1. Introduction
Breast cancer is still the most frequently diagnosed cancer in women around the world. In 2022, the Global Cancer Observatory (GLOBOCAN) reported more than two million new cases.[
1] Among its molecular subtypes, luminal A and luminal B—defined by the presence of estrogen and/or progesterone receptor expression—comprise the majority of diagnoses and are traditionally associated with a more favorable biological and clinical profiles compared to their HER2-positive and triple-negative counterparts.[
2,
3] However, recent evidence highlights considerable heterogeneity in individuals with these subtypes as shown by variabilities in clinical presentations as well as histopathological architecture, suggesting underlying genomic alterations.[
4]
This genomic alterations-derived variability is known to arise not only from somatic alterations but also from inherited germline variants, including pathogenic variants and variants of uncertain significance (VUS) in genes such as
BRCA1,
BRCA2,
PALB2, and others involved in DNA repair pathways.[
5] While tumors that carry pathogenic germline variants may phenotypically appear similar to the sporadic cases, they often differ in their molecular biology and clinical courses as they follow distinct molecular trajectories.[
6,
7] These distinctions are important because they can affect tumor behavior, inform the risk assessment, and steer treatment and surveillance strategies. This is especially true for patients with significant family histories or confirmed pathogenic germline variants.
Emerging evidence from research undertaken in East and Southeast Asia indicates marked heterogeneity in both the frequency and distribution of hereditary pathogenic variants among individuals with breast malignancies. A Japanese cohort reported that pathologic variants were found in 5.7% of cases overall, with the majority falling in the group of women aged before 40, at 15%. This rate significantly dropped to 3.2% in patients aged 80 and older. Moreover,
BRCA1 and
BRCA2 comprised about two-thirds of all pathogenic variants across various age groups. [
8] In a Thai study, pathogenic germline variants were reported in 12.5% (8/64) of cases, comprising
BRCA1 (4.7%),
BRCA2 (6.3%),
ATM (1.6%), and
PALB2 (1.6%), with one patient exhibiting concomitant variants in
BRCA2 and
ATM.[
9] Meanwhile, a Chinese study of 356 patients found deleterious germline variants in 21.6% of cases across a panel of 48 cancer-related genes, with
BRCA1/2 pathogenic variants accounting for the most (7.0%), followed by
RAD50 and
ATM pathogenic variants at 1.4% each.[
10]
Despite these associations being increasingly explored in East-Asian and Western populations, Indonesia remains underrepresented in germline variant profiling. The prevalence, spectrum, and clinical implications of pathogenic variants and VUS among Indonesian patients with luminal breast cancer subtypes remain largely unknown. This represents a significant barrier to implementing personalized cancer care, especially in a setting where stage at diagnosis remains advanced in most cases, and molecular testing is not routinely integrated into clinical workflows.
In this context, the present pilot study aimed to characterize the spectrum of germline variants detected by multigene panel testing in Indonesian women with luminal A and luminal B breast cancer, and to explore potential associations between pathogenic or likely pathogenic variants and baseline clinicopathological features. The findings are intended to provide hypothesis-generating data to inform larger validation studies and future development of tailored genetic risk assessment in this population.
2. Materials and Methods
This cross-sectional study was conducted at Dharmais National Cancer Center Hospital, Jakarta, Indonesia. Women aged ≥18 years with a recent diagnosis of luminal A or luminal B breast cancer were recruited. Subtyping was confirmed by immunohistochemical assessment performed at the same institution. Patients were eligible if they had not received any prior systemic therapy and did not have a diagnosis of primary cancer in any other organ. The diagnosis period spanned from January 2025 to May 2025.
Patients who consented to genetic testing underwent peripheral blood collection (5 mL) stored in EDTA-containing tubes. Genomic DNA was isolated from the buffy coat fraction using the QIAamp DNA Mini Kit (Qiagen, Germany), following the manufacturer’s protocol. DNA quality and quantity were assessed spectrophotometrically to ensure suitability for downstream analysis. Samples that met quality thresholds were subjected to targeted sequencing using the TruSight Hereditary Cancer Panel (113 genes) (Illumina, USA).
Library preparation and target enrichment were carried out using the Illumina DNA Prep protocol. Sequencing was carried out using the Illumina NextSeq 550 platform. Primary sequencing data were processed through secondary and tertiary analyses using the DRAGEN Bio-IT Platform (Illumina), generating Variant Call Format (VCF) files. Variant annotation was conducted using the Variant Effect Predictor (VEP) tool from Ensembl. All identified variants were categorized according to the American College of Medical Genetics and Genomics (ACMG) standards based on clinical relevance.
Clinical and pathological data—including demographic characteristics, personal and family medical history (pedigree), hematological profiles, tumor stage at diagnosis, histopathological findings, and tumor grade—were collected via direct patient interviews and retrieved from the hospital’s electronic medical record system.
