
Submitted:
07 January 2026
Posted:
08 January 2026
You are already at the latest version
Abstract
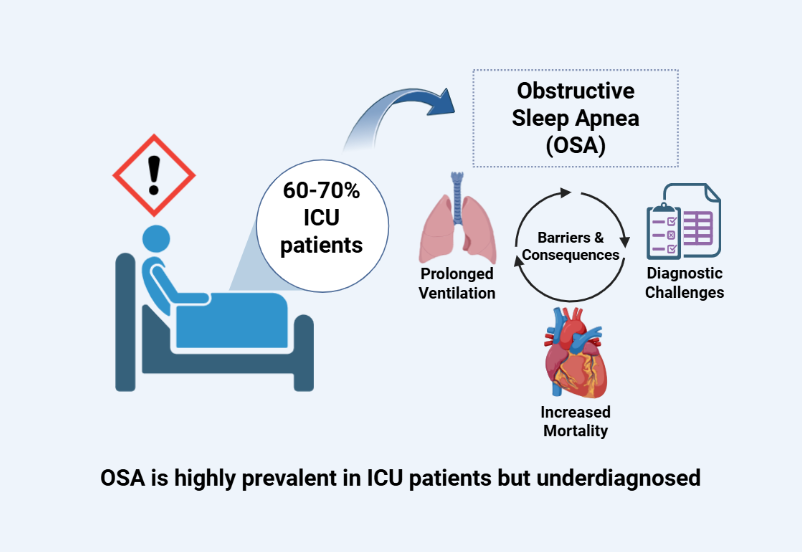
Obstructive sleep apnea (OSA) is a highly prevalent yet frequently underdiagnosed condition that is associated with significant cardiopulmonary, metabolic, and neurocognitive outcomes. Risk factors for OSA overlap with illnesses commonly observed in intensive care unit (ICU) patients, resulting in a disproportionately elevated burden in healthcare. This study evaluates the prevalence, diagnostic challenges, and management limitations of OSA in the ICU to identify strategies to improve awareness and outcomes in critically ill populations. An analysis of published literature was conducted using PubMed, EMBASE, and Scopus. Key search terms included “obstructive sleep apnea,” “ICU,” and “critical illness.” Results showed that OSA is present in up to 60–70% of ICU patients, yet only ~5% are formally diagnosed during hospitalization. Underdiagnosis is linked to prolonged mechanical ventilation, extubation failure as high as 30%, 2-fold higher perioperative complication rates, cardiovascular instability, 1.8-fold greater 30-day ICU readmission, and 2.2-fold mortality. Standard screening tools have limited applicability in ICU patients. Emerging alternatives, such as overnight oximetry, polygraphy, and machine learning models lack validation. Our analyses reveal that current diagnostic and treatment strategies are poorly adapted to critically ill patients. Integration of OSA as a part of ICU management, diagnosis, and intervention may reduce readmissions and mortality.
Keywords:
ICU
; obstructive sleep apnea
; critical care
; sleep-disordered breathing
; OSA screening
1. Introduction
Obstructive sleep apnea (OSA) is a highly prevalent but often underdiagnosed disorder characterized by recurrent episodes of upper airway collapse during sleep, resulting in intermittent hypoxia, hypercapnia, and sleep fragmentation [1]. The pathophysiology of OSA involves a complex mix of anatomical, neuromuscular, and ventilator control abnormalities, all of which synergistically contribute to repetitive airway obstruction [2,3]. During these obstructive events, pharyngeal airway collapse leads to airway cessation despite ongoing respiratory effort, resulting in large negative intrathoracic pressure swings, intermittent hypoxemia, and hypercapnia. The sum of these physiological disturbances triggers cortical arousals, leading to sleep fragmentation. These apneic events lead to activation of the sympathetic nervous system (SNS), oxidative stress, systemic inflammation, and endothelial dysfunction, all of which contribute to a higher risk of cardiovascular, metabolic, and neuropsychiatric comorbidities [4,5].
The global burden of OSA is substantial, with an estimated 936 million adults from ages 30 to 69 years old worldwide diagnosed with mild to severe OSA, and in which 425 million have moderate to severe disease, according to several modeling studies [6,7,8]. In the United States alone, data from the Wisconsin Sleep Cohort Study estimates that 13% of men and 6% of women have moderate to severe (AHI ≥ 15 events/ hour), with prevalence of OSA positively increasing with age and body mass index [9]. However, it is estimated that 80-90% of individuals with moderate to severe OSA remain underdiagnosed, revealing a substantial gap in public health. The underdiagnosis and undertreatment of OSA not only worsens individual health outcomes but also amplifies societal costs and public safety risks. Addressing this burden requires greater public awareness, standardized screenings, and integrated care strategies that particularly cater towards high-risk and underserved populations [7,10].
Concerningly, OSA is associated with a wide range of deleterious health outcomes. Cardiovascular complications have been well documented in association with OSA, including systemic hypertension (HTN), arrhythmia, coronary artery disease, heart failure, and stroke [11,12,13]. The Sleep Heart Health Study and other large cohort studies have shown that untreated OSA increases the risk of cardiovascular events and mortality [14]. Metabolically, OSA is also linked to insulin resistance, dyslipidemia, and poor glycemic control, serving as an independent risk factor for type 2 diabetes mellitus (T2DM) [12]. Neurologically, OSA has been associated with impaired attention, memory deficits, executive dysfunction, and mood disorders, all of which can negatively impact quality of life. OSA is further linked to increased perioperative complications, postoperative respiratory events, and higher mortality, especially in patients with undiagnosed OSA [15,16]. During the COVID-19 pandemic, OSA was seen to worsen hospitalized patient outcomes in regard to increased incidence of respiratory failure and heart failure [17,18]. Despite these risks, treatment with continuous positive airway pressure (CPAP) can improve patient quality of life and may mitigate some consequences of cardiovascular and neurocognitive adverse events, though evidence for cardiovascular event reduction is mixed, possibly due to the heterogenous nature of OSA and variable patient compliance to treatment adherence [11,19]. Recent research has emphasized the importance of identifying pathophysiological traits to guide personalized treatment strategies and targeted therapies to better or further improve patient outcomes and alleviate the public health burden of OSA [20,21,22]. This review examines the high prevalence of OSA in the ICU, focusing on challenges in accurate diagnosis, increased complications related to comorbidities, and limitations of current treatment strategies. The study selection process is summarized in a PRISMA flow diagram in Figure 1.
Epidemiology and Prevalence of OSA in ICU Settings
Intensive Care Unit (ICU) usage is a complicated and financially expensive healthcare infrastructure. With approximately 5.7 million annual patient admissions in the US, ICU associated costs exceed $82 billion, greater than 4.1% of national healthcare expenses [23]. ICU hospitalizations are linked to a wide variety of complications, including but not limited to delirium, 1 in 6 patients developing sepsis-associated acute kidney injury, and the development of Post Intensive Care syndrome as characterized by a range of physical, mental, and cognitive impairments persisting after discharge [24,25,26]. In particular, sleep disturbances and disorders frequently occur in the ICU, with a prevalence of 66% [27]. Up to 80% of ICU patients reported experiencing significant sleep deprivation during their stay [28]. These disturbances are not only common but also clinically remarkable as impaired sleep quality in critically ill patients results in poor outcomes such as prolonged weaning, delayed extubation, and complete disappearance of REM sleep [29]. In general, untreated sleep apnea is associated with an elevated risk of morbidity and mortality [30].
OSA has been highly associated with hospitalizations. In patients hospitalized for CVD, OSA prevalence is estimated to be as high as 48% [31]. However, a low percentage –- 4.8-5.8% -- of hospitalized patients are formally diagnosed with OSA and provided CPAP therapy during the hospital stay [32]. Within the ICU, sleep disorders are known to be common yet frequently undiagnosed [33]. Approximately 68% out of 129 patients were discovered to have an apnea-hypopnea index (AHI) value ≥ 5, and 40% of those patients had an AHI >15 [34]. AHI, or apnea-hypoxia index, quantifies the episodes of apnea and hypopneas throughout sleep. An AHI <5 is normal, 5–14 indicates mild OSA, and ≥15 indicates moderate OSA [35]. Hence, an overwhelming majority of ICU patients exhibit varying degrees of OSA, indicating that the frequency and under-diagnosis of OSA in ICU is a critical issue. The proposed mechanisms linking obstructive sleep apnea to adverse outcomes in critically ill patients are illustrated in Figure 2.
ICU patients often have underlying medical conditions that exacerbate their likelihood of developing OSA, such as acute respiratory failure, sepsis, and COPD [36,37,38]. Naranjo et al., discovered that in patients hospitalized for COPD exacerbations with no prior formal diagnosis of OSA, screening revealed approximately 46.6% of patients had OSA, with greater OSA severity correlated with increased odds of hospital readmission and mortality [39]. Sepsis is known to activate a cascade of pro-inflammatory cytokines such as IL-6 and TNF-α [40]. Pro-inflammatory cytokines have been linked to the progression of lung disease via increased vascular permeability and decreased lung compliance, referring to the lung’s capacity to expand in response to pressure [41]. Sepsis-induced inflammation impairs gas exchange and inflicts respiratory distress, significantly impairing sleep and breathing in patients with underlying, undiagnosed OSA [42]. Furthermore, the most cited risk factors for OSA include male sex, obesity, and older age [43]. ICU admissions have been likewise found to be more likely for ages 50+, male sex, and obesity [44]. The equivalent risk factors for both OSA and ICU strongly underscore the likelihood that a significant portion of critically ill patients have underlying OSA, potentially exacerbating clinical outcomes and recovery times.
