
Submitted:
14 January 2026
Posted:
15 January 2026
You are already at the latest version
Abstract
INTRODUCTION
Major Depressive Disorder (MDD) is a leading cause of disability worldwide and contributes significantly to the global burden of disease. Recent data show an increasing prevalence of Treatment-Resistant Depression (TRD). Patients with Autism Spectrum Disorder (ASD) often exhibit MDD as a comorbidity and it is often resistant to conventional treatments. ASD determines emotional dysregulation and a reduced ability to understand mental states (mentalization). These features can lead to suicidal ideation and/or behaviour. Intranasal Esketamine, approved for TRD, may offer a novel therapeutic option for this population.
METHODS
Our study evaluates the clinical response to intranasal Esketamine in patients with autism and TRD. The sample was composed of three young patients (n=3, F/M 2:1, age range 20-25 y) with light to moderate autism (Level 1 or 2). Esketamine was administered in augmentation with Selective Serotonin Reuptake Inhibitors (SSRIs) or Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs). A structured follow-up protocol was set to monitor depressive symptoms, social cognition and mentalization. Follow-up during treatment was maintained for six months and psychometric evaluations were performed at six time points: baseline (T0), 1 week (T1), 1 month (T2), 2 months (T3), 3 months (T4) and 6 months (T5). Also, subjective quality of life was investigated before and after the observation period.
RESULTS
Despite differences in clinical profile, all patients showed good efficacy of Esketamine in reducing depressive symptoms: two patients experienced clinical remission (MADRS decrease > 50% from T0 to T5), while one patient showed partial remission (dMADRS=43.24%). No major side effects were reported. Significant improvements were observed after the first week of treatment (P1: MADRS_T0=37, MADRS_T1=12. P2: MADRS_T0=32, MADRS_T1=21. P3: MADRS_T0=25, MADRS_T1=12). Depressive relapses occurred (e.g. P1, T3-T4) but they were not associated with hospitalizations and/or suicidal attempts. Suicidal ideation, when present, decreased by the end of the follow-up period. Lack in mentalization and in social cognition were noted, with just mild improvements during therapy. Subjective quality of life improved significantly for all patients (P1: 28% at T0, 73% at T5. P2: 25% at T0, 71% at T5. P3: 35% at T0, 80% at T5).
CONCLUSIONS
Intranasal Esketamine showed a favourable efficacy and safety profile in these three cases of TRD in comorbidity with ASD (at six months: total remission=66.66%, partial remission=33.33%, inefficacy=0%, drop-out=0, severe adverse events=0). Besides improvements in depressive symptoms, Esketamine was associated with a constant decrease in suicidal thoughts. The small sample size doesn’t allow us to formalize statistical conclusions; preliminary data warrant further investigation in larger and randomized control studies to validate the therapeutic potential of Esketamine in this population.
Keywords:
case report
; major depressive disorder
; treatment-resistant depression
; autism spectrum disorder
; esketamine
; suicidal ideation
; mentalization
; social cognition
1. Introduction
Major Depressive Disorder (MDD) is a major cause of disability and contributes to suicide deaths worldwide. In 2018 MDD was ranked third in terms of disease burden, and it is predicted to rank first by 2030[1]. The prevalence of MDD in 2025 is 5.7% among the worldwide population and is more prevalent in women (6.9%) than in men (4.6%)[2]. At the same time, the prevalence of Treatment-Resistant Depression (TRD) is increasing. TRD is defined as a depressive episode that does not improve adequately after almost two pharmacological trials appropriate in dose and duration[3]. Major depression is a very frequent comorbidity, considering both medical and psychiatric conditions[4]. Autism Spectrum Disorder (ASD) is frequently associated with anxious and/or depressive symptoms, with a reported prevalence of 20% and 9% respectively[5]. Patients diagnosed with ASD and MDD often present frequent suicidal ideation (SI). A meta-analysis suggests that the relative risk of suicide in people with ASD is almost three times higher compared to neurotypical population[6]. This finding could be explained by the impairment in mentalization skills. The difficulty in understanding mental states can reduce tolerance to everyday life stressors -i.e., family, work, relationships- and suicidal thoughts can develop as an “escape path”. Resistance to change, rigid thought patterns and emotional dysregulation are common symptoms in ASD and they could contribute to an increase in suicidal risk[7,8,9]. Emotional dysregulation was associated with suicidal behaviours especially in young patients[10]. MDD in ASD represents a serious pathological condition that requires early diagnosis and efficient treatment. ASD patients show lower response to pharmacological treatments due to several factors, such as genetic variability[11], cognitive rigidity and comorbid conditions. There are no approved pharmacological treatments for the core symptoms of ASD: available medications focus on managing symptoms without targeting the underlying neurobiological mechanisms[12]. A personalized approach can be recommended, combining a target therapy to major symptoms and non-pharmacological interventions (behavioural, dietary, environmental)[13]. In our experience we focused on depressive symptoms in ASD considering a potential treatment-resistant profile. We administered intranasal Esketamine (Spravato) to three young ASD patients who had severe depressive symptoms and SI, not responding to conventional pharmacological therapy. Esketamine is approved in Italy as a therapeutic option in TRD used in augmentation with SSRI or SNRI medications[14]. It is the S-enantiomer of ketamine and a non-selective and non-competitive N-methyl-D-aspartate (NMDA) receptor antagonist. The molecule binds receptors on GABAergic interneurons (inhibitory), causing release of glutamate in synaptic gaps; glutamate via α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) receptor determines excitatory stimulation in the cortex and in the limbic system, with an augmented production of neurotrophic factors. The fast antidepressant effects of Esketamine were associated with direct stimulation of the mammalian target of rapamycin complex 1 (mTORC1) and the stimulation of a molecular pathway involved in brain-derived neurotrophic factor (BDNF) synthesis[15]. Remodulation involving the glutamate pathway and neurotrophic factors could be potentially useful in autism comorbidity, which has been associated with molecular mechanisms like glutamate-induced excitotoxicity and oxidative stress (e.g., neuro-inflammation)[16].
2. Methods
2.1. Study Design and Setting
This study is organized as a small case series with real-life patients, recruited in a public Mental Health Service.
Inclusion criteria: patients with ASD and moderate to severe MDD, which had not responded to two or more pharmacological treatments.
