
Submitted:
04 January 2026
Posted:
05 January 2026
You are already at the latest version
Abstract
Cantrell syndrome (CS) is a rare congenital disorder involving defects in the thoraco-abdominal midline, the diaphragm, the pericardium, the sternum and the heart. Since the first description of the syndrome, 165 well-documented cases in humans have been reported, reflecting remarkable heterogeneity ranging from complete pentalogy to partial or atypical variants. We conducted a systematic review and classified body wall defects and associated anomalies into the following nine categories: midline defects, lateral defects, and special cases. Each case was reassessed for umbilical cord status, body wall morphology, cardiac anomalies and additional malformations. Midline defects predominated (152/165), with variants of supraumbilical defect being the most frequent; umbilical hernias accounted for ten cases as a distinct subgroup. Lateral defects were rare (nine cases, 5.5%), typically presenting with thoracogastroschisis or lateral thoracoabdominoschisis, and often associated with normal cords. Across all categories, cardiac anomalies were universal, with ventricular and atrial septal defects being the most common. Reclassification revealed that many cases originally labelled as 'classic PC' were better defined as partial or atypical forms. This unified framework clarifies the epidemiology, enhances diagnostic accuracy and, from a One Health perspective, highlights CS as a shared developmental vulnerability across species.
Keywords:
Cantrell’s syndrome
; ectopia cordis
; body stalk anomaly (BSA)
; thoracoabdominal anomalies
; mesodermal fusion failure
; ventral body wall closure
; lateral folding disruption
; cardiogenic field migration
; developmental continuum
; comparative embryology
; One Health
1. Introduction
First described in 1958, Cantrell’s syndrome (CS) is a rare congenital anomaly that disrupts multiple midline structures, including the sternum, diaphragm, pericardium, thoracoabdominal wall, and heart [1]. This study reports 165 cases of Cantrell’s syndrome in human medicine [2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103]. However, the variability and inconsistent classification of these cases have hindered progress in understanding the developmental origins of the syndrome. The defining feature, ectopia cordis (EC), has been categorized in various ways, often conflating different pathological mechanisms and obscuring the embryological basis of these malformations Cozar et al., [104]. From a developmental perspective, CS offers a valuable opportunity to study the fundamental processes of embryogenesis. During gastrulation, mesodermal cells migrate and differentiate into distinct lineages, including the lateral plate mesoderm [NMA and Avedillo 2019 Cantrell; Pechriggl et al., 2022; Solerte and Cosmi 2022; So et al., 2023 [105,106,107,108]. This lineage contributes to the formation of the ventral body wall, diaphragm, pericardium, and cardiac structures. Proper fusion of the lateral plate mesoderm at the ventral midline is essential for continuity across thoracoabdominal structures [105,106]. Failures in this fusion event can result in multisystem anomalies, including sternal clefts, diaphragmatic defects, and EC [105,106]. Conversely, lateral defects, such as gastroschisis, arise from localized disruptions in body wall folding. These defects reflect paraumbilical failures of morphogenetic closure, rather than systemic errors in mesodermal fusion [109,110,111,112,113,114,115]. It is important to recognize this distinction: midline defects represent global failures of embryonic integration, while lateral defects reflect localized disturbances in morphogenetic movements. The cardiogenic field, derived from the splanchnic mesoderm, undergoes a complex migration and folding process to form the primitive heart tube [116]. Disruptions to this process, especially when accompanied by incomplete ventral mesodermal fusion, can result in EC and other cardiac malformations (Ma and Adelstein 2014) [117]. Similarly, the diaphragm originates from several embryonic sources, including the septum transversum and the pleuroperitoneal folds. These structures depend on the coordinated development of the mesoderm. Disruption of these pathways provides a mechanistic explanation for the range of anomalies observed in CS [106]. Comparative embryology offers valuable insights into these conditions. In veterinary medicine, especially in canine models, EC has been systematically classified into different types [Cozar 104], offering a structured framework that can be applied to human cases. This approach clarifies diagnostic differences between Cantrell’s syndrome and related conditions, such as body stalk anomaly (BSA), and highlights conserved embryological mechanisms across species. Within a One Health framework, cross-species analyses emphasize the interconnectedness of human and animal developmental biology. These analyses highlight the potential of comparative approaches to advance our understanding of congenital anomalies.
Thus, this review reexamines the existing literature on Cantrell’s syndrome through the lens of comparative development. Integrating veterinary classifications into the analysis of human cases aims to improve diagnostic accuracy, shed light on shared mesodermal pathways, and propose a unified framework for understanding the embryogenesis of thoracoabdominal anomalies.
2. CS Classification
The syndrome’s defining feature, EC, has been inconsistently classified, which limits the ability to compare cases and understand their embryological origins (Cozar et al.,) [104]. To address this issue, a structured classification system for midline and lateral defects has been proposed (Table 1). Midline defects include: UThAb (umbilical thoracoabdominoschisis with an abnormal umbilical cord and omphalocele), SUThAb (supraumbilical thoracoabdominoschisis with a normal umbilical cord), SUStAb (supraumbilical sternal abdominoschisis with a normal umbilical cord), UAb+DD (umbilical abdominoschisis with a diaphragmatic defect and an abnormal umbilical cord and omphalocele), SUAb+DD (supraumbilical abdominoschisis with a diaphragmatic hernia), SUICD (supraumbilical incomplete central defect), and UH+DD (umbilical hernia with a diaphragmatic defect). Lateral defects (LAb and gastroschisis) are further subdivided into ThLAb (thoraco-lateral abdominoschisis) and StLAb (sternal lateral abdominoschisis).
When these diverse anomalies are diagnosed as CS, the distinction between midline and lateral defects becomes blurred, and the syndrome is defined too broadly. This conflation can obscure the underlying mechanisms, as midline defects represent systemic failures of embryonic fusion, while lateral defects reflect localized folding errors (Pechriggl et al., 2022) [106]. It is crucial to recognize this difference. If all such situations are labeled as CS, the clinical and embryological specificity of the diagnosis is lost. This complicates comparisons across cases and hinders progress in understanding the syndrome’s true origins. Therefore, it is essential to carefully distinguish between CS and related anomalies to avoid diagnostic dilution and preserve the integrity of clinical and embryological analyses. Figure 1 shows a flowchart illustrating the midline classification framework for CS.
Figure 1 summarizes the distribution of body wall defects reported in human cases of Cantrell syndrome, as determined by a comprehensive literature review. The defects are organized into midline and lateral categories. Midline anomalies represent most documented cases. Midline defects include umbilical cord–related and non–umbilical cord defects. These range from thoracoabdominal and abdominal/omphalocele presentations to various supraumbilical abnormalities, such as supraumbilical thoracoabdominal defects, isolated cord defects, and umbilical hernias. The most frequently described subtype is supraumbilical abdominal defects. In contrast, lateral defects are far less common and consist exclusively of non-umbilical cord anomalies, including thoracic defects, lateral thoracoabdominal defects, and lateral abdominal defects. Overall, the figure reflects the predominance of midline structural abnormalities in published human cases and highlights the anatomical variability documented in the literature. In veterinary medicine, particularly in dogs, EC has been documented and systematically categorized into distinct types (Cozar et al.,) [104]. This classification system can be applied to human cases, offering greater clarity in distinguishing CS from related anomalies, such as BSA. This framework integrates human and veterinary data from a One Health perspective.
3. CS in Human Medicine
CS is characterized by a combination of five midline defects that affect the abdominal wall, sternum, diaphragm, pericardium, and heart [1,105,108]. The clinical presentation can vary greatly, ranging from complete to partial or atypical forms, which complicates diagnosis. Although 165 cases have been documented, the heterogeneity of diagnostic criteria has limited the ability to establish standardized prognostic frameworks. Mortality remains high, especially in cases involving severe cardiac malformations, underscoring the necessity of more precise classification systems. Current approaches often group diverse anomalies under a single label, obscuring pathogenetic distinctions and complicating clinical management and developmental interpretation.
To clarify and standardize the analysis of CS, the 165 documented cases were reorganized into nine tables based on the morphology and topography of body wall defects, umbilical cord status, and associated anomalies. The cases in all tables are numbered chronologically according to their order of publication. When a publication reported more than one case, each case was assigned to and retained under the original author’s reference number. This ensured accurate case tracking and maintained precision when individual cases were cited or discussed later. Midline defects, representing the majority of cases, were subdivided into seven tables to capture the spectrum of supraumbilical, thoracic, abdominal, and umbilical ring presentations (Table 2, Table 3, Table 4, Table 5, Table 6, Table 7 and Table 8). Lateral defects, though rare, were grouped into a separate table to emphasize their distinctive asymmetric characteristics (Table 9). A ninth table was reserved for special cases that did not conform to traditional definitions, including those without body wall involvement or mixed supraumbilical–thoracic anomalies (Table 10). Separating the cases into these nine tables allows for a systematic comparison across subtypes. It also ensures transparent documentation of the original designations of the authors and our reclassifications. This approach underscores the heterogeneity of CS while maintaining a unified framework for interpretation. Table 2, Table 3, Table 4, Table 5, Table 6, Table 7 and Table 8 presents the subtypes of midline defects, along with case details including gender, associated anomalies, and the authors’ and proposed diagnoses.
Table 2 presents seven cases of thoracoabdominoschisis (ThAb) associated with UCD. All cases exhibit full-thickness disruption of the midline extending from the thorax into the abdomen with exposure of cardiac structures and abdominal viscera. The presence of a UCD, such as a short cord, cysts, abnormal coiling, or a single umbilical artery, was confirmed through direct image review. These cases consistently demonstrate high rates of EC and complex intracardiac anomalies, which reinforces the severe phenotype associated with ThAb. Each entry includes the original author designation, our post hoc reclassification, umbilical cord status, type of cardiac exposure, and overlay tags for PC class and BSA type, when applicable. This subgroup represents the most extensive form of midline defect in the Cantrell spectrum, highlighting the diagnostic importance of cord morphology and thoracoabdominal continuity.
The term BSA was originally used to describe human congenital malformations [118,119,120,121]. However, the formal BSA classification was first developed in pigs as a comparative model pig [122]. This framework was then applied to human cases human [123] and later extended to other species, such as dogs and cats, in which similar patterns of ventral closing defects were observed [dogs cats [124,125]. This system recognizes eight major BSA types, as well as several additional complexes, such as the sternal body wall complex (STBWC), spinal body wall complex (SPBWC), spinal limb body wall complex (SPLBWC), and sternal spinal body wall complex (SSBWC) [current 126]. These complexes have already been applied to pigs, cats, and dogs to capture mixed constellations of sternal, spinal, and limb involvement [122,124,125]. In this review, we apply these complexes to human cases for the first time, providing a unified, comparative framework that aligns human and veterinary classifications. This approach reinforces the one health perspective by demonstrating that CS and related body stalk anomalies share conserved developmental pathways across species [Cozar 104]. Table 2 shows that six of the seven cases of ThAb were diagnosed within the BSA framework. This finding highlights the significant overlap between CS and BSA phenotypes. A common feature across these cases was the presence of UCD, which appears to be a defining characteristic of this subgroup. The distribution included BSA Type VI with STBWC III, BSA Type V with SSBWC III, BSA Type V with SPLBWC III, and BSA Type II with STBWC I, as well as SPBWC III and ABS classifications. Most cases were assigned to PC Class 2, reflecting probable but incomplete pentalogy. Several cases showed EC or associated anomalies. This clustering indicates that ThAb with cord pathology tends to align with higher-order BSA types, in which ventral defects is accompanied by sternal, spinal, or limb involvement. These findings reinforce the diagnostic value of cord morphology in distinguishing severe BSA-related complexes. They also suggest that umbilical cord anomalies may be a unifying feature linking CS to the broader spectrum of BSA across species.
Table 3 summarizes three cases of thoracoschisis (Th) in which the umbilical cord appeared normal with no evidence of structural anomalies, such as a single umbilical artery, cysts, abnormal coiling, or velamentous insertion. In this subgroup, Th is characterized by a full-thickness defect of the thoracic wall that is typically lateral or paramedian with variable degrees of cardiac exposure. Unlike UCD-positive Th, these cases demonstrate that severe thoracic wall disruption can occur independently of cord pathology. Each entry documents the author’s original designation, our post hoc reclassification, cord status, type of EC, and overlay tags for PC class and BSA type, when applicable. This small but distinct subgroup underscores the heterogeneity of CS, demonstrating that thoracic wall defects can present with normal cord morphology yet still involve significant cardiac pathology.
Table 4 summarizes 19 cases of Ab in which umbilical cord anomalies were documented. Ab in this subgroup is characterized by a full-thickness midline abdominal wall defect and is frequently associated with abnormal cord morphology, such as a single umbilical artery, cysts, a short cord, or atypical coiling. These cord anomalies were confirmed through direct image review and serve as consistent markers of this phenotype. The table includes the original designations of the authors and our post hoc reclassification alongside details of cord status, type of EC (ExEC), and overlay tags for PC class and BSA type. The predominance of PC Class 2 assignments indicates partial or probable pentalogy, and several cases align with higher-order BSA complexes. Together, these cases highlight the strong link between Ab and umbilical cord pathology. This emphasizes the importance of cord anomalies in diagnosing severe forms of CS within the broader spectrum of BSA. In Table 4, which compiles 19 cases of Ab with umbilical cord anomalies, five were further classified within the BSA framework. These included BSA Type VIII with STBWC IV, BSA Type VII with SSBWC IV, and one case of BSA Type II with STBWC I. The majority of these BSA-associated cases were assigned to PC Class 2 or 3, reflecting partial or incomplete pentalogy, while a smaller proportion fell into PC Class 1. Notably, EC was documented in several of these cases, reinforcing the severity of the phenotype. The clustering of Ab with cord pathology into higher-order BSA types highlights the strong developmental link between ventral wall disruption and umbilical cord anomalies. This subgroup demonstrates that cord anomalies are not incidental but rather integral markers of complex body stalk involvement, bridging CS with the broader comparative classification of ventral wall defects across species.
Table 5 summarizes the 23 cases classified as SUThAb in which the umbilical cord was reported as normal. These cases serve as an essential comparison group for evaluating the role of cord anomalies in the pathogenesis and phenotypic variability of Ab. By isolating cases without cord pathology, the table provides a clearer assessment of the abdominal wall defect itself and helps distinguish primary SUThAb features from secondary changes associated with cord abnormalities. Individual case references are retained to ensure traceability and accuracy in subsequent discussion.
Table 6 compiles 63 reported cases of SUAb in which the umbilical cord was described as normal. By excluding cases with associated cord anomalies, this dataset provides a clearer assessment of the intrinsic characteristics of the SUAb defect and allows for comparison with cases presenting umbilical cord pathology.
Table 7 summarizes the 28 reported cases classified as a supraumbilical incomplete central defect (SUICD). These cases represent a distinct subgroup of supraumbilical abdominal wall defects, characterized by partial or incomplete disruption of the central supraumbilical region. Presenting these cases separately allows for a clearer delineation of their anatomical features and facilitates comparison with complete supraumbilical abdominoschisis (SUAb) and other related phenotypes.
Table 8 summarizes the ten reported cases diagnosed as umbilical hernias. The cases are presented separately to distinguish the true herniation of abdominal contents through the umbilical ring from the other congenital abdominal wall defects included in the review. Detailing this subset allows for a clearer comparison of anatomical features, associated findings, and clinical outcomes across the broader spectrum of umbilical and supraumbilical anomalies.
Table 9 summarizes nine reported cases of lateral abdominal wall defects. These defects are characterized by an opening located lateral to the midline. This distinguishes them anatomically and developmentally from supraumbilical and central defects. Presenting these cases as a separate subgroup enables clearer comparisons of their morphological features, associated anomalies, and proposed pathogenetic mechanisms within the broader spectrum of abdominal wall defects.
Table 10 includes three cases that were classified as “special cases” due to features that do not fit neatly into the main categories of abdominal wall defects analyzed in this review. The case reported by Angoulvant et al. [51] exhibits a diaphragmatic defect, a pericardial defect, and cardiac defects, such as an atrial septal defect and anomalous pulmonary venous return, but shows no body wall defect or umbilical cord defect. However, the absence of ventral body wall involvement suggests a more appropriate diagnosis of congenital heart disease with associated midline structural defects rather than incomplete PC. Similarly, the case described by Hubbard et al. [85] lacks a body wall defect and UCD, but presents with a sternal defect, multiple cardiac defects, including a ventricular septal defect, single coronary artery, and atrial septal defect, as well as an external EC and additional anomalies, such as an encephalocele, craniofacial dysmorphism, and a cleft palate. Although the authors labeled it as PC, the constellation of findings aligns more closely with EC accompanied by broader craniofacial and thoracic abnormalities. The third case, from Martadiansyah et al. [103], includes an umbilical incomplete central defect, a sternal defect, diaphragmatic defect, and patent ductus arteriosus, as well as significant cardiac defects. Although it is described as EC complicated by PC, the pattern of anomalies is more consistent with PC, specifically Class 1 in association with a body stalk anomaly (BSA) Type VIII, which corresponds to STBWC IV. Together, these cases demonstrate how overlapping phenotypes, particularly when UCDs, craniofacial anomalies, or lateralized defects are present, blur the distinction between PC and other embryologically distinct processes, highlighting the need for clearer differentiation.
4. Veterinary Perspective: Ectopia Cordis and Cantrell’s Syndrome
In contrast, veterinary medicine has advanced a systematic classification of BSA in pigs, dogs and cats [122,124,125,126], and EC in dogs [104], distinguishing cases by anatomical location and associated thoracoabdominal defects for EC and skeletal structural defects for BSA. This structured approach provides clarity in differentiating between variations in presentation and embryological origin. Importantly, canine cases represent naturally occurring models of rare congenital anomalies, offering insights into mesodermal development and ventral body wall formation. These observations highlight the role of comparative embryology, as dogs provide a biologically relevant framework for understanding anomalies that mirror human conditions.
A retrospective descriptive analysis was performed on 19 published cases of congenital thoracoabdominal and cardiac anomalies in dogs and cats historically associated with Pentalogy of Cantrell (PC) or related midline developmental defects. The presence or absence of the five classic PC components (abdominal wall defect, sternal defect, diaphragmatic defect, pericardial defect, and intracardiac anomalies) was extracted for each case, along with additional malformations, such as ectopia cordis, limb defects, craniofacial anomalies, and body stalk abnormalities. The reported diagnoses from the original authors were then compared to a standardized reclassification using contemporary PC criteria (classes 1–3) and complementary systems, including BSA types and STBWC/SSBWC categories. We recorded species, sex, and defect combinations to identify patterns, misclassifications, and phenotypic clusters.
Table 11 summarizes nineteen reported cases of congenital thoracoabdominal and cardiac malformations in dogs and cats that fall within the spectrum of Pentalogy of Cantrell (PC) and related midline defects. For each case, the table lists the presence or absence of the five classic PC components: abdominal wall, sternal, diaphragmatic, pericardial, and cardiac defects. It also lists additional anomalies, such as ectopia cordis, limb defects, craniofacial defects, and body stalk abnormalities. The table also compares the original diagnosis given by each author with a standardized reclassification using current PC criteria. Overall, the table shows that most animals have multiple midline defects. Incomplete PC is the most common form, while the most severe cases—often those with ThAb—meet the criteria for complete PC. The table highlights the wide phenotypic variability of these conditions and illustrates how modern classification systems can more accurately reinterpret earlier case reports.
Table 12 summarizes six cases of porcine congenital malformations consistent with Pentalogy of Cantrell (PC) reported by Martín-Alguacil and Avedillo [105]. Each piglet exhibited a remarkably uniform pattern of defects beginning with ThAb as the primary body wall abnormality. This severe midline disruption is accompanied by consistent umbilical cord abnormalities, including short cords, abnormal coiling patterns (ACP), dispersed umbilical vessels (DUV), and, in some cases, single or hypoplastic umbilical arteries (SUA or HUA). All cases exhibit the five classical components of PC: body wall defect, sternal defect, diaphragmatic defect, pericardial defect, and intracardiac anomalies. These cases fulfill the criteria for PC Class 1 (complete PC). Cardiac defects vary among individuals and include atrial septal defects (ASD), ventricular septal defects (VSD), globular heart morphology (GHM), hypoplastic auricles, a single coronary artery, and severe anomalies, such as transposition of the great arteries (TGA) and mitral valve atresia (MAV). All piglets also present with ectopia cordis, which is an external manifestation of the most severe PC phenotypes. Additional visceral anomalies, such as ectopic caecum (EcC), ectopic liver (EcL), and amorphous liver masses (LAM), reinforce the profound disruption of ventral midline development. The proposed diagnosis consistently reclassifies all six cases as PC Class 1 accompanied by BSA Type VI and STBWC Type III, reflecting extensive involvement of the thoracic, abdominal, and umbilical structures. These uniform classifications indicate that these piglets exhibit a consistent and severe expression of the Cantrell spectrum with overlapping BSA features.
