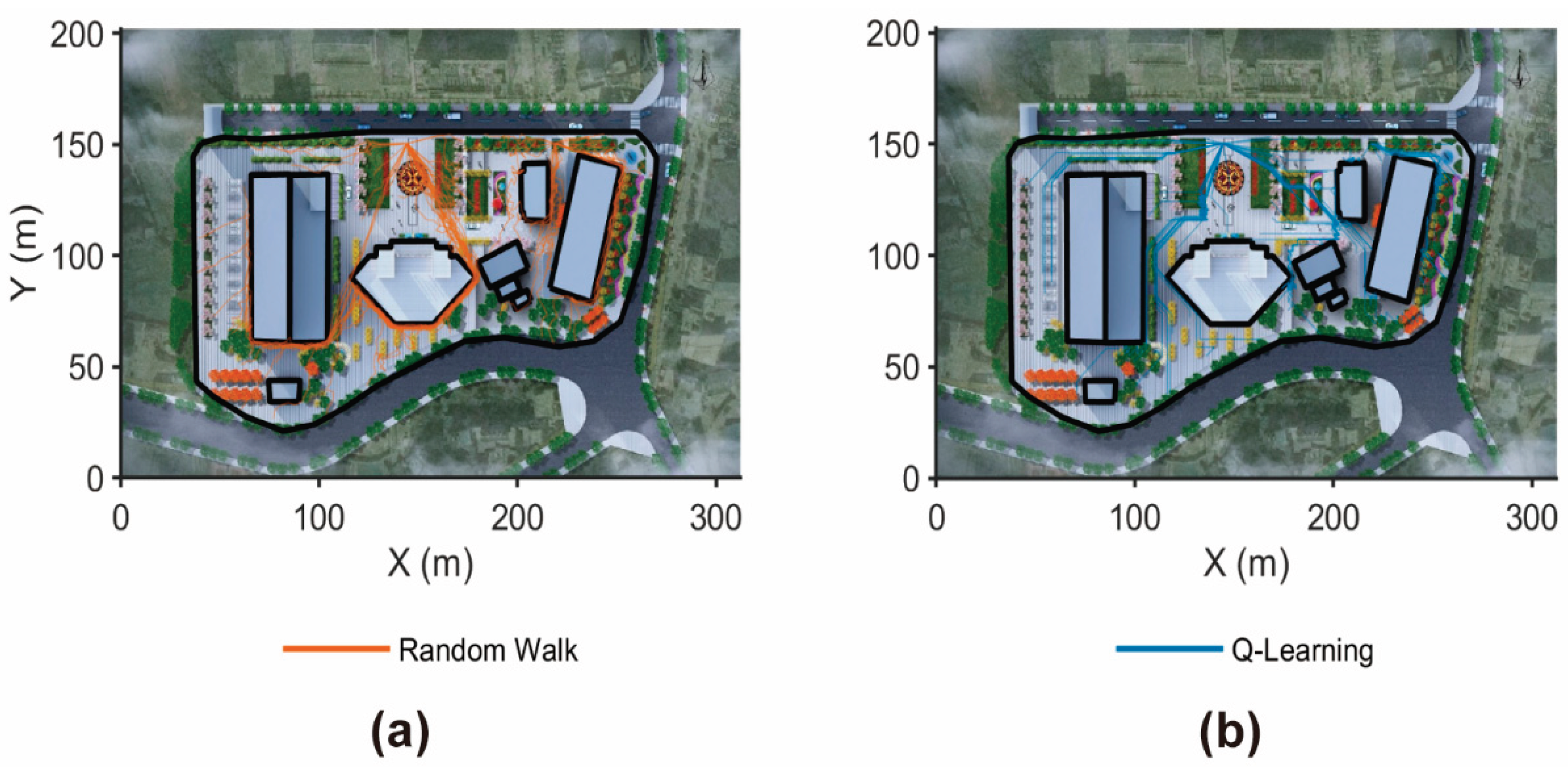
Figure A4.
Visual comparison of agent evacuation trajectories under different strategies. (a) Random Walk baseline: trajectories exhibit high-entropy movement patterns characterized by inefficient wandering, redundant backtracking, and frequent directional changes. (b) Q-learning strategy: trajectories show directed and streamlined movement toward exits, reflecting optimized spatial flow and reduced unnecessary detours. This visual evidence supplements the quantitative findings by illustrating how AI-driven policies improve spatial navigation efficiency.
Figure A4.
Visual comparison of agent evacuation trajectories under different strategies. (a) Random Walk baseline: trajectories exhibit high-entropy movement patterns characterized by inefficient wandering, redundant backtracking, and frequent directional changes. (b) Q-learning strategy: trajectories show directed and streamlined movement toward exits, reflecting optimized spatial flow and reduced unnecessary detours. This visual evidence supplements the quantitative findings by illustrating how AI-driven policies improve spatial navigation efficiency.
References
- State Council of the People’s Republic of China. Healthy China 2030 planning outline. Available online: https://www.gov.cn/xinwen/2016-10/25/content_5124174.htm (accessed on 27 October 2025).
- United Nations Transforming Our World: The 2030 Agenda for Sustainable Development. Available online: https://sdgs.un.org/2030agenda (accessed on 20 January 2026).
- Zhang, Y.; Wu, T.; Yu, H.; Fu, J.; Xu, J.; Liu, L.; Tang, C.; Li, Z. Green Spaces Exposure and the Risk of Common Psychiatric Disorders: A Meta-Analysis. SSM - Popul. Health 2024, 25, 101630. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Li, J.; Chen, X.; Shen, Y. Combined Concrete and Cable Restrainers to Prevent Longitudinal Unseating of Highway Bridges during Earthquakes. Engineering Structures 2024, 314, 118388. [Google Scholar] [CrossRef]
- Bruneau, M.; Reinhorn, A. Exploring the Concept of Seismic Resilience for Acute Care Facilities. Earthquake Spectra 2007, 23, 41–62. [Google Scholar] [CrossRef]
- Schultz, C.; Koenig, K.; Lewis, R. Implications of Hospital Evacuation after the Northridge, California, Earthquake. The New England journal of medicine 2003, 348, 1349–1355. [Google Scholar] [CrossRef]
- Ceferino, L.; Mitrani-Reiser, J.; Kiremidjian, A.; Deierlein, G.; Bambarén, C. Effective Plans for Hospital System Response to Earthquake Emergencies. Nat Commun 2020, 11, 4325. [Google Scholar] [CrossRef]
- Al Khatib, I.; Samara, F.; Ndiaye, M. A Systematic Review of the Impact of Therapeutical Biophilic Design on Health and Wellbeing of Patients and Care Providers in Healthcare Services Settings. Front. Built Environ. 2024, 10. [Google Scholar] [CrossRef]
- Wang, J.; Luo, Y.; Zhou, X.; Zhao, W.; Lei, Y.; Xie, W. Impact of Assistance Behavior on Evacuation Efficiency in High-Rise Hospital Inpatient Buildings: An Agent-Based Simulation Study. J. Build. Eng. 2025, 112, 113780. [Google Scholar] [CrossRef]
- Ali, S.; Abdullah; Armand, T.P.T.; Athar, A.; Hussain, A.; Ali, M.; Yaseen, M.; Joo, M.-I.; Kim, H.-C. Metaverse in Healthcare Integrated with Explainable AI and Blockchain: Enabling Immersiveness, Ensuring Trust, and Providing Patient Data Security. Sens. 2023, 23, 565. [Google Scholar] [CrossRef]
- Chen, C.; Koll, C.; Wang, H.; Lindell, M.K. An Interdisciplinary Agent-Based Evacuation Model: Integrating the Natural Environment, Built Environment, and Social System for Community Preparedness and Resilience. [CrossRef]
- Fattahi Maassoum, A.S.; Farkisch, H.; Taji, M. AI-Based Hospital Design Process through Neuro-Symbolic Strategies. Arch. Bone Jt. Surg. 2025, 13, 442–456. [Google Scholar] [CrossRef]
- Islas-Toski, M.; Cuevas, E.; Pérez-Cisneros, M.; Escobar, H. Agent-Based Evacuation Modeling: Enhancing Building Safety in Emergency Scenarios. Smart Cities 2024, 7, 3165–3187. [Google Scholar] [CrossRef]
- Haghpanah, F.; Ghobadi, K.; Schafer, B.W. Multi-Hazard Hospital Evacuation Planning during Disease Outbreaks Using Agent-Based Modeling. Int J Disaster Risk Reduct 2021, 66, 102632. [Google Scholar] [CrossRef] [PubMed]
- Wan, Z.; Yang, F.; Zhou, T.; Li, C. The Effects of Spatial Layout on Efficiency of Safe Evacuation After Conversion of an Exhibition Building to a Fangcang Shelter Hospital. Buildings 2025, 15, 2880. [Google Scholar] [CrossRef]
- Geoerg, P.; de Schot, L.; Lovreglio, R. Decoding Hospital Evacuation Drills: Pre-Movement and Movement Analysis in New Zealand. Fire Technol 2025, 61, 4303–4329. [Google Scholar] [CrossRef]
- Wang, G.; Badal, A.; Jia, X.; Maltz, J.S.; Mueller, K.; Myers, K.J.; Niu, C.; Vannier, M.; Yan, P.; Yu, Z.; et al. Development of Metaverse for Intelligent Healthcare. Nat. Mach. Intell. 2022, 4, 922–929. [Google Scholar] [CrossRef]
- Buragohain, D.; Khichar, S.; Deng, C.; Meng, Y.; Chaudhary, S. Analyzing Metaverse-Based Digital Therapies, Their Effectiveness, and Potential Risks in Mental Healthcare. Sci. Rep. 2025, 15. [Google Scholar] [CrossRef]
- Building Climate-Resilient Health Systems. Available online: https://www.who.int/teams/environment-climate-change-and-health/climate-change-and-health/country-support/building-climate-resilient-health-systems (accessed on 8 November 2025).
- Gesler, W.M. Therapeutic Landscapes: Medical Issues in Light of the New Cultural Geography. Soc. Sci. Med. 1992, 34, 735–746. [Google Scholar] [CrossRef]
- Healing Gardens: Therapeutic Benefits and Design Recommendations; Marcus, C.C., Barnes, M., Eds.; Wiley series in healthcare and senior living design; Wiley: New York, 1999; ISBN 978-0-471-19203-9.