2.1. Statistical Analysis
Statistical analyses were carried out using IBM SPSS Statistics version 25.0 (IBM Corp., Armonk, NY, USA). The characteristics of the cohort were summarized descriptively. Categorical data were reported as counts with corresponding percentages, while continuous data were summarized as mean values with their standard deviations. Bivariate analyses were performed to assess associations between germline variant status—categorized as “no finding or variant of uncertain significance (VUS)” versus “likely pathogenic or pathogenic”—and selected clinical and pathological variables. Pearson’s Chi-Square test was applied for comparisons involving adequate sample sizes, while Fisher’s exact test (two-sided) was used in cases with small expected cell counts. The clinical variables evaluated included age group (≤40 vs. >40 years), menopausal status, stage at diagnosis (early vs. advanced), molecular subtype, Ki67 proliferation index (<20% vs. ≥20%), histological type, histological grade, and first-degree relatives’ history of breast cancer. Odds ratios (ORs) with 95% confidence intervals (CIs) were computed to assess the strength of associations. Statistical significance was defined as a p-value < 0.05.
3. Results
3.1. Patient Characteristics
Table 1 shows the demographic data of the total of 31 female patients with luminal-type breast cancer who were enrolled in this study. The mean age at diagnosis was 47.87 ± 9.52 years, with the majority (77.4%) aged over 40. Educational attainment was predominantly at the senior high school level or higher (80.6%). Most participants were multiparous (83.9%), and over half (54.8%) had a history of hormonal contraceptive use. Passive smoking exposure was reported by 22.6% of the patients.
Approximately two-thirds (64.5%) of the patients were premenopausal at the time of diagnosis. Obesity, based on Asia-Pacific BMI criteria, was common in 51.6% of cases. Notably, 74.2% of patients had advanced-stage disease (Stage IIIB or IV), highlighting a worrying delay in diagnosis.
With regard to molecular subtypes, 48.4% had Luminal B HER2-positive tumors, 35.5% had Luminal B HER2-negative, and 16.1% had Luminal A subtype. A high Ki67 index (≥20%), suggestive of elevated tumor proliferative activity, was seen in 80.6% of cases. The predominant histological type was invasive breast carcinoma of no special type (NST), accounting for 87.1% of cases. Mixed histological patterns were observed in 9.7% of patients. More than half of the tumors (58.1%) were poorly differentiated (grade III), reflecting a more aggressive phenotype.
3.2. Germline Variant Profiles
Germline variants were detected in 87.1% (27/31) of the patients (
Table 2). Among these, 18 patients (58.1%) harbored variants of uncertain significance (VUS), while three (9.7%) and six (19.4%) carried likely pathogenic and pathogenic variants, respectively. The most frequently encountered genes across the entire variant spectrum were
BARD1, POLE, and
RECQL4.
Notably, among the VUS, BARD1 variants were observed in five different patients (16.1%), POLE in four patients, and RECQL4 in three patients. These variants are not currently annotated in either ClinVar or gnomAD, suggesting they may represent population-specific polymorphisms or previously uncharacterized variants with uncertain clinical relevance.
Pathogenic and likely pathogenic variants were identified in seven distinct genes: BRCA2, PALB2, RECQL4, NF1, CDKN2A, ERCC3, SPINK1, and MUTYH. BRCA2 and RECQL4 were the most recurrent among these. Several patients exhibited multiple germline alterations, including combinations of pathogenic and VUS variants, highlighting the genetic complexity of breast carcinogenesis in this study.
3.3. Association Between Germline Variants and Clinical Variables
Bivariate analysis (
Table 3) revealed several clinically significant associations. A notable correlation was identified between the existence of pathogenic or likely pathogenic variants and a family record of breast cancer in relatives of the first degree (p = 0.022, Chi-square; p = 0.077, Fisher's exact), with an odds ratio of 15.0 (95% CI: 1.1–204.5).
Histological type was also significantly associated with variant classification (p = 0.019). All patients with mixed-type invasive carcinoma harbored pathogenic or likely pathogenic variants, compared to only 22.3% of those with NST histology. These findings suggest a possible connection between histological differences and underlying germline pathogenicity.
No significant associations were found between variant classification and age, menopausal status, tumor stage, molecular subtype, Ki67 index, or tumor grade (all p > 0.05).
4. Discussion
This study contributes to the germline variant landscape of luminal subtype breast cancer in the underrepresented Indonesian population. Of the 31 patients included in this study, 87.1% of the subjects carried detectable variants, including those with pathogenic, likely-pathogenic, and VUS. This finding is disproportionately very high, compared to the similar study conducted by Biancolella et al. for the 51 subjects from Burkina Faso, showing that only 24% of the subjects carried pathogenic variants, VUS, and novel undescribed variants.[
11] With 66,271 new cases per year reported with a mortality rate of 22,598 cases in Indonesia itself,[
1] this should raise concern for more precise risk stratification in the target population when they first present to the healthcare facility, as it would benefit both the patients and clinicians in providing more comprehensive information, particularly regarding treatment strategies. As also noted by a previous British study, cancer genetics should be progressively integrated into the practice of general practitioners, breast surgeons, oncologists, and nurses with regard to ethical matters.[
12]
A notable finding revealed a statistically significant association between histological type and variant status (p = 0.019), with all cases of mixed invasive carcinoma harboring likely pathogenic or pathogenic variants. This study emphasizes the necessity of incorporating genetic testing into clinical practice, serving as a fundamental element for future risk modeling and stratification in newly diagnosed patients, as well as a crucial instrument for informing treatment strategies, despite prior research indicating that mixed invasive carcinomas do not consistently exhibit a poorer biological profile compared to invasive carcinoma of no special type (NST).[
13,
14,
15].
