
Submitted:
19 February 2025
Posted:
20 February 2025
You are already at the latest version
Abstract
The incidence of cancer increases with age. Immunosenescence, characterized by a decline in adaptive immunity and chronic low-grade inflammation, may influence the efficacy of immune checkpoint inhibitors (ICIs) in elderly patients. Background/Objectives: While some studies suggest comparable efficacy of ICIs across age groups, others report reduced response due to immune system dysregulation. This study aimed to assess the prognostic value of age in ICI therapy for metastatic non-small cell lung cancer (mNSCLC). Methods: A retrospective, single-center cohort study included 105 mNSCLC patients treated with pembrolizumab or atezolizumab at the Sumy Regional Clinical Oncology Center (Ukraine). Data on demographics, tumor histology, immunotherapy regimen, treatment response, survival outcomes, and immune-related adverse events (irAEs) were collected in medical records. Statistical analyses included chi-square tests, Kaplan-Meier survival analysis, and multivariate Cox regression. Results: The cohort comprised 89 males (84.8%) and 16 females (15.2%), with a mean age of 60.8 years. No significant differences were observed in treatment duration (p=0.9718), objective response rate (χ2=0.7112; p=0,701), or disease control rate (χ2=0.1103; p=0,946) among age groups. Median progression-free survival (PFS) was 6.3, 7.0, and 12.3 months for patients <60, 60–69, and ≥70 years, respectively (p=0.5254). Overall survival (OS) also showed no significant age-related differences (p=0.5441). However, older patients exhibited a higher incidence of irAEs (p=0.035). Multivariate analysis identified ICI treatment duration (p=0.0001) and objective response rate (p=0.009) as independent predictors of PFS. Conclusions: Age does not significantly impact ICI therapy efficacy in mNSCLC patients. However, elderly patients require careful monitoring due to an increased risk of irAEs.
Keywords:
age
; non-small cell lung cancer
; immune checkpoint inhibitors
; toxicity
; treatment duration
1. Introduction
The risk of developing malignant neoplasms steadily increases with age. In 2050, approximately 6.9 million cancer cases will be registered among individuals over 80 years old. In men, lung cancer, colorectal cancer, and prostate cancer will be the most commonly diagnosed, whereas in women, breast cancer, lung cancer, and colorectal cancer will prevail [1]. According to the World Health Organization (WHO), individuals aged 60–75 are considered elderly in developing countries, while those older than 75 are classified as senile. However, alternative classifications exist. The International Society of Geriatric Oncology (SIOG) suggests defining individuals aged 70 and older as senile [2].
Senescence leads to a decline in the functional capabilities of the human body. The accumulation of DNA damage in cells may contribute to carcinogenesis [3]. Elderly individuals experience changes in various organs and systems, including the immune system. Immunosenescence is a natural phenomenon characterized by a decline in adaptive immunity and an increased risk of malignant tumor development [4]. Interestingly, despite weakening the body's defense mechanisms, elderly and senile individuals develop a pro-inflammatory status. Elevated inflammatory markers in peripheral blood indicate low-grade chronic inflammation. The precise causes of this condition remain unclear, but one of the most plausible explanations is the impact of infectious agents on the weakened immune system [5,6].
Immunosenescence is closely linked to involutional changes in the thymus, an immune organ responsible for developing acquired and innate immunity. Senescence mainly affects T cells. Functionally and morphologically defective T lymphocytes fail to ensure reliable antitumor immunity, increasing the risk of cancer [7,8].
Thus, the incidence of cancer increases with the growing elderly population. Treating elderly cancer patients presents significant challenges, particularly for those with metastatic disease requiring systemic therapy (chemotherapy, targeted therapy, and immunotherapy) [9]. Elderly patients often have chronic conditions that may be exacerbated during chemotherapy. Moreover, cytotoxic treatment alone does not lead to high overall survival (OS) [10].
Immune checkpoint inhibitors (ICIs) are a promising alternative to chemotherapy. They can be used as monotherapy or in combination with chemotherapy, significantly improving treatment outcomes. Immunotherapy is associated with fewer adverse effects, better tolerability, and improved quality of life [11,12]. Based on the theory of immunosenescence, ICIs might be expected to be less effective in elderly and senile individuals. On the other hand, low-grade chronic inflammation could enhance the response to immunotherapy.
The scientific literature does not provide a definitive answer regarding the efficacy of ICIs in elderly and senile patients with metastatic non-small cell lung cancer (mNSCLC). Some authors advocate for immunotherapy regardless of patient age. For example, Yamaguchi et al. [13] found that ICI therapy improved survival in elderly patients, with similar safety and efficacy profiles to younger patients. Conversely, Al-Danakh et al. [14] concluded that senile patients had a poorer response to ICI therapy than younger patients due to immunosenescence and qualitative and quantitative alterations in tumor-infiltrating immune cells. The authors suggested that immune system dysregulation leads to immune cell exhaustion and diminished response to ICI therapy. Consequently, the prognostic significance of age in ICI therapy remains unclear. This study aimed to investigate the prognostic value of age in ICI therapy for mNSCLC, using age thresholds defined by WHO and SIOG.
2. Materials and Methods
2.1. The Ethics Committee
The study was approved by the Commission on Bioethics in Experimental and Clinical Research of the Educational and Scientific Medical Institute of Sumy State University (№ 3/12, date of approval 17 December 2024). All patients who were alive at the start of the study signed an informed consent form.
