
Submitted:
19 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Background/Objectives: Clinical reasoning is an essential competency for all healthcare practitioners, particularly in the context of neurological rehabilitation, where patient management is complex and multifactorial. This paper proposes a unified framework for clinical reasoning in neurological physiotherapy, integrating the aspects of physical function with the World Health Organization’s International Classification of Functioning, Disability, and Health (ICF). Methods: The proposed framework incorporates a biopsychosocial approach, focusing on a patient-centred and goal-oriented methodology that allows for a comprehensive evaluation of the patient’s needs across multiple domains, including body functions, activities, and participation. By integrating clinical reasoning theories from various disciplines, this framework seeks to enhance the decision-making process and improve communication among healthcare professionals. Results: The model provides a systematic approach to assessing and addressing deficits in motor control, sensory functions, and other aspects of neurological rehabilitation. This work highlights the importance of interdisciplinary collaboration and emphasizes the role of physiotherapists in managing neurological impairments. Conclusions: The Biopsychosocial Reasoning Approach In Neurophysiotherapy (BRAIN) framework aims to improve functional outcomes by offering a more adaptable, multidisciplinary, and evidence-based approach to clinical reasoning in neurological physiotherapy.
Keywords:
clinical reasoning
; neurological rehabilitation
; physiotherapy
; ICF
; biopsychosocial model
; motor control
; BRAIN framework
1. Introduction
Clinical reasoning is often regarded as the backbone of clinical practice [1]. Several authors have described it as a multidimensional construct, emphasizing its complexity and integration of various domains [2]. It is considered one of the essential competencies for healthcare professionals and has been extensively studied by different healthcare professionals [2,3]. Its definition changes based on the discipline, being more focused on diagnosis when adopted by physicians or on the decision-making process when used by psychologists, physiotherapists or occupational therapists [4]. However, clinical reasoning can be defined as “the mental process that happens when a healthcare professional encounters a patient and is expected to draw a conclusion about (a) the nature and possible causes of complaints or abnormal conditions of the patient, (b) a likely diagnosis, and (c) patient management actions to be taken” [5].
The clinical reasoning process encompasses a variety of interacting factors, including the patient, the clinician, and the clinical environment. It can generally be categorized into two primary types: inductive (or forward) reasoning and deductive (or backwards) reasoning [6,7]. Inductive reasoning comprises two subsystems: the first relies on pattern recognition, predominantly driven by the clinician’s expertise and experiential knowledge; the second involves a slower, more effortful analytical thinking process [8]. These two systems lie on a cognitive continuum, ranging from immediate, intuitive recognition to deliberate and prolonged analytical reasoning [8,9]. Conversely, deductive clinical reasoning involves constructing a mental model, or a set of models, derived from general knowledge, established theoretical principles, and clinical guidelines. These models are used to generate hypotheses regarding the patient’s presentation and possible outcomes. Clinicians then systematically evaluate these hypotheses by collecting and analyzing evidence to confirm or refute them. When no disconfirming evidence is found during clinical assessment, the initial mental models are reinforced, thereby supporting valid clinical conclusions and facilitating sound clinical decision-making [10].
Clinical reasoning is an essential competency for physiotherapists. It must be an ongoing process that evolves along the continuum of the patient’s rehabilitation, carried out in a multidisciplinary manner, integrating cognitive, psychomotor and affective skills [4,11]. When focusing on neurologic physiotherapy, we can observe an evolution in the decision-making process, from initial theories that, from a neurophysiological point of view, aimed to achieve better rehabilitation outcomes based on personal experiences [12], to more scientific approaches within the biopsychosocial model [13,14].
However, these last clinical reasoning models are not fully explained and have not yet been applied in clinical settings, as they are not adapted to physiotherapy and most of them are derived from Neurodevelopmental Therapies (NDT) [15], which have failed to demonstrate their efficacy in improving functional outcomes in people with neurological deficits [16,17]. The primary aim of this study is to present an updated and operational model of clinical reasoning specific to neurological physiotherapy, which facilitates decision-making, improves interdisciplinary communication, and optimizes patients’ functional outcomes.
2. Foundations and Development of Clinical Reasoning Models in Physiotherapy
In 1970, Brunnstrom published her book “Movement Therapy in Hemiplegia: A Neurophysiological Approach”, basing her hypotheses on experiments carried out on animals at the beginning of the 20th century [18]. These studies provide the fundamental bases for recovery after brain damage, where authors such as Sherrington began to observe the phenotypes of spasticity based on the location and severity of the lesion [19,20,21].
The fundamental scientific principle behind Brunnstrom’s therapeutic approach is that the synergies observed in patients are essentially the same as the stereotypical reflexes found in healthy individuals [22]. However, due to the stroke, these reflexes are no longer regulated by higher centers, leading Brunnstrom to view the CNS as reverting to an earlier developmental stage [22]. Similar to Twitchell, Brunnstrom emphasizes spasticity as a key feature of the paresis phenotype, without differentiating between hypertonia and hyperreflexia at rest and the synergies observed during movement [22]. Based on this premise, she argues that spasticity must be resolved before normal movement can be restored; however, several authors have questioned this statement [22,23]. Different studies also suggest that physiotherapy has little to no effect on spasticity with various treatments or approaches; however, that is a debated topic with mixed evidence [24,25,26].
Aligned with this perspective, NDT emerged, with the Bobath concept being particularly prominent among them. This concept is currently defined as a problem-solving framework for assessing and treating individuals with impairments in function, movement, and muscle tone resulting from central nervous system lesions, utilizing key points of handling and reflex patterns to facilitate the performance of specific movements and exercises [27,28]. Since its inception, this approach has been characterized as complex, multidimensional, and response-based to the individual, focusing on “how” a task is completed avoiding compensatory movements [29].
Therefore, the clinical reasoning behind the Bobath concept is based on neurophysiological grounds that aim to achieve ‘normal movement’ in individuals with brain damage through the facilitation of movement to enhance motor learning [30]. Therefore, motor control is the main axis of the reasoning, understood as the continuous interaction between the individual, the task, and the environment, looking for movement through the motor, cognitive, and sensory systems, with special emphasis on the latter [31,32]. Its lack of reproducibility, due to the absence of a clearly defined framework, has supposed a significant barrier to its definition and research [15,30]. Moreover, recent evidence does not support its implementation in clinical settings due to its lack of effectiveness and because its theoretical foundations contradict the latest trends in motor learning and recovery for patients with neurological deficits [33]. Current approaches emphasize increasing the dose and intensity of treatments while allowing patients to experience some errors, thereby facilitating the acquisition of competencies needed to achieve greater functionality and independence [33,34,35,36].
In 2001, the International Classification of Functioning, Disability and Health (ICF) was approved by the World Health Organization, following a global collaboration that provided a comprehensive conceptualization of disability [37,38]. ICF was a step forward in decision-making based on the biopsychosocial model in physiotherapy [39,40]. The ICF model classifies disability based on health status, considered as the disease or disorders that affect the patient, body functions and body structures; which refers to the physiological functions of body systems (including psychological functions) for the first term and anatomical parts of the body such as organs, limbs and their components for the lasts, activity; ability to complete an action or a task and participation, which implies patient’s involvement in social situations [22,38] (Figure 1), emphasizing activity and participation as the core concepts of rehabilitation [41].
This tool has promoted the use of a common language among professionals in the field of neurological rehabilitation. In this area, collaborative work across disciplines (multidisciplinary, interdisciplinary, or transdisciplinary) is particularly important due to the complexity of the patients [13,33]. Thus, ICF was introduced as a significant element of clinical reasoning in neurological rehabilitation, thereby giving rise to the patient-centred approach [42].
To focus therapy on the patient, goal-oriented approaches have emerged. Goal planning is the collaborative process in which a healthcare professional and the service user define and commit to achieving a specific behavioral objective within a set timeframe [43]. This approach leads to SMART objectives, which consider that the goals set with patients must be “specific”, “measurable”, “achievable/attainable”, “realistic/relevant”, and “timed” [44]. To quantify these objectives and transfer this methodology to the research, the Goal Attainment Scale (GAS) was developed [45]. GAS establishes a 5-point Likert scale to assess the achievement of the proposed objectives with the patient, where 0 represents the expected outcome after intervention, +1 represents a +2 represents a much greater than expected outcome, -1 represents a less than expected outcome, and -2 represents a much less than expected outcome [46].
Furthermore, the American Physical Therapy Association (APTA) developed a physiotherapy practice guideline in 1995 [47], setting out the principles that must be integrated into a model of clinical reasoning specifically oriented to physiotherapy and physiotherapists [48]. The classical APTA clinical reasoning proposal encompasses patient management based on the following stages: examination, evaluation, diagnosis, prognosis, intervention, and outcomes (Figure 2) [49]. Within this model, the examination comprises the assessment of different spheres related to the patient’s disability in order to approach the multidimensional aspects of physical function mentioned by Kisner and Colby [50]: neuromuscular control/coordination; muscle performance; cardiopulmonary/endurance; mobility/flexibility; balance/postural equilibrium; stability, (Figure 3) [49].
3. Actual Framework for Clinical Reasoning in Physiotherapy
The clinical reasoning approach presented in this article aims to unify the classical model of clinical reasoning in physiotherapy promoted by the APTA [49] and WHO decision-making models driven by the ICF [38], adapting them to neurological physiotherapy by incorporating the interrelated aspects of function mentioned by Kisner and Colby [50]. To propose a useful clinical reasoning model applicable to this branch of physiotherapy, it is essential to incorporate the function model within the ICF, so that physiotherapy is included as one of the health professions involved in the multidisciplinary rehabilitation approach for neurological patients.