Table 13 summarizes 16 cases of ruminants—mostly calves and two lambs—with congenital midline defects involving the thoracic region. There is a strong predominance of ectopia cordis (EC). Unlike pigs and carnivores, in which pentalogy of Cantrell (PC) is common, the ruminants in this dataset exhibit a distinct pattern dominated by cervical or cervico-pectoral EC, with minimal or absent involvement of the abdominal wall. Nearly all cases exhibit an absent body wall defect, and the umbilical cord is either normal or not reported. This indicates that these anomalies primarily affect the upper thoracic and cervical midline rather than the abdominal region. Every case in the table exhibits sternal defects and external ectopia cordis, confirming a consistent failure of thoracic midline closure. Many animals also exhibit pericardial defects and complex cardiac malformations, such as double apex, duplicated cranial vena cava, ventricular septal defects, anomalous pulmonary venous return, a single coronary artery, and a double-outlet right ventricle. These cardiac anomalies are often accompanied by nonstructural spinal defects, cleft palate, colonic stenosis, and visceral abnormalities, such as hepatic fibrosis or amorphous liver masses. These abnormalities reflect broader disruptions of embryonic midline development. Most cases were originally diagnosed as cervical, cervico-pectoral, or thoracic ectopia cordis, and the proposed diagnosis confirms this interpretation. Only one case (Case 38) meets the criteria for PC Class 2 due to the presence of an umbilical hernia, a diaphragmatic defect, a pericardial defect, and multiple intracardiac anomalies. All other cases lack the abdominal wall component required for PC and are classified as ectopia cordis (EC). Overall, the table shows that ruminants have a typical EC-dominant phenotype with sternal defects and severe cardiac malformations, but not the abdominal wall defects that are common in PC. These characteristics distinguish ruminant presentations from those of pigs and carnivores, suggesting species-specific patterns in ventral midline developmental failure.
5. Comparative Analysis: Applying Veterinary Classification to Human Cases
Applying the canine and pig classification system to human cases reveals that several anomalies historically labeled as CS align more closely with BSA. This reclassification suggests that CS and BSA may represent points along a continuum of malformative processes rather than discrete syndromes. Recognizing this continuum is critical for refining diagnostic accuracy and avoiding conflation of distinct pathogenetic mechanisms. Comparative analysis thus underscores the value of veterinary models in sharpening human diagnostic frameworks and clarifying the developmental variability observed across cases.
A combined analysis of 165 human cases and veterinary data from carnivores, pigs, and ruminants shows that CS and other ventral midline defects form a continuous spectrum of developmental disruption across species, though there are clear species-specific patterns. In humans, stratifying cases across Table 2, Table 3, Table 4, Table 5, Table 6, Table 7, Table 8, Table 9 and Table 10 reveals that the severity and anatomical extent of the defect correlate strongly with umbilical cord morphology. ThAb with cord anomalies (Table 2) is the most severe condition on this spectrum. It is characterized by full-thickness thoracoabdominal disruption, external ectopia cordis, and complex intracardiac defects. These cases frequently correspond to higher-order BSA types and sternal-spinal-limb complexes, similar to the porcine model in which all reported piglets exhibit ThAb, abnormal cords, and complete PC. Abdominoschisis with cord anomalies (Table 4) follows a similar pattern at the abdominal level. There is strong clustering into BSA types VII–VIII and II, and predominant assignment to PC class 2 or 3. Conversely, thoracoschisis with normal cords (Table 3), SUThAb and SUAb with normal cords (Table 5 and Table 6), and SUICD (Table 7) demonstrate that significant thoracic or abdominal wall defects can occur independently of cord pathology and typically manifest as milder or more localized expressions of the Cantrell/BSA field.
The carnivore dataset closely parallels the human distribution. Like humans, dogs and cats exhibit the full range of phenotypes, from complete PC with ThAb and cord anomalies (analogous to human Table 2) to incomplete PC and SUICD-like presentations (resembling human cases in Table 5, Table 6, Table 7 and Table 8). As in humans, ThAb in carnivores is strongly associated with severe cardiac defects, sternal agenesis, and high-order BSA classifications. Cases with normal cords, on the other hand, tend to fall into PC Class 3 or remain outside the PC spectrum. This alignment reinforces developmental continuity between human and carnivore presentations, supporting the use of BSA and STBWC/SSBWC complexes as comparative tools across species.
Pigs occupy a unique position within this comparative framework. All six porcine cases exhibit a highly uniform and extreme phenotype consisting of ThAb, severe umbilical cord anomalies, external ectopia cordis, and complex intracardiac malformations. These cases are consistently classified as PC Class 1 with BSA Type VI and STBWC III. This homogeneity contrasts with the broader phenotypic variability seen in humans and carnivores, suggesting that pigs express a particularly severe and stable form of ventral midline defects. Notably, the BSA classification was initially developed in pigs, subsequently applied to humans, and then to carnivores [122,123,124,125,126]. The porcine data in this review reaffirm the value of this system for capturing high-order, multisystem involvement.
By contrast, ruminants display a distinct, largely non-abdominal phenotype. Calf and lamb cases are characterized by cervical, cervicothoracic, or thoracic ectopia cordis, along with sternal defects and complex cardiac anomalies, though there is no abdominal wall disruption or umbilical cord pathology. These cases do not align well with the human ThAb, Ab, SUAb, or SUICD groups. Instead, they resemble a small subset of human thoracoschisis cases with normal cords (Table 3). The consistent cranial displacement of the defect in these cases suggests a species-specific vulnerability of the upper thoracic and cervical midline. This distinguishes ruminants from the thoracoabdominal and umbilical patterns seen in humans, pigs, and carnivores.
Taking together, these findings highlight two major axes that define the comparative expression of Cantrell-related defects across species: the craniocaudal level of the ventral defect and the presence or absence of umbilical cord anomalies. Humans, pigs, and carnivores share a common pattern: ThAb or Ab combined with cord pathology marks the most severe BSA-associated phenotypes, while defects with normal cords tend to be milder or anatomically restricted. Ruminants, however, cluster into a separate ectopia cordis phenotype that is focused cranially and minimally involves the umbilical region. This comparative perspective reinforces the one health concept by demonstrating that CS, BSA, and related ventral defects arise from conserved developmental pathways, yet manifest differently depending on species-specific embryologic constraints. It also underscores the diagnostic value of umbilical cord morphology as a cross-species marker of high-order body stalk involvement and provides a unified framework for interpreting human and veterinary cases within a shared developmental continuum.
6. Embryological Insights and Pathogenetic Mechanisms
CS is characterised by a range of midline defects affecting the thoracoabdominal wall, sternum, diaphragm, pericardium and heart [1,104,105,108]. Understanding its embryological origins is crucial for grasping why midline defects, and less commonly lateral defects, can occur. From an embryological perspective, ventral body wall anomalies represent a spectrum of developmental failures that occur at different stages and through distinct mechanisms. Omphalocele arises when the physiological herniation of the midgut, which usually occurs during weeks 6–10 of human embryogenesis, does not resolve properly, resulting in abdominal contents herniating into the umbilical cord within a membranous sac. In contrast, supraumbilical midline defects, as seen in Cantrell’s syndrome, originate much earlier — between human days 14–18 and canine days 14–35 — when the lateral plate mesoderm fails to fuse at the ventral midline [104,106]. This produces systemic anomalies involving the sternum, diaphragm, pericardium and abdominal wall. Within this same developmental window, sternal defects result from the incomplete fusion of paired sternal bars derived from the somatic mesoderm (Scaal 2020) [143]. This leads to clefts or agenesis of the sternum. Diaphragmatic defects, meanwhile, reflect the abnormal migration and incorporation of the septum transversum and pleuroperitoneal membranes [144,145]. This produces anterior diaphragmatic gaps that often accompany the Cantrell spectrum. Gastroschisis is characterised by a localized disruption to the folding of the lateral body wall around weeks 4–6 in humans, typically just to the right of the umbilicus [114]. This results in a paraumbilical opening without a covering sac, and is usually not associated with cardiac or diaphragmatic anomalies. Finally, rectus diastasis is a milder defect of ventral body wall development caused by incomplete fusion of the linea alba, which is derived from the lateral plate mesoderm (Sadler 2010) [146,147]. Unlike the other anomalies, it does not involve a true wall defect or herniation, but rather manifests as a separation of the rectus muscles along the midline. Taken together, these conditions demonstrate how disturbances in mesodermal fusion, folding and midgut migration can generate a range of thoracoabdominal malformations, from severe open defects to subtle connective tissue abnormalities, in both human and canine embryogenesis.
In vertebrates, the body wall comprises the skin, muscles, and supportive connective tissues. Its formation depends on a series of tightly regulated, sequential events during embryonic development (Pechriggl et al., 2022) [106]. The formation of the two body cavities and the sealing of the body wall depend on the coordinated interaction of numerous developmental processes. Disruption to these processes during embryogenesis can result in serious structural anomalies in newborns, including congenital diaphragmatic hernia and ventral body wall defects such as gastroschisis and omphalocele (Pechriggl et al., 2022) [106,114]. To understand this process, we present a detailed overview of the essential mechanisms for the correct development of the abdominal and thoracic walls. This analysis offers valuable insights into body wall formation and, importantly, clarifies the embryological differences between lateral and midline defects. Following fertilization, the zygote undergoes cleavage and compaction to form the blastocyst. After compaction, the morula develops into a blastocyst, losing its totipotent capacity in the process (Pechriggl et al., 2022) [106]. The inner cell mass gives rise to the embryoblast, while the outer layer differentiates into the trophoblast. The trophoblast supports implantation into the endometrium and provides nutrition. Within the embryoblast, two distinct cell populations emerge: the epiblast, which is positioned next to the amniotic cavity, and the hypoblast, which is oriented towards the blastocyst cavity. Amnioblasts lie adjacent to the trophoblast and remain continuous with the epiblast. The epiblast cells are arranged radially and become enclosed by the amniotic cavity. Meanwhile, the hypoblast (visceral endoderm) cells delaminate from the epiblast and are separated by a basal lamina. They subsequently line the secondary yolk sac. The establishment of these two layers — the epiblast and the hypoblast — defines the embryo’s dorsoventral axis. During gastrulation, the initially two-dimensional structure remodels into a three-dimensional trilaminar disc, ultimately forming the three germ layers. By the end of the second week, the primitive streak appears, marking the beginning of further morphogenetic events, as it does in dogs at a comparable stage (Sheng et al., 2021) [148,149,150]. This marks the start of gastrulation, which results in the formation of a trilaminar embryo. The notochord then directs neurulation and somite differentiation. The rapid expansion of the somites and the lateral plate mesoderm initiates the folding process, incorporating the yolk sac into the embryonic body and establishing the common body cavity (Sadler 2010) [146]. By around week 3 in humans and day 20 in dogs, the umbilical cord and connecting stalk begin to develop [150]. By week 7 in humans and around day 30 in dogs, the cord is fully formed and takes on metabolic functions. The pleuroperitoneal folds then begin to fuse between weeks 4 and 6, with complete closure of the pleuroperitoneal canals occurring by the end of week 7. In dogs, the equivalent process occurs between days 20 and 35 of embryogenesis, with fusion of the pleuroperitoneal folds and closure of the canals completed by approximately day 35 [124]. In humans, the transverse septum emerges around day 22 of embryogenesis. Physiological herniation of the intestine normally occurs by week 6 in humans and day 30 in dogs, resolving by week 10 in humans and day 35 in dogs [151,152]. If this retraction fails, an omphalocele develops. Conversely, rupture of the amnion between weeks 8–10 in humans or days 30–35 in dogs leads to gastroschisis [115]. During the early fusion window (days 14–18 in humans and days 14–35 in dogs), disruption to the fusion of the mesoderm can result in supraumbilical midline defects, sternal defects, diaphragmatic defects, pericardial defects and rectus diastasis. These anomalies collectively define the spectrum of CS, representing failures of early ventral body wall formation. In contrast, omphalocele and gastroschisis arise later, during the stages of intestinal herniation and body wall closure.
The midline and lateral body wall defects arise from disruptions in the complex morphogenetic processes that shape the ventral body wall during early embryogenesis. They represent a spectrum of anomalies—including omphalocele, gastroschisis, ectopia cordis, and bladder exstrophy—that reflect failures in midline fusion or lateral folding of the embryonic body wall (Pechriggl et al., 2022) [106]. As shown in Figure 2, the critical windows of ventral body wall development define the embryonic stages at which defects such as Cantrell’s spectrum, gastroschisis and omphalocele may occur.
Evidence from different species suggests that disruptions in the development of the lateral plate mesoderm represent the main mechanism underlying Cantrell’s syndrome and related thoracoabdominal anomalies (Aldeiri et al 2018; NMA and Avedillo 2020; So et al., 2023; Cozar et al., 2025) [104,105,108,153]. During gastrulation, mesodermal cells migrate and differentiate into the lateral plate mesoderm, contributing to the ventral body wall, diaphragm, pericardium and cardiogenic field. The prevailing theory places this critical period between days 14–18 of human embryogenesis (Goetzinger 2018; Palacios et al., 2022) [154,155], which corresponds to approximately days 14–35 in canine development. During this time, mesodermal folds must migrate and fuse towards the ventral midline (Meena and Meena 2016) [78]. Failures in this fusion process result in systemic midline defects affecting the sternum, diaphragm, pericardium and abdominal wall [104,105,108,153,154,155] (Aldeiri et al 2018; NMA and Avedillo 2020; So et al., 2023; Cozar et al., 2025; Goetzinger 2018; Palacios et al., 2022). In contrast, localized disruptions to body wall folding generate lateral anomalies such as gastroschisis, which typically do not involve the heart or diaphragm. Further explanations for the occurrence of ectopia cordis and associated cardiac malformations lie in perturbations in cardiogenic field migration and folding (Carmi and Boughman, 1992) [156]. Additionally, defective development of the septum transversum, which normally contributes to the formation of the diaphragm and the pericardium, exacerbates these anomalies. Taken together, human and animals embryological evidence highlights how a narrow developmental window of lateral plate mesodermal activity governs the range of thoracoabdominal malformations observed in different species.
Table 14 offers a side-by-side comparison of the embryological pathways that lead to ventral body wall defects in humans and dogs, highlighting their similarities and differences. It summarizes key developmental processes, including midline folding, sternal and diaphragmatic formation, cardiac descent, and umbilical ring closure, and maps them onto the specific defects observed in each species. By comparing the timing of embryonic disruption, the anatomical structures affected, and the resulting characteristic phenotypes, the table highlights conserved mechanisms underlying Cantrell-related anomalies and illustrates species-specific differences in expression. This summary helps readers understand how similar developmental failures can produce parallel patterns of thoracoabdominal defects in humans and dogs. It also reinforces the value of comparative embryology in interpreting complex ventral wall defects.
Omphaloceles result from continued physiological midgut herniation. The displaced intestine fails to return to the abdominal cavity, ultimately causing intestinal malrotation and abnormal positioning (Pechriggl et al., 2022)[106,114]. Gastroschisis is a congenital structural abnormality of the abdominal wall, characterised by the extrusion of visceral organs through a paraumbilical defect (Pechriggl et al., 2022) [106,114,115]. Unlike omphalocele, the herniated intestine lacks an amniotic covering and is therefore directly immersed in amniotic fluid (Chauaire Noack 2021) [110]. Several pathogenetic mechanisms have been proposed to explain its origin over the past decades: impaired mesodermal development (Duhamel, 1963) [158]; rupture of the amnion adjacent to the umbilical ring (Lammer et al., 2008) [110]; oestrogen-induced thrombosis of the umbilical vein (Lubinsky, 2024) [111]; malformation of the right vitelline artery (Hoyme et al., 1983) [112]; and defective invagination of the secondary yolk sac and omphalomesenteric duct, despite normal abdominal wall formation otherwise (Stevenson et al., 2009) [113].
The convergence of human and canine data highlights conserved developmental pathways and emphasizes the importance of comparative embryology in congenital anomaly research. By integrating veterinary and human findings, a unified framework emerges that links mesodermal morphogenetic failures to the spectrum of thoracoabdominal malformations. This perspective advances both clinical and developmental biology by situating Cantrell’s Syndrome within broader embryological processes rather than treating it as an isolated clinical entity.
7. Discussion
CS remains a rare and complex anomaly with significant heterogeneity in clinical presentation and embryological interpretation. The comparative approach adopted here, which involves applying veterinary classifications of ectopia cordis and body wall defects to human cases, provides new insights into diagnosing and categorizing this syndrome. In both humans and animals, CS is fundamentally linked to the complex process of body cavity closure. The variety of ways in which CS presents clinically reflects the points at which these developmental events can be disrupted. Failures in mesodermal fusion, ventral folding, or incorporation of the septum transversum result in the range of anomalies that define Cantrell’s pentalogy. Understanding these embryological foundations clarifies the variability of the syndrome and provides a framework for distinguishing it from related ventral body wall malformations. The literature fully supports the theory that CS results from a failure of the lateral plate mesoderm to migrate and fuse at the ventral midline during early embryogenesis (Arraf et al., 2016, 2020) [158,159]. This mechanism can explain why midline defects are so common, since the sternum, diaphragm, pericardium, abdominal wall, and heart all originate from the ventral mesodermal field. The rare occurrence of lateral defects suggests that the embryological insult may sometimes be more extensive or involve adjacent developmental fields (Arraf et al., 2016) [158]. The comparative analysis of human and veterinary cases presented in this review sustain this idea, showing that across species, the severity and anatomical distribution of ventral body wall defects consistently reflect the timing, location, and extent of mesodermal disruption. The animal data fully endorse this embryological model. In carnivores, for instance, ThAb accompanied by UCD closely resembles the most severe human cases. Dogs and cats exhibit the full range of phenotypes, from complete PC with ThAb and sternal agenesis to complex cardiac anomalies, to incomplete forms resembling human SUICD and supraumbilical defects. These parallels reinforce the idea that the same ventral mesodermal field is vulnerable across species and that the presence of umbilical cord anomalies reliably indicates high-order body stalk involvement. Porcine cases provide an even more striking comparison: all piglets exhibit a uniform, extreme phenotype consisting of ThAb, severe cord anomalies, external ectopia cordis, and complex intracardiac defects. They are consistently classified as PC Class 1 with BSA Type VI [105]. This homogeneity suggests that pigs express a particularly severe and stable form of ventral midline defects, offering a powerful model for understanding the upper end of the Cantrell/BSA spectrum. In contrast, ruminants display a distinct cranial phenotype, which is dominated by cervical or cervicothoracic ectopia cordis, along with sternal and cardiac defects, but with minimal abdominal involvement and no cord pathology [137,138,139,140,141,142]. This pattern resembles only a small subset of human thoracoschisis cases, highlighting species-specific differences in the craniocaudal vulnerability of the ventral midline. One of the most significant contributions of the canine model is its systematic classification of ectopia cordis types. This classification allows for more precise differentiation of cases that would otherwise be grouped under the broad umbrella of CS. Upon re-examining the 165 revised human cases, it was found that several could be more accurately classified as BSA, underscoring the necessity of a unified framework that transcends species boundaries. The porcine BSA classification, which was originally developed in pigs and later applied to humans, dogs, and cats, further supports this integrative approach [122,123,124,125,126]. These cross-species classifications clarify the embryological mechanisms involved and underscore the importance of mesodermal developmental defects as a common pathogenetic pathway.
Reports of abnormalities in the formation of the abdominal cavity and wall have become increasingly frequent in recent years. However, the physiological and pathophysiological mechanisms underlying these malformations remain poorly understood. Current evidence suggests that epigenetic influences play a significant role, while chromosomal aberrations account for only a small percentage of cases. This emphasizes the importance of future research focusing on environmental factors and their role in the pathogenesis of abdominal wall defects [106](Pechriggl et al., 2022). Understanding the chronological, spatial, and morphogenetic progression of organogenesis is necessary to grasp the impact of both external and internal disruptions on organ system differentiation (Pechriggl et al., 2022) [106](. Adopting a One Health perspective strengthens this analysis further by framing congenital anomalies as a shared concern across species. Veterinary data, often overlooked in human medicine, provide valuable comparative models for rare syndromes. Canine ectopia cordis provides insight into human cases, and the porcine BSA classification system improves diagnostic categories and deepens our understanding of embryological mechanisms. Together, these models bridge gaps in classification and diagnosis, demonstrating how veterinary embryology can inform human clinical practice, and vice versa.
