
Submitted:
14 July 2025
Posted:
15 July 2025
You are already at the latest version
Abstract
Background/Objectives: The pharmacovigilance aims to identify, assess and minimize drug risks. Therefore, spontaneous reports play a central role. However, the high level of underreporting and the varying data quality are limitations that should be minimized by prospective cohort studies. Methods: The spontaneous reports reported to the Drug Commission of the German Medical Association (AkdÄ) within one year were compared with the adverse drug reaction (ADR) cases systematically recorded in the hospital emergency departments. The frequencies of the demographic patient characteristics and the odds ratios as the relationship between suspected and concomitant medication were calculated. Results: In the spontaneous reports, the reported cases were a median of 12 years younger, and the group of very old people was less strongly represented (10.8% versus 27.3% in the prospective cohort study). Within the study, cases with polypharmacy were documented significantly more often (median 7 drugs [IQR 3;10] versus median 2 drugs [IQR 1;5] in the spontaneous reports). New drugs and drugs discussed in the media were frequently reported as causing ADRs, whereas drugs with an effect on the central nervous system were more often suspected in the emergency department setting. Conclusions: Both sources of ADRs provide complementary information that can improve risk signal detection. The aim for the future is to further increase awareness of spontaneous reports and to identify specific issues using structured investigations.
Keywords:
spontaneous reports
; drug safety
; adverse drug reaction
; prospective cohort study
; emergency department
1. Introduction
Spontaneous reports are still considered the cornerstone of pharmacovigilance [1,2,3]. By far the greatest advantage is the ability to quickly recognize “signals” and therefore potential drug risks even with a small number of reported cases [3]. The spontaneous reports are considered as a conceptually simple, inexpensive and universally applicable instrument [1,3,4]. The main limitation is the varying data quality and the low reporting rate (`underreporting`) [3,4], which can be up to 95% [1,5]. Prospective case cohort studies [4], or retrospective surveillance data [1] can be used to close this data gap. The high requirements for prospective data collection lead to high data quality and a good detection rate [4]. However, this is a costly and time-consuming method that requires trained personnel [4], but they make it possible to answer specific scientific questions quantitatively.
The aim of this work was to compare two different ways of recording ADRs - spontaneous reports and prospective cohort studies - in terms of their feasibility for risk signal detection.
2. Materials and Methods
2.1. Comparison Groups
All cases reported to the Drug Commission of the German Medical Association (AkdÄ) in 2017 were used for the spontaneous reports, excluding reports on blood products and vaccines. The year 2017 is in the middle of the data collected in the multicenter prospective cohort study ADRED (Adverse Drug Reactions in Emergency Departments) between 2015-2018 (Phase I).
Spontaneous reports are a continuous method of recording ADRs. Healthcare professionals (regardless of their specialization and professional experience) are obliged to submit these reports in accordance with their professional code of conduct [6,7]. The reports are made using a defined questionnaire [8,9]. Further information such as physicians’ letters can be optionally attached. The high level of diversification among the reporters inevitably leads to greater heterogeneity in the data.
In contrast, the prospective multicenter cohort study ADRED systematically collected ADRs that led to emergency treatment at four hospitals in Germany. The study was based on a study plan and was conducted by specially trained healthcare professionals (physicians and pharmacists) between 2015 and 2018 (Phase I). Training and regular telephone conferences ensured a defined causality assessment and a high level of consistency for all study centres. The methods and results of the ADRED study (Phase I) have already been published and can be found in detail here [10,11,12].
2.2. Data Adjustment
To ensure comparability between the two groups, the data adjustment and classification of spontaneous reports by the AkdÄ was done manually, analogous to the ADRED study data (Phase I). This led to the exclusion of minors, reports of unknown age, reports of intentional self-harm (suicide/ suicidal behaviour and intentional overdose), omission cases, i.e. cases in which patients disregarded treatment adherence and cases with medication errors such as prescription, dispensing and/or administration errors. Also excluded were reports that were falsely based on vaccines or blood products, as well as medical devices and dietary supplements without detailed information on ingredients. Cases with the ADR “suicidal ideation” were not excluded if there was no active self-harming behaviour. The process of data adjustment is shown in Figure 1 as a flow chart.
2.3. Data Classification
The severity of ADRs is classified in non-serious and serious. Within the serious reactions there is a subdivision into death, life-threatening, hospitalization, disability and other serious reactions (only in the spontaneous reports). To calculate the number of active ingredients, combination drugs were divided into their individual active ingredients. The drugs were assigned to the anatomical-therapeutic-chemical (ATC) classification [13].
2.4. Statistical Analysis
For the comparison, the demographic and clinical data such as age, sex, number of suspected and taken drugs and the severity of the ADR were analysed descriptively. The data was divided into three age groups: Adults (18 - 64 years), young-old (65 - 79 years) and old-old (≥ 80 years). Categorical variables were given as absolute and percentage values. Continuous variables were given as median and interquartile range [IQR] due to a lack of normal distribution in the Kolmogorov-Smirnov test.
To estimate the probability of a drug being reported or recorded as suspected or concomitant in the respective population (spontaneous reports or ADRED study) the corresponding odds ratio (OR) with 95% confidence interval (95% CI) were calculated. The 95% CI was corrected using Bonferroni. An OR with a 95% CI greater than 1 indicates that the drug group was disproportionately frequently reported or recorded as suspected. At 1, the ratio is balanced and at less than 1, the drug group is found disproportionately frequently in the concomitant medication. Statistically significant is α ≤ 0.05. The statistical software used was SPSS® from IBM, version 26 - 28.
