
Submitted:
30 January 2026
Posted:
04 February 2026
You are already at the latest version
Abstract
Background: Hyperbaric oxygen therapy (HBOT) has regenerative effects in various tissues, but its impact on hair follicles is unclear. This preliminary study evaluated HBOT-induced changes in hair and scalp characteristics in healthy adults. Methods: Nine healthy volunteers completed 50 HBOT sessions over three months (2.0 ATA, 100% oxygen, 90 minutes per session). Objective assessments included follicle density, hairs per follicle, hair volume, and shaft thickness using the Becon phototrichogram system. Subjective evaluations were conducted via a 7-point Likert questionnaire on scalp appearance, hair density, thickness, growth, and shedding. Pre- and post-treatment data were compared using paired statistical tests. Results: Positive trends were observed in follicle density (61.3→66.8 counts/cm²), hairs per follicle (1.24→1.33), and hair volume (24.9→27.7%), though not statistically significant. Hair shaft thickness decreased significantly (0.18→0.10 mm, p=0.011), consistent with early anagen-phase regrowth. Subjective assessments showed significant improvements across all domains (p<0.05). Scalp imaging visually supported these findings. Conclusions: HBOT may enhance hair follicle activation and scalp health in healthy adults. These preliminary findings justify further controlled studies to explore HBOT as a non-pharmacological approach to hair regeneration.
Keywords:
hyperbaric oxygen therapy
; hair follicle
; hair growth
; phototrichogram
; tissue regeneration
1. Introduction
Hair and hair follicles are biologically significant structures that play a crucial role in thermoregulation, protection, and sensory function. Although hair loss is not a life-threatening condition, it can have profound psychological and emotional consequences, significantly affecting an individual’s quality of life. [1,2] Alopecia can occur regardless of age or gender, and the incidence of depression among patients with hair loss has been reported to be notably high. The formation of hair begins with the development of the initial hair follicles from the epidermis. Hair growth follows a well-defined cycle consisting of the anagen (growth), catagen (regression), telogen (resting), and subsequent return to anagen phases. Disruption of this cycle may result in various types of hair loss, with causes including hormonal imbalances, immune system dysfunction, nutritional deficiencies, certain medications, childbirth, high fever, surgery, or psychological stress. [3] Among these, androgenetic alopecia—commonly known as male-pattern hair loss—is the most prevalent form. It is primarily driven by the action of dihydrotestosterone (DHT), a metabolite of testosterone, which causes miniaturization of hair follicles. Currently, FDA-approved treatments include oral finasteride and topical minoxidil. [4,5] Other types of hair loss include telogen effluvium, which often occurs after childbirth or extreme dieting, and alopecia areata, which is related to autoimmune dysfunction. These conditions often improve upon the resolution of the underlying causes. However, senile alopecia associated with aging lacks effective treatments and is generally managed through lifestyle modifications, as it stems from a diminished regenerative capacity of hair follicles.
Hyperbaric oxygen therapy (HBOT) involves inhaling 100% oxygen at pressures exceeding 1.4 absolute atmospheres (ATA). [6,7] HBOT was initially introduced in the 1960s to treat acute carbon monoxide poisoning in Korea. HBOT is recognized for its clinical benefits, including wound healing, radiation injury, and chronic infections, resulting from its effects on tissue oxygenation, inflammation modulation, and cell regeneration. In Korea, the widespread installation of HBOT chambers in the 1980s declined over time due to shifts in the source of the heating fuel and limited clinical application beyond carbon monoxide intoxication. [8]
The Undersea and Hyperbaric Medical Society (UHMS) recommends therapeutic administration of hyperbaric oxygen therapy (HBOT) at pressures between 2.0 and 3.0 Atmospheres Absolute (ATA) for 90 to 120 minutes for most medical indications. Despite the proven benefits of HBOT in tissue regeneration and inflammation control, few studies have examined its potential effects on hair follicle physiology. Emerging evidence suggests that the secondary mechanisms of HBOT, such as anti-hypoxia effects, capillary regeneration, and mitigation of ischemia-reperfusion injury, may extend benefits to other tissues, including the scalp. [9] These mechanisms have demonstrated efficacy in treating spinal cord injuries and compromised skin grafts or flaps, suggesting a potential role in supporting hair follicle health and promoting hair regrowth. [10] Given this background, the present study aims to evaluate the effects of hyperbaric oxygen therapy on hair follicles and hair characteristics in healthy adult subjects. By analyzing pre- and post-therapy morphological changes, this research seeks to explore the regenerative potential of HBOT in a novel domain and assess its implications for both medical and aesthetic applications.
2. Materials and Methods
2.1. Study Design and Ethical Approval
This study is a prospective, preliminary clinical trial involving 50 sessions of hyperbaric oxygen therapy (HBOT) conducted over three months in nine healthy adult participants at two HBOT centers. It was designed to observe and analyze changes in the condition of hair follicles and hair following HBOT. This study is a prospective, preliminary clinical trial conducted over three months at two HBOT centers, involving a total of 50 HBOT sessions in nine healthy adult participants. Initially, 16 volunteers were screened for eligibility; however, three individuals were excluded during the screening process (one due to claustrophobia and two due to personal reasons), and four participants were lost to follow-up before completing the intervention, resulting in a final cohort of nine participants. This study hypothesized that the secondary mechanisms of hyperbaric oxygen therapy, such as the anti-hypoxic effect and the promotion of capillary regeneration, could aid hair follicle cell regeneration by enhancing peripheral oxygen supply and promoting tissue regeneration.
