Submitted:
09 January 2026
Posted:
09 January 2026
You are already at the latest version
Abstract
Background: Pressure injuries (PIs) in surgical settings is a major patient safety concern, contributing to increased morbidity, prolonged hospitalization, and greater healthcare costs. Prolonged immobility, anesthesia, surgical positioning, and device-related pressure place perioperative patients at particularly high risk. This mini review synthesizes contemporary literature on PIs prevention and risk assessment in perioperative environments, with emphasis on the use of specialized tools, particularly the Munro Scale and evidence-based strategies such as optimized support surfaces, positioning, moisture management, and early skin assessment. Comparative findings indicate that the Munro Scale offers superior predictive accuracy for surgical patients compared with the widely used Braden Scale. The review also highlights persistent challenges, including limited implementation, lack of standardization, and insufficient knowledge among perioperative staff. A multidisciplinary, proactive, and individualized approach is essential to effective PI prevention, while future work should prioritize EHR-integrated risk tools, enhanced staff training, and broader adoption of periopera-tive prevention bundles.
Keywords:
pressure injury
; perioperative care
; surgical patients
; munro scale
; risk assessment
; prevention
1. Introduction
PIs represent a major global health concern, particularly within hospital and perioperative settings. Also known as pressure ulcers, PIs are defined as localized damage to the skin and/or underlying tissue resulting from sustained pressure, shear, or a combination of both, leading to ischemia and tissue necrosis [1].
The incidence of perioperative or intraoperative pressure injuries varies widely across surgical populations and study designs. Operating room–acquired pressure injuries have been reported in approximately 5.8% of surgical patients in a Turkish cross-sectional study [2]. Among older adults aged ≥65 years, perioperative cohorts demonstrate incidence rates of around 18.8%, highlighting the increased vulnerability of geriatric surgical patients [3]. In high-risk surgical populations, intraoperative acquired pressure injuries (IAPI) have been reported at approximately 15.6% among orthopedic surgical patients, based on a prospective observational study involving 422 participants [4], and nearly 25% among open-heart surgical patients according to prospective studies and meta-analytic findings [5]. Consequently, large-scale reviews and expert commentaries summarize a broad overall incidence range of 0.3%–66%, reflecting heterogeneity in surgery type, procedural duration, patient-specific risk factors, and methodological variations in PI classification [6].
Surgical patients are often immobilized for extended periods, increasing the risk of excessive pressure on bony prominences such as the sacrum, heels, scapula, and face, depending on intraoperative positioning. In addition, the use of intraoperative medical devices, such as headrests, ECG cables, and body supports, can contribute to medical device–related pressure injuries [7,8]. A retrospective analysis further identified low preoperative albumin levels and elevated lactate concentrations as significant independent predictors of postoperative pressure injuries [9]. Collectively, these risk factors underscore the importance of timely perioperative assessment and tailored preventive strategies.
Despite technological advancements and improvements in surgical safety, intraoperative PIs remain under-monitored and frequently excluded from standard postoperative assessments. Consequently, PIs development contributes to increased morbidity, prolonged hospital stays, and higher healthcare expenditures [10,11,12]. Beyond physical complications, PIs also exert profound psychological and social impacts, including anxiety, depression, and reduced self-esteem, especially when they impair mobility or result in long-term dependency [13,14].
Given these multifactorial risks and consequences, adopting an evidence-based, proactive, and interdisciplinary approach is crucial to minimize PIs occurrence in perioperative care. Accordingly, this mini review synthesizes the current scientific evidence on PIs prevention and measurement strategies in perioperative settings, while evaluating the comparative effectiveness of the Munro Scale and Braden Scale as clinical risk assessment tools guiding nursing decision-making.
2. Data Source, Search and Extraction
This mini review utilized an integrative approach to synthesize empirical and guideline-based evidence related to perioperative pressure injury prevention and risk assessment. The literature search encompassed studies published between 2010 and 2025 and was conducted using a structured keyword strategy.
Searches were performed in PubMed, Scopus, and CINAHL using the Boolean operators (“pressure injury” OR “pressure ulcer”) AND (“perioperative” OR “intraoperative” OR “surgical patients”) AND (“prevention” OR “assessment” OR “Munro Scale” OR “Braden Scale”). Inclusion criteria comprised peer-reviewed original studies, systematic reviews, meta-analyses, and clinical guidelines published in English, while studies focusing exclusively on non-surgical or ICU-based populations were excluded.
A thematic analysis framework was applied to categorize the evidence into theree themes: (1) preoperative prevention, (2) intraoperative prevention, (3) postoperative prevention. Evidence synthesis into narrative approach.
3. Pressure Injury Prevention in Perioperative Setting
Perioperative PIs have a multifactorial etiology, and both patient-related and procedure-related characteristics significantly contribute to risk. Several studies have highlighted that patient-related intrinsic factors such as advanced age, poor nutritional status, low serum albumin levels, comorbid conditions (e.g., diabetes mellitus, cardiovascular and respiratory diseases), and reduced mobility increase susceptibility to pressure injuries by diminishing tissue tolerance to sustained pressure and shear forces [15,16]. Furthermore, procedure-related factors including the duration and type of surgery and anesthesia have been consistently identified as major contributors; prolonged operative time is associated with higher incidence of PIs due to extended periods of immobility and sustained mechanical load on bony prominences [3,17]. Intraoperative hemodynamic instability, such as episodes of hypotension and significant blood loss, further exacerbates tissue ischemia and predisposes patients to injury [18,19]. Additionally, characteristics of intraoperative positioning and the quality of support surfaces influence focal pressure distribution and shear forces, increasing susceptibility in areas such as the sacrum, heels, and other bony prominences [15,17].
The fundamental principle of PIs prevention is the early identification of risk factors and the implementation of systematic, continuous, and evidence-based preventive interventions [10]. These preventive efforts span three key perioperative phases: preoperative, intraoperative, and postoperative.
3.1. Preoperative Phase
The preoperative phase is essential for establishing baseline PIs risk and initiating proactive preventive measures before surgery. Patients undergoing surgical procedures are at increased risk of developing PIs due to prolonged immobility, reduced sensation under anesthesia, and exposure to positioning devices, factors that can compromise tissue perfusion and skin integrity if not anticipated [20].
