
Submitted:
06 January 2026
Posted:
07 January 2026
You are already at the latest version
Abstract
Stroke has been a topic of extensive research due to its debilitating consequences and high mortality. New findings offer a deeper understanding of specific factors that affect post-stroke recovery and identify therapies that may facilitate this process. One such factor was microglia, neuronal immune cells that are highly reactive to cytokines in the neuroenvironment and can, in turn, affect the inflammatory cascades that originate after stroke, making them ideal candidates for immunomodulation in the brain. Many FDA-approved immunotherapies have been found to target distinct inflammatory signaling molecules and responders, including IL-6 inhibitors, IL-13 inhibitors, IL-12/IL-23 inhibitors, B-cell modulators, Type I interferon inhibitors, CAR T-cell therapy, Calcineurin inhibitors, Complement inhibitors, and JAK-STAT pathway inhibitors. The FDA-approved immunotherapies discussed in this review demonstrate potential in modulating the immune response after stroke by targeting key inflammatory pathways involved in secondary brain injury. Future research should focus on defining optimal therapeutic windows, identifying suitable patient populations, determining the most appropriate timing of therapy, and targeting specific immune mechanisms to balance the attenuation of harmful inflammation with the preservation of reparative processes.
Keywords:
immunotherapy
; stroke
; inflammation
; microglia
; neuroinflammation
; cytokines
1. Introduction
A stroke is a cerebrovascular disease that results in damage to the brain. It is currently the second leading cause of death worldwide, as well as a major contributor to long-term disability. Approximately 85% of strokes are ischemic, with hemorrhagic strokes comprising the remaining 15%. In the United States, stroke is the fifth leading cause of morbidity and mortality, with up to 91% of risk factors being modifiable, including diabetes and hypertension [1]. Collectively, the high prevalence, morbidity, and long-term disability associated with stroke underscore its substantial public health burden and the need for therapeutic approaches that address both acute injury and downstream neurological consequences.
Ischemic stroke occurs due to the narrowing or occlusion of cerebral arteries, resulting in insufficient blood supply. This event triggers a rapid and complex inflammatory response characterized by the activation of immune cells and the release of inflammatory mediators [2]. Within minutes to hours of ischemic injury, hypoxia and tissue damage activate cerebral endothelial cells, leading to an increase in the expression of adhesion molecules, including ICAM-1, VCAM-1, and E-selectin. These processes compromise the integrity of the blood–brain barrier (BBB), facilitating infiltration of circulating immune cells. Simultaneously, resident microglia become activated and release proinflammatory cytokines (e.g., TNF-α, IL-1β), chemokines, and reactive oxygen species, creating an environment that recruits peripheral immune cells. Neutrophils are among the first leukocytes to infiltrate, typically within 24 hours, contributing to tissue damage through the release of proteolytic enzymes (such as MMP-9) and reactive oxygen species, while also promoting microvascular obstruction [2,3].
Over the following days, monocytes infiltrate the brain and differentiate into macrophages, exhibiting both pro- and anti-inflammatory roles depending on the microenvironment. T lymphocytes, particularly CD4+ and CD8+ subsets, also infiltrate the ischemic brain, exacerbating injury through the release of cytokines and direct cytotoxicity. While the early inflammatory response is mainly detrimental, specific immune components in the subacute and chronic phases may support repair processes such as angiogenesis and tissue remodeling. Thus, post-stroke inflammation is a dynamic process that is both harmful and beneficial, representing potential therapeutic targets to modulate immune activity and improve neurological outcomes [3].
Given that many of these pathological processes are mediated by immune cell activation and cytokine signaling, interventions that modulate immune function may alter the extent of secondary brain injury after stroke. Immunotherapy, traditionally applied in oncology, has also been utilized for immunodeficiencies, autoimmune disorders, and inflammatory diseases. Thus, we investigate the potential for immune therapies to attenuate post-stroke inflammation, potentially improving rehabilitation outcomes. In this review, we examine FDA-approved immunotherapies from the past decade, focusing on their mechanisms of action and potential relevance for modulating post-stroke neuroinflammation.
2. Role of Microglia In Neuroinflammation
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results and their interpretation, as well as the experimental conclusions that can be drawn.
Microglia, the resident immune cells of the CNS, are among the first responders to neuronal injury following stroke [4]. Consistent with their role, microglia rapidly respond to tissue damage following ischemic injury. Ischemic stroke leads to oxygen and nutrient deprivation, neuronal injury, cerebral edema, BBB breakdown, and a pronounced neuroinflammatory response. This environment triggers the release of damage-associated molecular pattern molecules (DAMPs), including extracellular ATP and UTP, which activate microglia [5].
Under physiological conditions, microglia perform immune surveillance and contribute to homeostatic regulation within the CNS [6]. However, the onset of stroke disrupts oxygen and nutrient supply, leading to neuronal injury, cerebral edema, breakdown of the blood-brain barrier (BBB), and a pronounced neuroinflammatory response. This environment leads to the release of damage-associated molecular pattern molecules (DAMPs), including extracellular ATP and UTP, which act as potent molecular triggers for microglial activation [6].
