
Submitted:
16 January 2026
Posted:
16 January 2026
You are already at the latest version
Abstract
Background: Surgical removal of jaw cysts frequently results in bone defects that may compromise healing and delay functional rehabilitation. Laser photobiomodulation (PBM) has been proposed as a minimally invasive adjuvant capable of enhancing osteogenic activity; however, translational evidence based on freshly harvested human jaw bone tissue remains limited. Objective: To investigate the effects of intraoperative laser photobiomodulation on osteogenic differentiation and cellular viability in human bone explants obtained during cystectomy, using a paired experimental design. Materials and Methods: This translational experimental study included 20 patients undergoing surgical treatment for medium to large maxillary or mandibular cysts. From each patient, paired bone explants were harvested intraoperatively, with one explant exposed to diode laser photobiomodulation and the contralateral explant serving as an untreated control. Explants were cultured under standardized conditions and assessed for osteogenic differentiation using morphometric analysis, immunofluorescence staining for alkaline phosphatase (ALPL) and osteocalcin (OCN), and confocal microscopy. Cell viability was evaluated using a live/dead fluorescence assay. Results: Biologically viable osteogenic cultures were obtained from 8 patients and included in the final paired analysis. In the majority of responsive cases, laser-treated explants demonstrated an increased number of osteoblast-like cellular structures, greater osteoblastic surface area occupancy, and enhanced expression of ALPL and OCN compared with paired controls. No evidence of laser-induced cytotoxicity was observed. Conclusions: Intraoperative laser photobiomodulation enhanced osteogenic activity in human jaw bone explants in a subset of cases, supporting its potential role as a biologically active adjuvant in maxillofacial cyst surgery. Inter-individual variability highlights the need for further optimization of irradiation protocols and larger controlled studies to identify predictive factors for clinical responsiveness.
Keywords:
jaw cysts
; oral and maxillofacial surgery
; bone explant
; photobiomodulation
; diode laser
; osteogenic differentiation
; alkaline phosphatase
; osteocalcin
; confocal microscopy
; regenerative medicine
1. Introduction
To date, most evidence regarding photobiomodulation-induced osteogenesis has been derived from animal models or isolated cell cultures, and data based on freshly harvested human jaw bone tissue exposed intraoperatively remain scarce [1,2]. Bone regeneration represents a critical aspect of contemporary oral and maxillofacial surgery, particularly following the surgical management of cystic jaw lesions [1,2,3]. Although these lesions are generally benign, their surgical removal results in bone defects, which may compromise local structural integrity and delay functional rehabilitation. Consequently, there is interest in therapeutic strategies to enhance bone healing while minimizing surgical morbidity [4,5].
Autologous bone remains the gold standard for skeletal regeneration due to its osteogenic, osteoinductive, and osteoconductive properties [6]. However, the biological behavior of bone tissue following surgical trauma is influenced by multiple factors, including local vascularization, cellular viability, and the microenvironment of the defect [7,8]. In this context, the use of bone explants harvested intraoperatively offers a unique opportunity to investigate osteogenic potential under clinically relevant conditions, closely reflecting the biological reality encountered in maxillofacial surgery [9,10].
Mesenchymal stem cells derived from bone tissue play a central role in bone regeneration through their capacity to proliferate and differentiate into osteoblasts [11,12,13]. The modulation of osteoblastic activity represents a key target in regenerative strategies, aiming to accelerate matrix synthesis and mineralization [14,15]. Experimental models based on human bone explants allow direct assessment of cellular viability, differentiation markers, and functional activity, providing valuable translational insights [13,14].
Laser photobiomodulation has emerged as a promising adjuvant therapy in regenerative medicine [16,17]. Low-level laser therapy has been shown to influence mitochondrial activity, cellular metabolism, and gene expression, thereby promoting cell proliferation and differentiation [18,19]. In bone tissue, photobiomodulation has been associated with increased osteoblastic activity, enhanced expression of osteogenic markers, and improved mineralization [20,21]. Despite encouraging results, the biological effects of laser therapy remain dependent on irradiation parameters and the biological context in which it is applied [22].
Within the field of oral and maxillofacial surgery, the potential role of laser photobiomodulation as an adjunct to the surgical treatment of jaw cysts remains insufficiently explored, particularly in experimental models using human bone tissue [9,10]. Investigating the response of bone explants obtained during cyst surgery may contribute to the development of minimally invasive, biologically optimized therapeutic protocols [23].
The present study evaluates the effects of laser photobiomodulation on human bone explants harvested during surgical treatment of jaw cysts, with a focus on osteogenic differentiation, cellular viability, and functional activity. By integrating surgical practice with experimental laboratory analysis, this research aims to provide a translational framework for optimizing bone regeneration in maxillofacial surgery [24,25].
2. Materials and Methods
2.1. Study Design
This study was designed as a translational experimental investigation evaluating the effects of intraoperative laser photobiomodulation (PBM) on the osteogenic behavior of human jaw bone explants harvested during surgical treatment of cystic lesions. A paired-sample experimental design was employed, whereby laser-treated and non-treated explants were obtained from the same patient, allowing direct intra-individual comparison and minimizing biological variability inherent to human tissue–based models.
The primary outcomes were osteogenic differentiation, osteoblast-like cellular organization, and cellular viability, assessed under standardized in vitro conditions.
2.2. Study Population and Ethical Approval
Bone explants were harvested from 20 consecutive patients undergoing surgical treatment for medium to large cystic lesions of the maxilla or mandible at the Department of Oral and Maxillofacial Surgery, Emergency County Clinical Hospital of Târgu Mureș, Romania, between January and December 2023.
Eligibility criteria included patients presenting cystic lesions of sufficient size to permit safe harvesting of adjacent bone tissue through the standard surgical approach [26]. Exclusion criteria included a history of radiotherapy or chemotherapy in the head and neck region, osteonecrosis or osteoradionecrosis, active cystic infection or suppuration, and systemic diseases or treatments known to impair bone metabolism significantly [27].
The study protocol was approved by the Institutional Ethics Committee (approval no. 13555/21.06.2022) and conducted in accordance with the Declaration of Helsinki. Bone harvesting did not require additional surgical maneuvers beyond routine clinical procedures. All specimens were anonymized before laboratory processing.
2.3. Bone Explant Harvesting Procedure
Bone explants were collected intraoperatively during cystectomy procedures. Following surgical exposure of the cystic cavity via a standard vestibular approach, small cortical bone fragments were obtained from the surgical access area, without removing perilesional bone tissue or modifying the standard surgical protocol.
Only cystic lesions of medium to large dimensions were included, as smaller lesions do not allow reliable or reproducible explant harvesting. Immediately after collection, bone fragments were placed under sterile conditions in transport medium and prepared for experimental processing (Figure 1).
2.4. Experimental Groups and Laser Photobiomodulation Protocol
For each patient, two morphologically comparable bone explants were harvested and assigned as follows:
- -
- Control explant: no laser exposure
- -
- Laser-treated explant: subjected to intraoperative photobiomodulation
Laser irradiation was performed using a diode dental laser (Litemedics Prime, Litemedics, Romania) (Figure 2) with the following parameters:
- -
- Wavelength: 980 nm
- -
- Output power: 1 W
- -
- Emission mode: pulsed
- -
- Operating mode: biostimulation
- -
- Fiber diameter: 320 μm
- -
- Irradiation distance: 50 mm (non-contact)
- -
- Exposure time: 40 seconds
The laser fiber was positioned perpendicular to the explant surface to ensure uniform irradiation while avoiding direct contact and thermal tissue effects. Based on the output power (1 W), exposure time (40 s), and estimated irradiation area at a distance of 50 mm, the calculated energy delivered per explant was approximately 40 J, corresponding to an estimated energy density within the biostimulatory range reported for bone tissue (J/cm²). These parameters were selected to promote photobiomodulation while minimizing the risk of thermal effects.
