
Submitted:
16 January 2026
Posted:
19 January 2026
You are already at the latest version
Abstract
Heavy drinking is prevalent in young adulthood, yet its relationship with psychosocial well-being remains com-plex. This study examines the association between heavy drinking and social isolation among young adults and tests whether this relationship varies by sexual orientation. Using pooled, nationally representative data from the 2022 and 2024 Health Information National Trends Survey (HINTS), we analyzed adults aged 18–29 (N = 723). Perceived social isolation was measured using the PROMIS Social Isolation Short Form. Weighted multivariable linear regression models assessed interactions between sexual orientation and heavy drinking occasions (0 vs. 1+), adjusting for sociodemographics and psychological distress. 45.5% reported heavy drinking. Lesbian/gay (B = 5.39, p < .001) and bisexual (B = 1.49, p < .001) young adults reported higher isolation than straight peers; heavy drinking was inversely associated with isolation (B = −1.34, p < .001). A significant interaction indicated that among lesbian/gay young adults, heavy drinking was associated with lower perceived isolation (B = −5.90, p < .001). These findings suggest that alcohol-centered social spaces may play a distinct role in fostering community belonging for lesbian/gay young adults. Interventions should account for the social meanings of alcohol use to avoid unintentionally increasing isolation among sexual minoritized populations.
Keywords:
social isolation
; intersectionality
; young adults
; heavy episodic drinking
; alcohol
; sexual minorities
1. Introduction
Heavy episodic drinking, defined as alcohol consumption of 5 or more drinks for males or 4 or more drinks for females within 2 hours, is highly prevalent in the United States (U.S.) with 7.9% of adolescents and young adults aged 12-20 reporting heavy drinking episodes in 2024 and no significant change in these rates over the past 4 years (Substance Abuse and Mental Health Services Administration [SAMHSA], 2025). Developmental research consistently demonstrates that alcohol use escalates during young adulthood, with heavy episodic drinking peaking as young adults navigate transitions related to education, employment, and social belonging (Brown et al., 2008, 2009; Quigley & Marlatt, 1996; Schulenberg & Maggs, 2002). Heavy drinking in young adulthood has been linked to adverse mental health outcomes, including elevated symptoms of depression and anxiety, as well as increased risk for alcohol-related problems and longer-term substance use disorders (Gates et al., 2016; White & Jackson, 2004). At the same time, alcohol use in this age group is deeply embedded in social contexts, frequently occurring in peer-centered environments where drinking may function as a mechanism for social facilitation, stress reduction, and perceived connection (Brook & Willoughby, 2016; White & Jackson, 2004). This dual role of alcohol use underscores that while heavy drinking is associated with significant psychological harm, it may also coincide with greater social engagement and perceived connectedness, complicating its relationship with psychosocial well-being during the transition to adulthood (Mathes Winnicki et al., 2023; Villar et al., 2022).
Perceived social isolation refers to an individual’s subjective sense of social disconnection, loneliness, or lack of belonging and is conceptually distinct from objective indicators of social isolation such as network size, frequency of social contact, or living arrangements. Importantly, individuals may report high levels of perceived isolation despite having extensive social networks, underscoring the primacy of perceived social quality over structural measures of social integration (Cacioppo & Hawkley, 2009; Cadigan et al., 2023). Perceived social isolation is particularly salient during young adulthood, a developmental period in which peer affiliation, social acceptance, and identity-affirming relationships are central to psychological well-being and emerging adult functioning. Disruptions to perceived connectedness during this life stage have been linked to elevated psychological distress, including depressive and anxiety symptoms, as well as maladaptive coping behaviors such as increased substance use and alcohol consumption (Cadigan et al., 2023; Rapier et al., 2019). Growing evidence further suggests that perceived social isolation may shape longer-term health risk trajectories by influencing stress processes, emotional regulation, and health behaviors across the life course (Campagne, 2019). In population-based research, perceived social isolation is increasingly assessed using the Patient-Reported Outcomes Measurement Information System (PROMIS) Social Isolation measure, a validated instrument grounded in item response theory that captures subjective social disconnection and allows for standardized comparisons across populations and studies (Hahn et al., 2010). PROMIS-based measures have been widely applied in behavioral and public health research, including studies of young adults and digital social environments, supporting their utility for examining social isolation as a critical psychosocial determinant of health (Primack et al., 2017; Thakur et al., 2025; Whaite et al., 2018).
Sexual minority stress theory provides a central framework for understanding disparities in social and mental health among sexual minoritized individuals by positing that stigma-related stressors, including discrimination, social exclusion, identity concealment, and internalized stigma, operate in addition to general life stressors to undermine psychological well-being (Alessi, 2014; Hoy-Ellis, 2023; Pitoňák, 2017). These chronic stress processes are closely linked to experiences of social disconnection, as sexual minoritized individuals may encounter rejection within families, peer networks, and broader social institutions, or may limit social engagement to avoid stigma exposure (Pachankis et al., 2020). Consistent with this framework, lesbian, gay, and bisexual young adults report higher levels of loneliness, perceived social isolation, and psychological distress compared with their heterosexual peers, disparities that emerge early and persist across developmental stages (Argyriou et al., 2021; Garcia et al., 2020). Importantly, sexual minoritized populations are not monolithic; meaningful heterogeneity exists across sexual identity groups, with bisexual individuals often experiencing distinct and, in some cases, heightened vulnerability related to identity invisibility, marginalization from both heterosexual and lesbian/gay communities, and differential coping strategies (McCormack, 2023). Such heterogeneity extends to health behaviors and social contexts, underscoring the importance of disaggregating sexual orientation groups when examining social isolation, mental health, and related risk behaviors among young adults.
A substantial body of research documents elevated alcohol use and heavier drinking patterns among sexual minoritized populations, particularly among young adults and bisexual individuals, who often report higher prevalence of heavy episodic drinking and alcohol-related consequences compared with heterosexual peers (Cerezo et al., 2020; Dyar & Kaysen, 2022; Talley et al., 2016). These disparities are frequently framed within minority stress processes, wherein alcohol use may function as a coping strategy for managing stigma-related stressors such as discrimination, identity concealment, and internalized stigma (Kalb et al., 2018; Miller et al., 2025). At the same time, alcohol use among sexual minoritized individuals is deeply embedded in social contexts. Alcohol-centered venues, including bars, clubs, and social gatherings, have historically served as critical spaces for community formation, identity affirmation, and access to social support in the context of broader societal marginalization (Fairlie et al., 2018; Parks & Heller, 2013). Engagement in these settings may therefore reflect social affiliation and community connectedness rather than exclusively maladaptive coping, particularly among young adults navigating identity development and belonging (Cogger et al., 2012; Feinstein et al., 2017). This dual function of alcohol use suggests that the association between heavy episodic drinking and perceived social isolation may differ by sexual orientation, with heavy drinking potentially coinciding with lower perceived isolation for some sexual minoritized groups while remaining a marker of psychological distress for others, underscoring the importance of examining effect heterogeneity across sexual identity groups.