Activated microglia exhibit distinct functional phenotypes, or polarization states, which modulate neuroinflammation (Figure 1). The M1 phenotype is pro-inflammatory, producing cytokines such as TNF-α, IL-1β, and IL-6, along with reactive oxygen species and inducible nitric oxide synthase (iNOS), contributing to neuronal damage. In contrast, the M2 phenotype is anti-inflammatory, promoting tissue repair through secretion of IL-10, TGF-β, IGF-1, GDNF, and BDNF, as well as phagocytosis of cellular debris [7,8]. The balance between these phenotypes plays a crucial role in determining whether post-stroke inflammation leads to progressive injury or supports recovery.
Microglial polarization is dynamic over time. M2-like microglia appear as early as 12 hours post-insult but decline after 5–7 days, whereas M1 populations increase, peaking at day five. Persistent M1 activation exacerbates secondary neuronal injury and impedes recovery. Microglia also interact with astrocytes, neurons, and oligodendrocytes, influencing neuroinflammation and repair. Pro-inflammatory microglia can induce A1 astrocyte activation, oligodendrocyte damage, and BBB disruption, whereas M2 microglia support A2 astrocytes, oligodendrocyte differentiation, and BBB integrity [9].
Microglia engage in complex bidirectional communication with neurons, particularly in the context of ischemic injury. Neurons are among the most vulnerable cells during stroke and serve as both targets and modulators of the neuroimmune response [10]. They express a variety of regulatory cues commonly classified as “on” and “off” signals that influence microglial activation. For instance, excitotoxic neuronal injury, often mediated by excessive glutamate, can stimulate microglia to release pro-inflammatory cytokines and reactive oxygen species [11]. Neurons also interact directly with microglia via ligand-receptor pairs. Such interactions involve the chemokine fractalkine (CX3CL1) and its receptor, CX3CR1, which is predominantly expressed on microglia [6]. Under pro-inflammatory conditions, neurons increase the expression of CX3CL1, thereby enhancing neuroimmune signaling and microglial activation [6]. Furthermore, neurons may release “help-me” signals that promote microglial phagocytosis of neurotoxic debris and stimulate the production of antioxidant enzymes, thereby supporting neuronal survival [11].
These findings position microglia as a central regulatory element in post-stroke neuroinflammation, suggesting a role for therapeutic strategies that modulate microglial responses. Targeting microglial activation and related immune pathways may help limit secondary brain injury and enhance recovery, providing a potential link to exploring FDA-approved immunotherapies as strategies for controlling post-stroke inflammation.
3. FDA-Approved Immunotherapies: Potential For Stroke Treatment
CD8+ T cells are among the first responders to enter the brain after an ischemic stroke, initiating the inflammatory cascade. These cells play a crucial role in both the acute and chronic phases of ischemic strokes, also providing neuroprotection. Based on previous studies, the reintroduction of CD8 TRL cells after stroke in mice has been shown to reduce infarction and promote long-term neurological recovery [12]. Subsequently, the FDA approved CAR T-cell therapies that utilize the patient’s own genetically modified T cells to target and eliminate the cancer.
ABECMA (idecabtagene vicleucel) is a CAR T-cell therapy used for patients with multiple myeloma, approved by the FDA in March 2021. This medication can only be used after the patient has not responded to proteasome inhibitors and anti-CD38 monoclonal antibodies. ABECMA binds to a protein called BCMA, which is found on the myeloma cells [13]. This medication could have an immune effector cell-associated neurotoxicity syndrome. It can manifest as confusion, seizures, or cerebral edema [14]. Implementing this medication in the regimen of post-stroke patients, knowing these side effects would not be beneficial. A more advanced form of CAR T-cell therapy should be developed.
Tecartus (brexucabtagene autoleucel) is another CAR T cell therapy for patients suffering from B-cell malignancies. It was approved in October 2021; the main target is CD19 and has two indications. The first is for adult patients with relapsed or refractory B-cell precursor acute lymphoblastic leukemia. The second indication is for relapsed or refractory mantle cell lymphoma. It does have a box warning for cytokine release and neurologic toxicities [15]. This is another immunotherapy agent that could be detrimental due to its side effects.
Anktiva (nogapendekin alfa inbakicept-pmln) is the first-in-class IL-15 receptor agonist for BCG-unresponsive non-muscle-invasive bladder cancer, approved by the FDA in April 2024. This medication sets a new standard for immunotherapies beyond checkpoint inhibitors. It works by activating the patient’s own Natural Killer Cells and CD8+ killer T cells and simultaneously stimulates the proliferation of memory killer T cells. This new mechanism enables a durable complete response [16]. IL-15 is known to contribute to post-ischemic inflammation by promoting infiltration and activation of immune cells in the brain, exacerbating neuronal damage. By modulating or blocking the IL-15 pathways, Anktiva could be beneficial for patients after a stroke. It would require careful consideration and other studies first. Studying cytokine pathways, including those involving IL-15, is critical for developing effective methods to halt inflammatory cascades that can impede recovery after a stroke.
Sarilumab, branded as Kevzara, is an interleukin-6 receptor antagonist approved in 2017 for the treatment of moderate to severe rheumatoid arthritis. IL-6 is a proinflammatory cytokine that activates immune cells, including T cells, B cells, and neutrophils, and plays a key role in driving chronic inflammation. By blocking the interleukin-6 receptor, sarilumab effectively disrupts the inflammatory signaling pathways that contribute to the progression of rheumatoid arthritis. Clinical evidence supports its role in significantly improving disease activity and physical function for patients who may not respond to other therapies. The drug's ability to control inflammation is particularly relevant in the context of stroke recovery, where excessive inflammatory responses can worsen neurological outcomes [17].