4.1. Pathogenic and Likely-Pathogenic Variants and Their Clinical Correlations
This study also highlights an important finding where 100% of the subjects with mixed invasive carcinoma subtype carry either pathological or likely-pathological variants, including
RECQL4,
NF1, and
MUTYH–alongside additional VUS such as
BRCA2,
RAD51,
CTAGE1, and
RB1. These variants have been proven to play a role in the pathogenesis of breast cancer in several mechanisms, including dysfunction in homologous recombination (HR) and base excision repair (BER), as well as regulation failure in the RAS/MAPK signaling pathway. Previous clinical research showed that elevated
RECQL4 expression correlates with more aggressive cancer types[
16], while breast tumors associated with
NF1 typically have a worse prognosis and are frequently expressing negativitiees for estrogen receptor (ER) and progesterone receptor (PR). Women with pathogenic
NF1 germline variants exhibit a markedly elevated risk of breast cancer—up to fivefold before to age 50, and roughly 3.5 times higher overall.[
17] Tumors in individuals with a monoallelic
MUTYH pathogenic germline variants exhibited significantly larger sizes, higher histologic grades, and more high-risk biomarker characteristics (including HER2-positivity and triple-negative subtype) compared to breast cancer patients with other susceptibility genes, excluding
BRCA1.[
18]
Genetic alterations and copy number gains of the
RECQL4 gene—which encodes a helicase essential for DNA replication and repair—have been linked to breast cancer through several oncogenic mechanisms.
RECQL4 plays a key role in homologous recombination (HR) and base excision repair (BER), and its dysfunction compromises the repair of double-strand breaks and oxidative DNA damage. A missense germline variant, such as the Proline-to-Serine substitution at position 448 identified in this study, may disrupt the structural integrity of the helicase domain or hinder its interaction with other DNA repair proteins. This alteration contributes to genomic instability and an elevated mutation burden. In addition to point mutations, some breast tumors exhibit
RECQL4 copy number gains and overexpression. This dysregulation promotes accelerated S-phase progression, promotes DNA replication, and drives uncontrolled cell proliferation by upregulating genes involved in the cell cycle and mitosis.[
19,
20] Moreover,
RECQL4 dysregulation affects hormone receptor–positive breast cancers by interfering with cell cycle checkpoints and disrupting estrogen receptor–associated gene expression.[
21] From a therapeutic perspective, these findings are in line with those reported by Liu et al. (2024), which demonstrated that pathogenic