Exclusion criteria: patients with active psychotic symptoms and severe cardiological conditions. Patients selected for the study started a trial with intranasal Esketamine according to EPA/AIFA guidelines (see below). Pharmacological treatment and clinical follow-up were carried out in Mental Health Services of Pavia (P1 and P2) and Milan (P3). All participants received treatment as outpatients, P2 underwent the first part of the follow-up (T0 and T1) during his inpatient stay in the Psychiatric Ward of Pavia.
2.2. Participants
Three autistic patients were recruited from 2023 to 2025. Clinical and socio-demographical information were summarized in Table 1.
Autism diagnosis was carried out with a multidisciplinary approach, combining neuropsychological tests and the clinical opinion given by expert psychiatrists. Neuropsychological evaluation was carried out with the Auism Diagnostic Observation Scale (ADOS), Social Responsiveness Scale (SRS) and the Wechsler Adult Intelligence Scale (WAIS-IV). Patients enrolled were affected by mild to moderate autism (Level 1 or 2, according to Diagnostic and Statistical Manual of Mental Disorders 5, Text Revised). At baseline all patients were characterized by resistant depressive symptoms with or without suicidal ideation. P2 and P3 were treated with Esketamine for the first time in this protocol. P1 had already undergone a previous trial with Esketamine (2021) with partial benefit, interrupted for subjective improvement (see below, “Results – Patient 1”). A preliminary visit was performed to assess the necessity of the intervention and patient compliance, providing all information about Esketamine and psychometric evaluation.
2.3. Intervention
Esketamine treatment was performed in accordance with the EPA/AIFA guidelines: All patients received administration twice a week for the first month and weekly for the second month. After this period, a personalized frequency of therapy was set depending on clinical picture: patients with slight improvement or clinical stability maintained two administrations/month, patients with significant improvement shifted to one administration per month. When depressive relapse occurred, the return to weekly administrations was prescribed. None of three patients showed serious side effects during treatment and they all received the maximum dosage of Esketamine (84 mg per administration, continued for the whole observation period). Dose adjustment was not required. During treatment, oral pharmacotherapy with an SSRI or SNRI was continued with good compliance (P1: Sertraline 200 mg/day. P2: Venlafaxine 300 mg/day. P3: Escitalopram 20 mg/day). After Esketamine administration, patients remained under clinical observation for at least one hour, monitored by clinicians and nurses.
2.4. Outcomes
The primary outcome was to evaluate clinical response to Esketamine which has been defined as a decrease in MADRS total score ≥ 50% from baseline (T0). Secondary outcomes were evaluating changes in social cognition and/or mentalization; assessing the severity of psychache; focusing on suicidal ideation and/or behaviours; at last, highlighting patients ‘experience in terms of quality of life and subjective condition.
The psychometric assessment was composed of six tests and scales (Table 2), administered by clinicians at six time points.
- -
- Montgomery-Asberg Depression Rating Scale (MADRS): a 10-item questionnaire used to monitor depressive symptoms and define the severity of MDD during follow-up.
- -
- Psychache Scale (PS): a 13-item scale used to assess the profile of psychological pain. Some questions demand a frequency rating (from “never” to “always”), while other ones demand an agreement rating (from “strongly disagree” to “strongly agree”).
- -
- Columbia-Suicide Severity Rating Scale (C-SSRS): a structured test to evaluate suicidal ideation and/or behaviour. It is composed by 10 categories of which the majority calls for a binary response yes/no (e.g., suicidal attempts yes/no). When suicidal thoughts and/or behaviour were present, the sub-scale which measures the intensity of ideation (1-5) was reported and considered as a follow-up tool.
- -
- Quality of Life Enjoyment and Satisfaction Questionnaire (Q-LES-Q): a subjective investigation about quality of life, which includes different domains (school, work, housework, social relationships, physical state, leisure time, general activities). Every sub-score can be associated with a percentage of satisfaction: the mean of these eight percentages defines the global quality of life perceived by patients.
- -
- Reading the Mind in the Eyes Test (RMET): a specific test which measures the Theory of Mind and the ability to recognize mental states in other people. It consists of 36 different photographs: for each, patient should indicate what person in the picture is feeling/thinking. It has been noticed that autistic people under-perform on this test as compared to neurotypical population[17].
- -
- Reflective Functioning Questionnaire – 8 items (RFQ-8): a brief, easy to administer screening to evaluate mentalization, coming from a 54-item test[18]. It is focused on reflective functioning intended as the ability to recognize our feelings and our mental states before acting. This test is organized as a Likert-type scale, with responses from “completely agree” (7) to “completely disagree” (1). Higher scores in the RFQ-8 show a lower ability in mentalization.
These tests were administered at T0 (before Esketamine), T1 (1 week of treatment), T2 (1 month), T3 (2 months), T4 (3 months), and T5 (6 months). In our study design blind rating was not feasible due to logistic limitation (clinicians that administered the tests were the same ones responsible for pharmacological treatment). Window period for tests and administrations was ±5 days for each time point. Q-LES-Q was evaluated only at T0 and T5: this choice was motivated by the nature of the questionnaire, which investigates domains with slow modifications (e.g., work, school, social relationships). A month-by-month analysis could have been less informative because patient could not recognize significant changes from a time point to the subsequent one.
2.5. Data Collection and Statistical Analysis
Patients’ information and clinical data were collected in a database, where clinicians were responsible for data entry. The database was organized on Microsoft Excel, and it consisted of seven pages (socio-demographical information + 6 time points with clinical scores). Statistical analyses were carried out on Microsoft Excel, and they were focused on descriptive measures according to the small sample size. The study design was oriented to show real-world experiences, so in the following sections a lot of raw data will be reported.
2.6. Ethical Considerations
Before being enrolled, patients filled out an informed consent form for the analysis and publication of their clinical data during treatment. No off-label procedures were performed. All study procedures were conducted in accordance with Good Clinical Practice (GCP) guidelines and the principles of the Declaration of Helsinki. Ethical approval for the study was granted by the Pavia Ethics Committee during its session on August 27, 2021 (Opinion No. 84157/21), with a subsequent amendment issued under No. 0102231/21.