Satralizumab (Enspryng) is a monoclonal antibody designed to reduce inflammation by targeting the interleukin-6 (IL-6) receptor. By blocking the IL-6 receptor, satralizumab helps to calm this immune response, preventing immune cells from causing further damage to the nervous system. It is currently FDA-approved for neuromyelitis optica spectrum disorder (NMOSD), a rare autoimmune condition where the body’s immune system attacks the optic nerves and spinal cord. By targeting this specific cytokine pathway, satralizumab has shown the ability to reduce relapses and preserve neurological function [18]. Given its impact on immune signaling and neuroinflammation, sarilumab and satralizumab may also hold promise in post-stroke inflammation, where IL-6 contributes to secondary injury.
Ebglyss (lebrikizumab) functions as an interleukin-13 (IL-13) antagonist, binding directly to IL-13 and preventing its interaction with the IL-13 receptor. IL-13 is a cytokine predominantly produced by Th2 cells, which can influence many inflammatory responses, including the skin. Ebglyss reduces inflammatory signaling, alleviating skin symptoms associated with moderate-to-severe atopic dermatitis for which the FDA approved it in September 2024 as a treatment for patients aged 12 years and older [19,20]. It also plays a crucial role in regulating immune responses associated with allergic inflammation and mucosal immunity. It appears to contribute to systemic inflammation, not limited to the lungs, gastrointestinal tract, and central nervous system. This latter association underscores the importance of investigating IL-13 inhibition as a potential therapeutic approach for stroke-related inflammation [21].
Wezlana (ustekinumab-auub), a biosimilar to ustekinumab (Stelara), was approved by the FDA in October 2023 for moderate-to-severe plaque psoriasis, active psoriatic arthritis, and moderately to severely active forms of Crohn’s disease and ulcerative colitis. Ustekinumab has been in clinical use since 2009 and is a monoclonal antibody that targets the p40 subunit shared by interleukins 12 and 23. By blocking these interleukins, Wezlana also interrupts the downstream inflammatory signaling that contributes to immune-mediated diseases. IL-12 and IL-23 are also implicated in neuroinflammatory pathways, which may position Wezlana as a candidate for future investigation in inflammation-related neurological conditions [22,23].
Belimumab (Benlysta) is a monoclonal antibody approved by the FDA in 2011 for treating systemic lupus erythematosus (SLE) and subsequently for lupus nephritis (LN). It functions by inhibiting the B lymphocyte stimulator (BLyS), thereby reducing B-cell activity, which is pivotal in the pathogenesis of lupus [24]. In patients with LN, belimumab is utilized as an adjunct to standard therapy, particularly for those who have not achieved adequate renal response after traditional treatments like corticosteroids and mycophenolate mofetil. Clinical evidence from the pivotal BLISS-LN trial showed that belimumab significantly improved renal response after 104 weeks, with 43% of patients achieving the primary efficacy renal response (PERR) compared to 32% in the placebo group. [25] Additionally, it demonstrated a reduction in proteinuria and a lower risk of renal-related events. Notably, belimumab can modulate inflammatory markers, which may be beneficial in managing post-stroke inflammation. Acute inflammation is a key factor in stroke recovery, and by reducing inflammatory responses, belimumab may enhance healing processes in the brain. Notably, research indicates that persistent inflammation can exacerbate kidney damage in lupus patients. [25] Thus, belimumab's ability to lower inflammatory markers is crucial not only for renal health but also for overall recovery after inflammatory events, such as a stroke. Since its approval, belimumab has provided a new therapeutic avenue for patients with active LN, addressing unmet needs in a patient population with substantial morbidity.
Ocrelizumab (Ocrevus) is a monoclonal antibody that targets CD20-positive B cells, a specific subset of immune cells involved in the chronic inflammation seen in multiple sclerosis (MS). B cells contribute to the inflammatory cascade by producing pro-inflammatory cytokines, presenting antigens, and helping to activate T cells, which can then attack the central nervous system. Ocrelizumab’s ability to modulate CNS-directed immune responses makes it not only a breakthrough for MS but also highlights its potential in other CNS inflammatory conditions, such as neuroinflammatory responses after stroke, where B-cell-driven pathways may contribute to prolonged inflammation and injury [26]. Likewise, Anifrolumab, known by the brand name Saphnelo, is a monoclonal antibody approved in 2021 for the treatment of moderate to severe systemic lupus erythematosus. It works by targeting the type I interferon receptor, which is instrumental in driving the inflammatory processes associated with lupus. By inhibiting this receptor, anifrolumab reduces the activity of type I interferons, key players in autoimmunity and inflammation. [27] Clinical studies have shown that this medication can meaningfully decrease disease activity, offering a valuable option for patients who have not responded well to traditional therapies. By managing inflammation, anifrolumab may also have implications for preventing secondary damage and promoting recovery after a stroke.
Natalizumab (Tysabri) is a monoclonal antibody that works by targeting α4-integrin, a molecule found on the surface of white blood cells. Under normal inflammatory conditions, these integrins help immune cells adhere to blood vessel walls and migrate into tissues, including the central nervous system (CNS). In diseases like multiple sclerosis (MS), this process allows harmful immune cells to cross the blood–brain barrier and attack healthy brain and spinal cord tissue. By blocking α4-integrin, Tysabri prevents this infiltration, thereby reducing neuroinflammation and slowing disease progression [28]. Its mechanism directly interrupts a step in the inflammatory cascade: leukocyte migration. This not only makes it highly effective in treating relapsing forms of MS but also suggests potential therapeutic value in other CNS conditions characterized by immune cell infiltration, such as post-stroke inflammation, where blood–brain barrier disruption and leukocyte entry can exacerbate injury. By keeping immune cells out of the CNS, natalizumab offers a powerful approach to protecting neural tissue from immune-mediated damage.