RECQL4 germline variants – particularly when co-occurring with alterations in
BRCA2 and
PALB2—may enhance tumor susceptibility to targeted therapies, including PARP inhibitors.[
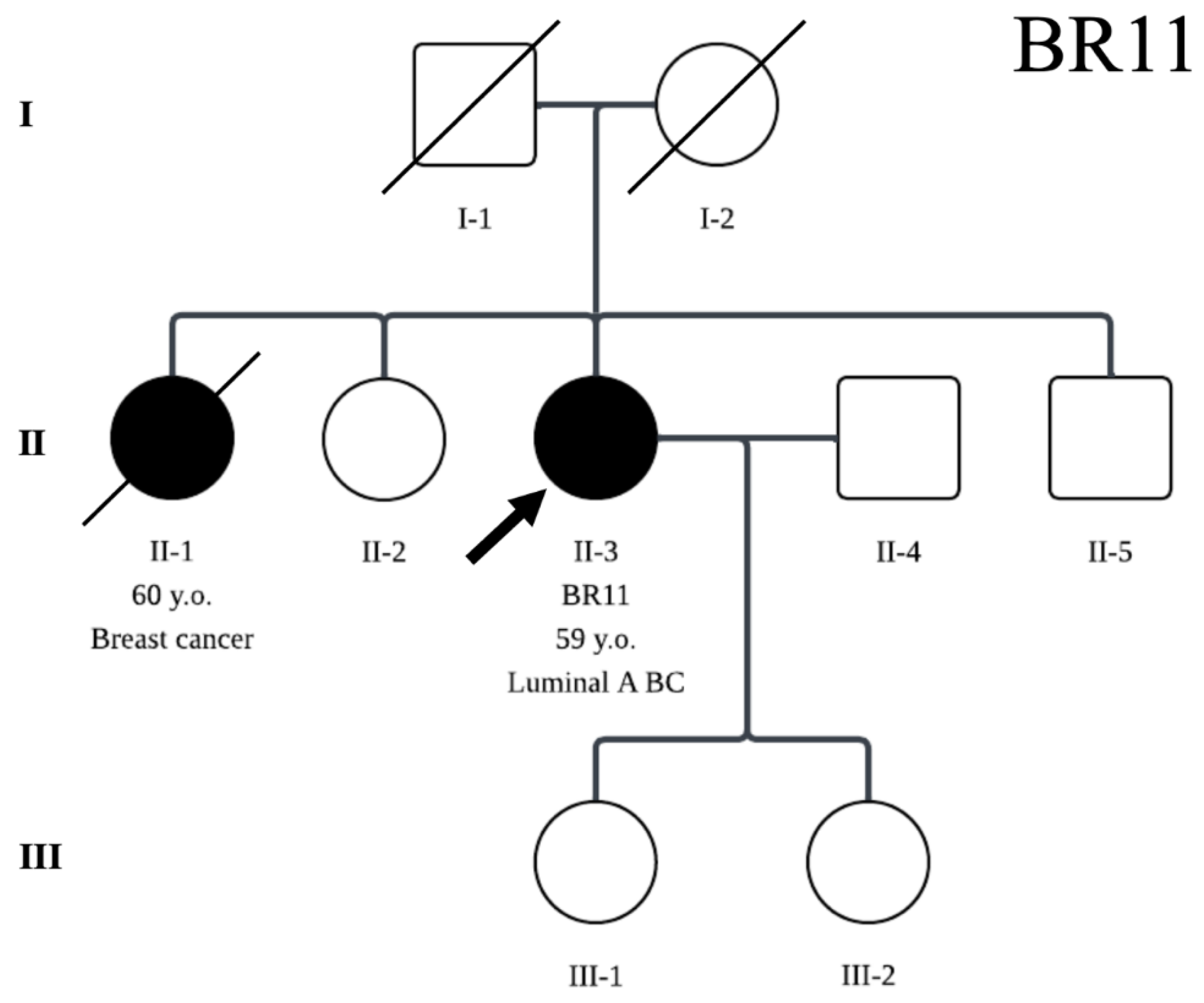
22] The
BRCA2 variant identified in this study is currently classified as a VUS and necessitates further validation to assess its clinical relevance. Additionally, the potential co-segregation of
RECQL4 and
BRCA2 germline variants within the family warrants further investigation, particularly given the patient’s reported family history of breast cancer involving an affected elder sister (
Figure 1).
Another notable finding is a single-nucleotide variant in the
NF1 gene (c.3817A>G; p.Thr1273Ala).
NF1 is a tumor suppressor gene known for its importance in predicting outcomes in various malignancies, including breast cancer. Alterations in
NF1 have been linked to worse survival rates in breast cancer patients. Moreover, individuals with germline
NF1 pathogenic variants exhibit an elevated lifetime risk of acquiring numerous cancers, including those of the breast, ovary, liver, lung, bone, thyroid, and gastrointestinal tract.[
23] Neurofibromin, encoded by the
NF1 gene, acts as a GTPase-activating protein that inhibits the RAS signaling pathway, which encompasses HRAS, NRAS, and KRAS. The absence of neurofibromin results in persistent RAS activation, promoting cancer progression. Mouse models of chromosomal instability have demonstrated that
NF1 deletions are prevalent in mammary adenocarcinomas, underscoring
NF1’s role as an essential tumor suppressor and a key factor in breast cancer formation. These results emphasize the cancer-promoting effects of disrupted RAS/MAPK signaling after
NF1 loss.[
24]
NF1 is classified as a moderate-penetrance gene,[
25,
26] with cancer risk estimates comparable to those associated with pathogenic variants in
ATM,
CHEK2, and
NBN. The National Comprehensive Cancer Network (NCCN) guidelines recommend annual mammography starting at age 30 and suggest considering contrast-enhanced breast MRI between ages 30 and 50 for individuals carrying pathogenic
NF1 germline variants.[
27] Through a similar biological context, this study identified a likely pathogenic
NF1 germline variant co-occurring with an
RB1 germline variant of uncertain significance (VUS).
RB1 is a tumor suppressor gene, the inactivation of which results in a defect of G1/S checkpoint control, although the synergistic impact of
NF1 and
RB1 as a VUS in this case should be further investigated.
A pathogenic germline variant in the
MUTYH gene was also identified in this study.
