Submitted:
29 January 2026
Posted:
30 January 2026
You are already at the latest version
Abstract
Background/Objectives: The consumption of ultra-processed foods (UPFs) has increased markedly in recent decades and has been associated with adverse health outcomes. In childhood, the family environment plays a central role in shaping dietary habits and oral health behaviors. This study investigated the association between UPF consumption by caregivers and children, its relationship with caregivers’ periodontal health–related quality of life and described children’s dietary practices and oral hygiene habits. Methods: This cross-sectional observational study was conducted with caregivers of children participating in the Happy Smile Project in Birigui, São Paulo, Brazil. UPF consumption was assessed using a questionnaire based on the NOVA classification, considering intake in the 24 hours prior to data collection. Caregivers’ periodontal health–related quality of life was evaluated using the OHIP-14-PD. Statistical analyses included the Mann–Whitney U test, Spearman correlation, and binary logistic regression adjusted for caregiver education level and household income. Results: A high frequency of UPF consumption was observed among both caregivers and children. Children whose caregivers had high UPF consumption were more likely to also present high consumption (OR = 8.66; 95% CI: 5.00–14.99; p < 0.001). Higher caregiver education was associated with lower odds of high UPF consumption among children. Children in the high-consumption group were older and showed higher consumption of sweetened milk beverages (p < 0.001). Risk behaviors for oral health, such as nighttime use of sweetened bottles and absence of toothbrushing afterward, were frequently reported. Regarding periodontal health–related quality of life, only the physical disability domain of the OHIP-14-PD showed significantly higher scores among caregivers with high UPF consumption (p = 0.014). Conclusions: In conclusion, high consumption of ultra-processed foods by caregivers significantly increased the odds of children’s consumption and was associated with a