
Submitted:
19 January 2026
Posted:
20 January 2026
You are already at the latest version
Abstract
Background: Epstein-Barr virus related acute pharyngotonsillitis is common in children and adolescents, and is generally managed successfully with positive outcomes by both ENT specialists and the pediatricians. However, a variety of acute, life-threating complications can occur, including upper airway obstruction and infectious or dysimmune sequelae. Methods: This paper describes our recent experience with four pediatric patients presenting with severe ENT manifestations of infectious mononucleosis (IM) that led to life-threating complications, all managed over the past three years at our tertiary pediatric hospital. Results: We report four cases (two boys and two girls) aged 5 to 16 years, hospitalized with complicated EBV-related pharyngotonsillitis. Presentations included respiratory distress (cases 1 and 2), fatal hemophagocytic lymphoistiocitytosis (case 3), and a retropharyngeal abscess (case 4). Conclusions: The prognosis of IM in the pediatric population is generally favourable. However, acute life-threating complications may arise. In such cases, timely and coordinated multidisciplinary management involving ENT specialists, pediatricians, and anesthesiologists is critical.
Keywords:
tonsillitis
; EBV
; mononucleosis
; children
; airway obstruction
1. Introduction
Infectious mononucleosis (IM) is an acute viral infection that most commonly affects children and young adults with an incidence of approximately 6 to 8 cases per 1,000 person-years [1].
Epstein-Barr virus (EBV), a double-stranded DNA virus belonging to the Herpesviridae family, is the primary cause of IM, accounting for approximately 90% of cases. A minority of cases (about 10%) are attributed to other viruses, including cytomegalovirus (CMV), human herpes-virus 6 (HHV-6), herpes simplex virus type 1 (HSV-1) and human immunodeficiency virus (HIV) [2].
The primary mode of disease transmission is through close personal contact with an infected person, particularly via their saliva. It is estimated that more than 98% of the world’s adult population has been infected with EBV [3].
Infectious clinical manifestations occur when a high viral load accumulates in the palatine tonsils and adenoids, leading to acute exudative pharyngotonsillitis and adenoiditis, characterized by lymphatic hyperplasia and exudative debris. EBV infects epithelial cells and resting B cells in the oropharynx, begins replicating, and subsequently spreads throughout the body. This process represents the incubation period, which lasts about six weeks and results in the activation of cytotoxic T lymphocytes and natural killer cells.
There is currently not specific treatment for IM; management is supportive, with monitoring for potential complications. Most cases are associated with a favourable prognosis and can be effectively managed with antipyretic or analgesic therapy. In more symptomatic cases, where high fever and pain lead to reduced intake of fluids and food, patients are often admitted to hospital -frequently to an ENT unit- for supportive care, including hydration, analgesia, and antipyretic treatment. Antibiotics are generally not required, unless there is a confirmed bacterial superinfection.
IM typically presents with fever, acute pharyngotonsillitis, and constitutional symptoms related to the involvement of lymph nodes, liver, and spleen. It is often accompanied by hematologic abnormalities such as lymphocytosis.
One of the most frequent presenting symptoms is sore throat, which frequently leads to consultation with pediatricians or ear-nose-throat (ENT) specialists. Most cases are self-limiting and carry an excellent prognosis; however, in rare instances, acute complications may occur, including splenic rupture, hepatitis, and airway obstruction due to tonsillar hypertrophy. Tonsillar enlargement can sometimes lead to severe snoring and restless sleep, accompanied by respiratory pauses that may progress to hypopnea or even obstructive sleep apnoea events. Airway obstruction occurs more frequently in younger children, and it is one of the most common indications for hospitalization [4]. Nevertheless, progressive airway obstruction develops in less than 5% of all patients [5]. Most patients with significant upper airway obstruction can be effectively managed with clinical observation, continuous pulse oximetry monitoring, intravenous hydration, humidification, and systemic corticosteroids. Occasionally, patients with more severe airway compromise may require temporary endotracheal intubation to secure the airway in cases of respiratory distress.
If persistent upper airway obstruction is due to severe tonsillar hyperplasia, surgical intervention should be considered. In such cases, tonsillectomy -generally performed in conjunction with adenoidectomy- should be scheduled as soon as possible [6]. In fewer than 1% of cases, if upper airway obstruction gets worsens and a “cannot intubate cannot oxygenate” scenario arises, an emergency tracheotomy may be required. Tracheal obstruction leading to respiratory failure is the most common cause of death and the most lethal complication of IM [7].
In some patients, a Streptococcus pyogenes (Group A Streptococcus, or Strep A) infection can overlap with EBV-related pharyngotonsillitis. In such cases, the characteristic lymphocytosis with atypical lymphocytes typically observed in a complete blood count is replaced by neutrophilia, distinguishing the condition as a bacterial infection that requires appropriate antibiotic treatment. EBV impairs the bacterial defence mechanisms within the tonsillar niche, by depleting local IgG and secretory-IgA levels, thereby increasing susceptibility to secondary bacterial superinfection, which may subsequently progress to other possible complications, such as the peritonsillar abscess formation [8].
Beyond local complications EBV-related acute pharyngotonsillitis -which are commonly managed by the ENT specialists and pediatricians - IM may occasionally lead to a range of potentially life-threatening neurologic, hematologic, and systemic sequelae. These complications should be promptly recognized and managed, including by ENT physicians. According to Jenson’s [5], these complications include: splenic or liver rupture (<0.5%); neurological complications (1-5%) such as encephalitis or meningoencephalitis, seizure, cerebellitis, cranial nerve neuritis, and Guillain-Barrè syndrome; hematologic complications including hemolytic anemia (3%), thrombocytopenia (25-50%), and neutropenia (50-80%); hepatic involvement, such as hepatitis or asymptomatic elevation of transaminases (50-80%); respiratory complications, including interstitial pneumonia and pleuritis; cardiac complications, such as myocarditis and pericarditis; musculoskeletal complications, including rhabdomyolysis; neuropsychiatric complications, including psychosis and other psychiatric disorders.