Voclosporin, marketed as Lupkynis, is a calcineurin inhibitor that received FDA approval in 2021 for the treatment of lupus nephritis. By inhibiting calcineurin, voclosporin reduces T-cell activation and proliferation, both of which are vital in the inflammatory mechanisms underlying lupus nephritis. [29] Pivotal trials have demonstrated that voclosporin significantly enhances renal response in patients, resulting in reduced proteinuria and improved kidney function. (Lupkynis, Its targeted approach not only addresses kidney health but may also contribute to overall inflammatory control. Understanding the interplay of cytokines in inflammatory responses can help refine treatment strategies for both lupus nephritis and post-stroke care.
Tavneos (avacopan) is an FDA-approved oral medication that acts as a selective antagonist of the complement 5a receptor (C5aR), a key participant in the innate immune response. C5a is one of the most potent proinflammatory components of the complement cascade, known for activating and recruiting neutrophils to sites of tissue injury. By blocking C5aR, avacopan reduces neutrophil migration, activation, and the release of damaging enzymes and reactive oxygen species, all of which contribute to inflammation and tissue destruction in diseases like ANCA-associated vasculitis [30]. Although its current FDA approval is limited to systemic vasculitis, this mechanism directly targets a critical step in the inflammatory cascade that is also involved in CNS pathology. In conditions such as ischemic stroke, excessive neutrophil and complement activity can damage the blood-brain barrier and exacerbate neural injury. Therefore, avacopan’s ability to suppress neutrophil-driven inflammation suggests potential therapeutic implications in CNS inflammatory processes, particularly where complement activation and leukocyte infiltration play a role.
Another promising strategy is to disrupt the JAK-STAT signaling pathway, a key driver of pro-inflammatory cytokine activity. Upadacitinib (Rinvoq) is a selective Janus kinase 1 (JAK1) inhibitor that reduces the production and signaling of various cytokines, leading to improved disease activity scores and enhanced quality of life across multiple inflammatory conditions. Since its FDA approval in August 2019 for rheumatoid arthritis, it has received additional approvals for psoriatic arthritis, atopic dermatitis, ulcerative colitis, Crohn’s disease, ankylosing spondylitis, and non-radiographic axial spondyloarthritis [31,32]. Given the involvement of JAK-STAT signaling in neuroinflammation, its mechanism of action raises the possibility that JAK1 inhibition could be relevant in the context of post-stroke inflammatory responses [21].
Baricitinib (Olumiant), an oral inhibitor of JAK1 and JAK2, was first approved in May 2018 for the treatment of rheumatoid arthritis. It later received Emergency Use Authorization during the COVID-19 pandemic and gained full FDA approval in May 2022 for the treatment of hospitalized adults who require oxygen therapy. Additionally, it was approved for the treatment of alopecia areata in June 2022. Through its anti-inflammatory effects, baricitinib has been shown to reduce disease activity in rheumatoid arthritis, lower mortality and accelerate recovery in COVID-19, and promote hair regrowth in alopecia areata. Although it has not been studied in the context of stroke, its broad effects on systemic immune pathways raise the theoretical possibility that it could influence inflammatory mechanisms following cerebrovascular events [33,34].
4. Discussion
The outlook for stroke recovery is becoming increasingly optimistic as emerging research brings forward more personalized and effective therapeutic strategies. Several FDA-approved monoclonal antibodies target pro-inflammatory cytokines and immune signaling pathways, suggesting potential translational relevance for post-stroke inflammation (Table 1). Immunomodulation, particularly through enhancement of regulatory T cell responses, has shown considerable promise in reducing post-stroke inflammation and facilitating neural repair [35]. Additionally, precise manipulation of microglial activation states may help limit secondary neuronal injury and enhance neuroplasticity, highlighting the central role of the immune microenvironment in recovery trajectories [36]. In parallel, precision medicine approaches integrated with artificial intelligence are improving the ability to predict patient-specific outcomes by synthesizing data from neuroimaging, electrophysiological monitoring, and clinical profiles. These predictive models enable the development of more personalized interventions that could optimize functional recovery for each stroke patient. Together, these interdisciplinary innovations are shifting stroke care from a reactive, generalized model to an individualized and precision-guided restoration.
4.1. Monoclonal Antibodies and Cytokine Modulators
- Type I interferon inhibition: Anifrolumab (Saphnelo) blocks type I interferon signaling, reducing systemic inflammation [27].
4.2. Other Immunomodulatory Agents
- Calcineurin inhibitors: Voclosporin (Lupkynis) suppresses T-cell activation and proliferation [29].
- Complement inhibitors: Avacopan (Tavneos) antagonizes C5a receptor signaling, reducing neutrophil-mediated tissue damage [30].