greater negative impact on caregivers’ periodontal health–related quality of life. In addition, children exhibited a high frequency of oral health–damaging behaviors. These findings highlight the importance of family-centered strategies aimed at reducing the intake of ultra-processed foods and promoting healthier oral health behaviors to improve overall quality of life.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Sociodemographic and Health Data
2.2. Assessment of Ultra-Processed Food Consumption
2.3. Children’s Dietary Practices, Oral Hygiene Habits, and Caregivers’ Perceptions
2.4. Periodontal Health–Related Quality of Life
2.5. Statistical Analysis
3. Results
3.1. Caregivers’ Sociodemographic and Clinical Characteristics
3.2. Children’s Sociodemographic and Behavioral Characteristics
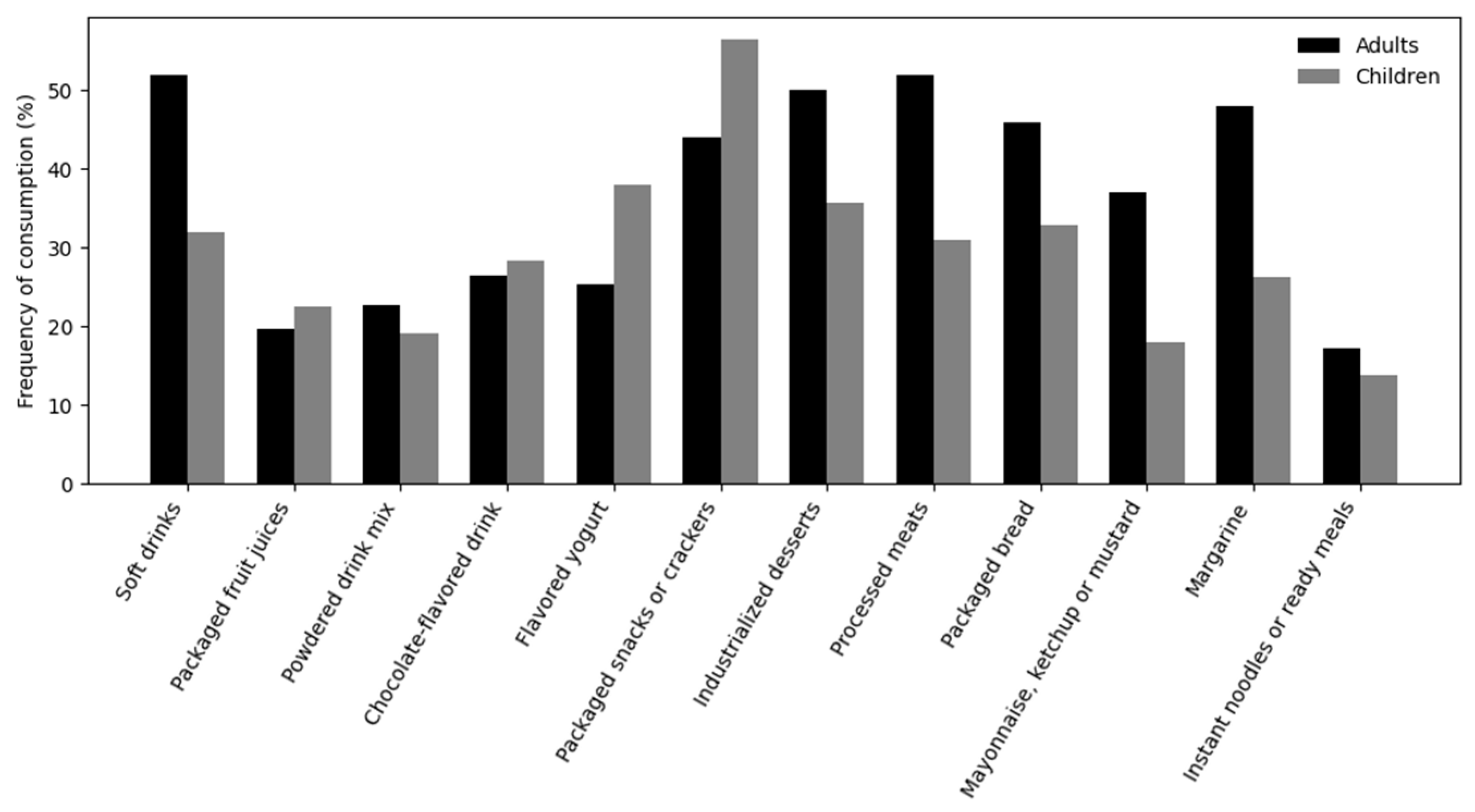
3.3. Frequency of UPF Intake
3.4. Association Between Caregivers’ and Children’s UPF Consumption
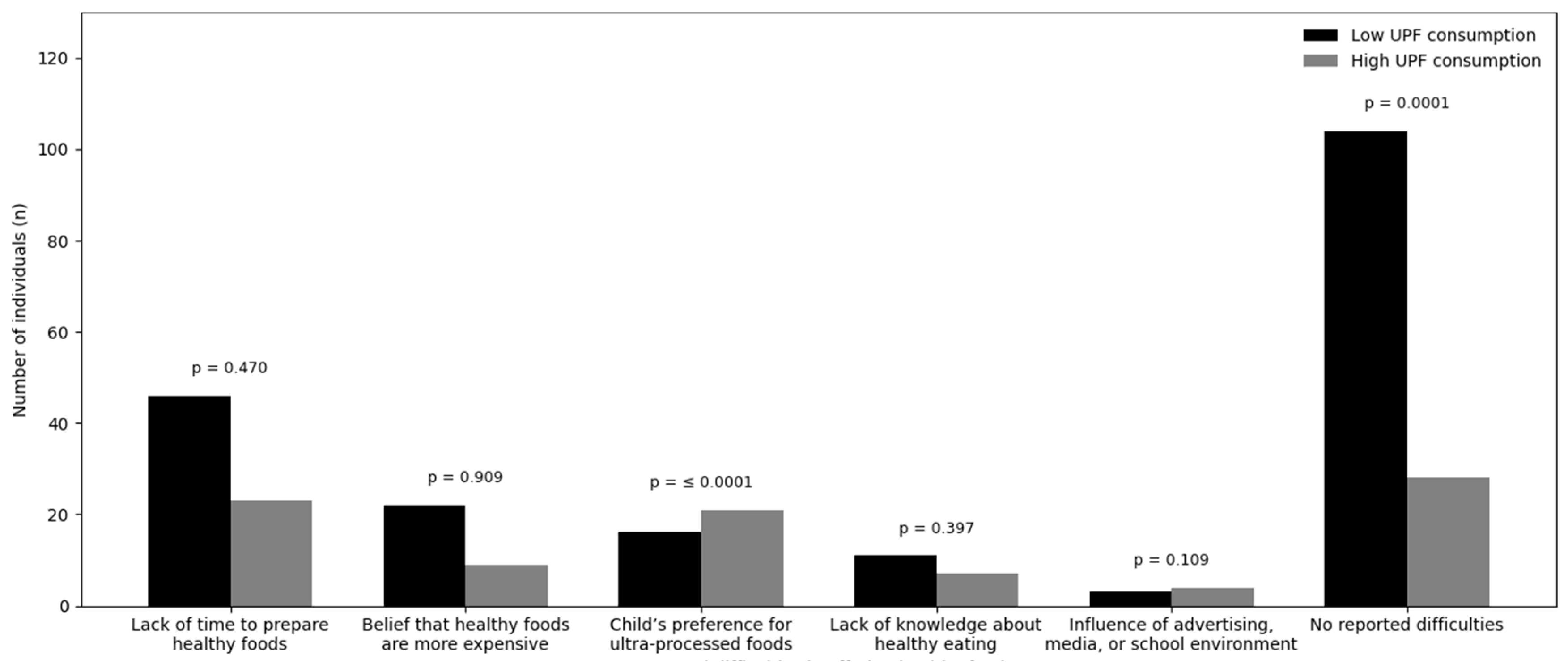
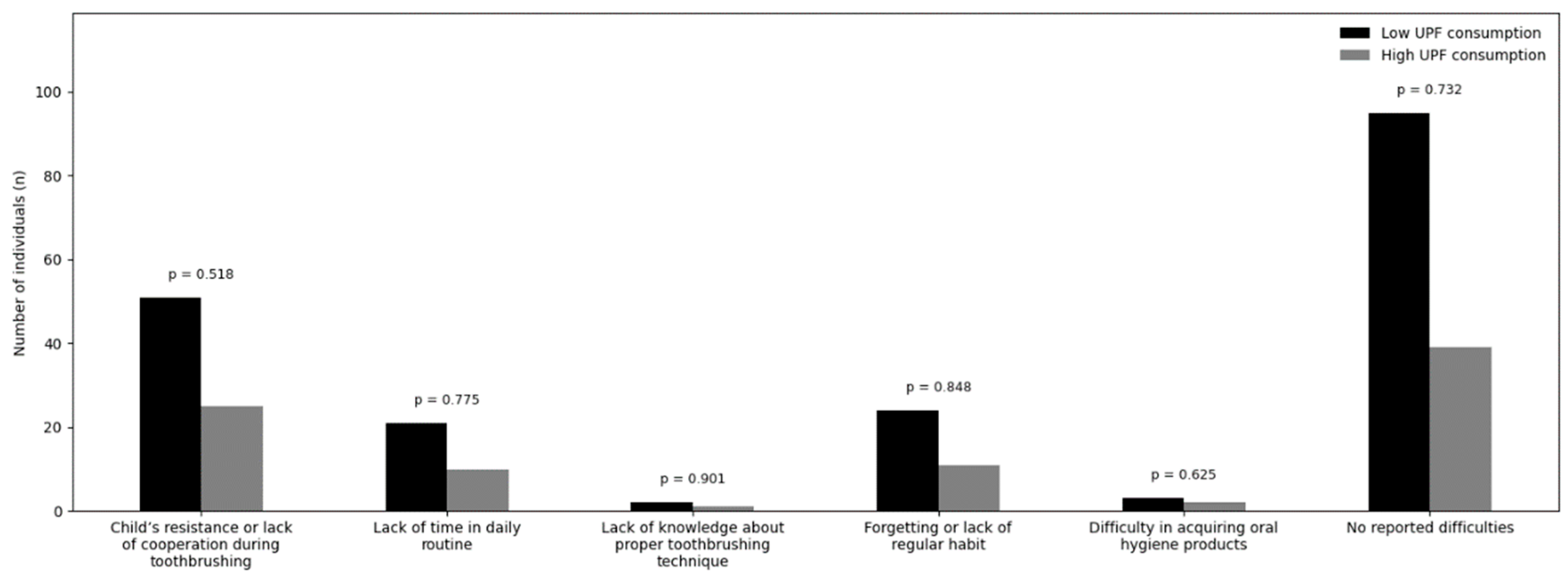
3.5. Reported Difficulties in Offering a Healthy Diet and Oral Hygiene
3.6. Knowledge, Frequency, and Motives Related to UPF Consumption
3.7. Association Between UPF Consumption and Periodontal Health–Related Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| OHIP-14-PD | Oral Health Profile applied to Periodontal Diseases |
| OR | Odds Ratio |
| SPSS | Statistical Package for the Social Sciences |
| SD | Standard Deviation |
| UPF | Ultra-processed food |
| UPFs | Ultra-processed foods |
References
- de Menezes, R.C.E.; Oliveira, J.S.; Almendra, R.; de Lira, P.I.C.; Costa, E.C.; Leal, V.S.; Santana, P. Influence of Food Environment on Ultra-Processed Drinks Consumption among an Economically Vulnerable Population in a Metropolitan Area in Brazil: A Multilevel Analysis. Health Place 2022, 77, 102869. [CrossRef]
- Monteiro, C.A.; Levy, R.B.; Claro, R.M.; Castro, I.R.R. de; Cannon, G. A New Classification of Foods Based on the Extent and Purpose of Their Processing. Cad. Saúde Pública 2010, 26, 2039–2049. [CrossRef]