MUTYH encodes a DNA glycosylase involved in the BER pathway,[
28] which prevents G:C to T:A transversions caused by oxidative DNA damage. Specifically, oxidative stress can lead to the formation of 8-oxo-7,8-dihydro-2-deoxyguanosine (8-oxoG), which results in adenine mispairs during DNA replication; failure to correct this error via
MUTYH-mediated repair results in G:C to T:A transversions.[
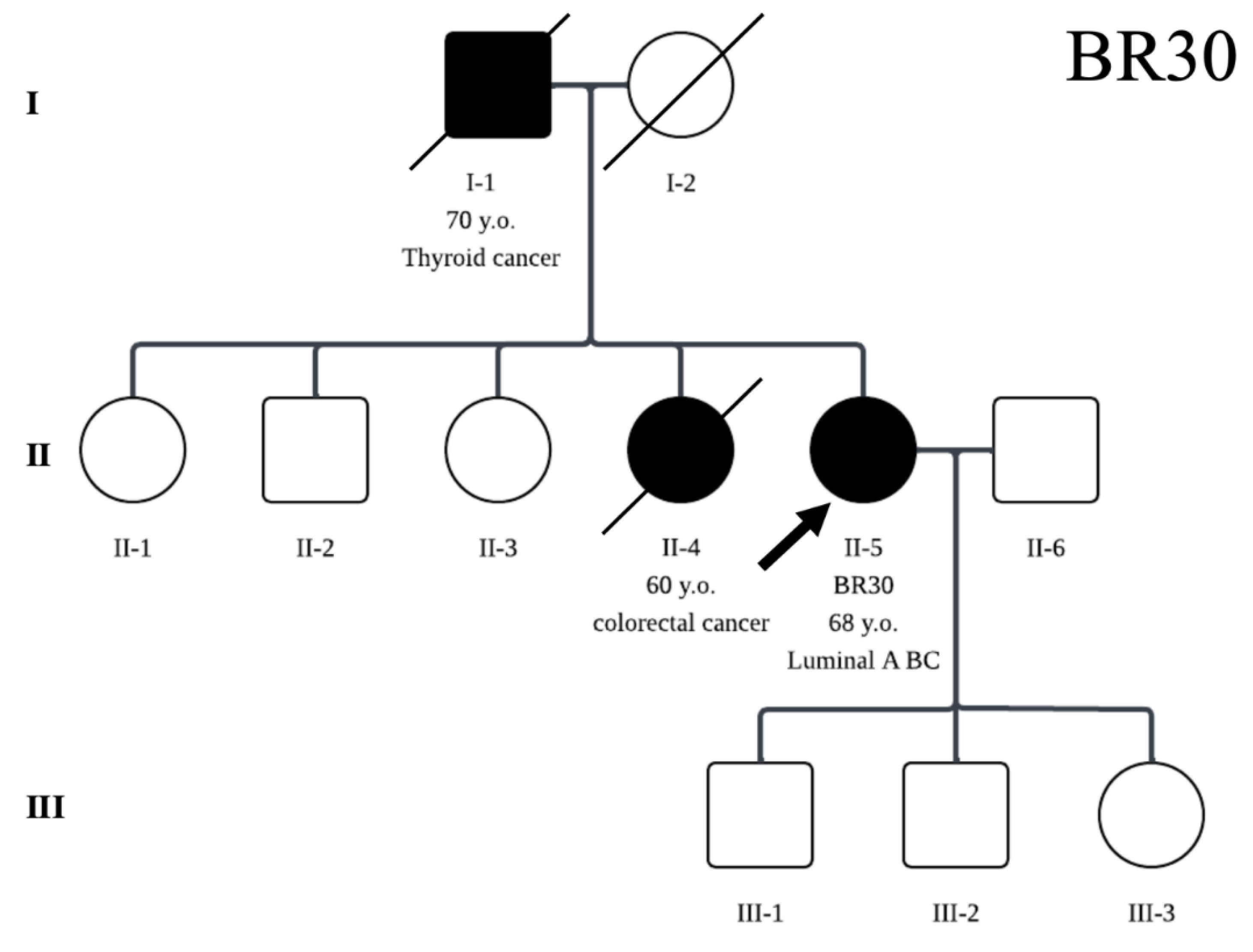
29] In this study, a nonsense pathogenic germline variant (c.383G>A; p.Trp128Ter) was detected in the subject with a family history of colorectal cancer in her elder sister and thyroid cancer in her father (
Figure 2). Biallelic pathogenic variants in
MUTYH are well-established causes of
MUTYH-associated polyposis (MAP), an autosomal recessive disorder that elevates the risk of colorectal cancer. The family history observed in this case warrants further investigation into the potential contribution of
MUTYH pathogenic germline variants to both breast and colorectal cancer risk in closely related individuals. This finding aligns with prior studies showing that this particular variant has been prevalent among Dutch patients with adenomatous polyposis, accounting for approximately 75% of
MUTYH pathogenic variants.[
30] Notably, this variant has also been reported in Egyptian families with a history of familial breast cancer, as well as in Dutch families with co-occurring breast and colorectal cancers.[
31,
32] Thus, this study’s findings may contribute to the growing evidence supporting the involvement of
MUTYH pathogenic germline variants in breast cancer susceptibility and may inform future risk assessment strategies and therapeutic development.
4.2. Family History and Variant Status
Although the association between family history of breast cancer and the presence of pathogenic germline variants did not reach statistical significance by Fisher's exact test (p = 0.077), it was found to be significant using Chi-Square analysis (p = 0.022). This discrepancy shows the study's limited statistical power. However, it matches wider observations that pathogenic germline variants often cluster in families with a history of cancer.[
33] Furthermore, this study corroborates previous findings, as two of the three patients with mixed histology types, harboring likely pathogenic and pathogenic variants, all had a family history of cancer in their first-degree relatives (
Figure 1 and
Figure 2).
