
Submitted:
01 January 2026
Posted:
02 January 2026
You are already at the latest version
Abstract
In people with dementia, sleep disturbances and circadian rhythm disruption, as well as heightened stress responses and behavioral and psychological symptoms of dementia (BPSD), constitute major drivers of nighttime agitation, delirium, falls, infections, emergency visits, hospitalization, and institutionalization, thereby sharply increasing caregiving burden and healthcare and long-term care costs. At the same time, conventional sleep hygiene and BPSD management approaches tend to rely on complex self-management models that presuppose “correct instruction,” which are prone to implementation failure in dementia due to impairments in executive function, attention, and memory. The purpose of this paper is not to present new efficacy data, but rather to reorganize existing evidence on sleep and stress/BPSD management from the perspective of “core active ingredients,” and to propose a reconfigured intervention framework that can realistically function in dementia care settings: the Dementia-adapted Sleep & Stress Management (D-SSM) framework. The proposed program retains three minimal core elements: (1) anchoring daily rhythms (fixed wake time and morning light exposure); (2) proactive removal of triggers for nighttime agitation and delirium (e.g., pain, constipation, dehydration, sleep deprivation); and (3) consistent, reassurance-oriented communication and standardized responses based on the DICE approach. This design suppresses reliance on complex self-judgment and multi-stage behavior change tasks. Future evaluation should prioritize implementation-focused outcomes that are directly linked to costs—such as nighttime caregiving frequency, incidence of delirium and BPSD, psychotropic medication use, and emergency visits—rather than focusing exclusively on falls or cognitive indices.
Keywords:
dementia
; sleep disturbance
; circadian rhythm
; behavioral and psychological symptoms of dementia (BPSD)
; stress management
; non-pharmacological intervention
; implementation science
; caregiver support
1. Introduction
Sleep disturbances in people with dementia—such as difficulty initiating sleep, nocturnal awakenings, and day–night reversal—and disruptions of circadian rhythms frequently lead to nighttime wandering, falls, and caregiver exhaustion. Through delirium and BPSD (including irritability, agitation, depression, and apathy), these disturbances readily precipitate acute exacerbations and hospitalization. These relationships can be conceptualized as a cascade (Figure 1), in which sleep and circadian disruption function as upstream destabilizing factors that, through nighttime confusion and stress-related BPSD, propagate sequentially to falls, delirium, emergency visits, hospitalization, and functional decline. The relationship between sleep and neurodegeneration is bidirectional, and disruption of sleep and circadian rhythms has been suggested to trigger symptom worsening (Musiek & Holtzman, 2016; Wang & Holtzman, 2020).
Similarly, the emergence and exacerbation of stress responses and BPSD accelerate cognitive and ADL decline, increase emergency visits and hospitalization, and lead to the addition or escalation of psychotropic medications—thereby elevating fall and delirium risk—and represent one of the most powerful drivers of increased medical and long-term care costs. Rather than being a direct expression of neurodegeneration per se, BPSD often emerge and worsen as reactions to physical discomfort, environmental changes, and interpersonal stressors, as summarized in multiple reviews and guidelines (Livingston et al., 2017; Kales et al., 2015). This framing aligns with the structure depicted in Figure 1, which conceptualizes sleep disturbance, physical discomfort, environmental factors, and inconsistent caregiving responses as interacting elements that amplify adverse outcomes including BPSD.
Accordingly, international guidelines position non-pharmacological interventions as the first-line approach for BPSD, with a focus on identifying causes and modifying environments and interactions (Livingston et al., 2017; Kales et al., 2015).
However, sleep hygiene and stress coping strategies often implicitly assume that individuals can understand instructions, monitor themselves, and flexibly adjust behavior. In dementia, impairments in attention, working memory, and executive function undermine these assumptions even at mild-to-moderate stages. As a result, theoretically sound interventions may fail to achieve sufficient adherence and dosage, producing an “implementation gap.” This pattern mirrors findings from the PrAISED trial in the exercise intervention field, where theoretically intensive interventions did not necessarily improve primary outcomes (Booth et al., 2018; Harwood et al., 2023).
