
Submitted:
12 January 2026
Posted:
13 January 2026
You are already at the latest version
Abstract
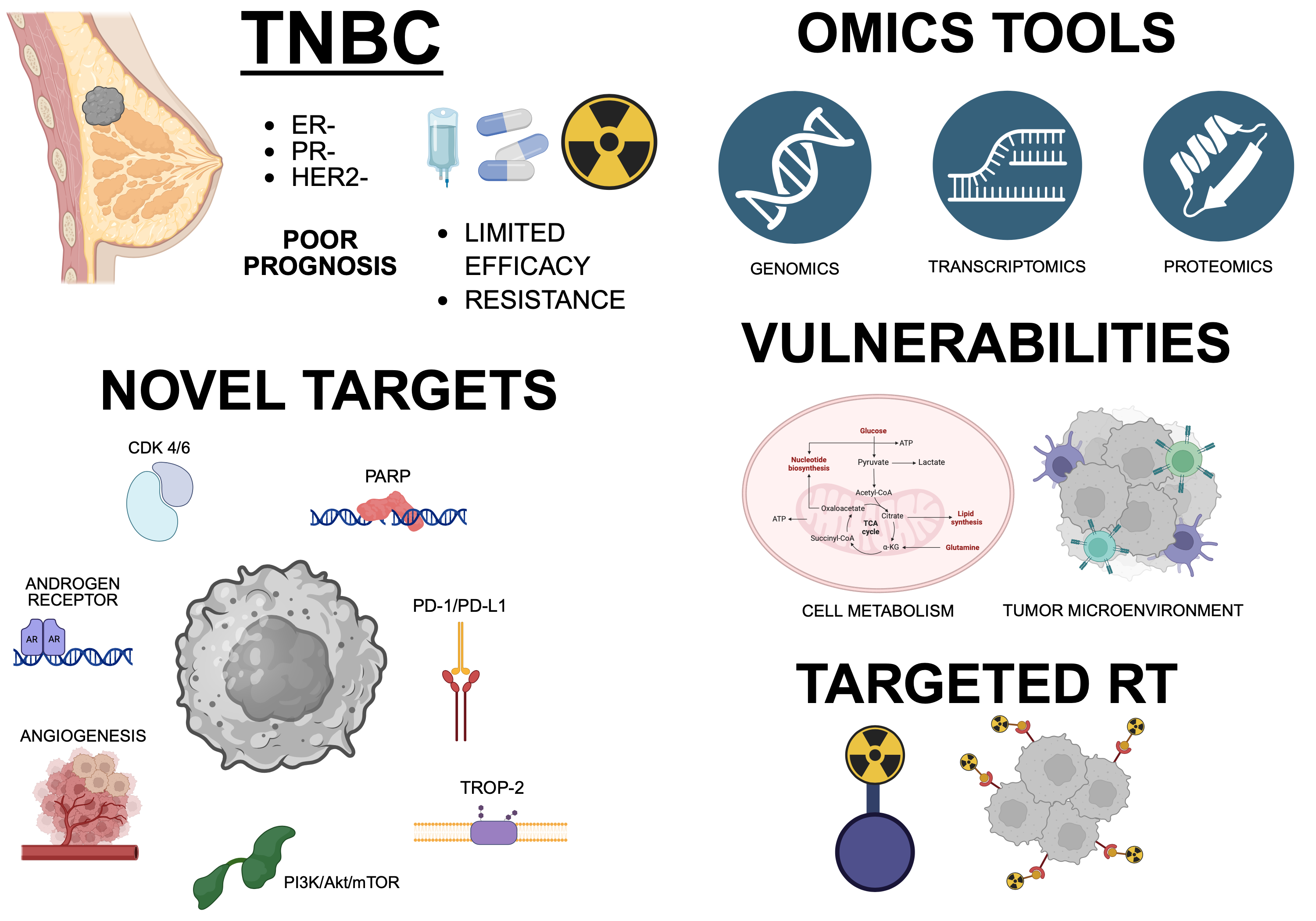
Triple-negative breast cancer (TNBC) remains one of the most aggressive and therapeutically challenging breast cancer subtypes, lacking expression of estrogen receptor, progesterone receptor, and HER2. Conventional chemotherapy and immune check-point inhibitors provide some benefit, but resistance and relapse are frequent. The search for novel targets has therefore become central to developing more effective and durable therapies. Recent advances in proteomics, structural biology, and targeted protein degradation are rapidly expanding the repertoire of actionable molecules in TNBC. This review summarizes current and emerging therapeutic strategies for TNBC, with a focus on targeted approaches designed to address tumor heterogeneity and resistance mechanisms. To the aim, recent advances in targeted therapies are examined, including immune checkpoint inhibitors, PARP inhibitors, Trop-2–directed antibody–drug conjugates, anti-angiogenic agents, PI3K/Akt/mTOR pathway inhibitors, androgen receptor antagonists, and CDK4/6 inhibitors, highlighting results from completed and ongoing clinical trials. In addition, we explore novel targets identified through integrative omics approaches, as well as the role of the tumor microenvironment in modulating therapeutic efficacy.
Finally, we outline innovative radiotherapy strategies based on targeted radiation delivery and biological integration with systemic therapies.
Collectively, this review provides an updated overview of the evolving TNBC therapeutic landscape and high-lights promising directions for the development of next-generation, biomarker-driven treatment strategies aimed at improving patient outcomes.
Keywords:
triple negative breast cancer
; targeted therapy
; omics
1. Introduction
Breast cancer (BC) is a complex and heterogeneous neoplasia, and it can be classified into different molecular subgroups based on the expression of specific markers, mainly represented by Hormone Receptors (HRs) and Human Epidermal growth factor Receptor-2 (HER2). HRs are the Progesterone receptor (PR) and the Estrogen Receptor (ER). The different phenotypes that derive from the combination of the expression of these cellular markers are classified into the following categories: HR-positive/HER2−negative (HR+/HER2−), which accounts for nearly 70% of the total cases; HER2−positive (HER2+), which represents 15–20% of total BCs; triple-negative breast cancer (TNBC), with a cellular expression of PR and ER of ≤1% and HER2 expression of 0 to 1+ by immunohistochemistry (IHC, according to the American Society of Clinical Oncology/College of American Pathologists ASCO/CAP) and that represents 10–20% of the total cases of BC [1,2,3].
Each of the three receptors represents a validated target for BC therapy and targeted drugs allow a very high therapeutic success, with a survival rate of about 90% at 5 years. For example, for women diagnosed between 2015 and 2021, relative survival is approximately 96% for HR+/HER2-, ~92% for HR+/HER2+ and about 87% for HR-/HER2+ tumors [4]. However, this statistic is much lower, around 78%, for HR-/HER2- TNBC.
This review summarizes the most recent innovative therapeutic approaches and outlines promising directions for developing next-generation therapeutics to address heterogeneity and resistance in TNBC, covering cell surface proteins and receptors, intracellular pathways of interest and the role of the tumor microenvironment (TME) in current and under-investigation therapies. We will initially focus on completed clinical trials and their results and then move to AI identified protein targets derived from omics data, metabolic alterations and observations regarding the TME. We will finally summarize the current and innovative radiotherapy (RT) approaches based on the use of radiosensitizers and targeted radiation delivery.
1.1. Epidemiology, Risk Factors and Prognosis
TNBC is a common cancer in women, with roughly 2 000 000 of cases diagnosed worldwide in 2022 [5]. In fact, it accounts for approximately 10% – 20% of all breast carcinomas. Moreover, epidemiological data show that TNBC is diagnosed mostly in premenopausal young women under 40 years old [5]. In addition, this tumor appears to be more frequent in African or Hispanic women [2], with African Americans having a worse prognosis compared to other groups [3]. Other non-modifiable risk factors are, as cited above, mutations in BRCA1 and BRCA2 genes, as well as TP53 gene mutations, familiar history and breast tissue density [3]. Among modifiable risk factors are unhealthy lifestyles and radiation exposure (secondary tumors after radiation therapy, RT) [1,3].
TNBC displays a worse prognosis when compared to the other subtypes of BC. It accounts for 5% of all cancer-caused deaths every year [5]. The median Overall Survival (OS) reaches 10.2 months with current therapies and the 5-year survival rate is around 60-65% for regional tumors, and only 11% for metastatic tumors [2,6]. The mortality rate gets higher in the first 3 months after relapse, reaching 75% [5]. Distant metastases are quite common, occurring in nearly 46% of patients.
1.2. Molecular, Histological and Clinical Classification
TNBC is, therefore, characterized by the lack of expression of all the three key molecular targets validated for therapy, an aggressive phenotype and an invasive behavior, with genetic instability and mutations in typical genes like Tumor Protein 53 (TP53), mutated in >80% of TNBC cases, PhosphatiIdylinositol-4,5-biphosphate 3-Kinase Catalytic subunit Alpha gene (PIK3CA) and BReast CAncer gene 1 (BRCA1). More than 85% of breast cancers developed following BRCA1 germline mutations display a triple-negative phenotype [2]. However, the genetic expression, the transcriptional profile and the histological phenotype differ widely [2]. In fact, from a molecular point of view, TNBCs can be classified into the following categories, proposed by Burstein et al. in 2015 [7], based on gene expression/transcriptional profile:
- Basal-Like Immuno Suppressed (BLIS), characterized by downregulation of B, T and natural killer (NK) cell immune-regulating pathways and cytokine pathways;
- Basal-Like Immune Activated (BLIA), displaying an opposite transcriptional profile with respect to the BLIS subtype, with upregulation of genes involved in immune cells activity;
- Mesenchymal (M or MES), enriched for genes involved in cell motility, Epithelial-Mesenchymal Transition (EMT), DNA Damage Response (DDR) pathways and growth factors pathways like the Insulin Growth Factor-1 (IGF-1) one. This type of cells constitutes metaplastic carcinomas with preferential metastasis to lungs, and shows defects in PhosphoInositide 3-Kinase (PI3K)/protein kinase B (Akt)/mechanistic Target Of Rapamycin (mTOR) (PI3K/Akt/mTOR) pathway;
- Luminal Androgen Receptor (LAR), characterized by Androgen Receptor (AR) signaling and hormonally regulated pathways, including the one of the ER. This feature is due to a small (~1%) subpopulation of LAR TNBC cells that show low ER activation, but these BCs are still classified as triple-negative because this subpopulation is too small to be detected by immunohistochemistry. This cell type causes a low-grade lobular carcinoma, with increased frequency of lymph node involvement. It represents 11% of all TNBCs [7,8].
Two more categories are also taken into account, according to the transcriptional features of Tumor-Infiltrating Lymphocytes (TILs) and tumor-associated stromal cells:
- Mesenchymal Stem-Like (MSL), which is enriched for stem cell-associated genes expression and angiogenesis genes expression;
- Immuno Modulatory (IM), whose tumor tissue overexpresses immune cell markers, like Nuclear Factor kappa B (NFKB), Tumor Necrosis Factor (TNF), Janus Kinase (JAK) and immune regulators like Cytotoxic T-Lymphocyte-Associated protein 4 (CTLA4), Programmed Death-1 and Programmed cell Death Ligand-1 (PD-1 and PD-L1), and displays the better prognosis among TNBCs. More than a proper tumoral subclass, this phenotype has been defined as the result of an immune modulation of the tumor generated by lymphocyte infiltration in the cancer microenvironment. Moreover, there is evidence that the presence of TILs might be a positive prognostic factor [2,8,9,10,11].
In 2016, Lehmann et al. [12] proposed a novel categorization of TNBCs, keeping the M and LAR classes and adding two more: the Basal-Like 1 (BL1) class, a ductal, high-grade carcinoma characterized by high expression of genes involved in cell cycle progression and DDR pathways. It displays impairments in Homology Directed Repair (HDR) mechanisms, a characteristic that makes this class sensitive to genotoxic therapies; and the Basal-Like 2 (BL2) class, a subgroup of metaplastic carcinoma that largely expresses genes coding for growth factors and for key enzymes of glycolysis and gluconeogenesis [2,8,11]. Along with the M subtype, the BL2 subclass frequently harbors alterations in the PI3K pathway genes (as very often observed in TNBC) and in the Wnt pathway genes, but mutations of β-catenin are remarkably infrequent in these tumors [2]. The BL1 subclass represents 18% of total TNBC cases, while the BL2 class accounts for 13% of TNBCs [8]. Another subgroup of TNBC is the so-called “claudin low”, characterized by low to null expression of luminal differentiation markers, high expression of EMT markers and cancer stem cell–like features, but according to Burstein’s classification this subgroup is included into the M category [11].
The division in transcriptionally different categories is a tool that can be used to predict the tumor response to different chemotherapeutics, and this helps the stratification of the patients to provide them with tailored therapy [11]. For example, the BL1 subtype seems to be highly responsive to DNA-targeting drugs like Anthracycline and Cyclophosphamide followed by Taxane (ACT) (52% of pathological Complete Responses, pCRs), while the BL2 and the LAR subtypes show the opposite effect with 0 and 10% pCRs, respectively. These data highlight the differences between BL1 and BL2 subtypes, even though they are both basal-like tumors [8]. Instead, LAR, M and MSL subtypes are more sensitive to the inhibition of the PI3K/Akt/mTOR pathway [2,8,13]. For what concerns the MSL and IM classes, TILs carry a gene expression profile marked by an increased expression of immune checkpoint regulators such as PD1, PD-L1 and CTLA4 which act as molecular targets for therapy [8].
The clinical behavior of TNBC is characterized by aggressiveness, invasiveness and frequent relapses. The outcome of TNBC metastasis is often lethal and involves the brain and visceral organs [2,14]. High proliferation rate, alteration in DNA repair genes and increased genomic instability are other TNBC typical markers. Histologically, it displays a poorly differentiated phenotype [15].
1.3. Current Therapies and Unmet Therapeutic Needs
Due to its low to absent cellular expression of actionable molecular targets, TNBC is not sensitive to endocrine therapy or molecular targeted therapy [6,16]. Therefore, the current therapies include nonspecific chemotherapy (neoadjuvant or adjuvant), surgery and radiotherapy [16].
Chemotherapy is mainly carried out through anthracyclines (e.g., doxorubicin) and taxanes (e.g., paclitaxel), which act inhibiting mitosis and blocking DNA topoisomerase activity, respectively, in combination with cyclophosphamide and platinum-based drugs (e.g., carboplatin) [17,18]. However, these treatments are associated with severe side effects and resistance, as well as frequent relapse, and this data is confirmed by the 70 – 80% of TNBC patients that do not achieve a complete response [16]. These patients are likely to suffer a recurrence and a lethal tumor metastasis [17]. The treatment of TNBC metastatic disease involves anthracyclines, platinum-based drugs and taxanes, as previously described, capecitabine, gemcitabine, vinorelbine, eribulin. For tumors carrying BRCA1/2 germline mutations, monoclonal antibodies conjugated or not with drugs like Sacituzumab Govitecan (SG) or Bevacizumab are implemented. PD-L1-overexpressing cancer patients are treated with atezolizumab or pembrolizumab [17]. However, TNBC is characterized by intrinsic chemoresistance, mainly due to cancer stem cells (CSCs) presence, ATP-binding cassette (ATP) transporters (e.g., multidrug resistance protein-1 and, MRP [10]), hypoxia and avoidance of apoptosis [17].
For radiotherapy (RT), current guidelines do not differentiate irradiation protocols for the various breast cancer subtypes and the molecular subtyping of TNBC has not been integrated with RT protocols yet [19]. Despite this, the role of RT in the treatment of TNBC remains crucial, as described by Haque et al. in 2019 [20]. In this study, out of 8526 TNBC patients older than 70 years, 74% received adjuvant RT and 26% did not. After a median follow-up of 38 months the 5-year OS was significantly higher in the group that received adjuvant RT (77.2% vs 55.3%, p<0.001) and this effect was also maintained after stratification for age, stage and chemotherapy implementation [20]. In another comparative study conducted by Abdulkarim et al. [21], locoregional recurrence was reduced with the addition of adjuvant RT in 768 TNBC patients, after a median follow-up of 7.2 years (p<0.01). The American Society of Radiation Oncology published guidelines about the use of radiotherapy after mastectomy, only for patients who failed to achieve a complete nodal response. However, for patients who responded well to neoadjuvant chemotherapy, no definite recommendations were given [22]. Although adjuvant RT can improve the local progression and recurrence of TNBC, there is a percentage of TNBC patients resistant to RT, revealing a radioresistance characteristic in TNBC [19].
The poor prognosis of TNBC patients with the current therapies and the heterogeneity of this tumor drive the research towards new therapeutical strategies.
2. Current Approaches and Clinical Trials
2.1. Targeted Therapy in TNBC Patients
The lack of expression of the three known, key extra- and intracellular receptors for molecules involved in cell growth in TNBC imposes the development of alternative therapeutic strategies. Possible approaches could be targeting immune checkpoints (e.g., PD-1 and PDL-1), administration of Poly ADP-ribose polymerase (PARP) inhibitors (presently used mainly for BRCA-mutated TNBCs) or Tumor-associated calcium signal transducer 2 (Trop-2) inhibitors, possibly through antibody-drugs conjugates (ADCs), antiangiogenic agents, PI3K/Akt/mTOR pathway inhibitors, cyclin-dependent kinase (CDK) 4/6 blockers and AR inhibitors for LAR subtypes. The use of the above-mentioned therapeutics is strictly related to the molecular biomarkers of each single tumor and to other factors like cancer stage and grade [6,11,23,24].
2.2. Current Treatments and Clinical Trials
The phase II clinical trial FASCINATE-N (NCT05582499) serves as a key example of how multiple therapeutic strategies can converge in TNBC. This neoadjuvant precision-based platform assigns patients to distinct treatment arms according to their tumor’s molecular profile, integrating immune-based therapies, DNA-damage–targeting agents, and additional pathway-specific treatments. By evaluating diverse targeted approaches within a single platform structure, the study demonstrates how the heterogeneity of TNBC can be addressed through complex, multi-layered therapeutic designs, effectively connecting and reinforcing different therapeutic targets. FASCINATE-N goal is to test the efficacy of novel drugs alone or in combination with standard chemotherapy. In particular, patients with different types of TNBC were randomly divided into groups according to molecular typing and subtyping and received targeted treatment or conventional neoadjuvant chemotherapy. As a result, 53 subgroups with specific molecular features were formed. A specific clinical profile could be present in more than one molecularly-defined group to test different combinations of drugs, to cover as many therapeutic options as possible in order to figure out the best treatment regimens for each subset. Novel agents being tested include CDK 4/6 inhibitors, PD-1/PD-L1 monoclonal antibodies, PARP inhibitors, HER2 inhibitors, Trop-2 inhibitors, and angiogenesis inhibitors. pCR is set as the primary outcome measure; secondary endpoints will be invasive disease-free survival (iDFS), overall/objective response rate (ORR), evaluation of adverse effects using the Common Terminology Criteria for Adverse Events (CTCAE) scale (v 4.0), evaluation of gene expression profile during treatment and number of peripheral blood mononuclear cells (PBMCs) during treatment. The study started in 2022 and is planned to be completed by 2028 [25].
Below is an extensive review of the currently available targeted therapies and ongoing clinical trials on TNBC patients. The ClinicalTrials.gov database [26] was consulted in December 2025. Table 1 summarizes clinical trials investigating targeted therapeutic approaches in triple-negative breast cancer (TNBC). Trials are grouped according to their molecular target and type of intervention, and are classified by study status (recruiting, terminated, or withdrawn). For each trial, we report the ClinicalTrials.gov identifier, investigational drug, years of trial development, clinical phase, corresponding citation (when available), and main published outcomes. This comprehensive overview highlights both ongoing efforts and past challenges in advancing targeted therapies for TNBC.
PD-1/PD-L1 Inhibitors
PD-1 is a member of the immunoglobulin superfamily, with a fundamental role in apoptosis. It is a type I transmembrane glycoproteic receptor of 50–55 kDa, with a cytoplasmic tail containing the Immune receptor Tyrosine-based Inhibitory Motif (ITIM) and an Immune receptor inhibitory Tyrosine-based Switch Motif (ITSM) necessary to its immune function. PD-1 is expressed on mature T cells, B cells and monocytes [27,28]. PD-L1 and PD-L2 are the ligands of PD-1. This ligand-receptor interaction negatively regulates the activity of immune cells, and, when this happens in the TME, it results in an immune suppression against cancer cells. When activated by PD-L1 expressed by tumor cells, in fact, PD-1 brings T cells to apoptosis, and this phenomenon permits tumor cells to evade immune surveillance. Immunotherapy with PD-1 and PD-L1 inhibitors aims to block this interaction and promote T cell activation to generate an anti-tumor immune effect [28]. PD-1/PD-L1 inhibitors are becoming the standard therapy for various cancers and represent valid tools for immunotherapy [28]. Subtypes of TNBC can be PD-L1-positive (PD-L1+) [29], and, therefore, they are eligible for a therapy based on PD-1/PD-L1 inhibitors. Among these, pembrolizumab and nivolumab (anti PD-1), and atezolizumab, avelumab and durvalumab (anti PD-L1), are the most well-studied monoclonal antibodies (mAb) for immunotherapy in the last decade.
In TNBC patients, anti PD-1 mAbs JS001 and PDR001 (spartalizumab) have been demonstrated to be well tolerated during phase I-II clinical trials (NCT02838823 and NCT02404441, respectively). Their anti-tumor activity, however, has been shown to be moderate [30,31]. Pembrolizumab is a humanized mAb with high affinity for PD-1. It has been commercialized under the name Keytruda since 2017 and, after years of clinical trials, it is currently used in the treatment of melanoma, non-small cell lung cancer (NSCLC), Merkel-cell carcinoma and lymphomas. The Food and Drug Administration (FDA) approved pembrolizumab for advanced and metastatic TNBC treatment in 2020, and this regimen is now the standard of care first line treatment for PD-L1+ TNBC patients [32].
Several clinical trials using anti PD-L1 mAbs in TNBC are ongoing. Among them, the phase III clinical trial TROPION-Breast05 (ClinicalTrials.gov ID: NCT06103864) challenges pembrolizumab efficacy, testing the anti-tumoral effects of datopotamab deruxtecan (Dato-DXd), an anti Trop-2 mAb (see below), with or without durvalumab (Imfinzi, already in use for urothelial carcinoma and NSCLC, [33]) in comparison with pembrolizumab [34].
Atezolizumab (commercialized as Tecentriq) and currently used in the treatment of urothelial carcinoma, NSCLC, small cell lung cancer SCLC, hepatocellular carcinoma HCC and melanoma and avelumab (Bavencio), already in use in the treatment of Merkel cell carcinoma and metastatic urothelial carcinoma [35], are two anti PD-L1 mAbs under investigation in TNBC patients in phase I clinical trials NCT03170960 and NCT04360941 (PAveMenT), respectively. The main goal of these studies is, besides determining safety, to assess the efficacy of these mAbs. The study on atezolizumab is expanded to 18 cohort-specific tumors, and the first results on urothelial, gastric, prostate and renal cancer have already been published [35,36,37,38].