2.2. Patient Population
This retrospective, single-center cohort study included 105 mNSCLC patients who received ICI therapy at the Sumy Regional Clinical Oncology Center (Ukraine) between 2016 and 2024. Inclusion criteria were age ≥18 years, histologically confirmed NSCLC, metastatic disease, and at least one dose of pembrolizumab or atezolizumab. Exclusion criteria included small cell lung cancer, NSCLC stages I–III, or the presence of another malignant tumor.
2.3. Data Collection
Data on patient sex, age, tumor histology, immunotherapy regimen, therapy line, type of ICI, treatment duration, metastatic sites, and immune-related adverse events (irAEs) were obtained from medical records. The severity of irAEs was assessed using the Common Terminology Criteria for Adverse Events (CTCAE, version 5). Tumor response was evaluated using the immune Response Evaluation Criteria in Solid Tumors (iRECIST). Mortality data were retrieved from the cancer registry of Sumy Regional Clinical Oncology Center.
2.3. Statistical Analysis
Categorical variables were expressed as percentages and frequencies. Associations between categorical variables were analyzed using the chi-square test. The Shapiro-Wilk test was used to assess normality contribution. Continuous variables across three age groups were compared using the Kruskal-Wallis test. Objective response rate (ORR) was defined as the proportion of patients achieving complete or partial response. Disease control rate (DCR) was defined as the proportion of patients achieving complete response, partial response, or stable disease. Progression-free survival (PFS) was calculated as the time from the first infusion of ICI therapy to disease progression, and OS was defined as the time from the start of ICI therapy to death. Kaplan-Meier curves were used to visualize survival stratified by age (<60 years, 60–69 years, ≥70 years). The log-rank test assessed survival differences. Multivariate Cox regression analysis identified prognostic factors for PFS and OS. Statistical analysis was performed using Stata V.18.0 (StataCorp, Texas, USA; https://www.stata.com), with p<0.005 considered statistically significant.
3. Results
3.1. Patient Characteristics
Among the 105 patients with mNSCLC, 89 (84.8%) were male, and 16 (15.2%) were female. The mean patient age was 60.8 years (range: 34–78 years). The proportion of patients aged <60, 60–69, and ≥70 years was 39.0%, 46.7%, and 14.3%, respectively. Table 1 presents the stratified patient characteristics by age group.
A statistically significant association was observed between age groups, pleural metastases, and irAEs. Among patients of senile age (≥70 years), pleural metastases were registered in 53.3% of cases, whereas among elderly (60–69 years) and younger patients (<60 years), the rates were only 4.1% and 4.9%, respectively (χ²=30.3724; p=0.0001). This finding suggests an age-related difference in the frequency of pleural metastases.
Immune-related adverse events were also more common in patients aged ≥70. In this group, 60.0% experienced irAEs, compared to 22.4% of patients aged 60–69 and 17.1% younger than 60 (χ²=8.0142; p=0.018). Other factors, such as sex, histological tumor subtype, metastatic sites (brain, lungs, liver, bones), therapy line, immunotherapy regimen, and ICI type, did not show statistically significant differences between the three age groups.
3.2. Treatment duration
The median duration of ICI therapy in the studied cohort was 8.0 months (range: 1.0–24.0 months). No significant association was observed between treatment duration and age groups (p=0.9718, Table 2).
3.3. Treatment Response
Complete response was observed in 6/105 (5.7%) patients, partial response in 48/105 (45.7%), stable disease in 37/105 (35.2%), and progressive disease in 14/105 (13.4%). Consequently, the ORR was 51.4%, and the DCR was 86.6%. No statistically significant association was observed between treatment response and age groups (Table 3).
3.4. Survival Analysis
Disease progression was recorded in 96/105 (91.4%) patients during the follow-up period. The median PFS in patients aged <60, 60–69, and ≥70 years was 6.3, 7.0, and 12.3 months, respectively. No statistically significant differences in PFS were observed between age groups (Log-rank p=0.5254, Figure 1).
Mortality was recorded in 100/105 (95.2%) patients, including 96/100 (96.0%) deaths due to mNSCLC progression and 4/100 (4.0%) from other causes. The median overall OS in patients aged <60, 60–69, and ≥70 years was 14.1, 16.8, and 11.6 months, respectively. No statistically significant differences in OS were found among age groups (Log-rank p=0.5441, Figure 2).
3.5. Independent Predictors of Survival
Multivariate regression analysis demonstrated that ORR and ICI treatment duration were independent predictors of PFS. Patients who achieved a complete or partial response to ICI therapy had better PFS than those with stable or progressive disease (HR=2.64, 95% CI: 1.27–5.48, p=0.009). Patients who received ICI therapy for at least 8.0 months had significantly improved PFS compared to those treated for less than 8.0 months (HR=41.09, 95% CI: 12.99–129.99, p=0.0001).
ICI treatment duration was also identified as an independent predictor of OS. Patients who received ICI therapy for at least 8.0 months had superior OS (HR=6.61, 95% CI: 3.07–14.22, p=0.0001). Other factors, including age, sex, tumor histology, metastatic sites (brain, lungs, pleura, liver, bones), therapy line, immunotherapy regimen, ICI type, and immune-related adverse events, did not significantly affect survival (Table 4).
3.6. Immune-Related Adverse Events
Patients aged 70 years and older had a higher prevalence of irAEs than younger patients (p=0.035), particularly hyperthyroidism. However, when analyzing grade 3 or higher toxicity, the results were comparable across all age groups (p=0.874). The comparative analysis of ICI-related toxicity in age-stratified patient groups is presented in Table 5.