3. Results
The comparative analysis was based on 2022 reports from the AkdÄ and 2215 cases from the ADRED study (Phase I). In the ADRED study, the patients were 12 years older (median 61 vs. 73 years) and took a median of 7 [IQR 3;10] drugs per day [11] versus 2 [IQR 1;5] drugs in the spontaneous reporting system. In the spontaneous reports, the number of reported drugs increased significantly with age (Spearman rank correlation: 0.260, p. < 0.001). In both, spontaneous reports (median 1 [IQR 1;1]) and emergency department admissions (median 1 [IQR 1;2]), one drug was suspected to have caused the ADR in most cases [11]. An overview of the main data for both groups can be found in Table 1.
Almost 50% of all spontaneous reports were classified as non-serious versus 12% in the ADRED study [11]. The reason for this can be seen in the written consent of the patient required for the study [11]. In the spontaneous reports, is an increasing proportion of serious events (except for “other serious events”) with increasing age. For example, the proportion of deaths increased sixfold between adults and the old-olds (2.5% versus 15.5%). This could not be shown in the ADRED study. Here, the proportion of serious events is more balanced [12]. The distribution of the age groups in relation to the severity is shown in Table 1 and is graphically illustrated in Figure 2.
The most frequently taken drugs in the spontaneous reports are lipid-modifying drugs, antithrombotics, ACE inhibitors/ AT-1 antagonists, antidiabetics and beta blockers (12.1%, 8.4%, 8.0%, 7.0% and 5.7%, respectively). For the ADRED study these are: antithrombotics, diuretics, beta blockers, ACE inhibitors/ AT-1 antagonists and drugs for acid-related diseases (10.4%, 7.6%, 6.7%, 6.6% and 6.6%, respectively) [11]. In this respect, the drug groups that are most often suspected of causing an ADR are in the spontaneous reports: lipid-modifying drugs, antithrombotics, antineoplastic drugs, antibiotics and immunosuppressants (21.2%, 13.0%, 7.9%, 7.4% and 7.2%, respectively) and for the ADRED study: antithrombotics, antineoplastic and immunmodulating drugs, beta blockers, diuretics and non-opioid analgesics (19.1%, 14.8%, 7.2%, 7.1% and 5.2%, respectively) [11]. The drug groups with a high probability of being suspected with a corresponding OR (95 CI) > 1 are summarized in Table 2 and graphically illustrated as forest plots in Figure 3a and 3b [11].
There are similarities for: antineoplastic drugs, antibiotics and antithrombotics. Differences can be seen for gynaecologics and sex hormones, lipid-modifying drugs and drugs affecting the nervous system. In the spontaneous reports, intrauterine contraception with progestogen (levonorgestrel) with 53 of 56 reported cases represents the majority of gynaecologicals. In addition, hormonal contraceptives for systemic use consisting of a fixed combination of progestogen and estrogen with dienogest/ethinylestradiol (n = 10) and levonorgestrel/ethinylestradiol (n = 6) were reported as sex hormones. The statins atorvastatin (n = 107), simvastatin (n = 65) and fluvastatin (n = 43) are suspected of having triggered an ADR in almost half of all cases (44.5%), followed by ezetimibe (n = 54) and the PCSK-9 inhibitors evolucumab (n = 46) and alirocumab (n = 43). In the ADRED study, the five most frequently suspected drugs with an influence on the nervous system are citalopram (n = 42), oxycodone (n = 37), metamizole (n = 34), pregabalin (n = 32) and mirtazapine (n = 28) [11].
4. Discussion
For both methods, it was shown that drug groups with a narrow therapeutic range, such as antineoplastic, immunomodulating, antibiotic and antithrombotic drugs, are frequently suspected of causing ADRs [11]. Side effects of cytostatic drugs have been scientifically proven for decades [14,15] and are well known by healthcare professionals and patients respectively. The same applies to antithrombotics. The pharmacodynamic influence of antithrombotics on the tendency to bleed is therapeutically desirable and at the same time a risk factor for ADRs [16,17]. This pronounced awareness and the good detectability of these ADRs may explain the high detection rate.
In addition, the spontaneous reports often included drugs that were either new to the market or had been discussed in the media. For example, drugs with an influence on lipid metabolism accounted for a relevant rate. The approval of a new drug group, such as PCSK-9 inhibitors, was subjected to the benefit assessment procedure within the Joint Federal Committee (G-BA) in accordance with §35a SGB V. Dietary and lipid-lowering therapeutics in particular statin drug therapy were considered as a comparative option for the new approval [18,19]. This additional regulatory monitoring with the call to report ADRs can lead to an increased reporting rate.
Hormonal contraceptives and their influence on possible psychiatric ADRs were discussed in the media. A petition (extension of the package insert with regard to psychiatric symptoms) [20] led to scientific analyses [21] and a red-handed letter [22]. The topic was also of great interest outside Germany and led to increased reporting rates [23,24].
Complementary to the spontaneous reports, drugs with an influence on the central nervous system were disproportionately often suspected of causing an ADR in the ADRED study [11]. Many drugs with an influence on the central nervous system are considered as potentially inappropriate medication (PIM) for geriatric patients [25,26,27] and therefore as a risk factor for the occurrence of ADRs [28,29,30]. Altered pharmacodynamics and kinetics with age [31] can lead to a generally higher potency due to a reduced volume of distribution and slower metabolization [32]. Dehydration can further aggravate this effect and showed the greatest age dependence in the ADRED study [12]. In the future, it will be crucial to scientifically examine these physiological correlations in the context of the changing global climate and to establish recommendations for action for patients and healthcare professionals.
