
Submitted:
04 January 2026
Posted:
06 January 2026
You are already at the latest version
Abstract
Rift Valley fever (RVF) is an acute, notifiable emerging arthropod-borne disease with epidemic and zoonotic potential. It poses a significant threat to public health, livestock, and food security in some African countries, including Nigeria. A phlebovirus causes RVF, a large group of RNA viruses of the family Bunyaviridae with potential for international spread and bioterrorism. RVF virus can infect several domestic and wild animals as well as humans. It is transmitted through direct contact with infected blood or body fluids, animal tissue, infected mosquito bites, etc. In humans, RVF is mostly associated with mild flu-like symptoms, which may develop into severe symptoms including encephalitis, hepatic disease, and hemorrhagic fever, while in animals, it causes high rates of abortion and perinatal mortality. Limited information is available in Nigeria on RVF. To gain a better understanding of the infection in livestock, we screened 368 sera collected at slaughter from cattle (n = 184) and camels (n = 184) at Kano abattoir between May and June 2022 for RVF virus antibodies. The sera were analysed using a commercial ELISA kit. Among the samples examined, female animals constituted the largest at 69.02% (254/368), compared to males at 30.97% (114/368). An overall seropositivity rate of 8.15% (30/368, CI: 5.67-11.29) was recorded. The seropositivity was higher in cattle, 8.69% (16/184, CI: 5.233-13.45), than in camels, 7.60% (14/184, CI: 4.396-12.15). Based on sex, seropositivity was slightly higher in female animals, at 8.27% (21/254, CI: 5.33-12.15), compared to males, at 7.89% (9/114, CI: 3.19-13.99). Our findings revealed that cattle and dromedary camels presented for slaughter in the Kano abattoir, northern Nigeria, have evidence of exposure to RVF virus. This may be a potential risk to humans working at the abattoir and other animal populations. A One-Health investigation is recommended to understand the risk factors, associated vectors, and human exposure to the virus to mitigate the health and socioeconomic threats posed by RVF in the region.
Keywords:
Rift Valley Fever
; one-health
; seropositivity
; public health risk
; surveillance
Introduction
Globally, zoonotic diseases, transmitted between animals and humans, pose a significant health risk to public, environmental, and animal health. Rift Valley fever (RVF) is an emerging, vector-borne viral zoonotic disease endemic in Sub-Saharan Africa and has been reported in the Arabian Peninsula and other African countries (Tigoi et al., 2020. RVF is caused by the RVF virus, a member of the phlebovirus genus in the Bunyaviridae (Adams et al., 2017; ICTV, 2024). Rift Valley Fever Virus (RVFV) is transmitted to humans through direct contact with infected blood, animal tissue, abortus foetus, birthing fluid, or infected mosquito bites belonging to the Aedes or Culex genera and possibly other biting insects like gnats and ticks (Tigoi et al., 2020; Socha et al., 2022; Tinto et al., 2023). Therefore, occupational groups like the abattoir workers, butchers, livestock handlers, breeders, dairy farmers, pastoralists, veterinarians and animal health workers are all at risk of infection (Mahendra et al., 2021; Tinto et al., 2023) as contact with diseased livestock is the primary way through which humans contract even though infected mosquito bites can also infect humans (Mansfield et al., 2015). In humans, it is asymptomatic, causing febrile illness with flu-like symptoms, and in some cases, it can develop into severe symptoms such as encephalitis and hemorrhagic fever disease with high case-fatality rates. Ocular, liver, and kidney disease are also common complications (Tigoi et al., 2020). In addition, a significant association between RVFV infections during pregnancy and an increased risk for miscarriage in humans has recently been demonstrated (Baudin et al., 2016). In livestock, RVFV causes abortions and perinatal mortality which vary from 5-100% (WOAH, 2023) therefore leading to serious economic repercussions as result of risks to food and nutrition insecurity due to significant losses in animal production (meat and milk), expensive management expenses, closure of livestock markets and stringent trade restrictions (Fawzy and Helmy, 2019; Tinto et al., 2023). This impacts negatively on affected communities’ socio-economic livelihoods that can lead to increased poverty (Jansen et al., 2018), and there is concern that RVF may emerge and spread to unaffected geographical regions due to international travel and livestock trade as a result of importation or exportation of disease-carrying insects or animals from endemic regions (Cẽtre-Sossah et al., 2012; Lapa et al., 2024; Hestianah et al., 2025). Therefore, the World Health Organization and many countries in Africa have prioritized it with respect to assigning it more urgent research and development for preparedness and response to public health emergencies (Faburay et al., 2017; Petrova et al., 2020; WHO, 2024) because of its high-consequence and ability to cause serious disease in both humans and animals during an outbreak, making it a major zoonotic disease that can transmit a list “A” disease internationally (Tomori and Oluwayelu, 2023). One-humped camels (Camelus dromedarius) have been associated with possible reservoirs and intermediate hosts for the transmission of potential zoonotic diseases as they are susceptible to several infectious diseases (Harrak et al., 2011; Kandeel and Al-Mubarake, 2022; Khalafalla, 2023). Previous studies have provided insight into the virus occurrence in camels and other domestic animals slaughtered in abattoirs in Nigeria (Opayele et al., 2019; Adamu et al., 2021; Alhaji et al., 2020). Poor disease reporting, surveillance, or monitoring systems have led to a scarcity of information on RVFV and other diseases status among camels in Nigeria, despite the high influx of camel trade and movement across porous borders into the country, which aids in the dissemination of disease. In Nigeria, camel meat and camel products consumption is on the increase due to poor economy, perceived nutritional value of camel meat, and a claimed curative property (Akpa et al., 2017; Kadim et al., 2018; Al Zahrani et al., 2023). However, diseases from these animals can spill over to humans due to the close contact and interface. Therefore, our overall hypothesis is that livestock slaughtered for human consumption in abattoirs in northern Nigeria are carriers of RVFV, an emerging zoonosis, therefore posing a public health risk.