4. Discussion
We found that elderly patients with mNSCLC (aged ≥70 years) had a higher incidence of pleural metastases and irAEs than younger patients. However, we did not observe significant differences in the effectiveness of ICIs among different age groups. Age was not a determining factor for PFS or OS. Instead, the duration of ICI therapy was identified as an independent predictor of both PFS and OS. Furthermore, achieving an objective response to treatment (complete or partial response) was a favorable prognostic factor for PFS. Although elderly patients had a higher rate of irAEs, this did not impact ICI therapy efficacy.
The interaction between tumors and the immune system is highly complex. In peripheral blood, malignant cells undergo apoptosis, releasing antigens that are then processed by antigen-presenting cells. Through antigen-specific T-cell activation, an adaptive immune response is initiated [15]. Upon entering the tumor microenvironment, antigen-specific T cells recognize malignant cells via their receptors, triggering a tumor-specific immune response [16].
Multiple inhibitory and activating factors influence the interaction between tumor and immune cells, with immune checkpoints playing a pivotal role. Programmed cell death protein 1 (PD-1) is a key inhibitory receptor expressed on T cells, regulating their proliferation in response to activation [17]. Immune checkpoint pathways control immune responses at the interface of antigen-presenting cells and T cells, with a particularly critical role in the effector phase within the tumor microenvironment. PD-1 and its ligand (PD-L1) have become major therapeutic targets for ICIs, demonstrating remarkable clinical benefits across various malignancies [18,19,20].
Senescence is associated with functional alterations in the immune system, including a decline in T and B lymphocyte populations, increased regulatory T cells, and reduced antigen-presenting cell activity [21]. The most pronounced changes occur in adaptive immunity, where shifts in memory T-cell pools impair antigen recognition and weaken overall immune responses [22].
These physiological changes raise concerns about the effectiveness of ICI therapy in older patients. However, the prognostic significance of age remains unclear. A meta-analysis by Sun et al. [23], including 2,662 patients younger than 65 years and 1,971 patients aged ≥65 years, reported no significant differences in ICI efficacy between age groups. Similarly, Arias et al. [24] studied nivolumab in 188 patients aged ≥70 years and found no deviation in safety and efficacy compared to the global population. Luciani et al. [25] examined survival outcomes in 86 patients aged ≥75 years with locally advanced or metastatic NSCLC treated with ICIs and found no differences in efficacy or toxicity between younger and older patients.
In contrast, Lichtenstein et al. [26] reported age-related differences in ICI efficacy and toxicity. Their retrospective study of 245 NSCLC patients receiving PD-1/PD-L1 inhibitors categorized patients into four age groups: <60, 60–69, 70–79, and ≥80 years. The worst PFS (1.64 months) and OS (3.63 months) were observed in the ≥80-year-old cohort. Regression analysis identified age ≥80 years as a negative prognostic factor. Xu et al. [27] similarly reported lower ICI efficacy in patients aged ≥75 years. However, the prevalence of non-hematologic irAEs did not differ significantly between groups.
In the present study, the mean patient age was 60.8 years, with only 14.3% of patients aged ≥70 years. The absence of survival and efficacy differences among age groups may be attributed to the low percentage of patients aged ≥75 years and the complete absence of those ≥80 years. Immunosenescence may be more pronounced in the oldest age groups. However, Mebarki et al. [28] challenged this hypothesis, reporting comparable ICI efficacy in patients younger than 80 and those aged ≥80 years.
Most studies suggest that ICI toxicity profiles do not significantly differ by age. However, older patients have a higher risk of treatment discontinuation and mortality due to severe irAEs [29,30]. In our study, patients aged ≥70 years had a higher incidence of irAEs, but this did not affect PFS or OS. Similar findings were reported by Ramos et al. [31] and Mebarki et al. [28], who examined ICI efficacy and safety in mNSCLC patients.
We have established that the duration of ICI therapy is an independent prognostic factor for PFS and OS. The longer treatment period in patients with mNSCLC is associated with better clinical outcomes. Overall, the benefits of fixed-duration versus continuous ICI therapy in patients with metastatic disease remain a topic of debate. Bogani et al. [32], in a meta-analysis of 57 studies including 22,977 patients, found that prolonged ICI administration (beyond two years) was associated with improved OS compared to fixed-duration treatment. Kim et al. [33] compared clinical outcomes in mNSCLC patients who received ICI therapy for six months versus 24 months and discontinued treatment without disease progression. The authors concluded that patients treated for 24 months had better PFS. However, those who received ICI therapy for only six months also largely achieved a durable response. In our study, no patients received ICI therapy beyond 24 months; however, we observed better treatment outcomes in patients who underwent at least eight months of ICI therapy.
This study has several limitations, including its retrospective design, a relatively small percentage of patients aged ≥70 years, and the absence of molecular testing of tumor tissue.
5. Conclusions
Age is not a primary determinant of ICI therapy efficacy in mNSCLC patients. However, elderly patients require closer monitoring due to the higher incidence of immune-related adverse events. The duration of ICI therapy was identified as an independent predictor of both PFS and OS. Additionally, achieving an objective response to treatment was a favorable prognostic factor for PFS.
Author Contributions
Conceptualization Y.M.; methodology Y.M.; investigation Y.M. and R.M.; resources Y.M., O.Y., and R.M.; data curation Y.M.; writing—original draft preparation Y.M.; writing—review and editing R.M. and Y.M.; visualization K.S., T.I. and O.V.; supervision R.M.; project administration R.M.; funding acquisition YM, RM. All authors have read and agreed to the published version of the manuscript.
Funding
This research has been performed with the financial support of grants of the external aid instrument of the European Union for the fulfillment of Ukraine's obligations in the Framework Program of the European Union for Scientific Research and Innovation "Horizon 2020" No. RN/ 11 – 2023 "The role of the DNA repair system in the pathogenesis and immunogenicity of lung cancer.".
