
Submitted:
08 January 2026
Posted:
23 January 2026
You are already at the latest version
Abstract
Older patients with unresectable locally advanced non-small cell lung cancer (NSCLC) frequently receive concurrent chemoradiotherapy (CCRT) with daily low-dose carboplatin; however, real-world data on its efficacy, safety, and prognostic factors remain limited. We aimed to retrospectively evaluate the clinical outcomes of this regimen and examined whether systemic inflammation-based indices predict prognosis in this setting. We reviewed 52 consecutive patients with locally advanced NSCLC treated with first-line CCRT using daily low-dose carboplatin at three Japanese institutions between April 2007 and December 2019. The median progression-free survival (PFS) and overall survival (OS) were 11.5 and 40.1 months, respectively. Twenty patients received durvalumab as maintenance therapy. In the overall cohort, multivariate analysis identified the Glasgow Prognostic Score (GPS) as an independent predictor of PFS. A GPS of 0–1 was also associated with a significantly longer OS in univariate analysis. CCRT with daily low-dose carboplatin provided durable disease control with acceptable toxicity in older patients with unresectable stage II/III NSCLC. The GPS appears to be a simple marker for PFS in this population and may aid in pretreatment risk stratification alongside histology and consolidation strategies.
Keywords:
chemoradiotherapy
; efficacy
; Glasgow Prognostic Score
; low-dose carboplatin
; non-small cell lung cancer
1. Introduction
Lung cancer is the leading cause of cancer-related mortality worldwide [1]. Among these, unresectable, locally advanced non-small cell lung cancer (NSCLC) represents approximately 30–35% of the overall NSCLC cases [2]. The disease predominantly affects older adults; the median age at diagnosis is 71 years, and nearly 70% of patients are aged >65 years at presentation [3,4]. Platinum-based concurrent chemoradiotherapy (CCRT) is the standard of care for individuals with unresectable locally advanced NSCLC. Nevertheless, its therapeutic impact is modest, with a reported median overall survival (OS) of only 22–25 months and a 5-year OS rate of approximately 20% [5].
The randomized phase 3 Japan Clinical Oncology Group (JCOG) 0301 trial, conducted by the JCOG, demonstrated that CCRT consisting of 60 Gy thoracic irradiation with daily low-dose carboplatin (30 mg/m², 5 days per week for 4 weeks) provided superior survival and acceptable toxicity compared with radiotherapy alone in patients aged >70 years with unresectable stage IIIA–IIIB NSCLC and performance status (PS) 0–2 [6]. Based on these findings, the current Japanese guidelines recommend daily low-dose carboplatin–based CCRT for older patients with unresectable stage II/III NSCLC. In addition, the pivotal phase 3 PACIFIC trial established that consolidation therapy with durvalumab following definitive chemoradiotherapy significantly improved both progression-free survival (PFS) and OS compared with placebo [7,8]. Consequently, the National Comprehensive Cancer Network guidelines recommend durvalumab consolidation for patients with unresectable stage II/III NSCLC who maintain an Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0–1 and exhibit no disease progression after CCRT.
A substantial proportion of patients with lung cancer develop a systemic inflammatory response (SIR) and cancer-associated weight loss, both of which are central components of cancer cachexia [9,10]. Therefore, numerous SIR-based indices—including the Glasgow Prognostic Score (GPS), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and Advanced Lung Cancer Inflammation Index (ALI)—have been evaluated as prognostic biomarkers. The GPS incorporates serum C-reactive protein (CRP) and albumin levels [9], and multiple studies have demonstrated its independent prognostic significance in advanced NSCLC [11,12,13,14,15,16]. However, the association between the GPS and treatment response to daily low-dose carboplatin–based CCRT in older patients with unresectable stage II/III NSCLC remains unclear. Similarly, although NLR has shown prognostic utility across various malignancies [17] and several studies have confirmed its prognostic relevance in NSCLC [18,19], its association with outcomes following CCRT in this specific population remains unclear. Systematic reviews have indicated that NLR predicts therapeutic efficacy and survival in NSCLC [20]. An elevated PLR, another marker of systemic inflammation, is associated with poor OS in lung cancer, particularly in NSCLC [21,22]. ALI, which reflects inflammatory and nutritional status, is also correlated with unfavorable OS in multiple cancer types [23], and baseline ALI is an independent predictor of poor prognosis in advanced NSCLC [24]. Moreover, prior work on body composition suggests that body mass index (BMI) influences survival outcomes in NSCLC [25,26]. Nevertheless, the potential prognostic associations between BMI, GPS, NLR, PLR, and ALI and therapeutic efficacy in older patients receiving daily low-dose carboplatin–based CCRT for unresectable stage II/III NSCLC have not yet been evaluated.
Therefore, this study aimed to investigate whether BMI, GPS, NLR, PLR, and ALI can serve as predictive markers for treatment effectiveness in patients receiving this regimen. Although daily low-dose carboplatin is widely used in Japan in older patients with unresectable stage II/III NSCLC, studies focusing on its real-world performance are scarce. Furthermore, the clinical effectiveness and toxicity profiles of this CCRT regimen in older patients have not been thoroughly characterized in real-world practice. Therefore, this retrospective analysis aimed to assess both the safety and therapeutic efficacy of daily low-dose carboplatin–based CCRT in routine clinical care for older patients with unresectable stage II/III NSCLC and to help refine the treatment strategies for this population.
2. Materials and Methods
2.1. Participants
This retrospective study involved a comprehensive review of electronic medical records. We identified consecutive patients with locally advanced NSCLC who received CCRT with low-dose carboplatin between April 2007 and December 2019 at three Japanese institutions: Saitama Medical University International Medical Center, Gunma Prefectural Cancer Center, and National Hospital Organization Asahikawa Medical Center. Patients were required to have a minimum follow-up period of 60 months, with data censored on December 31, 2024. The Institutional Ethics Committee of Saitama Medical University International Medical Center approved the study protocol (approval number 2024-048) and waived the need for written informed consent owing to the retrospective nature of this study. All the procedures conformed to the principles of the Declaration of Helsinki.
Eligible patients met the following criteria: (i) cytological or histological confirmation of NSCLC, (ii) unilateral hemithoracic disease with regional nodal involvement suitable for treatment within a single radiation field, and (iii) receipt of first-line CRT. Histological subtyping followed the 2015 World Health Organization classification, and clinical staging was based on the Eighth Edition of the Union for International Cancer Control tumor-node-metastasis (TNM) system [2]. Adverse event severity was graded using the Common Terminology Criteria for Adverse Events version 5.0. Institutional standards for CRT eligibility typically included neutrophil count ≥1.5×10³/mm³, platelet count ≥1.0×10⁵/mm³, serum creatinine ≤1.5 mg/dL, total bilirubin ≤2.0 mg/dL, and transaminases ≤100 U/L.
Pretreatment evaluation for TNM staging consisted of a physical examination, chest radiography, contrast-enhanced computed tomography (CT) of the chest and abdomen, CT or magnetic resonance imaging of the brain, and bone scintigraphy or 18F-fluorodeoxyglucose positron emission tomography.
2.2. Treatment
2.2.1. Chemotherapy
Chemotherapy selection, in accordance with approved product labeling, was determined by the treating physicians. The patients received daily intravenous low-dose carboplatin (30 mg/m² infused over 30 min) administered 1 h before radiotherapy for the initial 20 fractions. Treatment was discontinued in cases of disease progression, unacceptable toxicity, or withdrawal of consent. After the regulatory approval of durvalumab, eligible patients received consolidation therapy 1–42 days after completion of CRT. Durvalumab was intravenously administered at a dose of 10 mg/kg every 2 weeks for up to 12 months.
2.2.2. Radiotherapy
Radiotherapy was administered according to the JCOG0301 protocol [6]. Briefly, radiotherapy was administered to the thoracic lesion once daily, 5 days per week, over 6–9 weeks. The total dose to the planning target volume was 60 Gy delivered in 30 fractions. Both three-dimensional conformal radiotherapy and intensity-modulated radiotherapy were accepted to use with the institutional practice. Respiratory motion management strategies were implemented as necessary. Appropriate image guidance using on-board images, portal vision, and/or cone-beam CT was performed during the treatment session.
