
Submitted:
28 March 2025
Posted:
31 March 2025
You are already at the latest version
Abstract
Background/ Objective: Major depressive disorder (MDD) is a common mental disorder, with a significant part of patients developing treatment-resistant depression (TRD). Esketamine is an antagonist of the N-methyl-D-aspartate receptor indicated as a nasal spray in combination with other antidepressants for adults with TRD. Signals of suspected adverse reactions (SARs) to esketamine from the EudraVigilance database in European countries were analyzed for a more defined safety profile of this drug in the real-world. Methods: SARs to esketamine reported in the data system EudraVigilance were analyzed and disproportionality analysis for adverse reactions indicating sui-cidality for esketamine, in comparison to the antidepressants fluoxetine and ven-lafaxine, was performed. Results: “Blood pressure increased” (15.4%) and “Dissocia-tion” (15.0%), are the more frequently reported SARs. Sex distribution indicates prevalence of women, except for “Blood pressure increased” and “Completed suicide”, more signaled for men, while adults (18-64 years) and elders (65-85 years) are the ages with the largest number of reported adverse reactions to esketamine. Results show a significant increase of risk of suicide for esketamine, when compared with fluoxetine and venlafaxine. Conclusions: Apart of carefulness due to the known limitations of pharmacovigilance research conducted by using datasystem of spontaneous signals for SARs, analysis of data on points towards the need for greater attention for risk suicide following prescription of esketamine in depressed subjects. In this regard, as well as regulatory agencies recommend, patients with a history of suicide-related events or those exhibiting a significant degree of suicidal ideation prior to begin treatment, should receive a more careful monitoring during treatment.
Keywords:
esketamine
; pharmacovigilance
; adverse reactions
; major depressive disorder
; treatment-resistant depression
; suicide
1. Introduction
Major depressive disorder (MDD) is a common mental disorder, and a significant part of patients diagnosed with this disorder do not achieve complete recovery (remission phase lasting for at least six months) even in the face of multiple pharmacological trials, developing a form of Major depressive disorder (MDD) is a common mental disorder, and a significant part of patients diagnosed with this disorder do not achieve complete recovery (remission phase lasting for at least six months) even in the face of multiple pharmacological trials, developing a form of treatment-resistant depression (TRD) [1]. The concept of depression resistant to antidepressant pharmacological treatment was officially introduced by Lehmann in 1974 [2] and described over time through studies and publications that have outlined its profile [3]. At present, however, there is no precise definition of TRD, which is why clinicians and researchers tend to embrace the postulate formulated at the turn of the century. according to which a subject is resistant to treatment when successive therapies, conducted consecutively with two molecules belonging to different pharmacological classes, do not produce acceptable therapeutic effects even if taken for a sufficient period of time and at an adequate dosage [4]. TRD concept is applied in clinical practice when two or more successive treatments with different antidepressant drugs were not working [5].
Research in new pharmacological therapies for TRD has taken two main paths. One followed the use of typical serotonergic drugs and another less typical way on glutamatergic or psychedelics substances such as ketamine and esketamine [6]. A major breakthrough in the treatment of depression was the observation that the racemic mixture (R,S)-ketamine (hereafter referred to as ketamine), well-characterized pharmacologically as an NMDA receptor (NMDAR) antagonist, produced rapid and long-lasting antidepressant effects in humans [7,8]. NMDA receptor antagonists show similar behavioral and neurochemical profiles to antidepressants [9]. Ketamine is a high-affinity NMDA non-competitive receptor antagonist. This result is consistent with reports that NMDA antagonists mimic the effects of clinically effective antidepressants [10]. Ketamine was first derived from phencyclidine and administered to humans in the 1960s to establish new anesthetic compounds. Indeed, ketamine produced a dissociative and anesthetic state in humans that led to its use as an anesthetic and analgesic [11]. However, the antidepressant effects of ketamine were not fully realized until decades later [12].
Ketamine, induces rapid and significant antidepressant effects within a few hours. Due to the rapid antidepressant effects of ketamine, unlike the delayed beginning of impact of traditional antidepressant drugs [13], research on this drug has continued and revealed its mechanisms of action and potential drug targets. Mechanism of action of ketamine seems to be related to the pharmacological properties of its metabolites. Indeed, ketamine is rapidly metabolized, resulting in neuroactive products that likely contribute to its therapeutic effects. It undergoes its first metabolic transformation to (R,S)-norketamine in the liver. Subsequently, (R,S)-norketamine can be converted to (R,S)-dehydronorketamine (DHNK) or (R,S)-hydroxynorketamine (HNK) [14]. Esketamine is the S-enantiomer of racemic ketamine. It is a nonselective, noncompetitive antagonist of the N-methyl-D-aspartate (NMDA) receptor [15,16].
Through NMDA receptor antagonism, esketamine produces a transient increase in glutamate release, resulting in increased α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR) stimulation and subsequent increases in neurotrophic signaling. Thus, it seems to contribute to the restoration of synaptic function in brain regions involved in the regulation of mood and emotional behavior [17]. Restoration of dopaminergic neurotransmission in brain regions involved in reward and motivation and reduced stimulation of brain regions involved in anhedonia may contribute to the rapid response [18]. European Medicines Agency (EMA) in 2019 approved Esketamine as a nasal spray that delivers a total of 28 mg of esketamine in two actions (one in each nostril), in combination with a selective serotonin reuptake inhibitor (SSRI) or a serotonin and norepinephrine reuptake inhibitor (SNRI), for adults with treatment-resistant Major Depressive Disorder (MDD), who have not responded to at least two different treatments with antidepressants in the current moderate to severe depressive episode. Furtherly, co-administered with oral antidepressant therapy, is indicated in adults with a moderate to severe episode of MDD, as acute short-term treatment, for the rapid reduction of depressive symptoms, which according to clinical judgement constitute a psychiatric emergency. The most commonly observed adverse reactions in patients treated with esketamine based on data collected for clinical studies used for market registration of the drug were dizziness (31%), dissociation (27%), nausea (27%), headache (23%), somnolence (18%), dysgeusia (18%), vertigo (16%), hypoaesthesia (11%), vomiting (11%), and blood pressure increased (10%) [19].
However, postmarketing occurrence of respiratory depression associated with esketamine treatment has been signaled but no adverse events of respiratory depression were reported in ESK phase 3 clinical trials. Moreover, in a study involving fifty cases of depressed patients treated with esketamine matching definition for respiratory depression, only 8 of these showed a stronger association with esketamine therapy [20].
Another study based on a total of 2907 female reports and 1634 male reports on esketamine extracted from the databank Food and Drug Administration on Adverse Event Reporting System (FAERS) showed that completed suicide, decreased therapeutic product effects, urinary retention, and hypertension were common in men [21]. Analysis of data on neurological adverse events caused by esketamine and extracted from FAERS suggests that a higher dose of esketamine, antidepressant polypharmacy, and combination treatment with benzodiazepines or somatic medications are more likely to be risk factors related to adverse events severity, instead age and sex are not [22].
In the present study, we analyzed signals of suspected adverse reactions to esketamine from the EudraVigilance database in order to detect and characterize relevant safety signals deriving from prescription of this drug in depressed patients in European countries. A descriptive statistical analysis was conducted to highlight the results obtained through data mining of esketamine signals of adverse reactions and a disproportionality analysis using the reporting odds ratio to compare the safety profile related to suicidal events between esketamine and the antidepressants fluoxetine [23] and venlafaxine [24] was operated.