2. Aim of the Reported Cases
We describe four pediatric patients with life-threatening ENT manifestations of IM that lead to life-threatening complications selected in the period included between January 2022 and June 2025 among all children admitted to our paediatric or ENT clinics for severe IM. We decided to specifically clinical management of the ones with more severe disease associated with life-threatening complications including respiratory distress, septic systemic involvement, or deep neck space abscess.
Our case series includes two boys and two girls, aged between 5 and 16 years, who were hospitalized between October 2022 and April 2025. They presented with complicated EBV-related pharyngotonsillitis associated with respiratory distress (cases 1 and 2), fatal hemophagocytic lymphoistiocitytosis (case 3), and a retropharyngeal abscess (case 4).
These cases were managed at a tertiary-level pediatric hospital by multidisciplinary clinical teams, including ENT specialists, pediatricians, infectivologists, anaesthesiologists, and intensive care unit physicians. The aim of these case reports is to highlight the possibility of unexpected complications associated with IM and to emphasize the importance of multidisciplinary collaboration in patient management.
3.1. Case Report 1
A 14-years old female, previously in good health, presented to our Pediatric Emergency Department (pED) in October 2022 with pharyngodynia and fever, following a first-line antibiotic treatment with cefixime. On ENT evaluation, the patient was eupnoeic but exhibited stomatolalia due to grade IV tonsillar hypertrophy, with the tonsils covered in purulent, caseous exudates. She also reported dysphagia and progressive airway compromise, without objective dyspnoea at rest, but with noticeable difficulty during speech. Hospitalization was deemed necessary to initiate supportive therapy, including corticosteroids, antipyretics, and parenteral nutrition. The clinical suspicion of EBV infection was confirmed by elevated EBV viral capsid antigen (VCA) IgM levels ( >160 U/mL). Additional relevant laboratory findings included leucocytosis with lymphomonocytoses, elevated aspartate transaminase (AST, 117 U/L), alanine aminotransferase (ALT, 130 U/L), gamma-glutamyl transferase (GGT, 110U/L), and lactatedehydrogenase (LDH, 590 U/L).
During hospitalization in the pediatric ward, a neck and complete abdominal ultrasound were planned to rule out possible suppurative cervical lymphadenitis, and involvement of the liver, spleen, or abdominal lymph nodes. However, during the examination, the patient experienced a cardio-circulatory arrest, likely of hypoxic origin due to massive tonsillar hypertrophy causing oropharyngeal collapse in the supine position. Anesthesiologists were immediately alerted and performed an emergency intubation which was successful on the second attempt. Cardiopulmonary resuscitation was initiated and successfully completed, after which the patient was transferred to our Pediatric Intensive Care Unit (pICU). A subsequent ENT evaluation, revealed that the entire oro- and hypopharyngeal space was occupied by severely hypertrophic tonsils with a necrotic-hemorrhagic appearance.
After clinical stabilization and recovery of vital signs, a computed tomography (CT) scan of the neck (Figure 1), chest, abdomen, and brain was performed. The imaging revealed marked adenotonsillar hypertrophy and multiple reactive cervical lymphoadenopaties, with no acute pathological findings at the brain level.
A few days later, due to persistent tonsillar hypertrophy that rendered extubation impossible despite maximal maximal corticosteroid therapy, the patient underwent bilateral microdebrider-assisted intracapsular tonsillotomy. Histopathological examination of the tonsillar tissue confirmed benign reactive lymphoid hyperplasia, with no evidence suggestive of lymphoproliferative disorders.
The patient was successfully extubated on postoperative day two. However, due to persistent neurological slowing and aphasia of uncertain origin, a brain MRI was performed, which showed no significant abnormalities. A gradual improvement in neurological status was observed, although aphasia persisted, characterized by coherent ideation.
Due to significant bleeding from both the tonsillar lodges on the second day after surgery, a surgical revision was required; a right extracapsular tonsillectomy and a revision of the left intracapsular tonsillectomy were performed. The following day, another bleeding episode occurred, necessitating urgent intubation and subsequent surgical revision. Coagulation tests were normal, and second-level immunological screening was negative. Upon extubation, neurological evaluation revealed dysarthria, dysphonia and a mild gait disturbance, which progressively improved during the hospital stay.
Repeated neurological and psychiatric assessments ruled out hypoxic brain injury, and were both suggestive of post-traumatic stress disorder. Additionally, during hospitalization, anxious-panic traits and a specific learning disability were identified, and the patient was referred to a psychotherapy centre.
The patient underwent an extensive rehabilitation program, including behavioural therapy, speech therapy, and physiotherapy, achieving full recovery nine months after hospital discharge.
3.2. Case report 2
A five years-old otherwise healthy male presented to our pED in July 2023 with progressive dyspnoea and deterioration of general clinical condition during an episode of acute pharyngotonsillitis. He had been receiving treatment for two days with amoxicillin at 50 mg/kg/die for fever and sore-throat, following a positive rapid swab for Group A beta-hemolytic streptococcus (GABHS). On clinical evaluation, the patient exhibited evident dyspnoea with retractions and sudden O2 desaturation, necessitating emergency intubation and transfer to the pICU. Initial ENT evaluation, performed while the patient was intubated, revealed grade 2 tonsillar hypertrophy with a friable, white-coated exudate and multiple bilateral non-fluctuant cervical lymphadenopathies. Flexible nasopharyngeal endoscopy, showed non-obstructive adenoidal hypertrophy.
