
Submitted:
01 January 2026
Posted:
04 January 2026
You are already at the latest version
Abstract
Immunotherapy has transformed cancer management. Patients receiving immune checkpoint inhibitors frequently experience concurrent pain and sleep disturbances that affect quality of life, treatment adherence, and overall survival. Nursing interventions addressing both symptoms remain poorly defined. This scoping review searched the Scopus, ScienceDirect, PubMed, and CINAHL for updates from 2019 to 2025 following PRISMA-ScR guidelines; ten studies were included (randomized controlled trials, systematic reviews, and observational studies for all cancers since focusing on melanoma alone would not give enough results. Nurse-led interventions included education, physical therapies (massage, reflexology, acupressure), behavioral approaches, and digital platforms (telehealth, electronic patient-reported outcomes). The patients achieved moderate short-term pain reductions, significantly improved quality of life, enhanced treatment adherence, and reduced emergency department visits by up to 45%. However, only 2/10 studies used validated instruments to measure sleep quality, and none designed primary interventions specifically targeting sleep disturbances in patients receiving immunotherapy. Long-term sustainability of pain interventions was questionable, with most effects attenuating beyond eight weeks except for psycho-educational approaches. Future research should develop integrated, nurse-delivered interventions addressing pain and sleep as interconnected symptoms, with extended follow-up periods and enhanced accessibility across diverse healthcare settings. Validated instruments to measure sleep quality should be employed.
Keywords:
cancer
; immunotherapy
; immune checkpoint inhibitors
; pain management
; sleep
; nursing interventions
; sleep quality
; psycho-educational
; quality of life
; melanoma
Simple summary
Cancer patients receiving immunotherapy frequently experiences two interconnected problems: chronic pain and sleep disturbances that significantly compromise their quality of life and treatment outcomes. While nurses have developed various interventions to address pain alone, no integrated approaches exist that target both symptoms together in immunotherapy treated patients. This review examined ten recent studies on nursing interventions for cancer pain management and assessed whether sleep quality was considered in these interventions. The findings reveal that educational programs and counseling delivered by nurses produced the most sustained improvements, while physical therapies like massage provided rapid but short-lived relief. Digital tools that allow patients to report symptoms from home showed promise in reducing emergency visits and improving treatment adherence. However, a critical gap remains: most interventions focused solely on pain, with only two studies measuring sleep quality and none specifically designed for immunotherapy patients. These findings highlight the urgent need for nurse-led interventions that address pain and sleep as interconnected symptoms, with better tools to track both problems simultaneously. Future research should develop and test integrated approaches that can be delivered across diverse healthcare settings, ensuring all cancer patients benefit from comprehensive symptoms management.
1. Introduction
Cancer pain affects approximately 60% of patients with advanced malignancy, with nearly 20% experiencing moderate to severe pain that significantly impacts their quality of life and treatment adherence [1]. Sleep disturbances present an equally significant burden, particularly in patients receiving immune checkpoint inhibitors (ICIs), a revolutionary cancer immunotherapy approved since 2011 that reinvigorates the host immune system to combat tumor cells, including melanoma [2]. Recent evidence indicates that 51.9% of ICI treated patients experience clinically relevant sleep disturbances, and the mean Pittsburgh sleep quality index (PSQI) Score was 7.54 ± 5.39), with sleep disturbances prevalence in the broader cancer population ranging from 25% to 59% [3,4].
The clinical significance of these symptoms extends beyond patient comfort. Sleep disturbances are independent predictors of worse progression-free and overall survival rates in cancer patients on ICI including melanoma [5], being potentially mediated by elevated proinflammatory cytokines, such as interleukins and tumor necrosis factor (IL-1, IL-6, TNF-α) that regulate sleep wake homeostasis and promote tumor progression [3]. Independent predictors of sleep disturbances included Eastern Cooperative Oncology Group (ECOG) performance status ≥1 (Odds ratio or OR 2.33, P=0.015), second line therapy or beyond (OR 2.43, p=0.021), and ≥2 metastasis sites (OR 2.10, p= 0.021) [3], similarly, inadequate pain management not only increases suffering but compromises treatment effectiveness [1].
Nursing interventions for cancer pain by itself have been extensively studied, with a comprehensive scoping review identifying 22 types of nursing support from 72 studies [1]. Education programs constitute the most researched intervention (31 studies), followed by physical interventions (massage, reflexology, exercises), cognitive behavior approaches, and comfort nursing strategies that integrate physiologic, psychologic, and social dimension [6]. However, a critical gap exist: while nursing interventions demonstrate short-term effectiveness, long-term sustainability remains controversial and unproven [7]. More importantly, no integrated approaches addressing both pain and sleep simultaneously in ICI-treated patients has been designed, despite their shared inflammatory mechanisms [3] and high co-prevalence in this population [1,4].
Current patient-reported outcome (PRO) instruments inadequately capture ICI-specific symptoms, with 29% of adverse events remaining uncovered/unaddressed [4]. Instruments used to report PRO symptom-related toxicities covered 45% of the most frequently reported AEs, whereas 23% of AEs were partially covered and 29% were not covered at all. Of non-covered AEs, 59% referred to the dermatologic system. Partially covered AEs related to endocrine and specific types of pain [4]. These symptoms may be caused or enhanced by ICIs. Innovative technology-based approaches, such as the cancer pain monitoring system (CAPAMOS), have shown promise in reducing symptoms and emergency visits [8]; however, their application to integrated pain sleep management in ICI remains unexplored. Furthermore, while specialized oncology nurses effectively manage ICI toxicities through education, symptoms monitoring and evidence-based triage tools [9], interventions for community and non-specialized healthcare settings remain underdeveloped.
Therefore, this scoping review aimed to update nursing interventions for cancer pain management in patients receiving immunotherapy and to examine to what extent sleep quality has been assessed or targeted by these interventions for cancer patients in general, including melanoma. The review seeks to identify effective strategies, characterize technology-based approaches, examine integrated symptom management models, and highlight gaps requiring future investigation.
2. Materials and Methods
This scoping review was conducted and reported in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guidelines [10].
2.1. Search Strategy
A comprehensive search was conducted across four major electronic databases: Scopus, ScienceDirect, MEDLINE/PubMed, and CINHAL (Cumulated Index to Nursing and Allied Health Literature). It utilized a combination of keywords, including ("nursing intervention" OR "nurse-led" OR "oncology nursing" OR "nursing care") AND ("cancer" OR "neoplasm " OR "malignancy" OR "tumor") AND ("immunotherapy" OR "immune checkpoint inhibitor " OR "cancer treatment") AND ("pain" OR "sleep quality" OR "sleep disturbance" OR "symptom management"). The search started from January 2019 to November 2025, as the team is interested in updated literature so this manuscript can be more focused and concise. This is also the typical time span that a scoping review is generally performed. We used the preferred reporting items for systematic reviews and meta-analyses (PRISMA) methodology. The search was for all cancers to ensure generalizability and to give enough results.