The assessment practices are essential to early detection of existing skin compromise and perioperative PIs risk, as evidence indicates that prevention depends heavily on early and accurate risk assessment of patients at risk for PIs [21]. A comprehensive baseline skin assessment should be conducted preoperatively, documenting any existing redness, moisture-associated skin damage, tears, fragile skin, or other abnormalities that may predispose patients to pressure injury development (Figure 1). Such structured skin assessments provide critical clinical information beyond standardized risk scales and ensure subtle skin changes are captured at the earliest opportunity [22]. However, integration of PI risk assessment into preoperative checklists ensures that PI screening is embedded within established surgical safety workflows, including anesthesia and surgical time-outs. Embedding these assessments into safety checklists promotes consistency and reduces the risk that opportunities for intervention are overlooked in high-pressure clinical environments [23]. These tools provide a structured and evidence-based framework for early risk detection and facilitate effective communication among perioperative team members to guide risk-based planning
During this period, a comprehensive risk assessment should be conducted to categorize patients as low, moderate, or high risk, enabling clinicians to implement proportionate and targeted interventions [24,25]. While the Braden Scale has been widely used to assess PI risk, its original design for general inpatient care limits its capacity to capture perioperative-specific variables such as anesthesia duration, operative positioning, and hemodynamic instability [26,27]. The Braden Scale assesses six domains include sensory perception, moisture, activity, mobility, nutrition, and friction/shear, making it most appropriate for ward-based care where patients are awake and able to reposition themselves voluntarily [28]. Although the Scale demonstrates moderate predictive validity in adult inpatient populations, as shown in a systematic review and meta-analysis [29], it does not explicitly include perioperative-specific factors that significantly influence tissue tolerance during surgery [30]. As a result, its applicability and usefulness in the operating room setting are limited compared with tools designed to include surgical risk variables.
In contrast, the Munro Pressure Injury Risk Assessment Scale was specifically developed for perioperative pressure injury prevention by addressing dynamic physiological and procedural changes across preoperative, intraoperative, and postoperative phases [25].
The tool incorporates parameters such as ASA physical status classification, type and duration of anesthesia, surgical position, temperature regulation, and intraoperative blood loss, all of which are highly relevant to pressure injury risk among surgical patients [24,31]. The Munro Scale evaluates multiple patient-specific factors that influence susceptibility to pressure injuries [25]. The preoperative component of the Munro Scale assesses intrinsic risk variables such as mobility status, nutritional profile (including recent weight changes and validated nutritional indices), body mass index (BMI), age, and the presence of comorbid conditions such as diabetes mellitus or vascular disease [25]. These variables are essential because impaired mobility, compromised nutrition, and chronic health conditions have been linked with decreased tissue tolerance and an increased likelihood of pressure-related injury [24,32]. Preoperative evaluation also incorporates inspection of skin integrity and functional limitations to identify additional vulnerabilities that may not be captured by more common tools, such as the Braden Scale, which has limited assessment components in a perioperative setting [33]. The detailed comparison between the Munro and Braden Scales is presented in Table 1.
Furthermore, instead of perioperative setting, the Braden Scale may be well-suited for ongoing monitoring in wards and ICUs. Moreover, the Munro Scale provides a phase-based, procedure-centered evaluation ideal for perioperative settings. The AORN explicitly more recommends the Munro Scale or equivalent perioperative-specific tools due to their higher sensitivity and contextual alignment with surgical risk factors [24].
Another measurement tools can be used to measure PIs, including the Perioperative Risk Assessment Measure for Skin (PRAMS) [34,35] and Scott Triggers Tool [36]. PRAMS evaluates six indicators (age ≥70, diabetes, preexisting ulcer, prior surgery, Braden ≤16, duration ≥5h), while the Scott Triggers Tool integrates physiological and procedural markers (albumin <3.5 g/dL, BMI <18.5, ASA ≥III, and procedure duration >2h). Therefore, structured preoperative risk stratification, by identifying risk of PIs, enhances interdisciplinary communication and handover, ensuring that preventive plans are effectively conveyed to anesthesia, surgical, and nursing teams, ultimately fostering continuity of care throughout the intraoperative and postoperative continuum [33].
Nutritional status is also a recognized modifiable risk factor for pressure injury prevention and healing. Evidence from systematic reviews and meta-analyses indicates that poor nutrition and malnutrition are linked with higher pressure injury incidence, and that patients with better nutritional profiles have a lower risk of injury development [37]. Although evidence on specific supplementation strategies remains mixed, clinical guidelines emphasize the importance of preoperative nutritional screening and optimization, including adequate energy and protein intake to support tissue integrity and enhance resistance to pressure-related damage [37,38].
Additionally, clinicians can provide evidence-based preventive actions, including the use of pressure-redistributing support surfaces, application of prophylactic dressings on high-risk sites, nutritional optimization, and individualized positioning strategies both before and during surgery [39]
3.2. Intraoperative Phase
The intraoperative phase carries the highest risk for pressure injuries due to prolonged immobility under anesthesia and sustained mechanical pressure [10,24]. Preventive measures prioritize pressure redistribution, microclimate regulation, and perfusion maintenance.
3.2.1. Pressure-Redistribution
First, pressure-redistributing support surfaces are a core component of perioperative pressure injury prevention, designed to reduce mechanical load on bony prominences during prolonged immobility. Systematic evidence indicates that high-technology support surfaces, such as alternating-pressure air mattresses, gel overlays, and advanced viscoelastic foam surfaces, significantly redistribute interface pressure and reduce the incidence of pressure injuries compared with standard surgical table surfaces (Figure 2) [40]. Meta-analytic findings show that high-tech surfaces were associated with large reductions in pressure injury risk in the intraoperative period. International perioperative nursing standards also recommend placing patients on surfaces that reduce the potential for pressure injury by redistributing pressure during surgery [10].
Second, prophylactic application of silicone foam dressings to high-risk anatomical sites during surgery has been shown to be an effective measure for preventing intraoperatively acquired pressure injuries (IAPIs) (Figure 3), particularly in patients undergoing prolonged procedures. In a randomized, self-controlled study involving patients receiving spinal surgery, soft silicone foam dressings applied to the chest and iliac crest areas significantly reduced the incidence of stage 1 IAPIs compared with non-dressed sites immediately after surgery and at follow-up assessments [41]. Specifically, areas covered with soft silicone foam dressings had markedly lower rates of pressure injury than non-dressed areas, and no injuries were observed in dressed sites one week postoperatively [41]. These findings support the preventive use of silicone dressings on high-risk contact points during surgical positioning to cushion vulnerable tissues, reduce shear and friction forces, and mitigate the development of early pressure injuries when integrated with comprehensive perioperative risk assessment.
Third, individualized positioning strategies aim to minimize focal pressure and shear by adjusting the patient’s alignment and using positioning aids tailored to surgical needs (Figure 4). Integrative reviews of perioperative practice highlight positioning aids and careful planning of surgical body alignment as key strategies to reduce the risk of pressure injuries, particularly in lengthy procedures [42]. Collaboration between perioperative nurses, anesthesia, and surgical teams is essential to select safe positions and reposition support devices throughout the operative period, considering both anatomical vulnerability and procedural requirements.
3.2.2. Microclimate Regulation
Microclimate refers to the local temperature and humidity at the interface between the skin and support surfaces and plays an important role as an extrinsic risk factor in the development of pressure injuries by influencing skin tolerance to mechanical forces such as pressure, shear, and friction. Elevated skin temperature and increased moisture at the skin surface interface can weaken the stratum corneum, increase friction, and raise metabolic demand in loaded tissues, thereby lowering the threshold for skin and soft tissue damage under sustained pressure [43,44].