- Resende Cunha, V.C.; Borges, C.A.; Canella, D.S. Incorporação da classificação NOVA na produção científica em alimentação e nutrição na América Latina: uma revisão cienciométrica. Arch. Latinoam. Nutr. 2022, 72, 109–124. [CrossRef]
- Cassiano, L.S.; Peres, M.A.; Motta, J.V.S.; Demarco, F.F.; Horta, B.L.; Ribeiro, C.C.; Nascimento, G.G. Periodontitis Is Associated with Consumption of Processed and Ultra-Processed Foods: Findings from a Population-Based Study. Nutrients 2022, 14, 3735. [CrossRef]
- Whelan, K.; Bancil, A.S.; Lindsay, J.O.; Chassaing, B. Ultra-Processed Foods and Food Additives in Gut Health and Disease. Nat. Rev. Gastroenterol. Hepatol. 2024, 21, 406–427. [CrossRef]
- Zhu, Y.; Garcia-Larsen, V.; Bromage, S.; Martinez-Steele, E.; Curi-Hallal, A.L.; Rebholz, C.M.; Matsuzaki, M. Association Between Ultraprocessed Food Intake and Self-Reported Arthritis. Am. J. Prev. Med. 2025, 68, 1109–1119. [CrossRef]
- Castilho, A.R.F. de; Mialhe, F.L.; Barbosa, T. de S.; Puppin-Rontani, R.M. Influence of Family Environment on Children’s Oral Health: A Systematic Review. J. Pediatr. (Rio J.) 2013, 89, 116–123. [CrossRef]
- Cavalcante, M.B.; Franco, R.D.S.; Costa, S.K.; Meira, G.D.F. A influência dos pais ou responsáveis na saúde bucal de crianças de 0 a 12 anos. Res. Soc. Dev. 2022, 11, e161111638207. [CrossRef]
- Mahmood, L.; Flores-Barrantes, P.; Moreno, L.A.; Manios, Y.; Gonzalez-Gil, E.M. The Influence of Parental Dietary Behaviors and Practices on Children’s Eating Habits. Nutrients 2021, 13, 1138. [CrossRef]
- Lima, L.H.G.; Rocha, N.B.D.; Antoniassi, C.P.; Moura, M.S.D.; Fujimaki, M. Prevalência e severidade da cárie dentária em escolares do Ensino Fundamental de um município vulnerável. Rev. Odontol. UNESP 2020, 49, e20200063. [CrossRef]
- Nascimento, G.G.; Alves-Costa, S.; Romandini, M. Burden of Severe Periodontitis and Edentulism in 2021, with Projections up to 2050: The Global Burden of Disease 2021 Study. J. Periodontal Res. 2024, 59, 823–867. [CrossRef]
- Trindade, D.; Carvalho, R.; Machado, V.; Chambrone, L.; Mendes, J.J.; Botelho, J. Prevalence of Periodontitis in Dentate People between 2011 and 2020: A Systematic Review and Meta-Analysis of Epidemiological Studies. J. Clin. Periodontol. 2023, 50, 604–626. [CrossRef]