2.2. Inclusion Criteria and Exclusion Criteria
Inclusion criteria are: quantitative, qualitative, or mixed methods research on cancer patients receiving ICI therapy or studies whose findings are applicable to patients on immunotherapy; nursing interventions for pain and/or sleep management; reported outcomes on pain intensity, pain control, sleep quality, or related to PROs published in English between 2019 to 2025. Exclusion criteria are: unrelated to nursing interventions or not meeting inclusion criteria. Given that preliminary searches focusing exclusively on ICI-specific populations yielded insufficient studies for a comprehensive scoping review, we adopted a pragmatic approach by including (1) studies specifically conducted in ICI-treated populations with cancer, AND (2) studies in general cancer populations where nursing interventions were feasible for adaptation to immunotherapy settings based on:
- Mechanism of action (symptom management principles)
- Nursing delivery models (education, physical therapies, technology-based)
- Symptom overlap between general cancer and ICI populations.
Of the 10 included studies [9,11,12,13,14,15,16,17,18,19], 4 (40%) were ICI-specific [9,12,13,18], while 6 (60%) examined general cancer populations with interventions deemed transferable to ICI contexts [11,14,15,16,17,19]. No minimum follow-up duration was specified in the inclusion criteria, as this scoping review aimed to map the breadth of available evidence, regardless of study duration. However, follow-up periods were systematically extracted and documented to assess the existing evidence base for the long-term sustainability of nursing. Two authors (O.A. and P.T.) independently reviewed eligible study of title and abstract screening, followed by full-text assessment. Any discrepancies or disagreements were resolved through discussion and re-examination of the articles. A third researcher (E.Y.) was available to arbitrate if consensus could not be reached.
2.3. Risk of Bias Assessment Tool
Two independent reviewers (O.A. and P.T.) extracted data using a standardized form, with discrepancies resolved through discussion with a third reviewer (E.Y.) if necessary. Due to the heterogeneous nature of the included studies (randomized controlled trials, systematic reviews, and observational studies with varying methodologies), a formal quality assessment was not performed; however, study characteristics including design type, sample size, and outcome measures were systematically documented.
3. Results
3.1. Characteristics of Selected Studies
The systematic search across PubMed/MEDLINE, Scopus, ScienceDirect, and CINAHL databases yielded 485 records. After removal of duplicated titles and checking abstracts and full tests, 10 studies were included in the final review (Figure 1). These comprised two randomized controlled trials (RCTs) [11,12], four systematic reviews and meta-analyses [13,14,15,16], and four observational studies [9,17,18,19](Table 1). Studies were conducted across multiple countries: five from China [11,12,16,17,19], one from Denmark [18], one from Canada [14], one from South Korea [15] and two multi-country collaborations [9,13]. The combined sample included approximately 4,300+ patients from primary studies and 55+ patients from RCTs and systematic reviews [13,14,15,16]. Cancer types varied, with melanoma [13,18] being one of the most common pathologies.
3.2. Nursing Intervention Types and Components
Thematic analysis identified categories of nursing interventions: educational, physical, cognitive-behavioral, integrated symptoms management, and technology-based approaches. Intervention characteristics are detailed in Table 2.
3.2.1. Educational Interventions
Six studies examined education interventions delivered by oncology nurses [9,11,13,14,15,17]. Individualized 20–30-minute consultations incorporated baseline quality of life screening, symptom anticipation counseling, and personalized care planning [17].
Mind mapping is a combination of images and logical thinking in the form of pictures and text. It was used as structured teaching tool to present pain education and perioperative care precautions [11]. Nurses created and used it to structure pain-education content. Mind maps visually organize:
- ▪ Pain mechanisms
- ▪ Expected postoperative pain trajectory
- ▪ Analgesic options
- ▪ Non-pharmacological pain strategies
- ▪ Self-management steps
Psycho-educational interventions achieved medium short-term effect sizes for pain reduction (Hedge’s=0.43, P˂0.001) and significant improvements in pain management knowledge (g=0.91, P˂0.001)[15]. Long-term effects were small but significant (g=0.25, P=0.022), though sustainability remained controversial [15].
3.2.2. Physical Interventions
A systematic review of 17 RCTs evaluated physical non pharmacological [16]. Massage therapy showed a standardized mean difference (SMD) of −1.0 (95% CI: −1.08 to −0.92; P<0.001) with high heterogeneity (I²=88%)[16]. Reflexology, aromatherapy and acupressure also significantly reduced cancer related pain (all P˂0.001)[16]. Physical interventions achieved medium short term effect sizes (g=0.47) but only small non-significant long-term effects (g= 0.16)[15].
3.2.3. Cognitive-Behavioral and Integrated Interventions
Personalized nursing programs combining symptom assessment, psychological support, and lifestyle counseling results in significantly greater quality of life improvements (∆+ 13.2 ± 7.6 vs + 5.1 ± 6.8, P˂0.001)[17]. Treatment adherence improved (91.2% vs 78.6%, P=0.006) with fewer unplanned healthcare visits (12.4% vs 23.4%, P=0.014)[17]. Weekly symptom self-reported questionnaires tracking 16 symptoms over three weeks revealed pain prevalence decreased from 73.8% to 48.5% (34.3% reduction), while insomnia decreased from 53.1% to 44.6% (16.0% reduction) [19].
3.2.4. Technology Based Approaches
An eHealth PRO monitoring system using tablet-based PRO version of the common terminology criteria for adverse events (PRO-CTCAE) achieved 100% patient satisfaction with ≥90% agreement on tool usefulness [18]. However; 30-40% of patients expressed concerns about lack of clinician review [18]. An ePRO follow up model with automated alerts demonstrated significant benefits: serous immune related adverse effects (irAEs) occurred in 20.6% vs 33.6% (Hazard ratio or HR=0.51, P=0.01), emergency department (ED) visits were 16.3 % vs 29.9% (HR=0.46, P=0.01), and treatment discontinuations was 3.6% vs 11.0% (HR=0.30, P=0.02)[12]. Telehealth interventions significantly reduced pain severity (SMD -0.54, P˂0.05) but showed no significant differences in hospitalizations [14].
3.3. Outcomes and Effectiveness (Table 3)
3.3.1. Pain Outcomes
Nursing-led non pharmacological interventions demonstrated moderate short term effect sizes for pain reduction (g=0.39; 95 % CI: 0.25-0.52; P˂0.001) across 22 studies [15]. Long-term pain effects were substantially diminished (g= 0.10;95% CI: -0.05 – 0.26; P=0.187), except for psycho-educational interventions which maintained small but significant effects (g=0.25, P=0.022)[15]. All five physical intervention modalities significantly reduced cancer pain (P˂0.001), with acupuncture showing the largest effect (SMD -2.09) and massage showing the most consistent results (I2=0%)[16]. Visual analog scale pain scores were significantly lower in pain-education nursing groups (P˂0.05), with ≥40% pain reduction achieved [11].