In his original description of the syndrome, Cantrell emphasized a supraumbilical midline defect as a defining hallmark, reflecting a specific embryologic failure of the ventral body wall during early thoracoabdominal development [1]. However, as more human cases were documented, clinicians and researchers recognized that the range of midline abnormalities was broader than initially proposed (Table 5, Table 6 and Table 7). Additional defects, some of which were umbilical or variably positioned along the midline, were gradually accepted as part of the syndrome’s phenotypic range (Table 4). Recently, some authors have included lateral body wall defects despite their distinct embryologic origins and later timing in embryonic development (Table 9). This raises questions about whether these anomalies arise from the same pathogenic mechanism. The inclusion of body stalk anomalies, particularly when the umbilical cord is malformed or absent, further complicates matters, as these defects stem from an even earlier and more global disruption of embryonic folding. Taken together, the expanding list of associated defects suggests that what has been grouped under “Cantrell syndrome” may actually represent multiple developmental processes with overlapping but not identical pathways, rather than a single, unified entity. Therefore, it may be time to reconsider the classification and distinguish these processes more clearly to improve diagnostic precision and better understand the underlying embryologic mechanisms.Nevertheless, limitations must be acknowledged. The number of documented veterinary cases is relatively small compared to human reports, and species-specific embryological differences may prevent direct extrapolation. The retrospective nature of case analysis introduces variability in diagnostic criteria and reporting standards. These challenges underscore the necessity of prospective, standardized studies in both veterinary and human medicine to validate the proposed comparative framework. Despite these limitations, using animal models to compare the classification of Cantrell’s syndrome represents a constructive step forward. It shows how veterinary findings can enrich human medicine, encourages adopting cross-species perspectives in congenital anomaly research, and paves the way for future interdisciplinary studies.
Future research on congenital anomalies should focus on developing a standardized, cross-species classification system for ectopia cordis and related malformations. This system should integrate veterinary and human perspectives to create a unified framework. Strong interdisciplinary collaboration, bringing together veterinarians, physicians, embryologists, and geneticists, is essential for conducting comparative research that transcends species boundaries. Systematically collecting prospective data using standardized diagnostic criteria across human and veterinary medicine will reduce variability and strengthen the reliability of case documentation. Concurrently, embryological research must expand to investigate mesodermal developmental defects as a shared pathogenetic pathway, utilizing animal models to supplement human studies. Integrating these efforts into the One Health framework emphasizes congenital anomalies as a shared challenge across species and ensures that rare syndromes benefit from cross-species insights. Ultimately, translating these comparative findings into clinical applications could lead to improved diagnostic protocols and earlier detection strategies in both human and veterinary medicine, as well as potentially preventive measures.
8. Conclusion
This review shows that CS and other ventral body wall defects are part of a single spectrum of midline developmental disorders caused by disruptions in the ventral mesoderm during early embryogenesis. By integrating 165 human cases with comparative data from dogs, cats, pigs, and ruminants, we demonstrate that the embryological mechanisms underlying these anomalies are conserved across species despite varying anatomical expression. The human dataset reveals clear stratification of phenotypes based on defect location and umbilical cord morphology. ThAb and abdominoschisis accompanied by cord anomalies represent the most severe body-stalk-associated forms. Carnivores closely mirror this distribution, while pigs consistently express an extreme, uniform phenotype that aligns with complete CS and high-order BSA types. In contrast, ruminants exhibit a distinct cranial pattern dominated by cervical and cervicothoracic ectopia cordis, which highlights species-specific differences in ventral midline vulnerability. Together, these findings underscore the importance of a comparative, cross-species approach to understanding the embryological origins and phenotypic variability of Cantrell-related anomalies. Veterinary models, particularly the canine ectopia cordis classification and the porcine BSA system, provide powerful tools for refining human diagnoses and clarifying the developmental pathways involved. This One Health approach emphasizes that congenital ventral body wall defects are not limited to human medicine, but rather reflect shared biological processes across mammals. Future progress will depend on standardized, prospective data collection and deeper interdisciplinary collaboration among clinicians, veterinarians, embryologists, and geneticists. These efforts will improve diagnostic accuracy, enable earlier detection, and ultimately enhance outcomes for individuals affected by these rare yet clinically significant malformations.
Author Contributions
Conceptualization, N.M.A. and L.A.; methodology, N.M.A. and L.A.; validation, N.M.A. and L.A.; formal analysis, N.M.A. and L.A.; investigation, N.M.A. and L.A.; resources, N.M.A. and L.A.; writing—original draft preparation, N.M.A.; writing—review and editing, N.M.A.; visualization, N.M.A. and L.A.; supervision, N.M.A.; All authors have read and agreed to the published version of the manuscript.
Funding
Please add: This research received no external funding.
Institutional Review Board Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AA | Anal atresia |
| AAA | Aplasia of the aortic arch |
| AADT | Aortic arch dog type |
| AAH | Anterior abdominal hernia |
| Ab | Abdominoschisis |
| AbEC | Abdominal ectopia cordis |
| ABS | Amniotic band syndrome |
| ACP | Abnormal coiling pattern |
| AE | Adrenal ectopia |
| AH | Alobar holoprosencephaly |
| AMV | Atresia of the mitral valve |
| AN | Anencephaly |
| ASD | Atrial septal defect |
| AOP | Anophthalmia |
| APVR | Anomalous pulmonary venous return |
| AvC | Atrioventricular canal |
| AVS | Aortic valve stenosis |
| BAV | Bicuspid aortic valve |
| BCh | Bilateral cheiloschisis |
| BG | Bilobed gallbladder |
| BvD | Biventricular diverticulum |
| BvH | Biventricular hypertrophy |
| BWD | Body wall defect |
| CA | Cerebellar aplasia |
| CAWD | Cranioventral abdominal wall defect |
| Cch | Cranioschisis |
| CD | Cardiac defect |
| CDH | Congenital diaphragmatic hernia |
| Cf | Calf |
| CH | Cerebellar hypoplasia |
| CHD | Congenital heart disease |
| CHt | Cardiac heterotaxia |
| CL | Cleft lip |
| CM | Cardiomegaly |
| CoA | Coarctation of the aorta |
| CP | Cleft palate |
| Crch | Craniorachischisis |
| CrfD | Craniofacial dysmorphism |
| CS | Cantrell syndrome |
| CSq | Cantrell sequence |
| CSt | Colonic stenosis |
| Ct | Cat |
| CtD | Costal defect |
| CVCD | Cranial vena cava duplicated |
| CyH | Cystic hygroma |
| D | Dog |
| DA | Dextroposition of the aorta |
| DbA | Double apex |
| Dc | Dextrocardia |
| DD | Diaphragmatic defect |
| Di | Distorted at the umbilicus |
| DILV | Double-inlet left ventricle |
| DORV | Double-outlet right ventricle |
| DRM | Diastasis of the abdominal recti muscles |
| DTV | Dysplasia of the tricuspid valve |
| DUV | Dispersed umbilical vessels |
| EC | Ectopia cordis |
| Ecc | Encephalocele |
| EcC | Ectopic caecum |
| EcL | Ectopic liver |
| Ect | Ectrodactyly |
| Ee | Exencephaly |
| EH | Epigastric hernia |
| Ep | Epignathus |
| ExEC | External ectopia cordis |
| FK | Fibrotic kidneys |
| G | Gastrochisis |
| GA | Gallbladder agenesis |
| GEH | Grossly enlarged heart |
| GH | Globular heart |
| H | Hydrocephaly |
| HAs | Hypoplastic auricles |
| HCy | Hepatic cyst |
| HD | Hepatic defect |
| HF | Hepatic fibrosis |
| HHS | Hyperplastic and hard spleen |
| HLHS | Hypoplastic left heart syndrome |
| HLV | Hypoplasia of the left ventricle |
| HRVS | Hypoplastic right ventricle syndrome |
| HR | Hypoplastic ribs |
| HT | Hypertelorism |
| HUA | Hypoplastic umbilical artery |
| Hy | Hydramnios |
| ICD | Intracardiac defect |
| IDBK | Increased distance between the kidneys and the adrenal glands |
| IM | Intestinal malrotation |
| Lm | Lamb |
| L | Left |
| LAb | Lateral abdominoschisis |
| LAM | Liver amorphous mass without lobulation |
| LSVC to CS | Left superior vena cava draining to coronary sinus |
| L-SE | Low-set ears |
| LThAb | Lateral thoracoabdominoschisis |
| LVA | Left ventricular aneurysm |
| LVD | Left ventricular diverticulum |
| Mc | Mesocardia |
| MD | Musculoskeletical deformities |
| MOP | Microphthalmia |
| MVA | Mitral valve agenesis |
| MVS | Mitral valve stenosis |
| Myc | Myelomeningocele |
| NR | Non reported |
| NS | Non studied |
| NSt-GuD, | Non structural genitourinary defects |
| NSt-LD | Non structural limb defect |
| NSt-SpD | Non structural spinal defect |
| O | Omphalocele |
| OD | Other defects |
| OmT | Oromandiular tumor |
| ONTD | Open neural tube defect |
| P | Pig |
| PAA | Pulmonary artery atresia |
| PAH | Pulmonary artery hypoplasia |
| PCD | Pulmonary congenital defect |
| PD | Pericardial defect |
| PDA | Patent ductus arteriosus |
| PLSVC | Persistent left superior vena cava |
| PLCVC | Persistent left cranial vena cava |
| PP | Primary palatoschisis |
| PPDH | Peritoneo-pericardial diaphragmatic hernia |
| Ps | Polisplenia |
| PS | Pulmonary stenosis |
| PSDH | Pars sternalis diaphragmatic hernia |
| PTA | Persistent truncus arteriosus |
| R | Right |
| RAV | Right azygos vein |
| RD | Rectal diastasis |
| RVD | Right ventricular dilatation |
| RVH | Right ventricular hipertrofy |
| SA | Single atrium |
| Sc | Supercoiled |
| SCA | Single coronary artery |
| SIL | Situs inversus of the liver |
| SL | Split liver |
| SP | Secondary palatoschisis |
| SPV | Single pulmonary vein |
| SS | Situs solitus |
| St-GuD | Structural genitourinary defects |
| St-LD | Structural limb defect |
| St-SpD | Structural spinal defect |
| StD | Sternal defect |
| SUA | Single umbilical artery |
| SUAb | Supra-umbilical-abdominoschisis |
| SUICD | Supraumbilical incomplete central defect |
| SUThAb | Supra-umbilical-thoraco-abdominoschisis |
| SV | Single ventricle |
| TA | Tricuspid atresia |
| TF | Tetralogy of Fallot |
| TGA | Transposition of the great arteries |
| Th | Thoracoschisis |
| ThAb | Thoracoabdominoschisis |
| ThAbEC | Thoraco-abdominal ectopia cordis |
| ThG | Thoracogastroschisis |
| TRAPS | Twin reversed arterial perfusion sequence |
| TVD | Tricuspid valve dysplasia |
| U | Unilateral |
| Uc | Uncoiled |
| UCD | Umbilical cord defect |
| UH | Umbilical hernia |
| URC | Unroofed coronary sinus |
| VAD | Vena azygos duplicated |
| VD | Ventricular diverticulum |
| VEH | Ventral epigastric hernia |
| VH | Ventral hernia |
| VSD | Ventricular septal defect |
References
- Cantrell, J.R.; Haller, J.A.; Ravitch, M.M. A syndrome of congenital defects involving the abdominal wall, sternum, diaphragm, pericardium, and heart. Surg Gynecol Obstet 1958, 107, 602–614. [Google Scholar]
- Hori, A.; Roessmann, U.; Eubel, R.; Ulbrich, R.; Dietrich-Schott, B. Exencephaly in Cantrell-Haller-Ravitsch Syndrome. Acta Neuropathol (Berl) 1984, 65, 158–162. [Google Scholar] [CrossRef]
- Zachariou, Z; Daum, R; Roth, H; Benz, G. Das Cantrellsche Syndrom [Cantrell’s syndrome]. Z Kinderchir 1987, 42, 255–259. [Google Scholar] [CrossRef] [PubMed]
- Milne, L.W.; Morosin, A.M.; Campbell, J.R.; Harrison, M.W. Pars sternalis diaphragmatic hernia with omphalocele: a report of two cases. J Pediatr Surg 1990, 25, 726–730. [Google Scholar] [CrossRef]
- Achiron, R.; Schimmel, M.; Farber, B.; Glaser, J. Prenatal sonographic diagnosis and perinatal management of ectopia cordis. Ultrasound Obstet Gynecol 1991, 1, 431–434. [Google Scholar] [CrossRef] [PubMed]
- Peer, D.; Moroder, W.; Delucca, A. Pränatale Diagnose einer Cantrellschen Pentalogie kombiniert mit Exenzephalie und Amnionbridensyndrom [Prenatal diagnosis of the pentalogy of Cantrell combined with exencephaly and amniotic band syndrome]. Ultraschall Med 1993, 14, 94–95. [Google Scholar] [CrossRef] [PubMed]
- Abdallah, H.I.; Marks, L.A.; Balsara, R.K.; Davis, D.A.; Russo, P.A. Staged repair of pentalogy of Cantrell with tetralogy of Fallot. Ann Thorac Surg 1993, 56, 979–980. [Google Scholar] [CrossRef]
- Bogers, A.J.; Hazebroek, F.W.; Hess, J. Left and right ventricular diverticula, ventricular septal defect and ectopia cordis in a patient with Cantrell’s syndrome. Eur J Cardiothorac Surg 1993, 7, 334–335. [Google Scholar] [CrossRef]
- Dembinski, J.; Heyl, W.; Steidel, K.; Hermanns, B.; Hörnchen, H.; Schröder, W. The Cantrell-sequence: a result of maternal exposure to aminopropionitriles? Am J Perinatol 1997, 14, 567–571. [Google Scholar] [CrossRef]
- Fernández, M.S.; López, A.; Vila, J.J.; Lluna, J.; Miranda, J. Cantrell’s pentalogy. Report of four cases and their management. Pediatr Surg Int 1997, 12, 428–431. [Google Scholar] [CrossRef]
- Vazquez-Jimenez, J.F.; Muehler, E.G.; Daebritz, S.; Keutel, J.; Nishigaki, K.; Huegel, W.; Messmer, B.J. Cantrell’s syndrome: a challenge to the surgeon. Ann Thorac Surg 1998, 65, 1178–1185. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.Y.; Lee, C.C.; Chang, C.C.; Tsai, H.D.; Hsu, T.Y.; Tsai, C.H. Prenatal sonographic diagnosis of Cantrell’s pentalogy with cystic hygroma in the first trimester. J Clin Ultrasound 1998, 26, 409–412. [Google Scholar] [CrossRef]
- Katranci, A.O.; Semih Görk, A.; Rizalar, R.; Giinaydin, M.; Aritiirk, E.; Bernay, F.; Gürses, N. Pentalogy of Cantrell. Indian J Pediatr 1998, 65, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Laloyaux, P.; Veyckemans, F.; Van Dyck, M. Anaesthetic management of a prematurely born infant with Cantrell’s Pentalogy. Paediatric Anaesthesis 1998, 8, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Pivnick, E.K.; Kaufman, R.A.; Velagaleti, G.V.; Gunther, W.M.; Abramovici, D. Infant with midline thoracoabdominal schisis and limb defects. Teratology 1998, 58, 205–208. [Google Scholar] [CrossRef]
- Song, A.; McLeary, M.S. MR imaging of pentalogy of Cantrell variant with an intact diaphragm and pericardium. Pediatr Radiol 2000, 30, 638–639. [Google Scholar] [CrossRef]
- Falcao, J.L.; Falcao, S.N.; Sawicki, W.C.; Liberatori, A.W.; Lopes, A.C. Cantrell syndrome. Case report of an adult. Arq Bras Cardiol 2000, 75, 323–328. [Google Scholar] [CrossRef]
- Alayunt, A.; Yagdi, T.; Alat, I.; Posacioglu, H.; Büket, S. Left ventricular diverticulum associated with Cantrell’s syndrome and tetralogy of Fallot in an adult. Scand Cardiovasc J 2001, 35, 55–57. [Google Scholar] [CrossRef]