Rather than interpreting this as evidence that sleep and stress interventions are ineffective, this paper reframes the problem as one of design mismatch and proposes a framework for reconstructing sleep and stress/BPSD management in a form that can function under the cognitive constraints of dementia.
2. Evidence Base for Sleep and Stress Management
2.1. Sleep and Neurodegeneration: Controlling “Conditions for Worsening,” Not Treatment
Sleep and neurodegeneration are bidirectionally linked: circadian and sleep-structure disruption are associated with neurodegenerative processes, while pathological progression further destabilizes sleep (Musiek & Holtzman, 2016; Wang & Holtzman, 2020). However, large-scale randomized controlled trials demonstrating that sleep interventions definitively slow disease progression after dementia diagnosis are not yet established. Clarifying this boundary is essential to avoid unrealistic therapeutic expectations.
Accordingly, the most defensible goal of sleep interventions is not halting pathology, but controlling “conditions for worsening” that precipitate nighttime agitation, delirium, falls, and hospitalization, thereby containing costs and preventing caregiving breakdown.
2.2. Stress, Emotion, and BPSD Management: Non-Pharmacological Interventions as First Line
BPSD readily emerge and worsen in response to physical discomfort (pain, constipation, dehydration, infection), sleep deprivation, environmental changes, and communication mismatches. Thus, management centers on iterative cycles of “cause exploration → non-pharmacological modification → evaluation” (Kales et al., 2015).
Prior research repeatedly emphasizes core elements of BPSD management: (1) systematic identification of physical and environmental triggers; (2) proactive removal of discomfort; (3) reassurance-oriented communication that avoids negation or correction; and (4) shared and standardized response strategies within care teams. Kales et al. conceptualize BPSD not as “symptoms” but as “meaningful behavioral responses,” and propose the Describe–Investigate–Create–Evaluate (DICE) framework as a first-line non-pharmacological approach (Kales et al., 2015).
3. Why Standard Sleep Hygiene and Stress Coping Often Fail in Dementia
3.1. Cognitive and Executive Constraints
Sleep diaries, stimulus control, staged behavior change, and selection of stress coping strategies all require self-monitoring, self-regulation, and planning. In dementia, these cognitive resources are constrained, rendering even “correct” interventions ineffective through reduced adherence.
3.2. Nighttime Problems as Environmental Design Issues, Not Patient Effort
Nighttime awakenings and agitation are difficult to control by patient intention alone. Inconsistent caregiver responses increase unpredictability, amplifying emotional load and BPSD. Evidence suggests that the meaning attributed to stimuli and interactions strongly shapes behavioral responses, and that standardized responses can improve emotional stability and engagement (Cohen-Mansfield et al., 2010).
3.3. More Is Not Always Better: The Implementation Gap Highlighted by PrAISED
As shown in exercise interventions, intensity and complexity can backfire in dementia by reducing adherence and increasing fatigue or refusal (Harwood et al., 2023). The same principle applies to sleep and stress interventions: designs that “work with minimal components” are central.
3.4. Redefining Design Assumptions for Sleep and Stress Interventions
Although many theoretically sound non-pharmacological interventions for sleep disturbance and stress/BPSD exist, they often fail in dementia care settings. This gap reflects not flawed content, but mismatched design assumptions.
Standard sleep hygiene and stress coping strategies implicitly presuppose: (1) introspective awareness of one’s state; (2) selection among multiple behavioral options; and (3) adaptive adjustment and maintenance of behavior. These abilities depend heavily on attention, working memory, and executive function, which deteriorate early in dementia.