According to this paradigm, the interrelated aspects of function (Figure 3) should be assessed during the examination phase of the classical model and must be included in the ‘body function’ section of the ICF, which refers to deficits in the physiological functions of body systems. This implies modifying the ICF classical scheme, following its own separation of sections that is reflected within itself, and adapting it to our proposal, as shown in Figure 4.
It is essential to emphasize that the classical model refers to the “neuromusculoskeletal and movement-related functions.” Therefore, the remaining health professionals should assess the patient’s deficits in all other categories belonging to the body functions section (i.e., mental functions, voice and speech functions). Due to the competences of physiotherapists, it may be of interest to carry out an adaptation of the classical model proposed by Kisner and Colby, including sensory functions within it, and changing neuromuscular coordination to motor control what will be discussed below, thus obtaining the modified model of Kisner and Colby adapted to neurophysiotherapy reflected in Figure 5.
Considering this approach, the physiotherapist must conduct a neurological examination by assessing the proposed domains. Muscle performance, defined as the capacity of muscle to produce tension and do physical work, integrating strength, power, and muscular endurance [49,50], should be assessed through a muscle balance scale or by using a dynamometer [51,52]; cardiopulmonary/endurance, that refers to the process of oxygen intake, oxygen consumption and energy conversion [53], must be assessed with submaximal exercise test such as submaximal treadmill test or submaximal cycle ergometer test, obtaining a value of VO2max [54]; mobility/flexibility, that comprehends the ability of the patient to get full range of motion on his joints due to the influence of muscle, tendons and bones, and it’s measured with a goniometer or electro goniometer [55,56,57]. It is important to note that in neurological patients, hyperresistance would be included in mobility/flexibility, being essential to distinguish between the types of hyperresistance that may be present in the neurological patient, neural hyperresistance (spasticity or spastic dystonia [58]), and non-neural hyperresistance [59]. Furthermore, the presence of hyperresistance can have an impact on other body function domains such as strength or balance [60,61]. Balance, known as the ability, to distribute the body mass during functions [62], must be assessed by an optimal posturography [63]; stability, defined as the state of a joint remaining or promptly returning to proper alignment through an equalization of forces [64], could be assessed through different orthopedic tests [65,66]. Sensory functions are related to the functions of the senses, which, in physiotherapy, would be related to proprioceptive function, touch function, and pain sensation [38]. According to our approach, proprioceptive function could be measured through the Fugl-Meyer Assessment proprioception subscale, which involves a leg/arm movement mirror-matching test [67,68], while touch function must be measured with Semmes-Weinstein monofilaments to assess the mechanical detection threshold [69]. Sensory components of pain, on the other hand, could be assessed through pain detection threshold, that can include both thermal and mechanical thresholds, as well as the intensity of pain, which can be measured using a visual analogue scale [70,71]. However, if pain is the main problem or limits a patient’s participation, it must be continually assessed through an anamnesis of the pain, a classification of the pathophysiological mechanisms of pain, and an evaluation of the contributing factors from a biopsychosocial perspective [72].
Finally, before discussing neuromuscular control/coordination, it is important to note that Kisner and Colby define it as “the interaction of the sensory and motor systems that enables synergists, agonists and antagonists, as well as stabilizers and neutralizers to anticipate or respond to proprioceptive and kinesthetic information and, subsequently, to work in the correct sequence to create coordinated movement” [50,73]. Neuromuscular control/coordination is also referred to by different terms in the literature, particularly in neurology-related articles, which often use the term “motor control” [74]. Other definitions of motor control describe it as “how the nervous system interacts with other body parts and the environment to produce purposeful, coordinated actions” [75]. This perspective emphasizes that, following the ideation of an action, the final movement results from a decision-making process involving sensorimotor and cognitive areas, which is in line with the earlier statement about neuromuscular control/coordination [76]. However, according to that definition, motor control should be allocated in the “activity” section of the ICF.
To establish a more specific clinical reasoning for patients with neurological impairment, the term ‘motor control’ should be included in the section “body functions” and should be defined as “the ability to move a single joint isolated”. This definition aligns with the pathological sign that occurs due to brain damage and suggests that individuals with central nervous system disorders often move with synergies [77,78]. The term “synergy” refers to either systematic coupling/coarticulation across different joints or to a fixed pattern of coactivation of muscles related to the time domain of the activity due to an injury in the corticospinal tract and a possible hyperexcitability of the reticulospinal tract, and an activation of the non-damaged corticospinal tract [79,80,81]. Therefore, considering this definition, motor control could be assessed using the Fugl-Meyer scale, although kinematics and muscle activations could also be used for testing it [22,82,83].
On the other hand, physiotherapy should specifically assess the domain d4 mobility of ICF. Other domains must be evaluated in different areas, such as neuropsychology, occupational therapy, and speech therapy, working together with a transdisciplinary, multidisciplinary, or interdisciplinary methodology to have a significant impact on patients’ lives. People with neurological deficits represent a highly heterogeneous group, making the assessment of their functional capacity crucial for classifying their ability to perform various activities [84,85,86,87]. Functional Ambulation Category (FAC), enables clinicians to classify patients in six different categories based on how they are able to walk; 0, nonfunctional ambulator, the patient is not able to walk at all or needs the help of two therapists; 1, ambulator dependent on physical assistance (level II), the patient requires continuous manual contact to support body weight as well as to maintain balance or to assist coordination; 2, ambulator dependent on physical assistance (level I), the patient requires intermittent or continuous light touch to assist balance or coordination; 3, ambulator, dependent on supervision, the patient can ambulate on lever surface without manual contact of another person but requires standby guarding of one person either for safety or for verbal cueing; 4, ambulator, independent, lever surface only, the patient can ambulate independently on lever surface but requires supervision to negotiate (e.g. stairs, inclines, nonlevel surfaces); 5, ambulator, independent, the patient can walk everywhere independently, including stairs [88,89]. Thus, the selection of tests to assess the patient’s activity depends on the patient’s functional capacity and must be conducted according to the recommendations made by the APTA and the Academy of Neurologic Physical Therapy [90] as reflected in Figure 6. Following this guideline recommendations, activities assessed by the physiotherapist are: balance during functional activities (Berg Balance Scale) [91,92,93,94]; walking balance (Functional Gait Assessment) [93,95]; balance confidence (Activities-specific Balance Confidence Scale) [96,97,98]; walking speed (10 Meter Walk Test) [99]; walking distance (6 Minutes Walking Test) [100,101,102]; and transfers (5 Times Sit-to-Stand) [103].
It’s important to note that this classification system is considered for lower limb activities, so other assessments must be applied to evaluate upper limb activity. Instruments like the Action Research Arm Test [104,105], the Box and Block Test [106,107] or the Nine-Hole Peg Test [108,109,110], are indicated for assessing upper limb activity in patients with neurologic deficits, as long as their functional capabilities allow for the administration of the test.
Finally, participation is usually assessed through questionnaires like Stroke Impact Scale [111] or Canadian Occupational Performance Measure [112], but other scales can be used for assessing the perceived participation of the patient in different activities of daily living such as the Motor Activity Log by its Amount of Use subscale, both in its upper and lower limb versions [113].
Making this decision-making process evaluation provides the physical therapist with a clear picture of the patient’s deficits. However, neurologic patients’ management is complex, and it’s nearly impossible to approach all these deficits at the same time without losing the effectiveness of the treatment. That’s the reason why this framework makes much more sense within the biopsychosocial paradigm and goal-oriented approach. Therefore, the decision-making process must initially be based on an analysis of the patient’s deficits in body functions, activities and participation in a general context, to subsequently select the body functions that prevent the patient from achieving their goal based on their impairments in activities. This requires adapting the classical APTA model to suit the specific needs of physiotherapists treating patients with neurological impairments.
Thus, carrying out the first clinical reasoning, potential deficits could be identified that need to be addressed at an early stage, even if they do not interfere with the objective, in order to reduce secondary complications that may arise. However, if these deficits do not imply a long-term issue, the physiotherapist should focus on addressing the problems that prevent the patient from achieving their goals to improve their participation and quality of life [43].