4.3. Implications for Histopathological Interpretation
These results also emphasize that mixed histological types—traditionally considered ambiguous or rare—may be phenotypic markers of underlying hereditary pathogenic variants, particularly in DNA repair and cell-cycle regulation genes. The statistically significant enrichment of pathogenic/likely-pathogenic germline variants in mixed histology tumors provides a strong rationale for histopathology-directed genetic testing, which could optimize resource allocation in low-to-middle-income countries.
4.4. Study Strengths and Limitations
This study also underscores that mixed histological subtype—often regarded as uncommon or diagnostically ambiguous—may serve as phenotypic indicators of underlying hereditary pathogenic variants, particularly in DNA repair and cell cycle regulation genes. The statistical significance of pathogenic and likely pathogenic variants in tumors with mixed histology supports the implementation of histopathology-guided genetic testing. Such an approach may be particularly valuable for optimizing genetic testing strategies and resource utilization in low- and middle-income settings.
5. Conclusions
This pilot study provides the first description of germline pathogenic and likely pathogenic variants in Indonesian women with luminal A and luminal B breast cancer. Approximately one-third of patients were found to carry clinically relevant germline variants, most frequently involving BRCA2, PALB2, and RECQL4. Exploratory analyses suggest potential enrichment of pathogenic variants among patients with mixed invasive histology and those with a positive first-degree family history of breast cancer.
These findings should be interpreted as hypothesis-generating and require validation in larger prospective cohorts. Nevertheless, the results highlight the genetic heterogeneity of luminal breast cancer in this under-represented population and provide an initial foundation for future population-adapted genetic risk assessment and screening strategies in Indonesia.
Supplementary Materials
The datasets produced and/or examined in this study are not openly accessible owing to the sensitive genomic information involved and the need to protect participant confidentiality. However, the data may be obtained from the corresponding author upon reasonable request and following the necessary institutional clearances.
Author Contributions
NS contributed to the conceptualization, collected the data, validation, supervision, resource provision, writing of the original draft, project administration, and funding acquisition; YHP contributed to the conceptualization, methodology, collected the data, formal analysis, investigation, data curation, visualization, and writing of the original draft; FS was involved in the methodology, formal analysis, investigation, data curation, and visualization; RK participated in the conceptualization, collected the data, validation, supervision, resource provision, and review and editing of the manuscript.
All authors have reviewed and approved the final manuscript, confirm adherence to the authorship criteria specified, and assert that the manuscript constitutes honest and original work.
Funding
This study was funded by Universitas Indonesia under Contract No. NKB-283/UN2.RST/HKP.05.00/2024, as part of the International Indexed Publication Grant (Publikasi Terindeks Internasional; PUTI) Q1.
Institutional Review Board Statement
The study protocol received approval from the Medical Research Ethics Committee at Dharmais National Cancer Center Hospital, Jakarta, Indonesia (Approval No. 305/KEPK/IX/2023). Written informed consent was obtained from every participant prior to enrolment. The study procedures adhered to the ethical standards set forth in the Declaration of Helsinki.
Informed Consent Statement
Written consent for publication of anonymised data was obtained from all participants.
Data Availability Statement
In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Please refer to suggested Data Availability Statements in section “MDPI Research Data Policies” at
https://www.mdpi.com/ethics. If the study did not report any data, you might add “Not applicable” here.
Conflicts of Interest
Conflict of interest relevant to this article was not reported.
References
- Ferlay J, Ervik M, Lam F, Laversanne M, Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I, Bray F (2024). Global Cancer Observatory: Cancer Today. Lyon, France: International Agency for Research on Cancer. Available from: https://gco.iarc.who.int/today, accessed [15 June 2025].
- Sibghatullah H, Verma H, Sangi S, Memon F, Soomro S. Retrospective Five-Year Survival Evaluation: Analyzing Breast Cancer Molecular Subtypes through Comprehensive Clinical Profiles and Prognostic Survival Trends. Transylvanian Review. 2024 Nov 8;32(3).
