
Submitted:
19 January 2026
Posted:
27 January 2026
You are already at the latest version
Abstract
Malignant biliary obstruction (MBO) represents a critical clinical challenge characterized by bile duct compromise leading to severe complications including intractable jaundice, recurrent cholangitis, biliary cirrhosis, and hepatic failure. Classification into distal MBO (DMBO) and hilar MBO (HMBO) guides therapeutic decision-making, with the former predominantly caused by pancreatic head adenocarcinoma and extrahepatic cholangiocarcinoma, while perihilar cholangiocarcinoma represents the principal etiology of the latter. The high morbidity and mortality associated with MBO necessitate prompt, expert intervention. While endoscopic retrograde cholangiopancreatography (ERCP) with transpapillary biliary drainage (TBD) has traditionally served as the cornerstone of management for unresectable tumors, endoscopic ultrasound (EUS)-guided biliary drainage has emerged as a compelling alternative, particularly when conventional ERCP proves technically unsuccessful or anatomically unfeasible. This review comprehensively examines current endoscopic strategies for MBO, emphasizing the complementary roles of ERCP and EUS-based techniques. Optimal outcomes require intervention by experienced endoscopists at high-volume tertiary centers, with individualized treatment selection based on anatomical considerations, tumor characteristics, patient factors, and local expertise.
Keywords:
endoscopy
; malignant biliary obstruction
; endoscopic ultrasound
; endoscopic retrograde cholangiopancreatography
; transpapillary biliary drainage
1. Introduction
Malignant biliary obstruction (MBO) constitutes a biliary pathology associated with substantial morbidity and mortality [1,2]. The condition arises from bile duct blockage that compromises normal bile flow, precipitating severe complications such as intractable jaundice, cholangitis, biliary cirrhosis, and ultimately hepatic failure [3,4,5]. MBO is anatomically classified as either distal (DMBO) or hilar (HMBO) based on the obstruction site, though some patients present with multifocal involvement [6].
The majority of DMBO cases result from adenocarcinoma of the pancreatic head and extrahepatic cholangiocarcinoma, with less common etiologies including gallbladder cancer, ampullary neoplasms, lymphoma, and metastatic disease [7,8,9]. Perihilar cholangiocarcinoma (Klatskin tumor), classified using the Bismuth-Corlette system, represents the predominant cause of HMBO. This classification system proves crucial for both interventional planning and resectability assessment. Additional HMBO etiologies include gallbladder carcinoma, hepatocellular carcinoma, lymphoma, and metastatic malignancies [10].
A major clinical challenge lies in the late diagnosis of MBO, particularly for HMBO patients classified as Bismuth-Corlette stage III-IV, who typically present at an inoperable stage. Median survival for inoperable disease ranges from 7 to 16 months, [10,11] shifting therapeutic goals toward palliation with emphasis on biliary decompression, infection prevention, and optimization for systemic therapy.
Traditionally, transpapillary endoscopic biliary drainage (TBD) via ERCP has served as the gold standard approach regardless of palliative status, offering the advantage of achieving both decompression and tissue diagnosis in a single intervention [12,13]. It is important to note that most EUS-guided biliary drainage procedures are performed following failed ERCP attempts, and ERCP expertise remains more universally available compared to interventional EUS expertise. Therefore, interventional EUS in MBO is an adjunct to conventional ERCP rather than a replacement, only when ERCP is unsuccessful or anatomically infeasible. Ongoing innovation continues to refine endoscopic strategies and broaden their role in comprehensive MBO management.
This review provides a comprehensive overview of current therapeutic strategies for malignant biliary obstruction and critically assesses novel interventions that may expand future clinical options.
2. Transpapillary Biliary Drainage
2.1. TBD in Unresectable Distal Malignant Biliary Obstruction
Transpapillary biliary drainage with self-expanding metal stent (SEMS) placement during ERCP currently represents the gold standard treatment for achieving decompression of DMBO, with technical success rates ranging from 87.5% to 95% [14]. Anatomical and technical difficulties related to tumor characteristics constitute the most common causes of procedural failure [6,15,16]. TBD demonstrates superiority over surgical bypass owing to lower morbidity and mortality rates, despite higher recurrent biliary obstruction rates [17].
Compared to percutaneous transhepatic biliary drainage (PTBD), TBD offers several advantages including fewer complications, reduced need for subsequent procedures, shorter hospitalization, and lower costs. Additionally, patients undergoing PTBD experience diminished quality of life and face risks of catheter dislodgement [12,14,18,19,20].
Stent selection remains a critical consideration in DMBO management. Following the introduction of plastic stenting in the 1980s and subsequent emergence of SEMS in the 1990s, [21,22] multiple comparative studies have demonstrated SEMS superiority in terms of patency duration, resulting in fewer recurrent obstruction episodes and reduced need for reinterventions [23,24,25]. Despite higher initial costs, SEMS achieve cost equivalence with plastic stents at one year due to prolonged functional duration [26]. This cost-effectiveness was corroborated by Bor et al., who reported similar cumulative treatment costs between groups, with plastic stents actually incurring higher costs in patients surviving 2-4 months (2888€ vs 2258€) [27]. However, SEMS demonstrate a higher incidence of post-ERCP pancreatitis, occurring approximately five times more frequently than with plastic stents [28,29,30,31].
These advantages have led guidelines to recommend SEMS over plastic stents in DMBO. The choice between uncovered SEMS (U-SEMS) and covered SEMS (C-SEMS), which includes partially covered (PC-SEMS) and fully covered (FC-SEMS) variants, presents a more nuanced decision. Each type carries distinct risks: U-SEMS face increased neoplastic ingrowth through metal meshes, while C-SEMS demonstrate higher rates of stent migration, tumor overgrowth, and sludge formation [32,33,34].
Numerous studies comparing C-SEMS with U-SEMS for DMBO have reported no clear superiority regarding patency, safety, or patient survival [35,36,37,38]. However, a retrospective cohort study published in September 2025 found FC-SEMS significantly prolonged stent patency (445 vs 348 days, p=0.02) without major differences in postoperative complications [39]. A 2018 meta-analysis of 11 randomized controlled trials comparing FC-SEMS, PC-SEMS, and U-SEMS reported a non-significant 32% risk reduction for both stent failure and patient mortality in the C-SEMS group, with no significant differences in adverse events [32]. More recent analyses have demonstrated significantly longer time to recurrent biliary obstruction for C-SEMS (mean difference 45.51 days; 95% CI 11.79-79.24), [40] while Vanella et al. reported reduced time to recurrent biliary obstruction for FC-SEMS (238 days, 95% CI 191-286) versus PC-SEMS (369 days, 95% CI 290-449) [33].
A comprehensive systematic review and meta-analysis published in June 2025, comprising 21 studies and 5,753 patients, revealed that C-SEMS demonstrated higher post-ERCP acute cholecystitis rates (RR 1.71, 95% CI 1.12-2.62), lower tumor ingrowth rates (RR 0.13, 95% CI 0.06-0.25), and higher stent migration rates (RR 7.53, 95% CI 4.60-12.32). Notably, this study performed the first subanalysis based on gallbladder presence, with findings significant for both groups [41]. Table 1 provides a comprehensive comparison of different stent types.
2.2. TBD in Resectable Distal Malignant Biliary Obstruction
The American College of Gastroenterology (ACG) 2023 guidelines recommend against preoperative TBD in most resectable DMBO cases. Notable exceptions include acute cholangitis, severe pruritus, markedly elevated serum bilirubin, and patients undergoing neoadjuvant therapy or experiencing anticipated surgical delays [12,14]. A meta-analysis of 25 studies (3 RCTs and 22 retrospective studies) demonstrated that preoperative biliary drainage associated with higher overall complications (OR 1.40, 95% CI 1.14-1.72) and wound infections (OR 1.94, 95% CI 1.48-2.53), without meaningful differences in mortality, pancreatic fistula, or intra-abdominal abscess formation. Notably, this analysis did not stratify outcomes by stent type [42]. A landmark multicenter RCT in NEJM by van der Gaag et al. (2010) demonstrated that routine preoperative biliary drainage in patients with resectable pancreatic head cancer significantly increased serious complications compared to surgery alone (74% vs 39%; RR 0.54, 95% CI 0.41-0.71; P<0.001), despite successful drainage in 94% of patients. This trial established the evidence base for current guidelines recommending against routine preoperative drainage in resectable disease, reserving it for specific indications such as acute cholangitis, severe pruritus, or patients requiring neoadjuvant therapy [43].