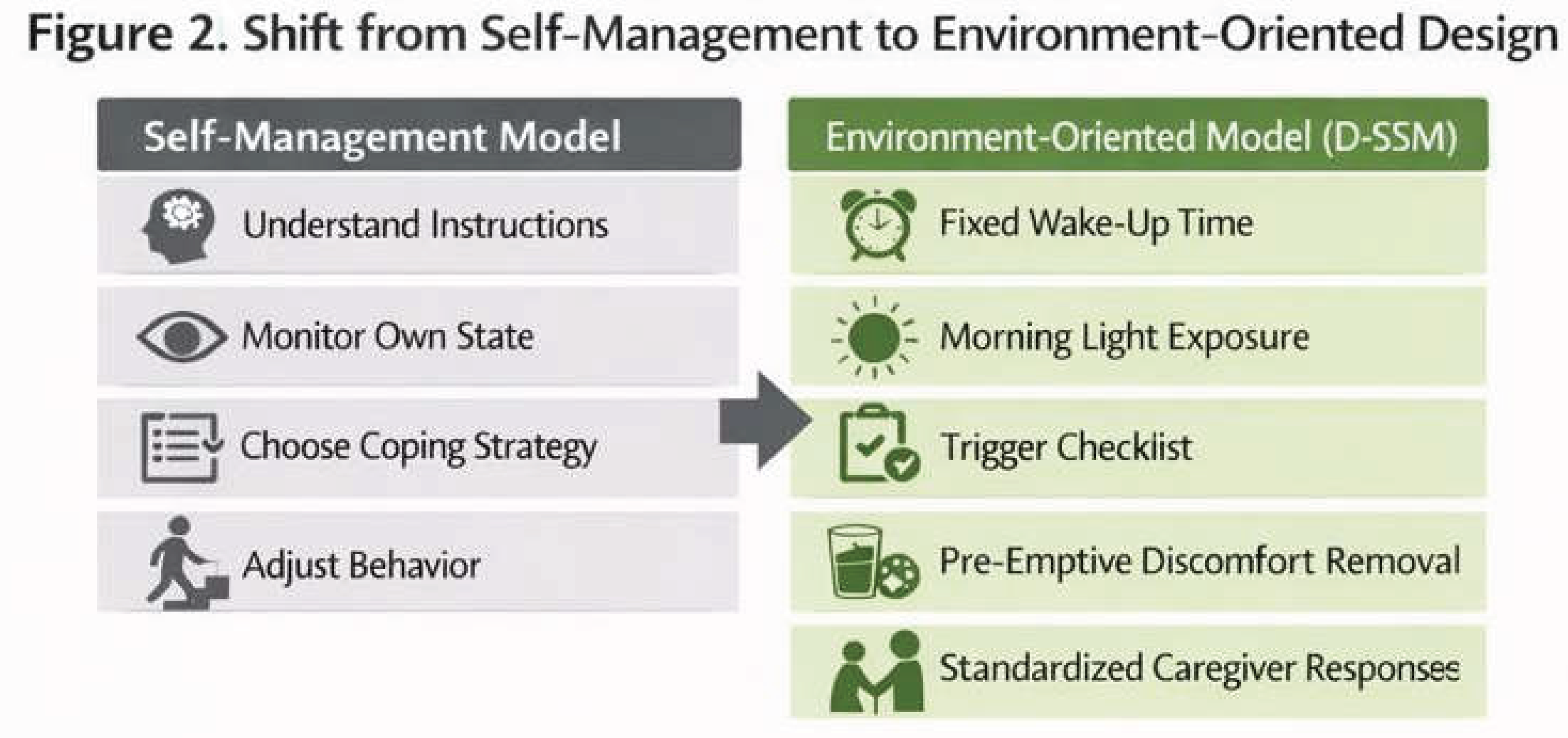
Consequently, interventions that are “correct but complex”—such as sleep diaries, stimulus control, staged behavior change, and coping-skill selection—lose effectiveness through reduced adherence. This mirrors the structural pattern observed in the PrAISED trial. Therefore, in dementia-targeted sleep and stress interventions, the core challenge is not enabling patients to choose correct behaviors, but designing environments that minimize choice and judgment. This shift is not an indictment of patient effort, but a design transformation that maximizes feasibility under cognitive decline. The conceptual contrast is illustrated in Figure 2.
4. Dementia-Adapted Sleep & Stress Management Framework (D-SSM)
This section presents a reproducible intervention protocol that retains the active ingredients of sleep and stress/BPSD management while suppressing assumptions—self-judgment and complex behavior change—that are fragile in dementia. Based on the design philosophy in Figure 2, D-SSM reframes sleep and stress management as a caregiving environment design problem rather than a patient self-regulation task.
4.1. Design Principles
The framework is built on four principles:
Principle 1: No requirement for patient judgment or choice
Decisions regarding implementation, order, and timing are fixed and not delegated to the patient. This is not a convenience measure but a prerequisite for adherence under executive dysfunction.