- Hamilton, D.K.; Watkins, D.H. Evidence-Based Design for Multiple Building Types; Wiley: Hoboken (N.J), 2009; ISBN 978-0-470-12934-0. [Google Scholar]
- Stier-Jarmer, M.; Throner, V.; Kirschneck, M.; Immich, G.; Frisch, D.; Schuh, A. The Psychological and Physical Effects of Forests on Human Health: A Systematic Review of Systematic Reviews and Meta-Analyses. International Journal of Environmental Research and Public Health 2021, 18, 1770. [Google Scholar] [CrossRef]
- Ulrich, R.S. View through a Window May Influence Recovery from Surgery. Science 1984, 224, 420–421. [Google Scholar] [CrossRef] [PubMed]
- Guo, F.; Miao, S.; Xu, S.; Luo, M.; Dong, J.; Zhang, H. Multi-Objective Optimization Design for Cold-Region Office Buildings Balancing Outdoor Thermal Comfort and Building Energy Consumption. Energies 2025, 18, 62. [Google Scholar] [CrossRef]
- Liu, T.; Wang, J.; Zhou, D.; Meng, X.; Luo, X.; Wang, Y. Research on Optimization Design Strategies for Natural Ventilation in Living Units of Institutional Elderly Care Facilities Based on Computational Fluid Dynamics Simulation. Buildings 2024, 14, 1648. [Google Scholar] [CrossRef]
- Shao, L.; Tang, W.; Zhang, Z.; Chen, X. Medical Metaverse: Technologies, Applications, Challenges and Future. J. Mech. Med. Biol. 2023, 23, 2350028. [Google Scholar] [CrossRef]
- Katsoulakis, E.; Wang, Q.; Wu, H.; Shahriyari, L.; Fletcher, R.; Liu, J.; Achenie, L.; Liu, H.; Jackson, P.; Xiao, Y.; et al. Digital Twins for Health: A Scoping Review. npj Digital Med. 2024, 7, 77. [Google Scholar] [CrossRef] [PubMed]
- Ringeval, M.; Sosso, F.A.E.; Cousineau, M.; Paré, G. Advancing Health Care with Digital Twins: Meta-Review of Applications and Implementation Challenges. J Med Internet Res 2025, 27, e69544. Available online: https://www.jmir.org/2025/1/e69544. [CrossRef] [PubMed]
- Rehan, M.W.; Rehan, M.M. Survey, Taxonomy, and Emerging Paradigms of Societal Digital Twins for Public Health Preparedness. npj Digital Med. 2025, 8, 520. [Google Scholar] [CrossRef] [PubMed]
- Tudor, B.H.; Shargo, R.; Gray, G.M.; Fierstein, J.L.; Kuo, F.H.; Burton, R.; Johnson, J.T.; Scully, B.B.; Asante-Korang, A.; Rehman, M.A.; et al. A Scoping Review of Human Digital Twins in Healthcare Applications and Usage Patterns. npj Digital Med. 2025, 8, 587. [Google Scholar] [CrossRef]
- Asciak, L.; Kyeremeh, J.; Luo, X.; Kazakidi, A.; Connolly, P.; Picard, F.; O’Neill, K.; Tsaftaris, S.A.; Stewart, G.D.; Shu, W. Digital Twin Assisted Surgery, Concept, Opportunities, and Challenges. npj Digital Med. 2025, 8, 32. [Google Scholar] [CrossRef]
- Vallée, A. Digital Twin for Healthcare Systems. [CrossRef]
- Dinu Roman Szabo, M.; Dumitras, A.; Mircea, D.-M.; Doroftei, D.; Sestras, P.; Boscaiu, M.; Brzuszek, R.F.; Sestras, A.F. Touch, Feel, Heal. The Use of Hospital Green Spaces and Landscape as Sensory-Therapeutic Gardens: A Case Study in a University Clinic. [CrossRef]
- Sung, W.-P.; Huang, C.-S.; Wang, P.-T.; Yang, M.-Y. Integrating AI Generation and CFD Simulation in Coastal Hospital Landscape Design: A Case Study of Penghu, Taiwan. Buildings 2025, 15, 3283. [Google Scholar] [CrossRef]
- Bonabeau, E. Agent-Based Modeling: Methods and Techniques for Simulating Human Systems. Proc. Natl. Acad. Sci. 2002, 99, 7280–7287. [Google Scholar] [CrossRef] [PubMed]
- Helbing, D.; Farkas, I.; Vicsek, T. Simulating Dynamical Features of Escape Panic. Nature 2000, 407, 487–490. [Google Scholar] [CrossRef]
- Park, J.S.; O’Brien, J.; Cai, C.J.; Morris, M.R.; Liang, P.; Bernstein, M.S. Generative Agents: Interactive Simulacra of Human Behavior. In Proceedings of the Proceedings of the 36th Annual ACM Symposium on User Interface Software and Technology, 2023; Association for Computing Machinery: New York, NY, USA; pp. 1–22. [Google Scholar]
- Macal, C.M.; North, M.J. Tutorial on Agent-Based Modelling and Simulation. Journal of Simulation 2010, 4, 151–162. [Google Scholar] [CrossRef]
- An, L.; Grimm, V.; Sullivan, A.; Turner, B.L., II; Malleson, N.; Heppenstall, A.; Vincenot, C.; Robinson, D.; Ye, X.; Liu, J.; et al. Challenges, Tasks, and Opportunities in Modeling Agent-Based Complex Systems. Ecological Modelling 2021, 457, 109685. [Google Scholar] [CrossRef]
- Manson, S.M.; Sun, S.; Bonsal, D. Agent-Based Modeling and Complexity. In Agent-Based Models of Geographical Systems; Heppenstall, A.J., Crooks, A.T., See, L.M., Batty, M., Eds.; Springer Netherlands: Dordrecht, 2012; pp. 125–139. ISBN 978-90-481-8927-4. [Google Scholar]
- Grimm, V.; Railsback, S.F.; Vincenot, C.E.; Berger, U.; Gallagher, C.; DeAngelis, D.L.; Edmonds, B.; Ge, J.; Giske, J.; Groeneveld, J.; et al. The ODD Protocol for Describing Agent-Based and Other Simulation Models: A Second Update to Improve Clarity, Replication, and Structural Realism. J. Artif. Soc. Soc. Simul. 2020, 23, 7. [Google Scholar] [CrossRef]
- Manson, S.; An, L.; Clarke, K.C.; Heppenstall, A.; Koch, J.; Krzyzanowski, B.; Morgan, F.; O’Sullivan, D.; Runck, B.C.; Shook, E.; et al. Methodological Issues of Spatial Agent-Based Models. J. Artif. Soc. Soc. Simul. 2020, 23, 3. [Google Scholar] [CrossRef]
- Huang, R.; He, H.; Su, Q. Towards a Fossil-Free Urban Transport System: An Intelligent Cross-Type Transferable Energy Management Framework Based on Deep Transfer Reinforcement Learning. Applied Energy 2024, 363, 123080. [Google Scholar] [CrossRef]
- Tian, W.; Fu, G.; Xin, K.; Zhang, Z.; Liao, Z. Improving the Interpretability of Deep Reinforcement Learning in Urban Drainage System Operation. Water Research 2024, 249, 120912. [Google Scholar] [CrossRef]
- Shen, J.; Zheng, F.; Ma, Y.; Deng, W.; Zhang, Z. Urban Travel Carbon Emission Mitigation Approach Using Deep Reinforcement Learning. Sci Rep 2024, 14, 27778. [Google Scholar] [CrossRef]
- Equihua, J.; Beckmann, M.; Seppelt, R. Connectivity Conservation Planning through Deep Reinforcement Learning. Methods in Ecology and Evolution 2024, 15, 779–790. [Google Scholar] [CrossRef]
- Heinbach, B.; Burggräf, P.; Steinberg, F. From Theory to Application: Investigating the Generalizability of Facility Layout Problems Using a Deep Reinforcement Learning Approach. Prod. Eng. Res. Devel. 2025, 19, 975–991. [Google Scholar] [CrossRef]
- Chung, K.T.; Lee, C.K.M.; Tsang, Y.P. Neural Combinatorial Optimization with Reinforcement Learning in Industrial Engineering: A Survey. Artificial Intelligence Review 2025, 58, 130. [Google Scholar] [CrossRef]
- Liang, H.; Wang, S.; Li, H.; Zhou, L.; Chen, H.; Zhang, X.; Chen, X. Sponet: Solve Spatial Optimization Problem Using Deep Reinforcement Learning for Urban Spatial Decision Analysis. International Journal of Digital Earth 2024, 17, 2299211. [Google Scholar] [CrossRef]
- Kakooee, R.; Dillenburger, B. Reimagining Space Layout Design through Deep Reinforcement Learning. J Comput Des Eng 2024, 11, 43–55. [Google Scholar] [CrossRef]
- Kool, W.; van Hoof, H.; Gromicho, J.; Welling, M. Deep Policy Dynamic Programming for Vehicle Routing Problems. In Proceedings of the Integration of Constraint Programming, Artificial Intelligence, and Operations Research; Schaus, P., Ed.; Springer International Publishing: Cham, 2022; pp. 190–213. [Google Scholar]
- Chiboub, A.; Francois, J.; Alix, T.; Dupas, R. Contribution of Deep Reinforcement Learning to Solve Reconfigurable Facilities Layout Problems. Manuf. Lett. 2025, 46, 16–20. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, X.; Zeng, T.; Duan, J.; Wu, C.; Wu, D.; Chen, X. Task Placement and Resource Allocation for Edge Machine Learning: A GNN-Based Multi-Agent Reinforcement Learning Paradigm. IEEE Trans. Parallel Distrib. Syst. 2023, 34, 3073–3089. [Google Scholar] [CrossRef]
- Xu, Y.; Fang, M.; Chen, L.; Xu, G.; Du, Y.; Zhang, C. Reinforcement Learning with Multiple Relational Attention for Solving Vehicle Routing Problems. IEEE Trans. Cybern. 2022, 52, 11107–11120. [Google Scholar] [CrossRef]
- Kool, W.; van Hoof, H.; Welling, M. Attention, Learn to Solve Routing Problems! 2019.