- Thi-Qar, T.-Q.D.O.E.I.; Al-Hilali, K.A.; Aljawher, R.Q.; Faris, S.A. Protein expression of estrogen, progesterone, and human epidermal growth factor receptors in young Iraqi women with breast cancer. Ukr. Biochem. J. 2024, 96, 38–43, . [CrossRef]
- Testa, U.; Castelli, G.; Pelosi, E. Breast Cancer: A Molecularly Heterogenous Disease Needing Subtype-Specific Treatments. Med Sci. 2020, 8, 18, . [CrossRef]
- Nik-Zainal, S.; Davies, H.; Staaf, J.; Ramakrishna, M.; Glodzik, D.; Zou, X.; Martincorena, I.; Alexandrov, L.B.; Martin, S.; Wedge, D.C.; et al. Landscape of somatic mutations in 560 breast cancer whole-genome sequences. Nature 2016, 534, 47–54, . [CrossRef]
- Ajaz, S.; Zaidi, S.-E.; Ali, S.; Siddiqa, A.; Memon, M.A. Germline Mutation Analysis in Sporadic Breast Cancer Cases With Clinical Correlations. Front. Genet. 2022, 13, 820610, . [CrossRef]
- Waks, A.G.; Kim, D.; Jain, E.; Snow, C.; Kirkner, G.J.; Rosenberg, S.M.; Oh, C.; Poorvu, P.D.; Ruddy, K.J.; Tamimi, R.M.; et al. Somatic and Germline Genomic Alterations in Very Young Women with Breast Cancer. Clin. Cancer Res. 2022, 28, 2339–2348, . [CrossRef]
- Momozawa, Y.; Iwasaki, Y.; Parsons, M.T.; Kamatani, Y.; Takahashi, A.; Tamura, C.; Katagiri, T.; Yoshida, T.; Nakamura, S.; Sugano, K.; et al. Germline pathogenic variants of 11 breast cancer genes in 7,051 Japanese patients and 11,241 controls. Nat. Commun. 2018, 9, 1–7, . [CrossRef]
- Sukpan, P.; Kanokwiroon, K.; Sriplung, H.; Laochareonsuk, W.; Choochuen, P.; Auseng, N.; Wanawanakorn, K.; Sangkhathat, S. Prevalence of Pathogenic Germline Mutations in 13 Hereditary Cancer-Related Genes in Breast Cancer Patients in Narathiwat Province, Thailand. Asian Pac. J. Cancer Prev. 2023, 24, 525–530, . [CrossRef]
- Zhang, J.; Wang, N.; Zheng, T.; Lu, T.; Zhang, R.; Ran, R.; Li, K.; Huang, Y.; Xie, F.; Zhang, Y.; et al. Germline Mutational Landscape in Chinese Patients With Advanced Breast Cancer. Front. Oncol. 2022, 12, 745796, . [CrossRef]
- Biancolella, M.; Ouédraogo, N.L.M.; Zongo, N.; Zohoncon, T.M.; Testa, B.; Rizzacasa, B.; Latini, A.; Conte, C.; Compaore, T.R.; Ouedraogo, C.M.R.-N.; et al. Breast cancer in West Africa: molecular analysis of BRCA genes in early-onset breast cancer patients in Burkina Faso. Hum. Genom. 2021, 15, 1–11, . [CrossRef]
- Ardern-Jones, A.; Kenen, R.; Eeles, R. Too much, too soon? Patients and health professionals' views concerning the impact of genetic testing at the time of breast cancer diagnosis in women under the age of 40. Eur. J. Cancer Care 2005, 14, 272–281, . [CrossRef]
- Budzik, M.P.; Fudalej, M.M.; Badowska-Kozakiewicz, A.M. Histopathological analysis of mucinous breast cancer subtypes and comparison with invasive carcinoma of no special type. Sci. Rep. 2021, 11, 1–9, . [CrossRef]
- Rechsteiner, A.; Dietrich, D.; Varga, Z. Prognostic relevance of mixed histological subtypes in invasive breast carcinoma: a retrospective analysis. J. Cancer Res. Clin. Oncol. 2022, 149, 4967–4978, . [CrossRef]
- Dayan, D.; Lukac, S.; Rack, B.; Ebner, F.; Fink, V.; Leinert, E.; Veselinovic, K.; Schütze, S.; El Taie, Z.; Janni, W.; et al. Effect of histological breast cancer subtypes invasive lobular versus non-special type on survival in early intermediate-to-high-risk breast carcinoma: results from the SUCCESS trials. Breast Cancer Res. 2023, 25, 1–15, . [CrossRef]
- Arora, A.; Agarwal, D.; Abdel-Fatah, T.M.; Lu, H.; Croteau, D.L.; Moseley, P.; A Aleskandarany, M.; Green, A.R.; Ball, G.; A Rakha, E.; et al. RECQL4 helicase has oncogenic potential in sporadic breast cancers. J. Pathol. 2015, 238, 495–501, . [CrossRef]
- Yan, K.; Gao, Y.; Heller, S.L. Breast Cancer Screening Utilization and Outcomes in Women With Neurofibromatosis Type 1. Clin. Breast Cancer 2023, 23, e200–e205, . [CrossRef]
- Keske, A.; Weisman, P.; Ospina-Romero, M.; Raut, P.; Smith-Simmer, K.; Zakas, A.L.; Flynn, C.; Xu, J. Breast cancers in monoallelic MUTYH germline mutation carriers have clinicopathological features overlapping with those in BRCA1 germline mutation carriers. Breast Cancer Res. Treat. 2023, 204, 151–158, . [CrossRef]