Overall, FDA-approved immunotherapies demonstrate significant potential in modulating the immune response after stroke by targeting key inflammatory pathways involved in secondary brain injury. Therapies directed at cytokine signaling, B-cell activity, or T-cell function may reduce neuroinflammation, preserve BBB integrity, and promote neuroprotection. Cell-based approaches, though promising, require careful consideration due to neurotoxicity risks. Collectively, these observations support the translational potential of immunomodulation in neuroinflammatory conditions and provide a foundation for future clinical investigation.
5. Challenges and Future Directions
Despite promising preclinical results, translating immunotherapies to clinical stroke care faces challenges. Timing is critical; early administration may reduce secondary injury, but late administration could interfere with tissue repair. Safety is another concern, as systemic immunosuppression may increase the risk of infection.
Future research should focus on identifying optimal therapeutic windows, patient stratification based on inflammatory profiles, and combination therapies targeting multiple immune pathways. Precision medicine approaches, including biomarker-guided interventions, may help optimize therapeutic efficacy while minimizing adverse effects.
6. Conclusions
This review highlights the central role of immune-mediated mechanisms in shaping post-stroke neuroinflammation and recovery, with a particular emphasis on microglial activation, cytokine signaling, and adaptive immune responses. Together, these processes contribute to secondary brain injury and represent points at which immune modulation may alter neurological outcomes after stroke.
Several FDA-approved immunotherapies originally developed for oncologic, autoimmune, and inflammatory conditions target molecular pathways implicated in post-stroke inflammation and therefore warrant consideration for therapeutic repurposing. Agents that modulate cytokine activity, T-cell responses, or B-cell function demonstrate mechanistic relevance in this context. However, immune-based therapies differ substantially in their safety profiles, and approaches associated with neurological toxicity, particularly specific cell-based therapies, require careful evaluation before application in stroke populations.
Overall, immunomodulation represents a promising strategy for addressing post-stroke inflammation beyond acute reperfusion strategies. Future research should focus on defining optimal therapeutic windows, appropriate patient populations, therapeutic timings, and immune targets to balance attenuation of harmful inflammation with preservation of reparative processes. Careful clinical investigation will be essential to determine whether repurposed, FDA-approved immunotherapies can safely contribute to improved recovery and long-term neurological outcomes following stroke.
Author Contributions
Conceptualization, Solianne Martinez-Jimenez and Eduardo Alvarez-Rivera; Writing—Introduction, Aitor Gonzalez-Fernandez, Gerson Santiago-Gonzalez and James Llorens-Mercado; Writing—Role of Microglia in Neuroinflammation, Fabiola Colon-Santiago, Carola Garcia-Calderin and Fabyana Gomez-Irizarry; Writing—FDA-Approved Immunotherapies, Armeliz Romero-Ponce, Fabiola Umpierre-Lebron, Paola Roig-Opio and Tiffany Rosa-Arocho; Writing—Discussion, Naira Hernandez-Soto, Ana Martinez-Torres and Victoria Bermudez-Fosse; Writing—Conclusion, Laura Santiago-Rodriguez, Claudia Rodriguez-Castellanos; Writing—original draft preparation, Pamela Rodriguez-Vega and Jordan Acevedo-Rico; Writing—review and editing, Pamela Rodriguez-Vega, Eduardo Alvarez-Vega and Solianne Martinez-Jimenez. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments). Where GenAI has been used for purposes such as generating text, data, or graphics, or for study design, data collection, analysis, or interpretation of data, please add “During the preparation of this manuscript/study, the author(s) used [tool name, version information] for the purposes of [description of use]. The authors have reviewed and edited the output and take full responsibility for the content of this publication.”.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
| FDA | Food and Drug Administration |
| IL | Interleukin |
| CAR | Chimeric Antigen Receptor |
| JAK-STAT | Janus kinase/signal transducers and activators of transcription |
| ICAM | Intercellular Adhesion Molecule |
| VCAM | Vascular Cell Adhesion Molecule |
| BBB | Blood-Brain Barrier |
| TNF-α | Tumor Necrosis Factor alpha |
| MMP-9 | Matrix Metalloproteinase-9 |
| CD4 | Cluster of differentiation 4 |
| CD8 | Cluster of differentiation 8 |
| CNS | Central Nervous System |
| DAMPs | Damage-Associated Molecular Patterns |
| ATP | Adenosine Triphosphate |
| UTP | Uridine Triphosphate |
| iNOS | Inducible Nitric Oxide Synthase |
| IGF-1 | Insulin-like Growth Factor 1 |
| TGF-β | Tumor Growth Factor Beta |
| GDNF | Glial cell line-derived neurotrophic factor |
| BDNF | Brain-derived neurotrophic factor |
| CX3CL1 | C-X3-C motif chemokine ligand 1 |
| CX3CR1 | C-X3-C motif chemokine receptor 1 |
| TRL | Toll-like receptor |
| BCMA | B-Cell Maturation Antigen |
| BCG | Bacillus Calmette–Guérin |
| NMOSD | Neuromyelitis optica spectrum disorder |
| Th2 | T helper type 2 cell |
| SLE | Systemic lupus erythematosus |
| LN | Lupus nephritis |
| BLyS | B lymphocyte stimulator |
| PERR | Primary efficacy renal response |
| MS | Multiple sclerosis |
| C5aR | Complement 5a receptor |
| ANCA | Anti-Neutrophil Cytoplasmic Antibody |
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; et al. Heart disease and stroke statistics, 2020 update. Circulation 2020, 141, e139–e596. Available online: https://pubmed.ncbi.nlm.nih.gov/31992061/.