Materials and Methods
Study Area
The study was carried out in Kano State, Nigeria, located in the Northwestern geo-political region of Nigeria (Figure 1). Samples were collected in the central abattoir, which is located at a longitude of 12.0144°N and latitude of 8.5184° E, respectively (Figure 2). It is well-known for slaughtering and meat processing of camels, cattle, sheep, and goats in the region.
Blood Sample Collection and Processing
Between May and June 2022, blood samples were collected at slaughter from cattle (n = 184) and camels (n = 184) at Kano abattoir, in sterile, non-anticoagulant sample vials, and were inclined at 45º until clotted. Sera were then harvested from the clotted blood into sterile and properly labeled 1.5 ml cryotubes. The serum samples were transported under a cold chain to NVRI, Vom, Nigeria, and stored at –20 ◦C until further use.
Antibody Detection by Competitive Enzyme-Linked Immunosorbent Assay (cELISA)
The bovine and camel sera were analysed for RVFV-specific IgG antibodies using a commercial ID Screen® RVF competition multispecies ELISA kit (ID-Vet, Grabels, France). The ELISA has shown 100% specificity and sensitivity (Kim et al., 2015; Hassine et al., 2017; Pérez-Ramírezet al., 2020), showing excellent performance, better than the other commercial kit, as a relatively low-cost, easy-to-use surveillance tool for the African context (Bronsvoort et al., 2019; Pedarrieu et al., 2021). As described by the manufacturer’s procedure, cELISA was performed as follows: Briefly, using a micropipette, 50 μl aliquots of test sera, as well as positive and negative control sera, were transferred undiluted to a 96-well RVFV antigen-coated microplate and were incubated for 45 min at 37°C. After incubation, the plates were washed three times with 300 μl of wash solution. Thereafter, 50 μl of diluted antibody-peroxidase conjugate was added to each well, incubated for 30 min at 21°C. The plates were then washed three more times with the wash buffer and 100 μl of the substrate solution was added. The reaction was stopped using 100 μl of the stopping solution added to each well. The results were read by using BioChek ELISA reader (Smart Vet Diagnostic, Reeuwwijk, Netherlands), and the optical density (OD) was determined at 450 nm. When test samples produced an optical density < 50 % of the mean of the negative controls were considered positive for RVFV antibodies, while if the optical density was ≥ 50 %, they were declared negative.
Statistical Analysis
Data were analysed using the SPSS version 20.0 statistics package. Positivity rate and Confidence intervals were calculated to summarize the variables. Levels of association between sero-positivity and sex, animal species were obtained using the chi-square test. Values of p ≤ 0.05 were regarded as statistically significant.
Results
The study recorded an overall seropositivity rate of 8.15% (30/368, CI: 5.67-11.29). Slightly higher seropositivity was recorded in cattle, 8.70% (16/184, CI: 5.233-13.45), compared to camels with 7.60% (14/184, CI: 4.396-12.15) (Figure 2). Taking both species together, based on seropositivity was slighlty higher in female animals, 8.27% (21/254, CI: 5.33-12.15), than in males, 7.89% (9/114, CI: 3.919-13.99), with no significant association between RVF and sex (p > 0.05) (Table 1).