For borderline resectable tumors, ACG guidelines specifically recommend SEMS due to significantly longer patency and reduced cholangitis events, minimizing interruptions to neoadjuvant or palliative chemotherapy. Lower reintervention rates and reduced stent-related hospitalizations contribute to improved general and disease-specific quality of life compared with plastic stents [12,23,25,44]. For surgical DMBO candidates, FC-SEMS is recommended over U-SEMS due to ease of removal prior to surgery. However, if U-SEMS placement occurs in potential pancreaticoduodenectomy candidates, the proximal end should be positioned at least 1.5 cm below the biliary confluence to ensure adequate healthy duct length for biliary-enteric anastomosis [45,46,47].
2.3. TBD in Unresectable Hilar Malignant Biliary Obstruction
Patients with HMBO typically present at an unresectable stage, precluding surgical intervention in most cases. Specific surgical contraindications include severe medical comorbidities, distant metastases, major vascular structure involvement not amenable to reconstruction, bilateral segmental ductal involvement, unilateral segmental ductal extension with contralateral vascular involvement, and inadequate future remnant liver volume. Instead, palliative endoscopic TBD via ERCP and PTBD represent the most commonly employed approaches [48,49].
The Bismuth-Corlette classification guides HMBO management. Type 1 and 2 obstructions are typically managed similarly to DMBO, utilizing endoscopic TBD [14]. However, management of type 3 and 4 disease remains less clearly defined. Asian-Pacific consensus and European Society of Gastrointestinal Endoscopy (ESGE) guidelines recommend PTBD or combined PTBD-ERCP rather than endoscopic drainage alone for high-level stenosis (Bismuth type III or IV), considering technical difficulties and complication risks [14,50]. ACG guidelines adopt a more individualized approach, suggesting that selection should be based on disease characteristics, patient factors (comorbidities, life expectancy, anesthesia tolerance), local expertise availability, and patient preferences [12].
Optimal drainage approach selection for HMBO requires careful consideration of multiple factors, including technical feasibility, patient suitability, technique durability, and complication rates [51]. Paik et al. demonstrated superior technical success for percutaneous SEMS compared with endoscopic SEMS (92.7% vs 77.3%, P=0.049) for high-grade hilar cholangiocarcinoma, with similar complications, stent patency, and survival [52,53].
However, PTBD complications including external catheter-related pain and discomfort, technical difficulties with ascites, liver metastases, or coagulopathy, non-dilated biliary systems, and risks of tube dislodgement or peri-catheter leak have led to increasing preference for endoscopic palliation. Additionally, endoscopic TBD utilizes physiological drainage pathways, offering greater convenience compared with PTBD.
For advanced HMBO, debate continues, with Asia-Pacific and ESGE guidelines favoring PTBD while ASGE guidelines suggest individualized decisions based on patient preference, local expertise, and disease characteristics [14,49,53]. Importantly, these approaches should be viewed as complementary rather than competing modalities.
Drainage of at least 50% of liver volume represents a crucial target, as this threshold significantly predicts drainage effectiveness, correlating with lower cholangitis risk and longer patient survival in HMBO [54]. Achieving this typically requires bilateral stenting, though debate persists regarding unilateral versus bilateral approaches. While unilateral drainage offers technical simplicity and lower adverse event rates, guidelines recommend multiple stent placement to achieve >50% liver volume drainage in advanced HMBO due to incomplete drainage concerns [55,56,57,58].
Multiple stent placement presents greater technical challenges and may increase adverse outcomes such as acute cholangitis. Risk mitigation strategies include pre-procedural 3D-CT/MRCP for detailed image analysis and performance by experienced endoscopists at high-volume tertiary centers. A 2019 systematic review and meta-analysis of 9 studies with 782 patients comparing unilateral versus bilateral stenting for inoperable high-grade biliary strictures reported markedly lower reintervention rates for bilateral stenting (OR 0.59, 95% CI 0.40-0.87, P=0.009), without differences in technical success, early complications, late complications, or stent malfunction [57].
Regarding stent type for hilar obstruction, guidelines favor U-SEMS due to superior long-term drainage, reduced reintervention requirements, and preservation of cystic and intrahepatic duct outflow. Plastic stents retain utility when initial decompression is required before definitive drainage planning [12]. A February 2025 systematic review and meta-analysis of 7 studies reported C-SEMS technical and clinical success rates of 96.7% (95% CI 92.6-98.6) and 91.6% (95% CI 86.1-95.0), respectively. Overall adverse events occurred in 16.6% of cases (95% CI 11.2-23.9), including cholangitis (7.4%), pancreatitis (5.9%), liver abscess (5.9%), and cholecystitis (2.8%). Stent migration and recurrent biliary obstruction occurred in 8.9% and 49.6% of cases, with median time to recurrent biliary obstruction of 142 days. Reintervention succeeded in 92.5% of cases (95% CI 83.1-96.9) [58].
When performing bilateral stenting, the choice between side-by-side (SBS) and stent-in-stent (SIS) techniques requires consideration. A 2022 meta-analysis found that while SIS demonstrated more favorable technical success and early complication rates, SBS achieved longer stent patency [59]. However, a more recent 2025 retrospective analysis of 62 HMBO patients reported shorter stent patency in the SBS group compared with SIS (147 days vs 252 days to recurrent biliary obstruction) [60].
2.4. TBD in Resectable Hilar Malignant Biliary Obstruction
Preoperative TBD is generally not recommended for resectable HMBO, with notable exceptions including low future liver remnant (FLR) volume (<30%), cholangitis, intractable pruritus, hyperbilirubinemia-induced malnutrition, hepatic or renal insufficiency, prior to neoadjuvant therapy, and anticipated surgical delays [48]. In cases of inadequate FLR, portal vein embolization and preoperative TBD are required to achieve remnant liver hypertrophy and decrease hepatic insufficiency risk, respectively [61]. A 2017 meta-analysis of retrospective studies found preoperative TBD associated with higher post-surgical infectious complications without survival benefit (40% vs 17%), potentially due to biliary microbiome shifts promoting resistant bacteria [62].
No consensus exists regarding optimal drainage technique for patients requiring preoperative drainage. Two meta-analyses comparing endoscopic TBD and PTBD reported lower cholangitis risk with PTBD, particularly in Bismuth III/IV disease. However, a randomized controlled trial comparing these approaches was prematurely terminated due to higher mortality in the PTBD group (41% vs 11%, P=0.03) [62,63,64]. While some studies advocate nasobiliary drain use over endoscopic stenting and PTBD, prolonged hospitalization, self-removal risk, and patient discomfort limit its application [66].
Bilirubin >3 mg/dL following preoperative biliary drainage serves as a negative survival indicator. Furthermore, delaying surgery beyond 2 weeks after drainage has been associated with bacterial translocation and tumor dissemination. Therefore, surgery should proceed promptly after achieving target bilirubin levels, with prophylactic antibiotics administered [67].
2.5. Endoscopic Ultrasound-Guided Biliary Drainage
Although ERCP has served as the mainstay for therapeutic MBO management, endoscopic ultrasound-guided biliary drainage (EUS-BD) has gained substantial popularity over the past two decades due to its ability to bypass tumor invasion and avoid pancreatic duct instrumentation.
A meta-analysis of six randomized controlled trials involving 570 patients compared EUS-BD with ERCP, finding no significant differences in stent patency (mean difference 8.18 days, 95% CI -22.55 to 38.91), procedure time (mean difference -6.31 minutes, 95% CI -12.68 to 0.06), survival (mean difference 4.59 days, 95% CI -34.23 to 43.40), technical success (RR 1.04, 95% CI 0.96-1.13), clinical success (RR 1.02, 95% CI 0.96-1.08), overall adverse events (RR 0.58, 95% CI 0.24-1.43), or cholangitis (RR 1.19, 95% CI 0.39-3.61). However, EUS-BD demonstrated significantly shorter hospital stays (mean difference -1.03 days, 95% CI -1.53 to -0.53) and significantly lower risks of reintervention (RR 0.57, 95% CI 0.37-0.88), post-procedural pancreatitis (RR 0.15, 95% CI 0.03-0.66), and tumor ingrowth/overgrowth (RR 0.28, 95% CI 0.11-0.70) [68,69].
A more recent 2025 systematic review and meta-analysis comparing EUS-BD to ERCP (339 vs 331 patients) across 8 studies demonstrated that EUS-BD significantly reduced stent dysfunction risk (RR 0.46, 95% CI 0.33-0.64), post-procedure pancreatitis (RR 0.24, 95% CI 0.07-0.83), and tumor ingrowth or overgrowth (RR 0.27, 95% CI 0.11-0.65). EUS-BD also showed lower adverse event risk compared with PTBD (RR 0.37, 95% CI 0.14-0.97) and reduced hospital stay compared with both ERCP and PTBD (weighted mean difference -1.03, 95% CI -1.53 to -0.53) [70]. Table 2 provides a comprehensive comparison of EUS-BD techniques.