Far from PIM, the increase in drug therapies due to comorbidities with increasing age is scientifically proven [33,34,35] and polypharmacy is a significant risk factor for the occurrence of ADRs [36]. In an ageing society, it is therefore more important than ever to sensitize healthcare professionals to the most common ADRs [37] and to work together with the professional societies to find adequate solutions.
The median number of suspected drugs for both methods is 1 and thus shows a strong tendency for one suspected drug to be identified [11]. There are differences in the number of taken drugs. In the ADRED study, all taken drugs were systematically collected and documented. This may explain the significantly higher number of concomitant drugs [11] compared to the spontaneous reports. The underreporting as well as the incompleteness of the data is well known [3,4]. This could be partly explained by the fact that the federal standardized medication plan (BMP), which has been obligatory since October 2016 [38], is not used consistently in practice [39] and is often neither up-to-date nor complete [38,39,40]. This makes it difficult for healthcare specialists to obtain a complete overview of the taken drugs by the patient and, consequently, to be able to report them. A digitally available patient file that also contains the BMP and is available to all healthcare professionals across all sectors could provide a remedy. This would not only close data gaps, but also increase drug safety [38,40].
Author Contributions
Conceptualization: V.G., J.S. and H.D.; methodology: V.G, J.S., K.S.J and H.D.; software: V.G.; validation: H.D., J.S., K.S.J. and A.E.; formal analysis: V.G.; investigation: V.G.; resources: J.S.; data curation: V.G.; writing—original draft preparation: V.G.; writing—review and editing: H.D., J.S., K.S.J. and A.E.; visualization: V.G.; supervision: H.D. and A.E.; project administration: V.G. and H.D.; funding acquisition: M.W. All authors have read and agreed to the published version of the manuscript.
Funding
The ADRED study (Phase I) was funded by the framework of the AMTS focus of the German Federal Ministry of Health (BMG), grant number ZMVI5-2514ATS004.
Institutional Review Board Statement
The ADRED study (Phase I) was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Bonn (202/15) and reviewed positively by the respective ethical committees of the study centres of the Universities of Erlangen-Nürnberg (43_16Bc), Tübingen (113/16) and Ulm (493/2016BO1) for studies involving humans. The ADRED study (Phase I) trial is registered at the German Clinical Trial Register (DRKS-ID: DRKS00008979).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the ADRED study.
Data Availability Statement
Data are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bouvy, J.C.; Bruin, M.L.; Koopmanschap, M.A. Epidemiology of adverse drug reactions in Europe: a review of recent observational studies. Drug Saf. 2015, 38, 437–53. [Google Scholar] [CrossRef] [PubMed]
- Durrieu, G.; Jacquot, J.; Mège, M.; Bondon-Guitton, E.; Rousseau, V.; Montastruc, F.; Montastruc, J.-L. Completeness of Spontaneous Adverse Drug Reaction Reports Sent by General Practitioners to a Regional Pharmacovigilance Centre: A Descriptive Study. Drug Saf. 2016, 39, 1189–95. [Google Scholar] [CrossRef] [PubMed]
- Waller, P.C. Making the most of spontaneous adverse drug reaction reporting. Basic Clin Pharmacol Toxicol. 2006, 98, 320–3. [Google Scholar] [CrossRef] [PubMed]
- Laatikainen, O.; Sneck, S.; Turpeinen, M. Medication-related adverse events in health care-what have we learned? A narrative overview of the current knowledge. Eur J Clin Pharmacol. 2022, 78, 159–70. [Google Scholar] [CrossRef] [PubMed]
- Hazell, L.; Shakir, S.A.W. Under-reporting of adverse drug reactions: a systematic review. Drug Saf. 2006, 29, 385–96. [Google Scholar] [CrossRef] [PubMed]
- Bundesärztekammer. (Muster-)Berufsordnung für die in Deutschland tätigen Ärztinnen und Ärzte. Available online: https://www.bundesaerztekammer.de/fileadmin/user_upload/BAEK/Themen/Recht/_Bek_BAEK_Musterberufsordnung-AE.pdf. (accessed on 24 June 2025).
- Bundes-Apothekerordnung: BApO, vom 05.06.1968 (Ausfertigungsdatum). In der Fassung der Bekanntmachung vom 19.07.1989 (BGBl. I S. 1478, 1842), die zuletzt durch Artikel 8 Absatz 3a des Gesetzes vom 27.09.2021 (BGBl. I S. 4530) geändert worden ist. Available online: https://www.gesetze-im-internet.de/bapo/BJNR006010968.html (accessed on 24 June 2025).
- Arzneimittelkommission der deutschen Ärzteschaft (AkdÄ). Bericht über unerwünschte Arzneimittelwirkungen. Available online: https://www.akdae.de/Arzneimittelsicherheit/UAW-Meldung/UAW-Berichtsbogen.pdf. (accessed on 24 June 2025).
- Arzneimittelkommission der deutschen Apotheker (AMK). Berichtsbogen-Formulare. Available online: https://www.abda.de/fuer-apotheker/arzneimittelkommission/berichtsbogen-formulare/. (accessed on 24 June 2025).