Three clinical trials on PD-1/PD-L1 inhibitors were terminated without any specific outcome (NCT02936102, NCT04916002, NCT03549000).
2.3. PARP Inhibitors
In recent years, PARP inhibitors have emerged as an important treatment option and are now considered part of the standard of care for TNBC patients carrying germline BRCA1/2 mutations [39]. Although numerous agents are currently under investigation as potential treatments for TNBC, PARP inhibitors olaparib and talazoparib remain the most clinically validated and widely adopted options [40,41]. The mechanism can be summarized as follows: beyond simply inhibiting PARP’s enzymatic function, PARP inhibitors can also trap PARP proteins on DNA, forming cytotoxic PARP–DNA complexes. Importantly, the ability to trap PARP does not correlate with catalytic inhibition and differs markedly among available PARP inhibitors. Preclinical studies suggest that this trapping effect may contribute more to antitumor activity than enzymatic inhibition alone [39].
Veliparib (NCT01306032), olaparib (DORA, NCT03167619 and NCT00679783), rucaparib (BRE09-146, NCT01074970), niraparib (TOPACIO/KEYNOTE-162, NCT02657889), talazoparib (BMN-673, NCT02401347) were tested in phase II clinical trials in TNBC patients.
Briefly, veliparib was demonstrated to be well tolerated and showed promising activity in a subset of patients with BRCA mutations (NCT01306032; [42,43]), as well as niraparib when administered in combination with pembrolizumab (TOPACIO/KEYNOTE-162, NCT02657889; [44]) in terms of Objective Response Rate (ORR) and Disease Control Rate (DCR). Promising results and good tolerability were observed also by administrating olaparib in combination with durvalumab in advanced or metastatic TNBC patients (DORA, NCT03167619; [45]). The combination of olaparib and the heat shock protein 90 (HSP90) inhibitor onalespib (phase I clinical trial, NCT02898207) showed preliminary evidence of anti-tumor activity. However, single-agent administration of olaparib failed to provide a successful efficacy [46]. On the contrary, the outcome of a clinical trial on talazoparib as a single-agent in HER2-negative BC without germline mutations in BRCA1/2, but with either homologous-recombination pathway gene mutations (e.g., Partner and Localizer of BRCA2 PALB2, CHEK2, etc.) or high tumor Homologous Recombination Deficiency (HRD) scores, showed an interesting anti-tumor effects in terms of partial response and Clinical Benefit Rate (CBR, [47]). These data suggest that talazoparib can be active in a subset of advanced TNBC/HER2-negative breast cancers even in the absence of BRCA1/2 mutations, provided that other HR-pathway defects are present. Finally, the combination of rucaparib with canonical cisplatin did not significantly improve 2-year DFS, nor 5-year DFS in TNBC patients [48].
Pamiparib (BGB-290) underwent a phase I trial (NCT03150810) in combination with the alkylating agent temozolomide (TMZ) in patients with locally advanced or metastatic solid tumors including those with advanced or metastatic TNBC. The study demonstrated that pamiparib combined with low-dose TMZ is feasible and tolerable in heavily pretreated metastatic/advanced solid-tumor population and shows modest anti-tumor activity; benefits appear more likely in tumors with HR-repair deficiency rather than unselected cases [49].
Two recruiting trials illustrate complementary strategies being tested in early and advanced-stage TNBC settings to improve outcomes for breast cancer patients through biomarker-driven intensification and novel agents. The randomized phase II-III study (NCT03150576), in which the PARP inhibitor olaparib is combined with a platinum-taxane backbone, showed an increased pCR and an improvement of long-term outcomes in TNBC and/or germline BRCA-mutant patients. An early-phase clinical trial (NCT05933265) using LP-184 in refractory-disease, showed good results as a first-in-human dose-finding and safety, and preliminary data show an augmented activity in tumors with DNA damage repair defects. While not limited to breast cancer, its focus on pharmacokinetics, tolerability, and exploratory biomarker correlations provides evidences that LP-184 could, if active and tolerable, be considered as a later-line option for patients who progress after standard and targeted neoadjuvant/adjuvant therapies or offer mechanistic insight relevant to PARP-sensitive biology.
It is worth to mention that between 2015 and 2024, several early-phase clinical trials investigating PARP inhibitors in combination with other agents were terminated before completion, primarily due to issues related to funding, slow enrollment, or sponsor decisions (NCT03875313 on the glutaminase inhibitor CB-839 in combination with talazoparib; NCT03801369 on olaparib combined with durvalumab, selumetinib, capivasertib or ceralasertib in TNBC; NCT04916002 on the effects of cemiplimab with vidutolimod in advanced cancers; NCT05252390 which evaluated NUV-868 alone and in combination with olaparib or enzalutamide; NCT02419495 which assessed selinexor combined with multiple chemotherapy or immunotherapy regimens in advanced malignancies).
2.4. Trop-2-Targeted Antibodies
Trop-2 is a transmembrane glycoprotein that was initially described in trophoblast and fetal tissues, then subsequent studies have demonstrated its overexpression in a wide range of solid tumors such as breast cancer. This cancer-associated overexpression, in contrast with limited expression in the normal condition in adult tissues, highlights the rationale for targeting Trop-2 therapeutically. Nowadays, there are many new approaches related to Trop-2-targeted ADCs for breast cancer treatment. ADCs [50] are molecules composed of a monoclonal antibody directed against a tumor-associated antigen, linked via a chemical bound to a cytotoxic payload. Upon binding to the antigen on cancer cells, the ADC is internalized, and the toxic payload is released, causing cell death with the aim of maximizing tumor killing while minimizing damage to normal tissues and overcoming some of the limitations of conventional chemotherapy in TNBC [51,52,53].
Two important molecules of this category are Sacituzumab Govitecan (SG) and Dato-DXd that showed an antitumor activity. Thus, there are many new approaches in which Trop2-directed ADCs are combined with other forms of therapy, including immunotherapy, targeted therapies, and small molecule inhibitors [54,55,56]. The ASPRIA trial (NCT04434040), for example, combines SG and atezolizumab to target minimal residual disease detectable through circulating tumor DNA. SG is the protagonist of the phase I/II basket trial NCT01631552, which evaluated SG combined with the active metabolite of irinotecan (SN-38) in patients with metastatic TNBC who had already received at least two prior systemic therapies for metastatic disease. Overall, this study provided early evidence that SG has clinically meaningful activity in heavily pretreated metastatic TNBC, justifying further development, evidence which later supported regulatory approval of the drug in this indication. The toxicity profile of SG in this study was considered manageable and consistent with its mechanism [57,58,59].
Several ongoing clinical trials are actively exploring Trop-2-targeted ADCs as a promising therapeutic approach for advanced or metastatic TNBC either as monotherapy or in combination with immunotherapy or other targeted modalities, aiming to expand options for patients who have already received prior treatments. The NCT05749588 and NCT06649331 trials, for example, investigate a Trop-2-directed ADC alone or combined with immunotherapy, assessing objective response rates across different TNBC molecular subtypes, while also monitoring Progression Free Survival (PFS) and Oversall Survival (OS), Duration of Response (DoR), disease control and safety. Similarly, NCT06851299 explores multiple therapeutic strategies, including ADC monotherapy, ADC with immunotherapy, and a triple combination with anti-angiogenic therapy, using Topoisomerase 1 (TOP1) inhibitor–based ADCs, to determine both clinical efficacy and safety across diverse patient cohorts.
Similarly, NCT06841354 is testing the efficacy of sacituzumab tirumotecan, either alone or in combination with pembrolizumab, versus standard chemotherapy in PD-L1–low TNBC patients.
Other adaptive platform clinical studies, such as NCT06649331, employ Bayesian response-adaptive designs to evaluate rechallenge with Trop-2, HER2, HER3, and Nectin-4 ADCs in heavily pretreated metastatic breast cancer. These trials seek to identify the most effective regimens based on objective response, molecular signatures, and PFS, while continuously optimizing the study arms for maximum benefit. Single-arm studies, like NCT06793332, are exploring the combination of bispecific antibodies, such as ivonescimab (AK112), with Trop-2 ADCs, particularly in patients with brain metastases, with the dual goals of confirming safety and demonstrating both intracranial and extracranial antitumor activity in populations with historically poor prognosis.
Innovative imaging strategies are also being integrated into the evaluation of Trop-2 ADCs. The exploratory trial NCT07046455 uses the positron emission tomography (PET) probe 89Zr-DFO-hSR7 to monitor Trop-2 expression and treatment response in patients receiving SG, correlating imaging signals with tissue expression and clinical outcomes, while also exploring mechanisms of resistance and biodistribution. Complementing these efforts, multicenter studies such as NCT06878625 assess Trop-2 ADCs in combination with PD-1 blockade, with or without additional anti-angiogenic therapy, focusing primarily on PFS while incorporating extensive biomarker and safety analyses.
Several pivotal trials are establishing the role of Trop-2 ADCs in both metastatic and neoadjuvant settings. NCT06841354 evaluates sacituzumab tirumotecan, alone or combined with pembrolizumab, in previously untreated, unresectable or metastatic TNBC, with endpoints including overall and PFS, objective response, and DoR.
Dato-DXd, mentioned before, is also being investigated in multiple trials, including NCT06974604 and the already cited TROPION-Breast05 (NCT06103864).
Together, these trials represent a concerted effort to define the therapeutic potential of Trop2-targeted ADCs across different clinical contexts, from heavily pretreated metastatic disease to neoadjuvant therapy, and from monotherapy to rationally designed combinations, reflecting the growing emphasis on precision medicine and biomarker-driven treatment strategies in TNBC.
Only one trial (NCT03901469) was prematurely terminated due to the fact that an interim analysis indicated insufficient efficacy, with no safety issues involved. This trial investigated the combination of ZEN003694, a BET inhibitor, with talazoparib, a PARP inhibitor, in TNBC patients who were BRCA wild-type, including those who had previously received Trop-2 ADCs. While Trop-2 ADCs directly deliver cytotoxic payloads to Trop-2 expressing cells, the ZEN003694 plus talazoparib combination exploitsed epigenetic modulation and DNA repair inhibition, potentially overcoming resistance mechanisms and expanding therapeutic options for TNBC.
2.5. Anti-Angiogenic Agents
Angiogenesis is the process of development of new immature and disorganized blood vessels within tumorigenesis that let cancer cells get the oxygen and nutrients they need to proliferate. The expansion of the tumor increases oxygen consumption and generates regions of the malignant mass that lie far from blood vessels, leading these areas to experience hypoxic conditions. This crucial step in tumor development is called angiogenic switch. Hypoxia triggers the nuclear translocation of Hypoxia-Inducible Factors (HIFs) in cancer cells. HIF-1α dimerizes with HIF-1β and the complex binds the Hypoxia Response Element (HRE) on the DNA, acting as a transcriptional factor for pro-angiogenic mediators like Vascular Endothelial Growth Factor (VEGF), Placental Growth Factor (PlGF), Fibroblast Growth Factor (FGF) and Platelet-Derived Growth Factor (PDGF). When these factors reach their receptors on tip and stalk cells, specialized endothelial cells that emerge during angiogenesis to form sprouts, their activated pathway crosstalk and determine the sprouting of blood vessels towards the hypoxic regions of the tumor. The persistent and deregulated presence of pro-angiogenic factors marks a difference with the normal genesis of arteries, veins and capillaries, and causes the formation of abnormal, disorganized and chaotic vessels: tumor-induced vessels, in fact, are characterized by heterogenous size and caliber and irregular blood flow, which fail to provide oxygen and nutrients to all cancer cells, leaving hypoxic areas. The abnormal structure of the tumor vessels and the impaired blood perfusion block the infiltrations of immune cells, which creates an immunosuppressive tumor microenvironment, and interferes with drug delivery. Therefore, in a counterintuitive approach, targeting angiogenesis to restore a normal blood flow in the TME would permit the perfusion of drugs and immune cells in the microenvironment [60,61,62].
Bevacizumab, commercialized as Avastin and used to treat metastatic breast cancer, NSCLC, glioblastoma, renal cell carcinoma, ovarian cancer and cervical cancer, is an anti VEGF mAb (32335505). Its safety and efficacy in TNBC have been tested in phase II clinical trials NCT03577743 (RIBBON-2) and NCT06817525. While the first one showed positive results (22415477), the outcomes of the latter have not been published yet.
Other anti-angiogenic agents are under investigation. Lenvatinib (commercialized as Lenvima) is a powerful antiangiogenic agent, tyrosine kinase inhibitor, already in use to treat medullary, anaplastic thyroid, adenoid cystic and endometrial cancer [63]. The phase II clinical trial MK-7902-005/E7080-G000-224/LEAP-005 (NCT03797326) tested its efficacy and safety in combination with anti-PD-1 mAb Pembrolizumab on a cohort of patients with solid tumors, including TNBC, and demonstrated antitumor activity with a manageable safety profile [64].
Another tyrosine kinase inhibitor anti-angiogenic agent is anlotinib (commercial name FOCUS V, AL3818), already approved by China Food and Drug Administration (CFDA) for the treatment of NSCLC [65]. Its efficacy in combination with anti-PD-1 mAb sintilimab on TNBC is under investigation in the context of phase II clinical trial NeoSACT (NCT04877821). The combined treatment exhibited a very rapid response, with 96.6% of patients achieving tumor reduction by ≥30% after just one cycle of treatment [66].
An innovative anti-angiogenic molecule is B1962, a bispecific antibody against PD-L1 and VEGF with a high anti-angiogenic activity, which is being studied in phase II clinical trial NCT06724263, after phase I demonstrated excellent safety and promising therapeutic effects.
2.6. PI3K/Akt/mTOR Pathway Inhibitors
Among the multiple molecular pathways activated in TNBC, PI3K/Akt/mTOR signaling pathway plays a fundamental role in protein synthesis, cell proliferation and survival. Its deregulated activation in TNBC (25% of cases) leads to increased cell proliferation and abnormal cell behavior. Therefore, it is considered a promising molecular target for TNBC treatment [67,68].
Buparlisib (BKM120), PQR309 and gedatolisib (PF-05212384) are three different PI3K inhibitors which, in their clinical trials (NCT01629615, PIQHASSO NCT02723877 and NCT01920061, respectively), displayed different results. Buparlisib, despite its molecular effects on PI3K, may not be sufficient as a single agent in TNBC [69], while its use in combination with gedatolisib resulted in dose-limiting toxicities in 10% of patients and a complete response in one patient in each TNBC arm [70].
In the context of PI3K inhibitors, several clinical trials are ongoing using different molecules. BCTOP-T-M03 reached phase III clinical study (NCT05954442) on anti-tumoral activity and effects on quality of life. Tenalisib (δ- and γ-PI3K specific inhibitor) and MEN1611 (selective inhibitor of α- β- and γ-PI3K, with reduced activity on δ isoform) are being tested in phase II clinical trials (NCT06189209 and SABINA NCT05810870, respectively), in which safety and efficacy are the main endpoints.
β-PI3K inhibitor AZD8186 safety, tolerability and efficacy on TNBC are being tested in a phase I clinical study (NCT03218826). The first results showed that the Maximum Tolerated Dose (MTD) was not reached and the most frequent adverse events were anemia (57%), diarrhea (43%) and fatigue (43%) [71].
Four clinical trials on PI3K inhibitors have been terminated, of which two due to excessive toxicity of the tested compounds (GDC-094 NCT01918306 and taselisib NCT02457910). Studies no. NCT04216472 and NCT02476955 were terminated, the first one due to low participation.
2.7. Androgen Receptor Inhibitors
The AR is expressed in many human tissues, including BC tissue. In fact, it has been noted that 70–90% of BC patients overexpress AR, making this marker a possible drug target. For what concerns TNBC, LAR subtype is characterized by AR expression and, considering the lowest rate of pCR to chemotherapy (21.4% vs 65.6% of BL TNBCs), this can be used as a prognostic factor [72,73]. When androgens (testosterone, T, or dihydrotestosterone, DHT) enter the cells and bind their receptor located in the cytoplasm, the complex moves to the nucleus and binds to the Androgen Responsive Element (ARE) on the DNA. This results in a change of gene expression altering apoptosis, differentiation, angiogenesis and proliferation. There is an interesting crosstalk between AR and PI3K pathways, supported by the fact that, in TNBC, the frequency of PIK3CA mutations in AR+ tumors seems higher than that in AR-negative tumors. Androgen signaling upregulates Phosphatase and TENsin homolog (PTEN) expression. PTEN is PI3K main counterpart, as it dephosphorylates phosphatidyl-inositol-3,4,5-triphosphate (PIP3) in phosphatidyl-inositol-4,5-biphosphate (PIP2). The activation of PTEN restrains PI3K action which weakens AR activity. In TNBC, AR and PI3K overexpression is often paired, and in these cases the abundance of PI3K bypasses AR-mediated PTEN upregulation. Therefore, targeting only AR will result in a lack of support of PTEN activity, paving the way for PI3K proliferative activity. Hence, dual targeting of the AR and PI3K may produce a synergistic anti-tumor effect [74].
2.8. CDK 4/6 Inhibitors
CDKs are the fundamental regulatory enzymes that control cell cycle progression until cell division. Their activity relies on cyclin activation. CDK 4/6 is the key regulator of the G1/S transition and activator of the cell cycle. In particular, cyclin D1 binds to CDK 4 and CDK 6, forming a complex that, when activated by CDK-Activating Kinases (CAKs), phosphorylates the tumor suppressor Retinoblastoma protein (Rb). Dephosphorylated Rb remains bound to the E2F transcription factor, keeping it inactive, but its inactivation through CDK4/6-mediated phosphorylation sets E2F free, which positively regulates cyclin E and DNA synthesis gene expression, driving the cell cycle progression through G1/S transition. Aberrancies in this pathway lead to uncontrolled cellular proliferation, the basis of cancer development. Therefore, CDK 4/6 inhibition can represent a potential therapeutic target, inducing cell cycle arrest in the G1 phase and resulting in a blockade of tumor growth. In TNBC, Rb dysfunctions are present in approximately 30% of cases [77,78,79,80]. Finn et al. [81] discovered that TNBC cell lines showed sensitivity to CDK 4/6 inhibition, even though less than ER+ cell lines. Loss of Rb (observed in 7–20% of TNBC) and overexpression of cyclin E can explain this partial resistance to CDK4/6 inhibitors in TNBC cell lines [78].
Trilaciclib is a CDK 4/6 inhibitor whose safety and efficacy on TNBC in combination with other chemotherapeutics have been cleared in clinical trials NCT05112536 (phase II) and NCT04799249 (PRESERVE 2, phase III). Phase II revealed a correlation between the presence of TILs (measured as CD8+ T cell number and high ratio of CD8+ over T regulatory cells) and favorable outcomes, while the results of phase III are under quality control review currently [82].
Ribociclib and Palbociclib are two CDK 4/6 inhibitors under investigation in phase I and II clinical trials named CHARGE (NCT04315233) and CAREGIVER (NCT05067530), respectively. Both drugs are already in use drugs: ribociclib is commercialized under the name Kisqali and used in the treatment of HR+ BC [83], while Palbociclib is commercialized as Ibrance and is used for HR+/HER2- BC [84] treatment.
It is worth mentioning two studies on CDK2 inhibitors under investigation: AVZO-021 (NCT05867251, phase I-II) and NKT3964 (NCT06586957, phase I). Both studies focus on tolerability, pharmacokinetics and pharmacodynamics of these molecules on a panel of solid tumors including TNBC.
Four clinical trials on CDK 4/6 inhibitors (of which two on trilaciclib, a small molecule used to prevent bone marrow suppression by anticancer therapies, [85]) were terminated, though none of them for safety- or inefficacy-related reasons.
3. New Possible Targets Identified by Omics Approaches
Deposited omics data yield unique TNBC marker combinations. Integrative analyses that span transcriptomics, genomics, proteomics, epigenomics, and, in one instance, metabolomics report cancer-specific signatures. For example, gene panels ranging from three to 100 markers achieve classification accuracies up to 98.9% and concordance indices of 0.7573, while a 29-protein signature reached 88% accuracy and showed strong survival correlations. Validation approaches are still needed and include experimental methods (cell lines, CRISPR screens, western blot) and in silico analyses (public datasets, survival curves). In order to extract the most significant studies and results, we took advantage of the Elicit AI research assistant to perform a literature research and data extraction based on evidence-based answers with citations. We performed a semantic search using the query “Among the deposited omics data is it possible to identify unique combinations of markers for triple negative breast cancer? Select also targets which are not known to be drugged” across over 138 million academic papers from the Elicit search engine, which includes all Semantic Scholar and OpenAlex. We retrieved the 498 papers most relevant to the query.
Among the molecules that this approach identified as associated with TNBC pathogenesis and progression are nine proteins: GGH, TYMS, PTK6, TOP1MT, SMO, CSF1R, EPHB3, TRIB1, and LAD1 (Table 2). These proteins span diverse functional categories, including nucleotide metabolism, DNA topology, kinase signaling, developmental pathways, and cytoskeletal interactions. Notably, several of them are implicated in cell proliferation, apoptosis resistance, immune modulation, and metastatic behavior, that represent hallmarks of aggressive TNBC phenotypes.
3.1. γ-Glutamyl Hydrolase (GGH)
The key function of γ-Glutamyl Hydrolase (GGH), an enzyme mainly located in the lysosome, is to eliminate polyglutamate residues from folates and antifolates. GGH can then be released into the extracellular space, where it maintains its enzymatic activity [98,99] (UniProt: Q92820). It has an effect on DNA methylation, synthesis, and repair. GGH has been found to be a significant molecular marker in a number of cancers, such as pancreatic adenocarcinoma, lung adenocarcinoma, and kidney renal clear cell carcinoma [100]. GGH is found in tumour tissues in TNBC, indicating a possible function in promoting fast proliferation via folate metabolism [101,102]. It has been demonstrated that GGH regulation influences the chemosensitivity of cancer cells to antifolates like methotrexate and 5-fluorouracil, probably by changing intracellular absorption of drugs and folate polyglutamate concentrations [103]. Although increased GGH expression in breast cancer has been linked to poor clinical outcomes, its particular prognostic function in TNBC remains unclear [102].