- Halbertsma, F.J.; van Oort, A.; van der Staak, F. Cardiac diverticulum and omphalocele: Cantrell’s pentalogy or syndrome. Cardiol Young 2002, 12, 71–74. [Google Scholar] [CrossRef]
- León, G.; Chedraui, P.; San Miguel, G. Prenatal diagnosis of Cantrell’s pentalogy with conventional and three-dimensional sonography. J Matern Fetal Neonatal Med 2002, 12, 209–211. [Google Scholar] [CrossRef]
- Davies, B.R.; Duran, M. The confused identity of Cantrell’s pentad: ectopia cordis is related either to thoracoschisis or to a diaphragmatic hernia with an omphalocele. Pediatr Pathol Mol Med 2003, 22, 383–390. [Google Scholar]
- Nanda, S.; Nanda, S.; Agarwal, U.; Sen, J.; Sangwan, K. Cantrell’s syndrome - report of two cases with one atypical variant. Arch Gynecol Obstet 2003, 268, 331–332. [Google Scholar] [CrossRef] [PubMed]
- Bittmann, S.; Ulus, H.; Springer, A. Combined pentalogy of Cantrell with tetralogy of Fallot, gallbladder agenesis, and polysplenia: a case report. J Pediatr Surg 2004, 39, 107–109. [Google Scholar] [CrossRef] [PubMed]
- Uygur, D.; Kiş, S.; Sener, E.; Günçe, S.; Semerci, N. An infant with pentalogy of Cantrell and limb defects diagnosed prenatally. Clin Dysmorphol 2004, 13, 57–58. [Google Scholar] [CrossRef] [PubMed]
- Di Bernardo, S.; Sekarski, N.; Meijboom, E. Left ventricular diverticulum in a neonate with Cantrell syndrome. Heart 2004, 90, 1320. [Google Scholar] [CrossRef]
- Polat, I.; Gül, A.; Aslan, H.; Cebeci, A.; Ozseker, B.; Caglar, B.; Ceylan, Y. Prenatal diagnosis of pentalogy of Cantrell in three cases, two with craniorachischisis. J Clin Ultrasound 2005, 33, 308–311. [Google Scholar] [CrossRef]
- Staboulidou, I.; Wüstemann, M.; Schmidt, P.; Günter, H.H.; Scharf, A. Erhöhte fetale Nackentransparenz als Prädiktor für eine Cantrellsche,Pentalogie – eine Kasuistik. Z Geburtsh Neonatol 2005, 209–234. [Google Scholar] [CrossRef]
- Araujo Júnior, E.; Zanforlin Filho, S.M.; Guimarães Filho, H.A.; Pires, C.R.; Nardozza, L.M.; Moron, A.F. Diagnosis of Pentalogy of Cantrell by three-dimensional ultrasound in third trimester of pregnancy. A case report. Fetal Diagn Ther 2006, 21, 544–547. [Google Scholar] [CrossRef]
- St Louis, J.D. Pentalogy of Cantrell associated with hypoplastic left heart syndrome and herniation of the ventricular mass into the abdominal cavity. Interact Cardiovasc Thorac Surg. 2006, 5, 200–201. [Google Scholar] [CrossRef]
- Knirsch, W.; Dodge-Khatami, A.; Bolz, D.; Valsangiacomo Büchel, E. Cantrell’s Syndrome forme fruste in a newborn diagnosed by transthoracic echocardiography and cardiac magnetic resonance imaging. Pediatr Cardiol 2006, 27, 652–654. [Google Scholar] [CrossRef]
- Marijon, E.; Hausse-Mocumbi, A.O.; Ferreira, B. Cantrell’s syndrome. Cardiol Young 2006, 16, 95–96. [Google Scholar] [CrossRef]
- Grethel, E.J.; Hornberger, L.K.; Farmer, D.L. Prenatal and postnatal management of a patient with pentalogy of Cantrell and left ventricular aneurysm. A case report and literature review. Fetal Diagn Ther 2007, 22, 269–273. [Google Scholar] [CrossRef] [PubMed]
- Wheeler, D.S.; St Louis, J.D. Pentalogy of Cantrell associated with hypoplastic left heart syndrome. Pediatr Cardiol 2007, 28, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Loureiro, T.; Oliveira, C.; Aroso, J.; Ferreira, M.J.; Vieira, J. Prenatal sonographic diagnosis of a rare Cantrell’s pentalogy variant with associated open neural tube defect - a case report. Fetal Diagn Ther 2007, 22, 172–174. [Google Scholar] [CrossRef]
- Korver, A.M.; Haas, F.; Freund, M.W.; Strengers, J.L. Pentalogy of Cantrell: successful early correction. Pediatr Cardiol 2008, 29, 146–149. [Google Scholar] [CrossRef] [PubMed]
- Chelli, D.; Dimassi, K.; Jallouli-Bouzguenda, S.; Ebdellah, E.; Hermi, F.; Zouaoui, B.; Sfar, E.; Kitova, T.; Chelli, H.; Channoufi, M.B.; Gaigi, S. Prenatal diagnosis of ectopia cordis: case report. Tunis Med 2008, 86, 171–173. [Google Scholar]
- Okamoto, Y.; Harada, Y.; Uchita, S. Fontan operation through a right lateral thoracotomy to treat Cantrell syndrome with severe ectopia cordis. Interact Cardiovasc Thorac Surg 2008, 7, 278–279. [Google Scholar] [CrossRef]
- Marcì, M.; Ajovalasit, P.; Calvaruso, D.; Cipriani, A.; Lucente, M.; Petrucelli, D.; Marcelletti, C.F. Double-outlet right ventricle in a neonate with Cantrell’s syndrome. J Cardiovasc Med (Hagerstown) 2008, 9, 506–507. [Google Scholar] [CrossRef]
- Hou, Y.J.; Chen, F.L.; Ng, Y.Y.; Hu, J.M.; Chen, S.J.; Chen, J.Y.; Su, P.H. Trisomy 18 syndrome with incomplete Cantrell syndrome. Pediatr Neonatol 2008, 49, 84–87. [Google Scholar] [CrossRef]
- Turbendian, H.K.; Carroll, S.J.; Chen, J.M. Repair of left ventricular diverticulum in setting of Cantrell’s syndrome. Cardiol Young 2008, 18, 532–533. [Google Scholar] [CrossRef]
- Zidere, V.; Allan, L.D. Changing findings in pentalogy of Cantrell in fetal life. Ultrasound Obstet Gynecol 2008, 32, 835–387. [Google Scholar] [CrossRef]
- Chen, C.P.; Tzen, C.Y.; Chen, C.Y.; Tsai, F.J.; Wang, W. Concomitant exencephaly and limb defects associated with pentalogy of Cantrell. Taiwan J Obstet Gynecol 2008, 47, 476–477. [Google Scholar] [CrossRef]
- Gao, Z.; Duan, Q.J.; Zhang, Z.W.; Ying, L.Y.; Ma, L.L. Images in cardiovascular medicine: Pentalogy of Cantrell associated with thoracoabdominal ectopia cordis. Circulation 2009, 119, e483-5. [Google Scholar] [CrossRef] [PubMed]
- Mitsukawa, N.; Yasunaga, H.; Tananari, Y. Chest wall reconstruction in a patient with Cantrell syndrome. J Plast Reconstr Aesthet Surg 2009, 62, 814–818. [Google Scholar] [CrossRef]
- Meeker, T.M. Pentalogy of Cantrell: reviewing the syndrome with a case report and nursing implications. J Perinat Neonatal Nurs 2009, 23, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Suehiro, K.; Okutani, R.; Ogawa, S.; Nakada, K.; Shimaoka, H.; Ueda, M.; Shigemoto, T. Perioperative management of a neonate with Cantrell syndrome. J Anesth 2009, 23, 572–575. [Google Scholar] [CrossRef]
- Sowande, O.A.; Anyanwu, L.J.; Talabi, A.O.; Babalola, O.R.; Adejuyigbe, O. Pentalogy of cantrell: a report of three cases. J Surg Tech Case Rep 2010, 2, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Herman, T.E.; Siegel, M.J. Cantrell syndrome. J Perinatol 2010, 30, 298–299. [Google Scholar] [CrossRef]
- Singh, N.; Bera, M.L.; Sachdev, M.S.; Aggarwal, N.; Joshi, R.; Kohli, V. Pentalogy of Cantrell with left ventricular diverticulum: a case report and review of literature. Congenit Heart Dis 2010, 5, 454–457. [Google Scholar] [CrossRef]
- Quandt, D.; Dave, H.; Valsangiacomo Buechel, E. Heart with a trunk: form fruste of Cantrell’s Syndrome. Eur Heart J 2011, 32, 123. [Google Scholar] [CrossRef]
- Angoulvant, D.; Sanchez, I.; Boussel, L. Late diagnosis of incomplete Cantrell’s syndrome on CT scan. Arch Cardiovasc Dis 2011, 104, 208–210. [Google Scholar] [CrossRef]
- Balderrábano-Saucedo, N.; Vizcaíno-Alarcón, A.; Sandoval-Serrano, E.; Segura-Stanford, B.; Arévalo-Salas, L.A.; de la Cruz, L.R.; Espinosa-Islas, G.; Puga-Muñuzuri, F.J. Pentalogy of Cantrell: Forty-two Years of Experience in the Hospital Infantil de Mexico Federico Gomez. World J Pediatr Congenit Heart Surg 2011, 2, 211–218. [Google Scholar] [CrossRef]
- Smigiel, R.; Jakubiak, A.; Lombardi, M.P.; Jaworski, W.; Slezak, R.; Patkowski, D.; Hennekam, R.C. Co-occurrence of severe Goltz-Gorlin syndrome and pentalogy of Cantrell - Case report and review of the literature. Am J Med Genet A 2011, 155A, 1102–1105. [Google Scholar] [CrossRef] [PubMed]
- Wen, L.; Jun-lin, L.; Jia, H.; Dong, Z.; Li-guang, Z.; Shu-hua, D.; Wei-jin, L.; Yun-hua, G. Cantrell syndrome with complex cardiac malformations: a case report. J Pediatr Surg 2011, 46, 1455–1458. [Google Scholar] [CrossRef] [PubMed]
- Brochut, A.C.; Baumann, M.U.; Kuhn, A.; Di; Naro, E; Tutschek, B.; Surbek, D.; Raio, L. Pentalogy or hexalogy of Cantrell? Pediatr Dev Pathol 2011, 14, 396–401. [Google Scholar] [CrossRef]
- Ranganath, P.; Pradhan, M. Complete Pentalogy of Cantrell with craniorachischisis: a case report. J Prenat Med 2012, 6, 10–12. [Google Scholar] [PubMed]
- Sakasai, Y.; Thang, B.Q.; Kanemoto, S.; Takahashi-Igari, M.; Togashi, S.; Kato, H.; Hiramatsu, Y. Staged repair of pentalogy of Cantrell with ectopia cordis and ventricular septal defect. J Card Surg 2012, 27, 390–392. [Google Scholar] [CrossRef]
- Ergenoğlu, M.A.; Yeniel, A.Ö.; Peker, N.; Kazandı, M.; Akercan, F.; Sağol, S. Prenatal diagnosis of Cantrell pentalogy in first trimester screening: case report and review of literature. J Turk Ger Gynecol Assoc 2012, 13, 145–148. [Google Scholar] [CrossRef]
- Kinoshita, M.; Park, S.; Shiraishi, T.; Ueno, S. Thoracoabdominoplasty with umbilicoplasty for Cantrell’s syndrome. J Plast Surg Hand Surg 2012, 46, 367–370. [Google Scholar] [CrossRef]
- El Kouache, M.; Labib, S.; El Madi, A.; Babakhoya, A.; Atmani, S.; Abouabdilah, Y.; Harandou, M. Left Ventricle Diverticulum with Partial Cantrell’s Syndrome. Case Rep Cardiol 2012, 2012, 309576. [Google Scholar] [CrossRef]
- Chandran, S.; Ari, D. Pentalogy of Cantrell: an extremely rare congenital anomaly. J Clin Neonatol 2013, 2, 95–97. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.P.; Huang, M.C.; Chern, S.R.; Wu, P.S.; Su, J.W.; Wang, W. Discordant anencephaly and Cantrell syndrome in monozygotic twins conceived by ICSI and IVF-ET. Taiwan J Obstet Gynecol 2013, 52, 297–299. [Google Scholar] [CrossRef] [PubMed]
- Magadum, S.; Shivaprasad, H.; Dinesh, K.; Vijay, K. Incomplete Cantrell’s Pentalogy-A Case Report. Indian J Surg 2013, 75 Suppl 1, 350–352. [Google Scholar] [CrossRef]
- Kachare, M.B.; Patki, V.K.; Saboo, S.S.; Saboo, S.H.; Ahlawat, K.; Saboo, S.S. Pentalogy of Cantrell associated with exencephaly and spinal dysraphism: antenatal ultrasonographic diagnosis. Case report. Med Ultrason 2013, 15, 237–239. [Google Scholar] [CrossRef]
- Ito, H.; Ota, N.; Murata, M.; Sakamoto, K. Fontan operation for the Cantrell syndrome using a clamshell incision. Interact Cardiovasc Thorac Surg 2013, 17, 754–756. [Google Scholar] [CrossRef]
- Puvabanditsin, S.; Di Stefano, V.; Garrow, E.; Wong, R.; Eng, J.; Balbin, J. Case Report Ectopia cordis, Hong Kong. Med J 2013, 19, 447–450. [Google Scholar] [CrossRef]
- Kaouthar, H.; Jihen, A.; Faten, J.; Hela, M.; Fatma, O.; Lilia, C.; Rafik, B. Cardiac anomalies in Cantrell’s pentalogy: From ventricular diverticulum to complete thoracic ectopia cordis. Cardiol Tunis 2013, 9, 94–97. [Google Scholar] [PubMed]
- Cakiroglu, Y.; Doger, E.; Yildirim Kopuk, S.; Babaoglu, K.; Caliskan, E.; Yucesoy, G. Prenatal Diagnosis of Cantrell’s Pentalogy Associated with Agenesis of Left Limb in a Twin Pregnancy. Case Rep Obstet Gynecol 2014, 2014, 314284. [Google Scholar] [CrossRef]
- Kheir, A.E.M.; Bakhiet, E.A.; Elhag Karrar, M.Z. Pentalogy of Cantrell: case report and review of the literature. Sudan J Paediatr 2014, 14, 85–88. [Google Scholar]
- Restrepo, M.S.; Cerqua, A.; Turek, J.W. Pentalogy of Cantrell with ectopia cordis totalis, total anomalous pulmonary venous connection, and tetralogy of Fallot: a case report and review of the literature. Congenit Heart Dis 2014, 9, E129-34. [Google Scholar] [CrossRef]
- Zhang, X.; Xing, Q.; Sun, J.; Hou, X.; Kuang, M.; Zhang, G. Surgical treatment and outcomes of pentalogy of Cantrell in eight patients. J Pediatr Surg 2014, 49, 1335–1340. [Google Scholar] [CrossRef] [PubMed]
- Pirasteh, A.; Carcano, C.; Kirsch, J.; Mohammed, T.L. Pentalogy of Cantrell with Ectopia Cordis: CT Findings. J Radiol Case Rep 2014, 8, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Naburi, H.; Assenga, E.; Patel, S.; Massawe, A.; Manji, K. Class II pentalogy of Cantrell. BMC Res Notes 2015, 8, 318. [Google Scholar] [CrossRef] [PubMed]
- Timur, H.; Tokmak, A.; Bayram, H.; Şükran Çakar, E.; Danışman, N. Coincidence of Incomplete Pentalogy of Cantrell and Meningomyelocele in a Dizygotic Twin Pregnancy. Case Rep Obstet Gynecol 2015, 2015, 629561. [Google Scholar] [CrossRef]
- Türkçapar, A.F.; Sargın Oruc, A.; Öksüzoglu, A.; Danışman, N. Diagnosis of pentalogy of cantrell in the first trimester using transvaginal sonography and color Doppler. Case Rep Obstet Gynecol 2015, 2015, 179298. [Google Scholar] [CrossRef]
- Madžarac, V.; Matijević, R.; Škrtić, A.; Duić, Ž.; Fistonić, N.; Partlm, J.Z. Pentalogy of Cantrell with Unilateral Kidney Evisceration: A Case Report and Review of Literature. Fetal Pediatr Pathol 2016, 35, 43–49. [Google Scholar] [CrossRef]
- Yang, Y.; Jiang, Z.; Ding, F. One-stage surgical treatment for Cantrell syndrome without repairing the left ventricular diverticulum: a case report. Cardiol Young 2016, 26, 191–193. [Google Scholar] [CrossRef]
- Meena, R.; Meena, V. Pentalogy of Cantrell with single umbilical artery: a rare fetal anomaly. Int J Contemp Pediatr 2016, 4, 280–282. [Google Scholar] [CrossRef]
- Zani-Ruttenstock, E.; Zani, A.; Honjo, O.; Chiu, P. Pentalogy of Cantrell: Is Echocardiography Sufficient in the Neonatal Period? European J Pediatr Surg Rep 2017, 5, e9–e11. [Google Scholar] [CrossRef]
- Pius, S.; Abubakar Ibrahim, H.; Bello, M.; Bashir Tahir, M. Complete Ectopia Cordis: A Case Report and Literature Review. Case Rep Pediatr 2017, 2017, 1858621. [Google Scholar] [CrossRef]
- Salinas-Torres, V.M.; De La O-Espinoza, E.A.; Salinas-Torres, R.A. Severe Intrauterine Amputations in One Dichorionic Twin With Pentalogy of Cantrell: Further Evidence and Consideration for Mechanical Teratogenesis. Pediatr Dev Pathol 2017, 20, 440–443. [Google Scholar] [CrossRef]
- Swarray-Deen, A.; Seffah, J.D.; Antwi-Agyei, D.A. Two cases of Pentalogy of Cantrell diagnosed antenatally at Korle Bu Teaching Hospital, Accra. Ghana Med J 2017, 51, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Mărginean, C.; Mărginean, C.O.; Gozar, L.; Meliţ, L.E.; Suciu, H.; Gozar, H.; Crişan, A.; Cucerea, M. Cantrell Syndrome-A Rare Complex Congenital Anomaly: A Case Report and Literature Review. Front Pediatr 2018, 6, 201. [Google Scholar] [CrossRef] [PubMed]
- Grigore, M.; Furnica, C.; Esanu, I.; Gafitanu, D. Pentalogy of Cantrell associated with unilateral anophthalmia: Case report and literature review. Medicine (Baltimore) 2018, 97(31), e11511. [Google Scholar] [CrossRef]
- Hubbard, R.; Hayes, S.; Gillis, H.; Lindsey, S.; Malhotra, P.; Wani, T.; Tobias, J.D.; Beltran, R. Management challenges in an infant with Pentalogy of Cantrell, giant anterior encephalocele, and craniofacial anomalies: A Case Report. A A Pract 2018, 11, 238–240. [Google Scholar] [CrossRef]
- Madi, J.M.; Festugatto, J.R.; Rizzon, M.; Agostini, A.P.; Araújo, B.F.; Garcia, R.M.R. Ectopia Cordis Associated with Pentalogy of Cantrell-A Case Report. Rev Bras Ginecol Obstet 2019, 41, 352–356. [Google Scholar] [CrossRef] [PubMed]
- Delgado, A. L.; Matongo, K. M.; Dumo, B.; Mzayiya, N.; Mrara, B. Pentalogy of Cantrell with Total Ectopia Cordis and a Major Omphalocele—A Case Report. J Pharm Pharmacol 2019, 7, 621–622. [Google Scholar] [CrossRef]
- Kylat, R.I. Complete and Incomplete Pentalogy of Cantrell. Children (Basel) 2019, 6(10), 109. [Google Scholar] [CrossRef]