The study was approved by the approval of the Yonsei University Wonju Severance Christian Hospital Research Ethics Committee (IRB approval number: CR322058), as well as by the Public Institutional Review Board designated by the Ministry of Health and Welfare of Korea (approval number: P01-202311-01-005). Along with obtaining IRB approval, it was registered with the Clinical Research Information Service (CRIS) (Trial Registration No.: KCT0011058), which is a primary registry of the WHO International Clinical Trials Registry Platform (ICTRP) and thus ensures international compatibility. This clinical study complied with the International Conference on Harmonization (ICH) Guidelines and the principles of the Declaration of Helsinki, and was conducted in accordance with the Korean Good Clinical Practice (KGCP) and related regulations, taking into account the rights and safety of the subjects. All participants provided written informed consent.
2.2. Medical Device and HBOT Protocol for Clinical Trials
A hyperbaric oxygen chamber, IBEX LIGHT (IBEX Medical Systems Co., Ltd., Republic of Korea), was used to administer hyperbaric oxygen therapy (HBOT). This single-person, medical-grade monoplace chamber is designed for clinical applications. It delivers 100% oxygen at pressures up to 2 atmospheres absolute (ATA), making it suitable for enhanced tissue oxygenation conditions. We utilized the hyperbaric oxygen treatment protocol number 9, which was established by the US Navy. We modified it by lowering the target pressure to 2.0 ATA, shortening the treatment time, and gradually increasing and decreasing the pressure over 15 minutes, allowing patients to adapt to the pressure change smoothly (Figure 1). [11]
2.3. Phototrichogram Analysis Using the Becon System (Quantitative Evaluation)
The Becon system (Becon AI Scanner, Becon Co., Ltd., Seoul, Republic of Korea) was employed to perform phototrichogram-based scalp analysis. This digital diagnostic tool is equipped with an optical camera and multiple integrated sensors, enabling the real-time capture of high-resolution scalp images at 30 frames per second. [12] The system simultaneously assesses scalp and hair health by measuring parameters such as scalp temperature, moisture levels, and volatile organic compounds (VOCs), which serve as indicators of heat, dryness, odor, and sensitivity. The device wirelessly connects to a dedicated mobile or tablet application, which processes and analyzes the collected data. A high-magnification (20×) lens provides detailed imaging of the scalp surface, while embedded biosensors acquire biological signals that are translated into clinically relevant diagnostic metrics through proprietary software. The Becon system evaluates 11 scalp health parameters, among which four key indicators are directly related to hair loss: follicle density, number of hairs per follicle, hair thickness, and hair volume. [13,14]
- Follicle density refers to the number of follicles per square centimeter (cm²), automatically assessed using machine learning algorithms. Higher density indicates healthier, fuller hair, while low density suggests thinning.
- Number of hairs per follicle measures how many hairs emerge from a single follicle. The system uses color-coded visualization (e.g., red for one hair, yellow for two, green for three) to aid interpretation. A greater number of hairs per follicle is indicative of healthier hair.
- Hair thickness is automatically calculated across all visible strands within a 1 cm² area and reported as an average in millimeters. Thicker hairs suggest better hair health and coverage.
- Hair volume (coverage) is presented as a percentage, representing the visible amount of hair within a 1 cm² area.
To evaluate the severity of hair loss, the Becon system compares measurements from two regions: a "Healthy Scalp Area" and a "Scalp Concern Area". Each of the four metrics is compared between the two areas. Based on the cumulative difference in the four metrics, a comprehensive Health Loss Health Score is generated, ranging from 0 to 100. Depending on the degree of deviation, the system categorizes the result as “Healthy (85 points and above),” “Good (65 to 84 points),” “Caution (36 to 64 points),” or “Warning (35 points and below).” Finally, the Becon system enables longitudinal tracking of scalp and hair conditions. It monitors changes in follicle density, hair count per follicle, hair thickness, and overall coverage over time, providing precise visual and quantitative data on improvement or deterioration across treatment sessions.
2.4. Questionnaire (Qualitative Evaluation)
Table 1 shows the hair condition (scalp appearance, crown, amount of hair, hair thickness, hair growth rate, and frontal hairline) before and after hyperbaric oxygen therapy was evaluated using a 7-point Likert scale from “very worse (1 point)” to “very improved (7 points).”
2.5. Study Flow and Protocol Overview
The overall study protocol was structured into three main phases: pre-screening and baseline assessment, HBOT intervention, and final evaluation (Figure 2). Participants were recruited based on specific inclusion criteria, including adults aged 19 to 65 who were capable of undergoing HBOT in a hyperbaric monochamber, with no history of hair loss diagnosis or treatment in the previous six months. Exclusion criteria included pregnancy, incarceration, institutionalization, contraindications for HBOT, and possession of specific medical devices. During the screening and baseline phases, participants underwent a comprehensive physical examination, a medical history review, and safety assessments, including otoscopic and cardiovascular evaluations. Scalp and hair condition were objectively assessed using the Becon phototrichogram system, and subjective perceptions were recorded through structured questionnaires. The HBOT intervention was administered at 2.0 ATA (atmospheres absolute) with 100% oxygen for 90 minutes per session (15 minutes compression, 60 minutes oxygenation, 15 minutes decompression), at least four times a week for a total of 50 sessions over three months. All treatments were conducted in a controlled chamber environment, with safety protocols strictly followed, including pre-treatment education on pressure equalization techniques and restrictions on prohibited items. After completing the 3-month intervention, participants underwent the same evaluations as those conducted during the baseline phase to assess changes in hair and scalp condition, subjective perceptions, and to monitor for any adverse effects. This structured flow ensured both clinical safety and methodological consistency throughout the study.
