
Submitted:
31 December 2025
Posted:
02 January 2026
You are already at the latest version
Abstract
Background: Recurrent pregnancy loss (RPL) and infertility are associated with significant psychological morbidity, including stress, anxiety, and depression. While these impacts are well-documented globally, their prevalence and severity in the Omani population remain unexplored. This study investigates the mental health outcomes of Omani women with RPL and infertility compared to fertile controls. Objectives: To assess the prevalence of stress, anxiety, and depression in women with recurrent pregnancy loss (RPL) and infertility, and compare these rates to women with no fertility concerns in an Omani population. Design: A prospective, cross-sectional study. Setting: Sultan Qaboos University Hospital and Royal Hospital in Muscat, Oman. Participants: 111 women with RPL, 131 women with infertility, and 210 antenatal controls with no fertility issues. Interventions: No clinical interventions were administered as this was an observational study. Participants completed validated psychological assessments (DASS-42 and BDI-II). Primary and secondary outcome measures: Primary outcomes were the prevalence rates of stress, anxiety, and depression assessed using DASS-42 and BDI-II. Secondary outcomes included sociodemographic correlates and risk factors Results: The study included 111 women in the RPL group, 131 in the infertility group, and 210 controls. Among RPL patients, 31% reported stress, ranging from mild to extremely severe, while 35.9% of infertility patients reported stress, compared to 17.1% in the control group (p = 0.003). Anxiety was present in 45% of RPL patients, 45.5% of infertility patients, and 28.1% of controls (p = 0.019). Depression, measured by the DASS-42, was most prevalent in the RPL group (34.2%), followed by the infertility group (33.6%), and controls (13.8%) (p < 0.001). Similar results were observed with the BDI-II, with depression rates of 23.4% in the RPL group, 19.1% in the infertility group, and 7.6% in controls (p = 0.02). Conclusions: Women with RPL and infertility in Oman experience significantly higher levels of stress, anxiety, and depression compared to women without fertility concerns. This study did not assess the mental health of male partners, highlighting the need for further research on the psychological impact on both partners. Future studies should focus on developing psychological support interventions and evaluating their impact on patient outcomes.
Keywords:
recurrent pregnancy loss
; infertility
; depression
; anxiety
; stress
; psychological morbidity
; omani population
1. Introduction
Miscarriage, the most common pregnancy complication defined as pregnancy loss before fetal viability [1], affects 15–25% of pregnancies, with prevalence increasing with advanced maternal age [2]. Recurrent pregnancy loss (RPL), defined by the European Society of Human Reproduction and Embryology (ESHRE) and the American Society of Reproductive Medicine (ASRM) as the consecutive loss of two or more pregnancies [1], impacts 3–5% of women globally and 0.8% in Oman [3]. RPL poses significant challenges, leading to higher levels of depression, anxiety, and reduced self-esteem in affected couples [4]. Approximately 50% of women who experience miscarriage report psychological morbidity, including elevated anxiety and depressive symptoms, with 10–50% developing major depressive disorder [5]. Kolte et al. reported that 8.6% of women with RPL experience moderate to severe depression, and 41.2% report high stress levels [6] .
Infertility, defined by the World Health Organization (WHO) as the failure to achieve pregnancy after 12 months of regular unprotected intercourse [7], affects 10–15% of couples globally. It is a major life event with significant physical and emotional impacts, often causing turmoil, frustration, depression, anxiety, hopelessness, guilt, and feelings of worthlessness [8] . The prevalence of depression in infertile couples ranges from 15–58%, with 8–28% experiencing elevated anxiety levels [9]. The stigma related to infertility was related was related to the stress experienced as per a recent study [10].
Despite extensive research globally, the psychological impact of RPL and infertility in the Omani population remains unexplored. This study aims to evaluate the prevalence and severity of stress, anxiety, and depression in Omani women with RPL and infertility, comparing them to fertile controls.
2. Materials and Methods
2.1. Participants
Women attending the RPL and infertility clinics at Sultan Qaboos University Hospital (SQUH) and Royal Hospital, Muscat, Oman, were invited to participate. The RPL group included patients with ≥2 consecutive miscarriages, and the infertility group included women unable to conceive after 12 months of regular unprotected intercourse, excluded women with secondary infertility with recurrent pregnancy loss. Between September 2018 and July 2021, 111 women with RPL, 131 with infertility, and 210 controls (from antenatal clinics) were recruited. Women attending high-risk pregnancy clinics or antenatal clinics with prior RPL or infertility were excluded from the control group. Additional exclusions included non-Omani women and those with incomplete sociodemographic data or questionnaires.
2.2. Sample Size Calculation
Sample size was calculated using G*Power 3.1.9.2, considering an expected prevalence of anxiety (40%) and depression (10%) among RPL and infertility subjects and lower prevalence in controls (3% for depression and 20% for anxiety). For depression, 418 participants (209 in each group) were required, with a 5% alpha error, 80% power, and a 1:1 allocation ratio. For anxiety, the required sample size was 180 (90 per group). The larger sample size of 418 ensured adequate representation for both outcomes, with 209 subjects in the study group (evenly split between RPL and infertility) and 209 in the control group.