The selected parameters were chosen to promote cellular photobiomodulation while minimizing the risk of thermal alteration.
2.5. Transport and Laboratory Processing
Bone explants were transported to the laboratory within a maximum interval of three hours following harvesting. All subsequent experimental procedures were carried out at the Department of Immunology, Center for Advanced Medical and Pharmaceutical Research (CCAMF), George Emil Palade University of Medicine, Pharmacy, Science and Technology of Târgu Mureș.
Upon arrival, explants were processed under sterile conditions according to a standardized protocol applied uniformly to all samples.
2.6. Explant Culture and Cell Isolation
Bone fragments were rinsed with Dulbecco’s phosphate-buffered saline (DPBS) to remove blood residues and transferred to culture flasks containing Dulbecco’s Modified Eagle Medium (DMEM) supplemented with fetal bovine serum and antibiotics.
Explants were cultured using the explant technique, allowing spontaneous migration of cells from the bone fragments. Cultures were maintained at 37°C, in a 5% CO₂ humidified atmosphere, with periodic medium replacement. Cellular outgrowth from the explants was monitored microscopically.
Once sufficient cell confluence was achieved, bone fragments were removed, and adherent cells were detached using enzymatic dissociation and prepared for further expansion or differentiation assays.
2.7. Osteogenic Differentiation Protocol
Cells derived from explant cultures were induced toward osteogenic differentiation using a standard osteogenic induction medium containing β-glycerophosphate, L-ascorbic acid, and dexamethasone.
Cultures were maintained under controlled conditions with regular medium changes until the appropriate stages of osteogenic differentiation were reached, allowing assessment of early and late osteoblastic markers.
2.8. Immunofluorescence Staining and Confocal Microscopy
Osteogenic differentiation was evaluated by immunofluorescence staining for alkaline phosphatase (ALPL) and osteocalcin (OCN), established markers of osteoblastic differentiation and matrix maturation.
Cells were fixed, permeabilized, and incubated with primary antibodies against ALPL and OCN, followed by fluorochrome-conjugated secondary antibodies. Nuclear counterstaining was performed using 4′,6-diamidino-2-phenylindole (DAPI).
Image acquisition was performed using a Leica TCS SP8 confocal microscope (Leica Microsystems, Germany). Identical acquisition parameters, including magnification, laser power, detector gain, and field of view, were applied to all samples to allow reliable qualitative and morphometric comparisons between laser-treated and control cultures.
Morphometric analysis was performed using ImageJ/Fiji software (National Institutes of Health, USA). Osteoblast-like structures were identified through manual and threshold-assisted segmentation based on fluorescence intensity and morphological criteria, including cell size, shape, and marker positivity. Identical segmentation thresholds and analysis parameters were applied uniformly across paired control and laser-treated samples to ensure consistency.
2.9. Cell Viability Assessment
Cell viability was assessed using a live/dead fluorescence assay based on Calcein AM and Ethidium Homodimer III. Viable cells were identified by green cytoplasmic fluorescence, whereas non-viable cells exhibited red nuclear staining.
Stained cultures were imaged immediately using confocal microscopy, and viability was assessed qualitatively by comparison between paired laser-treated and control samples.
2.10. Experimental Yield and Data Analysis
Due to the inherent biological variability associated with primary human bone explant cultures, measurable osteogenic differentiation and viable cell populations were obtained in 8 out of 20 patients. These cases constituted the final experimental cohort included in the comparative analysis.
Data analysis followed a paired descriptive approach, with each laser-treated explant directly compared to its corresponding control. Results were expressed as cell counts, morphometric parameters, and relative differences between groups.
Because of the natural biological variability of primary human bone explant cultures, detectable osteogenic differentiation and viable cell populations were achieved in samples from 8 of the 20 patients. This yield is consistent with previously reported success rates for primary cultures derived from surgically harvested human bone tissue, where variability in cellular viability, vascularization, and local bone quality can significantly affect culture establishment.
The remaining explants failed to generate sufficient cellular outgrowth or osteogenic differentiation for reliable morphometric and immunofluorescence analysis and were therefore excluded before comparative evaluation.
Given the limited number of biologically responsive paired samples and the exploratory nature of this translational study, formal inferential statistical testing was not performed. Instead, results were analyzed descriptively on a paired basis, focusing on consistent biological trends across multiple outcome measures. This approach was selected to avoid overinterpretation of statistically underpowered data while preserving biological relevance.
3. Results
3.1. Study Cohort and Experimental Yield
Bone explants were harvested from 20 patients undergoing surgical treatment for cystic lesions of the maxilla or mandible and processed according to the standardized experimental protocol.
Analysis of excluded samples indicated no systematic clustering with respect to anatomical localization (maxilla versus mandible), patient age, or cyst type. Both maxillary and mandibular explants were represented among excluded cases, suggesting that explant viability was influenced predominantly by local biological factors rather than demographic or anatomical variables.
Due to the inherent biological variability associated with primary human bone explant cultures, measurable osteogenic differentiation and viable cell populations were obtained in 8 out of 20 patients. These 8 cases constituted the final experimental cohort included in the paired comparative analysis between laser-treated and non-treated explants. The remaining samples did not yield sufficient cellular viability or osteogenic differentiation for reliable morphometric and immunofluorescence evaluation and were therefore excluded from further analysis.
A flow diagram summarizing patient inclusion, explant processing, and final sample selection is presented in Figure 3.
The demographic characteristics and anatomical harvesting sites of the patients included in the final experimental group are summarized in Table 1.
3.2. Osteoblast-Like Cellular Structures: Quantitative Paired Analysis
Quantitative morphometric analysis revealed consistent differences between laser-treated and control explants in terms of the number of osteoblast-like cellular structures.
In 7 out of 8 patients, explants exposed to photobiomodulation demonstrated a higher number of osteoblast-like cellular structures compared with their paired controls. This increase suggests a stimulatory effect of laser photobiomodulation on osteogenic cellular activity. The magnitude of this effect varied among patients, reflecting individual biological variability.
Across the analyzed samples, laser-treated explants generally exhibited a greater density of smaller, more uniformly distributed osteoblast-like cellular structures, whereas control explants displayed fewer but larger cellular aggregates.
Detailed quantitative values for each paired comparison are provided in Table 2, and a graphical comparison of cellular structure counts between experimental groups is illustrated in Figure 4.
Cumulative area values represent pixel-based measurements obtained from digital image analysis and are expressed in relative units, reflecting the number of pixels occupied by segmented osteoblast-like structures within a defined field of view; these values were used exclusively for paired intra-sample comparisons and not as absolute dimensional measurements.
Paired quantitative analysis demonstrates a higher number of osteoblast-like cellular structures in laser-treated explants compared with corresponding non-treated controls in the majority of analyzed patients.
3.3. Morphometric Analysis of Osteoblastic Area Occupancy
To further characterize osteogenic behavior beyond simple cell counts, a morphometric analysis was performed to assess the percentage of surface area occupied by osteoblast-like cellular structures in control and laser-treated cultures.