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Commission on Bioethics in Experimental and Clinical Research of the Educational and Scientific Medical Institute of Sumy State University (№ 3/12, date of approval 17 December 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
We kindly thank Ihor Vynnychenko and Oleksandr Vynnychenko for consultations.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| WHO | World Health Organization |
| SIOG | International Society of Geriatric Oncology |
| ICI | Immune checkpoint inhibitor |
| mNSCLC | Metastatic non-small cell lung cancer |
References
- Pilleron S, Soto-Perez-de-Celis E, Vignat J, Ferlay J, Soerjomataram I, Bray F, Sarfati D. Estimated global cancer incidence in the oldest adults in 2018 and projections to 2050. Int J Cancer. 2021 Feb 1;148(3):601-608. [CrossRef]
- Ferrat E, Paillaud E, Caillet P, Laurent M, Tournigand C, Lagrange JL, Droz JP, Balducci L, Audureau E, Canouï-Poitrine F, Bastuji-Garin S. Performance of Four Frailty Classifications in Older Patients With Cancer: Prospective Elderly Cancer Patients Cohort Study. J Clin Oncol. 2017 Mar;35(7):766-777. [CrossRef]
- Kudlova N, De Sanctis JB, Hajduch M. Cellular Senescence: Molecular Targets, Biomarkers, and Senolytic Drugs. Int J Mol Sci. 2022 Apr 10;23(8):4168. [CrossRef]
- Liu Z, Liang Q, Ren Y, Guo C, Ge X, Wang L, Cheng Q, Luo P, Zhang Y, Han X. Immunosenescence: molecular mechanisms and diseases. Signal Transduct Target Ther. 2023 May 13;8(1):200. [CrossRef]
- Franceschi C, Bonafè M, Valensin S, Olivieri F, De Luca M, Ottaviani E, De Benedictis G. Inflamm-aging. An evolutionary perspective on immunosenescence. Ann N Y Acad Sci. 2000 Jun;908:244-54. [CrossRef]
- Santoro A, Bientinesi E, Monti D. Immunosenescence and inflammaging in the aging process: age-related diseases or longevity? Ageing Res Rev. 2021 Nov;71:101422. [CrossRef]
- Gulla S, Reddy MC, Reddy VC, Chitta S, Bhanoori M, Lomada D. Role of thymus in health and disease. Int Rev Immunol. 2023;42(5):347-363. [CrossRef]
- Goronzy JJ, Weng NP. The immunology and cell biology of T cell aging. Semin Immunol. 2023 Nov;70:101843. [CrossRef]
- Dale W, Klepin HD, Williams GR, Alibhai SMH, Bergerot C, Brintzenhofeszoc K, Hopkins JO, Jhawer MP, Katheria V, Loh KP, Lowenstein LM, McKoy JM, Noronha V, Phillips T, Rosko AE, Ruegg T, Schiaffino MK, Simmons JF Jr, Subbiah I, Tew WP, Webb TL, Whitehead M, Somerfield MR, Mohile SG. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Systemic Cancer Therapy: ASCO Guideline Update. J Clin Oncol. 2023 Sep 10;41(26):4293-4312. [CrossRef]
- Matsuda S, Kitagawa Y, Okui J, Okamura A, Kawakubo H, Takemura R, Muto M, Kakeji Y, Takeuchi H, Watanabe M, Doki Y. Old age and intense chemotherapy exacerbate negative prognostic impact of postoperative complication on survival in patients with esophageal cancer who received neoadjuvant therapy: a nationwide study from 85 Japanese esophageal centers. Esophagus. 2023 Jul;20(3):445-454. [CrossRef]
- Kim SY, Halmos B. Choosing the best first-line therapy: NSCLC with no actionable oncogenic driver. Lung Cancer Manag. 2020 Jul 24;9(3):LMT36. [CrossRef]
- Choucair K, Naqash AR, Nebhan CA, Nipp R, Johnson DB, Saeed A. Immune Checkpoint Inhibitors: The Unexplored Landscape of Geriatric Oncology. Oncologist. 2022 Sep 2;27(9):778-789. [CrossRef]
- Yamaguchi O, Imai H, Minemura H, Suzuki K, Wasamoto S, Umeda Y, Osaki T, Kasahara N, Uchino J, Sugiyama T, Ishihara S, Ishii H, Naruse I, Mori K, Kotake M, Kanazawa K, Minato K, Kagamu H, Kaira K. Efficacy and safety of immune checkpoint inhibitor monotherapy in pretreated elderly patients with non-small cell lung cancer. Cancer Chemother Pharmacol. 2020 Apr;85(4):761-771. [CrossRef]
- Al-Danakh A, Safi M, Jian Y, Yang L, Zhu X, Chen Q, Yang K, Wang S, Zhang J, Yang D. Aging-related biomarker discovery in the era of immune checkpoint inhibitors for cancer patients. Front Immunol. 2024 Mar 15;15:1348189. [CrossRef]
- Shanmugam G, Das S, Paul S, Rakshit S, Sarkar K. Clinical relevance and therapeutic aspects of professional antigen-presenting cells in lung cancer. Med Oncol. 2022 Sep 29;39(12):237. [CrossRef]
- Wang C, Chen L, Fu D, Liu W, Puri A, Kellis M, Yang J. Antigen presenting cells in cancer immunity and mediation of immune checkpoint blockade. Clin Exp Metastasis. 2024 Aug;41(4):333-349. [CrossRef]
- Granier C, Gey A, Roncelin S, Weiss L, Paillaud E, Tartour E. Immunotherapy in older patients with cancer. Biomed J. 2021 Jun;44(3):260-271. [CrossRef]