There is a lack of clinical data regarding the precise prevalence of OSA in the ICU setting due to diagnostic barriers. Historically, OSA data has been influenced by evolving definitions of hypopnea, AHI criteria, and changes in PSG (polysomnography methods) [45]. The lack of universal criteria for defining OSA presents a challenge for diagnoses, particularly in the ICU as PSG is highly time consuming, labor intensive, and expensive [46]. Furthermore, even diagnosing OSA was projected to cost nearly $2.4 billion, with CPAP therapy – the gold standard for treating OSA – costing around $3.4 billion in the US [47]. In the ICU where 80-90% of patients present with multiple morbidities, it’s plausible to assume that screening, diagnosis, and treatment for OSA will often not be of the utmost priority within the ICU [48]. It’s imperative to also understand that this dilemma extends to a global scale applied to other clinical settings as well.
2. Results
Clinical Implications of Unrecognized OSA in the ICU
The underdiagnosis of OSA has been linked with an increased duration of mechanical ventilation in critically ill patients. Key clinical outcomes and complications associated with obstructive sleep apnea in critically ill patients are summarized in Table 1. The pathophysiological hallmarks of OSA relating to intermittent hypoxia and increased negative intrathoracic pressure exacerbate respiratory efforts and increased difficulty of weaning patients off ventilation [49,50,51]. ICU patients with underdiagnosed OSA require significantly longer durations of invasive ventilation compared to non-OSA patients. For example, in pediatric patients, underdiagnosed OSA was associated with more than a 5-fold increase in the need for mechanical ventilation, as well as an extra day in the hospital [49]. Hospitalized adult patients with pneumonia or COPD with suspected OSA were also linked to higher rates of invasive and noninvasive ventilation, increased risk of clinical deterioration, and longer lengths of stay [50,51]. Reduced ventilatory drive, compromised upper airway tone, and blunted arousal tone in OSA patients all contribute to extubating delays and extend ventilator dependence.
Extubation failure is also a significant contributor to ICU patient mortality and morbidity, which is more common in patients with underdiagnosed OSA. The loss of pharyngeal muscle tone during sleep in OSA predisposed patients to upper airway collapse post-extubation, especially during the immediate period of post-sedation [52,53]. Rates as high as 30% have been reported in studies reporting re-intubation rates in ICU patients with high-risk STOP-BANG scores compared to 10-15% of the general population [54]. This phenomenon may further be compounded by unmonitored desaturations, unrecognized apneic events, and ineffective airway clearance during spontaneous breathing trials [55].
The perioperative period also presents numerous challenges to patients with underdiagnosed OSA. Most patients with moderate-to-severe OSA remain undiagnosed prior to surgery, lacking preventative risk management [56,57]. Notably, these patients have an increased risk for hypoventilation, desaturation, airway obstruction, and opioid sensitivity; all increased in risk following the administration of general anesthesia [58,59,60,61]. Post-operatively, patients with undiagnosed or high-risk OSA are nearly at double risk of complications compared to low-risk patients. The susceptibility of upper airway collapse and anesthesia-related respiratory depression may precipitate critical respiratory events during the recovery period [58,59]. The use of anesthetic and sedative agents can exacerbate upper airway collapse and depress central respiratory drive, which makes intraoperative and postoperative management more complex.
OSA induces substantial autonomic dysregulation with sympathetic overactivity and cyclical surges in blood pressure and heart rate during apneic episodes [11,60,61,62]. In the ICU, patients typically have limited physiological reserves, and the presence of OSA can further destabilize cardiovascular status. Episodes of hypoxia and intrathoracic pressure swings lead to an increase in myocardial oxygen demand while reducing coronary artery perfusion, leading to a heightened risk of life-threatening arrhythmias and myocardial injury. OSA has been shown to be independently associated with new-onset atrial fibrillation, ventricular ectopy, and sudden cardiac death in high-acuity patients. These life-threatening symptoms may even go unnoticed due to sedation masking typical OSA presentation and events [60,61]. Of note, women with OSA and acute coronary syndrome may face even greater long-term cardiovascular risks compared to men [63].
The implications of underdiagnosed OSA extend beyond the initial ICU stay. Recurrent hospitalizations increased 30-day ICU readmission rates, and higher long-term mortality have all been linked to untreated OSA [12,60,64,65]. Patients with unrecognized OSA have been shown to have a 1.8-fold increase of ICU readmission within 30 days and a 2.2-fold increase in one-year mortality compared to matched controls. Chronic intermittent hypoxia also contributes to higher systemic inflammation, endothelial dysfunction, and metabolic dysregulation, compounding risks for adverse patient outcomes, even independent from obesity as a risk factor. Neurocognitive impairments from undiagnosed OSA can also lead to a reduced quality of life, increased work-related injuries, and greater healthcare utilization [66]. Despite its prevalence, OSA remains underdiagnosed in high-risk populations, especially in the ICU, due to a lack of systemic screening [60,67]. Given these findings, there is a compelling need for early therapeutic intervention for ICU patients at risk for OSA.
3. Discussion
3.1. Diagnostic Challenges in the ICU
Atypical presentations in the critically ill, particularly in the ICU, can mask the symptoms of OSA, contributing to underdiagnosis and exacerbated outcomes. The typical clinical presentation of OSA include disruptive snoring, witnessed apneas, and excessive daytime sleepiness [68]. On average, 39.5% of ICU patients are receiving mechanical ventilation at any given hour [69]. Therefore, most ICU patients are not visually exhibiting classical symptoms that would arouse suspicion for clinical diagnosis of OSA. Furthermore, critically ill patients often present with atypical sleep, with a lack of sleep spindles and K complexes [70]. This poses a significant challenge in determining if the abnormal sleep pattern is a consequence of the underlying reason for ICU admission or a persistent condition attributable to OSA. Furthermore, undiagnosed and untreated OSA can significantly increase the likelihood of developing acute and post-operative delirium [71]. Delirium is particularly prevalent in the ICU, affecting 83% of ICU patients on mechanical ventilation with a 3.2-fold increase in 6-month mortality [72,73].
Diagnosis of true OSA in the ICU is clinically challenging in terms of differentiation from sedation effects, underlying respiratory failure (i.e. ARDS), and ventilator-induced breathing patterns. The usage of opioids and sedative medications within the ICU is significantly elevated, with a 56.1% reported prevalence [74]. Anesthetics and opioids are well-associated causes of respiratory depression, and opioids specifically impact the peripheral and central carbon dioxide chemoreflex loops to diminish respiratory capacity [75]. Specifically, opioids, in conjunction with benzodiazepines, are associated with increased episodes of apnea and hypoxemia in patients [76]. Opioids lead to shallow breathing, a slowed respiratory rate < 8 bpm, and a decreased SpO2, a close resemblance to the hypoventilation witnessed in OSA [77]. Neuromuscular blocking agents, or NMBAs, are frequently utilized for critically ill patients for mechanical ventilation and muscle relaxation. One common complication is residual neuromuscular block, in which upper airway muscles and pharyngeal muscle function are diminished [78]. With patients exhibiting hypoxic ventilatory response, the usage of anesthetics, neuromuscular blockers, and opioids can mask the symptoms of OSA, leading to misdiagnosis and/or lack of diagnosis. A proposed clinical workflow for screening and diagnosing obstructive sleep apnea in hospitalized patients is shown in Figure 3.
3.2. Current Approaches to Screening, Diagnosis, and Management
Currently, there are several validated questionnaires employed in outpatient and preoperative settings to estimate the probability of OSA. A summary of commonly used obstructive sleep apnea screening tools and their reported performance characteristics is provided in Table 2. The most widely used is the STOP-BANG Questionnaire that incorporates eight parameters: snoring, tiredness, observed apneas, high blood pressure, BMI > 35, age > 50, neck circumference > 40 cm, and male gender [79,80,81]. This method is favored for its ease of use, high sensitivity of up to 93% for moderate-to-severe OSA (though specificity is modest below 50%), and rapid administration. Alternatively, the Berlin Questionnaire stratifies patients based on their snoring behavior, daytime somnolence, and comorbid HTN/BMI, with a specificity around 70-80% [81]. The American Society of Anesthesiologists (ASA) has a similar OSA checklist intended for preoperative use to stratify patient risk prior to anesthesia, however this method lacks robust validation in ICU settings [82]. The application of these tools in critically ill patients presents significant limitations. Often, ICU patients are sedated, mechanically ventilated, or nonverbal, which makes subjective questionnaires appear to be inapplicable. Further, physiologic confounders such as fluid overload, altered state of consciousness, or acute respiratory distress can mask or mimic features of OSA [83,84,85]. Metrics such as neck circumference or BMI may be distorted by the presence of edema or critical illness-related catabolism, resulting in limited discriminatory power in the ICU. Despite these drawbacks, modified versions of the STOP-BANG and Berlin Questionnaire criteria have been implemented informally in some ICU studies, though no consensus has been reached regarding best practices [83,84].