- Guo, W.; Wang, R.; Xu, Y.; Jin, Y. Unified and Generalizable Reinforcement Learning for Facility Location Problems on Graphs; 29 January 2025. [Google Scholar]
- Oroojlooyjadid, A.; Nazari, M.; Snyder, L.V.; Takáč, M. A Deep Q-Network for the Beer Game: Deep Reinforcement Learning for Inventory Optimization. Manufacturing & Service Operations Management 2021. [Google Scholar] [CrossRef]
- Spanò, S.; Cardarilli, G.C.; Di Nunzio, L.; Fazzolari, R.; Giardino, D.; Matta, M.; Nannarelli, A.; Re, M. An Efficient Hardware Implementation of Reinforcement Learning: The Q-Learning Algorithm. IEEE Access 2019, 7, 186340–186351. [Google Scholar] [CrossRef]
- Qi, L.; Sun, Y.; Luan, W. Large-Scale Traffic Signal Control Based on Multi-Agent Q-Learning and Pressure. IEEE Access 2024, 12, 1092–1101. [Google Scholar] [CrossRef]
- Zhou, C.; Stephen, A.; Tan, K.C.; Chew, E.P.; Lee, L.H. Multiagent Q-Learning Approach for the Recharging Scheduling of Electric Automated Guided Vehicles in Container Terminals. Transp. Sci. 2024, 58, 664–683. [Google Scholar] [CrossRef]
- Sharma, J.; Andersen, P.-A.; Granmo, O.-C.; Goodwin, M. Deep Q-Learning with Q-Matrix Transfer Learning for Novel Fire Evacuation Environment. IEEE Trans. Syst., Man, Cybern., Syst. 2021, 51, 7363–7381. [Google Scholar] [CrossRef]
- Takabatake, T.; Asai, K.; Kakuta, H.; Hasegawa, N. Optimizing Evacuation Paths Using Agent-Based Evacuation Simulations and Reinforcement Learning. Int. J. Disaster Risk Reduct. 2025, 117, 105173. [Google Scholar] [CrossRef]
- Zhang, D.; Wang, M.; Mango, J.; Li, X.; Xu, X. A Survey on Applications of Reinforcement Learning in Spatial Resource Allocation. Computational Urban Science 2024, 4, 14. [Google Scholar] [CrossRef]
- Zhao, Y.; Duan, D. Workshop Facility Layout Optimization Based on Deep Reinforcement Learning. Processes 2024, 12, 201. [Google Scholar] [CrossRef]
- Zheng, Y.; Lin, Y.; Zhao, L.; Wu, T.; Jin, D.; Li, Y. Spatial Planning of Urban Communities via Deep Reinforcement Learning. Nat Comput Sci 2023, 3, 748–762. [Google Scholar] [CrossRef]
- Li, D.; Zhang, Z.; Alizadeh, B.; Zhang, Z.; Duffield, N.; Meyer, M.A.; Thompson, C.M.; Gao, H.; Behzadan, A.H. A Reinforcement Learning-Based Routing Algorithm for Large Street Networks. International Journal of Geographical Information Science 2023, 38, 183–215. [Google Scholar] [CrossRef]
- Klar, M.; Langlotz, P.; Aurich, J.C. A Framework for Automated Multiobjective Factory Layout Planning Using Reinforcement Learning. Procedia CIRP 2022, 112, 555–560. [Google Scholar] [CrossRef]
- Zhao, Y.; Duan, D. Workshop Facility Layout Optimization Based on Deep Reinforcement Learning. Processes 2024, 12, 201. [Google Scholar] [CrossRef]
- The People’s Hospital of Puge County. Available online: https://www.scpgyy.com/ (accessed on 6 November 2025).
- Harrell, S. Ways of Being Ethnic in Southwest China; Studies on ethnic groups in China; University of Washington Press: Seattle, 2001; ISBN 978-0-295-80407-1.
- Sun, Q.; Xue, X.; Chen, C. How the Body Gets Healthy: An Empirical Case of Animism and Naturalism Working Together in the Treatment of Disease among the Nuosu People of Southwest China. Religions 2025, 16, 533. [Google Scholar] [CrossRef]
- Lu, H.; Ismail, S. binti; Rahman, K.A.A. bin A. A Study on the Expression of Three Colors - Black, Red, and Yellow and Related Aesthetic Ideas of the Yi People | Journal of Namibian Studies : History Politics Culture. 2023.
- Meng, K.; Li, H.; Shu, Y.; Chen, M.; Han, X.; He, L. Database Construction and Remodeling Method on Traditional Yi Nationality Patterns of China with GAN Model. Npj Herit. Sci. 2025, 13, 181. [Google Scholar] [CrossRef]
- Kokal, I.; Engel, A.; Kirschner, S.; Keysers, C. Synchronized Drumming Enhances Activity in the Caudate and Facilitates Prosocial Commitment - If the Rhythm Comes Easily. [CrossRef] [PubMed]
- Shamay-Tsoory, S.G.; Mendelsohn, A. Real-Life Neuroscience: An Ecological Approach to Brain and Behavior Research. Perspect. Psychol. Sci. 2019, 14, 841–859. [Google Scholar] [CrossRef]
- Durkheim, E. The Elementary Forms of the Religious Life; CreateSpace Independent Publishing Platform, 2014; ISBN 978-1-4973-3220-1.
- Collins, R. Interaction Ritual Chains; Princeton University Press: Princeton, 2014; ISBN 978-0-691-12389-9.
- Earth Science Data Systems, N. ASTER Global Digital Elevation Model V003 | NASA Earthdata 2025.
- DataV GeoAtlas: Web-Based Geospatial Toolkit Series. Available online: https://datav.aliyun.com/portal/school/atlas/area_selector (accessed on 6 November 2025).
- 3D Model Library for 3ds Max (Aigei). Available online: https://www.aigei.com/3d/model/ (accessed on 8 November 2025).
- Peng, W.; Jin, C.; Chen, X.; Wang, X. Assessing Urban Human Settlement Quality via Ecological Niche-Fitness: A Case Study of Wuhan Metropolitan Area. Sustainability 2025, 17, 9578. [Google Scholar] [CrossRef]
- Amap Open Platform: Amap Maps API. Available online: https://lbs.amap.com/ (accessed on 8 November 2025).
- Stichler, J.F.; Hamilton, D.K. Evidence-Based Design: What Is It? Herd 2008, 1, 3–4. [Google Scholar] [CrossRef] [PubMed]
- Alfonsi, E.; Capolongo, S.; Buffoli, M. Evidence Based Design and Healthcare: An Unconventional Approach to Hospital Design. Ann. Ig.: Med. Prev. Comunita 2014, 26, 137–143. [Google Scholar] [CrossRef]
- Edelstein, L. The Hippocratic Oath: Text, Translation and Interpretation; Johns Hopkins Press, 1943; ISBN 978-0-8018-0184-6. [Google Scholar]
- Helbing, D.; Molnár, P. Social Force Model for Pedestrian Dynamics. Phys. Rev. E 1995, 51, 4282–4286. [Google Scholar] [CrossRef]
- Drury, J.; Cocking, C.; Reicher, S. Everyone for Themselves? A Comparative Study of Crowd Solidarity among Emergency Survivors. Br J Soc Psychol 2009, 48, 487–506. [Google Scholar] [CrossRef]
- Rahgozar, N.; Rahgozar, N. Experimental and Numerical Investigation on Flexural Strengthening of Precast Concrete Corbel Connections with Fiber-Reinforced Plastic Sheet. Buildings 2024, 14, 387. [Google Scholar] [CrossRef]
- Rieke, N.; Hancox, J.; Li, W.; Milletarì, F.; Roth, H.R.; Albarqouni, S.; Bakas, S.; Galtier, M.N.; Landman, B.A.; Maier-Hein, K.; et al. The Future of Digital Health with Federated Learning. npj Digital Med. 2020, 3, 119. [Google Scholar] [CrossRef] [PubMed]
- Mandel, J.C.; Kreda, D.A.; Mandl, K.D.; Kohane, I.S.; Ramoni, R.B. SMART on FHIR: A Standards-Based, Interoperable Apps Platform for Electronic Health Records. J. Am. Med. Inf. Assoc. 2016, 23, 899–908. [Google Scholar] [CrossRef]
- API Document for Machine Translation | iFLYTEK Open Platform Documents. Available online: https://global.xfyun.cn/doc/nlp/xftrans/API.html#description-of-the-interface (accessed on 20 January 2026).
- Baichuan AI Baichuan Large Language Model Documentation. Available online: https://platform.baichuan-ai.com/docs/api (accessed on 20 January 2026).
- Shang, X.; Jiang, R.; Wong, S.C.; Gao, Z.; Weng, W. Advancing Lane Formation and High-Density Simulations in Bidirectional Flow: A Humanoid Pedestrian Model Incorporating Gait Dynamics and Body Rotation. Transportation Research Part C: Emerging Technologies 2025, 174, 105086. [Google Scholar] [CrossRef]
- Yang, J.; Zang, X.; Chen, W.; Luo, Q.; Wang, R.; Liu, Y. Improved Social Force Model Based on Pedestrian Collision Avoidance Behavior in Counterflow. Physica A: Statistical Mechanics and its Applications 2024, 642, 129762. [Google Scholar] [CrossRef]
- Deighan, M.T.; Ayobi, A.; O’Kane, A.A. Social Virtual Reality as a Mental Health Tool: How People Use VRChat to Support Social Connectedness and Wellbeing. In Proceedings of the Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems; Association for Computing Machinery: New York, NY, USA, April 19 2023; pp. 1–13. 1–13.
- Wang, Y.; Duan, B.; Chen, X.; Song, Y.; Liu, X. The Application of Metaverse in Mental Health. Front. Public Health 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Stefanidi, Z.; Margetis, G.; Ntoa, S.; Papagiannakis, G. Real-Time Adaptation of Context-Aware Intelligent User Interfaces, for Enhanced Situational Awareness. IEEE Access 2022, 10, 1–1. [Google Scholar] [CrossRef]
- Carrera-Rivera, A.; Larrinaga, F.; Lasa, G.; Martinez-Arellano, G.; Unamuno, G. AdaptUI: A Framework for the Development of Adaptive User Interfaces in Smart Product-Service Systems. User Modeling and User-Adapted Interaction 2024, 34, 1929–1980. [Google Scholar] [CrossRef]
- Hatfield, E.; Cacioppo, J.T.; Rapson, R.L. Emotional Contagion; Cambridge University Press: Cambridge, 2002; ISBN 978-0-521-44948-9. [Google Scholar]
- Helbing, D.; Farkas, I.; Vicsek, T. Simulating Dynamical Features of Escape Panic. Nature 2000, 407, 487–490. [Google Scholar] [CrossRef]
- McCrae, R.R.; Jr, P.T.C. Personality in Adulthood: A Five-Factor Theory Perspective; The Guilford Press: New York, NY, 2006; ISBN 978-1-59385-260-3. [Google Scholar]
Figure 1.
