
Submitted:
05 January 2026
Posted:
06 January 2026
You are already at the latest version
Abstract
Background: Chronological age does not always accurately reflect biological matura-tion in children, particularly in the presence of systemic diseases. Dental age assess-ment is widely used as a biological maturity indicator; however, the effect of juvenile diabetes mellitus on dental maturation remains insufficiently clarified, with incon-sistent findings reported across populations. Objective: This study aimed to compare dental age estimated using the Demirjian method with chronological age in children with juvenile diabetes and in age- and sex-matched healthy controls. Materials and Methods: This observational comparative study included panoramic radiographs from 30 children aged 8–15 years: 15 patients diagnosed with juvenile diabetes mellitus and 15 systemically healthy controls, all presenting Angle Class I malocclusion. Dental age was assessed using the Demirjian method and compared with chronological age. Ap-propriate parametric or non-parametric statistical tests were applied based on data distribution. Results: Children with juvenile diabetes exhibited a statistically signifi-cant advancement in dental age relative to chronological age, with a mean DA–CA difference of 1.36 years (p = 0.0066). No statistically significant differences between dental and chronological age were observed in the control group. Sexual dimorphism was evident from crown completion stages onward, with females demonstrating earli-er dental maturation. Conclusions: Juvenile diabetes mellitus is associated with accel-erated dental maturation. These findings have clinical implications for orthodontic treatment timing and growth assessment and indicate a potential risk of age overesti-mation in forensic contexts. Dental age should therefore be interpreted alongside skel-etal and chronological indicators, particularly in pediatric patients with systemic metabolic conditions.
Keywords:
dental age estimation
; Demirjian method
; juvenile diabetes mellitus
; biological matu-ration
; orthodontic treatment timing
1. Introduction
Accurate assessment of growth and maturation in children and adolescents is fundamental to clinical decision-making in dentistry, orthodontics, pediatrics, and forensic science [1,2]. Although chronological age (CA) is widely used for administrative, legal, and clinical purposes, it frequently fails to reflect an individual’s true developmental status [3]. Biological maturation is a complex and heterogeneous process influenced by genetic, nutritional, environmental, and systemic factors, resulting in substantial inter-individual variability and frequent divergence from CA [3,4]. Moreover, growth does not proceed uniformly across biological systems; skeletal, dental, somatic, and sexual maturation follow distinct developmental trajectories, as demonstrated by classical growth models proposed by Scammon, Tanner, Hägg, and Taranger [5,6,7]. Consequently, chronological age may lead to inaccurate diagnoses or suboptimal timing of therapeutic interventions, particularly in growth-dependent disciplines such as orthodontics [8].
For these reasons, biological age indicators have gained increasing prominence as more reliable tools for assessing developmental status. Among these, dental age (DA) is regarded as one of the most robust and reproducible markers of biological maturation [9,10]. Dental development—particularly tooth calcification—is a genetically regulated and continuous process extending from crown initiation to root apex closure. Compared with skeletal maturation, dental mineralization is relatively resistant to the effects of malnutrition, hormonal imbalance, and environmental stressors [11]. This relative biological stability makes DA estimation especially valuable in children affected by systemic diseases or growth disturbances, in whom other maturity indicators may be altered or unreliable [11,12].
Dental age assessment has broad clinical and scientific applications. In pediatric dentistry, it supports preventive strategies, monitoring of eruption patterns, and interceptive treatment planning [13,14,15]. In orthodontics, DA contributes to identifying critical developmental phases relevant to orthopedic and orthodontic interventions, thereby optimizing treatment timing in relation to craniofacial growth [2,16,17]. In pediatrics and endocrinology, dental maturation serves as a complementary indicator for evaluating growth disorders and monitoring systemic conditions [18,19,20]. Additionally, DA estimation plays a pivotal role in forensic science for determining the age of unidentified minors and human remains [21,22], as well as in anthropology and archaeology for reconstructing growth patterns in past populations [23,24,25,26].
Numerous methods have been proposed for estimating dental age. Early approaches based on clinical tooth eruption proved unreliable due to their susceptibility to local and environmental factors, such as premature tooth loss, impaction, ankylosis, and crowding [27,28]. Consequently, radiographic assessment of tooth calcification has become the preferred approach [29,30]. Among the various radiographic methods described in the literature—including those developed by Nolla [1], Cameriere et al. [31,32,33], and Willems [32]—the method introduced by Demirjian, Goldstein, and Tanner in 1973 remains the most widely used and extensively validated worldwide in both clinical and research contexts [1,10,33,34,35].
The Demirjian method is based on the systematic evaluation of tooth calcification stages, which reflect a genetically regulated and biologically stable process less susceptible to environmental and systemic influences than tooth eruption or skeletal growth. It assesses the developmental stages (A–H) of seven permanent mandibular teeth, excluding the third molar, using panoramic radiographs. Sex-specific maturity scores are assigned to each tooth and subsequently converted into an estimated dental age [1,10,33,35]. The method’s enduring relevance in both clinical and research settings can be attributed to its methodological simplicity, clearly defined staging criteria, and high intra- and inter-observer reliability [33,34,35,36]. Consistent with established patterns of biological maturation, dental development assessed using this approach exhibits sexual dimorphism, with females generally demonstrating earlier advancement in calcification stages than males, particularly from stage Donward [37,38,39].
In its original formulation, dental age is assessed by examining the seven permanent left mandibular teeth, excluding the third molar, on panoramic radiographs. The mandibular teeth were selected due to their consistent visualization, reduced superimposition, and symmetrical development between the left and right sides of the jaw. In cases where a tooth is missing or cannot be reliably evaluated, the corresponding tooth on the contralateral side may be assessed instead, without compromising the validity of the method [40].
Each tooth is assigned one of eight discrete developmental stages, designated from A to H, based on clearly defined morphological criteria describing crown and root formation. These stages represent successive events in tooth mineralization, from the initial appearance of calcified cusps to complete root apex closure. The standardized nature of these stages facilitates high intra- and inter-observer reproducibility and allows for consistent application across different populations.
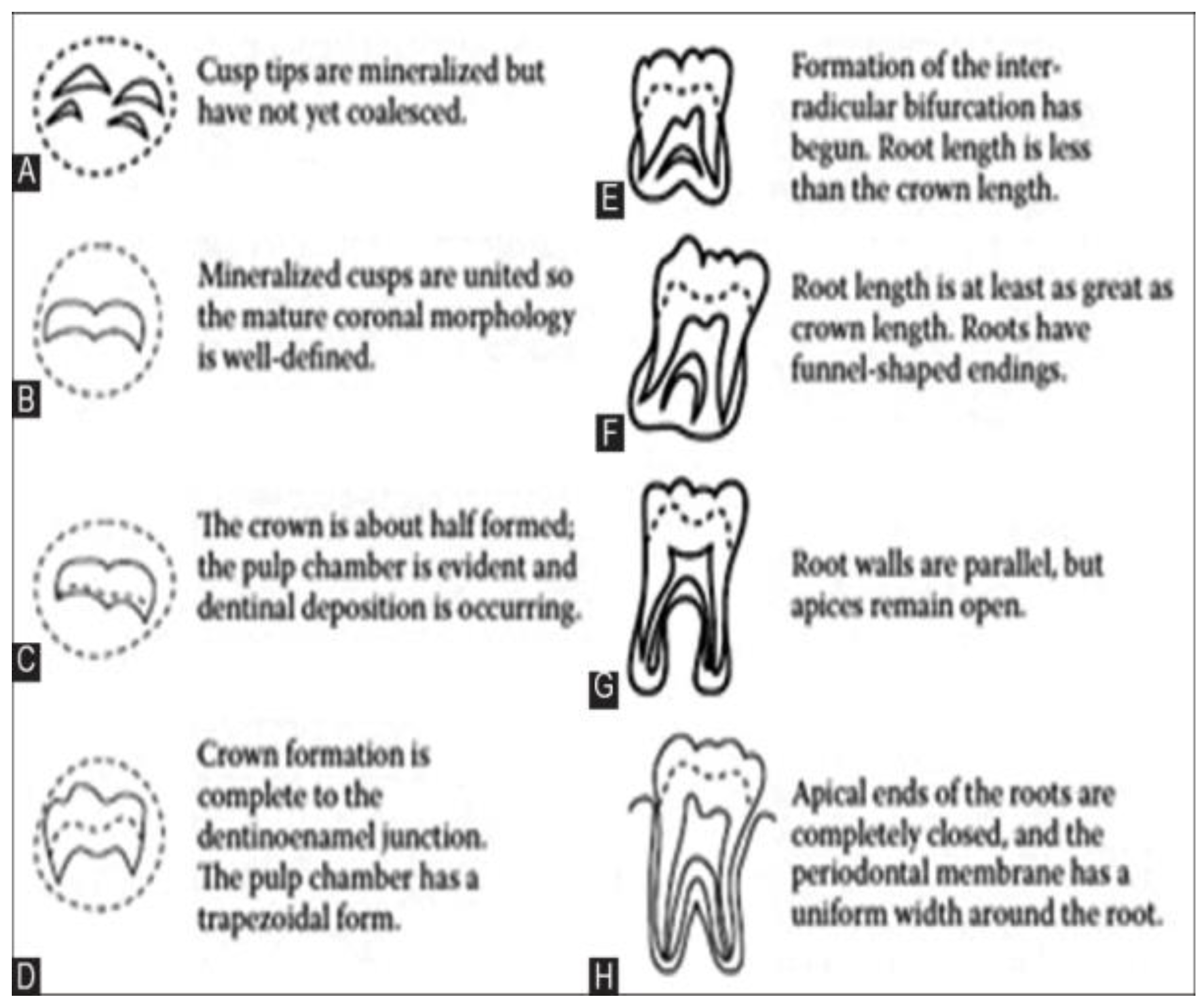
Figure 1.