Currently, PSG is the main standard for the formal diagnosis of sleep and sleep disordered breathing [85]. In the ICU, usage of PSG is simply not practical mainly due to the quantity of equipment needed and the deviating mental statuses of the patients [33,34]. In fact, the PADIS guidelines (Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption) established by the Society of Critical Care Medicine has deemed PSG utilization in ICU as unfeasible since 2018 [86]. Given the impracticality of utilizing full polysomnography (PSG) in ICU settings, simplified diagnostic alternatives have been explored, such as overnight pulse oximetry, which assesses nocturnal oxygen desaturation index (ODI) [87,88]. ODI presents a practical, portable, and cost-effective tool in resource-limited or high-acuity settings. However, oximetry may be confounded by supplemental oxygen, unstable hemodynamics and frequent desaturations unrelated to OSA. Alternatively, respiratory polygraphy can capture airflow, respiratory effort, and oxygen saturation without electroencephalography (EEG) [89]. This method retains acceptable diagnostic accuracy in non-intubated and stable patients, though data in ICU settings remain sparse. In one prospective study of 124 ICU patients, polygraphy detected moderate-to-severe OSA in 70% of subjects, suggesting significant underdiagnosis [33,34]. However, motion artifacts, supine positioning, and irregular respiratory patterns in critically ill patients may reduce diagnostic reliability. To overcome these diagnostic challenges, recent advances in machine learning (ML) algorithms and wearable biosensors have emerged trained on electronic heath record (EHR) data, including demographic variables, comorbidities, and physiologic trends for predicting underdiagnosed OSA [86,87,88,89]. ML models using easily accessible parameters such as age, BMI, heart rate, and select biomarkers have been successfully integrated into cloud-based markers to support clinical decision making [90]. Accelerometer-based actigraphy, thoracic effort bands, and peripheral arterial tone sensors are also increasingly being utilized in hospital settings [91,92]. FDA-approved devices are better equipped at sensing real-time respiratory event detection and autonomic metrics. However, recognizing the unique challenges of the ICU has led to the development of new frameworks and metrics with simplified clinical observations, such as respiratory effort during sleep or sedation weaning trials [89]. Alternatively, ventilator waveforms of apnea indices from overnight mechanical ventilation data can be used to infer OSA risk. While promising for the unique needs and challenges of ICU patients, these tools are in the early validation phases and have not yet been incorporated into standard practices [86].
With respect to treatment, effective management is highly dependent upon early identification and effective airway management that uniquely tailors to each patient’s needs. Currently, continuous positive airway pressure (CPAP) is utilized as the gold standard for moderate to severe OSA treatment. By applying a consistent positive pressure throughout the respiratory cycle, CPAP helps keep the airways open and decrease the AHI value back within the normal range [87]. CPAP also improves ventilation-perfusion matching (V/Q) and decreases the risk of atelectasis, effectively diminishing the likelihood of developing hypoxia and associated adverse outcomes [88]. However, most ICU patients present with contraindications to CPAP, including altered level of consciousness, inability to protect the airway, respiratory arrest, and unstable cardiorespiratory status [89].
For ICU patients with contraindications, there exists various non-CPAP treatment options, such as positional therapy, hypoglossal nerve stimulation, myofunctional therapy, and maxillofacial surgery [90]. An alternative avenue of treatment is low-dose fentanyl and/or dexmedetomidine to improve compliance until criteria for CPAP therapy is met [88]. Dexmedetomidine is an a2-agonist with analgesic, anxiolytic, and sympatholytic sedative properties that maximizes patient comfort while minimizing respiratory depression [91]. It has been shown to improve efficacy and comfort alongside BiPAP therapy, thereby optimizing outcomes [91]. BIPAP can be more effective than CPAP in ICU patients, providing higher pressure during inspiration and lower pressure during expiration [92] while lowering PaCO2 levels [92,93]. Given the association between hypercapnia, ICU readmissions, and elevated mortality rates [94], BiPAP can help optimize patient outcomes. Furthermore, BiPAP machines provide a backup rate for patients with central hypoventilation and unpredictable IPAP (inspiratory positive airway pressure) and EPAP (expiratory positive airway pressure) levels due to muscle weakness [95]. Critically ill patients in the ICU often present with multiple comorbidities as well as reduced respiratory drive because of sedation and opioid medication usage [96]. Hence, BiPAP can be of great benefit for ICU patients who are greatly vulnerable to rapid declines in respiratory function. Ultimately, a combination of proactive airway management, vigilant observation of respiratory status, and monitoring of medication usage must be undertaken to minimize the risk of worsening OSA in ICU patients.
3.3. Future Research Directions
Despite advancements and growing knowledge regarding the high prevalence of OSA in critically ill populations, there remain substantial knowledge gaps and areas for clinical improvement. The ICU setting poses several unique diagnostic challenges for patients due to their status of acuity, respiratory pathophysiology, and impracticality of conventional screening and diagnostic protocols [97,98,99]. For instance, current screening instruments, such as the STOP-BANG and BERLIN Questionnaires, were developed and validated in ambulatory and perioperative patient populations that rely heavily on patient reported symptoms, rendering them impractical for sedated, intubated, and nonverbal ICU patients [100,101,102,103]. There is an urgent need for the development of a tool that accounts for ICU-specific variables, such as ventilator waveforms, sedation levels, fluid shifts, and physiologic instability
Current literature remains sparse on prospective studies linking OSA screening or diagnosis within ICU settings to meaningful patient-centered outcomes, such as mortality, length of stay, ventilator duration, or readmission risk [104]. Most existing studies are retrospective, observational, or limited either by small sample size or heterogenous methodology. This necessitates high-quality, prospective cohort studies and randomized controlled trials to determine whether early management and targeted intervention of OSA in the ICU can alter clinical outcomes, especially in high-risk populations with heart failure, obesity, hypoventilation, or postoperative respiratory failure. [105,106,107,108]
The integration of OSA screening and diagnostic workflows in the ICU practice currently remains inconsistent and underdeveloped [109]. Developing institutional protocols, defining clear criteria for screening, setting diagnostic thresholds, and extubation management strategies is crucial [110]. The creation of ICU outpatient follow-up pathways for high-risk patients with OSA could facilitate easier definitive diagnosis and long-term treatment management. Engagement of multidisciplinary teams consisting of intensivists, sleep specialists, and respiratory specialists can also help ensure practical and sustainable protocol development. Timely diagnosis and CPAP treatment in high-risk hospitalized patients may reduce resource utilization, and as such should be investigated in ICU settings. Establishing evidence-based policies surrounding OSA management in critical care settings may improve both short and long-term outcomes, improving critical care standards.
4. Materials and Methods
A critical analysis of published literature was conducted using PubMed, EMBASE, and Scopus. Key search terms included “obstructive sleep apnea,” “ICU,” “critical illness,” and “sleep-disordered breathing.” The study selection process is summarized in a PRISMA flow diagram in Figure 1.
During the preparation of this work, the author(s) used Consensus to assist with initial literature surveying and to identify current research trends. All final article selection, critical appraisal, synthesis, interpretation, and manuscript writing were performed by the authors. After using this tool, the author(s) reviewed, verified, and edited the content as needed and take full responsibility for the accuracy and integrity of the published work.
5. Conclusions
OSA continues to be a prevalent disorder globally. OSA is associated with adverse outcomes, such as arrythmias, heart failure, insulin resistance, and inflammation, which is exacerbated the longer it’s undiagnosed. Notably, the ICU presents a challenge to the detection and diagnosis of OSA. Here we highlight various aspects of the ICU and its patient population that elevate the risk of undiagnosed OSA, including shared risk factors such as obesity. Although limited, previous research studies underscored the detrimental effects of delayed OSA recognition in critically ill patients, such as higher risk of hospital readmission, delirium, extubation delays, and elevated mortality risk. Current screening measures, including STOP-BANG and BERLIN questionnaire, fail to be applicable to ICU patients. Moreover, sedation and failure to protect the airway prevent patients from achieving maximal benefit via CPAP, the traditional gold standard treatment. Future research should focus on identifying the most effective diagnostic and treatment approaches for OSA in ICU patients to improve long-term clinical outcomes and reduce the burden on the healthcare system.
Author Contributions
Conceptualization: Christine Gharib, Catherine Kim, Madhu Varma, Methodology: Christine Gharib, Catherine Kim, Investigation: Christine Gharib, Catherine Kim, Writing – Original Draft: Christine Gharib, Catherine Kim, Writing – Review & Editing: Christine Gharib, Catherine Kim, Jun Ling, Madhu Varma, Supervision: Jun Ling, Madhu Varma. All authors have read and agreed to the published version of the manuscript.