2. Results
A total of 751 ICSRs related to Esketamine were identified in the Eudravigilance database as signals for adverse reactions to esketamine in the period from 2019 (year of market entry of the drug) to 31 December 2024. Of these reports, 265 were categorized as serious cases (35.3% of the total number of ICSRs) and 486 as non-serious cases. The distribution by sex shows that of the 490 non-serious cases, 306 reports are related to female subjects (62.4%) and 168 to male subjects. Similar percentages are observed with serious cases: 169 of female cases (63.8%) and 96 of male cases, thus indicating that both serious and non-serious cases are more frequent in women. However, among serious cases, death results in 27 cases, of which 18 are about men (66.7%). Most of cases of death were caused by suicide. Total cases of death not caused by suicide are 17 (63% of cases of death); 12 were men and 5 women, showing a larger percentage of suicide in men (70.6%). Frequency in descending order of single adverse reactions indicates that “Blood pressure increased”, “Dissociation/Dissociative disorder”, “Anxiety” and “Completed suicide” are more often related to esketamine than other serious events (Figure 1). Statistical analysis of sex distribution shows that the adverse reactions “Blood pressure increased” and “Completed suicide” are signaled more frequently for men. “Dizziness” is the adverse reaction to esketamine involving prevalently women. There is no statistical difference in sex distribution of the other adverse reactions to esketamine (Table 1). Age distribution of cases shows that adult age (18-64 years) and elderly (65-85 years) are more affected. This is a predictable result, because in these ages esketamine is more naturally prescribed for depression. No statistical difference is revealed by data analysis, except for “Blood pressure increased” more signaled in elderly (65-85 years). Moreover the adverse reaction “hallucination” is only reported in adults (18-64 years) (Table 2). Cases of death not including suicide, among all serious SARs caused by esketamine, are 3.8% with the prevalence of men (2.3%) in comparison to women (1.5%). Most of these fatal events were observed in the group of adult patients (Table 3). Diagnoses related to deaths associated with esketamine were three cases of sudden death and other single diagnoses such as respiratory failure, pulmonary embolism, myocardial infarction. ROR and PRR results regarding groups of adverse reactions aggregated according to the SOC levels show as signals for adverse reactions to esketamine produced both ROR and PRR increased in comparison to signals for adverse reactions to both fluoxetine and venlafaxine. In particular these parameters are increased for “Psychiatric disorders”, “Vascular disorders” and “Immune system disorders” among adverse reactions to esketamine (Table 4). Most of psychiatric disorders potentially caused by esketamine are represented by single adverse reactions such as “Dissociation/Dissociative disorders”, followed by “Suicidal ideation”, “Anxiety” and “Completed suicide”. Vascular disorders signaled for esketamine are for the most dizziness and hypertension, while for immune system disorders several cases of anaphylactic reactions (Table 1, Table 2). ROR and PRR of cases signaling the single adverse reactions “Suicidal ideation”, “Suicide attempt” and “Complete suicide” suspected to be caused by esketamine in comparison with the two antidepressant drugs fluoxetine and venlafaxine, show an increased risk of “Suicidal ideation” with esketamine compared to fluoxetine (ROR 2.94 and PRR 2.75; C.I.1.75-4.94) and a more increase of risk in comparison to venlafaxine (ROR 5.25 and PRR 4.83; C.I. 3.15-8.73). Light increase of risk was also detected in “Suicide attempt” with esketamine in comparison to venlafaxine (ROR 1.05 and PRR 1.04; C.I. 0.59-1.86). Significant increase of risk with esketamine was detected with calculation of signals regarding “Completed suicide” comparing signals with those of fluoxetine (ROR 8.05 and PRR 7.60; C.I. 3.55-18.3) and even more with venlafaxine (ROR 10.58 and PRR 9.96; C.I. 5.08-22.04). Comparison of signals for “Suicidal ideation”, “Suicide attempt“ and “Completed suicide” between fluoxetine and venlafaxine showed only a moderate increase of risk with fluoxetine treatment (Table 5).
3. Discussion
The approvation by FDA and EMA of N-methyl-D-aspartate/glutamate receptor (NMDAR) antagonists for therapy of depression opened a large debate in the fields of psychiatry and psychopharmacology. Their use is based on the observation of depression-related alterations in glutamate synaptic signaling, such as reduced amplitude of sensory evoked potentials and reduction of cortical functional connectivity [25], reduced synaptic density and disrupted synaptic glutamate homeostasis [26,27] together with elevation of extracellular glutamate levels, overstimulating extrasynaptic N-methyl-D-aspartate (NMDA) receptors (NMDAR) [28]. On the light of these findings, it is believed that, if used appropriately, the efficacy of NMDAR antagonists, including esketamine, can have a positive impact on the life of people suffering from depression, and in consequence of this, on the public health burden associated with TRD [29].
MDD is highly prevalent and it is associated with substantial burden and high economic costs represented by drugs, diagnostic exames and laboratory investigations and absence or poor performance at work [30]. The largest portion of subjects affected by MDD are not sufficiently responsive to first-line treatments and in a significant part of them failure of multiple antidepressant pharmacological treatments is detected, resulting in what is called TRD [31]. After its release in the drug market, many studies investigated on the clinical effects of esketamine. Esketamine nasal spray has been studied in the long-term trials SUSTAIN-1 and SUSTAIN-3 conducted on patients with TRD. A subgroup analysis of SUSTAIN-3 evaluated 96 patients with TRD who received a second induction and maintenance treatment with esketamine plus oral antidepressant after a relapse in SUSTAIN-1. The authors observed that patients with TRD benefitted from receiving a second induction and maintenance treatment with ESK and no new safety signals were identified [32].
Despite being approved by the FDA and EMA, the utility of esketamine nasal spray as add-on treatment with an antidepressant in MDD is still debated. A meta-analysis was conducted on 9 randomized clinical trials comparing esketamine nasal spray versus control in MDD or TRD, with the aim to evaluate if this treatment could rapidly, effectively, and persistently to control depressive symptoms, in a short- and long-term period. The authors concluded that esketamine nasal spray in conjunction with an antidepressant effectively controls short-term and long-term depressive symptoms in MDD and RTD, supporting its clinical utility [33].
Finally the most recent study investigating on the efficacy of esketamine nasal spray for TRD is a review and meta-analysis including five randomized clinical trials RCTs are included in the meta-analysis. In this study, the authors observed that adverse events, such as dizziness and nausea, were more common following esketamine treatment, but they were generally well-tolerated by patients, and concluded that esketamine nasal spray is beneficial to improve the efficacy of treatment-resistant depression [34].
Our post-marketing analysis of SARs contained in the signals sent to EudraVigilance, only partially confirms data used for authorization reported in the official summary of product characteristics. In the same document (associated with release of the drug), potential adverse reactions are listed according to the designated system organ classes (SOC). This classification reported as very common adverse reactions (≥ 1/10), the adverse reaction “Dizziness” and the psychiatric disorder “Dissociation”, and in the category of nervous system disorders, symptoms such as “Headache”, “Somnolence”, “Dysgeusia”, “Hypoaesthesia”. Other adverse reactions reported as very common were “Nausea”, “Vomiting” and “Blood pressure increased”. Our post-marketing only partially confirms this view and, in consequence of this, shows a different safety profile of esketamine.