Principle 2: Prioritize upstream rhythm anchors
Intervention centers on fixed wake time and morning light exposure rather than optimization of bedtime behaviors.
Principle 3: Treat BPSD as reactions, not outcomes
Behavioral issues are addressed as responses to physical discomfort or environmental stressors, with standardized proactive trigger removal.
Principle 4: Embed caregiver support as a condition of intervention
Monitoring, verbal reassurance, environmental adjustment, and shared response strategies are integral components of the intervention itself.
5. D-SSM Intervention Protocol (for Implementation)
5.1. Overall Structure
- Duration: Continuous (minimum 12 weeks)
- Frequency: Daily (each item requires only a few minutes)
- Recording: Simple caregiver checklist
- Setting: Home or institutional care
5.2. Sleep and Daily Rhythm Module (Three Mandatory Items)
(S1) Fixed wake time (±30 minutes)
Purpose: Establish a circadian anchor.
Implementation: Wake at the same time daily.
(S2) Light exposure within one hour of waking
Purpose: Circadian entrainment and daytime alertness.
(S3) Nap management (≤30 minutes, before 3 p.m.)
Purpose: Maintain nighttime sleep pressure.
5.3. Stress, Emotion, and BPSD Module (Three Mandatory Items + DICE)
(E1) Systematic check for BPSD triggers
Rationale: BPSD are reactions to modifiable factors (Kales et al., 2015).
(E2) Proactive removal of discomfort
Rationale: Addressing physical discomfort is foundational (Livingston et al., 2017).
(E3) Reassurance-oriented communication
Rationale: Meaning attribution influences behavior (Cohen-Mansfield et al., 2010).
(E4) DICE framework as needed
Rationale: Kales et al. (2015).
5.4. Weekly Standardization Meeting
Once weekly, family or staff briefly share effective responses and standardize communication and environmental adjustments (Cohen-Mansfield et al., 2010; Kales et al., 2015).
5.5. Progression Rule
Avoid adding or complicating items; when symptoms worsen, return to the basic set.
5.6. Key Performance Indicators (Cost-Linked)
Nighttime caregiving frequency, BPSD frequency, psychotropic medication use, emergency visits, and hospitalization.
6. Implications for Research, Practice, and Policy
Focusing exclusively on cognitive outcomes risks underestimating intervention value. Adherence and exposure should be treated as central mechanistic indicators.
7. Conclusion
Sleep disturbances and stress responses/BPSD in dementia are major accelerators of healthcare costs and caregiving breakdown. By redefining these issues as conditions for worsening rather than treatment targets, this paper proposes a minimal, dementia-adapted program (D-SSM) designed for real-world implementation. Future work should prioritize implementation-focused evaluation.
Appendix A
Implementation Manual for People with Dementia
Sleep & Stress / BPSD Management
(An Implementation Guide for Caregiving and Care Settings)
0. Positioning of This Manual
This manual is an implementation guideline that organizes responses to sleep disturbances and stress responses / Behavioral and Psychological Symptoms of Dementia (BPSD) in a form that can be implemented in caregiving and care settings.
This manual is not a treatment manual intended to achieve the following:
- To cure dementia itself
- To stop or reverse disease progression
Instead, this manual has the following primary aims:
- To reduce the frequency and severity of nighttime agitation, delirium, and BPSD
- To prevent acute events such as falls, emergency visits, and hospitalization
- To reduce the number of nighttime responses required of caregivers and to alleviate caregivers’ psychological and physical burden
In other words, this manual is positioned as a minimal and repeatable implementation guide focused on removing conditions that exacerbate sleep- and stress-related problems in dementia.
1. Why Sleep and Stress / BPSD Should Be Treated as an Integrated Set
In dementia care settings, the following chain is often observed:
- Sleep disturbance and breakdown of circadian rhythms
- Nighttime agitation and confusion
- Manifestation of BPSD (irritability, refusal, wandering, etc.)
- Falls, delirium, and emergency visits
- Hospitalization, abrupt decline in ADL, and institutionalization
In this chain, sleep disturbance and BPSD are not independent problems; they are elements that influence each other. In particular, many nighttime problems arise from overlapping factors such as:
- Physical discomfort (pain, constipation, dehydration, urinary urgency, etc.)