Funding
Research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in this study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
During the preparation of this work, the author(s) used Consensus to assist with initial literature surveying and to identify current research trends. All final article selection, critical appraisal, synthesis, interpretation, and manuscript writing were performed by the authors. After using this tool, the author(s) reviewed, verified, and edited the content as needed and take full responsibility for the accuracy and integrity of the published work. The authors would like to acknowledge the faculty and staff of the California University of Science and Medicine for their academic guidance and institutional support. The authors also thank colleagues and mentors who provided valuable feedback during the development of this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| OSA | Obstructive sleep apnea |
| ICU | Intensive care unit |
| SNS | Sympathetic nervous system |
| T2DM | Type 2 diabetes mellitus |
| CPAP | Continuous positive airway pressure |
| PSG | Polysomnography methods |
| HTN | Hypertension |
| ARDS | Acute respiratory distress syndrome |
| ASA | American Society of Anesthesiologists |
| PADIS | Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption |
| ODI | Oxygen desaturation index |
| STOP-BANG | Snoring, tiredness, observed apneas, high blood pressure, BMI > 35, age > 50, neck circumference > 40 cm, male gender |
| EEG | Electroencephalography |
| ML | Machine learning |
| EHR | Electronic heath record |
| V/Q | Ventilation-perfusion |
| EPAP | Expiratory positive airway pressure |
| HST | Home sleep testing |
References
- Chronic intermittent hypoxia in obstructive sleep apnea: A narrative review from pathophysiological pathways to a precision clinical approach | Sleep and Breathing. (2020). https://link.springer.com/article/10.1007/s11325-019-01967-4.
- McNicholas, W. T.; Korkalainen, H. Translation of obstructive sleep apnea pathophysiology and phenotypes to personalized treatment: A narrative review. Frontiers in Neurology 2023, 14. [Google Scholar] [CrossRef]
- McNicholas, W. T.; Pevernagie, D. Obstructive sleep apnea: Transition from pathophysiology to an integrative disease model. Journal of Sleep Research 2022, 31(4), e13616. [Google Scholar] [CrossRef]
- Lindenauer, P. K.; Stefan, M. S.; Johnson, K. G.; Priya, A.; Pekow, P. S.; Rothberg, M. B. Prevalence, Treatment, and Outcomes Associated With OSA Among Patients Hospitalized With Pneumonia. CHEST 2014, 145(5), 1032–1038. [Google Scholar] [CrossRef] [PubMed]
- Shih, Chun-Ying; Wang, An-Yi; Chang, Kai-Mei; et al. Dynamic Prevalence of Sleep Disturbance among Critically Ill Patients in Intensive Care Units and after Hospitalisation: A Systematic Review and Meta-Analysis. Intensive and Critical Care Nursing 2023, 75, 103349. [Google Scholar] [CrossRef]
- Vasu, Tajender S., Ritu Grewal, and Karl Doghramji. “Obstructive Sleep Apnea Syndrome and Perioperative Complications: A Systematic Review of the Literature.” Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep Medicine 8, no. 2. (2012). 199–207. [CrossRef]
- P22 Undiagnosed obstructive sleep apnoea in the perioperative period: Prevalence and management | BMJ Open Respiratory Research. 2022. Available online: https://bmjopenrespres.bmj.com/content/10/Suppl_1/A22.2.
- Benjafield, A. V.; Ayas, N. T.; Eastwood, P. R.; Heinzer, R.; Ip, M. S. M.; Morrell, M. J.; Nunez, C. M.; Patel, S. R.; Penzel, T.; Pépin, J.-L.; Peppard, P. E.; Sinha, S.; Tufik, S.; Valentine, K.; Malhotra, A. Estimation of the global prevalence and burden of obstructive sleep apnoea: A literature-based analysis. The Lancet. Respiratory Medicine 2019, 7(8), 687–698. [Google Scholar] [CrossRef] [PubMed]
- Peppard, P. E.; Young, T.; Barnet, J. H.; Palta, M.; Hagen, E. W.; Hla, K. M. Increased Prevalence of Sleep-Disordered Breathing in Adults. American Journal of Epidemiology 2013, 177(9), 1006–1014. [Google Scholar] [CrossRef] [PubMed]
- Sun, Baisheng; Lei, Mingxing; Zhang, Jiaqi; Kang, Hongjun; Liu, Hui; Zhou, Feihu. Acute Lung Injury Caused by Sepsis: How Does It Happen? Frontiers in Medicine 2023, 10. [Google Scholar] [CrossRef]
- An umbrella review of systematic reviews and meta-analyses of observational investigations of obstructive sleep apnea and health outcomes | Sleep and Breathing. (2022). https://link.springer.com/article/10.1007/s11325-021-02384-2.
- Slowik, Jennifer M.; Sankari, Abdulghani; Collen, Jacob F. Obstructive Sleep Apnea. In StatPearls; StatPearls Publishing, 2025; Available online: http://www.ncbi.nlm.nih.gov/books/NBK459252/.
- Grimm, Jessica. Sleep Deprivation in the Intensive Care Patient. Critical Care Nurse 2020, 40(no. 2), e16–24. [Google Scholar] [CrossRef]
- Budhiraja, R.; Quan, S. F. Long-term All-Cause Mortality Risk in Obstructive Sleep Apnea Using Hypopneas Defined by a ≥3 Percent Oxygen Desaturation or Arousal. Southwest Journal of Pulmonary & Critical Care 2021, 23, 23–35. [Google Scholar] [CrossRef]
- Hariyanto, T. I.; Kurniawan, A. Obstructive sleep apnea (OSA) and outcomes from coronavirus disease 2019 (COVID-19) pneumonia: A systematic review and meta-analysis. Sleep Medicine 2021, 82, 47–53. [Google Scholar] [CrossRef]
- Marchasson, Laura; Rault, Christophe; Le Pape, Sylvain; et al. Impact of Sleep Disturbances on Outcomes in Intensive Care Units. Critical Care 2024, 28(no. 1), 331. [Google Scholar] [CrossRef]
- Du, W.; Xu, H.; Chang, Y.; Feng, B.; Wang, Q.; Li, W. Impact of obstructive sleep apnea on inpatient outcomes of COVID-19: A propensity-score matching analysis of the US Nationwide Inpatient Sample. (2020). Frontiers in Medicine 2025, 12. [Google Scholar] [CrossRef]
- Kim, Lindsay; Garg, Shikha; O’Halloran, Alissa; et al. Risk Factors for Intensive Care Unit Admission and In-Hospital Mortality Among Hospitalized Adults Identified through the US Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET). Clinical Infectious Diseases 2021, 72(no. 9.), e206–14. [Google Scholar] [CrossRef]
- Moyer, C. A.; Sonnad, S. S.; Garetz, S. L.; Helman, J. I.; Chervin, R. D. Quality of life in obstructive sleep apnea: A systematic review of the literature. Sleep Medicine 2001, 2(6), 477–491. [Google Scholar] [CrossRef]
- Eckert, D. J. Phenotypic approaches to obstructive sleep apnoea – New pathways for targeted therapy. Sleep Medicine Reviews 2018, 37, 45–59. [Google Scholar] [CrossRef]
- Randerath, W.; de Lange, J.; Hedner, J.; Ho, J. P. T. F.; Marklund, M.; Schiza, S.; Steier, J.; Verbraecken, J. Current and novel treatment options for obstructive sleep apnoea. ERJ Open Research 2022, 8(2). [Google Scholar] [CrossRef] [PubMed]
- Niu, Y.; Sun, S.; Wang, Y.; Chen, L.; Shao, Y.; Zhang, X. Spatiotemporal Trends in the Prevalence of Obstructive Sleep Apnoea Across China: A Multilevel Meta-Analysis Incorporating Geographic and Demographic Stratification (2000-2024). Nature and Science of Sleep 2025, 17, 879–903. [Google Scholar] [CrossRef] [PubMed]
- Ren, Yuanfang; Loftus, Tyler J.; Guan, Ziyuan; et al. Computable Phenotypes to Characterize Changing Patient Brain Dysfunction in the Intensive Care Unit; arXiv, 2023. [Google Scholar] [CrossRef]
- Erel, Selin; Macit Aydın, Eda; Nazlıel, Bijen; et al. Evaluation of Delirium Risk Factors in Intensive Care Patients. Turkish Journal of Anaesthesiology and Reanimation, ahead of print, Turkish Journal of Anaesthesiology and Reanimation 2024. [Google Scholar] [CrossRef] [PubMed]
- White, Kyle C.; Serpa-Neto, Ary; Hurford, Rod; et al. Sepsis-Associated Acute Kidney Injury in the Intensive Care Unit: Incidence, Patient Characteristics, Timing, Trajectory, Treatment, and Associated Outcomes. A Multicenter, Observational Study. Intensive Care Medicine 2023, 49(no. 9.), 1079–89. [Google Scholar] [CrossRef]
- Ayenew; Temesgen; Gete, Menberu; Gedfew, Mihretie; et al. Prevalence of Post-Intensive Care Syndrome among Intensive Care Unit-Survivors and Its Association with Intensive Care Unit Length of Stay: Systematic Review and Meta-Analysis. PLOS One 2025, 20(no. 5), e0323311. [Google Scholar] [CrossRef]
- Wunsch, Hannah; Wagner, Jason; Herlim, Maximilian; Chong, David; Kramer, Andrew; Halpern, Scott D. ICU Occupancy and Mechanical Ventilator Use in the United States. Critical Care Medicine 2013, 41(no. 12). [Google Scholar] [CrossRef] [PubMed]
- Devlin, John W.; Skrobik, Yoanna; Gélinas, Céline; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Critical Care Medicine 2018, 46(no. 9), e825. [Google Scholar] [CrossRef]
- Metrics of sleep apnea severity: Beyond the apnea-hypopnea index | SLEEP | Oxford Academic. 2021. Available online: https://academic.oup.com/sleep/article/44/7/zsab030/6164937.