3.2. ThYMidylate Synthase (TYMS)
By catalyzing the reductive methylation of dUMP to dTMP using 5,10-methylenetetrahydrofolate as a one-carbon donor, ThYMidylate Synthase (TYMS) plays a crucial part in nucleotide metabolism. TYMS promotes both cytosolic and de novo mitochondrial thymidylate synthesis pathways via its presence in the nucleus, cytoplasm, and several mitochondrial compartments, including the matrix and inner membrane [104,105] (UniProt: P04818). Increased proliferation, improved DNA repair ability, and resistance to antifolate-related chemotherapies are often linked to the expression of TYMS in malignancies [106,107,108,109]. In a number of cancers, such as kidney renal clear cell carcinoma, liver hepatocellular carcinoma, lung adenocarcinoma, and pancreatic adenocarcinoma, increased levels of TYMS have been discovered to be prognostic biomarkers related to poor survival outcome [100,106,107,108]. Preclinical models have demonstrated that high TYMS levels in TNBC are associated with a poor prognosis, a dedifferentiated tumour phenotype, and a reduction in response to thymidylate-pathway-targeting therapies [110,111,112].
3.3. Protein-Tyrosine Kinase 6 (PTK6)
Protein-tyrosine kinase 6 (PTK6) is a non-receptor tyrosine kinase that is a member of the Tyr protein kinase family's BRK/PTK6/SIK subfamily [113,114] (UniProt: Q13882). It is also referred to as breast tumour kinase (BRK) [113,114] (UniProt: Q13882). This enzyme regulates a number of signalling pathways that control the development of tumours as well as the differentiation and survival of healthy epithelial tissues [114,115]. PTK6's biological impacts are extremely context-specific and differ based on the type of cell and its subcellular location. For example, it may stimulate apoptosis or differentiation when it is located in the nucleus, but it more frequently promotes oncogenic signalling when it is located in the cytoplasm [115,116]. The RNA-binding proteins SAM68, SLM1, SLM2, and PSF; transcription factors STAT3 and STAT5; and signalling molecules p190RhoGAP, paxillin, BTK/AKT, and STAP2 are among the many substrates of PTK6 that have been found [116,117]. PTK6 has been demonstrated to enhance metastasis and tumor cells survival in TNBC. It is increased in response to low oxygen (hypoxia) and glucocorticoid-induced stress through an HIF/GR/PELP1 signalling network [118]. Furthermore, PTK6 suppression in TNBC cell lines decreases migration and increases E-cadherin levels by stimulating the proteasomal degradation of the EMT driver SNAIL [119]. Furthermore, RhoA and the Aryl hydrocarbon Receptor (AhR) seem to be activated by the SH2 domain of PTK6 in TNBC, which drives both cell mobility and paclitaxel resistance [114]. Clinically, TNBC patients with high PTK6 expression levels have decreased survival rates over time and lymph-node metastasis, indicating PTK6 as a possible diagnostic marker and therapeutic target [119,120].
3.4. Mitochondrial DNA Topoisomerase I (TOP1MT)
TOP1MT (mitochondrial DNA topoisomerase I), a kind of IB topoisomerase, reduces supercoiling and twisting contraction in mtDNA by partially cleaving and reassembling one strand of the DNA double helix (UniProt: Q969P6) [121]. Its catalytic tyrosine creates a covalent DNA–(3′-phosphotyrosyl) intermediate, facilitating strand rotation and potential religation despite a requirement for ATP (UniProt: Q969P6) [121]. Divalent metal ions like Ca2+ or Mg2+ are necessary for this enzymatic process (UniProt: Q969P6) [121]. TOP1MT is widely expressed, but its RNA quantities are especially significant in tissues that require a lot of energy, like the heart, brain, skeletal muscle, and foetal liver (UniProt: Q969P6) [121]. Because its loss alters the topology of mtDNA and reduces the expression of mitochondrial genes, TOP1MT is essential for the maintenance of mitochondrial DNA [122]. TOP1MT dysregulation has been connected to tumour formation; either high expression or inadequate expression could contribute to the development of cancer, possibly via impacts on DNA damage, oxidative stress, and mitochondrial function [123]. Furthermore, in some tumours, such as liver hepatocellular carcinoma and renal carcinomas, a high TOP1MT level is linked to a poor prognosis [123]. Decreased mtDNA content, compromised respiration in the mitochondria, and a change in metabolic rate towards glycolysis are common characteristics of severe TNBC tumours [124]. While this data does not appear to directly link to TOP1MT, it suggests that mitochondrial–maintenance enzymes like TOP1MT might have a significant part in TNBC pathophysiology.
3.5. Smoothened Receptor (SMO)
The SMOothened receptor (SMO) is a multi-pass cell-surface G-protein-coupled receptor that mediates the Hedgehog signalling pathway, regulating cell fate, proliferation and tissue patterning. The Hedgehog (Hh) pathway is frequently dysregulated in TNBC, with overexpression of SHH, PTCH1, SMO, and GLI genes correlating with higher grade and worse prognosis [125]. In TNBC, Hh signaling promotes proliferation, invasion, and especially CSC maintenance, contributing to chemoresistance [125]. Importantly, SMO can mediate both autocrine and paracrine Hh activation: TNBC cells often secrete Hh ligands, whereas SMO-positive stromal fibroblasts respond by remodelling the TME and supporting CSC niches [126]. SMO inhibition in preclinical TNBC models reduces CSC markers, suppresses invasion, and sensitizes tumors to taxanes [126]. Clinically, the SMO inhibitor sonidegib combined with docetaxel demonstrated preliminary benefit in the EDALINE phase I trial, with a subset of metastatic TNBC patients achieving clinical responses [126]. However, some basal-like/TNBC subtypes activate GLI transcription factors independently of SMO — for example via FOXC1 — suggesting intrinsic resistance to SMO-targeted therapy [127]. Despite these limitations, SMO remains a promising target in TNBC subsets characterized by ligand-dependent, stromal-driven Hh activation, supporting further development of biomarker-guided SMO-based combination therapies [126,127].
3.6. Colony-Stimulating Factor 1receptor (CSF1R)
CSF1R is a receptor tyrosine kinase for colony-stimulating factor 1 and interleukin-34, playing a central role in the survival, proliferation and differentiation of mononuclear phagocytes, and linking tumour cells to the immune/mesenchymal microenvironment. The CSF1–CSF1R axis is a key driver of the immunosuppressive tumor microenvironment in TNBC, where high CSF1 expression by tumor cells recruits and polarizes tumor-associated macrophages (TAMs) toward a pro-tumorigenic M2-like phenotype [128]. These TAMs promote invasion, angiogenesis, CSC maintenance, and resistance to therapy, making CSF1R a central regulator of TNBC aggressiveness [129]. Elevated CSF1R expression in breast cancer tissues correlates with poor prognosis, increased TAM infiltration, and an immunosuppressive microenvironment [130]. In preclinical TNBC models, pharmacologic CSF1R inhibition reduces TAM abundance, suppresses tumor growth and metastasis, and enhances chemotherapy efficacy [128]. Additional studies indicate that CSF1R signalling extends beyond macrophages, influencing stromal and myeloid populations that support tumor progression [131]. Given these findings, CSF1R blockade—alone or in combination with chemotherapy or immunotherapy—represents a promising strategy for targeting the TNBC microenvironment [132]. However, because CSF1R is essential for normal myeloid homeostasis, therapeutic benefit will likely require biomarker-guided patient selection and rational combination approaches [128,130].
3.7. Ephrin Type B Receptor 3 (EPHB3)
EPHB3 is a member of the Eph receptor family of receptor tyrosine kinases that binds ephrin-B ligands in a contact-dependent manner, modulating cell–cell adhesion, migration, angiogenesis and developmental cell positioning. It shows consistent overexpression in TNBC across multiple transcriptomic datasets, including TCGA [133] and METABRIC [134,135], where its expression is enriched in basal-like subtypes and associated with proliferative and invasive signatures. Despite this reproducible omics-level signal, no functional studies have yet defined the role of EPHB3 in TNBC, distinguishing it from other Eph receptors (such as EPHB2 or EPHB6) that have already established mechanistic links to breast cancer progression. Though EPHB3 looks like a TNBC-specific candidate whose biological significance remains to be elucidated, it has been functionally implicated in several malignancies outside TNBC, with strongly context-dependent roles. In NSCLC, EPHB3 is overexpressed and promotes tumor cell growth, survival, migration and metastasis in a largely kinase-independent manner [136]. In contrast, a subsequent study in NSCLC showed that forced activation of EPHB3 kinase suppresses cell migration and metastatic seeding via a PP2A/RACK1/Akt signalling complex, revealing a tumour-suppressive pathway when ligand-induced signalling is restored [137]. In papillary thyroid cancer, EPHB3 acts as a tumour promoter, enhancing in vitro migration and in vivo metastasis through a kinase-dependent Vav2–Rho GTPase axis [138]. In colorectal cancer, several lines of evidence instead support a tumour-suppressor role: over-expression of EPHB3 in HT-29 colon cancer cells strengthens cell–cell contacts and suppresses tumour growth [139], and EPHB3 is frequently silenced in human colorectal cancer through “decommissioning” of a transcriptional enhancer [140]. Clinicopathological analyses further show that EPHB3 expression tends to be higher in early colorectal lesions and reduced in advanced tumours, with loss of EPHB3 correlating with poorer prognosis [141]. Recent comprehensive reviews of the Eph/ephrin system in cancer highlight EPHB3 as a prototypical example of a receptor whose activity can be either oncogenic or tumour-suppressive depending on ligand availability, phosphorylation state and tissue context [142].
3.8. Tribbles Pseudokinase 1(TRIB1)
TRIB1 is a pseudokinase/adaptor protein that engages with ubiquitin-ligases and signalling modules to regulate MAPK cascades, substrate degradation and cellular responses to stress or differentiation cues. TRIB1, a member of the Tribbles pseudokinase family, has emerged as a regulator of oncogenic pathways relevant to TNBC. TRIB1 is frequently overexpressed in breast cancer, where it promotes tumor progression through modulation of MAPK/ERK and NF-κB signaling [143]. Elevated TRIB1 expression has been associated with poor prognosis and increased tumor aggressiveness in breast cancer cohorts, including basal-like subtypes that overlap with TNBC [143]. Mechanistically, TRIB1 enhances survival and chemoresistance through stabilization of oncogenic proteins and suppression of apoptosis pathways [144]. In macrophages, TRIB1 is required for the differentiation of M2-like tumor-associated macrophages (TAMs) [145], suggesting that TRIB1-positive tumors may foster an immunosuppressive microenvironment—an established hallmark of TNBC. Furthermore, TRIB1 regulates inflammatory cytokine production and interacts with COP1, influencing degradation of transcription factors involved in tumor immune evasion [144]. Together, these findings indicate that TRIB1 contributes to TNBC biology, both at the cell level, by promoting survival and oncogenic signaling, and at the TME level, by supporting TAM-mediated immunosuppression. These dual functions position TRIB1 as a potential prognostic marker and a candidate therapeutic target in TNBC.
3.9. Ladinin-1 (LAD1)
LAD1 (Ladinin-1) is an anchoring-filament protein that resides in the basement-membrane zone, contributing to epithelial–mesenchymal interface integrity and intercellular adhesion. It has recently been implicated in cancer progression through effects on cytoskeletal dynamics and cell motility. Quantitative proteomics identified LAD1 as a filamin-binding regulator of actin remodeling and reported its association with aggressive breast tumors [146]. Beyond breast cancer, LAD1 overexpression has been linked to poor clinical outcomes in multiple malignancies. In lung adenocarcinoma, high LAD1 expression promotes proliferation and migration and correlates with reduced overall survival[147]. In colorectal cancer, LAD1 upregulation is associated with metastatic potential and adverse prognosis, suggesting involvement in EMT and extracellular matrix remodeling [148]. More recently, LAD1 was shown to localize to actin-rich structures at invasive tumor fronts in oral squamous cell carcinoma, reinforcing its role in cytoskeletal reorganization during invasion [149]. Although functional studies of LAD1 in TNBC are currently lacking, its recurrent association with aggressiveness across several cancer types highlights LAD1 as a compelling candidate biomarker and potential mediator of invasion whose role in TNBC warrants focused investigation.

Table 3.
Summary of role and evidence of potential targets derived from omics.
| Protein | Role in Cancer Pathogenesis | Evidence in TNBC / Relevance | References |
|---|---|---|---|
| SMO (Smoothened) |
Aberrant activation of SMO promotes proliferation, invasion, stem-cell-like traits and therapy resistance in various cancers. | SMO (and GLI1) expression correlates with higher grade, node positivity, poorer prognosis. | [125,150] |
| CSF1R (Colony-stimulating factor 1 receptor) |
Promotes tumour-associated macrophage (TAM) support, immune evasion, angiogenesis and metastatic spread. | High CSF1R expression has been associated with inferior survival, and preclinical models show CSF1R inhibition reduces brain metastasis in TNBC. | [151] |
| EPHB3 (Ephrin type-B receptor 3) |
Dysregulation can promote invasion/metastasis in cancers. | In TNBC, integrative genomic analyses have flagged EPHB3 as a hyperactivated gene and a potential target. | [139] |
| TRIB1 (Tribbles pseudokinase 1) |
Over-expression correlates with poor prognosis; promotes resistance to therapy. | In breast cancer, elevated TRIB1 correlates with worse survival. | [152] |
| LAD1 (Ladinin-1) | Over-expression has been associated with more aggressive phenotypes in various cancers (breast, lung). | Higher LAD1 links to increased migration/metastatic potential; genomics in TNBC flag LAD1 as potential target. | [148,153] |
4. Metabolic Vulnerabilities in TNBC
Metabolic plasticity is a powerful tool for cancer cells to survive in extremely stressing conditions. Cancer cells can adapt to environmental stress with different strategies. According to recent studies in TNBC the most frequent metabolic switches involve (i) enhanced glycolysis, (ii) enhanced oxidative phosphorylation, and (iii) fatty acid oxidation. Targeting proteins involved in the regulation of such relevant metabolic salvage pathways can offer good therapeutic approaches in difficult to treat and heterogenous cancers like TNBC. As proved by Warburg and colleagues in 1927 [154] cancer cells rely on improved glycolysis even in normoxic conditions to increase the energetic metabolism required for fast proliferation. According to several reports, TNBC cells show increased dependency on the glycolytic flux to proliferate and metastasize. This metabolic rewiring, driven prevalently by TP53 or Kras mutations, myc amplification and, in general, dysregulated pro-proliferative pathways, causes increased expression of glycolytic enzymes (i.e., lactate dehydrogenase, LDH) and glucose transporters (i.e., GLUT).
Glucose transporter 1 (GLUT-1) is central in supporting this metabolic alteration, indeed, GLUT-1 alterations are frequent in cancers. In BC, high GLUT-1 expression correlates with increased proliferative activity, high histologic grade and drug resistance, and is associated prevalently with basal-like carcinoma (ER-, PR-, HER-), the more represented subtype of TNBC [155]. In pre-clinical models of TNBC, inhibition of GLUT-1 using either small molecules like STF-31, WZB-117 or BAY-876, or shRNA, showed a marked anti-proliferative effect, supporting the possibility to target GLUT-1 for TNBC therapy [156,157,158,159]. Overexpression of glycolytic enzymes such as hexokinase 2 (HK2) and Lactate Dehydrogenase (LDH) promotes tumor growth and survival under hypoxic conditions [160]. HK2, an enzyme which catalyzes the first step of glycolysis, is upregulated in TNBC and its upregulation is associated with enhanced energy production and resistance to pro-apoptotic signaling [161,162]. HK2 is anchored to the mitochondrial voltage-dependent anion channel (VDAC) and this interaction favors energy production and apoptosis escape by coupling glycolysis to ATP production. One possible strategy to target glucose metabolism in TNBC is to disrupt such an interaction to reduce energy availability and successfully trigger pro-apoptotic pathways [163]. In preclinical models, direct targeting of HK2 has been attempted by using 2-deoxy-D-glucose (2-DG), a glucose analog which competitively inhibits HK2, causing ATP depletion and endoplasmic reticulum stress. The results reported by O’Neill et al. [164] have shown that 2-DG reduces viability of TNBC cells and enhances sensitivity to chemotherapeutics such as doxorubicin and paclitaxel. Ganapathy-Kanniappan et al. [165,166] have also showed in vivo marked inhibition of HK2 by using more specific small molecules like 3-bromopyruvate (3-BrPA) and lonidamine in xenograft models [167]. The data obtained showed significant tumor regression but also elevated systemic toxicity. HK2 expression can also be reduced by administering metformin which acts through AMPK pathway activation and activates p53 pro-apoptotic signaling [168].
Another glycolytic enzyme which is overexpressed in TNBC and is relevant to support tumor growth, invasion and immune escape is LDH, which catalyzes the conversion of pyruvate to lactate, regenerating the NAD⁺ required to sustain glycolysis even in hypoxic environments typical of solid tumors. IndeedHIF-1α directly upregulates both HK2 and LDH transcription, enabling TNBC cells to survive and proliferate under oxygen deprivation [169]. Elevated LDH-A isoform expression in TNBC correlates with poor prognosis and enhances invasion and immune evasion, very likely by promoting an acidic tumor microenvironment [170,171,172,173]. Pharmacological inhibition of LDH using small molecules such as FX11 and GNE-140 have shown efficacy in preclinical TNBC models, reducing tumor growth and enhancing cell death [174,175]. Combination strategies integrating glycolytic inhibition with immune checkpoint inhibitors are being investigated to potentiate antitumor immunity and overcome metabolic resistance [176,177].
Glutamine addiction is another critical driver for metabolic plasticity observed in TNBC. Glutamine is the main extracellular source of carbon and nitrogen to fuel the tricarboxylic acid cycle (TCA) but is also involved in nucleotides synthesis and redox homeostasis [ref]. Glutamine transporters such as SNAT2/SLC38A2 and SLC7A5 are often overexpressed in TNBC cells [178,179]. Their blockade using specific inhibitors has been shown to reduce glutamine uptake and suppress tumor growth in in vitro and in vivo systems [180,181,182]. Another hallmark of glutamine addiction in TNBC is the overexpression of glutaminase 1 (GLS1), the enzyme which catalyzes the conversion of glutamine into glutamic acid providing key precursors for the TCA cycle and antioxidant molecules and supporting ATP production [183,184]. Inhibition of GLS using small molecules like telaglenastat has proved effective in preclinical models by reducing the energetic metabolism, cell proliferation and enhancing cancer cells sensitivity to immune checkpoints and standard chemotherapeutic agents [185,186].
Another relevant metabolic change often observed in cancer cells is aberrant lipid metabolism which significantly contributes to cancer cells aggressiveness, metastasization and resistance to therapy [187,188,189]. Also, TNBC cells rely on de novo lipogenesis and fatty acid oxidation to sustain adaptation to nutrient and oxygen stress [190,191]. Overexpression of Fatty Acid SyNthetase (FASN) is a hallmark of TNBC and correlates with poor prognosis and therapeutic response [192,193], thereof, FASN could be a valid target for targeted anti-metabolic TNBC therapy. In vitro inhibition of FASN using small molecules (i.e., TVB-2640 or C75) has been proved effective in reducing cell proliferation, in activating apoptosis and sensitizing TNBC cells to combined therapy [194,195,196].
Fatty Acid Oxidation (FAO) is catalyzed by several enzymes, among them Carnitine Palmitoyltransferase 1A (CPT1A) has a key role as rate-limiting enzyme in mitochondrial FAO. CPT1A is often upregulated in TNBC and its pharmacological inhibition by etomoxir or perhexiline has been attempted in preclinical models of TNBC with good results as for inhibition of cell proliferation and tumor metastasis [197,198,199]. Another route to target lipid metabolism in cancer cells is the inhibition of Sterol Regulatory Element-Binding Proteins (SREBPs) which transcriptionally regulate lipid biosynthesis and are up-regulated in TNBC [200]. Presently, there are no records of successful targeting of SREBPs in TNBC in vitro or in vivo models.
All in all, targeting metabolism in TNBC is a promising route for improved therapy, but systemic toxicity and off-target effect limit the use of this approach into the clinics, which requires further effort in improving targeting selectivity and localization. Moreover, as proved by Cai et al. subsets of TNBC also exhibit metabolic plasticity [201], suggesting that combination strategies targeting multiple metabolic pathways may be required to achieve durable therapeutic responses. Thereof, beside targeted therapy, robust biomarkers are needed to guide patients’ stratification and improve personalized and targeting selection to optimize the risk/benefit ratio.
Main metabolic pathways altered in TNBC are summarized in Table 4.
5. Tumor Microenvironment and Immune-Modulating Factors
The Tumor microenvironment (TME) is a complex ecosystem composed of epithelial cells, adipocytes, fibroblasts, immune cells, and soluble factors that collectively influence tumor progression and therapeutic response. In TNBC, the immune composition of the TME plays a decisive role in shaping disease behavior. TNBCs can be broadly divided into “hot” and “cold” tumors: hot tumors exhibit abundant immune infiltration and active antitumor immunity, whereas cold tumors are characterized by poor T-cell infiltration, defective antigen presentation, and enrichment in immunosuppressive cell types such as TAMs and Myeloid-Derived Suppressor Cells (MDSCs) [203]. These immune-excluded tumors typically show resistance to Immune Checkpoint Inhibitors (ICIs), although therapeutic interventions may reprogram the immune context and promote conversion toward more inflamed phenotypes [204]. Recent studies have further stratified TNBC into four Tumor Immune MicroEnvironment (TIME) subtypes: ID (Immune-Desert), MR (Margin-Restricted), SR (Stroma-Restricted), and FI (Fully-Inflamed), defined by distinct spatial patterns of CD8⁺ T-cell localization [205,206]. ID and MR tumors, both poorly infiltrated, display fibrosis and B7-H4 expression, correlating with poor prognosis. SR tumors show CD8⁺ T-cell accumulation restricted to the stroma, with IL-17⁺ cells, neutrophils, and stromal PD-L1/IDO1 expression creating an immunosuppressive environment. In contrast, FI tumors exhibit widespread infiltration of activated CD8⁺GzmB⁺ T cells, strong type I interferon signatures, and high checkpoint expression (PD-L1, LAG-3, TIM-3, TIGIT, CTLA-4), features that are associated with improved prognosis and sensitivity to immunotherapy [206].