Regarding the dose constraints of the normal organs, the lung V20 (percentage of lung volume receiving ≥20 Gy) should be <30%, the heart V40 should be <20%, and the maximum dose to the spinal cord should be <45 Gy.
2.3. Assessment of Metabolic and Inflammatory Indices
The baseline BMI was calculated as body weight (kg) divided by height squared (m²). Following established Japanese population data, a BMI cutoff of 22.0 kg/m² was applied (high BMI ≥22.0, low BMI <22.0) [27]. Serum CRP and albumin levels measured on the day before or on the day of CRT initiation were used to compute the GPS, which was categorized as follows:
0: CRP <1.0 mg/dL and albumin ≥3.5 mg/dL
1: CRP elevation or hypoalbuminemia
The NLR was defined as the absolute neutrophil count divided by the absolute lymphocyte count, with a cutoff of 5.0 to differentiate low-risk (<5.0) and high-risk (≥5.0) groups [28,29]. The PLR was calculated similarly, with a cutoff of 185 used to classify patients into low-risk (<185) and high-risk (≥185) categories [21]. The ALI was defined as (BMI×albumin)/NLR, with a cutoff of 24 distinguishing low (<24) from high (≥24) ALI groups [23].
2.4. Evaluation of the Treatment Response
Tumor response was assessed based on the best overall response and maximum tumor shrinkage. Responses were classified according to the Response Evaluation Criteria in Solid Tumors, version 1.1 [30], as complete response, partial response, stable disease, progressive disease, or not evaluable. In case of treatment failure, subsequent therapy was selected at the discretion of the treating physician.
2.5. Statistical Analyses
Categorical variables were analyzed using Fisher’s exact test, and continuous variables were analyzed using Welch’s t-test. PFS was defined as the interval from treatment initiation to disease progression or death from any cause, whereas OS was defined as the interval from treatment initiation to death or last follow-up. Survival curves were estimated using the Kaplan–Meier method and compared using the log-rank test. Statistical significance was set at a two-sided p-value < 0.05. All analyses were performed using the JMP software, version 11.0 (SAS Institute, Cary, NC, USA).
3. Results
3.1. Patient Characteristics and Treatment Efficacy
Fifty-two patients were included in this study. The baseline characteristics are summarized in Table 1.
The cohort comprised 41 men (78.8%) and 11 women (21.2%), with a median age of 76 (range, 71–86) years. Most patients (51/52, 98.1%) had an ECOG PS of 0–1, whereas one (1.9%) patient had a PS of 2. Adenocarcinoma and squamous cell carcinoma were observed at equal frequencies (23 patients each, 44.2%). Seven (13.5%) patients harbored driver alterations (EGFR, ALK, or ROS1), whereas the remaining patients were either negative or untested, and no additional oncogenic alterations were identified. The median BMI was 22.2 (range, 16.1–27.6) kg/m². Two (3.8%) patients were unable to complete the radiotherapy, and the median delivered dose was 60 Gy (range, 45–66 Gy). Twelve (23.1%) patients discontinued carboplatin prematurely, and the median number of carboplatin administrations was 20 (range, 4–20). At the data cutoff, 16 (30.8%) patients were alive. Twenty (38.5%) patients received durvalumab maintenance therapy, and 32 (61.5%) did not. Among the 20 patients receiving durvalumab, 13 (65.0%) were unable to complete 1 year of treatment. Causes of discontinuation included disease progression (6/13, 46.2%) and treatment-related adverse events (7/13, 53.8%) (Table S1). Patterns of distant recurrence following CRT are listed in Table S2. Among the 40 patients who developed distant metastases, the bone (12 patients, 30.0%) and brain (6 patients, 15.0%) were the most frequent sites. Table S3 summarizes the systemic therapies administered after recurrence. Treatment response data are presented in Table 2.
The overall response rate (ORR) was 51.9% (95% confidence interval [CI], 38.6–64.8%). There were no statistically significant differences in either the ORR or disease control rate between patients who received durvalumab maintenance therapy and those who did not.
3.2. Survival Analysis
All the patients had a minimum follow-up period of 60 months. Over a median follow-up period of 29.8 (range, 3.4–91.3) months, the median PFS and OS periods were 11.5 months (95% CI, 8.1–24.5) and 40.1 months (95% CI, 16.6–50.6), respectively (Figure 1a and Figure 1b).
At the data cutoff (December 31, 2024), 36 patients died and 16 survived. Univariate and multivariate analyses of PFS and OS are summarized in Table 3.
In the univariate analysis, GPS was significantly associated with PFS. Multivariate analysis confirmed that GPS (0–1 vs. 2) was an independent factor for PFS (hazard ratio, 0.36; p=0.0294). Univariate analysis identified significant associations between histology and GPS; however, multivariate analysis did not identify any independent predictors of OS. The Kaplan–Meier survival curves are shown in Figure 2.
Patients with a GPS of 0–1 had significantly longer PFS and OS than those with a GPS of 2 (both p<0.05). The median PFS periods were 13.7 months for GPS 0–1 and 5.6 months for GPS 2 (log-rank p=0.0165, Figure 2a), and the median OS periods were 45.6 and 13.0 months, respectively (log-rank p=0.0094, Figure 2b).
3.3. Toxicity
Treatment-related adverse events are shown in Table 4.
All 52 patients were evaluable for safety. Myelosuppression was the most common toxicity, with grade 3–4 decreased white blood cell counts in 25.0% of the patients, grade 3–4 decreased neutrophil counts in 23.1%, and febrile neutropenia in one (1.9%). Grade 3–4 decreased platelet counts were observed in nine (17.3%) patients. Severe nonhematological toxicities were rare; grade 3–4 skin rashes occurred in 3.8% of the patients. Treatment discontinuation due to adverse events occurred in 12 of the 52 (23.1%) patients. No treatment-related deaths occurred. Among the 20 patients receiving durvalumab maintenance therapy, 7 discontinued treatment because of adverse events, including 6 cases of pneumonitis and 1 of myositis (Table S1).
3.4. Subsequent Treatment After Chemoradiotherapy
Post-CRT treatments are summarized in Table S3. Of the 40 patients who experienced recurrence, best supportive care was frequently selected; however, 26 (65.0%) received systemic therapy. Nivolumab monotherapy was the most common subsequent regimen, followed by platinum-based combination chemotherapy. Nine patients received up to third-line therapy, and four patients received more than four lines of treatment.
4. Discussion
This study assessed the real-world efficacy and safety of CCRT with daily low-dose carboplatin in older patients with unresectable stage II/III NSCLC and evaluated the prognostic utility of BMI, GPS, NLR, PLR, and ALI. Multivariate analysis identified the GPS as an independent predictor of PFS, highlighting its potential as a clinically meaningful biomarker. To the best of our knowledge, this is the first study to explore the prognostic relevance of these inflammation- and nutrition-based indices, specifically in patients receiving daily low-dose carboplatin CCRT for unresectable locally advanced NSCLC.
Findings from the JCOG0301 randomized phase 3 trial demonstrated that adding daily low-dose carboplatin to thoracic radiotherapy provided significant clinical benefits with acceptable toxicity in older patients with locally advanced NSCLC, yielding a median PFS period of 8.9 months and a median OS period of 22.4 months [6]. In our cohort, the median PFS and OS periods were 11.5 months and 40.1 months, respectively—outcomes that appear more favorable than those reported in JCOG0301. Several factors may explain this discrepancy. Our cohort included patients who received durvalumab maintenance therapy (n=20), individuals with stage II disease (n=4), patients experiencing postoperative recurrence (n=7), and those who subsequently received modern systemic therapies not available during the JCOG0301 trial period—including third-generation EGFR tyrosine kinase inhibitors (TKIs), second-generation ALK TKIs, and immune checkpoint inhibitor monotherapy. These agents have demonstrated substantial efficacy in advanced NSCLC [31,32,33,34,35,36] and likely contributed to the improved OS observed in this study. The effect of durvalumab maintenance may also have influenced PFS prolongation.
