
Submitted:
31 December 2025
Posted:
01 January 2026
You are already at the latest version
Abstract
Background/Objectives: Nutritional risk screening is critical in the management of gynaecologic oncology (GO) surgical patients. Malnutrition is prevalent in this population and is associated with poorer surgical outcomes, including increased morbidity, prolonged hospital stays, and reduced survival rates. Nevertheless, the optimal nutritional screening tools for this patient group remain undefined. Methods: We conducted a narrative review to critically appraise commonly used nutritional screening and assessment tools in surgical GO patients. To highlight practical challenges in accurately identifying at-risk individuals, we incorporated findings from our recent clinical audit. Results: Several nutritional screening and assessment tools were identified. The results varied considerably between tools. The presence of ascites and rapid deterioration in oral intake were frequently overlooked, leading to under-recognition of malnutrition. These issues were corroborated by our audit findings. Emerging strategies including determining body composition from routine preoperative CT scans show promise. Conclusions: Accurate nutritional assessment is imperative to improve surgical outcomes in surgical GO patients. As currently no gold standard currently exists for this population, bespoke approaches to address disease-specific nutritional considerations are urgently needed to identify those at risk and allow for timely nutritional interventions. Integrating CT-based body composition analysis can provide an objective solution, thus requiring further investigation.
Keywords:
gynaecologic oncology surgery
; nutritional screening
; malnutrition
1. Introduction
Malnutrition - referring to undernutrition – is prevalent in women with a gynaecological oncology (GO) diagnosis and is associated with poorer surgical outcomes [1,2,3]. Significant nutritional challenges can arise in this patient group owing to the tumour burden impairing oral intake, including low appetite, early satiety and gastrointestinal symptoms, further exacerbated by disease and treatment-related metabolic demands and side effects. Therefore, prompt identification and management of nutritional risk is paramount [4]. Accurately screening GO surgical patients presents challenges; the impact of ascites on body weight and oral intake, in addition to rapid peri-operative nutritional changes, owing to elevated nutritional requirements, often coupled with reduced appetite, gastrointestinal symptoms, and potential post-operative ileus. These factors can obscure the need for timely specialist nutritional input. This review examines commonly used nutrition screening and assessment tools for GO surgical patients, with a focus on the inpatient setting. We incorporate findings from our recent clinical audit evaluating the accuracy of nutritional screening in this patient group to inform recommendations.
2. Materials and Methods
2.1. Literature Search
A literature search was conducted across the following databases: PubMed, Web of Science and MEDLINE on 23/03/2025. Full search terms and eligibility criteria are presented in Appendix A. In brief, keywords included “nutritional screening” or “nutritional assessment” and “surgery” and “gynaecological oncology”. Studies on nutritional assessment or screening in GO surgical patients in the pre-, peri- or post-operative period were included. A narrative review was undertaken, with studies too heterogeneous in nature to undertake meta-analysis.
2.2. Clinical Audit
A retrospective audit was undertaken to evaluate the accuracy of routine nutritional screening scores compared to formal dietetic assessments in GO surgical patients. The audit was conducted in a UK tertiary specialist centre, where nursing staff performed nutritional screening based on the Malnutrition Universal Screening Tool (MUST) upon admission and weekly thereafter [5]. The MUST score recorded closest to the time of dietetic referral was compared to the GO surgical dietitian's initial assessment (patients under another dietetic team during admission were excluded, n=6). The data, collected from November 2023 to April 2024, was registered in the Local Audit Database (LOC0822).
3. Results
3.1. Literature Review
After removing duplicates, 53 records were screened, of which 25 met inclusion criteria (Figure 1.) A summary of key characteristics for each study is presented in Table 1. The most commonly employed nutritional screening and/or assessment methods were: Nutritional Risk Index -2002 [6,7,8,9]; Malnutrition Screening Tool [10]; Academy of Nutrition and Dietetics - American Society for Parenteral and Enteral Nutrition [10]; Subjective Global Assessment (SGA) [11]; GLIM [11]; anthropometrics [8,11,12,13,14,15,16]; body composition [8,11,17,18,19,20]; patient generated-SGA [9,12,13,17,18]; Malnutrition Universal Screening Tool [14] and biochemical indicators [8,9,12,13,14,16,19,21,22,23,24,25,26,27,28,29,30]. These tools will be discussed within the context of clinical expertise.
Anthropometrics and Body Composition (BC)
Physical measurements were undertaken by several studies, often in tandem with other approaches [8,11,12,13,14,15,16]. Two studies defined a body mass index (BMI) <18.5kg/m2 as malnourished [8,16], while another study employed a cut-off <22kg/m2 [13]. Debate exists regarding the most appropriate BMI cut-off values, particularly for certain ethnicities, age groups and disease states, with no widely accepted GO surgical-specific recommendations [32,33]. Similarly, two studies defined a >5% weight loss in the last six months as malnourished [14,15]; however, many others widely accepted screening tools would not count <10% weight loss in isolation as high risk of malnutrition [5]. Another study calculated percentage weight loss within a one-month period [12]. This underscores the difficulty of relying on a single anthropometric measure to assess nutritional risk. For this reason, additive factors are used in most nutritional screening approaches, as shortly explored. Imperatively, a significant proportion of women with gynaecological cancers experience ascites, which hampers accurate determination of BMI and unintentional weight loss, rendering singular measures likely insufficient.
Body composition (BC) measures offer a more accurate insight into body proportions. This was explored in a number of studies [8,17,18,19,20], some of which also included anthropometrics [11,12]. One study calculated fat mass index (FMI) and fat-free mass index (FFMI) from waist and hip circumference and skinfold thickness pre- and post-GO surgery, showing significant reduction in these parameters, along with BMI [11]. Handgrip strength was measured during hospital admission in one cross-sectional study, which found it predicted malnutrition [12]. Another study measured BC with bioelectrical impedance analysis (BIA) pre-operatively in 70 women with advanced epithelial ovarian cancer, showing significantly lower values in those with residual disease and peri-operative complications [20]. Nevertheless, considering the high volume of ascites in this patient group, the BIA approach may not be the most accurate means of assessing BC. As an alternative, BC can be directly measured from routine clinical CT scans. Two retrospective studies found that BMI and skeletal muscle index (SMI) were significantly decreased post-surgery and were associated with higher radiotherapy toxicities [17,18]. A case note review of ovarian cancer patients treated with debulking surgery and adjuvant chemotherapy found that SMI loss was independently associated with all-cause mortality [19].
Malnutrition Screening Tool (MST)
The MST records self-reported unintentional weight loss (in raw values), and binary response regarding reduced oral intake due to decreased appetite. While simple, it may be less sensitive than MUST [34]. One study found that only 15% of GO patients who screened positive on the MST in the outpatient setting were identified as ‘at risk’ on hospital screening tool [10]. Importantly, in this patient group, fluid shifts may mask dry weight loss.
Nutritional Risk Screening (NRS)-2002
The NRS-2002 consists of initial screening and, if indicated, final screening. Initial screening assesses: BMI, weight loss in the last three months, reduced oral intake in last week and disease severity. It is European Society of Clinical Nutrition and Metabolism (ESPEN) endorsed [35]. In pre-operative hospital screening of GO patients, those identified as malnourished on NRS-2002 had a longer hospital stay [6]. Limitations of NRS-2002 include inconsistent validity in different hospital populations and age groups [34]. Prevalence of pre-operative malnutrition varied between 19-70% according to NRS-2002 in papers identified in this review [7,8]. This variability may be attributed to several clinical factors. For instance, Nasser et al. [8] observed that patients aged >65 years old, with ascites exceeding 500mls and platinum-resistant disease had a significantly higher risk of elevated NRS-2002 scores. These higher scores were, in turn, associated with reduced progression-free and overall survival [8]. Such clinical heterogeneity complicates the interpretation of nutritional risk across the GO surgical population.