- Khan, M.W.; Cruz De Jesus, V.; Mittermuller, B.-A.; Sareen, S.; Lee, V.; Schroth, R.J.; Hu, P.; Chelikani, P. Role of Socioeconomic Factors and Interkingdom Crosstalk in the Dental Plaque Microbiome in Early Childhood Caries. Cell Rep. 2024, 43, 114635. [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45. [CrossRef]
- Villoria, G.E.M.; Fischer, R.G.; Tinoco, E.M.B.; Meyle, J.; Loos, B.G. Periodontal Disease: A Systemic Condition. Periodontol. 2000 2024, 96, 7–19. [CrossRef]
- Cascaes, A.M.; Silva, N.R.J. da; Fernandez, M. dos S.; Bomfim, R.A.; Vaz, J. dos S. Ultra-Processed Food Consumption and Dental Caries in Children and Adolescents: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2023, 129, 1370–1379. [CrossRef]
- Savage, J.S.; Fisher, J.O.; Birch, L.L. Parental Influence on Eating Behavior. J. Law Med. Ethics J. Am. Soc. Law Med. Ethics 2007, 35, 22–34. [CrossRef]
- Costa, C.D.S.; Sattamini, I.F.; Steele, E.M.; Louzada, M.L.D.C.; Claro, R.M.; Monteiro, C.A. Consumo de alimentos ultraprocessados e associação com fatores sociodemográficos na população adulta das 27 capitais brasileiras (2019). Rev. Saúde Pública 2021, 55, 47. [CrossRef]
- Martins-Cruz, T.M.; Soares, K.H.; Leal, J.H.G.; Flecha, O.D.; Douglas-De-Oliveira, D.W.; Gonçalves, P.F. Brazilian Version of the OHIP 14 Periodontal Disease Questionnaire: Cross Cultural Adaptation and Validation. Braz. Oral Res. 2025, 39, e002. [CrossRef]
- Dutra, L.V.; Lopes, L.J.; Rodrigues, C.T.; Franceschini, S.D.C.C.; Novaes, J.F.D.; Vieira, L.L.; Priore, S.E. Disponibilidade domiciliar de alimentos por grau de processamento e formas de aquisição no Brasil: uma análise da interferência socioeconômica e territorial. Segur. Aliment. E Nutr. 2025, 31, e024038. [CrossRef]
- Levy, R.B.; Andrade, G.C.; Cruz, G.L.D.; Rauber, F.; Louzada, M.L.D.C.; Claro, R.M.; Monteiro, C.A. Três décadas da disponibilidade domiciliar de alimentos segundo a NOVA – Brasil, 1987–2018. Rev. Saúde Pública 2022, 56, 75. [CrossRef]
- Silveira, V.N.C.; Dos Santos, A.M.; França, A.K.T.C. Determinants of the Consumption of Ultra-Processed Foods in the Brazilian Population. Br. J. Nutr. 2024, 132, 1104–1109. [CrossRef]