- Environmental factors (noise, lighting, temperature, schedule changes)
- Variability in caregivers’ responses
Therefore, rather than treating sleep and stress / BPSD separately, it is practically reasonable from an implementation perspective to design an integrated approach that combines daily rhythm, physical factors, environmental adjustment, and response methods.
2. Basic Principles
This manual is structured around the following four principles. These translate the design principles of the D-SSM framework presented in the main text into on-site implementation guidance.
Principle 1: A design that does not ask the person to make judgments or choices
- Do not leave behavioral choice, memory, or self-regulation to the person
- Fix the contents, order, and timing of what is done
- Avoid exceptional operations as much as possible
Principle 2: Prioritize “waking” over “going to bed”
- Do not center the approach on handling sleepless nights
- Improve nighttime sleep indirectly by stabilizing wake time and the morning environment
Principle 3: Understand BPSD not as “symptoms” but as “reactions”
- Do not interpret anger, refusal, or agitation as intentional behavior
- Treat them as reactions to some form of discomfort or difficulty
Principle 4: Incorporate caregiver stability as an intervention condition
- Do not adopt designs that assume caregiver exhaustion
- Emphasize operations that are short, simple, and shareable among multiple people
3. Daily Items to Implement (Required Set)
A. Sleep and Daily Rhythm Management (Required: 3 items)
A-1. Fixing the Wake Time (±30 minutes)
- Wake up at the same time every day regardless of bedtime
- Do not “adjust” by sleeping in
Check item
- Did the person wake up at the scheduled time today?
A-2. Light Exposure Within One Hour After Waking
- Use natural outdoor light exposure as the default (about 5–15 minutes)
- If difficult, substitute with a bright indoor environment
Check item
- Did the person receive sufficient light after waking?
A-3. Managing Naps
- Limit naps to within 30 minutes
- Keep naps before 3:00 p.m.
- If possible, use a chair rather than a bed
Check item
- Was the nap short and taken early in the day?
B. Stress / BPSD-Related Items (Required: 3 items)
B-1. Checking Physical and Environmental Triggers
Before behavioral problems appear, check the following items:
- Lack of sleep
- Urinary urgency / toileting discomfort
- Constipation
- Possible pain
- Dehydration
- Hunger
- Environmental stimuli such as noise and lighting
- Sudden changes in schedule or environment
If even one applies, respond to it first.
B-2. Preemptive Removal of Discomfort Factors
- Do not make it standard practice to respond only after behavioral problems become apparent
- Adjust physical discomfort and environmental stimuli in advance
Examples:
- If restlessness is observed, first guide to the toilet or provide fluids
- If irritability is high, move to a low-stimulation environment
B-3. Communication That Prioritizes a Sense of Safety
Use the following as principles:
- Do not deny
- Do not correct
- Do not rush
Examples of easy-to-use phrases:
- “It’s okay.”
- “Let’s do it together.”
- “I’m here with you.”
4. Organizing Problems When Nighttime Issues Occur (Simplified DICE)
- Describe: What happened, when, and where
- Investigate: Whether urinary urgency, pain, sleepiness, or environmental stimulation were present
- Create: Environmental adjustment, changes in verbal approach, preemptive responses
- Evaluate: Share and evaluate the response the next day
Records only need to be a simple one-line entry.
5. Weekly Standardization of Responses (Once Per Week)
Once per week, in a short session (about 5 minutes), do the following:
- Share among family or staff what responses worked well
- Standardize verbal approaches and environmental adjustments
The purpose is to prevent responses from becoming person-dependent and to increase predictability.
6. Implementation Cautions (Actions Not Recommended)
As a rule, avoid the following:
- Viewing sleep problems as the person’s responsibility
- Forcing the person to go to bed
- Physically restraining behavior
- Changing responses depending on each situation
- Having a caregiver handle problems alone without support
7. Evaluation Indicators
To evaluate the effectiveness of this manual, use the following indicators:
- Number of nighttime responses required
- Frequency of agitation / irritable behavior
- PRN use or dose increases of psychotropic medications
- Occurrence of falls, emergency visits, and hospitalization
Rather than focusing on sleep duration itself, emphasize changes in care response load and acute events.