Dental developmental stages (A–H) according to Demirjian. Source: Adapted from Demirjian, Goldstein, and Tanner (1973) [40].
Figure 1.
Dental developmental stages (A–H) according to Demirjian. Source: Adapted from Demirjian, Goldstein, and Tanner (1973) [40].
The eight stages of dental formation are defined as follows [40]:
- Stage A: Initial crown mineralization is observed in both monoradicular and multiradicular teeth. Calcification appears as separate cusp tips without fusion bridges.
- Stage B: The mineralized cusps coalesce, forming a continuous and regularly contoured occlusal surface.
- Stage C: Enamel formation is complete at the occlusal surface; dentin mineralization begins. The pulp chamber exhibits a curved outline toward the occlusal surface.
- Stage D: Crown mineralization is complete up to the cemento-enamel junction. In monoradicular teeth, the pulp chamber assumes a well-defined shape, while in multiradicular teeth it becomes trapezoidal, with pulp horns resembling an “umbrella tip.” Initial root formation is evident.
- Stage E: In monoradicular teeth, the pulp chamber becomes more clearly contoured, and root length remains shorter than crown height. In multiradicular teeth, the beginning of bifurcation appears as a mineralized crescent.
- Stage F: Root length becomes equal to or greater than crown height. In monoradicular teeth, the pulp chamber walls converge, forming an isosceles triangular shape with a funnel-shaped apex. In multiradicular teeth, the bifurcation is well developed.
- Stage G: The walls of the root canal are parallel, with the apical end still partially open, particularly in the distal roots of molars.
- Stage H: Root development is complete, with full closure of the apical foramen. The periodontal ligament uniformly surrounds the root and apex.
Following stage assignment, each tooth is converted into a numerical maturity score using sex-specific conversion tables, reflecting established differences in maturation tempo between males and females. The individual tooth scores are then summed to produce a total dental maturity score, which is subsequently transformed into an estimated dental age using standardized reference tables provided by the authors. Dental age thus represents the mean chronological age at which a given maturity score is observed in the reference population.
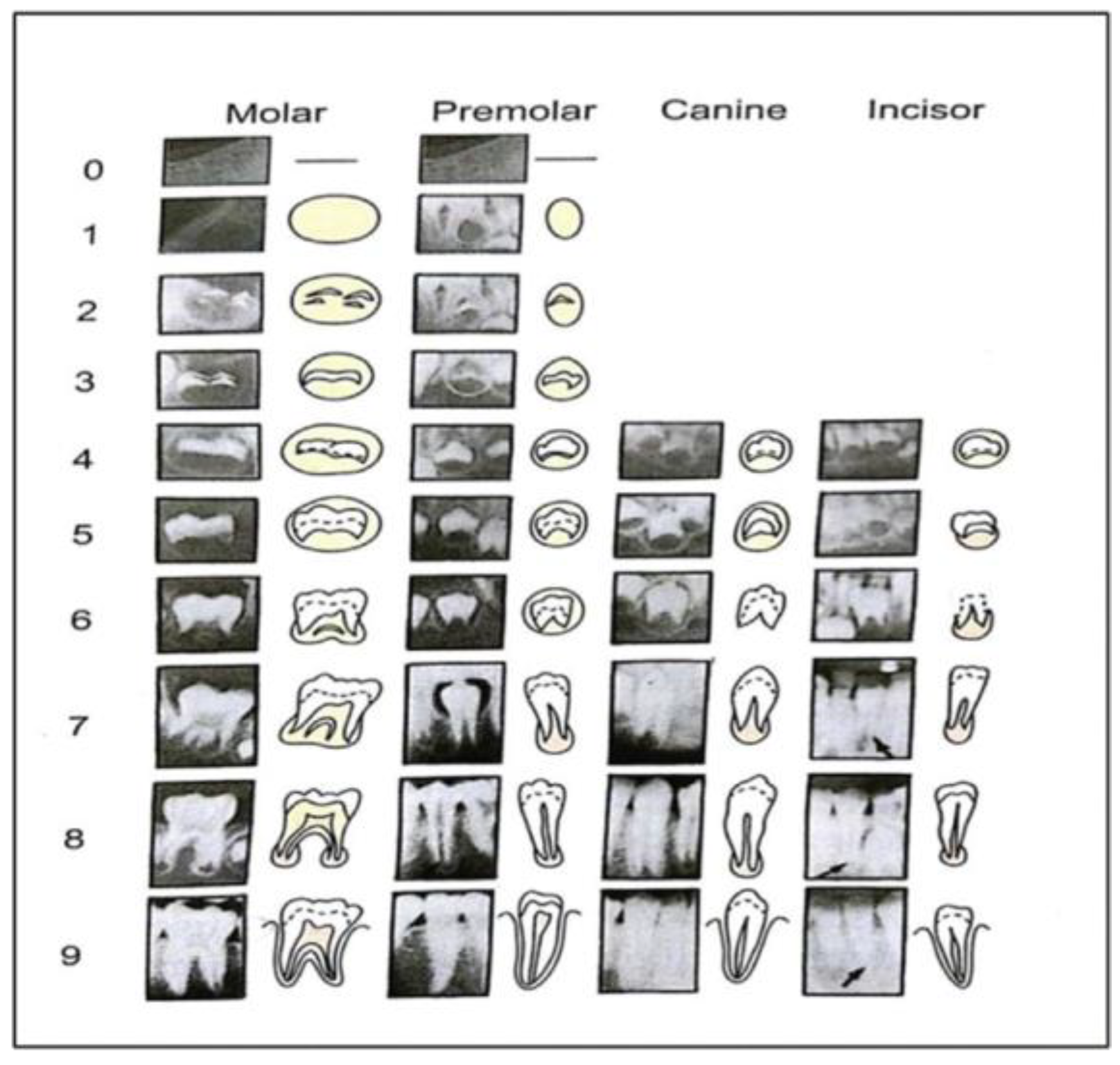
Figure 2.
Radiographic illustration of the eight stages of dental development (A–H) according to Demirjian. Source: Demirjian et al. (1973) [40].
Figure 2.
Radiographic illustration of the eight stages of dental development (A–H) according to Demirjian. Source: Demirjian et al. (1973) [40].
Following stage assignment, each tooth is converted into a numerical maturity score using sex-specific conversion tables, reflecting established differences in maturation tempo between males and females. The individual tooth scores are then summed to produce a total dental maturity score, which is subsequently transformed into an estimated dental age using standardized reference tables provided by the authors. Dental age thus represents the mean chronological age at which a given maturity score is observed in the reference population.
Chronological age, used for comparison, is calculated by subtracting the patient’s date of birth from the date of radiographic examination and expressed in decimal years.