2.6. Endoscopic Ultrasound-Guided Choledochoduodenostomy
EUS-guided choledochoduodenostomy (EUS-CDS) creates a communication between the duodenum and common bile duct to bypass tumor-related obstruction. While the procedure has existed for years, it has been substantially simplified by lumen-apposing metal stents (LAMS) compared with plastic stents or SEMS. SEMS were initially preferred over plastic stents due to higher peritonitis and occlusion risks with plastic stents, resulting in cholangitis and repeat interventions. Furthermore, SEMS offered increased drainage diameter and stent patency [71,72]. Following LAMS introduction, multiple meta-analyses have compared these stent types. A 2021 meta-analysis pooling 31 studies with 820 patients undergoing EUS-CDS with either SEMS or LAMS found similar performance regarding technical and clinical success and adverse events, though LAMS placement appeared faster [72]. In contrast, a more recent December 2024 meta-analysis including 6 RCTs and 583 patients concluded that EUS-CDS with LAMS demonstrated significantly higher technical success compared with EUS-CDS with SEMS (RR 1.21, 95% CI 1.07-1.37) and ERCP (RR 1.17, 95% CI 1.07-1.28) [73].
Several meta-analyses have evaluated EUS-CDS technical and clinical outcomes, reporting technical success rates of 93.5-96%, clinical success rates of 88-96%, and overall complication rates of 5.2-20% [72,74,75,76,77,78]. The most frequent complications include cholangitis and cholecystitis. Other possible complications encompass peritonitis, bleeding, bilioperitoneum, pneumoperitoneum, stent migration, abdominal pain, and double mucosa puncture [79]. A meta-analysis reported pooled adverse event rates of 14% for EUS-CDS (4% cholangitis, 4% bleeding, 4% bile leak, 3% perforation) [80]. Despite high success rates, understanding factors determining success is crucial. A 2025 retrospective analysis of 296 patients across 23 centers identified multivariate risk factors for technical failure including CBD diameter ≤15 mm, duodenal stenosis, wired technique, and low operator experience (≤10 LAMS procedures) [81]. Another multivariate analysis of 2 RCTs with 152 patients similarly found extrahepatic bile duct diameter ≤15 mm associated with higher stent misdeployment and technical failure risk [82].
Stent misdeployment represents an important complication requiring prompt management. Beunon et al. achieved endoscopic rescue in 53% of patients via guidewire placement and FC-SEMS, and in 22% by positioning a new LAMS. Alternative approaches include ERCP, EUS-HGS, and gallbladder drainage. Overall endoscopic rescue success reached 77%, reducing severe complications, though 12% of technical failures still resulted in 30-day mortality [81].
EUS-CDS dysfunction, a long-term complication characterized by bilirubin rise or cholangitis onset, leads to impaired biliary drainage requiring reintervention, with reported rates ranging from 2.7-55% [71]. Vanella et al. identified duodenal invasion as an independent predictor of LAMS dysfunction and proposed a five-type classification system for stent dysfunction: stone impaction (33.3%), food impaction (18.5%), LAMS invasion or compression on the duodenal side (11.1%), and other types [83]. Key management strategies include coaxial double-pigtail stent insertion through the LAMS, balloon-assisted stent lumen clearance, and downstream gastrointestinal obstruction treatment without direct LAMS manipulation. Endoscopic reintervention effectively restores patency in most cases, with percutaneous or surgical drainage reserved for refractory situations. New EUS-CDS or PTBD placement may be feasible when needed. Additionally, the existing LAMS may serve as an access route for guidewire advancement for antegrade SEMS deployment or facilitating a rendezvous approach [71].
Given the high morbidity and mortality associated with stent dysfunction, prevention strategies merit consideration. The two most reported approaches include routine placement of either a coaxial double-pigtail stent or covered SEMS within the LAMS. The double-pigtail stent functions as a spacer, preventing opposite bile duct wall collapse against the LAMS and subsequent lumen obstruction. A covered SEMS provides similar protection while directing biliary flow toward the duodenal anastomosis side, encouraging drainage alongside the LAMS rather than through its lumen, thereby minimizing clogging and reflux [71].
2.7. Endoscopic Ultrasound-Guided Hepaticogastrostomy
EUS-guided hepaticogastrostomy (EUS-HGS), first utilized by Giovannini et al. in 2003, represents a palliative biliary drainage technique for inoperable hepatic hilar obstruction, performed under EUS guidance by creating an anastomosis between the dilated left hepatic duct and stomach [84,85]. EUS-HGS serves as a valuable option for biliary drainage in MBO when ERCP fails or proves unfeasible. Contraindications include abundant ascites, hepatic lesions obstructing biliary puncture, and interposed vessels, particularly in portal hypertension settings [85,86]. Current ESGE guidelines recommend EUS-CDS over EUS-HGS for DMBO management due to lower adverse event rates [14,80]. EUS-HGS may be preferred when duodenal access is impossible, such as in gastric outlet obstruction or post-surgical altered anatomy, where the intrahepatic approach using EUS-HGS represents the optimal alternative [85].
A 2024 meta-analysis of nine non-randomized studies and two RCTs involving 537 patients (225 EUS-HGS, 312 EUS-CDS) evaluated technical and clinical success, adverse effects, and mean procedure time. No differences emerged in technical success (OR 0.83, 95% CI 0.41-1.68) or clinical success (OR 0.96, 95% CI 0.51-1.81). However, adverse effects were markedly higher in the EUS-HGS group (OR 2.01, 95% CI 1.14-3.59). No significant difference in mean procedure time was observed [87].
A study examining EUS-HGS long-term effects found median overall survival of 144 days post-procedure. Adverse events occurred during follow-up in 65 patients (33%). Multivariate analysis revealed PC-SEMS use associated with lower recurrent biliary obstruction risk (HR 0.47, 95% CI 0.24-0.95, p=0.034). Additionally, patients with distal stenoses demonstrated better stent patency. Recurrent biliary obstruction developed in 38 cases (19.1%), with tumor ingrowth causing 36.8% of these. Other major adverse effects included abdominal pain (12.1%), infection (18.3%), peritonitis (5.6%), bleeding (6.1%), cholangitis (4.5%), biloma (3.2%), and cholecystitis (1.1%) [88]. This study notably represented the largest cohort examining EUS-HGS longer-term impact rather than early adverse event rates such as stent migration or bile leakage.
2.8. EUS-Guided Rendezvous
EUS-guided rendezvous (EUS-RV), also termed EUS-assisted bile duct access, represents a technically demanding rescue technique performed after failed ERCP. It constitutes an alternative permitting transpapillary stenting via ERCP over a guidewire previously inserted through EUS-guided intra- or extrahepatic biliary access. Technical success rates range between 72-96%, with a mean of 84-86% in expert hands. However, adverse events occur in 10-34% of cases. Current ESGE guidance restricts its indication mainly to benign biliary disease with normal anatomy after a second failed ERCP. A recent retrospective observational study found EUS-RV for malignant disease associated with worse outcomes and higher adverse effects compared with benign pathology [89].
2.9. EUS-Guided Antegrade Drainage
EUS-guided antegrade drainage (EUS-AG) involves biliary access with guidewire advancement through the stricture into the small bowel lumen, followed by antegrade metal stent deployment through the papilla or anastomosis in altered anatomy. Though technically difficult with high failure rates, this technique preserves normal anatomy. A recent systematic review of 9 studies with 210 patients reported overall technical success of 92% and overall adverse event rate of 14%, with pancreatitis representing the predominant post-procedure complication [14,90].
2.10. EUS-Guided Gallbladder Drainage
EUS-guided gallbladder drainage (EUS-GBD), long utilized for cholecystitis treatment, has recently gained popularity for biliary drainage when ERCP is contraindicated. Three recent meta-analyses evaluating EUS-GBD role in DMBO reported clinical success rates of 85-89%, adverse events in 10-13%, technical success of 99.2-100%, and dysfunction rates of 9% [91,92,93]. Most included studies were retrospective from expert tertiary centers, potentially skewing results favorably toward EUS-GBD.
The multicenter GALLBLADEUS study compared EUS-CDS (37 patients) versus EUS-GBD (41 patients), finding similar clinical and technical success rates (87.8% vs 89.2%), but higher late morbidity (>24h) in the EUS-CDS group (21.6% vs 7.3%) [94].