8. Limitations of This Manual
This manual does not guarantee the following:
- Cure of dementia
- Elimination of all BPSD
- Stopping of disease progression
However, it may reduce the frequency of events such as nighttime agitation, delirium, falls, hospitalization, and caregiving breakdown.
9. Summary
In responding to sleep- and stress-related problems in people with dementia, the most realistic and implementable strategy is not to address nighttime problems directly, but to stabilize waking and remove discomfort factors.
References
- Amieva, H.; Stoykova, R.; Matharan, F.; Helmer, C.; Antonucci, T. C.; Dartigues, J. F. What aspects of social network are protective for dementia? Not the quantity but the quality of social interactions is protective up to 15 years later. Psychosomatic Medicine 2010, 72(9), 905–911. [Google Scholar] [CrossRef] [PubMed]
- Booth, V.; Hood-Moore, V.; Logan, P.; et al. Promoting activity, independence and stability in early dementia and mild cognitive impairment (PrAISED): Development of an intervention. Clinical Rehabilitation 2018, 32(7), 855–864. [Google Scholar] [CrossRef] [PubMed]
- Cohen-Mansfield, J.; Thein, K.; Dakheel-Ali, M.; Marx, M. S. The underlying meaning of stimuli: Impact on engagement of persons with dementia. Psychiatry Research 2010, 177(1–2), 216–222. [Google Scholar] [CrossRef] [PubMed]
- Harwood, R. H.; Goldberg, S. E.; Brand, A.; et al. Promoting Activity, Independence and Stability in Early Dementia and Mild Cognitive Impairment (PrAISED): A randomised controlled trial. BMJ 2023, 382, e074787. [Google Scholar] [CrossRef] [PubMed]
- Kales, H. C.; Gitlin, L. N.; Lyketsos, C. G. Assessment and management of behavioral and psychological symptoms of dementia. BMJ 2015, 350, h369. [Google Scholar] [CrossRef] [PubMed]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; et al. Dementia prevention, intervention, and care. The Lancet 2017, 390(10113), 2673–2734. [Google Scholar] [CrossRef] [PubMed]
- Musiek, E. S.; Holtzman, D. M. Mechanisms linking circadian clocks, sleep, and neurodegeneration. Science 2016, 354(6315), 1004–1008. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Holtzman, D. M. Bidirectional relationship between sleep and Alzheimer’s disease: Role of amyloid, tau, and other factors. Neuropsychopharmacology 2020, 45(1), 104–120. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
A conceptual cascade linking sleep disturbance, stress responses, and adverse outcomes in dementia. Sleep deprivation and breakdown of circadian rhythms function as upstream destabilizing factors, causing nighttime confusion and stress responses expressed as behavioral and psychological symptoms (BPSD). These reactions increase the risk of falls, delirium, emergency visits, and hospitalization, ultimately accelerating functional decline. Furthermore, physical discomfort, environmental factors, and inconsistency in caregivers’ responses amplify this cascade.
Figure 1.
A conceptual cascade linking sleep disturbance, stress responses, and adverse outcomes in dementia. Sleep deprivation and breakdown of circadian rhythms function as upstream destabilizing factors, causing nighttime confusion and stress responses expressed as behavioral and psychological symptoms (BPSD). These reactions increase the risk of falls, delirium, emergency visits, and hospitalization, ultimately accelerating functional decline. Furthermore, physical discomfort, environmental factors, and inconsistency in caregivers’ responses amplify this cascade.