- Diaz-Serani, R.; Sepulveda, W. Trisomy 18 in a First-Trimester Fetus with Thoraco-Abdominal Ectopia Cordis. Fetal Pediatr Pathol 2020, 39, 78–84. [Google Scholar] [CrossRef]
- Zvizdic, Z.; Sefic-Pasic, I.; Mesic, A.; Terzic, S.; Vranic, S. The complete spectrum of pentalogy of Cantrell in one of a set of dizygotic twins: A case report of a rare congenital anomaly. Medicine (Baltimore). 2021, 100, e25470. [Google Scholar] [CrossRef]
- Desikan, S.; Coumary, A. S.; Habeebullah, S. Pentalogy of Cantrell with encephalocele – A case report with review of literature. Indian J Obstet Gynecol Res 2021, 8, 275–278. [Google Scholar] [CrossRef]
- Shrestha, N. A Baby Born with Ectopia Cordis, Omphalocele, Cleft Lips and Palate: A Case Report. JNMA J Nepal Med Assoc 2022, 60, 183–186. [Google Scholar] [CrossRef]
- Sulistyowati, R.; Sensusiati, A.D. Radiological findings of partial expression pentalogy of Cantrell and other multiple congenital anomalies: A rare case report. Radiol Case Rep 2022, 17, 3172–3178. [Google Scholar] [CrossRef]
- Fazea, M.; Alhameli, M.; Ahmed, F.; Askarpour, M.R; Murshed, W.; Jarwsh, A.; Alkbous, A. Pentalogy of Cantrell Associated with Ectopia Cordis: A Case Report. Pediatric Health Med Ther 2022, 13, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Zheng, B.; Zhai, B.; Mo, J.; Yang, K.; Huo, Y. Clinical and ultrasound findings of pentalogy of Cantrell in a newborn: A case report. Front Pediatr 2022, 10, 998495. [Google Scholar] [CrossRef] [PubMed]
- Liao, J.; Huang, H.; Li, X. Surgical treatment of neonatal Cantrell pentalogy: a case report and literature review. AME Case Rep 2023, 7, 22. [Google Scholar] [CrossRef] [PubMed]
- Mraihi, F.; Basly, J.; Mezni, A.; Ghali, Z.; Hafsi, M.; Chelli, D. The pentalogy of Cantrell: A rare and challenging prenatal diagnosis. Int J Surg Case Rep 2023, 112, 108941. [Google Scholar] [CrossRef]
- Faisal, N.; Jeyakumar, P.; Pandey, N.N.; Choudhary, S.K.; Reddy, P.R.; Ramakrishnan, S. Pulsating abdominal mass in a newborn - Pentalogy of Cantrell with left ventricular diverticulum. Ann Pediatr Cardiol 2023, 16, 475–477. [Google Scholar] [CrossRef]
- Fabijan, A.; Korabiewska-Pluta, S.; Puzio, T.; Polis, B.; Moszura, T. Images of Extremely Rare Cantrell Phenomenon. Diagnostics (Basel). 2024, 14, 1003. [Google Scholar] [CrossRef]
- Garofalo, S.; Guanà, R.; Suteu, L.; Alhellani, H.; Cortese, M.G.; Lonati, L.; Gennari, F. Epignathus and thoracoabdominal ectopia cordis in a neonate. Pediatr Neonatol 2024, 65, 410–411. [Google Scholar] [CrossRef]
- Dusuri, E.; Asante, C.G.; Gyamfi, B.A.; Nartey, E.T.; Amaning, O.A.; Arkorful, J. Complete pentalogy of Cantrell associated with ectopia cordis and multiple anomalies: A case report from a low-resource setting. Radiol Case Rep 2025, 20, 1948–1952. [Google Scholar] [CrossRef]
- Maheshwari, V.; Sahoo, M. Anesthesia for Pentalogy of Cantrell with Surgical Repair of Tetralogy of Fallot Along with Absent Diaphragm: A Case Study. Ann Card Anaesth 2025, 28, 181–183. [Google Scholar] [CrossRef] [PubMed]
- Martadiansyah, A.; Bernolian, N.; Mirani, P.; Lestari, P.M.; Nugraha, A.; Stevanny, B. Complex management of ectopia cordis complicated by pentalogy of cantrell: Report of two cases and review of current evidence. Int J Surg Case Rep 2025, 131, 111353. [Google Scholar] [CrossRef]
- Cozar, J.M.; Avedillo, L.; Martín-Alguacil, N. Embryonic Disruption Syndromes in Dogs: Exploring the Overlap and Divergence of Cantrell Syndrome, Amniotic Bands, and Body Stalk Anomalies. Preprint.org 2025. [Google Scholar] [CrossRef]
- Martín-Alguacil, N.; Avedillo, L. Cantrell Syndrome (Thoracoabdominal Ectopia Cordis; Anomalous Umbilical Cord; Diaphragmatic, Pericardial and Intracardiac Defects) in the Pig (Sus scrofa domesticus). J Comp Pathol 2020, 174, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Pechriggl, E.; Blumer, M.; Tubbs, R.S.; Olewnik, Ł.; Konschake, M.; Fortélny, R.; Stofferin, H.; Honis, H.R.; Quinones, S.; Maranillo, E.; Sanudo, J. Embryology of the Abdominal Wall and Associated Malformations-A Review. Front Surg 2022, 9, 891–896. [Google Scholar] [CrossRef]
- Solerte, M.L.; Cosmi, E. Abdominal Wall Defects in Prenatal Medicine. Ann Hematol Oncol 2022, 9(2), 1394. [Google Scholar] [CrossRef]
- So, W.; Donahoe, S.L.; Podadera, J.M.; Mazrier, H. Pentalogy of Cantrell in Two Neonate Littermate Puppies: A Spontaneous Animal Model Suggesting Familial Inheritance. Animals (Basel) 2023, 13, 2091. [Google Scholar] [CrossRef]
- Chuaire Noack, L. New clues to understand gastroschisis. Embryology, pathogenesis and epidemiology. Colomb Med (Cali) 2021, 52(3), e4004227. [Google Scholar] [CrossRef]
- Lammer, E.J.; Iovannisci, D.M.; Tom, L.; Schultz, K.; Shaw, G.M. Gastroschisis: a gene-environment model involving the VEGF-NOS3 pathway. Am J Med Genet C 2008, 148c(3), 213–8. [Google Scholar] [CrossRef]
- Lubinsky, M. A vascular and thrombotic model of gastroschisis. Am J Med Genet A 2014, 164A(4), 915–7. [Google Scholar] [CrossRef] [PubMed]
- Hoyme, H.E.; Jones, M.C.; Jones, K.L. Gastroschisis: abdominal wall disruption secondary to early gestational interruption of the omphalomesenteric artery. Semin Perinatol 1983, 7(4), 294–8. [Google Scholar]
- Stevenson, R.E.; Rogers, R.C.; Chandler, J.C.; Gauderer, M.W.; Hunter, A.G. Escape of the yolk sac: a hypothesis to explain the embryogenesis of gastroschisis. Clin Genet 2009, 75(4), 326–33. [Google Scholar] [CrossRef]
- Martín-Alguacil, N.; Avedillo, L. Body Wall Defects: Gastroschisis and Omphalocoele in Pigs (Sus scrofa domesticus). J Comp Pathol 2020, 175, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Martín-Alguacil, N.; Avedillo, L. Body wall defects and amniotic band syndrome in pig (Sus scrofa domesticus). Anat Histol Embryol 2020, 49, 144–149. [Google Scholar] [CrossRef]
- Abu-Issa, R.; Kirby, M. Heart field: from mesoderm to heart tube. Ann Rev Cell Devel Biol 2007, 23, 45–68. [Google Scholar] [CrossRef]
- Ma, X.; Adelstein, R.S. A point mutation in Myh10 causes major defects in heart development and body wall closure. Circ Cardiovasc Genet 2014, 7(3), 257–65. [Google Scholar] [CrossRef]
- Takeuchi, K.; Fujita, I.; Nakajima, K.; Kitagaki, S.; Koketsu, I. Body stalk anomaly: prenatal diagnosis. Int J Gynaecol Obstet 1995, 51, 49–52. [Google Scholar] [CrossRef]
- Costa, M.L.; Couto, E.; Furlan, E.; Zaccaria, R.; Andrade, K.; Barini, R.; Nomura, M.L. Body stalk anomaly: adverse maternal outcomes in a series of 21 cases. Prenat Diagn 2012, 32, 264–267. [Google Scholar] [CrossRef]
- Kocherla, K.; Kumari, V.; Kocherla, P. Prenatal diagnosis of body stalk complex: A rare entity and review of literature. Indian J Radiol Imaging 2015, 25, 67–70. [Google Scholar] [CrossRef] [PubMed]
- Gică, N.; Apostol, L.M.; Huluță, I.; Panaitescu, A.M.; Vayna, A.M.; Peltecu, G.; Gana, N. Body Stalk Anomaly. Diagnostics (Basel). 2024, 14(5), 518. [Google Scholar] [CrossRef]
- Martín-Alguacil, N.; Avedillo, L. Body stalk anomalies in pig-Definition and classification. Mol Genet Genomic Med 2020, 8(6), e1227. [Google Scholar] [CrossRef]
- Martín-Alguacil, N. Anatomy-based diagnostic criteria for complex body wall anomalies (CBWA). Mol Genet Genomic Med 2020, 8(10), e1465. [Google Scholar] [CrossRef] [PubMed]
- Martín-Alguacil, N.; Cozar, J.M.; Avedillo, L. Complex Body Wall Closure Defects in Seven Dog Fetuses: An Anatomic and CT Scan Study. Animals (Basel) 2025, 15(14), 2030. [Google Scholar] [CrossRef] [PubMed]
- Martín-Alguacil, N.; Cozar, J.M.; Avedillo, L. Body stalk anomalies and their relationship to amniotic band disruption complex in six cats. J Feline Med Surg 2025, 27(6), 1098612X251341068. [Google Scholar] [CrossRef]
- Martín-Alguacil, N.; Cozar, J.M.; Avedillo, L.J. Body Stalk Anomalies in Pigs: Current Trends and Future Directions in Classification. Animals (Basel) 2025, 15(3), 460. [Google Scholar] [CrossRef]
- Butler, H. C. Repair of Congenital Diaphragmatic Hernia and Umbilical Hernia in a Dog. JAVMA 1960, 136, 559–560. [Google Scholar]
- Bellah, J.R.; Spencer, C.P.; Brown, D.J.; Whitton, D.L. Congenital cranioventral abdominal wall, caudal sternal, diaphragmatic, pericardial, and intracardiac defects in Cocker Spaniel littermates. J Am Vet Med Assoc 1989, 194, 1741–1746. [Google Scholar] [CrossRef]
- Benlloch-Gonzalez, M.; Poncet, C. Sternal Cleft Associated with Cantrell’s Pentalogy in a German Shepherd Dog. J Am Anim Hosp Asso 2015, 51, 279–284. [Google Scholar] [CrossRef]
- Khan, S.; Sajik, D.; Calvo, I.; Philips, A. Novel peritoneopericardial diaphragmatic hernia in a dog. Vet Rec Case Rep 2019, 7(3), e000896. [Google Scholar] [CrossRef]
- Williams, P.; Booth, M.; Rossanese, M. Incomplete pentalogy of Cantrell in a Border terrier puppy. Vet Rec Case Rep 2020, 8, e001188. [Google Scholar] [CrossRef]
- Hennink, I.; Düver, P.; Rytz, U.; Meneses, F.; Moioli, M.; Adamik, K.N.; Kovacevic, A. Case Report: Unusual Peritoneopericardial Diaphragmatic Hernia in an 8-Month-Old German Shepherd Dog, Associated With a Pericardial Pseudocyst and Coexisting Severe Pericardial Effusion Resulting in Right-Sided Heart Failure. Front Vet Sci 2021, 8, 673543. [Google Scholar] [CrossRef] [PubMed]
- Ozdemir-Salci, E. S.; Yildirim, K. Thoracic ectopia cordis, sternal agenesis, partial ectopia hepatica and fissure abdominalis in a German Shepherd puppy with milder incomplete pentalogy of Cantrell. Clinical case. Revista Científica, FCV-LUZ 2024, XXXIV, rcfcv–e34306. [Google Scholar] [CrossRef]
- Lopez, M.M.; Kuzma, A.B.; Margiocco, M.L.; Cheng, T.; Enberg, T.B.; Head, L. Cardiac malposition (ectopia cordis) in a cat. J Vet Emerg Crit Care (San Antonio) 2015, 25, 783–788. [Google Scholar] [CrossRef]
- Eiger, S.N.; Mison, M.B.; Aronson, L.R. Congenital sternal defect repair in an adult cat with incomplete pentalogy of Cantrell. J Am Vet Med Assoc 2019, 254, 1099–1104. [Google Scholar] [CrossRef]
- Kokkinos, P.; Pratschke, K. Combined pentalogy of Cantrell with ectrodactyly and surgical implant-free repair of a sternal cleft and supraumbilical hernia in an adult cat. Vet Rec Case Reports 2022, 10, e364. [Google Scholar] [CrossRef]
- Hiraga, T.; Abe, M.; Iwasa, K.; Takehana, K.; Tanigaki, A. Cervico-pectoral ectopia cordis in two Holstein calves. Vet Pathol 1993, 30, 529–534. [Google Scholar] [CrossRef]
- Windberger, U.; Forstenpointner, G.; Grabenwöger, F.; Kopp, E.; Künzel, W.; Mayr, B.; Pernthaner, A.; Simon, P.; Losert, U. Cardiac function, morphology and chromosomal aberrations in a calf with ectopia cordis cervicalis. Zentralbl Veterinarmed A 1992, 39, 759–768. [Google Scholar] [CrossRef]
- Eröksüz, H.; Metin, N.; Eröksüz, Y. Total pectoral ectopia cordis and other congenital malformations in a calf. Vet Rec 1998, 142, (16):437. [Google Scholar] [CrossRef] [PubMed]
- Floeck, M.; Weissengruber, G.E.; Froehlich, W.; Forstenpointner, G.; Shibly, S.; Hassan, J.; Franz, S.; Polsterer, E. First report of pentalogy of Cantrell in a calf: a case report. Vet Med - Czech 2008, 53, 676–679. [Google Scholar] [CrossRef]
- Onda, K.; Sugiyama, M.; Niho, K.; Sato, R.; Arai, S.; Kaneko, K.; Ito, S.; Muto, M.; Suganuma, T.; Wakao, Y.; Wada, Y. Long-term survival of a cow with cervical ectopia cordis. Can Vet J 2011, 52, 667–669. [Google Scholar] [PubMed]
- Cerqueira, L.A.; Mâcedo, I.L; Sousa, D.E.R.; Amorim, H.A.L.; Borges, J.R.J.; Ximenes, F.H.B.; Câmara, A.C.L.; Castro, M.B. Complete Thoracic Ectopia Cordis in Two Lambs. Animals (Basel) 2024, 14(15), 2213. [Google Scholar] [CrossRef] [PubMed]
- Scaal, M. Development of the amniote ventrolateral body wall. Dev Dynam 2020, 250, 39–59. [Google Scholar] [CrossRef]
- Carmona, R.; Cañete, A.; Cano, E.; Ariza, L.; Rojas, A.; Muñoz-Chápuli, R. Conditional deletion of WT1 in the septum transversum mesenchyme causes congenital diaphragmatic hernia in mice. eLife 2016, 5, e16009. [Google Scholar] [CrossRef] [PubMed]
- Clugston, R.; Greer, J. Diaphragm development and congenital diaphragmatic hernia. Semin Pediatr Surg 2007, 16, 94–100. [Google Scholar] [CrossRef]
- Sadler, T. The embryologic origin of ventral body wall defects. Semin Pediatr Surg 2010, 19, 209–214. [Google Scholar] [CrossRef]
- Formstone, C.; Aldeiri, B.; Davenport, M.; Francis-West, P. Ventral body wall closure: Mechanistic insights from mouse models and translation to human pathology. Dev Dynam 2024, 254, 102–141. [Google Scholar] [CrossRef]
- Sheng, G.; Arias, M.; Sutherland, A. The primitive streak and cellular principles of building an amniote body through gastrulation. Science 2021, 374(6572), abg1727. [Google Scholar] [CrossRef]
- Holst, P.; Phemister, R. The prenatal development of the dog: preimplantation events. BOR 1971, 5, 194–206. [Google Scholar] [CrossRef]
- Pretzer, S. Canine embryonic and fetal development: a review. Theriogenology 2008, 70, 300–303. [Google Scholar] [CrossRef]
- Ueda, Y.; Yamada, S.; Uwabe, C.; Kose, K.; Takakuwa, T. Intestinal Rotation and Physiological Umbilical Herniation During the Embryonic Period. Anat Rec 2016, 299, 197–206. [Google Scholar] [CrossRef]
- Ginzel, M.; Martynov, I.; Haak, R.; Lacher, M.; Kluth, D. Midgut development in rat embryos using microcomputed tomography. Commun Biol 2021, 4(1), 190. [Google Scholar] [CrossRef]
- Aldeiri, B.; Roostalu, U.; Albertini, A.; Behnsen, J.; Wong, J.; Morabito, A.; Cossu, G. Abrogation of TGF-beta signalling in TAGLN expressing cells recapitulates Pentalogy of Cantrell in the mouse. Sci Rep 2018, 8(1), 3658. [Google Scholar] [CrossRef] [PubMed]
- Goetzinger, K. Pentalogy of Cantrell. Obstetric Imaging: Fetal Diagnosis and Care (Second Edition); Copel, JA, Dálton, ME, Tutschek, B., Eds.; Elsevier: Amsterdam, Netherlands, 2018; pp. pp 567–569.e1. [Google Scholar] [CrossRef]
- Palacios, M.; Idrobo, B.; Mosquera, L.; Soler, J. Pentalogy of Cantrell. A stillbirth case report. Case reports 2022, 253357363. [Google Scholar] [CrossRef]
- Carmi, R.; Boughman, J.A. Pentalogy of Cantrell and associated midline anomalies: a possible ventral midline developmental field. Am J Med Genet 1992, 42, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Duhamel, B. Embryology of exomphalos and allied malformations. Arch Dis Child 1963, 38, 142–147. [Google Scholar] [CrossRef]
- Arraf, A.; Yelin, R.; Reshef, I.; Kispert, A.; Schultheiss, T. Establishment of the visceral embryonic midline is a dynamic process that requires bilaterally symmetric BMP signalling. Dev Cell 2016, 37, 571–580. [Google Scholar] [CrossRef]
- Arraf, A.; Yelin, R.; Reshef, I.; Jadon, J.; Abboud, M.; Zaher, M.; Schneider, J.; Vladimirov, F.; Schultheiss, T. Hedgehog signalling regulates epithelial morphogenesis to position the ventral embryonic midline. Developmental Cell 2020. [Google Scholar] [CrossRef]
Figure 1.
Cantrell Syndrome body wall defects classification.
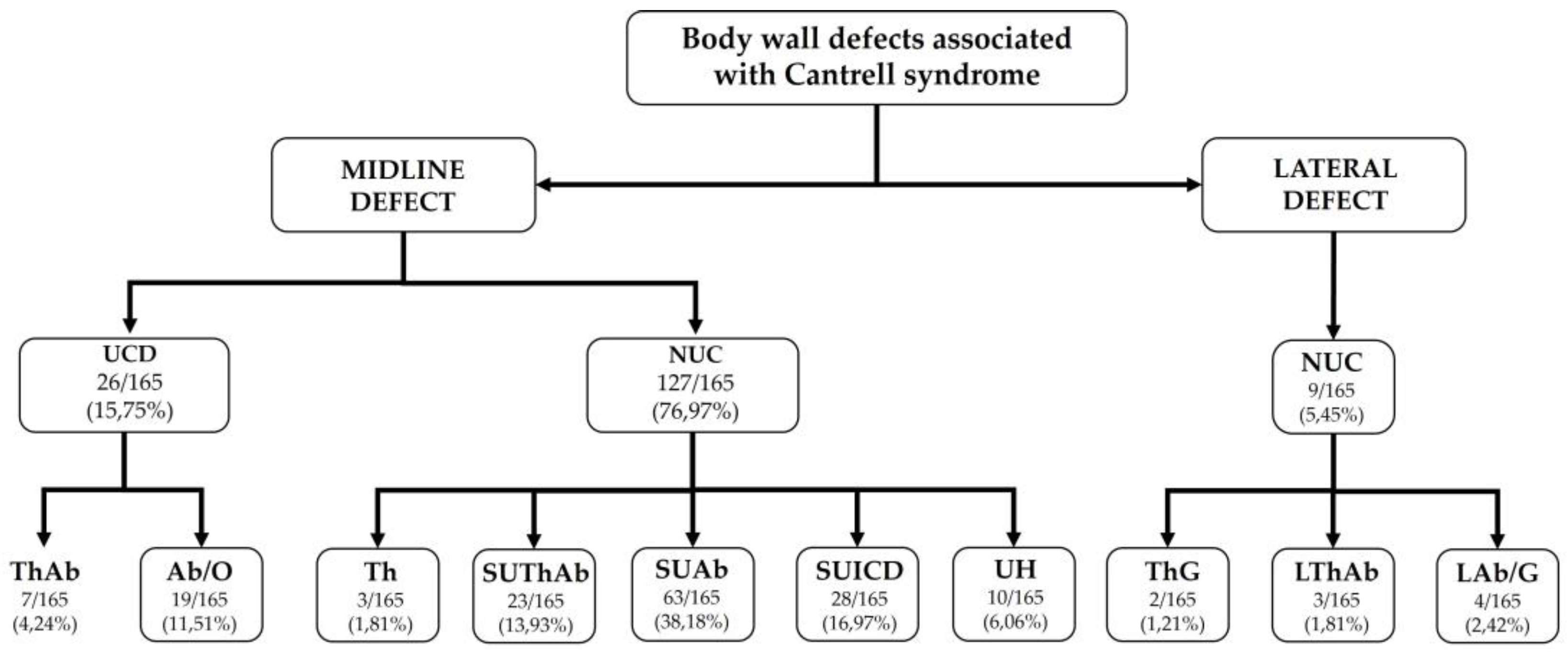
Figure 2.
Critical stages of ventral body wall development, showing the timing of these stages in embryos and the corresponding anomalies observed in humans and dogs.
Figure 2.
Critical stages of ventral body wall development, showing the timing of these stages in embryos and the corresponding anomalies observed in humans and dogs.
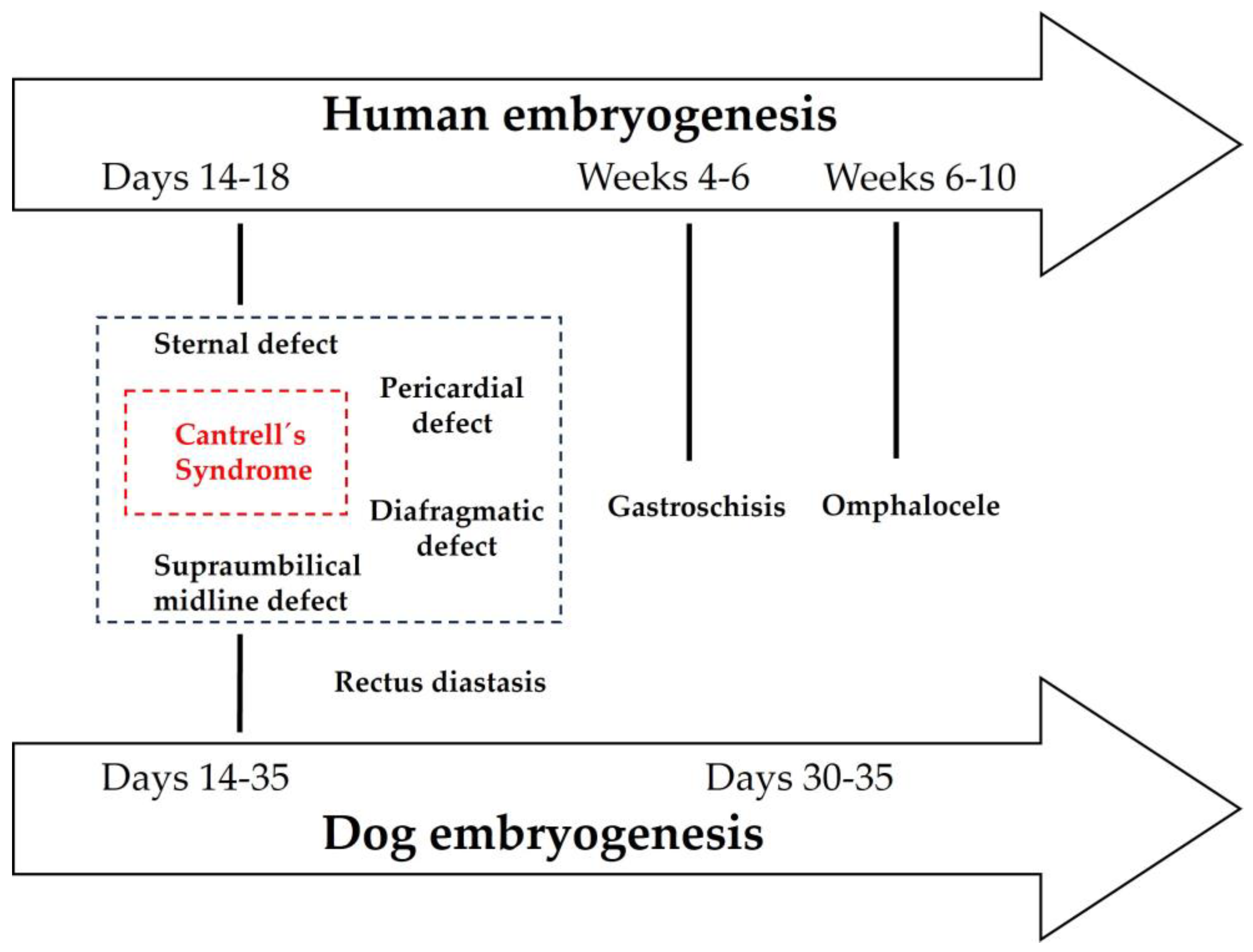

Table 1.