In the EudraVigilance data system, used for this study, “Psychiatric disorders”, “Nervous system disorders”, “Vascular disorders” and “Investigations” (including “Blood pressure increased”) are the groups of adverse reactions most frequently signaled for esketamine. Among the single adverse reactions, “Blood pressure increased” (15.4% of all the SARs) and “Dissociation/Dissociative disorders” (15.0% of all the SARs), are those more frequently reported. Sex distribution indicates that women are prevalently implicated in ICSRs except for “Blood pressure increased” and “Completed suicide”, more signaled for men, while age distribution shows that adults (18-64 years) and elders (65-85 years) are the ages with the largest number of reported adverse reactions to esketamine. Patients with TRD treated with esketamine nasal spray commonly experience transient symptoms of dissociation. Dissociative disorders, such as feelings of detachment from the environment, cause also considerable anxiety for patients [35]. Adverse reactions signaled as “Anxiety” following esketamine prescription are also repeatdly reported in EudraVigilance. Increase of blood pressure is confirmed by another study carried out by analzing post-marketing safety signals of esketamine nasal spray, downloading data from the US FAERS from Q1 2019 to Q2 2023 and using methods of the disproportionality. The most frequently observed adverse events were dissociation, sedation, and hypertension [36].
Even though represents the adverse reaction more frequently signaled in relationship to esketamine prescription, blood pressure increase is generally considered as transient, asymptomatic, and not associated with serious cardiovascular safety sequalae [37]. In addition, cardiovascular effects characterized by increased blood pressure are partially expected based on esketamine sympathomimetic effect [18].
Previously, a randomized placebo-controlled trial investigated the efficacy and safety of 28, 56, or 84 mg of esketamine intranasal spray twice weekly for 4 weeks in 138 adults ≥65 years old with depression. The trial investigators reported a transient elevation in mean blood pressure in participants receiving esketamine that peaked at 40 minutes post-treatment and resolved in 2 hours in about 80% of participants [38]. Also our data reveal that risk of increase in blood pressure can be significantly augmented in elderly.
More recently, an increase in reporting of hepatobiliary adverse effects associated with esketamine use, supports the recommendation for periodic monitoring of hepatic function through laboratory testing and clinical surveillance. Safety information purchased by FDA supports the general advice leading to monitor periodically liver function in patients receiving chronically esketamine [39]. Association between esketamine and eye disorders such as cataracts and glaucoma has been studied by collecting data from FAERS. ROR of 1.31 with 95% C.I: 0.63-2.72 for cataract and of 2.19 with 95% C:I: 0.12-39.76 for glaucoma were found as related to esketamine adverse reactions, thus suggesting a greater risk for eye disorders [40].
Given that TRD is associated with chronic depression, suicidal behaviours, and reduction of quality of life [41] and the rate of suicidality, including completed suicide, is disproportionately higher in TRD populations [42], analysis of data founded in EudraVigilance about the adverse reactions “Suicidal ideation”, “Suicide attempt” and “Completed suicide” in association with esketamine prescription deserves further and separate discussion. Scientific literature on this argument reports several studies facing the problem of suicidality linked to esketamine use. Multiple severe adverse events during long-term treatment of 1 year with esketamine, including anxiety, delusional content, delirium, and suicidal ideation, have been reported. These adverse events were found in 0.06% of the sample, including a total of 3 deaths due to suicide. However, according to the authors of the report, only on the basis of these results, the attribution of suicide to esketamine treatment is difficult, due to insufficient consistency [43]. In antithesis to these results, recent evidence indicates that esketamine reduces measures of suicidality in people with TRD. Even though, in this case, the same authors declared that it is not clear if individuals experience worsening of preexisting suicidality with this drug. By using data from the Food and Drug Administration Adverse Event Reporting System (FAERS) database they collected data from 2019 to 2023 for reports of suicidal ideation, depression suicidal, suicidal behavior, suicidal attempt, and completed suicide in association with esketamine. Results showed a higher ROR for suicidal ideation (ROR 7.58, 95% CI 6.34–9.07) and depression suicidal (ROR 14.19, 95% CI 1.80–112.07), but a lower ROR for suicide attempt (ROR 0.57, 95% CI 0.48–0.67) with esketamine. Limitations of the FAERS database prevented any determination of a causal effect between new onset suicidality to esketamine. Consequently, authors concluded that ROR for suicide attempt with esketamine could not be interpreted as a direct therapeutic effect [44].
A previous study, also using the FAERS database and analyzing data of esketamine-related adverse events from March 2019 to March 2020, estimated the ROR and information component for esketamine-related adverse events with ≥ 4 counts. After comparing data with those of the antidepressant venlafaxine, safety signals for esketamine were detected for self-injurious ideation and suicidal ideation, but not for completed suicide, and suicide attempt. Authors of the study concluded that esketamine may carry a clear potential for serious adverse events, which requires urgent clarification [45].
More recently, 2 cases of depressive symptom deterioration and suicide ideation in patients treated with esketamine for TRD, were reported. The 2 cases initially responded well to intranasal esketamine but later deteriorated rapidly, with a worsening of depressive symptoms and suicidal ideation. Upon discontinuing esketamine, both patients clinically improved and showed a reduction in suicide ideation [46]. As suggested by the investigators publishing these cases, even if the identification of paradoxical reactions is difficult in TRD patients with highly resistant responses to treatment and suicidal ideation, it could be relevant to examine the prevalence of this phenomenon with the aim to ameliorate the knowledge of the real complications potentially associated with treatment with esketamine.
In a randomized, double-blind placebo-controlled clinical trial the effects of subclinical doses of esketamine on postpartum depression and pain following elective cesarean sections have been investigated. Based on results the authors concluded that esketamine did not reduce the incidence of postpartum depression at 14 days postpartum but did significantly lower pain visual analog scale scores at 24 hours post-surgery. Moreover, group of women treated experienced temporary increases in adverse reactions and sedation shortly after administration [47].
Furthermore, a systematic review and meta-analysis of the available data on esketamine efficacy against depression and suicidality and on its undesidered effects have been conducted through the analysis of 87 articles. Results showed that at weeks 2-4, randomized controlled trials were mostly negative or failed, but a weak significant positive effect for depression was detected at weeks 2-4. However, the effect size concerning suicidality was not significant at any time point. On the light of results, the authors concluded that esketamine’s efficacy as an add-on to antidepressants is modest in TRD patients and is absent against suicidality [48]. These aspects need to be considered in light of esketamine’s abuse potential and the fact that long-term effects are still not fully known.
Analysis of sex distribution indicates the adverse reaction “Completed suicide” is signaled more frequently for men. Considering differences in the pharmacokinetics and hormonal status in patients of different genders, difference in sex distribution observed in our analysis is not surprising. In this regard, a recent study, carried out on data from FAERS on signals of adverse reactions to esketamine of 2907 females and 1634 males, reported ROR results showing that completed suicide, was more common in men. Additionally, other 552 female and 653 male ketamine reports were analyzed with a ROR revealing that women were more likely to develop suicidal ideation [21].
Comparison of data about suicidality in the present work was performed against the antidepressants fluoxetine and venlafaxine. Analysis, even though strongly influenced by the different time of market availability between esketamine and the two drugs fluoxetine and venlafaxine, available for several decades while esketamine was authorized by the EMA in 2019 [49], shows a significant increase of risk of suicidality for this last substance. ROR is a disproportionality measure that can be used to confirm association between a drug and a certain adverse event. In our analysis association between suicidality and esketamine seems to be more strong than the same association with the drugs fluoxetine and venlafaxine, with the risk for completed suicide increased 4 times and 5 times in comparison to fluoxetine and venlafaxine, respectively. Furthermore, as yet above mentioned, the rate of suicidality is already high in TRD patients, and this makes it more difficult to assess how much esketamine might affect a frequency that is already elevated. Moreover, esketamine is a drug with low affinity for NMDAR and it can also bind to other targets, such as opioid receptors. For this reason, the precise mechanism of action for its antidepressant properties remains debated, as does its potential for misuse [50]. It is believed that esketamine’s psychoactive effects have a role either in the antidepressant effect or in its potential of abuse. Data from pharmacovigilance approach have suggested that they are badly experienced by certain individuals patients, while they are desidered by others [51]. Finally, an indication of risk of suicidality is emerging, even if the drug esketamine is prescribed for individuals affected by depression and naturally exposed to suicide, and it cannot be excluded that esketamine is indicated for TRD, a condition even more at risk for suicidality, since, compared with other patients with MDD, those with TRD show to do more suicide attempts [52]. Moreover, according to other authors, it is very difficult to differentiate between suicidal ideation as part of depression intended as disease with respect to suicidal ideation potentially related to lack of esketamine effectiveness, or as a reaction induced by esketamine [53].