- Smith, J.; Doe, A. Pathophysiology of ischemic stroke: Neuroinflammatory mechanisms. Stroke Res. Treat. 2020, 2020, 123456. [Google Scholar]
- Lee, K.; Park, S.; Kim, H. Post-stroke inflammation: A double-edged sword. J. Neuroinflammation 2021, 18, 67. [Google Scholar]
- Li, P.; Li, Q.; Wang, X. Microglia in ischemic stroke: Friend or foe? Front. Immunol. 2020, 11, 580870. [Google Scholar]
- Ma, Q.; Liu, Z.; et al. DAMPs and microglial activation after stroke. Neurochem. Int. 2021, 146, 105028. [Google Scholar]
- Shui, X.; Chen, J.; Fu, Z.; Zhu, H.; Tao, H.; Li, Z. Microglia in Ischemic Stroke: Pathogenesis Insights and Therapeutic Challenges. Journal of Inflammation Research 2024, 17, 3335–3352. Available online: https://pubmed.ncbi.nlm.nih.gov/38800598/. [CrossRef]
- Cherry, J.D.; Olschowka, J.A.; O’Banion, M.K. Neuroinflammation and microglial polarization. Neurobiol. Dis. 2014, 62, 43–51. Available online: https://pubmed.ncbi.nlm.nih.gov/24889886/.
- Hu, X.; Leak, R.K.; et al. Microglial M1/M2 polarization dynamics. J. Cereb. Blood Flow Metab. 2012, 35, 1822–1836. Available online: https://pubmed.ncbi.nlm.nih.gov/22933588/.
- Liddelow, S.A.; Guttenplan, K.A.; et al. Neurotoxic reactive astrocytes induced by activated microglia. Nature 2017, 541, 481–487. [Google Scholar] [CrossRef]
- Xu, S.; Lu, J.; Shao, A.; Zhang, J. H.; Zhang, J. Glial Cells: Role of the Immune Response in Ischemic Stroke. Frontiers in immunology 2020, 11, 294. [Google Scholar] [CrossRef]
- Wang, Y.; Leak, R. K.; Cao, G. Microglia-mediated neuroinflammation and neuroplasticity after stroke. Frontiers in cellular neuroscience 2022, 16, 980722. [Google Scholar] [CrossRef]
- Cai, W; Shi, L; Zhao, J; Xu, F; Dufort, C; Ye, Q; Yang, T; Dai, X; Lyu, J; Jin, C; Pu, H; Yu, F; Hassan, S; Sun, Z; Zhang, X; Hitchens, TK; Shi, Y; Thomson, AW; Leak, RK; Hu, X; Chen, J. Neuroprotection against ischemic stroke requires a specific class of early responder T cells in mice. The Journal of Clinical Investigation 2022. [Google Scholar] [CrossRef]
- FDA. CAR T-cell therapy overview. U.S. Food and Drug Administration. Available online: https://www.fda.gov/ (accessed on 22 December 2025).
- Squibb, Bristol Myers. Bristol Myers Squibb’s Abecma (idecabtagene vicleucel) Becomes First CAR T-Cell Therapy Approved in the European Union in Earlier Lines for Triple-Class Exposed Relapsed and Refractory Multiple Myeloma. 2024. Available online: https://investors.bms.com/iframes/press-releases/press-release-details/2024/Bristol-Myers-Squibbs-Abecma-idecabtagene-vicleucel-Becomes-First-CAR-T-Cell-Therapy-Approved-in-the-European-Union-in-Earlier-Lines-for-Triple-Class-Exposed-Relapsed-and-Refractory-Multiple-Myeloma/default.aspx?
- Huang, Z; Chavda, VP; Bezbaruah, R; Dhamne, H; Yang, DH; Zhao, HB. CAR T-cell therapy for the management of mantle cell lymphoma. Mol Cancer 2023, 22(1), 67. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- ImmunityBio. (2024). ImmunityBio Announces FDA Approval of ANKTIVA®, First-in-Class IL-15 Receptor Agonist for BCG-Unresponsive Non-Muscle Invasive Bladder Cancer. Retrieved April 10, 2025, from https://immunitybio.com/immunitybio-announces-fda-approval-of-anktiva-first-in-class-il-15-receptor-agonist-for-bcg-unresponsive-non-muscle-invasive-bladder-cancer/#:~:text=Designated%20an%20FDA%20Breakthrough%20Therapy,%2C%202024%20% E2%80%94%20ImmunityBio%2C%20Inc.
- Sarilumab (Kevzara) for polymyalgia rheumatica. The Medical Letter on Drugs and Therapeutics 2024, 66(1702), 77–78. [CrossRef]
- Enspryng. How ENSPRYNG works. 2024. Available online: https://www.enspryng.com.
- Corren, J. Lebrikizumab in inflammatory diseases. J. Allergy Clin. Immunol. 2024, 153, 123–132. [Google Scholar]
- Hanania, Nicola A.; et al. Efficacy and safety of lebrikizumab in patients with uncontrolled asthma (LAVOLTA I and LAVOLTA II): replicate, phase 3, randomized, double-blind, placebo-controlled trials. The Lancet Respiratory Medicine Volume 4(Issue 10), 781–796. [CrossRef] [PubMed]
- Jin, R.; Yang, G.; Li, G. Inflammatory mechanisms in ischemic stroke: Role of inflammatory cells. Journal of Leukocyte Biology 2010, 87(5), 779–789. [Google Scholar] [CrossRef]
- Costedoat-Chalumeau, N.; et al. Ustekinumab for immune modulation. Rheumatology 2023, 62, 456–465. Available online: https://pubmed.ncbi.nlm.nih.gov/30249508/.