2.6. Statistical Analysis
Statistical analyses were conducted using SPSS Statistics (Version 28.0, IBM Corp., Armonk, NY, USA). To evaluate the effects of hyperbaric oxygen therapy (HBOT), appropriate statistical tests were applied according to the type and distribution of each variable. For continuous variables (e.g., follicle density, hair per follicle, hair volume, hair thickness, and total score), normality was assessed using the Shapiro-Wilk test. If the data were normally distributed, a paired t-test was used to compare the means before and after HBOT. When normality was not satisfied, the non-parametric Wilcoxon signed-rank test was employed. For categorical variables (e.g., presence or absence of symptoms or complications), the McNemar test was used to assess changes in paired proportions before and after treatment. Subjective outcomes were evaluated using six self-reported items rated on a 7-point Likert scale (e.g., “The overall appearance of the scalp is improving”, “The crown of the head is growing longer”, “The amount of hair falling out is decreasing”, “The hair is getting thicker”, “The hair growth rate is getting faster”, and “The front hairline is improving”). Given the ordinal nature of these responses, pre- and post-treatment comparisons were conducted using the Wilcoxon signed-rank test. To visually illustrate changes in response patterns, frequency distribution plots were generated. All statistical tests were two-tailed, and a p-value of less than 0.05 was considered statistically significant. Statistical methods were reviewed and refined as necessary based on consultation with domain experts.
3. Results
Table 2 describes the characteristics and medical history of the participants. A total of nine healthy adult participants were enrolled in the study, comprising five females (55.6%) and four males (44.4%). The mean age was 39.3±10.8 years, and the median age was 37 years with an interquartile range (IQR) of 31.5 to 45 years. Age group distribution was as follows: one participant (11.1%) in their 20s, four (44.4%) in their 30s, three (33.3%) in their 40s, none in their 50s, and one (11.1%) in their 60s. All participants were free of known past medical conditions and did not undergo a physical examination, including anthropometric assessment and chest radiography, at the time of data collection.
3.1. Objective Evaluation of Hair Condition Before and After HBOT
To complement the subjective assessments, quantitative hair measurements were conducted before and after HBOT. As summarized in Table 3, the overall hair health score showed an increasing trend from 73.11±4.76 point to 75.44±3.88 point, although the change did not reach statistical significance (t=-1.871, p=0.098). A similar upward trend was observed in follicle density, which increased from 61.33±13.00 counts/cm² to 66.78±6.32 counts/cm² (t=-1.342, p=0.216), suggesting a potential enhancement in scalp follicular activity. Furthermore, the average number of hairs per follicle rose from 1.24±0.03 counts to 1.33±0.14 counts (t=-1.860, p=0.099), and hair volume increased from 24.89±3.63 % to 27.69±4.87 % (t=-1.880, p=0.097). While these changes were not statistically significant, the consistent directional improvements across multiple parameters may indicate a meaningful biological response to HBOT. Interestingly, a statistically significant reduction was observed in hair shaft thickness, decreasing from 0.18±0.08 mm to 0.10±0.02 mm (t=3.278, p=0.011). This finding may reflect early-stage hair regeneration, characterized by the production of thinner, newly growing hair shafts. Taken together, these objective measurements suggest a trend toward improved hair characteristics, reinforcing the positive outcomes observed in the subjective assessments.
The standardized scalp images were obtained using the Becon imaging system before and after the HBOT sessions to visually corroborate. As shown in Figure 3, a series of top-view photographs illustrates noticeable changes in scalp and hair condition across multiple participants. Consistent lighting and positioning allowed for reliable visual comparison between the pre- and post-treatment states. Post-HBOT images typically show a noticeable improvement in hair density and coverage, particularly in the vertex and crown areas. Several subjects display a reduction in scalp exposure and an increase in darkening or thickening of hair, suggesting improved follicular activity. These changes align with the quantitative trends observed in hair volume, follicle density, and subjective perception, thus reinforcing the therapeutic potential of HBOT for hair regeneration. While visual assessments are inherently qualitative, the consistency of improvement across a broad range of subjects further supports the positive impact of HBOT on scalp health and hair appearance.
3.2. Assessment for Improvement in Hair Condition Before and After HBOT
To assess subjective improvement in hair condition following hyperbaric oxygen therapy (HBOT), a structured questionnaire comprising six items was administered before and after the intervention. As shown in Figure 4, all questionnaire items demonstrated statistically significant improvement post-HBOT. Participants reported a substantial improvement in the overall appearance of the scalp, with mean scores increasing from 2.89±0.78 to 5.00±0.71 (Z=-2.687, p=0.007). Similarly, perceived hair growth at the crown of the head significantly improved (2.33±1.00 to 5.11±0.78; Z=-2.684, p=0.007). A notable reduction in hair shedding was also observed (2.78±0.97 to 5.00±1.00; Z=-2.536, p=0.011). Moreover, participants reported an increase in hair thickness (2.11±0.60 to 5.00±1.12; Z=-2.699, p=0.007) and hair growth rate (4.00±0.00 to 4.89±1.05; Z=-2.060, p=0.039). Improvement in the anterior hairline was also significant (3.78±0.44 to 4.78±0.97; Z=-2.060, p=0.039). These findings positively contribute to the overall outcomes of this study.
4. Discussion
This study investigated the potential regenerative effects of HBOT on hair and scalp health through both objective measurements and structured subjective assessments. Although most objective parameters, including overall hair health score, follicle density, hair volume, and the average number of hairs per follicle, did not reach statistical significance, they exhibited consistent positive trends following HBOT. Notably, a significant decrease in hair shaft thickness was observed, which may be indicative of early anagen-phase regrowth, where newly formed vellus or intermediate hairs are typically finer in diameter. This observation aligns with early signs of follicular reactivation. These findings are in concordance with prior studies that support the biological plausibility of HBOT in promoting hair regeneration. It demonstrated that normobaric hyperoxia significantly enhanced hair growth and delayed the catagen phase in mice, highlighting the importance of oxygen levels in follicular cycling.15 HBOT has been shown to upregulate angiogenic factors such as vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF), both of which are critical for maintaining perifollicular vascularization and follicle health.16, 17 Enhanced vascularity and oxygenation may thus create a favorable microenvironment for the activation of hair follicle stem cells and dermal papilla cells.18
Subjective assessments in this study revealed statistically significant improvements across all evaluated domains, including perceived hair density, thickness, reduced shedding, and improved anterior hairline. These self-reported outcomes are consistent, noting improvements in hair thickness and perifollicular microcirculation following HBOT in patients with alopecia areata.19 Furthermore, the observed enhancement in the frontal hairline, often refractory to conventional treatments such as topical minoxidil, suggests that HBOT may have a unique capacity to improve perfusion in typically unresponsive regions of the scalp.