In the majority of cases, laser-treated explants demonstrated an increased percentage of osteoblastic area occupancy compared with paired controls. This finding suggests that photobiomodulation affects not only the number of osteogenic cells but also their spatial organization and surface coverage, which are crucial features of effective osteogenic differentiation.
Notably, in several patients, laser-treated explants exhibited both increased cellular density and improved distribution of osteoblast-like cellular structures across the culture surface. Individual morphometric values are presented in Table 3, and a comparative graphical representation of osteoblastic area occupancy is shown in Figure 5.
The percentage of osteoblastic area (%Area) was calculated as the proportion of the image surface occupied by osteoblast-like structures relative to the total analyzed field, based on pixel-based morphometric analysis.
3.4. Immunofluorescence Assessment of Osteogenic Marker Expression
Immunofluorescence staining demonstrated the presence of alkaline phosphatase (ALPL) and osteocalcin (OCN) in both control and laser-treated explants, confirming osteogenic differentiation in cultured cells derived from human bone tissue.
In laser-treated explants, ALPL and OCN signals were generally more intense and more widely distributed compared with paired controls. This pattern is consistent with enhanced osteoblastic differentiation and matrix maturation following photobiomodulation.
Confocal microscopy revealed that laser-exposed cultures exhibited a higher number of ALPL-positive cells at earlier differentiation stages, as well as increased OCN expression in more mature osteoblast-like cells.
3.5. Cell Viability Analysis
Live/dead fluorescence assays demonstrated preserved cellular viability in both experimental groups. In laser-treated explants, viable cells predominated, with a high proportion of Calcein AM-positive cells and minimal Ethidium Homodimer III nuclear staining.
No evidence of laser-induced cytotoxicity or increased cell death was observed under the applied photobiomodulation parameters. In contrast, several control explants exhibited areas of reduced cell density and sporadic non-viable cells, particularly in cultures with limited cellular outgrowth.
These observations indicate that the applied photobiomodulation protocol was biologically safe and did not adversely affect cell viability.
3.6. Summary of Experimental Findings
Collectively, the results demonstrate a consistent trend toward enhanced osteogenic activity in human bone explants exposed to intraoperative laser photobiomodulation. Compared with paired non-treated controls, laser-treated explants exhibited:
- -
- Increased numbers of osteoblast-like cellular structures
- -
- Greater osteoblastic surface area occupancy
- -
- Enhanced expression of osteogenic markers (ALPL and OCN)
- -
- Preserved cellular viability
Despite inter-individual variability and a limited number of biologically responsive samples, the concordance of findings across quantitative, morphometric, and qualitative endpoints supports a biologically relevant osteostimulatory effect of photobiomodulation in human jaw bone tissue.
4. Discussion
Bone regeneration following surgical management of cystic lesions of the maxilla and mandible remains a fundamental concern in oral and maxillofacial surgery, particularly in cases involving medium to large defects where spontaneous bone healing may be delayed or incomplete [28,29]. Although cystic lesions are generally benign, the resulting bone defects can compromise structural stability, delay functional rehabilitation, and complicate subsequent implant or prosthetic treatment [31,32]. Consequently, considerable interest has been directed toward adjuvant strategies to enhance osteogenesis while maintaining a minimally invasive surgical approach [31,32,33].
In this translational experimental study, we evaluated the effects of intraoperative laser photobiomodulation (PBM) on osteogenic behavior in human jaw bone explants harvested during cystectomy procedures [34]. By employing a paired-sample design, laser-treated explants were directly compared with non-treated controls obtained from the same patient, thereby minimizing inter-individual biological variability and strengthening the internal validity of the findings [35].
4.1. Photobiomodulation-Induced Osteogenic Activity in Human Bone Explants
The results of the present study demonstrate a consistent trend toward enhanced osteogenic activity in bone explants exposed to photobiomodulation [18,19,21,22,25,34]. Laser-treated samples exhibited increased numbers of osteoblast-like cellular structures, greater osteoblastic surface area occupancy, and enhanced expression of osteogenic markers when compared with paired controls. These findings support the hypothesis that PBM can positively modulate osteogenic differentiation in human bone tissue [18,19,21,22,25,34].
Previous experimental studies have shown that low-level laser irradiation stimulates osteoblastic proliferation and differentiation through mitochondrial activation, increased adenosine triphosphate synthesis, and modulation of intracellular signaling pathways involved in bone metabolism [25,34,35]. The present findings are consistent with these reports and extend existing knowledge by demonstrating similar biological effects in freshly harvested human jaw bone explants, a model that preserves native cell–matrix interactions and more closely reflects the clinical environment [34,35].
Importantly, the use of human explant-derived cells distinguishes this study from many investigations based on animal models or immortalized cell lines, which, although valuable, do not fully reproduce the complexity of human bone tissue [36,37]. The observed osteogenic response, therefore, carries particular translational relevance for oral and maxillofacial surgery.
The applied irradiation parameters fall within ranges previously reported to enhance osteogenic activity without inducing cytotoxic or thermal effects, as described in established photobiomodulation guidelines and experimental studies.
4.2. Morphometric and Organizational Effects of Laser Photobiomodulation
In addition to increasing the number of osteoblast-like cellular structures, photobiomodulation was associated with changes in cellular organization and surface distribution, as reflected by the morphometric analysis of osteoblastic area occupancy [38,39]. In most cases, laser-treated explants exhibited a greater percentage of surface area covered by osteoblast-like cellular structures, suggesting a more organized and functionally active osteogenic environment [38,39,40].
Effective bone regeneration depends not only on the presence of osteogenic cells but also on their spatial distribution and coordinated matrix deposition. The tendency toward smaller, more uniformly distributed osteoblast-like cellular structures in laser-treated cultures may indicate a more proliferative and metabolically active osteogenic phenotype, potentially favoring subsequent mineralization and tissue maturation [40,41].
4.3. Osteogenic Marker Expression and Cellular Viability
Immunofluorescence analysis confirmed the expression of alkaline phosphatase (ALPL) and osteocalcin (OCN) in explant-derived cultures, validating successful osteogenic differentiation under the applied experimental conditions. Laser-treated explants generally exhibited more intense and widespread expression of these markers, consistent with enhanced osteoblastic differentiation and matrix maturation [42,43].
Equally important, the live/dead viability assays demonstrated that the applied photobiomodulation protocol did not induce cytotoxic effects [43,44]. On the contrary, laser-treated explants frequently displayed preserved or improved cellular viability compared with controls. This finding supports the biological safety of intraoperative PBM and is particularly relevant in the surgical context, where maintaining cell viability is essential for successful regeneration [18,19,21,22,25,34,43,44].
4.4. Clinical and Translational Significance
From a clinical perspective, the observed enhancement of osteogenic parameters following PBM supports its potential role as an adjuvant therapy in the surgical management of jaw cysts [44,45]. Improved osteogenic activity at the cellular level may translate into faster bone healing, improved defect filling, and more predictable regenerative outcomes, particularly in extensive defects where spontaneous regeneration may be unreliable [22,25,44,45].
The intraoperative application of PBM, as used in this study, offers practical advantages. It can be easily integrated into standard surgical workflows, does not require additional surgical sites, and adds minimal operative time or morbidity. As such, PBM represents a promising strategy for biologically optimizing bone healing without increasing the invasiveness of treatment [40,45,46].
4.5. Biological Variability and Response Heterogeneity
A notable observation in this study was the variability in biological response among harvested explants. Although bone samples were obtained from 20 patients, biologically valid osteogenic responses were observed in a subset of cases. This variability reflects the inherent heterogeneity of human bone tissue and the challenges associated with primary explant culture models [47].