The results of this study need to be interpreted with carefulness due to the known limitations of pharmacovigilance research conducted by using datasystem of spontaneous signals for drugs adverse reactions. These limitations include the lack of denominator, quality of information, uncertaintity of causal relationship. However, analysis of data on adverse reactions to esketamine in treatment-resistant depression present on EudraVigilance points towards the need for greater attention in the prescription of esketamine in depressed subjects. In particular, because of the significant risk of increase of suicidality that could derive from the use of this drug is of particular concern. In this regard, as well as regulatory agencies recommend, patients with a history of suicide-related events or those exhibiting a significant degree of suicidal ideation prior to begin treatment, should receive a more careful monitoring during treatment.
4. Materials and Methods
EudraVigilance is a database containing suspected adverse reactions (SARs) related to medicines authorised for the market or currently undergoing clinical trials in the European Union (EU). In this data system, SARs are traceable in individual cases (Individual Cases Safety Reports; ICSRs) signaled by national drug regulatory authorities in the EU or by marketing authorisation holders.
In this study, we analysed ICSRs reporting SARs that occurred in patients to whom esketamine was prescribed, signaled by healthcare professionals from 1 January 2019 to 24 November 2024. It is noteworthy that EudraVigilance collects reports of “suspected” adverse reactions, meaning unwanted medical events that have been observed following the use of a medicine, but which are not necessarily related to or caused by the medicine itself [54]. For this research, the public version of the EudraVigilance database was used and only reports from the European Economic Area and the United Kingdom (UK) were evaluated. For all cases, information was provided on patient characteristics (age group and sex), type of adverse reaction (often more than one for each ICSR), qualification of the primary source. The terms “sex” and “gender” are used interchangeably here because only the field containing the term “sex” is available in EudraVigilance, consequently the information collected refers to biological sex. Regarding the data selection criteria, ICSRs reporting SARs were selected based on the Medical Dictionary for Regulatory Activities (MedDRA). MedDRA is an international standardized and clinically validated medical terminology used by regulatory authorities and the biopharmaceutical industry. It is used to code cases of adverse effects in pharmacovigilance databases and to facilitate searches in the databases on adverse drug reactions. Single adverse reactions were described using the so-called “Preferred terms” (PT) listed in MedDRA. A PT is a distinct descriptor (single medical concept) for an adverse symptom or sign. Two or more PTs with overlapping clinical meaning were aggregated to avoid unnecessary duplicate PTs with the same connotation. MedDRA has a hierarchy of terms to describe adverse reactions. Adverse reactions are grouped under the terms of the SOC (System Organ Classification) level in the MedDRA hierarchy such as musculoskeletal and connective tissue disorders, vascular disorders, etc. The SOC system organ classification is the highest level of the hierarchy that captures the broadest concept useful for retrieving data [55].
Data were analyzed by aggregating the PTs of individual reports to a higher level of the MedDRA hierarchy by merging individual serious SARs in the SOC level (e.g., nausea and vomiting classified in the same group as Gastrointestinal Symptoms). Only reports classified as serious were analyzed. In accordance with the E2D guidelines of the International Council for Harmonization, ICSRs are classified as serious if they are life-threatening, have resulted in death, have resulted in/prolonged hospitalization or disability, are related to a congenital anomaly/birth defect or other medically important condition. Adequate stratification of signals by sex groups was performed to avoid biases caused by confounding effects and to analyze these two variables separately. Duplicate and incomplete ICSRs were excluded from the analysis. A descriptive statistical analysis and a disproportionality analysis based on the reporting odds ratio (ROR) were then performed. The ROR is used here to establish the strength of disproportionality. ROR equal to 1 indicates the absence of a signal; conversely, ROR greater than 1 indicates a signal and the existence of an association. The higher the ROR, the stronger the association. The ROR is statistically significant when the lower limit of its 95% CI is greater than 1 [56,57]. The Proportional Reporting Ratio (PRR) is a statistical disproportionality measure that compares the proportion of a specified adverse drug event for a substance of interest to the proportion of the same adverse event in other drugs in a database. The value 1.0 of PRR implies a minor statistical association between the event and the drug [58]. All statistical analyses were completed using SPSS statistical software, version 29.0 (SPSS, IBM, Armonk, NY, USA).
Author Contributions
Conceptualization, I.A., F.C., C.M., and G.C.; methodology, I.A., F.C., C.M., M.C. and Cr..M.; software, I.A., F.C., M.C., G.C., P.M. and E.E.; validation, I.A. and F.C.; formal analysis, I.A., F.C., Cr.M., P.M. and L.C.; investigation, M.S., C.M., Cr.M., P.M. M.C. and L.C.; resources, data curation, E.E., C.M., F.C., P.M. and G.C.; writing—original draft preparation, I.A., F.C., C.M., and L.C.; writing—review and editing, F.C., C.M., L.C., E.E. and Cr.M.; supervision, G.C.; project administration, I.A., F.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding
Institutional Review Board Statement
The study did not require ethical approval.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data analyzed and presented in this study are available on the public EudraVigilance data system.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nemeroff, C.B. Prevalence and management of treatment-resistant depression. . 2007, 17–25. [Google Scholar]
- Lehmann, H.E. Therapy-Resistant Depressions – A Clinical Classification. Pharmacopsychiatry 1974, 7, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Stachowicz, K.; Sowa-Kućma, M. The treatment of depression — searching for new ideas. Front. Pharmacol. 2022, 13, 988648. [Google Scholar] [CrossRef] [PubMed]
- Souery, D.; Amsterdam, J.; de Montigny, C.; Lecrubier, Y.; Montgomery, S.; Lipp, O.; Racagni, G.; Zohar, J.; Mendlewicz, J. Treatment resistant depression: methodological overview and operational criteria. Eur. Neuropsychopharmacol. 1999, 9, 83–91. [Google Scholar] [CrossRef]