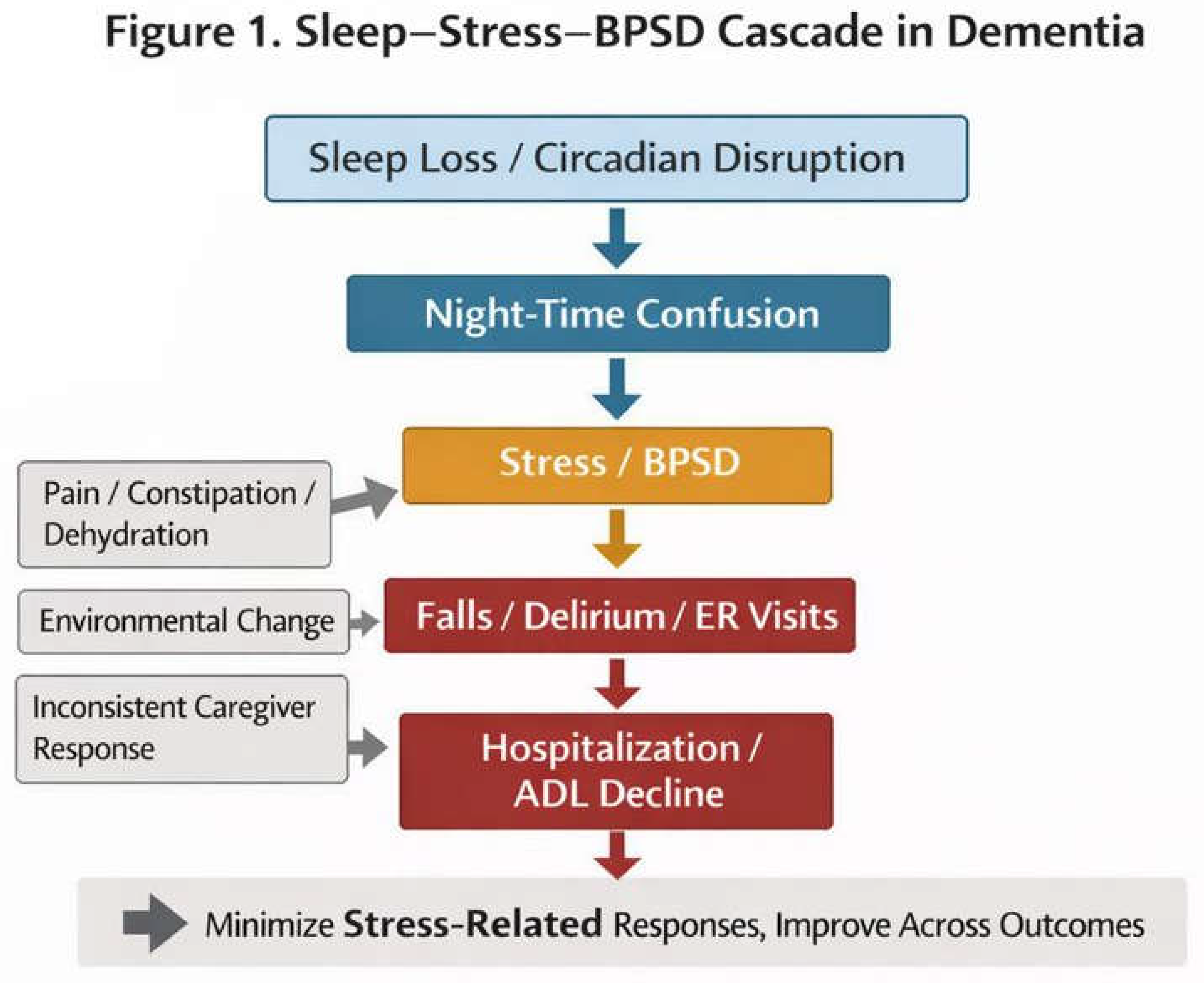
Figure 2.
A design shift in dementia care from self-management interventions to environment-design implementation. Conventional sleep and stress interventions implicitly assume that patients can grasp their own condition, make judgments, and adjust their behavior. In dementia, however, these assumptions often do not hold. The proposed dementia-adapted Sleep & Stress Management framework (Dementia-adapted Sleep & Stress Management: D-SSM) aims to maintain exposure to the core active ingredients while minimizing the cognitive burden required of patients by reallocating the initiative of the intervention to the care environment and caregivers.
Figure 2.
A design shift in dementia care from self-management interventions to environment-design implementation. Conventional sleep and stress interventions implicitly assume that patients can grasp their own condition, make judgments, and adjust their behavior. In dementia, however, these assumptions often do not hold. The proposed dementia-adapted Sleep & Stress Management framework (Dementia-adapted Sleep & Stress Management: D-SSM) aims to maintain exposure to the core active ingredients while minimizing the cognitive burden required of patients by reallocating the initiative of the intervention to the care environment and caregivers.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