The PACIFIC trial showed that durvalumab maintenance following platinum-based CCRT significantly extended PFS and OS compared with placebo, with median PFS periods of 16.8 and 5.6 months and median OS periods of 47.5 and 29.1 months, respectively [7,8]. In our analysis, patients receiving durvalumab maintenance therapy exhibited a numerical, but not statistically significant, improvement in PFS and OS. There are several possible explanations for these results. First, our cohort was considerably older (median age, 76 years) than the PACIFIC population (median age, 64 years), consistent with the PACIFIC subgroup analysis in which age >65 years was correlated with a diminished OS benefit [37]. Another potential factor is the chemoradiation regimen. The PACIFIC trial did not administer a daily, low-dose carboplatin regimen. Although a retrospective study provided real-world data on durvalumab consolidation maintenance after chemoradiotherapy [38], including patients who received a daily low-dose carboplatin regimen, no focused analysis was performed on this population. Therefore, the clinical significance of durvalumab maintenance therapy following chemoradiotherapy with low-dose carboplatin remains unclear. However, a recent Japanese phase II study (NEJ039A) reported that durvalumab maintenance therapy after chemoradiotherapy with daily low-dose carboplatin was effective and well-tolerated in older patients with unresectable locally advanced NSCLC [39]. In this study, the median PFS and OS periods were 12.3 and 28.1 months, respectively. The average follow-up period from the first enrollment was 19.0 months in this study. Although the median observation periods differed and direct comparison with that study’s results was not possible, the PFS was similar to that in our cohort. Furthermore, a recent retrospective study comparing patients who received durvalumab maintenance therapy after CCRT with daily low-dose carboplatin versus those who did not suggested that durvalumab maintenance therapy after CCRT with daily low-dose carboplatin did not provide a significant clinical benefit in older patients with unresectable stage II/III NSCLC [40]. This was a small, retrospective study that compared 16 patients who received durvalumab maintenance therapy with 20 patients who did not. Owing to the small sample size in this retrospective study, it is possible that no statistically significant difference was observed. Our current analysis, which compared 20 patients who received durvalumab maintenance therapy with 32 who did not, was also a small-sample retrospective study and may have yielded similar results.
The GPS has emerged as a significant predictor of PFS. Studies have demonstrated the prognostic significance of the GPS in NSCLC, irrespective of the disease stage, and it is commonly used as a prognostic marker in clinical research [10,11,12,13,14,15,16]. The GPS is associated with altered drug metabolism, adipokine levels, elevated cytokine levels, weight loss, muscle wasting, and compromised PS [10,41,42,43,44,45,46]. Previous studies have evaluated the GPS in the context of first-line cytotoxic drug treatment for NSCLC, whereas no study has evaluated the GPS with respect to CCRT with daily low-dose carboplatin. In the present study, the GPS 2 group (n=9) was smaller than the GPS 0–1 group (n=43). This may be because locally advanced NSCLC, unlike metastatic NSCLC with distant metastases, is characterized by lesions confined to the unilateral thoracic region.
The GPS is an indicator calculated from serum CRP and albumin levels, both of which can be routinely and easily measured in daily clinical practice in most medical institutions. Multivariate analysis demonstrated that the GPS was independently associated with PFS (Table 3). Although PS has long been considered a primary prognostic factor in both clinical trials and real-world practice, its assessment is inherently subjective and dependent on the physician’s judgment. In the population analyzed here, only one of the 52 patients had a PS of 2, precluding the evaluation of patients with poor PS. In contrast to the PS, the GPS is an objective and highly reproducible index that stratifies patients using a simple three-point scoring system. This objectivity may allow for a more accurate and standardized pretreatment risk assessment than conventional prognostication based on PS alone [47]. Notably, a GPS of 2, defined by elevated CRP levels and hypoalbuminemia at treatment initiation, was associated with inferior treatment efficacy, suggesting that systemic inflammation and nutritional status substantially influence the outcomes. These findings support the clinical integration of the GPS into treatment decision-making for patients with locally advanced NSCLC receiving CCRT with daily low-dose carboplatin.
In contrast, other inflammation- and nutrition-related indices, including NLR, PLR, ALI, and BMI, were not independently associated with survival in the multivariate analyses. Although prior studies on advanced NSCLC have suggested the prognostic relevance of these markers, the results have been inconsistent, likely reflecting heterogeneous patient populations, variable treatment settings, and differing cutoff values [18,19,21,22,24,25,26]. The relatively small sample size of the present cohort may have limited the statistical power. Future investigations in larger, well-defined cohorts treated with uniform CCRT regimens are required to establish optimal cutoff values and account for ethnic differences, particularly with respect to BMI, when extrapolating these indices beyond Japanese populations.
Daily low-dose carboplatin treatment was well-tolerated. No grade ≥3 pneumonitis was observed, in contrast with the 1% incidence reported in JCOG0301. Rates of grade ≥3 hematological toxicities and febrile neutropenia were also lower than those observed in JCOG0301. No treatment-related death occurred during the study period. These findings suggest that daily low-dose carboplatin combined with thoracic radiotherapy is a safe and feasible treatment regimen for older patients. Among patients receiving durvalumab maintenance therapy, seven of 20 discontinued treatment due to adverse events, predominantly pneumonitis (n=6). Although no grade 4–5 events were observed, the high rate of pneumonitis-related discontinuation warrants caution when administering durvalumab maintenance therapy to older patients after low-dose carboplatin CCRT.
This study has some limitations. This retrospective design introduced potential variability in clinical assessments and outcome documentation. The small sample size limits the statistical power and may obscure differences between clinical subgroups. Finally, the introduction of modern systemic therapies, including durvalumab consolidation, during the study period may have influenced the long-term outcomes in ways that cannot be fully disentangled.
5. Conclusions
CCRT with low-dose carboplatin is an effective and well-tolerated treatment option for older patients with unresectable stage II/III NSCLC. The GPS is a simple, objective, and clinically valuable predictor of PFS, outperforming other inflammation-based indices and offering a practical tool for pretreatment risk stratification. Although durvalumab maintenance therapy is feasible, a survival benefit is not clearly observed in this older population. Collectively, these findings support the continued use of daily low-dose carboplatin CCRT in routine practice and highlight the importance of incorporating the GPS into individualized treatment planning for older patients with locally advanced NSCLC.
Supplementary Materials
The following supporting information can be downloaded at Preprints.org: Table S1. Durvalumab maintenance therapy; Table S2. Sites of metastases at recurrence; Table S3. Subsequent treatment of 40 patients with recurrence after chemoradiotherapy.
Author Contributions
All the authors have read and approved the final version of the manuscript. Conceptualization and methodology, Y.M. and H. I.; formal analysis and data curation, H. I. and K. K.; project administration, visualization, and writing—original draft preparation, Y.M. and H. I.; supervision, S.K. and H.K.; investigation and resources, S.E., K.H., O.Y., A.M., K.M., T.M., Y.F., and S.K.; and writing, review, and editing, all authors.
Funding
This research received no external funding.
Institutional Review Board Statement
The study protocol was approved by the Institutional Ethics Committee of the International Medical Center of Saitama Medical University (approval number 2024-048).
Informed Consent Statement
The need for written informed consent was waived by the Ethics Committee of Saitama Medical University owing to the retrospective nature of the study.
Data Availability Statement
The data generated in this study are available upon request from the corresponding author. The data are not publicly available due to ethical restrictions.