Figure 1. Research framework and process.
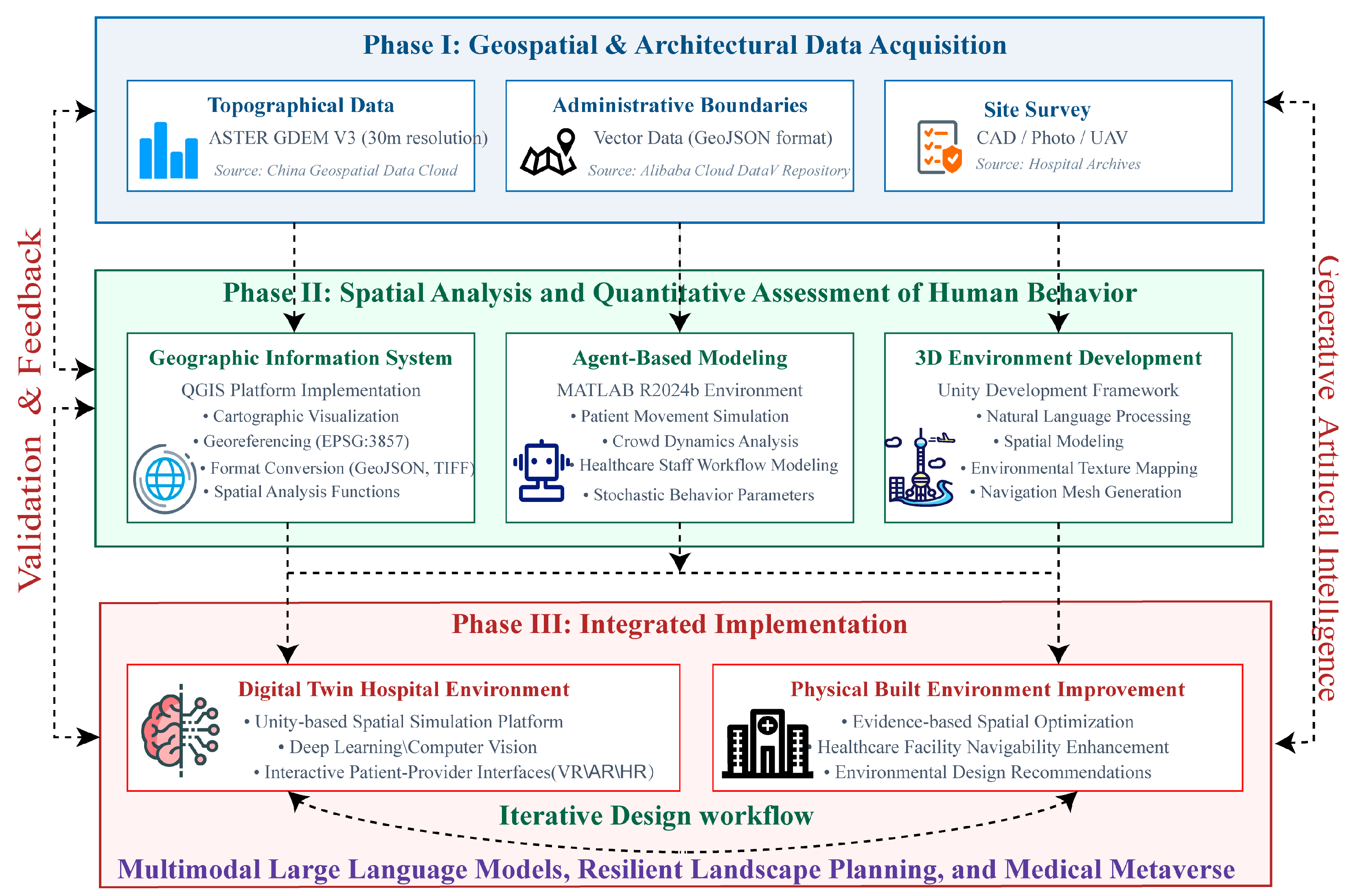
Figure 2.
Figure 2. Location of Puge County People’s Hospital and its regional context.
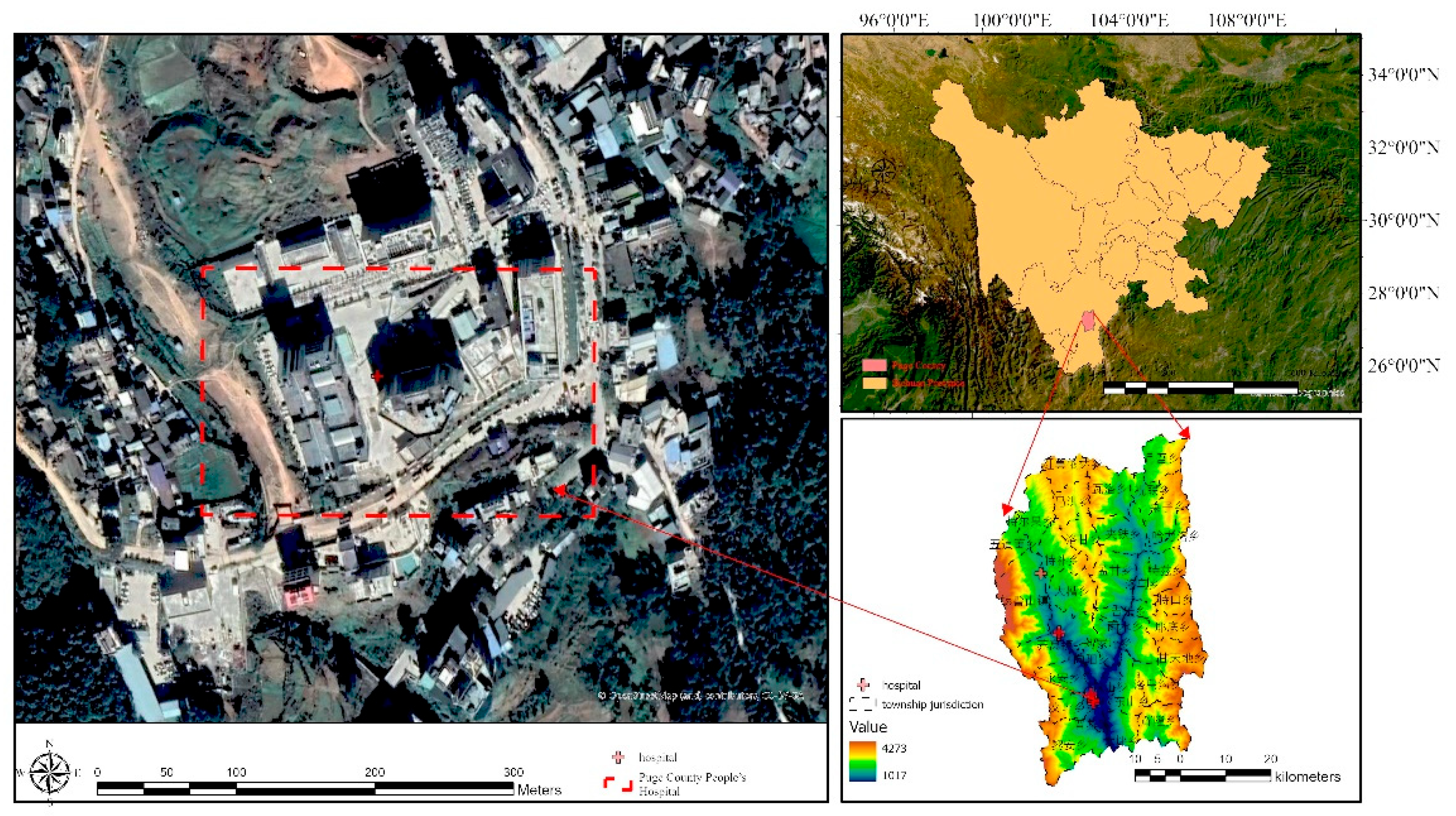
Figure 3.
Figure 3. The traditional ‘Duoluohe’ dance performed during the Puge Torch Festival. Photo courtesy of the Puge County Government.
Figure 3.
Figure 3. The traditional ‘Duoluohe’ dance performed during the Puge Torch Festival. Photo courtesy of the Puge County Government.

Figure 4.
Figure 4. Evidence-based design framework linking problem diagnosis to design interventions.
Figure 4.
Figure 4. Evidence-based design framework linking problem diagnosis to design interventions.