There are many practical difficulties that nurses encounter in pain management [20,21]. Researchers are continually trying to resolve them by improving the knowledge of the nurses and these should be included in the nursing training curriculum and continuous professional development after graduation [22].
3.3.2. Sleep Quality Outcomes
Critical evidence gap identified: only 2 of 10 studies explicitly measured sleep quality using validated instruments [17,19]. Sleep disturbances affect 51.9% of ICI-treated patients (mean PSQI score: 7.54±5.39), with independent predictors including ECOG performance status ≥1 (Odds ratio (OR) 2.33, P=0.015), second-line or beyond therapy (OR 2.43, P=0.015), and ≥2 metastasis sites (OR 2.10, P= 0.021)[19]. Sleep disturbances independently predict worse progression free and overall survival in ICI recipients [19]. Insomnia prevalence decreased from 53.1% (week 1) to 44.6% (week 3) in one longitudinal study, representing 16% improvement [19]. No studies designed primary interventions targeting sleep disturbances in ICI treated populations, representing a substantial evidence gap [19].
Sleep disturbances and pain have been extensively studied in the general cancer population—with established interventions such as cognitive behavioral therapy for insomnia (CBT-I) demonstrating large effect sizes, and comprehensive symptom-cluster research available across multiple cancer types [23,24]. Ye, et al from China reported 365 patients who completed questionnaires: symptom cluster class 1 ("low symptom burden" class), class 2 ("fatigue-insomnia" class), and class 3 ("high symptom burden" class), with a percentage of 54.5%, 38.6%, and 6.8%, respectively [23]. The quality-of-life score, introversion/extroversion, economic burden, Karnofsky Performance Status, albumin level, and exercise self-efficacy were significantly different among the 3 classes (P<0.05). They concluded that exercise self-efficacy is important for personalized interventions and improving symptom management efficiency [23]. In United States, intervention also helps with sleep quality and negative emotions [25].
Patients receiving ICIs present unique characteristics. Unlike those undergoing traditional chemotherapy, individuals treated with ICIs exhibit sleep disturbances that are independent predictors of progression-free and overall survival [19](Bu et al., 2025). These disturbances are mediated through elevations in pro-inflammatory cytokines (IL-1, IL-6, TNF-α), which simultaneously regulate sleep–wake homeostasis and promote tumor progression [19,26]. This intricate relationship between immunity, sleep, and the tumor microenvironment is distinct to immunotherapy [27] and varies based on cancer type and pre-existing patient factors. Furthermore, circadian rhythm disruptions in immunotherapy patients may offer unique opportunities to optimize treatment outcomes, as sleep quality directly influences immune checkpoint inhibitor efficacy [28]. Given the promising improvements in cancer outcomes with ICIs and the high prevalence of sleep disturbances (51.9%) in this population [19], these knowledge gaps regarding integrated sleep and pain management should not be ignored. Addressing circadian rhythm disturbances and sleep quality may provide novel strategies to enhance immunotherapy efficacy, reduce symptom burden, and improve quality of life in this specific and vulnerable population.
3.3.3. Quality of Life and Patient Satisfaction
Personalized nursing interventions demonstrated comprehensive QoL benefits: overall QoL scores improved +13.2 ± 7.6 points in intervention vs +5.1 ± 6.8 in control (P˂0.001), representing 158% greater improvement [17]. Physical, emotional, cognitive, and social functioning all significantly improved (P˂0.01). Patient satisfaction with eHealth PRO platforms was 100% with ≥90% agreements on ease of use [18]. Two of three reactive telehealth studies reported improved quality of life, and all telehealth interventions showed reduction in symptom severity [14].
3.3.4. Health Services Utilization
Emergency department visits were reduced by 45% (16.3% vs 29.9%, HR 0.46, P=0.01) with ePRO monitoring [12]. Treatment discontinuation was reduced by 67 % (3.6% vs 11.0%, HR 0.30, P = 0.02)[12]. Mean follow up time was reduced by 77% (8.2 ±3.9 vs 36.1 ±15.3 minutes, P˂0.001)[12]. However, no statistically significant differences in hospitalizations or unscheduled clinic visits were found between nurse led telehealth and usual care groups [12].
3.4. Implementation Factors and Future Research
Specialized oncology nurses effectively manage ICI toxicities for different types of cancer through evidence-based education, systematic assessment, nurse led clinics, and specialized triage protocols, though efficacy in community settings remains underdeveloped [9]. Digital literacy disparities were identified as a primary limitation, with 7.3% eligible patients excluded due to inability to use smartphones or computers [12]. Inadequate integration of PRO data into clinical workflows was another limiting factor [18]. Single-center study designs may limit generalizability to lower resource settings [17].
Only 2 of 10 studies measured sleep quality [17,19]. Most studies had follow up duration of ≤8 weeks, with only one achieving 6 months [14,17,19]. Nursing interventions demonstrated short-term effectiveness but long-term sustainability remains controversial [15]. Current PRO instruments inadequately capture ICI specific symptoms with 29% of adverse events remaining unaddressed, 50% of studies were conducted in China with limited representation from low resources settings and community healthcare environment [11,12,16,17,19].
This scoping review focuses on ICIs. There are other useful studies in general in the literature as well, e.g. the pain-sleep symptom cluster [29,30], massage therapy [31] and other non-pharmacological methods for insomnia [32,33]. Studies on chemotherapy in the past may also guide future immunotherapy research [34,35], which also linked perturbations in immune-inflammatory pathways by chemotherapy with insomnia among cancer patients [36].
4. Discussion
4.1. The Current Situation
ICI is increasingly used in treatment for various cancers [37]. It is interesting to know how the treatment of pain and insomnia caused or aggravated by ICI was reported in the literature globally. The present report provides a concise summary of the global view, with useful updated references for healthcare providers of different disciplines. Similar analogy can be applied to other cluster symptoms such as anxiety and depression, and in different countries [38]. In fact, androgen deprivation therapy or chemotherapy can also be associated with symptom clusters [39].
An illustrative case involves a 76-year-old man who experienced severe pain from a right femoral metastasis of melanoma despite receiving ICI. The pain was so severe that he could not sleep for several days. The patient was instructed to adjust his morphine over the weekend by a healthcare provider phoning him twice a day to monitor his response. An anti-emetic, stool-softener and laxative were also prescribed, to decrease his side effects from morphine which were not dealt with by family doctor. His pain lessened and he finally got a good sleep on Sunday. In the following week, a single-fraction radiotherapy was given. His quality of life was maintained for 4 months before dying of the cancer. The learning points were:
- The timely dedicated care can be offered by a nurse practitioner, member of the palliative care team (nurse or physician), family doctor, oncologist in the Canadian healthcare system. This highlights the importance of early palliative care referral, which should have been arranged by his rural family doctor at the same time of referral to the oncology service.
- How can we work smarter and save healthcare dollars at the same time?