Emerging clinical evidence from intraoperative settings suggests that local microclimate conditions at skin support interfaces may independently contribute to the development of pressure injuries during surgery. In a prospective observational study of patients positioned in the park bench position, changes in skin temperature were significantly associated with intraoperatively acquired pressure injury, even after adjusting for interface pressure and duration of surgery, indicating that elevated skin temperature at load points may increase tissue vulnerability under sustained compression [45]. This supports the rationale for microclimate regulation strategies including maintaining skin coolness, reducing excessive humidity, and selecting materials that facilitate heat and moisture dissipation as part of a comprehensive perioperative pressure injury prevention protocol [46]
3.2.3. Perfusion
Adequate tissue perfusion is a critical determinant of skin and soft-tissue tolerance to sustained pressure, shear, and mechanical loading, particularly in perioperative patients who are immobilized and exposed to hemodynamic perturbations during anesthesia and surgery. Impaired perfusion a state in which blood flow and oxygen delivery to tissues are insufficient increases susceptibility of local tissues to ischemia, hypoxia, and metabolic stress under pressure, thereby heightening the likelihood of pressure injury development [18]. Poor perfusion has been identified as one of the intrinsic contributory factors in pressure injury etiology, along with other factors such as nutrition and comorbidities, especially in critically ill and surgical patients where compromised circulatory dynamics may exacerbate tissue vulnerability [47,48].
In the perioperative context, monitoring perfusion involves attention to hemodynamic variables such as blood pressure, cardiac output, and tissue oxygenation, as well as metabolic indicators including lactate levels, because hypotension and reduced tissue perfusion have been associated with adverse outcomes and may compromise tissue tolerance to pressure during prolonged procedures [49]. Ensuring adequate perfusion through vigilant hemodynamic management, avoidance of prolonged hypotensive episodes, and optimization of cardiac output is therefore essential both for organ protection and for reducing the risk of pressure injuries in surgical patients [48,50].
3.2.4. Clinical Workflow Integration (Optional)
In addition to workflow integration, early risk identification and ongoing assessment play a critical role in preventing perioperative pressure injuries. Comprehensive preoperative skin assessment, combined with the use of validated risk assessment tools, enables clinicians to identify patients at higher risk and implement targeted preventive interventions in a timely manner [51]. Continuous reassessment throughout the intraoperative and postoperative phases, supported by clear documentation and interprofessional communication, facilitates early detection of skin changes and allows for prompt modification of prevention strategies. This proactive, team-based approach has been shown to reduce the incidence and severity of pressure injuries while reinforcing patient safety and quality outcomes across the perioperative continuum [33,52]
3.3. Postoperative Phase
Following surgery, patients remain highly vulnerable to pressure injuries due to residual anesthetic effects, postoperative pain, hemodynamic instability, and reduced mobility, all of which impair tissue tolerance and increase susceptibility to sustained pressure. Surgical patients are at elevated risk of developing pressure injuries throughout the perioperative period, particularly in the early postoperative phase when immobility, compromised perfusion, and surgical stress accumulate to compromise skin and soft tissue integrity [53]. Postoperative pressure injuries often become evident within the first 48–72 hours after surgery, reflecting the combined impact of prolonged immobilization, altered hemodynamics, and decreased sensory feedback once anesthesia wears off [54]
The postoperative period is therefore critical for early identification and mitigation of delayed pressure injury development. Effective prevention during this phase requires vigilant surveillance, timely intervention, and coordinated interdisciplinary nursing care to ensure continuity of preventive strategies initiated during the intraoperative phase, including systematic skin assessment, mobilization, and risk communication [55]
3.3.1. Systematic Skin Assessment and Surveillance
Immediately upon arrival in the Post-Anesthesia Care Unit (PACU) and continuing through the first 48–72 hours after surgery, nurses should perform systematic skin assessments focused on bony prominences and areas previously subjected to pressure or medical devices [18]. Intraoperatively acquired pressure injuries commonly manifest within the first 48–72 hours after surgery, emphasizing the need for frequent inspection and early documentation of skin integrity to detect subtle changes before they progress to more severe injury [56]
These assessments should be documented using standardized tools and communicated clearly during handovers to ensure continuity of preventive actions, as early detection and consistent risk communication enhance the effectiveness of evidence-based interventions in the postoperative period [26]
3.3.2. Repositioning and Mobilization
Postoperative repositioning and early mobilization are essential components of postoperative pressure injury prevention. Repositioning patients at regular intervals helps redistribute pressure away from vulnerable tissues and enhance local blood perfusion, which can mitigate sustained mechanical loading that contributes to tissue breakdown [57]. Evidence from systematic reviews indicates that more frequent repositioning schedules (e.g., every 2–3 hours compared with longer intervals) are associated with reductions in pressure injury incidence in at-risk populations, supporting the inclusion of structured repositioning in postoperative care plans [58]. Although evidence specifically linking early ambulation programs to reduced pressure injury incidence remains mixed, early mobilization contributes to overall circulatory function, reduces prolonged static loading of soft tissues, and is widely recommended as part of comprehensive patient recovery protocols following surgery [26]
3.3.3. Support Surfaces and Moisture
Appropriate support surfaces should be continued postoperatively, including pressure-redistributing mattresses, overlays, and integrated systems, to maintain reduced interface pressure as the patient gradually recovers mobility. Evidence indicates that specialized support surfaces are designed to redistribute pressure, reduce friction and shear forces, and aid microclimate management all of which are key factors in preventing the development of pressure injuries in at risk patients [57]
In addition to mechanical support, microclimate control remains important in the postoperative period; maintaining skin dryness, balanced humidity, and minimized heat at the skin-surface interface helps reduce the risk of moisture-associated skin damage, maceration, and consequent pressure injury progression [59]. Clinical literature and best practice guidelines recommend avoiding excessive moisture, managing humidity near the skin, and selecting textiles and linens that optimize moisture evaporation and heat dissipation to support skin integrity [44]. Moisture management strategies may include the use of absorbent linens with low friction properties, moisture barrier products where appropriate, and skin care protocols that minimize friction and shear during bedding changes and patient handling, all of which contribute to creating a skin-protective microenvironment [60]
3.3.4. Interdisciplinary Communication and Care
Structured communication among perioperative nurses, ward nurses, wound care specialists, physical therapists, and other members of the care team is vital for ensuring that postoperative prevention plans are consistently applied. Clear documentation of intraoperative risk factors, such as duration of surgery, patient positioning, and protective measures used — along with comprehensive handoff summaries, helps the receiving care team prioritize continued surveillance, skin assessment, and repositioning strategies throughout the postoperative period. Multifaceted interventions that include care bundles and team coordination have been shown to significantly reduce the incidence of pressure injuries by enhancing consistency in preventive practices and promoting shared responsibility across disciplines [61]
Interprofessional communication and structured team rounds further reinforce accountability and enhance compliance with prevention bundles across care settings. Effective communication among clinicians is strongly associated with improvements in patient safety outcomes and team performance, as communication errors are recognized as a leading contributor to adverse events in healthcare. Models such as structured interdisciplinary bedside rounds create a shared understanding of care priorities and role responsibilities, supporting improved coordination of pressure injury prevention measures throughout recovery [62]
4. Implication to Practice
Pressure injury prevention remains a core responsibility of perioperative nursing practice, particularly given the heightened vulnerability of surgical patients [63]. Prolonged immobility, altered sensory perception, and the use of surgical positioning devices substantially increase the risk of intraoperative acquired pressure injuries [63]. Consistent with recommendations from the AORN, this review highlights the importance of implementing comprehensive and evidence-based prevention strategies to mitigate pressure injury development and its associated consequences, including patient discomfort, prolonged hospitalization, and increased healthcare expenditure. Previous review indicate that evidence-based nursing and comprehensive nursing management are more effective than routine nursing care in reducing the severity of intraoperative acquired pressure injuries [64]. Pressure injuries are classified into six stages, Stage 1 to Stage 4, unstageable injuries, and deep tissue injuries, with mucosal pressure injuries recognized as a distinct category [65]. A higher proportion of Stage 1 injuries reflects lower injury severity and is associated with better recovery outcomes [64].