The principal strengths of the Demirjian method include its clear staging criteria, ease of application, and high reproducibility. These attributes, combined with its extensive validation across diverse populations, have established the method as a reference standard for dental age estimation in pediatric dentistry, orthodontics, forensic science, and anthropological research.
Systemic diseases may alter the tempo of biological maturation, including dental development [18,41,42]. Juvenile diabetes mellitus, in particular, has been associated with metabolic dysregulation, altered mineral homeostasis, early tooth eruption, and modifications in craniofacial growth, all of which may influence dental maturation patterns [43,44,45]. However, existing evidence regarding the impact of juvenile diabetes on dental age remains limited and inconsistent across populations, with reports of delayed, advanced, or unchanged dental maturation relative to chronological age [43,44,45,46]. These discrepancies may be attributable to differences in study design, age ranges, assessment methods, and population characteristics.
Despite growing interest in the interaction between systemic metabolic disorders and dental development, data directly comparing dental age and chronological age in children with juvenile diabetes—using standardized and widely validated methods such as Demirjian’s—remain scarce. Clarifying whether dental maturation is accelerated, delayed, or concordant in this population is clinically relevant, as inaccurate age estimation may affect orthodontic treatment timing, growth assessment, and forensic interpretation.
Therefore, the present study aimed to compare dental age estimated using the Demirjian method with chronological age in children diagnosed with juvenile diabetes and in age- and sex-matched healthy controls, thereby contributing to a more precise understanding of dental maturation patterns in the context of pediatric diabetes.
2. Materials and Methods
2.1. Ethical Considerations
This study was approved by the Ethics Committee of the “George Emil Palade” University of Medicine, Pharmacy, Science, and Technology of Târgu Mureș (Decision No. 1885, 12 October 2022) and adhered to the ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all participants and their guardians. This manuscript is reported in accordance with the STROBE 2021 reporting guideline and the RECORD 2015 extension for observational studies using routinely collected health data.
2.2. Study Design and Sample Selection
This observational, comparative study was conducted on panoramic radiographs obtained from pediatric patients aged between 8 and 15 years. The study population consisted of two groups with comparable dento-maxillary characteristics. The study group included 15 children diagnosed with juvenile diabetes mellitus and Angle Class I dento-maxillary anomalies. The control group comprised 15 systemically healthy children, matched for age, sex, and type of malocclusion (Angle Class I), with no history of diabetes or other systemic conditions known to influence growth and development.
Panoramic radiographs were selected based on diagnostic quality, absence of significant distortions, and clear visualization of mandibular permanent teeth. All radiographs were obtained as part of routine clinical care, following standard radiographic protocols.
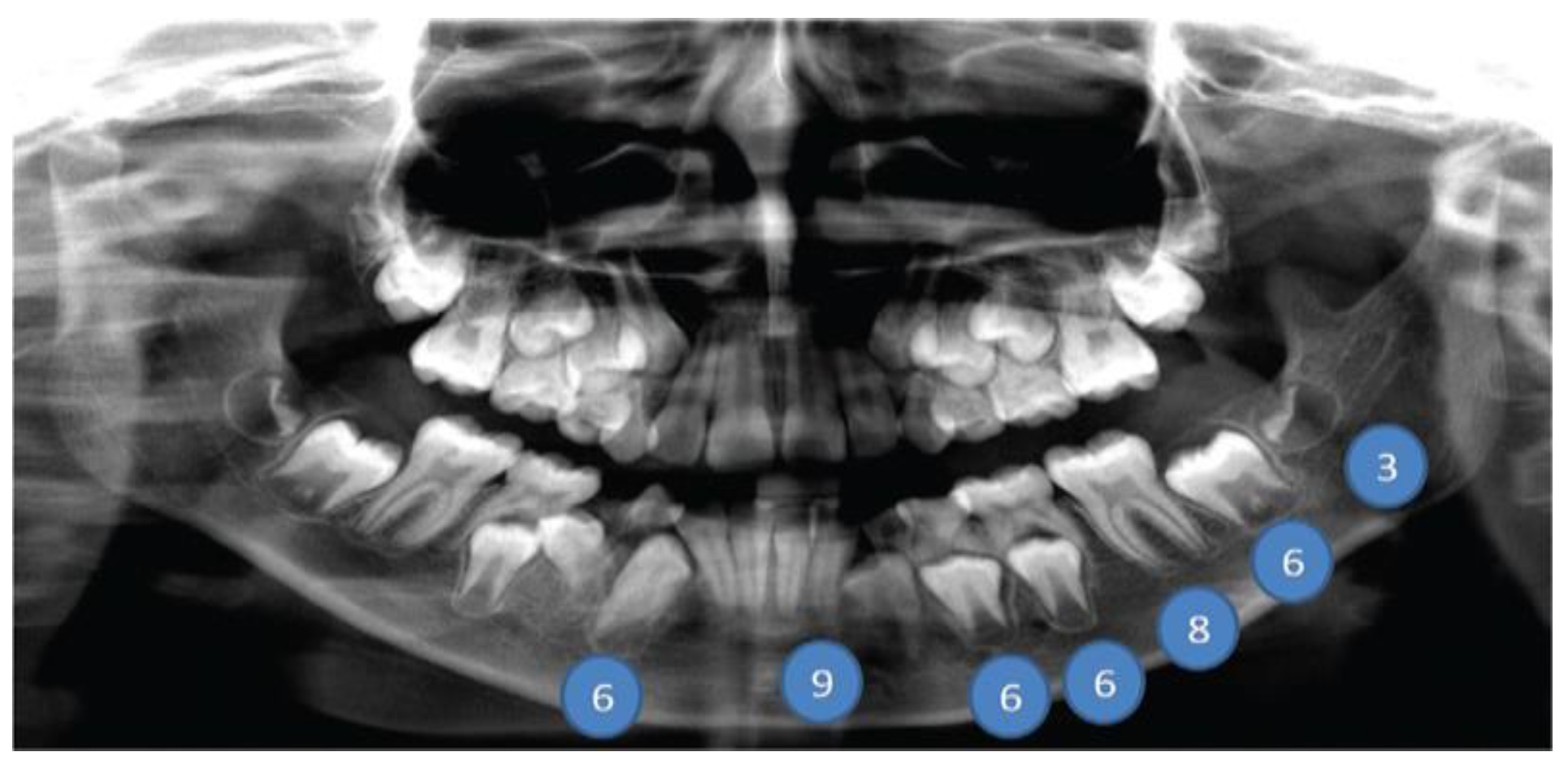
Figure 3.
Panoramic radiograph of a patient from the study group illustrating various stages of dental development.
Figure 3.
Panoramic radiograph of a patient from the study group illustrating various stages of dental development.
2.3. Dental Age Assessment
Dental age (DA) was estimated using the Demirjian method [10,12,33,34,36,37,38,39], which assesses the developmental stages (A–H) of seven left mandibular permanent teeth, excluding the third molar. Each tooth was assigned a specific developmental stage based on radiographic appearance, following the original criteria proposed by Demirjian et al. The corresponding maturity scores were then attributed according to sex-specific reference tables.
The individual tooth scores were summed to obtain a total maturity score, which was subsequently converted into dental age using the standardized conversion tables provided by the method’s authors. In cases of unilateral tooth extraction or radiographic artifacts affecting assessment, the homologous tooth on the contralateral side was evaluated, in accordance with Demirjian’s guidelines.
For comparative and illustrative purposes, quantitative assessment methods based on apical measurements, such as the Cameriere method [12,15,31,33], were considered. However, due to the increased complexity and time requirements of these measurements, they were not applied systematically in the present study.