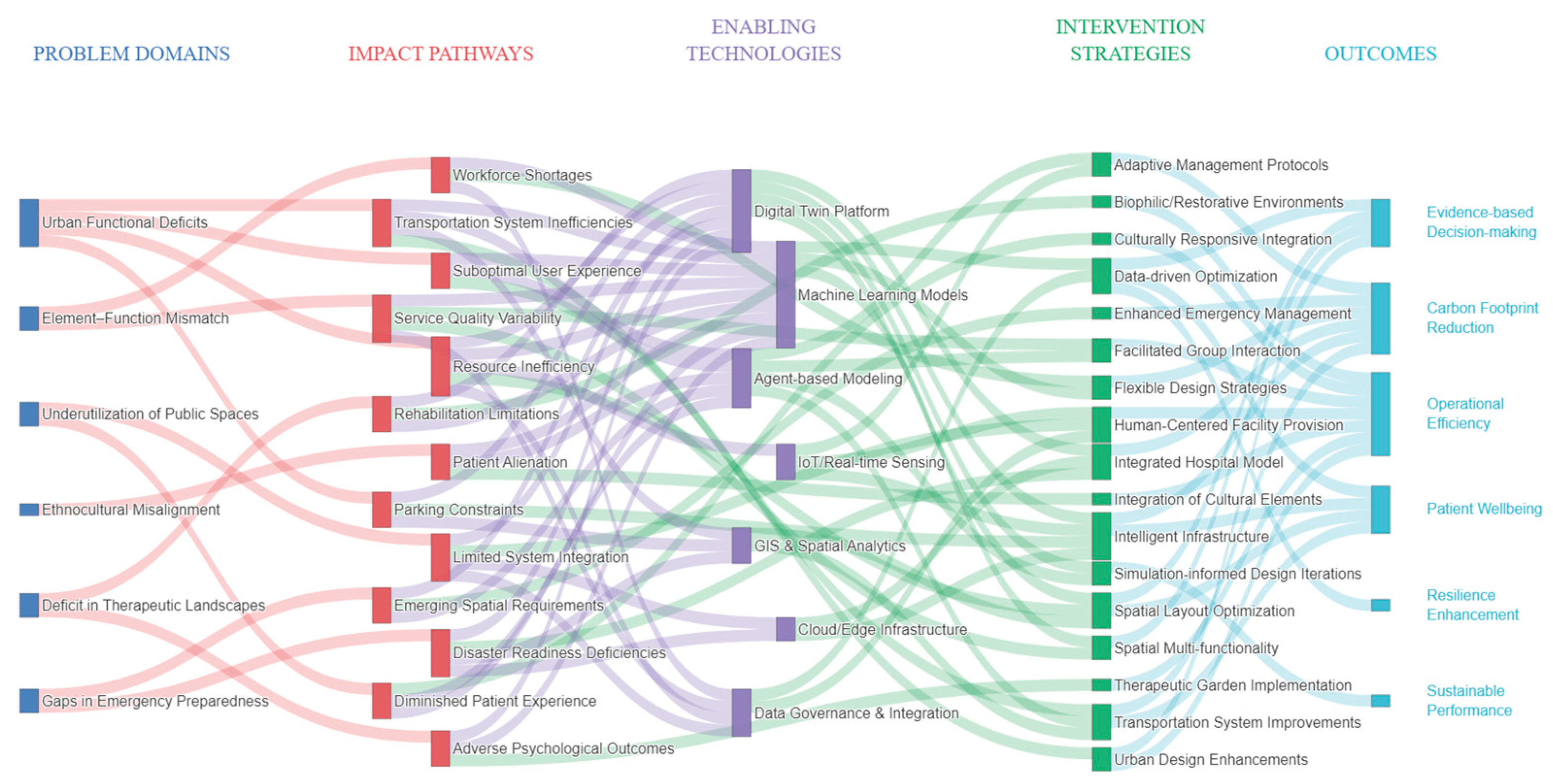
Figure 5.
Figure 5. Convergence behavior of the Q-learning algorithm during training. The blue curve represents the mean evacuation steps, exhibiting a decreasing trend, while the green curve denotes the evacuation success rate, which increases and stabilizes after approximately 100 episodes. Shaded regions indicate ±1 standard deviation across 20 independent runs, highlighting the stability of the learned policy.
Figure 5.
Figure 5. Convergence behavior of the Q-learning algorithm during training. The blue curve represents the mean evacuation steps, exhibiting a decreasing trend, while the green curve denotes the evacuation success rate, which increases and stabilizes after approximately 100 episodes. Shaded regions indicate ±1 standard deviation across 20 independent runs, highlighting the stability of the learned policy.
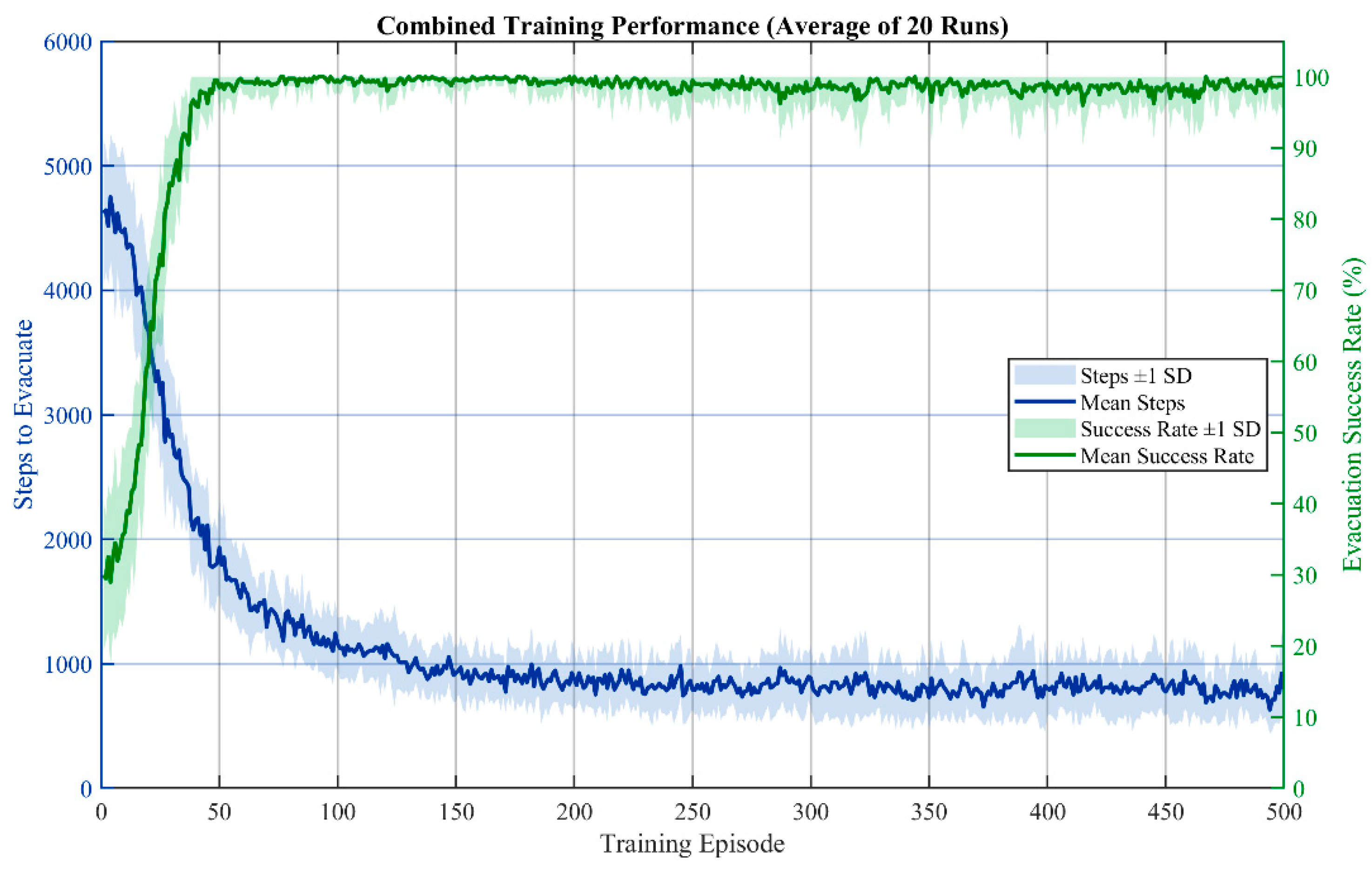
Figure 6.
Figure 6. Proposed System Architecture of the Medical Metaverse Platform. The proposed framework establishes a cloud-native computational platform designed to synchronize physical hospital environments with their digital counterparts through a robust human-in-the-loop architecture. At the sensing frontier, the Perception and Data Ingestion layer utilizes IoT and edge sensing technologies, including RTLS tags, wearables, and smart CCTV, to capture high-frequency environmental and physiological data streams. These multi-source data are ingested via a Kafka/Flink-based middle tier, which functions as a concurrent gateway. This setup ensures that data is simultaneously routed to a centralized Data Warehouse (archiving EMR, medical imaging, and demographics) for longitudinal analysis and to real-time processing pipelines for immediate operational response.
Figure 6.
Figure 6. Proposed System Architecture of the Medical Metaverse Platform. The proposed framework establishes a cloud-native computational platform designed to synchronize physical hospital environments with their digital counterparts through a robust human-in-the-loop architecture. At the sensing frontier, the Perception and Data Ingestion layer utilizes IoT and edge sensing technologies, including RTLS tags, wearables, and smart CCTV, to capture high-frequency environmental and physiological data streams. These multi-source data are ingested via a Kafka/Flink-based middle tier, which functions as a concurrent gateway. This setup ensures that data is simultaneously routed to a centralized Data Warehouse (archiving EMR, medical imaging, and demographics) for longitudinal analysis and to real-time processing pipelines for immediate operational response.