Factors such as patient age, anatomical location, local bone quality, vascularization, and systemic conditions may influence cellular viability and differentiation potential [48]. Rather than representing a limitation alone, this heterogeneity underscores the importance of human tissue–based translational research and suggests that individualized or optimized photobiomodulation protocols may be necessary to achieve consistent regenerative outcomes [47,48].
4.6. Study Limitations and Future Perspectives
Several limitations should be considered when interpreting the results of this study. The limited number of biologically responsive samples restricts statistical generalization and precludes definitive conclusions regarding clinical efficacy. Additionally, the study focused on short-term cellular and morphometric outcomes, without longitudinal assessment of mineralization dynamics, biomechanical properties, or clinical healing parameters.
Future investigations should aim to include larger patient cohorts, standardized laser dosimetry protocols, and correlations between cellular responses and clinical or radiological outcomes. The integration of molecular analyses may further clarify the mechanisms by which photobiomodulation influences osteogenic pathways in human bone tissue [17,46].
Within the limitations of this translational experimental model, the present study provides evidence that intraoperative laser photobiomodulation can enhance osteogenic differentiation, cellular organization, and viability in human jaw bone explants. The consistency of findings across multiple outcome measures supports the biological relevance of PBM as a modulator of bone regenerative processes.
5. Conclusions
This translational experimental study demonstrates that intraoperative laser photobiomodulation can enhance osteogenic differentiation, cellular organization, and osteogenic marker expression in human jaw bone explants harvested during cystectomy. Using a paired design, laser-treated explants exhibited increased osteoblast-like cellular structures and improved osteogenic surface occupancy compared with untreated controls, without evidence of cytotoxic effects.
Although biologically responsive cultures were obtained in a limited subset of patients, the consistency of findings across morphometric, immunofluorescence, and viability assessments supports the biological relevance of photobiomodulation in human bone tissue. These results suggest that laser photobiomodulation may serve as a minimally invasive adjunct for optimizing bone healing following cystic lesion removal.
Further studies with larger cohorts, refined laser dosimetry, and correlation with clinical and radiological outcomes are required to establish the clinical efficacy and reproducibility of photobiomodulation-assisted bone regeneration in oral and maxillofacial surgery.
References
- Starch-Jensen, T.; Deluiz, D.; Deb, S.; Bruun, N.H.; Tinoco, E.M.B. Harvesting of autogenous bone graft from the ascending mandibular ramus compared with the chin region: A systematic review and meta-analysis focusing on complications and donor site morbidity. J. Oral Maxillofac. Res. 2020, 11, e1. [Google Scholar] [CrossRef]
- Daoud, S.; Zoabi, A.; Kasem, A.; Totry, A.; Oren, D.; Redenski, I.; Srouji, S.; Kablan, F. Computer-assisted evaluation confirms spontaneous healing of donor site one year following bone block harvesting from mandibular retromolar region—A cohort study. Diagnostics 2024, 14, 504. [Google Scholar] [CrossRef]
- Nyimi, B.F.; Yifang, Z.; Liu, B. The changing landscape in treatment of cystic lesions of the jaws. J. Int. Soc. Prev. Community Dent. 2019, 9, 328–337. [Google Scholar] [CrossRef]
- Wang, J.; Yao, Q.Y.; Zhu, H.Y. Efficacy of bone grafts in jaw cystic lesions: A systematic review. World J. Clin. Cases 2022, 10, 2801–2810. [Google Scholar] [CrossRef]
- Tas, A.; Celebi, E.; Çukurova Yilmaz, Z. Assessment of bone healing after surgical management of odontogenic cysts utilizing fractal analysis—A retrospective cross-sectional study. PeerJ 2025, 13, e19745. [Google Scholar] [CrossRef] [PubMed]
- Sakdejayont, S.; Chobpenthai, T.; Suksirivecharuk, P.; Ninatkiattikul, I.F.; Poosiripinyo, T. A review on bone tumor management: Cutting-edge strategies in bone grafting, bone graft substitute, and growth factors for defect reconstruction. Orthop. Res. Rev. 2025, 17, 175–188. [Google Scholar] [CrossRef]
- Cao, H.; He, S.; Wu, M.; Hong, L.; Feng, X.; Gao, X.; Li, H.; Liu, M.; Lv, N. Cascaded controlled delivering growth factors to build vascularized and osteogenic microenvironment for bone regeneration. Mater. Today Bio 2024, 25, 101015. [Google Scholar] [CrossRef]
- Wang, Y.; Zhang, X.; Li, X.; Cheng, M.; Cui, X. The vascular microenvironment and its stem cells regulate vascular homeostasis. Front. Cell Dev. Biol. 2025, 13, 1544129. [Google Scholar] [CrossRef] [PubMed]
- Elsalanty, M.E.; Genecov, D.G. Bone grafts in craniofacial surgery. Craniomaxillofac. Trauma Reconstr. 2009, 2, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Nicolae, C.-L.; Pîrvulescu, D.-C.; Niculescu, A.-G.; Epistatu, D.; Mihaiescu, D.E.; Antohi, A.M.; Grumezescu, A.M.; Croitoru, G.-A. An Up-to-Date Review of Materials Science Advances in Bone Grafting for Oral and Maxillofacial Pathology. Materials 2024, 17, 4782. [Google Scholar] [CrossRef]