5.1. Pharmacological Targeting of EMT in TNBC
The process known as epithelial to mesenchymal transition (EMT) endows epithelial cells with enhanced motility and invasive potential. Although this phenomenon is common across various malignancies, in TNBC EMT is particularly promoted by the activation of the NF-κB signaling pathway [207]. This transition is frequently associated with therapeutic resistance and metastatic competence, largely due to the regulation of transcription factors involved in oxidative stress responses and the production of Reactive Oxygen Species (ROS) [208]. Several genes and molecular pathways have been identified as central regulators of EMT and thus represent promising therapeutic targets for the development of personalized strategies in TNBC [209]. Among these, inhibition of the receptor tyrosine kinase AXL has been shown to reduce cell migration and invasive behavior in mesenchymal TNBC cells, indicating that targeting AXL with R428 treatment may help regulate cell polarity [210]. Similarly, the Src/ABL inhibitor dasatinib induces epithelial polarization, sensitizing TNBC cells to paclitaxel, a conventional chemotherapeutical drug [211]. At the epigenetic level, pro-EMT and hypoxia-responsive genes are repressed using Bromodomain and Extra-Terminal (BET) inhibitors, thereby limiting tumor progression and metastatic dissemination [212]. Moreover, epigenetic modification induced by histone deacetylase can be another interesting target: indeed, its inhibition by panobinostat (LBH589) in combination with salinomycin, an antibiotic effective against breast cancer stem cells, downregulate mesenchymal markers, leading to tumor regression in xenograft models [213]. More recently, synergistic effects were highlighted also with napabucasin, a STAT3 inhibitor, in combination with paclitaxel; in particular, napabucasin impairs mitochondrial function and cell growth in paclitaxel-resistant TNBC models [214]. Furthermore, suppression of EMT transcription factors such as SLUG and the inhibition of its interaction with LSD1 may serve as an adjuvant therapy [215]; more recently, a phase 1 proof of concept study demonstrated antitumor activity and the suppression of the overexpressed Lysine-Specific Demethylase-1 (LSD1) EMT marker using phenelzine, an LSD1 inhibitor, in combination with nab-paclitaxel [216]. Collectively, these findings highlight the therapeutic relevance of interfering with key EMT-related pathways, including NF-κB, STAT3, and epigenetic regulators, as a promising strategy to overcome phenotypic plasticity, metastasis, and drug resistance in TNBC.
5.2. Cancer-Associated Adipocytes as Mediators of Immune Evasion and Metabolic Crosstalk
Cancer-Associated Adipocytes (CAAs) constitute a significant number of adipocytes in the TME. They produce several inflammatory factors, among which IL-1β, IL-6, IL-8, TNF-α, CCL2, leptin and free fatty acids [217]. CAAs are distinguished from mature adipocytes by their more elongated morphology, which tends to make them resemble fibroblasts, and by their irregular shape, their smaller size and the presence of small lipid droplets [218]. It has been observed that the production of IL-8 by CAAs causes a remodeling of the TME by suppressing CD4+ T and CD8+ T immune cell infiltration, but also by upregulating PD-L1 expression in TNBC. In this case, a promising therapeutic strategy is to target the IL-8 production pathway in association with immunotherapy by blocking the PD-1 pathway [219]. Another immunosuppressive strategy is the production by CAAs of CCL2, a cytokine that recalls monocytes and macrophages in the tissue, differentiating them into Myeloid-Derived Suppressor Cells (MDSCs) and M2 macrophages. A recently developed strategy to reverse this behavior exploits CCL2-targeted lipid-protamine-DNA nanoparticles, capable of suppressing CAAs, which increase T cell infiltration and decrease the population of immunosuppressive M2 macrophages and MDSCs [220]. The role of adipocytes adjacent to the tumor, however, is not yet fully explored; it has only recently been observed that CAAs and tumor cells can create gap junctions, through which an exchange of metabolites becomes possible, favoring tumor support and development [221]. CAAs can therefore not only release free fatty acids into the TME, but can also activate lipolysis processes to generate metabolites to be exchanged directly through gap junctions established with tumor cells. This discovery paves the way for the development of molecules and drugs that can re-modulate the expression of cell adhesion molecules. A key mediator discovered in the regulation of metabolic interactions between CAAs and tumor cells is ANGioPoieTin-Like 4 (ANGPTL4), a factor expressed on TNBC cells, which stimulates adipocyte-driven glycolysis and metastasis [222]. A new treatment technology that has been under development is the transplantation of generated adipocytes placed alongside cancer cells or xenografts, capable of upregulating UnCoupling Protein 1 (UCP1) with consequent suppression of tumor growth [223].
5.3. Cancer-Associated Fibroblasts as Drivers of Fibrosis, Hypoxia and Drug Resistance
In TME it is often possible to recognize a cellular component of Cancer-Associated Fibroblasts that are called CAFs. Their origin is not fully elucidated: CAFs might derive from adipocytes or from mesenchymal stem cells [224], but the most highly quoted hypothesis is that they derive from normal fibroblasts. CAFs display a more active phenotype than normal fibroblasts, such as increased proliferation, migration, invasion, tumorigenicity, and chemoresistance [225]. CAFs were associated with infiltration of CD163+ macrophages and lymphatic metastasis and may be potential prognostic predictors of TNBC [224]. A peculiar characteristic of CAFs associated with TNBC is the increased deposition of collagen in the extracellular matrix, which is associated with a higher risk of developing metastases. This mechanism is mediated by TGF-β; in fact, by using one of its antagonists, pirfenidone, a reduction in the proliferation and production of collagen is obtained in in vitro models. Moreover, reduced tumor growth and lung metastasis formation were observed in in vivo models with a synergistic combination of pirfenidone with doxorubicin [226]. Using xenograft models, attempts have also been made to use specific inhibitors for Fibroblast Activation Protein (FAP), a membrane protein expressed in CAFs, which has a gelatinolytic activity; promising anti-tumor results are obtained by inhibiting this protein [227]. One of the factors that induces resistance to therapies is hypoxia, and CAFs also have a role in the regulation of this pathway in TNBC: in particular, CAFs present in the hypoxic portion secrete very high levels of Colony-Stimulating Factor 3 (CSF3), a factor that activates the invasive behavior of TNBC cells, through PhosphoGlucoMutase 2-Like 1 (PGM2L1) [228]. This discovery highlights a new potential target for developing therapies especially in relapsing cases, with residual disease induced by hypoxic resistance. Extremely interesting new technologies for developing therapeutic approaches rely on formulations based on nanoparticles co-modified with anisamide, drug carrier, and CAF cell membranes, to load tetrandrine, a calcium channel blocker, as a CAF nano-regulator, which can precisely target and modulate CAFs [229].
5.4. Targeting Immune Cells in TME
TNBC is the BC subtype most suitable for immunotherapies; indeed, its TME is characterized by a high number of macrophages and cytotoxic T-cells, compared to other breast cancer subtypes [230]. Furthermore, recent studies have demonstrated the high heterogeneity of TNBC dividing this class into five immune subtypes based on four distinct expression signatures, (i) T/B-cell/IFN High, (ii) IFN/ Class Switch Recombination (CSR) High, (iii) CSR High, (iv) TGF-b High, and (v) Immune Low, derived from four core co-expression modules that capture distinct immune components and signaling programs (T/B-cell, IFN, TGF-b, and CSR) [231]. A highly expressed marker in TNBC is PD-L1: for this reason, PD-L1 antibodies, as monotherapy or a part of combined therapies, have been applied in multiple clinical trials, confirming that the combined therapy yields synergistic effects. ICIs Atezolizumab (a PD-L1 antibody) combined with paclitaxel has been approved as therapy for PD-L1–positive TNBC [232]. However, the rationale of the combination and successful application of anti–PD-L1 therapy relies on a comprehensive understanding of PD-L1 biology in tumor cells. It has been demonstrated that anti-VEGFR2 therapy is necessary to make TNBC cells more sensitive to ICIs; the combination of apatinib with camrelizumab and chemotherapy promote CD8+ T cell infiltration and activation within the TME, alongside antiangiogenic-induced PD-L1 upregulation [233]. Although ICIs have proven to be a very promising strategy, the relapse rate of TNBC remains high; for this reason, technologies have been developed that allow the transfer of engineered T cells such as chimeric antigen receptor T (CAR-T) cells. To make this technique effective, it is necessary to find antigens that have a higher level of expression in the tumor than in healthy tissues; however, it has been seen that CAR-T cells have a modest efficacy in solid tumors due to high cellular heterogeneity. For this purpose, it has been proposed to develop CAR-T cells capable of recognizing multiple markers simultaneously; optimizing CAR-T cells to recognize the CD276 and CSPG4 markers, encouraging results were obtained on TNBC Patient-Derived Xenograft (PDX) models [234]. Another interesting approach to increase the effectiveness of CAR-T treatment is the combination with radiotherapy: exposure to radiation favors the infiltration of T and NK cells, but also the expression of ICAM-1 in TNBC cells. EGFR-targeted CAR-T therapy combined with radiotherapy inhibits tumor progression and prolongs survival [235]. A similar technology is also being developed for CAR-M (where M stands for Marophages): currently, there are very encouraging data for HER2+ tumors with limited sensitivity to anti-PD1 monotherapy [236], and this seems to be an interesting path to explore and test also for TNBC. The immune system, however, can recognize cancer neoantigens that are mutant proteins/amino acid sequences. For this reason, neoantigen vaccines, that can induce neoantigen-specific CD8 and CD4 T cell responses and antitumor immunity, as well as neoantigen DNA vaccines, have been developed. DNA vaccination is a direct administration of recombinant DNA, and, in a phase 1 clinical trial, it was demonstrated that DNA vaccines are safe and well-tolerated in patients with persistent TNBC following neoadjuvant chemotherapy, with no significant adverse events. The neoantigen DNA vaccines were able to induce neoantigen-specific immune responses, with evidence of improved RFS [237].
5.5. Soluble Factors Released in TME as Modulator of TNBC Target Therapy
Cytokines and chemokines are among the main soluble factors present in the TME, and they are fundamental players in the modulation of the immune response. However, immune-modulation is not exclusive of these factors, and also proteins of the extracellular matrix, metabolites and exosomes can be potential therapeutic targets. Starting from transcriptomic data, it has been observed that, in TNBC, there is an upregulation of genes coding for the collagen family, while those of the integrin family are downregulated [238]. In matrix remodeling, metalloproteinases certainly have a decisive role: indeed, Matric Metalloprotease-14 (MMP14) and DDR2 have been proposed as diagnostic markers for metastatic TNBC [239]. An interesting new target to define the metastatic capacity of TNBC is O-glycosylation: different highly O-glycosylated protein coding genes, such as mmp9, ecm1, and ank2, were upregulated in a mouse model expressing the sugar Tn antigen (GalNAc-O-Thr/Ser), an antigen expressed in many adenocarcinomas and absent in healthy tissues. Incomplete O-glycosylation leads to the expression of an altered form of the Tn antigen, which might regulate their activity or interaction with different molecules, promotes cancer development and immunoregulation. The role of O-glycans in the identified molecules remains to be elucidated [240]. Therefore, soluble factors cannot currently be considered effective therapeutic targets but could rather be used as diagnostic or prognostic markers to monitor the progression of the disease. In this context, extracellular vesicles are also considered a promising diagnostic biomarker and a novel drug delivery system among the prospects for immunotherapy in TNBC [241].
6. Targeted Radiotherapy in TNBC
Current guidelines recommend the use of radiotherapy following surgical resection, with the aim of eliminating residual tumor cells and reducing the risk of recurrence, while minimizing toxicity as much as possible by the adoption of the optimal treatment plan [242]. Current studies are also developing new approaches to optimize the radiotherapy outcome, using radiosensitizer-enhancers and nano-radiotherapy. Radiosensitizer-enhanced radiotherapy is an approach that uses drugs capable of making tumor cells more sensitive to ionizing radiation [6]. With this perspective, nanomaterials such as AGuIX nanoparticles, polysiloxane nanoparticles containing the metal gadolinium (Gd) as a high atomic number element, are also being developed. In particular, it has been demonstrated that AGuIX nanoparticles may be used as effective radiosensitizers in TNBC, promoting not just DNA damage and apoptosis, but also ferroptosis by the NRF2-GSH-GPX4-dependent pathway after irradiation [243]. In an attempt to make these applications as direct as possible on molecular targets, a recent in vitro study has demonstrated that targeting Elongin B in TNBC holds great promise for improving radiotherapy outcomes: Elongin B role has been discovered to be pivotal in regulating mitochondrial function, via modulating mtDNA expression and activities of respiratory chain complexes. However, specific inhibitors for Elongin B are not yet known [244]. Gemcitabine also has a sensitizer effect; to make the treatment more effective, the drug has been combined with a radionuclide in 131I-labelled polydopamine encapsulated gold nanoparticles within a hydrogel formed from oxidized glucan and chitosan hydrochloride [245].
In the context of developing radiotherapy approaches that are directly targeted to specific molecular determinants, applications in TNBC remain extremely limited. To date, one of the few examples reported in the literature is the study by Sankaranarayanan et al. [246], which investigated a theranostic strategy in a TNBC xenograft mouse model through the radiolabeling of a close derivative of the PARP inhibitor olaparib (PARPi-01) with the Auger electron emitters 123/125I. Auger electron emitters release cascades of low-energy electrons upon radioactive decay, inducing highly localized DNA damage. Owing to the nuclear localization of PARP1, PARP inhibitors represent particularly suitable backbone molecules for radiolabeling with Auger emitters. Among these, 125I is one of the most efficient Auger emitters, capable of releasing up to 23 Auger electrons per decay, and is commercially available, making it a promising candidate for highly localized, molecularly targeted radiotherapy approaches in TNBC.
Overall, it is clear that a multimodal approach, which attacks the tumor from multiple fronts, is the most promising strategy, and targeted radiotherapy approaches deserve dedicated investigations also for TNBC treatment, especially with the goal of personalizing therapy as much as possible, to minimize the risk of recurrence and therapy-related side effects.
Funding
This work was co-funded by the IMAGEOMICS - PIANOFORTE project. The PIANOFORTE partnership has received funding from the European Union’s “EURATOM” research and innovation program under the 101061037 grant agreement.
Acknowledgments
This research is supported by: “Associazione Gian Franco Lupo—Un sorriso alla vita—ONLUS”. During the preparation of this manuscript/study, the author(s) used Elicit search engine for the purposes of searching research papers for each subsection of the Review, and ChatGPT to summarize data and produce tables. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
References
- Xiong, X.; Zheng, L.W.; Ding, Y.; Chen, Y.F.; Cai, Y.W.; Wang, L.P.; Huang, L.; Liu, C.C.; Shao, Z.M.; Yu, K. Da Breast Cancer: Pathogenesis and Treatments. Signal Transduct. Target. Ther. 2025, 10. [Google Scholar]
- Derakhshan, F.; Reis-Filho, J.S. Pathogenesis of Triple-Negative Breast Cancer. Annu. Rev. Pathol. Mech. Dis. 2021, 17, 181–204. [Google Scholar] [CrossRef]
- Almansour, N.M. Triple-Negative Breast Cancer: A Brief Review About Epidemiology, Risk Factors, Signaling Pathways, Treatment and Role of Artificial Intelligence. Front. Mol. Biosci. 2022, 9, 836417. [Google Scholar] [CrossRef]
- Breast Cancer Research Foundation | BCRF. Available online: https://www.bcrf.org/ (accessed on 8 January 2026).
- Yin, L.; Duan, J.J.; Bian, X.W.; Yu, S.C. Triple-Negative Breast Cancer Molecular Subtyping and Treatment Progress. Breast Cancer Res. 2020, 22. [Google Scholar] [CrossRef]
- Sarlak, S.; Pagès, G.; Luciano, F. Enhancing Radiotherapy Techniques for Triple-Negative Breast Cancer Treatment. Cancer Treat. Rev. 2025, 136. [Google Scholar] [CrossRef] [PubMed]
- Burstein, M.D.; Tsimelzon, A.; Poage, G.M.; Covington, K.R.; Contreras, A.; Fuqua, S.A.W.; Savage, M.I.; Osborne, C.K.; Hilsenbeck, S.G.; Chang, J.C.; et al. Comprehensive Genomic Analysis Identifies Novel Subtypes and Targets of Triple-Negative Breast Cancer. Clin. Cancer Res. 2015, 21, 1688–1698. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Jovanović, B.; Chen, X.; Estrada, M. V.; Johnson, K.N.; Shyr, Y.; Moses, H.L.; Sanders, M.E.; Pietenpol, J.A. Refinement of Triple-Negative Breast Cancer Molecular Subtypes: Implications for Neoadjuvant Chemotherapy Selection. PLoS One 2016, 11. [Google Scholar] [CrossRef] [PubMed]
- Yam, C.; Mani, S.A.; Moulder, S.L. Targeting the Molecular Subtypes of Triple Negative Breast Cancer: Understanding the Diversity to Progress the Field. Oncologist 2017, 22, 1086–1093. [Google Scholar] [CrossRef] [PubMed]
- Weng, L.; Zhou, J.; Guo, S.; Xu, N.; Ma, R. The Molecular Subtyping and Precision Medicine in Triple-Negative Breast Cancer---Based on Fudan TNBC Classification. Cancer Cell Int. 2024, 24, 120. [Google Scholar] [CrossRef]
- Vagia, E.; Mahalingam, D.; Cristofanilli, M. The Landscape of Targeted Therapies in TNBC. Cancers (Basel). 2020, 12. [Google Scholar] [CrossRef]
- Lehmann, B.D.; Jovanović, B.; Chen, X.; Estrada, M. V.; Johnson, K.N.; Shyr, Y.; Moses, H.L.; Sanders, M.E.; Pietenpol, J.A. Refinement of Triple-Negative Breast Cancer Molecular Subtypes: Implications for Neoadjuvant Chemotherapy Selection. PLoS One 2016, 11. [Google Scholar] [CrossRef]
- Anders, C.K.; Abramson, V.; Tan, T.; Dent, R. The Evolution of Triple-Negative Breast Cancer: From Biology to Novel Therapeutics. Am. Soc. Clin. Oncol. Educ. book. Am. Soc. Clin. Oncol. Annu. Meet. 2016, 35, 34–42. [Google Scholar] [CrossRef]
- Zhu, S.; Wu, Y.; Song, B.; Yi, M.; Yan, Y.; Mei, Q.; Wu, K. Recent Advances in Targeted Strategies for Triple-Negative Breast Cancer. J. Hematol. Oncol. 2023, 16. [Google Scholar] [CrossRef]
- Orrantia-Borunda, E.; Anchondo-Nuñez, P.; Acuña-Aguilar, L.E.; Gómez-Valles, F.O.; Ramírez-Valdespino, C.A. Subtypes of Breast Cancer. Breast Cancer 2022, 31–42. [Google Scholar] [CrossRef]
- Won, K.A.; Spruck, C. Triple-negative Breast Cancer Therapy: Current and Future Perspectives. Int. J. Oncol. 2020, 57, 1245–1261. [Google Scholar] [CrossRef]
- Ferrari, P.; Scatena, C.; Ghilli, M.; Bargagna, I.; Lorenzini, G.; Nicolini, A. Molecular Mechanisms, Biomarkers and Emerging Therapies for Chemotherapy Resistant TNBC. Int. J. Mol. Sci. 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhang, H.; Merkher, Y.; Chen, L.; Liu, N.; Leonov, S.; Chen, Y. Recent Advances in Therapeutic Strategies for Triple-Negative Breast Cancer. J. Hematol. Oncol. 2022, 15. [Google Scholar] [CrossRef]
- He, M.Y.; Rancoule, C.; Rehailia-Blanchard, A.; Espenel, S.; Trone, J.C.; Bernichon, E.; Guillaume, E.; Vallard, A.; Magné, N. Radiotherapy in Triple-Negative Breast Cancer: Current Situation and Upcoming Strategies. Crit. Rev. Oncol. Hematol. 2018, 131, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Haque, W.; Verma, V.; Hsiao, K.Y.; Hatch, S.; Arentz, C.; Szeja, S.; Schwartz, M.; Niravath, P.; Bonefas, E.; Miltenburg, D.; et al. Omission of Radiation Therapy Following Breast Conservation in Older (≥70 Years) Women with T1-2N0 Triple-Negative Breast Cancer. Breast J. 2019, 25. [Google Scholar] [CrossRef] [PubMed]
- Abdulkarim, B.S.; Cuartero, J.; Hanson, J.; Deschênes, J.; Lesniak, D.; Sabri, S. Increased Risk of Locoregional Recurrence for Women with T1-2N0 Triple-Negative Breast Cancer Treated with Modified Radical Mastectomy without Adjuvant Radiation Therapy Compared with Breast-Conserving Therapy. J. Clin. Oncol. 2011, 29. [Google Scholar] [CrossRef]
- He, M.Y.; Rancoule, C.; Rehailia-Blanchard, A.; Espenel, S.; Trone, J.C.; Bernichon, E.; Guillaume, E.; Vallard, A.; Magné, N. Radiotherapy in Triple-Negative Breast Cancer: Current Situation and Upcoming Strategies. Crit. Rev. Oncol. Hematol. 2018, 131. [Google Scholar] [CrossRef]
- Liu, Y.; Zou, Y.; Ye, Y.; Chen, Y. Advances in the Understanding of the Pathogenesis of Triple-Negative Breast Cancer. Cancer Med. 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Emara, H.M.; Allam, N.K.; Youness, R.A. A Comprehensive Review on Targeted Therapies for Triple Negative Breast Cancer: An Evidence-Based Treatment Guideline. Discov. Oncol. 2025, 16, 547. [Google Scholar] [CrossRef] [PubMed]
- Zuo, W.-J.; Chen, L.; Shen, Y.; Wang, Z.-H.; Liu, G.-Y.; Yu, K.-D.; Di, G.-H.; Wu, J.; Li, J.-J.; Shao, Z.-M. Rational and Trial Design of FASCINATE-N: A Prospective, Randomized, Precision-Based Umbrella Trial. Ther. Adv. Med. Oncol. 2024, 16, 17588359231225032. [Google Scholar] [CrossRef]
- Home | ClinicalTrials. Gov. Available online: https://clinicaltrials.gov/ (accessed on 7 January 2026).