Discussion
Rift Valley Fever is a viral emerging zoonosis that is considered a major veterinary and public health emergency. The importation and slaughtering of disease-carrying animals from endemic regions are contributing factors to the outbreaks (Hestianah et al., 2025). Therefore, the abattoir could be a strategic sentinel site to monitor unusual occurrences of zoonotic diseases (Falzon et al., 2021; Gerken et al., 2022; Fevre et al., 2023), as contact with infected livestock is the primary route through which humans contract RVF (Mansfield et al., 2015). This study detected antibodies to RVFV in dromedary camels and cattle slaughtered at the Kano abattoir, Northwestern Nigeria. The overall seropositivity rate of 8.15% (30/368, CI: 5.67-11.29) recorded in this study was significantly lower than previous reports in Nigeria: 19.9% (Andrew et al., 2021) among one-humped camels in Northern Nigeria, 20.7% (Hassan et al., 2021) among one-humped camels slaughtered in Maiduguri abattoir, Borno State, Nigeria. Oragwa et al. (2024) reported 18.4% in cattle and sheep populations in parts of Northern Nigeria. In Niger State, 11.3% was also reported by Alhaji et al. (2018). Sixteen (16.0%) also reported by Anejo-Okopi et al. (2020) in Jos, Plateau State. Other reports in Nigeria include 11.3% reported by Atuman et al. (2022) in Bauchi State and 18.7% reported by Olaleye et al. (1996). Other RVF cases in camels with relatively higher seroprevalence include reports by El Mamy et al. (2011), Rissmann et al. (2017), and Cosseddu et al. (2021), all from Mauritania, which recorded 32%, 33%, and 45%, respectively. In Tunisia, Selmi et al. (2020) reported 37% seroprevalence in camels. Abdallah et al. (2016), in Sudan, reported 9.6% in camels. In the Niger Republic, a higher seropositivity rate of 47.5% and 36.56% was also reported in by Mariner et al (1995) and Kadja et al. (2025). However, our findings are higher than the 0.7% reported by Opayele et al. (2019) among livestock in the Bodija Municipal abattoir in Ibadan, southwestern Nigeria, and the 5.3% reported in livestock handlers (Opayele et al., 2018). Using the hemagglutination-inhibition test (HI), Olaleye et al. (1996a, b) and Ezeifeka et al. (1982) reported seroprevalence of 3.3% and 3.13%, respectively. Other lower seroprevalence reported in other countries includes 5.85% in camels reported by Mroz et al. (2017) and 1.3% recorded in Turkey by Gür S. et al. (2017). Kalthoum et al. (2021) and Hassine et al. (2017), both from Tunisia, found 0% seropositivity in camels. The disparity in seropositivity rate in these studies may probably be attributed to differences in sampling season, as an increase in vector population during the rainy season tends to increase RVF outbreaks. This finding could potentially reflect the seasonal trend of the disease (Hassan et al., 2021). This might be the reason why a low rate of seropositivity was also recorded in this study, as samples were collected from May to June, which is still almost the dry season, which is not a suitable climatic period to provide optimal conditions for mosquito population blooms (Kortekaas, 2014; Chambaro et al., 2022; Tariku and Rebuma, 2024). Environmental factors, differences in sample size and sampling location, camel population dynamics together with seasonal movements and trade networks, and different diagnostic assays all could have also contributed to the different seropositivity rate, as previously reported (Rissmann et al., 2020; Kadja, 2025). Using ELISA, which is attributed to being more sensitive, 8.15% seroprevalence was recorded, which is higher than the 3.3% and 3.13% reported by Olaleye et al. (1996) and Ezeifeka et al. (1982) using HI. RVF is an arthropod-borne disease that occurs in specific ecologies, meaning that camels from different locations have varying exposure rates to different factors influencing the occurrence of the disease (Ikegami and Makiho, 2011). The antibodies against RVF recorded in these camels may suggest natural exposure to the RVF virus, as vaccination is not a common practice in camels, and all camels sampled were adult and without maternal antibodies. A higher seropositivity rate was recorded in female camels than in males. This might be attributed to differences in sample size, as more samples were collected from females than from males. This may also be due to the longer lifespan of females, which increases cumulative exposure, and the predominance of females in Saharan herds, as males are sometimes sold or slaughtered (Kadja et al., 2025). Hormonal factors may also increase susceptibility, which is in line with earlier findings that associate RVFV infection with increased incidence of female abortions (Sumaye et al., 2013; Hama et al., 2019). There is no statistically significant association between RVF antibodies and sex. This corroborates the findings of Hassan et al. (2021). However, this contrasts with the findings of Maturi et al. (2021) in Kenya, who reported a significant association between RVF and sex. This disparity may be attributed to the possible difference in animal husbandry practices and climatic zones of the study locations. This may also be a result of the small sample size collected, which failed to detect any association. A higher proportion of positive samples were recorded in cattle than in camels in this study, with no significant association between RVFV and breeds. This study provided evidence of RVFV in camels and cattle slaughtered in Nigeria using the cELISA method. The study was limited by a small sample size in both livestock. Samples were also collected for two months, May and June which coincide with the dry season in this study area when activity of the mosquito vector is less. Therefore, it is recommended that additional surveillance either passive or active should be conducted with a large sample size with sampling throughout the year or season and locations to understand the current status of RVFV in Nigeria. As establishing an active animal health surveillance system to detect new cases is crucial for providing veterinary and human public health authorities early warning because animal outbreaks of RVF precede human cases (Ishema et al., 2024). Creating awareness among abattoir workers on the importance of basic health precautions and the use of personal protective clothing when handling animals or during slaughter. A One-Health investigation was also recommended to understand the risk factors, associated vectors, and human exposure to the virus to mitigate the health and socioeconomic threats posed by RVF.