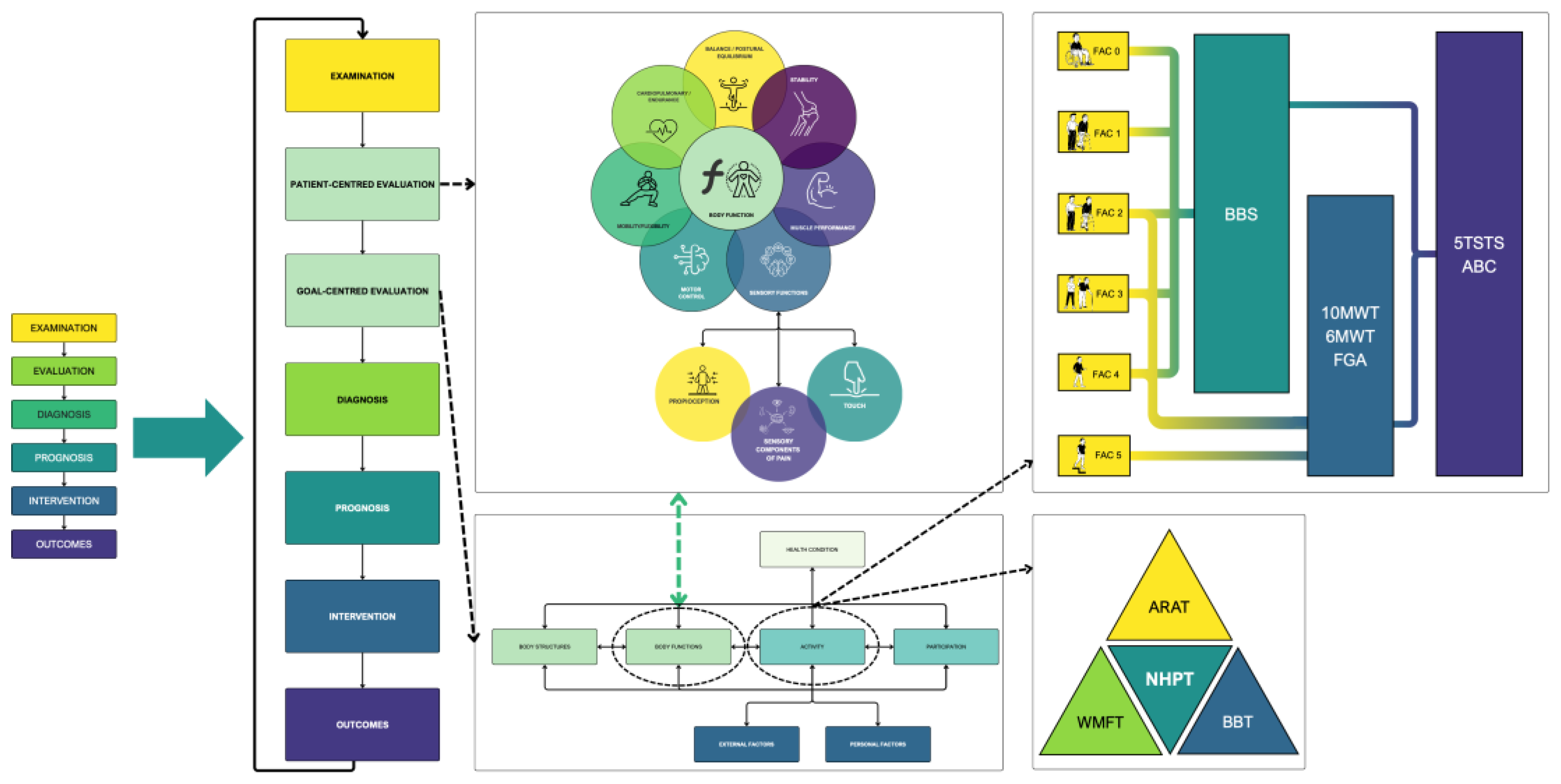
The Biopsychosocial Reasoning Approach In Neurophysiotherapy (BRAIN) framework provides a structured, multidimensional model for clinical reasoning in neurophysiotherapy. Grounded in the biopsychosocial paradigm, this approach integrates the ICF, a modified clinical decision-making process proposed by the APTA, and the interrelated physical function domains described by Kisner and Colby, adapted for neurophysiotherapy. Its goal-oriented structure enhances patient-centred care, supporting physiotherapists in making consistent, evidence-based decisions throughout the neurological rehabilitation process, as is reflected in Figure 7.
While other concepts have attempted to incorporate similar frameworks that are related to the biopsychosocial model [114], the lack of effectiveness of this paradigm involves a gap in the literature that needs to be filled to improve the effectiveness of physiotherapy treatments in care facilities.
4. Limitations
Although the proposed framework offers a comprehensive approach to clinical reasoning in neurological physiotherapy, several limitations must be considered. Firstly, the integration of the Kisner and Colby aspects of physical function and the ICF framework may require significant adaptation for use in diverse clinical settings, particularly in regions with varying healthcare infrastructures or limited access to resources. The application of the framework could be challenging in settings where multidisciplinary collaboration is less established, and physiotherapists may have limited interaction with other healthcare professionals, despite it being mandatory to include this type of approach in neurological patient management.
Additionally, it is important to note that the proposed model is theoretical and conceptual in nature. Although it is based on a comprehensive review of the scientific literature and previously validated frameworks such as the ICF, the classical APTA model and the interrelated aspects of physical function according to Kisner and Colby, it has not yet undergone a systematic process of empirical validation. Therefore, although it offers a coherent structure aligned with current trends in neurological rehabilitation, its practical applicability may vary depending on the clinical context and the degree of training of the professionals.
Likewise, it is recognized that studies are needed to validate and refine this model. In this sense, future research could include the application of consensus methods such as the Delphi technique with experts in neurological physical therapy, as well as pilot studies of progressive implementation in real clinical settings. These strategies would not only make it possible to assess the feasibility and acceptance of the model in clinical practice, but also to optimize its structure and operationalization according to the needs detected in interdisciplinary work.
Further empirical studies and clinical trials are needed to validate the framework’s effectiveness and its potential impact on neurological rehabilitation outcomes across different patient populations and healthcare settings.
On the other hand, all figures included in this manuscript have been designed using the viridis color palette, a perceptually uniform scale that optimizes visual accessibility. This palette has several advantages over other traditional scales, as it maintains a progressive luminance and is suitable for people with color vision deficiencies, including color blindness [109]. Its use has been recommended in scientific visualization to enhance interpretive clarity, particularly in academic or clinical contexts where visual accuracy is crucial.
5. Conclusions
In conclusion, this work presents a comprehensive framework for clinical reasoning in neurological physiotherapy, integrating the Kisner and Colby interrelated aspects of physical function within the classical APTA proposal and the ICF framework to create a more adaptable and patient-centred approach. By emphasizing the biopsychosocial model and goal-oriented strategies, the BRAIN framework enables physiotherapists to address the unique challenges of managing neurological patients, with a focus on enhancing patient participation and quality of life. This unified model encourages effective interdisciplinary collaboration and offers a clear pathway for improving rehabilitation outcomes, thereby addressing an existing gap in current clinical practice.
Supplementary Materials
Not applicable.
Author Contributions
Conceptualization, A.L.-C.; methodology, A.L.-C., R.F.-P. and S.L.-L.; writing—original draft preparation, A.L.-C.; writing—review and editing, R.F.-P. and S.L.-L.; visualization, A.L.-C.; supervision, R.F.-P. and S.L.-L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| APTA | American Physical Therapy Association |
| ARAT | Action Research Arm Test |
| ABC | Activities-specific Balance Confidence Scale |
| BRAIN | Biopsychosocial Reasoning Approach In Neurophysiotherapy |
| CNS | Central Nervous System |
| ESO | European Stroke Organization |
| FAC | Functional Ambulation Category |
| GAS | Goal Attainment Scale |
| ICF | International Classification of Functioning, Disability and Health |
| MAL | Motor Activity Log |
| NDT | Neurodevelopmental Therapies |
| QST | Quantitative Sensory Testing |
| SMART | Specific, Measurable, Achievable/Attainable, Realistic/Relevant, Timed |
| VO₂max | Maximum Oxygen Consumption |
| WHO | World Health Organisation |
References
- Mattingly, C. What is Clinical Reasoning? The American Journal of Occupational Therapy 1991, 45, 979–986. [Google Scholar] [CrossRef]
- Pelaccia, T; Tardif, J; Triby, E; Charlin, B. An analysis of clinical reasoning through a recent and comprehensive approach: the dual-process theory. Medical Education Online 2011, 16, 5890. [Google Scholar] [CrossRef]
- Charlin, B; Tardif, J; Boshuizen, HPA. Scripts and Medical Diagnostic Knowledge: Theory and Applications for Clinical Reasoning Instruction and Research. Academic Medicine 2000, 75, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Huhn, K; Gilliland, SJ; Black, LL; Wainwright, SF; Christensen, N. Clinical Reasoning in Physical Therapy: A Concept Analysis. Physical Therapy 2019, 99, 440–456. [Google Scholar] [CrossRef]
- Bowen JL, Ten Cate O. Prerequisites for Learning Clinical Reasoning. En: Ten Cate O, Custers EJFM, Durning SJ, editores. Principles and Practice of Case-based Clinical Reasoning Education [Internet]. Cham: Springer International Publishing; 2018 [citado 5 de enero de 2025]. p. 47-63. (Innovation and Change in Professional Education; vol. 15). Available online: http://link.springer.com/10.1007/978-3-319-64828-6_4.
- Durning, SJ; Artino, AR; Schuwirth, L; Van Der Vleuten, C. Clarifying Assumptions to Enhance Our Understanding and Assessment of Clinical Reasoning: Academic Medicine 2013, 88, 442–448. [PubMed]
- Fischer, R. Public Relations Problem Solving: Heuristics and Expertise. Journal of Public Relations Research 1998, 10, 137–153. [Google Scholar] [CrossRef]
- Custers, EJFM. Medical Education and Cognitive Continuum Theory: An Alternative Perspective on Medical Problem Solving and Clinical Reasoning. Academic Medicine 2013, 88, 1074–1080. [Google Scholar] [CrossRef]
- Kassirer, JP. Teaching Clinical Reasoning: Case-Based and Coached: Academic Medicine 2010, 85, 1118–1124.