Acknowledgments
The authors wish to thank Ms. Kyoko Nakagawa and Ms. Miho Ishida for their assistance with manuscript preparation and Editage (www.editage.jp) for the English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ALI | Advanced Lung Cancer Inflammation Index |
| BMI | body mass index |
| CCRT | concurrent chemoradiotherapy |
| CI | confidence interval |
| CRP | C-reactive protein |
| CT | computed tomography |
| GPS | Glasgow Prognostic Score |
| JCOG | Japan Clinical Oncology Group |
| NLR | neutrophil-to-lymphocyte ratio |
| NSCLC | non-small cell lung cancer |
| ORR | overall response rate |
| OS | overall survival |
| PLR | platelet-to-lymphocyte ratio |
| PS | performance status |
| SIR | systemic inflammatory response |
| TKIs | tyrosine kinase inhibitors |
| TNM | tumor-node-metastasis |
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74(3), 229–263. [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee, Advisory Boards, and Participating Institutions; International Association for the Study of Lung Cancer Staging and Prognostic Factors Committee Advisory Boards and Participating Institutions. The IASLC lung cancer staging project: proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM classification for lung cancer. J. Thorac. Oncol. 2016, 11(1), 39–51. [CrossRef]
- Venuta, F.; Diso, D.; Onorati, I.; Anile, M.; Mantovani, S.; Rendina, E.A. Lung cancer in elderly patients. J. Thorac. Dis. 2016, 8 (Suppl. 11), S908–S914. [CrossRef]
- Presley, C.J.; Reynolds, C.H.; Langer, C.J. Caring for the older population with advanced lung cancer. Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 587–596. [CrossRef]
- Hanna, N.; Neubauer, M.; Yiannoutsos, C.; McGarry, R.; Arseneau, J.; Ansari, R.; Reynolds, C.; Govindan, R.; Melnyk, A.; Fisher, W.; Richards, D.; Bruetman, D.; Anderson, T.; Chowhan, N.; Nattam, S.; Mantravadi, P.; Johnson, C.; Breen, T.; White, A.; Einhorn, L.; Hoosier Oncology Group; US Oncology. Phase III study of cisplatin, etoposide, and concurrent chest radiation with or without consolidation docetaxel in patients with inoperable stage III non-small-cell lung cancer: the Hoosier Oncology Group and U.S. Oncology. J. Clin. Oncol. 2008, 26(35), 5755–5760. [CrossRef]
- Atagi, S.; Kawahara, M.; Yokoyama, A.; Okamoto, H.; Yamamoto, N.; Ohe, Y.; Sawa, T.; Ishikura, S.; Shibata, T.; Fukuda, H.; Saijo, N.; Tamura, T.; Japan Clinical Oncology Group Lung Cancer Study Group. Thoracic radiotherapy with or without daily low-dose carboplatin in elderly patients with non-small-cell lung cancer: a randomised, controlled, phase 3 trial by the Japan Clinical Oncology Group (JCOG0301). Lancet Oncol. 2012, 13(7), 671–678. [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; Cho, B.C.; Bourhaba, M.; Quantin, X.; Tokito, T.; Mekhail, T.; Planchard, D.; Kim, Y.C.; Karapetis, C.S.; Hiret, S.; Ostoros, G.; Kubota, K.; Gray, J.E.; Paz-Ares, L.; de Castro Carpeño, J.; Wadsworth, C.; Melillo, G.; Jiang, H.; Huang, Y.; Dennis, P.A.; Özgüroğlu, M.; PACIFIC Investigators. Durvalumab after chemoradiotherapy in Stage III non-small-cell lung cancer. N. Engl. J. Med. 2017, 377(20), 1919–1929. [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; Cho, B.C.; Bourhaba, M.; Quantin, X.; Tokito, T.; Mekhail, T.; Planchard, D.; Kim, Y.C.; Karapetis, C.S.; Hiret, S.; Ostoros, G.; Kubota, K.; Gray, J.E.; Paz-Ares, L.; de Castro Carpeño, J.; Faivre-Finn, C.; Reck, M.; Vansteenkiste, J.; Spigel, D.R.; Wadsworth, C.; Melillo, G.; Taboada, M.; Dennis, P.A.; Özgüroğlu, M.; PACIFIC Investigators. Overall survival with durvalumab after chemoradiotherapy in Stage III NSCLC. N. Engl. J. Med. 2018, 379(24), 2342–2350. [CrossRef]
- McMillan, D.C. An inflammation-based prognostic score and its role in the nutrition-based management of patients with cancer. Proc. Nutr. Soc. 2008, 67(3), 257–262. [CrossRef]
- Proctor, M.J.; Talwar, D.; Balmar, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; Morrison, D.S.; McMillan, D.C. The relationship between the presence and site of cancer, an inflammation-based prognostic score and biochemical parameters. Initial results of the Glasgow Inflammation Outcome Study. Br. J. Cancer 2010, 103(6), 870–876. [CrossRef]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Comparison of an inflammation-based prognostic score (GPS) with performance status (ECOG) in patients receiving platinum-based chemotherapy for inoperable non-small-cell lung cancer. Br. J. Cancer 2004, 90(9), 1704–1706. [CrossRef]
- Gioulbasanis, I.; Pallis, A.; Vlachostergios, P.J.; Xyrafas, A.; Giannousi, Z.; Perdikouri, I.E.; Makridou, M.; Kakalou, D.; Georgoulias, V. The Glasgow Prognostic Score (GPS) predicts toxicity and efficacy in platinum-based treated patients with metastatic lung cancer. Lung Cancer 2012, 77(2), 383–388. [CrossRef]
- Leung, E.Y.; Scott, H.R.; McMillan, D.C. Clinical utility of the pretreatment Glasgow prognostic score in patients with advanced inoperable non-small cell lung cancer. J. Thorac. Oncol. 2012, 7(4), 655–662. [CrossRef]
- Jiang, A.G.; Chen, H.L.; Lu, H.Y. Comparison of Glasgow prognostic score and prognostic index in patients with advanced non-small cell lung cancer. J. Cancer Res. Clin. Oncol. 2015, 141(3), 563–568. [CrossRef]
- Takamori, S.; Takada, K.; Shimokawa, M.; Matsubara, T.; Fujishita, T.; Ito, K.; Toyozawa, R.; Yamaguchi, M.; Okamoto, T.; Yoneshima, Y.; Tanaka, K.; Okamoto, I.; Tagawa, T.; Mori, M. Clinical utility of pretreatment Glasgow prognostic score in non-small-cell lung cancer patients treated with immune checkpoint inhibitors. Lung Cancer 2021, 152, 27–33. [CrossRef]
- Imai, H.; Kishikawa, T.; Minemura, H.; Yamada, Y.; Ibe, T.; Yamaguchi, O.; Mouri, A.; Hamamoto, Y.; Kanazawa, K.; Kasai, T.; Kaira, K.; Kaburagi, T.; Minato, K.; Kobayashi, K.; Kagamu, H. Pretreatment Glasgow prognostic score predicts survival among patients with high PD-L1 expression administered first-line pembrolizumab monotherapy for non-small cell lung cancer. Cancer Med. 2021, 10(20), 6971–6984. [CrossRef]
- Templeton, A.J.; McNamara, M.G.; Šeruga, B.; Vera-Badillo, F.E.; Aneja, P.; Ocaña, A.; Leibowitz-Amit, R.; Sonpavde, G.; Knox, J.J.; Tran, B.; Tannock, I.F.; Amir, E. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J. Natl. Cancer Inst. 2014, 106(6), dju124. [CrossRef]
- Liu, Z.L.; Zeng, T.T.; Zhou, X.J.; Ren, Y.N.; Zhang, L.; Zhang, X.X.; Ding, Z.Y. Neutrophil–lymphocyte ratio as a prognostic marker for chemotherapy in advanced lung cancer. Int. J. Biol. Markers 2016, 31(4), e395–e401. [CrossRef]
- Liu, D.; Jin, J.; Zhang, L.; Li, L.; Song, J.; Li, W. The neutrophil to lymphocyte ratio may predict benefit from chemotherapy in lung cancer. Cell. Physiol. Biochem. 2018, 46(4), 1595–1605. [CrossRef]
- Platini, H.; Ferdinand, E.; Kohar, K.; Prayogo, S.A.; Amirah, S.; Komariah, M.; Maulana, S. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as prognostic markers for advanced non-small-cell lung cancer treated with immunotherapy: A systematic review and meta-analysis. Medicina (Kaunas) 2022, 58(8), 1069. [CrossRef]
- Ding, N.; Pang, Z.; Shen, H.; Ni, Y.; Du, J.; Liu, Q. The prognostic value of PLR in lung cancer, a meta-analysis based on results from a large consecutive cohort. Sci. Rep. 2016, 6, 34823. [CrossRef]
- Kinoshita, A.; Onoda, H.; Imai, N.; Iwaku, A.; Oishi, M.; Fushiya, N.; Koike, K.; Nishino, H.; Tajiri, H. Comparison of the prognostic value of inflammation-based prognostic scores in patients with hepatocellular carcinoma. Br. J. Cancer 2012, 107(6), 988–993. [CrossRef]
- Hua, X.; Chen, J.; Wu, Y.; Sha, J.; Han, S.; Zhu, X. Prognostic role of the advanced lung cancer inflammation index in cancer patients: a meta-analysis. World J. Surg. Oncol. 2019, 17(1), 177. [CrossRef]
- Jafri, S.H.; Shi, R.; Mills, G. Advance lung cancer inflammation index (ALI) at diagnosis is a prognostic marker in patients with metastatic non-small cell lung cancer (NSCLC): a retrospective review. B.M.C. Cancer 2013, 13, 158. [CrossRef]
- Ichihara, E.; Harada, D.; Inoue, K.; Sato, K.; Hosokawa, S.; Kishino, D.; Watanabe, K.; Ochi, N.; Oda, N.; Hara, N.; Hotta, K.; Maeda, Y.; Kiura, K. The impact of body mass index on the efficacy of anti-PD-1/PD-L1 antibodies in patients with non-small cell lung cancer. Lung Cancer 2020, 139, 140–145. [CrossRef]
- Imai, H.; Naito, E.; Yamaguchi, O.; Hashimoto, K.; Iemura, H.; Miura, Y.; Shiono, A.; Mouri, A.; Kaira, K.; Kobayashi, K.; Kagamu, H. Pretreatment body mass index predicts survival among patients administered nivolumab monotherapy for pretreated non-small cell lung cancer. Thorac. Cancer 2022, 13(10), 1479–1489. [CrossRef]
- Tokunaga, K.; Matsuzawa, Y.; Kotani, K.; Keno, Y.; Kobatake, T.; Fujioka, S.; Tarui, S. Ideal body weight estimated from the body mass index with the lowest morbidity. Int. J. Obes. 1991, 15(1), 1–5.