- Jiang, Y.; Chen, M.; Nie, H.; Yuan, Y. PD-1 and PD-L1 in Cancer Immunotherapy: Clinical Implications and Future Considerations. Hum. Vaccines Immunother. 2019, 15, 1111–1122. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.; Kang, K.; Chen, P.; Zeng, Z.; Li, G.; Xiong, W.; Yi, M.; Xiang, B. Regulatory Mechanisms of PD-1/PD-L1 in Cancers. Mol. Cancer 2024, 23. [Google Scholar] [CrossRef]
- Heater, N.K.; Warrior, S.; Lu, J. Current and Future Immunotherapy for Breast Cancer. J. Hematol. Oncol. 2024, 17. [Google Scholar] [CrossRef]
- Naing, A.; Gainor, J.F.; Gelderblom, H.; Forde, P.M.; Butler, M.O.; Lin, C.C.; Sharma, S.; Ochoa De Olza, M.; Varga, A.; Taylor, M.; et al. A First-in-Human Phase 1 Dose Escalation Study of Spartalizumab (PDR001), an Anti-PD-1 Antibody, in Patients with Advanced Solid Tumors. J. Immunother. Cancer 2020, 8. [Google Scholar] [CrossRef]
- Bian, L.; Zhang, H.; Wang, T.; Zhang, S.; Song, H.; Xu, M.; Yao, S.; Jiang, Z. JS001, an Anti-PD-1 MAb for Advanced Triple Negative Breast Cancer Patients after Multi-Line Systemic Therapy in a Phase I Trial. Ann. Transl. Med. 2019, 7, 435–435. [Google Scholar] [CrossRef]
- Kwok, G.; Yau, T.C.C.; Chiu, J.W.; Tse, E.; Kwong, Y.L. Pembrolizumab (Keytruda). Hum. Vaccines Immunother. 2016, 12, 2777–2789. [Google Scholar] [CrossRef]
- Arru, C.; De Miglio, M.R.; Cossu, A.; Muroni, M.R.; Carru, C.; Zinellu, A.; Paliogiannis, P. Durvalumab Plus Tremelimumab in Solid Tumors: A Systematic Review. Adv. Ther. 2021, 38, 3674–3693. [Google Scholar] [CrossRef]
- Schmid, P.; Oliveira, M.; O’Shaughnessy, J.; Cristofanilli, M.; Graff, S.L.; Im, S.-A.; Loi, S.; Saji, S.; Wang, S.; Cescon, D.W.; et al. TROPION-Breast05: A Randomized Phase III Study of Dato-DXd with or without Durvalumab versus Chemotherapy plus Pembrolizumab in Patients with PD-L1-High Locally Recurrent Inoperable or Metastatic Triple-Negative Breast Cancer. Ther. Adv. Med. Oncol. 2025, 17, 17588359251327992. [Google Scholar] [CrossRef]
- Collins, J.M.; Gulley, J.L. Product Review: Avelumab, an Anti-PD-L1 Antibody. Hum. Vaccines Immunother. 2019, 15, 891–908. [Google Scholar] [CrossRef]
- Pal, S.K.; Loriot, Y.; Necchi, A.; Singh, P.; Castellano, D.; Pagliaro, L.; Suarez, C.; McGregor, B.A.; Vaishampayan, U.N.; Hauke, R.J.; et al. COSMIC-021 Phase Ib Study of Cabozantinib Plus Atezolizumab: Results from the Locally Advanced or Metastatic Urothelial Carcinoma Cohorts. J. Clin. Oncol. 2025, 43, 1650–1662. [Google Scholar] [CrossRef]
- Li, D.; Loriot, Y.; Burgoyne, A.M.; Cleary, J.M.; Santoro, A.; Lin, D.; Aix, S.P.; Garrido-Laguna, I.; Sudhagoni, R.; Guo, X.; et al. Cabozantinib plus Atezolizumab in Previously Untreated Advanced Hepatocellular Carcinoma and Previously Treated Gastric Cancer and Gastroesophageal Junction Adenocarcinoma: Results from Two Expansion Cohorts of a Multicentre, Open-Label, Phase 1b Trial (…. EClinicalMedicine 2024, 67, 102376. [Google Scholar] [CrossRef]
- Pal, S.K.; McGregor, B.; Suárez, C.; Tsao, C.K.; Kelly, W.; Vaishampayan, U.; Pagliaro, L.; Maughan, B.L.; Loriot, Y.; Castellano, D.; et al. Cabozantinib in Combination With Atezolizumab for Advanced Renal Cell Carcinoma: Results From the COSMIC-021 Study. J. Clin. Oncol. 2021, 39, 3725–3736. [Google Scholar] [CrossRef] [PubMed]
- Barchiesi, G.; Roberto, M.; Verrico, M.; Vici, P.; Tomao, S.; Tomao, F. Emerging Role of PARP Inhibitors in Metastatic Triple Negative Breast Cancer. Current Scenario and Future Perspectives. Front. Oncol. 2021, 11, 769280. [Google Scholar] [CrossRef]
- Liu, X.; Wu, K.; Zheng, D.; Luo, C.; Fan, Y.; Zhong, X.; Zheng, H. Efficacy and Safety of PARP Inhibitors in Advanced or Metastatic Triple-Negative Breast Cancer: A Systematic Review and Meta-Analysis. Front. Oncol. 2021, 11, 742139. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef] [PubMed]
- Kummar, S.; Wade, J.L.; Oza, A.M.; Sullivan, D.; Chen, A.P.; Gandara, D.R.; Ji, J.; Kinders, R.J.; Wang, L.; Allen, D.; et al. Randomized Phase II Trial of Cyclophosphamide and the Oral Poly (ADP-Ribose) Polymerase Inhibitor Veliparib in Patients with Recurrent, Advanced Triple-Negative Breast Cancer. Invest. New Drugs 2016, 34, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Kummar, S.; Ji, J.; Morgan, R.; Lenz, H.J.; Puhalla, S.L.; Belani, C.P.; Gandara, D.R.; Allen, D.; Kiesel, B.; Beumer, J.H.; et al. A Phase I Study of Veliparib in Combination with Metronomic Cyclophosphamide in Adults with Refractory Solid Tumors and Lymphomas. Clin. Cancer Res. 2012, 18, 1726–1734. [Google Scholar] [CrossRef]
- Vinayak, S.; Tolaney, S.M.; Schwartzberg, L.; Mita, M.; McCann, G.; Tan, A.R.; Wahner-Hendrickson, A.E.; Forero, A.; Anders, C.; Wulf, G.M.; et al. Open-Label Clinical Trial of Niraparib Combined with Pembrolizumab for Treatment of Advanced or Metastatic Triple-Negative Breast Cancer. JAMA Oncol. 2019, 5, 1132–1140. [Google Scholar] [CrossRef]
- Tan, T.J.; Sammons, S.; Im, Y.H.; She, L.; Mundy, K.; Bigelow, R.; Traina, T.A.; Anders, C.; Yeong, J.; Renzulli, E.; et al. Phase II DORA Study of Olaparib with or without Durvalumab as a Chemotherapy-Free Maintenance Strategy in Platinum-Pretreated Advanced Triple-Negative Breast Cancer. Clin. Cancer Res. 2024, 30, 1240–1247. [Google Scholar] [CrossRef]
- Gelmon, K.A.; Tischkowitz, M.; Mackay, H.; Swenerton, K.; Robidoux, A.; Tonkin, K.; Hirte, H.; Huntsman, D.; Clemons, M.; Gilks, B.; et al. Olaparib in Patients with Recurrent High-Grade Serous or Poorly Differentiated Ovarian Carcinoma or Triple-Negative Breast Cancer: A Phase 2, Multicentre, Open-Label, Non-Randomised Study. Lancet Oncol. 2011, 12, 852–861. [Google Scholar] [CrossRef] [PubMed]
- Gruber, J.J.; Afghahi, A.; Timms, K.; DeWees, A.; Gross, W.; Aushev, V.N.; Wu, H.T.; Balcioglu, M.; Sethi, H.; Scott, D.; et al. A Phase II Study of Talazoparib Monotherapy in Patients with Wild-Type BRCA1 and BRCA2 with a Mutation in Other Homologous Recombination Genes. Nat. Cancer 2022, 3, 1181–1191. [Google Scholar] [CrossRef]
- Kalra, M.; Tong, Y.; Jones, D.R.; Walsh, T.; Danso, M.A.; Ma, C.X.; Silverman, P.; King, M.-C.; Badve, S.S.; Perkins, S.M.; et al. Cisplatin +/- Rucaparib after Preoperative Chemotherapy in Patients with Triple-Negative or BRCA Mutated Breast Cancer. NPJ breast cancer 2021, 7, 29. [Google Scholar] [CrossRef]
- Stradella, A.; Johnson, M.; Goel, S.; Park, H.; Lakhani, N.; Arkenau, H.T.; Galsky, M.D.; Calvo, E.; Baz, V.; Moreno, V.; et al. Phase 1b Study to Assess the Safety, Tolerability, and Clinical Activity of Pamiparib in Combination with Temozolomide in Patients with Locally Advanced or Metastatic Solid Tumors. Cancer Med. 2024, 13. [Google Scholar] [CrossRef]
- Pasquetto, M.V.; Vecchia, L.; Covini, D.; Digilio, R.; Scotti, C. Targeted Drug Delivery Using Immunoconjugates: Principles and Applications. J. Immunother. 2011, 34, 611–628. [Google Scholar] [CrossRef]
- Kubiatowski, T.; Kalinka, E. Antibody-Drug Conjugates in the Treatment of Advanced Triple-Negative Breast Cancer. Prz. menopauzalny = Menopause Rev. 2025, 24, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Khadela, A.; Soni, S.; Shah, A.C.; Pandya, A.J.; Megha, K.; Kothari, N.; Cb, A. Unveiling the Antibody-Drug Conjugates Portfolio in Battling Triple-Negative Breast Cancer: Therapeutic Trends and Future Horizon. Med. Oncol. 2022, 40, 25. [Google Scholar] [CrossRef] [PubMed]
- Al Jarroudi, O.; El Bairi, K.; Curigliano, G.; Afqir, S. Antibody–Drug Conjugates: A New Therapeutic Approach for Triple-Negative Breast Cancer. Cancer Treat. Res. 2023, 188, 1–27. [Google Scholar] [CrossRef]
- Tong, Y.; Fan, X.; Liu, H.; Liang, T. Advances in Trop-2 Targeted Antibody-Drug Conjugates for Breast Cancer: Mechanisms, Clinical Applications, and Future Directions. Front. Immunol. 2024, 15. [Google Scholar] [CrossRef]
- Vranic, S.; Gatalica, Z. Trop-2 Protein as a Therapeutic Target: A Focused Review on Trop-2-Based Antibody-Drug Conjugates and Their Predictive Biomarkers. Bosn. J. Basic Med. Sci. 2022, 22, 14–21. [Google Scholar] [CrossRef]
- Keskinkilic, M.; Sacks, R. Antibody-Drug Conjugates in Triple Negative Breast Cancer. Clin. Breast Cancer 2024, 24, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Spring, L.M.; Nakajima, E.; Hutchinson, J.; Viscosi, E.; Blouin, G.; Weekes, C.; Rugo, H.; Moy, B.; Bardia, A. Sacituzumab Govitecan for Metastatic Triple-Negative Breast Cancer: Clinical Overview and Management of Potential Toxicities. Oncologist 2021, 26, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Dri, A.; Arpino, G.; Bianchini, G.; Curigliano, G.; Danesi, R.; De Laurentiis, M.; Del Mastro, L.; Fabi, A.; Generali, D.; Gennari, A.; et al. Breaking Barriers in Triple Negative Breast Cancer (TNBC) – Unleashing the Power of Antibody-Drug Conjugates (ADCs). Cancer Treat. Rev. 2024, 123. [Google Scholar] [CrossRef] [PubMed]
- Bardia, A.; Messersmith, W.A.; Kio, E.A.; Berlin, J.D.; Vahdat, L.; Masters, G.A.; Moroose, R.; Santin, A.D.; Kalinsky, K.; Picozzi, V.; et al. Sacituzumab Govitecan, a Trop-2-Directed Antibody-Drug Conjugate, for Patients with Epithelial Cancer: Final Safety and Efficacy Results from the Phase I/II IMMU-132-01 Basket Trial. Ann. Oncol. 2021, 32, 746–756. [Google Scholar] [CrossRef]
- Chen, W.; Shen, L.; Jiang, J.; Zhang, L.; Zhang, Z.; Pan, J.; Ni, C.; Chen, Z. Antiangiogenic Therapy Reverses the Immunosuppressive Breast Cancer Microenvironment. Biomark. Res. 2021, 9, 59. [Google Scholar] [CrossRef]
- Lugano, R.; Ramachandran, M.; Dimberg, A. Tumor Angiogenesis: Causes, Consequences, Challenges and Opportunities. Cell. Mol. Life Sci. 2020, 77, 1745–1770. [Google Scholar] [CrossRef]
- Ikeda, H.; Kakeya, H. Targeting Hypoxia-Inducible Factor 1 (HIF-1) Signaling with Natural Products toward Cancer Chemotherapy. J. Antibiot. (Tokyo). 2021, 74, 687–695. [Google Scholar] [CrossRef]
- Hao, Z.; Wang, P. Lenvatinib in Management of Solid Tumors. Oncologist 2020, 25, e302–e310. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.C.; Saada-Bouzid, E.; Longo, F.; Yanez, E.; Im, S.A.; Castanon, E.; Desautels, D.N.; Graham, D.M.; Garcia-Corbacho, J.; Lopez, J.; et al. Lenvatinib plus Pembrolizumab for Patients with Previously Treated, Advanced, Triple-Negative Breast Cancer: Results from the Triple-Negative Breast Cancer Cohort of the Phase 2 LEAP-005 Study. Cancer 2024, 130, 3278–3288. [Google Scholar] [CrossRef]
- Shen, G.; Zheng, F.; Ren, D.; Du, F.; Dong, Q.; Wang, Z.; Zhao, F.; Ahmad, R.; Zhao, J. Anlotinib: A Novel Multi-Targeting Tyrosine Kinase Inhibitor in Clinical Development. J. Hematol. Oncol. 2018, 11. [Google Scholar] [CrossRef]
- Zhang, L.; Yang, L.; Ge, Y.; Zhu, Z.; Chen, B.; Yang, C.; Gao, H.; Yang, M.; Zhu, T.; Wang, K. Neoadjuvant Anlotinib/Sintilimab plus Chemotherapy in Triple-Negative Breast Cancer (NeoSACT): Phase 2 Trial. Cell Reports Med. 2025, 6. [Google Scholar] [CrossRef]
- Zhang, H.P.; Jiang, R.Y.; Zhu, J.Y.; Sun, K.N.; Huang, Y.; Zhou, H.H.; Zheng, Y.B.; Wang, X.J. PI3K/AKT/MTOR Signaling Pathway: An Important Driver and Therapeutic Target in Triple-Negative Breast Cancer. Breast Cancer 2024, 31, 539–551. [Google Scholar] [CrossRef]
- Massihnia, D.; Galvano, A.; Fanale, D.; Perez, A.; Castiglia, M.; Incorvaia, L.; Listì, A.; Rizzo, S.; Cicero, G.; Bazan, V.; et al. Triple Negative Breast Cancer: Shedding Light onto the Role of Pi3k/Akt/Mtor Pathway. Oncotarget 2016, 7, 60712–60722. [Google Scholar] [CrossRef]
- Garrido-Castro, A.C.; Saura, C.; Barroso-Sousa, R.; Guo, H.; Ciruelos, E.; Bermejo, B.; Gavilá, J.; Serra, V.; Prat, A.; Paré, L.; et al. Phase 2 Study of Buparlisib (BKM120), a Pan-Class I PI3K Inhibitor, in Patients with Metastatic Triple-Negative Breast Cancer. Breast Cancer Res. 2020, 22. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Shapiro, G.I.; Kristeleit, R.S.; Abdul Razak, A.R.; Leong, S.; Alsina, M.; Giordano, A.; Gelmon, K.A.; Stringer-Reasor, E.; Vaishampayan, U.N.; et al. A Phase 1B Open-Label Study of Gedatolisib (PF-05212384) in Combination with Other Anti-Tumour Agents for Patients with Advanced Solid Tumours and Triple-Negative Breast Cancer. Br. J. Cancer 2023, 128, 30–41. [Google Scholar] [CrossRef]
- Schram, A.M.; Takebe, N.; Chen, A.; Zhou, Q.; Iasonos, A.; Silber, J.; Reynolds, M.; Hussain, S.; Gavriliuc, M.; Smyth, L.M.; et al. A Phase I Study of AZD8186 in Combination with Docetaxel in Patients with PTEN-Mutated or PIK3CB-Mutated Advanced Solid Tumors. ESMO Open 2025, 10. [Google Scholar] [CrossRef] [PubMed]
- Vtorushin, S.; Dulesova, A.; Krakhmal, N. Luminal Androgen Receptor (LAR) Subtype of Triple-Negative Breast Cancer: Molecular, Morphological, and Clinical Features. J. Zhejiang Univ. Sci. B 2022, 23, 617–624. [Google Scholar] [CrossRef]
- Echavarria, I.; Lopez-Tarruella, S.; Picornell, A.; García-Saenz, J.A.; Jerez, Y.; Hoadley, K.; Gomez, H.L.; Moreno, F.; Del Monte-Millan, M.; Marquez-Rodas, I.; et al. Pathological Response in a Triple-Negative Breast Cancer Cohort Treated with Neoadjuvant Carboplatin and Docetaxel According to Lehmann’s Refined Classification. Clin. Cancer Res. 2018, 24, 1845–1852. [Google Scholar] [CrossRef]
- Chen, M.; Yang, Y.; Xu, K.; Li, L.; Huang, J.; Qiu, F. Androgen Receptor in Breast Cancer: From Bench to Bedside. Front. Endocrinol. (Lausanne). 2020, 11, 573. [Google Scholar] [CrossRef]
- Scholar, E. Bicalutamide. xPharm Compr. Pharmacol. Ref. 2007, 1–5. [Google Scholar] [CrossRef]
- Lee, A. Darolutamide: A Review in Metastatic Hormone-Sensitive Prostate Cancer. Target. Oncol. 2023, 18, 793–800. [Google Scholar] [CrossRef]
- Spring, L.M.; Wander, S.A.; Zangardi, M.; Bardia, A. CDK 4/6 Inhibitors in Breast Cancer: Current Controversies and Future Directions. Curr. Oncol. Rep. 2019, 21. [Google Scholar] [CrossRef]
- Saleh, L.; Wilson, C.; Holen, I. CDK4/6 Inhibitors: A Potential Therapeutic Approach for Triple Negative Breast Cancer. MedComm 2021, 2, 514–530. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Gao, J.; Wang, M.; Li, M. Potential Prospect of CDK4/6 Inhibitors in Triple-Negative Breast Cancer. Cancer Manag. Res. 2021, 13, 5223–5237. [Google Scholar] [CrossRef] [PubMed]
- Gerosa, R.; De Sanctis, R.; Jacobs, F.; Benvenuti, C.; Gaudio, M.; Saltalamacchia, G.; Torrisi, R.; Masci, G.; Miggiano, C.; Agustoni, F.; et al. Cyclin-Dependent Kinase 2 (CDK2) Inhibitors and Others Novel CDK Inhibitors (CDKi) in Breast Cancer: Clinical Trials, Current Impact, and Future Directions. Crit. Rev. Oncol. Hematol. 2024, 196. [Google Scholar] [CrossRef]
- Finn, R.S.; Dering, J.; Conklin, D.; Kalous, O.; Cohen, D.J.; Desai, A.J.; Ginther, C.; Atefi, M.; Chen, I.; Fowst, C.; et al. PD 0332991, a Selective Cyclin D Kinase 4/6 Inhibitor, Preferentially Inhibits Proliferation of Luminal Estrogen Receptor-Positive Human Breast Cancer Cell Lines in Vitro. Breast Cancer Res. 2009, 11. [Google Scholar] [CrossRef] [PubMed]
- Goel, S.; Tan, A.R.; Rugo, H.S.; Aftimos, P.; Andrić, Z.; Beelen, A.; Zhang, J.; Yi, J.S.; Malik, R.; O’Shaughnessy, J. Trilaciclib Prior to Gemcitabine plus Carboplatin for Metastatic Triple-Negative Breast Cancer: Phase III PRESERVE 2. Futur. Oncol. 2022, 18, 3701–3711. [Google Scholar] [CrossRef]
- Huang, J.; Zheng, L.; Sun, Z.; Li, J. CDK4/6 Inhibitor Resistance Mechanisms and Treatment Strategies (Review). Int. J. Mol. Med. 2022, 50. [Google Scholar] [CrossRef] [PubMed]
- Palbociclib for Breast Cancer. Aust. Prescr. 2018, 41, 127–128. [CrossRef]
- Trilaciclib. LiverTox Clin. Res. Inf. Drug-Induced Liver Inj. 2012.