Laboratory testing confirmed EBV infection, with a high viral load (97,393 EBV copies/mL in blood and 340,000 copies/mL from the tonsillar swab), and positive EBV serology (EBV-VCA IgM 129 U/mL). Additional findings included lymphomonocytosis, elevated liver function tests, and a mildly increased CRP level (1.20 mg/dL). Other co-infections were excluded through a repeat GABHS swab, which was negative, and a multiplex PCR respiratory panel performed on a nasopharyngeal aspirate. Given clinical suspicion of pneumonia, a chest X-ray was performed, showing bilateral accentuation of the hilar and perihilar bronchovascular markings, with a tendency toward confluence in the right upper and lower perihilar regions. An abdominal ultrasound also revealed mild splenomegaly (maximum diameter: 13 cm). Treatment with high-dose corticosteroids and amoxicillin/clavulanic acid at 75 mg/kg/day was continued.
Seventy-two hours after intubation, the first extubation attempt was unsuccessful. A second attempt, performed 48 hours later, with ENT assistance, resulted in successful extubation under video-laryngoscopic guidance. During the procedure, a video laryngo-tracheoscopy was conducted under spontaneous breathing, revealing a bulging of the posterior tracheal wall suggestive of mild and localized tracheomalacia of the pars membranacea. Despite this finding, the patient’s recovery was uneventful. A subsequent neck and chest CT scan confirmed preserved tracheal patency with no evidence of obstruction or structural compromise.
Progressive clinical and laboratory improvement followed. The child was discharged 20 days after admission, and an elective extracapsular tonsillectomy was successfully performed a few months later.
3.3. Case report 3
The third case involves a 14-years old previously healthy female who presented at our pED in October 2024 with general asthenia, fever and acute pharyngotonsillitis. She had been treated for a few days with amoxicillin/clavulanic acid prior to admission. Initial blood assessment revealed elevated liver enzymes (ALT: 298 U/L, AST: 380 U/L), and direct hyperbilirubinemia (4 mg/dL), while white blood cell count (with mild monocytosis) and CRP were within normal limits. EBV infection was confirmed by serology and a high viral load (344,800 copies/mL in blood).
The patient was admitted to the pediatric ward. Over the following days, her general conditions and laboratory profile progressively worsened, with the development of dysphagia and signs of cholestatic hepatitis. The initial ENT evaluation, revealed a severely ill appearance, grade 4 “kissing” tonsils with marke adenoid hypertrophy, complete activation of Waldeyer’s ring with friable, bleeding lymphatic tissue, and multiple painful lymphadenopathies.
A broad-spectrum antibiotic regimen was initiated with clindamycin (600 mg three times daily) and piperacillin/tazobactam (4.5 gr four times daily), along with high-dose methylprednisolone (initially 30 mg twice a daily, increased to 40 mg three times daily). Despite therapy, the patient showed no clinical improvement; fever persisted, and laboratory parameters continued to worsen. New findings included hyperferritinemia (1,485-2,636 mg/L) and cytopenia (hemoglobin 8.1 g/dL; platelets: 72 x 10e9/L), raising strong clinical suspicion for EBV-associated hemophagocytic lymphohistiocytosis (EBV-HLH). The patient was transferred to the pICU, where cyclosporin therapy (2mg/kg/die in two divided doses) was initiated.
As her respiratory function deteriorated and non-invasive ventilation became insufficient to maintain adequate oxygenation, endotracheal intubation was performed. To exclude EBV-driven lymphoproliferative disease, an ultrasound-guided cervical lymph node needle biopsy was obtained. Histopathological confirmed a lymphoma-like reactive lymphoid proliferation, consistent with infectious mononucleosis, according to the World Health Organization’s 2016 classification and the International Collaboration on Cancer Reporting’s 2022 refined criteria [9]. A contrast-enhanced CT scan of the neck and chest ruled out any suppurative complication. However, due to persistent bulky, hyperactivated lymphoid tissue in the upper airways that precluded safe extubation, a temporary tracheostomy was performed.
Despite intensive care measures and high-dose immunosuppressive therapy, the patient’s condition deteriorated further. Three weeks after the hospitalization, she developed sepsis and multi-organ failure, which led to death. The final EBV viral load measurement showed a markedly elevated level of 62,178,000 copies/mL in blood.