- Shin, HS. Reasoning processes in clinical reasoning: from the perspective of cognitive psychology. Korean J Med Educ. 2019, 31, 299–308. [Google Scholar] [CrossRef]
- Ajjawi, R; Higgs, J. Core components of communication of clinical reasoning: a qualitative study with experienced Australian physiotherapists. Adv in Health Sci Educ. 2012, 17, 107–119. [Google Scholar] [CrossRef]
- Partridge, C; Edwards, S. The bases of practice--neurological physiotherapy. Physiother Res Int. 1996, 1, 205–208. [Google Scholar] [CrossRef]
- Lexell, J; Brogårdh, C. The use of ICF in the neurorehabilitation process; Brogårdh, C, Lexell, J, Eds.; NRE, 2015; Volume 36, pp. 5–9. [Google Scholar]
- Sahrmann, SA. The Human Movement System: Our Professional Identity. Physical Therapy 2014, 94, 1034–1042. [Google Scholar] [CrossRef]
- Vaughan-Graham, J; Patterson, K; Zabjek, K; Cott, CA. Conceptualizing movement by expert Bobath instructors in neurological rehabilitation. Evaluation Clinical Practice 2017, 23, 1153–1163. [Google Scholar] [CrossRef] [PubMed]
- Dorsch, S; Carling, C; Cao, Z; Fanayan, E; Graham, PL; McCluskey, A; et al. Bobath therapy is inferior to task-specific training and not superior to other interventions in improving arm activity and arm strength outcomes after stroke: a systematic review. J Physiother. 2023, 69, 15–22. [Google Scholar] [CrossRef]
- Scrivener, K; Dorsch, S; McCluskey, A; Schurr, K; Graham, PL; Cao, Z; et al. Bobath therapy is inferior to task-specific training and not superior to other interventions in improving lower limb activities after stroke: a systematic review. J Physiother. 2020, 66, 225–235. [Google Scholar] [CrossRef]
- Brunnstrom, S. Movement Therapy in Hemiplegia: A Neurophysiological Approach, 1.a ed; 1970; 200p. [Google Scholar]
- Sherrington, CS. Decerebrate Rigidity, and Reflex Coordination of Movements. The Journal of Physiology 1898, 22, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Walshe, FMR. On the Genesis and Physiological Significance of Spasticity and Other Disorders of Motor Innervation: With a Consideration of the Functional Relationships of the Pyramidal System. Brain 1919, 42, 1–28. [Google Scholar] [CrossRef]
- Walshe, FMR. On the Role of the Pyramidal System in Willed Movements. Brain 1947, 70, 329–354. [Google Scholar] [CrossRef]
- Krakauer, JW; Carmichael, ST. Broken Movement: The Neurobiology of Motor Recovery after Stroke; The MIT Press, 2017; p. 30. [Google Scholar]
- Nair, KPS; Marsden, J. The management of spasticity in adults. BMJ 2014, 349, g4737–g4737. [Google Scholar] [CrossRef] [PubMed]
- Etoom, M; Khraiwesh, Y; Lena, F; Hawamdeh, M; Hawamdeh, Z; Centonze, D; et al. Effectiveness of Physiotherapy Interventions on Spasticity in People With Multiple Sclerosis: A Systematic Review and Meta-Analysis. Am J Phys Med Rehabil 2018, 97, 793–807. [Google Scholar] [CrossRef]
- Brusola, G; Garcia, E; Albosta, M; Daly, A; Kafes, K; Furtado, M. Effectiveness of physical therapy interventions on post-stroke spasticity: An umbrella review. NRE 2023, 52, 349–363. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, PHFDA; Glinsky, JV; Fachin-Martins, E; Harvey, LA. Physiotherapy interventions for the treatment of spasticity in people with spinal cord injury: a systematic review. Spinal Cord. 2021, 59, 236–247. [Google Scholar] [CrossRef] [PubMed]
- Bobath, B. Adult Hemiplegia Evaluation and Treatment, 3.a ed.; Butterworth-Heinemann, 1990. [Google Scholar]
- Raine, S. Defining the Bobath concept using the Delphi technique. Physiother Res Int. 2006, 11, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Cott, CA; Graham, JV; Brunton, K. When will the evidence catch up with clinical practice? Physiotherapy Canada 2011, 63, 387–390. [Google Scholar] [CrossRef]
- Vaughan-Graham, J; Cott, C; Wright, FV. The Bobath (NDT) concept in adult neurological rehabilitation: what is the state of the knowledge? A scoping review. Part I: conceptual perspectives. Disability and Rehabilitation 2015, 37, 1793–1807. [Google Scholar] [CrossRef]
- Shumway-Cook, A; Woollacott, MH. Motor Control. Translating Research into Clinical Practice; Wolters Kluwer: Philadelphia, 2013; Vol. 53, pp. 1689–1699. [Google Scholar]
- Vahdat, S; Darainy, M; Ostry, DJ. Structure of Plasticity in Human Sensory and Motor Networks Due to Perceptual Learning. J Neurosci. 2014, 34, 2451–2463. [Google Scholar] [CrossRef]
- Intercollegiate Stroke Working Party. National Clinical Guideline for Stroke for the UK and Ireland [Internet]. 2023 may. Available online: www.strokeguideline.org.
- Guadagnoli, MA; Lee, TD. Challenge Point: A Framework for Conceptualizing the Effects of Various Practice Conditions in Motor Learning. Journal of Motor Behavior 2004, 36, 212–224. [Google Scholar] [CrossRef]
- Hayward, KS; Kramer, SF; Dalton, EJ; Hughes, GR; Brodtmann, A; Churilov, L; et al. Timing and Dose of Upper Limb Motor Intervention After Stroke: A Systematic Review. Stroke 2021, 52, 3706–3717. [Google Scholar] [CrossRef]
- Kwakkel, G; Stinear, C; Essers, B; Munoz-Novoa, M; Branscheidt, M; Cabanas-Valdés, R; et al. Motor rehabilitation after stroke: European Stroke Organisation (ESO) consensus-based definition and guiding framework. European Stroke Journal 2023, 8, 880–894. [Google Scholar] [CrossRef]
- Bickenbach, JE; Chatterji, S; Badley, EM; Üstün, TB. Models of disablement, universalism and the international classification of impairments, disabilities and handicaps. Social Science & Medicine 1999, 48, 1173–1187. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability and Health (ICF). WHO [Internet]. 2001 [citado 22 de septiembre de 2020]. Available online: http://www.who.int/classifications/icf/en/.
- Maart S, Sykes C. Expanding on the use of The International Classification of Functioning, Disability and Health: Examples and resources. S Afr j physiother [Internet]. 17 de agosto de 2022 [citado 8 de enero de 2025];78(1). Available online: https://sajp.co.za/index.php/sajp/article/view/1614.
- Vargus-Adams, JN; Majnemer, A. International Classification of Functioning, Disability and Health (ICF) as a Framework for Change: Revolutionizing Rehabilitation. J Child Neurol. 2014, 29, 1030–1035. [Google Scholar] [CrossRef]
- Campos, TF; De Melo, LP; Dantas, AATSG; De Oliveira, DC; Oliveira, RANDS; Cordovil, R; et al. Functional activities habits in chronic stroke patients: A perspective based on ICF framework. NRE 2019, 45, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Alford, VM; Ewen, S; Webb, GR; McGinley, J; Brookes, A; Remedios, LJ. The use of the International Classification of Functioning, Disability and Health to understand the health and functioning experiences of people with chronic conditions from the person perspective: a systematic review. Disability and Rehabilitation 2015, 37, 655–666. [Google Scholar] [CrossRef] [PubMed]
- Rosewilliam, S; Roskell, CA; Pandyan, A. A systematic review and synthesis of the quantitative and qualitative evidence behind patient-centred goal setting in stroke rehabilitation. Clin Rehabil 2011, 25, 501–514. [Google Scholar]
- Bovend’Eerdt, TJ; Botell, RE; Wade, DT. Writing SMART rehabilitation goals and achieving goal attainment scaling: a practical guide. Clin Rehabil 2009, 23, 352–361. [Google Scholar]
- Bard-Pondarré, R; Villepinte, C; Roumenoff, F; Lebrault, H; Bonnyaud, C; Pradeau, C; et al. Goal Attainment Scaling in rehabilitation: An educational review providing a comprehensive didactical tool box for implementing Goal Attainment Scaling. J Rehabil Med. 2023, 55, jrm6498. [Google Scholar]
- Malec, JF. Goal Attainment Scaling in Rehabilitation. Neuropsychological Rehabilitation 1999, 9, 253–75. [Google Scholar] [CrossRef]