4.2. What Nurse-Led Interventions May Achieve
Only 2 of 10 studies measured sleep quality [17,19] in the past 7 years. Insomnia improved modestly (53.1% to 44.6%) as part of comprehensive nursing care [19]. This research gap is particularly concerning given shared inflammatory mechanisms (IL-1, IL-6, TNF-α) linking sleep, pain, and tumor progression [19]. Current PRO instruments inadequately capture ICI-specific symptoms, with 29% of adverse events unaddressed [13], likely contributing to under recognition of sleep disturbances.
Personalized nursing programs combining symptom assessment, psychological support, and lifestyle counseling achieved 158% greater quality of life improvement than usual care (+13.2% vs +5.1%, P<0.001)[17,42], with significant improvements across physical, emotional, cognitive, and social functioning. Treatment adherence improved (91.2% vs 78.6%, P=0.006) and unplanned healthcare visits decreased (12.4% vs 23.4%, P=0.014)[17], demonstrating that comprehensive nursing support enables effective home-based symptom management.
Nurse-led non-pharmacological interventions demonstrated moderate short-term effectiveness for pain reduction (g=0.39, P˂0.001) across diverse modalities [15]. Physical interventions, particularly massage therapy and reflexology, showed robust immediate effects, consistent with previous meta-analyses reporting significant pain relief with complementary therapies in oncology populations [16]. Aromatherapy is also very useful [43]. However, the substantial attenuation of long-term effects (g=0.10, P=0.187) except for psycho-educational interventions underscores a critical limitation: most interventions lack sustainable impact beyond the active treatment period. Educational interventions achieved notable improvements in pain management knowledge (g=0.25, P=0.002), suggesting that patient empowerment through education may facilitate sustained self-management [15]. The use of structured teaching tools such as mind mapping aligns with adult learning principle emphasizing visual and organizational strategies to enhance retention. These findings support the integration of multi-modal educational approaches tailored to individual patient’s needs, particularly given complex and evolving symptom profiles associated with ICI.
4.3. How New Technologies May Transform the Canadian Healthcare
Electronic patient reported outcome (ePRO) systems demonstrated significant improvements in safety outcomes, reducing serious immune-related adverse events by 39% (HR 0.51, P=0.01), emergency department visits by 45% (HR 0.46, P = 0.01), and treatment discontinuations by 67% (HR 0.30, P = 0.02). These benefits likely reflect early detection of the unpredictable, delayed-onset toxicities characteristic of ICIs [9]. Despite high patient satisfaction (100% with ≥90% usability agreement), 30–40% of patients expressed concerns about inadequate clinician review of submitted reports [18], revealing a critical implementation gap. Therefore, we must ensure nurses read these reports and highlight important message to treating clinicians. It is notable that 7.3% of eligible patients were excluded due to digital literacy barriers [12], highlighting equity concerns in technology-dependent interventions.
4.4. Limitations of This Report
Key limitations include heterogeneity of study designs, cancer types, and outcome measures precluding meta-analysis; geographic concentration (50% from China) limiting generalizability [11,12,16,17,19]; predominance of tertiary hospital settings with limited evidence for community care; lack of formal quality assessment; and English-language restriction potentially missing relevant studies. In addition, short follow-up durations (most ≤8 weeks, with only one study achieving 6 months) represent a critical limitation given that ICI therapy typically continues for months to years, with subsequent lines of treatment being common in melanoma and other malignancies. This temporal mismatch between intervention follow-up and treatment duration limits our ability to assess long-term sustainability and cumulative symptom burden management. The predominantly short follow-up periods may underestimate intervention attenuation over time and fail to capture late-onset sleep disturbances or chronic pain patterns characteristic of prolonged immunotherapy. Future studies should incorporate follow-up periods extending beyond 6 months to align with real-world ICI treatment durations and adequately evaluate intervention sustainability.
4.5. Clinical Implications
- Implement routine sleep screening: Given 51.9% prevalence and survival implications, systematically assess sleep disturbances in all ICI-treated patients [19].
- Address digital equity: Develop alternative monitoring strategies for patients with limited digital literacy or access [12].
- Design longitudinal interventions: Incorporate extended follow-up (minimum 6 months, ideally 12+ months) and maintenance strategies aligned with chronic immunotherapy duration rather than time-limited programs. Include booster sessions and ongoing support mechanisms to sustain intervention effects throughout the ICI treatment continuum [9,15].
- Target symptom clusters: Address pain, sleep, and fatigue as interconnected symptoms sharing inflammatory mechanisms [19].
5. Conclusion
Considering the prevalent concurrent pain and sleep disturbances in cancer patients receiving ICIs, integrated management of pain-sleep clusters may be the best target for further nursing interventions. Identifying the differences in symptom burden of ICIs among patients across disease stages, improving coping skills for symptom-related distress, and evidence-based nursing assessment may be powerful measures to improve the management of pain-sleep symptom complexity. Future research must develop nurse-delivered integrated interventions addressing these interconnected symptoms while ensuring equitable access across diverse healthcare settings. Hopefully this updated review can serve as a useful reference at the point of care, not only for nurses, but social workers, pharmacists, and clinicians.
Author Contributions
All authors have contributed to the writing, reading, editing and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable since this is a review, not involving humans or animals.
Informed Consent Statement
Not applicable since this study does not involve humans.
Data Availability Statement
No new data were created.