3.4. Case report 4
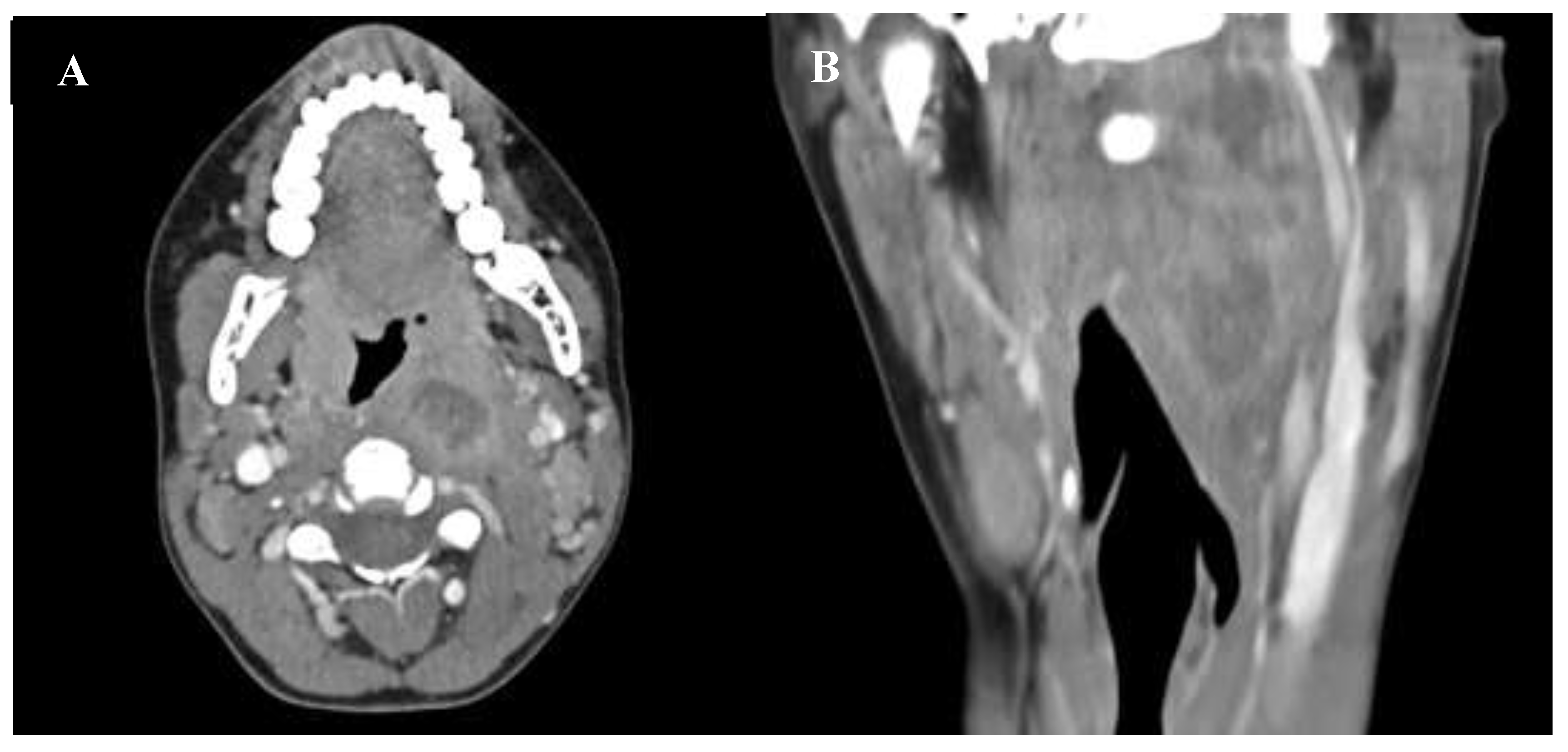
In March 2025 a 16-year-old previously healthy male with a recent diagnosis of EBV-related pharyngotonsillitis presented to the pED with neck pain, pharyngodynia, and intermittent fever persisting for 10 days. ENT evaluation revealed painful limitation of neck movement with mild swelling in the upper left laterocervical region, grade 2 tonsillar hypertrophy, and a left-sided retrotonsillar bulging. Video-laryngoscopy demonstrated swelling of the left oropharyngeal. Given the clinical suspicion of a retro-parapharyngeal asbscess, a contrast-enhanced neck CT scan was performed. Imaging revealed a swelling in the paramedian retropharyngeal space with a hypodense, non-homogeneous central area measuring approximately 16x24 mm on the axial plane and 59 mm in the craniocaudal direction. The mass protruded into the airway, displacing the left palatine tonsil anteromedially and extending toward the superficial neck, compressing the jugular vein (Figure 2).
Laboratory findings showed weak positivity on the Monospot-test, leukocytosis (21.20 x 10e9/L) with marked neutrophilia (17.53 x 10e9/L) and monocytosis (2.07 x 10e9/L), along with a significantly elevated CRP level (255.9 mg/L).
Based on these findings, the patient underwent surgical drainage of the abscess via a transoral approach. Access to the most cranial portion of the collection was achieved through a vertical incision on the left oropharyngeal wall, just posterior to the ipsilateral tonsillar lodge, allowing evacuation of a large volume of purulent secretions.
Following infectious disease consultation, empiric antibiotic therapy with ceftriaxone (2gr/day) and clindamycin (600 mg every 8 hours) was initiated. Subsequent culture of the pulurent material isolated multi-sensitive Arcanobacterium haemolitycum, allowing for simplification of the antibiotic regimen to ceftriaxone monotherapy.
The patient’s clinical conditions and laboratory parameters progressively improved. A follow-up CT scan performed seven days after surgery showed near-complete resolution of the previously noted hypodense areas of liquefaction. The patient was discharged 11 days after admission, with a recommendation to undergo elective tonsillectomy in the near future.
4. Discussion
We present four remarkable cases of EBV-related acute pharyngotonsillitis complicated by life threatening conditions, such as respiratory distress, EBV-associated hemophagocytic lymphohistiocytosis (EBV-HLH), and retro-pharyngeal abscess, occurring in children. We selected these cases, to draw attention to the potential fatal complications of EBV-infection, which, although rare, must be promptly recognized and treated to avoid a poor prognosis. Given the rarity of these complications, there is no a clear consensus on treatment strategy. We specifically selected the most severe cases that we had managed among all children hospitalised in the period 2022-2025 in our paediatric ENT, high or medium intensity paediatrics departments of our pediatric tertiary-level hospital in the city centre of Milan, for severe IM. In these small case-series we managed a broad panel of life-threatening complications, including certainly respiratory distress, but also the development of severe systemic septic evolution, including fatal hemophagocytic lymphohistiocitytosis, or retropharyngeal/deep neck space abscesses.
Despite EBV-related pharyngotonsillitis in the course of IM are frequent and generally have a benign and self-limiting evolution, in rare cases they may be associated with more severe clinical manifestations that may also have an inauspicious evolution. Such patients are often managed in a univalent manner by the paediatrician or, sometimes, by the ENT specialist alone. We believe, however, that in specific cases, the prognosis can be optimised by the support of a multidisciplinary team, which includes paediatricians, ENT specialists, infectivologists, radiologists and intensive care resuscitators.
Acute airway obstruction in patients with IM is rare, with an incidence reported between 1–3.5% [10,11,12]: this complication may present suddenly and requires prompt otolaryngologic and anaesthesiologic support. In some instances, the activation of pharyngeal lymphatic tissue is so florid and abrupt that even high-dose systemic steroid treatment is insufficient to reduce the swelling in a short period. When it occurs, appropriate airway management is essential; in severe cases, endotracheal intubation or emergency tracheostomy may be required.