- Ralls, Frank; Cutchen, Lisa. A Contemporary Review of Obstructive Sleep Apnea. Current Opinion in Pulmonary Medicine 2019, 25(no. 6), 578. [Google Scholar] [CrossRef]
- Suen, Colin; Wong, Jean; Ryan, Clodagh M.; et al. Prevalence of Undiagnosed Obstructive Sleep Apnea Among Patients Hospitalized for Cardiovascular Disease and Associated In-Hospital Outcomes: A Scoping Review. Journal of Clinical Medicine 2020, 9(no. 4.), 989. [Google Scholar] [CrossRef]
- Sleep monitoring by actigraphy in short-stay ICU patients | Critical Care | Full Text. 2012. Available online: https://ccforum.biomedcentral.com/articles/10.1186/cc10927.
- Bucklin, Abigail A.; Ganglberger, Wolfgang; Quadri, Syed A.; et al. High Prevalence of Sleep-Disordered Breathing in the Intensive Care Unit — a Cross-Sectional Study. Sleep & Breathing = Schlaf & Atmung 2023, 27(no. 3), 1013–26. [Google Scholar] [CrossRef]
- Bucklin, A. A.; Ganglberger, W.; Quadri, S. A.; Tesh, R. A.; Adra, N.; Da Silva Cardoso, M.; Leone, M. J.; Krishnamurthy, P. V.; Hemmige, A.; Rajan, S.; Panneerselvam, E.; Paixao, L.; Higgins, J.; Ayub, M. A.; Shao, Y.-P.; Ye, E. M.; Coughlin, B.; Sun, H.; Cash, S. S.; Westover, M. B. High prevalence of sleep-disordered breathing in the intensive care unit—A cross-sectional study. Sleep & Breathing = Schlaf & Atmung 2023, 27(3), 1013–1026. [Google Scholar] [CrossRef]
- “Apnea-Hypopnea Index (AHI).” Sleep Foundation, October 28, 2021. Available online: https://www.sleepfoundation.org/sleep-apnea/ahi.
- Franca; Aires, Suelene; Toufen, Carlos; Hovnanian, André Luiz D.; et al. The Epidemiology of Acute Respiratory Failure in Hospitalized Patients: A Brazilian Prospective Cohort Study. Journal of Critical Care 2011, 26(no. 3), 330.e1–330.e8. [Google Scholar] [CrossRef]
- Sakr, Yasser; Jaschinski, Ulrich; Wittebole, Xavier; et al. Sepsis in Intensive Care Unit Patients: Worldwide Data From the Intensive Care over Nations Audit. Open Forum Infectious Diseases 2018, 5(no. 12), ofy313. [Google Scholar] [CrossRef] [PubMed]
- Prediction of Extubation Failure in Intensive Care Units. Frontiers in Medicine 8. [CrossRef] [PubMed]
- Naranjo, Mario; Willes, Leslee; Prillaman, Barbara A.; Quan, Stuart F.; Sharma, Sunil. Undiagnosed OSA May Significantly Affect Outcomes in Adults Admitted for COPD in an Inner-City Hospital. CHEST 2020, 158(no. 3), 1198–207. [Google Scholar] [CrossRef]
- Nie, Jiali; Zhou, Ling; Tian, Weiwei; et al. Deep Insight into Cytokine Storm: From Pathogenesis to Treatment. Signal Transduction and Targeted Therapy 2025, 10(no. 1), 112. [Google Scholar] [CrossRef]
- Cheung; Hinson, Pak-Hin; Ye, Zi-Wei; Lee, Tak-Wang Terence; Chen, Honglin; Chan, Chi-Ping; Jin, Dong-Yan. PB1-F2 Protein of Highly Pathogenic Influenza A (H7N9) Virus Selectively Suppresses RNA-Induced NLRP3 Inflammasome Activation through Inhibition of MAVS-NLRP3 Interaction. Journal of Leukocyte Biology 2020, 108(no. 5), 1655–63. [Google Scholar] [CrossRef]
- Stansbury, R. C.; Strollo, P. J. Clinical manifestations of sleep apnea. Journal of Thoracic Disease 2015, 7(9). [Google Scholar] [CrossRef]
- Young, Terry; Skatrud, James; Peppard, Paul E. Risk Factors for Obstructive Sleep Apnea in Adults. JAMA 2004, 291(no. 16), 2013–16. [Google Scholar] [CrossRef]
- Investigating the Relationship between Obstructive Sleep Apnoea, Inflammation and Cardio-Metabolic Diseases. 2023. Available online: https://www.mdpi.com/1422-0067/24/7/6807.
- Franklin, Karl A.; Lindberg, Eva. Obstructive Sleep Apnea Is a Common Disorder in the Population—a Review on the Epidemiology of Sleep Apnea. Journal of Thoracic Disease 2015, 7(no. 8). [Google Scholar] [CrossRef]
- Natsky, Andrea N.; Vakulin, Andrew; Coetzer, Ching Li Chai; McEvoy, R. D.; Adams, Robert J.; Kaambwa, Billingsley. Economic Evaluation of Diagnostic Sleep Studies for Obstructive Sleep Apnoea: A Systematic Review Protocol. Systematic Reviews 2021, 10, 104. [Google Scholar] [CrossRef]
- Iannella, Giannicola; Pace, Annalisa; Bellizzi, Mario Giuseppe; et al. The Global Burden of Obstructive Sleep Apnea. Diagnostics 2025, 15(no. 9), 9. [Google Scholar] [CrossRef]
- Orwelius, Lotti; Wilhelms, Susanne; Sjöberg, Folke. Is Comorbidity Alone Responsible for Changes in Health-Related Quality of Life among Critical Care Survivors? A Purpose-Specific Review. Critical Care 2024, 28, 208. [Google Scholar] [CrossRef] [PubMed]
- The overlap of chronic obstructive pulmonary disease and obstructive sleep apnea in hospitalizations for acute exacerbation of chronic obstructive pulmonary disease | Journal of Clinical Sleep Medicine. 2024. [CrossRef]
- Pinto, Venessa L.; Sankari, Abdulghani; Sharma, Sandeep. Continuous Positive Airway Pressure. In StatPearls; StatPearls Publishing, 2025; Available online: http://www.ncbi.nlm.nih.gov/books/NBK482178/.
- Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome | Signal Transduction and Targeted Therapy. 2023. Available online: https://www.nature.com/articles/s41392-023-01496-3.
- Obstructive sleep apnea: Personalizing CPAP alternative therapies to individual physiology: Expert Review of Respiratory Medicine: Vol 16 , No 8—Get Access. (2022). https://www.tandfonline.com/doi/full/10.1080/17476348.2022.2112669.
- Liu, K.; Geng, S.; Shen, P.; Zhao, L.; Zhou, P.; Liu, W. Development and application of a machine learning-based predictive model for obstructive sleep apnea screening. Frontiers in Big Data 2024, 7. [Google Scholar] [CrossRef]
- Kaw, R.; Chung, F.; Pasupuleti, V.; Mehta, J.; Gay, P. C.; Hernandez, A. V. Meta-analysis of the association between obstructive sleep apnoea and postoperative outcome. British Journal of Anaesthesia 2012, 109(6), 897–906. [Google Scholar] [CrossRef]
- Fernandez-Bustamante, A.; Bartels, K.; Clavijo, C.; Scott, B. K.; Kacmar, R.; Bullard, K.; Moss, A. F. D.; Henderson, W.; Juarez-Colunga, E.; Jameson, L. Preoperatively Screened Obstructive Sleep Apnea Is Associated With Worse Postoperative Outcomes Than Previously Diagnosed Obstructive Sleep Apnea. Anesthesia & Analgesia 2017, 125(2), 593. [Google Scholar] [CrossRef]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S. A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C. M. STOP Questionnaire: A Tool to Screen Patients for Obstructive Sleep Apnea. Anesthesiology 2008, 108(5), 812. [Google Scholar] [CrossRef] [PubMed]
- Singh, M.; Liao, P.; Kobah, S.; Wijeysundera, D. N.; Shapiro, C.; Chung, F. Proportion of surgical patients with undiagnosed obstructive sleep apnoea. British Journal of Anaesthesia 2013, 110(4), 629–636. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fan, J.; Guo, R.; Hao, W.; Gong, W.; Yan, Y.; Zheng, W.; Ai, H.; Que, B.; Hu, D.; Ma, C.; Ma, X.; Somers, V. K.; Nie, S. Association of obstructive sleep apnoea with cardiovascular events in women and men with acute coronary syndrome. European Respiratory Journal 2023, 61(1). [Google Scholar] [CrossRef] [PubMed]
- Potential underdiagnosis of obstructive sleep apnoea in the cardiology outpatient setting | Heart. 2015. Available online: https://heart.bmj.com/content/101/16/1288.