- Huang, W.; Zhou, C.; Yu, Y.; et al. Functionalized mesenchymal stem cells for enhanced bone regeneration: Advances and challenges. Stem Cell Res. Ther. 2025, 16, 600. [Google Scholar] [CrossRef]
- Coccoluto, L.; Roberto, R.; Paola, P.; Francesca, R.; Raffaele, V. Osteoblastic differentiation and proliferation of human mesenchymal stem cells or osteoblast-like cells on bone scaffolds in oral and periodontal surgery: A systematic review of in vitro studies. J. Adv. Oral Res. 2025, 16, 121–139. [Google Scholar] [CrossRef]
- Han, Y.; Li, X.; Zhang, Y.; Han, Y.; Chang, F.; Ding, J. Mesenchymal Stem Cells for Regenerative Medicine. Cells 2019, 8, 886. [Google Scholar] [CrossRef]
- Lin, X.; Patil, S.; Gao, Y.G.; Qian, A. The bone extracellular matrix in bone formation and regeneration. Front. Pharmacol. 2020, 11, 757. [Google Scholar] [CrossRef]
- Collignon, A.M.; Lesieur, J.; Vacher, C.; Chaussain, C.; Rochefort, G.Y. Strategies Developed to Induce, Direct, and Potentiate Bone Healing. Front Physiol. 2017, 14, 8:927. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, P.; Basha, S.; Biswas, S.; Prabhu, V.; Prabhu, S.S.; Pai, A.R.; Mahato, K.K. From light to healing: Photobiomodulation therapy in medical disciplines. J. Transl. Med. 2025, 23, 1430. [Google Scholar] [CrossRef] [PubMed]
- Moscatel, M.B.M.; Pagani, B.T.; Trazzi, B.F.d.M.; Reis, C.H.B.; Ribeiro, C.A.; Buchaim, D.V.; Buchaim, R.L. Effects of Photobiomodulation in Association with Biomaterials on the Process of Guided Bone Regeneration: An Integrative Review. Ceramics 2025, 8, 94. [Google Scholar] [CrossRef]
- Rola, P.; Włodarczak, S.; Lesiak, M.; Doroszko, A.; Włodarczak, A. Changes in Cell Biology under the Influence of Low-Level Laser Therapy. Photonics 2022, 9, 502. [Google Scholar] [CrossRef]
- AlGhamdi, K.M.; Kumar, A.; Alfayez, M.; Mahmood, A. Influence of Low-Level Red Laser Irradiation on the Proliferation, Viability, and Differentiation of Human Embryonic Stem Cell-Derived Mesenchymal Stem Cells. Life 2025, 15, 1125. [Google Scholar] [CrossRef]
- Della Coletta, B.B.; Jacob, T.B.; Moreira, L.A.d.C.; Pomini, K.T.; Buchaim, D.V.; Eleutério, R.G.; Pereira, E.d.S.B.M.; Roque, D.D.; Rosso, M.P.d.O.; Shindo, J.V.T.C.; et al. Photobiomodulation Therapy on the Guided Bone Regeneration Process in Defects Filled by Biphasic Calcium Phosphate Associated with Fibrin Biopolymer. Molecules 2021, 26, 847. [Google Scholar] [CrossRef]
- Amaroli, A.; Colombo, E.; Zekiy, A.; Aicardi, S.; Benedicenti, S.; De Angelis, N. Interaction between Laser Light and Osteoblasts: Photobiomodulation as a Trend in the Management of Socket Bone Preservation—A Review. Biology 2020, 9, 409. [Google Scholar] [CrossRef]
- Iaria, R.; Vescovi, P.; De Francesco, P.; Giovannacci, I. Laser Photobiomodulation: What Are the Ideal Parameters for Each Type of Laser Used in Dental Practice to Promote Fibroblast Proliferation and Differentiation? A Systematic Review. Life 2025, 15, 853. [Google Scholar] [CrossRef] [PubMed]
- Rubio, E.D.; Mombrú, C.M. Spontaneous Bone Healing After Cysts Enucleation Without Bone Grafting Materials: A Randomized Clinical Study. Craniomaxillofac. Trauma Reconstr. 2015, 8, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Del Vecchio, A.; Tenore, G.; Pergolini, D.; Rocchetti, F.; Palaia, G.; Romeo, U. The Role of the Laser Photobiomodulation (PBM) in the Management of Patients at Risk or Affected by MRONJ. Oral 2022, 2, 7–15. [Google Scholar] [CrossRef]
- Saki, M.; Tahamtan, S.; Shavakhi, M.; Grzech-Leśniak, K.; Fekrazad, R. The effectiveness of photobiomodulation therapy on bone regeneration of oral and craniofacial defects: A systematic review of animal and in vitro studies. Lasers Med. Sci. 2025, 40, 384. [Google Scholar] [CrossRef] [PubMed]
- Irimia, A.; Moraru, L.; Ciubotaru, D.A.; Caruntu, C.; Farcasiu, A.-T.; Caruntu, A. Minimally Invasive Two-Staged Surgery in the Treatment of Large Cystic Lesions of the Jaw. Healthcare 2021, 9, 1531. [Google Scholar] [CrossRef]
- Juncar, M.; Popa, A. R.; Onișor, F.; Iova, G. M.; Popa, L. M. Descriptive Study on Influence of Systemic Conditions on Head and Neck Infections. Appl Med Inform 2011, 28, 62–68. Available online: https://ami.info.umfcluj.ro/index.php/AMI/article/view/65.
- La Rosa, G.R.M.; Priolo, C.Y.; Abiad, R.S.; Romeo, V.R.; Ambu, E.; Pedullà, E. Assessment of bone regeneration after maxillary radicular cyst enucleation with or without bone grafting materials: A retrospective cohort study. Clin. Oral Investig. 2024, 28, 213. [Google Scholar] [CrossRef]
- Sacher, C.; Holzinger, D.; Grogger, P.; et al. Calculation of postoperative bone healing of cystic lesions of the jaw—A retrospective study. Clin. Oral Investig. 2019, 23, 3951–3957. [Google Scholar] [CrossRef]
- Li, Y.; He, L.; Tang, Z.; Shao, L.; Zhang, W.; Su, J. Long-term implant success after treatment of a giant mandibular dentigerous cyst: A case report. Int. J. Surg. Case Rep. 2025, 135, 111831. [Google Scholar] [CrossRef]
- McLean, A.C.; Vargas, P.A. Cystic lesions of the jaws: The top 10 differential diagnoses to ponder. Head Neck Pathol. 2023, 17, 85–98. [Google Scholar] [CrossRef]
- Prajapati, A.; Gulia, A.; Gundavda, K.; Botchu, R.; Janu, A. Cystic bone lesions: Diagnostic pitfalls and therapeutic considerations. J. Clin. Orthop. Trauma 2025, 67, 103046. [Google Scholar] [CrossRef]