- American Physical Therapy Association. A Guide to Physical Therapist Practice, Volume I: A Description of Patient Management. Physical Therapy 1995, 75, 707–764. [Google Scholar] [CrossRef]
- American Physical Therapy Association. Guide to Physical Therapist Practice. Second Edition. American Physical Therapy Association. Phys Ther. 2001, 81, 9–746. [Google Scholar]
- American Physical Therapy Association. APTA guide to physical Therapist Practice 4.0. 2023. [Google Scholar]
- Kisner, C; Colby, LA. Therapeutic exercise: foundations and techniques, 5th ed.; F.A. Davis: Philadelphia, 2007; 928p. [Google Scholar]
- Bertrand, AM; Mercier, C; Bourbonnais, D; Desrosiers, J; Gravel, D. Reliability of maximal static strength measurements of the arms in subjects with hemiparesis. Clin Rehabil 2007, 21, 248–257. [Google Scholar] [CrossRef]
- Aguiar, LT; Martins, JC; Quintino, LF; De Brito, SAF; Teixeira-Salmela, LF; De Morais Faria, CDC. A Single Trial May Be Used for Measuring Muscle Strength With Dynamometers in Individuals With Stroke: A Cross-Sectional Study. PM&R 2019, 11, 372–378. [Google Scholar]
- Kispert, CP. Clinical Measurements to Assess Cardiopulmonary Function. Physical Therapy 1987, 67, 1886–1890. [Google Scholar] [CrossRef]
- Eng, JJ; Dawson, AS; Chu, KS. Submaximal exercise in persons with stroke: test-retest reliability and concurrent validity with maximal oxygen consumption. Arch Phys Med Rehabil 2004, 85, 113–118. [Google Scholar] [CrossRef]
- Bashardoust Tajali, S; MacDermid, JC; Grewal, R; Young, C. Reliability and Validity of Electro-Goniometric Range of Motion Measurements in Patients with Hand and Wrist Limitations. Open Orthop J. 2016, 10, 190–205. [Google Scholar] [CrossRef]
- Jung, IG; Yu, IY; Kim, SY; Lee, DK; Oh, JS. Reliability of ankle dorsiflexion passive range of motion measurements obtained using a hand-held goniometer and Biodex dynamometer in stroke patients. J Phys Ther Sci. 2015, 27, 1899–1901. [Google Scholar] [CrossRef]
- Micheo, W; Baerga, L; Miranda, G. Basic Principles Regarding Strength, Flexibility, and Stability Exercises. PM&R 2012, 4, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Puce, L; Currà, A; Marinelli, L; Mori, L; Capello, E; Di Giovanni, R; et al. Spasticity, spastic dystonia, and static stretch reflex in hypertonic muscles of patients with multiple sclerosis. Clinical Neurophysiology Practice 2021, 6. [Google Scholar] [CrossRef]
- van den Noort, JC; Bar-On, L; Aertbeliën, E; Bonikowski, M; Braendvik, SM; Broström, EW; et al. European consensus on the concepts and measurement of the pathophysiological neuromuscular responses to passive muscle stretch. European Journal of Neurology 2017, 24, 981–e38. [Google Scholar] [CrossRef] [PubMed]
- Abdollahi, I; Taghizadeh, A; Shakeri, H; Eivazi, M; Jaberzadeh, S. The relationship between isokinetic muscle strength and spasticity in the lower limbs of stroke patients. Journal of Bodywork and Movement Therapies 2015, 19, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Rahimzadeh Khiabani, R; Mochizuki, G; Ismail, F; Boulias, C; Phadke, CP; Gage, WH. Impact of Spasticity on Balance Control during Quiet Standing in Persons after Stroke. Stroke Research and Treatment 2017, 2017, 1–10. [Google Scholar] [CrossRef]
- Pollock, AS; Durward, BR; Rowe, PJ; Paul, JP. What is balance? Clin Rehabil 2000, 14, 402–406. [Google Scholar] [CrossRef]
- Pérennou, D; Chauvin, A; Piscicelli, C; Hugues, A; Dai, S; Christiaens, A; et al. Determining an optimal posturography dataset to identify standing behaviors in the post-stroke subacute phase. Cross-sectional study. Annals of Physical and Rehabilitation Medicine 2023, 66, 101707. [Google Scholar] [CrossRef]
- Riemann, BL; Lephart, SM. The sensorimotor system, part I: the physiologic basis of functional joint stability. J Athl Train. 2002, 37, 71–79. [Google Scholar] [PubMed]
- Pickering, GT; Fine, NF; Knapper, TD; Giddins, GEB. The reliability of clinical assessment of distal radioulnar joint instability. J Hand Surg Eur 2022, 47, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Beynon, A; Le May, S; Theroux, J. Reliability and validity of physical examination tests for the assessment of ankle instability. Chiropr Man Therap 2022, 30, 58. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, AM; Bourbonnais, D; Mercier, C. Differences in the magnitude and direction of forces during a submaximal matching task in hemiparetic subjects. Experimental Brain Research 2004, 157, 32–42. [Google Scholar] [CrossRef]
- Dukelow, SP; Herter, TM; Bagg, SD; Scott, SH. The independence of deficits in position sense and visually guided reaching following stroke. J NeuroEngineering Rehabil. 2012, 9, 72. [Google Scholar] [CrossRef]
- Suda, M; Kawakami, M; Okuyama, K; Ishii, R; Oshima, O; Hijikata, N; et al. Validity and Reliability of the Semmes-Weinstein Monofilament Test and the Thumb Localizing Test in Patients With Stroke. Frontiers in Neurology 2021, 11. [Google Scholar] [CrossRef]
- Heller, GZ; Manuguerra, M; Chow, R. How to analyze the Visual Analogue Scale: Myths, truths and clinical relevance. Scandinavian Journal of Pain 2016, 13, 67–75. [Google Scholar] [CrossRef]
- Mücke, M; Cuhls, H; Radbruch, L; Baron, R; Maier, C; Tölle, T; et al. Quantitative sensory testing (QST). Schmerz 2021, 35, 153–60. [Google Scholar] [CrossRef]
- Bäckryd, E. Pain assessment 3 × 3: a clinical reasoning framework for healthcare professionals. Scandinavian Journal of Pain 2023, 23, 268–272. [Google Scholar] [CrossRef]
- Lephart, S; Swanik, CB; Fu, F. Reestablishing Neuromuscular Control. En: Prentice WE, 5th, editores. Rehabilitation Techniques for Sports Medicine and Athletic Training; McGraw-Hill: New York, 2011; pp. 122–143. [Google Scholar]
- Abbas J. Neuromuscular Control Systems, Models of neuromotor control. En: Jaeger D, Jung R, editores. Encyclopedia of Computational Neuroscience [Internet]. New York, NY: Springer New York; 2014 [citado 30 de abril de 2025]. p. 1-9. Available online: https://link.springer.com/10.1007/978-1-4614-7320-6_711-1.
- Danion, F.; Latash, M.L. (Eds.) Motor control: theories, experiments, and applications; Oxford University Press: New York, 2011; 511p. [Google Scholar]
- Kandel, E.R.; Koester, J.; Mack, S.; Siegelbaum, S. (Eds.) Principles of neural science, Sixth edition; McGraw Hill: New York, 2021; 1646p. [Google Scholar]
- McMorland AJC, Runnalls KD, Byblow WD. A Neuroanatomical Framework for Upper Limb Synergies after Stroke. Front Hum Neurosci [Internet]. 16 de febrero de 2015 [citado 22 de enero de 2025];9. Available online: http://journal.frontiersin.org/Article/10.3389/fnhum.2015.00082/abstract. [CrossRef]
- Israely, S; Leisman, G; Carmeli, E. Neuromuscular synergies in motor control in normal and poststroke individuals. Reviews in the Neurosciences 2018, 29, 593–612. [Google Scholar] [CrossRef]
- Zaaimi, B; Edgley, SA; Soteropoulos, DS; Baker, SN. Changes in descending motor pathway connectivity after corticospinal tract lesion in macaque monkey. Brain 2012, 135, 2277–2289. [Google Scholar] [CrossRef]
- McPherson, JG; Chen, A; Ellis, MD; Yao, J; Heckman, CJ; Dewald, JPA. Progressive recruitment of contralesional cortico-reticulospinal pathways drives motor impairment post stroke. The Journal of Physiology 2018, 596, 1211–1225. [Google Scholar] [CrossRef] [PubMed]
- Schwerin, S; Dewald, JPA; Haztl, M; Jovanovich, S; Nickeas, M; MacKinnon, C. Ipsilateral versus contralateral cortical motor projections to a shoulder adductor in chronic hemiparetic stroke: implications for the expression of arm synergies. Exp Brain Res. 2008, 185, 509–519. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A; Jääskö, L; Leyman, I; Olsson, S; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance - PubMed. Scand J Rehabil Med 1975, 7, 13–31. [Google Scholar] [CrossRef]