3. Emerging Developments and Future Directions
3.1. EUS-Guided Gastroenterostomy Versus Surgical Gastrojejunostomy
Current gold standard treatment for gastric outlet obstruction (GOO) involves either surgical gastroenterostomy or endoscopic stenting (ES). Surgery carries invasiveness with high adverse event rates, while ES demonstrates high reintervention rates and stent patency limitations. EUS-guided gastroenterostomy (EUS-GE) has emerged as an alternative potentially providing longer stent patency without surgical invasiveness. (95, 96)
A systematic review and meta-analysis of 5 studies (507 patients), including 1 RCT and 4 matched-control studies, reported statistically significant differences between EUS-GE and ES in clinical success (OR 2.81, 95% CI 1.58-4.99, P<0.001). The study concluded EUS-GE represents a reasonable option for malignant GOO treatment with high success rates, particularly at tertiary centers [95].
The ENDURO trial, a multicenter RCT published in The Lancet in December 2025, compared endoscopic versus surgical gastroenterostomy for malignant GOO palliation in 98 patients (48 endoscopic, 50 surgical). The endoscopic group demonstrated shorter time to solid oral intake (median 1 vs 3 days). Both groups had comparable persistent or recurrent obstructive symptoms requiring reintervention (5 vs 6 patients). Overall adverse events occurred in 28 (58%) endoscopic patients versus 32 (64%) surgical patients (RR 0.91, 95% CI 0.66-1.25). Three fatal events occurred in the surgical group compared with one in the endoscopic group [96]. These promising results in both clinical outcomes and cost-effectiveness warrant additional randomized studies.
3.2. Artificial Intelligence in Predicting Stent Failure and Complications
Artificial intelligence (AI) use in gastroenterology has expanded rapidly in recent years. For MBO, emerging studies have explored AI-based model ability to predict outcomes such as stent failure and complications including cholangitis. Earlier and more accurate high-risk scenario identification may support future targeted preventive strategies.
A retrospective study of 218 patients investigated how machine learning could inform cholangitis risk factors post-ERCP stent implantation. Twenty-seven clinical variables served as input for seven models subsequently trained and tested for classification prediction. The Reinforcement Fine-Tuning (RFT) model achieved high success with reported accuracies up to 0.86 and area under the receiver operator characteristics curve (AUROC) up to 0.87 [97].
A comparative analysis of 285 patients published in 2025 compared logistic regression and artificial neural network (ANN) models in predicting early mortality following stent placement in MBO. The logistic regression model using CA19-9 and prior ERCP as key predictors achieved moderate discriminative performance (AUC 0.727, accuracy 65%). In contrast, the ANN model incorporating five clinical variables demonstrated superior overall performance (AUC 0.813, accuracy 88.2%), with notably higher specificity (95.5% vs 83.3%), but marginally lower sensitivity (61.1% vs 61.2%) [98].
A retrospective multicenter study examining AI’s ability to predict post-ERCP cholangitis (PEC) in MBO patients selected radiofrequency ablation, white blood cell count, jaundice severity, and serum amylase as independent PEC risk factors. These were then inputted into 6 machine learning models and tested on 395 patients. Among the six models, XGBoost performed best on external patients with an AUC of 0.7270 [99].
These studies show promise that AI may eventually help predict complications in high-risk patients, allowing early individualized treatment planning and hopefully preventing these complications. Further development and testing with larger cohorts remains necessary.
4. Conclusion
Malignant biliary obstruction requires timely expert intervention to prevent severe morbidity and mortality [1,2,3,4,5]. While ERCP with SEMS placement remains the gold standard for most cases, [12,13,14] EUS-guided biliary drainage has emerged as a valuable complementary approach with reduced reintervention rates, lower pancreatitis risk, and shorter hospitalizations [67,68,69].
For distal MBO, FC-SEMS demonstrates superior patency compared to U-SEMS (445 vs 348 days), [39] though migration risk remains a consideration [32,33,34,40,41]. In hilar MBO, achieving ≥50% liver volume drainage through bilateral stenting when feasible is crucial for optimal outcomes, [53] though technical complexity must be balanced against complication risk [56,57,58,59].
EUS-guided techniques offer distinct advantages: EUS-CDS achieves 93.5-96% technical success for DMBO with lower tumor ingrowth, [71,72,73,74,75,76,77] while EUS-GBD demonstrates lower late morbidity (7.3% vs 21.6%) [93]. EUS-HGS serves specific roles in HMBO and altered anatomy, though with higher adverse events [84,85,86,87]. For malignant gastric outlet obstruction, EUS-GE provides faster recovery, shorter hospitalization, and lower costs versus surgery [95,96].
Optimal outcomes require high-volume tertiary centers with experienced endoscopists [12,14]. Treatment selection must be individualized based on tumor characteristics (distal vs. hilar, resectable vs. unresectable), anatomical considerations, patient factors, and local expertise [12,47,48,49]. ERCP and EUS-BD should be viewed as complementary modalities, each offering distinct advantages in appropriate clinical contexts. Future priorities include head-to-head trials comparing EUS-BD with ERCP as first-line therapy, standardization of EUS-BD techniques, validation of AI-based predictive models for complication risk, [97,98,99] and development of novel stent designs to improve patency and reduce dysfunction.

Table 3.
Clinical Decision-Making Algorithm for Endoscopic Management of Malignant Biliary Obstruction.
Table 3.
Clinical Decision-Making Algorithm for Endoscopic Management of Malignant Biliary Obstruction.
| Clinical Scenario | First-Line Approach | Second-Line/Rescue | Key Considerations |
|---|---|---|---|
| Unresectable DMBO [12,14,23,24,25,32,33,39,40,41] | ERCP with FC-SEMS or U-SEMS | EUS-CDS with LAMS or EUS-GBD | SEMS preferred; C-SEMS for longer patency |
| Resectable/Borderline Resectable DMBO [12,14,42,43,44,45,46,47] | SEMS (FC-SEMS preferred) | Avoid preoperative drainage except: cholangitis, high bilirubin, neoadjuvant therapy | FC-SEMS allows easy removal; Place ≥1.5 cm below confluence |
| Unresectable HMBO (Bismuth I-II) [12,14] | ERCP with SEMS (U-SEMS preferred) | EUS-HGS or PTBD | Similar to DMBO management |
| Unresectable HMBO (Bismuth III-IV) [12,14,48,49,50,51,52,53,54,55,56,57,58,59,60] | Bilateral ERCP stenting (>50% liver volume) OR PTBD | EUS-HGS or Combined approach | High-volume center; 3D-CT/MRCP; U-SEMS preferred |
| Resectable HMBO [48,61,62,63,64,65,66,67] | Generally avoid drainage; If needed: ERCP or PTBD | Surgery within 2 weeks after target bilirubin | Indications: FLR <30%, cholangitis, high bilirubin, neoadjuvant therapy |
| Failed ERCP in DMBO [68,69,70,71,72,73,80,81,82,83] | EUS-CDS with LAMS OR EUS-GBD | PTBD | Lower reintervention, pancreatitis; CBD >15mm better; EUS-GBD lower late morbidity |
| Failed ERCP in HMBO [80,84,85,86,87,88] | EUS-HGS | PTBD | Higher adverse events; Avoid in ascites, portal hypertension; PC-SEMS reduces RBO |
| Gastric Outlet Obstruction + MBO [96] | EUS-GE with biliary drainage | Surgical gastrojejunostomy | Faster recovery (1 vs 3 days), shorter stay (3 vs 9 days), lower cost |
Abbreviations: DMBO, distal malignant biliary obstruction; HMBO, hilar malignant biliary obstruction; ERCP, endoscopic retrograde cholangiopancreatography; SEMS, self-expanding metal stent; FC-SEMS, fully covered SEMS; U-SEMS, uncovered SEMS; C-SEMS, covered SEMS; EUS-CDS, endoscopic ultrasound-guided choledochoduodenostomy; EUS-GBD, endoscopic ultrasound-guided gallbladder drainage; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; LAMS, lumen-apposing metal stent; PTBD, percutaneous transhepatic biliary drainage; FLR, future liver remnant; EUS-GE, endoscopic ultrasound-guided gastroenterostomy; RBO, recurrent biliary obstruction; CBD, common bile duct.
Table 4.