Conflicts of Interest
Authors declare no conflicts of interest”
Abbreviations
The following abbreviations are used in this manuscript:
| Abbreviations | Full Form |
| BPI | Brief pain inventory |
| CAPAMOS | cancer pain monitoring system |
| CBT-I | Cognitive behavioral therapy for insomnia |
| CI | Confidence interval |
| CINHAL | Cumulated Index to Nursing and Allied Health Literature |
| CRC | Colorectal cancer |
| CTLA-4 | Cytotoxic T-lymphocyte-associated protein 4 |
| ECOG | Eastern cooperative oncology group |
| ED | Emergency department |
| eHealth | Electronic health |
| EORTC QLQ-C30 | European organization for research and treatment of cancer quality of life questionnaire-Core 30 |
| EORTC-QLG-H&N35 | European organization for research and treatment of cancer quality of life questionnaire-head and neck 35 |
| ePRO | Electronic patients reported outcome |
| EQ-5D | Euro-QoL 5-dimension questionnaire, |
| FKSI-DRS | Functional assessment of cancer therapy -kidney symptom index-disease related symptoms |
| GU | genitourinary |
| HADS | Hospital anxiety and depression scale |
| HCC | Hepatocellular carcinoma |
| H&N | Head and neck journal |
| HR | Hazard ratio |
| HRQoL | Health-related quality of life, |
| ICI | Immune checkpoint inhibitor |
| int | Intervention group |
| irAE | Immune related adverse event |
| LCSS | Lung cancer symptom scale |
| N | Sample size |
| NRS | Numeric rating scale |
| PD-1 | Programmed cell death protein 1 |
| PD-L1 | Programmed death-ligand 1 |
| PRISMA-ScR | Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews |
| PRO | Patients reported outcome |
| PRO-CTCAE | Patient reported outcomes version of the common terminology criteria for adverse events |
| PSQI | Pittsburgh sleep quality index |
| QoL | Quality of life |
| RCT | Randomized controlled trial |
| SAS | Self-rating anxiety scale |
| SDS | Self-rating depression scale |
| SMD | Standardized mean difference |
| SMS | Short message service |
| STAI | state-trait anxiety inventory |
| USA | USA: united states of America |
| VAS | Visual analog scale |
| Vs | Versus |
References
- Morikawa, M; Kajiwara, K; Kobayashi, M; Kanno, Y; Nakano, K; Matsuda, Y; et al. Nursing support for pain in patients with cancer: a scoping review. Cureus 2023, 15(11), e38161938. [Google Scholar] [CrossRef]
- Dine, J; Gordon, R; Shames, Y; Kasler, MK; Barton-Burke, M; Burke, S; Lee, J; Patel, H; Wong, A; Chen, L; et al. Immune checkpoint inhibitors: an innovation in immunotherapy for the treatment and management of patients with cancer. Asia Pac J Oncol Nurs. 2017, 4(2), 127-135. [Google Scholar] [CrossRef] [PubMed]
- Aktepe, B. Sleep Quality and Its Determinants Among Patients with Metastatic Cancer Treated with Immune Checkpoint Inhibitors: A Two-Center Cross-Sectional Study. Medicina 2025, 61(12), 2131. [Google Scholar] [CrossRef] [PubMed]
- Colomer-Lahiguera, S; Bryant-Lukosius, D; Rietkoetter, S; Martelli, L; Ribi, K; Fitzpatrick-Lewis, D; Sherifali, D; Orcurto, A; Juergens, R; Eicher, M. Patient-reported outcome instruments used in immune-checkpoint inhibitor clinical trials in oncology: a systematic review. J Patient Rep Outcomes 2020, 4(1), 58. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y; Zhang, Z; Gong, Q; Yang, G; Wu, Z; Yang, Z; Zhao, X. Analysis of primary nursing intervention for elderly patients with cancer pain on the improvement of potential risk and pain degree. Am J Transl Res. 2021, 13(10), 11890-11898. [Google Scholar]
- Miao, J; Wang, Y; Li, X; Zhang, L; Chen, H; Liu, Q. Effectiveness of comfort nursing combined with continuous nursing on patients with colorectal cancer chemotherapy. Evid Based Complement Alternat Med. 2022, 2022, 9647325. [Google Scholar] [CrossRef]
- Alfaro-Díaz, C; García-Sánchez, R; López-Montesinos, MJ; Martínez-Galiano, JM; Fernández-Alcántara, M; Cabañero-Martínez, MJ; Cabrero-García, J; Richart-Martínez, M; Andreu-Periz, L; Cabañero-Martínez, A; et al. Effectiveness of nursing interventions for patients with cancer and their family members: a systematic review. J Fam Nurs. 2022, 28(2), 95-114. [Google Scholar] [CrossRef]
- Yoshida, S; Sato, F; Tagami, K; Takahashi, S. Clinical Trial Protocol: Randomized Controlled Trial of Cancer Pain Monitoring System (CAPAMOS) in Patients with Advanced Cancer. Open J Nurs. 2022, 12(2), 113-124. [Google Scholar] [CrossRef]
- Mirzadeh, P; Pituskin, E; Au, I; Sneath, S; Buick, CJ. Cancer Immunotherapy: The Role of Nursing in Patient Education, Assessment, Monitoring, and Support. Curr Oncol. 2025, 32(7), 392. [Google Scholar] [CrossRef]
- Tricco, AC; Lillie, E; Zarin, W; O’Brien, KK; Colquhoun, H; Levac, D; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern Med. 2018, 169(7), 467-473. [Google Scholar] [CrossRef]
- Li, S; Zhang, Y; Wang, L; Chen, J; Liu, H; Zhao, Q. The effect of pain-education nursing based on a mind map on postoperative pain score and quality of life in patients with colorectal cancer. Medicine (Baltimore) 2023, 102(19), e33562. [Google Scholar] [CrossRef]
- Zhang, L; Shah, N; Li, J; Patel, S; Wang, Y; Chen, X; Brown, S; Lee, H; Gupta, R; Thompson, J; et al. Efficiency of electronic health record assessment of patient-reported outcomes after cancer immunotherapy: a randomized clinical trial. JAMA Netw Open. 2022, 5(3), e224427. [Google Scholar] [CrossRef] [PubMed]
- Hall, ET; Singhal, S; Dickerson, J; Gabster, B; Wong, HN; Aslakson, RA; Schapira, L; AAHPM Research Committee Writing Group. Patient-reported outcomes for cancer patients receiving checkpoint inhibitors: opportunities for palliative care—a systematic review. J Pain Symptom Manage 2019, 58(1), 137-156.e1. [Google Scholar] [CrossRef] [PubMed]
- Kwok, C; Lee, CF; Choi, KC; Chan, CW; Chair, SY; So, WK; Leung, DY; Ho, SS; Cheng, KK; Yates, P; et al. Nurse-led telehealth interventions for symptom management in patients with cancer receiving systemic or radiation therapy: a systematic review and meta-analysis. Support Care Cancer 2022, 30(9), 7119-7132. [Google Scholar] [CrossRef] [PubMed]
- Park, YJ; Lee, MK. Effects of nurse-led nonpharmacological pain interventions for patients with cancer: a systematic review and meta-analysis. J Nurs Scholarsh. 2022, 54(4), 422-433. [Google Scholar] [CrossRef]
- Yan, S; Liu, H; Wang, Y; Chen, L; Zhao, Q; Li, X; Zhang, M; Zhou, Y; Huang, J; Wu, P; et al. Assessment of non-pharmacological nursing strategies for pain management in tumor patients: a systematic review and meta-analysis. Front Pain Res. 2025, 6, 1447075. [Google Scholar] [CrossRef]
- Liu, Y.; Guo, H. Impact of personalized nursing on the quality of life in lung cancer patients. Front Oncol. 2025, 15, 650066. [Google Scholar] [CrossRef]
- Tolstrup, LK; Pappot, H; Bastholt, L; Zwisler, AD; Dieperink, KB; Johansen, C; Nielsen, DL; Andersen, MH; Schmidt, H; Larsen, MB; et al. Patient-reported outcomes during immunotherapy for metastatic melanoma: mixed methods study of patients’ and clinicians’ experiences. J Med Internet Res. 2020, 22(4), e14896. [Google Scholar] [CrossRef]
- Bu, L; Zhang, H; Chen, Y; Wang, X; Liu, Q; Zhao, M; Li, S; Huang, Y; Zhou, J; Fang, L; et al. A longitudinal study on symptom distress and management of transhepatic arterial interventional chemotherapy combined with targeted therapy and immunotherapy based on patient self-reported outcomes. Holist Integr Oncol. 2025, 4(1), 1-9. [Google Scholar]