- Dias, L.R.; Baptista, J.A.G.; Levy, R.B.; Leite, M.A. Alimentos ultraprocessados e preparações culinárias em promoções no maior aplicativo de delivery de alimentos do Brasil. Ciênc. Saúde Coletiva 2025, 30, e07512023. [CrossRef]
- Viola, P.C.D.A.F.; Ribeiro, S.A.V.; Carvalho, R.R.S.D.; Andreoli, C.S.; Novaes, J.F.D.; Priore, S.E.; Carvalho, C.A.D.; Franceschini, S.D.C.C. Socioeconomic Status, Screen Time, and Time Spent at School, and Children’s Food Consumption. Ciênc. Saúde Coletiva 2023, 28, 257–267. [CrossRef]
- Baraldi, L.G.; Martinez Steele, E.; Canella, D.S.; Monteiro, C.A. Consumption of Ultra-Processed Foods and Associated Sociodemographic Factors in the USA between 2007 and 2012: Evidence from a Nationally Representative Cross-Sectional Study. BMJ Open 2018, 8, e020574. [CrossRef]
- Heuchan, G.N.; Conway, R.E.; Tattan-Birch, H.; Heggie, L.; Llewellyn, C.H. Social and Economic Patterning in Ultra-Processed Food Intake in Toddlerhood and Middle Childhood: Longitudinal Data From the Gemini Cohort in the United Kingdom. J. Acad. Nutr. Diet. 2025, 125, 922-934.e11. [CrossRef]
- Pozveh, S.H.; Aktary, M.L.; Polsky, J.Y.; Moubarac, J.-C.; Vanderlee, L.; Olstad, D.L. Socioeconomic Inequalities in Intakes of Ultraprocessed and Minimally Processed Foods in Nationally Representative Samples of Adults in Canada: An Analysis of Trends between 2004 and 2015. J. Nutr. 2024, 154, 3088–3104. [CrossRef]
- Khandpur, N.; Cediel, G.; Obando, D.A.; Jaime, P.C.; Parra, D.C. Sociodemographic Factors Associated with the Consumption of Ultra-Processed Foods in Colombia. Rev. Saúde Pública 2020, 54, 19–19. [CrossRef]
- Silva, M.A.; Milagres, L.C.; Castro, A.P.P.; Filgueiras, M.D.S.; Rocha, N.P.; Hermsdorff, H.H.M.; Longo, G.Z.; Novaes, J.F. O consumo de produtos ultraprocessados está associado ao melhor nível socioecocômico das famílias das crianças. Ciênc. Saúde Coletiva 2019, 24, 4053–4060. [CrossRef]
- Simões, B.D.S.; Barreto, S.M.; Molina, M.D.C.B.; Luft, V.C.; Duncan, B.B.; Schmidt, M.I.; Benseñor, I.J.M.; Cardoso, L.D.O.; Levy, R.B.; Giatti, L. Consumption of Ultra-Processed Foods and Socioeconomic Position: A Cross-Sectional Analysis of the Brazilian Longitudinal Study of Adult Health. Cad. Saúde Pública 2018, 34. [CrossRef]