Classification of Defects in Cantrell’s Syndrome.
| Category | Type | Definition | Umbilical Cord | Associated defects |
|---|---|---|---|---|
| Midline Defects | UThAb | Umbilical thoracoabdominoschisis | Abnormal (omphalocele) | |
| SUThAb | Supraumbilical thoracoabdominoschisis | Normal | ||
| Th | Thoracoschisis | Normal | Sternal defect | |
| SUStAb | Supraumbilical sternal abdominoschisis | Normal | ||
| UAb+DD | Umbilical abdominoschisis | Abnormal (omphalocele) | Diaphragmatic defect | |
| SUAb+DD | Supraumbilical abdominoschisis | Normal | Diaphragmatic hernia | |
| SUICD | Supraumbilical incomplete central defect | Normal | Sternal defect | |
| UH+DD | Umbilical hernia | Normal | Diaphragmatic defect | |
| Lateral Defects | LTHAb |
Lateral thoracoabdominoschisis | Normal | |
| LTh | Lateral toracho | Normal | ||
| LAb | Lateral abdominoschisis | Normal (gastroschisis) |
Table 2.
Thoracoabdominoschisis (ThAb) with Umbilical Cord Defects (n = 7).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hori et al., 1984 [2] |
Case 1 ♀ |
ThAb | NR (+) |
NR | + | + | AAA | Type 1 | Ee, AE, Cch, CA, St-SpD | Ee in Cantrell-Haller-Ravitsch Syndrome | PC Class 2 BSA Type VI SPBWC III |
| Peer et al., 1993 [6] |
Case 17 ♂ |
ThAb | + SUA |
+ | + | NR | PDA, MVA, ASD | Type 1 | Ee, CL, CP, ABS | PC with Ee and ABS | PC Class 2 BSA Type VI STBWC III ABS |
| Kachare et al., 2013 [64] |
Case 113 NS |
O (ThAb) |
NR (+) |
+ | + | NR | VSD | Type 3 | Ee, St-SpD | PC with Ee and SpDs | PC Class 2 BSA Type V SSBWC III |
| Cakiroglu et al., 2014 [68] |
Case 119 ♀ |
(ThAb) | NR (+) |
+ | NR | NR | NR | Type 2 | HR, St-LD, St-SpD | PC associated with LD | BSA Type V SPLBWC III |
| Kheir et al., 2014 [69] |
Case 120 AG |
SUAb (ThAb) |
NR (+) |
+ | + | NR | NR | Type 1 | AA, St-GuD, NSt-LD | PC | BSA Type II STBWC I |
| Diaz-Serani and Sepulveda, 2020 [89] |
Case 146 ♂ |
ThAb | + SUA Cyst |
NR | NR | NR | NR | + | CL, CP, St-LD | ThAbEC | EC |
| Mraihi et al., 2023 [97] |
Case 158 C1, ♀ |
ThAb | + | + | + | NR | NR | Type 1 | NR | PC | BSA Type VI STBWC III |
AA, anal atresia; AAA, aplasia of the aortic arch; ABS, amniotic band syndrome; AE, adrenal ectopia; ASD, atrial septal defect; BSA, body stalk anomaly; BWD, body wall defects; CA, cerebellar aplasia; Cch, cranioschisis; CD, cardiac defects; CL, cleft lip; CP, cleft palate; DD, diaphragmatic defect; EC, Ectopia cordis; Ee, exencephaly; ExEC, external ectopia cordis; HR, hypoplastic ribs; LD, limb defect; MVA, mitral valve agenesis; NR, not reported; NSt-LD, non-structural limb defect; O, omphalocele; OD, other defects; PC, pentalogy of Cantrell; PD, pericardial defect; PDA, patent ductus arteriosus; SPBWC, spinal body wall complex; SpDs, spinal dysraphism; SPLBWC, spinal limb body wall complex; SSBWC, sternal spinal body wall complex; StD, sternal defect; STBWC, sternal body wall complex; STD, esternal defect; St-GuD, genitourinary defects; St-LD, structural limb defect; St-SpD, structural spinal defect; SUA, single umbilical artery; ThAb, thoracoabdominoschisis; ThAbEC, toraco-abdominal ectopia cordis; UCD, umbilical cord defect; VSD, ventricular septal defect.
Table 3.
Thoracoschisis (Th) with Normal Umbilical Cord – (n = 3).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Davies and Duran, 2003 [21] |
Case 37 C4, NS |
Th | - | + | NR | + | NR | Type 3 | NR | PC | PC Class 3 |
| Pius et al., 2017 [80] |
Case 137 ♀ |
Th | - | + | NR | + | NR | Type 3 | NR | EC | EC |
| Sulistyowati and Sensusiati, 2022 [90] |
Case 154 ♀ |
Th | - | + | + | ASD, VSD | Type 3 | BCL, CP, CrfD, ABS | PC | PC Class 2 |
Ab, abdominoschisis; ABS, amniotic band syndrome; ASD, atrial septal defect; BSA, body stalk anomaly; BWD, body wall defects; BCL, bilateral cleft lip; CD, cardiac defects; CP, cleft palate; CrfD, craniofacial dysmorphism; DD, diaphragmatic defect; EC, Ectopia cordis; ExEC, external ectopia cardiaca; NR, not reported; O, omphalocele; OD, other defects; PC, Pentalogy of Cantrell; PD, pericardial defect; PDA, patent ductus arteriosus; STBWC, sternal body wall complex; StD, sternal defect; SUICD, supraumbilical incomplete central defect; TF, tetralogy of Fallot; Th, thoracoschisis; UCD, umbilical cord defect; VSD, ventricular septal defect.
Table 4.
Abdominoschisis (Ab) with Umbilical Cord Defect — (n = 19).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Zachariou et al., 1987 [3] |
Case 3 S.D., ♂ |
O (Ab) |
+ | NR | + | + | TF | Type 1 | NR | PC | PC Class 2 |
| Case 4 F.M., ♀ |
O (Ab) |
+ | NR | + | NR | Dc, VSD | - | PCD, CtD, NSt-LD | PC | PC Class 3 | |
| Abdallah, et al., 1993 [7] |
Case 15 ♂ |
O (Ab) |
NR (-) |
+ | + | + | TF, PDA | Type 1 | H, PCD | PC with TF | PC Class 1 |
| Fernández et al., 1997 [10] |
Case 21 C3, ♀ |
O (Ab) |
NR (+) |
+ | + | + | TF, RVD | Type 1 | CrfD | PC | PC Class 1 |
| Halbertsma et al., 2002 [19] |
Case 32 ♂ |
O (Ab) |
+ | NR | + | + | ASD, VSD, LVD | Type 1 | NR | PC with LVD and O | PC Class 2 |
| León et al., 2002 [20] |
Case 33 NR |
O (Ab) |
NR (+) |
NR | + | + | CHD | Type 1 | NR | PC | PC Class 2 |
| Davies and Duran, 2003 [21] |
Case 34 C1, NR |
O (Ab) |
+ | NR | + | NR | NR | Type 1 | AN, CP, NSt-LD | EC and O | PC Class 3 |
| Polat et al., 2005 [26] |
Case 45 C3, ♂ |
O (Ab) |
NR (+) |
+ | NR | NR | - | Type 2 | NR | PC | PC Class 3 BSA Type VIII STBWC IV |
| Marijon et al., 2006 [31] |
Case 51 ♂ |
O (Ab) |
NR (+) |
NR | + | NR | VSD, LVD | Type 1 | NR | PC | PC Class 3 |
| Meeker, 2009 [45] |
Case 65 ♂ |
Ab | NR (+) |
+ | + | + | Dc, PS, BAV | - | NR | PC | PC Class 1 BSA Type VIII STBWC IV |
| Suehiro et al., 2009 [46] |
Case 67 ♂ |
Ab | (+) | + | NR | NR | VSD, LVD, PDA | Type 2 | NR | PC | PC Class 3 BSA Type VIII STBWC IV |
| Brochut et al., 2011 [55] |
Case 97 ♂ |
O (Ab) |
Sc Short |
NR | NR | NR | VSD, TA | + | NR | PC | PC Class 3 |
| Case 98 ♀ |
Ab | Uc Short |
NR | NR | NR | NR | + | TRAPS | PC | EC | |
| Case 99 ♂ |
O (Ab) |
Uc Short SUA |
NR | NR | NR | NR | + | AA, IM | PC | EC | |
| Ranganath et al., 2012 [56] |
Case 108 ♀ |
O (Ab) |
NR (+) |
+ | + | + | TGA | Type 1 | Ee, ABS, St-SpD, NSt-LD | PC with Crch | PC Class 1 BSA Type VII SSBWC IV |
| Ito et al., 2013 [65] |
Case 112 ♂ |
O (Ab) |
NR (+) |
NR | + | NR | TGA, VSD, HRV | Type 1 | NR | PC | PC Class 3 |
| Meena and Meena, 2017 [78] |
Case 136 ♀ |
O (Ab) |
+ SUA |
+ | + | NR | NR | Type 1 | NR | PC with SUA | PC Class 3 |
| Madi et al., 2019 [86] |
Case 149 ♀ |
(Ab) | + Cyst |
+ | + | + | ASD, VSD | Type 1 | NR | EC associated with PC | PC Class 1 BSA Type VIII STBWC IV |
| Faisal et al., 2024 [98] |
Case 156 NR |
O (Ab) |
+ | NR | + | + | Mc, LVD, VSD | Type 1 | NR | PC with LVD | PC Class 2 |
AA, anal atresia; Ab, abdominoschisis; ABS, amniotic band syndrome; AN, anencephaly; ASD, atrial septal defect; BAV, bicuspid aortic valve; BSA, Body Stalk Anomalies; BWD, body wall defect; CD, cardiac defects; Crch, craniorachischisis; CrfD, craniofacial dysmorphism; CtD, costal defects; CHD, congenital heart disease; CP, cleft palate; Dc, dextrocardia; DD, diaphragmatic defect; Ee, exencephaly; EC, Ectopia cordis; ExEC, external ectopia cordis; H, hydrocephaly; HRV, hypoplastic right ventricle syndrome; IM, intestinal malrotation; LVD, left ventricular diverticulum; Mc, mesocardia; NR, not reported; NSt-LD, non-structural limb defect; O, omphalocele; OD, other defects; PC, Pentalogy of Cantrell; PCD, pulmonary congenital defect; PD, pericardial defect; PDA, patent ductus arteriosus; PS, pulmonary stenosis; RVD, right ventricular dilatation; Sc, supercoiled; SSBWC, sternal spinal body wall complex; STBWC, sternal body wall complex; StD, sternal defect; St-SpD, structural spinal defect; SUA, single umbilical artery; TA, tricuspid atresia; TF, tetralogy of Fallot; TGA, transposition of the great arteries; TRAPS, twin reversed arterial perfusion sequence; Uc, uncoiled; UCD, umbilical cord defect; VSD, ventricular septal defect.
Table 5.
Supraumbilical thoracoabdominoschisis (SUThAb) Cases with Normal Umbilical Cord (n = 23).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Achiron, et al., 1991 [5] |
Case 14 ♀ |
SUThAb | NR (-) |
+ | NR | NR | VSD, TGA | Type 3 | NR | EC | PC Class 3 |
| Dembinski et al., 1997 [9] |
Case 18 ♀ |
SUThAb | - | + | + | + | ASD, PDA | Type 3 | CrfD, CH, St-SpD, St-LD, St-GuD | CSq | PC Class 1 |
| Fernández et al., 1997 [10] |
Case 19 C1, ♂ |
SUThAb | NR (-) |
+ | + | + | VSD, ASD, DORV | Type 3 | NSt-GuD | PC | PC Class 1 |
| Case 20 C2, ♀ |
SUThAb | NR | + | + | NR | DORV, ASD, VSD | - | L-SE, HT, GA, AA, St-GuD, NSt-SpD | PC | PC Class 2 | |
| Hsieh et al., 1998 [12] |
Case 23 C1, ♂ |
SUThAb | NR (-) |
+ | + | + | NS | Type 1 | CyH | PC with CyH | PC Class 3 |
| Pivnick et al., 1998 [15] |
Case 27 ♀ |
SUThAb | - | + | + | NR | NR | Type 3 | AOP(R), MOP(L), BCL, PCD, St-GuD, St-LD | Midline ThAb and LD | PC Class 3 |
| Nanda et al., 2003 [22] |
Case 39 NS |
O (SUThAb) |
NR (-) |
+ | NR | NR | VSD | Type 3 | NR | PC | PC Class 3 |
| Uygur et al., 2004 [24] |
Case 42 ♂ |
SUThAb | NR (-) |
+ | + | NR | ASD, PDA | Type 3 | GA, St-LD | PC and LD | PC Class 2 |
| Chen et al., 2008 [42] |
Case 55 ♀ |
SUThAb | - | + | + | + | VSD | Type 3 | Ee | PC with Ee and LD | PC Class 1 |
| Smigiel et al., 2011 [53] |
Case 101 ♀ |
O + DRM (SUThAb) |
NR (-) |
+ | + | - | - | Type 3 | AA, CrfD, NSt-LD, NSt-GuD | Goltz–Gorlin Syndrome and PC | PC Class 3 |
| Sakasai et al., 2012 [57] |
Case 109 ♂ |
O (SUThAb) |
NR (-) |
+ | + | + | VSD, PDA | Type 3 | NR | PC with EC and VSD | PC Class 1 |
| Chen et al., 2013 [62] |
Case 111 ♂ |
(SUThAb) | NR (-) |
+ | + | NR | NR | Type 3 | AN | CS with AN | EC |
| Kaouthar, et al., 2013 [67] |
Case 115 C2, ♀ |
SUThAb | NR (-) |
+ | NR | + | DORV, TGA | Type 3 | NR | PC | PC Class 2 |
| Puvabanditsin et al., 2013 [66] |
Case 117 ♂ |
(SUThAb) | NR (-) |
+ | + | + | DORV, TGA, PS, VSD | Type 3 | NR | EC | PC Class 1 |
| Restrepo et al., 2013 [70] |
Case 118 NS |
O (SUThAb) |
NR (-) |
+ | NR | + | ASD, TF, APVR | Type 3 | PCD, ABS | PC with EC, APVR and TF | PC Class 2 |
| Araujo et al., 2006 [28] |
Case 135 ♀ |
O (SUThAb) |
NR (-) |
+ | + | + | VSD | Type 3 | Hy | PC | PC Class 1 |
| Swarray-Deen et al., 2017 [82] |
Case 140 C2, ♀ |
(SUThAb) | NR (-) |
+ | + | + | NR | Type 3 | NR | PC | PC Class 3 |
| Delgado et al., 2019 [87] |
Case 145 NS |
O (SUThAb) |
NR (-) |
+ | + | + | PDA, LSVC to CS | Type 3 | NR | PC with total EC and a major O | PC Class 1 |
| Desikan et al., 2021 [91] |
Case 150 NS |
SUThAb | NR (-) |
+ | NR | NR | VSD | Type 3 | NR | Ec, NSt-LD | PC Class 3 |
| Shrestha, 2022 [92] |
Case 153 ♀ |
SUThAb | NR (-) |
+ | NR | + | NS | Type 3 | BCL, CP | EC, O, BCL and CP | PC Class 3 |
| Fabijan et al., 2024 [99] |
Case 160 ♀ |
O (SUThAb) |
NR (-) |
+ | NR | + | TF, APVR, LSVC to CS | Type 3 | HR | PC and EC | PC Class 2 |
| Garofalo et al., 2024 [100] |
Case 161 ♀ |
SUThAb | NR (-) |
NR | NR | NR | TGA, ASD, VSD, PS | + | Ep, OmT | Ep and ThAbEC | EC |
| Martadiansyah et at., 2025 [103] |
Case 164 C1, ♀ |
SUThAb | - | + | + | + | ASD, PDA | Type 3 | NR | EC complicated by PC | PC Class 1 |
AA, anal atresia; ABS, amniotic band syndrome; AN, anencephaly; ASD, atrial septal defect; AOP, anophthalmia; APVR, anomalous pulmonary venous return; BCL, bilateral cleft lip; BWD, body wall defect; CD, cardiac defects; CH, cerebellar hypoplasia; CrfD, craniofacial dysmorphism; CP, cleft palate; CrfD, craniofacial dysmorphism; CS, Cantrell syndrome; CSq, Cantrell sequence; CyH, cystic hygroma; DD, diaphragmatic defect; DORV, double-outlet right ventricle; DRM, diastasis of the abdominal recti muscles; EC, Ectopía cordis; Ee, exencephaly; EC, Ectopia cordis; Ep, epignathus; ExEC, external ectopia cordis; GA, gallbladder agenesis; HR, hypoplastic ribs; HT, hypertelorism; Hy, hydramnios; L, left; LSVC to CS, left superior vena cava draining to coronary sinus; L-SE, low-set ears; MOP, microphthalmia; NR, not reported; NSt-GuD, non-structural genitourinary defects; NSt-LD, non-structural limb defect; O, omphalocele; OD, other defects; OmT, oromandiula tumor; PC, Pentalogy of Cantrell; PCD, pulmonary congenital defect; PD, pericardial defect; PDA, patent ductus arteriosus; PS, pulmonary stenosis; R, riht; St-GuD, structural genitourinary defects; St-SpD, spinal defect; St-LD, structural limb defect; StD, sternal defect; SUThAb, supra-umbilical-thoraco-abdominoschisis; TF, tetralogy of Fallot; TGA, transposition of the great arteries; ThAb, thoracoabdominoschisis; ThAbEC, toraco-abdominal ectopia cordis; UCD, umbilical cord defect; VSD, ventricular septal defect.
Table 6.