Tonsillar enlargement occupying more than 75% of the oropharyngeal inlet can rapidly lead to severe airway compromise, even though the patient may initially appear deceptively calm [13]. This progression is more common in younger children, where respiratory distress can develop surprisingly quickly due to the relatively small size of the oro-laryngopharyngeal space in comparison to the enlarged tonsils. In such cases, the presence of anesthesiologists experienced in pediatric care and access to a pediatric intensive or sub-intensive care unit are mandatory to ensure safe management. Given the unpredictability of this evolution, multidisciplinary sharing bewteen ENT specialists, pediatricians, and anesthesiologists from the patient’s arrival is highly desirable, especially in cases at greatest risk for the development of complications.
When significant tonsillar hypertrophy results in upper airway obstruction, ugent tonsillectomy may be required to restore the patency of the oropharyngeal lumen. However, the increased risk of both primary and secondary bleeding due to acute, florid inflammation should be taken into account. In this context, intracapsular tonsillectomy (i.e., tonsillotomy) may be the preferred option compared to traditional extracapsular tonsillectomy (i.e., complete tonsillar removal) during the acute phase of the disease, as it carries a lower -though not negligible- risk of hemorray [14]. In our specific case (patient N° 1), intracapsular tonsillectomy enhabled successful extubation, although two post-operative bleeding occurred, each requiring surgical revision.
Historically, it has been repeatedly suggested that tonsillectomy may shorten the clinical course in patients with IM presenting with marked tonsillar involvement. This concept dates back to the 1930s through the 1970s. Case reports, retrospective studies, and expert commentaries described significantly improved clinical outcomes following tonsillectomy, with earlier recovery and no increase in complication rates [15].
Nevertheless, these studies were neither randomized nor included control groups, and no randomized controlled trials on the role of tonsillectomy in the treatment of IM were published between 1984 and 2014. Moreover, clinical practice guidelines for tonsillectomy in children from the USA, France, and other countries do not list IM as an indication for the procedure.
According to Windfuhr et al. [6], tonsillectomy should not be routinely performed for symptom control or to shorten the course of the disease. However, it may be considered in selected patients with clinically significant upper airway obstruction caused by severe inflammatory tonsillar hyperplasia.
When considering wether to perform a tonsillectomy or a tonsillotomy, the chosen surgical approach should aim to minimize the risk of hemorrhage. The literature presents varying rates of post-operative bleeding. For example, Lloyd [16] reported a series of patients who underwent intracapsular tonsillectomy (tonsillotomy), none of whom experienced postoperative bleeding, symptoms recurrence, or required readmission for hemorrage.
In contrast, particularly in older studies, some authors have advocated for acute tonsillectomy to relieve upper airway obstruction unresponsive to corticosteroid therapy [17]. However, this approach is not widely adopted due to the high risk of perioperative bleeding, with rates reported as high as 13% [18].
Our third dramatic case compelled the ENT and pediatric teams to confront a very rare complication of EBV infection -EBV-associated hemophagocytic lymphohistiocytosis (EBV-HLH). According to the literature [19], EBV-HLH is a rare and potentially life-threatening syndrome characterized by fever, pancytopenia, organomegaly, multiorgan dysfunction, and hemophagocytosis, which is mediated by an excessive number of activated macrophages infiltrating the bone marrow and other tissues. The syndrome has been described in familial (genetic) forms or as a secondary condition triggered by infections, malignancies, or autoimmune diseases. Among infectious triggers, EBV is the most frequently reported cause of secondary HLH. Although EBV–HLH likely results from underlying immune dysregulation, the precise nature of host susceptibility remains poorly understood. Notably, most cases occur in previously healthy, immunocompetent individuals [20].
The diagnostic guidelines for HLH [21] identify eight criteria, of which five must be met for diagnosis. These include: 1) persistent fever; 2) splenomegaly; 3) cytopenias affecting at least two of three blood cell lineages; 4) hypertriglyceridemia and/or hypofibrinogenemia, 5) evidence of hemophagocytosis in bone marrow, spleen, or lymph nodes. Additionally, the following criteria have been introduced: 6) low or absent natural killer (NK) cell activity; 7) hyperferritinemia; 8) elevated soluble interleukin-2 receptor (sIL-2r) levels. Among these, a ferritin level above 500 µg/L is considered a particularly valuable biomarker for the diagnosis of HLH.
According to a recent multicenter retrospective study [22], the overall survival (OS) of children with EBV-HLH ranges from a few weeks to several years. While some children achieve complete remission and long-term survival through immunotherapy or chemotherapy, others may die within months- even after undergoing allogeneic hematopoietic stem cell transplantation (allo-HSCT). For example, in a 2021 retrospective analysis by Kwak et al. [23] the 5-year OS rate was reported as 72.1%.
The combination of etoposide and dexamethasone, as outlined in the HLH-2004/94 protocol [24], remains the standard of care for treating EBV-HLH. Allogeneic HSCT is selectively employed after induction therapy, particularly in cases of primary HLH, as noted in the case series by Contreras-Chavez [25].
Due to the rarity of this severe condition -estimated at an annual incidence of 1 in 800,000 individuals [26]-, there are limited studies focused specifically on EBV-HLH secondary to IM in adolescents. One of the most recent is a Japanese retrospective analysis involving 133 patients aged ≥14 years and older, which reported an overall mortality rate of 82.1%. This study also highlighted that patients who received HSCT had significantly better survival rates than those who did not [27]. Our case supports the conclusions of this analysis: non-response to first-line treatment with high-dose corticosteroids and immunosuppressants is associated with a poorer prognosis, and a rapidly progressive clinical course.
The final case describes a rare complication of EBV-related acute pharyngotonsillitis: a retropharyngeal abscess caused by a bacterial superinfection. EBV infection induces transient immunosuppression, particularly a reduction in T-cell-mediated immunity, which can predispose patients to secondary bacterial infections, by allowing commensal oral flora to become pathogenic. In this case, the retropharyngeal abscess extended into the space between the alar fascia and the prevertebral fascia of the neck, providing a direct route to the mediastinum and pleural spaces. This anatomical progression can lead to descending necrotizing mediastinitis, a life-threatening condition. A 2020 literature review [26] identified only eight reported cases of retropharyngeal abscess progressing to mediastinitis during EBV infection, highlighting the rarity of this complication.