3. Results
3.1. Patient 1
G. is a 25-year-old Italian young woman presenting with moderate ASD (Level 2) without intellectual disability (IQ 107). She is currently enrolled in the University of Pavia and works part-time as an assistant for a local writer. Family history is notable for psychiatric disorders (mother: mild-to-moderate depression, father: panic disorder). No neurodevelopmental disorder was diagnosed during childhood. The first depressive episode occurred in 2019 after enrolling in university. She was hospitalized in the Psychiatric Department of Pavia due to the development of SI. During hospitalization, symptoms of hyperactivity and racing thoughts were observed, resulting in an initial diagnosis of bipolar disorder. She was discharged with a prescription for Aripiprazole and Lithium, but depressive symptoms and SI recurred. Subsequent treatments with Vortioxetine and Lurasidone yielded no significant improvement. Rigid thinking, hyper-focus on restricted/repetitive activities and difficulty in recognizing emotions led clinicians to the suspicion of autism, which was confirmed. She began Fluoxetine, later switched to Sertraline (200 mg/day). Additionally, she participated in weekly group psychotherapy, which offered further support. In early 2021, due to the persistence of depressive symptoms and self-harming behaviours (cutting and cigarette burns), a trial with Esketamine was carried out. After six months of treatment, the patient requested to stop administration due to a subjective well-being. After about a year of stable functioning in both social and occupational domains, a new depressive episode occurred. She resumed treatment with Esketamine in January 2023, and she maintained treatment for six months, during which the follow-up protocol was carried out. She received the last administration of the drug in June 2023. Since then, G. has been monitored through periodic outpatient evaluations. In 2024, she discontinued group psychotherapy maintaining psychiatric follow-up. Nowadays (2025) clinical picture is substantially stable.
G. showed a good clinical response to Esketamine, with a partial reduction in depressive symptoms from T0 (MADRS=37) to T5 (MADRS=21). A minor side effect was reported (one episode of nausea with vomiting, T4) without serious consequences for patient. A major worsening during treatment (T3-T4) was observed in response to a traumatic trigger (sexual intercourse with a guy). Before the traumatic event, G. showed a solid response maintained for more than a month (MADRS=12 at T1, confirmed at T2) SI was present at T0 with high intensity (5/5) and was totally suppressed at T5 despite the depressive relapse, when there was a minor restart (2/5 at T3). Psychache maintained high values during all the observation period, decreasing only at T5 (13): it is interesting that high values were reached after trauma (T3=60, T4=60). Mentalization was underperforming at T0, but RFQ-8 reached its highest score (=greater lack of mentalization) at T3, when G. reported a self-harming episode (cutting). RMET score 31.33±2.66 showed a good social cognition which seemed to improve during therapy. Q-LES-Q reported a significant improvement in quality of life (T0=28%, T5=73%), particularly in leisure time (T0=32%, T5=80%).
Figure 1.
P1 outcomes (depressive symptoms).
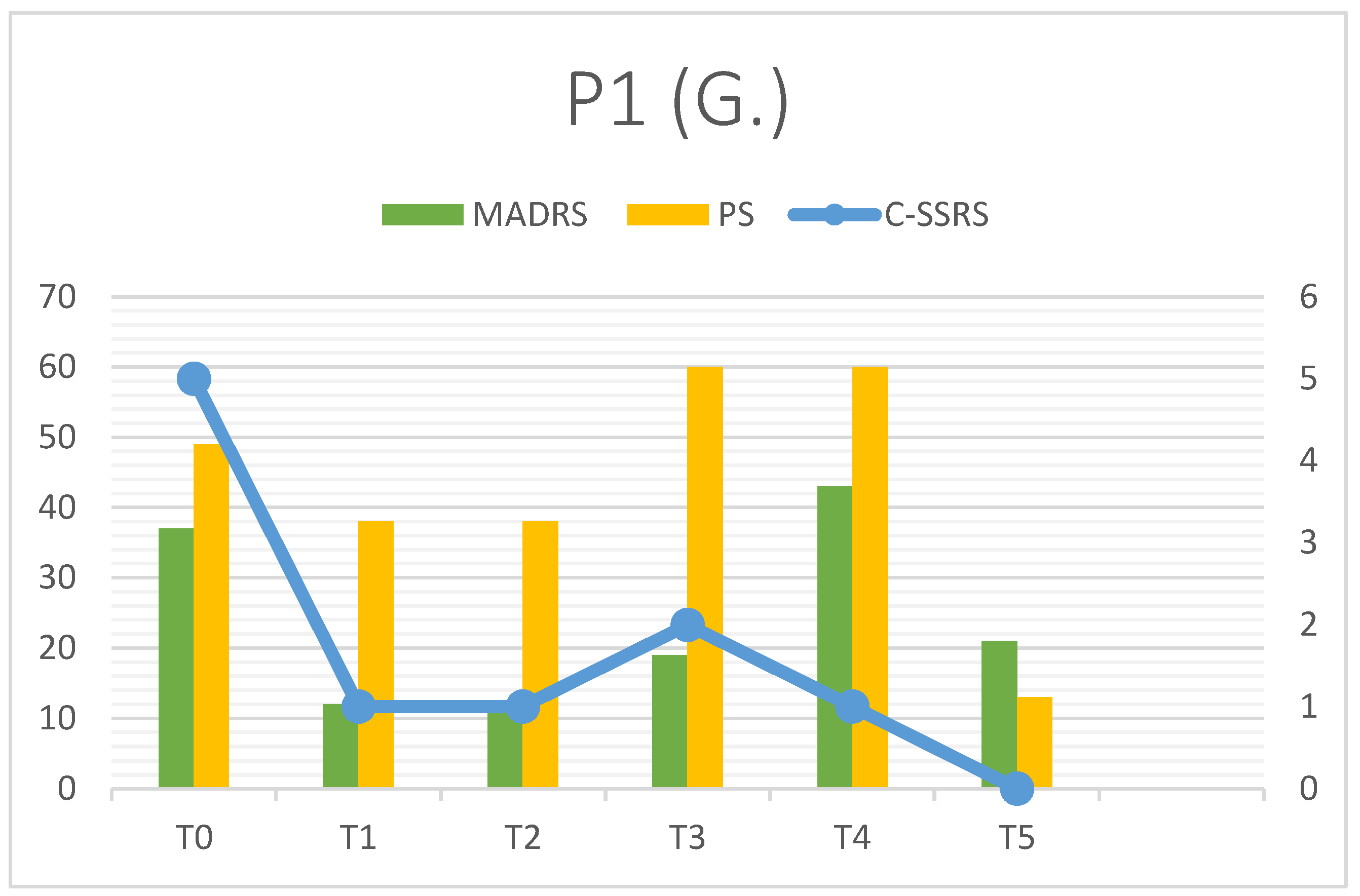

Table 3.