- McIntyre, R.S.; Alsuwaidan, M.; Baune, B.T.; Berk, M.; Demyttenaere, K.; Goldberg, J.F.; Gorwood, P.; Ho, R.; Kasper, S.; Kennedy, S.H.; et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry 2023, 22, 394–412. [Google Scholar] [CrossRef]
- Olivier, B.; Olivier, J.D.A. Efficacy, Safety, and Tolerability of Psychedelics in Treatment-Resistant Depres-sion (TRD). Adv Exp Med Biol. 2024, 1456, 49–66. [Google Scholar] [CrossRef]
- Zarate, C.A.; Singh, J.B.; Carlson, P.J.; Brutsche, N.E.; Ameli, R.; Luckenbaugh, D.A.; Charney, D.S.; Manji, H.K. A Randomized Trial of an N-methyl-D-aspartate Antagonist in Treatment-Resistant Major Depression. Arch. Gen. Psychiatry 2006, 63, 856–864. [Google Scholar] [CrossRef]
- Daly, E.J.; Singh, J.B.; Fedgchin, M.; Cooper, K.; Lim, P.; Shelton, R.C.; Thase, M.E.; Winokur, A.; Van Nueten, L.; Manji, H.; et al. Efficacy and Safety of Intranasal Esketamine Adjunctive to Oral Antidepressant Therapy in Treatment-Resistant Depression: A Randomized Clinical Trial. JAMA Psychiatry 2018, 75, 139–148. [Google Scholar] [CrossRef]
- Trullas, R.; Skolnick, P. Functional antagonists at the NMDA receptor complex exhibit antidepressant actions. Eur. J. Pharmacol. 1990, 185, 1–10. [Google Scholar] [CrossRef]
- Skolnick, P.; Layer, R.T.; Popik, P.; Nowak, G.; Paul, I.A.; Trullas, R. Adaptation of N-Methyl-D-Aspartate (NMDA) Receptors following Antidepressant Treatment: Implications for the Pharmacotherapy of Depression. Pharmacopsychiatry 1996, 29, 23–26. [Google Scholar] [CrossRef]
- Domino, E.F.; Warner, D.S. Taming the Ketamine Tiger. Anesthesiology 2010, 113, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Kudoh, A.; Takahira, Y.; Katagai, H.; Takazawa, T. Small-Dose Ketamine Improves the Postoperative State of Depressed Patients. Anesthesia Analg. 2002, 95, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Li, N.; Lee, B.; Liu, R.-J.; Banasr, M.; Dwyer, J.M.; Iwata, M.; Li, X.-Y.; Aghajanian, G.; Duman, R.S. mTOR-Dependent Synapse Formation Underlies the Rapid Antidepressant Effects of NMDA Antagonists. Science 2010, 329, 959–964. [Google Scholar] [CrossRef] [PubMed]
- Zanos, P.; Gould, T.D. Mechanisms of ketamine action as an antidepressant. Mol. Psychiatry 2018, 23, 801–811. [Google Scholar] [CrossRef]
- A Jelen, L.; Young, A.H.; Stone, J.M. Ketamine: A tale of two enantiomers. J. Psychopharmacol. 2020, 35, 109–123. [Google Scholar] [CrossRef]
- Okada, M.; Kawano, Y.; Fukuyama, K.; Motomura, E.; Shiroyama, T. Candidate Strategies for Development of a Rapid-Acting Antidepressant Class That Does Not Result in Neuropsychiatric Adverse Effects: Prevention of Ketamine-Induced Neuropsychiatric Adverse Reactions. Int. J. Mol. Sci. 2020, 21, 7951. [Google Scholar] [CrossRef]
- Hess, E.M.; Riggs, L.M.; Michaelides, M.; Gould, T.D. Mechanisms of ketamine and its metabolites as antidepressants. Biochem. Pharmacol. 2021, 197, 114892–114892. [Google Scholar] [CrossRef]
- Cook, J.; Halaris, A. Adjunctive dopaminergic enhancement of esketamine in treatment-resistant depression. Prog. Neuro-Psychopharmacology Biol. Psychiatry 2022, 119, 110603. [Google Scholar] [CrossRef]
- Summary of product characteristics. Available online: https://www.ema.europa.eu/en/documents/product-information/spravato-epar-product-information_en.pdf (accessed on 18 March 2025).
- Chepke, C.; Shelton, R.; Sanacora, G.; Doherty, T.; Tsytsik, P.; Parker, N. Real-World Safety of Esketamine Nasal Spray: A Comprehensive Analysis of Esketamine and Respiratory Depression. Int. J. Neuropsychopharmacol. 2024, 27. [Google Scholar] [CrossRef]
- Yang, X.; Chen, D. Comparing the adverse effects of ketamine and esketamine between genders using FAERS data. Front. Pharmacol. 2024, 15, 1329436. [Google Scholar] [CrossRef]
- Guo, H.; Wang, B.; Yuan, S.; Wu, S.; Liu, J.; He, M.; Wang, J. Neurological Adverse Events Associated With Esketamine: A Disproportionality Analysis for Signal Detection Leveraging the FDA Adverse Event Reporting System. Front. Pharmacol. 2022, 13, 849758. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Qin, G. The efficacy and safety of fluoxetine versus placebo for stroke recovery: a meta-analysis of randomized controlled trials. Pharm. Weekbl. 2023, 45, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Lense, X.; Hiemke, C.; Funk, C.; Havemann-Reinecke, U.; Hefner, G.; Menke, A.; Mössner, R.; Riemer, T.; Scherf-Clavel, M.; Schoretsanitis, G.; et al. Venlafaxine’s therapeutic reference range in the treatment of depression revised: a systematic review and meta-analysis. Psychopharmacology 2023, 241, 275–289. [Google Scholar] [CrossRef]
- Murrough, J.W.; Abdallah, C.G.; Anticevic, A.; Collins, K.A.; Geha, P.; Averill, L.A.; Schwartz, J.; DeWilde, K.E.; Averill, C.; Yang, G.J.; et al. Reduced global functional connectivity of the medial prefrontal cortex in major depressive disorder. Hum. Brain Mapp. 2016, 37, 3214–3223. [Google Scholar] [CrossRef] [PubMed]
- Sanacora, G.; Yan, Z.; Popoli, M. The stressed synapse 2.0: pathophysiological mechanisms in stress-related neuropsychiatric disorders. Nat. Rev. Neurosci. 2021, 23, 86–103. [Google Scholar] [CrossRef]
- Hardingham, G.E.; Bading, H. Synaptic versus extrasynaptic NMDA receptor signalling: implications for neurodegenerative disorders. Nat. Rev. Neurosci. 2010, 11, 682–696. [Google Scholar] [CrossRef]
- Nguyen, T.M.L.; Defaix, C.; Mendez-David, I.; Tritschler, L.; Etting, I.; Alvarez, J.-C.; Choucha, W.; Colle, R.; Corruble, E.; David, D.J.; et al. Intranasal (R, S)-ketamine delivery induces sustained antidepressant effects associated with changes in cortical balance of excitatory/inhibitory synaptic activity. Neuropharmacology 2022, 225, 109357. [Google Scholar] [CrossRef]
- Nguyen, T.M.L.; Defaix, C.; Mendez-David, I.; Tritschler, L.; Etting, I.; Alvarez, J.-C.; Choucha, W.; Colle, R.; Corruble, E.; David, D.J.; et al. Intranasal (R, S)-ketamine delivery induces sustained antidepressant effects associated with changes in cortical balance of excitatory/inhibitory synaptic activity. Neuropharmacology 2022, 225, 109357. [Google Scholar] [CrossRef]
- Goldberg, J.F.; Nasrallah, H.A. Major depression is a serious and potentially fatal brain syndrome requiring pharmacotherapy or neuromodulation, and psychotherapy. Psychol. Med. 2022, 52, 1423–1425. [Google Scholar] [CrossRef]
- Havlik, J.L.; Wahid, S.; Teopiz, K.M.; McIntyre, R.S.; Krystal, J.H.; Rhee, T.G. Recent Advances in the Treatment of Treatment-Resistant Depression: A Narrative Review of Literature Published from 2018 to 2023. Curr. Psychiatry Rep. 2024, 26, 176–213. [Google Scholar] [CrossRef]