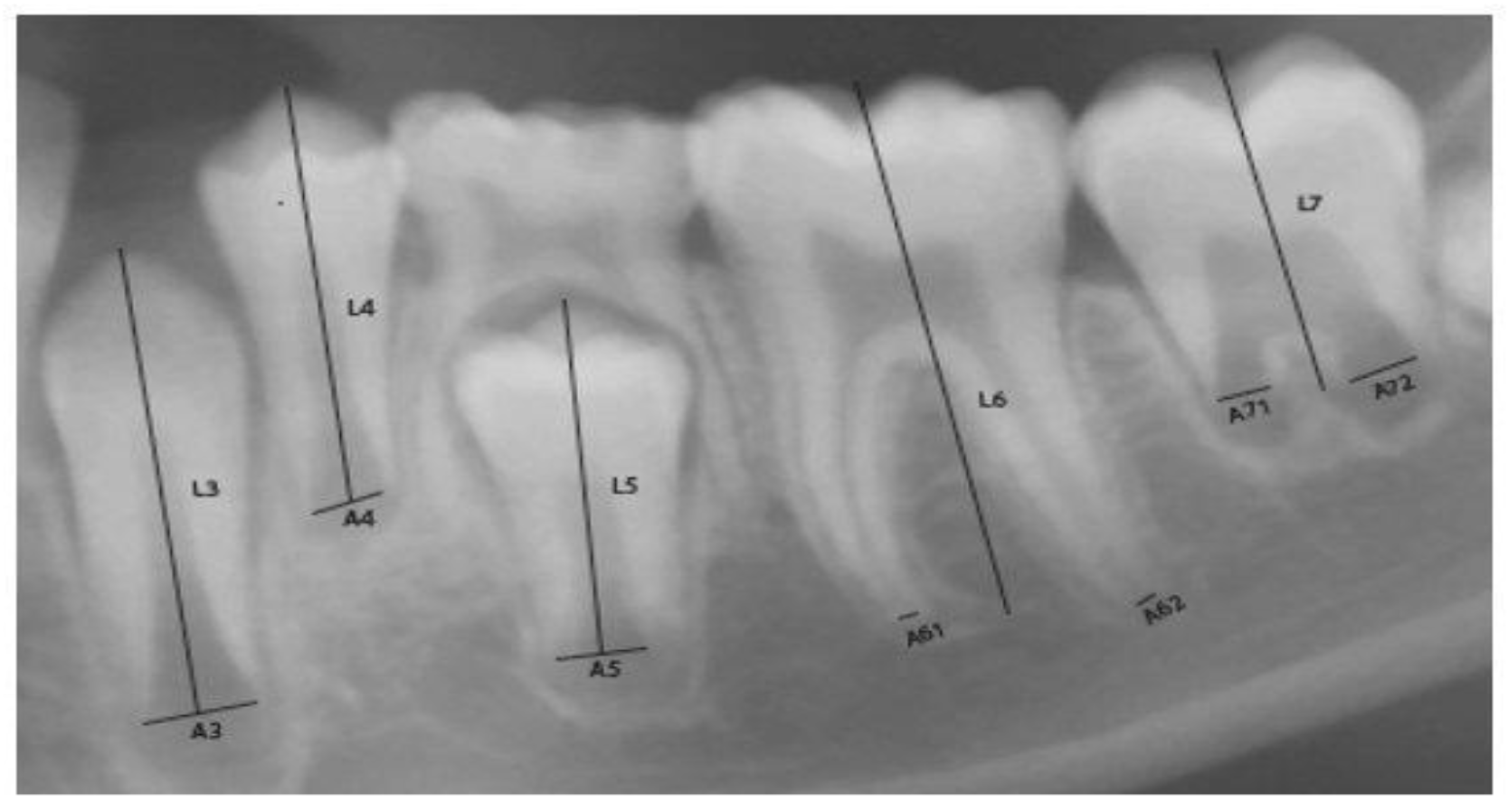
Figure 4.
Cameriere’s measurements of mandibular teeth (xi = Ai/Li) for seven left mandibular permanent teeth, illustrating quantitative assessment of dental maturity.
Figure 4.
Cameriere’s measurements of mandibular teeth (xi = Ai/Li) for seven left mandibular permanent teeth, illustrating quantitative assessment of dental maturity.
2.4. Statistical Analysis
Chronological age (CA) was calculated by subtracting the date of birth from the date of radiographic examination and expressed in decimal years. Dental age (DA) was obtained using the Demirjian method, and the difference between DA and CA (DA–CA) was calculated for each participant.
Descriptive statistics were computed for all variables, including means, standard deviations, medians, and ranges. Before inferential analysis, the distribution of continuous variables was assessed for normality using the Shapiro–Wilk test. Given the limited sample size, normality assessment was complemented by visual inspection of histograms and Q–Q plots.
For variables showing an approximately normal distribution, comparisons between dental age and chronological age within each group were performed using paired-sample t-tests. Between-group comparisons of DA–CA differences (juvenile diabetes vs. control group) were conducted using independent-sample t-tests when normality assumptions were met. In cases where data deviated from normal distribution, the corresponding non-parametric tests (Wilcoxon signed-rank test for paired comparisons and Mann–Whitney U test for independent samples) were applied.
Sex-related differences in dental maturation were evaluated using independent-sample t-tests or Mann–Whitney U tests, as appropriate. All statistical tests were two-tailed, and the level of statistical significance was set at p < 0.05. Statistical analyses were performed using standard statistical software.
3. Results
3.1. Sexual Dimorphism in Dental Development
In the early stages of dental calcification (stages A, B, and C), no notable differences were observed between male and female participants. However, beginning with stage D, corresponding to the completion of crown formation, females exhibited earlier and more rapid progression through subsequent developmental stages. This finding supports the use of sex-specific scoring systems when assessing dental maturity.
3.2. Dental Age Versus Chronological Age
Children with juvenile diabetes demonstrated marked discrepancies between dental age and chronological age, with differences reaching up to two years in some cases. This advancement in dental maturation has potential implications for intra- and inter-arch balance and orthodontic treatment planning.
In the control group, 75% of subjects exhibited dental development consistent with their chronological age, while 25% showed delayed dental maturation. Across the entire control group, the mean difference between DA and CA was approximately 1.4 years, without reaching statistical significance.

Figure 5.
Digital panoramic radiograph used for dental age estimation.
3.3. Demirjian Scores and Group Comparisons
Sex-specific Demirjian maturity scores were applied using standardized reference tables.

Table 1.
Demirjian maturity scores by tooth and developmental stage for girls.
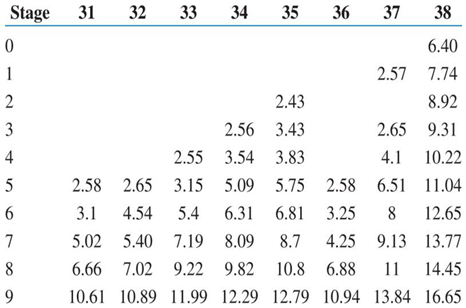 |
Table 2.
Demirjian maturity scores by tooth and developmental stage for boys.
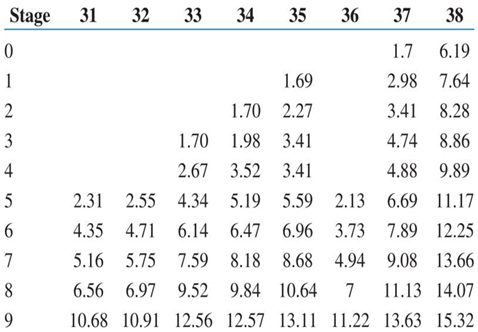 |
Box plot analysis revealed a consistent advancement, compared to controls, of dental age relative to chronological age in children with diabetes.
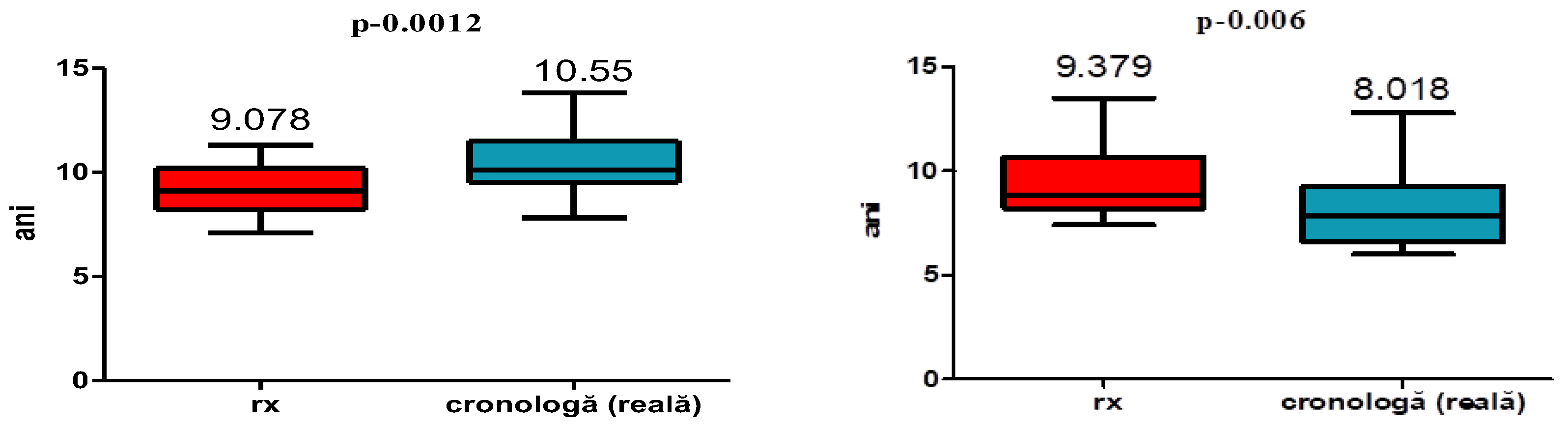
Figure 6.