- Abraham, J.E.; O’Connor, L.O.; Grybowicz, L.; Alba, K.P.; Dayimu, A.; Demiris, N.; Harvey, C.; Drewett, L.M.; Lucey, R.; Fulton, A.; et al. Neoadjuvant PARP Inhibitor Scheduling in BRCA1 and BRCA2 Related Breast Cancer: PARTNER, a Randomized Phase II/III Trial. Nat. Commun. 2025, 16. [Google Scholar] [CrossRef] [PubMed]
- Abraham, J.E.; Pinilla, K.; Dayimu, A.; Grybowicz, L.; Demiris, N.; Harvey, C.; Drewett, L.M.; Lucey, R.; Fulton, A.; Roberts, A.N.; et al. The PARTNER Trial of Neoadjuvant Olaparib with Chemotherapy in Triple-Negative Breast Cancer. Nature 2024, 629, 1142–1148. [Google Scholar] [CrossRef]
- Woitek, R.; McLean, M.A.; Ursprung, S.; Rueda, O.M.; Garcia, R.M.; Locke, M.J.; Beer, L.; Baxter, G.; Rundo, L.; Provenzano, E.; et al. Hyperpolarized Carbon-13 MRI for Early Response Assessment of Neoadjuvant Chemotherapy in Breast Cancer Patients. Cancer Res. 2021, 81, 6004–6017. [Google Scholar] [CrossRef]
- Kulkarni, A.; Zhou, J.; Biyani, N.; Kathad, U.; Banerjee, P.P.; Srivastava, S.; Prucsi, Z.; Solarczyk, K.; Bhatia, K.; Ewesuedo, R.B.; et al. LP-184, a Novel Acylfulvene Molecule, Exhibits Anticancer Activity against Diverse Solid Tumors with Homologous Recombination Deficiency. Cancer Res. Commun. 2024, 4, 1199–1210. [Google Scholar] [CrossRef]
- Sun, C.; Fang, Y.; Labrie, M.; Li, X.; Mills, G.B. Systems Approach to Rational Combination Therapy: PARP Inhibitors. Biochem. Soc. Trans. 2020, 48, 1101–1108. [Google Scholar] [CrossRef]
- Bardia, A.; Rugo, H.S.; Tolaney, S.M.; Loirat, D.; Punie, K.; Oliveira, M.; Brufsky, A.; Kalinsky, K.; Cortes, J.; Shaughnessy, J.O.; et al. Final Results from the Randomized Phase III ASCENT Clinical Trial in Metastatic Triple-Negative Breast Cancer and Association of Outcomes by Human Epidermal Growth Factor Receptor 2 and Trophoblast Cell Surface Antigen 2 Expression. J. Clin. Oncol. 2024, 42, 1738–1744. [Google Scholar] [CrossRef]
- Naito, Y.; Nakamura, S.; Kawaguchi-Sakita, N.; Ishida, T.; Nakayama, T.; Yamamoto, Y.; Masuda, N.; Matsumoto, K.; Kogawa, T.; Sudo, K.; et al. Preliminary Results from ASCENT-J02: A Phase 1/2 Study of Sacituzumab Govitecan in Japanese Patients with Advanced Solid Tumors. Int. J. Clin. Oncol. 2024, 29, 1684–1695. [Google Scholar] [CrossRef] [PubMed]
- Frentzas, S.; Mislang, A.R.A.; Lemech, C.; Nagrial, A.; Underhill, C.; Wang, W.; Wang, Z.M.; Li, B.; Xia, Y.; Coward, J.I.G. Phase 1a Dose Escalation Study of Ivonescimab (AK112/SMT112), an Anti-PD-1/VEGF-A Bispecific Antibody, in Patients with Advanced Solid Tumors. J. Immunother. Cancer 2024, 12. [Google Scholar] [CrossRef]
- Zhao, Y.; Chen, G.; Chen, J.; Zhuang, L.; Du, Y.; Yu, Q.; Zhuang, W.; Zhao, Y.; Zhou, M.; Zhang, W.; et al. AK112, a Novel PD-1/VEGF Bispecific Antibody, in Combination with Chemotherapy in Patients with Advanced Non-Small Cell Lung Cancer (NSCLC): An Open-Label, Multicenter, Phase II Trial. EClinicalMedicine 2023, 62, 102106. [Google Scholar] [CrossRef]
- Kharenko, O.A.; Patel, R.G.; Calosing, C.; van der Horst, E.H. Combination of ZEN-3694 with CDK4/6 Inhibitors Reverses Acquired Resistance to CDK4/6 Inhibitors in ER-Positive Breast Cancer. Cancer Gene Ther. 2022, 29, 859–869. [Google Scholar] [CrossRef]
- Tan, A.R.; Wright, G.S.; Thummala, A.R.; Danso, M.A.; Popovic, L.; Pluard, T.J.; Han, H.S.; Vojnović, Ž.; Vasev, N.; Ma, L.; et al. Trilaciclib plus Chemotherapy versus Chemotherapy Alone in Patients with Metastatic Triple-Negative Breast Cancer: A Multicentre, Randomised, Open-Label, Phase 2 Trial. Lancet Oncol. 2019, 20, 1587–1601. [Google Scholar] [CrossRef]
- Tan, A.R.; Wright, G.S.; Thummala, A.R.; Danso, M.A.; Popovic, L.; Pluard, T.J.; Han, H.S.; Vojnović, Ž.; Vasev, N.; Ma, L.; et al. Trilaciclib Prior to Chemotherapy in Patients with Metastatic Triple-Negative Breast Cancer: Final Efficacy and Subgroup Analysis from a Randomized Phase II Study. Clin. Cancer Res. 2022, 28, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Chave, K.J.; Auger, I.E.; Galivan, J.; Ryan, T.J. Molecular Modeling and Site-Directed Mutagenesis Define the Catalytic Motif in Human γ-Glutamyl Hydrolase. J. Biol. Chem. 2000, 275, 40365–40370. [Google Scholar] [CrossRef] [PubMed]
- Yao, R.; Schneider, E.; Ryan, T.J.; Galivan, J. Human Gamma-Glutamyl Hydrolase: Cloning and Characterization of the Enzyme Expressed in Vitro. Proc. Natl. Acad. Sci. U. S. A. 1996, 93, 10134–10138. [Google Scholar] [CrossRef] [PubMed]
- Uhlén, M.; Fagerberg, L.; Hallström, B.M.; Lindskog, C.; Oksvold, P.; Mardinoglu, A.; Sivertsson, Å.; Kampf, C.; Sjöstedt, E.; Asplund, A.; et al. Tissue-Based Map of the Human Proteome. Science (80-. ). 2015, 347. [Google Scholar] [CrossRef]
- Zhu, M.; Liu, N.; Lin, J.; Wang, J.; Lai, H.; Liu, Y. HDAC7 Inhibits Cell Proliferation via NudCD1/GGH Axis in Triple-Negative Breast Cancer. Oncol. Lett. 2023, 25, 33. [Google Scholar] [CrossRef]
- Shubbar, E.; Helou, K.; Kovács, A.; Nemes, S.; Hajizadeh, S.; Enerbäck, C.; Einbeigi, Z. High Levels of γ-Glutamyl Hydrolase (GGH) Are Associated with Poor Prognosis and Unfavorable Clinical Outcomes in Invasive Breast Cancer. BMC Cancer 2013, 13. [Google Scholar] [CrossRef]
- Kim, S.E.; Cole, P.D.; Cho, R.C.; Ly, A.; Ishiguro, L.; Sohn, K.J.; Croxford, R.; Kamen, B.A.; Kim, Y.I. γ-Glutamyl Hydrolase Modulation and Folate Influence Chemosensitivity of Cancer Cells to 5-Fluorouracil and Methotrexate. Br. J. Cancer 2013, 109, 2175–2188. [Google Scholar] [CrossRef]
- Phan, J.; Steadman, D.J.; Koli, S.; Ding, W.C.; Minor, W.; Bruce Dunlap, R.; Berger, S.H.; Lebioda, L. Structure of Human Thymidylate Synthase Suggests Advantages of Chemotherapy with Noncompetitive Inhibitors. J. Biol. Chem. 2001, 276, 14170–14177. [Google Scholar] [CrossRef]
- Andersona, D.D.; Quintero, C.M.; Stovera, P.J. Identification of a de Novo Thymidylate Biosynthesis Pathway in Mammalian Mitochondria. Proc. Natl. Acad. Sci. U. S. A. 2011, 108, 15163–15168. [Google Scholar] [CrossRef]
- Kumar, A.; Singh, A.K.; Singh, H.; Thareja, S.; Kumar, P. Regulation of Thymidylate Synthase: An Approach to Overcome 5-FU Resistance in Colorectal Cancer. Med. Oncol. 2023, 40. [Google Scholar] [CrossRef]
- Chamizo, C.; Zazo, S.; Dómine, M.; Cristóbal, I.; García-Foncillas, J.; Rojo, F.; Madoz-Gúrpide, J. Thymidylate Synthase Expression as a Predictive Biomarker of Pemetrexed Sensitivity in Advanced Non-Small Cell Lung Cancer. BMC Pulm. Med. 2015, 15. [Google Scholar] [CrossRef]
- Geng, Y.; Xie, L.; Wang, Y.; Wang, Y. Unveiling the Oncogenic Significance of Thymidylate Synthase in Human Cancers. Am. J. Transl. Res. 2024, 16, 5228–5247. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhang, J.; Chen, J.; Yang, X.; Sun, H.; Zhao, Z.; Zhou, H.; Shen, H. Thymidylate Synthase Promotes Esophageal Squamous Cell Carcinoma Growth by Relieving Oxidative Stress through Activating Nuclear Factor Erythroid 2-Related Factor 2 Expression. PLoS One 2023, 18. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Schneider, B.P.; Li, L. A Bioinformatics Approach for Precision Medicine Off-Label Drug Selection among Triple Negative Breast Cancer Patients. J. Am. Med. Informatics Assoc. 2016, 23, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Tian, B.; Zhang, M.; Gao, X.; Jie, L.; Liu, P.; Li, J. Diagnostic and Prognostic Value of Thymidylate Synthase Expression in Breast Cancer. Clin. Exp. Pharmacol. Physiol. 2021, 48, 279–287. [Google Scholar] [CrossRef]
- Siddiqui, A.; Gollavilli, P.N.; Schwab, A.; Vazakidou, M.E.; Ersan, P.G.; Ramakrishnan, M.; Pluim, D.; Coggins, S.A.; Saatci, O.; Annaratone, L.; et al. Thymidylate Synthase Maintains the De-Differentiated State of Triple Negative Breast Cancers. Cell Death Differ. 2019, 26, 2223–2236. [Google Scholar] [CrossRef]
- Brauer, P.M.; Tyner, A.L. Building a Better Understanding of the Intracellular Tyrosine Kinase PTK6 - BRK by BRK. Biochim. Biophys. Acta - Rev. Cancer 2010, 1806, 66–73. [Google Scholar] [CrossRef]
- Dwyer, A.R.; Kerkvliet, C.P.; Krutilina, R.I.; Playa, H.C.; Parke, D.N.; Thomas, W.A.; Smeester, B.A.; Moriarity, B.S.; Seagroves, T.N.; Lange, C.A. Breast Tumor Kinase (Brk/PTK6) Mediates Advanced Cancer Phenotypes via SH2-Domain Dependent Activation of RhoA and Aryl Hydrocarbon Receptor (AhR) Signaling. Mol. Cancer Res. 2021, 19, 329–345. [Google Scholar] [CrossRef] [PubMed]
- Aubele, M.; Walch, A.K.; Ludyga, N.; Braselmann, H.; Atkinson, M.J.; Luber, B.; Auer, G.; Tapio, S.; Cooke, T.; Bartlett, J.M.S. Prognostic Value of Protein Tyrosine Kinase 6 (PTK6) for Long-Term Survival of Breast Cancer Patients. Br. J. Cancer 2008, 99, 1089–1095. [Google Scholar] [CrossRef]
- Qiu, L.; Levine, K.; Gajiwala, K.S.; Cronin, C.N.; Nagata, A.; Johnson, E.; Kraus, M.; Tatlock, J.; Kania, R.; Foley, T.; et al. Small Molecule Inhibitors Reveal PTK6 Kinase Is Not an Oncogenic Driver in Breast Cancers. PLoS One 2018, 13. [Google Scholar] [CrossRef]
- Burmi, R.S.; Box, G.M.; Wazir, U.; Hussain, H.A.; Davies, J.A.; Court, W.J.; Eccles, S.A.; Jiang, W.G.; Mokbel, K.; Harvey, A.J. Breast Tumour Kinase (Brk/PTK6) Contributes to Breast Tumour Xenograft Growth and Modulates Chemotherapeutic Responses In Vitro. Genes (Basel). 2022, 13. [Google Scholar] [CrossRef]
- Regan Anderson, T.M.; Ma, S.H.; Raj, G. V.; Cidlowski, J.A.; Helle, T.M.; Knutson, T.P.; Krutilina, R.I.; Seagroves, T.N.; Lange, C.A. Breast Tumor Kinase (Brk/PTK6) Is Induced by HIF, Glucocorticoid Receptor, and PELP1-Mediated Stress Signaling in Triple-Negative Breast Cancer. Cancer Res. 2016, 76, 1653–1663. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Park, S.H.; Nayak, A.; Byerly, J.H.; Irie, H.Y. PTK6 Inhibition Suppresses Metastases of Triple-Negative Breast Cancer via SNAIL-Dependent E-Cadherin Regulation. Cancer Res. 2016, 76, 4406–4417. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Qu, W.; Tu, J.; Yang, L.; Gui, X. Prognostic Impact of PTK6 Expression in Triple Negative Breast Cancer. BMC Womens. Health 2023, 23. [Google Scholar] [CrossRef]
- Zhang, H.; Barceló, J.M.; Lee, B.; Kohlhagen, G.; Zimonjic, D.B.; Popescu, N.C.; Pommier, Y. Human Mitochondrial Topoisomerase I. Proc. Natl. Acad. Sci. U. S. A. 2001, 98, 10608–10613. [Google Scholar] [CrossRef]
- Baechler, S.A.; Factor, V.M.; Dalla Rosa, I.; Ravji, A.; Becker, D.; Khiati, S.; Miller Jenkins, L.M.; Lang, M.; Sourbier, C.; Michaels, S.A.; et al. The Mitochondrial Type IB Topoisomerase Drives Mitochondrial Translation and Carcinogenesis. Nat. Commun. 2019, 10. [Google Scholar] [CrossRef]
- Fei, L.; Lu, Z.; Xu, Y.; Hou, G. A Comprehensive Pan-Cancer Analysis of the Expression Characteristics, Prognostic Value, and Immune Characteristics of TOP1MT. Front. Genet. 2022, 13, 920897. [Google Scholar] [CrossRef]
- Guha, M.; Srinivasan, S.; Raman, P.; Jiang, Y.; Kaufman, B.A.; Taylor, D.; Dong, D.; Chakrabarti, R.; Picard, M.; Carstens, R.P.; et al. Aggressive Triple Negative Breast Cancers Have Unique Molecular Signature on the Basis of Mitochondrial Genetic and Functional Defects. Biochim. Biophys. Acta - Mol. Basis Dis. 2018, 1864, 1060–1071. [Google Scholar] [CrossRef]
- Habib, J.G.; O’Shaughnessy, J.A. The Hedgehog Pathway in Triple-Negative Breast Cancer. Cancer Med. 2016, 5, 2989–3006. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Borrego, M.; Jimenez, B.; Antolín, S.; García-Saenz, J.A.; Corral, J.; Jerez, Y.; Trigo, J.; Urruticoechea, A.; Colom, H.; Gonzalo, N.; et al. A Phase Ib Study of Sonidegib (LDE225), an Oral Small Molecule Inhibitor of Smoothened or Hedgehog Pathway, in Combination with Docetaxel in Triple Negative Advanced Breast Cancer Patients: GEICAM/2012–12 (EDALINE) Study. Invest. New Drugs 2019, 37, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Han, B.; Qu, Y.; Jin, Y.; Yu, Y.; Deng, N.; Wawrowsky, K.; Zhang, X.; Li, N.; Bose, S.; Wang, Q.; et al. FOXC1 Activates Smoothened-Independent Hedgehog Signaling in Basal-like Breast Cancer. Cell Rep. 2015, 13, 1046–1058. [Google Scholar] [CrossRef] [PubMed]
- de Souza, A.Q.; Pegorari, M.S.; Nascimento, J.S.; de Oliveira, P.B.; Tavares, D.M. dos S. Incidence and Predictive Factors of Falls in Community-Dwelling Elderly: A Longitudinal Study. Cienc. e Saude Coletiva 2019, 24, 3507–3516. [Google Scholar] [CrossRef]
- Choi, J.; Naito, K.; Curry, E.J.; Li, X. Anterior Cruciate Ligament Reconstruction With Achilles Tendon Allograft in a Patient With Ehlers-Danlos Syndrome. Orthop. J. Sport. Med. 2018, 6, 2325967118785170. [Google Scholar] [CrossRef]
- Li, Q.; Pang, J.; Deng, Y.; Zhang, S.; Wang, Y.; Gao, Y.; Yuan, X.; Wei, Y.; Zhang, H.; Tan, J.; et al. Adverse Cardiovascular Effects of Phenylephrine Eye Drops Combined With Intravenous Atropine. Front. Pharmacol. 2020, 11, 596539. [Google Scholar] [CrossRef]
- Khatiban, M.; Tohidi, S.; Shahdoust, M. The Effects of Applying an Assessment Form Based on the Health Functional Patterns on Nursing Student’s Attitude and Skills in Developing the Nursing Process. Int. J. Nurs. Sci. 2019, 6, 329–333. [Google Scholar] [CrossRef]
- Vingiani, A.; Lorenzini, D.; Conca, E.; Volpi, C.C.; Trupia, D.V.; Gloghini, A.; Perrone, F.; Tamborini, E.; Dagrada, G.P.; Agnelli, L.; et al. Pan-TRK Immunohistochemistry as Screening Tool for NTRK Fusions: A Diagnostic Workflow for the Identification of Positive Patients in Clinical Practice. Cancer Biomarkers 2023, 38, 301–309. [Google Scholar] [CrossRef]
- The Cancer Genome Atlas Program (TCGA) - NCI. Available online: https://www.cancer.gov/ccg/research/genome-sequencing/tcga (accessed on 7 January 2026).
- Curtis, C.; Shah, S.P.; Chin, S.F.; Turashvili, G.; Rueda, O.M.; Dunning, M.J.; Speed, D.; Lynch, A.G.; Samarajiwa, S.; Yuan, Y.; et al. The Genomic and Transcriptomic Architecture of 2,000 Breast Tumours Reveals Novel Subgroups. Nature 2012, 486, 346–352. [Google Scholar] [CrossRef]
- Pereira, B.; Chin, S.F.; Rueda, O.M.; Vollan, H.K.M.; Provenzano, E.; Bardwell, H.A.; Pugh, M.; Jones, L.; Russell, R.; Sammut, S.J.; et al. The Somatic Mutation Profiles of 2,433 Breast Cancers Refines Their Genomic and Transcriptomic Landscapes. Nat. Commun. 2016, 7. [Google Scholar] [CrossRef] [PubMed]
- Ji, X.D.; Li, G.; Feng, Y.X.; Zhao, J.S.; Li, J.J.; Sun, Z.J.; Shi, S.; Deng, Y.Z.; Xu, J.F.; Zhu, Y.Q.; et al. EphB3 Is Overexpressed in Non-Small-Cell Lung Cancer and Promotes Tumor Metastasis by Enhancing Cell Survival and Migration. Cancer Res. 2011, 71, 1156–1166. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Ji, X.D.; Gao, H.; Zhao, J.S.; Xu, J.F.; Sun, Z.J.; Deng, Y.Z.; Shi, S.; Feng, Y.X.; Zhu, Y.Q.; et al. EphB3 Suppresses Non-Small-Cell Lung Cancer Metastasis via a PP2A/RACK1/Akt Signalling Complex. Nat. Commun. 2012, 3. [Google Scholar] [CrossRef]
- Li, J.J.; Sun, Z.J.; Yuan, Y.M.; Yin, F.F.; Bian, Y.G.; Long, L.Y.; Zhang, X.L.; Xie, D. EphB3 Stimulates Cell Migration and Metastasis in a Kinase-Dependent Manner through Vav2-Rho GTPase Axis in Papillary Thyroid Cancer. J. Biol. Chem. 2017, 292, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Chiu, S.T.; Chang, K.J.; Ting, C.H.; Shen, H.C.; Li, H.; Hsieh, F.J. Over-Expression of EphB3 Enhances Cell-Cell Contacts and Suppresses Tumor Growth in HT-29 Human Colon Cancer Cells. Carcinogenesis 2009, 30, 1475–1486. [Google Scholar] [CrossRef]
- Jägle, S.; Rönsch, K.; Timme, S.; Andrlová, H.; Bertrand, M.; Jäger, M.; Proske, A.; Schrempp, M.; Yousaf, A.; Michoel, T.; et al. Silencing of the EPHB3 Tumor-Suppressor Gene in Human Colorectal Cancer through Decommissioning of a Transcriptional Enhancer. Proc. Natl. Acad. Sci. U. S. A. 2014, 111, 4886–4891. [Google Scholar] [CrossRef]
- Jang, B.G.; Kim, H.S.; Bae, J.M.; Kim, W.H.; Hyun, C.L.; Kang, G.H. Expression Profile and Prognostic Significance of EPHB3 in Colorectal Cancer. Biomolecules 2020, 10. [Google Scholar] [CrossRef]
- Pasquale, E.B. Eph Receptors and Ephrins in Cancer Progression. Nat. Rev. Cancer 2024, 24, 5–27. [Google Scholar] [CrossRef]
- Weigel, C.; Schmezer, P.; Plass, C.; Popanda, O. Epigenetics in Radiation-Induced Fibrosis. Oncogene 2015, 34, 2145–2155. [Google Scholar] [CrossRef]
- Yamada, K.; Ito, M.; Kobayashi, H.; Hasegawa, Y.; Fukuda, S.; Yamaguchi, S.; Taketani, T. Flavin Adenine Dinucleotide Synthase Deficiency Due to FLAD1 Mutation Presenting as Multiple Acyl-CoA Dehydrogenation Deficiency-like Disease: A Case Report. Brain Dev. 2019, 41, 638–642. [Google Scholar] [CrossRef]
- González-Fernández, M.; Ghosh, N.; Ellison, T.; McLeod, J.C.; Pelletier, C.A.; Williams, K. Moving beyond the Limitations of the Visual Analog Scale for Measuring Pain: Novel Use of the General Labeled Magnitude Scale in a Clinical Setting. Am. J. Phys. Med. Rehabil. 2014, 93, 75–81. [Google Scholar] [CrossRef]
- Roth, L.; Srivastava, S.; Lindzen, M.; Sas-Chen, A.; Sheffer, M.; Lauriola, M.; Enuka, Y.; Noronha, A.; Mancini, M.; Lavi, S.; et al. SILAC Identifies LAD1 as a Filamin-Binding Regulator of Actin Dynamics in Response to EGF and a Marker of Aggressive Breast Tumors. Sci. Signal. 2018, 11. [Google Scholar] [CrossRef]
- Chang, C.Y.; Huang, Y.C.; Chiang, H.H.; Wu, Y.Y.; Wu, K.L.; Chang, Y.Y.; Liu, L.X.; Tsai, Y.M.; Hsu, Y.L. Ladinin 1 Shortens Survival via Promoting Proliferation and Enhancing Invasiveness in Lung Adenocarcinoma. Int. J. Mol. Sci. 2022, 24. [Google Scholar] [CrossRef] [PubMed]