P1 results.
| P1 | MADRS | C-SSRS | PS | RFQ-8 | RMET | Q-LES-Q(%) |
| T0 | 37 | 5 | 49 | 4.125 | 27 | 28 |
| T1 | 12 | 1 | 38 | 4.25 | 31 | - |
| T2 | 12 | 1 | 38 | 4.25 | 30 | - |
| T3 | 19 | 2 | 60 | 4.5 | 32 | - |
| T4 | 43 | 1 | 60 | 3.125 | 34 | - |
| T5 | 21 | 0 | 13 | 2.75 | 34 | 73 |
3.2. Patient 2
E. is a 20-year-old Italian male diagnosed with Level 2 ASD with a high cognitive profile (IQ 137). He graduated from high school in 2023 with a qualification as a surveyor and now he is currently employed on a farm through a rehabilitation program coordinated by the Mental Health Service of Pavia. His family history is positive for psychiatric conditions (mother diagnosed with bipolar disorder). E. first accessed psychiatric services in summer 2023 for a serious self-harming episode (he intentionally set himself on fire at home). The self-destructive act resulted in extensive third-degree burns to his face, trunk, upper limbs, abdomen, and proximal lower limbs. He underwent multiple homografts resulting in a long hospitalization, which was complicated by sepsis (caused by ESBL-producing S. aureus and A. baumannii) and bilateral femoral deep vein thrombosis.
Upon the transfer to the Psychiatric Ward of Pavia, clinical observations suggested high-functioning autism characterized by rigid thought patterns, restricted interests, limited social network, hyper-academic performance, reduced emotional sharing, resistance to change, controlling behaviours and childhood-onset motor tics. The severe self-harming event was described with emotional detachment and attributed to impulsivity triggered by stressful life events. Antidepressant therapy with Sertraline resulted in sub-optimal results and was subsequently replaced with Venlafaxine (300 mg/day), leading to improvement and discharge. Aripiprazole was also prescribed, with a good effect in mood stabilization. Depressive relapse occurred in late 2023 and he was re-hospitalized for SI; Esketamine was introduced during his inpatient stay (February 2024). The administration followed a consultation with an internist to manage hypertension related to severe obesity and metabolic syndrome (propranolol was prescribed). After the first 14 days of treatment, the patient was discharged and continued Esketamine as an outpatient: therapy with Esketamine is still ongoing but our follow-up ended in August 2024. Besides Esketamine he is receiving group psychotherapy and educative support. Nowadays E. is maintaining a quite good functioning considering job and relationships. No more suicidal behaviours occurred. In 2025 Aripiprazole was switched to Lurasidone due to some gambling episodes, reported by E. to clinicians.
Also E. showed a good clinical response to Esketamine with a constant decrease in MADRS and PS scores from T0 to T5. SI showed a complex trend: it was elevated at T0 (intensity 5/5), after a significant improvement at T1 (1/5) it has maintained high values for two months, decreasing only in the terminal part of the follow-up. SI did not determine other suicidal or para-suicidal behaviours, and this may be associated with a good ability of mentalization (RFQ-8 2.125±0.209), which apparently improved during therapy. Discharge from hospital occurred little before T2 and in our opinion this could explain SI restart (patient returned home, where he organized the suicidal attempt). Psychache showed a solid, constant decrease (47 at T0, 24 at T2-T3, 15 at T5). On the other hand, RMET 23.33±1.36 underlined significative impairment in social cognition, as described in the neurodivergent population (see before).
E. perceived an improvement in quality of life (T0=25%, T5=71%) where the main part was represented by work domain: he was unemployed at T0, at T5 the rehabilitative program was just started and patient reported 92% of functioning.
Figure 2.
P2 outcomes (depressive symptoms).
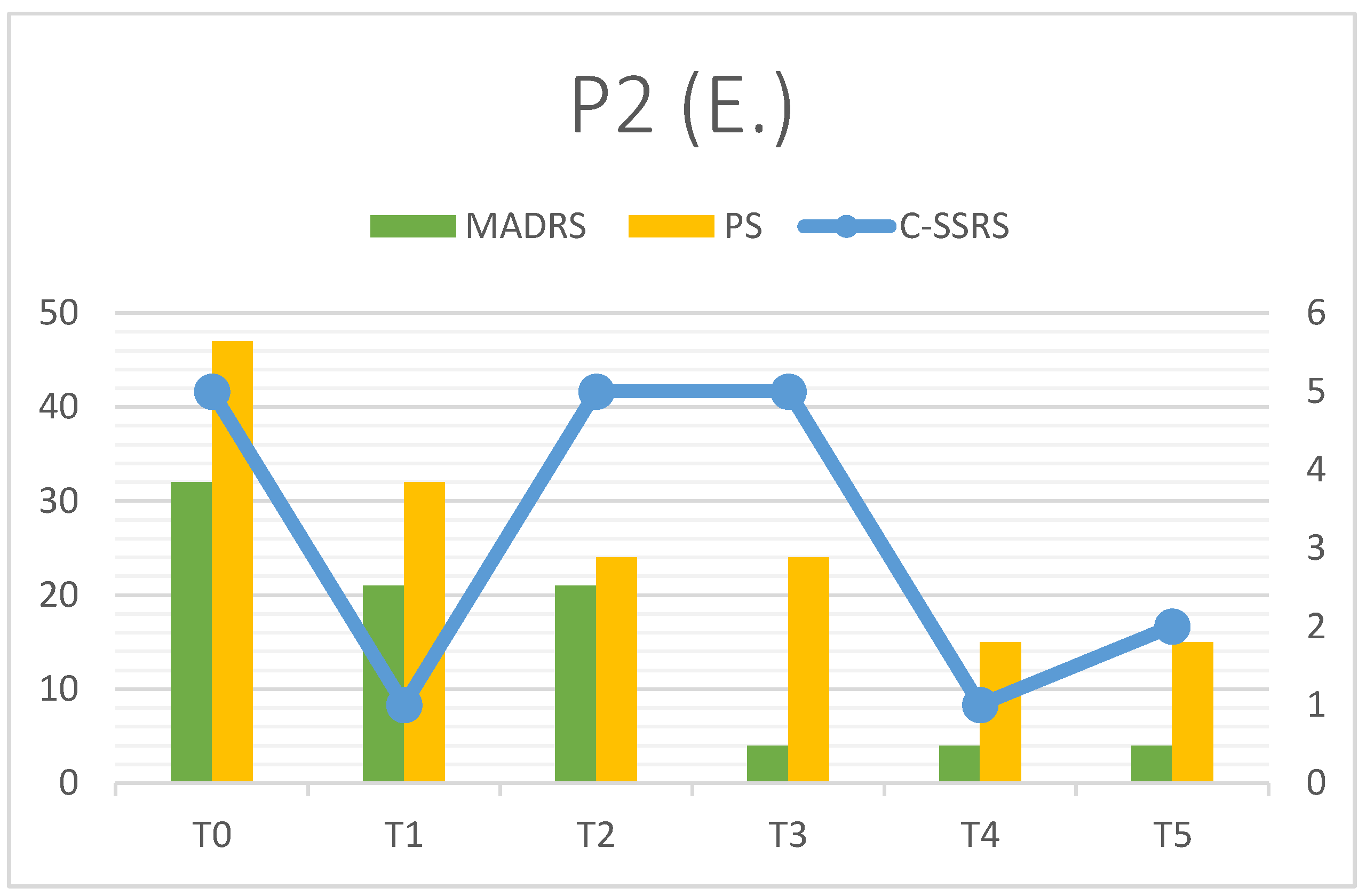
Table 4.