Evidence-based nursing and comprehensive nursing management demonstrated higher incidences of Stage 1 injuries and ranked more favorably in probabilistic comparisons, suggesting their superiority in early prevention and damage limitation [64,66]. Evidence-based nursing, which integrates the best available research evidence with clinical expertise and patient preferences, provides a structured framework for improving perioperative care quality [64]. Previous reviews have identified integrated or comprehensive nursing approaches as the most effective interventions for accelerating intraoperative acquired pressure injuries healing [64]. From a health system perspective, the implications are substantial: annual expenditures for treating IAPI among surgical patients in the United States are estimated to range from USD 750 million to 1.5 billion [64,67], while critically ill patients who develop IAPI face nearly a fourfold increase in mortality risk [68,69]. Therefore, strengthening the adoption of evidence-based and comprehensive nursing interventions in perioperative settings is not only essential for improving patient outcomes and quality of life, but also represents a crucial strategy for reducing preventable healthcare costs and adverse clinical outcomes [70,71].
Technological innovation is also reshaping perioperative PI risk detection and management. AI-assisted imaging systems, sensor-based pressure mapping, and predictive algorithms integrated within electronic health records (EHRs) have shown promise in enabling earlier identification of pressure-related risks [8]. When aligned with validated clinical assessment frameworks, these digital tools may strengthen diagnostic accuracy while reducing documentation burden.
A key insight from recent studies is the essential role of multidisciplinary collaboration. Effective PI prevention depends on coordinated efforts among perioperative nurses, anesthesiologists, surgeons, and wound care specialists. Embedding prevention strategies within surgical safety checklists, team briefings, and intraoperative time-outs enhances shared situational awareness and promotes early risk recognition [72]. Sustained improvements are most evident when prevention bundles are supported by strong leadership, real-time performance feedback, and regular auditing mechanisms.
From a policy perspective, national health authorities and professional organizations should consider incorporating comprehensive pressure injury prevention strategies into national clinical guidelines, accreditation standards, and patient safety indicators. Standardized risk assessment, positioning protocols, and intraoperative skin surveillance should be emphasized to ensure consistency across healthcare settings [20]. Strengthening national guidelines and institutional policies to support evidence-based nursing practice may contribute to improved patient outcomes, reduced healthcare costs, and enhanced quality of perioperative care [73].
5. Conclusion
Pressure injury prevention in perioperative settings is achievable through early risk identification, precise intraoperative protection, and vigilant postoperative monitoring. Implementing standardized, evidence-based strategies across all phases of surgery, combined with technological innovation and multidisciplinary collaboration, can significantly reduce the incidence of preventable PIs and improve patient outcomes.
Author Contributions
Conceptualization, A.E. and T.P.; methodology, A.E.; validation, T.P. and M.R.; formal analysis, A.E.; investigation, A.E. and T.P; data curation, T.P. and M.R.; writing—original draft preparation, A.E.; writing—review and editing, T.P. and M.R., and A.E.; and supervision, T. P. All authors have read and agreed to the published version of the manuscript.
Funding
APC was funded by the University of Padjadjaran.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
MDPI Research Data Policies.
Acknowledgments
During the preparation of this manuscript, the author(s) used ChatGPT 5.0 for the purposes of English proofreading. The authors have reviewed and edited the manuscript and take full responsibility for the content of this manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PI | Pressure Injury |
| PIs | Pressure Injuries |
| AORN | Association of periOperative Registered Nurses |
| ASA | American Society of Anesthesiologists |
| BMI | Body Mass Index |
| EHR | Electronic Health Record |
| IAPI | Intraoperatively Acquired Pressure Injury |
| ICU | Intensive Care Unit |
| PACU | Post-Anesthesia Care Unit |
| NPIAP | National Pressure Injury Advisory Panel |
| PRAMS | Perioperative Risk Assessment Measure for Skin |
References
- Suh, D.; Kim, S.Y.; Yoo, B.; Lee, S. An Exploratory Study of Risk Factors for Pressure Injury in Patients Undergoing Spine Surgery. Anesth Pain Med (Seoul) 2020, 16, 108. [Google Scholar] [CrossRef] [PubMed]
- Savcı, A.; Karacabay, K.; Aydın, E. Incidence and Risk Factors of Operating Room–Acquired Pressure Injury: A Cross-Sectional Study. Wound Manag Prev 2024, 70. [Google Scholar] [CrossRef] [PubMed]
- Guler, B.; Gurkan, A. Effect of Different Positioning before, during and after Surgery on Pressure Injury: A Randomized Controlled Trial Protocol. Int J Clin Trials 2024, 11, 45–52. [Google Scholar] [CrossRef]
- Li, N.; Cui, D.; Shan, L.; Li, H.; Feng, X.; Zeng, H.; Li, L. The Prediction Model for Intraoperatively Acquired Pressure Injuries in Orthopedics Based on the New Risk Factors: A Real-World Prospective Observational, Cross-Sectional Study. Front Physiol 2023, 14. [Google Scholar] [CrossRef]
- Fang, Z.; Chen, T.; Zheng, W.; Chen, Q.; Chen, P.; Zhuo, Q. Incidence and Risk Factors of Intraoperative Acquired Pressure Injury in Open Heart Surgical Patients: A Meta-Analysis of Prospective Studies. European Journal of Medical Research 2025, 30 30, 814. [Google Scholar] [CrossRef]
- Peng, X.; Xiong, X.; Lan, W. Prevention of Pressure Injuries in the Operating Room: Challenges and Strategies. J Adv Nurs 2024. [Google Scholar] [CrossRef]