A summary of the top five papers over the past two years regarding MBO.
| Authors, year | Title | Type of study | Number of studies/ patients | Key findings |
|---|---|---|---|---|
| Lopimpisuth et al., 2025 [41] | Postprocedural cholecystitis following covered self-expandable metal stent placement in patients with distal malignant biliary obstruction |
Systematic Review and Meta-Analysis | 21 studies 5753 patients |
CSEMS showed higher post-ERCP acute cholecystitis rates, lower tumor in growth rates, and higher rates of stent migration |
| Chung et al., 2025 [58] | Efficacy and safety of covered self-expandable metal stents for malignant hilar biliary obstruction |
Systematic Review and Meta-Analysis | 7 studies 194 patients |
High technical and clinical success rates of CSEMS placement in MHBO. Adverse events: cholangitis, cholecystitis, and pancreatitis, were <10%. |
| Zafar et al., 2025 [70] | Efficacy of endoscopic ultrasound-guided biliary drainage of malignant biliary obstruction | Systematic Review and Meta-Analysis | 8 studies 670 patients |
EUS-BD performed better than ERCP-BD and PTBD in reducing stent dysfunction, postprocedural pancreatitis, and tumor ingrowth or overgrowth. |
| Lauri et al., 2024 [73] | Primary drainage of distal malignant biliary obstruction |
A comparative network meta-analysis | 6 RCTs 583 patients |
EUS-CDS with LAMS had the highest technical and clinical success rates and was significantly superior to ERCP as the upfront technique for dMBO treatment. |
| van de Pavert et al., 2025 [96] | Endoscopic versus surgical gastroenterostomy for palliation of malignant gastric outlet obstruction (ENDURO) |
Multicenter RCT | 98 patients (48 endoscopic, 50 surgical) |
Endoscopic group demonstrated shorter time to solid oral intake (1 vs 3 days). Comparable reintervention rates (5 vs 6 patients). Overall adverse events 58% endoscopic vs 64% surgical (RR 0.91, 95% CI 0.66-1.25). Three fatal events in surgical group vs one in endoscopic group. |
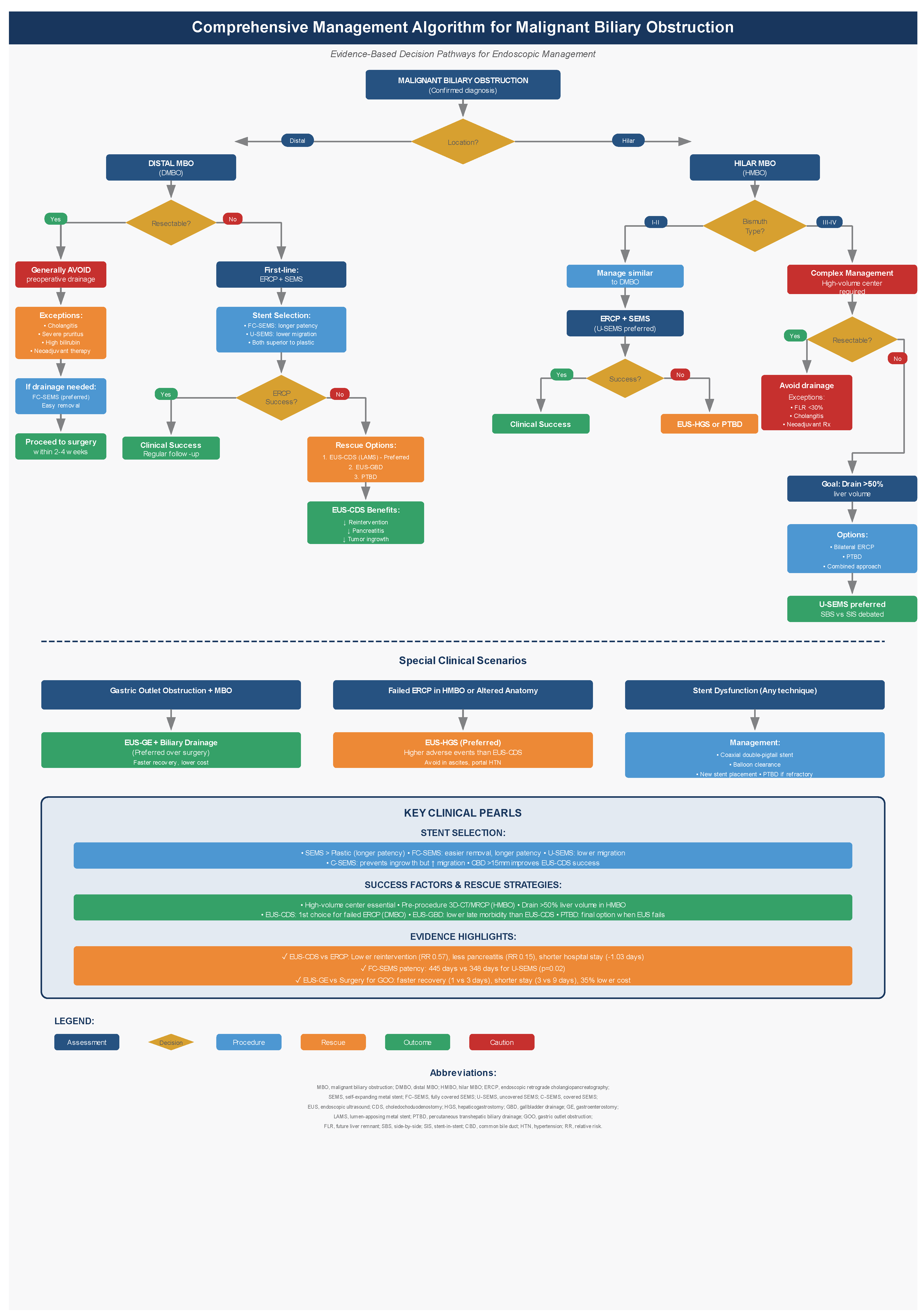
Figure 1.
Comprehensive Management Algorithm for Malignant Biliary Obstruction. Decision-making flowchart for endoscopic intervention selection based on anatomical location, resectability status, and technical feasibility.
Figure 1.
Comprehensive Management Algorithm for Malignant Biliary Obstruction. Decision-making flowchart for endoscopic intervention selection based on anatomical location, resectability status, and technical feasibility.
References
- Okamoto, T. Malignant biliary obstruction due to metastatic non-hepato-pancreato-biliary cancer. World J Gastroenterol. 2022, 28, 985–1008. [Google Scholar] [CrossRef]
- Qiu, Feng MM; Yang, Tianchi MM; Han, Wei, PhD. Comparison of Biliary Drainage Techniques for MBO: A Meta-Analysis. Pancreas 2025, 54(9), p e796–e805. [Google Scholar] [CrossRef]
- Mikalsen, I. M.; Breder, S.; Medhus, A. W.; Folseraas, T.; Aabakken, L.; Ånonsen, K. V. ERCP for the initial management of malignant biliary obstruction – real world data on 596 procedures. Scandinavian Journal of Gastroenterology 2024, 59(3), 369–377. [Google Scholar] [CrossRef]
- Tsetis, D; Krokidis, Μ; Negru, D; et al. Malignant biliary obstruction: the current role of interventional radiology. Ann Gastroenterol. 2016, 29(1), 33–36. [Google Scholar]
- Pachisia, AV; Govil, D. Ultrasound-guided bedside percutaneous transhepatic biliary drainage in critically ill: a friend indeed. Indian J Crit Care Med. 2023, 27, 4–5. [Google Scholar]
- Binda, C.; Trebbi, M.; Coluccio, C.; Giuffrida, P.; Perini, B.; Gibiino, G.; Fabbri, S.; Liverani, E.; Fabbri, C. Endoscopic management of malignant biliary obstructions. Annals of gastroenterology 2024, 37(3), 291–302. [Google Scholar] [CrossRef] [PubMed]
- Canakis, A; Kahaleh, M. Endoscopic palliation of malignant biliary obstruction. World J Gastrointest Endosc 2022, 14, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, Y; Viesca, M; Arvanitakis, M. Early diagnosis and management of malignant distal biliary obstruction: a review on current recommendations and guidelines. Clin Exp Gastroenterol 2019, 12, 415–432. [Google Scholar] [CrossRef]
- Fugazza, A; Fabbri, C; Di Mitri, R; i-EUS Group. EUS-guided choledochoduodenostomy for malignant distal biliary obstruction after failed ERCP: a retrospective nationwide analysis. Gastrointest Endosc 2022, 95, 896–904. [Google Scholar] [CrossRef]
- Pietrzak, J.; Przybyłkowski, A. Endoscopic Treatment of Malignant Hilar Biliary Obstruction. Cancers 2023, 15(24), 5819. [Google Scholar] [CrossRef] [PubMed]
- Mosconi, C.; Renzulli, M.; Giampalma, E.; Galuppi, A.; Balacchi, C.; Brandi, G.; Ercolani, G.; Bianchi, G.; Golfieri, R. Unresectable perihilar cholangiocarcinoma: Multimodal palliative treatment. Anticancer. Res. 2013, 33, 2747–2753. [Google Scholar]
- Elmunzer, BJ; Maranki, JL; Gómez, V; et al. ACG Clinical Guideline: Diagnosis and management of biliary strictures. Am J Gastroenterol 2023, 118, 405–426. [Google Scholar] [CrossRef]
- van der Merwe, SW; van Wanrooij, RLJ; Bronswijk, M; et al. Therapeutic endoscopic ultrasound: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022, 54, 185–205. [Google Scholar] [CrossRef]
- Dumonceau, JM; Tringali, A; Papanikolaou, IS; et al. Endoscopic biliary stenting: indications, choice of stents, and results: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline – Updated October 2017. Endoscopy 2018, 50, 910–930. [Google Scholar] [CrossRef]
- Ekkelenkamp, VE; de Man, RA; Ter Borg, F; et al. Prospective evaluation of ERCP performance: results of a nationwide quality registry. Endoscopy 2015, 47, 503–507. [Google Scholar] [CrossRef] [PubMed]
- de Jong, M. J. P.; van Delft, F.; van Geenen; et al. Endoscopic ultrasound-guided choledochoduodenostomy results in fewer complications than percutaneous drainage following failed ERCP in malignant distal biliary obstruction. Endoscopy 2025, 57(9), 1004–1015. [Google Scholar] [CrossRef] [PubMed]
- Alves de Lima, SL; Bustamante, FAC; Hourneaux de Moura, EG; et al. Endoscopic palliative treatment vs surgical bypass in malignant low bile duct obstruction:a systematic review and meta-analysis. Int J Hepatobiliary Pancreat Dis. 2015, 5, 35–45. [Google Scholar] [CrossRef]
- Inamdar, S; Slattery, E; Bhalla, R; Sejpal, DV; Trindade, AJ. Comparison of adverse events for endoscopic vs percutaneous biliary drainage in the treatment of malignant biliary tract obstruction in an inpatient national cohort. JAMA Oncol. 2016, 2, 112–117. [Google Scholar] [CrossRef]
- Deniz, S; Öcal, O; Wildgruber, M; et al. Percutaneous transhepatic biliary drainage (PTBD) in patients with biliary leakage: Technical and clinical outcomes. Medicine (Baltimore) 2023, 102, e35213. [Google Scholar] [CrossRef]