Supraumbilical Abdominoschisis (SUAb) with Normal Umbilical Cord (n = 63).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Zachariou et al., 1987 [3] |
Case 2 L.A., ♂ |
SUAb | - | NR | + | NR | VSD | - | PCD | PC | PC Class 3 |
| Milne et al., 1990 [4] |
Case 5 J.L.C., ♀ |
O (SUAb) |
NR (-) |
- | + | + | - | - | NR | PSDH with O | PC Class 3 |
| Case 6 N.K., ♀ |
O (SUAb) |
NR (-) |
- | + | + | Dc | - | NR | PSDH with O | PC Class 3 | |
| Case 7 A.J.T., NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD | - | IM | PSDH with O | PC Class 1 | |
| Case 8 M.A, NS |
O (SUAb) |
NR (-) |
+ | + | + | BvD | - | NR | PSDH with O | PC Class 1 | |
| Case 9 B.G.H, NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD, PS, DORV | - | NR | PSDH with O | PC Class 1 | |
| Case 10 H.E.P, NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD, PTA type IV |
- | PCD | PSDH with O | PC Class 1 | |
| Case 11 A.M.S, NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD, ASD, PAA | - | IM | PSDH with O | PC Class 1 | |
| Case 12 B.G.H, NS |
O (SUAb) |
NR (-) |
- | + | + | HLV, APVR | - | PCD, MD, CtD, St-GuD | PSDH with O | PC Class 2 | |
| Case 13 R.M., NS |
O (SUAb) |
NR (-) |
+ | + | + | - | Type 1 | PCD, IM, St-LD | PSDH with O | PC Class 3 | |
| Bogers et al., 1993 [8] |
Case 16 ♀ |
O + DRM (SUAb) |
NR (-) |
+ | + | + | VSD, BvD | Type 1 | CtD, SS | CS with BvD, VSD and EC | PC Class 1 |
| Katranci et al., 1998 [13] |
Case 24 C1, ♀ |
O (SUAb) |
NR (-) |
+ | + | + | TF | - | HCy | PC | PC Class 1 |
| Case 25 C2, ♂ |
O (SUAb) |
NR (-) |
+ | + | + | CHD | - | NSt-GuD | PC | PC Class 1 | |
| Vazquez-Jimenez et al., 1998 [11] |
Case 28 ♂ |
SUAb | NR (-) |
+ | + | NR | Dc, VSD, ASD, LVD, RVH |
- | NR | Partial PC | PC Class 2 |
| Falcao et al., 2000 [17] |
Case 29 ♂ |
SUAb | NR (-) |
+ | + | + | Mc, TF, VD, SCA | - | NR | PC | PC Class 1 |
| Song and McLeary, 2000 [16] |
Case 30 ♂ |
O (SUAb) |
NR (-) |
+ | - | - | Dc, CM, SV, PAA, TA | - | NR | PC with an intact diaphragm and pericardium | PC Class 3 |
| Alayunt et al., 2001 [18] |
Case 31 ♀ |
DRM, SUAb | NR (-) |
+ | + | + | Dc, VSD, LVD, TF, ASD | - | NR | LVD with PC and TF | PC Class 1 |
| Bittmann, et al., 2004 [23] |
Case 40 ♂ |
O (SUAb) |
NR (-) |
+ | + | + | HRV, VSD, ASD, PS | - | PCD, GA, Ps | PC with TF, GA and PS | PC Class 1 |
| Di Bernardo et al., 2004 [25] |
Case 41 NS |
SUAb | - | + | + | + | LVD, LSCV to CS | Type 3 | NR | PC with LVD | PC Class 1 |
| St. Louis, 2005 [29] |
Case 46 ♀ |
O (SUAb) |
NR (-) |
+ | + | + | HLHS | Type 3 | NR | PC with HLHS | PC Class 1 |
| Staboulidou et al., 2005 [27] |
Case 47 ♀ |
SUAb | NR (-) |
+ | + | + | NR | Type 3 | NR | PC | PC Class 2 |
| Araujo et al., 2006 [28] |
Case 48 NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD | Type 3 | Hy | PC | PC Class 1 |
| Grethel et al., 2007 [32] |
Case 49 ♂ |
SUAb | - | + | + | + | Dc, LVA, ASD | - | NSt-GuD | PC and LVA | PC Class 1 |
| Loureiro et al., 2007 [34] |
Case 52 NS |
SUAb | NR (-) |
+ | + | NR | PTA, VSD | Type 3 | Ecc, Myc, H | PC with ONTD, St-SpD, NSt-LD |
PC Class 2 |
| Wheeler, & St. Louis, 2007 [33] |
Case 53 ♀ |
SUAb | NR (-) |
+ | + | + | HLHS | Type 3 | NR | PC with HLHS | PC Class 1 |
| Hou et al., 2008 [39] |
Case 56 ♂ |
SUAb | NR (-) |
+ | + | NR | Dc, PDA, AVC, VSD, BvH, RVD | Type 3 | CrfD, L-SE, CH, St-SpD, NSt-LD, NSt-GuD | Incomplete PC |
PC Class 2 |
| Korver et al., 2008 [35] |
Case 57 ♂ |
SUAb | - | + | + | NR | Dc, VSD, LVD | Type 3 | NR | PC | PC Class 2 |
| Okamoto et al., 2008 [37] |
Case 59 ♀ |
SUAb | NR (-) |
+ | NR | NR | TA | Type 3 | H | PC with severe EC | PC Class 3 |
| Turbendian et al., 2008 [40] |
Case 60 ♀ |
O (SUAb) |
NR (-) |
- | + | + | LVD | + | NR | PC | PC Class 2 |
| Zidere and Allan, 2008 [41] |
Case 61 C1, NS |
O (SUAb) |
NR (-) |
+ | + | + | DORV | - | IM, NSt-GuD |
PC | PC Class 1 |
| Case 62 C2, NS |
O (SUAb) |
NR (-) |
+ | + | + | ASD | - | PCD | PC | PC Class 1 | |
| Case 63 C3, NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD, ASD | - | PCD | PC | PC Class 1 | |
| Balderrábano-Saucedo et al., 2011 [52] |
Case 70 C3, NS |
O (SUAb) |
NR (-) |
+ | + | + | LVD, VSD | Type 3 | NR | PC with EC | PC Class 1 |
| Case 71 C4, NS |
O (SUAb) |
NR (-) |
+ | + | + | DORV, PTA, PS, PDA, SCA | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 73 C6, NS |
O (SUAb) |
NR (-) |
+ | + | + | SA, SV, AVC, TGA, PS, PDA | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 76 C9, NS |
O (SUAb) |
NR (-) |
+ | + | + | DORV, PS | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 78 C11, NS |
O (SUAb) |
NR (-) |
+ | + | + | SV, PTA | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 80 C13, NS |
O (SUAb) |
NR (-) |
+ | + | + | DORV | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 81 C14, NS |
O (SUAb) |
NR (-) |
+ | + | + | BVD, TF | - | NR | PC without EC | PC Class 1 | |
| Case 84 C16, NS |
O (SUAb) |
NR (-) |
+ | + | + | DILV, PS | - | NR | PC without EC | PC Class 1 | |
| Case 85 C17, NS |
O (SUAb) |
NR (-) |
+ | + | + | DILV, ASD, PS, PDA | - | NR | PC without EC | PC Class 1 | |
| Case 86 C18, NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD, ASD, PDA | - | NR | PC without EC | PC Class 1 | |
| Case 87 C20, NS |
O (SUAb) |
NR (-) |
+ | + | + | LVD, DORV, PS | - | NR | PC without EC | PC Class 1 | |
| Case 88 C21, NS |
O (SUAb) |
NR (-) |
+ | + | + | VSD | - | NR | PC without EC | PC Class 1 | |
| Herman and Siegel, 2010 [48] |
Case 90 ♀ |
O (SUAb) |
NR (-) |
NR | + | + | ASD, VSD, PDA | - | NR | PC | PC Class 2 |
| Brochut et al., 2011 [55] |
Case 100 ♂ |
O (SUAb) |
- | + | + | + | Dc, APVR | Type 3 | NR | PC | PC Class 1 |
| Wen et al., 2011 [54] |
Case 102 ♂ |
O (SUAb) |
NR (-) |
+ | + | AVC, ASD, VSD, TGA, PS | Type 3 | NR | PC with complex cardiac malformations | PC Class 2 | |
| Ergenoğlu et al., 2012 [58] |
Case 103 ♂ |
O (SUAb) |
- | NR | NR | NR | NR | + | St-SpD, St-LD | PC | EC |
| Kinoshita, et al., 2012 [59] |
Case 107 C3, ♂ |
O (SUAb) |
NR (-) |
+ | + | + | ASD | - | NR | PC | PC Class 1 |
| Pirasteh et al., 2014 [72] |
Case 121 ♀ |
O (SUAb) |
NR (-) |
NR | + | + | LVD, DORV, VSD, PAH, TGA, HRV | + | NR | PC with EC | PC Class 2 |
| Naburi et al., 2015 [73] |
Case 130 ♀ |
SUAb | NR (-) |
+ | + | NR | VSD, ASD | Type 3 | NR | PC Class 2 | PC Class 2 |
| Türkçapar et al., 2015 [75] |
Case 132 NS |
O (SUAb) |
NR (-) |
NR | + | NR | NR | + | CyH, St-SpD | PC | EC |
| Madžarac et al, 2016 [76] |
Case 133 ♂ |
SUAb | NR (-) |
+ | + | + | VSD | Type 3 | HD, NSt-GuD | PC with unilateral kidney evisceration | PC Class 1 |
| Yang et al., 2016 [77] |
Case 134 ♀ |
O (SUAb) |
NR (-) |
+ | + | + | VSD, ASD, LVD | Type 3 | NR | PC | PC Class 1 |
| Swarray-Deen et al., 2017 [82] |
Case 139 C1, ♀ |
O (SUAb) |
NR (-) |
NR | + | + | VSD, TF | Type 3 | NSt-LD | PC | PC Class 2 |
| Zani-Ruttenstock, et al., 2017 [79] |
Case 141 ♀ |
O + DRM (SUAb) |
NR (-) |
+ | + | NR | VSD, ASD, APVR, PDA, LVD | Type 3 | NR | PC | PC Class 2 |
| Grigore et al., 2018 [84] |
Case 142 NS |
SUAb | NR (-) |
NR | + | + | NS | + | UAOP, CrfD | PC with UAOP | PC Class 3 |
| Kylat, 2019 [88] |
Case 147 C1, ♀ |
O (SUAb) |
- | + | + | + | VSD, PDA, PS | Type 3 | NR | PC | PC Class 1 |
| Zvizdic et al., 2021 [90] |
Case 151 ♂ |
O (SUAb) |
NR (-) |
+ | + | + | ASD, VSD | Type 3 | NR | PC | PC Class 1 |
| Fazea et al., 2022 [94] |
Case 152 ♂ |
O (SUAb) |
NR (-) |
+ | + | NR | CHD | Type 3 | SpD | PC with EC | PC Class 2 |
| Mraihi et al., 2023 [97] |
Case 159 C2, NS |
O (SUAb) |
NR (-) |
NR | + | NR | NR | + | NR | PC | EC |
| Dusuri et al., 2025 [101] |
Case 162 ♂ |
O (SUAb) |
NR (-) |
+ | + | NR | NS | Type 3 | AH, St-SpD, NSt-LD |
Complete PC with EC and multiple anomalies |
PC Class 3 |
| Maheshwari & Sahoo, 2025 [102] |
Case 163 ♂ |
O + DRM (SUAb) |
NR (-) |
+ | + | NR | TF | Type 3 | NR | PC with TF and Absent Diaphragm | PC Class 2 |
AH, alobar holoprosencephaly; ASD, atrial septal defect; APVR, anomalous pulmonary venous return; AVC, atrioventricular canal; BvH, biventricular hypertrophy; BvD, biventricular diverticulum; BSA, body stalk anomalies; BWD, body wall defect; CD, cardiac defects; CH, cerebellar hypoplasia; CHD, congenital heart disease; CrfD, craniofacial dysmorphism; CtD, costal defects; CM, cardiomegaly; CrfD, craniofacial dysmorphism; CS, Cantrell syndrome; CyH, cystic hygroma; Dc, dextrocardia; DD, diaphragmatic defect; DILV, double-inlet left ventricle; DORV, double-outlet right ventricle; DRM, diastasis of the abdominal recti muscles; EC, Ectopia cordis; Ecc, encephalocele; ExEC, external ectopia cordis; GA, gallbladder agenesis; H, hydrocephaly; HD, hepatic defect; HCy, hepatic cyst; HLHS, hypoplastic left heart syndrome; HLV, hypoplastic left ventricle; HRV, hypoplastic right ventricle syndrome; Hy, hydramnios; IM, intestinal malrotation; LSVC to CS, left superior vena cava draining to coronary sinus; L-SE, low-set ears; LVA, left ventricular aneurysm; LVD, left ventricular diverticulum; Mc, mesocardia; MD, musculoskeletical deformities; Myc, myelomeningocele; NR, not reported; NSt-GuD, genitourinary defects; NSt-LD, non-structural limb defect; O, omphalocele; OD, other defects; ONTD, open neural tube defect; PAA, pulmonary artery atresia; PAH, pulmonary artery hipoplasia; PC, Pentalogy of Cantrell; PCD, pulmonary congenital defect; PD, pericardial defect; PDA, patent ductus arteriosus; PTA, persistent truncus arteriosus; Ps, polisplenia; PS, pulmonary stenosis; PSDH, pars sternalis diaphrgmatic hernia; PTA, persistent truncus arteriosus; RVD, right ventricular dilatation; RVH, right ventricular hipertrofy; SA, single atrium; SCA, single coronary artery; SpD, spinal defect; SS, situs solitus; St-LD, structural limb defect; St-GuD, structural genitourinary defects; St-SpD, spinal defect; StD, sternal defect; SUAb, supra-umbilical-abdominoschisis; SV, single ventricle; TA, tricuspid atresia; TF, tetralogy of Fallot; TGA, transposition of the great arteries; UAOP, unilateral anophthalmia; UCD, umbilical cord defect; VD, ventricular diverticulum; VSD, ventricular septal defect.
Table 7.
Supraumbilical Incomplete Central Defect (SUICD) (n = 28).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Fernández et al., 1997 [10] |
Case 22 C4, ♀ |
VEH (SUICD) |
- | + | NR | + | VSD, ASD, AVS, PDA | - | Hy, L-SE, CP, St-GuD, NSt-SpD |
PC | PC Class 2 |
| Knirsch et al., 2006 [30] |
Case 50 NS |
(SUICD) | - | + | NR | NR | VSD, ASD, URC, LVD | Type 3 | NR | PC | PC Class 3 |
| Gao et al., 2009 [43] |
Case 64 ♀ |
(SUICD) | NR (-) |
+ | + | + | PTA, VSD, ASD, PDA | Type 3 | NR | PC with ThAbEC | PC Class 1 |
| Mitsukawa et al., 2009 [44] |
Case 66 ♀ |
(SUICD) | - | NR | + | + | VSD, ASD | + | NR | PC | PC Class 2 |
| Balderrábano-Saucedo et al., 2011 [52] |
Case 72 C5, NS |
RD (SUICD) |
NR (-) |
+ | + | + | CoA, VSD | Type 3 | NR | PC with EC | PC Class 1 |
| Case 74 C7, NS |
RD (SUICD) |
NR (-) |
+ | + | + | SV, LSVC to CS |
Type 3 | NR | PC with EC | PC Class 1 | |
| Case 75 C8, NS |
RD (SUICD) |
NR (-) |
+ | + | + | LVD, ASD | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 77 C10, NS |
RD (SUICD) |
NR (-) |
+ | + | + | DORV, SCA | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 79 C12, NS |
RD (SUICD) |
NR (-) |
+ | + | + | LVD, VSD | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 83 C15, NS |
RD (SUICD) |
NR (-) |
+ | + | + | HRVS, PTA, VSD, LSVC to CS | - | NR | PC without EC | PC Class 1 | |
| Singh et al., 2010 [49] |
Case 92 ♀ |
RD (SUICD) |
NR (-) |
+ | + | + | Mc, DORV, VSD, LVD |
Type 3 | NR | PC | PC Class 1 |
| Sowande et al., 2010 [47] |
Case 93 C1, ♀ |
(SUICD) | - | + | NR | NR | NS | Type 3 | NR | PC | PC Class 3 |
| Case 94 C2, ♀ |
(SUICD) | - | + | NR | NR | Mc, GH | Type 3 | NR | PC | PC Class 3 | |
| Case 95 C3, ♂ |
(SUICD) | - | + | NR | NR | Mc, GH | Type 3 | NR | PC | PC Class 3 | |
| Kinoshita, et al., 2012 [59] |
Case 106 C2, ♀ |
RD (SUICD) |
NR (-) |
+ | + | DORV, PAA, VSD, PDA | Type 3 | NR | PC Class 2 | ||
| Magadum et al., 2013 [63] |
Case 116 ♂ |
(SUICD) | + | + | + | NR | Type 3 | HD | Incomplete PC | PC Class 3 | |
| Zhang et al., 2014 [71] |
Case 122 C1, ♀ |
(SUICD) | NR (-) |
+ | + | NR | DORV, VSD, LSVC | Type 3 | NR | PC | PC Class 2 |
| Case 123 C2, ♂ |
(SUICD) | NR (-) |
+ | + | NR | VSD, LSVC | Type 3 | CL | PC | PC Class 2 | |
| Case 124 C3, ♀ |
(SUICD) | NR (-) |
+ | + | NR | ASD | - | NR | PC | PC Class 2 | |
| Case 125 C4, ♂ |
(SUICD) | NR (-) |
+ | + | NR | VSD | Type 3 | NR | PC | PC Class 2 | |
| Case 126 C5, ♂ |
(SUICD) | NR (-) |
+ | + | NR | DORV, VSD, ASD, PS, LSVC | Type 3 | NR | PC | PC Class 2 | |
| Case 127 C6, ♂ |
(SUICD) | NR (-) |
+ | + | NR | VSD, ASD, LSVC | - | PCD | PC | PC Class 2 | |
| Case 128 C7, ♂ |
(SUICD) | NR (-) |
+ | + | NR | VSD, ASD, LSVC | - | NR | PC | PC Class 2 | |
| Case 129 C8, ♂ |
(SUICD) | NR (-) |
+ | + | NR | VSD, ASD, LVD, LSVC | Type 3 | CL | PC | PC Class 2 | |
| Salinas-Torres et al., 2017 [81] |
Case 138 ♂ |
(SUICD) | - | + | + | + | HLV | Type 3 | CrfD, ABS | PC with severe amputations | PC Class 1 |
| Màrginean et al., 2018 [83] |
Case 144 ♂ |
RD (SUICD) |
NR (-) |
NR | NR | NR | TA, VDS, PAH | + | NR | PC | EC |
| Wang et al., 2022 [95] |
Case 155 ♂ |
RD (SUICD) |
NR (-) |
+ | + | + | LVD, ASD, VSD, PDA | + | NR | PC | PC Class 1 |
| Liao et al., 2023 [96] |
Case 157 ♂ |
RD (SUICD) |
- | + | - | + | VSD, ASD, CoA, PDA, PLSVC | Type 3 | NR | PC | PC Class 2 |
ABS, amniotic band syndrome; ASD, atrial septal defect; AVS, aortic valve stenosis; BWD, body wall defect; CD, cardiac defects; CrfD, craniofacial dysmorphism; CL, cleft lip; CoA, coarctation of the aorta; CP, cleft palate; CrfD, craniofacial dysmorphism; DD, diaphragmatic defect; DORV, double-outlet right ventricle; EC, Ectopia cordis; ExEC, external ectopia cordis; GH, globular heart; ; HD, hepatic defect; HLV, hypoplastic left ventricle; HRVS, hypoplastic right ventricle syndrome; Hy, hydramnios; LSVC to CS, left superior vena cava draining to coronary sinus; L-SE, low-set ears; LVD, left ventricular diverticulum; Mc, mesocardia; NR, not reported; NSt-SpD, non-structural spinal defect; OD, other defects; PAA, pulmonary artery atresia; PAH, pulmonary artery hipoplasia; PC, Pentalogy of Cantrell; PCD, pulmonary congenital defect; PD, pericardial defect; PDA, patent ductus arteriosus; PLSVC, persistent left superior vena cava; PS, pulmonary stenosis; PTA, persistent truncus arteriosus; RD, rectal diastasis; SCA, single coronary artery; St-GuD, genitourinary defects; StD, sternal defect; SUA, single umbilical artery; SUICD, supra-umbilical central defect; SV, single ventricle; TA, tricuspid atresia; ThAbEC, toraco-abdominal ectopia cordis; UCD, umbilical cord defect; URC, unroofed coronary sinus; VEH, ventral epigastric hernia; VSD, ventricular septal defect.
Table 8.