- Madroñero-Miguel, B; Cuesta-García, C. Spanish consensus of occupational therapists on upper limb assessment tools in stroke. British Journal of Occupational Therapy 2023, 86, 648–658. [Google Scholar] [CrossRef] [PubMed]
- Gupta, S; Jaiswal, A; Norman, K; DePaul, V. Heterogeneity and Its Impact on Rehabilitation Outcomes and Interventions for Community Reintegration in People With Spinal Cord Injuries: An Integrative Review. Topics in Spinal Cord Injury Rehabilitation 2019, 25, 164–185. [Google Scholar] [CrossRef]
- Greenland, JC; Williams-Gray, CH; Barker, RA. The clinical heterogeneity of Parkinson’s disease and its therapeutic implications. Eur J of Neuroscience 2019, 49, 328–338. [Google Scholar] [CrossRef]
- Han, E; Kim, TH; Koo, H; Yoo, J; Heo, JH; Nam, HS. Heterogeneity in costs and prognosis for acute ischemic stroke treatment by comorbidities. J Neurol. 2019, 266, 1429–1438. [Google Scholar] [CrossRef] [PubMed]
- Muir, KW. Heterogeneity of Stroke Pathophysiology and Neuroprotective Clinical Trial Design. Stroke 2002, 33, 1545–1550. [Google Scholar] [CrossRef]
- Mehrholz, J; Wagner, K; Rutte, K; Meiβner, D; Pohl, M. Predictive Validity and Responsiveness of the Functional Ambulation Category in Hemiparetic Patients After Stroke. Archives of Physical Medicine and Rehabilitation 2007, 88, 1314–1319. [Google Scholar] [CrossRef]
- Holden, MK; Gill, KM; Magliozzi, MR. Gait Assessment for Neurologically Impaired Patients. Physical Therapy 1986, 66, 1530–1539. [Google Scholar] [CrossRef] [PubMed]
- Moore, JL; Potter, K; Blankshain, K; Kaplan, SL; O’Dwyer, LC; Sullivan, JE. A Core Set of Outcome Measures for Adults With Neurologic Conditions Undergoing Rehabilitation: A CLINICAL PRACTICE GUIDELINE. Journal of Neurologic Physical Therapy 2018, 42, 174–220. [Google Scholar] [CrossRef]
- Gustavsen, M; Aamodt, G; Marit Mengshoel, A. Measuring balance in sub-acute stroke rehabilitation. Advances in Physiotherapy 2006, 8, 15–22. [Google Scholar] [CrossRef]
- Lemay, JF; Nadeau, S. Standing balance assessment in ASIA D paraplegic and tetraplegic participants: Concurrent validity of the Berg Balance Scale. Spinal Cord. 2010, 48, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Leddy, AL; Crowner, BE; Earhart, GM. Functional Gait Assessment and Balance Evaluation System Test: Reliability, Validity, Sensitivity, and Specificity for Identifying Individuals With Parkinson Disease Who Fall. Physical Therapy 2011, 91, 102–113. [Google Scholar] [CrossRef]
- Paltamaa, J; Sarasoja, T; Leskinen, E; Wikström, J; Mälkiä, E. Measuring Deterioration in International Classification of Functioning Domains of People With Multiple Sclerosis Who Are Ambulatory. Physical Therapy 2008, 88, 176–190. [Google Scholar] [CrossRef]
- Lin, JH; Hsu, MJ; Hsu, HW; Wu, HC; Hsieh, CL. Psychometric Comparisons of 3 Functional Ambulation Measures for Patients With Stroke. Stroke 2010, 41, 2021–2025. [Google Scholar] [CrossRef]
- Alghwiri, AA; Khalil, H; Al-Sharman, A; El-Salem, K. Psychometric properties of the Arabic Activities-specific Balance Confidence scale in people with multiple sclerosis: Reliability, validity, and minimal detectable change. NRE 2020, 46, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Ishige, S; Wakui, S; Miyazawa, Y; Naito, H. Reliability and validity of the Activities-specific Balance Confidence scale-Japanese (ABC-J) in community-dwelling stroke survivors. Phys Ther Res. 2020, 23, 15–22. [Google Scholar] [CrossRef]
- Shah, G; Oates, AR; Arora, T; Lanovaz, JL; Musselman, KE. Measuring balance confidence after spinal cord injury: the reliability and validity of the Activities-specific Balance Confidence Scale. The Journal of Spinal Cord Medicine 2017, 40, 768–776. [Google Scholar] [CrossRef] [PubMed]
- Rossier, P; Wade, DT. Validity and reliability comparison of 4 mobility measures in patients presenting with neurologic impairment. Archives of Physical Medicine and Rehabilitation 2001, 82, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Perera, S; Mody, SH; Woodman, RC; Studenski, SA. Meaningful Change and Responsiveness in Common Physical Performance Measures in Older Adults. J American Geriatrics Society 2006, 54, 743–749. [Google Scholar]
- Scivoletto, G; Tamburella, F; Laurenza, L; Foti, C; Ditunno, JF; Molinari, M. Validity and reliability of the 10-m walk test and the 6-min walk test in spinal cord injury patients. Spinal Cord 2011, 49, 736–740. [Google Scholar] [CrossRef]
- Learmonth, YC; Dlugonski, DD; Pilutti, LA; Sandroff, BM; Motl, RW. The reliability, precision and clinically meaningful change of walking assessments in multiple sclerosis. Mult Scler 2013, 19, 1784–1791. [Google Scholar] [CrossRef]
- Paul, SS; Canning, CG; Sherrington, C; Fung, VSC. Reproducibility of measures of leg muscle power, leg muscle strength, postural sway and mobility in people with Parkinson’s disease. Gait & Posture 2012, 36, 639–642. [Google Scholar]
- Fernández-Solana, J; Pardo-Hernández, R; González-Bernal, JJ; Sánchez-González, E; González-Santos, J; Soto-Cámara, R; et al. Psychometric Properties of the Action Research Arm Test (ARAT) Scale in Post-Stroke Patients—Spanish Population. IJERPH 2022, 19, 14918. [Google Scholar] [CrossRef]
- Platz, T; Pinkowski, C; Van Wijck, F; Kim, IH; Di Bella, P; Johnson, G. Reliability and validity of arm function assessment with standardized guidelines for the Fugl-Meyer Test, Action Research Arm Test and Box and Block Test: a multicentre study. Clin Rehabil 2005, 19, 404–411. [Google Scholar] [CrossRef]
- Chen, HM; Chen, CC; Hsueh, IP; Huang, SL; Hsieh, CL. Test-Retest Reproducibility and Smallest Real Difference of 5 Hand Function Tests in Patients With Stroke. Neurorehabil Neural Repair 2009, 23, 435–440. [Google Scholar] [CrossRef]
- Oña, ED; Sánchez-Herrera, P; Cuesta-Gómez, A; Martinez, S; Jardón, A; Balaguer, C. Automatic Outcome in Manual Dexterity Assessment Using Colour Segmentation and Nearest Neighbour Classifier. Sensors 2018, 18, 2876. [Google Scholar] [CrossRef]
- Ekstrand, E; Lexell, J; Brogårdh, C. Test−Retest Reliability and Convergent Validity of Three Manual Dexterity Measures in Persons With Chronic Stroke. PM&R 2016, 8, 935–943. [Google Scholar] [CrossRef]
- Proud, EL; Bilney, B; Miller, KJ; Morris, ME; McGinley, JL. Measuring Hand Dexterity in People With Parkinson’s Disease: Reliability of Pegboard Tests. The American Journal of Occupational Therapy 2019, 73, 7304205050p1-8. [Google Scholar] [CrossRef] [PubMed]
- Hervault, M; Balto, JM; Hubbard, EA; Motl, RW. Reliability, precision, and clinically important change of the Nine-Hole Peg Test in individuals with multiple sclerosis. International Journal of Rehabilitation Research 2017, 40, 91–93. [Google Scholar] [CrossRef] [PubMed]
- Duncan, PW; Bode, RK; Lai, SM; Perera, S. Rasch analysis of a new stroke-specific outcome scale: the Stroke Impact Scale. Archives of physical medicine and rehabilitation 2003, 84, 950–963. [Google Scholar] [CrossRef] [PubMed]
- Phipps, S; Richardson, P. Occupational Therapy Outcomes for Clients With Traumatic Brain Injury and Stroke Using the Canadian Occupational Performance Measure. The American Journal of Occupational Therapy 2007, 61, 328–334. [Google Scholar] [CrossRef]
- Santamaría-Peláez, M; Pardo-Hernández, R; González-Bernal, JJ; Soto-Cámara, R; González-Santos, J; Fernández-Solana, J. Reliability and Validity of the Motor Activity Log (MAL-30) Scale for Post-Stroke Patients in a Spanish Sample. Int J Environ Res Public Health 2022, 19, 14964. [Google Scholar] [CrossRef]
- Michielsen, M; Vaughan-Graham, J; Holland, A; Magri, A; Suzuki, M. The Bobath concept – a model to illustrate clinical practice. Disability and Rehabilitation 2019, 41, 2080–2092. [Google Scholar] [CrossRef]
Figure 1.
International Classification of Functioning.
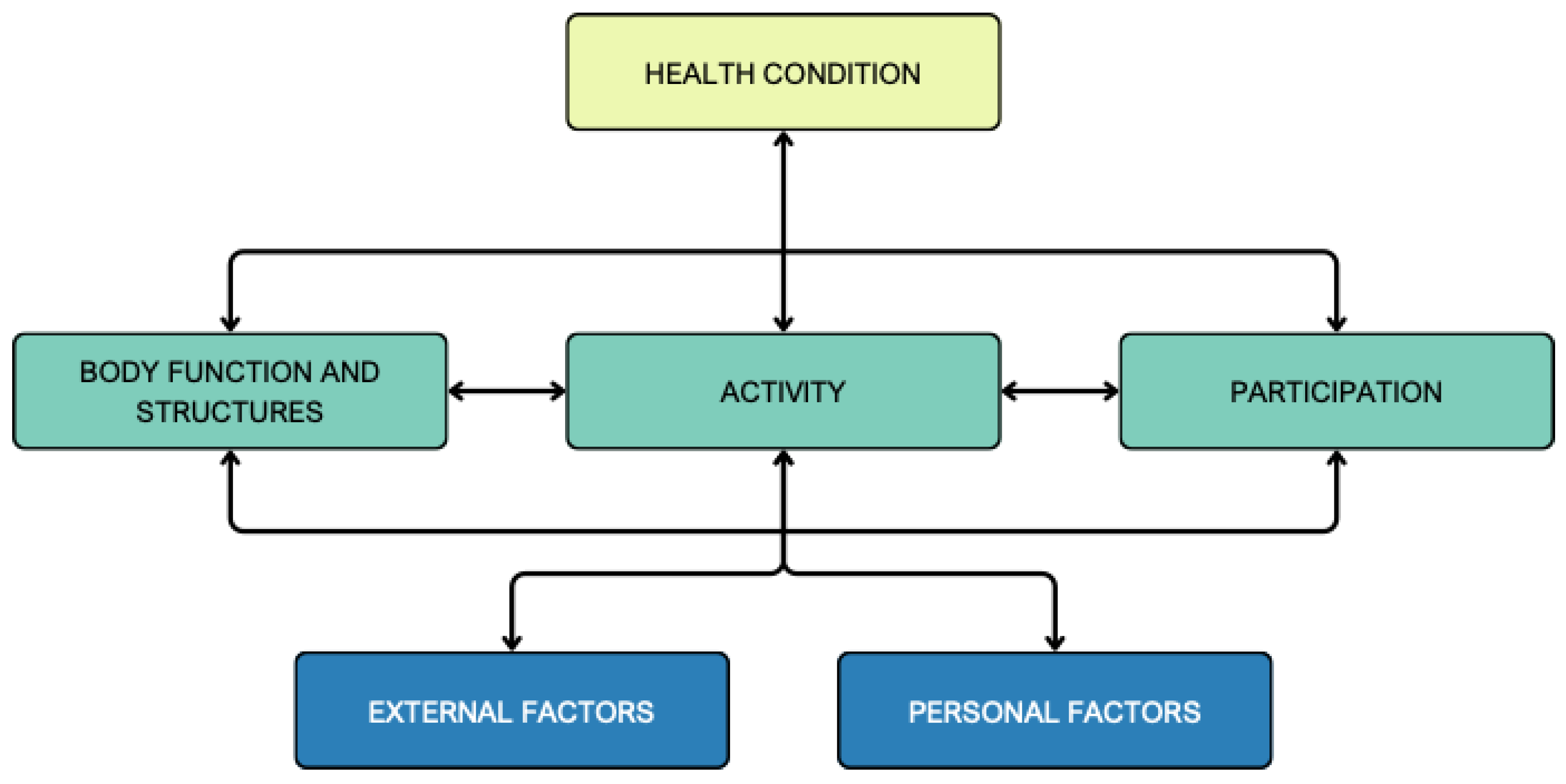
Figure 2.