- Tang S, Qin C, Hu H, Liu T, He Y, Guo H, Yan H, Zhang J, Tang S, Zhou H. Immune Checkpoint Inhibitors in Non-Small Cell Lung Cancer: Progress, Challenges, and Prospects. Cells. 2022 Jan 19;11(3):320. [CrossRef]
- Fasano M, Corte CMD, Liello RD, Viscardi G, Sparano F, Iacovino ML, Paragliola F, Piccolo A, Napolitano S, Martini G, Morgillo F, Cappabianca S, Ciardiello F. Immunotherapy for head and neck cancer: Present and future. Crit Rev Oncol Hematol. 2022 Jun;174:103679. [CrossRef]
- Yang YN, Wang LS, Dang YQ, Ji G. Evaluating the efficacy of immunotherapy in gastric cancer: Insights from immune checkpoint inhibitors. World J Gastroenterol. 2024 Aug 28;30(32):3726-3729. [CrossRef]
- Li H, Lin S, Wang Y, Shi Y, Fang X, Wang J, Cui H, Bian Y, Qi X. Immunosenescence: A new direction in anti-aging research. Int Immunopharmacol. 2024 Nov 15;141:112900. [CrossRef]
- Smith A, Boby JM, Benny SJ, Ghazali N, Vermeulen E, George M. Immunotherapy in Older Patients with Cancer: A Narrative Review. Int J Gen Med. 2024 Jan 30;17:305-313. [CrossRef]
- Sun YM, Wang Y, Sun XX, Chen J, Gong ZP, Meng HY. Clinical Efficacy of Immune Checkpoint Inhibitors in Older Non-small-Cell Lung Cancer Patients: A Meta-Analysis. Front Oncol. 2020 Sep 23;10:558454. [CrossRef]
- Arias Ron D, Areses Manrique MC, Mosquera Martínez J, García González J, Afonso Afonso FJ, Lázaro Quintela M, Fernández Núñez N, Azpitarte Raposeiras C, Amenedo Gancedo M, Santomé Couto L, García Campelo MR, Muñoz Iglesias J, Ruiz Bañobre J, Vilchez Simo R, Casal Rubio J, Campos Balea B, Carou Frieiro I, Alonso-Jaudenes Curbera G, Anido Herranz U, García Mata J, Fírvida Pérez JL. Efficacy and safety of Nivolumab in older patients with pretreated lung cancer: A subgroup analysis of the Galician lung cancer group. J Geriatr Oncol. 2021 Apr;12(3):410-415. [CrossRef]
- Luciani A, Marra A, Toschi L, Cortinovis D, Fava S, Filipazzi V, Tuzi A, Cerea G, Rossi S, Perfetti V, Rossi A, Giannetta L, Sala L, Finocchiaro G, Pizzutilo EG, Carelli S, Agustoni F, Cergnul M, Zonato S, Siena S, Bidoli P, Ferrari D. Efficacy and Safety of Anti-PD-1 Immunotherapy in Patients Aged ≥ 75 Years With Non-small-cell Lung Cancer (NSCLC): An Italian, Multicenter, Retrospective Study. Clin Lung Cancer. 2020 Nov;21(6):e567-e571. [CrossRef]
- Lichtenstein MRL, Nipp RD, Muzikansky A, Goodwin K, Anderson D, Newcomb RA, Gainor JF. Impact of Age on Outcomes with Immunotherapy in Patients with Non-Small Cell Lung Cancer. J Thorac Oncol. 2019 Mar;14(3):547-552. [CrossRef]
- Xu Y, Wang Q, Xie J, Chen M, Liu H, Zhan P, Lv T, Song Y. The Predictive Value of Clinical and Molecular Characteristics or Immunotherapy in Non-Small Cell Lung Cancer: A Meta-Analysis of Randomized Controlled Trials. Front Oncol. 2021 Sep 7;11:732214. [CrossRef]
- Mebarki S, Pamoukdjian F, Pierro M, Poisson J, Baldini C, Widad Lahlou, Taieb J, Fabre E, Canoui-Poitrine F, Oudard S, Paillaud E. Safety and efficacy of immunotherapy according to the age threshold of 80 years. Bull Cancer. 2023 May;110(5):570-580. [CrossRef]
- Tagliamento M, Frelaut M, Baldini C, Naigeon M, Nencioni A, Chaput N, Besse B. The use of immunotherapy in older patients with advanced non-small cell lung cancer. Cancer Treat Rev. 2022 May;106:102394. [CrossRef]
- Huang X, Wu S, Chen S, Qiu M, Zhao Y, Wei J, He J, Zhao W, Tan L, Su C, Zhou S. Prognostic impact of age in advanced non-small cell lung cancer patients undergoing first-line checkpoint inhibitor immunotherapy and chemotherapy treatment. Int Immunopharmacol. 2024 May 10;132:111901. [CrossRef]
- Ramos MJ, Mendes AS, Romão R, Febra J, Araújo A. Immunotherapy in Elderly Patients-Single-Center Experience. Cancers (Basel). 2023 Dec 27;16(1):145. [CrossRef]
- Bogani G, Cinquini M, Signorelli D, Pizzutilo EG, Romanò R, Bersanelli M, Raggi D, Alfieri S, Buti S, Bertolini F, Bonomo P, Marandino L, Rizzo M, Monteforte M, Aiello M, Tralongo AC, Torri V, Di Donato V, Giannatempo P. A systematic review and meta-analysis on the optimal treatment duration of checkpoint inhibitoRS in solid tumors: The OTHERS study. Crit Rev Oncol Hematol. 2023 Jul;187:104016. [CrossRef]
- Kim H, Kim DW, Kim M, Lee Y, Ahn HK, Cho JH, Kim IH, Lee YG, Shin SH, Park SE, Jung J, Kang EJ, Ahn MJ. Long-term outcomes in patients with advanced and/or metastatic non-small cell lung cancer who completed 2 years of immune checkpoint inhibitors or achieved a durable response after discontinuation without disease progression: Multicenter, real-world data (KCSG LU20-11). Cancer. 2022 Feb 15;128(4):778-787. [CrossRef]
Figure 1.