- Schurig, A.M.; Böhme, M.; Just, K.S.; Scholl, C.; Dormann, H.; Plank-Kiegele, B.; Seufferlein, T.; Gräff, I.; Schwab, M.; Stingl, J.C. Adverse Drug Reactions (ADR) and Emergencies. Dtsch Arztebl Int. 2018, 115, 251–8. [Google Scholar] [CrossRef] [PubMed]
- Just, K.S.; Dormann, H.; Böhme, M.; Schurig, M.; Schneider, K.L.; Steffens, M.; Dunow, S.; Plank-Kiegele, B.; Ettrich, K.; Seufferlein, T.; et al. Personalising drug safety-results from the multi-centre prospective observational study on Adverse Drug Reactions in Emergency Departments (ADRED). Eur J Clin Pharmacol. 2020, 76, 439–48. [Google Scholar] [CrossRef] [PubMed]
- Just, K.S.; Dormann, H.; Schurig, M.; Böhme, M.; Steffens, M.; Plank-Kiegele, B.; Ettrich, K.; Seufferlein, T.; Gräff, I.; Igel, S.; et al. The phenotype of adverse drug effects: Do emergency visits due to adverse drug reactions look different in older people? Results from the ADRED study. Br J Clin Pharmacol. 2020, 86, 2144–54. [Google Scholar] [CrossRef] [PubMed]
- Bundesinstitut für Arzneimittel und Medizinprodukte (BfArM). ATC-Klassifikation: ATC-Klassifikation mit definierten Tagesdosen DDD. Available online: https://www.bfarm.de/DE/Kodiersysteme/Klassifikationen/ATC/_node.html. (accessed on 24 June 2025).
- Adel, N. Overview of chemotherapy-induced nausea and vomiting and evidence-based therapies. Am J Manag Care. 2017, 23, 259–65. [Google Scholar]
- Blijham, G.H. Prevention and treatment of organ toxicity during high-dose chemotherapy: an overview. Anticancer Drugs. 1993, 4, 527–33. [Google Scholar] [CrossRef] [PubMed]
- Kauppila, M.; Backman, J.T.; Niemi, M.; Lapatto-Reiniluoto, O. Incidence, preventability, and causality of adverse drug reactions at a university hospital emergency department. Eur J Clin Pharmacol. 2021, 77, 643–50. [Google Scholar] [CrossRef] [PubMed]
- Ujeyl, M.; Köster, I.; Wille, H.; Stammschulte, T.; Hein, R.; Harder, S.; Gundert-Remy, U.; Bleek, J.; Ihle, P.; Schröder, H.; et al. Comparative risks of bleeding, ischemic stroke and mortality with direct oral anticoagulants versus phenprocoumon in patients with atrial fibrillation. Eur J Clin Pharmacol. 2018, 74, 1317–25. [Google Scholar] [CrossRef] [PubMed]
- Gemeinsamer Bundesausschuss (G-BA). Nutzenbewertungsverfahren zum Wirkstoff Alirocumab. Available online: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/199/. (accessed on 24 November 2024).
- Gemeinsamer Bundesausschuss (G-BA). Nutzenbewertungsverfahren zum Wirkstoff Evolocumab. Available online: https://www.g-ba.de/bewertungsverfahren/nutzenbewertung/189/. (accessed on 24 November 2024).
- change.org. Beipackzettel der Hormonspirale vervollständigen. Available online: https://www.change.org/p/arzneimittelkommission-der-dt-ärzteschaft-und-bundesinstitut-f-arzneimittel-u-medizinprodukte-beipackzettel-der-hormonspirale-vervollständigen. (accessed on 24 June 2025).
- Skovlund, C.W.; Mørch, L.S.; Kessing, L.V.; Lange, T.; Lidegaard, Ø. Association of Hormonal Contraception With Suicide Attempts and Suicides. Am J Psychiatry. 2018, 175, 336–42. [Google Scholar] [CrossRef] [PubMed]
- Bundesinstitut für Arzneimittel und Medizinprodukte (BfArM). Rote-Hand-Brief zu hormonellen Kontrazeptiva: Neuer Warnhinweis zu Suizidalität als mögliche Folge einer Depression unter der Anwendung hormoneller Kontrazeptiva. 2019. Available online: https://www.bfarm.de/SharedDocs/Risikoinformationen/Pharmakovigilanz/DE/RHB/2019/rhb-hormonelle-kontrazeptiva.pdf. (accessed on 24 June 2025).