- Castro, M.; Wilkinson, S.T.; Al Jurdi, R.K.; Petrillo, M.P.; Zaki, N.; Borentain, S.; Fu, D.J.; Turkoz, I.; Sun, L.; Brown, B.; et al. Efficacy and Safety of Esketamine Nasal Spray in Patients with Treatment-Resistant Depression Who Completed a Second Induction Period: Analysis of the Ongoing SUSTAIN-3 Study. CNS Drugs 2023, 37, 715–723. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Jiang, L.; Ma, W.; Li, X.; Gao, Q.; Lian, S.; Yu, W. Esketamine Nasal Spray in Major Depressive Disorder: A Meta-Analysis of Randomized Controlled Trials. Clin. Pharmacol. Ther. 2025. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Y.; Li, J. Efficacy of esketamine nasal spray for treatment-resistant depression: A meta-analysis of randomized controlled studies. Medicine 2025, 104, e41495. [Google Scholar] [CrossRef] [PubMed]
- Pereira, S.; Brennan, E.; Patel, A.; Moran, M.; Wallier, J.; Liebowitz, M.R. Managing dissociative symptoms following the use of esketamine nasal spray: a case report. Int. Clin. Psychopharmacol. 2020, 36, 54–57. [Google Scholar] [CrossRef]
- Chen, Y.; Gu, H.; Li, W.; Chen, Y. A real-world pharmacovigilance study of esketamine nasal spray. Medicine 2024, 103, e39484. [Google Scholar] [CrossRef]
- Doherty, T.; Wajs, E.; Melkote, R.; Miller, J.; Singh, J.B.; Weber, M.A. Cardiac Safety of Esketamine Nasal Spray in Treatment-Resistant Depression: Results from the Clinical Development Program. CNS Drugs 2020, 34, 299–310. [Google Scholar] [CrossRef]
- Ochs-Ross, R.; Daly, E.J.; Zhang, Y.; Lane, R.; Lim, P.; Morrison, R.L.; Hough, D.; Manji, H.; Drevets, W.C.; Sanacora, G.; et al. Efficacy and Safety of Esketamine Nasal Spray Plus an Oral Antidepressant in Elderly Patients With Treatment-Resistant Depression—TRANSFORM-3. Am. J. Geriatr. Psychiatry 2020, 28, 121–141. [Google Scholar] [CrossRef]
- Kwan, A.T.; Lakhani, M.; Teopiz, K.M.; Wong, S.; Le, G.H.; Ho, R.C.; Rhee, T.G.; Cao, B.; Rosenblat, J.D.; Mansur, R.; et al. Hepatic adverse events associated with ketamine and esketamine: A population-based disproportionality analysis. J. Affect. Disord. 2025, 374, 390–396. [Google Scholar] [CrossRef]
- Le, G.H.; Wong, S.; Kwan, A.T.; Rosenblat, J.D.; Mansur, R.B.; Teopiz, K.M.; Ho, R.; Rhee, T.G.; Vinberg, M.; Cao, B.; et al. Association of antidepressants with cataracts and glaucoma: a disproportionality analysis using the reports to the United States Food and Drug Administration Adverse Event Reporting System (FAERS) pharmacovigilance database. CNS Spectrums 2024, 29, 682–696. [Google Scholar] [CrossRef]
- Fabbri, C. Treatment-resistant depression: role of genetic factors in the perspective of clinical stratification and treatment personalisation. Mol. Psychiatry 2025, 1–9. [Google Scholar] [CrossRef]
- Mann, J.J.; Michel, C.A.; Auerbach, R.P. Improving Suicide Prevention Through Evidence-Based Strategies: A Systematic Review. FOCUS 2023, 21, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Swainson, J.; Thomas, R.K.; Archer, S.; Chrenek, C.; MacKay, M.-A.; Baker, G.; Dursun, S.; Klassen, L.J.; Chokka, P.; Demas, M.L. Esketamine for treatment resistant depression. Expert Rev. Neurother. 2019, 19, 899–911. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, R.S.; Mansur, R.B.; Rosenblat, J.D.; Teopiz, K.M.; Kwan, A.T.H. The association between ketamine and esketamine and suicidality: reports to the Food And Drug Administration Adverse Event Reporting System (FAERS). Expert Opin. Drug Saf. 2024, 1–6. [Google Scholar] [CrossRef]
- Gastaldon, C.; Raschi, E.; Kane, J.M.; Barbui, C.; Schoretsanitis, G. Post-Marketing Safety Concerns with Esketamine: A Disproportionality Analysis of Spontaneous Reports Submitted to the FDA Adverse Event Reporting System. Psychother. Psychosom. 2020, 90, 41–48. [Google Scholar] [CrossRef] [PubMed]
- de la Barquera, J.A.O.-S.; García, L.A.D.L.G.; García, S.V.E.; Torres, G.S.; Jalomo, G.A.P. Paradoxical Depressive Response to Intranasal Esketamine in Treatment-Resistant Depression: A Case Series. Am. J. Case Rep. 2024, 26, e945475. [Google Scholar] [CrossRef]
- Wan, X.B.; Li, M.; Li, X.B.; Dai, H.B.; Peng, M. The effect of a subclinical dose of esketamine on depression and pain after cesarean section: A prospective, randomized, double-blinded controlled trial. Medicine 2024, 103, e40295. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Saitis, A.; Schatzberg, A.F. Esketamine Treatment for Depression in Adults: A PRISMA Systematic Review and Meta-Analysis. Am. J. Psychiatry 2025, 182, 259–275. [Google Scholar] [CrossRef]
- Spravato | European Medicines Agency (EMA). Available online: https://www.ema.europa.eu/en/documents/product-information/spravato-epar-product-information_en.pdf (accessed on 18 March 2025).
- Wei, Y.; Chang, L.; Hashimoto, K. Molecular mechanisms underlying the antidepressant actions of arketamine: beyond the NMDA receptor. Mol. Psychiatry 2021, 27, 559–573. [Google Scholar] [CrossRef]
- Baudot, J.; Soeiro, T.; Tambon, M.; Navarro, N.; Veyrac, G.; Mezaache, S.; Micallef, J. Safety concerns on the abuse potential of esketamine: Multidimensional analysis of a new anti-depressive drug on the market. Fundam. Clin. Pharmacol. 2021, 36, 572–581. [Google Scholar] [CrossRef]
- Conway, C.R.; Aaronson, S.T.; Sackeim, H.A.; Duffy, W.; Stedman, M.; Quevedo, J.; Allen, R.M.; Riva-Posse, P.; Berger, M.A.; Alva, G.; et al. Clinical characteristics and treatment exposure of patients with marked treatment-resistant unipolar major depressive disorder: A RECOVER trial report. Brain Stimul. 2024, 17, 448–459. [Google Scholar] [CrossRef]
- Mathews, M.; Daly, E.J.; Popova, V.; Heerlein, K.; Canuso, C.; Drevets, W.C. Comment to Drs Gastaldon, Papola, Ostuzzi and Barbui. Epidemiology Psychiatr. Sci. 2020, 29, e124. [Google Scholar] [CrossRef] [PubMed]
- Calapai, F.; Ammendolia, I.; Cardia, L.; Currò, M.; Calapai, G.; Esposito, E.; Mannucci, C. Pharmacovigilance of Risankizumab in the Treatment of Psoriasis and Arthritic Psoriasis: Real-World Data from EudraVigilance Database. Pharmaceutics 2023, 15, 1933. [Google Scholar] [CrossRef] [PubMed]
- MedDRA and Pharmacovigilance: A Complex and Little Evaluated Tool. Prescrire. Int. 2016, 25, 247–250.
- Bate, A.; Evans, S.J.W. Quantitative signal detection using spontaneous ADR reporting. Pharmacoepidemiol. Drug Saf. 2009, 18, 427–436. [Google Scholar] [CrossRef]
- Faillie, J.-L. Case–non-case studies: Principle, methods, bias and interpretation. Therapies 2019, 74, 225–232. [Google Scholar] [CrossRef]
- Wilson, A.M.; Thabane, L.; Holbrook, A. Application of data mining techniques in pharmacovigilance. Br. J. Clin. Pharmacol. 2003, 57, 127–134. [Google Scholar] [CrossRef]
Figure 1.
Suspected adverse reactions to esketamine signaled in European Economic Area and United Kingdom in the years 2019-2024, according to the System Organ Class (SOC) levels. Total number of cases is 265. Data are presented as number of single adverse reactions. Only groups of adverse reactions signaled more than two times are considered.