P2 results.
| P2 | MADRS | C-SSRS | PS | RFQ-8 | RMET | Q-LES-Q(%) |
| T0 | 32 | 5 | 47 | 2.5 | 26 | 25 |
| T1 | 21 | 1 | 32 | 2.25 | 22 | - |
| T2 | 21 | 5 | 24 | 2 | 23 | - |
| T3 | 4 | 5 | 24 | 2 | 23 | - |
| T4 | 4 | 1 | 15 | 2 | 23 | - |
| T5 | 4 | 2 | 15 | 2 | 23 | 71 |
3.3. Patient 3
A. is a 25-year-old woman born in Romania, but who was lived in United Kingdom, where she graduated in Neurosciences at the University of Cardiff. After graduation she moved to Milan to attend a PhD in Neuropsychopharmacology. During childhood she faced early scholastic difficulties. Intellectual disability and specific learning disorders were excluded so hypothesis of a neurodevelopmental disorder was made. A diagnosis of ADHD was carried out considering the profile of hyperactivity and inattention which are responsible for most difficulties at school. Methylphenidate was prescribed but early interrupted due to poor compliance. Nevertheless, her academic path was completed without rejections. At the age of 22 the diagnosis of ASD Level 1 was performed in consideration of persistent social avoidance, rigid thinking and/or behavioural pattern and hypersensitivity. IQ was evaluated and good cognitive functioning was confirmed (130). The first MDD occurred in 2018 during high school; after remission, she underwent 3 depressive episodes not requiring hospitalization. No evidence of family psychopathology. Many pharmacological approaches were used: several SSRIs were prescribed without significant effect, SNRIs were poorly tolerated (different and quite unclear side effects) and a Tricyclic Antidepressant (Amitriptyline) determined only a partial response. Augmentation strategies with Mood Stabilizers (Lamotrigine) and Second-Generation Antipsychotics (Risperidone, Aripiprazole, Quetiapine, Amisulpride) were useless. Methylphenidate was prescribed again in Italy (50 mg/day), and it offered a partial improvement considering cognitive symptoms. In accordance with the patient. Esketamine was prescribed in 2025 adding-on oral therapy with Escitalopram up to 20 mg/day; this therapy is still ongoing.
With Esketamine A. underwent a significative improvement, testified by a rapid decrease in MADRS and PS scores. It is possible to notice an isolated peak in MADRS score (18) at T3, when A. confessed that she has suspended Methylphenidate for a second time. This led to a rapid worsening in cognitive symptoms detected with MADRS. This also showed the importance of specific treatment in ADHD comorbidity; despite some resistances, A. demonstrated good compliance to therapy, resuming the pharmacotherapy with Methylphenidate soon after the visit. SI was absent from the beginning and C-SSRS=0 remained stable during follow-up. Psychache also saw a solid improvement (54 at T0, 18 at T5) and like MADRS it showed a relative peak at T3 (40). Mentalization was sufficient at T0 (2) but it was characterized by an apparent worsening during follow-up (T5=4) in the absence of dysregulation episodes. RMET score 26.83±1.47 was comparable to neurotypical mean and showed a little increase in six months.
A. reported an increased quality of life at T5 (80% vs 35% at T0), the bigger improvement was noted in social relations (percentage of satisfaction moved from 30% at T0 to 84% at T5).
Figure 3.
P3 outcomes (depressive symptoms).