Box plots comparing chronological age and dental age in the study (diabetic) and in the control group.
Figure 6.
Box plots comparing chronological age and dental age in the study (diabetic) and in the control group.
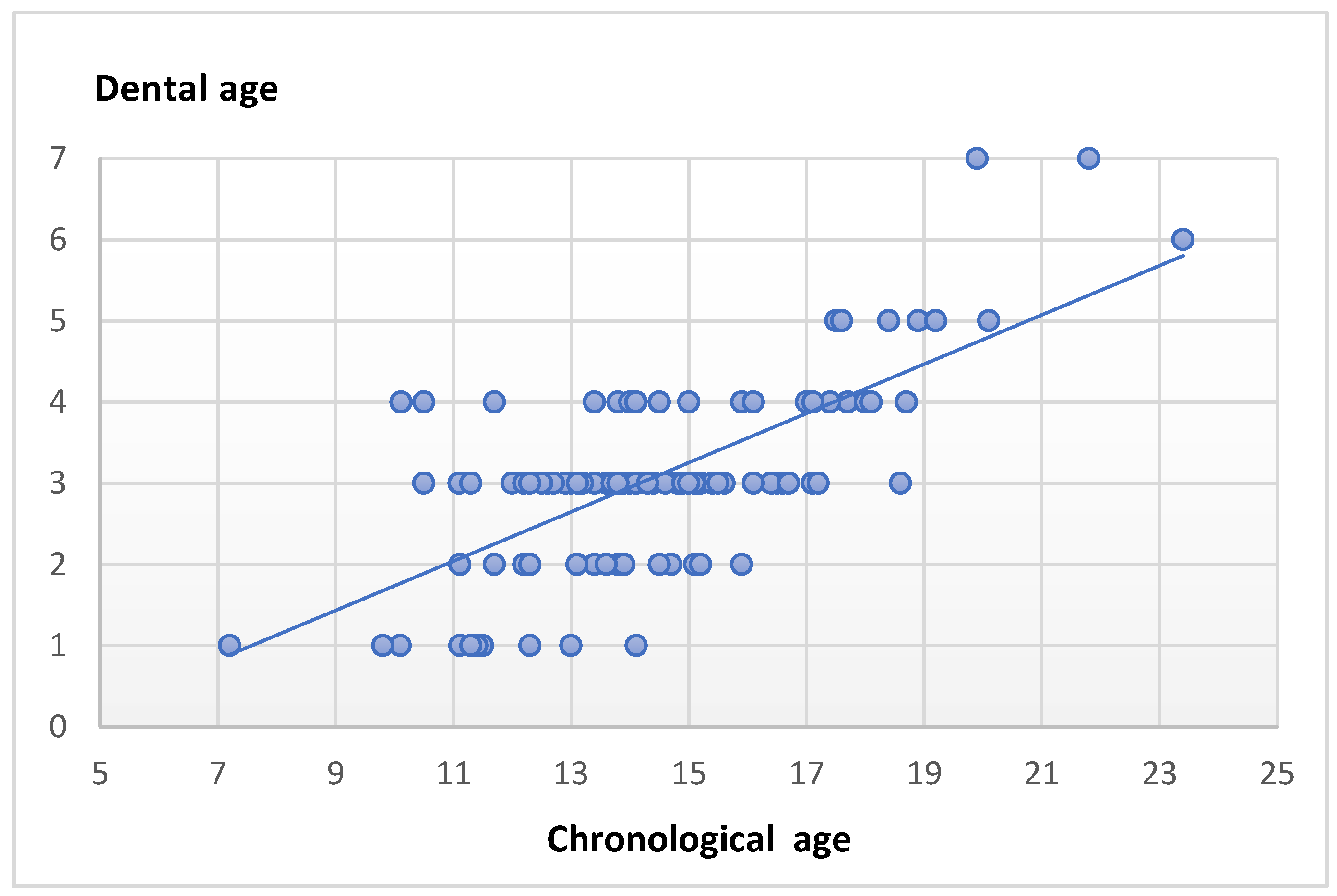
In the diabetic group, the mean DA–CA difference was 1.36 years, and this difference was statistically significant (p = 0.0066), indicating accelerated dental maturation.
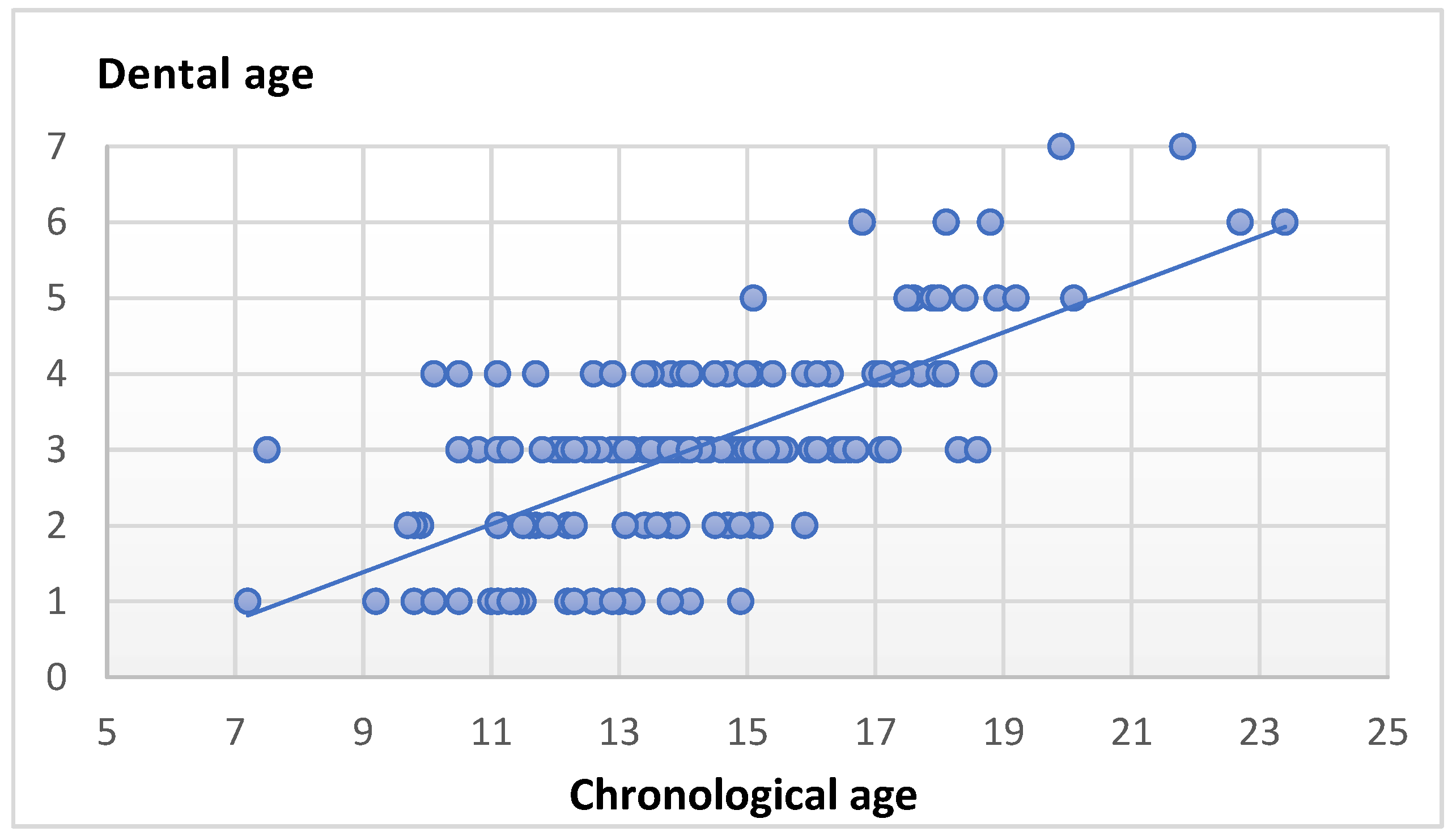
Figure 7.