- Bagley, S.J.; Kothari, S.; Aggarwal, C.; Bauml, J.M.; Alley, E.W.; Evans, T.L.; Kosteva, J.A.; Ciunci, C.A.; Gabriel, P.E.; Thompson, J.C.; Stonehouse-Lee, S.; Sherry, V.E.; Gilbert, E.; Eaby-Sandy, B.; Mutale, F.; DiLullo, G.; Cohen, R.B.; Vachani, A.; Langer, C.J. Pretreatment neutrophil-to-lymphocyte ratio as a marker of outcomes in nivolumab-treated patients with advanced non-small-cell lung cancer. Lung Cancer 2017, 106, 1–7. [CrossRef]
- Suh, K.J.; Kim, S.H.; Kim, Y.J.; Kim, M.; Keam, B.; Kim, T.M.; Kim, D.W.; Heo, D.S.; Lee, J.S. Post-treatment neutrophil-to-lymphocyte ratio at week 6 is prognostic in patients with advanced non-small cell lung cancers treated with anti-PD-1 antibody. Cancer Immunol. Immunother. 2018, 67(3), 459–470. [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; Rubinstein, L.; Shankar, L.; Dodd, L.; Kaplan, R.; Lacombe, D.; Verweij, J. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45(2), 228–247. [CrossRef]
- Ramalingam, S.S.; Vansteenkiste, J.; Planchard, D.; Cho, B.C.; Gray, J.E.; Ohe, Y.; Zhou, C.; Reungwetwattana, T.; Cheng, Y.; Chewaskulyong, B.; Shah, R.; Cobo, M.; Lee, K.H.; Cheema, P.; Tiseo, M.; John, T.; Lin, M.C.; Imamura, F.; Kurata, T.; Todd, A.; Hodge, R.; Saggese, M.; Rukazenkov, Y.; Soria, J.C.; FLAURA Investigators. Overall survival with osimertinib in untreated, EGFR-mutated advanced NSCLC. N. Engl. J. Med. 2020, 382(1), 41–50. [CrossRef]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.W.; Ou, S.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; Zeaiter, A.; Mitry, E.; Golding, S.; Balas, B.; Noe, J.; Morcos, P.N.; Mok, T.; ALEX Trial Investigators. Alectinib versus crizotinib in Untreated ALK-Positive non-small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377(9), 829–838. [CrossRef]
- Shaw, A.T.; Bauer, T.M.; de Marinis, F.; Felip, E.; Goto, Y.; Liu, G.; Mazieres, J.; Kim, D.W.; Mok, T.; Polli, A.; Thurm, H.; Calella, A.M.; Peltz, G.; Solomon, B.J.; CROWN Trial Investigators. First-line lorlatinib or crizotinib in advanced ALK-positive lung cancer. N. Engl. J. Med. 2020, 383(21), 2018–2029. [CrossRef]
- Camidge, D.R.; Kim, H.R.; Ahn, M.J.; Yang, J.C.H.; Han, J.Y.; Lee, J.S.; Hochmair, M.J.; Li, J.Y.C.; Chang, G.C.; Lee, K.H.; Gridelli, C.; Delmonte, A.; Garcia Campelo, R.; Kim, D.W.; Bearz, A.; Griesinger, F.; Morabito, A.; Felip, E.; Califano, R.; Ghosh, S.; Spira, A.; Gettinger, S.N.; Tiseo, M.; Gupta, N.; Haney, J.; Kerstein, D.; Popat, S. Brigatinib versus crizotinib in ALK-Positive non-small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379(21), 2027–2039. [CrossRef]
- Borghaei, H.; Gettinger, S.; Vokes, E.E.; Chow, L.Q.M.; Burgio, M.A.; de Castro Carpeno, J.; Pluzanski, A.; Arrieta, O.; Frontera, O.A.; Chiari, R.; Butts, C.; Wójcik-Tomaszewska, J.; Coudert, B.; Garassino, M.C.; Ready, N.; Felip, E.; García, M.A.; Waterhouse, D.; Domine, M.; Barlesi, F.; Antonia, S.; Wohlleber, M.; Gerber, D.E.; Czyzewicz, G.; Spigel, D.R.; Crino, L.; Eberhardt, W.E.E.; Li, A.; Marimuthu, S.; Brahmer, J. Five-year outcomes from the randomized, Phase III trials CheckMate 017 and 057: nivolumab versus docetaxel in previously treated non-small-cell lung cancer. J. Clin. Oncol. 2021, 39(7), 723–733. [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; Majem, M.; Fidler, M.J.; de Castro, G.; Garrido, M.; Lubiniecki, G.M.; Shentu, Y.; Im, E.; Dolled-Filhart, M.; Garon, E.B. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): a randomised controlled trial. Lancet 2016, 387(10027), 1540–1550. [CrossRef]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; Rimner, A.; Wu, Y.L.; Özgüroğlu, M.; Lee, K.H.; Kato, T.; de Wit, M.; Kurata, T.; Reck, M.; Cho, B.C.; Senan, S.; Naidoo, J.; Mann, H.; Newton, M.; Thiyagarajah, P.; Antonia, S.J. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in Stage III non-small-cell lung cancer. J. Clin. Oncol. 2022, 40(12), 1301–1311. [CrossRef]
- Girard, N.; Bar, J.; Garrido, P.; Garassino, M.C.; McDonald, F.; Mornex, F.; Filippi, A.R.; Smit, H.J.M.; Peters, S.; Field, J.K.; Christoph, D.C.; Sibille, A.; Fietkau, R.; Haakensen, V.D.; Chouaid, C.; Markman, B.; Hiltermann, T.J.N.; Taus, A.; Sawyer, W.; Allen, A.; Chander, P.; Licour, M.; Solomon, B. Treatment characteristics and real-world progression-free survival in patients with unresectable Stage III NSCLC who received durvalumab after chemoradiotherapy: findings from the PACIFIC-R study. J. Thorac. Oncol. 2023, 18(2), 181–193. [CrossRef]
- Mouri, A.; Kisohara, A.; Morita, R.; Ko, R.; Nakagawa, T.; Makiguchi, T.; Isobe, K.; Ishikawa, N.; Kondo, T.; Akiyama, M.; Bessho, A.; Honda, R.; Yoshimura, K.; Kagamu, H.; Kato, S.; Kobayashi, K.; Kaira, K.; Maemondo, M. A phase II study of daily carboplatin plus irradiation followed by durvalumab therapy for older adults (≥75 years) with unresectable III non-small-cell lung cancer and performance status of 2: NEJ039A. E.S.M.O. Open 2024, 9(10), 103939. [CrossRef]
- Yamauchi, K.; Komuta, R.; Tanabe, H.; Yokoyama, M.; Takata, S.O.; Yanase, T.; Hosono, Y.; Satoh, S.; Morishita, N.; Suzuki, H. Real-world outcomes of durvalumab consolidation in elderly patients with unresectable NSCLC following CCRT with daily low-dose carboplatin. Anticancer Res. 2025, 45(1), 369–378. [CrossRef]
- Brown, D.J.; Milroy, R.; Preston, T.; McMillan, D.C. The relationship between an inflammation-based prognostic score (Glasgow Prognostic Score) and changes in serum biochemical variables in patients with advanced lung and gastrointestinal cancer. J. Clin. Pathol. 2007, 60(6), 705–708. [CrossRef]
- Kerem, M.; Ferahkose, Z.; Yilmaz, U.T.; Pasaoglu, H.; Ofluoglu, E.; Bedirli, A.; Salman, B.; Sahin, T.T.; Akin, M. Adipokines and ghrelin in gastric cancer cachexia. World J. Gastroenterol. 2008, 14(23), 3633–3641. [CrossRef]
- Giannousi, Z.; Gioulbasanis, I.; Pallis, A.G.; Xyrafas, A.; Dalliani, D.; Kalbakis, K.; Papadopoulos, V.; Mavroudis, D.; Georgoulias, V.; Papandreou, C.N. Nutritional status, acute phase response and depression in metastatic lung cancer patients: correlations and association prognosis. Support. Care Cancer 2012, 20(8), 1823–1829. [CrossRef]
- Naito, T.; Tashiro, M.; Yamamoto, K.; Ohnishi, K.; Kagawa, Y.; Kawakami, J. Impact of cachexia on pharmacokinetic disposition of and clinical responses to oxycodone in cancer patients. Eur. J. Clin. Pharmacol. 2012, 68(10), 1411–1418. [CrossRef]
- McMillan, D.C. The systemic inflammation-based Glasgow Prognostic Score: a decade of experience in patients with cancer. Cancer Treat. Rev. 2013, 39(5), 534–540. [CrossRef]
- Kim, S.J.; Ryu, K.J.; Hong, M.; Ko, Y.H.; Kim, W.S. The serum CXCL13 level is associated with the Glasgow Prognostic Score in extranodal NK/T-cell lymphoma patients. J. Hematol. Oncol. 2015, 8, 49. [CrossRef]
- Dajczman, E.; Kasymjanova, G.; Kreisman, H.; Swinton, N.; Pepe, C.; Small, D. Should patient-rated performance status affect treatment decisions in advanced lung cancer? J. Thorac. Oncol. 2008, 3(10), 1133–1136. [CrossRef]
Figure 1.