- Shah, N.; Logani, A.; Kumar, V. A minimally invasive surgical approach for large cyst-like periapical lesions: A case series. Gen. Dent. 2014, 62, e1–e5. [Google Scholar] [PubMed]
- Hosseinpour, S.; Tunér, J.; Fekrazad, R. Photobiomodulation in oral surgery: A review. Photobiomodul. Photomed. Laser Surg. 2019, 37, 814–825. [Google Scholar] [CrossRef]
- Gao, X.; Xing, D. Molecular mechanisms of cell proliferation induced by low power laser irradiation. J. Biomed. Sci. 2009, 16, 4. [Google Scholar] [CrossRef]
- Klassmann, F.A.; Ervolino, E.; Kluppel, L.E.; Theodoro, L.H.; Mulinari-Santos, G.; Garcia, V.G. A randomized trial of bone formation after maxillary sinus floor augmentation with bovine hydroxyapatite (Cerabone®) and photobiomodulation: Histomorphometric and immunohistochemical analysis. J. Clin. Exp. Dent. 2023, 15, e542–e550. [Google Scholar] [CrossRef]
- Razaghi, P.; Moradi Haghgou, J.; Khazaei, S.; Farhadian, N.; Fekrazad, R.; Gholami, L. The effect of photobiomodulation therapy on the stability of orthodontic mini-implants in human and animal studies: A systematic review and meta-analysis. J. Lasers Med. Sci. 2022, 13, e27. [Google Scholar] [CrossRef]
- Deana, A.M.; de Souza, A.M.; Teixeira, V.P.; Mesquita-Ferrari, R.A.; Bussadori, S.K.; Fernandes, K.P.S. The impact of photobiomodulation on osteoblast-like cells: A review. Lasers Med. Sci. 2018, 33, 1147–1158. [Google Scholar] [CrossRef] [PubMed]
- Na, S.; TruongVo, T.; Jiang, F.; et al. Dose analysis of photobiomodulation therapy on osteoblast, osteoclast, and osteocyte. J. Biomed. Opt. 2018, 23, 075008. [Google Scholar] [CrossRef] [PubMed]
- Vigliar, M.F.R.; Marega, L.F.; Duarte, M.A.H.; Alcalde, M.P.; Rosso, M.P.d.O.; Ferreira Junior, R.S.; Barraviera, B.; Reis, C.H.B.; Buchaim, D.V.; Buchaim, R.L. Photobiomodulation therapy improves repair of bone defects filled by inorganic bone matrix and fibrin heterologous biopolymer. Bioengineering 2024, 11, 78. [Google Scholar] [CrossRef]
- De Pace, R.; Iaquinta, M.R.; Benkhalqui, A.; D'Agostino, A.; Trevisiol, L.; Nocini, R.; Mazziotta, C.; Rotondo, J.C.; Bononi, I.; Tognon, M.; Martini, F.; Mazzoni, E. Revolutionizing bone healing: The role of 3D models. Cell Regen. 2025, 14, 7. [Google Scholar] [CrossRef]
- Lazăr, L.; Manu, D.R.; Dako, T.; Mârțu, M.-A.; Suciu, M.; Ormenișan, A.; Păcurar, M.; Lazăr, A.-P. Effects of Laser Application on Alveolar Bone Mesenchymal Stem Cells and Osteoblasts: An In Vitro Study. Diagnostics 2022, 12, 2358. [Google Scholar] [CrossRef]
- Pagin, M.T.; de Oliveira, F.A.; Oliveira, R.C.; et al. Laser and light-emitting diode effects on pre-osteoblast growth and differentiation. Lasers Med. Sci. 2014, 29, 55–59. [Google Scholar] [CrossRef]
- Paim, E.D.; Branchini, G.; Lamers, M.; et al. Effect of photobiomodulation on viability and proliferation of squamous cell carcinoma in vitro. Lasers Med. Sci. 2025, 40, 462. [Google Scholar] [CrossRef] [PubMed]
- Gioga, C.; Bănățeanu, A.-M.; Voinea-Georgescu, R.-N.; Dobrescu, A.-M. Surgical management of a large mandibular cyst: A case report. Romanian Journal of Oral Rehabilitation 2024, 16(4). [Google Scholar] [CrossRef]
- Lu, P.; Peng, J.; Liu, J.; Chen, L. The role of photobiomodulation in accelerating bone repair. Prog. Biophys. Mol. Biol. 2024, 188, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Maglio, M.; Fini, M.; Sartori, M.; Codispoti, G.; Borsari, V.; Dallari, D.; Ambretti, S.; Rocchi, M.; Tschon, M. An Advanced Human Bone Tissue Culture Model for the Assessment of Implant Osteointegration In Vitro. Int. J. Mol. Sci. 2024, 25, 5322. [Google Scholar] [CrossRef]
- Kostadinova, M.; Raykovska, M.; Simeonov, R.; Lolov, S.; Mourdjeva, M. Recent Advances in Bone Tissue Engineering: Enhancing the Potential of Mesenchymal Stem Cells for Regenerative Therapies. Curr. Issues Mol. Biol. 2025, 47, 287. [Google Scholar] [CrossRef]
- Abdellatife, T.A.; Zaki, M.H. Impact of photobiomodulation on postoperative pain and bone healing following cystic enucleation: A randomized clinical trial. Oral Maxillofac. Surg. 2025. [Google Scholar] [CrossRef]
Figure 1.
Handling of a tissue-like specimen in a liquid medium under controlled laboratory conditions. The sample was transferred using sterile forceps into a test tube and prepared for subsequent analyses. All procedures were performed under standard aseptic conditions.
Figure 1.
Handling of a tissue-like specimen in a liquid medium under controlled laboratory conditions. The sample was transferred using sterile forceps into a test tube and prepared for subsequent analyses. All procedures were performed under standard aseptic conditions.
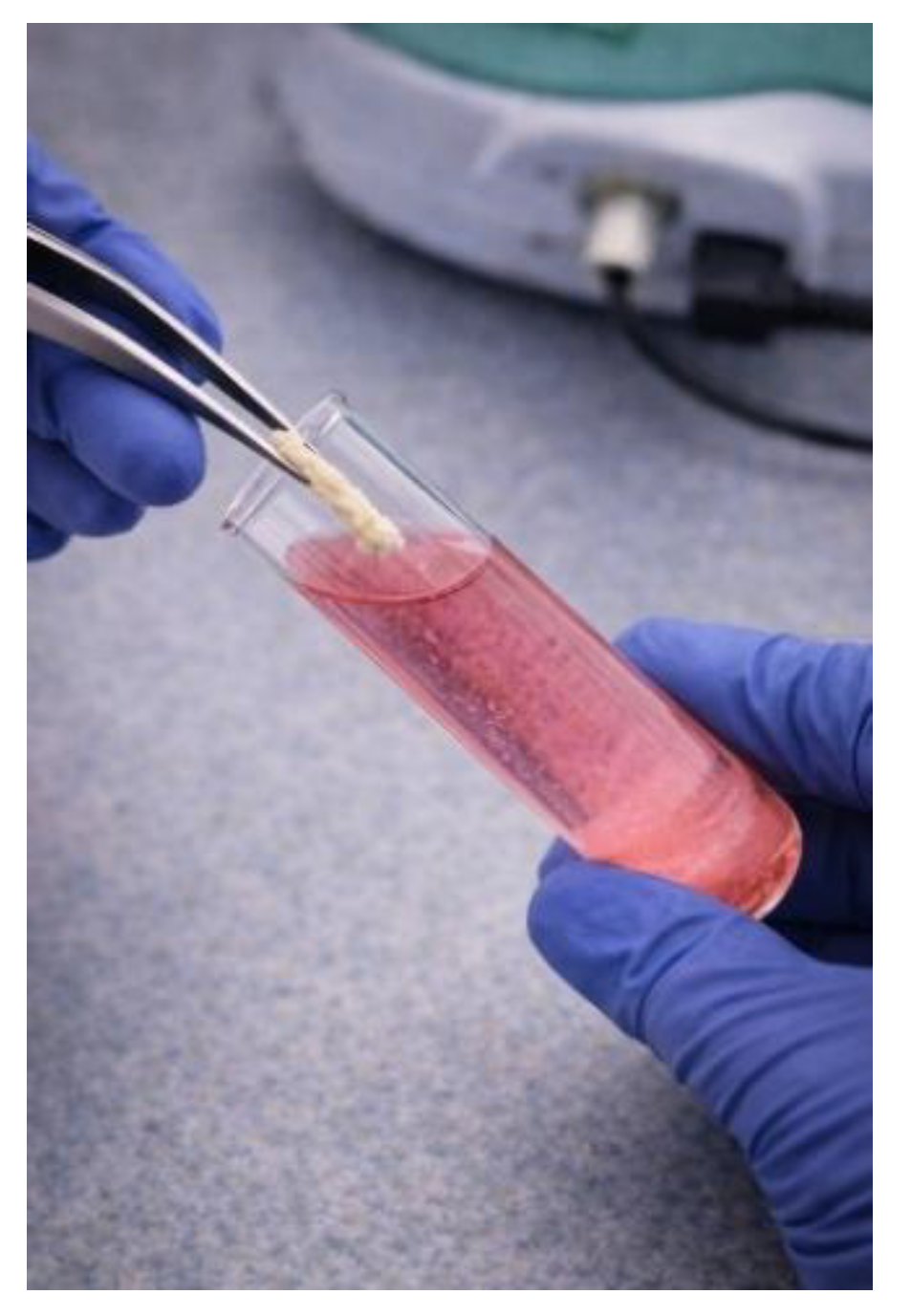
Figure 2.
Experimental setup for dental laser application under controlled laboratory conditions. A Lite Medics laser unit was operated in therapy mode at an output power of 1.0 W, delivering focused laser energy to a tissue-like sample positioned in a sterile Petri dish and stabilized with precision forceps, illustrating laser–tissue interaction in a simulated clinical environment.
Figure 2.
Experimental setup for dental laser application under controlled laboratory conditions. A Lite Medics laser unit was operated in therapy mode at an output power of 1.0 W, delivering focused laser energy to a tissue-like sample positioned in a sterile Petri dish and stabilized with precision forceps, illustrating laser–tissue interaction in a simulated clinical environment.