Patient managing stages by American Physical Therapy Association.
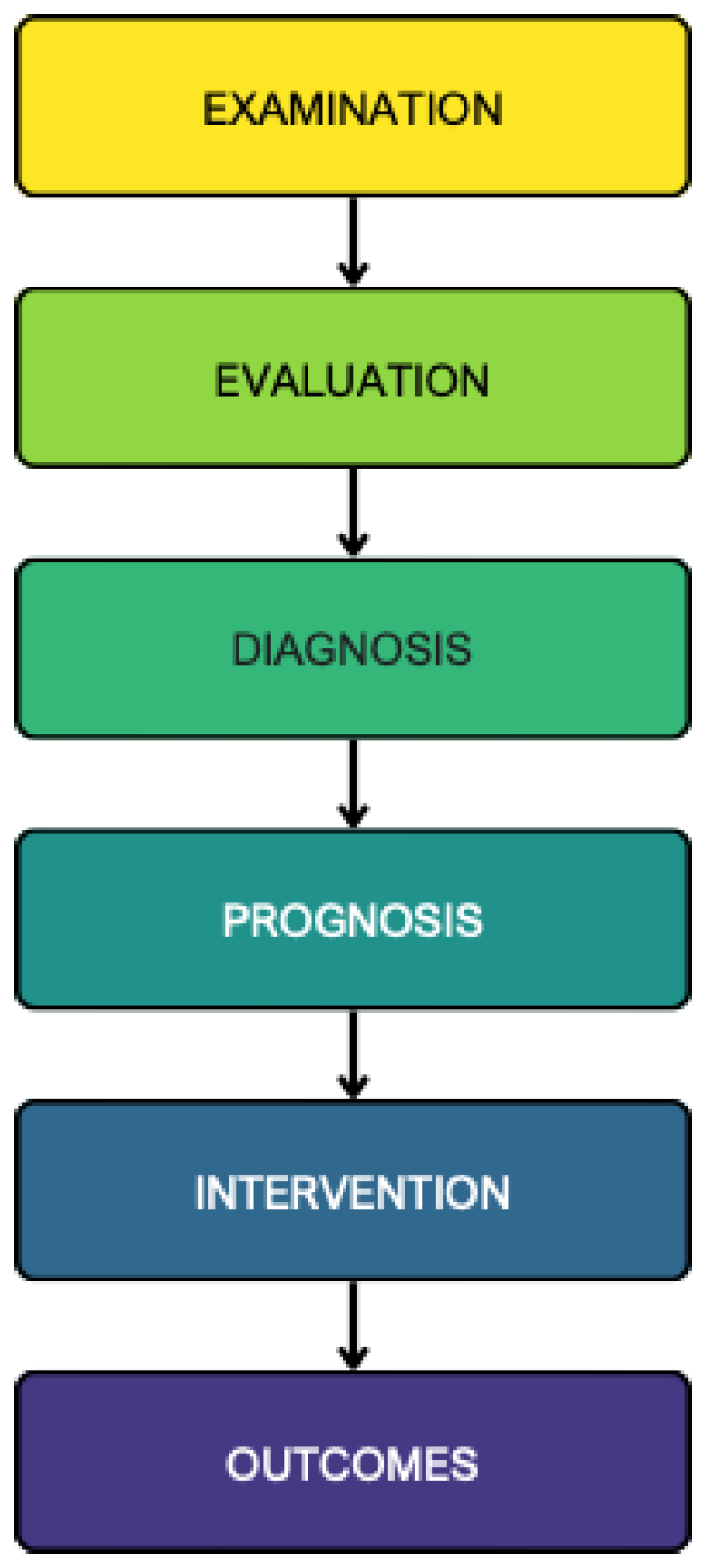
Figure 3.
Interrelated aspects of function.
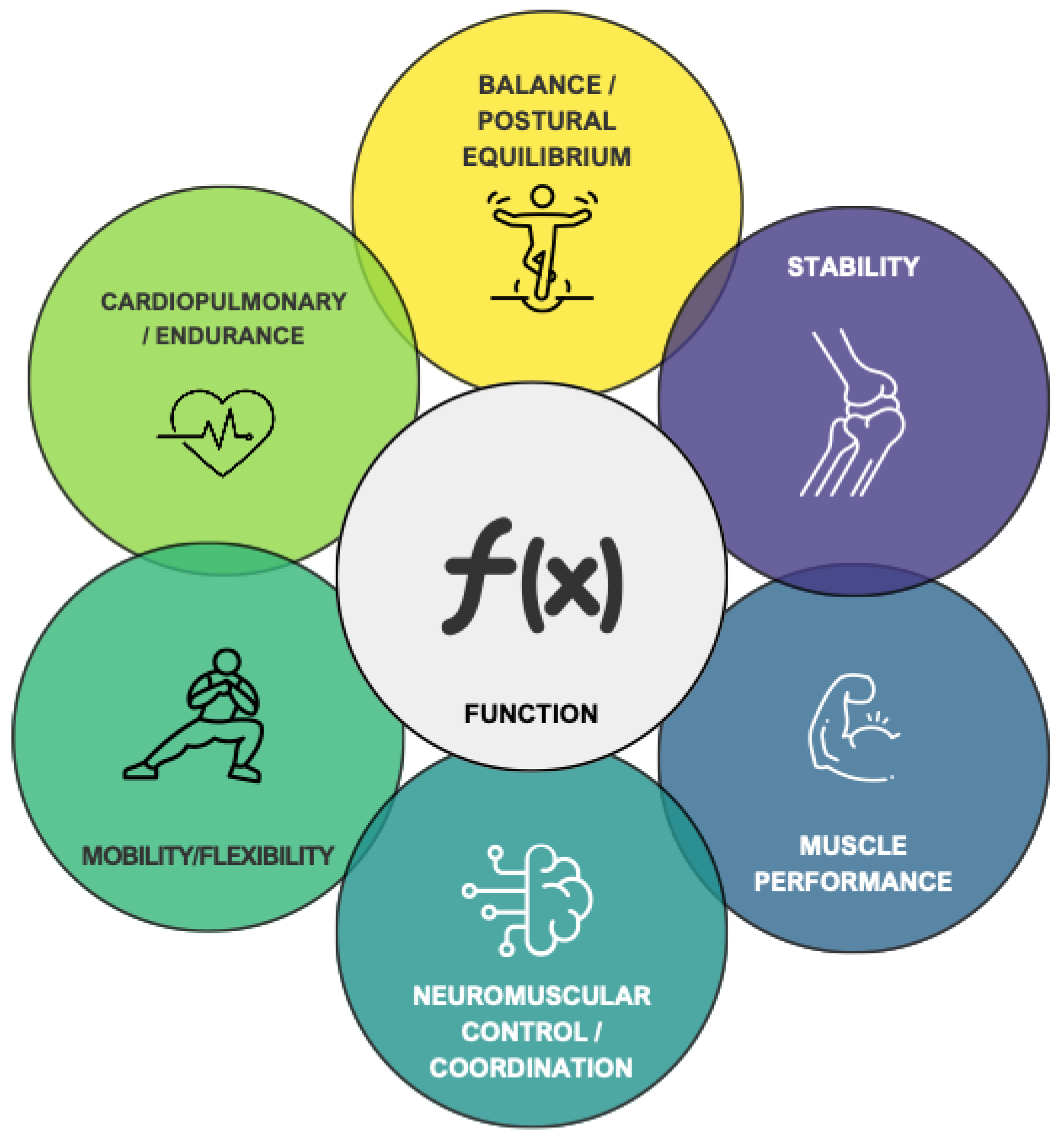
Figure 4.
Multidimensional aspects of physical functions integrated into body functions section of ICF and adapted to patients with neurological conditions.
Figure 4.
Multidimensional aspects of physical functions integrated into body functions section of ICF and adapted to patients with neurological conditions.