Figure 1.
Suspected adverse reactions to esketamine signaled in European Economic Area and United Kingdom in the years 2019-2024, according to the System Organ Class (SOC) levels. Total number of cases is 265. Data are presented as number of single adverse reactions. Only groups of adverse reactions signaled more than two times are considered.
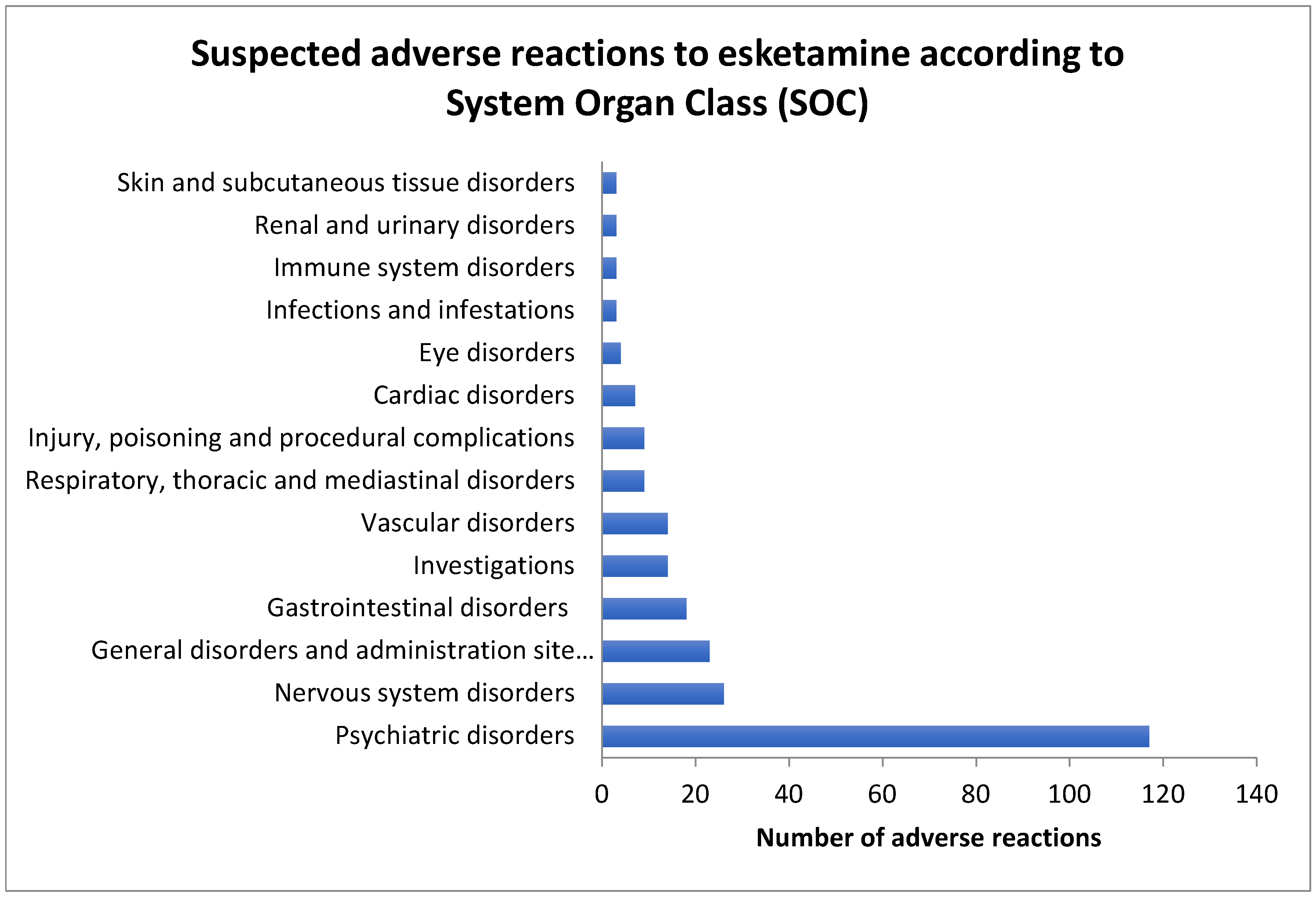

Table 1.
Sex distribution of suspected adverse reactions to esketamine signaled in the European Economic Area and United Kingdom in the years 2019-2024. The total number of Individual Cases Safety Reports (ICSRs) is 265.
Table 1.
Sex distribution of suspected adverse reactions to esketamine signaled in the European Economic Area and United Kingdom in the years 2019-2024. The total number of Individual Cases Safety Reports (ICSRs) is 265.
| Adverse reaction | Male cases Number and % |
Female cases Number and % |
Male and female cases | % of all adverse reactions | Significance level (P) |
|---|---|---|---|---|---|
| Blood pressure increased | 23 (53.5%) |
20 (46.5%) |
43 | 16.2% | 0.016410* |
| Dissociation/Dissociative disorder | 14 (33.3%) |
28 (66.6%) |
42 | 15.8% | 0.802393 |
| Suicidal ideation | 9 (34.6%) |
17 (65.4%) |
26 | 9.8% | 0.972193 |
| Anxiety | 5 (21.7%) |
18 (78.3%) |
23 | 8.7% | 0.198565 |
| Dizziness | 2 (11.1%) |
16 (88.9%) |
18 | 6.8% | 0.041125* |
| Completed suicide | 12 (70.6%) |
5 (29.4%) |
17 | 6.4% | 0.005334* |
| Drug ineffective | 5 (29.4%) |
12 (70.6%) |
17 | 6.4% | 0.685521 |
| Suicide attempt | 3 (21.4%) |
11 (78.6%) |
14 | 5.0% | 0.369206 |
| Loss of consciousness | 6 (46.1%) |
7 (53.8%) |
13 | 4.9% | 0.639931 |
| Hallucination | 4 (33.3%) |
8 (66.7%) |
12 | 4.5% | 0.925157 |
| Generalised tonic clonic seizure | 4 (50.0%) |
4 (50.0%) |
8 | 3.0% | 0.653024 |
| Diplopia | 2 (28.6%) |
5 (71.4%) |
7 | 2.6% | 0.977208 |
| Aggression | 0 (0%) |
5 (100%) |
5 | 1.9% | N.A. |
| Bradycardia | 4 (80.0%) |
1 (20%) |
5 | 1.9% | 0.112688 |
Data are presented as number of cases and percentage of single adverse reactions. Only adverse reactions signaled more than 5 times are included in the table. N.A. = not applicable; * = p < 0.05 vs Male or Female cases.
Table 2.
Age distribution of individual case safety reports (ICSRs) signaling more frequent serious suspected adverse reactions (SARs) associated with esketamine use in European Economic Area (EEA) and United Kingdom collected by EudraVigilance in the years 2019-2024. The total number of cases signaled for adults (18-64 years) and elders (65-85 years) is 260.
Table 2.