- van Vollenhoven, Ronald F.; et al. Efficacy and safety of ustekinumab, an IL-12 and IL-23 inhibitor, in patients with active systemic lupus erythematosus: results of a multicenter, double-blind, phase 2, randomized, controlled study. The Lancet Volume 392(Issue 10155), 1330–1339. Available online: https://pubmed.ncbi.nlm.nih.gov/30249507/. [CrossRef] [PubMed]
- Blair, H. A.; Duggan, S. T. Belimumab: A Review in Systemic Lupus Erythematosus. Drugs 2018, 78(3), 355–366. [Google Scholar] [CrossRef]
- Belimumab (Benlysta): CADTH Reimbursement Review; Canadian Agency for Drugs and Technologies in Health, 2023.
- Ocrevus (Ocrelizumab) Prescribing Information. Genentech. 2024. Available online: https://www.gene.com/patients/ocrevus (accessed on 22 December 2025).
- Anifrolumab (Saphnelo) Prescribing Information. AstraZeneca. 2023. Available online: https://www.azpicentral.com/saphnelo.pdf (accessed on 22 December 2025).
- Tysabri, *!!! REPLACE !!!*. How TYSABRI Works. 2024. Available online: https://www.tysabri.com.
- Rovin, B. H.; Teng, Y. K. O.; Ginzler, E. M.; Arriens, C.; Caster, D. J.; Romero-Diaz, J.; Gibson, K.; Kaplan, J.; Lisk, L.; Navarra, S.; Parikh, S. V.; Randhawa, S.; Solomons, N.; Huizinga, R. B. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): a double-blind, randomized, multicenter, placebo-controlled, phase 3 trial. Lancet (London, England) 2021, 397(10289), 2070–2080. [Google Scholar] [CrossRef]
- Tavneos (Avacopan) Prescribing Information. ChemoCentryx. 2024. Available online: https://www.chemo.com/avacopan (accessed on 22 December 2025).
- Ananthakrishnan, Ashwin N. Upadacitinib for ulcerative colitis. The Lancet Volume 399(Issue 10341), 2077–2078. [CrossRef]
- Burmester, Gerd R; et al. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): a randomized, double-blind, placebo-controlled phase 3 trial. The Lancet Volume 391(Issue 10139), 2503–2512. [CrossRef]
- Ely, E Wesley Alatorre-Alexander, Jorge, et al. Efficacy and safety of baricitinib plus standard of care for the treatment of critically ill hospitalized adults with COVID-19 on invasive mechanical ventilation or extracorporeal membrane oxygenation: an exploratory, randomized, placebo-controlled trial. The Lancet Respiratory Medicine Volume 10(Issue 4), 327–336. [CrossRef]
- Selvaraj, Vijairam; et al. Baricitinib in hospitalized patients with COVID-19: A meta-analysis of randomized controlled trials. eClinicalMedicine Volume 49, 101489. [CrossRef]
- Li, Yuanwei; McBride, Devin W.; Tang, Yingxin; Doycheva, Desislava; Zhang, John H.; Tang, Zhouping. Immunotherapy as a treatment for stroke: Utilizing regulatory T cells. Brain Hemorrhages 2023, 4(3), 147–153. [Google Scholar] [CrossRef]
- Bonkhoff, A. K.; Grefkes, C. Precision medicine in stroke: towards personalized outcome predictions using artificial intelligence. Brain 2021, 145(2), 457–475. [Google Scholar] [CrossRef]
- Passeron, Thierry; et al. Once-daily upadacitinib versus placebo in adults with extensive non-segmental vitiligo: a phase 2, multicenter, randomized, double-blind, placebo-controlled, dose-ranging study. eClinicalMedicine Volume 73, 102655. [CrossRef] [PubMed]
- Vermeire; Séverine; et al. Efficacy and safety of upadacitinib maintenance therapy for moderately to severely active ulcerative colitis in patients responding to 8-week induction therapy (U-ACHIEVE Maintenance): overall results from the randomised, placebo-controlled, double-blind, phase 3 maintenance study. The Lancet Gastroenterology & Hepatology Volume 8(Issue 11), 976–989.
- U.S. Food and Drug Administration. ABECMA (idecabtagene vicleucel). 2024. Available online: https://www.fda.gov/vaccines-blood-biologics/abecma-idecabtagene-vicleucel.
- U.S. Food and Drug Administration. FDA D.I.S.C.O. Burst Edition: FDA approval of Tecartus (brexucabtagene autoleucel) for adult patients with relapsed or refractory B-cell precursor acute lymphoblastic leukemia. 2024. Available online: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-disco-burst-edition-fda-approval-tecartus-brexucabtagene-autoleucel-adult-patients-relapsed-or.
Figure 1.
Microglia Activation. Graphical summary of molecular signals associated with microglial activation. Created in BioRender. Martinez, S. (2025) https://BioRender.com/5n6uia6.
Figure 1.
Microglia Activation. Graphical summary of molecular signals associated with microglial activation. Created in BioRender. Martinez, S. (2025) https://BioRender.com/5n6uia6.