Despite extensive research on alcohol use, mental health, and social well-being among young adults and sexual minoritized populations, several critical gaps remain. First, much of the existing literature has focused on psychological distress or substance use outcomes independently, with comparatively limited attention to perceived social isolation as a distinct psychosocial determinant that may both shape and be shaped by alcohol use behaviors. Second, studies examining alcohol use among sexual minoritized populations frequently aggregate lesbian, gay, and bisexual individuals, obscuring important heterogeneity in social contexts, coping strategies, and health behaviors across sexual identity groups. Third, few population-based studies explicitly test whether the association between heavy drinking and psychosocial outcomes differs by sexual orientation, despite theoretical and empirical evidence suggesting that alcohol use may function both as a coping response to minority stress and as a mechanism for social affiliation and community connectedness. Finally, much of the existing evidence is derived from convenience samples or pre-pandemic data, limiting generalizability and relevance to contemporary social environments. Addressing these gaps using nationally representative data and analytic approaches that allow for effect modification is essential to advancing understanding of how heavy episodic drinking intersects with perceived social isolation across sexual identity groups during young adulthood.
The purpose of this study was to examine the association between heavy drinking occasions and perceived social isolation among young adults aged 18–29 in the U.S., and to assess whether this association differs by sexual orientation. Using pooled, nationally representative data from the 2022 and 2024 cycles of the Health Information National Trends Survey (HINTS), this study extends prior research by focusing on perceived social isolation as a key psychosocial outcome and by explicitly testing effect heterogeneity across sexual identity groups. Guided by minority stress theory and social affiliation frameworks, we hypothesized that sexual minoritized young adults would report higher levels of perceived social isolation than their straight/heterosexual counterparts. We further hypothesized that heavy drinking would be associated with perceived social isolation overall, but that the magnitude and direction of this association would vary by sexual orientation, reflecting differences in social contexts, coping mechanisms, and community connectedness across lesbian/gay, bisexual, and straight young adults.
2. Materials and Methods
2.1. Study Design and Data
This study used data from the Health Information National Trends Survey (HINTS), pooling responses from HINTS 6 (2022) and HINTS 7 (2024). HINTS is a nationally representative, cross-sectional survey administered by the National Cancer Institute to monitor how U.S. adults aged 18 years and older seek, access, and use health information, along with related health behaviors (National Cancer Institute, 2025). The survey samples the noninstitutionalized U.S. adult population across all 50 states and the District of Columbia using a stratified, probability-based sampling design. Both survey cycles employ comparable methodologies, enabling pooled analyses across years to increase statistical power and enhance population-level inference. Detailed information regarding sampling procedures, survey administration, and weighting strategies is available in the publicly accessible HINTS methodology documentation. This study met criteria for exemption from institutional review board (IRB) review.
2.2. Measures
2.2.1. Sociodemographic Measures
Participants reported a range of sociodemographic characteristics that were examined in relation to heavy drinking occasions (0 vs. 1+). Analyses were restricted to a subset of young adults aged 18–29 years, with age treated as a continuous variable. Biological sex, or sex assigned at birth, was self-reported and categorized as male or female. Sexual orientation was classified as lesbian/gay, straight, or bisexual; respondents identifying as something else were excluded due to small cell sizes. Race and ethnicity were measured using standard federal classification categories and grouped as non-Hispanic (NH) White, NH Black, Hispanic, NH Asian, and NH other.
Educational attainment reflected the highest level of education completed and was categorized as less than high school, high school graduate, some college or associate degree, and bachelor’s degree or higher. Household income was assessed in six categories: < $20,000; $20,000 – < $35,000; $35,000 – < $50,000; $50,000 – < $75,000; $75,000 – < $100,000; and $100,000 +. Household composition was captured as the number of adults living in the household and dichotomized as 1 versus 2 + adults. Survey year (HINTS 6 [2022] vs. 7 [2024]) was included as a covariate in pooled analyses to account for potential secular trends and between-cycle differences across survey waves.
2.2.2. Psychological Distress
Symptoms of depression and anxiety were measured using the Patient Health Questionnaire-4 (PHQ-4), an established ultra-brief screening instrument for psychological distress (Kroenke et al., 2009). The PHQ-4 includes four items derived from longer validated scales, with two items capturing anxiety symptoms (General Anxiety Disorder [GAD]-2) and two assessing depressive symptoms (PHQ-2). Respondents indicated how frequently they experienced each symptom during the prior two weeks using a four-point response scale ranging from 0 (“not at all”) to 3 (“nearly every day”).
Item responses were summed to create a total score ranging from 0 to 12, with higher values reflecting greater overall distress. The PHQ-4 has been shown to demonstrate strong psychometric properties and is commonly used in population-based and clinical research to efficiently assess mental health symptom burden.
2.2.3. Perceived Social Isolation
Perceived social isolation was assessed using the PROMIS Social Isolation Short Form, which captures individuals’ subjective experiences of social disconnection and loneliness (Hahn et al., 2010). The measure includes items reflecting feelings of exclusion, lack of companionship, and social detachment. Participants rated how often they experienced each feeling using a five-point Likert scale, with response options typically ranging from “never” to “always.” Higher scores indicate greater perceived isolation.
Raw scores were converted to PROMIS T-scores standardized to the U.S. general population (mean = 50, SD = 10), allowing for comparability across studies and populations. T-scores above 50 represent higher-than-average levels of perceived social isolation, whereas scores below 50 indicate lower perceived isolation. The PROMIS Social Isolation measure is grounded in item response theory and has demonstrated strong reliability and validity despite its brief format, making it well suited for population health and behavioral research examining social disconnection and related health outcomes.