Standardized scalp imaging using the Becon system provided visual corroboration of therapeutic effect, revealing apparent increases in hair density and coverage, particularly in the vertex and crown regions.20 These visual changes were consistent with both subjective feedback and objective data trends, further supporting the hypothesis that HBOT may contribute to follicular health and scalp rejuvenation.21 However, the use of photographic assessment also presents a potential source of variability. Factors such as lighting, camera angle, and hair dye could influence perceived changes, particularly in a study without a control group.22
Despite the promising nature of these findings, several limitations must be acknowledged. First and foremost, the small sample size (n=9) restricts the statistical power of the study and limits its generalizability. A larger cohort is needed to confirm these preliminary trends and to assess treatment efficacy more robustly. Second, the lack of a control group hinders the ability to attribute observed changes solely to HBOT. Without comparison to a placebo or non-treatment arm, potential placebo effects or confounding factors—such as seasonal hair changes or grooming habits—cannot be ruled out. Third, although the study involved 50 treatment sessions over three months, this duration may have been insufficient to observe the full extent of follicular transformation, particularly the conversion of vellus hairs into terminal hairs. Hair growth is a slow process, and longer follow-up periods are necessary to evaluate the sustainability and progression of treatment effects. Fourth, the HBOT protocol used in this study was adapted from the US Navy protocol rather than a dermatologically standardized regimen. This modification, intended to accommodate participant compliance and safety, may limit direct comparability with other HBOT studies and underscores the need for standardized treatment protocols in future trials. Fifth, the discrepancy between subjective improvement and largely non-significant objective findings (except hair shaft thickness) raises important questions. While the consistent positive trends across objective parameters suggest biological response, it is also possible that the subjective benefits were influenced by expectancy effects. Integrating histological analyses, such as scalp biopsies or trichoscopy, in future research could provide more definitive evidence of follicular regeneration at the cellular level. Sixth, while photographs offered a valuable visual tool for evaluating hair condition, the resolution was insufficient to demonstrate individual follicle-level changes. Additionally, hair dyeing status, which was not standardized, may have affected visual perception of hair thickness or color. Future studies should incorporate high-resolution imaging technologies and control for such variables to ensure more accurate visual assessment. Lastly, while no adverse effects (e.g., barotrauma, dizziness, oxygen toxicity) were reported during the intervention period, a formal evaluation and documentation of safety outcomes should be included in future research. Establishing a favorable safety profile is essential for broader clinical application.
Taken together, these limitations highlight the preliminary nature of the current study. However, the convergence of subjective improvements, positive trends in objective parameters, and visual enhancements supports the hypothesis that HBOT may play a supportive role in hair follicle activation and scalp health. Future studies should incorporate larger sample sizes, randomized controlled designs, histological validation, and extended follow-up periods to substantiate these early findings and clarify the clinical utility of HBOT in the field of trichology.
5. Conclusions
Hyperbaric oxygen therapy (HBOT) remains an underutilized modality in South Korea, largely due to limited awareness of its therapeutic potential. This study explored the effects of HBOT on hair and follicle health in healthy adults, revealing positive changes supported by both subjective perceptions and objective measures. These preliminary findings suggest that HBOT may contribute to scalp health and follicular activation, offering a promising non-pharmacological approach to hair care. While the current study had limitations, including a small sample size, absence of long-term follow-up, and use of a modified HBOT protocol, the observed trends warrant further investigation. Future research incorporating standard protocols, histological analysis, and inclusion of patients with alopecia will be essential to clarify the clinical applicability of HBOT in trichology.
Author Contributions
Conceptualization, S.C.K and Y.S.L.; methodology, S.C.K and Y.S.L; validation, J.Y.L..; formal analysis, H.Y.L.; investigation, J.Y.L..; data curation, S.C.K. and Y.S.L.; writing—original draft preparation, H.Y.L.; writing—review and editing, H.Y.L., J.Y.L. and Y.S.L.; supervision, Y.S.L.; project administration, S.C.K and Y.S.L.; funding acquisition, S.C.K and Y.S.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Excellent Young Researcher Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Science and ICT (MSIT) (Grant No.: RS-2025-00514272).
Institutional Review Board Statement
The study was approved by the approval of the Yonsei University Wonju Severance Christian Hospital Research Ethics Committee (IRB approval number: CR322058), as well as by the Public Institutional Review Board designated by the Ministry of Health and Welfare of Korea (approval number: P01-202311-01-005). Along with obtaining IRB approval, it was registered with the Clinical Research Information Service (CRIS) (Trial Registration No.: KCT0011058), which is a primary registry of the WHO International Clinical Trials Registry Platform (ICTRP) and thus ensures international compatibility. This clinical study complied with the International Conference on Harmonization (ICH) Guidelines and the principles of the Declaration of Helsinki, and was conducted in accordance with the Korean Good Clinical Practice (KGCP) and related regulations, taking into account the rights and safety of the subjects.
Informed Consent Statement
Written informed consent has been obtained from the patients.
Data Availability Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Acknowledgments
We would like to thank all medical staff at the participating institutions for their dedicated support in administering the hyperbaric oxygen therapy.
Conflicts of Interest
The authors declare that they have no conflicts of interest in this work.