- Nennstiel, S; Weber, A; Frick, G; et al. Drainage-related complications in percutaneous transhepatic biliary drainage:an analysis over 10 years. J Clin Gastroenterol. 2015, 49, 764–770. [Google Scholar] [CrossRef] [PubMed]
- Park, C. H.; Park, S. W.; Jung, J. H.; Jung, E. S.; Kim, J. H.; Park, D. H. Comparative Efficacy of Various Stents for Palliation in Patients with Malignant Extrahepatic Biliary Obstruction: A Systematic Review and Network Meta-Analysis. Journal of personalized medicine 2021, 11(2), 86. [Google Scholar] [CrossRef]
- Walta, D.C.; Fausel, C.S.; Brant, B. Endoscopic biliary stents and obstructive jaundice. Am. J. Surg. 1987, 153, 444–447. [Google Scholar] [CrossRef]
- A Almadi, M.; Barkun, A.; Martel, M. Plastic vs. self-expandable metal stents for palliation in malignant biliary obstruction: A series of meta-analyses. Am. J. Gastroenterol. 2017, 112, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Isayama, H.; Hamada, T.; Yasuda, I.; et al. TOKYO criteria 2014 for transpapillary biliary stenting. Dig. Endosc. 2015, 27, 259–264. [Google Scholar] [CrossRef] [PubMed]
- Sawas, T.; Al Halabi, S.; Parsi, M.A.; Vargo, J. Self-expandable metal stents versus plastic stents for malignant biliary obstruction: A meta-analysis. Gastrointest. Endosc. 2015, 82, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Walter, D.; Van Boeckel, P.G.A.; Groenen, M.J.; et al. Cost efficacy of metal stents for palliation of extrahepatic bile duct obstruction in a randomized controlled trial. Gastroenterology 2015, 149, 130–138. [Google Scholar] [CrossRef]
- Bor, R.; Fábián, A.; Szűcs, M.; et al. Comparison of therapeutic efficacy and treatment costs of self-expandable metal stents and plastic stents for management of malignant biliary obstruction. BMC Gastroenterol 2023, 23, 41. [Google Scholar] [CrossRef]
- Tamura, T; Ashida, R; Kawaji, Y; et al. Self-expandable metal vs. plastic stents for preoperative biliary drainage in patients receiving neoadjuvant chemotherapy. Clin Endosc. 2025, 58(6), 817–825. [Google Scholar] [CrossRef]
- Endo, Y; Tanaka, M; Kitago, M; et al. Comparison between plastic and metallic biliary stent placement for preoperative patients with pancreatic head cancer: a systematic review and meta-analysis. Ann Surg Oncol 2024, 31, 1319–1327. [Google Scholar] [CrossRef]
- Coté, GA; Kumar, N; Ansstas, M; et al. Risk of post-ERCP pancreatitis with placement of self-expandable metallic stents. Gastrointest Endosc 2010. [Google Scholar] [CrossRef]
- Tamura, T; Yamai, T; Uza, N; et al. Adverse events of self-expandable metal stent placement for malignant distal biliary obstruction: a large multicenter study. Gastrointest Endosc 2024, 99, 61–72. [Google Scholar] [CrossRef]
- Tringali, A; Hassan, C; Rota, M; et al. Covered vs. uncovered self-expandable metal stents for malignant distal biliary strictures: a systematic review and meta-analysis. Endoscopy 2018, 50(06), 631–41. [Google Scholar]
- Vanella, G; Coluccio, C; Cucchetti, A; et al. Fully covered versus partially covered self-expandable metal stents for palliation of distal malignant biliary obstruction: a systematic review and meta-analysis. Gastrointest Endosc. 2024, 99(3), 314–322. [Google Scholar] [CrossRef] [PubMed]
- Park, C. H.; Park, S. W.; Jung, J. H.; Jung, E. S.; Kim, J. H.; Park, D. H. Comparative Efficacy of Various Stents for Palliation in Patients with Malignant Extrahepatic Biliary Obstruction: A Systematic Review and Network Meta-Analysis. Journal of personalized medicine 2021, 11(2), 86. [Google Scholar] [CrossRef] [PubMed]
- Lee, JH; Krishna, SG; Singh, A; et al. Comparison of the utility of covered metal stents versus uncovered metal stents in the management of malignant biliary strictures in 749 patients. Gastrointest Endosc. 2013, 78, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Isayama, H; Komatsu, Y; Tsujino, T; et al. A prospective randomised study of “covered”versus “uncovered”diamond stents for the management of distal malignant biliary obstruction. Gut 2004, 53, 729–734. [Google Scholar] [CrossRef]
- Kitano, M; Yamashita, Y; Tanaka, K; et al. Covered self-expandable metal stents with an anti-migration system improve patency duration without increased complications compared with uncovered stents for distal biliary obstruction caused by pancreatic carcinoma: a randomized multicenter trial. Am J Gastroenterol. 2013, 108, 1713–1722. [Google Scholar] [CrossRef]
- Ghazi, R; AbiMansour, JP; Mahmoud, T; et al. Uncovered versus fully covered self-expandable metal stents for the management of distal malignant biliary obstruction. Gastrointest Endosc. 2023, 98, 577–584. [Google Scholar] [CrossRef]
- Zhang, D.; Luo, T.; Gao, F.; et al. Comparison of fully covered versus uncovered self-expandable metallic stents in treating inoperable malignant distal biliary obstruction: a retrospective study. Therapeutic advances in gastrointestinal endoscopy 2025, 18. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y; Tachikawa, A; Shimokawa, T; et al. Covered versus uncovered metal stent for endoscopic drainage of a malignant distal biliary obstruction: Meta-analysis. Dig Endosc. 2022, 34, 938–951. [Google Scholar] [CrossRef]
- Lopimpisuth, C; Vedantam, S; Danpanichkul, P; et al. Postprocedural cholecystitis following covered self-expandable metal stent placement in patients with distal malignant biliary obstruction: a systematic review and meta-analysis. Gastrointest Endosc 2025. [Google Scholar] [CrossRef]
- Scheufele, F; Schorn, S; Demir, IE; et al. Preoperative biliary stenting versus operation first in jaundiced patients due to malignant lesions in the pancreatic head: A meta-analysis of current literature. Surgery 2017, 161, 939–950. [Google Scholar] [CrossRef]
- van der Gaag, NA; Rauws, EA; van Eijck, CH; Bruno, MJ; van der Harst, E; Kubben, FJ; Gerritsen, JJ; Greve, JW; Gerhards, MF; de Hingh, IH; Klinkenbijl, JH; Nio, CY; de Castro, SM; Busch, OR; van Gulik, TM; Bossuyt, PM; Gouma, DJ. Preoperative biliary drainage for cancer of the head of the pancreas. N Engl J Med 2010, 362(2), 129–37. [Google Scholar] [CrossRef]
- Jang, S; Stevens, T; Parsi, MA; et al. Superiority of self-expandable metallic stents over plastic stents in treatment of malignant distal biliary strictures. Clinical Gastroenterology and Hepatology 2022, 20(2), e182-95. [Google Scholar] [CrossRef]
- Aadam, AA; Evans, DB; Khan, A; et al. Efficacy and safety of self-expandable metal stents for biliary decompression in patients receiving neoadjuvant therapy for pancreatic cancer: a prospective study. Gastrointestinal endoscopy 2012, 76(1), 67–75. [Google Scholar] [CrossRef]