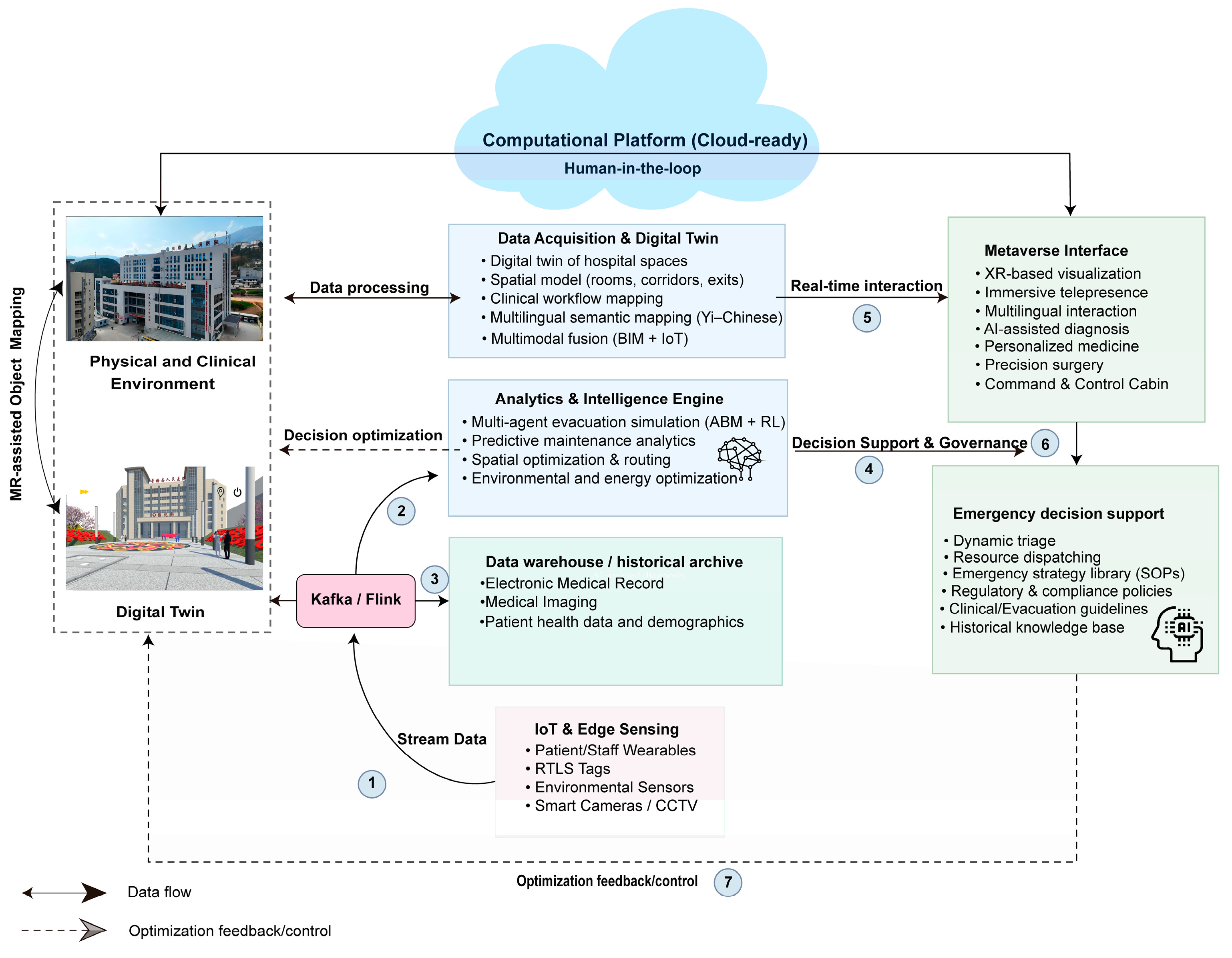
Figure 7.
XR-Based Immersive Visualization of the Hospital Digital Twin. A user interacts with the medical metaverse platform through a head-mounted display (HMD), navigating a 360° panoramic view of the digitalized hospital environment. The system enables real-time spatial exploration, emergency route planning, and interactive decision-making within the virtual replica of the physical healthcare facility.
Figure 7.
XR-Based Immersive Visualization of the Hospital Digital Twin. A user interacts with the medical metaverse platform through a head-mounted display (HMD), navigating a 360° panoramic view of the digitalized hospital environment. The system enables real-time spatial exploration, emergency route planning, and interactive decision-making within the virtual replica of the physical healthcare facility.

Figure 8.
Yi-Chinese Bilingual Medical Metaverse Interface. (a) Virtual hospital entrance with Yi cultural elements; (b) Bilingual patient registration system; (c) Interactive health education module; (d) Multilingual information board; (e) Virtual healthcare assistant with natural language support; (f) Emergency evacuation simulation scenario.
Figure 8.
Yi-Chinese Bilingual Medical Metaverse Interface. (a) Virtual hospital entrance with Yi cultural elements; (b) Bilingual patient registration system; (c) Interactive health education module; (d) Multilingual information board; (e) Virtual healthcare assistant with natural language support; (f) Emergency evacuation simulation scenario.
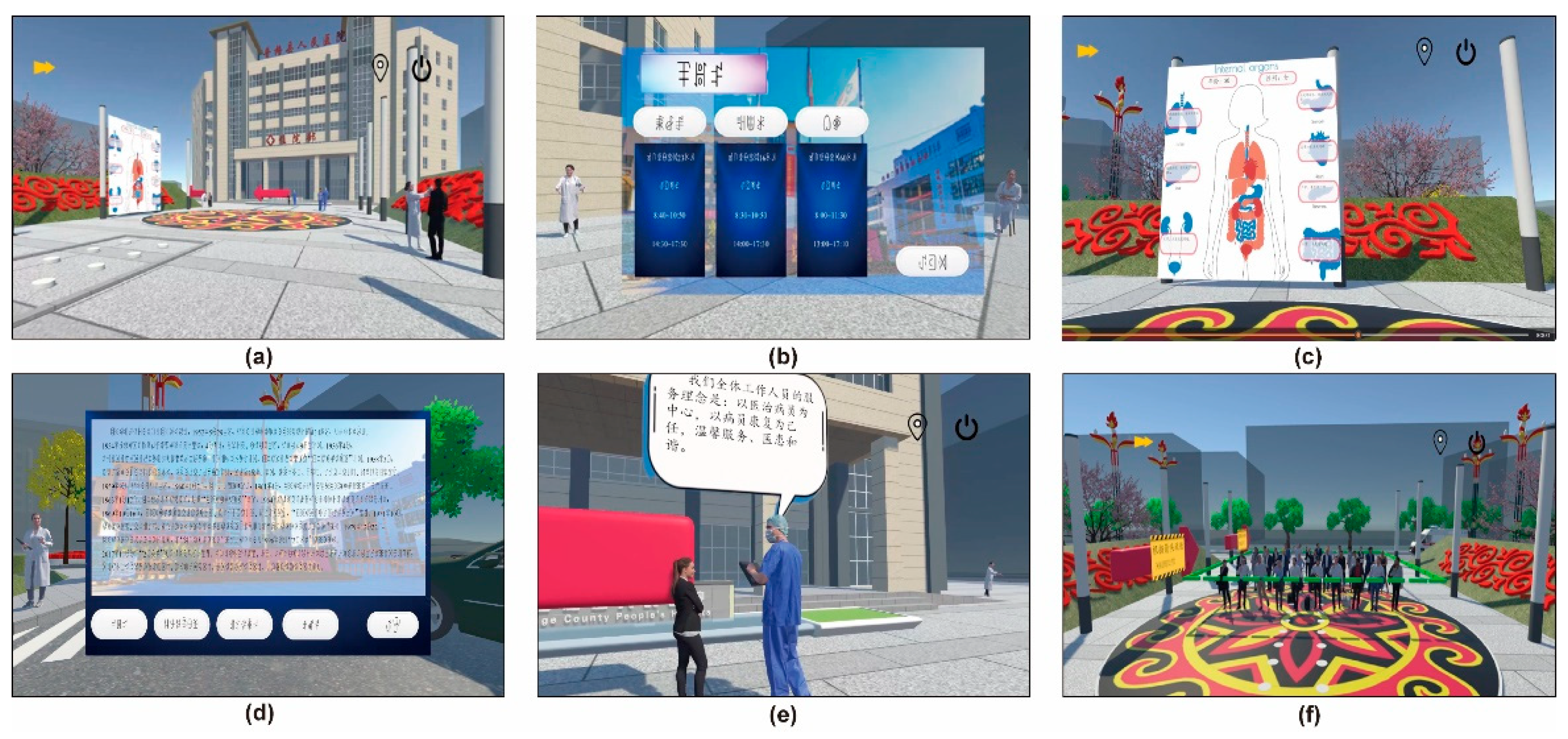
Figure 9.
Comparative analysis of evacuation trajectory patterns. (a–c) Baseline Random Walk scenarios for Doctors, Nurses, and Patients, exhibiting high-entropy stochastic movement and significant path redundancy. (d–f) Optimized Q-learning scenarios, where agents demonstrate streamlined, goal-oriented navigation. Note the significant reduction in trajectory dispersion for Patients (f) compared to the baseline (c), indicating enhanced safety for vulnerable groups.
Figure 9.
Comparative analysis of evacuation trajectory patterns. (a–c) Baseline Random Walk scenarios for Doctors, Nurses, and Patients, exhibiting high-entropy stochastic movement and significant path redundancy. (d–f) Optimized Q-learning scenarios, where agents demonstrate streamlined, goal-oriented navigation. Note the significant reduction in trajectory dispersion for Patients (f) compared to the baseline (c), indicating enhanced safety for vulnerable groups.
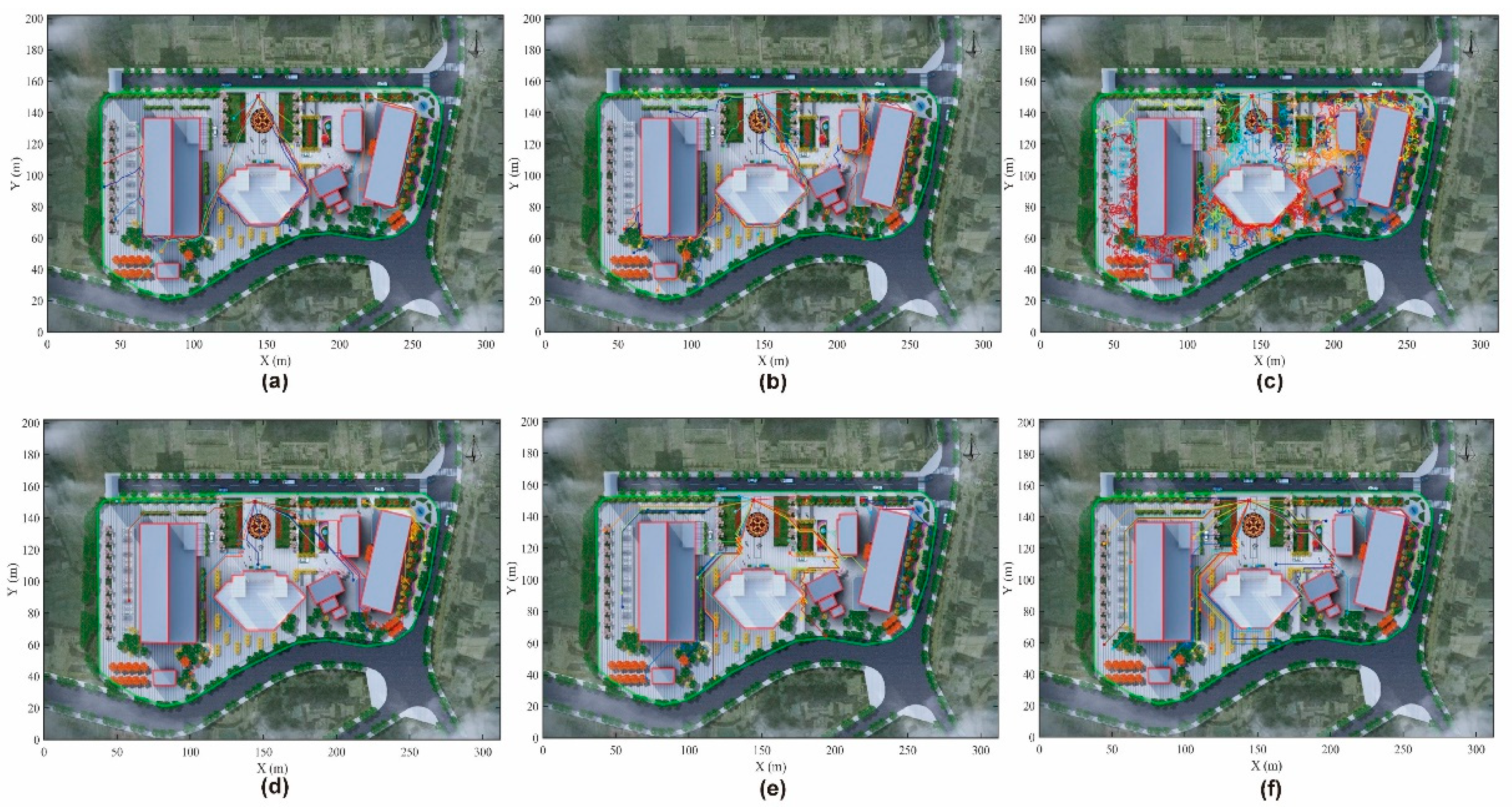
Figure 10.