- Dicken, S.J.; Qamar, S.; Batterham, R.L. Who Consumes Ultra-Processed Food? A Systematic Review of Sociodemographic Determinants of Ultra-Processed Food Consumption from Nationally Representative Samples. Nutr. Res. Rev. 2024, 37, 416–456. [CrossRef]
- Pedro-Botet, L.; Muns, M.D.; Solà, R.; Fontané, L.; Climent, E.; Benaiges, D.; Flores-Le Roux, J.A.; Pedro-Botet, J. Level of Understanding and Consumption of Ultra-Processed Food in a Mediterranean Population: A Cross-Sectional Study. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 889–896. [CrossRef]
- Ponce-Carreón, A.; Monrroy-Campos, R.; Rucano Paucar, F.H.; Talavera-Mendoza, F. Associations between Ultra-Processed Food Consumption and Food Literacy in Preadolescents. Discov. Food 2025, 5, 296. [CrossRef]
- Rusfianti, A.; Widyaningsih, V.; Hikmayani, N.H. The Impact of Video Nutrition Education on Nutrition Knowledge, Food Selection, and Ultra-Processed Food Consumption in Adolescents. AcTion Aceh Nutr. J. 2025, 10, 603. [CrossRef]
- da Silva, N.R.J.; de Camargo, M.B.J.; dos Vaz, J.S.; Correa, M.B.; Matijasevich, A.; da Silva dos Santos, I.; Cascaes, A.M. Ultra-Processed Food Consumption and Dental Caries in Adolescents from the 2004 Pelotas Birth Cohort Study. Community Dent. Oral Epidemiol. 2023, 51, 1180–1186. [CrossRef]
- Rocha, A.C.; Crema, A.F. de A.; Menoncin, B.L.V.; Fraiz, G.M.; Crispim, S.P.; Fraiz, F.C. Consumption of Cariogenic Ultra-Processed Foods and Maternal Report of Dental Caries and Dental Pain among Preschool Children. Pesqui. Bras. Em Odontopediatria E Clínica Integrada 2025, 25, e240112. [CrossRef]
- Crema, A.F. de A.; Menoncin, B.L.V.; Crispim, S.P.; Fraiz, F.C. Factors Associated with the Intake of Ultra-Processed Cariogenic Foods by Preschoolers During the COVID-19 Pandemic. Pesqui. Bras. Em Odontopediatria E Clínica Integrada 2023, 23, e220080. [CrossRef]
- Ribeiro, G.J.S.; de Araújo Pinto, A. Consumption of Ultra-Processed Foods in Brazilian Children: An Analysis of Regional Trends. J. Pediatr. Nurs. 2021, 61, e106–e111. [CrossRef]