In contrast to peritonsillar abscesses- where the most commonly isolated bacteria include viridans group streptococci, beta-hemolytic streptococci, Fusobacterium necrophorum, Staphylococcus aureus, Prevotella species, and Bacteroides species [29], - abscesses associated with EBV infection predominantly involve anaerobic microorganisms of the oropharyngeal flora. EBV-induced mmunosuppression may serve as the initial trigger in the cascade of events leading to these potentially life-threating infections [30].
The incidence of serious and potentially fatal acute upper airway obstruction during primary EBV infection increases with age [14]. Respiratory symptoms -such as pleuritic involvement and dyspnoea- and an unusually prolonged fever lasting more than 10 days in patients with IM should be considered clinical ‘red flags’ for life-threatening complications [16]. The risk of respiratory failure or severe involvement of neck muscles, blood vessels, and cranial nerves can only be mitigated through early diagnosis and prompt medical and surgical intervention. However, the diagnostic and therapeutic pathways remain controversial, as there are no universally accepted criteria for distinguishing between cases than can be managed conservatively with antibiotics and those that require surgical intervention.
In the literature [31], two main mechanisms for the development of mediastinitis have been described. The first involves direct extension of the abscess through the space between the alar and prevertebral fascia. The second involves hematogenous spread through septic thrombophlebitis, as seen in Lemierre’s syndrome.
In reference to our case, since no signs of peritonsillar abscess were observed during oroscopy, we can hypothesize the presence of concomitant retropharyngeal reactive lymphadenitis due to bacterial superinfection, with probable abscess formation (colliquation) originating from the involved retropharyngeal lymph node stations. This pathogenetic mechanism is quite unique, particularly given the patient’s age and the lack of comparable cases reported in the literature.
As outlined in a recent narrative review by Esposito et al. in 2022 [13], in most cases of peritonsillar, retropharyngeal or parapharyngeal abscesses, if the patient has not received antibiotic therapy, an initial trial of empiric intravenous antibiotics is recommended, followed by a clinical re-evaluation after 48 hours. However, younger age, the presence of underlying chronic diseases, and involvement of the retropharyngeal space are all considered risk factors for complications such as mediastinitis. In such cases, these factors should prompt consideration of surgical intervention as the first-line approach [13].
Several surgical treatment options, are available for deep neck space infections, including needle aspiration, incision and drainage, and abscess tonsillectomy. Among these, needle aspiration is generally considered the safest and best-tolerated option. For peritonsillar both and retropharyngeal abscesses, an oral surgical approach is preferred when feasible. However, surgery must be preceded by a through evaluation of airways patency, as the risk of airway obstruction can be significant in some cases.
Although endotracheal intubation typically resolves airway concerns, it can be technically challenging or risky in the presence of laryngeal edema and abscess protrusion. In certain situations, intubation may worsen edema or cause rupture of the abscess, leading to aspiration of pus. When airway management proves difficult or hazardous, emergency tracheotomy may be necessary. Postoperative respiratory monitoring should continue for at least 48 hours due to the potential for progressive edema in the immediate recovery period.
In cases of life threatening retropharyngeal abscess, there is broad consensus in the literature on the need for elective tonsillectomy, once the acute episode ha resolved. However, tonsillectomy should not be performed routinely for symptom control in cases of mononucleosis-associated tonsillitis. In contrast, a tonsillotomy (intracapsular tonsillectomy) is indicated in acute settings where with clinically significant upper airway obstruction results from inflammatory tonsillar hyperplasia [32], as previously discussed.
5. Conclusions
The prognosis for IM in the pediatric population is generally favourable, although a range of acute complications can occur. Severe complications are rare, and most resolve spontaneously without the need for specific intervention. However, the most serious or fatal cases often result from an uncontrolled lymphoproliferative response that lead to immune system compromise. The case reports described underline the diagnostic challenges that ENT specialist may face when managing cases of IM. ENT specialist, in particular, play a crucial role in identifying when EBV-related tonsillitis may progress to more severe sequelae and should be aware of these rare complications. It is essential to consider the systemic effects of mononucleosis and to evaluate the need for surgical intervention- particularly in cases of upper airway obstruction or superinfections that prove refractory to medical management- in such a vulnerable population as children.
Multidisciplinary collaboration with pediatricians and pediatric intensivists is fundamental. Decisions regarding invasive and potentially high-risk surgical procedures, must be made jointly, weighing the risks and benefits with careful clinical judgment.
Due to the rarity of these emergent presentations, the literature lacks standardized guidelines for managing life-threatening complications of EBV-related acute tonsillitis in children. To date, such cases have been managed on an individual basis, often relying on the experience and expertise of the healthcare team. However, there is a clear need for further research and the development of evidence-based protocols to guide optimal care in these complex scenarios.
Author Contributions
Conceptualization, ST; methodology, ST; investigation, LG, MG, GG, PM, SB; writing—original draft preparation, AC; writing—review and editing, ST, GP; visualization, LG. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Ethical review and approval were waived for this report given that the article describes only individual case reports, and does not constitute a structured study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request due to privacy/ethical restrictions.