Subjective Global Assessment (SGA)
Nutritional parameters in SGA include percentage weight loss in the last two weeks and six months, degree of change in nutrient intake, presence of symptoms affecting oral intake, functional capacity, metabolic demand alongside a physical examination for indices of muscle wasting, loss of subcutaneous fat, and the presence of oedema or ascites. One study that employed the SGA found that 17% of GO surgical patients were mildly or moderately malnourished preoperatively, rising to 34% post-operatively [11]. There were also significant reductions in BMI, waist and hip circumference, triceps thickness, body fat, fat mass, and FMI post-surgery, suggesting that the assessment tool detects nutritional status changes [11]. Notably, the study also assessed nutritional status using the GLIM criteria and found that malnutrition prevalence in the same patient group increased from 7.5% to 15.1% pre- and postoperatively, respectively [11]. This highlights the substantial prevalence of malnutrition amongst GO patients, which is further accentuated by surgery. However, significant variability existed between screening and assessment tools. The SGA was not ubiquitously used in the hospital setting, potentially owing to its complexity.
Patient-Generated Subjective Global Assessment (PG-SGA)
The PG-SGA is completed by the patient. While several studies employed PG-SGA, malnutrition detected varied between 10-57% [12,18]. The observed differences were likely influenced by varying clinical characteristics and the timing of nutritional assessment. This is because PG-SGA assesses dietary changes over the preceding 2-4 weeks, which may inadequately reflect the rapid nutritional deterioration post-surgery. Additionally, questions pertaining to activity levels may be less applicable following major surgery, when patients are typically immobilised or acutely unwell and therefore this tool might not be ubiquitously employed across the GO surgical group. This is an important consideration as onward referrals often depend on nutritional screening scores. Inconsistencies between tools may yield differing responses, potentially impacting nutritional care.
Albumin and other biochemical markers of nutritional status
Biochemical markers were commonly employed by studies and were linked to survival outcomes [16,21,22,23,24,25,26,27,28,29]. However, attributing their findings to nutritional status is challenging, particularly given the retrospective nature of these studies and the confounding effect of the disease burden. One study found that hypoalbuminemia (<35 g/L) did not correlate with percentage weight loss, NRI or MUST nor intra- or post-operative complications or 30-day mortality [14]. Similarly, preoperative albumin was not significantly associated with PG-SGA score in 97 GO patients planned for surgery [13]. Another study found that 27% were malnourished according to albumin levels (≤30 g/L) compared to 47% using PG-SGA [9], with the discordance suggestive of distinct measures.
Clinically, albumin and other biochemical markers are rarely considered direct markers of nutritional status. Albumin is an acute-phase reactant, and its production is downregulated with the metabolic stress of surgery. Further hampering the accuracy of albumin in this patient group is the dilutional effect of ascites and oedema on serum levels. Similarly, other blood markers, such as white cell count and haemoglobin, are too intrinsically linked with the surgery and the underlying disease itself to be considered independent markers of nutritional status. Therefore, biochemical values must be considered within the clinical context. For example, a systematic review of severely undernourished, but otherwise healthy individuals, found serum albumin levels were normal [36].
Academy of Nutrition and Dietetics - American Society for Parenteral and Enteral Nutrition (AND-ASPEN) criteria for malnutrition and Global Leadership Initiative on Malnutrition (GLIM)
The AND-ASPEN criteria for malnutrition include inadequate energy intake, weight loss, muscle and subcutaneous fat loss, fluid accumulation (including ascites) and reduced functional status [37]. While including many pertinent measures, it requires nutritional expertise for calculations and would be challenging to ubiquitously implement within a clinical setting without a dedicated dietitian. One study employed AND-ASPEN criteria for malnutrition, measured by a dietitian, in conjunction with an in-house hospital nutritional screening tool [10]. Despite its comprehensive design, only 4% out of 107 ovarian cancer patients undergoing surgical cytoreduction were identified as malnourished according to AND-ASPEN, compared to 15% with an in-house hospital screening tool [10].
The GLIM recommends a two-step model; the first involves screening and those “at risk” with any validated screening tool, the second employing their diagnostic assessment criteria and severity grading approach [38]. The latter diagnostic assessment includes weight and muscle mass loss, low BMI and reduced food intake along with disease burden [38]. Akin to AND-ASPEN, etiological criteria would necessitate specialist nutritional knowledge, impeding its more global use within the hospital setting. One study employed GLIM criteria and reported a 7.5% and 15.1% prevalence of malnutrition pre- and post-operatively, respectively, which was approximately half that identified by SGA in this cohort [11].
Malnutrition Universal Screening Tool (MUST)
MUST is commonly used, endorsed by ESPEN [33]. It assesses BMI, percentage unintentional body weight loss and actual or anticipated minimal nutritional intake for ≥5 days [5]. Frequently, only those identified as ‘high risk’ of malnutrition meet dietetic referral criteria [5]. Strengths of MUST include its simplicity, strong validation and outperformance of other similar tools [34,39,40].
One retrospective study found no correlation between MUST score and post-operative morbidity [14]. However, the high volume of ascites in these surgical GO patients hampers accurate assessment of both BMI and percentage weight loss. Although mid-upper arm (MAC) could be considered as an alternative, interpreting the degree of undernutrition by this measure remains challenging [35]. From clinical experience, MAC is infrequently employed in hospital wards and patient groups where weight can be obtained, albeit inaccurately. There is also no section in the MUST tool detailing barriers to oral intake outside of minimal intake. Based on clinical experience, the tool lacks specificity for this patient group, prompting further investigation via a local audit.
3.2. Clinical Experience: An Audit of Accuracy of Nutritional Screening GO Surgical Patients in a UK Tertiary Hospital
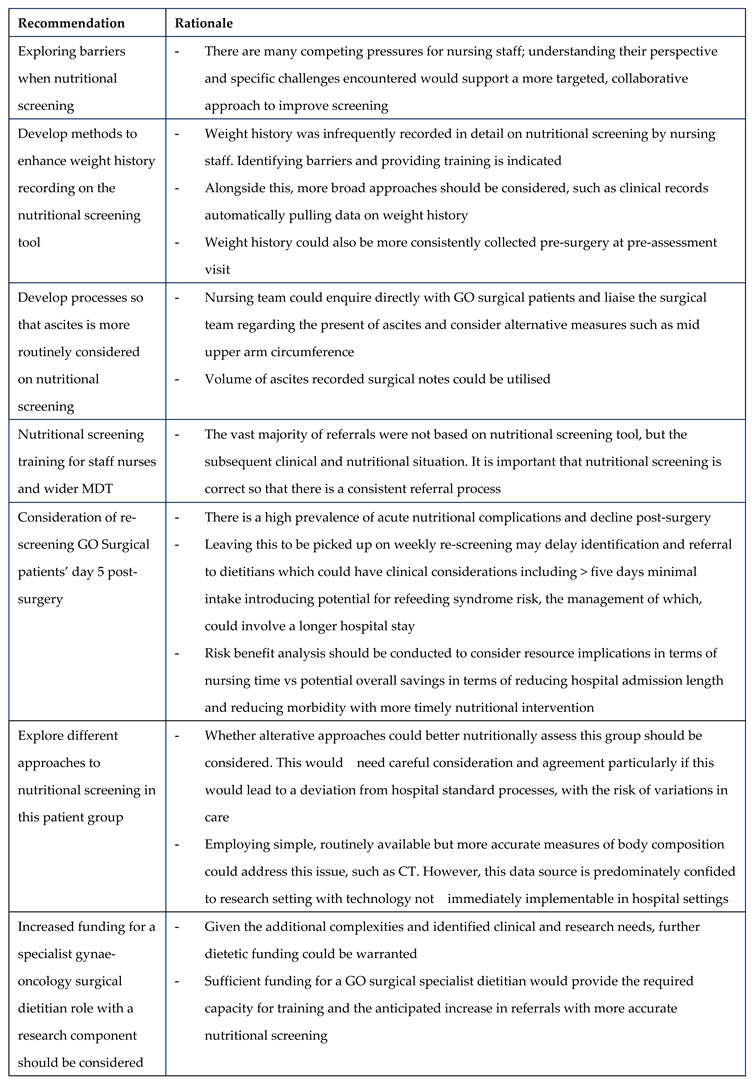
We carried out a retrospective audit assessing the accuracy of nutritional screening scores in surgical GO patients compared to subsequent dietetic assessments. Of the 34 dietetic referrals analysed, all women with a GO diagnosis had undergone elective midline laparotomies. Referrals were made on average five days post-admission (SD 3.5). A key finding was that most dietetic referrals were prompted by the wider multidisciplinary team (MDT), based on clinical judgement, rather than by the nutritional screening itself. Nutritional screening was completed in 28 (82%) of patients (national target 100%); however, only two (7%) were identified as high risk by nursing staff. A re-calculation based on dietetic records identified 24 patients (71%) as high risk. Acute deterioration in oral intake post-surgery was the main driver of high-risk classification, present in 83% of these patients (20/24). For eight patients (33%), ascites interfered with weight assessments. These discrepancies were not adequately captured by initial screening.