References
- Stenn, K.S.; Paus, R. Controls of hair follicle cycling. Physiol. Rev. 2001, 81, 449–494. [Google Scholar] [CrossRef]
- Hunt, N.; McHale, S. The psychological impact of alopecia. BMJ 2005, 331, 951–953. [Google Scholar] [CrossRef]
- Paus, R.; Cotsarelis, G. The biology of hair follicles. N. Engl. J. Med. 1999, 341, 491–497. [Google Scholar] [CrossRef]
- Kaufman, K.D. Androgen metabolism as it affects hair growth in androgenetic alopecia. Dermatol. Clin. 1996, 14, 697–711. [Google Scholar] [CrossRef]
- Gupta, A.K.; Talukder, M.; Venkataraman, M.; Bamimore, M.A. Minoxidil: A comprehensive review. J. Dermatolog. Treat. 2022, 33, 1896–1906. [Google Scholar] [CrossRef]
- Thom, S.R. Hyperbaric oxygen: Its mechanisms and efficacy. Plast. Reconstr. Surg. 2011, 127, 131S–141S. [Google Scholar] [CrossRef]
- Hyperbaric Oxygen Therapy Indications, 13th ed.; Gesell, L.B., Ed.; Undersea and Hyperbaric Medical Society: North Palm Beach, FL, USA, 2014. [Google Scholar]
- Lee, S.M.; Heo, T.; Kim, G.W.; et al. Current status and development direction of hyperbaric medicine in Korea. J. Korean Med. Assoc. 2022, 65, 232–238. [Google Scholar] [CrossRef]
- Heyboer, M., III; Sharma, D.; Santiago, W.; McCulloch, N. Hyperbaric oxygen therapy: Side effects defined and quantified. Adv. Wound Care 2017, 6, 210–224. [Google Scholar] [CrossRef]
- Jones, S.R.; Carpin, K.M.; Woodward, S.M.; Khiabani, K.T.; Stephenson, L.L.; Wang, W.Z.; Zamboni, W.A. Hyperbaric oxygen inhibits ischemia–reperfusion–induced neutrophil CD18 polarization by a nitric oxide mechanism. Plast. Reconstr. Surg. 2010, 126, 403–411. [Google Scholar] [CrossRef]
- Kessler, L.; Bilbault, P.; Ortega, F.; et al. Hyperbaric oxygenation accelerates the healing rate of nonischemic chronic diabetic foot ulcers: A prospective randomized study. Diabetes Care 2003, 26, 2378–2382. [Google Scholar] [CrossRef]
- Van Neste, D.; Dumortier, M.; De Coster, W. Phototrichogram analysis: Technical aspects and problems in relation to automated quantitative evaluation of hair growth by computer-assisted image analysis. Trends in Human Hair Growth and Alopecia Research 1989, 155–165. [Google Scholar]
- Mai, W.; Sun, Y.; Liu, X.; Lin, D.; Lu, D. Characteristic findings by phototrichogram in southern Chinese women with female pattern hair loss. Skin Res. Technol. 2019, 25, 447–455. [Google Scholar] [CrossRef]
- Kang, H.; Kang, T.W.; Lee, S.D.; et al. The changing patterns of hair density and thickness in South Korean women with hair loss: Clinical office-based phototrichogram analysis. Int. J. Dermatol. 2009, 48, 14–21. [Google Scholar] [CrossRef]
- Kato, H.; Kinoshita, K.; Saito, N.; et al. The effects of ischemia and hyperoxygenation on hair growth and cycle. Organogenesis 2020, 16, 83–94. [Google Scholar] [CrossRef]
- Fan, Z.X.; Gan, Y.; Qu, Q.; et al. The effect of hyperbaric oxygen therapy combined with hair transplantation surgery for the treatment of alopecia. J. Cosmet. Dermatol. 2021, 20, 917–921. [Google Scholar] [CrossRef]
- Peña-Villalobos, I.; Casanova-Maldonado, I.; Lois, P.; et al. Hyperbaric oxygen increases stem cell proliferation, angiogenesis and wound-healing ability of WJ-MSCs in diabetic mice. Front. Physiol. 2018, 9, 995. [Google Scholar] [CrossRef]
- Helmers, R.; Milstein, D.M.; van Hulst, R.A.; de Lange, J. Hyperbaric oxygen therapy accelerates vascularization in keratinized oral mucosal surgical flaps. Head Neck 2014, 36, 1241–1247. [Google Scholar] [CrossRef]
- Hwang, D.; Lee, H.; Lee, J.; et al. Micro-current stimulation has potential effects of hair growth promotion on human hair follicle-derived papilla cells and animal model. Int. J. Mol. Sci. 2021, 22, 4361. [Google Scholar] [CrossRef]
- D’Amico, D.; Vaccaro, M.; Guarneri, F.; Borgia, F.; Cannavò, S.P.; Guarneri, B. Phototrichogram using videomicroscopy: A useful technique in the evaluation of scalp hair. Eur. J. Dermatol. 2001, 11, 17–20. [Google Scholar]
- Dhurat, R.; Saraogi, P. Hair evaluation methods: Merits and demerits. Int. J. Trichology 2009, 1, 108–119. [Google Scholar] [CrossRef]
- Van Neste, D.J.; De Brouwer, B.; De Coster, W. The phototrichogram: Analysis of some technical factors of variation. Skin Pharmacol. Physiol. 1994, 7, 67–72. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Hyperbaric oxygen therapy protocol.