- Fang, H.; Nie, L.; Chi, Z.; Liu, J.; Guo, D.; Lu, X.; Hei, T.K.; Balajee, A.S.; Zhao, Y. RecQL4 Helicase Amplification Is Involved in Human Breast Tumorigenesis. PLOS ONE 2013, 8, e69600, . [CrossRef]
- Balajee, A.S. Human RecQL4 as a Novel Molecular Target for Cancer Therapy. Cytogenet. Genome Res. 2021, 161, 305–327, . [CrossRef]
- Pylkäs, K.; Vuorela, M.; Otsukka, M.; Kallioniemi, A.; Jukkola-Vuorinen, A.; Winqvist, R. Rare Copy Number Variants Observed in Hereditary Breast Cancer Cases Disrupt Genes in Estrogen Signaling and TP53 Tumor Suppression Network. PLOS Genet. 2012, 8, e1002734, . [CrossRef]
- Liu, Y.; Yang, H.; Fu, X.; Zhong, L.; Xu, P.; Fang, F.; Liu, Y.; Li, Q.; Yan, Y.; Wei, S.; et al. BRCA2, PALB2, RECQL4 Germline Pathogenic Variants, and Somatic TP53 Mutation in Triple Metachronous Malignancies: A Case Report and Literature Review. Int. Med Case Rep. J. 2024, ume 17, 23–29, . [CrossRef]
- O Seminog, O.; Goldacre, M.J. Risk of benign tumours of nervous system, and of malignant neoplasms, in people with neurofibromatosis: population-based record-linkage study. Br. J. Cancer 2012, 108, 193–198, . [CrossRef]
- Dischinger, P.S.; Tovar, E.A.; Essenburg, C.J.; Madaj, Z.B.; Gardner, E.E.; Callaghan, M.E.; Turner, A.N.; Challa, A.K.; Kempston, T.; Eagleson, B.; et al. NF1 deficiency correlates with estrogen receptor signaling and diminished survival in breast cancer. npj Breast Cancer 2018, 4, 1–14, . [CrossRef]
- Ntowe, K.W.; Thomas, S.M.; Dalton, J.C.; Olunuga, E.; Wang, T.; Chiba, A.; Plichta, J.K. Demographics and Clinical Decision Making in Patients with Germline Moderate Penetrance Non-BRCA Mutations in Breast Cancer Related Genes. Ann. Surg. Oncol. 2024, 31, 7290–7300, . [CrossRef]
- Stewart, D.R.; Korf, B.R.; Nathanson, K.L.; Stevenson, D.A.; Yohay, K. Care of adults with neurofibromatosis type 1: a clinical practice resource of the American College of Medical Genetics and Genomics (ACMG). Anesthesia Analg. 2018, 20, 671–682, . [CrossRef]
- Tung, N.; Domchek, S.M.; Stadler, Z.; Nathanson, K.L.; Couch, F.; Garber, J.E.; Offit, K.; Robson, M.E. Counselling framework for moderate-penetrance cancer-susceptibility mutations. Nat. Rev. Clin. Oncol. 2016, 13, 581–588, . [CrossRef]
- Kairupan, C.; Scott, R.J. Base excision repair and the role of MUTYH. Hered. Cancer Clin. Pr. 2007, 5, 199–209, . [CrossRef]
- Boesaard, E.P.; Vogelaar, I.P.; Bult, P.; AP Wauters, C.; van Krieken, J.H.J.; Ligtenberg, M.J.; van der Post, R.S.; Hoogerbrugge, N. Germline MUTYH gene mutations are not frequently found in unselected patients with papillary breast carcinoma. Hered. Cancer Clin. Pr. 2014, 12, 1–4, . [CrossRef]
- Cheadle, J.P.; Sampson, J.R. MUTYH-associated polyposis—From defect in base excision repair to clinical genetic testing. DNA Repair 2007, 6, 274–279, . [CrossRef]
- Nassar, A.; Zekri, A.-R.N.; Kamel, M.M.; Elberry, M.H.; Lotfy, M.M.; Seadawy, M.G.; Hassan, Z.K.; Soliman, H.K.; Lymona, A.M.; Youssef, A.S.E.-D. Frequency of Pathogenic Germline Mutations in Early and Late Onset Familial Breast Cancer Patients Using Multi-Gene Panel Sequencing: An Egyptian Study. Genes 2022, 14, 106, . [CrossRef]
- Wasielewski, M.; Out, A.A.; Vermeulen, J.; Nielsen, M.; Ouweland, A.v.D.; Tops, C.M.J.; Wijnen, J.T.; Vasen, H.F.A.; Weiss, M.M.; Klijn, J.G.M.; et al. Increased MUTYH mutation frequency among Dutch families with breast cancer and colorectal cancer. Breast Cancer Res. Treat. 2010, 124, 635–641, . [CrossRef]
- Easton, D.F.; Pharoah, P.D.; Antoniou, A.C.; Tischkowitz, M.; Tavtigian, S.V.; Nathanson, K.L.; Devilee, P.; Meindl, A.; Couch, F.J.; Southey, M.; et al. Gene-Panel Sequencing and the Prediction of Breast-Cancer Risk. New Engl. J. Med. 2015, 372, 2243–2257, . [CrossRef]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).