Limitations of the audit included small sample size, retrospective design and lack of contemporaneous between screening and dietitian assessments. Improved harmonisation of nutritional screening approaches would enable more accurate data collection on nutritional parameters within and between countries to identify areas for enhancing surgical outcomes. The audit rationale assumes that improved screening will directly lead to better outcomes, but the projected impact needs be explored. Nevertheless, our audit revealed that nutritional screening scores were not an accurate reflection of nutritional status at the time of dietetic assessment, mainly due to acute declines in oral intake, not detected by weekly screening. Recommendations for clinical practice are detailed in Table 2.
4. Discussion
Malnutrition is both common and costly amongst women with gynaecological cancer, increasing the risk of post-operative complications [1,2]. Accurate and timely nutritional screening and assessment are essential to ameliorate these risks. However, no specific or universally accepted tools exist for this population. Instead, practice is often dictated by local protocols, national guidelines, and practitioner familiarity. Although a gold standard is lacking, certain tools may be less reliable due to unique nutritional considerations faced by this patient group.
A fundamental consideration is ascites, which can mask true bodyweight and hinder accurate calculation of BMI and percentage dry body weight loss. Therefore, more precise methods of BC assessment are required. Routine CT imaging in GO patients can provide a practical tool for accurate BC measures. To date, studies in GO surgical patients have been confined to case note reviews, showing associations with BMI, toxicities and all-cause mortality [17,18,19]. Specific to ovarian cancer patients, CT-based BC measures have correlated with survival rates [2], hospital length [41], and chemotherapy complications [42]. Although predominantly confined to research settings, advances in artificial intelligence-based automation could provide sophisticated assessments of BC and refine nutritional screening [43]. Prospective studies are urgently required.
An additional consideration is the integration of BC measures with tailored novel nutritional screening tools specifically designed for this patient group. Disease-specific nutritional screening tools are available for conditions such as liver and renal disease. In this context, our audit findings suggest that more frequent re-screening may be necessary to detect rapid postoperative nutritional changes.
In conclusion, current nutritional screening approaches may inaccurately identify malnutrition amongst GO surgical patients, potentially leading to under-recognition and delayed nutritional support. This highlights the urgent need for further research to improve screening methods.
Author Contributions
Laura Rachel Caley: Conceptualization, Methodology, Investigation, Data Curation, Project administration, Formal analysis, Writing - Original Draft. Iman Mustafa: Validation, Writing - Review & Editing. Oliver Jagus: Investigation, Writing - Review & Editing. Helen Hutchinson: Investigation, Writing - Review & Editing. Amudha Thangavelu: Writing - Review & Editing. Timothy Broadhead: Writing - Review & Editing. David Nugent: Writing - Review & Editing. Alexandros Laios: Conceptualization, Methodology, Formal analysis, Supervision, Writing - Original Draft, - Review & Editing
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interests.
Appendix A
Supplementary Methods of literature review
Search Strategy
Pubmed
(("Nutritional Screening" OR "Nutritional Assessment" OR "nutritional screening"[tiab] OR "nutritional assessment"[tiab] OR "nutritional evaluation"[tiab] OR "malnutrition screening"[tiab] OR "nutrition risk"[tiab] OR "undernutrition screening"[tiab]) AND ("Surgical Procedures, Operative"[Mesh] OR "surgery"[tiab] OR "surgical"[tiab] OR "operative"[tiab] OR "surgical procedures"[tiab] OR "surgical patients"[tiab]) AND ("Gynecologic Neoplasms" OR "gynecologic oncology"[tiab] OR "gynaecologic oncology"[tiab] OR "gynecologic neoplasm*"[tiab] OR "gynaecologic neoplasm*"[tiab] OR "ovarian cancer"[tiab] OR "cervical cancer"[tiab] OR "endometrial cancer"[tiab] OR "uterine cancer"[tiab] OR "vulvar cancer"[tiab] OR "vaginal cancer"[tiab]))
Web of Science
("nutritional screening" OR "nutritional assessment" OR "nutritional evaluation" OR "malnutrition screening" OR "nutrition risk" OR “undernutrition screening”) AND ("surgery" OR "surgical" OR "operative" OR "surgical procedures" OR "surgical patients") AND ("gynecologic oncology" OR "gynaecologic oncology" OR "gynecologic neoplasm*" OR "gynaecologic neoplasm*" OR "ovarian cancer" OR "cervical cancer" OR "endometrial cancer" OR "uterine cancer" OR "vulvar cancer" OR "vaginal cancer")
Medline via Ovid
1. exp Nutrition Screening.mp.
2. exp Nutritional Assessment/
3. ("nutritional screening" OR "nutritional assessment" OR "nutritional evaluation" OR "malnutrition screening" OR "nutrition risk" OR “undernutrition screening”).ti,ab.
4. 1 OR 2 OR 3
5. exp Surgical Procedures, Operative/
6. (surgery OR surgical OR operative OR "surgical procedures" OR "surgical patients").ti,ab.
7. 5 OR 6
8. exp Gynecologic Neoplasms/
9. ("gynecologic oncology" OR "gynaecologic oncology" OR "gynecologic neoplasm*" OR "gynaecologic neoplasm*" OR "ovarian cancer" OR "cervical cancer" OR "endometrial cancer" OR "uterine cancer" OR "vulvar cancer" OR "vaginal cancer").ti,ab.
Eligibility Criteria for inclusion in literature review
Inclusion criteria
- -
- Gynae-oncology surgical patients
- -
- Assessment of nutrition in pre-, peri- or post-operative period
- -
- Adults (18+ years old)
- -
- English language
- -
- Data where assessment of nutrition under routine clinical care can be extracted
- -
- Published within the last 10 years
Exclusion criteria
- -
- Reviews
- -
- Conference abstracts
- -
- Not undergone or undergoing gynae-oncology (GO) surgery
- -
- Non-English language
- -
- < 18 years old
- -
- Mixed cohort where it is not possible to separate nutritional data for GO surgical patients
- -
- Nutritional assessment integrated with other assessments (e.g. frailty), where results on nutrition status cannot be isolated
- -
- Dietary/nutritional intervention studies where pre-intervention or without-intervention data cannot be isolated
- -
- Focus on assessing nutritional status for another treatment modality, such as chemotherapy or radiotherapy, where nutritional data for surgery cannot be isolated
- -
- Case studies
- -
- Published >10 years ago
- -
- No details on method of nutritional screening or assessment tool provided
References
- Goins, E.C.; Weber, J.M.; Truong, T.; Moss, H.A.; Previs, R.A.; Davidson, B.A.; Havrilesky, L.J. Malnutrition as a risk factor for post-operative morbidity in gynecologic cancer: Analysis using a national surgical outcomes database. Gynecol Oncol 2022, 165, 309–316. [Google Scholar] [CrossRef]
- Raia, G.; Del Grande, M.; Colombo, I.; Nerone, M.; Manganaro, L.; Gasparri, M.L.; Papadia, A.; Del Grande, F.; Rizzo, S. Whole-Body Composition Features by Computed Tomography in Ovarian Cancer: Pilot Data on Survival Correlations. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Benna-Doyle, S.; Baguley, B.J.; Laing, E.; Kiss, N. Nutritional interventions during treatment for ovarian cancer: A narrative review and recommendations for future research. Maturitas 2024, 183, 107938. [Google Scholar] [CrossRef] [PubMed]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. ESPEN practical guideline: Clinical nutrition in surgery. Clin Nutr 2021, 40, 4745–4761. [Google Scholar] [CrossRef] [PubMed]
- BAPEN. Malnutrition Universal Screening Tool. Available online: https://www.bapen.org.uk/pdfs/must/must_full.pdf.