- Siddiqui, AA; Mehendiratta, V; Loren, D; et al. Self-expanding metal stents (SEMS) for preoperative biliary decompression in patients with resectable and borderline-resectable pancreatic cancer: outcomes in 241 patients. Digestive diseases and sciences 2013, 58(6), 1744–50. [Google Scholar] [CrossRef] [PubMed]
- Ballard, DD; Rahman, S; Ginnebaugh, B; et al. Safety and efficacy of self-expanding metal stents for biliary drainage in patients receiving neoadjuvant therapy for pancreatic cancer. Endoscopy International Open 2018, 6(06), E714-21. [Google Scholar] [CrossRef] [PubMed]
- Mansour, JC; Aloia, TA; Crane, CH; et al. Hilar cholangiocarcinoma: expert consensus statement. HPB (Oxford) 2015, 17, 691–9. [Google Scholar] [CrossRef] [PubMed]
- Lee, TH. Proper management of inoperable malignant hilar biliary obstruction. International Journal of Gastrointestinal Intervention 2021, 10(3), 120–7. [Google Scholar] [CrossRef]
- Rerknimitr, R; Angsuwatcharakon, P; Ratanachu-ek, T; et al. Asia-Pacific consensus recommendations for endoscopic and interventional management of hilar cholangiocarcinoma. J Gastroenterol Hepatol. 2013, 28, 593–607. [Google Scholar] [CrossRef]
- Dhar, J.; Gupta, P.; Samanta, J. The role of endoscopy in malignant hilar obstruction. Annals of gastroenterology 2023, 36(4), 347–359. [Google Scholar] [CrossRef]
- Paik, WH; Park, YS; Hwang, JH; et al. Palliative treatment with self-expandable metallic stents in patients with advanced type III or IV hilar cholangiocarcinoma: a percutaneous versus endoscopic approach. Gastrointest Endosc. 2009, 69, 55–62. [Google Scholar] [CrossRef]
- Qumseya, BJ; Jamil, LH; Elmunzer, BJ; et al. ASGE guideline on the role of endoscopy in the management of malignant hilar obstruction. Gastrointest Endosc. 2021, 94, 222–234. [Google Scholar] [CrossRef]
- Vienne, A; Hobeika, E; Gouya, H; et al. Prediction of drainage effectiveness during endoscopic stenting of malignant hilar strictures: the role of liver volume assessment. Gastrointest Endosc. 2010, 72, 728–735. [Google Scholar] [CrossRef]
- Lee, TH; Moon, JH; Choi, JH; et al. Prospective comparison of endoscopic bilateral stent-in-stent versus stent-by-stent deployment for inoperable advanced malignant hilar biliary stricture. Gastrointest Endosc. 2019, 90, 222–230. [Google Scholar] [CrossRef] [PubMed]
- De Palma, GD; Galloro, G; Siciliano, S; et al. Unilateral versus bilateral endoscopic hepatic duct drainage in patients with malignant hilar biliary obstruction: results of a prospective, randomized, and controlled study. Gastrointest Endosc. 2001, 53, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Ashat, M.; Arora, S.; Klair, J. S.; et al. Bilateral vs unilateral placement of metal stents for inoperable high-grade hilar biliary strictures: A systemic review and meta-analysis. World journal of gastroenterology 2019, 25(34), 5210–5219. [Google Scholar] [CrossRef]
- Chung, KH; Lee, KJ; Joseph, AA; et al. Efficacy and safety of covered self-expandable metal stents for malignant hilar biliary obstruction: systematic review and meta-analysis. Gastrointest Endosc. 2025, 101(2), 350–357. [Google Scholar] [CrossRef]
- Chen, L.; Gao, G. M.; Li, D. L.; Chen, Z. K. Side-by-side versus stent-in-stent bilateral stenting for malignant hilar biliary obstruction: a meta-analysis. Videosurgery and other miniinvasive techniques 2022, 17(2), 279–288. [Google Scholar] [CrossRef]
- Imamura, S.; Watanabe, K.; Inoue, K.; et al. Side-by-side versus stent-in-stent technique for stent deployment during systemic chemotherapy in biliary tract cancer patients. DEN open 2025, 5(1), e70075. [Google Scholar] [CrossRef] [PubMed]
- Wiggers, JK; Groot Koerkamp, B; Cieslak, KP; et al. Postoperative mortality after liver resection for perihilar cholangiocarcinoma. J Am Coll Surg. 2016, 223, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Celotti, A; Solaini, L; Montori, G; et al. Preoperative biliary drainage in hilar cholangiocarcinoma: Systematic review and meta-analysis. Eur J Surg Oncol. 2017, 43, 1628–1635. [Google Scholar] [CrossRef] [PubMed]
- Hameed, A; Pang, T; Chiou, J; et al. Percutaneous vs. endoscopic pre-operative biliary drainage in hilar cholangiocarcinoma. HPB (Oxford) 2016, 18, 400–410. [Google Scholar] [CrossRef] [PubMed]
- Al Mahjoub, A; Menahem, B; Fohlen, A; et al. Preoperative biliary drainage in patients with resectable perihilar cholangiocarcinoma. J Vasc Interv Radiol. 2017, 28, 576–582. [Google Scholar] [CrossRef]
- Coelen, RJS; Roos, E; Wiggers, JK; et al. Endoscopic versus percutaneous biliary drainage in patients with resectable perihilar cholangiocarcinoma. Lancet Gastroenterol Hepatol. 2018, 3, 681–690. [Google Scholar] [CrossRef]
- Kawakami, H; Kuwatani, M; Onodera, M; et al. Endoscopic nasobiliary drainage is the most suitable preoperative biliary drainage method. J Gastroenterol. 2011, 46, 242–248. [Google Scholar] [CrossRef]
- Paik, WH; Loganathan, N; Hwang, JH. Preoperative biliary drainage in hilar cholangiocarcinoma: when and how? World J Gastrointest Endosc. 2014, 6, 68–73. [Google Scholar] [CrossRef]
- Barbosa, EC; do Espírito Santo, PA; Baraldo, S; et al. EUS- versus ERCP-guided biliary drainage for malignant biliary obstruction. Gastrointest Endosc 2024, 100, 395–405. [Google Scholar] [CrossRef]
- Paik, WH; Lee, TH; Park, DH; et al. EUS-Guided Biliary Drainage Versus ERCP for the Primary Palliation of Malignant Biliary Obstruction: A Multicenter Randomized Clinical Trial. Am J Gastroenterol. 2018, 113, 987–997. [Google Scholar] [CrossRef]
- Zafar, Y; Azam, H; Azhar, MAB; Shaheen, F; Javaid, SS; Manzoor, L; Masood, M; Krishnamoorthi, R. Efficacy of endoscopic ultrasound-guided biliary drainage of malignant biliary obstruction: a systematic review and meta-analysis of randomized controlled trials. Clin Endosc. 2025, 58(4), 533–543. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lambin, T.; Leblanc, S.; Napoléon, B. Advances in EUS-Guided Biliary Drainage for the Management of Pancreatic Cancer. Cancers 2025, 17(21), 3428. [Google Scholar] [CrossRef]
- Amato, A.; Sinagra, E.; Celsa, C.; et al. Efficacy of Lumen-Apposing Metal Stents or Self-Expandable Metal Stents for Endoscopic Ultrasound-Guided Choledochoduodenostomy. Endoscopy 2021, 53, 1037–1047. [Google Scholar] [CrossRef] [PubMed]
- Lauri, G; Archibugi, L; Arcidiacono, PG; et al. Primary drainage of distal malignant biliary obstruction: A comparative network meta-analysis. Dig Liver Dis. 2024, 56(12), 2004–2010. [Google Scholar] [CrossRef] [PubMed]
- Uemura, R.S.; Khan, M.A.; Otoch, J.P.; et al. EUS-Guided Choledochoduodenostomy Versus Hepaticogastrostomy. J. Clin. Gastroenterol. 2018, 52, 123–130. [Google Scholar] [CrossRef]