- Interactions of Obstructive Sleep Apnea With the Pathophysiology of Cardiovascular Disease, Part 1: JACC State-of-the-Art Review | JACC. 2024. [CrossRef]
- Obstructive Sleep Apnea: A Cardiometabolic Risk in Obesity and the Metabolic Syndrome | JACC. 2012. [CrossRef]
- Devaraj, U.; Rajagopala, S.; Kumar, A.; Ramachandran, P.; Devereaux, P. J.; D’Souza, G. A. Undiagnosed Obstructive Sleep Apnea and Postoperative Outcomes: A Prospective Observational Study. Respiration 2017, 94(1), 18–25. [Google Scholar] [CrossRef]
- Huang, J.; Zhuang, J.; Zheng, H.; Yao, L.; Chen, Q.; Wang, J.; Fan, C. A Machine Learning Prediction Model of Adult Obstructive Sleep Apnea Based on Systematically Evaluated Common Clinical Biochemical Indicators. Nature and Science of Sleep 2024, 16, 413–428. [Google Scholar] [CrossRef]
- Diagnostic accuracy of screening questionnaires for obstructive sleep apnoea in adults in different clinical cohorts: A systematic review and meta-analysis | Sleep and Breathing. 2022. [CrossRef]
- Spurr, Kathy F.; Graven, Michael A.; Gilbert, Robert W. Prevalence of Unspecified Sleep Apnea and the Use of Continuous Positive Airway Pressure in Hospitalized Patients, 2004 National Hospital Discharge Survey. Sleep and Breathing 2008, 12(no. 3), 229–34. [Google Scholar] [CrossRef]
- Best Clinical Practices for the Sleep Center Adjustment of Noninvasive Positive Pressure Ventilation (NPPV) in Stable Chronic Alveolar Hypoventilation Syndromes. Journal of Clinical Sleep Medicine: JCSM : Official Publication of the American Academy of Sleep Medicine 2010, 6(no. 5), 491–509. [CrossRef]
- Current Opinion in Anesthesiology. 2009. Available online: https://journals.lww.com/co-anesthesiology/abstract/2009/06000/screening_for_obstructive_sleep_apnea_before.18.aspx.
- Sleep-disordered breathing in patients with cardiovascular diseases cannot be detected by ESS, STOP-BANG, and Berlin questionnaires | Clinical Research in Cardiology. 2018. Available online: https://link.springer.com/article/10.1007/s00392-018-1282-7.
- Wolfe, R. M.; Pomerantz, J.; Miller, D. E.; Weiss-Coleman, R.; Solomonides, T. Obstructive Sleep Apnea: Preoperative Screening and Postoperative Care. The Journal of the American Board of Family Medicine 2016, 29(2), 263–275. [Google Scholar] [CrossRef]
- Eschbach, Erin; Wang, Jing. Sleep and Critical Illness: A Review. Frontiers in Medicine 2023, 10, 1199685. [Google Scholar] [CrossRef]
- Nadler, J. W.; Evans, J. L.; Fang, E.; et al. A Randomised Trial of Peri-Operative Positive Airway Pressure for Postoperative Delirium in Patients at Risk for Obstructive Sleep Apnea after Regional Anaesthesia with Sedation or General Anaesthesia for Joint Arthroplasty. Anaesthesia 2017, 72(no. 6), 729–36. [Google Scholar] [CrossRef]
- Ali, Mohammed; Cascella, Marco. ICU Delirium. In StatPearls; StatPearls Publishing, 2025; Available online: http://www.ncbi.nlm.nih.gov/books/NBK559280/.
- Outcomes Associated with ICU Delirium. Available online: https://www.icudelirium.org/medical-professionals/delirium/outcomes-associated-with-icu-delirium?ut (accessed on 30 June 2025).
- Eadie, Rebekah; McKenzie, Cathrine A.; Hadfield, Daniel; et al. Opioid, Sedative, Preadmission Medication and Iatrogenic Withdrawal Risk in UK Adult Critically Ill Patients: A Point Prevalence Study. International Journal of Clinical Pharmacy 2023, 45(no. 5), 1167–75. [Google Scholar] [CrossRef]
- Verbraecken, Johan; Dieltjens, Marijke; Op de Beeck, Sara; et al. Non-CPAP Therapy for Obstructive Sleep Apnoea. Breathe 2022, 18(no. 3), 220164. [Google Scholar] [CrossRef] [PubMed]
- Boland, Jason; Boland, Elaine; Brooks, David. Importance of the Correct Diagnosis of Opioid-Induced Respiratory Depression in Adult Cancer Patients and Titration of Naloxone. Clinical Medicine 2013, 13(no. 2), 149–51. [Google Scholar] [CrossRef] [PubMed]
- Anesthesia & Analgesia. 2016. Available online: https://journals.lww.com/anesthesia-analgesia/abstract/2016/05000/does_obstructive_sleep_apnea_influence.18.aspx.
- Murphy, Glenn S.; Brull, Sorin J. Residual Neuromuscular Block: Lessons Unlearned. Part I: Definitions, Incidence, and Adverse Physiologic Effects of Residual Neuromuscular Block. Anesthesia & Analgesia 2010, 111(no. 1), 120. [Google Scholar] [CrossRef]
- Holfinger, S. J.; Lyons, M. M.; Keenan, B. T.; Mazzotti, D. R.; Mindel, J.; Maislin, G.; Cistulli, P. A.; Sutherland, K.; McArdle, N.; Singh, B.; Chen, N.-H.; Gislason, T.; Penzel, T.; Han, F.; Li, Q. Y.; Schwab, R.; Pack, A. I.; Magalang, U. J. Diagnostic Performance of Machine Learning-Derived OSA Prediction Tools in Large Clinical and Community-Based Samples. CHEST 2022, 161(3), 807–817. [Google Scholar] [CrossRef] [PubMed]
- Chiu, H.-Y.; Chen, P.-Y.; Chuang, L.-P.; Chen, N.-H.; Tu, Y.-K.; Hsieh, Y.-J.; Wang, Y.-C.; Guilleminault, C. Diagnostic accuracy of the Berlin questionnaire, STOP-BANG, STOP, and Epworth sleepiness scale in detecting obstructive sleep apnea: A bivariate meta-analysis. Sleep Medicine Reviews 2017, 36, 57–70. [Google Scholar] [CrossRef]
- Chaudhry, R. A.; Zarmer, L.; West, K.; Chung, F. Obstructive Sleep Apnea and Risk of Postoperative Complications after Non-Cardiac Surgery. Journal of Clinical Medicine 2024, 13(9), Article 9. [Google Scholar] [CrossRef]
- Anesthesia & Analgesia. 2017. Available online: https://journals.lww.com/anesthesia-analgesia/abstract/2017/08000/preoperatively_screened_obstructive_sleep_apnea_is.34.aspx.
- Aboussouan, Loutfi S.; Bhat, Aparna; Coy, Todd; Kominsky, Alan. “Treatments for Obstructive Sleep Apnea: CPAP and Beyond.” Review. Cleveland Clinic Journal of Medicine 2023, 90(no. 12), 755–65. [Google Scholar] [CrossRef]
- Ehrenberg, Madeline; Kongpakpaisarn, Kullatham; Intihar, Taylor; Doyle, Margaret; Knauert, Melissa. 0846 Prevalence of Obstructive Sleep Apnea Among Medical ICU Patients. Sleep 2023, 46, no. Supplement_1, A373. [Google Scholar] [CrossRef]
- The Effects of Obstructive Sleep Apnea on the Cardiovascular System: A Comprehensive Review. 2024. Available online: https://www.mdpi.com/2077-0383/13/11/3223.
- Prediletto, Irene; Giancotti, Gilda; Nava, Stefano. COPD Exacerbation: Why It Is Important to Avoid ICU Admission. Journal of Clinical Medicine 2023, 12(no. 10), 3369. [Google Scholar] [CrossRef]
- Validation of the STOP-Bang questionnaire as a screening tool for obstructive sleep apnoea in patients with cardiovascular risk factors: A systematic review and meta-analysis | BMJ Open Respiratory Research. 2021. Available online: https://bmjopenrespres.bmj.com/content/8/1/e000848.
- The accuracy of simple, feasible alternatives to polysomnography for assessing sleep in intensive care: An observational study—Australian Critical Care. 2023. Available online: https://www.australiancriticalcare.com/article/S1036-7314(22)00030-3/abstract.
- Masa, J. F.; Corral, J.; Pereira, R.; Duran-Cantolla, J.; Cabello, M.; Hernández-Blasco, L.; Monasterio, C.; Alonso, A.; Chiner, E.; Rubio, M.; Garcia-Ledesma, E.; Cacelo, L.; Carpizo, R.; Sacristan, L.; Salord, N.; Carrera, M.; Sancho-Chust, J. N.; Embid, C.; Vázquez-Polo, F.-J.; Montserrat, J. M. Effectiveness of home respiratory polygraphy for the diagnosis of sleep apnoea and hypopnoea syndrome. 2011. [Google Scholar] [CrossRef]
- Enhanced machine learning approaches for OSA patient screening: Model development and validation study | Scientific Reports. 2024. Available online: https://www.nature.com/articles/s41598-024-70647-5.