- Aynaci, G.; Guksu, Z. Nutritional screening and the impact of malnutrition on poor postoperative outcomes in gynecological oncology patients. Prog. Nutr. 2019, 21, 127–134. [Google Scholar] [CrossRef]
- Hertlein, L.; Kirschenhofer, A.; Fürst, S.; Beer, D.; Göß, C.; Lenhard, M.; Friese, K.; Burges, A.; Rittler, P. Malnutrition and clinical outcome in gynecologic patients. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 174, 137–140. [Google Scholar] [CrossRef]
- Nasser, S.; Bilir, E.; Derin, X.; Richter, R.; Grabowski, J.P.; Ali, P.; Kulbe, H.; Chekerov, R.; Braicu, E.; Sehouli, J. Pre-Operative Malnutrition in Patients with Ovarian Cancer: What Are the Clinical Implications? Results of a Prospective Study. Cancers 2024, 16. [Google Scholar] [CrossRef]
- Tian, M.; Fu, H.P.; Du, J. Application value of NRS2002 and PG-SGA in nutritional assessment for patients with cervical cancer surgery. Am. J. Transl. Res. 2021, 13, 7186–7192. [Google Scholar]
- Eurich, K.E.; Deckert, A.; Smith, B.; Kolahi, K.; Pennington, K.P. The feasibility of screening for malnutrition in the outpatient setting and the prevalence of malnutrition in patients with newly-diagnosed ovarian carcinoma. Gynecol. Oncol. Rep. 2022, 43. [Google Scholar] [CrossRef]
- Gounitsioti, I.S.; Poulimeneas, D.; Grammatikopoulou, M.G.; Kotzamanidis, C.; Gkiouras, K.; Nigdelis, M.P.; Tsolakidis, D.; Papanikolaou, A.; Tarlatzis, B.C.; Bogdanos, D.P.; et al. Objective and Subjective Appetite Assessment in Patients with Gynecological Cancer: A Pre- and Post-Operative Pilot Study. Int. J. Environ. Res. Public Health 2022, 19. [Google Scholar] [CrossRef]
- Ho, C.Y.; Ibrahim, Z.; Abu Zaid, Z.; Mat Daud, Z.A.; Md Yusop, N.B. Clinical malnutrition predictive model among gynecologic cancer patients prior to elective operation: A cross-sectional study. Clin. Nutr. (Edinb. Scotl. ) 2021, 40, 4373–4379. [Google Scholar] [CrossRef] [PubMed]
- Chantragawee, C.; Achariyapota, V. Utilization of a Scored Patient-Generated Subjective Global Assessment in Detecting a Malnourished Status in Gynecologic Cancer Patients. Asian Pac. J. Cancer Prev.: APJCP 2016, 17, 4401–4404. [Google Scholar] [PubMed]
- Benoit, L.; Boudebza, A.; Bentivegna, E.; Nguyen-Xuan, H.-T.; Azais, H.; Bats, A.-S.; Koual, M. What is the most pertinent definition of malnutrition in epithelial ovarian cancer to assess morbidity and mortality? Gynecol. Oncol. 2024, 181, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Pache, B.; Grass, F.; Hübner, M.; Kefleyesus, A.; Mathevet, P.; Achtari, C. Prevalence and Consequences of Preoperative Weight Loss in Gynecologic Surgery. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Zhang, G.; Zhang, Y.; He, F.; Wu, H.; Wang, C.; Fu, C. Preoperative controlling nutritional status (CONUT) score is a prognostic factor for early-stage cervical cancer patients with high-risk factors. Gynecol. Oncol. 2021, 162, 763–769. [Google Scholar] [CrossRef]
- Lee, J.; Chen, T.-C.; Jan, Y.-T.; Li, C.-J.; Chen, Y.-J.; Wu, M.-H. Association of Patient-Reported Outcomes and Nutrition with Body Composition in Women with Gynecologic Cancer Undergoing Post-Operative Pelvic Radiotherapy: An Observational Study. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Lee, J.; Lin, J.B.; Chen, T.C.; Jan, Y.T.; Sun, F.J.; Chen, Y.J.; Wu, M.H. Progressive Skeletal Muscle Loss After Surgery and Adjuvant Radiotherapy Impact Survival Outcomes in Patients With Early Stage Cervical Cancer. Front. Nutr. 2022, 8. [Google Scholar] [CrossRef]
- Lee, J.; Weng, C.-S.; Chang, C.-L.; Hsu, W.-H.; Jan, Y.-T.; Wu, K.-P. Association of prognostic nutritional index with muscle loss and survival in patients with ovarian cancer treated with primary debulking surgery and chemotherapy. Support. Care Cancer: Off. J. Multinatl. Assoc. Support. Care Cancer 2023, 31, 267. [Google Scholar] [CrossRef]
- Uccella, S.; Mele, M.C.; Quagliozzi, L.; Rinninella, E.; Nero, C.; Cappuccio, S.; Cintoni, M.; Gasbarrini, A.; Scambia, G.; Fagotti, A. Assessment of preoperative nutritional status using BIA-derived phase angle (PM) in patients with advanced ovarian cancer: Correlation with the extent of cytoreduction and complications. Gynecol. Oncol. 2018, 149, 263–269. [Google Scholar] [CrossRef]
- Chen, J.; Jin, L.; Luo, R.; Zhang, X.; Chen, Y.; Han, Z.; Liu, T. Predictive value of preoperative systemic immune-inflammation index and prognostic nutrition index in patients with epithelial ovarian cancer. J. Ovarian Res. 2025, 18, 45. [Google Scholar] [CrossRef]
- Feng, Z.; Wen, H.; Ju, X.; Bi, R.; Chen, X.; Yang, W.; Wu, X. The preoperative prognostic nutritional index is a predictive and prognostic factor of high-grade serous ovarian cancer. BMC Cancer 2018, 18, 883. [Google Scholar] [CrossRef] [PubMed]