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abdallah, M.M.; Adam, I.A.; Abdalla, T.M.; Abdelaziz, S.A.; Ahmed, M.E.; Aradaib, I.E. A survey of rift valley fever and associated risk factors among the one-humped camel (Camelus dromedaries) in Sudan. Ir Vet J 2016, 69, 6. [Google Scholar] [CrossRef]
- Adamu, A.M; Allam, L.; Sackey, A.K.B.; Nma, A.B.; Mshelbwala, P.P.; Machunga-Mambula, S.; Idoko, S.I; Adikwu, A.A.; Nafarnda, W.D.; Garba, B.S.; Owolodun, O.A.; Dzikwi, A.A.; Balogun, E.O; Simon, A.Y. Risk factors for Rift Valley fever virus seropositivity in one-humped camels (Camelus dromedarius) and pastoralist knowledge and practices in Northern Nigeria. One Health 2021, 13, 100340. [Google Scholar] [CrossRef]
- Adam,s M.J.; E.J.; Lefkowitz, A.M.; King, B.; Harrach, R.L.; Harrison, N.J.; Knowles, A. M.; Kropinski, M.; Krupovic, J.H.; Kuhn, A.R.; Mushegian, M. Nibert et al., Changes to taxonomy and the International Code of Virus Classification and Nomenclature ratified by the International Committee on Taxonomy of Viruses (2017), Arch. Virol. 2017. 162 (8) 2505–2538 [CrossRef]
- Al Zahrani, A; Alfakeeh, A; Alghareeb, W; Bakhribah, H; Basulaiman, B; Alsuhail, A; et al. Use of camel urine is of no benefit to cancer patients: observational study and literature review. East Mediterr Health J 2023, 29(8), 657–663. [Google Scholar] [CrossRef] [PubMed]
- Akpa, GN; Abbaya, HY; Saley, ME. Comparative evaluation of the influence of species, age and sex on carcass characteristics of camels, cattle, sheep and goats in Sahel environment. Anim Res Int. 2017, 14, 2588. [Google Scholar]
- Alhaji, NB; Babalobi, OO; Wungak, Y; Ularamu, HG. Participatory survey of Rift Valley fever in nomadic pastoral communities of North-central Nigeria: The associated risk pathways and factors. PLoS Negl Trop Dis. 2018, 12(10), e0006858. [Google Scholar] [CrossRef] [PubMed]
- Anejo-Okopi, J.; Oragwa, A.O.; Okojokwu, O.J.; Joseph, S.; Chibueze, G.; Adetunji, J.; Okwori, J.A.; Amanyi, D.O.; Ujah, O.I.; Audu, O. Seroprevalence of Rift Valley fever virus infection among slaughtered ruminants in Jos, north-central, Nigeria. Hosts and viruses 2020, 7, 109–115. [Google Scholar] [CrossRef]
- Anyangu, AS; Gould, LH; Sharif, SK; Nguku, PM; Omolo, JO; Mutonga, D; Rao, CY; Lederman, ER; Schnabel, D; Paweska, JT; Katz, M; Hightower, A; Njenga, MK; Feikin, DR; Breiman, RF. Risk factors for severe Rift Valley fever infection in Kenya, 2007. Am J Trop Med Hyg. 2010, 83(2 Suppl), 14–21. [Google Scholar] [CrossRef]
- Bolajoko, M.B.; Babalobi, O.O. Evaluation of the effectiveness of animal diseases reporting system in Oyo State, Nigeria (1995-2005). Journal of Commonwealth Veterinary Association 2011, 27, 264–267. [Google Scholar]
- Bronsvoort; Bagninbom, JM; Ndip, L; Kelly, RF; Handel, I; Tanya, VN; Morgan, KL; Ngu Ngwa, V; Mazeri, S; Nfon, C. Comparison of Two Rift Valley Fever Serological Tests in Cameroonian Cattle Populations Using a Bayesian Latent Class Approach. Front Vet Sci 2019, 6, 258. [Google Scholar] [CrossRef] [PubMed]
- Cêtre-Sossah, C.; Pédarrieu, A.; Guis, H.; Defernez, C.; Bouloy, M.; Favre, J.; Girard, S.; Cardinale, E.; Albina, E. Prevalence of Rift Valley fever among ruminants, Mayotte. Emerg. Infect. Dis. 2012, 18(6), 972–975. [Google Scholar] [CrossRef]
- Chambaro, HM; Hirose, K; Sasaki, M; Libanda, B; Sinkala, Y; Fandamu, P; et al. An unusually long Rift valleyfever inter-epizootic period in Zambia: Evidence for enzootic virus circulation and risk for diseaseoutbreak. PLoS Negl Trop Dis [Internet] cited. 2022, 16(6). [Google Scholar] [CrossRef] [PubMed]
- El Mamy, AB; Baba, MO; Barry, Y; Isselmou, K; Dia, ML; El Kory, MO; Diop, M; Lo, MM; Thiongane, Y; Bengoumi, M; Puech, L; Plee, L; Claes, F; de La Rocque, S; Doumbia, B. Unexpected Rift Valley fever outbreak, northern Mauritania. Emerg Infect Dis. 2011, 17(10), 1894–6. [Google Scholar] [CrossRef] [PubMed]
- Ezeifeka, G.O.; Umoh, J.U.; Belino, E.D.; Ezeokoli, C.D. A serological survey for Rift Valley fever antibodies in food animals in Kaduna and Sokoto States of Nigeria. Int. J. Zoonoses. 1982, 9, 147–151. [Google Scholar] [PubMed]
- Falzon, L.C.; Ogola, J.G.; Odinga, C.O.; Naboyshchikov, L.; Fevre, E.M.; Berezowski, J. Electronic data collection to enhance disease surveillance at the slaughterhouse in a smallholder production system. Sci. Rep. 2021, 11, 19447. [Google Scholar] [CrossRef]
- Faburay, B.; Labeaud, A.D.; Mcvey, D.S.; Wilson, W.C.; Richt, J.A. Current status of Rift Valley fever vaccine development. Vaccines 2017, 5(3), 29. [Google Scholar] [CrossRef] [PubMed]
- Fawzy, M.; Helmy, Y.A. The one health approach is necessary for the control of Rift Valley fever infections in Egypt: a comprehensive review. Viruses 2019, 11(2), 139. [Google Scholar] [CrossRef] [PubMed]
- FAO. FOOSTAT; Food and Agriculture Organization of the United Nations: Rome, 2018; Available online: http://www.fao.org/faostat/en/#data/QA (accessed on 08 March 2025).