- Cavalcanti, E. de O.; Kamada, I. MEDICAL-DEVICE-RELATED PRESSURE INJURY ON ADULTS: AN INTEGRATIVE REVIEW. Texto & Contexto - Enfermagem 2020, 29. [Google Scholar] [CrossRef]
- Xu, X.; Miao, M.; Shi, G.; Zhang, P.; Liu, P.; Zhao, B.; Jiang, L. Operative Positioning and Intraoperative-Acquired Pressure Injury: A Retrospective Cohort Study. Adv Skin Wound Care 2024, 37, 148–154. [Google Scholar] [CrossRef]
- Kim, J.M.; Lee, H.; Ha, T.; Na, S. Perioperative Factors Associated with Pressure Ulcer Development after Major Surgery. Korean J Anesthesiol 2017, 71, 48. [Google Scholar] [CrossRef]
- Spruce, L. Prevention of Perioperative Pressure Injury. AORN J 2023, 117, 317–323. [Google Scholar] [CrossRef]
- Padula, W. V.; Delarmente, B.A. The National Cost of Hospital-acquired Pressure Injuries in the United States. Int Wound J 2019, 16, 634. [Google Scholar] [CrossRef] [PubMed]
- Triantafyllou, C.; Chorianopoulou, E.; Kourkouni, E.; Zaoutis, T.E.; Kourlaba, G. Prevalence, Incidence, Length of Stay and Cost of Healthcare-Acquired Pressure Ulcers in Pediatric Populations: A Systematic Review and Meta-Analysis. Int J Nurs Stud 2021, 115, 103843. [Google Scholar] [CrossRef] [PubMed]
- Afridi, A.; Rathore, F.A. Are Risk Assessment Tools Effective for the Prevention of Pressure Ulcers Formation?: A Cochrane Review Summary with Commentary. Am J Phys Med Rehabil 2020, 99, 357–358. [Google Scholar] [CrossRef] [PubMed]
- Roussou, E.; Fasoi, G.; Stavropoulou, A.; Kelesi, M.; Vasilopoulos, G.; Gerogianni, G.; Alikari, V. Quality of Life of Patients with Pressure Ulcers: A Systematic Review. Med Pharm Rep 2023, 96, 123–130. [Google Scholar] [CrossRef]
- Cebeci, F.; Şenol Çelik, S. Knowledge and Practices of Operating Room Nurses in the Prevention of Pressure Injuries. J Tissue Viability 2022, 31, 38–45. [Google Scholar] [CrossRef]
- Özdemir, E.D.; Uslu, Y. Pressure Injuries in the Operating Room: Who Are at Risk? https://doi.org/10.12968/jowc.2023.32.Sup7a.cxxviii 2023, 32, CXXVIII–CXXXVI. [Google Scholar] [CrossRef]
- AKAN, C.; SAYIN, Y.Y.; AKAN, C.; SAYIN, Y.Y. Prevalence of Pressure Injuries and Risk Factors in Long-Term Surgical Procedures. Bezmialem Science 2021, 9, 75–83. [Google Scholar] [CrossRef]
- İlkhan, E.; Sucu Dag, G. The Incidence and Risk Factors of Pressure Injuries in Surgical Patients. J Tissue Viability 2023, 32, 383–388. [Google Scholar] [CrossRef]
- Celik, B.; Karayurt, Ö.; Ogce, F. The Effect of Selected Risk Factors on Perioperative Pressure Injury Development. AORN J 2019, 110, 29–38. [Google Scholar] [CrossRef]
- AORN Updates to Guideline for Pressure Injury | Periop Today | AORN. Available online: https://www.aorn.org/article/key-takeaways-pressure-injury-guideline-updates-2023 (accessed on 26 December 2025).
- Picoito, R.; Manuel, T.; Vieira, S.; Azevedo, R.; Nunes, E.; Alves, P. Recommendations and Best Practices for the Risk Assessment of Pressure Injuries in Adults Admitted to Intensive Care Units: A Scoping Review. Nursing Reports 2025, Vol. 15 15, 128. [Google Scholar] [CrossRef]
- AHRQ Preventing Pressure Ulcers in Hospitals | Agency for Healthcare Research and Quality. Available online: https://www.ahrq.gov/patient-safety/settings/hospital/resource/pressureulcer/tool/index.html?utm (accessed on 11 December 2025).
- Song, H.; Qu, T.; Zheng, C.; Wei, N. Clinical Application of Checklist Management in the Prevention of Pressure Injuries among Oncologic Surgical Patients. Supportive Care in Cancer 2025, 33, 1154. [Google Scholar] [CrossRef] [PubMed]
- AORN GUIDELINES FOR PERIOPERATIVE PRACTICE. 2023.
- Munro, C.A. The Development of a Pressure Ulcer Risk-Assessment Scale for Perioperative Patients. AORN J 2010, 92, 272–287. [Google Scholar] [CrossRef] [PubMed]
- Betts, H.; Scott, D.; Makic, M.B.F. Using Evidence to Prevent Risk Associated With Perioperative Pressure Injuries. Journal of PeriAnesthesia Nursing 2022, 37, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Wang, W.; Qian, Q.; Wu, B. Comparison of Four Risk Assessment Scales in Predicting the Risk of Intraoperative Acquired Pressure Injury in Adult Surgical Patients: A Prospective Study. Journal of International Medical Research 2023, 2023, 1–13. [Google Scholar] [CrossRef]
- Bergstrom, N.; Demuth, P.J.; Braden, B.J. A Clinical Trial of the Braden Scale for Predicting Pressure Sore Risk. Nursing Clinics of North America 1987, 22, 417–428. [Google Scholar] [CrossRef]
- Huang, C.; Ma, Y.; Wang, C.; Jiang, M.; Loretta; Foon, Y.; Lv, | Lin; Han, L. Predictive Validity of the Braden Scale for Pressure Injury Risk Assessment in Adults: A Systematic Review and Meta-Analysis. 2021. [Google Scholar] [CrossRef]
- Haesler, E. National Pressure Injury Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Alliance. Prevention and Treatment of Pressure Ulcers/Injuries: Quick Reference Guide; The International Guideline: Fourth Edition, 2025. [Google Scholar]
- Lei, L.; Zhou, T.; Xu, X.; Wang, L. Munro Pressure Ulcer Risk Assessment Scale in Adult Patients Undergoing General Anesthesia in the Operating Room. J Healthc Eng 2022, 2022. [Google Scholar] [CrossRef]
- Sousa, C.S.; Acunã, A.A. Implantação Da Escala Munro de Avaliação de Risco de Lesão Por Pressão No Perioperatório. Revista SOBECC 2022, 27. [Google Scholar] [CrossRef]
- AORN Updates to Guideline for Pressure Injury | Periop Today | AORN. Available online: https://www.aorn.org/article/key-takeaways-pressure-injury-guideline-updates-2023 (accessed on 19 December 2025).
- Meehan, A.J.; Beinlich, N.R.; Hammonds, T.L. A Nurse-Initiated Perioperative Pressure Injury Risk Assessment and Prevention Protocol. AORN J 2016, 104, 554–565. [Google Scholar] [CrossRef]
- Meehan, A.J.; Beinlich, N.R.; Bena, J.F.; Mangira, C. Revalidation of a Perioperative Risk Assessment Measure for Skin. Nurs Res 2019, 68, 398–404. [Google Scholar] [CrossRef]
- Mosher, R. Enhancing Perioperative Care: Implementing the Scott Triggers Tool to Prevent Hospital-Acquired Pressure Injuries in Vascular Surgery Patients - PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/40013702/ (accessed on 10 June 2025).