- Sparrenberger, K.; Friedrich, R.R.; Schiffner, M.D.; Schuch, I.; Wagner, M.B. Ultra-Processed Food Consumption in Children from a Basic Health Unit. J. Pediatr. (Rio J.) 2015, 91, 535–542. [CrossRef]
- Moran, A.J.; Khandpur, N.; Polacsek, M.; Rimm, E.B. What Factors Influence Ultra-Processed Food Purchases and Consumption in Households with Children? A Comparison between Participants and Non-Participants in the Supplemental Nutrition Assistance Program (SNAP). Appetite 2019, 134, 1–8. [CrossRef]
- Yeum, D.; Hua, S.; Thapaliya, G.; Duck, S.A.; Melhorn, S.J.; Roth, C.L.; Schur, E.A.; Carnell, S.; Sewaybricker, L.E. The Impact of Eating Behaviors on Ultraprocessed Food Consumption Over 12 Months in Children. Obesity 2025, 33, 1704–1712. [CrossRef]
- Alghamdi, R.A.; Alzamil, H.A.; Alzamil, H.A.; Alotaibi, R.Y.; Albishi, S.M.; Sallam, A.M.; Alhufaiyan, N.S.; Alahdal, E.M.; Baeesa, D.A.; Aljohani, S.M. Exploring the Interplay between Diet and Oral Inflammation. Int. J. Community Med. Public Health 2024, 11, 3245–3248. [CrossRef]
- Casarin, M.; Da Silveira, T.M.; Bezerra, B.; Pirih, F.Q.; Pola, N.M. Association between Different Dietary Patterns and Eating Disorders and Periodontal Diseases. Front. Oral Health 2023, 4, 1152031. [CrossRef]
- Fan, R.-Y.; Chen, J.-X.; Chen, L.-L.; Sun, W.-L. Assessing Periodontitis Risk from Specific Dietary Patterns: A Systematic Review and Meta-Analysis. Clin. Oral Investig. 2025, 29, 43. [CrossRef]


| Demographic data | Low consumption of UPFs | High consumption of UPFs | Total | Spearman's correlation (p-value) |
|
Gender (n= 390) Female Male Not specified |
179 39 1 |
146 25 0 |
325 64 1 |
0,463 |
|
Education level (n= 376) Elementary school High school Undergraduate degree Postgraduate degree |
22 130 47 11 |
29 101 26 10 |
51 231 73 21 |
0,06 |
|
Income (n= 385) Below R$1000 R$1000 e R$2500 2500 a 8000 R$8.000 e R$20.000 Above R$20.000 |
16 82 105 11 0 |
19 71 74 7 0 |
35 153 179 18 0 |
0,130 |
|
N° of residents (n= 309) Up to 2 people 3-4 people 5 people or more |
19 127 22 |
19 103 19 |
38 230 41 |
0,760 |