Umbilical Hernia (n = 10).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Laloyaux et al., 1998 [14] |
Case 26 ♂ |
UH, RD | NR (-) |
+ | + | + | VSD, ASD, TA, PS | Type 3 | NR | PC | PC Class 1 |
| Marcí et al., 2008 [38] |
Case 58 ♂ |
UH | NR (-) |
NR | + | NR | LVD, DORV | + | NR | PC with DORV | PC Class 3 |
| Balderrábano-Saucedo et al., 2011 [52] |
Case 68 C1, NS |
UH | NR (-) |
+ | + | + | SA, SV, AvC, PS | Type 3 | NR | PC with EC | PC Class 1 |
| Case 69 C2, NS |
UH | NR (-) |
+ | + | + | LVD, VSD, PDA, SCA | Type 3 | NR | PC with EC | PC Class 1 | |
| Case 82 NS |
UH | NR (-) |
+ | + | + | LVD, DORV | - | NR | PC without EC | PC Class 1 | |
| Case 89 C22, NS |
UH | NR (-) |
+ | + | + | LVD, DORV | - | NR | PC without EC | PC Class 1 | |
| Quandt et al., 2010 [50] |
Case 91 ♀ |
UH RD |
NR (-) |
NR | NR | NR | SS, ASD, LVD | + | NR | PC | PC Class 3 |
| El Kouache et al., 2012 [60] |
Case 104 ♀ |
UH | NR (-) |
+ | + | + | Dc, LVD, triatrial SS VSD, ASD, PDA | Type 3 | NR | LVD with partial PC | PC Class 1 |
| Kaouthar, et al., 2013 [67] |
Case 114 C1, ♀ |
UH, RD | NR (-) |
+ | + | NR | Dc, DORV, TGA, LSVC to CS | Type 3 | SS | PC | PC Class 2 |
| Kylat, 2019 [88] |
Case 148 C2, ♂ |
UH | - | + | NR | NR | ASD, LSVC to CS | Type 3 | NR | Incomplete PC | PC Class 3 |
ASD, atrial septal defect; AvC, atrioventricular canal; BWD, body wall defect; CD, cardiac defects; Dc, dextrocardia; DD, diaphragmatic defect; DORV, double-outlet right ventricle; EC, Ectopia cordis; ExEC, external ectopia cordis;; LSVC to CS, left superior vena cava draining to coronary sinus; LVD, left ventricular diverticulum; NR, not reported; OD, other defects; PC, Pentalogy of Cantrell; PD, pericardial defect; PDA, patent ductus arteriosus; PS, pulmonary stenosis; RD, rectal diastasis; SA, single atrium; SCA, single coronary artery; SS, situs solitus; StD, sternal defect; SV, single ventricle; TA, tricuspid atresia; TGA, transposition of the great arteries; UCD, umbilical cord defect; UH, umbilical hernia; VSD, ventricular septal defect.
Table 9.
Lateral Abdominal Wall Defects (n = 9).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Davies and Duran, 2003 [21] |
Case 35 C2, NS |
ThG | - | + | NR | NR | NR | Type 4 | NR | EC and ThG | PC Class 3 |
| Case 36 C3, NS |
ThG | - | + | NR | NR | NR | Type 4 | NR | EC and ThG | PC Class 3 | |
| Nanda et al., 2003 [22] |
Case 38 C1, ♀ |
LThAb | (-) | + | + | + | VSD | Type 1 | St-SpD, NSt-LD | PC | PC Class 1 |
| Polat et al., 2005 [26] |
Case 43 C1, ♀ |
O (LThAb) |
NR (-) |
+ | NR | NR | - | Type 3 | Ee, Hy, St-SpD, NSt-LD | PC | PC Class 3 |
| Case 44 C2, ♀ |
O (LAb/G) |
NR (-) |
NR | NR | NR | - | + | Ee, Hy, St-SpD, NSt-LD | PC | EC | |
| Chelli et al., 2008 [36] |
Case 54 ♀ |
ThAb (LAb/G) |
- | NR | NR | NR | NR | + | Ht, CrfD, NSt-LD | EC | EC |
| Kinoshita, et al., 2012 [59] |
Case 105 C1, ♂ |
O + RD (LAb/G) |
NR (-) |
+ | + | + | NR | Type 4 | NR | PC | PC Class 3 |
| Chandran and Ari, 2013 [61] |
Case 110 ♂ |
O (LThAb) |
(-) | + | + | + | ASD, VSD, PDA | Type 1 | BCL | PC | PC Class 1 |
| Timur et al., 2015 [74] |
Case 131 ♂ |
O (LAb/G) |
NR (-) |
+ | + | NR | VSD | - | NR | PC | PC Class 2 |
ASD, atrial septal defect BCL, cleft lip; BSA, body stalk anomaly; BWD, body wall defect; CD, cardiac defects; CrfD, craniofacial dysmorphism; DD, diaphragmatic defect; RD, rectal diastasis; Ee, exencephaly; EC, Ectopia cordis; ExEC, external ectopia cordis; G, gastrochisis; Ht, hypertelorism; Hy, hydramnios; LAb, lateral abdominoschisis; LThAb, lateral thoracoabdominoschisis;; NR, not reported; NSt-LD, non-structural limb defect; O, omphalocele; OD, other defects; PC, Pentalogy of Cantrell; PD, pericardial defect; PDA, patent ductus arteriosus; SSBWC, sternal spinal body wall complex; STBWC, sternal body wall complex; StD, sternal defect; St-SpD, structural spinal defect; ThAb, thoracoabdominoschisis; ThG, thoracogastroschisis; UCD, umbilical cord defect; VSD, ventricular septal defect.
Table 10.
Special Cases (n = 3).
| AUTHOR(S) | Case / Gender | BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Angoulvant et al., 2011 [51] |
Case 96 ♂ |
- | - | NR | + | + | ASD, APVR | - | NR | Incomplete PC | CHD |
| Hubbard et al., 2018 [85] |
Case 143 ♀ |
- | - | + | NR | NR | VSD, SCA, ASD | + | Ecc, CrfD, CP | PC | EC |
| Martadiansyah et at., 2025 [103] |
Case 165 C2, ♀ |
UICD | + | + | + | + | ASD, TF, PDA | Type 2 | NR | EC complicated by PC | PC Class 1 BSA Type VIII STBWC IV |
ASD, atrial septal defect; APVR, anomalous pulmonary venous return; BWD, body wall defect; CD, cardiac defects; CHD, congenital heart disease; CP, cleft palate; CrfD, craniofacial dysmorphism; DD, diaphragmatic defect; EC, ectopia cordis; Ecc, encephalocele ExEC, external ectopia cordis; NR, not reported; OD, other defects; PC, Pentalogy of Cantrell; PD, pericardial defect; SCA, single coronary artery; UCD, umbilical cord defect; UICD, umbilical incomplete central defect; VSD, ventricular septal defect.
Table 11.
Summary of Literature Reviewed: Carnivore Cases Classification and Proposed Diagnosis Following Critical Data Analysis.
Table 11.
Summary of Literature Reviewed: Carnivore Cases Classification and Proposed Diagnosis Following Critical Data Analysis.
| AUTHOR(S) | Case / Species/ Gender |
BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Butler, 1960 [127] |
Case 1 D, ♂ |
UH | NR (-) |
NR | + | NR | NR | + | NR | CDH an UH | PC Class 3 |
| Bellah et al., 1989 [128] |
Case 2 D, C1, ♀ |
(SUICD) | NR (-) |
+ | + | + | VSD | Type 3 | NR | CAWD, StD, DD, PD and CD | PC Class1 |
| Case 3 D, C2, ♀ |
(SUICD) | NR (-) |
+ | + | + | VSD | Type 3 | NR | CAWD, StD, DD, PD and CD | PC Class1 | |
| Case 4 D, C3, ♂ |
(SUICD) | NR (-) |
+ | + | + | VSD | Type 3 | NR | CAWD, StD, DD, PD and CD | PC Class1 | |
| Case 5 D, C4, ♂ |
(SUICD) | NR (-) |
+ | + | + | - | Type 3 | NR | CAWD, StD, DD and PD | PC Class 3 | |
| Case 6 D, C5, ♂ |
(SUICD) | NR (-) |
+ | + | + | - | Type 3 | NR | CAWD, StD, DD and PD | PC Class 3 | |
| Benllock-González and Poncet, 2015 [129] |
Case 7 D, ♂ |
UH | NR (-) |
+ | + | + | PDA, PLCVC | Type 3 | NR | Sternal cleft associated with PC | PC Class1 |
| Khan et al., 2019 [130] |
Case 8 D, ♂ |
UH | NR (-) |
+ | + | + | NR | - | NR | PPDH | PC Class 3 |
| Williams et al., 2020 [131] |
Case 9 D, ♂ |
DRM (SUICD) |
NR (-) |
+ | + | + | NR | Type 3 | NR | Incomplete PC | PC Class 3 |
| Hennink et al., 2021 [132] |
Case 10 D, ♂ |
UH | NR (-) |
+ | + | + | NR | - | Pericardial pseudocyst | Unusual PPDH associated with a pericardial pseudocyst | PC Class 3 |
| So et al., 2023 [108] |
Case 11 D, C1, ♂ |
ThAb | NR (+) |
+ | + | + | NS | Type 1 | St-LD, | PC | PC Class 3 BSA TYPE V STLBWC III |
| Case 12 D, C2, ♂ |
Ab | NR (+) |
+ | + | NR | NS | - | NR | PC | PC Class 3 BSA TYPE VIII STBWC IV |
|
| Ozdemir-Salci and Yildirim 2024 [133] |
Case 13 D, ♂ |
ThAb | NR (+) |
+ | - | - | - | Type 2 | NR | Thoracic EC, sternal agenesis, partial ectopia hepática and fissure abdominalis | BSA TYPE VI STBWC III |
| Cózar et al., 2025 [104] |
Case 14 D, ♀ |
ThAb | + | + | + | + | MVS, ASD, HLV, TVD | Type 1 | BCh, PP, ABS | PC Class 1 BSA TYPE VI STBWC III ABS |
PC Class 1 BSA TYPE VI STBWC III |
| Case 15 D, ♂ |
ThAb | + | + | + | + | GH, VSD, RVH | Type 1 | SP, St-SpD, NSt-GuD |
BSA TYPE V SSBWC III PC Class 1 |
PC Class 1 BSA TYPE V SSBWC III |
|
| Case 16 D, ♂ |
LThAb | - | + | + | - | RVH | Type 4 | NSt-SpD, NSt-GuD | PC Class 2 | PC Class 2 | |
| López et al., 2015 [134] |
Case 17 Ct, ♂ |
- | NR (-) |
NR | + | + | Dc | + | HF | Cardiac malposition (EC) | EC |
| Eiger et al., 2019 [135] |
Case 18 Ct, ♀ |
UH | NR (-) |
+ | + | + | NR | Type 3 | NR | StD with PC | PC Class 3 |
| Kokkinos and Pratschke, 2022 [136] |
Case 19 Ct, ♀ |
(SUICD) | NR (-) |
+ | + | + | AVS, BAV, DA | Type 3 | Ect, SL, BG, IDBK | PC with Ect | PC Class 1 |
Ab, abdominoschisis; ABS, amniotic band syndrome; ASD, atrial septal defect; AVS, aortic valve stenosis; BAV, bicuspid aortic valve; BCh, bilateral cheiloschisis; BG, bilobed gallbladder; BSA, body stalk anomaly; BWD, body wall defect; CDH, congenital diaphragmatic hernia; CAWD, cranioventral abdominal wall defect; CD, cardiac defects; Ct, cat; GH, globular heart; D, dog; DA, dextroposition of the aorta; Dc, dextrocardia; DD, diaphragmatic defect; DRM, diastasis of the abdominal recti muscles; Ect, ectrodactyly; ExEC, external ectopia cordis; HF, hepatic fibrosis; HLV, hypoplasia of the left ventricle; IDBK, increased distance between the kidneys and the adrenal glands; LThAb, lateral thoracoabdominoschisis; MVS, mitral valve stenosis; NR, non reported; NS, non studied; NSt-GuD, non structural genitourinary defects; NSt-SpD, non structural spinal defect OD, other defects; PD, pericardial defect; PDA, patent ductus arteriosus; PLCVC, persistent left cranial vena cava; PP, primary palatoschisis; PPDH, peritoneo-pericardial diaphragmatic hernia; RVH, right ventricular hypertrophy; SL, Split liver; SP, secondary palatoschisis; SSBWC, spinal sternal body wall complex; STBWC, sternal body wall complex; StD, sternal defect; St-LD, structural limb defect; St-SpD, structural spinal defect; SUICD, supraumbilical incomplete central defect; ThAb, thoracoabdominoschisis; TVD, tricuspid valve dysplasia; UCD, umbilical cord defect; UH, umbilical hernia; VSD, ventricular septal defect.
Table 12.
Summary of Literature Reviewed: Porcine Cases Classification and Proposed Diagnosis Following Critical Data Analysis.
Table 12.
Summary of Literature Reviewed: Porcine Cases Classification and Proposed Diagnosis Following Critical Data Analysis.
| AUTHOR(S) | Case / Species/ Gender |
BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Martín-Alguacil and Avedillo, 2020 [105] |
Case 20 C1, ♂ |
(ThAb) | + Short ACP DUV HUA |
+ | + | + | ASD | Type 1 | EcC | Cantrell Syndrome | PC Class 1 BSA Type VI STBWC III |
| Case 21 C2, ♀ |
(ThAb) | + Short ACP DUV |
+ | + | + | VSD, GH | Type 1 | EcL | Cantrell Syndrome | PC Class 1 BSA Type VI STBWC III |
|
| Case 22 C3, ♂ |
(ThAb) | + Short ACP DUV HUA |
+ | + | + | VSD, GH | Type 1 | NR | Cantrell Syndrome | PC Class 1 BSA Type VI STBWC III |
|
| Case 23 C4, ♂ |
(ThAb) | + Short ACP DUV SUA |
+ | + | + | ASD, AMV, SCA | Type 1 | LAM | Cantrell Syndrome | PC Class 1 BSA Type VI STBWC III |
|
| Case 24 C5, ♀ |
(ThAb) | + Short ACP DUV |
+ | + | + | HAs, TGA, VSD | Type 1 | NR | Cantrell Syndrome | PC Class 1 BSA Type VI STBWC III |
|
| Case 25 C6, ♀ |
(ThAb) | + Short ACP DUV |
+ | + | + | ASD | Type 1 | NR | Cantrell Syndrome | PC Class 1 BSA Type VI STBWC III |
ACP, abnormal coiling pattern; AMV, atresia of the mitral valve; ASD, atrial septal defect; BSA, body stalk anomaly; BWD, body wall defect; CD, cardiac defects; GH, globular heart; DD, diaphragmatic defect; DUV, dispersed umbilical vessels; EcC, ectopic caecum; EcL, ectopic liver; ExEC, external ectopia cordis; HAs, hypoplastic auricles; HUA, hypoplastic umbilical artery; LAM, liver amorphous mass without lobulation; NR, non reported; OD, other defects; PD, pericardial defect; SCA, single coronary artery; STBWC, sternal body wall complex; StD, sternal defect; SUA, single umbilical artery; TGA, transposition of the great arteries; ThAb, thoracoabdominoschisis; UCD, umbilical cord defect; VSD, ventricular septal defect.
Table 13.
Summary of Literature Reviewed: Classification and Proposed Diagnosis of Ruminant Cases Following Critical Data Analysis.
Table 13.
Summary of Literature Reviewed: Classification and Proposed Diagnosis of Ruminant Cases Following Critical Data Analysis.
| AUTHOR(S) | Case / Species/ Gender |
BWD | UCD | StD | DD | PD | CD | ExEC | OD | AUTHOR’S DIAGNOSIS | PROPOSED DIAGNOSIS |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Hiraga and Abe, 1986 [137] |
Case 26 Cf, C1, ♀ |
- | NR (-) |
+ | NR | (+) | DbA, CVCD | + | AADT, NSt-SpD | Cervical EC | EC |
| Case 27 Cf, C2, ♀ |
- | NR (-) |
+ | NR | (+) | DbA, CVCD | + | AADT, CP | Cervical EC | EC | |
| Case 28 Cf, C3, ♂ |
- | NR (-) |
+ | NR | (+) | DbA, CVCD, VAD | + | AADT, NSt-SpD | Cervical EC | EC | |
| Case 29 Cf, C4, ♂ |
- | NR (-) |
+ | NR | (+) | DbA, CVCD, PDA | + | AADT | Cervical EC | EC | |
| Case 30 Cf, C5, ♀ |
- | NR (-) |
+ | NR | (+) | DbA, VAD, SCA | + | AADT, NSt-SpD | Cervical EC | EC | |
| Case 31 Cf, C6, ♀ |
- | NR (-) |
+ | + | (+) | DbA, CVCD, SCA | + | AADT, NSt-SpD, CP | Cervical EC | EC | |
| Case 32 Cf, C7, ♂ |
- | NR (-) |
+ | NR | (+) | DbA, CVCD, VAD | + | AADT, NSt-SpD, CSt | Cervical EC | EC | |
| Case 33 Cf, C8, ♂ |
- | NR (-) |
+ | NR | (+) | DbA, CVCD | + | AADT, NSt-SpD | Cervical EC | EC | |
| Windberger et al., 1992 [138] |
Case 34 Cf, ♂ |
- | NR (-) |
+ | NR | NR | CVCD, SPV | + | Chromosomal aberrations | Cervical EC | EC |
| Hiraga et al., 1993 [137] |
Case 35 Cf, C1, ♂ |
- | NR (-) |
+ | NR | + | GH, DbA, CVCD, VAD, SPV | + | St-SpD, NSt-GuD, CP | Cervico-pectoral EC | EC |
| Case 36 Cf, C2, ♀ |
- | NR (-) |
+ | NR | + | GEH, SPV, RAV | + | NSt-SpD, NSt-GuD, CP | Cervico-pectoral EC | EC | |
| Erösüz et al., 1998 [139] |
Case 37 Cf, ♀ |
- | NR (-) |
+ | NR | + | APVR | + | HF, LAM, FK, HHS | Total pectoral EC and and other congenital malformations |
EC |
| Floeck et al. 2008 [140] |
Case 38 Cf, ♀ |
UH | NR (-) |
NR | + | + | ASD, VSD, DORV, PDA | + | SIL | PC with Taussig-Bing syndrome and SIL | PC Class 2 |
| Onda et al., 2011 [141] |
Case 39 Cf, ♀ |
- | NR (-) |
+ | NR | NR | CHt, DTV | + | NR | Cervical EC | EC |
| Cerqueira et al., 2024 [142] |
Case 40 Lm, C1, ♂ |
- | NR (-) |
+ | NR | + | NR | + | NR | Complete Thoracic EC | EC |
| Case 41 Lm, C2, ♂ |
- | NR (-) |
+ | NR | + | NR | + | CtD | Complete Thoracic EC | EC |
AADT, aortic arch dog type; APVR, anomalous pulmonary venous return; ASD, atrial septal defect; BWD, body wall defect; CD, cardiac defects; Cf, calf; CHt, cardiac heterotaxia; CP, cleft palate; CSt, colonic stenosis; CtD, costal defects; CVCD, cranial vena cava duplicated; GH, globular heart; DbA, double apex; DD, diaphragmatic defect; DORV, double-outlet right ventricle; DTV, dysplasia of the tricuspid valve; ExEC, external ectopia cordis; FK, fibrotic kidneys; GEH, grossly enlarged heart; HF, hepatic fibrosis; HHS, hyperplastic and hard spleen; Lm, Lamb; LAM, liver amorphous mass without lobulation; NSt-GuD, non-structural genitourinary defect; NSt-SpD, non-structural spinal defect; NR, non reported; OD, other defects; PD, pericardial defect; PDA, patent ductus arteriosus; RAV, right azygos vein; SCA, single coronary artery; SIL, situs inversus of the liver; SPV, single pulmonary vein; StD, sternal defect; St-SpD, structural spinal defect; UCD, umbilical cord defect; UH, umbilical hernia; VAD, vena azygos duplicated; VSD, ventricular septal defect.
Table 14.
Comparative Embryological Summary of Ventral Body Wall Defects in Humans and Dogs: Developmental Origins, Timing and Characteristic Features.
Table 14.
Comparative Embryological Summary of Ventral Body Wall Defects in Humans and Dogs: Developmental Origins, Timing and Characteristic Features.
| Defect | Embryologic Origin | Timing (Human) | Timing (Dog) | Characteristic features |
|---|---|---|---|---|
| Omphalocele | Failure of midgut return after physiologic herniation | Weeks 6-10 | ~ Days 30-35 | Sac-covered herniation at umbilicus |
| Supraumbilical defect | Failure of lateral plate mesoderm fusion at ventral midline | Days 14-18 | Days 14-35 | Multisystem anomalies (sternum, diaphragm, pericardium, abdominal wall) |
| Sternal defect | Incomplete fusion of paired sternal bars (somatic mesoderm) | Days 14-18 | Days 14-35 | Sternal cleft or agenesis |
| Diaphragmatic defect | Abnormal septum transversum and pleuroperitoneal membrane incorporation | Days 14-18 | Days 14-35 | Ventral diaphragmatic gaps, often with Cantrell’ spectrum |
| Gastroschisis | Localized disruption of lateral body wall folding | Weeks 4-6 | ~ Days 30-35 | Paraumbilical opening, no sac, isolated defect |
| Rectus diastasis | Incomplete fusion of linea alba (lateral plate mesoderm) | Days 14-18 | Days 14-35 | Separation of rectus muscles, no true wall defect |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