- Postma, L.G.M.; Donyai, P. The cooccurrence of heightened media attention and adverse drug reaction reports for hormonal contraception in the United Kingdom between 2014 and 2017. Br J Clin Pharmacol. 2021, 87, 1768–77. [Google Scholar] [CrossRef] [PubMed]
- Langlade, C.; Gouverneur, A.; Bosco-Lévy, P.; Gouraud, A.; Pérault-Pochat, M-C.; Béné, J.; Miremont-Salamé, G.; Pariente, A. Adverse events reported for Mirena levonorgestrel-releasing intrauterine device in France and impact of media coverage. Br J Clin Pharmacol. 2019, 85, 2126–33. [Google Scholar] [CrossRef] [PubMed]
- Hefner, G.; Hahn, M.; Toto, S.; Hiemke, C.; Roll, S.C.; Wolff, J.; Klimke, A. Potentially inappropriate medication in older psychiatric patients. Eur J Clin Pharmacol. 2021, 77, 331–9. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.; Schmiedl, S.; Thürmann, P.A. Potentially inappropriate medications in the elderly: the PRISCUS list. Dtsch Arztebl Int. 2010, 107, 543–51. [Google Scholar] [CrossRef] [PubMed]
- Lucchetti, G.; Lucchetti, A.L.G. Inappropriate prescribing in older persons: A systematic review of medications available in different criteria. Arch Gerontol Geriatr. 2017, 68, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Halli-Tierney, A.D.; Scarbrough, C.; Carroll, D. Polypharmacy: Evaluating Risks and Deprescribing. Am Fam Physician. 2019, 100, 32–8. [Google Scholar] [PubMed]
- Earl, T.R.; Katapodis, N.D.; Schneiderman, S.R.; Shoemaker-Hunt, S.J. Using Deprescribing Practices and the Screening Tool of Older Persons’ Potentially Inappropriate Prescriptions Criteria to Reduce Harm and Preventable Adverse Drug Events in Older Adults. J Patient Saf. 2020, 16, 23–35. [Google Scholar] [CrossRef] [PubMed]
- Fahrni, M.L.; Azmy, M.T.; Usir, E.; Aziz, N.A.; Hassan, Y. Inappropriate prescribing defined by STOPP and START criteria and its association with adverse drug events among hospitalized older patients: A multicentre, prospective study. PLoS One. 2019, 14, e0219898. [Google Scholar] [CrossRef] [PubMed]
- Andres, T.M.; McGrane, T.; McEvoy, M.D.; Allen, B.F.S. Geriatric Pharmacology: An Update. Anesthesiol Clin. 2019, 37, 475–92. [Google Scholar] [CrossRef] [PubMed]
- Akhtar, S.; Ramani, R. Geriatric Pharmacology. Anesthesiol Clin. 2015, 33, 457–69. [Google Scholar] [CrossRef] [PubMed]
- Lavan, A.H.; Gallagher, P.F.; O’Mahony, D. Methods to reduce prescribing errors in elderly patients with multimorbidity. Clin Interv Aging. 2016, 11, 857–66. [Google Scholar] [CrossRef] [PubMed]
- Payne, R.A. The epidemiology of polypharmacy. Clin Med (Lond). 2016, 16, 465–9. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, J.K.; Fouts, M.M.; Kotabe, S.E.; Lo, E. Polypharmacy as a risk factor for adverse drug reactions in geriatric nursing home residents. Am J Geriatr Pharmacother. 2006, 4, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Parish, A.L. Polypharmacy and Medication Management in Older Adults. Nurs Clin North Am. 2017, 52, 457–68. [Google Scholar] [CrossRef] [PubMed]
- Pohontsch, N.J.; Heser, K.; Löffler, A.; Haenisch, B.; Parker, D.; Luck, T.; Riedel-Heller, S.G.; Maier, W.; Jessen, F.; Scherer, M. General practitioners’ views on (long-term) prescription and use of problematic and potentially inappropriate medication for oldest-old patients-A qualitative interview study with GPs (CIM-TRIAD study). BMC Fam Practice. 2017, 18, 22. [Google Scholar] [CrossRef] [PubMed]
- Dormann, H.; Maas, R.; Eickhoff, C.; Müller, U.; Schulz, M.; Brell, D.; Thürmann, P.A. Der bundeseinheitliche Medikationsplan in der Praxis : Die Pilotprojekte MetropolMediplan 2016, Modellregion Erfurt und PRIMA. [Standardized national medication plan : The pilot projects MetropolMediplan 2016, model region Erfurt, and PRIMA]. Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz. 2018, 61, 1093–102. [Google Scholar] [CrossRef] [PubMed]
- Mueller, M.A.; Opitz, R.; Grandt, D.; Lehr, T. The federal standard medication plan in practice: An observational cross-sectional study on prevalence and quality. Res Social Adm Pharm. 2020, 16, 1370–8. [Google Scholar] [CrossRef] [PubMed]
- Amelung, S.; Bender, B.; Meid, A.; Walk-Fritz, S.; Hoppe-Tichy, T.; Haefeli, W.E.; Seidling, H.M. Wie vollständig ist der Bundeseinheitliche Medikationsplan? Eine Analyse bei Krankenhausaufnahme. [How complete is the Germany-wide standardised medication list ("Bundeseinheitlicher Medikationsplan")? An analysis at hospital admission]. Dtsch Med Wochenschr. 2020, 145, e116–22. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flowchart of the data adjustment of spontaneous reports from 2017 with presentation of the inclusion and exclusion criteria.
Figure 1.
Flowchart of the data adjustment of spontaneous reports from 2017 with presentation of the inclusion and exclusion criteria.