Comparison between dental age and chronological age in children with juvenile diabetes.
4. Discussion
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
The present study demonstrates that children affected by juvenile diabetes exhibit a statistically significant advancement in dental maturation relative to their chronological age, whereas healthy controls with comparable dento-maxillary characteristics show general concordance between dental and chronological age. These findings support the hypothesis that systemic metabolic disturbances, particularly those related to endocrine regulation, may influence the tempo of dental development [43,45,47].
Dental maturation is a complex, genetically regulated biological process characterized by a highly ordered sequence of events, including initial mineralization, crown formation, root elongation, and apical closure [48]. Owing to its relative resistance to short-term environmental fluctuations, dental development has long been regarded as a reliable indicator of biological maturity [2,12,49]. However, the extent to which dental maturation reflects overall somatic or skeletal development remains controversial.
An important distinction that warrants emphasis is that between accelerated dental maturation and accelerated tooth eruption, two phenomena that are biologically and clinically distinct. Dental maturation refers to the progression of tooth calcification and root development, as assessed radiographically, whereas eruption describes the axial movement of teeth into the oral cavity. Although early eruption has been reported in children with diabetes [43,44,45], eruption timing can be influenced by local factors such as space availability, periodontal conditions, and occlusal forces [27,28]. In contrast, calcification-based dental age assessment reflects intrinsic developmental processes and is less susceptible to local disturbances. The present study specifically evaluated dental maturation rather than eruption, thereby providing insight into the underlying tempo of odontogenesis rather than the clinical emergence of teeth.
The observed advancement in dental age among children with juvenile diabetes may be explained, at least in part, by alterations in endocrine and metabolic regulation. Insulin and insulin-like growth factors (IGFs) play a central role in cellular proliferation, differentiation, and matrix synthesis in mineralized tissues. Experimental and clinical evidence suggests that these pathways influence odontoblast activity and dentin formation, potentially accelerating tooth development independently of skeletal maturation [44,45,47]. This mechanism may account for the dissociation observed between dental maturation and other growth indicators, supporting the notion that dental age represents a partially independent biological clock.
The relationship between dental age, skeletal age, and chronological age has been extensively investigated, yet remains inconsistent across studies [8,50,51]. Early investigations by Demirjian et al. and Bedia et al. reported strong associations between skeletal and somatic maturity but weak or absent correlations between dental and skeletal development [52,53]. Similarly, Kanbur et al. [54] found no significant differences between dental and chronological age in adolescents with constitutional growth delay, suggesting that dental maturity may be relatively preserved despite alterations in somatic growth. In contrast, Engström and Sagne [55] reported a positive correlation between dental and skeletal maturation, indicating partial synchronization during certain growth periods.
Subsequent studies have produced heterogeneous results. Sierra and Vallejo-Bolaños [56,57] emphasized methodological variability as a key contributor to inconsistent findings, whereas Saraç [58], Palanisamy [50], and Krailassiri [59] reported stronger correlations between dental and skeletal age. Conversely, Ghergie et al. [49], in patients with Class II malocclusion, observed weak or insignificant associations. Collectively, these discrepancies underscore that dental and skeletal maturation, while influenced by shared genetic and hormonal factors, are not uniformly coupled and may respond differently to systemic conditions.
In the context of juvenile diabetes, altered metabolic control has been associated with accelerated growth patterns, including early tooth eruption, increased number of erupted teeth, and modifications in mineralization processes [43,44,45,47]. Such changes may predispose affected children to enamel defects, increased caries susceptibility, and dento-maxillary disharmony resulting from asynchronous dental and skeletal development [44,45,46,47]. The advanced dental age observed in the present study aligns with these reports and reinforces the concept that metabolic dysregulation can selectively accelerate odontogenesis.
Among the various methods proposed for dental age estimation, the Demirjian method remains one of the most widely applied and validated techniques [40,61]. Its strengths include clearly defined developmental stages, sex-specific scoring systems, and high intra- and inter-observer reliability, with Cohen’s kappa values frequently exceeding 0.75 [40,61]. Nevertheless, its limited correlation with skeletal maturity supports its use as a complementary rather than standalone indicator of overall biological development.
From a clinical perspective, accurate assessment of biological maturity is essential in orthodontics and pediatric dentistry, particularly for growth-dependent interventions. Orthopedic treatment outcomes are closely linked to the timing of the pubertal growth spurt, which is more reliably predicted by skeletal maturity indicators than by chronological or dental age alone [46]. While dental age assessment offers practical advantages—such as accessibility and avoidance of additional radiation exposure—it should be interpreted within a broader diagnostic framework that includes skeletal and chronological parameters.
The present study has certain limitations. The relatively small sample size reflects the low prevalence of juvenile diabetes in pediatric dental populations and the ethical constraints associated with radiographic exposure in children beyond routine clinical indications. Consequently, this investigation was designed as an exploratory comparative study. To enhance internal validity, strict inclusion criteria and careful matching for age, sex, and dento-maxillary characteristics were applied, resulting in a homogeneous sample. While these measures mitigate biological variability, the findings should be interpreted with caution, and further studies involving larger and more diverse cohorts are warranted.
5. Conclusions
Children with juvenile diabetes show significantly accelerated dental maturation relative to chronological age, unlike healthy peers. Dental age, assessed by the Demirjian method, may be influenced by systemic metabolic conditions and progress independently of skeletal maturation, underscoring the biological autonomy of dental development, particularly in the presence of endocrine disturbances. While clinically informative, dental age should not be used in isolation, as skeletal age remains the most reliable marker of overall maturity; therefore, integrated assessment is essential, particularly in pediatric patients with systemic disease.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, STROBE 2021 reporting guideline, and the RECORD 2015 extension for observational studies using routinely collected health data.