- Food, J. M. Immunity and charismatic camel. Lab Anim. 2013, 42, 159. [Google Scholar] [CrossRef]
- Gerken, K.N.; Ndenga, B.A.; Owuor, K.O.; Winter, C.A.; Seetah, K.; LaBeaud, A.D. Leveraging livestock movements to urban slaughterhouses for wide-spread Rift Valley fever virus surveillance in Western Kenya. One Health 2022, 15, 100457. [Google Scholar] [CrossRef]
- Gür, S; Kale, M; Erol, N; Yapici, O; Mamak, N; Yavru, S. The first serological evidence for Rift Valley fever infection in the camel, goitered gazelle and Anatolian water buffaloes in Turkey. Trop Anim Health Prod 2017, 49(7), 1531–1535. [Google Scholar] [CrossRef] [PubMed]
- Hama, M. A.; Ibrahim, A. I.; Alassane, A.; Gagara, H.; Alambedji, R. B. Séroprévalence de la fièvre de la vallée du Rift chez les ruminants domestiques dans la région de Tahoua/Niger. International Journal of Biological and Chemical Sciences 2019, 13(7), Article 7. [Google Scholar] [CrossRef]
- Harrak, MEB. Faye, M. Bengoum, Main pathologies of camels, breeding of camels, constraints, benefits and perspectives, in: Conf. OIE, 2011, pp. 1–6.
- Hassine, T.B.; Amdouni, J.; Monaco, F.; Savini, G.; Sghaier, S.; Selimen, I.B.; Chandoul, W.; Hamida, K.B; Hammami, S. Emerging vector-borne diseases in dromedaries in Tunisia: West Nile, bluetongue, epizootic haemorrhagic disease and Rift Valley fever. Onderstepoort. J Vet Res. 2017, 84(1), e1–e3. [Google Scholar] [CrossRef] [PubMed]
- Hestianah, EP; Khairullah, AR; Effendi, MH; Budiastuti, B; Tyasningsih, W; Budiarto, B; Permatasari, DA; Moses, IB; Ahmad, RZ; Wardhani, BWK; Kusala, MKJ; Kurniasih, DAA; Fauziah, I; Wibowo, S; Ugbo, EN; Fauzia, KA. Rift Valley fever: A zoonotic disease with global potential. Open Vet J 2025, 15(6), 2312–2328. [Google Scholar] [CrossRef]
- ICTV (International Committee on Taxonomy of Viruses). ICTV 2023 Master Species List (MSL#39). 2024. Available online: https://ictv.global/.
- Ishema, L; Colombe, S; Ndayisenga, F; Uwibambe, E; Van Damme, E; Meudec, M; Rwagasore, E; Mugwaneza, D; Van Bortel, W; Shyaka, A. One Health investigation and response to a nationwide outbreak of Rift Valley fever in Rwanda - March to December 2022. One Health 2024, 19, 100854. [Google Scholar] [CrossRef]
- Jansen van Vuren, P; Kgaladi, J.; Patharoo, V.; Ohaebosim, P.; Msimang, V.; Nyokong, B.; Paweska, J.T. Human cases of Rift Valley fever in South Africa, 2018. Vector Borne Zoonot. Dis. 2018, 18(12), 713–715x. [Google Scholar] [CrossRef] [PubMed]
- Kadim, IT; Mahgoub, O; Purchas, RW. A review of the growth, and of the carcass and meat quality characteristics of the one-humped camel (Camelus dromedaries). Meat Sci. 2018, 80, 555–69. [Google Scholar] [CrossRef] [PubMed]
- Kadja Mireille Catherine , Karimou Hamidou Ibrahim, Edmond Onidje, Souahibou Sourokou Sabi, Amadou Yahaya Mahamane, Haladou Gagara , Benjamin Obukowho Emikpe, Rianatou Bada Alambedji (2025). Seroprevalence of Rift Valley Fever Viruses Antibodies in Domestic Livestock in the Tahoua Region of Niger Veterinaria Italiana, Vol. 61 No. 3. [CrossRef]