2.3. Statistical Analysis
All analyses incorporated the complex sampling structure of the HINTS survey. Person-level final weights were applied to produce estimates representative of the U.S. adult population. These weights account for unequal selection probabilities, survey nonresponse, and alignment with national population benchmarks using iterative proportional fitting procedures. To obtain valid variance estimates, the set of HINTS-provided jackknife replicate weights was used, consistent with the survey’s stratified, two-stage sampling design. Prior to analysis, the survey design was specified by assigning the final person-level weight as the probability weight and incorporating all 100 replicate weights over both cycles for variance estimation.
Weighted descriptive statistics, including frequencies, proportions, means, and standard errors, were calculated to summarize sample characteristics. Descriptive analyses were conducted for the overall sample and stratified by reported number of heavy drinking occasions. Group differences in categorical variables were evaluated using Rao–Scott adjusted chi-square tests, while differences in continuous measures (age, PHQ-4 scores and PROMIS Social Isolation T-scores) were assessed using weighted one-way analysis of variance (ANOVA).
Weighted, multivariable linear regression models were estimated to examine the association between heavy drinking occasions and perceived social isolation. Perceived social isolation, operationalized as the PROMIS Social Isolation T-score, was modeled as a continuous outcome. All models accounted for the complex HINTS survey design through the application of person-level sampling weights and replicate weights. An interaction term between sexual orientation and heavy drinking occasions (0 vs. 1 +) was included to assess whether the association between heavy drinking and social isolation differed by sexual orientation. Models were adjusted for sociodemographic covariates and survey year. Adjusted regression coefficients and 95% confidence intervals are reported. All statistical analyses were conducted using Stata 19.5 (StataCorp, College Station, TX, USA).
3. Results
3.1. Sample Distribution and Bivariate Comparisons
The analytic sample included 723 U.S. adults aged 18–29 pooled from the 2022 and 2024 HINTS cycles (Table 1). Overall, the weighted mean age was 23.6 years, and the standard error (SE) was 0.05. Just over half of respondents identified as female (52.1%), and the majority identified as straight (84.7%), followed by bisexual (10.8%) and lesbian/gay (4.5%) identities. Slightly more than half of the sample identified as NH White (53.3%), with the remainder identifying as Hispanic (22.3%), NH Asian (11.0%), NH Black (8.6%), or another NH race/ethnicity (5.0%). Approximately one-third of respondents had completed a bachelor’s degree or higher, and household income was broadly distributed across categories. Most respondents lived in households with two or more adults (88.4%).
Nearly half of the sample reported one or more heavy drinking occasions (45.5%; Table 1). Significant differences by heavy drinking status were observed across multiple sociodemographic characteristics. Individuals reporting one or more heavy drinking occasions were older on average than those reporting none (p < .001). Heavy drinking was also more prevalent among males than females (49.7% vs. 40.2%, p < .001) and varied by sexual orientation (p = .012), with lower prevalence observed among lesbian/gay (38.2%) respondents compared with bisexual (44.9%) and straight (46.2%) respondents.
Heavy drinking occasions differed significantly across racial and ethnic groups (p < .001), with higher prevalence among Hispanic (51.3%) and NH White (49.4%) respondents and lower prevalence among NH Black (27.4%) and NH Asian (28.1%) respondents. Educational attainment was also associated with heavy drinking status (p < .001), with higher prevalence among those with less than a high school education (63.0%) and those with a college degree or higher (51.5%). Household income demonstrated a graded association with heavy drinking (p < .001), with the highest prevalence observed among respondents in the highest income category (65.0%). The number of adults in the household was not significantly associated with heavy drinking occasions.
Heavy drinking prevalence differed by survey cycle, with a greater proportion of respondents reporting one or more heavy drinking occasions in 2024 compared with 2022 (p < .001). In bivariate comparisons of psychosocial measures, individuals reporting one or more heavy drinking occasions had significantly higher psychological distress scores as measured by the PHQ-4 (p < .001). Perceived social isolation also differed by heavy drinking status, with lower PROMIS Social Isolation T-scores observed among those reporting one or more heavy drinking occasions compared with those reporting none (p = .025).
3.2. Weighted Linear Regressions
Table 2 presents weighted, adjusted linear regression models estimating associations with perceived social isolation, measured by PROMIS Social Isolation T-scores, among U.S. adults aged 18–29. Model 1 included main effects only, while Model 2 added an interaction between sexual orientation and heavy drinking occasions to assess effect modification. In Model 1, several sociodemographic factors were significantly associated with social isolation. Older age was associated with lower social isolation scores (B = -0.11, SE = 0.03, p < .001), whereas males reported higher isolation than females (B = 1.32, SE = 0.22, p < .001). Compared with straight respondents, lesbian/gay (B = 5.39, SE = 0.59, p < .001) and bisexual individuals (B = 1.49, SE = 0.34, p < .001) reported significantly higher social isolation. NH Black (B = -3.71, SE = 0.64, p < .001) and Hispanic respondents (B = -1.92, SE = 0.24, p < .001) reported lower social isolation than NH White respondents, while NH Asian (B = 1.17, SE = 0.49, p < .05) and NH Other respondents (B = 4.26, SE = 0.47, p < .001) reported higher isolation. Lower household income was associated with higher social isolation, particularly among respondents earning less than $20,000 annually (B = 2.79, SE = 0.50, p < .001) compared to those earning over $100,000. Lower educational attainment (less than high school) was also associated with lower isolation scores relative to college graduates (B = -1.40, SE = 0.62, p < .05). Survey cycle was also significant, with respondents in the 2022 cycle reporting slightly higher isolation than those surveyed in 2024 (B = 0.62, SE = 0.30, p < .05). Psychological distress was strongly and positively associated with social isolation, with each one-point increase in PHQ-4 score corresponding to a substantial increase in PROMIS Social Isolation T-score (B = 2.15, SE = 0.05, p < .001). Heavy drinking occasions were inversely associated with social isolation; respondents reporting one or more heavy drinking occasions had significantly lower isolation scores (B = -1.34, SE = 0.19, p < .001) compared with those reporting none.
Figure 1 displays predicted PROMIS Social Isolation T-scores by sexual orientation and heavy drinking status among U.S. adults aged 18–29 illustrating the association between heavy drinking and perceived social isolation by sexual orientation, representing the significant interaction observed in the regression analysis (Model 2). Social isolation is plotted separately for lesbian/gay, straight, and bisexual respondents, with blue bars representing individuals reporting no heavy drinking occasions and red bars representing those reporting one or more heavy drinking occasions. Error bars indicate 95% confidence intervals. Among lesbian/gay respondents, predicted social isolation scores were substantially higher for those reporting no heavy drinking compared with those reporting heavy drinking, suggesting a marked inverse association between heavy drinking and perceived isolation in this group. For straight respondents, social isolation scores were slightly higher among those with no heavy drinking, but differences were smaller than for lesbian/gay respondents. Among bisexual respondents, predicted social isolation was similar between heavy drinking and non-heavy drinking groups, with overlapping confidence intervals, indicating little difference by drinking status.