Author Contributions
Conceptualization, M.S.D. and M.P.; methodology, M.C.T.; software, A.Z.; validation, S.M.B., E.B., and M.C.T.; formal analysis, I.E.M.; investigation, M.S.D., M.P., and S.M.B.; resources, E.B. and E.D.; data curation, A.Z. and I.E.M.; writing—original draft preparation, M.S.D. and M.P.; writing—review and editing, S.M.B.; visualization, E.B. and E.D.; supervision, M.C.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.”.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the “George Emil Palade” University of Medicine, Pharmacy, Science, and Technology of Târgu Mureș (Decision No. 1885, 12 October 2022) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and their guardians. Written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Moga, L.I.; Moca, A.E.; Iurcov, R.; Slăvescu, D.; Vaida, L.L. Evaluating the Nolla Method for Dental Age Estimation in Children from Northwestern Romania. Children 2025, 12, 69. [Google Scholar] [CrossRef]
- Lyros, I.; Vastardis, H.; Tsolakis, I.A.; Kotantoula, G.; Lykogeorgos, T.; Tsolakis, A.I. Growth Prediction in Orthodontics: ASystematic Review of Past Methods up to Artificial Intelligence. Children 2025, 12, 1023. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.U. Aging Unequally: Functional Age Disparities Between Developmental and Non-Developmental Disabilities. Healthcare 2025, 13, 2412. [Google Scholar] [CrossRef] [PubMed]
- Domaradzki, J.; Alvarez, C.; Szafraniec, R.; Koźlenia, D. Biological maturation determines the beneficial effects of high-intensity functional training on cardiorespiratory fitness in male adolescents. PeerJ 2025, 13, e19756. [Google Scholar] [CrossRef]
- Roche, A.F.; Garn, S.M.; Reynolds, E.L.; Robinow, M.; Sontag, L.W. The first seriatim study of human growth and middle aging. Am. J. Phys. Anthropol. 1981, 54, 23–24. [Google Scholar] [CrossRef] [PubMed]
- Miller, B.S.; Sarafoglou, K.; Addo, O.Y. Development of Tanner stage–age adjusted CDC height curves for research and clinical applications. J. Endocr. Soc. 2020, 4, bvaa098. [Google Scholar] [CrossRef]
- Hägg, U.; Taranger, J. Maturation indicators and the pubertal growth spurt. Am. J. Orthod. 1982, 82, 299–309. [Google Scholar] [CrossRef]
- Adarsh, K.; Goyal, J.D.; Kaur, G.P.; Neeharika, T.; Samal, S.; Datla, P.K.V.; Ravuri, P. Longitudinal study on the impact of orthodontic treatment timing on skeletal and dental development in adolescents. J. Pharm. Bioallied Sci. 2025, 17, S460–S462. [Google Scholar] [CrossRef]
- Salehizeinabadi, M.; Ameli, N.; Kouchehbaghi, K.; Arastoo, S.; Neghab, S.; Kornerup, I.M.; Pacheco-Pereira, C. Dental age prediction from panoramic radiographs using machine learning techniques. PLOS Digit. Health 2025, 4, e0001077. [Google Scholar] [CrossRef]
- Vieira, I.; Pereira, M.L.; Caldas, I.M. The applicability of the Demirjian and Willems standards to age estimation of 6–9-year-old Portuguese children. Humans 2025, 5, 6. [Google Scholar] [CrossRef]
- Rebouças, P.R.M.; Alencar, C.R.B.; Arruda, M.J.A.L.L.A.; Lacerda, R.H.W.; Melo, D.P.; Bernardino, Í.M.; Bento, P.M. Identification of dental calcification stages as a predictor of skeletal development phase. Dent. Press J. Orthod. 2021, 26, e2119292. [Google Scholar] [CrossRef]
- Altan, H.; Sönmezgöz, E.; Belevcikli, M.; Altunok Ünlü, N.; Gül, A.; Demiray, M.D.; Altan, A. Dental Age Estimation by Demirjian, Willems, and Cameriere Methods in Children with Familial Mediterranean Fever: A Case–Control Study. Children 2025, 12, 1458. [Google Scholar] [CrossRef]
- Han, S.-Y.; Chang, C.-L.; Wang, Y.-L.; Wang, C.-S.; Lee, W.-J.; Vo, T.T.T.; Chen, Y.-L.; Cheng, C.-Y.; Lee, I.-T. A Narrative Review on Advancing Pediatric Oral Health: Comprehensive Strategies for the Prevention and Management of Dental Challenges in Children. Children 2025, 12, 286. [Google Scholar] [CrossRef] [PubMed]
- Tavares, B.S.; Bittencourt, J.M.; Ramos-Jorge, J.; Paiva, S.M.; Lopes-Silva, J.; Bendo, C.B. Path Model of Risk Factors for Age at Primary Tooth Eruption: A Cohort Study of Preterm and Term Infants. Int. J. Environ. Res. Public Health 2025, 22, 1837. [Google Scholar] [CrossRef]
- Saygili, S.; Tasyapan, S.A.; Cameriere, R.; Cakir Karabas, H.; Koruyucu, M.; Kasimoglu, Y. Dental age estimation in children and adolescents with amelogenesis imperfecta. BMC Oral Health 2025, 25, 1562. [Google Scholar] [CrossRef]
- Kim, N.-H.; Lee, J.-H.; Lee, S.; Choi, Y.J.; Chung, C.J.; Lee, K.-J.; Kim, K.-H. Growth velocity and the pubertal growth spurt across skeletal maturity stages in class II malocclusion: A longitudinal analysis. Children 2025, 12, 1612. [Google Scholar] [CrossRef]
- Badrov, J.; Lauc, T.; Nakaš, E.; Galić, I. Dental age and tooth development in orthodontic patients with agenesis of permanent teeth. Biomed. Res. Int. 2017, 2017, 8683970. [Google Scholar] [CrossRef] [PubMed]
- Teodorescu, I.M.; Preoteasa, E.; Preoteasa, C.T.; Murariu-Măgureanu, C.; Teodorescu, C. Association of Systemic Pathologies on Dental, Periodontal and Orthodontic Status in Children. Biomedicines 2025, 13, 2137. [Google Scholar] [CrossRef]
- Partyka, M.; Chałas, R.; Dunin- Wilczyńska, I.; Drohomyretska, M.; Klatka, M. Influence of growth hormone therapy on selected dental and skeletal system parameters. Ann Agric Environ Med 2018, 25, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Tabakcilar, D.; Bundak, R.; Gencay, K. Dental age in precocious and delayed puberty periods. Eur. J. Dent. 2021, 15, 539–545. [Google Scholar] [CrossRef]
- Espinoza-Silva, P.V.; López-Lázaro, S.; Fonseca, G.M. Forensic odontology and dental age estimation research: a scoping review a decade after the NAS report on strengthening forensic science. Forensic Sci Med Pathol 2023, 19, 224–235. [Google Scholar] [CrossRef]
- Bjelopavlovic, M.; Zeigner, A.-K.; Hardt, J.; Petrowski, K. Forensic Dental Age Estimation: Development of New Algorithm Based on the Minimal Necessary Databases. J. Pers. Med. 2022, 12, 1280. [Google Scholar] [CrossRef]
- Rathmann, H.; Reyes-Centeno, H.; Ghirotto, S.; et al. Reconstructing human population history from dental phenotypes. Sci Rep 2017, 7, 12495. [Google Scholar] [CrossRef]
- Velsko, I.M.; Fagernäs, Z.; Tromp, M.; et al. Exploring the potential of dental calculus to shed light on past human migrations in Oceania. Nat Commun 2024, 15, 10191. [Google Scholar] [CrossRef]
- Ubelaker, D.H.; Khosrowshahi, H. Estimation of age in forensic anthropology: Historical perspective and recent methodological advances. Forensic Sci. Res. 2019, 4, 1–9. [Google Scholar] [CrossRef]
- Griffith, J.I.; James, H.F.; Ordoño, J.; Fernández-Crespo, T.; Gerritzen, C.T.; Cheung, C.; Spros, R.; Claeys, P.; Goderis, S.; Veselka, B.; Snoeck, C. Reconstructing prehistoric lifeways using multi-isotope analyses of human enamel, dentine, and bone from Legaire Sur, Spain. PLoS ONE 2025, 20, e0316387. [Google Scholar] [CrossRef]
- Roulias, P.; Kalantzis, N.; Doukaki, D.; Pachiou, A.; Karamesinis, K.; Damanakis, G.; Gizani, S.; Tsolakis, A.I. Teeth Eruption Disorders: A Critical Review. Children 2022, 9, 771. [Google Scholar] [CrossRef]
- Yamaguchi, T.; Hosomichi, K.; Shirota, T.; Miyamoto, Y.; Ono, W.; Ono, N. Primary failure of tooth eruption: Etiology and management. Jpn. Dent. Sci. Rev. 2022, 58, 258–267. [Google Scholar] [CrossRef]
- Panchbhai, A.S. Dental radiographic indicators, a key to age estimation. Dentomaxillofac. Radiol. 2011, 40, 199–212. [Google Scholar] [CrossRef]
- Ratson, T.; Dagon, N.; Aderet, N.; Dolev, E.; Laviv, A.; Davidovitch, M.; Blumer, S. Assessing Children’s Dental Age with Panoramic Radiographs. Children 2022, 9, 1877. [Google Scholar] [CrossRef]
- Hostiuc, S.; Diaconescu, I.; Rusu, M.C.; Negoi, I. Age Estimation Using the Cameriere Methods of Open Apices: A Meta-Analysis. Healthcare 2021, 9, 237. [Google Scholar] [CrossRef]
- Birant, S.; Şirinoğlu Çapan, B. Dental age estimation using Willems methods in children. Int. Dent. J. 2024, 74, S151. [Google Scholar] [CrossRef]
- Carelli, J.; da Silva, G.S.; Gomes, M.V.; Vilalba, T.; Baratto-Filho, F.; Armando Brancher, J.; Beisel-Memmert, S.; Kirschneck, C.; Lopes, C.M.C.d.F.; Moro, A.; et al. Demirjian’s and Cameriere’s Methods for the Assessment of Dental Age Estimation in Children from a Southern Brazilian City. Diagnostics 2024, 14, 1513. [Google Scholar] [CrossRef]
- De Donno, A.; Angrisani, C.; Mele, F.; Introna, F.; Santoro, V. Dental age estimation: Demirjian’s versus the other methods in different populations. A literature review. Med. Sci. Law 2021, 61, 125–129. [Google Scholar] [CrossRef]
- Švábová, P.; Soták, M.; Galis, B.; Kroupová, P.; Bundová, L.; Vojtušová, A.; Masnicová, S.; Beňuš, R. Dental Age Assessment Based on Developmental Stages and Maturity Index of Third Molars for Medico-Legal Purposes. Diagnostics 2024, 14, 1559. [Google Scholar] [CrossRef]
- Tomás, L.F.; Mónico, L.S.; Tomás, I.; et al. The accuracy of estimating chronological age from Demirjian and Nolla methods in a Portuguese and Spanish sample. BMC Oral Health 2014, 14, 160. [Google Scholar] [CrossRef]
- Merdietio Boedi, R.; Angelakopoulos, N.; Franco, A.; et al. Evaluation of Demirjian staging method reproducibility and reliability for dental age estimation between eight forensic experts. Int. J. Legal Med. 2025, 139, 2883–2890. [Google Scholar] [CrossRef]
- Paddenberg, E.; Dees, A.; Proff, P.; Kirschneck, C. Individual dental and skeletal age assessment according to Demirjian and Baccetti: Updated norm values for Central-European patients. J. Orofac. Orthop. 2024, 85, 199–212. [Google Scholar] [CrossRef]
- Ferrillo, M; Migliario, M; Curci, C; Renò, F; Giudice, A; De Sire, A. Skeletal maturation evaluation: which is the reliability of dental calcification Demirjian method versus hand-wrist X-ray in growing subjects? A systematic review. Acta Odontol Scand. Published. 2024, 83, 230–237. [Google Scholar] [CrossRef]
- Demirjian, A.; Goldstein, H.; Tanner, J.M. A new system of dental age assessment. Hum. Biol. 1973, 45, 211–227. Available online: https://pubmed.ncbi.nlm.nih.gov/4714564/.