- Moon, B.; Yang, S.J.; Park, S.M.; Lee, S.H.; Song, K.S.; Jeong, E.J.; Park, M.; Kim, J.S.; Yeom, Y. Il; Kim, J.A. LAD1 Expression Is Associated with the Metastatic Potential of Colorectal Cancer Cells. BMC Cancer 2020, 20, 1180. [Google Scholar] [CrossRef]
- Abé, T.; Yamazaki, M.; Nozumi, M.; Maruyama, S.; Takamura, K.; Ohashi, R.; Ajioka, Y.; Tanuma, J.I. Ladinin-1 in Actin Arcs of Oral Squamous Cell Carcinoma Is Involved in Cell Migration and Epithelial Phenotype. Sci. Rep. 2024, 14. [Google Scholar] [CrossRef]
- Jeng, K.S.; Sheen, I.S.; Leu, C.M.; Tseng, P.H.; Chang, C.F. The Role of Smoothened in Cancer. Int. J. Mol. Sci. 2020, 21, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Riaz, N.; Burugu, S.; Cheng, A.S.; Leung, S.C.Y.; Gao, D.; Nielsen, T.O. Prognostic Significance of Csf-1r Expression in Early Invasive Breast Cancer. Cancers (Basel). 2021, 13, 5769. [Google Scholar] [CrossRef]
- Singh, K.; Showalter, C.A.; Manring, H.R.; Haque, S.J.; Chakravarti, A. “Oh, Dear We Are in Tribble”: An Overview of the Oncogenic Functions of Tribbles 1. Cancers (Basel). 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Guda, C. Integrative Exploration of Genomic Profiles for Triple Negative Breast Cancer Identifies Potential Drug Targets. Med. (United States) 2016, 95. [Google Scholar] [CrossRef]
- Warburg, O. and W.F. and N.E. The Metabolism of Tumors in the Body. J Gen Physiol 1927, 8, 519--530. [CrossRef] [PubMed]
- Hussein, Y.R.; Bandyopadhyay, S.; Semaan, A.; Ahmed, Q.; Albashiti, B.; Jazaerly, T.; Nahleh, Z.; Ali-Fehmi, R. Glut-1 Expression Correlates with Basal-like Breast Cancer. Transl. Oncol. 2011, 4, 321–327. [Google Scholar] [CrossRef]
- Wu, Q.; ba-alawi, W.; Deblois, G.; Cruickshank, J.; Duan, S.; Lima-Fernandes, E.; Haight, J.; Tonekaboni, S.A.M.; Fortier, A.M.; Kuasne, H.; et al. GLUT1 Inhibition Blocks Growth of RB1-Positive Triple Negative Breast Cancer. Nat. Commun. 2020, 11. [Google Scholar] [CrossRef]
- Zhao, F.; Ming, J.; Zhou, Y.; Fan, L. Inhibition of Glut1 by WZB117 Sensitizes Radioresistant Breast Cancer Cells to Irradiation. Cancer Chemother. Pharmacol. 2016, 77, 963–972. [Google Scholar] [CrossRef]
- Chan, D.A.; Sutphin, P.D.; Nguyen, P.; Turcotte, S.; Lai, E.W.; Banh, A.; Reynolds, G.E.; Chi, J.T.; Wu, J.; Solow-Cordero, D.E.; et al. Targeting GLUT1 and the Warburg Effect in Renal Cell Carcinoma by Chemical Synthetic Lethality. Sci. Transl. Med. 2011, 3, 94ra70. [Google Scholar] [CrossRef] [PubMed]
- Pliszka, M.; Szablewski, L.; Pliszka, M.; Szablewski, L. Glucose Transporters as a Target for Anticancer Therapy. Cancers 2021, Vol. 13, 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Li, X.; Xie, X.; Ye, F.; Chen, B.; Song, C.; Tang, H.; Xie, X. High Expressions of LDHA and AMPK as Prognostic Biomarkers for Breast Cancer. Breast 2016, 30, 39–46. [Google Scholar] [CrossRef]
- Lim, S.O.; Li, C.W.; Xia, W.; Lee, H.H.; Chang, S.S.; Shen, J.; Hsu, J.L.; Raftery, D.; Djukovic, D.; Gu, H.; et al. EGFR Signaling Enhances Aerobic Glycolysis in Triple-Negative Breast Cancer Cells to Promote Tumor Growth and Immune Escape. Cancer Res. 2016, 76, 1284–1296. [Google Scholar] [CrossRef]
- Han, G.; Bai, X.; Li, F.; Huang, L.; Hao, Y.; Li, W.; Bu, P.; Zhang, H.; Liu, X.; Xie, J. Long Non-Coding RNA HANR Modulates the Glucose Metabolism of Triple Negative Breast Cancer via Stabilizing Hexokinase 2. Heliyon 2024, 10, e23827. [Google Scholar] [CrossRef]
- Patra, K.C.; Wang, Q.; Bhaskar, P.T.; Miller, L.; Wang, Z.; Wheaton, W.; Chandel, N.; Laakso, M.; Muller, W.J.; Allen, E.L.; et al. Hexokinase 2 Is Required for Tumor Initiation and Maintenance and Its Systemic Deletion Is Therapeutic in Mouse Models of Cancer. Cancer Cell 2013, 24, 213–228. [Google Scholar] [CrossRef]
- O’Neill, S.; Porter, R.K.; McNamee, N.; Martinez, V.G.; O’Driscoll, L. 2-Deoxy-D-Glucose Inhibits Aggressive Triple-Negative Breast Cancer Cells by Targeting Glycolysis and the Cancer Stem Cell Phenotype. Sci. Reports 2019 91 2019, 9, 3788. [Google Scholar] [CrossRef] [PubMed]
- Ganapathy-Kanniappan, S.; Vali, M.; Kunjithapatham, R.; Buijs, M.; Syed, L.H.; Rao, P.P.; Ota, S.; Kwak, B.K.; Loffroy, R.; Geschwind, J.F. 3-Bromopyruvate: A New Targeted Antiglycolytic Agent and a Promise for Cancer Therapy. Curr. Pharm. Biotechnol. 2010, 999, 1–13. [Google Scholar] [CrossRef]
- Ganapathy-Kanniappan, S.; Geschwind, J.F.H. Tumor Glycolysis as a Target for Cancer Therapy: Progress and Prospects. Mol. Cancer 2013 121 2013, 12, 152. [Google Scholar] [CrossRef]
- Bhutia, Y.D.; Babu, E.; Ganapathy, V. Re-Programming Tumour Cell Metabolism to Treat Cancer: No Lone Target for Lonidamine. Biochem. J. 2016, 473, 1503–1506. [Google Scholar] [CrossRef]
- Meng, X.; Lu, Z.; Lv, Q.; Jiang, Y.; Zhang, L.; Wang, Z. Tumor Metabolism Destruction via Metformin-Based Glycolysis Inhibition and Glucose Oxidase-Mediated Glucose Deprivation for Enhanced Cancer Therapy. Acta Biomater. 2022, 145, 222–234. [Google Scholar] [CrossRef]
- Semenza, G.L. Hypoxia-Inducible Factors: Mediators of Cancer Progression and Targets for Cancer Therapy. Trends Pharmacol. Sci. 2012, 33, 207. [Google Scholar] [CrossRef] [PubMed]
- Naik, A.; Decock, J. Lactate Metabolism and Immune Modulation in Breast Cancer: A Focused Review on Triple Negative Breast Tumors. Front. Oncol. 2020, 10, 598626. [Google Scholar] [CrossRef]
- Fang, T.; Hu, L.; Chen, T.; Li, F.; Yang, L.; Liang, B.; Wang, W.; Zeng, F. Lactate Dehydrogenase-A-Forming LDH5 Promotes Breast Cancer Progression. Breast cancer (Dove Med. Press. 2025, 17, 157–170. [Google Scholar] [CrossRef]
- Kwon, Y.J.; Seo, E.B.; Jeong, A.J.; Lee, S.H.; Noh, K.H.; Lee, S.; Cho, C.H.; Lee, C.H.; Shin, H.M.; Kim, H.R.; et al. The Acidic Tumor Microenvironment Enhances PD-L1 Expression via Activation of STAT3 in MDA-MB-231 Breast Cancer Cells. BMC Cancer 2022, 22. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Xie, X.; Wang, H.; Xiao, X.; Yang, L.; Tian, Z.; Guo, X.; Zhang, L.; Tang, H.; Xie, X. PDL1 And LDHA Act as CeRNAs in Triple Negative Breast Cancer by Regulating MiR-34a. J. Exp. Clin. Cancer Res. 2017, 36, 129. [Google Scholar] [CrossRef]
- Le, A.; Cooper, C.R.; Gouw, A.M.; Dinavahi, R.; Maitra, A.; Deck, L.M.; Royer, R.E.; Vander Jagt, D.L.; Semenza, G.L.; Dang, C. V. Inhibition of Lactate Dehydrogenase A Induces Oxidative Stress and Inhibits Tumor Progression. Proc. Natl. Acad. Sci. U. S. A. 2010, 107, 2037–2042. [Google Scholar] [CrossRef]
- Mazzio, E.; Mack, N.; Badisa, R.B.; Soliman, K.F.A. Triple Isozyme Lactic Acid Dehydrogenase Inhibition in Fully Viable MDA-MB-231 Cells Induces Cytostatic Effects That Are Not Reversed by Exogenous Lactic Acid. Biomolecules 2021, 11, 1751. [Google Scholar] [CrossRef]
- Ma, G.; Li, C.; Zhang, Z.; Liang, Y.; Liang, Z.; Chen, Y.; Wang, L.; Li, D.; Zeng, M.; Shan, W.; et al. Targeted Glucose or Glutamine Metabolic Therapy Combined With PD-1/PD-L1 Checkpoint Blockade Immunotherapy for the Treatment of Tumors - Mechanisms and Strategies. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Shende, S.; Rathored, J.; Budhbaware, T. Role of Metabolic Transformation in Cancer Immunotherapy Resistance: Molecular Mechanisms and Therapeutic Implications. Discov. Oncol. 2025 161 2025, 16, 453. [Google Scholar] [CrossRef] [PubMed]
- Morotti, M.; Zois, C.E.; El-Ansari, R.; Craze, M.L.; Rakha, E.A.; Fan, S.J.; Valli, A.; Haider, S.; Goberdhan, D.C.I.; Green, A.R.; et al. Increased Expression of Glutamine Transporter SNAT2/SLC38A2 Promotes Glutamine Dependence and Oxidative Stress Resistance, and Is Associated with Worse Prognosis in Triple-Negative Breast Cancer. Br. J. Cancer 2021, 124, 494–505. [Google Scholar] [CrossRef]
- Huang, R.; Wang, H.; Hong, J.; Wu, J.; Huang, O.; He, J.; Chen, W.; Li, Y.; Chen, X.; Shen, K.; et al. Targeting Glutamine Metabolic Reprogramming of SLC7A5 Enhances the Efficacy of Anti-PD-1 in Triple-Negative Breast Cancer. Front. Immunol. 2023, 14. [Google Scholar] [CrossRef] [PubMed]
- Gauthier-Coles, G.; Bröer, A.; McLeod, M.D.; George, A.J.; Hannan, R.D.; Bröer, S. Identification and Characterization of a Novel SNAT2 (SLC38A2) Inhibitor Reveals Synergy with Glucose Transport Inhibition in Cancer Cells. Front. Pharmacol. 2022, 13. [Google Scholar] [CrossRef]
- Kanai, Y. Amino Acid Transporter LAT1 (SLC7A5) as a Molecular Target for Cancer Diagnosis and Therapeutics. Pharmacol. Ther. 2022, 230. [Google Scholar] [CrossRef]
- Bröer, S.; Bröer, S. Amino Acid Transporters as Targets for Cancer Therapy: Why, Where, When, and How. Int. J. Mol. Sci. 2020, Vol. 21(2020, 21), 1–20. [Google Scholar] [CrossRef]
- Martinez-Outschoorn, U.E.; Peiris-Pagés, M.; Pestell, R.G.; Sotgia, F.; Lisanti, M.P. Cancer Metabolism: A Therapeutic Perspective. Nat. Rev. Clin. Oncol. 2016 141 2016, 14, 11–31. [Google Scholar] [CrossRef]
- Vidula, N.; Yau, C.; Rugo, H.S. Glutaminase (GLS1) Gene Expression in Primary Breast Cancer. Breast Cancer 2023, 30, 1079–1084. [Google Scholar] [CrossRef]
- Gross, M.I.; Demo, S.D.; Dennison, J.B.; Chen, L.; Chernov-Rogan, T.; Goyal, B.; Janes, J.R.; Laidig, G.J.; Lewis, E.R.; Li, J.; et al. Antitumor Activity of the Glutaminase Inhibitor CB-839 in Triple-Negative Breast Cancer. Mol. Cancer Ther. 2014, 13, 890–901. [Google Scholar] [CrossRef]
- Harding, J.J.; Telli, M.; Munster, P.; Voss, M.H.; Infante, J.R.; DeMichele, A.; Dunphy, M.; Le, M.H.; Molineaux, C.; Orford, K.; et al. A Phase I Dose-Escalation and Expansion Study of Telaglenastat in Patients with Advanced or Metastatic Solid Tumors. Clin. Cancer Res. 2021, 27, 4994–5003. [Google Scholar] [CrossRef]
- Vasseur, S.; Guillaumond, F. Lipids in Cancer: A Global View of the Contribution of Lipid Pathways to Metastatic Formation and Treatment Resistance. Oncogenesis 2022, 11. [Google Scholar] [CrossRef]
- Yu, X.; Mi, S.; Ye, J.; Lou, G. Aberrant Lipid Metabolism in Cancer Cells and Tumor Microenvironment: The Player Rather than Bystander in Cancer Progression and Metastasis. J. Cancer 2021, 12, 7498–7506. [Google Scholar] [CrossRef] [PubMed]
- Germain, N.; Dhayer, M.; Boileau, M.; Fovez, Q.; Kluza, J.; Marchetti, P.; Germain, N.; Dhayer, M.; Boileau, M.; Fovez, Q.; et al. Lipid Metabolism and Resistance to Anticancer Treatment. Biol. 2020, Vol. 9 2020, 9, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Camarda, R.; Zhou, A.Y.; Kohnz, R.A.; Balakrishnan, S.; Mahieu, C.; Anderton, B.; Eyob, H.; Kajimura, S.; Tward, A.; Krings, G.; et al. Inhibition of Fatty Acid Oxidation as a Therapy for MYC-Overexpressing Triple-Negative Breast Cancer. Nat. Med. 2016, 22, 427–432. [Google Scholar] [CrossRef]
- Cai, X.X.; Zhang, Z.Z.; Yang, X.X.; Shen, W.R.; Yuan, L.W.; Ding, X.; Yu, Y.; Cai, W.Y. Unveiling the Impact of Lipid Metabolism on Triple-Negative Breast Cancer Growth and Treatment Options. Front. Oncol. 2025, 15, 1579423. [Google Scholar] [CrossRef] [PubMed]
- Wan, M.; Pan, S.; Shan, B.; Diao, H.; Jin, H.; Wang, Z.; Wang, W.; Han, S.; Liu, W.; He, J.; et al. Lipid Metabolic Reprograming: The Unsung Hero in Breast Cancer Progression and Tumor Microenvironment. Mol. Cancer 2025 241 2025, 24, 61. [Google Scholar] [CrossRef]
- Jiang, Y.; Qian, Z.; Wang, C.; Wu, D.; Liu, L.; Ning, X.; You, Y.; Mei, J.; Zhao, X.; Zhang, Y. Targeting B7-H3 Inhibition-Induced Activation of Fatty Acid Synthesis Boosts Anti-B7-H3 Immunotherapy in Triple-Negative Breast Cancer. J. Immunother. Cancer 2025, 13, 10924. [Google Scholar] [CrossRef]
- Al-Bahlani, S.; Al-Lawati, H.; Al-Adawi, M.; Al-Abri, N.; Al-Dhahli, B.; Al-Adawi, K. Fatty Acid Synthase Regulates the Chemosensitivity of Breast Cancer Cells to Cisplatin-Induced Apoptosis. Apoptosis 2017, 22, 865–876. [Google Scholar] [CrossRef]
- Serhan, H.A.; Bao, L.; Cheng, X.; Qin, Z.; Liu, C.J.; Heth, J.A.; Udager, A.M.; Soellner, M.B.; Merajver, S.D.; Morikawa, A.; et al. Targeting Fatty Acid Synthase in Preclinical Models of TNBC Brain Metastases Synergizes with SN-38 and Impairs Invasion. npj Breast Cancer 2024 101 2024, 10, 43. [Google Scholar] [CrossRef]
- Giró-Perafita, A.; Palomeras, S.; Lum, D.H.; Blancafort, A.; Viñas, G.; Oliveras, G.; Pérez-Bueno, F.; Sarrats, A.; Welm, A.L.; Puig, T. Preclinical Evaluation of Fatty Acid Synthase and EGFR Inhibition in Triple-Negative Breast Cancer. Clin. Cancer Res. 2016, 22, 4687–4697. [Google Scholar] [CrossRef] [PubMed]
- Camarda, R.; Zhou, A.Y.; Kohnz, R.A.; Balakrishnan, S.; Mahieu, C.; Anderton, B.; Eyob, H.; Kajimura, S.; Tward, A.; Krings, G.; et al. Inhibition of Fatty Acid Oxidation as a Therapy for MYC-Overexpressing Triple-Negative Breast Cancer. Nat. Med. 2016 224 2016, 22, 427–432. [Google Scholar] [CrossRef]
- Tan, Z.; Zou, Y.; Zhu, M.; Luo, Z.; Wu, T.; Zheng, C.; Xie, A.; Wang, H.; Fang, S.; Liu, S.; et al. Carnitine Palmitoyl Transferase 1A Is a Novel Diagnostic and Predictive Biomarker for Breast Cancer. BMC Cancer 2021, 21, 409. [Google Scholar] [CrossRef]
- Li, C.; Gao, T.; Zhao, Q.; Li, Z.; Wang, Z.; Ding, S.; Zhang, M.; Qin, Y.; Xue, X.; Zhang, X.; et al. Inhibition of CPT1A Activates the CGAS/STING Pathway to Enhance Neutrophil-Mediated Tumor Abrogation in Triple-Negative Breast Cancer. Cancer Lett. 2025, 633, 217991. [Google Scholar] [CrossRef]
- Rasmi, R.R.; Kovatich, R.; Farley, A.; Sakthivel, K.M.; Takiar, V.; Sertorio, M. Targeting SREBP2 in Cancer Progression: Molecular Mechanisms, Oncogenic Crosstalk, and Therapeutic Interventions. Cell. Signal. 2025, 135, 112044. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.X.; Zhang, Z.Z.; Yang, X.X.; Shen, W.R.; Yuan, L.W.; Ding, X.; Yu, Y.; Cai, W.Y. Unveiling the Impact of Lipid Metabolism on Triple-Negative Breast Cancer Growth and Treatment Options. Front. Oncol. 2025, 15. [Google Scholar] [CrossRef]
- Liu, Z.; Sun, Y.; Hong, H.; Zhao, S.; Zou, X.; Ma, R.; Jiang, C.; Wang, Z.; Li, H.; Liu, H. 3-Bromopyruvate Enhanced Daunorubicin-Induced Cytotoxicity Involved in Monocarboxylate Transporter 1 in Breast Cancer Cells. Am. J. Cancer Res. 2015, 5, 2673–2685. [Google Scholar] [PubMed]
- Zheng, H.; Siddharth, S.; Parida, S.; Wu, X.; Sharma, D. Tumor Microenvironment: Key Players in Triple Negative Breast Cancer Immunomodulation. Cancers (Basel). 2021, 13. [Google Scholar] [CrossRef]
- Yan, S.; Sun, X.; Wang, K. From Cold to Hot Tumors: Feasibility of Applying Therapeutic Insights to TNBC. Discov. Oncol. 2025, 16. [Google Scholar] [CrossRef]
- Meyer, L.; Jackson, H.W.; Eling, N.; Zhao, S.; Usui, G.; Dakhli, H.; Schraml, P.; Dettwiler, S.; Elfgen, C.; Varga, Z.; et al. A Stratification System for Breast Cancer Based on Basoluminal Tumor Cells and Spatial Tumor Architecture. Cancer Cell 2025, 43, 1637–1655.e9. [Google Scholar] [CrossRef]
- Gruosso, T.; Gigoux, M.; Manem, V.S.K.; Bertos, N.; Zuo, D.; Perlitch, I.; Saleh, S.M.I.; Zhao, H.; Souleimanova, M.; Johnson, R.M.; et al. Spatially Distinct Tumor Immune Microenvironments Stratify Triple-Negative Breast Cancers. J. Clin. Invest. 2019, 129, 1785–1800. [Google Scholar] [CrossRef]
- Sharma, P. Biology and Management of Patients With Triple-Negative Breast Cancer. Oncologist 2016, 21, 1050–1062. [Google Scholar] [CrossRef] [PubMed]
- Terragno, M.; Vetrova, A.; Semenov, O.; Sayan, A.E.; Kriajevska, M.; Tulchinsky, E. Mesenchymal–Epithelial Transition and AXL Inhibitor TP-0903 Sensitise Triple-Negative Breast Cancer Cells to the Antimalarial Compound, Artesunate. Sci. Rep. 2024, 14, 425. [Google Scholar] [CrossRef] [PubMed]
- Haque, M.; Shyanti, R.K.; Mishra, M.K. Targeted Therapy Approaches for Epithelial-Mesenchymal Transition in Triple Negative Breast Cancer. Front. Oncol. 2024, 14. [Google Scholar] [CrossRef]
- Zajac, O.; Leclere, R.; Nicolas, A.; Meseure, D.; Marchiò, C.; Vincent-Salomon, A.; Roman-Roman, S.; Schoumacher, M.; Dubois, T. AXL Controls Directed Migration of Mesenchymal Triple-Negative Breast Cancer Cells. Cells 2020, 9, 247. [Google Scholar] [CrossRef]
- Tian, J.; Al Raffa, F.; Dai, M.; Moamer, A.; Khadang, B.; Hachim, I.Y.; Bakdounes, K.; Ali, S.; Jean-Claude, B.; Lebrun, J.-J. Dasatinib Sensitises Triple Negative Breast Cancer Cells to Chemotherapy by Targeting Breast Cancer Stem Cells. Br. J. Cancer 2018, 119, 1495–1507. [Google Scholar] [CrossRef] [PubMed]
- da Motta, L.L.; Ledaki, I.; Purshouse, K.; Haider, S.; De Bastiani, M.A.; Baban, D.; Morotti, M.; Steers, G.; Wigfield, S.; Bridges, E.; et al. The BET Inhibitor JQ1 Selectively Impairs Tumour Response to Hypoxia and Downregulates CA9 and Angiogenesis in Triple Negative Breast Cancer. Oncogene 2017, 36, 122–132. [Google Scholar] [CrossRef]
- Kai, M.; Kanaya, N.; Wu, S. V.; Mendez, C.; Nguyen, D.; Luu, T.; Chen, S. Targeting Breast Cancer Stem Cells in Triple-Negative Breast Cancer Using a Combination of LBH589 and Salinomycin. Breast Cancer Res. Treat. 2015, 151, 281–294. [Google Scholar] [CrossRef]
- Yuan, L.; Zhu, Y.; Guan, G.; Liu, M. Napabucasin Targets Resistant Triple Negative Breast Cancer through Suppressing STAT3 and Mitochondrial Function. Cancer Chemother. Pharmacol. 2025, 95, 51. [Google Scholar] [CrossRef]
- Ferrari-Amorotti, G.; Chiodoni, C.; Shen, F.; Cattelani, S.; Soliera, A.R.; Manzotti, G.; Grisendi, G.; Dominici, M.; Rivasi, F.; Colombo, M.P.; et al. Suppression of Invasion and Metastasis of Triple-Negative Breast Cancer Lines by Pharmacological or Genetic Inhibition of Slug Activity. Neoplasia 2014, 16, 1047–1058. [Google Scholar] [CrossRef]