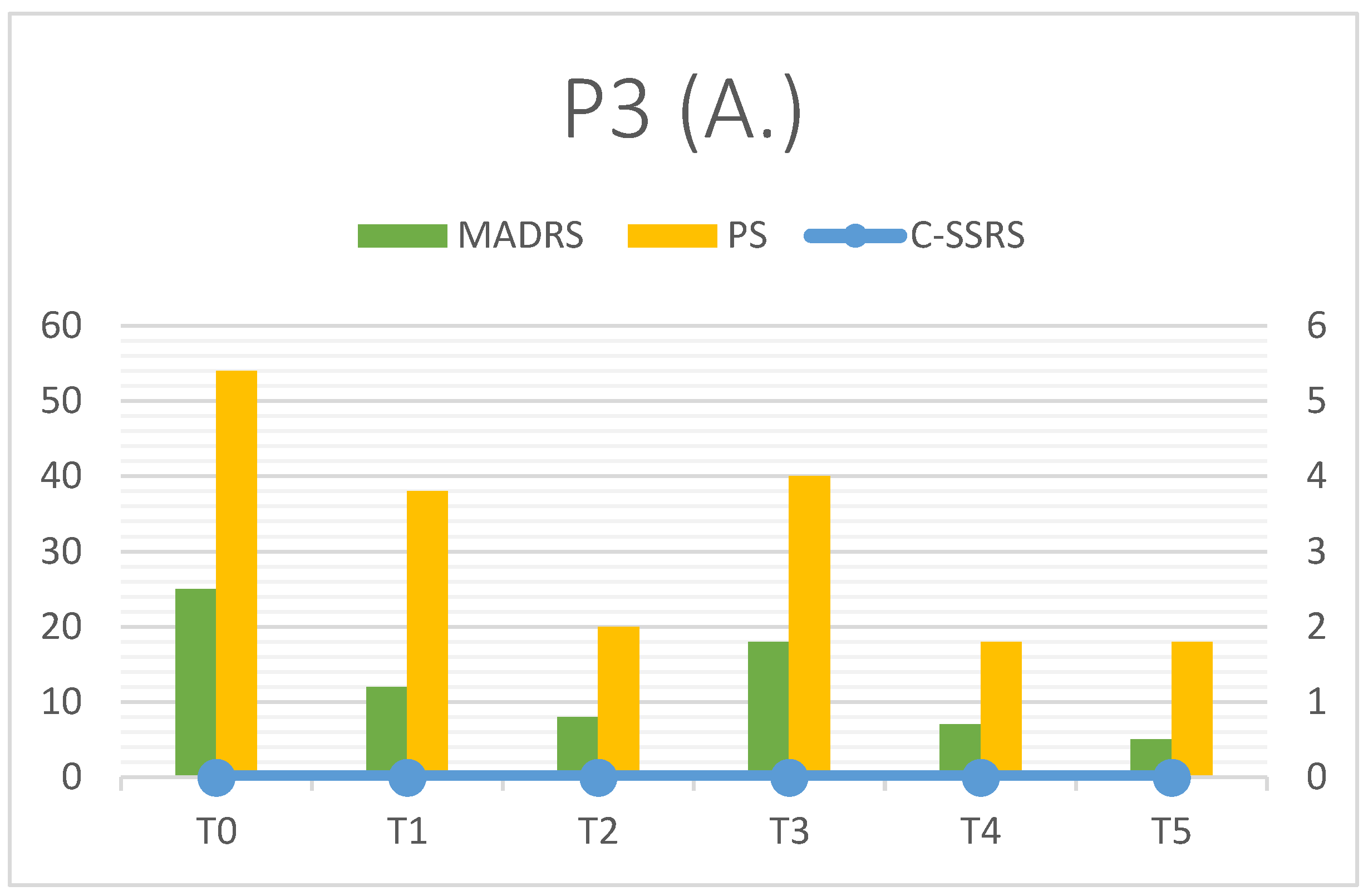
Table 5.
P3 results.
| P3 | MADRS | C-SSRS | PS | RFQ-8 | RMET | Q-LES-Q(%) |
| T0 | 25 | 0 | 54 | 2 | 26 | 35 |
| T1 | 12 | 0 | 38 | 3 | 27 | - |
| T2 | 8 | 0 | 20 | 4 | 25 | - |
| T3 | 18 | 0 | 40 | 3 | 26 | - |
| T4 | 7 | 0 | 18 | 4 | 28 | - |
| T5 | 5 | 0 | 18 | 4 | 29 | 80 |
4. Discussion
4.1. Summary of Findings and Interpretation
Our preliminary data is not enough to formalize statistical conclusions, so this small case series can be considered as an exploratory work. Even considering a very small sample size, Esketamine seemed to be efficacious in patients with TRD and ASD, with a good safety profile: all patients tolerated the pharmacological intervention well, in the absence of severe side effects. Nausea with vomiting was noted in one episode (P1, T4) confirming the profile of minor side effects known for Esketamine. Vital signs monitored during administrations (blood pressure, temperature, heart rate, blood oxygen saturation) showed no significant modifications in six months.
All patients observed showed a rapid decrease in MADRS total score (T0-T1). P1 and P3 reached a significant clinical response (dMADRS of 67.57% and 52% respectively), while P2 showed a partial but promising response (dMADRS=43.24%). Considering the whole observation period (T5), P2 and P3 achieved clinical remission in depressive symptoms (MADRS<10), P1 remission was incomplete due to a depressive relapse that occurred during treatment. Esketamine seemed to improve other symptoms investigated as secondary outcomes: psychache decreased in all patients such as suicidal ideation, which could be the most dangerous symptom in depression with autism comorbidity. It is interesting that suicidal thoughts, when present, are partially linked to depressive trend but they can follow a quite separate trajectory (Figure 1 and Figure 2). In our opinion this finding should point out the importance of a specific diagnosis and follow-up on suicidal ideation to prevent serious consequences for patients: in particular, patients with TRD and ASD may be associated with an elevated risk of suicide. Esketamine add-on showed promising results in decreasing suicidal ideation and this could be related to the specific pharmacological profile (NMDA receptors blocking with sedation and mild dissociative effect). Administration setting (repeated accesses in Mental Health Service, multiple contacts with clinicians and/or nurses) could also assume a significant role in suicidality prevention. Mentalization and social cognition did not show substantial modification during treatment, but data testified the clinical heterogeneity of these features in people affected with ASD, suggesting the importance of personalized approaches. Furthermore, subjective quality of life was characterised by constant increase in six months: this could suggest the efficacy of Esketamine in reducing the lack of functioning observed in depressive episodes, but also the good tolerance to therapy setting (frequent accesses in clinic, clinical monitoring). As our patients reported in follow-up visits, Esketamine administrations were not associated with organization problems and/or modifications in everyday life.