Comparison of PFS by age group in patients with mNSCLC.
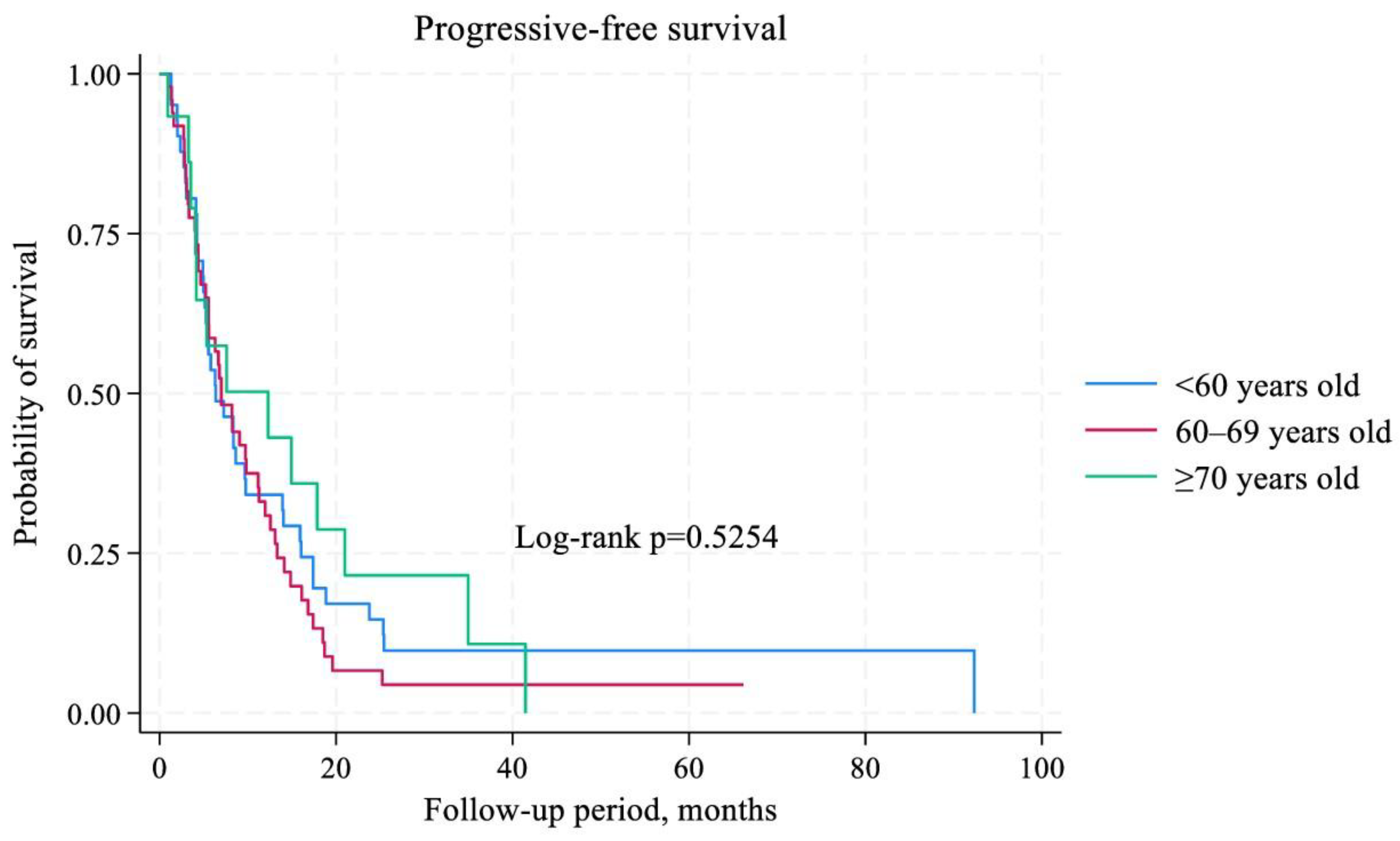
Figure 2.
Comparison of OS by age groups in patients with mNSCLC.