- Kalthoum Sana, Elena Arsevska, Kaouther Guesmi, Aymen Mamlouk, Jamel Cherni, Monia lachtar, Raja Gharbi, Bassem Bel Haj Mohamed, Wiem Khalfaoui, Anissa Dhaouadi, Mohamed Naceur Baccar, Haikel Hajlaoui, Samia Mzoughi, Chedia Seghaier, Lilia Messadi d , Malek Zrelli e , Soufien Sghaierf , Catherine C^etre-Sossah c,g , Pascal Hendrikx, Cecile Squarzoni-Diaw (2012) Risk-based serological survey of Rift Valley fever in Tunisia (2017–2018). [CrossRef]
- Kandeel, M.; Al-Mubarak, A.I.A. Camel viral diseases: Current diagnostic, therapeutic, and preventive strategies. Front. Vet. Sci. 2022, 9, 915475. [Google Scholar] [CrossRef]
- Khalafalla, AI. Zoonotic diseases transmitted from the camels. Front Vet Sci. 2023, 10, 1244833. [Google Scholar] [CrossRef]
- Kim, H.J.; Park, J.Y.; Jeoung, H.Y.; Yeh, J.Y.; Cho, Y.S.; Choi, J.S.; Lee, J.Y.; Cho, I.S.; Yoo, H.S. Serological surveillance studies confirm the Rift Valley fever virus free status in South Korea. Trop Anim Health Prod. 2015, 7, 1427–30. [Google Scholar] [CrossRef] [PubMed]
- Kortekaas, J. One Health approach to Rift Valley fever vaccine development. Antiviral Res 2014, 106. [Google Scholar] [CrossRef] [PubMed]
- Lapa, D; Pauciullo, S; Ricci, I; Garbuglia, AR; Maggi, F; Scicluna, MT; Tofani, S. Rift Valley Fever Virus: An Overview of the Current Status of Diagnostics. Biomedicines 2024, 12(3), 540. [Google Scholar] [CrossRef]
- Mansfield, K.L.; Banyard, A.C.; McElhinney, L.; Johnson, N.; Horton, D.L.; Hernández-Triana, L.M.; Fooks, A.R. Rift Valley fever virus: a review of diagnosis and vaccination, and implications for emergence in Europe. Vaccine 2015, 33(42), 5520–5531. [Google Scholar] [CrossRef]
- Mariner, JC; Morrill, J; Ksiazek, TG. Antibodies to hemorrhagic fever viruses indomestic livestock in Niger: Rift Valley fever and Crimean-Congo hemorrhagicfever. Am J Trop Med Hyg. 1995, 53, 217–2. [Google Scholar] [CrossRef]
- Mroz, C.; Gwida, M.; El-Ashker, M.; et al. Seroprevalence of Rift Valley fever virus in livestock during inter-epidemic period in Egypt, 2014/15. BMC Vet Res 2017, 13, 87. [Google Scholar] [CrossRef]
- Olaleye, O. D.; Tomori, O.; Schmitz, H. Rift Valley fever in Nigeria: infections in domestic animals. Revue scientifique ettechnique (International Office of Epizootics) 1996a, 15(3), 937–946. [Google Scholar] [CrossRef]
- Olaleye, O. D.; Tomori, O.; Ladipo, M. A.; Schmitz, H. Rift Valley fever in Nigeria: infections in humans. Revue scientifique et technique (International Office of Epizootics) 1996b, 15(3), 923–935. [Google Scholar] [CrossRef]
- Opayele, AV; Ndiana, LA; Odaibo, GN; Olaleye, DO. Serological evidence of Rift Valley fever virus infection in slaughtered ruminants in Nigeria. J Immunoassay Immunochem. 2019, 40(4), 367–377. [Google Scholar] [CrossRef]
- Pedarrieu, A; El Mellouli, F; Khallouki, H; Zro, K; Sebbar, G; Sghaier, S; Madani, H; Bouayed, N; Lo, MM; Diop, M; Ould El Mamy, AB; Barry, Y; Dakouo, M; Traore, A; Gagara, H; Souley, MM; Acha, S; Mapaco, L; Chang'a, J; Nyakilinga, D; Lubisi, BA; Tshabalala, T; Filippone, C; Heraud, JM; Chamassy, SB; Achiraffi, A; Keck, N; Grard, G; Mohammed, KAA; Alrizqi, AM; Cetre-Sossah, C. External quality assessment of Rift Valley fever diagnosis in countries at risk of the disease: African, Indian Ocean and Middle-East regions. PLoS One 2021, 16(5), e0251263. [Google Scholar] [CrossRef] [PubMed]