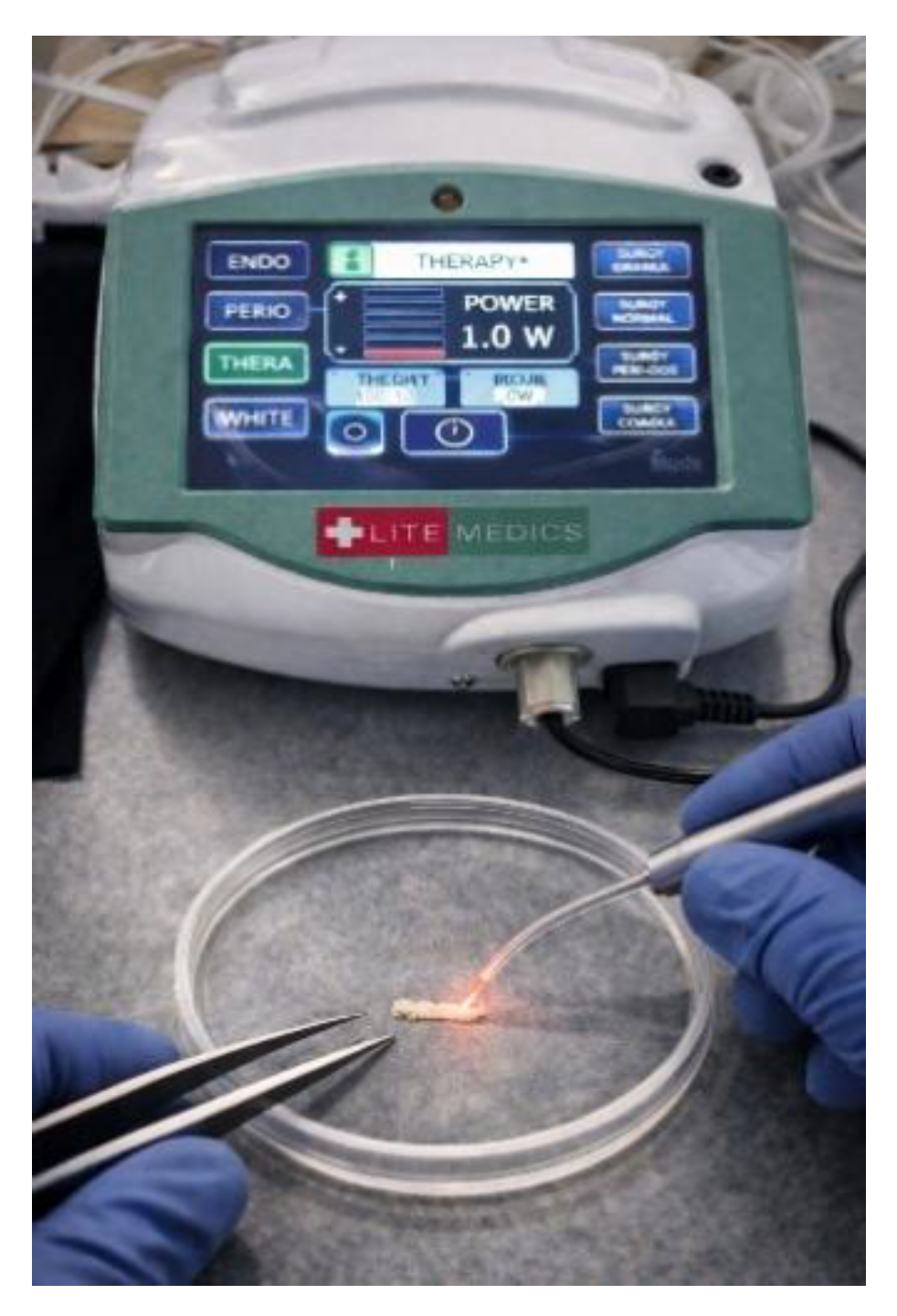
Figure 3.
Flow diagram of patient inclusion and explant processing (included vs. excluded samples).
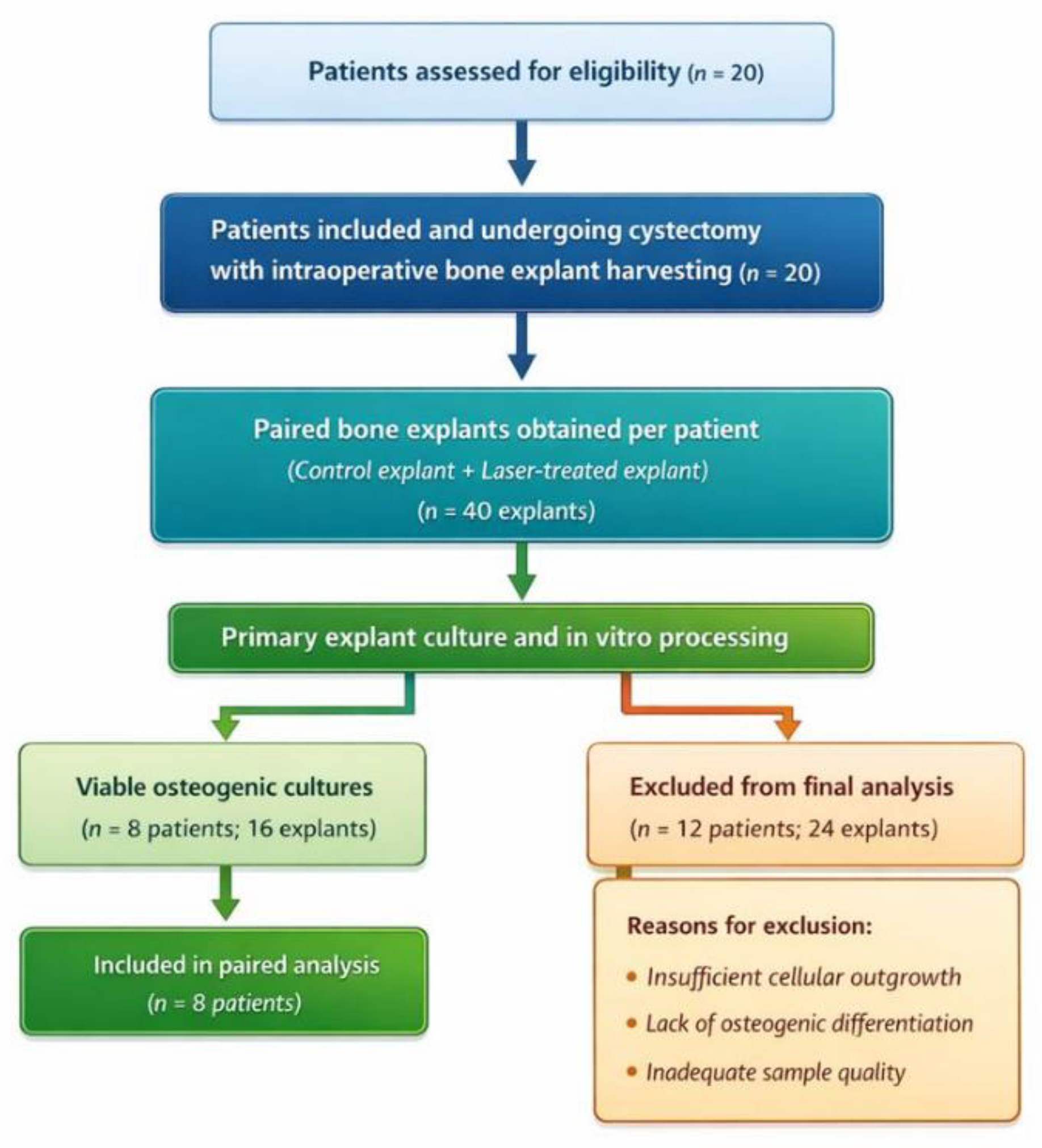
Figure 4.