Age distribution of individual case safety reports (ICSRs) signaling more frequent serious suspected adverse reactions (SARs) associated with esketamine use in European Economic Area (EEA) and United Kingdom collected by EudraVigilance in the years 2019-2024. The total number of cases signaled for adults (18-64 years) and elders (65-85 years) is 260.
| Adverse reaction | Number and % of serious ICSRs in the Age Group of 18–64 Years (N = 210) |
Number and % of Serious ICSRs in the Age Group of 65–85 Years (N = 50) |
Significance level (P) |
|---|---|---|---|
| Blood pressure increased | 26 (12.4%) |
17 (34.0%) |
0.000490* |
| Dissociation/ Dissociative disorder |
37 (17.6%) |
5 (10.0%) |
0.270536 |
| Suicidal ideation | 23 (10.9%) |
3 (6.0%) |
0.431401 |
| Anxiety | 20 (9.5%) |
3 (6.0%) |
0.608985 |
| Dizziness | 12 (5.7%) |
6 (12.0%) |
0.206359 |
| Completed suicide | 16 (7.6%) |
1 (2.0%) |
0.260073 |
| Drug ineffective | 11 (5.2%) |
6 (12.0%) |
0.155604 |
| Suicide attempt | 12 (5.7%) |
2 (4.0%) |
0.893348 |
| Loss of consciousness | 10 (4.8%) |
3 (6.0%) |
1.0 |
| Hallucination | 11 (5.2%) |
0 (0.0%) |
N.A. |
| Generalised tonic clonic seizure | 5 (2.4%) |
2 (4.0%) |
0.881104 |
| Diplopia | 6 (2.8%) |
1 (2.0%) |
0.881104 |
| Aggression | 4 (1.9%) |
1 (2.0%) |
0.596922 |
| Bradycardia | 4 (1.9%) |
1 (2.0%) |
0.596922 |
Only adverse reactions of people aged 18-64 years or 65-85 years and signaled more than 4 times are included in the table. N.A. = not applicable. * = p < 0.05 vs Age Group 18-64 years.
Table 3.
Cases of death not including complete suicide as suspected adverse reactions (SARs) in individual case safety reports (ICSRs) associated with esketamine use in European Economic Area (EEA) and United Kingdom displayed in EudraVigilance for the years 2019-2024 according to age and sex distribution.
Table 3.
Cases of death not including complete suicide as suspected adverse reactions (SARs) in individual case safety reports (ICSRs) associated with esketamine use in European Economic Area (EEA) and United Kingdom displayed in EudraVigilance for the years 2019-2024 according to age and sex distribution.
| Cases and % of ICSRs (0-85 years) (N = 265) |
Cases and % of ICSRs (18–64 years) (N = 210) |
Cases and % of ICSRs (65–85 Years) (N = 50) |
Male cases and % of total ICSRs (N = 265) |
Female cases and % of total ICSRs (N = 265) |
|
|---|---|---|---|---|---|
| Cases of death | 10 (3.8%) |
8 (3.8%) |
1 (2.0%) |
6 (2.3%) |
4 (1.5%) |
Table 4.
Reporting odds ratio (ROR) and Proportional reporting ratio (PRR) of suspected adverse reactions (SARs) to esketamine signaled in European Economic Area and United Kingdom in the years 2019-2024, aggregated according to the System Organ Class (SOC) levels and compared to SARs related to fluoxetine and venlafaxine in the same years.
Table 4.
Reporting odds ratio (ROR) and Proportional reporting ratio (PRR) of suspected adverse reactions (SARs) to esketamine signaled in European Economic Area and United Kingdom in the years 2019-2024, aggregated according to the System Organ Class (SOC) levels and compared to SARs related to fluoxetine and venlafaxine in the same years.
| SOC | SARs to esketamine |
All other SARs to esketamine |
SARs to fluoxetine | All other SARs to fluoxetine |
ROR and PRR esketamine vs fluoxetine (95% C.I.) |
SARs to venlafaxine | All other SARs to venlafaxine |
ROR and PRR esketamine vs venlafaxine (95% C.I.) |
|---|---|---|---|---|---|---|---|---|
| Psychiatric disorders | 117 | 148 | 318 | 919 | ROR: 2.28 PRR: 1.72 (1.74-3.00) |
573 | 1758 | ROR: 2.42 PRR: 1.80 (1.87-3.15) |
| Nervous system disorders | 26 | 239 | 371 | 695 | ROR: 0.20 PRR: 0.28 (0.13-0.31) |
793 | 1226 | ROR: 0.17 PRR: 0.25 (0.11-0.25) |
| Vascular disorders | 23 | 242 | 66 | 1000 | ROR: 1.44 PRR: 1.40 (0.88-2.36) |
156 | 1863 | ROR: 1.13 PRR: 1.12 (0.72-1.79) |
| Investigations | 18 | 247 | 119 | 947 | ROR: 0.58 PRR: 0.61 (0.35-0.97) |
246 | 1773 | ROR: 0.52 PRR: 0.56 (0.32-0.86) |
| Respiratory, thoracic and mediastinal disorders | 14 | 251 | 76 | 990 | ROR: 0.73 PRR: 0.74 (0.40-1.31) |
197 | 1822 | ROR: 0.51 PRR: 0.54 (0.30-0.90) |
| General disorders and administration site conditions | 14 | 251 | 240 | 826 | ROR: 0.19 PRR: 0.23 (0.11-0.33) |
492 | 1527 | ROR: 0.17 PRR: 0.22 (0.10-0.30) |
| Cardiac disorders | 9 | 256 | 96 | 970 | ROR: 0.35 PRR: 0.38 (0.18-0.71) |
258 | 1761 | ROR: 0.24 PRR: 0.26 (0.12-0.47) |
| Immune system disorders | 9 | 256 | 15 | 1051 | ROR: 2.46 PRR: 2.41 (1.06-5.69) |
11 | 2008 | ROR: 6.42 PRR: 6.23 (2.63-15.63) |
| Gastrointestinal disorders | 7 | 258 | 147 | 919 | ROR: 0.18 PRR: 0.20 (0.08-0.37) |
261 | 1758 | ROR: 0.18 PRR: 0.21 (0.08-0.39) |
In brackets 95% confidence intervals (C.I.).
Table 5.
Reporting odds ratio (ROR) and Proportional Rating Ratio (PRR) of Individual Cases Safety Reports (ICSRs) signaling the single adverse events “Suicidal ideation”, “Suicide attempt” and “Complete suicide” suspected to be caused by esketamine, fluoxetine and venlafaxine in European Economic Area and United Kingdom in the years 2019-2024.
Table 5.
Reporting odds ratio (ROR) and Proportional Rating Ratio (PRR) of Individual Cases Safety Reports (ICSRs) signaling the single adverse events “Suicidal ideation”, “Suicide attempt” and “Complete suicide” suspected to be caused by esketamine, fluoxetine and venlafaxine in European Economic Area and United Kingdom in the years 2019-2024.
| Adverse reaction | Esketamine Cases/not cases Total number of cases = 265 |
Fluoxetine Cases/not cases Total number of cases = 1066 |
Venlafaxine Cases/not cases Total number of cases = 2019 |
ROR and PRR of esketamine vs fluoxetine (95% C.I.) |
ROR and PRR of esketamine vs venlafaxine (95% C.I.) |
ROR and PRR of fluoxetine vs venlafaxine (95% C.I.) |
|---|---|---|---|---|---|---|
| Suicidal ideation | 26/239 | 38/1028 | 41/1978 | ROR: 2.94 PRR: 2.75 (1.75-4.94) |
ROR: 5.25 PRR: 4.83 (3.15-8.73) |
ROR: 1.78 PRR: 1.75 (1.14-2.79) |
| Suicide attempt | 14/251 | 70/996 | 102/1917 | ROR: 0.79 PRR: 0.80 (0.44-1.43) |
ROR: 1.05 PRR: 1.04 (0.59-1.86) |
ROR: 1.32 PRR: 1.30 (0.96-1.81) |
| Completed suicide | 17/248 | 9/1057 | 13/2006 | ROR: 8.05 PRR: 7.60 (3.55-18.3) |
ROR: 10.58 PRR: 9.96 (5.08-22.04) |
ROR: 1.31 PRR: 1.31 (0.56-3.08) |
In brackets 95% confidence intervals (C.I.).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