- Benedetti, D.; Olcese, U.; Bruno, S.; Barsotti, M.; Tassoni, M. M.; Bonanni, E.; Siciliano, G.; Faraguna, U. Obstructive Sleep Apnoea Syndrome Screening Through Wrist-Worn Smartbands: A Machine-Learning Approach. Nature and Science of Sleep 2022, 14, 941–956. [Google Scholar] [CrossRef]
- Johnson, Karin Gardner, and Douglas Clark Johnson. “Treatment of Sleep-Disordered Breathing with Positive Airway Pressure Devices: Technology Update.” Medical Devices (Auckland, N.Z.) 8. (2015). 425–37. [CrossRef]
- Zheng, Yizhong, Brendon J. Yee, Keith Wong, Ronald Grunstein, and Amanda Piper. “A Pilot Randomized Trial Comparing CPAP vs Bilevel PAP Spontaneous Mode in the Treatment of Hypoventilation Disorder in Patients with Obesity and Obstructive Airway Disease.” Journal of Clinical Sleep Medicine : JCSM : Official Publication of the American Academy of Sleep Medicine 18, no. 1. (2022). 99–107. [CrossRef]
- Nin, Nicolas; Muriel, Alfonso; Peñuelas, Oscar; et al. Severe Hypercapnia and Outcome of Mechanically Ventilated Patients with Moderate or Severe Acute Respiratory Distress Syndrome. Intensive Care Medicine 2017, 43(no. 2), 200–208. [Google Scholar] [CrossRef]
- Extubation failure in intensive care unit: Predictors and management. Indian Journal of Critical Care Medicine 2008, 12(1), 1–9. [CrossRef]
- Obstructive sleep apnoea heterogeneity and cardiovascular disease | Nature Reviews Cardiology. 2023. Available online: https://www.nature.com/articles/s41569-023-00846-6.
- DeMuro, Jonas P; Mongelli, Michael N; Hanna, Adel F. Use of Dexmedetomidine to Facilitate Non-Invasive Ventilation. International Journal of Critical Illness and Injury Science 2013, 3(no. 4), 274–75. [Google Scholar] [CrossRef] [PubMed]
- Extubation in neurocritical care patients: The ENIO international prospective study | Intensive Care Medicine. 2022. Available online: https://link.springer.com/article/10.1007/s00134-022-06825-8.
- Obstructive Sleep Apnea and Cardiovascular Disease: A Scientific Statement From the American Heart Association | Circulation. 2021. [CrossRef]
- Obstructive Sleep Apnea, Hypertension, and Cardiovascular Risk: Epidemiology, Pathophysiology, and Management | Current Cardiology Reports. 2020. Available online: https://link.springer.com/article/10.1007/s11886-020-1257-y.
- Prediletto, Irene; Giancotti, Gilda; Nava, Stefano. COPD Exacerbation: Why It Is Important to Avoid ICU Admission. Journal of Clinical Medicine 2023, 12(no. 10), 3369. [Google Scholar] [CrossRef] [PubMed]
- Role of ICU-acquired weakness on extubation outcome among patients at high risk of reintubation | Critical Care | Full Text. 2020. Available online: https://ccforum.biomedcentral.com/articles/10.1186/s13054-020-2807-9.
- Zhao, Q-Y; Wang, H; Luo, J-C; Luo, M-H; Liu, L-P; Yu, S-J; Liu, K; Zhang, Y-J; Sun, P; Tu, G-W; Luo, Z. Development and Validation of a Machine-Learning Model for Prediction of Extubation Failure in Intensive Care Units. Front. Med. 2021, 8, 676343. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Santos, D.; Amorim, P.; Silva Martins, T.; Monteiro-Soares, M.; Pereira Rodrigues, P. Enabling Early Obstructive Sleep Apnea Diagnosis With Machine Learning: Systematic Review. Journal of Medical Internet Research 2022, 24(9), e39452. [Google Scholar] [CrossRef]
- Khatana, J.; Thavamani, A.; Umapathi, K. K.; Sankararaman, S.; Roy, A. Obstructive Sleep Apnea Is Associated with Worsened Hospital Outcomes in Children Hospitalized with Asthma. Children 2024, 11(8), Article 8. [Google Scholar] [CrossRef] [PubMed]
- The prevalence of obstructive sleep apnea and its association with pregnancy-related health outcomes: A systematic review and meta-analysis | Sleep and Breathing. 2019. Available online: https://link.springer.com/article/10.1007/s11325-018-1714-7.
- Borsoi, L.; Armeni, P.; Donin, G.; Costa, F.; Ferini-Strambi, L. The invisible costs of obstructive sleep apnea (OSA): Systematic review and cost-of-illness analysis. PLOS ONE 2022, 17(5), e0268677. [Google Scholar] [CrossRef]
- Allen, A. J. M. H.; Bansback, N.; Ayas, N. T. The Effect of OSA on Work Disability and Work-Related Injuries. CHEST 2015, 147(5), 1422–1428. [Google Scholar] [CrossRef]
- Otto, M. Obstructive sleep apnea screening protocol and safety measures: advancing treatment quality and reducing medical emergency team activation in patients with atrial fibrillation, respiratory diseases, and frailty. J Clin Sleep Med. 2024, 20(5), 673–674. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abdul Jafar, N. K.; Mansfield, D. R. Obstructive Sleep Apnoea Screening and Diagnosis Across Adult Populations: Are We Ready? Respirology 2025, 30(no. 7), 555–557. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram. Flow diagram depicting the number of records identified, screened, excluded, and included, with reasons for exclusions at each stage of the review process.
Figure 1.
PRISMA flow diagram. Flow diagram depicting the number of records identified, screened, excluded, and included, with reasons for exclusions at each stage of the review process.
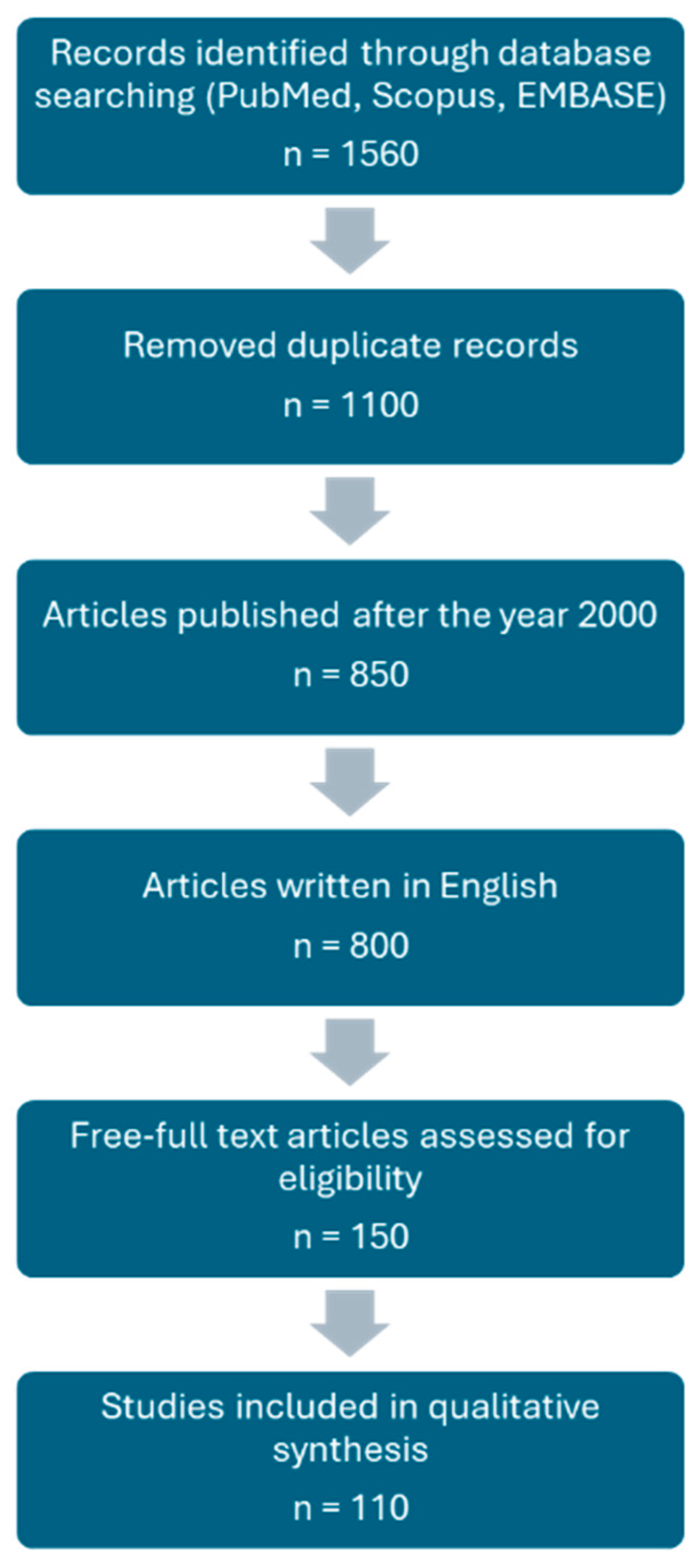
Figure 2.
Illustration of key risk factors for OSA. Conceptual model illustrating mechanisms by which obstructive sleep apnea contributes to hypoxemia, sympathetic activation, inflammation, and adverse cardiopulmonary outcomes in critically ill patients.
Figure 2.
Illustration of key risk factors for OSA. Conceptual model illustrating mechanisms by which obstructive sleep apnea contributes to hypoxemia, sympathetic activation, inflammation, and adverse cardiopulmonary outcomes in critically ill patients.