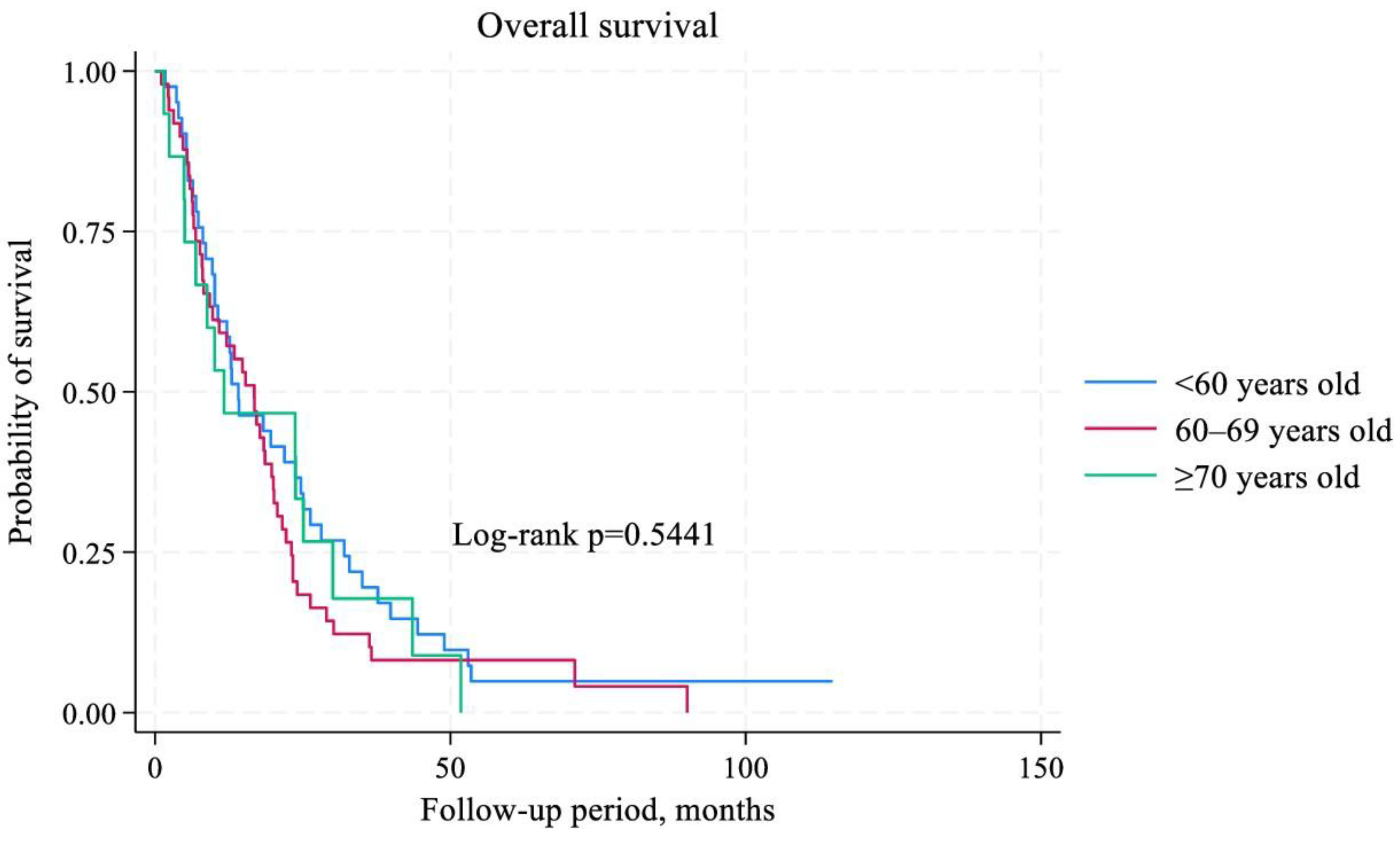

Table 1.
Stratified characteristics of patients by age group.
| Variables | <60 years, n=41 | 60–69 years, n=49 | ≥70 years, n=15 | χ2 (р) |
| Sex, n (%) Male Female |
34 (82,9) 7 (17,1) |
43 (87,8) 6 (12,2) |
12 (80,0) 3 (20,0) |
0,7101 (0,701) |
| Histology, n (%) Adenocarcinoma Squamous cell carcinoma |
26 (63,4) 15 (36,6) |
24 (49,0) 25 (51,0) |
8 (53,3) 7 (46,7) |
1,9068 (0,385) |
| Metastasis in the brain, n (%) Absent Present |
40 (97,6) 1 (2,4) |
48 (98,0) 1 (2,0) |
15 (100,0) 0 (0,0) |
0,3587 (0,836) |
| Metastasis in the lung, n (%) Absent Present |
21 (51,2) 20 (48,7) |
28 (57,1) 21 (42,9) |
7 (46,7) 8 (53,3) |
0,6272 (0,731) |
| Metastasis in the pleura, n (%) Absent Present |
39 (95,1) 2 (4,9) |
47 (95,9) 2 (4,1) |
7 (46,7) 8 (53,3) |
30,3724 (0,0001) |
| Metastasis in the liver, n (%) Absent Present |
33 (80,5) 8 (19,5) |
34 (69,4) 15 (30,6) |
9 (60,0) 6 (40,0) |
2,7177 (0,257) |
| Metastasis in the bones, n (%) Absent Present |
31 (75,6) 10 (24,4) |
29 (51,2) 20 (40,8) |
12 (80,0) 3 (20,0) |
3,8553 (0,145) |
| Treatment line, n (%) First Second |
36 (87,8) 5 (12,2) |
43 (87,8) 6 (12,2) |
14 (93,3) 1 (6,7) |
0,3921 (0,822) |
| Immunotherapy regimen, n (%) ICIs monotherapy Chemoimmunotherapy |
17 (41,5) 24 (58,5) |
16 (32,7) 33 (67,3) |
5 (33,3) 10 (66,7) |
0,8122 (0,666) |
| Type of ICIs, n (%) Atezolizumab Pembrolizumab |
18 (43,9) 23 (56,1) |
16 (32,7) 33 (67,3) |
5 (33,3) 10 (66,7) |
0,3187 (0,517) |
| irAE, n (%) Absent Present |
34 (82,9) 7 (17,1) |
38 (77,6) 11 (22,4) |
6 (40,0) 9 (60,0) |
8,0142 (0,018) |
Table 2.