- Al-Ghabeesh, SH; Bashayreh, IH; Saifan, AR; Rayan, A; Alshraifeen, AA. Barriers to Effective Pain Management in Cancer Patients From the Perspective of Patients and Family Caregivers: A Qualitative Study. Pain Manag Nurs. 2020, 21(3), 238–244. [Google Scholar] [CrossRef]
- Saifan, AR; Bashayreh, IH; Al-Ghabeesh, SH; Batiha, A; Alrimawi, I; Al-Saraireh, M; Al-Momani, MM. Exploring factors among healthcare professionals that inhibit effective pain management in cancer patients. Central European Journal of Nursing and Midwifery 2019, 10(1), 967–976. [Google Scholar] [CrossRef]
- Al Omari, D; Alhabahbeh, A; Subih, M; Aljabery, A. Pain management in the older adult: The relationship between nurses' knowledge, attitudes and nurses' practice in Ireland and Jordan. Appl Nurs Res. 2021, 57, 151388. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y; Zeng, K; Qin, L; Luo, J; Liu, S; Miao, J; et al. Differential characteristics of fatigue–pain–sleep disturbance–depression symptom cluster and influencing factors of patients with advanced cancer during treatment: a latent class analysis. Cancer Nurs. 2025, 48(5), 352–359. [Google Scholar] [CrossRef] [PubMed]
- Sheikh-Wu, SF; Downs, CA; Anglade, D. Interventions for managing a symptom cluster of pain, fatigue, and sleep disturbances during cancer survivorship: a systematic review. Oncol Nurs Forum 2020, 47(4), E107-E119. [Google Scholar] [CrossRef] [PubMed]
- Bai, L; Shi, Y; Zhou, S; Gong, L; Zhang, L; Tian, J. Intervention model under the Omaha system framework can effectively improve the sleep quality and negative emotion of patients with mid to late-stage lung cancer and is a protective factor for quality of life. Am J Cancer Res. 2024, 14(3), 1278–1291. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Miaskowski, C; Cooper, BA; Dhruva, A; Dunn, LB; Langford, DJ; Cataldo, JK; et al. Evidence of associations between cytokine genes and subjective reports of sleep disturbance in oncology patients and their family caregivers. PLoS One 2012, 7(7), e40560. [Google Scholar] [CrossRef]
- Balachandran, DD; Ganjoo, K; Patel, S; Chai, PR; Sullivan, M; Wang, K; et al. The impact of immunotherapy on sleep and circadian rhythms in patients with cancer. Front Oncol. 2023, 13, 1295267. [Google Scholar] [CrossRef]
- Zarogoulidis, P; Petridis, D; Kosmidis, C; Sapalidis, K; Nena, L; Matthaios, D; Papadopoulos, V; Perdikouri, EI; Porpodis, K; Kakavelas, P; et al. Non-small-cell lung cancer immunotherapy and sleep characteristics: the crossroad for optimal survival. Diseases 2023, 11(1), 26. [Google Scholar] [CrossRef]
- Arbour, C; Hjeij, D; Bilodeau, K.; 2024 — Nursing Sleep Education (Includes Pain-Related Sleep Disruption) Arbour. Managing sleep disruptions during cancer: practical tips for patient education. Can Oncol Nurs J 2024, 34(4). [Google Scholar]
- Brink. Nursing Management of Symptom Clusters (Pain + Sleep) Brink A. Understanding and managing symptom clusters: insights for oncology nurses. Oncol Nurs News 2024. [Google Scholar]
- Miladinia, M; Jahangiri, M; Kennedy, AB; Fagerström, C; Tuvesson, H; Safavi, SS; et al. Determining massage dose-response to improve cancer-related symptom cluster of pain, fatigue, and sleep disturbance: a 7-arm randomized trial in palliative cancer care. Palliat Med. 2023, 37(1), 108-119. [Google Scholar] [CrossRef] [PubMed]
- Munir, S; Connolly, M; Davies, AN. Non-pharmacological interventions for sleep disturbance (“insomnia”) in patients with advanced cancer: a scoping review. Support Care Cancer 2025, 33, 486. [Google Scholar] [CrossRef] [PubMed]
- Nissen, ER; Neumann, H; Knutzen, SM; Henriksen, EN; Amidi, A; Johansen, C; von Heymann, A; Christiansen, P; Zachariae, R. Interventions for insomnia in cancer patients and survivors—a comprehensive systematic review and meta-analysis. JNCI Cancer Spectr. 2024, 8(3), pkae041. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Schimmel, A; Kober, KM; Paul, SM; Cooper, BA; Harris, C; Shin, J; Hammer, MJ; Conley, YP; Dokiparthi, V; Olshen, A; et al. Sleep disturbance is associated with perturbations in immune-inflammatory pathways in oncology outpatients undergoing chemotherapy. Sleep Med. 2023, 101, 305-315. [Google Scholar] [CrossRef]
- Zhou, Z; Yang, Y; Sun, J; Dong, Y; Zhu, M; Wang, T; Teng, L. Heterogeneity of pain-fatigue-sleep disturbance symptom clusters in lung cancer patients after chemotherapy: a latent profile analysis. Support Care Cancer 2024, 32(12), 821. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y; Duan, Y; Zhou, Y; Yi, S; Dai, C; Luo, X; Kang, Y; Wan, Z; Qin, N; Zhou, X; Liu, X; Xie, J; Cheng, ASK. The Level of Psychological Distress Is Associated With Circadian Rhythm, Sleep Quality, and Inflammatory Markers in Adolescent and Young Adults With Gynecological Cancer. Cancer Nurs;Epub 2025, 48(5), E289–E295. [Google Scholar] [CrossRef] [PubMed]
- Tai, P; Alqaisi, O; Al-Ghabeesh, S; et al. Immune Checkpoint Inhibitors in Merkel Cell Carcinoma of the Skin: A 2025 Comprehensive Review. Cancers (Basel) Published. 2025, 17(19), 3272. [Google Scholar] [CrossRef]
- Song, L; Su, Z; He, Y; Pang, Y; Zhou, Y; Wang, Y; Lu, Y; Jiang, Y; Han, X; Song, L; Wang, L; Li, Z; Lv, X; Wang, Y; Yao, J; Liu, X; Zhou, X; He, S; Zhang, Y; Li, J; Wang, B; Tang, L. Association between anxiety, depression, and symptom burden in patients with advanced colorectal cancer: A multicenter cross-sectional study Top of Form. Cancer Med. 2024, 13(11), e7330. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, Y; Yan, Q; Zhou, J; Yao, X; Ye, X; Chen, W; Cai, J; Jiang, H; Li, H. Identification of distinct symptom profiles in prostate cancer patients with cancer-related cognitive impairment undergoing androgen deprivation therapy: A latent class analysis. Asia Pac J Oncol Nurs 2024, 11(6), 100497. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dennis, K; Harris, G; Kamel, R; Barnes, T; Balboni, T; Fenton, P; Rembielak, A. Rapid Access Palliative Radiotherapy Programmes. Clin Oncol (R Coll Radiol) 2020, 32(11), 704–712. [Google Scholar] [CrossRef] [PubMed]
- O'Reilly, E; Golshan, M; Chng, N; Bartha, LR; Drummond, L; Hoegler, D; Becker, N; Mou, B. Effect of Same-Day Volumetric Modulated Arc Therapy on Resource Utilization in Rapid Access Palliative Radiotherapy Clinics Using a Radiation Oncologist-Initiated Automated Planning Script. Cureus 2025, 17(10), e95165. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wei, M; Yusuf, A; Hsien, CCM; Marzuki, MA. Effects of behavioural activation on psychological distress among people with cancer: A systematic review and meta-analysis. Int J Nurs Stud;Epub 2025, 164, 104983. [Google Scholar] [CrossRef] [PubMed]
- Xie, SR; Ma, L; Xu, XY; Zhou, S; Xie, HM; Xie, CS. Effects of Aromatherapy on Physical and Mental Health of Cancer Patients Undergoing Radiotherapy and/or Chemotherapy: A Meta-Analysis. Chin J Integr Med 2024, 30(5), 449–457. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow diagram for Preferred reporting items for systematic review and meta-analysis-scoping review (PRISMA-ScR).