- Petrova, V.; Kristiansen, P.; Norheim, G.; Yimer, A.S. Rift Valley fever: Diagnostic challenges and investment needs for vaccine development. BMJ Glob. Health 2020, 5, e002694. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Ramírez, E; Cano-Gómez, C.; Llorente; Adzic, F; Al Ameer, B; Djadjovski, M; El Hage, I; El Mellouli, J; Goletic, F; Hovsepyan, T; Karayel-Hacioglu, H; Maksimovic Zoric, I; Mejri, J; Sadaoui, S; Salem, H; Sherifi, SH; Toklikishvili, K; Vodica, N; Monaco, A; Brun, F; Jiménez-Clavero, A; Fernández-Pinero, MÁ.J. External quality assessment of Rift Valley fever diagnosis in 17 veterinary laboratories of the Mediterranean and Black Sea regions. PLoS One 2020, 15(9), e0239478. [Google Scholar] [CrossRef] [PubMed]
- Rissmann, M; Eiden, M; El Mamy, BO; Isselmou, K; Doumbia, B; Ziegler, U; Homeier-Bachmann, T; Yahya, B; Groschup, MH. Serological and genomic evidence of Rift Valley fever virus during inter-epidemic periods in Mauritania. Epidemiol Infect 2017, 145(5), 1058–1068. [Google Scholar] [CrossRef]
- Selmi, R; Mamlouk, A; Ben; Said, M.; Ben, Yahia, H; Abdelaali, H; Ben Chehida, F. Daaloul-Jedidi M, Gritli A, Messadi L. First serological evidence of the Rift Valley fever Phlebovirus in Tunisian camels. Acta Trop. 2020 Jul;207:105462. doi: 10.1016/j.actatropica.2020.105462. Socha, W.; Kwasnik, M.; Larska, M.; Rola, J.; Rozek, W.; 2022. Vector-borne viral diseases as a current threat for human and animal health-one health perspective. J. Clin. Med. 11(11), 3026 [CrossRef]
- Sumaye, R. D.; Geubbels, E.; Mbeyela, E.; Berkvens, D. Inter-epidemic Transmission of Rift Valley Fever in Livestock in the Kilombero River Valley, Tanzania: A Cross-Sectional Survey. PLoS Neglected Tropical Diseases 2013, 7(8), 2356. [Google Scholar] [CrossRef]
- Tigoi, C.; Sang, R.; Chepkorir, E.; Orindi, B.; Arum, S.O.; Mulwa, F.; et al. High risk for human exposure to Rift Valley fever virus in communities living along livestock movementroutes: A cross-sectional survey in Kenya. PLoS Negl Trop Dis. 2020, 14(2), e0007979. [Google Scholar] [CrossRef]
- Tinto, B.; Quellec, J.; Cêtre-Sossah, C.; Dicko, A.; Salinas, S.; Simonin, Y. 2023. Rift Valley fever in West Africa: a zoonotic disease with multiple socio-economic consequences. One Health 17(1), 100583.Tomori, O. and Oluwayelu, D.O. 2023. Domestic animals as potential reservoirs of zoonotic viral diseases. Annu. Rev. Anim. Biosci. 11(1), 33–55. [CrossRef]
- World Health Organisation. Pathogens prioritization: a scientific framework for epidemic and pandemic research preparedness. Available online: https://www.who.int/teams/blueprint/who-r-and-d-blueprint-for-epidemics (accessed on 24 November 2025).
- World Animal Health Organization, Chapter 3.1.18 Rift Valley Fever, (n.d.). https ://www.woah.org/fileadmin/Home/eng/Health_standards/tahm/3.01.18_RVF.pdf (Accessed November 24, 2025).
Figure 1.
Map of Nigeria, showing Kano State (Red), Study area.
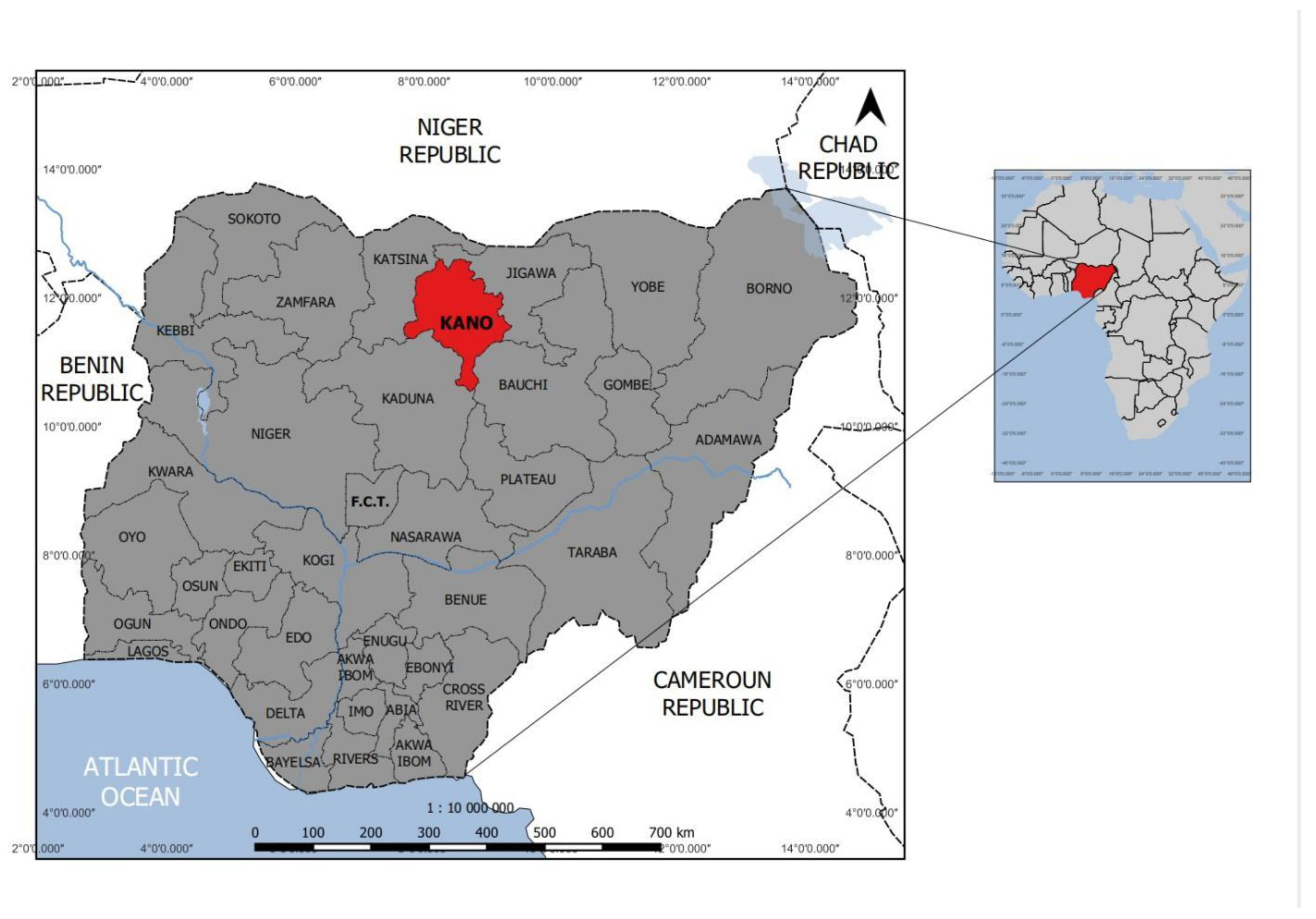
Figure 2.