Comparative Crowd Density Heatmaps under Random Walk (Top) vs. Q-Learning (Bottom). The color scale is saturated at 3.0 agents/m² to visualize low-density trails. (a–c) Baseline Scenario: Agents exhibit diffuse, high-entropy dispersion across the entire campus, indicating disorientation. (d–f) Optimized Scenario: Trajectories converge into efficient streamlines. Notably, while Doctors (d) maintain free-flow conditions (blue), Patients (f) generate distinct congestion hotspots (red/orange) at key intersections, revealing critical architectural bottlenecks despite optimized routing.
Figure 10.
Comparative Crowd Density Heatmaps under Random Walk (Top) vs. Q-Learning (Bottom). The color scale is saturated at 3.0 agents/m² to visualize low-density trails. (a–c) Baseline Scenario: Agents exhibit diffuse, high-entropy dispersion across the entire campus, indicating disorientation. (d–f) Optimized Scenario: Trajectories converge into efficient streamlines. Notably, while Doctors (d) maintain free-flow conditions (blue), Patients (f) generate distinct congestion hotspots (red/orange) at key intersections, revealing critical architectural bottlenecks despite optimized routing.
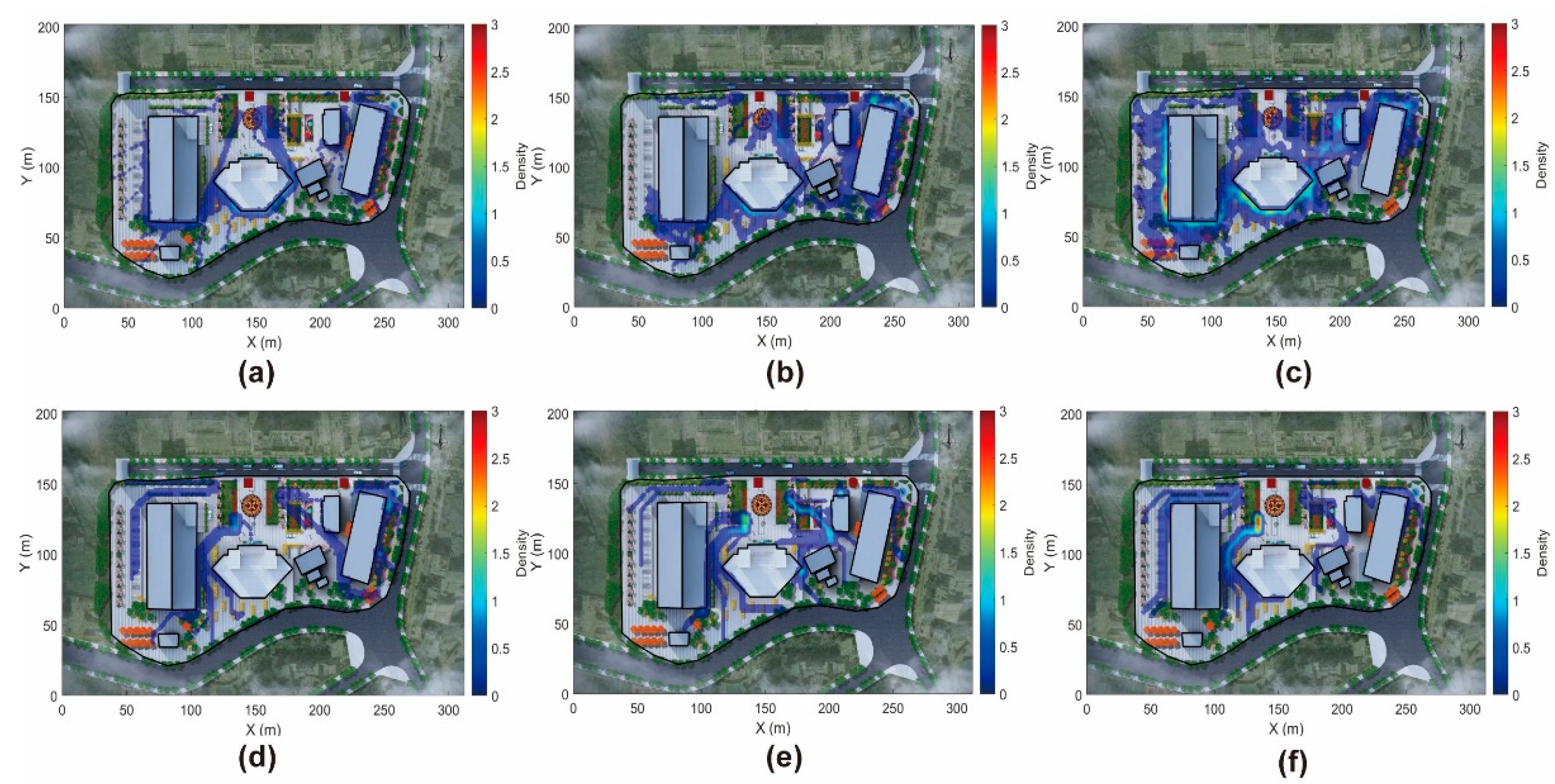
Figure 11.
Trajectory Overlay Analysis of the "Guiding Effect". Bold red lines represent Nurse agents (Guides), while thin green lines represent Patient agents (Followers). The spatial alignment of green trajectories with red paths illustrates the emergent flocking behavior, demonstrating how medical staff effectively anchor and streamline the movement of vulnerable occupants through complex intersections.
Figure 11.
Trajectory Overlay Analysis of the "Guiding Effect". Bold red lines represent Nurse agents (Guides), while thin green lines represent Patient agents (Followers). The spatial alignment of green trajectories with red paths illustrates the emergent flocking behavior, demonstrating how medical staff effectively anchor and streamline the movement of vulnerable occupants through complex intersections.
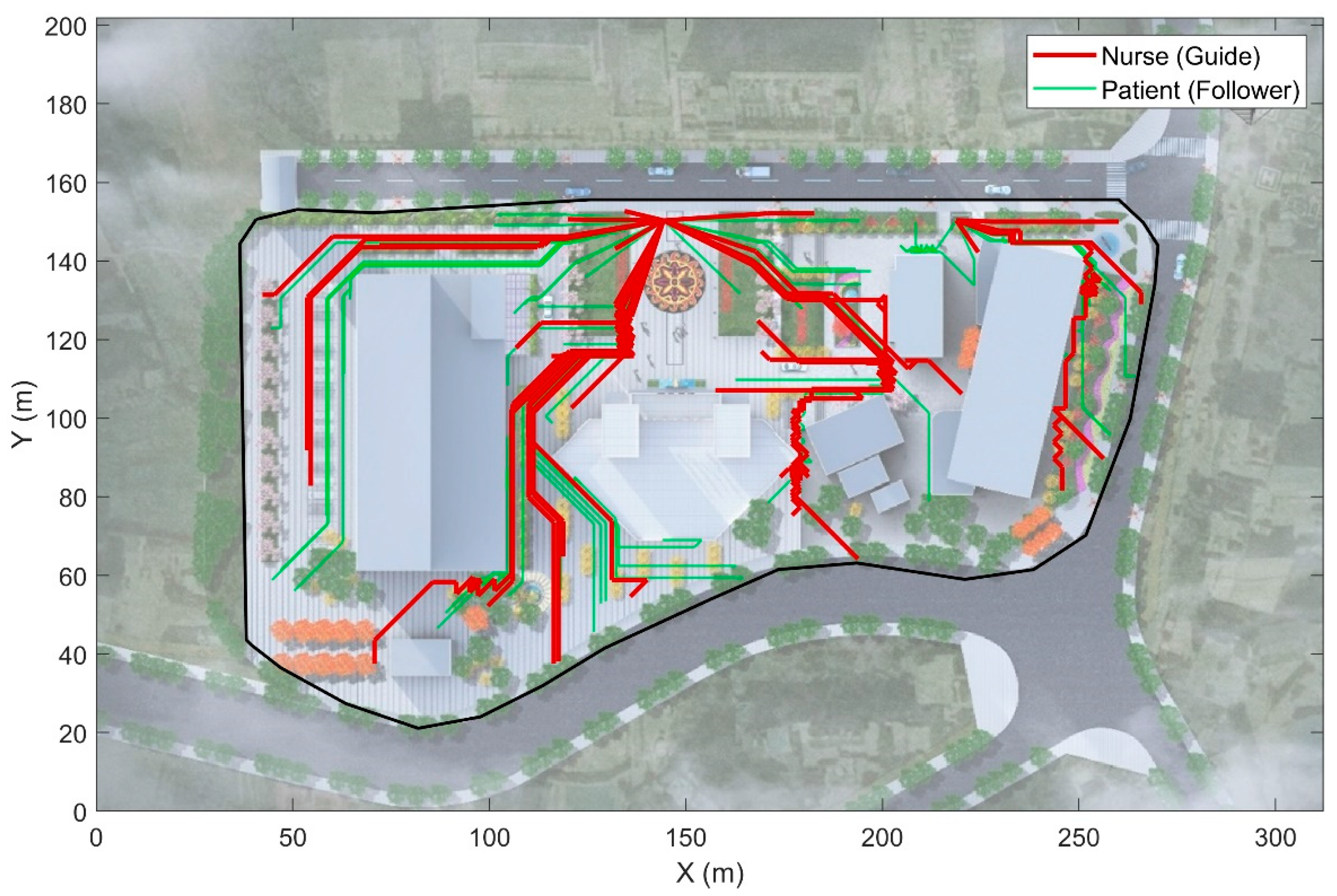
Figure 12.