Figure 1.
Flow diagram for Preferred reporting items for systematic review and meta-analysis-scoping review (PRISMA-ScR).
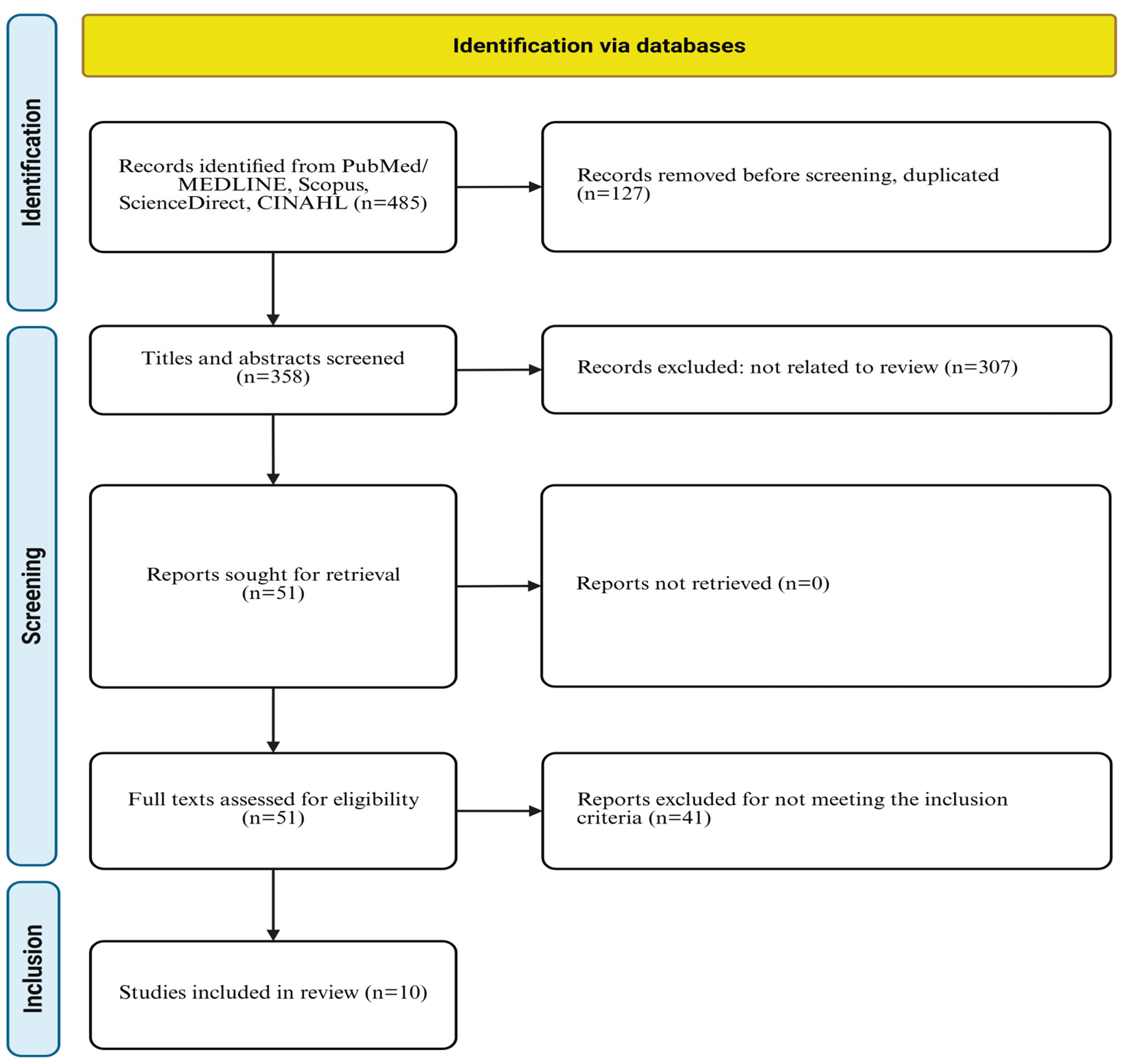

Table 1.
Characteristics of the ten studies.
| Authors/ years | Country | Study design | Settings | Cancer type | Sample size | Age (years) | ICIs used |
|---|---|---|---|---|---|---|---|
| Tolstrup [18] | Denmark | Mixed methods RCT | University hospital | Metastatic melanoma | N= 70 (57 surveyed) | Median 65 | Immunotherapy |
| Hall [13] | USA/multi country | Systematic review | Multi center trails | Melanoma, lung, GU, H&N | 15 RCTs | 44.1-67.3 | Nivolumab, pembrolizumab |
| Zhang [12] | China | RCT | 28 Tertiary hospitals | Gastric, esophageal, lung | N=278 (141 int.) | 58.8 ±12.7 | Multiple ICIs |
| Mirzadeh [9] | Canada | Perspective | Clinical practices | All ICI candidates | Review | Not specific | PD-1/PD-L/CTLA-4 |
| Yan [16] | China | Systematic review | Multiple databases | Various cancer types | 1,070 (17 RCTs) | Not specific | Various (review) |
| Kwok [14] | Multiple countries | Systematic review | Multiple settings | Various cancer types | 2,315 (10 studies) | Variable means | Various (review) |
| Liu [17] | China | Retrospective cohort | Hubei cancer hospital | Lung cancer (stage II-IV) | N = 291 (137 int.) | 65.1±7.9 vs 65.5±8.4 | Chemo, targeted, immune |
| Bu [19] | China | Longitudinal study | Tertiary hospital | Hepatocellular carcinoma | N = 130 | 46-69 (66.2%) | Immune+ targeted+ interventions |
| Li [11] |
China | Retrospective observational | 2 tertiary hospitals | Colorectal cancer | N = 100 (50 int.) | Not specified | Adjuvant / Chemotherapy |
| Park [15] | South Korea | Systematic review | Multiple databases | Various cancer type | 22 RCTs | 44.1-67.3 | Music, physical, psycho-educational |
CTLA-4: cytotoxic T-lymphocyte-associated protein 4, CRC: colorectal cancer, GU: genitourinary, H&N: head and neck, HCC: hepatocellular carcinoma, ICI: immune checkpoint inhibitor, PD-1: programmed cell death protein 1, PD-L1: programmed death-ligand 1, int.: interventions group, N: sample size, RCT: randomized controlled trial, USA: united states of America, vs: versus.