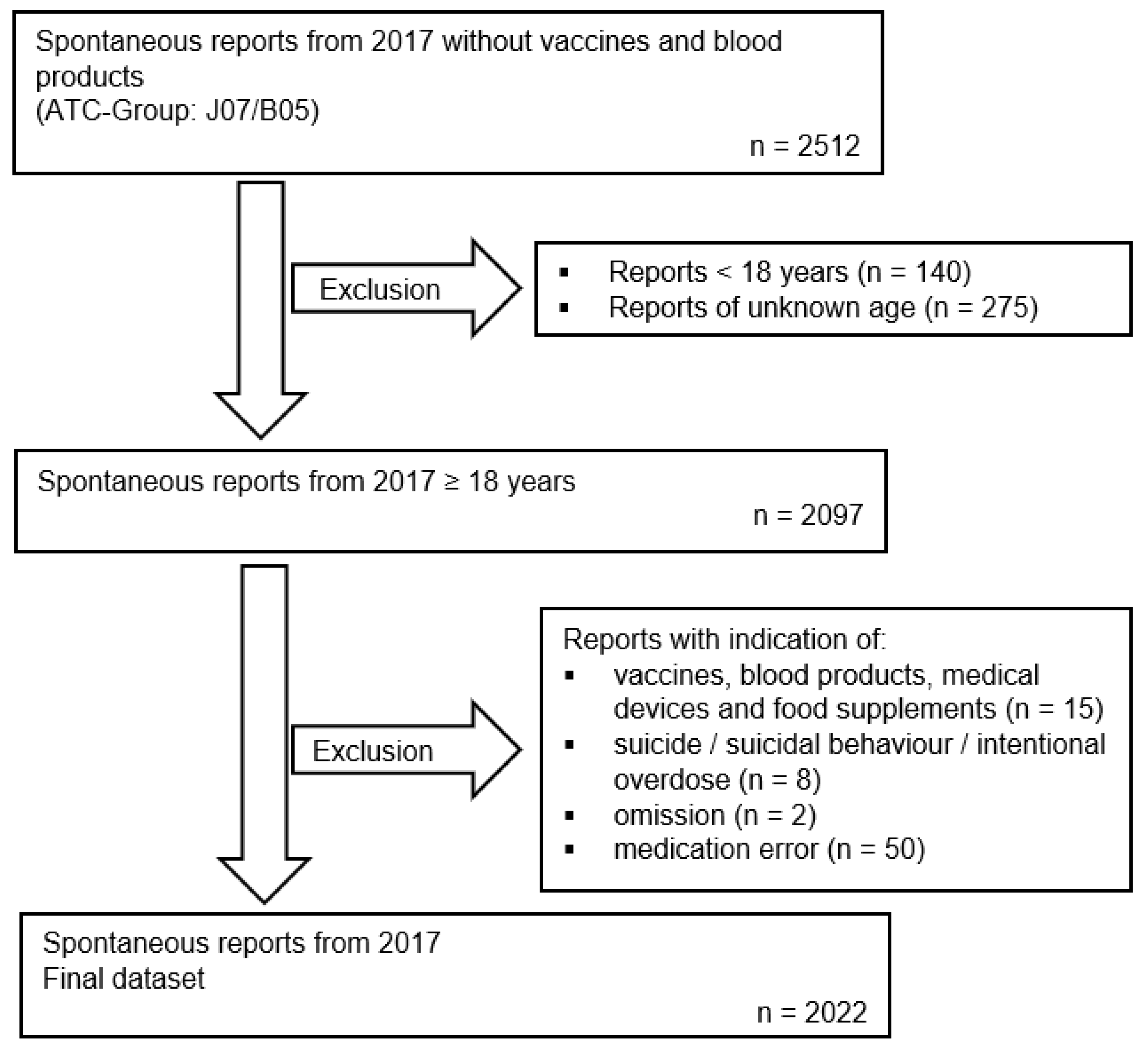
Figure 2.
Distribution of severity within the spontaneous reports and the ADRED study – total and for the three age groups.
Figure 2.
Distribution of severity within the spontaneous reports and the