Comparison of osteoblast-like cellular structure counts between control and laser-treated bone explants.
Figure 4.
Comparison of osteoblast-like cellular structure counts between control and laser-treated bone explants.
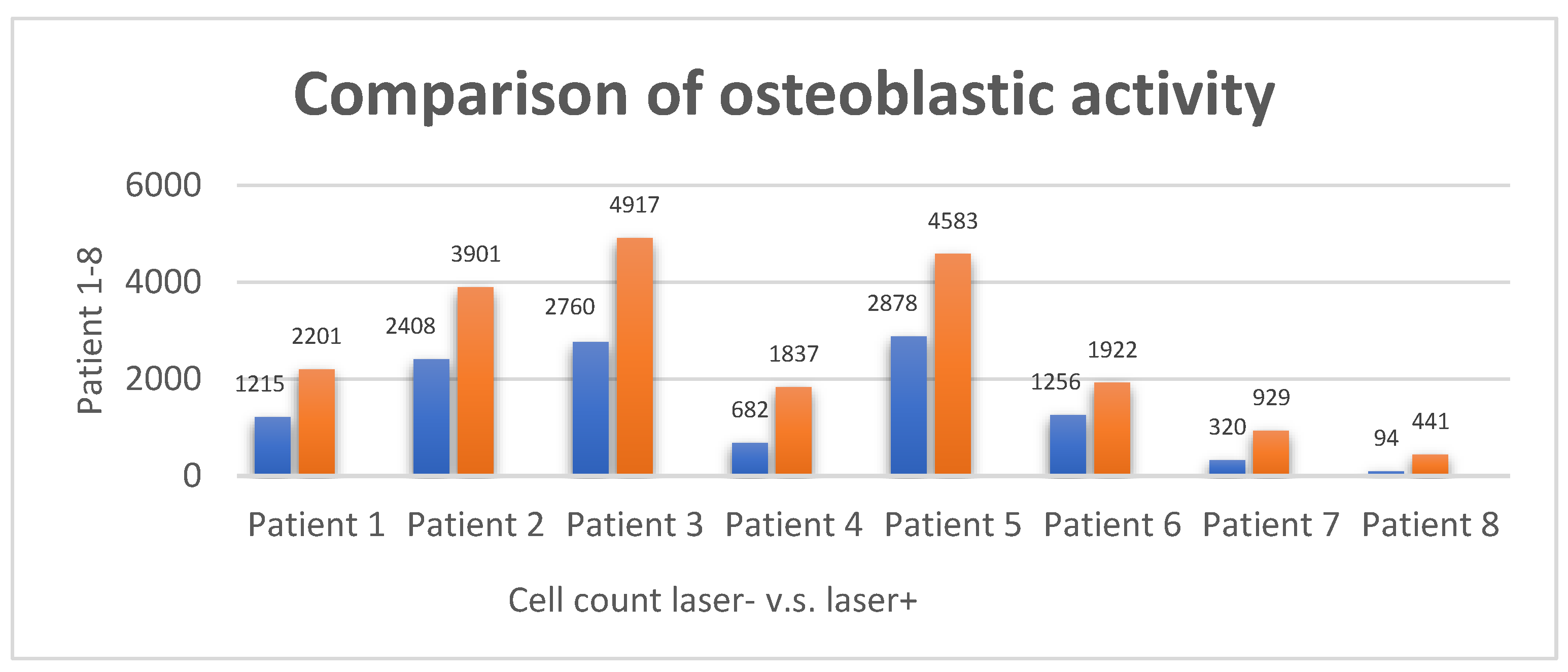
Figure 5.
Comparison of the percentage of osteoblastic area occupancy between control and laser-treated explants.

Table 1.
Demographic and clinical characteristics of patients included in the final experimental analysis.
Table 1.
Demographic and clinical characteristics of patients included in the final experimental analysis.
| Patient Number | Patient Age | Patient Gender | Anatomical Localization |
|---|---|---|---|
| Patient 1 | 26 | female | maxilla |
| Patient 2 | 29 | male | maxilla |
| Patient 3 | 19 | female | maxilla |
| Patient 4 | 39 | female | maxilla |
| Patient 5 | 40 | male | mandible |
| Patient 6 | 46 | female | mandible |
| Patient 7 | 50 | male | mandible |
| Patient 8 | 55 | female | mandible |
Table 2.
Paired quantitative and relative morphometric analysis of osteoblast-like cellular structures in control and laser-treated human bone explants.
Table 2.
Paired quantitative and relative morphometric analysis of osteoblast-like cellular structures in control and laser-treated human bone explants.
| Slice | Count | Cumulative Area (Relative Units) |
|---|---|---|
| Patient 1 LASER + | 2201 | 554123.852 |
| Patient 1 LASER - | 1215 | 1441762.407 |
| Patient 2 LASER + | 3901 | 644989.447 |
| Patient 2 LASER - | 2408 | 634447.68 |
| Patient 3 LASER + | 4917 | 533615.553 |
| Patient 3 LASER - | 2760 | 482853.707 |
| Patient 4 LASER + | 1837 | 239164.02 |
| Patient 4 LASER - | 682 | 133335.969 |
| Patient 5 LASER + | 4583 | 1079814.891 |
| Patient 5 LASER - | 2878 | 793648.215 |
| Patient 6 LASER + | 1922 | 621348.193 |
| Patient 6 LASER - | 1256 | 435137.329 |
| Patient 7 LASER + | 929 | 178271.067 |
| Patient 7 LASER - | 320 | 48918.086 |
| Patient 8 LASER + | 441 | 73910.588 |
| Patient 8 LASER - | 94 | 2791900.064 |
Table 3.
Paired morphometric evaluation of osteoblastic area occupancy in control and laser-treated human bone explants.
Table 3.
Paired morphometric evaluation of osteoblastic area occupancy in control and laser-treated human bone explants.
| Slice | Cumulative Osteoblastic Area (Relative Units) | Osteoblastic Area Occupancy (%) |
|---|---|---|
| Pacient 1 LASER + | 554123.852 | 11.556 |
| Pacient 1 LASER - | 1441762.407 | 28.777 |
| Pacient 2 LASER + | 644989.447 | 13.292 |
| Pacient 2 LASER - | 634447.68 | 12.136 |
| Pacient 3 LASER + | 533615.553 | 42.039 |
| Pacient 3 LASER - | 482853.707 | 35.527 |
| Pacient 4 LASER + | 239164.02 | 19.231 |
| Pacient 4 LASER - | 133335.969 | 11.216 |
| Pacient 5 LASER + | 1079814.891 | 22.55 |
| Pacient 5 LASER - | 793648.215 | 16.206 |
| Pacient 6 LASER + | 621348.193 | 12.85 |
| Pacient 6 LASER - | 435137.329 | 7.259 |
| Pacient 7 LASER + | 1782710067 | 18.906 |
| Pacient 7 LASER - | 48918.086 | 4.722 |
| Pacient 8 LASER + | 73910.588 | 7.541 |
| Pacient 8 LASER - | 279190006.4 | 0.685 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