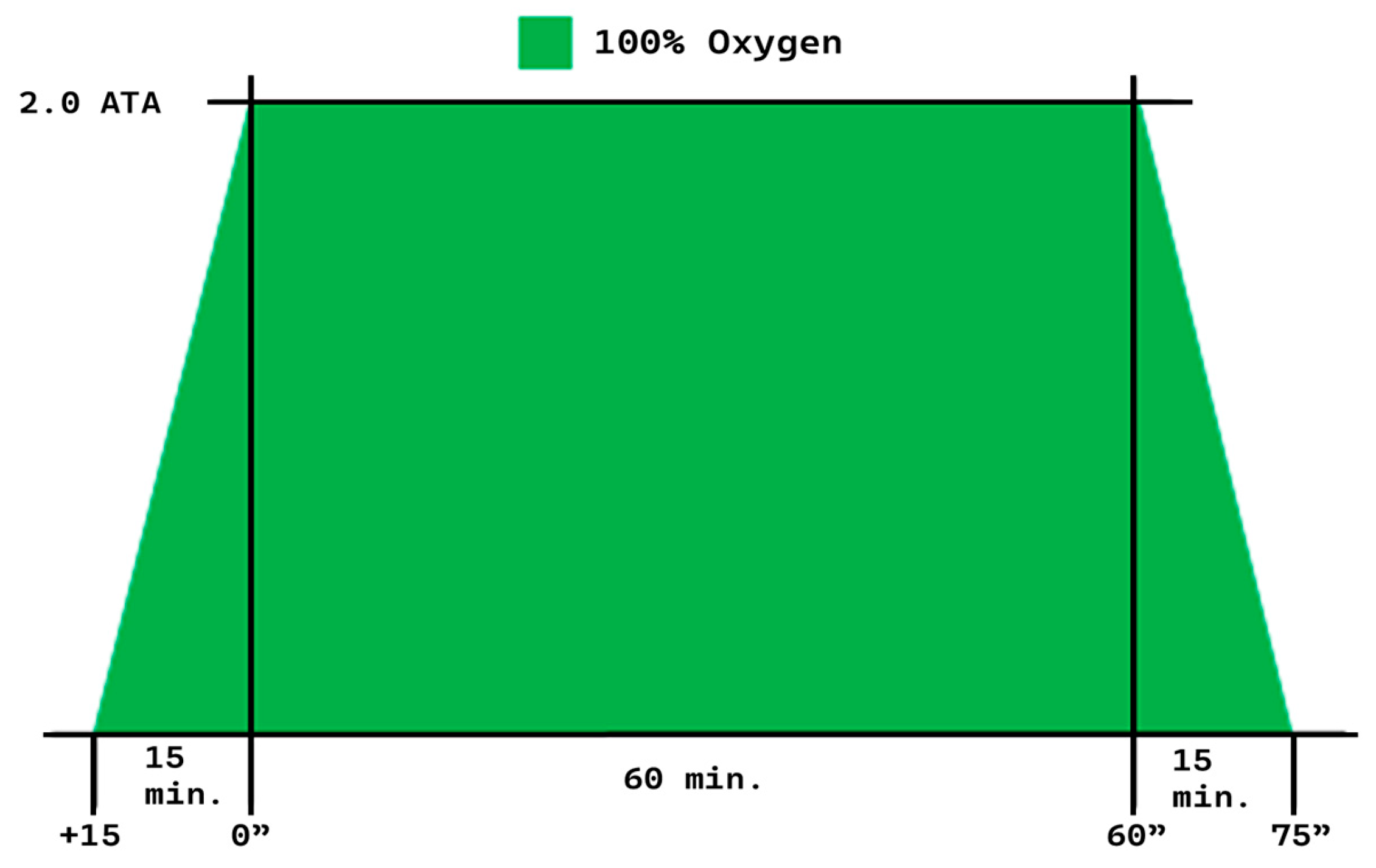
Figure 2.
Flowchart of clinical trials.
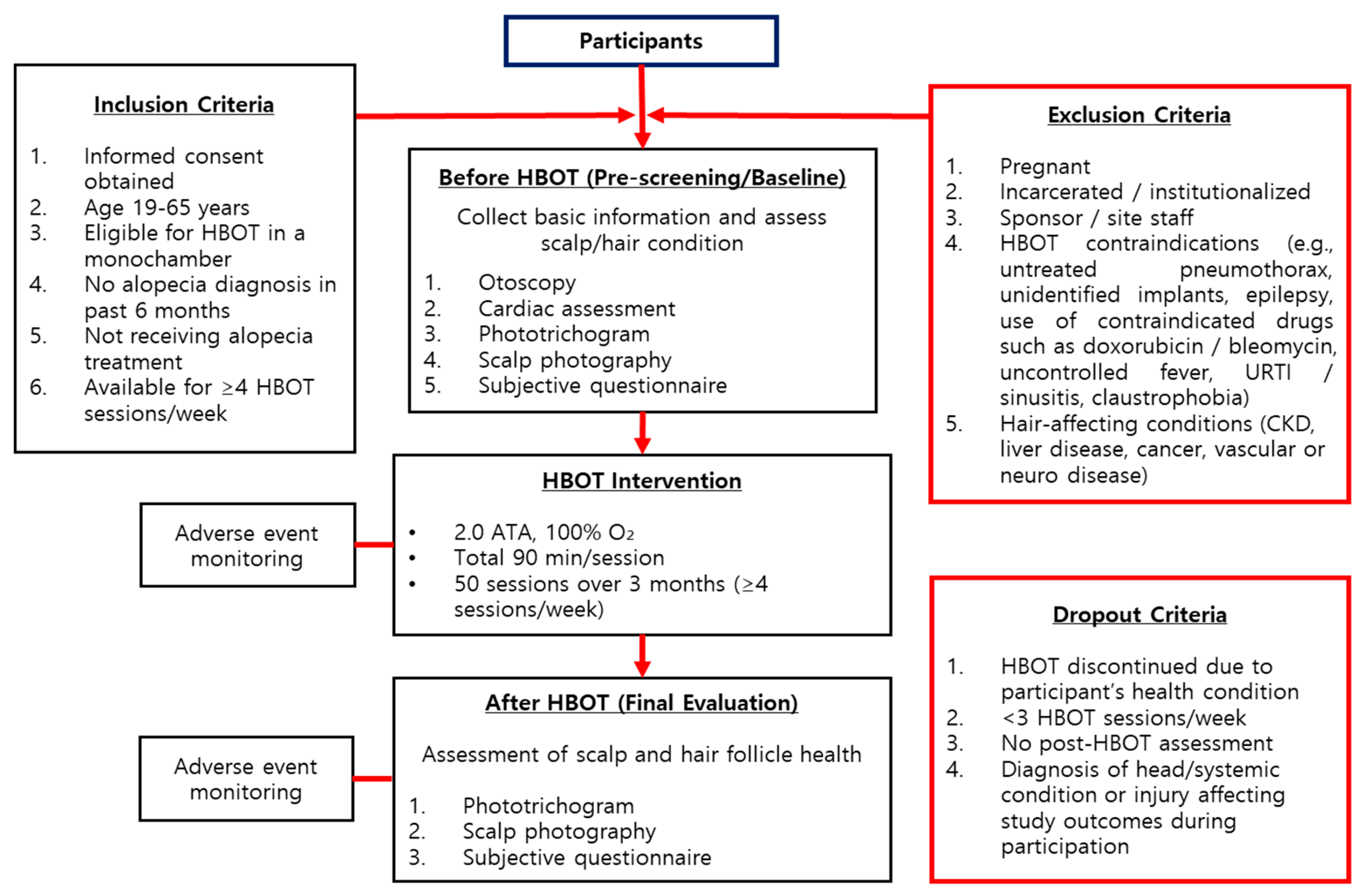
Figure 3.