- Chen, B.; Yang, Y.; Cai, F.; Zhu, C.; Lin, S.; Huang, P.; Zhang, L. Nutritional Status as a Predictor of the Incidence of Pressure Injury in Adults: A Systematic Review and Meta-Analysis. J Tissue Viability 2023, 32, 339–348. [Google Scholar] [CrossRef]
- Munoz, N.; Posthauer, M.E.; Cereda, E.; Schols, J.M.G.A.; Haesler, E. The Role of Nutrition for Pressure Injury Prevention and Healing: The 2019 International Clinical Practice Guideline Recommendations. Adv Skin Wound Care 2020, 33, 123–136. [Google Scholar] [CrossRef] [PubMed]
- AORN Pressure Injury Prevention: AORN Guideline Takeaways for Periop Nurses | AORN Periop Today | AORN. Available online: https://www-aorn-org.translate.goog/article/pressure-injury-prevention--aorn-guideline-takeaways-for-periop-nurses?_x_tr_sl=en&_x_tr_tl=id&_x_tr_hl=id&_x_tr_pto=sge (accessed on 2 June 2025).
- Beatriz Cunha Prado, C.; Alves Silva Machado, E.; Dal Sasso Mendes, K.; Cristina de Campos Pereira Silveira, R.; Maria Galvão, C. Support Surfaces for Intraoperative Pressure Injury Prevention: Systematic Review with Meta-Analysis*. Rev Latino-Am. Enfermagem 2021, 29, 3493. [Google Scholar] [CrossRef] [PubMed]
- Yang, T.Y.; Shin, S.H. Effect of Soft Silicone Foam Dressings on Intraoperatively Acquired Pressure Injuries: A Randomized Study in Patients Undergoing Spinal Surgery. Wound Manag Prev 2020, 66, 22–29. [Google Scholar] [CrossRef]
- Wang, I.; Walker, R.; Gillespie, B.M. Pressure Injury Prevention in the Perioperative Setting: An Integrative Review. Journal of Perioperative Nursing 2018, 31, 27-35–27–35. [Google Scholar] [CrossRef]
- Clark, M. Lecture as Part of a Series by Parafricta Microclimate and Pressure Ulcer Development; 2017. [Google Scholar]
- Kottner, J.; Black, J.; Call, E.; Gefen, A.; Santamaria, N. Microclimate: A Critical Review in the Context of Pressure Ulcer Prevention. Clinical Biomechanics 2018, 59, 62–70. [Google Scholar] [CrossRef]
- Yoshimura, M.; Nakagami, G.; Iizaka, S.; Yoshida, M.; Uehata, Y.; Kohno, M.; Kasuya, Y.; Mae, T.; Yamasaki, T.; Sanada, H. Microclimate Is an Independent Risk Factor for the Development of Intraoperatively Acquired Pressure Ulcers in the Park-Bench Position: A Prospective Observational Study. Wound Repair Regen 2015, 23, 939–947. [Google Scholar] [CrossRef]
- Xie, X.; Chen, M.; Wang, F.; Liao, B.; Yang, X.; Zhuang, C.; Huang, J. Prevention of Intraoperative Acquired Pressure Injury in Patients With Head and Neck Cancer and Its Effect on Skin Microclimate: A Single-Blind Randomised Controlled Trial. Int Wound J 2025, 22. [Google Scholar] [CrossRef]
- Alderden, J.; Rondinelli, J.; Pepper, G.; Cummins, M.; Whitney, J.A. Risk Factors for Pressure Injuries among Critical Care Patients: A Systematic Review. Int J Nurs Stud 2017, 71, 97–114. [Google Scholar] [CrossRef]
- Li, B.; Dai, Y.; Cai, W.; Sun, M.; Sun, J. Monitoring of Perioperative Tissue Perfusion and Impact on Patient Outcomes. Journal of Cardiothoracic Surgery 2025 20:1 2025, 20, 100. [Google Scholar] [CrossRef]
- Li, B.; Dai, Y.; Cai, W.; Sun, M.; Sun, J. Monitoring of Perioperative Tissue Perfusion and Impact on Patient Outcomes. Journal of Cardiothoracic Surgery 2025 20:1 2025, 20, 100. [Google Scholar] [CrossRef] [PubMed]
- Karadede, Ö.; Toğluk Yiğitoğlu, E.; Şeremet, H.; Özyilmaz Daştan, Ç. Incidence and Risk Factors for Perioperative Pressure Injuries: Prospective Descriptive Study. Journal of PeriAnesthesia Nursing 2025, 40, 596–603. [Google Scholar] [CrossRef] [PubMed]
- AORN 5 Essential Steps to Prevent Pressure Injuries in Surgery | AORN. Available online: https://www.aorn.org/article/5-essential-steps-to-prevent-pressure-injuries-in-surgery (accessed on 24 December 2025).
- Speth, J. Guidelines in Practice: Prevention of Perioperative Pressure Injury. In AORN J; PAGE:STRING:ARTICLE/CHAPTER, 2023; Volume 118, pp. 37–44. [Google Scholar] [CrossRef]
- Haisley, M.; Sørensen, J.A.; Sollie, M. Postoperative Pressure Injuries in Adults Having Surgery under General Anaesthesia: Systematic Review of Perioperative Risk Factors. BJS 2020, 107, 338–347. [Google Scholar] [CrossRef]
- İlkhan, E.; Sucu Dag, G. The Incidence and Risk Factors of Pressure Injuries in Surgical Patients. J Tissue Viability 2023, 32, 383–388. [Google Scholar] [CrossRef]
- Betts, H.; Scott, D.; Makic, M.B.F. Using Evidence to Prevent Risk Associated With Perioperative Pressure Injuries. Journal of PeriAnesthesia Nursing 2022, 37, 308–311. [Google Scholar] [CrossRef] [PubMed]
- Shang, Y.; Wang, F.; Cai, Y.; Zhu, Q.; Li, X.; Wang, R.; Tung, T.H. The Accuracy of the Risk Assessment Scale for Pressure Ulcers in Adult Surgical Patients: A Network Meta-Analysis. BMC Surg 2025, 25, 104. [Google Scholar] [CrossRef]
- NPIAP Support Surfaces — International Guideline. Available online: https://internationalguideline.com/surfaces (accessed on 24 December 2025).
- Avsar, P.; Moore, Z. Repositioning for Preventing Pressure Ulcers: A Systematic Review and Meta-Analysis. J Wound Care 2020, 29. [Google Scholar] [CrossRef]
- Lachenbruch, C. Microclimate Management So Much More than Just Airflow…. 2018. [Google Scholar]
- Haesler, E. WHAM Evidence Summary: Low Friction Fabric for Preventing Pressure Injuries. Wound Practice and Research 2020, 28, 97–98. [Google Scholar] [CrossRef]
- Kandula, U.R. Impact of Multifaceted Interventions on Pressure Injury Prevention: A Systematic Review. BMC Nursing 2024, 24 24, 11. [Google Scholar] [CrossRef]
- Dietl, J.E.; Derksen, C.; Keller, F.M.; Lippke, S. Interdisciplinary and Interprofessional Communication Intervention: How Psychological Safety Fosters Communication and Increases Patient Safety. Front Psychol 2023, 14, 1164288. [Google Scholar] [CrossRef] [PubMed]
- Pressure Injury Prevention: AORN Guideline Takeaways for Periop Nurses | AORN Periop Today | AORN. Available online: https://www.aorn.org/article/pressure-injury-prevention--aorn-guideline-takeaways-for-periop-nurses (accessed on 25 December 2025).