ADRED study – total and for the three age groups.
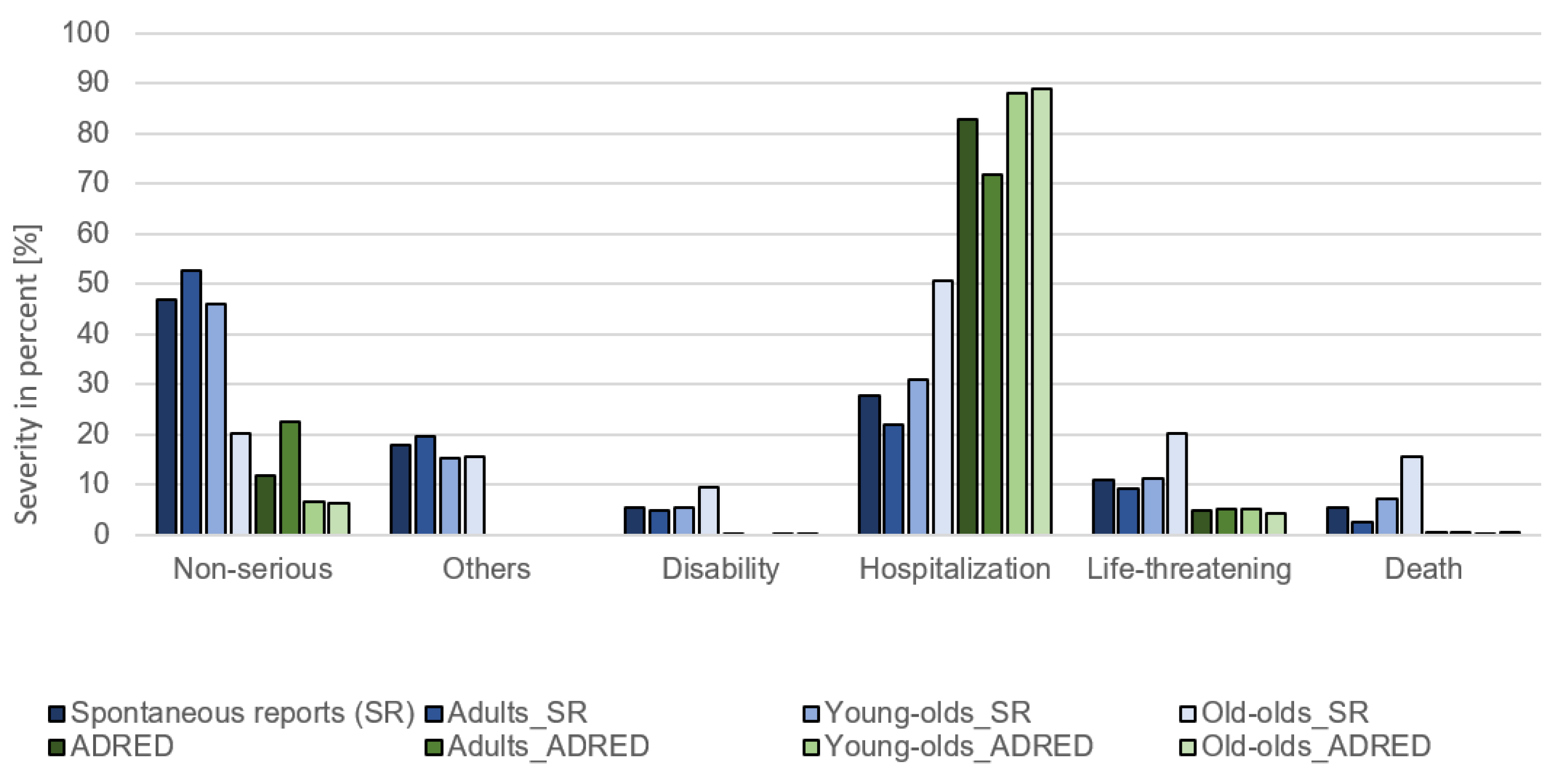
Figure 3.
Drug groups with an OR (95% CI) > 1 for (a) spontaneous reports and (b) ADRED study.
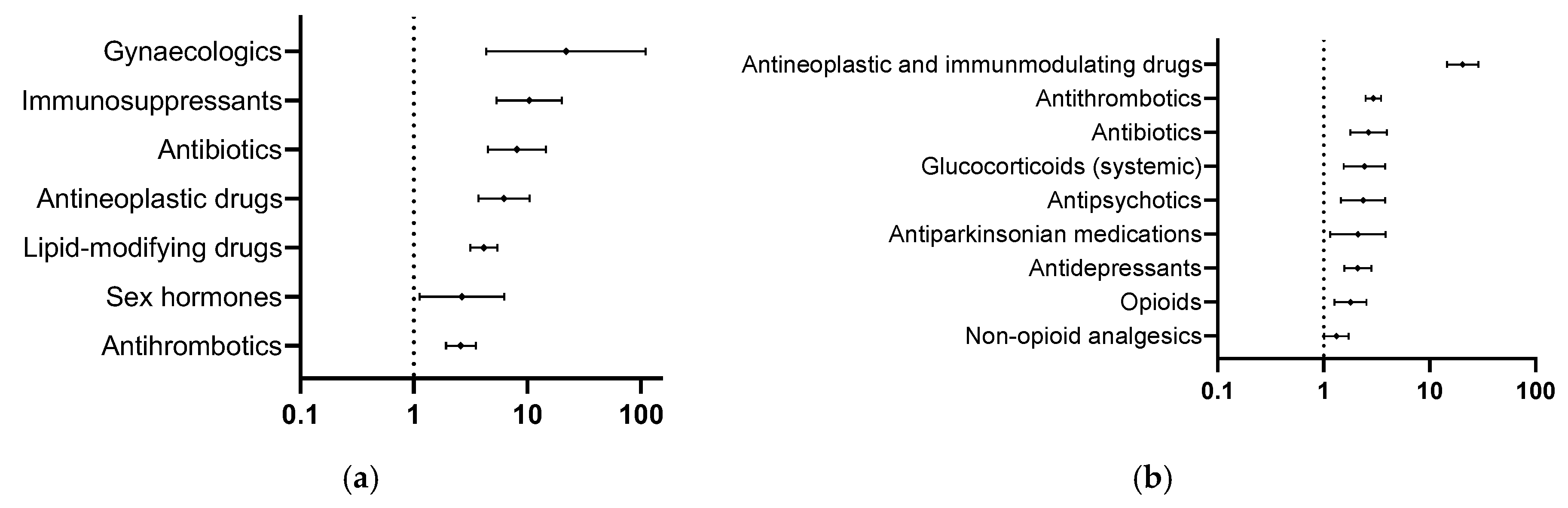

Table 1.