- Fumagalli, D.; Sonik, R.; De Vitis, L.A.; Rossi, V.; Bazzurini, L.; McGree, M.E.; Fought, A.J.; Mariani, A.; Cliby, W.A.; Kumar, A. Evaluating nutrition in advanced ovarian cancer: which biomarker works best? Gynecol. Oncol. 2024, 188, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.J.; Park, H.-P.; Kim, H.S.; Park, S. Preoperative Prognostic Nutritional Index Is a Prognostic Indicator of Cancer-Specific Survival in Patients Undergoing Endometrial Cancer Surgery. J. Korean Med. Sci. 2023, 38, e163. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Cong, R.; Wang, Y.T.; Kong, F.F.; Ma, J.; Wu, Q.J.; Ma, X.X. Naples prognostic score is an independent prognostic factor in patients with operable endometrial cancer: Results from a retrospective cohort study. Gynecol. Oncol. 2021, 160, 91–98. [Google Scholar] [CrossRef]
- Liu, X.; Li, M.; Zhao, Y.; Jiao, X.; Yu, Y.; Li, R.; Zeng, S.; Chi, J.; Ma, G.; Huo, Y.; et al. The impact of preoperative immunonutritional status on prognosis in ovarian cancer: a multicenter real-world study. J. Ovarian Res. 2025, 18, 30. [Google Scholar] [CrossRef]
- Ogura, S.; Seo, K.; Ichihara, M.; Ichizuka, K.; Nagatsuka, M. Clinical Utility of the Geriatric Nutritional Risk Index Before Surgical Intervention for Epithelial Ovarian Cancer Patients: A Retrospective Study. J. Clin. Med. Res. -Can. 2022, 14, 409–415. [Google Scholar] [CrossRef]
- Pergialiotis, V.; Thomakos, N.; Papalios, T.; Lygizos, V.; Vlachos, D.E.; Rodolakis, A.; Haidopoulos, D. Prognostic Nutritional Index as a Predictive Biomarker of Post-Operative Infectious Morbidity in Gynecological Cancer Patients: A Prospective Cohort Study. Nutr. Cancer 2024, 76, 364–371. [Google Scholar] [CrossRef]
- Miao, Y.; Li, S.; Yan, Q.; Li, B.; Feng, Y. Prognostic Significance of Preoperative Prognostic Nutritional Index in Epithelial Ovarian Cancer Patients Treated with Platinum-Based Chemotherapy. Oncol. Res. Treat. 2016, 39, 712–719. [Google Scholar] [CrossRef]
- Zhu, X.L.; Liu, X.J.; Tian, J.B.; He, C.S.; Huang, S. Nutritional assessment of Chinese gynecologic cancer survivors with post-surgical lower limb lymphedema: a cross-sectional study. Front. Nutr. 2024, 11. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clin. Res. ed.) 2021, 372, n71. [Google Scholar] [CrossRef]
- Caleyachetty, R.; Barber, T.M.; Mohammed, N.I.; Cappuccio, F.P.; Hardy, R.; Mathur, R.; Banerjee, A.; Gill, P. Ethnicity-specific BMI cutoffs for obesity based on type 2 diabetes risk in England: a population-based cohort study. lancet. Diabetes Endocrinol. 2021, 9, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; Van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition - An ESPEN Consensus Statement. Clin Nutr 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- van Bokhorst-de van der Schueren, M.A.; Guaitoli, P.R.; Jansma, E.P.; de Vet, H.C. Nutrition screening tools: does one size fit all? A systematic review of screening tools for the hospital setting. Clin Nutr 2014, 33, 39–58. [Google Scholar] [CrossRef] [PubMed]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN guidelines for nutrition screening 2002. Clin Nutr 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Lee, J.L.; Oh, E.S.; Lee, R.W.; Finucane, T.E. Serum Albumin and Prealbumin in Calorically Restricted, Nondiseased Individuals: A Systematic Review. Am. J. Med. 2015, 128, 1023.e1021–1022. [Google Scholar] [CrossRef]
- White, J.V.; Guenter, P.; Jensen, G.; Malone, A.; Schofield, M. Consensus statement: Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN. J. Parenter. Enter. Nutr. 2012, 36, 275–283. [Google Scholar] [CrossRef]
- Jensen, G.L.; Cederholm, T.; Correia, M.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; de Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. JPEN. J. Parenter. Enter. Nutr. 2019, 43, 32–40. [Google Scholar] [CrossRef]
- Ye, X.J.; Ji, Y.B.; Ma, B.W.; Huang, D.D.; Chen, W.Z.; Pan, Z.Y.; Shen, X.; Zhuang, C.L.; Yu, Z. Comparison of three common nutritional screening tools with the new European Society for Clinical Nutrition and Metabolism (ESPEN) criteria for malnutrition among patients with geriatric gastrointestinal cancer: a prospective study in China. BMJ Open 2018, 8, e019750. [Google Scholar] [CrossRef]
- Boléo-Tomé, C.; Monteiro-Grillo, I.; Camilo, M.; Ravasco, P. Validation of the Malnutrition Universal Screening Tool (MUST) in cancer. Br. J. Nutr. 2012, 108, 343–348. [Google Scholar] [CrossRef]
- Torres, M.L.; Hartmann, L.C.; Cliby, W.A.; Kalli, K.R.; Young, P.M.; Weaver, A.L.; Langstraat, C.L.; Jatoi, A.; Kumar, S.; Mariani, A. Nutritional status, CT body composition measures and survival in ovarian cancer. Gynecol Oncol 2013, 129, 548–553. [Google Scholar] [CrossRef]
- Del Grande, M.; Rizzo, S.; Nicolino, G.M.; Colombo, I.; Rossi, L.; Manganaro, L.; Del Grande, F. Computed Tomography-Based Body Composition in Patients With Ovarian Cancer: Association With Chemotoxicity and Prognosis. Front Oncol 2021, 11, 718815. [Google Scholar] [CrossRef]
- Müller, L. AI-based body composition measures in abdominal CT scans: prime time for clinical implementation? Eur. Radiol. 2025, 35, 517–519. [Google Scholar] [CrossRef]
Figure 1.
PRISMA 2020 flow diagram [31].
Figure 1.
PRISMA 2020 flow diagram [31].
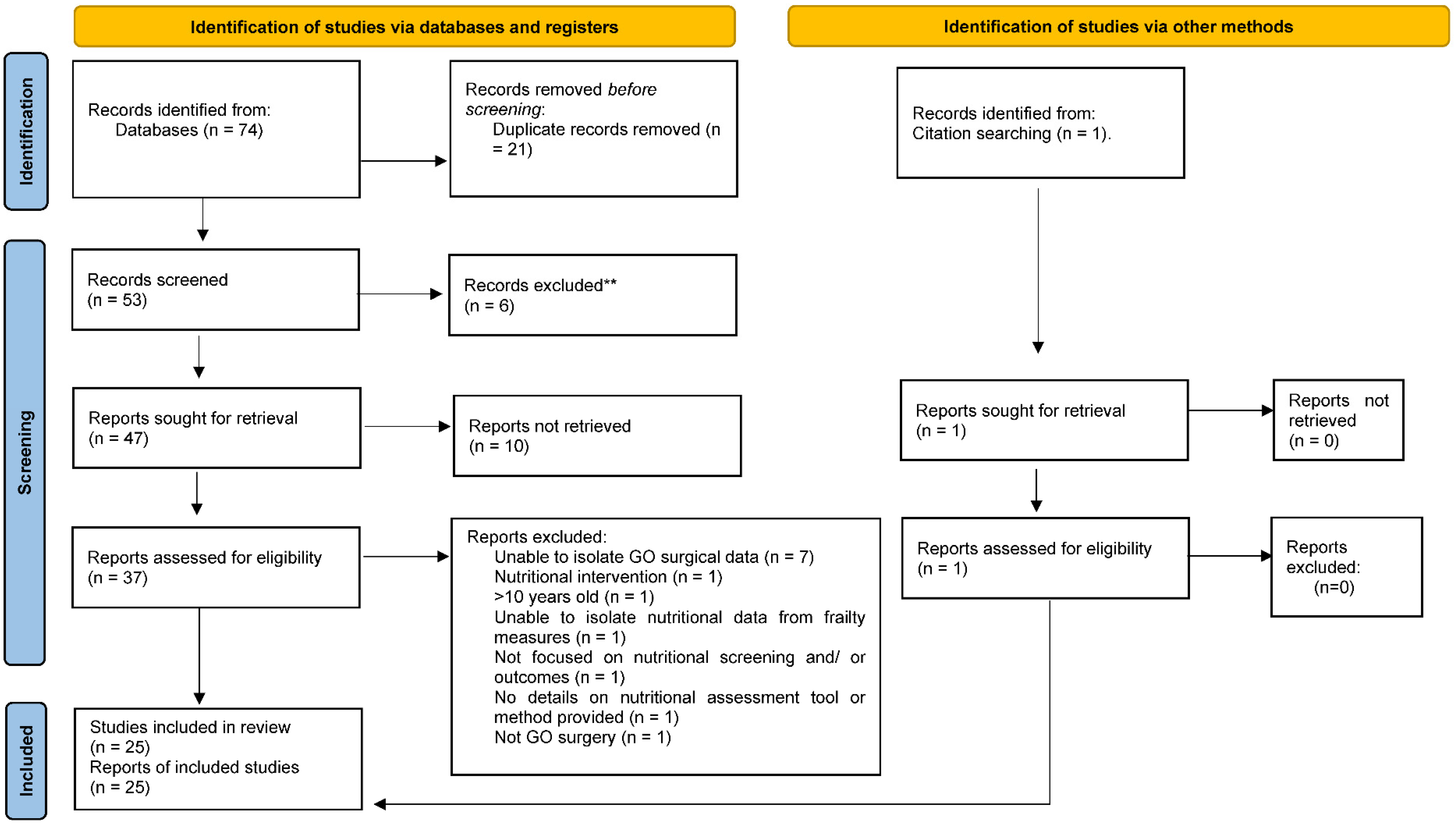

Table 1.