Last consideration is about clinical impact: we tried to explain the reason why these three patients with similar diagnoses showed different responses to Esketamine. This pharmacological intervention was substantially effective in all patients, as the rapid decrease in in depressive symptoms testified (see dMADRS T0-T1). Confirm in clinical response during observation period led to remission at T5 (P2 and P3) whereas P1 improvement was limited by an external factor (trauma) which caused a major relapse. Trauma was limited to a specific episode just before T3 (MADRS=19) but depressive symptoms were more pronounced at T4 (MADRS=43). After this time point, another improvement was observed with a strong decrease at T5 (MADRS=21) in the absence of clinical remission. Trauma represented a serious worsening factor but, in our opinion, also mentalization played a key role. Theory of Mind implicates understanding social situations but also facts and/or behaviours, allowing a better tolerance to everyday life stressors. P1 had been associated with the higher RFQ8 mean score (3.83±0.71) and after trauma showed a major relapse; P2 showed quite good mentalization ability during observation period (RFQ8=2.13±0.21) and this could have represented a protecting factor from suicidal behaviours observed in the past. P3 also scored high RFQ (3.33±0.82) but in the absence of precipitating causes worsening did not occur; it is important to notice that her anamnesis at baseline was negative for suicidal ideation/behaviours.
4.2. Comparison to Literature
Our research work was focused on efficacy and safety of intranasal Esketamine in a special population (people with TRD and comorbid ASD). Autism is a frequent comorbidity among psychiatric disorders and there are a lot of autistic patients who suffer from depressive episodes. Nevertheless, there are no studies which investigate the therapeutic role of Esketamine in people with ASD. MADRS score was selected to monitor depressive symptoms during follow-up as most of the studies which investigated Esketamine efficacy. Obviously, our sample size could not be associated with statistical analysis, so we adopted a descriptive approach. Reported results define a similar response to Esketamine in a six-month follow-up[19]. An early decrease in MADRS score was noted during induction phase (first month, two administrations/week) and it was confirmed during maintaining phase (second month, one administration/week; months 3 to 6, personalized frequency). The clinical trend seemed comparable to other studies for both timing and efficacy; in particular, a solid improvement during the first month of treatment was noted also in our patients with ASD as a comorbidity[20]. Considering the safety profile, adverse events reported by our patients were very mild and they include one nausea episode with vomiting (P1). Headache and major increases in blood pressure were never noted; mild dizziness was often described but it was reported as a quite pleasant event.
4.3. Strength and Limitations
In our opinion, the strong points of this case report are the focus on an understudied population (people who suffer from ASD and TRD) and the innovative approach with Esketamine+SSRI/SNRI to treat depressive symptoms. Also the presentation of raw data and test scores can be useful to draw a real-world experience and offer suggestions for further studies.
The main weakness of the research may be the elevated inter-individual variability with no standardisation (difference in oral antidepressant therapy, duration of Esketamine trial and administrations frequency). Other limitations are the lack of placebo controls, the lack of control group (neurotypical people treated with Esketamine for TRD), the short follow-up period and the absence of blinding (assessor bias). Publication bias is not mentioned because patients recruited for the study were the only patients with a co-diagnosis of TRD and ASD.
4.4. Future Research Directions
We hope that this case series can be the basis for larger studies. The first step could be an observational study with a bigger sample to confirm the preliminary results of efficacy and tolerance. Then, a case-control analysis could be set up: autistic patients treated with TRD treated with Esketamine could be compared to neurotypical patients, checking possible differences in terms of clinical response. Also, blind or double-blind studies would be easier to set up, investigating the effective action of Esketamine compared to placebo or other antidepressants. Finally, it will be interesting to consider other variables, such as neuro-functional biomarkers (fMRI and/or EEG correlates).
5. Conclusions
In our experience Esketamine represented a valid treatment for TRD in patients with ASD. It was characterized by a good efficacy, with a rapid and significant decrease in depressive symptoms including suicidal ideation (when present). The pharmacological profile was favourable in terms of safety and tolerability, no major side effects were reported. With more studies and scientific evidence, Esketamine could become a therapeutic option for patients with MDD and comorbid autism, who were often characterized by resistance to treatment and moderate to high suicidal risk.
References
- Malhi, GS; Mann, JJ. Depression. Lancet 2018, 392(10161), 2299–2312. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Depressive disorders (depression). 29 August 2025. Available online: www.who.int/news-room/fact-sheets/detail/depression.
- McIntyre, RS; Filteau, MJ; Martin, L; Patry, S; Carvalho, A; Cha, DS; Barakat, M; Miguelez, M. Treatment-resistant depression: definitions, review of the evidence, and algorithmic approach. J Affect Disord 2014, 156, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Gold, SM; Köhler-Forsberg, O; Moss-Morris, R; Mehnert, A; Miranda, JJ; Bullinger, M; Steptoe, A; Whooley, MA; Otte, C. Comorbid depression in medical diseases. Nat Rev Dis Primers 2020, 6(1), 69. [Google Scholar] [CrossRef] [PubMed]
- Lai, MC; Kassee, C; Besney, R; Bonato, S; Hull, L; Mandy, W; Szatmari, P; Ameis, SH. Prevalence of co-occurring mental health diagnoses in the autism population: a systematic review and meta-analysis. Lancet Psychiatry 2019, 6(10), 819–829. [Google Scholar] [CrossRef] [PubMed]