4. Discussion
Using nationally representative data from the 2022 and 2024 cycles of the HINTS, this study examined associations between heavy drinking occasions and perceived social isolation among U.S. young adults aged 18–29, with a particular focus on differences by sexual orientation. Consistent with minority stress theory and prior research, lesbian/gay and bisexual young adults reported higher levels of perceived social isolation than straight peers, even after adjustment for sociodemographic characteristics and psychological distress. Psychological distress was strongly and positively associated with perceived social isolation across models, underscoring the close linkage between mental health symptom burden and subjective social disconnection during young adulthood. In contrast, heavy drinking occasions were inversely associated with perceived social isolation overall, a finding that highlights the complex and potentially bidirectional relationship between alcohol use and social well-being in this life stage.
The primary contribution of this study is the identification of a significant interaction between sexual orientation and heavy drinking occasions. Among lesbian/gay young adults, reporting one or more heavy drinking occasions was associated with substantially lower perceived social isolation compared with lesbian/gay peers who reported no heavy drinking. This pattern was not observed among bisexual young adults, for whom perceived social isolation did not differ by heavy drinking status, nor was it as pronounced among straight respondents. These findings suggest that the social meaning and psychosocial correlates of heavy drinking may differ across sexual identity groups, with heavy drinking potentially reflecting social integration or community engagement rather than solely maladaptive coping for some sexual minoritized individuals.
The inverse association between heavy drinking and perceived social isolation among lesbian/gay young adults may be understood within the context of historically alcohol-centered LGBTQ+ social spaces. In the face of widespread structural stigma, exclusion from mainstream institutions, and limited access to affirming public spaces, bars, clubs, and nightlife venues have long served as critical sites of identity affirmation, community formation, and mutual support for lesbian and gay individuals (Beemyn, 2013; Wolfe, 1992). Sociological and historical scholarship highlights how queer nightlife environments function not merely as leisure spaces but as socially meaningful contexts where belonging, visibility, and collective identity are actively produced (Ghaziani, 2022, 2025; Hilderbrand et al., 2025). Within these environments, alcohol use is often normative and intertwined with social participation, such that engagement in drinking-related activities may coincide with greater perceived social integration and reduced feelings of isolation (Hunt et al., 2019). Empirical work further suggests that LGBTQ+ bars may operate as a safe haven, particularly in socially conservative contexts, offering opportunities for connection and emotional support that are less readily available elsewhere (Croff et al., 2017). In this context, abstaining from or avoiding alcohol-centered social spaces may inadvertently constrain access to key avenues of social interaction and community belonging, potentially contributing to higher perceived social isolation among lesbian/gay individuals who do not engage in heavy drinking.
In contrast to lesbian/gay young adults, bisexual young adults may experience distinct social and structural vulnerabilities that limit the extent to which alcohol-related social participation translates into perceived connectedness. Bisexual individuals often face marginalization from both straight/heterosexual and gay/lesbian communities, as well as identity invisibility and erasure, which can reduce access to affirming social spaces and community support (Alessi, 2014; McCormack, 2023; Pachankis et al., 2020). Consequently, participation in alcohol-centered social environments may not confer the same sense of belonging or reductions in perceived isolation observed among lesbian/gay peers. Instead, heavy drinking among bisexual young adults may be more strongly linked to coping with minority stress or normative young adult drinking behaviors rather than social integration, yielding no clear association with perceived social isolation (Kalb et al., 2018; Talley et al., 2016). This pattern underscores the heterogeneity within sexual minoritized populations and highlights the importance of considering identity-specific social and structural contexts when examining behavioral and psychosocial outcomes.
Notably, heavy drinking was associated with lower perceived social isolation in the overall sample, even after adjustment for psychological distress. This finding aligns with a growing body of literature indicating that alcohol use during young adulthood cannot be understood solely as an indicator of psychosocial vulnerability (Quigley & Marlatt, 1996; Schulenberg & Maggs, 2002; White & Jackson, 2004). Emerging adults often engage in alcohol consumption within peer-oriented contexts where drinking serves both social and recreational functions, facilitating social bonding, identity exploration, and perceived connectedness (Brook & Willoughby, 2016; Mathes Winnicki et al., 2023; Villar et al., 2022). Consequently, alcohol use may simultaneously function as a risk behavior and a marker of social engagement, highlighting the dual roles of drinking in young adulthood. These complexities complicate public health narratives that frame heavy drinking exclusively as maladaptive and underscore the importance of considering social context and subgroup heterogeneity when evaluating alcohol-related outcomes (Brown et al., 2008; Gates et al., 2016).
4.1. Limitations and Strengths
Several limitations should be considered when interpreting these findings. First, the cross-sectional design precludes causal inference, and it is not possible to determine whether heavy drinking reduces perceived social isolation, whether lower isolation increases opportunities for heavy drinking, or whether both are shaped by unmeasured factors such as social network characteristics. Second, heavy drinking was assessed using a dichotomous measure of one or more occasions, which does not capture frequency, intensity, or drinking context. Third, sexual orientation categories were limited by sample size, precluding examination of additional identities or intersections with sex. Fourth, all measures were self-reported and may be subject to recall or social desirability bias. Finally, while HINTS provides national representativeness, its primary focus is health information behaviors, which may limit the depth of alcohol-related measures.
Despite these limitations, this study has several important strengths, including the use of recent, nationally representative data; validated measures of perceived social isolation; and analytic approaches that explicitly test effect modification by sexual orientation. By focusing on perceived social isolation rather than objective social indicators alone, this study highlights a critical psychosocial dimension that may shape both mental health and substance use trajectories among young adults.
4.2. Intervention and Practice Implications
These findings have meaningful intervention and practice implications. Efforts to reduce alcohol-related harm among sexual minority young adults should be attentive to the social functions that alcohol use may serve, particularly for lesbian/gay individuals who rely on alcohol-centered spaces for community and belonging. Interventions that focus exclusively on reducing alcohol consumption without addressing underlying social needs may risk exacerbating social isolation. Expanding access to alcohol-free, identity-affirming social spaces and strengthening community-based sources of connection may represent important complementary strategies for promoting well-being while reducing alcohol-related risk.