- Zhu, W.; Pei, X.; Guo, Y.; Chen, L.; Zhang, H.; Li, Q. Effects of Different Nursing Interventions for Intraoperative Acquired Pressure Injuries: A Network Meta-Analysis. BMC Nurs 2025, 24, 1031. [Google Scholar] [CrossRef] [PubMed]
- Peterson, L. Intraoperative Pressure Injury Prevention. Nursing Clinics of North America 2025, 60, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Tang, S.; Qin, Y.; Zhou, S.; Zhang, L.; Huang, Y.; Chen, Z. A Predictive Model of Pressure Injury in Children Undergoing Living Donor Liver Transplantation Based on Machine Learning Algorithm. J Adv Nurs 2024, 81, 3003. [Google Scholar] [CrossRef]
- Spector, W.D.; Limcangco, R.; Owens, P.L.; Steiner, C.A. Marginal Hospital Cost of Surgery-Related Hospital-Acquired Pressure Ulcers. Med Care 2016, 54, 845–851. [Google Scholar] [CrossRef]
- Savcı, A.; Karacabay, K.; Aydın, E. Incidence and Risk Factors of Operating Room-Acquired Pressure Injury: A Cross-Sectional Study. Wound Manag Prev 2024, 70. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, L.; Rong, R.; Guo, L.; Pei, Y.; Lu, X. Constructing Nursing Quality Indicators for Intraoperative Acquired Pressure Injury in Cancer Patients Based on Guidelines. Int J Qual Health Care 2024, 36. [Google Scholar] [CrossRef]
- Lin, H.; Chen, H.; Wang, J.; Ma, X. Nomogram for Intraoperatively Acquired Pressure Injuries in Children Undergoing Cardiac Surgery with Cardiopulmonary Bypass: A Retrospective Study. BMC Pediatr 2024, 24. [Google Scholar] [CrossRef]
- Bates-Jensen, B.M.; Crocker, J.; Nguyen, V.; Robertson, L.; Nourmand, D.; Chirila, E.; Laayouni, M.; Offendel, O.; Peng, K.; Romero, S.A.; et al. Decreasing Intraoperative Skin Damage in Prone-Position Surgeries. Adv Skin Wound Care 2024, 37, 413–421. [Google Scholar] [CrossRef]
- Gefen, A.; Brienza, D.M.; Cuddigan, J.; Haesler, E.; Kottner, J. Our Contemporary Understanding of the Aetiology of Pressure Ulcers/Pressure Injuries. Int Wound J 2021, 19, 692. [Google Scholar] [CrossRef]
- Ratliff, C.R.; Droste, L.R.; Bonham, P.; Crestodina, L.; Johnson, J.J.; Kelechi, T.; Varnado, M.F.; Palmer, R.; Carroll, B. WOCN 2016 Guideline for Prevention and Management of Pressure Injuries (Ulcers): An Executive Summary. J Wound Ostomy Continence Nurs 2017, 44, 241–246. [Google Scholar] [CrossRef]
Figure 1.
Early localized skin changes suggestive of pressure-related erythema following prolonged prone positioning. Non-blanchable erythema (red arrows) was observed over the left forehead and left lateral chest wall immediately upon arrival in the Post-Anesthesia Care Unit (PACU) in a patient who underwent prolonged prone posterior stabilization surgery. These areas correspond to contact points exposed to sustained pressure during the surgical position. Skin assessment was performed within the first 24 hours postoperatively. Persistent non-blanchable erythema over pressure-prone areas may represent early pressure injury and warrants prompt preventive interventions and ongoing monitoring.
Figure 1.
Early localized skin changes suggestive of pressure-related erythema following prolonged prone positioning. Non-blanchable erythema (red arrows) was observed over the left forehead and left lateral chest wall immediately upon arrival in the Post-Anesthesia Care Unit (PACU) in a patient who underwent prolonged prone posterior stabilization surgery. These areas correspond to contact points exposed to sustained pressure during the surgical position. Skin assessment was performed within the first 24 hours postoperatively. Persistent non-blanchable erythema over pressure-prone areas may represent early pressure injury and warrants prompt preventive interventions and ongoing monitoring.

Figure 2.
Illustration of pressure-redistributing support surfaces. Figure 2.A illustrated a silicone head pillow, Figure 2.B illustrated a silicon prone positioner. The figure has no copy right and taken by author in our own institution.
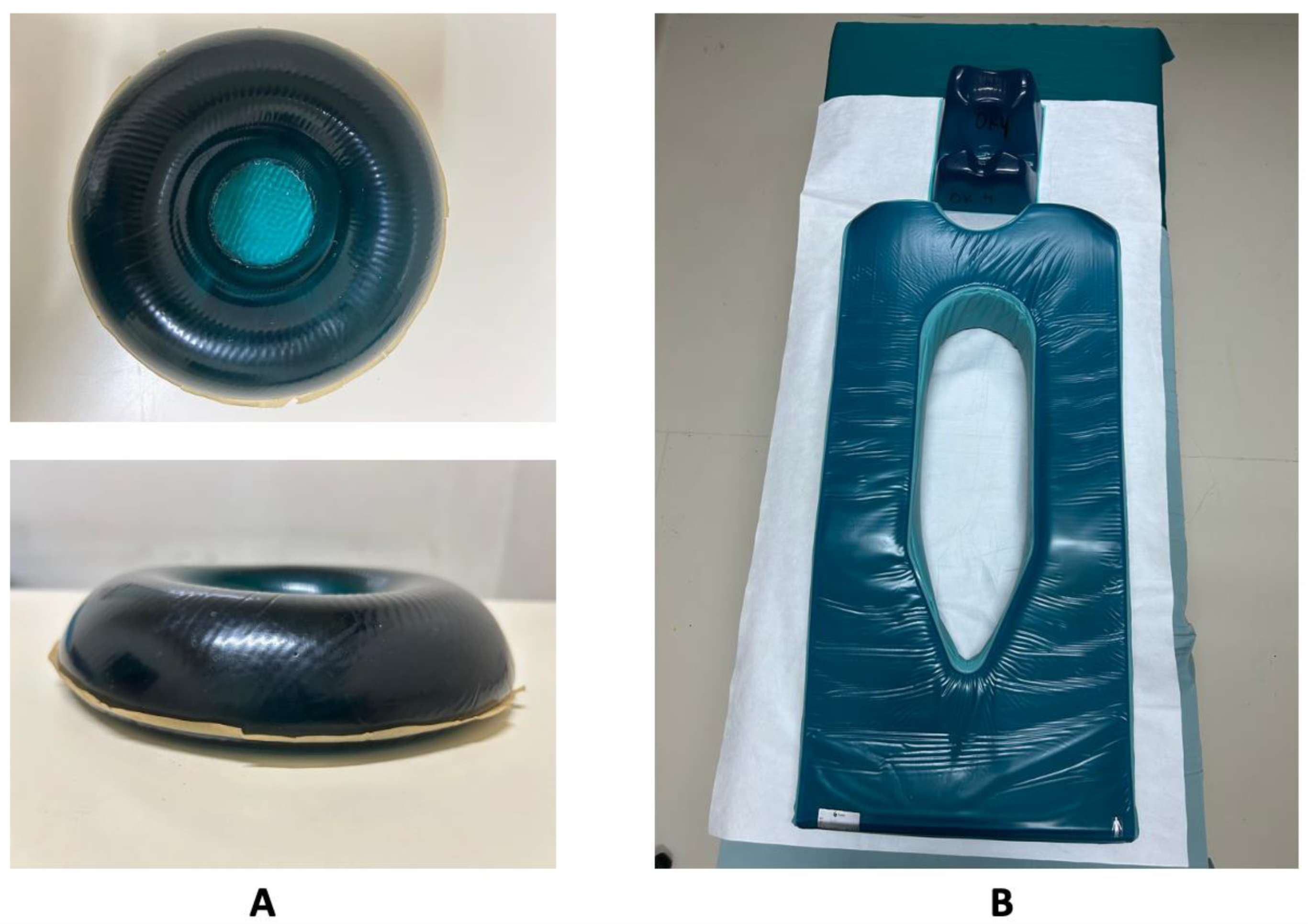
Figure 3.