Table 2.
Intervention details and populations.
| Study | Cancer stage | Intervention type | Key components | Duration | Delivery methods |
|---|---|---|---|---|---|
| Tolstrup [18] | Metastatic | eHealth PRO weekly | Weekly PRO-CTCAE symptoms reporting via tablet from home | Weekly during treatment | eHealth platform (home-based) |
| Hall [13] | Unresectable/metastatic (n=13), adjuvant (n=2) | PRO measurement | Systemic review of 15 ICI trials with PRO data | Various | Various clinical trial questionnaires |
| Zhang [12] | Mixed cancer types | ePRO follow up model with alerts | Questionnaire + image recognition for irAE grading; automated advice for grades 1-2; alert for grades 3-4 | 6 months or until treatment ends | Mobile app/ web-based + image recognition |
| Mirzadeh [9] | Various stages | Nursing education, assessment, monitoring | Patient education (multiple formats), symptoms assessment, nurse-led clinics, support services | Ongoing throughout treatment | In-person, telephone, video, written materials |
| Yan [16] | Various (systematic review) | Non-pharmacological pain management |
Reflexology, aromatherapy, acupressure, massage therapy, acupuncture. | Varied (1990-2023) | In-person therapy sessions |
| Kwok [14] | Various | Nurse-led telehealth | Telephone calls, video consultations, web-based systems, SMS, mobile apps (reactive/scheduled) | ≥ 4 weeks minimum | Telephone, video, web SMS, mobile applications |
| Liu [17] | Stage II-IV (72.3% stages III-IV) | Personalized nursing care |
20-30 minutes baseline consultation + telephone/video follow-ups on days 4 & 10 of each cycle | 8 weeks post-treatment initiation | Telephone & video consultations |
| Bu [19] | Advanced stage | Symptom self-report questionnaires | Symptoms assessment at weeks 1,2,3 using standardized scales | 3 weeks post intervention | Paper-based questionnaires (in-person) |
| Li [11] | Various | Pain education nursing with mind mapping | Nurses used mind map to guide pain education and perioperative care planning | Perioperative and postoperative | Repeated in-person education sessions |
| Park [15] | Various (systematic review) |
Nurse-led Non pharmacological interventions | Music interventions, physical exercises, psycho-educational programs | Various timeframes | Various (nursing delivered) |
CRC: colorectal cancer, eHealth: electronic health, ePRO: electronic patients reported outcome, HCC: hepatocellular carcinoma, ICI: immune checkpoint inhibitor, irAE: immune related adverse event, PRO: patients-reported outcome, PRO-CTCAE: patients reported outcomes version of the common terminology criteria for adverse events, SMS: short message service.
Table 3.
Primary outcomes and key findings in updates of past 7 years.
| Study | Instruments used | Primary outcomes | Future recommendations |
|---|---|---|---|
| Tolstrup [18] | Patients feedback form (13 items), interviews, focus group | Patient/clinician satisfaction, symptom awareness, patient involvement | Standardize PRO measurement; improve clinician-patients communication tracking; multicenter validation |
| Hall [13] | EORTC QLQ-C30 (80%), EQ-5D (67%), FKSI-DRS, LCSS, EORTC QLQ -H&N35 | HRQoL with ICIs vs other therapies | Develop ICI-specific PRO instruments; harmonize outcomes measurement; long-term HRQoL tracking |
| Zhang [12] | PRO-based QoL questionnaire, EORTC QLQ-C30 | Serious irAEs (Grades 3-4), ED visits, QoL, treatment discontinuation | Large-scale RCTs in diverse populations; cost effectiveness studies; digital literacy interventions |
| Mirzadeh [9] | Risk assessment tools, educational frameworks | Early detection of irAEs, patients’ educations effectiveness | Multi-setting evaluation of nursing roles; systematic protocols for early detection; international collaboration |
| Yan [16] | BPI, NRS, VAS | Cancer-related pain reduction | Standardized intervention protocols; dose-response studies; combination therapy trails; 6–12-month outcomes |
| Kwok [14] | EORTC QLQ-C30, EQ-5D, various symptom scales | Health services use, QoL, symptom severity | More nurse-led telehealth RCTs; consistent outcomes measurement; reactive vs scheduled comparison; cost-effectiveness |
| Liu [17] | EORTC QLQ-C30, HADS, STAI | Overall QoL improvement at 8 weeks | Multicenter RCTs with extended follow-up; diverse populations; cost-benefit analysis; mechanistic studies |
| Bu [19] | Symptom assessment scale (Likert 0-6) | Dynamic symptom changes over 3 weeks | Extended longitudinal studies; larger sample sizes; earlier intervention (pre-treatment); trajectory modeling |
| Li [11] | VAS (pain), SAS/SDS (anxiety/depression), EORTC QLQ-C30 | Postoperative pain, QoL, emotional distress, comfort | Multicenter trials; long-term follow-up; blinded design; economic evaluation; adaptability to different settings |
| Park [15] | Various pain measure, HRQoL instruments | Pain reduction, knowledge of pain management, pain coping | Standardized intervention protocols; optimal dosing guidelines; mechanism studies; patient-centered outcomes |
BPI: brief pain inventory, ED: emergency department, EORTC QLQ-C30: European organization for research and treatment of cancer quality of life questionnaire-Core 30, EORTC QLQ-H&N35: European organization for research and treatment of cancer quality of life questionnaire-head and neck 35, EQ-5D: Euro-QoL 5-dimension questionnaire, FKSI-DRS: functional assessment of cancer therapy -kidney symptom index-disease related symptoms, HADS: hospital anxiety and depression scale, HRQoL: health-related quality of life, irAEs: Immune related adverse events, ICI: immune checkpoint inhibitor, LCSS: lung cancer symptom scale, NRS :numeric rating scale, PRO: patients reported outcome, QoL: quality of life, RCT: randomized controlled trial, SAS: self-rating anxiety scale, SDS: self-rating depression scale, STAI: state-trait anxiety inventory, VAS: visual analog scale.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