(a) Kaplan–Meier curves for progression-free survival (PFS) among 52 patients who received chemoradiotherapy. The median PFS period was 11.5 months (95% confidence interval [CI], 8.1–24.5). (b) Kaplan–Meier curves for overall survival (OS) among 52 patients who received chemoradiotherapy. The median OS period was 40.1 months (95% CI, 16.6–50.6).
Figure 1.
(a) Kaplan–Meier curves for progression-free survival (PFS) among 52 patients who received chemoradiotherapy. The median PFS period was 11.5 months (95% confidence interval [CI], 8.1–24.5). (b) Kaplan–Meier curves for overall survival (OS) among 52 patients who received chemoradiotherapy. The median OS period was 40.1 months (95% CI, 16.6–50.6).
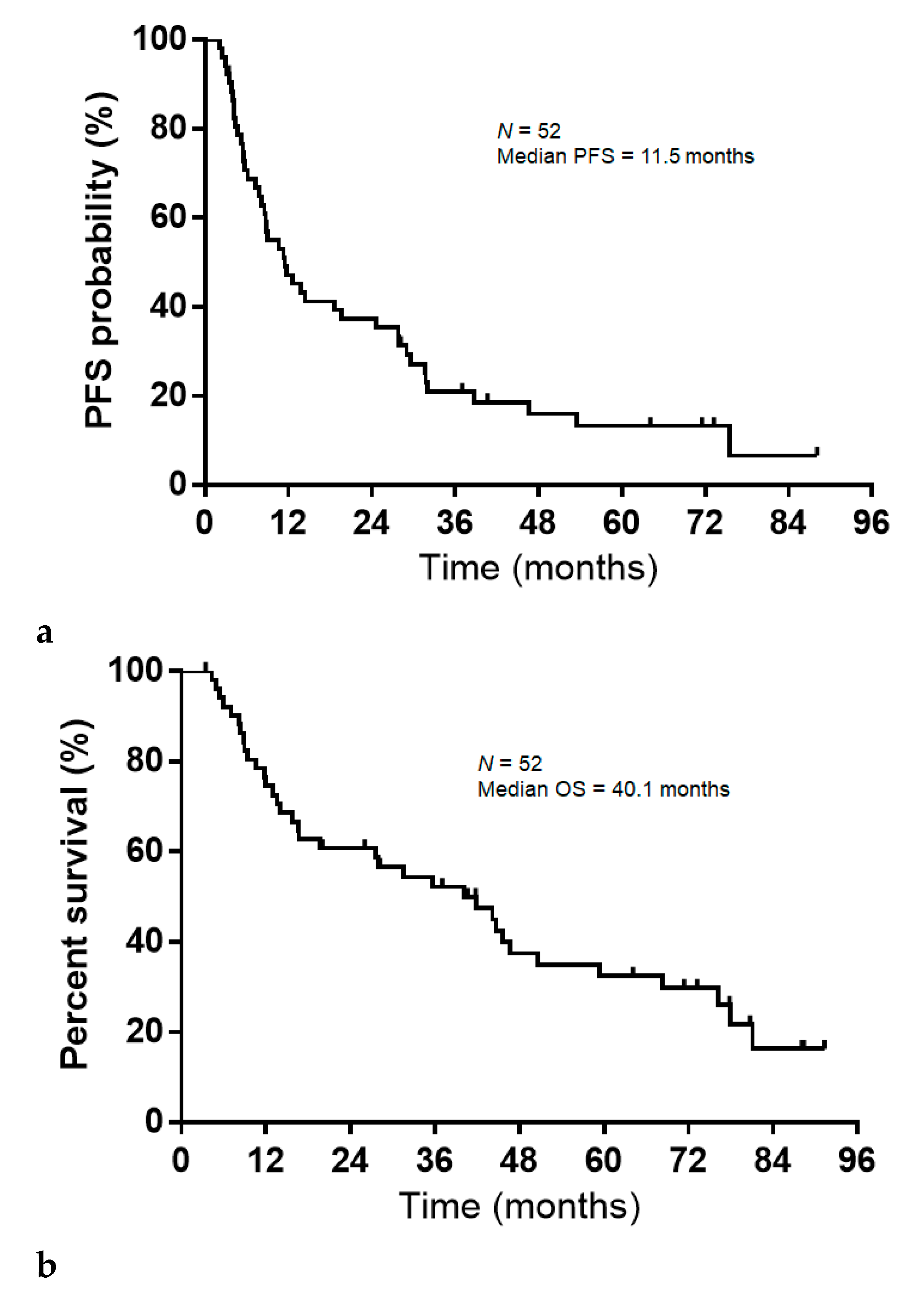
Figure 2.
(a) Progression-free survival (PFS) according to Glasgow Prognostic Score (GPS) at the initiation of chemoradiotherapy (GPS 0–1, median PFS=13.7 months; GPS 2, median PFS=5.6 months). (b). Overall survival (OS) according to Glasgow Prognostic Score (GPS) at the initiation of chemoradiotherapy (GPS 0–1, median OS=45.6 months; GPS 2, median OS=13.0 months).
Figure 2.
(a) Progression-free survival (PFS) according to Glasgow Prognostic Score (GPS) at the initiation of chemoradiotherapy (GPS 0–1, median PFS=13.7 months; GPS 2, median PFS=5.6 months). (b). Overall survival (OS) according to Glasgow Prognostic Score (GPS) at the initiation of chemoradiotherapy (GPS 0–1, median OS=45.6 months; GPS 2, median OS=13.0 months).