Acknowledgments
The paper was granted by the Italian Ministry of Health-Ricerca Corrente 2025 grant.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| IM | Infectious mononucleosis |
| EBV | Epstein-Barr Virus |
| ENT | Ear, nose, throat |
| pED | Pediatric emergency department |
| VCA | Anti-viral capsid antigen |
| AST | Aspartate transaminase |
| ALT | Alanine aminotransferase |
| GGT | Gamma-glutamyltransferase |
| LDH | Lactate dehydrogenase |
| pICU | Pediatric intensive care unit |
| CT | Computed tomography |
| SBEGA | Group A beta-hemolytic streptococcus |
| PCR | C-reactive protein |
| HLH | Hemophagocytic lymphohistiocytosis |
| OS | Overall survival |
References
- Sylvester, J.E.; Buckanan, B.K.; Silva, TW. Infectious mononucleosis: rapid evidence review. Am Fam Physician 2023, 107(1), 71–78. [Google Scholar] [PubMed]
- Hurt, C.; Tammaro, D. Diagnostic evaluation of mononucleosis-like illnesses. Am J Med 2007, 120(10), 911.e1–e8. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Lam, J.M.; Barankin, B. Infectious Mononucleosis: An Updated Review. Curr Pediatr Rev 2024, 20, 305–322. [Google Scholar] [CrossRef] [PubMed]
- Ganzel, T.M.; Goldman, J.L.; Padhya, T.A. Otolaryngologic clinical patterns in pediatric infectious mononucleosis. Am J Otolaryngol 1996, 17, 397–400. [Google Scholar] [CrossRef]
- Jenson, H.B. Acute complications of Epstein-Barr virus infectious mononucleosis. Current Opinion in Pediatrics 2000, 12, 263–268. [Google Scholar] [CrossRef] [PubMed]
- Windfuhr, J.P.; Toepfner, N.; Steffen, G.; et al. Clinical practice guideline: tonsillitis II. Surgical management. Eur Arch Otorhinolaryngol 2016, 273, 989–1009. [Google Scholar] [CrossRef]
- Kumar, S.; Hepat, S.; Acharya, S.; et al. Infectious Mononucleosis Presenting as Near-Fatal Tracheal Obstruction. J Glob Infect Dis 2022, 15, 28–30. [Google Scholar] [CrossRef]
- Räisänen, S. Bacterial penetration into tonsillar surface epithelium during infectious mononucleosis. J Laryngol Otol 2000, 114, 848–852. [Google Scholar] [CrossRef]
- Helliwell, T.R.; Judge, M.J.; Birdsong, G.G.; et al. The International Collaboration on Cancer Reporting (ICCR): 10 Years Progress in the Development of Cancer Pathology Datasets. Int J Gynecol Pathol 2022, 41, S3–S7. [Google Scholar] [CrossRef]
- Fukumasa, H.; Tanaka, C.; Kobayashi, M; et al. Nasopharyngeal airway for upper airway obstruction in infectious mononucleosis. Pediatrics International 2020, 62, 642–643. [Google Scholar] [CrossRef]
- Woolf, D.C.; Diedericks, R.J. Airway obstruction in infectious mononucleosis. A case report. S Afr Med J 1989, 17, 584–585. [Google Scholar]
- Johnsen, T.; Katholm, M.; Stangerup, S.E. Otolaryngological complications in infectious mononucleosis. J Laryngol Otol 1984, 98, 999–1001. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; De Guido, C.; Pappalardo, M. Retropharyngeal, Parapharyngeal and Peritonsillar Abscesses. Children (Basel) 2022, 26, 618. [Google Scholar] [CrossRef]
- Ravindran, B.; Paul, F.K.; Vyakarnam, P. Acute upper airway obstruction due to tonsillitis necessitating emergency cricothyroidotomy. BMJ Case Rep 2021, 14, e242500. [Google Scholar] [CrossRef]
- Mann, W.; Lange, G. Tonsillectomy for the acute anginous type of infectious mononucleosis. Laryngol Rhinol Otol 1974, 53, 826–830. [Google Scholar]
- Lloyd, A.M.; Reilly, B.K. Infectious Mononucleosis and Upper Airway Obstruction: Intracapsular Tonsillectomy and Adenoidectomy With Microdebrider for Prompt Relief. Ear, Nose & Throat Journal 2020, 100, 958S–960S. [Google Scholar] [CrossRef]
- Stevenson, D.S.; Webster, G.; Stewart, I.A. Acute tonsillectomy in the management of infectious mononucleosis. J Laryngol Otol 1992, 106, 989.991. [Google Scholar] [CrossRef] [PubMed]
- Giger, R.; Landis, B.N.; Dulguerov, P. Haemorrhage risk after quinsy tonsillectomy. Otolaryngol Head Neck Surg 2005, 133, 729–734. [Google Scholar] [CrossRef] [PubMed]
- Liapis, K; Apostolidis, J.; Delimpasis, S. EBV-associated hemophagocytic syndrome. Am J Hematol 2011, 86, 422. [Google Scholar] [CrossRef]
- Maakaroun, N.R.; Moanna, A.; Jacob, J.T.; et al. Viral infections associated with hemophagocytic syndrome. Rev Med Virol 2010, 20, 93–105. [Google Scholar] [CrossRef]
- Janka, G.E.; Schenider, E.M. Modern management of children withhaemophagocytic lymphohistiocytosis. Br J Haematol 2004, 124, 4–14. [Google Scholar] [CrossRef]
- Kong, Q.; Li, M.; Wang, J.; et al. Prognostic scoring system for pediatric Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis based on baseline characteristics: A multicenter retrospective study. Pediatr Blood Cancer 2024, 71, e30772. [Google Scholar] [CrossRef]
- Kwak, A.; Jung, N.; Shim, Y.J.; et al. A retrospective analysis of etiology and outcomes of hemophagocytic lymphohistiocytosis in children and adults. Yeungnam Univ J Med 2021, 38, 208–218. [Google Scholar] [CrossRef]
- Bergsten, E.; Horne, A.; Aricó, M.; et al. Confirmed efficacy of etoposide and dexamethasone in HLH treatment: long-term results of the cooperative HLH-2004 study. Blood 2017, 130, 2728–2738. [Google Scholar] [CrossRef]
- Contreras-Chavez, P.; Anampa-Guzmán, A.; Gaznabi, S.; et al. Epstein-Barr Virus Infection-associated Hemophagocytic Lymphohistiocytosis. Cureus 2020. [Google Scholar] [CrossRef] [PubMed]
- Ishii, E.; Ohga, S.; Imashuku, S.; et al. Nationwide survey of Hemophagocytic lymphohistiocytosis in Japan. Int J Hematol 2007. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.; Wang, Y.; Wang, J.; et al. Epstein-Barr virus-associated hemophagocytic lymphohistiocytosis in adults and adolescents—a life-threatening disease: analysis of 133 cases from a single center. Hematology 2018, 23, 810–816. [Google Scholar] [CrossRef] [PubMed]
- Van Noten, H.; Markowicz, S.; Cappeliez, S.; et al. Infectious Mononucleosis Resulting in Acute Necrotizing Mediastinitis: A Case Report and Literature Review. Eur J Case Rep Intern Med 2020, 7, 001829. [Google Scholar] [CrossRef] [PubMed]
- Klug, T.E.; Greve, T.; Hentze, M. Complications of peritonsillar abscess. Ann Clin Microbiol Antimicrob 2020, 19, 32. [Google Scholar] [CrossRef]
- Geerts, J.W.; van Driel, E.M.; Janssen, M.J. Descending mediastinitis in Epstein-Barr virus infection. J Clin Microbiol 2015. [Google Scholar] [CrossRef] [PubMed]
- Andrianakis, I.A.; Kotanidou, A.N.; Pitaridis, M.T.; et al. Life-threatening bilateral empyema and mediastinitis complicating infectious mononucleosis. Intensive Care Med 2022, 28, 663–664. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, H.D.; Lim, S.C. Predisposing Factors of Complicated Deep Neck Infection: An Analysis of 158 Cases. Yonsei Med J 2007, 48, 55–62. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Axial CT scan showing obstruction of the pharyngeal lumen at the upper (A) and lower third of the oropharynx due to hypertrophic tonsils.