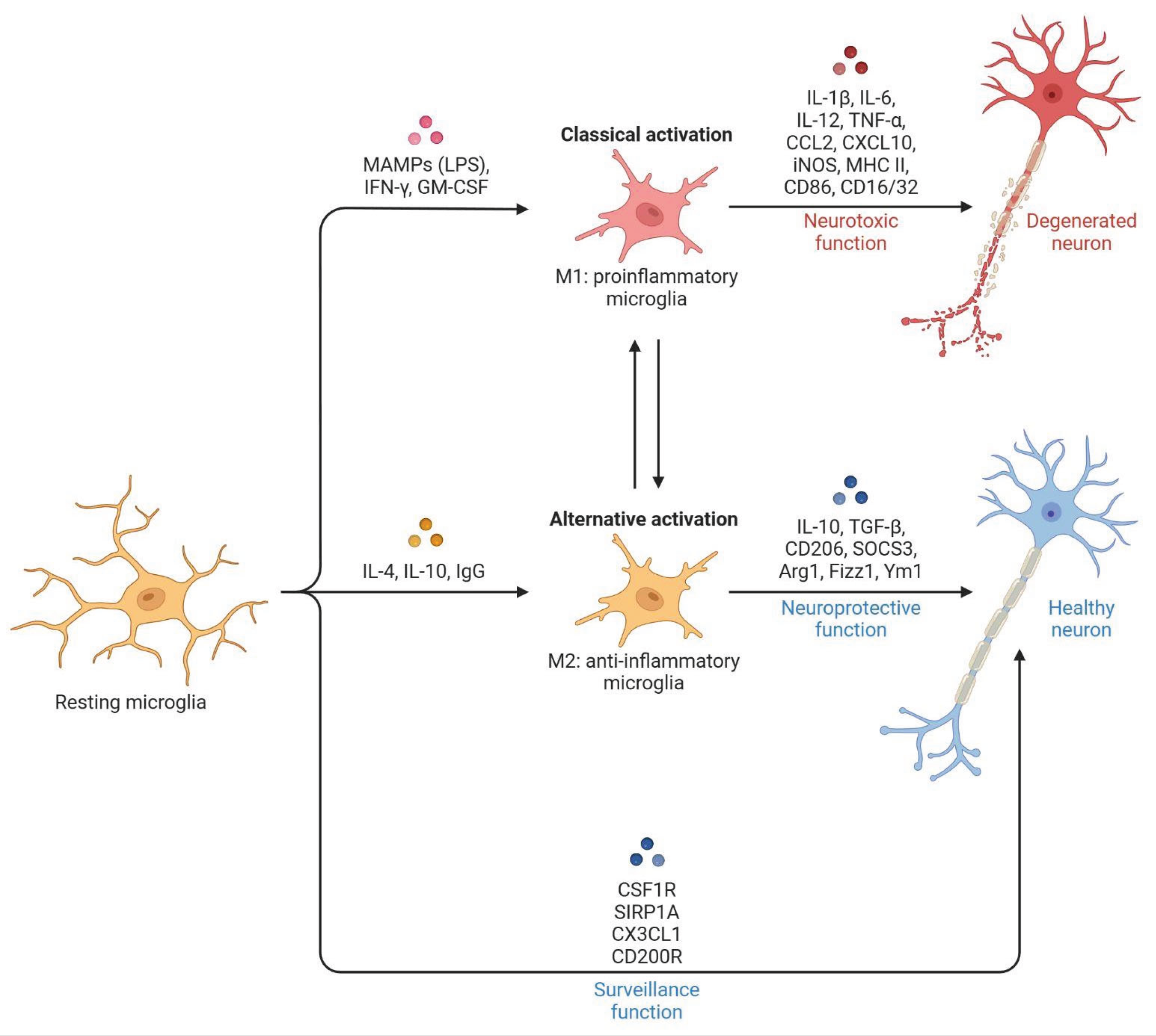

Table 1.
Immunotherapies Review Summary. Current FDA-approved immunotherapies target several signalling molecules implicated in the stroke inflammatory cascade, highlighting their therapeutic potential and need for further study.
Table 1.
Immunotherapies Review Summary. Current FDA-approved immunotherapies target several signalling molecules implicated in the stroke inflammatory cascade, highlighting their therapeutic potential and need for further study.
| Immunotherapy | Main Signaling Target | Approved Treatment |
| ABECMA | BMCA | Mylenoma |
| Tecartus | CD19 | B-Cell Malignancies |
| Anktiva | IL-15 | Bladder Cancer |
| Kevzara | IL-6 | Rheumatoid Arthritis |
| Enspryng | IL-6 | NMOSD |
| Ebglyss | IL-13 | Atopic Dermatitis |
| Wezlana | IL-12, IL-23 | Plaque Psoriasis, Psoriatic Arthritis, Crohn’s Disease, Ulcerative Colitis |
| Benlysta | BLyS | Systemic Lupus Erythematosus |
| Ocrevus | CD20+ B-Cells | Multiple Sclerosis |
| Tysabri | α4-integrin | Multiple Sclerosis |
| Lupkynis | Calcineurin | Lupus Nephritis |
| Tavneos | C5aR | Systemic Vasculitis |
| Rinvoq | JAK1 | Rheumatoid Arthritis |
| Oluminant | JAK1, JAK2 | COVID-19, Alopecia Areata, Rheumatoid Arthritis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