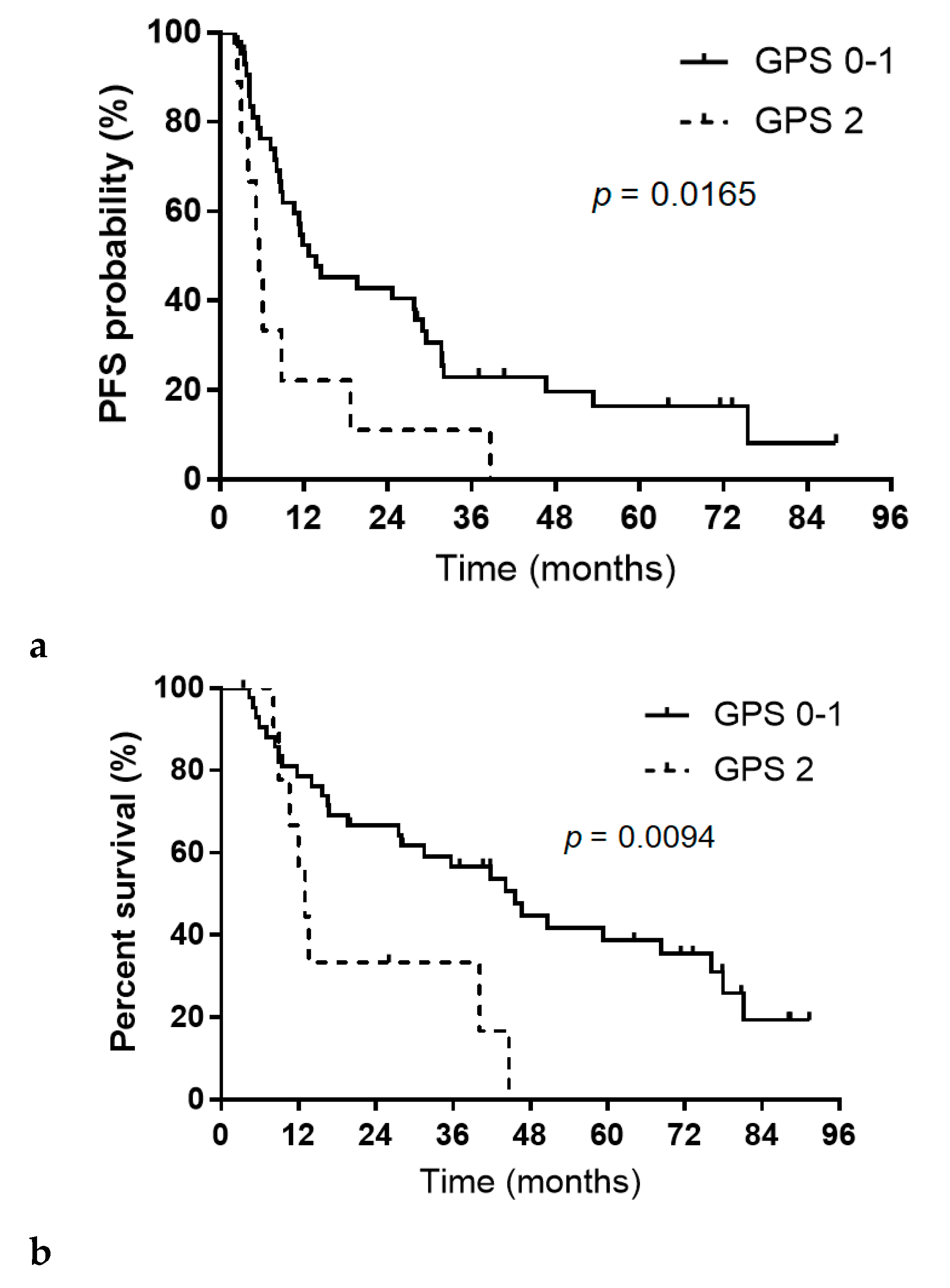

Table 1.
Patient characteristics.
| Characteristic | Total (n=52) | (%) |
With Durvalumab (n=20) |
(%) |
Without Durvalumab (n=32) |
(%) | p-Value |
| Sex | |||||||
| Men | 41 | 78.8 | 17 | 85.0 | 24 | 75.0 | 0.49 |
| Women | 11 | 21.2 | 3 | 15.0 | 8 | 25.0 | |
| Age (years) | |||||||
| Median | 76 | 76 | 76 | 0.23** | |||
| Range | 71–86 | 71–80 | 71–86 | ||||
| Performance status (ECOG-PS) | |||||||
| 0 | 29 | 55.8 | 9 | 45.0 | 20 | 62.5 | 0.28*** |
| 1 | 22 | 42.3 | 11 | 55.0 | 11 | 34.4 | |
| 2 | 1 | 1.9 | 0 | 0 | 1 | 3.1 | |
| Smoking status | |||||||
| Current or former | 43 | 82.7 | 17 | 85.0 | 26 | 81.3 | >0.99 |
| Never | 9 | 17.3 | 3 | 15.0 | 6 | 18.7 | |
| Histology | |||||||
| Adenocarcinoma | 23 | 44.2 | 8 | 40.0 | 15 | 46.9 | 0.31*** |
| Squamous cell carcinoma | 23 | 44.2 | 8 | 40.0 | 15 | 46.9 | |
| Others | 6 | 11.6 | 4 | 20.0 | 2 | 6.2 | |
| Driver mutations/translocations (EGFR, ALK, ROS-1) | |||||||
| Positive | 7 | 13.5 | 1 | 5.0 | 6 | 18.7 | - |
| Wild type or negative | 37 | 71.1 | 15 | 75.0 | 22 | 68.8 | |
| Others | 0 | 0 | 0 | 0 | 0 | 0 | |
| Not tested | 8 | 15.4 | 4 | 20.0 | 4 | 12.5 | |
| PD-L1 TPS (%) | |||||||
| <1 | 11 | 21.2 | 6 | 30.0 | 5 | 15.6 | - |
| 1–49 | 13 | 25.0 | 7 | 35.0 | 6 | 18.7 | |
| ≥50 | 9 | 17.3 | 3 | 15.0 | 6 | 18.7 | |
| Unknown | 19 | 36.5 | 4 | 20.0 | 15 | 46.9 | |
| Disease stage | |||||||
| II | 4 | 7.7 | 3 | 15.0 | 1 | 3.1 | 0.27*** |
| III | 41 | 78.8 | 15 | 75.0 | 26 | 81.3 | |
| Postoperative recurrence | 7 | 13.5 | 2 | 10.0 | 5 | 15.6 | |
| History of postoperative adjuvant chemotherapy | |||||||
| Yes | 0 | 0 | 0 | 0 | 0 | 0 | >0.99 |
| No | 52 | 100 | 20 | 100 | 32 | 100 | |
| BMI (kg/m2) | |||||||
| Median | 22.2 | 20.6 | 23.3 | 0.017** | |||
| Range | 16.1–27.6 | 16.1–26.8 | 18.2–27.6 | ||||
| Radiotherapy planned dose completion | |||||||
| Yes | 50 | 96.2 | 20 | 100 | 30 | 93.8 | 0.51 |
| No | 2 | 3.8 | 0 | 0 | 2 | 6.2 | |
| Irradiation dose (Gy) | |||||||
| Median | 60 | 60 | 60 | 0.51** | |||
| Range | 45–66 | 60 | 45–66 | ||||
| Administration of CBDCA planned dose completion | |||||||
| Yes | 40 | 76.9 | 14 | 70.0 | 26 | 81.3 | 0.5 |
| No | 12 | 23.1 | 6 | 30.0 | 6 | 18.7 | |
| Number of cycles CBDCA administered | |||||||
| Median | 20 | 20 | 20 | 0.37** | |||
| Range | 4–20 | 6–20 | 4–20 | ||||
| Reason for discontinuation of CBDCA administration | |||||||
| Progressive disease | 0 | 0 | 0 | 0 | 0 | 0 | - |
| Adverse events | 11 | 21.2 | 6 | 30.0 | 5 | 15.6 | |
| Worsening of PS | 0 | 0 | 0 | 0 | 0 | 0 | |
| Others | 1 | 1.9 | 0 | 0 | 1 | 3.1 | |
| Laboratory data, median [range] | |||||||
| CRP (mg/dL) | 0.3 (0.0–10.1) |
0.2 (0.0–10.1) |
0.3 (0.0–6.3) |
0.56** | |||
| Albumin (g/dL) | 3.7 (2.0–4.5) |
3.8 (2.0–4.4) |
3.7 (2.3–4.5) |
0.93** | |||
| Neutrophil (cells/mm3) | 4274 (2103–8116) |
4371 (2103–8116) |
4274 (2188–7200) |
0.39** | |||
| Lymphocyte (cells/mm3) | 1279 (530–10150) |
1203 (729–10150) |
1371 (530–2160) |
0.38** | |||
| Platelets (cells/mm3) | 246000 (116000–514000) |
256000 (131000–514000) |
234000 (116000–336000) |
0.23** | |||
| GPS | |||||||
| 0, 1 | 43 | 82.7 | 17 | 85.0 | 26 | 81.3 | >0.99 |
| 2 | 9 | 17.3 | 3 | 15.0 | 6 | 18.7 | |
| NLR | |||||||
| Low (<5) | 44 | 84.6 | 15 | 75.0 | 29 | 90.6 | 0.23 |
| High (≥5) | 8 | 15.4 | 5 | 25.0 | 3 | 9.4 | |
| PLR | |||||||
| Low (<185) | 23 | 44.2 | 6 | 30.0 | 17 | 53.1 | 0.15 |
| High (≥185) | 29 | 55.8 | 14 | 70.0 | 15 | 46.9 | |
| ALI | |||||||
| Low (<24) | 26 | 50.0 | 14 | 70.0 | 12 | 37.5 | 0.004 |
| High (≥24) | 26 | 50.0 | 6 | 30.0 | 20 | 62.5 | |
| Relapse at data cutoff | |||||||
| Yes | 44 | 84.6 | 15 | 75.0 | 29 | 90.6 | 0.23 |
| No | 8 | 15.4 | 5 | 25.0 | 3 | 9.4 | |
| Alive at data cutoff | |||||||
| Alive | 16 | 30.8 | 8 | 40.0 | 8 | 25.0 | 0.35 |
| Death | 36 | 69.2 | 12 | 60.0 | 24 | 75.0 |
ECOG, Eastern Cooperative Oncology Group; PS, performance status; PD-L1, programmed death-ligand 1; TPS, tumor proportion score; BMI, body mass index; CBDCA, carboplatin; CRP, C-reactive protein; GPS, Glasgow Prognostic Score; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; ALI, Advanced Lung Cancer Inflammation Index. *Seven of 20 patients completed 1 year of durvalumab maintenance therapy. **Welch’s t-test. ***Chi-squared test.