5. Conclusions
This study demonstrates that the association between heavy episodic drinking and perceived social isolation among young adults is not uniform but varies meaningfully by sexual orientation. Specifically, heavy drinking was associated with lower perceived social isolation among lesbian/gay young adults, whereas no such association was observed for bisexual peers. These findings highlight the importance of moving beyond one-size-fits-all models of risk and underscore the need to consider the broader social and community contexts in which alcohol use occurs. For lesbian/gay young adults, participation in alcohol-centered social spaces may provide opportunities for identity affirmation, peer connection, and community engagement, potentially mitigating feelings of isolation. In contrast, bisexual individuals often face unique structural and social vulnerabilities, including marginalization from both straight/heterosexual and gay/lesbian communities and reduced access to affirming social spaces, which may limit the extent to which alcohol-related participation confers social benefits. These results emphasize that the psychosocial significance of alcohol use in young adulthood is shaped by intersecting factors of identity, social environment, and subgroup-specific experiences, rather than representing a universally maladaptive behavior.
Author Contributions
[redacted].
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical approval was not required for this study as all data are deidentified, publicly available and deemed not human subject research.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are openly available at https:// https://hints.cancer.gov/ (accessed on 1 October 2025).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HINTS | Health Information National Trends Survey |
| PHQ | Personal Health Questionnaire |
| PROMIS | Patient-Reported Outcomes Measurement Information System |
References
- Alessi, E. J. A framework for incorporating minority stress theory into treatment with sexual minority clients. Journal of Gay & Lesbian Mental Health 2014, 18(1), 47–66. [Google Scholar] [CrossRef]
- Argyriou, A.; Goldsmith, K. A.; Rimes, K. A. Mediators of the disparities in depression between sexual minority and heterosexual individuals: A systematic review. Archives of Sexual Behavior 2021, 50(3), 925–959. [Google Scholar] [CrossRef] [PubMed]
- Beemyn, B. Creating a place for ourselves: Lesbian, gay, and bisexual community histories; Routledge, 2013. [Google Scholar]
- Brook, C. A.; Willoughby, T. Social anxiety and alcohol use across the university years: Adaptive and maladaptive groups. Developmental Psychology 2016, 52(5), 835. [Google Scholar] [CrossRef]
- Brown, S. A.; McGue, M.; Maggs, J.; Schulenberg, J.; Hingson, R.; Swartzwelder, S.; Martin, C.; Chung, T.; Tapert, S. F.; Sher, K. A developmental perspective on alcohol and youths 16 to 20 years of age. Pediatrics 2008, 121 (Supplement_4), S290–S310. [Google Scholar] [CrossRef]
- Brown, S. A.; McGue, M.; Maggs, J.; Schulenberg, J.; Hingson, R.; Swartzwelder, S.; Martin, C.; Chung, T.; Tapert, S. F.; Sher, K. Underage alcohol use: Summary of developmental processes and mechanisms: ages 16–20. Alcohol Research & Health 2009, 32(1), 41. [Google Scholar]
- Cacioppo, J. T.; Hawkley, L. C. Perceived social isolation and cognition. Trends in Cognitive Sciences 2009, 13(10), 447–454. [Google Scholar] [CrossRef] [PubMed]
- Cadigan, J. M.; Calhoun, B. H.; Rhew, I. C.; Lee, C. M. Trajectories of loneliness during COVID-19 pandemic and associations with mental health and substance use. Journal of Research on Adolescence 2023, 33(3), 816–827. [Google Scholar] [CrossRef]
- Campagne, D. M. Stress and perceived social isolation (loneliness). Archives of Gerontology and Geriatrics 2019, 82, 192–199. [Google Scholar] [CrossRef]
- Cerezo, A.; Williams, C.; Cummings, M.; Ching, D.; Holmes, M. Minority stress and drinking: Connecting race, gender identity and sexual orientation. The Counseling Psychologist 2020, 48(2), 277–303. [Google Scholar] [CrossRef]
- Cogger, A.; Conover, K. J.; Israel, T. Factors influencing alcohol use among sexual minority women in a non-urban community: A mixed methods study. Journal of LGBT Issues in Counseling 2012, 6(4), 293–309. [Google Scholar] [CrossRef]
- Croff, J. M.; Hubach, R. D.; Currin, J. M.; Frederick, A. F. Hidden rainbows: Gay bars as safe havens in a socially conservative area since the Pulse nightclub massacre. Sexuality Research and Social Policy 2017, 14(2), 233–240. [Google Scholar] [CrossRef]
- Dyar, C.; Kaysen, D. Multiple diverse drinking trajectories among sexual minority women: Unique and joint prediction by minority stress and social influence risk factors. Addictive Behaviors 2022, 129, 107273. [Google Scholar] [CrossRef]
- Fairlie, A. M.; Feinstein, B. A.; Lee, C. M.; Kaysen, D. Subgroups of young sexual minority women based on drinking locations and companions and links with alcohol consequences, drinking motives, and LGBTQ-related constructs. Journal of Studies on Alcohol and Drugs 2018, 79(5), 741–750. [Google Scholar] [CrossRef]
- Feinstein, B. A.; Dyar, C.; London, B. Are outness and community involvement risk or protective factors for alcohol and drug abuse among sexual minority women? Archives of Sexual Behavior 2017, 46(5), 1411–1423. [Google Scholar] [CrossRef]
- Garcia, J.; Vargas, N.; Clark, J. L.; Magaña Álvarez, M.; Nelons, D. A.; Parker, R. G. Social isolation and connectedness as determinants of well-being: Global evidence mapping focused on LGBTQ youth. Global Public Health 2020, 15(4), 497–519. [Google Scholar] [CrossRef]
- Gates, J. R.; Corbin, W. R.; Fromme, K. Emerging adult identity development, alcohol use, and alcohol-related problems during the transition out of college. Psychology of Addictive Behaviors 2016, 30(3), 345. [Google Scholar] [CrossRef]