Characteristics of included studies.
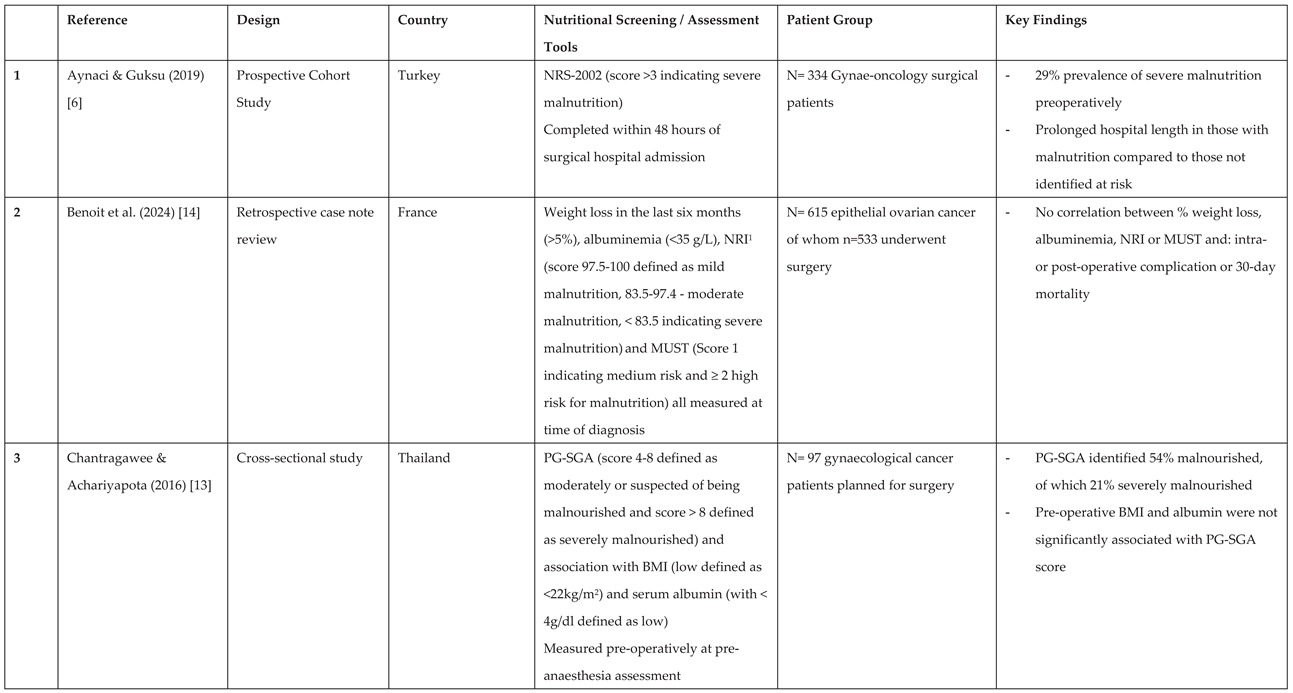
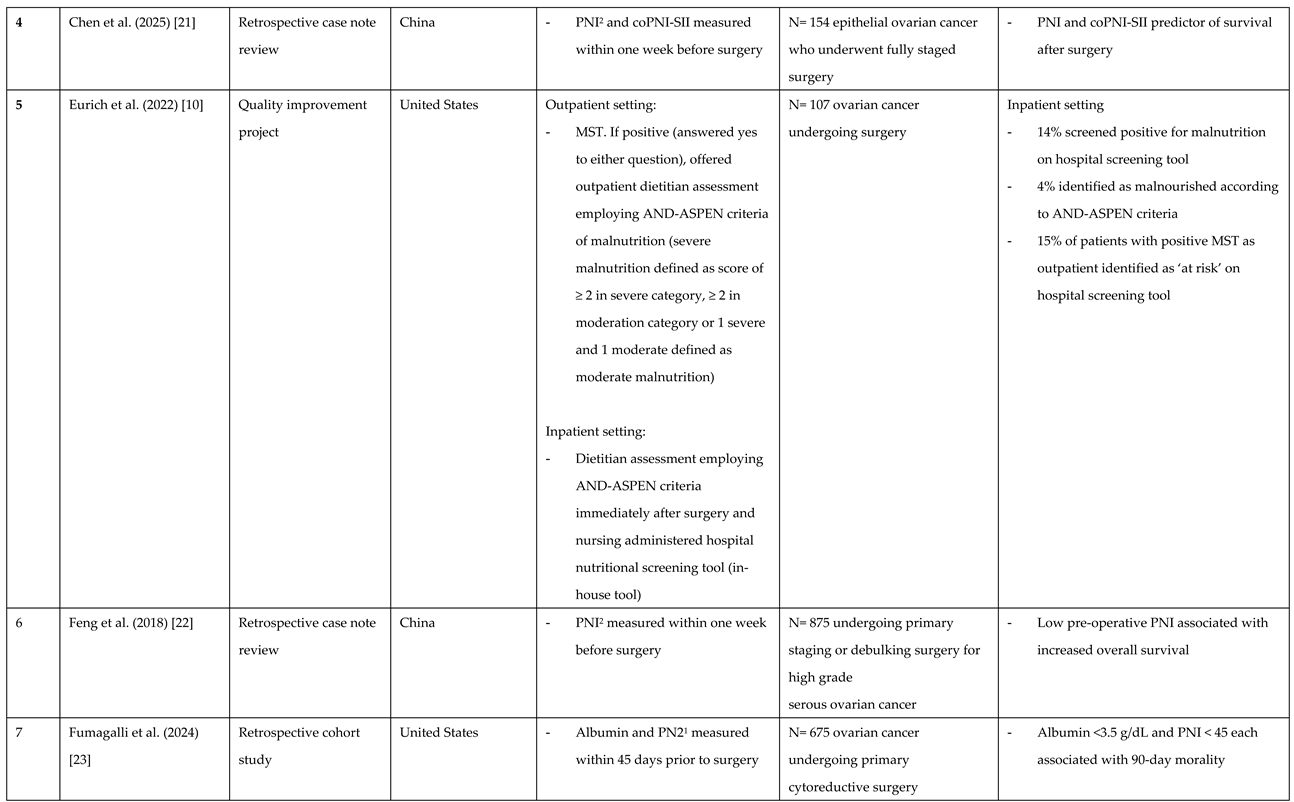
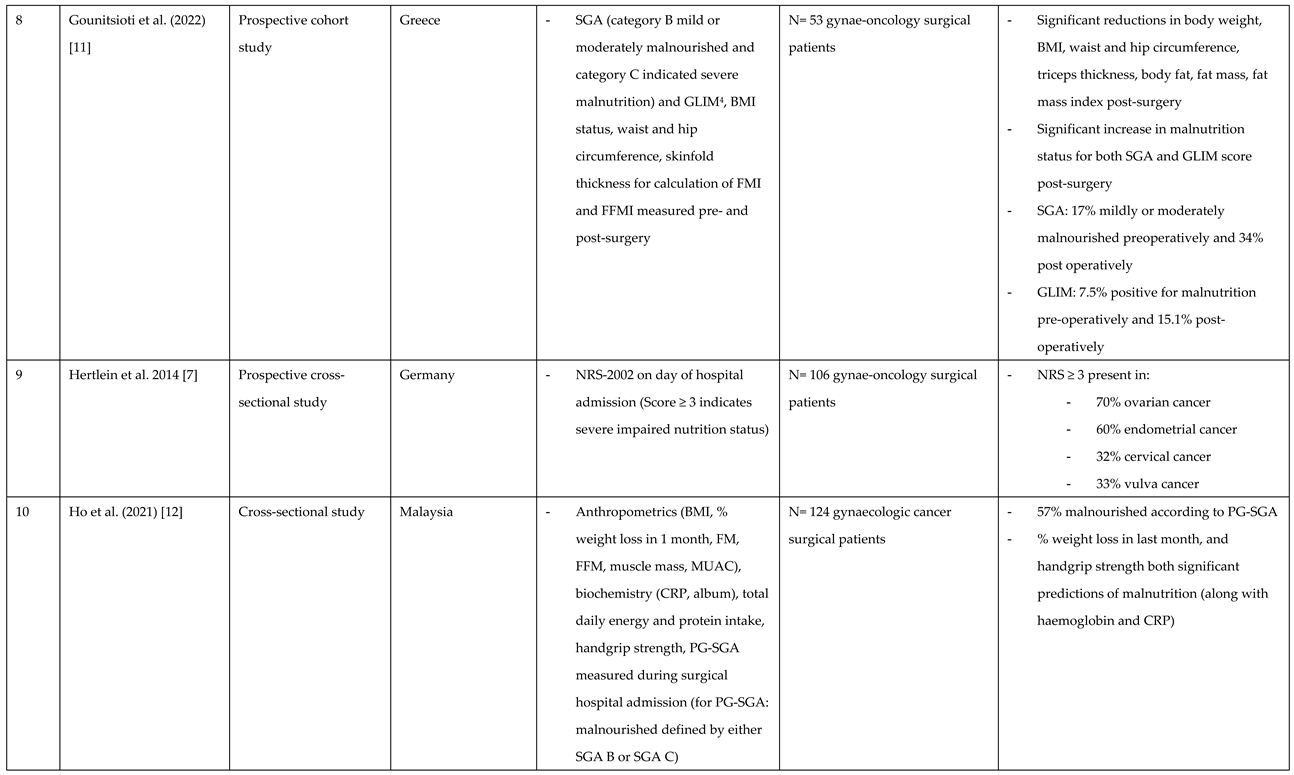