Characteristics of the comparison groups – Spontaneous reports and ADRED study.
| Spontaneous reports n = 2022 | Adult n = 1156 (57.2%) |
Young-old n = 647 (32.0%) |
Old-old n = 219 (10.8%) |
ADRED n = 2215 |
Adult n = 731 (33.0%) |
Young-old n = 880 (39.7%) |
Old-old n = 604 (27.3%) |
|
|---|---|---|---|---|---|---|---|---|
| Age (years) | 61 [48;73] | 50 [38;57] | 72 [68;76] | 84 [81;87] | 73 [58;80] | 51 [38;58] | 74[70;77] | 84 [82;87] |
| Sex, male | 895 (44.3%) | 476 (41.2%) | 335 (51.8%) | 84 (38.4%) | 1115 (50.3%) | 360 (49.2%) | 495 (56.3%) | 260 (43.0%) |
| Sex, not known | 10 (0.5%) | 6 (0.5%) | 3 (0.5%) | 1 (0.5%) | - | - | - | - |
| Number of suspected drugs | 1 [1;1] | 1 [1;1] | 1 [1;1] | 1 [1;1] | 1 [1;2] | 1 [1;2] | 2 [1;2] | 1 [1;2] |
| Number of taken drugs | 2 [1;5] | 1 [1;3] | 3 [1;6] | 4 [1;7] | 7 [3;10] | 3 [2;8] | 8 [5;11] | 8 [6;10] |
| Number of ADR per report/ case | 2 [1;3] | 2 [1;3] | 2 [1;3] | 2 [1;3] | 2 [1;4] | 2 [2;4] | 2 [1;4] | 2 [1;3] |
| Severity | Multiple choice possible2 | |||||||
| Non-serious | 950 (47.0%) | 609 (52.7%) | 297 (45.9%) | 44 (20.1%) | 261 (11.8%) | 165 (22.6%) | 58 (6.6%) | 38 (6.3%) |
| Others1 | 359 (17.8%) | 226 (19.6%) | 99 (15.3%) | 34 (15.5%) | - | - | - | - |
| Disability | 111 (5.5%) | 55 (4.8%) |
35 (5.4%) |
21 (9.6%) |
2 (0.1%) |
0 (0.0%) |
1 (0.1%) |
1 (0.2%) |
| Hospitalization | 562 (27.8%) | 252 (21.8%) | 199 (30.8%) | 111 (50.7%) | 1837 (82.9%) | 525 (71.8%) | 775 (88.1%) | 537 (88.9%) |
| Life-threatening | 223 (11.0%) | 106 (9.2%) | 73 (11.3%) | 44 (20.1%) | 107 (4.8%) |
37 (5.1%) |
45 (5.1%) | 25 (4.1%) |
| Death | 109 (5.4%) | 29 (2.5%) |
46 (7.1%) |
34 (15.5%) | 8 (0.4%) |
4 (0.5%) |
1 (0.1%) |
3 (0.5%) |
ADR: adverse drug reaction; 1Others: other serious reactions; 2within the spontaneous reports; continuous variables are shown as median [interquartile ranges, IQR], categorical variables are shown in absolute numbers (percentages).
Table 2.
Drug groups with an OR (95% CI) > 1 for the spontaneous reports and the ADRED study; sorted by OR (95% CI) in descending order.
Table 2.
Drug groups with an OR (95% CI) > 1 for the spontaneous reports and the ADRED study; sorted by OR (95% CI) in descending order.
| Spontaneous reports (n = 2022) ∑suspected = 2278; ∑total = 5755; m = 29, z = 3.12 |
Suspected drugs (n) |
Proportion of all suspected drugs (%) |
Total drugs (n) |
Proportion of all total drugs (%) |
OR (95% CI) |
|---|---|---|---|---|---|
| Gynaecologics | 56 | 2.5 | 60 | 1.0 | 21.88 (4.34 – 110.24) |
| Immunosuppressants | 165 | 7.2 | 191 | 3.3 | 10.36 (5.34 – 20.13) |
| Antibiotics | 168 | 7.4 | 202 | 3.5 | 8.06 (4.46 – 14.59) |
| Antineoplastic drugs | 179 | 7.9 | 226 | 3.9 | 6.22 (3.71 – 10.45) |
| Lipid-modifying drugs | 483 | 21.2 | 696 | 12.1 | 4.12 (3.14 – 5.42) |
| Sex hormones | 36 | 1.6 | 57 | 1.0 | 2.64 (1.12 – 6.25) |
| Antithrombotics | 296 | 13.0 | 486 | 8.4 | 2.58 (1.91 – 3.50) |
|
ADRED study (n = 2215) ∑suspected = 3985; ∑total = 15948; m = 28, z = 3.12 |
|||||
| Antineoplastic and immunomodulating drugs | 591 | 14.8 | 692 | 4.3 | 20.45 (14.54 – 28.77) |
| Antithrombotics | 763 | 19.1 | 1656 | 10.4 | 2.94 (2.49 – 3.47) |
| Antibiotics | 118 | 3.0 | 254 | 1.6 | 2.65 (1.78 – 3.95) |
| Glucocorticoids (systemic) | 87 | 2.2 | 196 | 1.2 | 2.43 (1.54 – 3.82) |
| Antipsychotics | 77 | 1.9 | 176 | 1.1 | 2.36 (1.46 – 3.81) |
| Antiparkinsonian medications | 46 | 1.2 | 112 | 0.7 | 2.11 (1.15 – 3.84) |
| Antidepressants | 196 | 4.9 | 483 | 3.0 | 2.10 (1.57 – 2.83) |
| Opioids | 129 | 3.2 | 349 | 2.2 | 1.79 (1.26 – 2.54) |
| Non-opioid analgesics | 208 | 5.2 | 687 | 4.3 | 1.32 (1.01 – 1.72) |
Drug groups found in more than 0.7% of all taken drugs in the dataset; Odds ratio (OR) = ((nsuspected drug group)/(∑suspected – nsuspected drug group))/((nconcomitant drug group)/(∑concomitant – nconcomitant drug group)) with concomitant = total – suspected; 95% confidence interval (95% CI) Bonferroni adjusted with m (number of testing) and a corresponding z value.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