Figure 12. Quantitative comparison of evacuation efficiency between the proposed Q-learning strategy and the Random Walk baseline. (a) Probability density distributions of evacuation time. The Q-learning curve (blue) exhibits a distinct leftward shift compared to the baseline (orange), indicating faster average performance. (b) Cumulative evacuation probability curves. The AI-driven strategy achieves a
Figure 12.
Figure 12. Quantitative comparison of evacuation efficiency between the proposed Q-learning strategy and the Random Walk baseline. (a) Probability density distributions of evacuation time. The Q-learning curve (blue) exhibits a distinct leftward shift compared to the baseline (orange), indicating faster average performance. (b) Cumulative evacuation probability curves. The AI-driven strategy achieves a
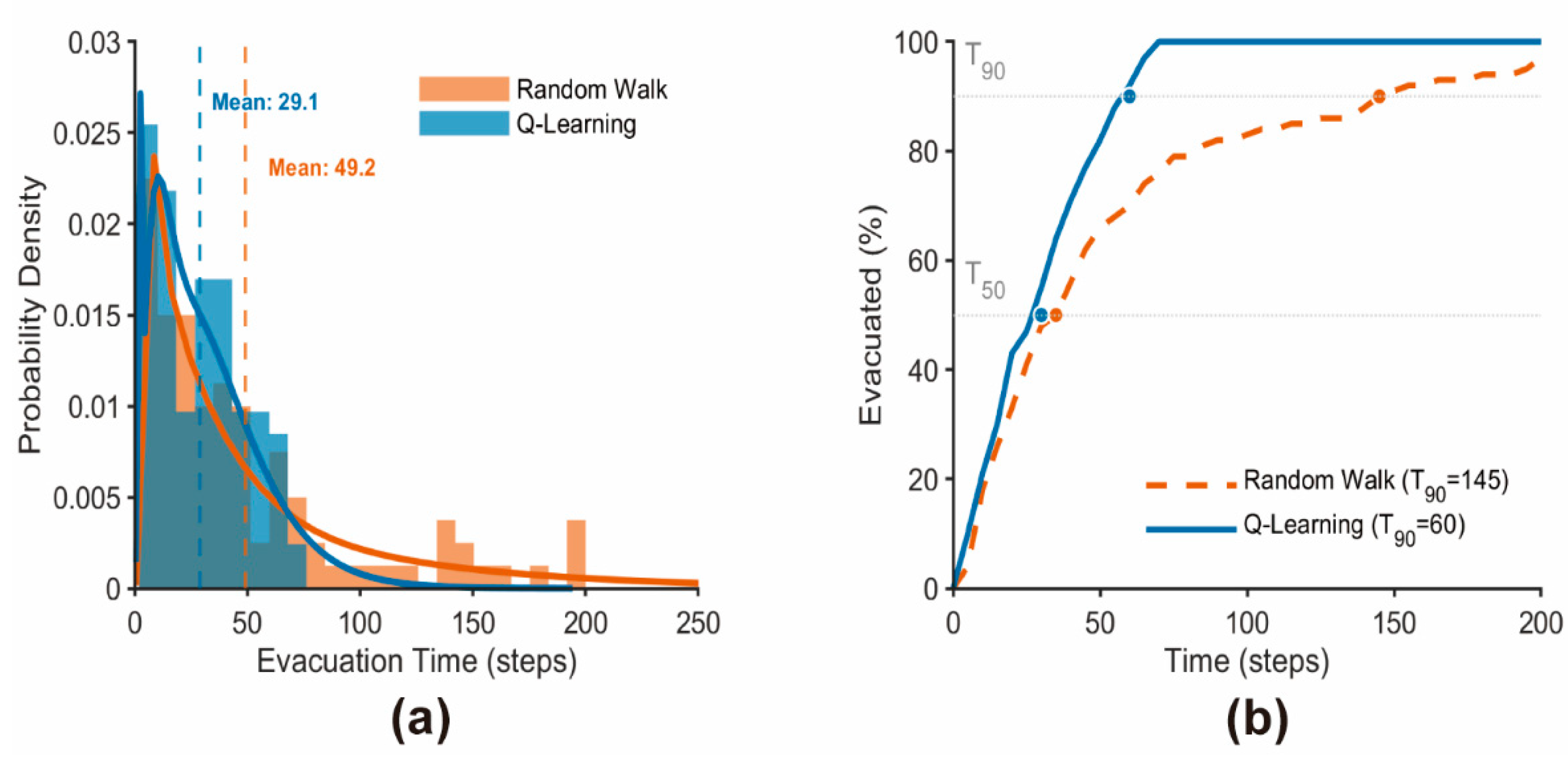
Figure 13.
Figure 13. Comparison of exit utilization patterns. While the Random Walk strategy (orange) leads to a quasi-random distribution between exits, the Q-Learning algorithm (blue) demonstrates strategic preference, effectively directing the majority of evacuees to the high-capacity primary exit (Exit 1) to maximize global evacuation efficiency.
Figure 13.
Figure 13. Comparison of exit utilization patterns. While the Random Walk strategy (orange) leads to a quasi-random distribution between exits, the Q-Learning algorithm (blue) demonstrates strategic preference, effectively directing the majority of evacuees to the high-capacity primary exit (Exit 1) to maximize global evacuation efficiency.
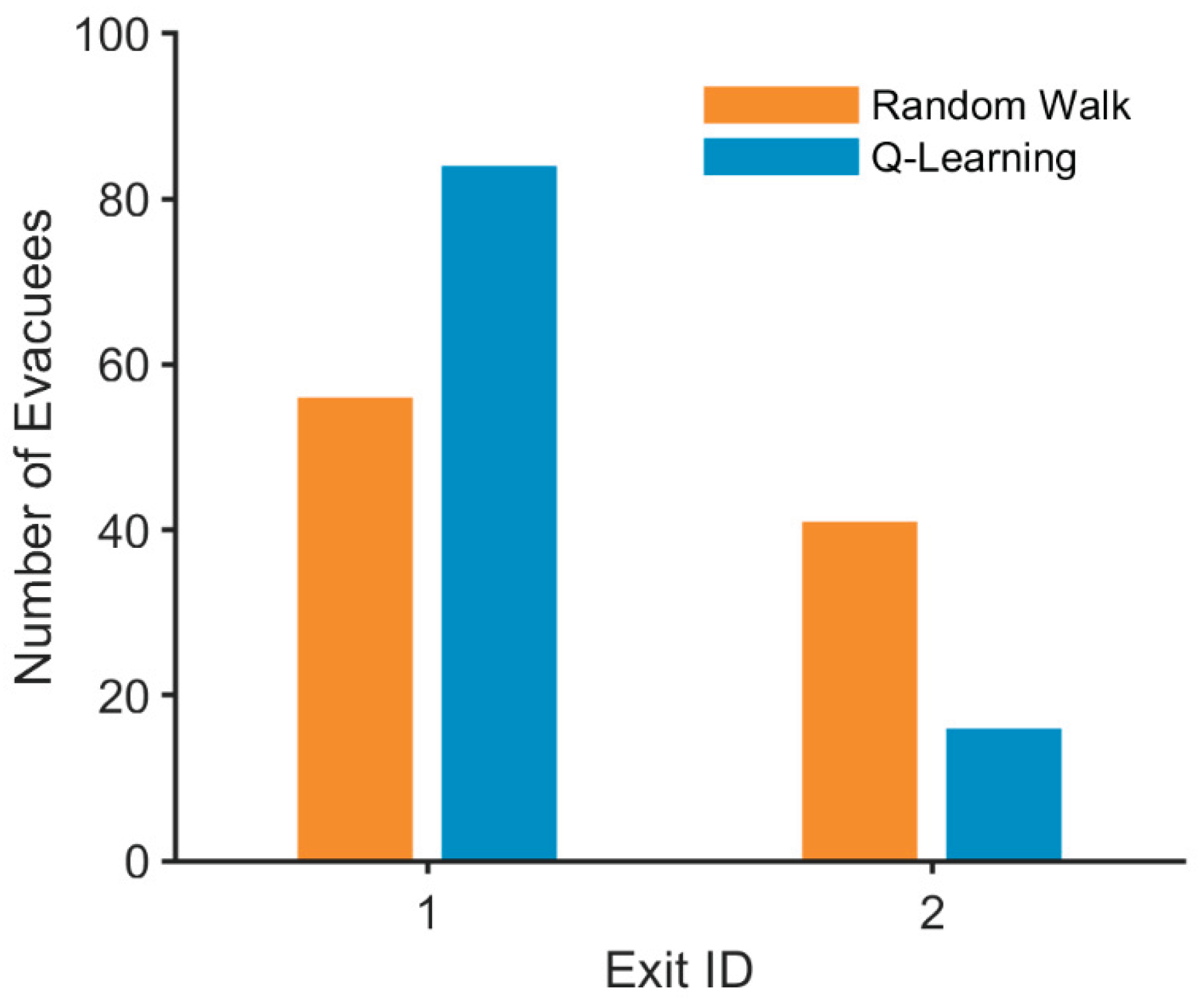

Table 1.
Stimulation Parameters for Agent Heterogeneity.
| Role | Speed Multiplier | Exit Knowledge | Behavioral Traits |
|---|---|---|---|
| Doctor | High (≈0.9) | Helping / Rescue | |
| Nurse | Medium (≈0.7) | Guiding / Flocking | |
| Patient | Low (≈0.2–0.5) | Following / Panic |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