Visual documentation of scalp condition before and after HBOT.
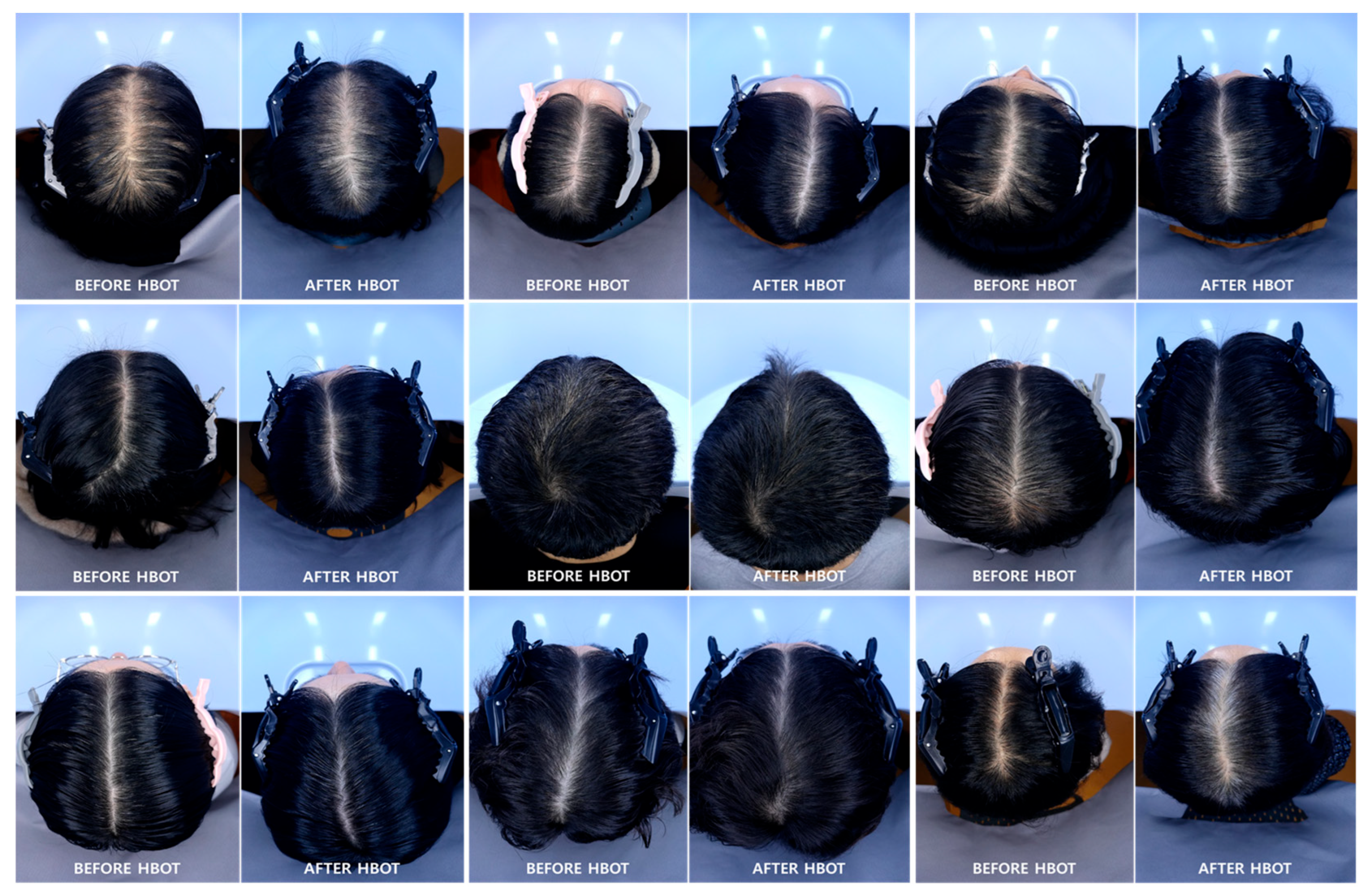
Figure 4.
Questionnaire evaluation before and after HBOT for improvement in hair condition.