Table 2.
Comparison of treatment responses between the overall population and patients with and without durvalumab maintenance therapy.
Table 2.
Comparison of treatment responses between the overall population and patients with and without durvalumab maintenance therapy.
| Response | n=52 | (%) | With Durvalumab (n=20) | Without Durvalumab (n=32) | p-Value |
| Complete response | 0 | 0 | 0 | 0 | |
| Partial response | 27 | 51.9 | 10 | 17 | |
| Stable disease | 22 | 42.3 | 10 | 12 | |
| Progressive disease | 3 | 5.8 | 0 | 3 | |
| Not evaluated | 0 | 0 | 0 | 0 | |
| Response rate (%) (95% CI) | 51.9 | 38.6–64.8 | 50.0 (28.0–71.9) | 53.1 (35.8–70.4) | >0.99 |
| Disease control rate (%) (95% CI) | 94.2 | 83.7–98.6 | 100 | 90.6 (80.5–100.7) | 0.27 |
CI, confidence interval.
Table 3.
Associations between clinical factors and progression-free survival (PFS) and overall survival (OS).
Table 3.
Associations between clinical factors and progression-free survival (PFS) and overall survival (OS).
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||||||||
| PFS | PFS | OS | OS | |||||||||||
| Factors | Median PFS (months) | HR | 95% CI | p-value | HR | 95% CI | p-value | Median OS (months) | HR | 95% CI | p-value | HR | 95% CI | p-value |
| Sex | ||||||||||||||
| Men/women | 10.6 / 24.5 | 1.1 | 0.55–2.37 | 0.78 | 35.7 / 44.1 | 0.91 | 0.44–2.07 | 0.82 | ||||||
| Age (years) at the start of chemoradiotherapy | ||||||||||||||
| 71–74/≥75 | 8.8 / 11.8 | 1.12 | 0.54–2.17 | 0.73 | 16.7 / 45.6 | 1.79 | 0.80–3.69 | 0.14 | ||||||
| Smoking status | ||||||||||||||
| Current or former/never | 11.3 / 13.7 | 1.05 | 0.51–2.46 | 0.88 | 27.9 / 50.6 | 1.42 | 0.63–3.78 | 0.41 | ||||||
| Histology | ||||||||||||||
| Adenocarcinoma/non-adenocarcinoma | 13.7 / 8.8 | 0.84 | 0.46–1.53 | 0.58 | 59.4 / 16.6 | 0.48 | 0.24–0.95 | 0.0353 | ||||||
| Driver mutations/translocations | ||||||||||||||
| Positive/negative or unknown | 11.3 / 11.8 | 1.37 | 0.55–2.93 | 0.46 | 51.8 / 31.5 | 0.89 | 0.33–2.01 | 0.80 | ||||||
| Disease stage at diagnosis | ||||||||||||||
| II–III/postoperative recurrence | 12.6 / 8.5 | 0.74 | 0.31–2.18 | 0.55 | 41.8 / 27.5 | 1.48 | 0.45–4.86 | 0.51 | ||||||
| BMI (kg/m2) | ||||||||||||||
| Low (<22.0)/high (≥22.0) | 10.4 / 11.5 | 1.04 | 0.57–1.89 | 0.88 | 40.1 / 41.8 | 1.24 | 0.64–2.41 | 0.50 | ||||||
| GPS | ||||||||||||||
| 0, 1/2 | 13.7 / 5.6 | 0.41 | 0.20–0.92 | 0.0329 | 0.36 | 0.16–0.89 | 0.0294 | 45.6 / 13.0 | 0.34 | 0.15–0.84 | 0.0218 | 0.42 | 0.16–1.18 | 0.09 |
| NLR | ||||||||||||||
| Low (<5)/high (≥5) | 12.6 / 7.3 | 0.58 | 0.27–1.45 | 0.23 | 0.55 | 0.20–1.60 | 0.26 | 44.1 / 13.3 | 0.42 | 0.17–1.17 | 0.09 | 0.66 | 0.22–2.13 | 0.47 |
| PLR | ||||||||||||||
| Low (<185)/high (≥185) | 11.3 / 12.6 | 1.05 | 0.56–1.93 | 0.85 | 0.98 | 0.47–2.08 | 0.96 | 45.6 / 31.5 | 0.83 | 0.42–1.61 | 0.59 | 1.13 | 0.50–2.55 | 0.76 |
| ALI | ||||||||||||||
| Low (<24)/high (≥24) | 10.4 / 11.5 | 0.74 | 0.40–1.34 | 0.32 | 0.49 | 0.21–1.07 | 0.07 | 13.3 / 45.6 | 1.53 | 0.78–2.98 | 0.20 | 1.2 | 0.50–2.78 | 0.66 |
| Durvalumab maintenance therapy | ||||||||||||||
| Yes/no | 24.3 / 10.6 | 0.61 | 0.31–1.12 | 0.11 | 40.1 / 41.8 | 1.02 | 0.48–2.04 | 0.95 | ||||||
The bold font indicates a statistically significant difference. PFS, progression-free survival; OS, overall survival; HR, hazard ratio; CI, confidence interval; BMI, body mass index; GPS, Glasgow Prognostic Score; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; ALI, Advanced Lung Cancer Inflammation Index.
Table 4.
Adverse events during chemoradiotherapy.
| Adverse Event | Any Grade | % | Grade≥3 | % |
| Led to discontinuation | 12 | 23.1 | 10 | 19.2 |
| Led to death | - | - | 0 | 0 |
| Treatment-related adverse events | ||||
| White blood cell decreased | - | - | 13 | 25.0 |
| Neutrophil count decreased | - | - | 12 | 23.1 |
| Platelet count decreased | - | - | 9 | 17.3 |
| Febrile neutropenia | - | - | 1 | 1.9 |
| Skin rash | - | - | 2 | 3.8 |
| Liver dysfunction | - | - | 1 | 1.9 |
| Infection | - | - | 1 | 1.9 |
Report adverse events of grade 3 or higher, excluding those leading to discontinuation of treatment.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