Figure 1.
Axial CT scan showing obstruction of the pharyngeal lumen at the upper (A) and lower third of the oropharynx due to hypertrophic tonsils.
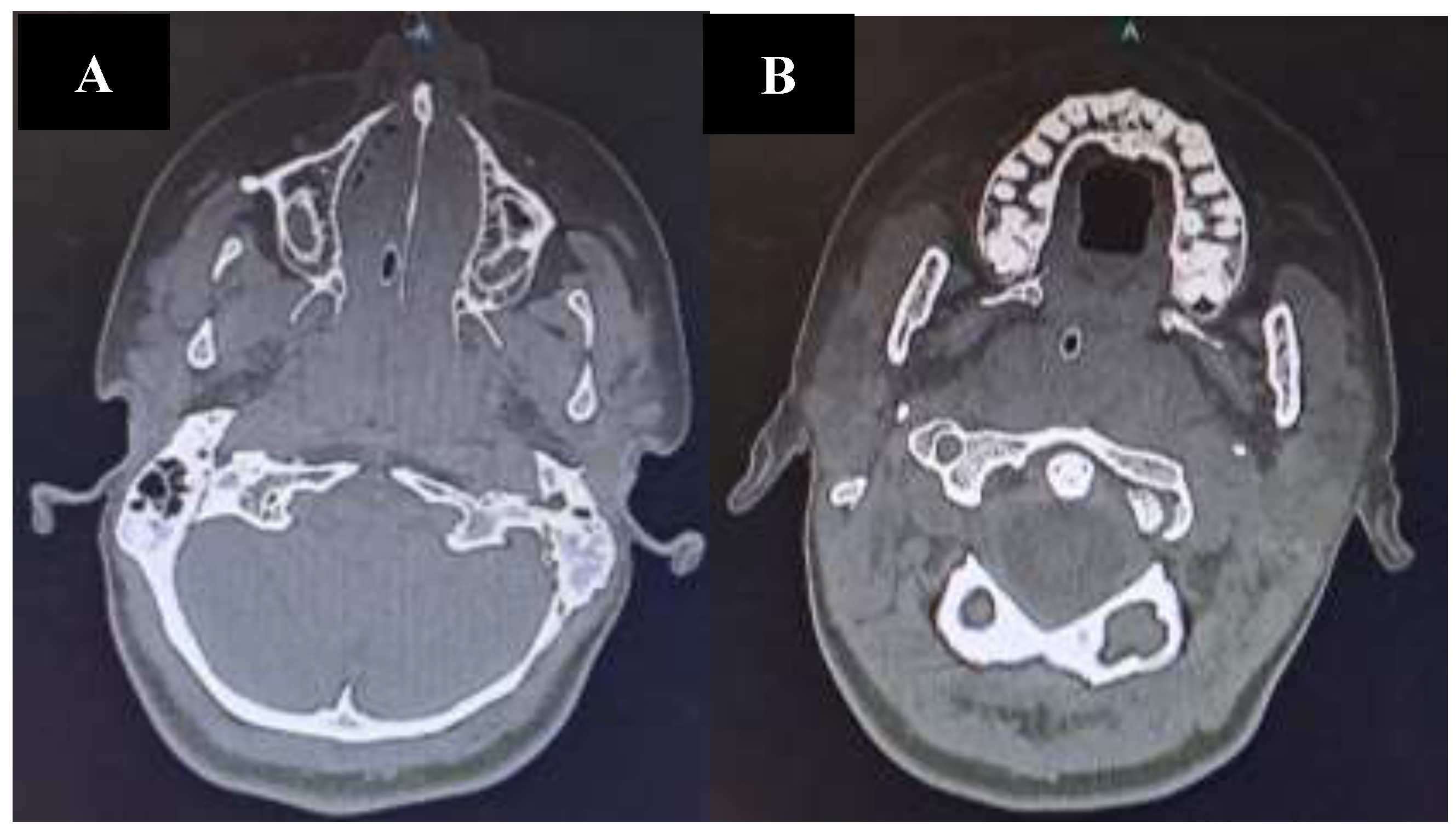
Figure 2.
Axial (A) and coronal (B) CT scan revealed a retropharyngeal abscess protruding into the oropharyngeal lumen.
Figure 2.
Axial (A) and coronal (B) CT scan revealed a retropharyngeal abscess protruding into the oropharyngeal lumen.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