Duration of ICI therapy in mNSCLC patients stratified by age group.
| Age groups | The median duration of ICI treatment (range), months | р |
| <60 years, n=41 | 7,8 (1,3–20,0) | 0,9718 |
| 60–69 years, n=49 | 7,6 (1,0–18,7) | |
| ≥70 years, n=15 | 8,8 (1,0–24,0) |
Table 3.
Comparison of treatment response among different age groups.
| Treatment response | <60 years, n (%) | 60–69, n (%) | ≥70 years, n (%) | χ2 (р) |
| ORR: Yes (n=54) No (n=51) |
19 (35,2) 22 (43,1) |
27 (50,0) 22 (43,1) |
8 (14,8) 7 (13,8) |
0,7112 (0,701) |
| DCR: Yes (n=91) No (n=14) |
35 (38,5) 6 (42,9) |
43 (47,3) 6 (42,9) |
13 (14,2) 2 (14,2) |
0,1103 (0,946) |
Table 4.
Multivariate regression analysis for predictors of PFS and OS in mNSCLC patients.
|
Variables |
PFS | OS | ||||
| HR | 95% CI | р | HR | 95% CI | р | |
| Age (<60 versus 60-69 versus ≥70 years old) | 1,27 | 0,89–1,81 | 0,184 | 1,21 | 0,86–1,70 | 0,254 |
| Sex (male versus female) | 1,37 | 0,58–3,23 | 0,460 | 1,12 | 0,45–2,76 | 0,804 |
| Histology (adenocarcinoma versus squamous cell carcinoma) | 0,92 | 0,56–1,51 | 0,759 | 1,17 | 0,70–1,94 | 0,539 |
| Metastasis in the brain (absent versus present) | 0,59 | 0,07–4,50 | 0,616 | 0,48 | 0,06–3,71 | 0,485 |
| Metastasis in the lung (absent versus present) | 1,34 | 0,83–2,16 | 0,225 | 1,12 | 0,71–1,77 | 0,618 |
| Metastasis in the pleura (absent versus present) | 0,85 | 0,27–1,51 | 0,693 | 1,45 | 0,64–3,25 | 0,364 |
| Metastasis in the liver (absent versus present) | 1,33 | 0,78–2,25 | 0,290 | 1,10 | 0,66–1,82 | 0,710 |
| Metastasis in the bones (absent versus present) | 1,03 | 0,65–1,64 | 0,879 | 0,86 | 0,53–1,40 | 0,555 |
| Treatment line (first versus second) | 0,50 | 0,22–1,16 | 0,111 | 0,65 | 0,25–1,72 | 0,396 |
| Immunotherapy regimen (ICI monotherapy versus chemoimmunotherapy) | 0,77 | 0,45–1,33 | 0,362 | 1,78 | 1,00–3,17 | 0,051 |
| Type of ICI (Atezolizumab versus Pembrolizumab) | 1,37 | 0,81–2,30 | 0,230 | 1,64 | 0,98–2,75 | 0,056 |
| irAE (absent versus present) | 1,00 | 0,56–1,80 | 0,985 | 0,82 | 0,45–1,51 | 0,534 |
| ORR (yes versus no) | 2,64 | 1,27–5,48 | 0,009 | 1,54 | 0,74–3,23 | 0,245 |
| DCR (yes versus no) | 2,43 | 0,91–6,51 | 0,076 | 1,61 | 0,61–4,22 | 0,330 |
| Duration of ICI treatment (≥8,0 versus <8,0 months) | 41,09 | 12,99–129,99 | 0,0001 | 6,61 | 3,07–14,22 | 0,0001 |
Table 5.
Immune-related adverse events in mNSCLC patients stratified by age.This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
Table 5.
Immune-related adverse events in mNSCLC patients stratified by age.This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
| irAE | <60 years old | 60–69 years old | ≥70 years old |
| Pruritus | 0 (0,0%) | 1 (2,0%) | 1 (6,7%) |
| Hypothyroidism | 0 (0,0%) | 1 (2,0%) | 0 (0,0%) |
| Hyperthyroidism | 2 (4,9%) | 2 (4,1%) | 2 (13,3%) |
| Hepatitis | 1 (2,4) | 1 (2,0%) | 0 (0,0%) |
| Pneumonitis | 0 (0,0%) | 1 (2,0%) | 1 (6,7%) |
| Nephritis | 0 (0,0%) | 1 (2,0%) | 1 (6,7%) |
| Colitis | 0 (0,0%) | 1 (2,0%) | 1 (6,7%) |
| Arthralgia | 0 (0,0%) | 1 (2,0%) | 0 (0,0%) |
| Myalgia | 0 (0,0%) | 0 (0,0%) | 1 (6,7%) |
| Bullous pemphigus | 1 (2,4%) | 0 (0,0%) | 0 (0,0%) |
| Onycholysis | 0 (0,0%) | 1 (2,0%) | 1 (6,7%) |
| Optic neuritis | 1 (2,4%) | 0 (0,%) | 0 (0,0%) |
| Rash | 1 (2,4%) | 0 (0,0%) | 0 (0,0%) |
| Aseptic bone necrosis | 1 (2,4%) | 0 (0,0%) | 0 (0,0%) |
| Infusion reaction | 0 (0,0%) | 1 (2,0%) | 1 (6,7%) |
| Total number of irAE of any grade of toxicity | 7 (17,1%) | 11 (22,4%) | 9 (60,0%) |
| Number of irAE ≥ grade 3 of toxicity | 5 (12,2%) | 3 (6,1%) | 1 (6,7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