| Age - mean (SD)(n=353) | 32,4 (7,2) | 31,2 (7,3) | 353 | 0,184 |
|
BMI(n=312) Underweight Normal weight Overweight Obesity class I Obesity class II Obesity class III |
4 56 59 43 16 10 |
1 42 37 29 10 5 |
5 99 96 72 26 15 |
0,681 |
|
Hypertension (n= 392) No Yes |
192 27 |
152 21 |
344 48 |
0,955 |
|
Diabetes (n= 392) No Yes |
201 18 |
163 10 |
364 28 |
0,353 |
|
Hypercholesterolemia (n= 392) No Yes |
210 9 |
167 6 |
377 15 |
0,743 |
| Demographic data | Low consumption of UPFs | High consumption of UPFs | Total | Spearman's correlation (p-value) |
|
Gender (n=392) Male Female |
142 134 |
61 55 |
203 189 |
0,838 |
| Age (months) - Median (IQR) (n=351) | 36 (25) | 36 (24) | 387 |
0,001 |
|
Nighttime bottle-feeding (n=392) No Yes |
99 177 |
44 72 |
143 249 |
0,893 |
|
Milk flavored with sugar, chocolate powder, or similar items (n= 392) No Yes |
176 100 |
43 73 |
219 173 |
0,0001 |
|
Toothbrushing after nighttime bottle-feeding (n= 392) No Yes |
155 121 |
53 63 |
208 184 |
0,058 |
| Caregiver's consumption of ultra-processed foods | |||
| OR | IC 95% | p value | |
| Low Consumption | 1,00 | - | - |
| High Consumption | 8,66 | 5 – 14,99 | < 0,001 |
| Caregiver's educational level | |||
| OR | IC 95% | p value | |
| Elementary school | 1,00 | - | - |
| High school | 0,39 | 0,19-0,81 | 0,012 |
| Undergraduate degree | 0,17 | 0,06-0,47 | 0,001 |
| Postgraduate degree | 0,44 | 0,12-1,6 | 0,22 |
| Family income | |||
| OR | IC 95% | p value | |
| Below R$ 1.000,00 | 1,00 | - | - |
| R$ 1.000,00 – R$ 2.500,00 | 0,6 | 0,24 – 1,48 | 0,27 |
| R$ 2.500,00 – R$ 8.000,00 | 0,42 | 0,16 – 1,06 | 0,06 |
| R$ 8.000,00 – R$ 20.000,00 | 0,38 | 0,07 – 1,98 | 0,25 |
| Domain | Low UPFs consumption | High UPFs consumption | p-value |
| Functional limitation | 0 (0-2) | 0 (0-2) | 0,999 |
| Physical pain | 2 (1-4) | 2 (1-4) | 0,889 |
| Psychological discomfort | 0 (0-2) | 0 (0-2) | 0,174 |
| Physical disability | 0 (0-3) | 1 (0-4) | 0,014 |
| Psychological disability | 0 (0-2) | 0 (0-3) | 0,509 |
| Social disability | 0 (0-0) | 0 (0-0) | 0,107 |
| Social disadvantage | 0 (0-3) | 0 (0-0) | 0,275 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