- Prasanna, T.; Malik, L.; McCuaig, R.D.; Tu, W.J.; Wu, F.; Lim, P.S.; Tan, A.H.Y.; Dahlstrom, J.E.; Clingan, P.; Moylan, E.; et al. A Phase 1 Proof of Concept Study Evaluating the Addition of an LSD1 Inhibitor to Nab-Paclitaxel in Advanced or Metastatic Breast Cancer (EPI-PRIMED). Front. Oncol. 2022, 12. [Google Scholar] [CrossRef]
- Suárez–Nájera, L.E.; Chanona–Pérez, J.J.; Valdivia–Flores, A.; Marrero–Rodríguez, D.; Salcedo–Vargas, M.; García–Ruiz, D.I.; Castro– Reyes, M.A. Morphometric Study of Adipocytes on Breast Cancer by Means of Photonic Microscopy and Image Analysis. Microsc. Res. Tech. 2018, 81, 240–249. [Google Scholar] [CrossRef]
- Yang, Z.; Zeng, H.; Li, J.; Zeng, N.; Zhang, Q.; Hou, K.; Li, J.; Yu, J.; Wu, Y. Dissecting the Emerging Role of Cancer-Associated Adipocyte-Derived Cytokines in Remodeling Breast Cancer Progression. Heliyon 2024, 10. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Wang, Z.; Hong, J.; Wu, J.; Huang, O.; He, J.; Chen, W.; Li, Y.; Chen, X.; Shen, K. Targeting Cancer-Associated Adipocyte-Derived CXCL8 Inhibits Triple-Negative Breast Cancer Progression and Enhances the Efficacy of Anti-PD-1 Immunotherapy. Cell Death Dis. 2023, 14, 703. [Google Scholar] [CrossRef]
- Liu, Y.; Tiruthani, K.; Wang, M.; Zhou, X.; Qiu, N.; Xiong, Y.; Pecot, C. V.; Liu, R.; Huang, L. Tumor-Targeted Gene Therapy with Lipid Nanoparticles Inhibits Tumor-Associated Adipocytes and Remodels the Immunosuppressive Tumor Microenvironment in Triple-Negative Breast Cancer. Nanoscale Horizons 2021, 6, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.; Camarda, R.; Malkov, S.; Zimmerman, L.J.; Manning, S.; Aran, D.; Beardsley, A.; Van de Mark, D.; Nakagawa, R.; Chen, Y.; et al. Tumor Cell-Adipocyte Gap Junctions Activate Lipolysis and Contribute to Breast Tumorigenesis. Nat. Commun. 2025, 16, 7438. [Google Scholar] [CrossRef] [PubMed]
- Yin, D.; Fang, N.; Zhu, Y.; Bao, X.; Yang, J.; Zhang, Q.; Wang, R.; Huang, J.; Wu, Q.; Ma, F.; et al. Adipocytes-Induced ANGPTL4/KLF4 Axis Drives Glycolysis and Metastasis in Triple-Negative Breast Cancer. J. Exp. Clin. Cancer Res. 2025, 44, 192. [Google Scholar] [CrossRef]
- Nguyen, H.P.; An, K.; Ito, Y.; Kharbikar, B.N.; Sheng, R.; Paredes, B.; Murray, E.; Pham, K.; Bruck, M.; Zhou, X.; et al. Implantation of Engineered Adipocytes Suppresses Tumor Progression in Cancer Models. Nat. Biotechnol. 2025. [Google Scholar] [CrossRef]
- Yang, D.; Liu, J.; Qian, H.; Zhuang, Q. Cancer-Associated Fibroblasts: From Basic Science to Anticancer Therapy. Exp. Mol. Med. 2023, 55, 1322–1332. [Google Scholar] [CrossRef]
- Brogna, M.R.; Varone, V.; DelSesto, M.; Ferrara, G. The Role of CAFs in Therapeutic Resistance in Triple Negative Breast Cancer: An Emerging Challenge. Front. Mol. Biosci. 2025, 12. [Google Scholar] [CrossRef]
- Takai, K.; Le, A.; Weaver, V.M.; Werb, Z. Targeting the Cancer-Associated Fibroblasts as a Treatment in Triple-Negative Breast Cancer. Oncotarget 2016, 7, 82889–82901. [Google Scholar] [CrossRef]
- Abe, K.; Watabe, T.; Kaneda-Nakashima, K.; Shirakami, Y.; Kadonaga, Y.; Naka, S.; Ooe, K.; Toyoshima, A.; Giesel, F.; Usui, T.; et al. Evaluation of Targeted Alpha Therapy Using [211At]FAPI1 in Triple-Negative Breast Cancer Xenograft Models. Int. J. Mol. Sci. 2024, 25, 11567. [Google Scholar] [CrossRef] [PubMed]
- Qin, W.; Chen, B.; Li, X.; Zhao, W.; Wang, L.; Zhang, N.; Wang, X.; Luo, D.; Liang, Y.; Li, Y.; et al. Cancer-Associated Fibroblasts Secrete CSF3 to Promote TNBC Progression via Enhancing PGM2L1-Dependent Glycolysis Reprogramming. Cell Death Dis. 2025, 16, 249. [Google Scholar] [CrossRef] [PubMed]
- Xian, P.; Zou, L.; Zhang, J.; Pan, X.; Song, Y.; Nan, Y.; Pu, Q.; Liu, H.; Green, D.; Ni, S.; et al. Precision Targeted Cancer-Associated Fibroblast Nano-Regulator Enhanced Chemo-Immunotherapy for Triple-Negative Breast Cancer. Biomaterials 2026, 326, 123679. [Google Scholar] [CrossRef]
- Xu, T.; Zhang, H.; Yang, B.B.; Qadir, J.; Yuan, H.; Ye, T. Tumor-Infiltrating Immune Cells State-Implications for Various Breast Cancer Subtypes. Front. Immunol. 2025, 16. [Google Scholar] [CrossRef]
- Amara, D.; Wolf, D.M.; van ’t Veer, L.; Esserman, L.; Campbell, M.; Yau, C. Co-Expression Modules Identified from Published Immune Signatures Reveal Five Distinct Immune Subtypes in Breast Cancer. Breast Cancer Res. Treat. 2017, 161, 41–50. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Li, S.; Xue, J.; Qi, M.; Liu, X.; Huang, Y.; Hu, J.; Dong, H.; Ling, K. PD-L1 Tumor-Intrinsic Signaling and Its Therapeutic Implication in Triple-Negative Breast Cancer. JCI Insight 2021, 6. [Google Scholar] [CrossRef]
- Liu, X.; Zhuang, C.; Liu, L.; Xiong, L.; Xie, X.; He, P.; Li, J.; Wei, B.; Yan, X.; Tian, T.; et al. Exploratory Phase II Trial of an Anti-PD-1 Antibody Camrelizumab Combined with a VEGFR-2 Inhibitor Apatinib and Chemotherapy as a Neoadjuvant Therapy for Triple-Negative Breast Cancer (NeoPanDa03): Efficacy, Safety and Biomarker Analysis. Signal Transduct. Target. Ther. 2025, 10, 237. [Google Scholar] [CrossRef]
- Stucchi, S.; Borea, R.; Garcia-Recio, S.; Zingarelli, M.; Rädler, P.D.; Camerini, E.; Marnata Pellegry, C.; O’Connor, S.; Earp, H.S.; Carey, L.A.; et al. B7-H3 and CSPG4 Co-Targeting as Pan-CAR-T Cell Treatment of Triple-Negative Breast Cancer. J. Immunother. Cancer 2025, 13, e011533. [Google Scholar] [CrossRef]
- Zhou, M.; Chen, M.; Shi, B.; Di, S.; Sun, R.; Jiang, H.; Li, Z. Radiation Enhances the Efficacy of EGFR-Targeted CAR-T Cells against Triple-Negative Breast Cancer by Activating NF-ΚB/Icam1 Signaling. Mol. Ther. 2022, 30, 3379–3393. [Google Scholar] [CrossRef] [PubMed]
- Pierini, S.; Gabbasov, R.; Oliveira-Nunes, M.C.; Qureshi, R.; Worth, A.; Huang, S.; Nagar, K.; Griffin, C.; Lian, L.; Yashiro-Ohtani, Y.; et al. Chimeric Antigen Receptor Macrophages (CAR-M) Sensitize HER2+ Solid Tumors to PD1 Blockade in Pre-Clinical Models. Nat. Commun. 2025, 16, 706. [Google Scholar] [CrossRef]
- Zhang, X.; Goedegebuure, S.P.; Chen, M.Y.; Mishra, R.; Zhang, F.; Yu, Y.Y.; Singhal, K.; Li, L.; Gao, F.; Myers, N.B.; et al. Neoantigen DNA Vaccines Are Safe, Feasible, and Induce Neoantigen-Specific Immune Responses in Triple-Negative Breast Cancer Patients. Genome Med. 2024, 16, 131. [Google Scholar] [CrossRef] [PubMed]
- Vora, H.H. Identification of Extra Cellular Matrix (ECM) Genes in Triple Negative Breast Cancer. Asian Pacific J. Cancer Biol. 2025, 10, 301–307. [Google Scholar] [CrossRef]
- Al-Temaimi, R.; Ahmad, R.; Al-Mulla, F. MMP14 and DDR2 Are Potential Molecular Markers for Metastatic Triple-Negative Breast Cancer. Sci. Rep. 2025, 15, 21630. [Google Scholar] [CrossRef]
- Festari, M.F.; Jara, E.; Costa, M.; Iriarte, A.; Freire, T. Truncated O-Glycosylation in Metastatic Triple-Negative Breast Cancer Reveals a Gene Expression Signature Associated with Extracellular Matrix and Proteolysis. Sci. Rep. 2024, 14, 1809. [Google Scholar] [CrossRef]
- Das, K.; Paul, S.; Ghosh, A.; Gupta, S.; Mukherjee, T.; Shankar, P.; Sharma, A.; Keshava, S.; Chauhan, S.C.; Kashyap, V.K.; et al. Extracellular Vesicles in Triple–Negative Breast Cancer: Immune Regulation, Biomarkers, and Immunotherapeutic Potential. Cancers (Basel). 2023, 15, 4879. [Google Scholar] [CrossRef]
- Hopkins, B.; Torres, M. Radiotherapy in Triple Negative Breast Cancer – Current Standards and Future Directions. Curr. Breast Cancer Rep. 2025, 17, 1. [Google Scholar] [CrossRef]
- Sun, H.; Cai, H.; Xu, C.; Zhai, H.; Lux, F.; Xie, Y.; Feng, L.; Du, L.; Liu, Y.; Sun, X.; et al. AGuIX Nanoparticles Enhance Ionizing Radiation-Induced Ferroptosis on Tumor Cells by Targeting the NRF2-GPX4 Signaling Pathway. J. Nanobiotechnology 2022, 20, 449. [Google Scholar] [CrossRef]
- Li, G.; Lin, X.; Wang, X.; Cai, L.; Liu, J.; Zhu, Y.; Fu, Z. Enhancing Radiosensitivity in Triple-Negative Breast Cancer through Targeting ELOB. Breast Cancer 2024, 31, 426–439. [Google Scholar] [CrossRef] [PubMed]
- AN, J.; CHU, K.; ZHOU, Q.; MA, H.; HE, Q.; ZHANG, Y.; LV, J.; WEI, H.; LI, M.; WU, Z.; et al. Radiosensitizer-Based Injectable Hydrogel for Enhanced Radio-Chemotherapy of TNBC. Chinese J. Anal. Chem. 2024, 52, 100414. [Google Scholar] [CrossRef]
- Sankaranarayanan, R.A.; Florea, A.; Allekotte, S.; Vogg, A.T.J.; Maurer, J.; Schäfer, L.; Bolm, C.; Terhorst, S.; Classen, A.; Bauwens, M.; et al. Correction: PARP Targeted Auger Emitter Therapy with [125I]PARPi-01 for Triple-Negative Breast Cancer. EJNMMI Res. 2023, 13. [Google Scholar] [CrossRef] [PubMed]
Table 1.
List of current and prematurely terminated clinical trials.
| TRIAL | INVESTIGATIONAL DRUG | TARGET | YEAR | PHASE | STATE | RESULTS | Reference |
|---|---|---|---|---|---|---|---|
| FASCINATE-N (ClinicalTrials.gov ID NCT05582499) |
New targeted drugs | PARPi,Trop-2, Antibody–drug conjugates, CDK 4/6 inhibitors, PD-L1 mAb, HER2 inhibitor, anti-angiogenic agents | 2022-2028 (estimated) | II | Recruiting | N.A. | [25] |
| TROPION-Breast05 (ClinicalTrials.gov ID: NCT06103864) | Durvalumab (Imfinzi) | Anti PD-L1 | 2023-2029 (estimated) | III | Recruiting | N.A. | [34] |
| NCT03170960 | Atezolizumab (Tecentriq) | Anti PD-L1 | 2017-2027 (estimated) | I | Active, not recruiting | N.A. | N.A. |
| PAveMenT (ClinicalTrials.gov ID: NCT04360941) | Avelumab (Bavencio) | Anti PD-L1 | 2026-2026 (estimated) | I | Recruiting | N.A. | N.A. |
| NCT02936102 | FAZ053 | Anti PD-L1 | 2016-2024 | I | Terminated | N.A. | N.A. |
| NCT04916002 | Cemiplimab | Anti PD-1 | 2021-2024 | II | Terminated | N.A. | N.A. |
| NCT03549000 |
PDR001 |
Anti PD-1 | 2018-2022 | I | Terminated | N.A. | N.A. |
| PARTNER (ClinicalTrials.gov ID NCT03150576) | Olaparib | PARP | 2016-2034 (estimated) | II-III | Recruiting | N.A. | [86,87,88] |
| NCT05933265 | LP-184 | PARP | 2023-2025 (estimated) | I-II | Recruiting | N.A. | [89] |
| NCT03875313 | Telaglenastat (CB-839), Talazoparib | PARP | 2019-2022 | I-II | Terminated | N.A. | N.A. |
| NCT03801369 | Olaparib | PARP | 2018-2024 | II | Terminated | N.A. | [90] |
| NCT04916002 | Vidutolimod, Cemiplimab | PARP | 2021-2024 | II | Terminated | N.A. | N.A. |
| NCT05252390 | NUV-868, Olaparib, Enzalutamide | PARP | 2022-2024 | I | Terminated | N.A. | N.A. |
| NCT02419495 | Selinexor (KPT-330) | PARP | 2015-2024 | I | Terminated | N.A. | N.A. |
| NCT02627430 | Talazoparib, Hsp90 Inhibitor AT13387 | PARP | 2016-2019 | I | Withdrawn | N.A. | N.A. |
| NCT07046455 | Sacituzumab Govitecan (SG) and PET Probes | Trop-2 | 2025-2027 (estimated) | N.A. | Recruiting | N.A. | N.A. |
| FUTURE2.0 (ClinicalTrials.gov ID NCT05749588) | SHR-A1811, TROP2 ADC, BP102 | Trop-2 | 2023-2026 (estimated) | II | Recruiting | N.A. | N.A. |
| BALISTA (ClinicalTrials.gov ID NCT06793332) | IvoneScimab, Trop2 ADC | Trop-2 | 2024-2027 (estimated) | II | Recruiting | N.A. | [91,92,93,94] |
| NCT06851299 | Trop2-ADC monotherapy | Trop-2 | 2025-2028 (estimated) | II | Recruiting | N.A. | N.A. |
| MK-2870-011/ TroFuse-011 (ClinicalTrials.gov ID NCT06841354) |
Sacituzumab Tirumotecan (Sac-TMT, MK-2870) and Pembrolizumab (MK-3475) | Trop-2 |
2025-2030 (estimated) | III | Recruiting | N.A. | N.A. |
| NCT06878625 | Trop-2 ADC Combination Therapy | Trop-2 | 2024-2027 (estimated) | II | Recruiting | N.A. | N.A. |
| NCT06649331 | Anti Trop-2 antibody-conjugated drugs (ADCs) | Trop-2 | 2024-2027 (estimated) | II | Recruiting | N.A. | N.A. |
| TROPION-DM (ClinicalTrials.gov ID NCT06974604) | Dexamethasone | Trop-2 | 2025-2029 (estimated) | II | Recruiting | N.A. | N.A. |
| NCT06103864 |
Dato-DXd | Trop-2 |
2023-2029 (estimated) | III | Recruiting | N.A. | [34] |
| NCT03901469 | ZEN003694, Talazoparib | Trop-2 | 2019-2024 | II | Terminated | N.A. | [95] |
| ASPRIA (ClinicalTrials.gov ID NCT04434040) | Sacituzumab govitecan, Atezolizumab |
Trop-2 | 2020-2027 (estimated) | II | Recruiting | N.A. | N.A. |
| NeoSACT (ClinicalTrials.gov ID: NCT04877821) | Anlotinib (FOCUS V) | Antiangiogenic agent | 2021-2025 | II | Active, not recruiting | pCR: 69% MRD: 86.2% 2y EFS: 92.4% |
[66] |
| NCT06724263 | B1962 | Antiangiogenic agent | 2024-2026 (estimated) | II | Not yet recruiting | N.A. | N.A. |
| NCT06189209 | Tenalisib | PI3K inhibitor | 2024-2026 (estimated) | II | Recruiting | N.A. | N.A. |
| NCT03218826 | AZD8186 | PI3K inhibitor | 2024-2026 (estimated) | I | Active, not recruiting | MTD: NR Anemia: 57% Diarrhea: 43% Fatigue: 43% |
[71] |
| SABINA (ClinicalTrials.gov ID NCT05810870) | MEN1611 | PI3K inhibitor | 2023-2027 (estimated) | II | Recruiting | N.A. | N.A. |
| BCTOP-T-M03 (ClinicalTrials.gov ID: NCT05954442) | Everolimus (Afinitor) | PI3K inhibitor | 2023-2026 (estimated) | III | Recruiting | N.A. | N.A. |
| NCT01918306 | GDC-0941 | PI3K inhibitor | 2013-2015 | I-II | Terminated | N.A. | N.A. |
| NCT02457910 | Taselisib | PI3K inhibitor | 2015-2022 | I-II | Terminated | N.A. | |
| NCT04216472 | Alpelisib | PI3K inhibitor | 2020-2025 | II | Terminated | N.A. | N.A. |
| NCT02476955 | ARQ-092 | PI3K inhibitor | 2015-2019 | I | Terminated | N.A. | N.A. |
| NCT03090165 | Bicalutamide (Casodex) | AR inhibitor | 2018-2025 (estimated) | I-II | Recruiting | N.A. | N.A. |
| NCT07016399 | Darolutamide (Nubeqa) | AR inhibitor | 2025-2033 (estimated) | II | Recruiting | N.A. | N.A. |
| CAREGIVER (ClinicalTrials.gov ID: NCT05067530) | Palbociclib (Ibrance) | CDK 4/6 inhibitor | 2022-2026 (estimated) | II | Not yet recruiting | N.A. | N.A. |
| CHARGE (ClinicalTrials.gov ID: NCT04315233) | Ribociclib | CDK 4/6 inhibitor | 2021-2026 (estimated) | I | Recruiting | N.A. | N.A. |
| NCT02978716 | Trilaciclib | CDK 4/6 inhibitor | 2017-2020 | II | Terminated | See publication | [96,97] |
| NCT05113966 | Trilaciclib | CDK 4/6 inhibitor | 2021-2024 | II | Terminated | PFS: 4.1 months ORR: 23.3% CBR: 46.7% DoR: 8.8 months OS: 15.9% |
N.A. |
| NCT03519178 | PF-06873600 | CDK 4/6 inhibitor | 2018-2024 | I-II | Terminated | N.A. | |
| NCT06264921 | NKT3447 | CDK 4/6 Inhibitor | 2024-2025 | I | Terminated | N.A. | N.A. |
N.A. = not available. pCR = pathological Complete Response. MRD = Minimal Residual Disease. MTD = Maximum Tolerated Dose. NR = Not Reached. EFS = Event-Free sSurvival. PFS = Progression-Free Survival. ORR = Overall Response Rate. CBR = Clinical Benefit Rate. DoR = Duration of Response. OS = Overall Survival.
Table 2.
New possible targets identified by omics with the Elicit AI research assistant (details in the text).
Table 2.
New possible targets identified by omics with the Elicit AI research assistant (details in the text).
| Gene Symbol | Protein Name | UniProt link |
|---|---|---|
| GGH | Gamma-glutamyl hydrolase | Q92820 (https://www.uniprot.org/uniprotkb/Q92820/entry) |
| TYMS | Thymidylate synthase | P04818 (https://www.uniprot.org/uniprotkb/P04818/entry) |
| PTK6 | Protein-tyrosine kinase 6 (BRK) | Q13882 (https://www.uniprot.org/uniprotkb/Q13882/entry) |
| TOP1MT | DNA topoisomerase I, mitochondrial | Q969P6 (https://www.uniprot.org/uniprotkb/Q969P6/entry) |
| SMO | Smoothened receptor | Q99835 (https://www.uniprot.org/uniprotkb/Q99835/entry) |
| CSF1R | Colony-stimulating factor 1 receptor | P07333 (https://www.uniprot.org/uniprotkb/P07333/entry) |
| EPHB3 | Ephrin type-B receptor 3 | P54753 (https://www.uniprot.org/uniprotkb/P54753/entry) |
| TRIB1 | Tribbles pseudokinase 1 | Q96RU8 (https://www.uniprot.org/uniprotkb/Q96RU8/entry) |
| LAD1 | Ladinin-1 | O00515 (https://www.uniprot.org/uniprotkb/O00515/entry) |
Table 4.
Altered metabolic pathways in TNBC.
| Altered metabolic pathway | Main molecular targets | Role in TNBC | Targeting strategies | Reference |
|---|---|---|---|---|
| Enhanced glycolysis (Warburg effect) | GLUT-1 | Increased glucose uptake; high proliferative index, high histological grade, drug resistance and basal-like phenotype | STF-31, WZB-117, BAY-876, shRNA | [156,157,158,159] |
| HK2 | Promotes ATP production and apoptosis resistance via interaction with VDAC | 2-deoxy-D-glucose (2-DG), 3-bromopyruvate, lonidamine, metformin | [164,167,168,202] | |
| LDH (LDH-A isoform) |
Sustains glycolysis under hypoxia; promotes invasion, immune evasion and acidic tumor microenvironment | FX11, GNE-140 | [174,175] | |
| Hypoxia-driven metabolic regulation | HIF-1α | Transcriptionally upregulates HK2 and LDH, enabling survival under oxygen deprivation | Indirect targeting through glycolytic inhibition | [62,169] |
| Glutamine addiction | Glutamine transporters (SNAT2/SLC38A2, SLC7A5) | Increased glutamine uptake, increased TCA cycle, nucleotide biosynthesis and redox homeostasis | Specific transporter inhibitors | [178,179,182] |
| GLS1 | Fuels TCA cycle, ATP production and antioxidant defenses | Telaglenastat | [184,186] | |
| De novo lipogenesis | FASN | Supports tumor growth, aggressiveness and therapy resistance; overexpression correlates with poor prognosis | TVB-2640, C75 | [195,196] |
| Fatty acid oxidation (FAO) | CPT1A | Promotes adaptation to nutrient and oxygen stress | Etomoxir, perhexiline | [198,199] |
| Lipid metabolism transcriptional control | SREBPs | Master regulators of lipid biosynthesis; frequently upregulated in TNBC | No effective validated inhibitors | [193,200] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