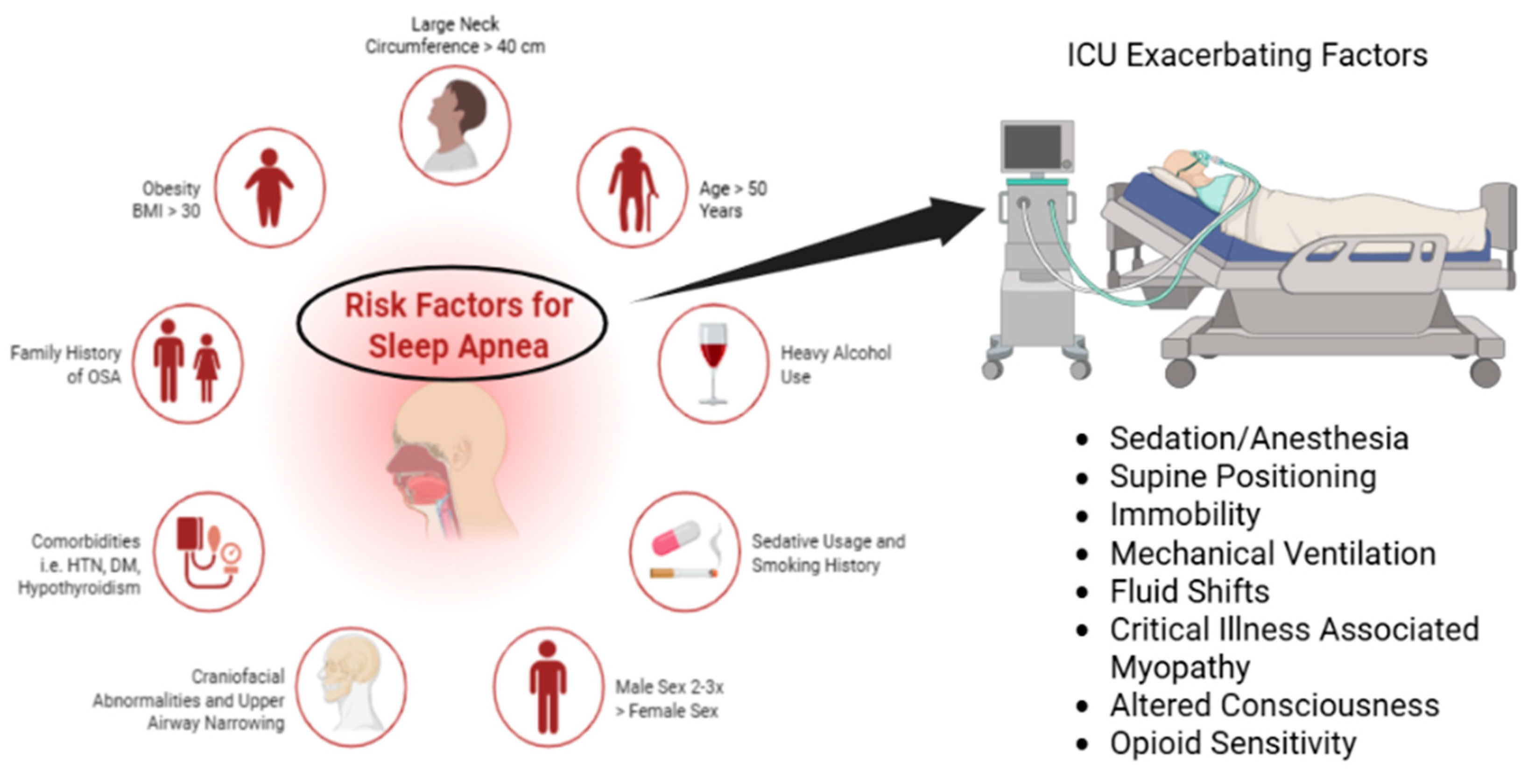
Figure 3.
Clinical warning criteria for OSA. Stepwise clinical workflow for screening, risk stratification, and diagnosis of obstructive sleep apnea in hospitalized and intensive care unit populations.
Figure 3.
Clinical warning criteria for OSA. Stepwise clinical workflow for screening, risk stratification, and diagnosis of obstructive sleep apnea in hospitalized and intensive care unit populations.
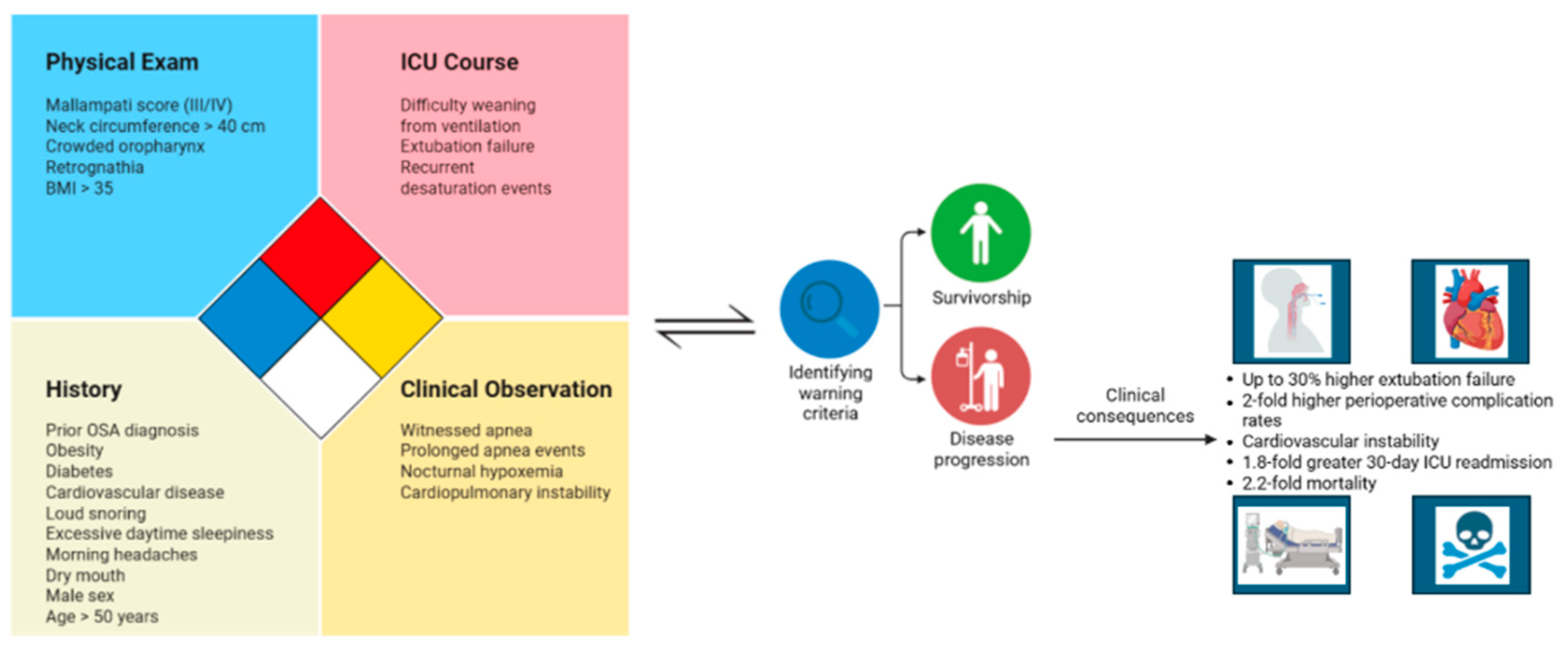

Table 1.
Summarized literature findings of current OSA clinical benchmarks. Summary of mechanical ventilation burden, extubation failure, perioperative complications, cardiovascular risk, ICU readmission, mortality, and neurocognitive outcomes derived from literature.
Table 1.
Summarized literature findings of current OSA clinical benchmarks. Summary of mechanical ventilation burden, extubation failure, perioperative complications, cardiovascular risk, ICU readmission, mortality, and neurocognitive outcomes derived from literature.
| Clinical Benchmarks | Findings from Literature | Clinical Relevance in ICU |
| Mechanical Ventilation |
|
|
| Extubation Failure |
|
|
| Perioperative Complications |
|
|
| Cardiovascular Risk |
|
|
| ICU Readmissions and Mortality |
|
|
| Neurocognitive/Functional Burden |
|
|
Table 2.
Summarized findings of current OSA diagnostic methods. Comparison of diagnostic approaches for obstructive sleep apnea in hospital settings, summarizing feasibility, accuracy, resource requirements, and practical limitations in critically ill patients.
Table 2.
Summarized findings of current OSA diagnostic methods. Comparison of diagnostic approaches for obstructive sleep apnea in hospital settings, summarizing feasibility, accuracy, resource requirements, and practical limitations in critically ill patients.
| Tool/Method | Description | Strengths | Limitations in ICU |
|
Overnight Oximetry / Overnight Pulse Oximetry |
|
|
|
| Machine Learning (ML) Models and Wearables |
|
|
|
| Respiratory Polygraphy / Home Sleep Testing (HST) |
|
|
|
| ASA OSA Checklist |
|
|
|
| STOP-BANG Questionnaire |
|
|
|
| Berlin Questionnaire |
|
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