- Ghaziani, A. Belonging in gay neighborhoods and queer nightlife. In Introducing the New Sexuality Studies; Routledge, 2022; pp. 540–550. [Google Scholar]
- Ghaziani, A. The sociology of queer nightlife. The Sociological Quarterly 2025, 66(4), 661–674. [Google Scholar] [CrossRef]
- Hahn, E. A.; DeVellis, R. F.; Bode, R. K.; Garcia, S. F.; Castel, L. D.; Eisen, S. V.; Bosworth, H. B.; Heinemann, A. W.; Rothrock, N.; Cella, D. Measuring social health in the patient-reported outcomes measurement information system (PROMIS): item bank development and testing. Quality of Life Research 2010, 19(7), 1035–1044. [Google Scholar] [CrossRef]
- Hilderbrand, L.; Adeyemi, K.; Cartier, M.; Garcia-Mispireta, L. M.; Ghaziani, A.; Gieseking, J. J.; Greene, T.; Khubchandani, K.; Mattson, G.; Rivera-Servera, R. H. The night is still young: A cross-disciplinary forum on Queer nightlife studies. The Sociological Quarterly 2025, 66(4), 887–909. [Google Scholar] [CrossRef]
- Hoy-Ellis, C. P. Minority stress and mental health: A review of the literature. Journal of Homosexuality 2023, 70(5), 806–830. [Google Scholar] [CrossRef] [PubMed]
- Hunt, G.; Antin, T.; Sanders, E.; Sisneros, M. Queer youth, intoxication and queer drinking spaces. Journal of Youth Studies 2019, 22(3), 380–400. [Google Scholar] [CrossRef]
- Kalb, N.; Roy Gillis, J.; Goldstein, A. L. Drinking to cope with sexual minority stressors: Understanding alcohol use and consequences among LGBQ emerging adults. Journal of Gay & Lesbian Mental Health 2018, 22(4), 310–326. [Google Scholar] [CrossRef]
- Kroenke, K; Spitzer, RL; Williams, JB; Löwe, B. An ultra-brief screening scale for anxiety and depression: the PHQ-4. Psychosomatics 2009, 50(6), 613–21. [Google Scholar]
- Mathes Winnicki, B. M.; Hinds, Z.; Newberger, N. G.; Livingston, N. A. Prospective associations between perceived social connection and alcohol use: A scoping review. Addiction Research & Theory 2023, 31(4), 250–259. [Google Scholar]
- McCormack, M. Issues in bisexual men’s lives: Identity, health and relationships. Current Opinion in Psychology 2023, 49, 101501. [Google Scholar] [CrossRef]
- Miller, L. A.; Åkerlund, A.; Fischer, S. The Role of Community Connectedness in Understanding the Connection Between LGBTQ+ Minority Stress and Problem Drinking. Substance Use & Misuse 2025, 1–11. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Health Information National Trends Survey. 2025. Available online: https://hints.cancer.gov/ (accessed on 1 October 2025).
- Pachankis, J. E.; Mahon, C. P.; Jackson, S. D.; Fetzner, B. K.; Bränström, R. Sexual orientation concealment and mental health: A conceptual and meta-analytic review. Psychological Bulletin 2020, 146(10), 831. [Google Scholar] [CrossRef]
- Parks, C. A.; Heller, N. R. The influence of early drinking contexts on current drinking among adult lesbian and bisexual women. Journal of the American Psychiatric Nurses Associaton 2013, 19(5), 241–254. [Google Scholar] [CrossRef] [PubMed]
- Pitoňák, M. Mental health in non-heterosexuals: Minority stress theory and related explanation frameworks review. Mental Health & Prevention 2017, 5, 63–73. [Google Scholar] [CrossRef]
- Primack, B. A.; Shensa, A.; Sidani, J. E.; Whaite, E. O.; yi Lin, L.; Rosen, D.; Colditz, J. B.; Radovic, A.; Miller, E. Social media use and perceived social isolation among young adults in the US. American Journal of Preventive Medicine 2017, 53(1), 1–8. [Google Scholar] [CrossRef] [PubMed]
- Quigley, L. A.; Marlatt, G. A. Drinking among young adults: Prevalence, patterns, and consequences. Alcohol Health and Research World 1996, 20(3), 185. [Google Scholar]
- Rapier, R.; McKernan, S.; Stauffer, C. S. An inverse relationship between perceived social support and substance use frequency in socially stigmatized populations. Addictive Behaviors Reports 2019, 10, 100188. [Google Scholar] [CrossRef]
- Schulenberg, J. E.; Maggs, J. L. A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. Journal of Studies on Alcohol 2002, Supplement(14), 54–70. [Google Scholar] [CrossRef] [PubMed]
- Substance Abuse and Mental Health Services Administration. 2024 Companion infographic report: Results from the 2021 to 2024 National Surveys on Drug Use and Health (SAMHSA Publication No. PEP25-07-006). 2025. Available online: https://www.samhsa.gov/data/report/2022-nsduh-annual-national-report (accessed on 1 October 2025).
- Talley, A. E.; Gilbert, P. A.; Mitchell, J.; Goldbach, J.; Marshall, B. D.; Kaysen, D. Addressing gaps on risk and resilience factors for alcohol use outcomes in sexual and gender minority populations. Drug and Alcohol Review 2016, 35(4), 484–493. [Google Scholar] [CrossRef] [PubMed]
- Thakur, M.; Mathiason, M. A.; Kim, C.; Pieczkiewicz, D.; Austin, R.; Rajamani, S. Social isolation, social media use, quality of health care, and trust in health care system: Findings from a National Health Information Survey. CIN: Computers, Informatics, Nursing 2025, 10.1097. [Google Scholar] [CrossRef]
- Villar, E.; Martínez-López, Z.; Mayo, M. E.; Braña, T.; Rodríguez, M.; Tinajero, C. A systematic review and narrative synthesis of the relationship between social support and binge drinking among adolescents and emerging adults. Youth 2022, 2(4), 570–586. [Google Scholar] [CrossRef]
- Whaite, E. O.; Shensa, A.; Sidani, J. E.; Colditz, J. B.; Primack, B. A. Social media use, personality characteristics, and social isolation among young adults in the United States. Personality and Individual Differences 2018, 124, 45–50. [Google Scholar] [CrossRef]
- White, H. R.; Jackson, K. Social and psychological influences on emerging adult drinking behavior. Alcohol Research & Health 2004, 28(4), 182. [Google Scholar]
- Wolfe, M. Invisible women in invisible places: Lesbians, lesbian bars, and the social production of people/environment relationships. Architecture and Behavior 1992, 8(2), 137–158. [Google Scholar]
Figure 1.