- Richa, S; Fahed, M; Khoury, E; Mishara, B. Suicide in autism spectrum disorders. Arch Suicide Res. 2014, 18(4), 327–39. [Google Scholar] [CrossRef] [PubMed]
- McDonald, R. G.; Cargill, M. I.; Khawar, S.; Kang, E. Emotion dysregulation in autism: A meta-analysis. Autism 2024, 28(12), 2986–3001. [Google Scholar] [CrossRef] [PubMed]
- Dell’Osso, L.; Massoni, L.; Battaglini, S.; De Felice, C.; Nardi, B.; Amatori, G.; Cremone, I. M.; Carpita, B. Emotional dysregulation as a part of the autism spectrum continuum: a literature review from late childhood to adulthood. Frontiers in psychiatry 2023, 14, 1234518. [Google Scholar] [CrossRef] [PubMed]
- Mazefsky, CA; Herrington, J; Siegel, M; Scarpa, A; Maddox, BB; Scahill, L; White, SW. The role of emotion regulation in autism spectrum disorder. J Am Acad Child Adolesc Psychiatry 2013, 52(7), 679–88. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- de la Torre-Luque, A; Essau, CA; Lara, E; Leal-Leturia, I; Borges, G. Childhood emotional dysregulation paths for suicide-related behaviour engagement in adolescence. Eur Child Adolesc Psychiatry 2023, 32(12), 2581–2592. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, B.; Wu, C.; Wang, J.; Sun, M. Autism Spectrum Disorder: Neurodevelopmental Risk Factors, Biological Mechanism, and Precision Therapy. International journal of molecular sciences 2023, 24(3), 1819. [Google Scholar] [CrossRef] [PubMed]
- Ruggieri, V. Autismo. Tratamiento farmacológico [Autism. Pharmacological treatment]; Medicina (B Aires): Spanish, Sep 2023; Volume 83, Suppl 4, pp. 46–51. [Google Scholar] [PubMed]
- Siafis, S.; Çıray, O.; Wu, H.; et al. Pharmacological and dietary-supplement treatments for autism spectrum disorder: a systematic review and network meta-analysis. Molecular Autism 2022, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Fedgchin, M; Trivedi, M; Daly, EJ; Melkote, R; Lane, R; Lim, P; Vitagliano, D; Blier, P; Fava, M; Liebowitz, M; Ravindran, A; Gaillard, R; Ameele, HVD; Preskorn, S; Manji, H; Hough, D; Drevets, WC; Singh, JB. Efficacy and Safety of Fixed-Dose Esketamine Nasal Spray Combined With a New Oral Antidepressant in Treatment-Resistant Depression: Results of a Randomized, Double-Blind, Active-Controlled Study (TRANSFORM-1). Int J Neuropsychopharmacol 2019, 22(10), 616–630. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vasiliu, O. Esketamine for treatment-resistant depression: A review of clinical evidence (Review). Exp Ther Med 2023, 25(3), 111. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Anashkina, AA; Erlykina, EI. Molecular Mechanisms of Aberrant Neuroplasticity in Autism Spectrum Disorders (Review). Sovrem Tekhnologii Med.;Epub 2021, 13(1), 78–91. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sato, W; Uono, S; Kochiyama, T; Yoshimura, S; Sawada, R; Kubota, Y; Sakihama, M; Toichi, M. Structural Correlates of Reading the Mind in the Eyes in Autism Spectrum Disorder. Front Hum Neurosci 2017, 11, 361. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fonagy, P; Luyten, P; Moulton-Perkins, A; Lee, YW; Warren, F; et al. Development and Validation of a Self-Report Measure of Mentalizing: The Reflective Functioning Questionnaire. PLOS ONE 2016, 11(7), e0158678. [Google Scholar] [CrossRef] [PubMed]
- Wajs, E; Aluisio, L; Holder, R; Daly, EJ; Lane, R; Lim, P; George, JE; Morrison, RL; Sanacora, G; Young, AH; Kasper, S; Sulaiman, AH; Li, CT; Paik, JW; Manji, H; Hough, D; Grunfeld, J; Jeon, HJ; Wilkinson, ST; Drevets, WC; Singh, JB. Esketamine Nasal Spray Plus Oral Antidepressant in Patients With Treatment-Resistant Depression: Assessment of Long-Term Safety in a Phase 3, Open-Label Study (SUSTAIN-2). J Clin Psychiatry 2020, 81(3), 19m12891. [Google Scholar] [CrossRef] [PubMed]
- Popova, V; Daly, EJ; Trivedi, M; Cooper, K; Lane, R; Lim, P; Mazzucco, C; Hough, D; Thase, ME; Shelton, RC; Molero, P; Vieta, E; Bajbouj, M; Manji, H; Drevets, WC; Singh, JB. Efficacy and Safety of Flexibly Dosed Esketamine Nasal Spray Combined With a Newly Initiated Oral Antidepressant in Treatment-Resistant Depression: A Randomized Double-Blind Active-Controlled Study doi: 10.1176/appi.ajp.2019.19020172. Epub 2019 May 21. Am J Psychiatry Erratum in: Am J Psychiatry. 2019 Aug 1;176(8):669. doi: 10.1176/appi.ajp.2019.1768correction1. PMID: 31109201. 2019, 176(6), 428–438. [Google Scholar] [CrossRef] [PubMed]
Table 1.
Clinical and demographical features.
| PATIENT 1 (G.) | PATIENT 2 (E.) | PATIENT 3 (A.) | |
| GENDER AND AGE | Female, 25y | Male, 20y | Female, 25y |
| JOB | Student Writer assistant |
Farm worker | Student |
| AUTISM SEVERITY | Level 2 | Level 2 | Level 1 |
| INTELLECTUAL DISABILITY | No (IQ 107) | No (IQ 137) | No (IQ 130) |
| FAMILIAR ANAMNESIS | Major depressive disorder (mother) Panic disorder (father) |
Bipolar Disorder (mother) | Negative |
| MEDICAL COMORBIDITIES | No | Sever obesity, hypertension | No |
| HOSPITALIZATIONS | Suicidal ideation (2021) | Suicidal attempt (2023) Suicidal ideation (2024) |
No |
| SUICIDAL ATTEMPTS | No | 1 (setting fire) | No |
| SELF-HARMING | Yes (cutting, cigarette burns) | No | No |
| DRUG USE | No | Alcohol (occasional) | No |
| ORAL PHARMACOTHERAPY | Sertraline 200 mg/day Aripiprazole 15 mg/day |
Venlafaxine 300 mg/day Lurasidone 74 mg/day |
Escitalopram 20 mg/day Methylphenidate 50 mg/day |
| ESKETAMINE POSOLOGY | 84 mg | 84 mg | 84 mg |
| ESKETAMINE DURATION | 6 months | 15 months (ongoing) | 9 months (ongoing) |
| HOSPITALIZATIONS DURING ESKETAMINE | No | No | No |
| SUICIDAL ATTEMPTS DURING ESKETAMINE | No | No | No |
| SELF-HARMING DURING ESKETAMINE | Yes (1 episode) | No | No |
Table 2.
Assessment tools.
| DOMAIN | SCALE | ABBREVIATION | SCORE |
| Depression | Montgomery-Asberg Depression Rating Scale | MADRS | 0-60 |
| Psychological pain | Psychache Scale | PS | 13-65 |
| Suicidality | Columbia Suicide Severity Rating Scale | C-SSRS | If present, assess “Ideation” subscale 1-5 |
| Social Cognition | Reading the Mind in the Eyes Test | RMET | 0-36 |
| Mentalization | Reflective Functioning Questionnaire (8th version) | RFQ8 | 1-7 |
| Quality of Life | Quality of Life Enjoyment and Satisfaction Questionnaire | Q-LES-Q | 0-100% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