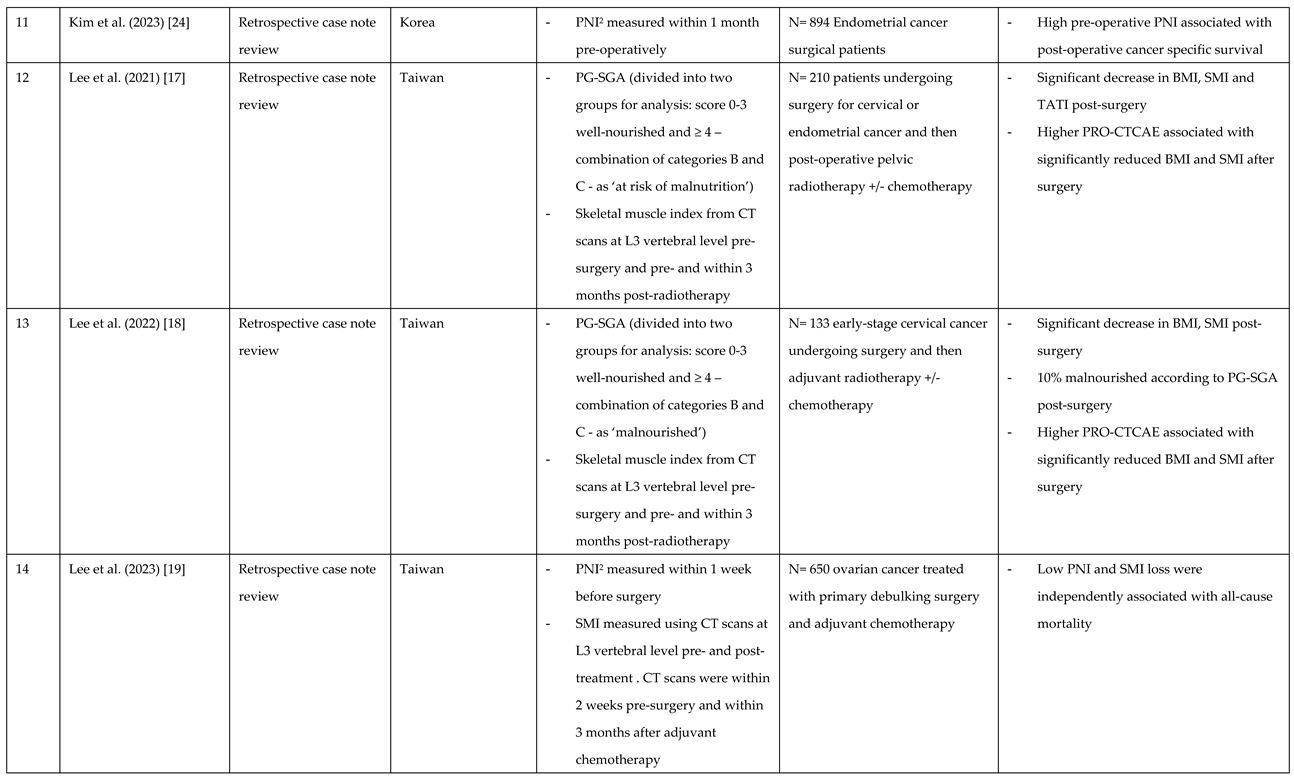
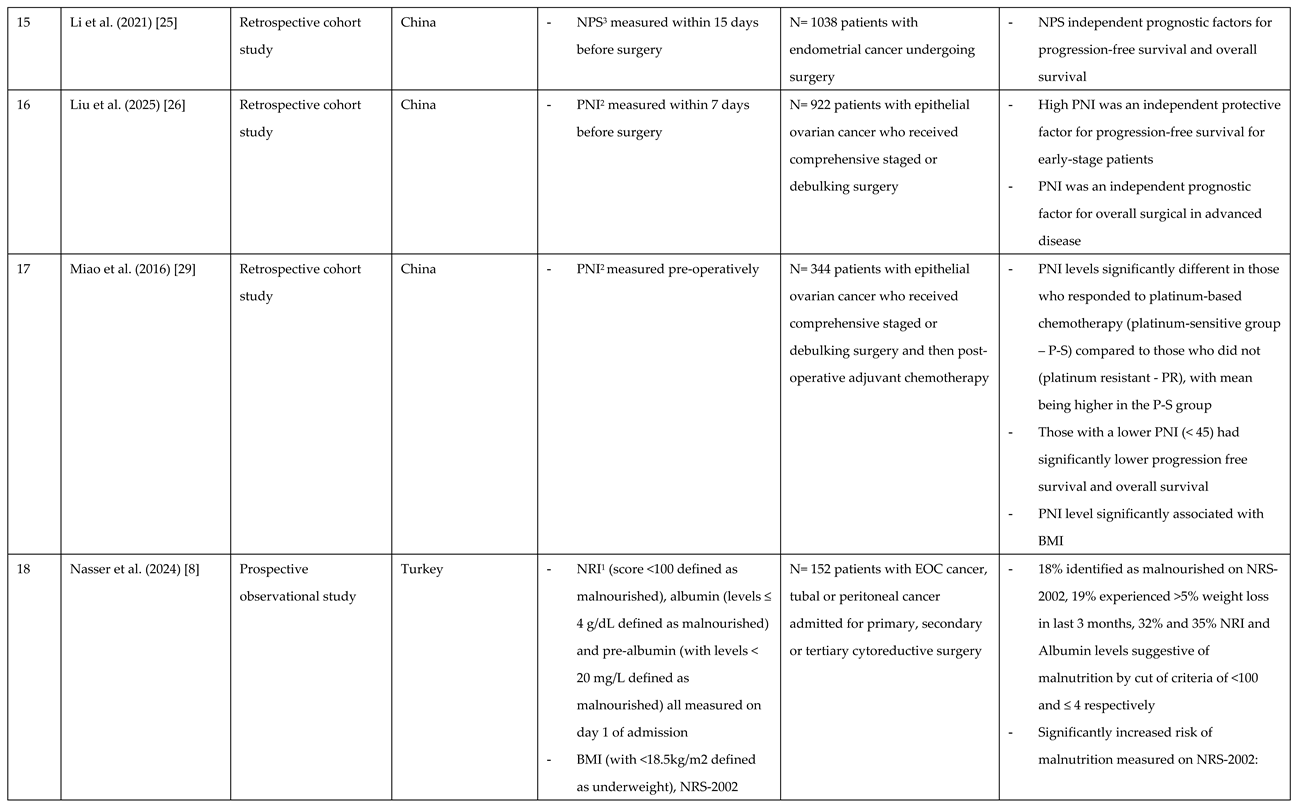
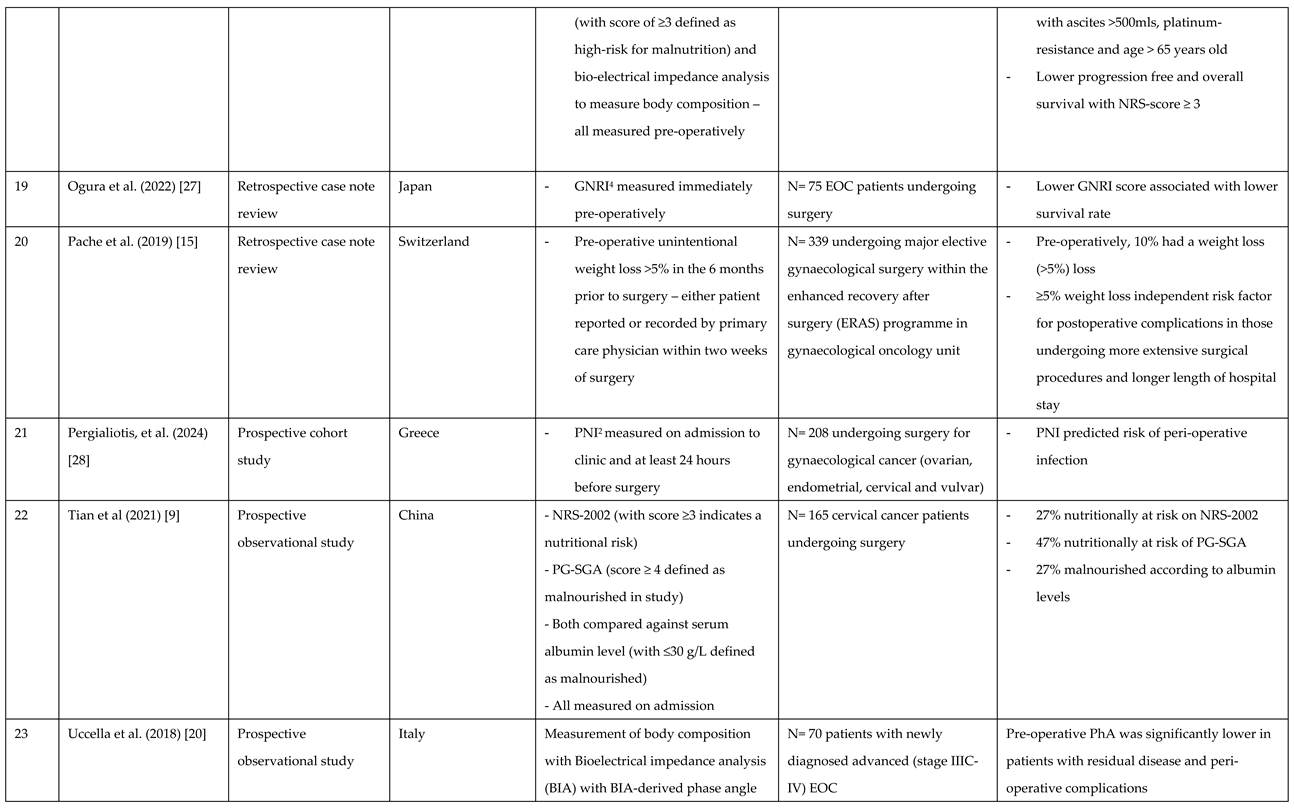
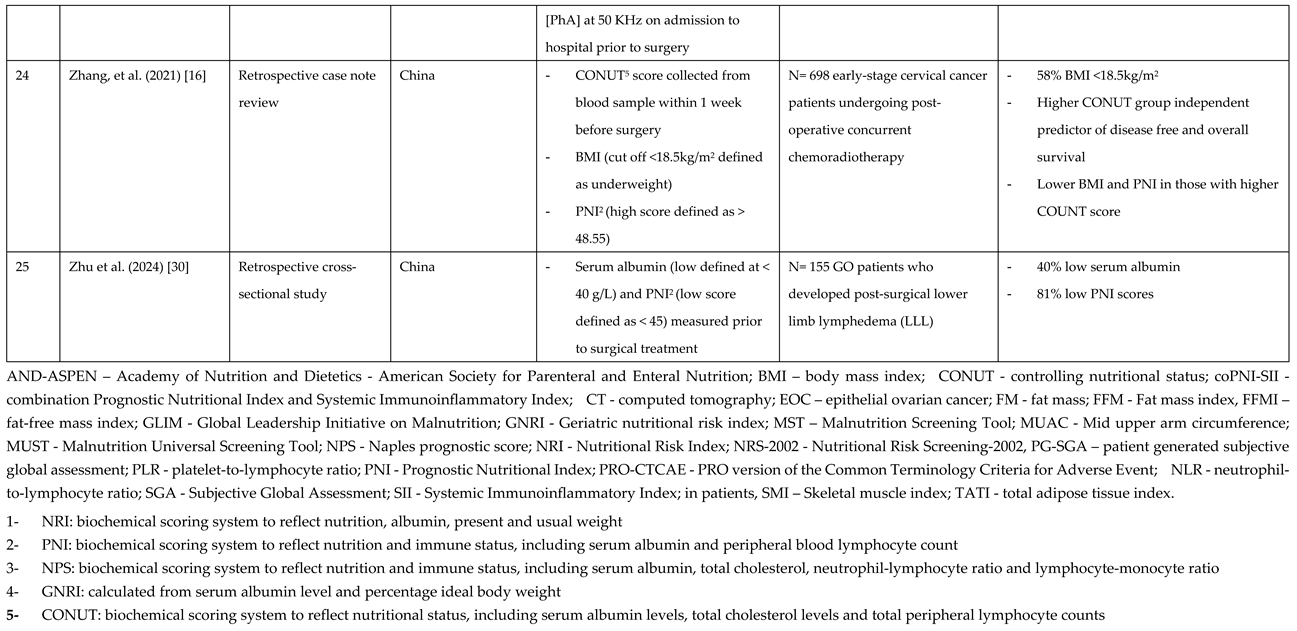
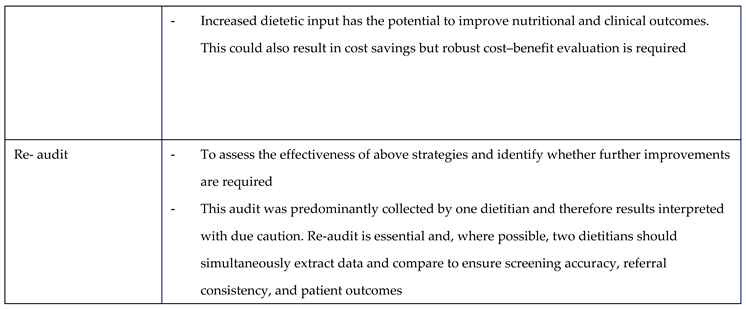
Table 2.
Audit Recommendations for Nutritional Screening in Gynaecological Surgical Patients.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