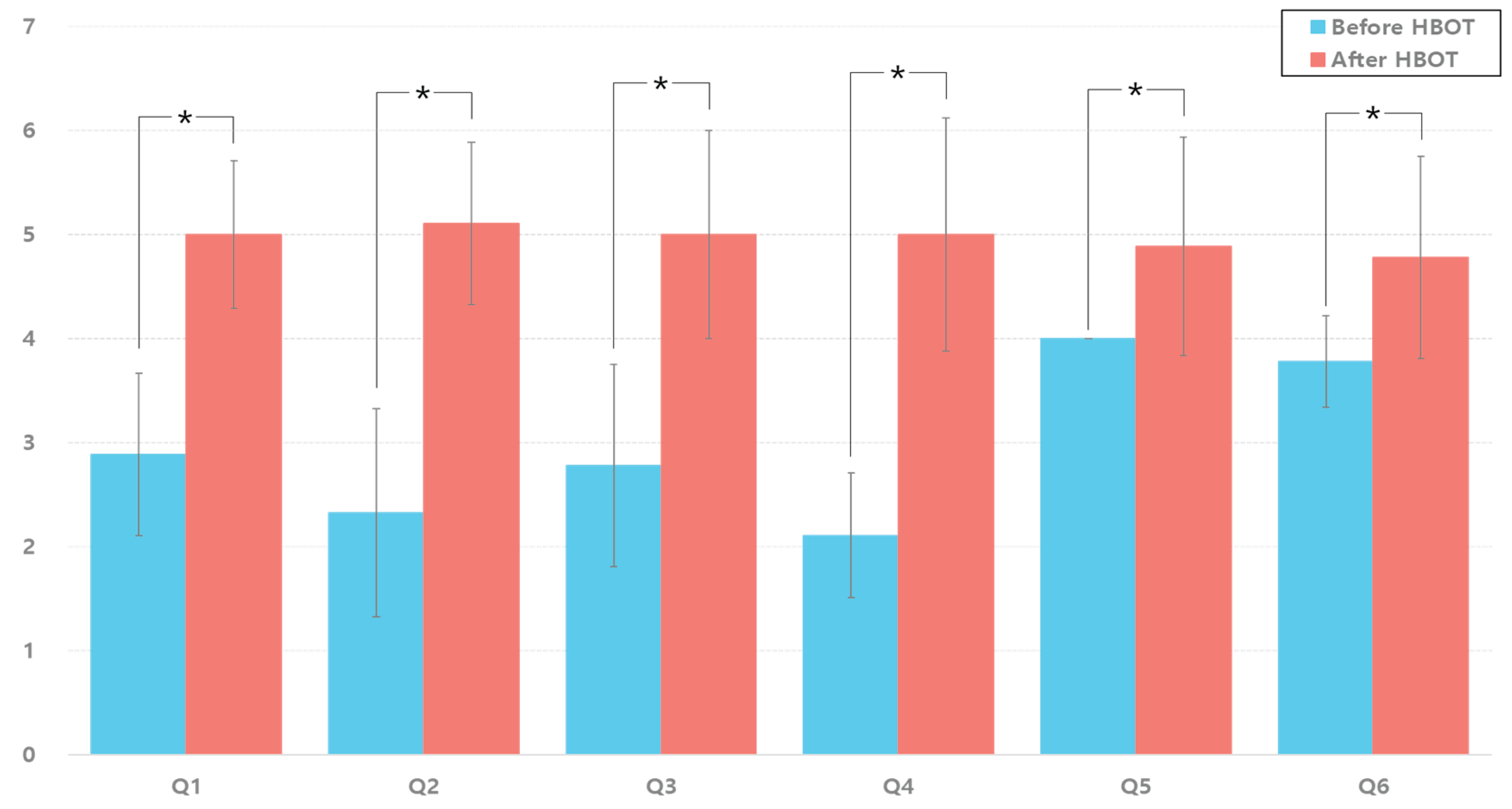

Table 1.
Questionnaire about hair condition before and after HBOT.
| Questions | Qualitative Evaluation | ||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| Q1. The overall appearance of the scalp is improving. | □ | □ | □ | □ | □ | □ | □ |
| Q2. The crown of the head is growing longer. | □ | □ | □ | □ | □ | □ | □ |
| Q3. The amount of hair falling out is decreasing. | □ | □ | □ | □ | □ | □ | □ |
| Q4. The hair is getting thicker. | □ | □ | □ | □ | □ | □ | □ |
| Q5. The hair growth rate is getting faster. | □ | □ | □ | □ | □ | □ | □ |
| Q6. The front hairline is improving. | □ | □ | □ | □ | □ | □ | □ |
Table 2.
Characteristics and medical history of participants (n = 9).
| Characteristic | Value |
| Sex, n (%) | |
| Female | 5 (55.6) |
| Male | 4 (44.4) |
| Age (years) | |
| Average (mean ± SD) | 39.3 ± 10.8 |
| Median ([IQR]) | 37 [31.5-45] |
| Age group, n (%) | |
| 20s | 1 (11.1) |
| 30s | 4 (44.4) |
| 40s | 3 (33.3) |
| 50s | 0 (0) |
| 60s | 1 (11.1) |
| History of past illness, n (%) | |
| None | 9 (100.0) |
| Physical examination performed, n (%) | |
| Otoscopy | 9 (100.0) |
| Chest x-ray | 9 (100.0) |
* Abbreviation: SD, standard deviation; IQR, inter-quartile range.
Table 3.
Changes in hair-related parameters before and after HBOT.
| Parameter | Before (Mean ± SD) | After (Mean ± SD) | t | p-value |
| Overall Score (point) | 73.11 ± 4.76 | 75.44 ± 3.88 | -1.871 | 0.098 |
| Follicle Density (counts/cm²) | 61.33 ± 13.00 | 66.78 ± 6.32 | -1.342 | 0.216 |
| Hair per Follicle (counts) | 1.24 ± 0.03 | 1.33 ± 0.14 | -1.860 | 0.099 |
| Hair Volume (%) | 24.89 ± 3.63 | 27.69 ± 4.87 | -1.880 | 0.097 |
| Thickness (mm) | 0.18 ± 0.08 | 0.10 ± 0.02 | 3.278 | 0.011 |
* Abbreviation: SD, standard deviation; IQR, inter-quartile range.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