Seropositivity rate of RVF in Camels and Cattle in Kano, Nigeria.
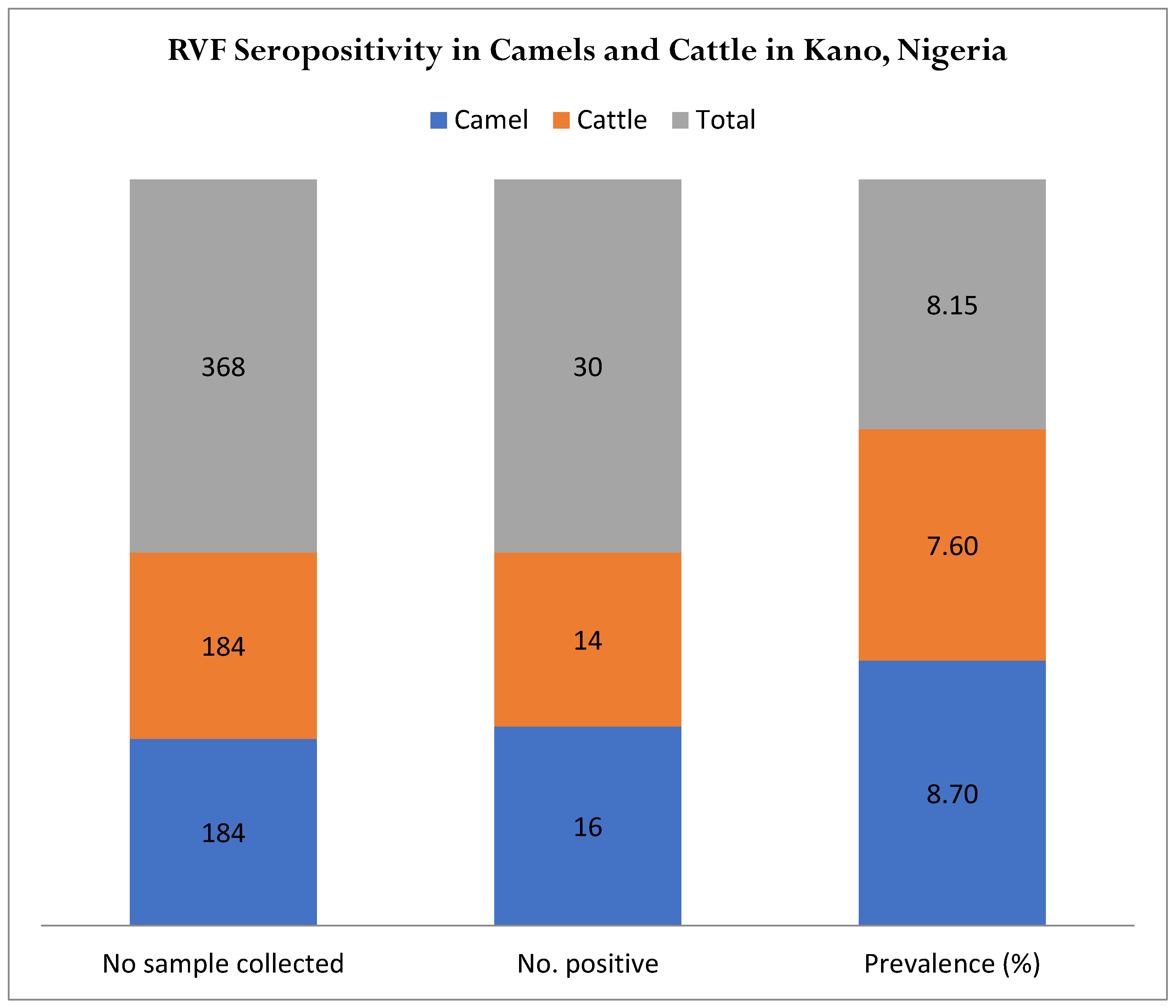

Table 1.
RVF Seropositivity rate in Nigeria based on sex.
| Sex | No. Sample Tested | No. Positive | % | Confidence Interval |
|---|---|---|---|---|
| Male | 114 | 9 | 7.89 | 3.19-13.99 |
| Female | 254 | 21 | 8.27 | 5.33-12.15 |
| Total | 368 | 30 |
p ≥ 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