- Taylor, S.; Miller, C.; Daley, J.O. Oral health considerations for patients with systemic disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2025; Available online: https://www.ncbi.nlm.nih.gov/books/NBK617063/.
- Oluwagbemigun, K.; Dietrich, T.; Pischon, N.; Bergmann, M.; Boeing, H. Association between number of teeth and chronic systemic diseases: A cohort study followed for 13 years. PLoS ONE 2015, 10, e0123879. [Google Scholar] [CrossRef]
- Özdemir Çelik, D.S.; Belevcikli, M. Evaluation of dental ages of children with type I diabetes using different dental age estimation methods: a retrospective cohort study. Sci Rep 2015, 44461. [Google Scholar] [CrossRef]
- El-Bialy, T.; Aboul-Azm, S.F.; El-Sakhawy, M. Study of craniofacial morphology and skeletal maturation in juvenile diabetics (Type I). Am. J. Orthod. Dentofacial Orthop. 2000, 118, 189–195. [Google Scholar] [CrossRef]
- Lal, S.; Cheng, B.; Kaplan, S.; et al. Accelerated tooth eruption in children with diabetes mellitus. Pediatrics 2008, 121, e1139–e1143. [Google Scholar] [CrossRef]
- Alexa, I.; Dumitrescu, R.; Chioran, D.; Balean, O.; Bolchis, V.; Sava-Rosianu, R.; Popescu, S.; Galuscan, A.; Jumanca, D. Determinants of Oral Health Outcomes and Quality of Life in Diabetic Patients from Western Romania: A Behavioral Model Approach. Dent. J. 2025, 13, 247. [Google Scholar] [CrossRef]
- Solomon, O.; Beuran, I.A.; Constantin, I.; Leata, R.; Grosu, R.M.; Petrea, M.; Calin, A.; Earar, K. The influence of diabetes in pediatric dentistry. Rom. J. Oral Rehabil. 2024, 169(4), 936–945. [Google Scholar] [CrossRef]
- Grgic, O.; Prijatelj, V.; Dudakovic, A.; Vucic, S.; Dhamo, B.; Trajanoska, K.; Monnereau, C.; Zrimsek, M.; Gautvik, K.M.; Reppe, S.; Shimizu, E.; Haworth, S.; Timpson, N.J.; Jaddoe, V.W.V.; Jarvelin, M.-R.; Evans, D.; Uitterlinden, A.G.; Ongkosuwito, E.M.; van Wijnen, A.J.; Medina-Gomez, C.; Rivadeneira, F.; Wolvius, E.B. Novel genetic determinants of dental maturation in children. J. Dent. Res. 2023, 102, 349–356. [Google Scholar] [CrossRef]
- Ghergie, M.; Ciobotaru, C.D.; Pop, R.; Colceriu-Șimon, I.; Bunta, O.; Pastrav, M.; Feștilă, D. Correlation Between Dental Age, Chronological Age, and Cervical Vertebral Maturation in Patients with Class II Malocclusion: A Retrospective Study in a Romanian Population Group. Children 2025, 12, 398. [Google Scholar] [CrossRef]
- Palanisamy, V.; Rao, A.; Shenoy, R.; Baranya, S.S. Correlation of dental age, skeletal age, and chronological age among children aged 9-14 years: A retrospective study. J Indian Soc Pedod Prev Dent 2016, 34(4), 310–314. [Google Scholar] [CrossRef]
- Kumar, V.; Venkataraghavan, K.; Krishnan, R.; Patil, K.; Munoli, K.; Karthik, S. The relationship between dental age, bone age and chronological age in underweight children. J. Pharm. Bioallied Sci. 2013, 5, S73–S79. [Google Scholar] [CrossRef]
- Demirjian, A.; Buschang, P.H.; Tanguay, R.; Patterson, D.K. Interrelationships among measures of somatic, skeletal, dental, and sexual maturity. Am. J. Orthod. 1985, 88, 433–438. [Google Scholar] [CrossRef]
- Bedia, A.S.; Bedia, S.V.; Mulla, S.A.; Patil, A. Comparative evaluation of dental age vs. chronological age in healthy and underweight children aged 8–16 years: A cross-sectional study. Cureus 2025, 17, e79619. [Google Scholar] [CrossRef]
- Kanbur, N.O.; Kanli, A.; Derman, O.; Eifan, A.; Ataç, A. The relationships between dental age, chronological age and bone age in Turkish adolescents with constitutional delay of growth. J. Pediatr. Endocrinol. Metab. 2006, 19, 979–985. [Google Scholar] [CrossRef]
- Engström, C.; Engström, H.; Sagne, S. Lower third molar development in relation to skeletal maturity and chronological age. Angle Orthod. 1983, 53, 97–106. [Google Scholar] [CrossRef]
- Sierra, A.M. Assessment of dental and skeletal maturity: A new approach. Angle Orthod. 1987, 57, 194–208. [Google Scholar] [CrossRef]
- Vallejo-Bolaños, E.; España-López, A.J.; Muñoz-Hoyos, A.; Fernandez-Garcia, J.M. The relationship between bone age, chronological age and dental age in children with isolated growth hormone deficiency. Int. J. Paediatr. Dent. 1999, 9, 201–206. [Google Scholar] [CrossRef]
- Saraç, F.; Baydemir Kılınç, B.; Çelikel, P.; Büyüksefil, M.; Yazıcı, M.B.; Şimşek Derelioğlu, S. Correlations between Dental Age, Skeletal Age, and Mandibular Morphologic Index Changes in Turkish Children in Eastern Anatolia and Their Chronological Age during the Pubertal Growth Spurt Period: A Cross-Sectional Study. Diagnostics 2024, 14, 887. [Google Scholar] [CrossRef] [PubMed]
- Krailassiri, S.; Anuwongnukroh, N.; Dechkunakorn, S. Relationships between dental calcification stages and skeletal maturity indicators in Thai individuals. Angle Orthod 2002, 72, 155–166. [Google Scholar] [CrossRef]
- Harano, T.; Asahara, M. Evolution of tooth morphological complexity and its association with the position of tooth eruption in the jaw in non-mammalian synapsids. PeerJ 2024, 12, e17784. [Google Scholar] [CrossRef] [PubMed]
- Levesque, G.Y.; Demirjian, A. The inter-examiner variation in rating dental formation from radiographs. J Dent Res. 1980, 59, 1123–1126. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