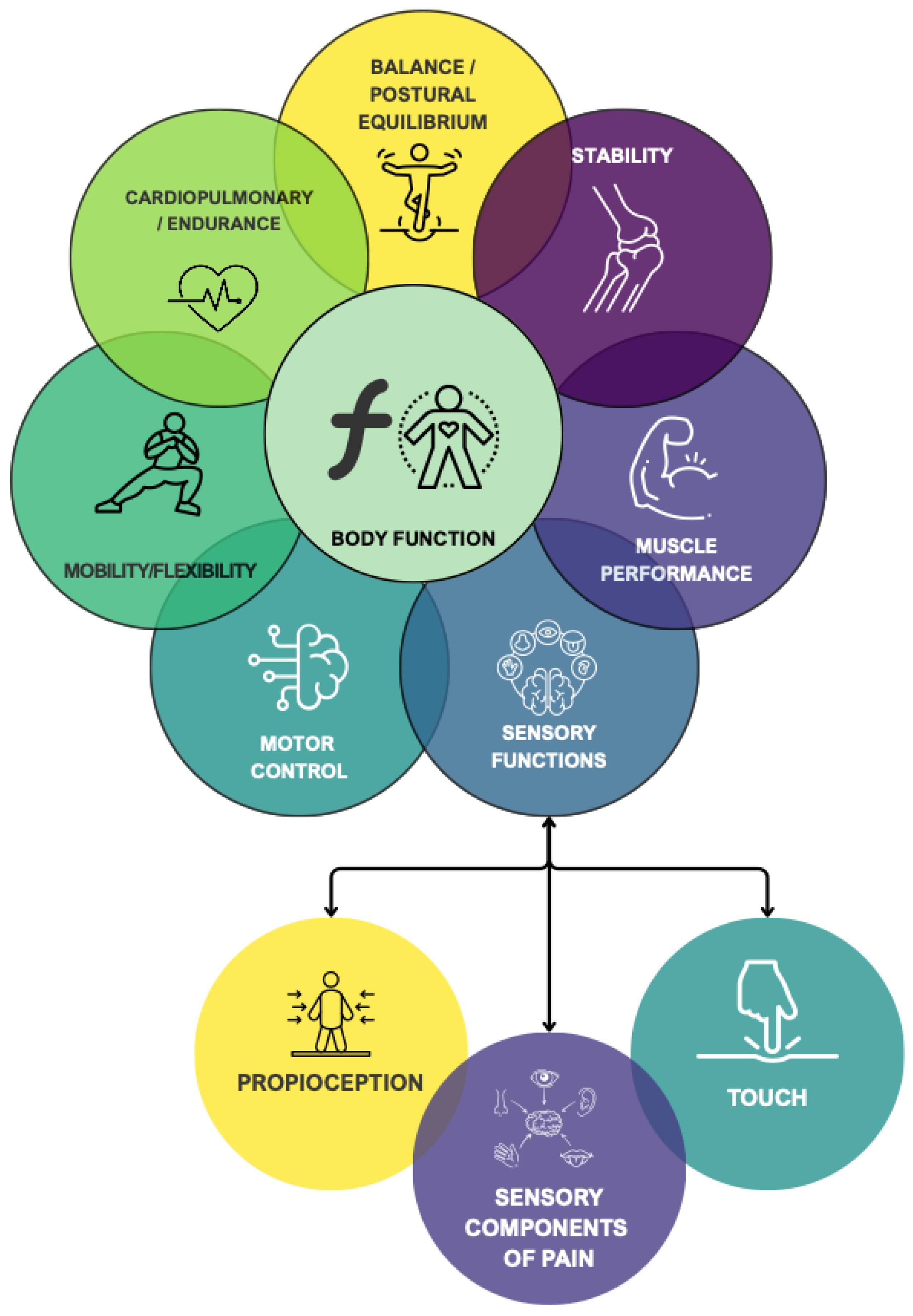
Figure 5.
Modified ICF scheme.
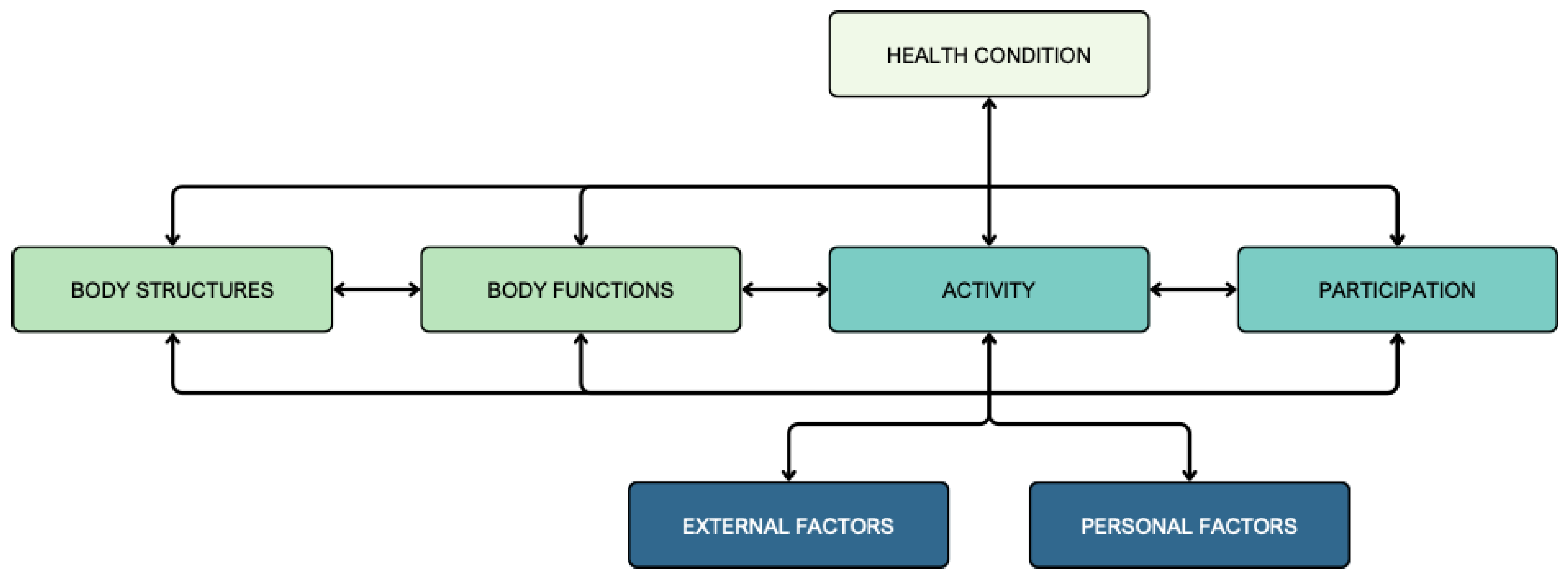
Figure 6.
Activity assessments related to gait.
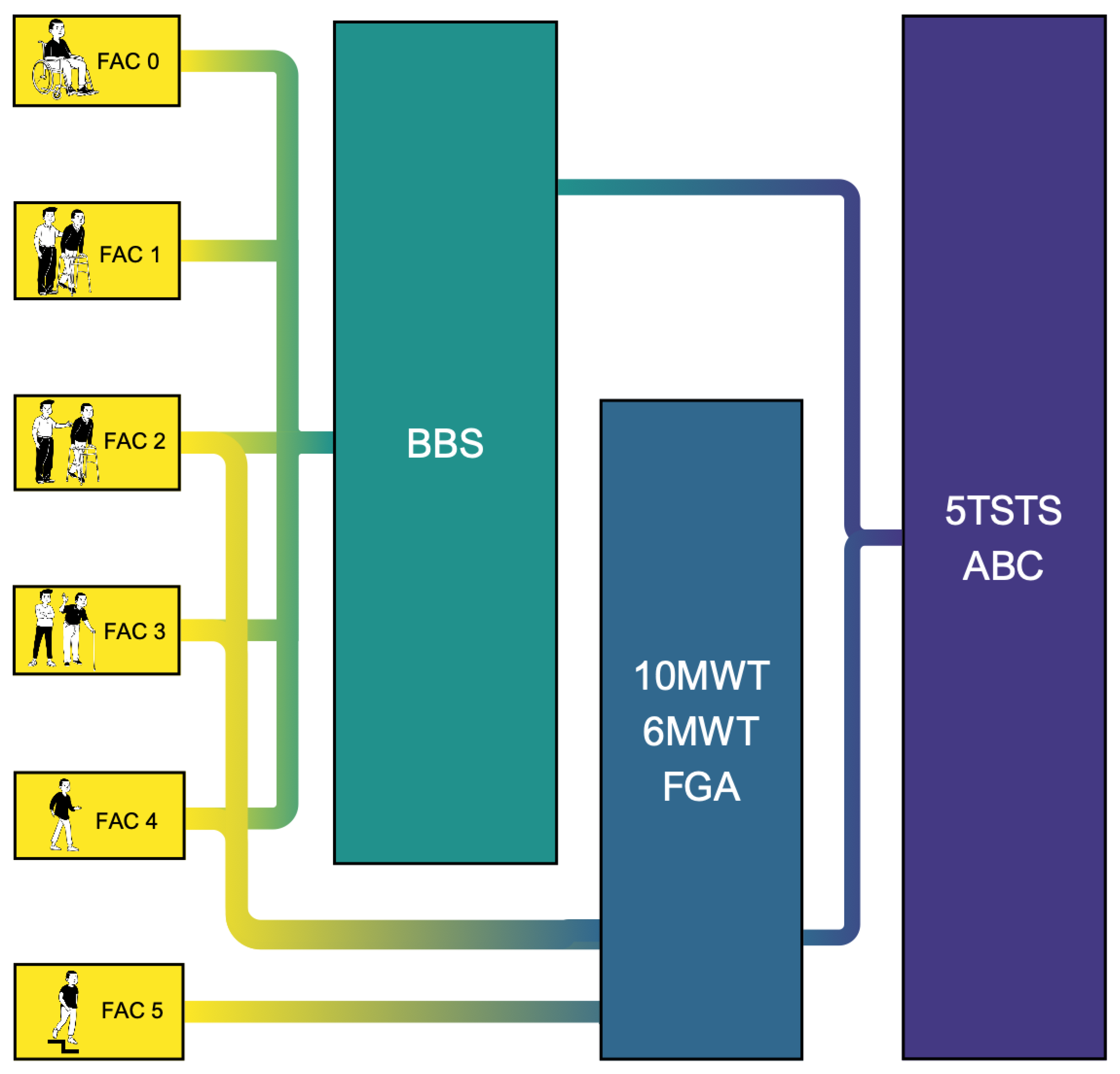
Figure 7.
Biopsychosocial Reasoning Approach in Neurophysiotherapy (BRAIN) framework.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