- Krishnamoorthi, R.; Dasari, C.S.; Chandrasekar, V.T.; et al. Effectiveness and Safety of EUS-Guided Choledochoduodenostomy Using Lumen-Apposing Metal Stents. Surg. Endosc. 2020, 34, 2866–2877. [Google Scholar] [CrossRef]
- Li, J.-S.; Tang, J.; Fang, J.; et al. Adverse Events in Endoscopic Ultrasound-Guided Choledochoduodenostomy with Lumen-Apposing Metal Stents. J. Gastroenterol. Hepatol. 2024, 39, 1769–1779. [Google Scholar] [CrossRef]
- Fugazza, A.; Khalaf, K.; Spadaccini, M.; et al. Outcomes Predictors in Endoscopic Ultrasound-Guided Choledochoduodenostomy with Lumen-Apposing Metal Stent. Endosc. Int. Open. 2024, 12, E456–E462. [Google Scholar]
- Khoury, T.; Sbeit, W.; Fumex, F.; et al. Endoscopic Ultrasound- versus ERCP-Guided Primary Drainage of Inoperable Malignant Distal Biliary Obstruction. Endoscopy 2024, 56, 955–963. [Google Scholar] [CrossRef]
- Ogura, T; Itoi, T. Technical Tips and Recent Development of Endoscopic Ultrasound-Guided Choledochoduodenostomy. DEN Open 2021, 1, e8. [Google Scholar] [CrossRef]
- Mohan, BP; Shakhatreh, M; Garg, R; et al. Efficacy and safety of endoscopic ultrasound-guided choledochoduodenostomy. J Clin Gastroenterol. 2019, 53, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Beunon, C; Debourdeau, A; Schaefer, M; et al. Technical failure of endoscopic ultrasound-guided choledochoduodenostomy. Endoscopy 2025, 57(9), 990–1000. [Google Scholar] [CrossRef]
- Chen, YI; Long, C; Sahai, AV; et al. Stent misdeployment and factors associated with failure in endoscopic ultrasound-guided choledochoduodenostomy. Endoscopy 2025, 57(4), 330–338. [Google Scholar] [PubMed]
- Vanella, G; Bronswijk, M; Dell’Anna, G; et al. Classification, risk factors, and management of lumen apposing metal stent dysfunction. Dig Endosc. 2023, 35, 377–388. [Google Scholar] [CrossRef]
- Giovannini, M.; Moutardier, V.; Pesenti, C.; et al. Endoscopic ultrasound-guided bilioduodenal anastomosis. Endoscopy 2001, 33, 898–900. [Google Scholar] [CrossRef]
- Mazza, S.; Masciangelo, G.; Mauro, A.; et al. Endoscopic Ultrasound-Guided Hepaticogastrostomy in Malignant Biliary Obstruction. Diagnostics 2024, 14(23), 2644. [Google Scholar] [CrossRef]
- van Wanrooij, R.L.J.; Bronswijk, M.; Kunda, R.; et al. Therapeutic Endoscopic Ultrasound: ESGE Technical Review. Endoscopy 2022, 54, 310–332. [Google Scholar] [CrossRef]
- Rizqiansyah, CY; Awatara, PID; Amar, N; et al. Efficacy and safety of EUS hepaticogastrostomy versus choledochoduodenostomy. JGH Open 2024, 8(10), e70037. [Google Scholar] [CrossRef] [PubMed]
- Hedjoudje, A; Pokossy Epée, J; Perez-Cuadrado-Robles, E; et al. Long-term outcomes of endoscopic ultrasound-guided hepaticogastrostomy. United European Gastroenterol J 2024, 12(8), 1044–1055. [Google Scholar] [CrossRef] [PubMed]
- Gornals, J. B.; Sumalla-Garcia, A.; Quintana, S.; et al. Endoscopic ultrasound-guided biliary rendezvous after failed cannulation. Annals of Medicine 2024, 56(1). [Google Scholar] [CrossRef]
- Iwashita, T; Uemura, S; Tezuka, R; et al. Current status of endoscopic ultrasound-guided antegrade intervention. Dig Endosc. 2023, 35, 264–274. [Google Scholar] [CrossRef]
- Khoury, T.; Farraj, M.; Sbeit, W.; et al. EUS-Guided Gallbladder Drainage of Inoperable Malignant Distal Biliary Obstruction. Cancers 2025, 17, 1983. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, G.E.M.; Crinò, S.F.; Vanella, G.; et al. EUS-Guided Gallbladder Drainage as a Rescue in Distal Malignant Biliary Obstruction. Endosc. Ultrasound 2025, 14, 41–47. [Google Scholar] [CrossRef]
- Kamal, F.; Khan, M.A.; Lee-Smith, W.; et al. Efficacy and Safety of EUS-Guided Gallbladder Drainage for Rescue Treatment. Endosc. Ultrasound 2022, 12, 8–15. [Google Scholar] [CrossRef]
- Debourdeau, A.; Daniel, J.; Caillo, L.; et al. Effectiveness of endoscopic ultrasound-guided choledochoduodenostomy vs. EUS-guided gallbladder drainage. Digestive endoscopy 2025, 37(1), 103–114. [Google Scholar] [CrossRef]
- Fernandes, Matheus Vanzin; et al. Endoscopic Ultrasound-Guided Gastroenterostomy vs Enteral Stenting for Malignant Gastric Outlet Obstruction: A Systematic Review and Meta-analysis. Techniques and Innovations in Gastrointestinal Endoscopy 2025, Volume 27(Issue 3). [Google Scholar] [CrossRef]
- van de Pavert, YL; et al. Endoscopic versus surgical gastroenterostomy for palliation of malignant gastric outlet obstruction (ENDURO). The Lancet Gastroenterology & Hepatology Volume 10(Issue 12), 1065–1074. [CrossRef]
- Zhao, R.; Gu, L.; Ke, X.; et al. Risk prediction of cholangitis after stent implantation based on machine learning. Sci Rep 2024, 14, 13715. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Qi, J.; Zhang, X.; et al. Development and application of an early warning model for predicting early mortality. Oncology letters 2025, 29(5), 237. [Google Scholar]
- Jin, H.; Sun, X.; Fu, C.; et al. Machine learning-based prediction model for post-ERCP cholangitis. Surg Endosc 2025, 39, 5107–5126. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Comparison of Stent Types for Malignant Distal Biliary Obstruction.
| Stent Type | Advantages | Disadvantages | Clinical Recommendations |
|---|---|---|---|
| Plastic Stents |
|
|
Limited role; consider for temporary drainage or very short life expectancy |
| Uncovered SEMS |
|
|
Suitable for unresectable DMBO; preferred for hilar obstruction |
| Covered SEMS (FC/PC) |
|
|
FC-SEMS preferred for resectable/borderline resectable disease; consider for unresectable DMBO |
Table 2.
Comparison of EUS-Guided Biliary Drainage Techniques.
| Technique | Primary Indication | Technical Success | Clinical Success | Major Complications |
|---|---|---|---|---|
| EUS-CDS | Failed ERCP in DMBO; preferred EUS-BD approach for distal obstruction | 93.5-96% | 88-96% |
|
| EUS-HGS | Failed ERCP in HMBO; gastric outlet obstruction; altered anatomy | Similar to EUS-CDS | Similar to EUS-CDS |
|
| EUS-RV | Failed ERCP (second attempt); benign biliary disease with normal anatomy | 72-96% (expert hands) | 84-86% |
|
| EUS-AG | Failed ERCP with preservation of normal anatomy | 92% | Not reported |
|
| EUS-GBD | Failed ERCP in DMBO; alternative to EUS-CDS with potentially lower late morbidity | 99.2-100% | 85-89% |
|
Abbreviations: EUS-CDS, endoscopic ultrasound-guided choledochoduodenostomy; EUS-HGS, endoscopic ultrasound-guided hepaticogastrostomy; EUS-RV, endoscopic ultrasound-guided rendezvous; EUS-AG, endoscopic ultrasound-guided antegrade; EUS-GBD, endoscopic ultrasound-guided gallbladder drainage; DMBO, distal malignant biliary obstruction; HMBO, hilar malignant biliary obstruction; ERCP, endoscopic retrograde cholangiopancreatography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