Illustration of silicone foam dressings.

Figure 4.
Illustration of positioning during intraoperative. Figure 4.A illustrated supine position, Figure 4.B illustrated reverse trendelenburg position, Figure 4.C illustrated trendelenburg position, figre 4.D illustrated prone position, Figure 4.E illustrated lithotomy position, Figure 4.F illustrated sitting/semi-sitting position, Figure 4.G illustrated lateral position. All figures are cited from AORN. (2022). Guideline for Patient Positioning in Guidelines for Perioperative Practice.
Figure 4.
Illustration of positioning during intraoperative. Figure 4.A illustrated supine position, Figure 4.B illustrated reverse trendelenburg position, Figure 4.C illustrated trendelenburg position, figre 4.D illustrated prone position, Figure 4.E illustrated lithotomy position, Figure 4.F illustrated sitting/semi-sitting position, Figure 4.G illustrated lateral position. All figures are cited from AORN. (2022). Guideline for Patient Positioning in Guidelines for Perioperative Practice.
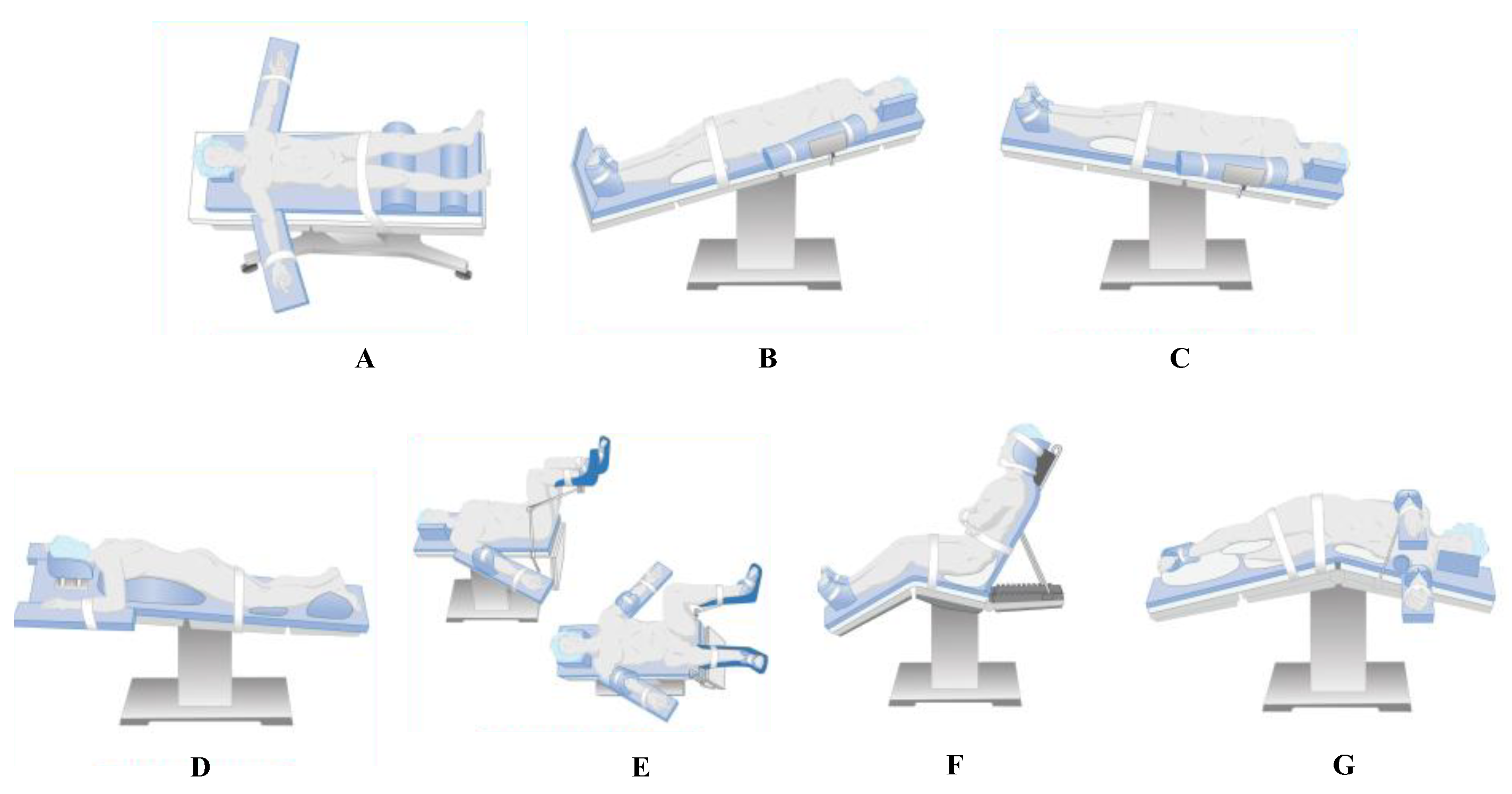

Table 1.
Comparison between Braden Scale and Munro Scale.
| Feature | Braden Scale | Munro Scale |
|---|---|---|
| Clinical Setting | General ward, long-term care | Operating theater, perioperative care |
| Assessment Timing | Static; at admission and daily reassessment | Dynamic; pre-, intra-, and postoperative reassessment |
| Focus | Functional and sensory impairment | Physiological and procedural risk factors |
| Variables | Six patient-based domains | Multi-phase domains (mobility, anesthesia, perfusion, positioning, blood loss) |
| Risk Scoring | 6–23 (lower = higher risk) | 0–100 (higher = higher risk, cumulative) |
| Suitability | General medical/surgical wards | Operating room and PACU |
Note: PACU= Post-Anesthetia care unit.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