Significant interaction between sexual orientation and heavy drinking occasions predicting PROMIS Social Isolation T-score among U.S. adults aged 18-29 (p < .001).
Figure 1.
Significant interaction between sexual orientation and heavy drinking occasions predicting PROMIS Social Isolation T-score among U.S. adults aged 18-29 (p < .001).
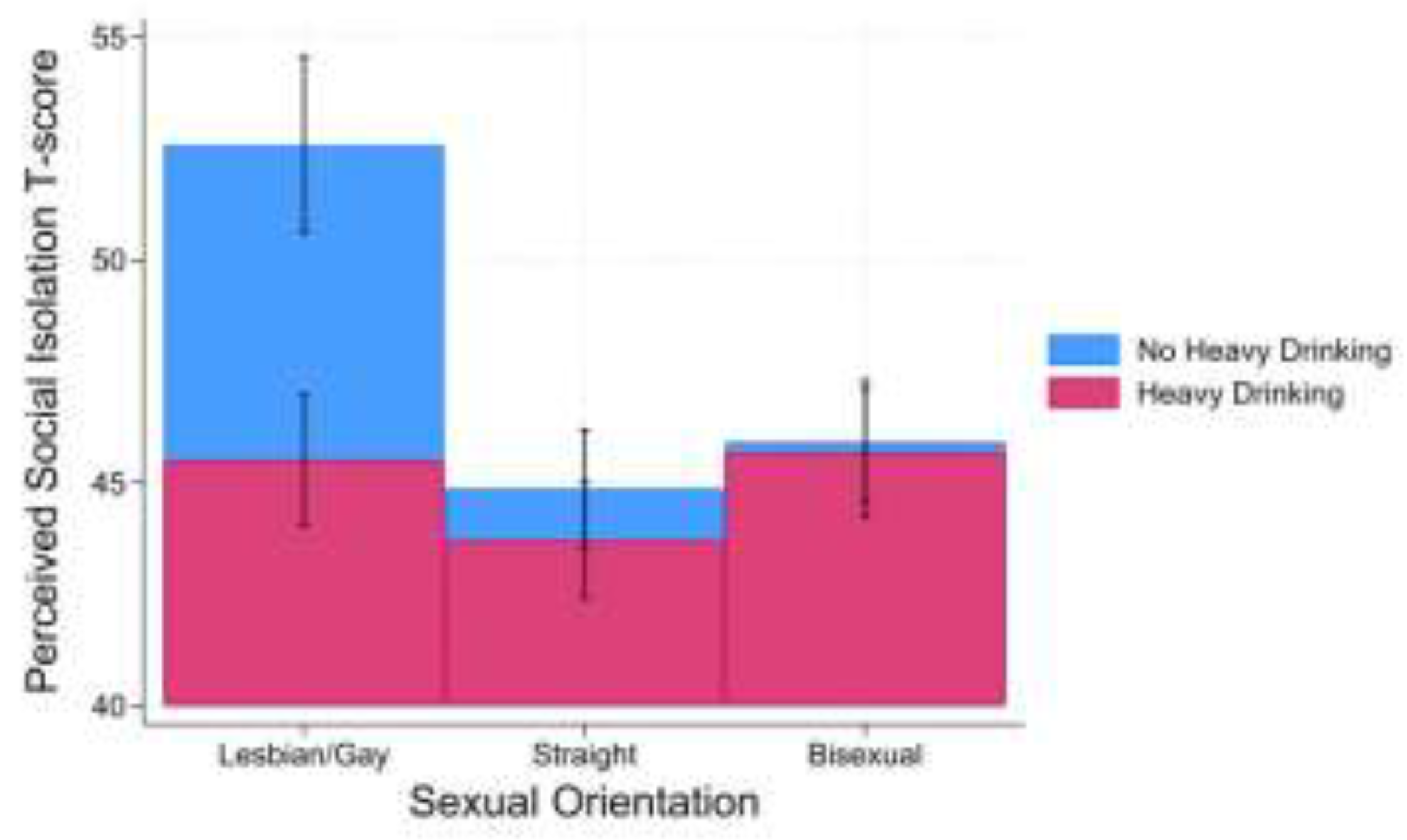

Table 1.
Sample distribution of U.S. adults aged 18-29 and comparison by number of heavy drinking occasions (0 vs. 1+), 2022 and 2024 (N=723).
Table 1.
Sample distribution of U.S. adults aged 18-29 and comparison by number of heavy drinking occasions (0 vs. 1+), 2022 and 2024 (N=723).
| Full Sample | Heavy drinking occasions* | p-Value† | ||
| None (n=394) | 1+ (n=329) | |||
| M (SE) or n (%) | M (SE) or % | M (SE) or % | ||
| Age | 23.6 (0.05) | 23.3 (0.06) | 24.0 (0.06) | < .001 |
| Sex | < .001 | |||
| Male | 460 (47.9) | 50.3 | 49.7 | |
| Female | 263 (52.1) | 59.8 | 40.2 | |
| Sexual orientation | .012 | |||
| Lesbian/gay | 39 (4.5) | 61.8 | 38.2 | |
| Straight | 576 (84.7) | 53.8 | 46.2 | |
| Bisexual | 108 (10.8) | 55.1 | 44.9 | |
| Race/ethnicity | < .001 | |||
| Non-Hispanic White | 336 (53.3) | 50.6 | 49.4 | |
| Non-Hispanic Black | 94 (8.6) | 72.6 | 27.4 | |
| Hispanic | 202 (22.3) | 48.7 | 51.3 | |
| Non-Hispanic Asian | 60 (11.0) | 71.9 | 28.1 | |
| Non-Hispanic Other | 31 (5.0) | 68.6 | 31.4 | |
| Education level | < .001 | |||
| Less than high school | 21 (6.1) | 37.0 | 63.0 | |
| High school graduate | 100 (18.4) | 64.7 | 35.3 | |
| Some college | 202 (41.4) | 59.3 | 40.7 | |
| College graduate or more | 400 (34.1) | 48.5 | 51.5 | |
| Household income | < .001 | |||
| <$20,000 | 112 (18.3) | 47.7 | 52.3 | |
| $20,000-<$35,000 | 75 (9.9) | 54.0 | 46.0 | |
| $35,000-<$50,000 | 114 (14.6) | 60.3 | 39.7 | |
| $50,000-<$75,000 | 153 (19.4) | 64.7 | 35.3 | |
| $75,000-<$100,000 | 188 (27.1) | 59.4 | 40.6 | |
| $100,000+ | 81 (10.8) | 35.0 | 65.0 | |
| Adults in household | .170 | |||
| 1 | 157 (11.6) | 57.1 | 42.9 | |
| 2+ | 258 (88.4) | 55.0 | 45.0 | |
| HINTS Cycle | < .001 | |||
| 6 (2022) | 432 (66.8) | 63.7 | 36.3 | |
| 7 (2024) | 291 (33.2) | 38.3 | 61.7 | |
| Personal Health Questionnaire (PHQ)-4 score | 3.3 (0.04) | 3.12 (0.05) | 3.5 (0.06) | < .001 |
| PROMIS Social Isolation T-score | 49.6 (0.15) | 49.9 (0.21) | 49.2 (0.22) | .025 |
Note. *Comparisons of weighted means (Ms) with standard errors (SEs) for continuous variables and weighted percentages for categorical variables. † p-value represents survey weighted one-way analysis of variance (ANOVA) for continuous variables and the Rao-Scott Chi-square test of weighted proportions for categorical variables. HINTS=Health Information National Trends Survey; PROMIS= Patient-Reported Outcomes Measurement Information System.
Table 2.
Weighted and adjusted linear regressions predicting PROMIS Social Isolation T-score of adults in the United States aged 18-29, 2022 and 2024 (N=723).
Table 2.
Weighted and adjusted linear regressions predicting PROMIS Social Isolation T-score of adults in the United States aged 18-29, 2022 and 2024 (N=723).
| Model 1 | Model 2 | |||||||
| 95% CI | 95% CI | |||||||
| B | SE | LL | UL | B | SE | LL | UL | |
| Intercept | 43.95*** | 0.77 | 42.41 | 45.48 | 43.52*** | 0.78 | 41.97 | 45.07 |
| Age | -0.11*** | 0.03 | -0.16 | -0.05 | -0.09** | 0.03 | -0.15 | -0.04 |
| Sex (ref.=female) | ||||||||
| Male | 1.32*** | 0.22 | 0.88 | 1.76 | 1.34*** | 0.22 | 0.91 | 1.78 |
| Sexual identity (ref.=straight) | ||||||||
| Lesbian/Gay | 5.39*** | 0.59 | 4.22 | 6.56 | 1.34*** | 0.22 | 0.91 | 1.78 |
| Bisexual | 1.49*** | 0.34 | 0.82 | 2.16 | 1.34* | 0.22 | 0.91 | 1.78 |
| Race/ethnicity (ref.=NH White) | ||||||||
| Non-Hispanic Black | -3.71*** | 0.64 | -4.99 | -2.43 | -3.60*** | 0.64 | -4.87 | -2.33 |
| Hispanic | -1.92*** | 0.24 | -2.40 | -1.44 | -1.93*** | 0.24 | -2.41 | -1.45 |
| Non-Hispanic Asian | 1.17* | 0.49 | 0.19 | 2.14 | 1.36** | 0.50 | 0.37 | 2.36 |
| Non-Hispanic Other | 4.26*** | 0.47 | 3.34 | 5.19 | 4.20*** | 0.47 | 3.27 | 5.12 |
| Education level (ref.=college graduate or more) | ||||||||
| Less than high school | -1.40* | 0.62 | -2.63 | -0.18 | -1.51* | 0.63 | -2.75 | -0.26 |
| High school graduate | 0.15 | 0.29 | -0.42 | 0.72 | 0.33 | 0.29 | -0.25 | 0.92 |
| Some college | -0.01 | 0.26 | -0.53 | 0.51 | 0.05 | 0.27 | -0.47 | 0.58 |
| Household income (ref.=$100,000+) | ||||||||
| <$20,000 | 2.79*** | 0.50 | 1.80 | 3.78 | 2.77*** | 0.50 | 1.78 | 3.77 |
| $20,000-<$35,000 | -1.41** | 0.48 | -2.36 | -0.46 | -1.49** | 0.48 | -2.44 | -0.54 |
| $35,000-<$50,000 | 1.47** | 0.51 | 0.45 | 2.49 | 1.29* | 0.51 | 0.28 | 2.31 |
| $50,000-<$75,000 | -0.16 | 0.50 | -1.15 | 0.84 | -0.34 | 0.49 | -1.31 | 0.62 |
| $75,000-<$100,000 | 0.30 | 0.47 | -0.63 | 1.23 | 0.26 | 0.47 | -0.67 | 1.19 |
| Adults in household (ref.=2+) | ||||||||
| 1 | 0.18 | 0.25 | -0.32 | 0.68 | 0.19 | 0.26 | -0.32 | 0.69 |
| HINTS Cycle (ref.=7[2024]) | ||||||||
| 6 (2022) | 0.62* | 0.30 | 0.02 | 1.22 | 0.68* | 0.30 | 0.08 | 1.28 |
| Personal Health Questionnaire (PHQ)-4 score | 2.15*** | 0.05 | 2.04 | 2.26 | 2.15*** | 0.05 | 2.04 | 2.26 |
| Heavy drinking occasions (ref.=0) | ||||||||
| 1+ | -1.34*** | 0.19 | -1.72 | -0.95 | -1.16*** | 0.21 | -1.57 | -0.75 |
| Interaction (ref.= Heavy drinking occasion=1+ * straight) | ||||||||
| Heavy drinking occasion=1+ * lesbian/gay | -5.90*** | 0.98 | -7.84 | -3.95 | ||||
| Heavy drinking occasion=1+ * bisexual | 0.92 | 0.56 | -0.19 | 2.04 | ||||
Note. B=unstandardized regression coefficient; SE=standard error; CI=confidence interval; LL=lower limit; UL=upper limit; PROMIS= Patient-Reported Outcomes Measurement Information System; * p < .05, ** p < .01, *** p < .001.Model 2 results were largely consistent with Model 1 after inclusion of the interaction term (Table 2). The main effect of heavy drinking remained significant, though slightly attenuated (B = -1.16, SE = 0.21, p < .001). A significant interaction was observed between heavy drinking occasions and lesbian/gay sexual identity. Among lesbian/gay respondents, reporting one or more heavy drinking occasions was associated with substantially lower social isolation compared with straight respondents who reported heavy drinking (B = -5.90, SE = 0.98, p < .001). In contrast, the interaction between heavy drinking and bisexual identity was not statistically significant, indicating that the association between heavy drinking and social isolation did not differ between bisexual and straight respondents.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