2.3. Data Collection
Ethical approval was obtained from institutional research and ethics committees at SQUH and Royal Hospital. Informed written consent was obtained from participants, who were provided with detailed explanations and written study information. Participants completed a paper-based survey covering sociodemographic and psychological assessments (BDI-II and DASS-42). These validated Arabic-language scales were administered to clinic attendees. Additional data, including demographic details, medical and obstetric history, and fertility treatments, were collected from electronic medical records. Participants with missing data were contacted by phone for completion. All data were treated confidentially, stored in an Excel sheet, and accessed solely by investigators.
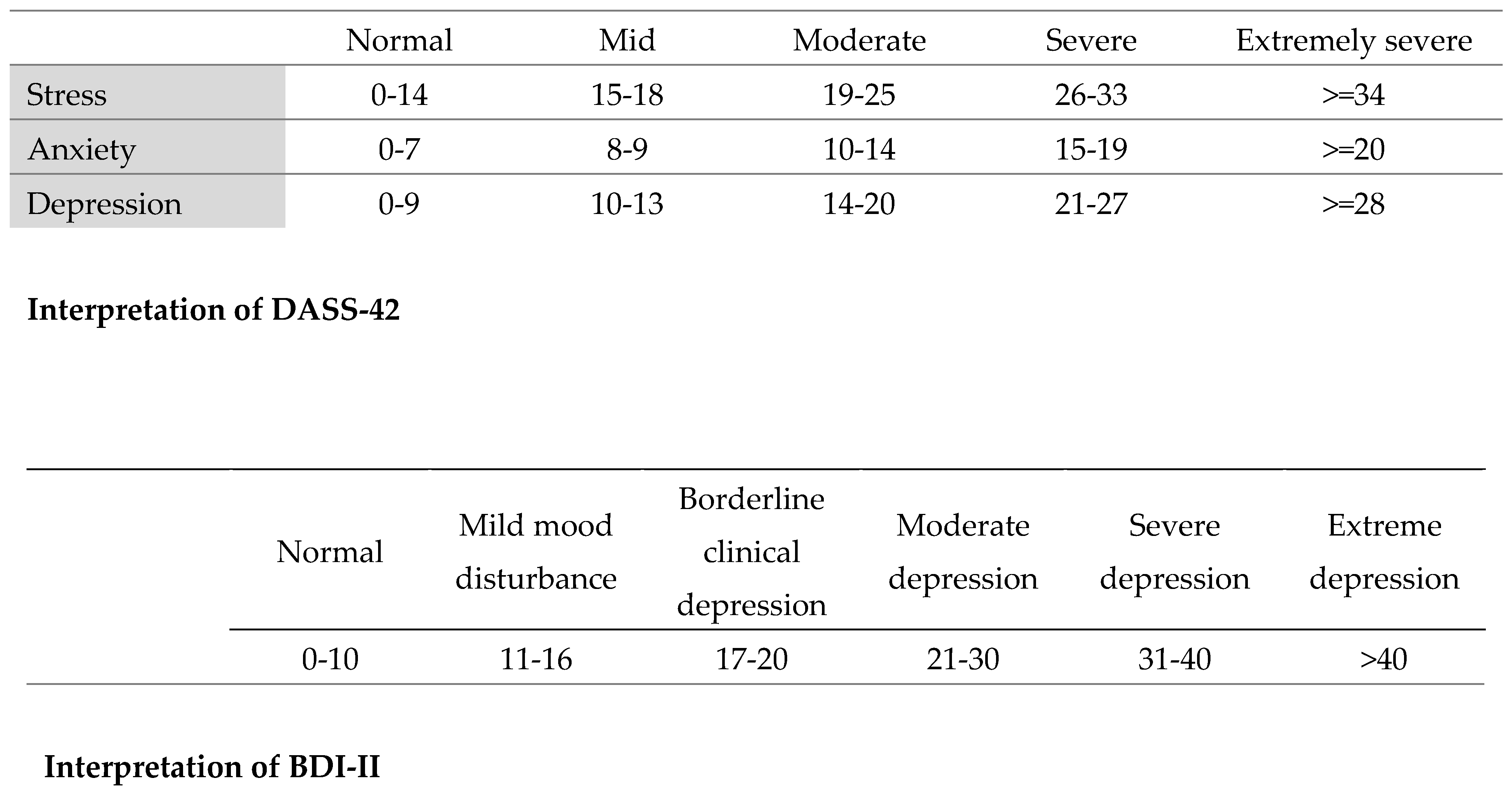
2.4. Questionnaire Interpretation
The DASS-42 assessed levels of stress, anxiety, and depression, while the BDI-II specifically evaluated depression. Interpretation guidelines for both scales are shown in the figures below.
2.5. Data Entry and Statistical Analysis
Data were entered into EpiData Entry Client version 4.4.2.0. Statistical analyses were performed using SPSS version 28.0.0.0. Chi-square test and student t test were used, and a P-value of <0.05 was considered statistically significant.
3. Results
3.1. Study Population Demographics
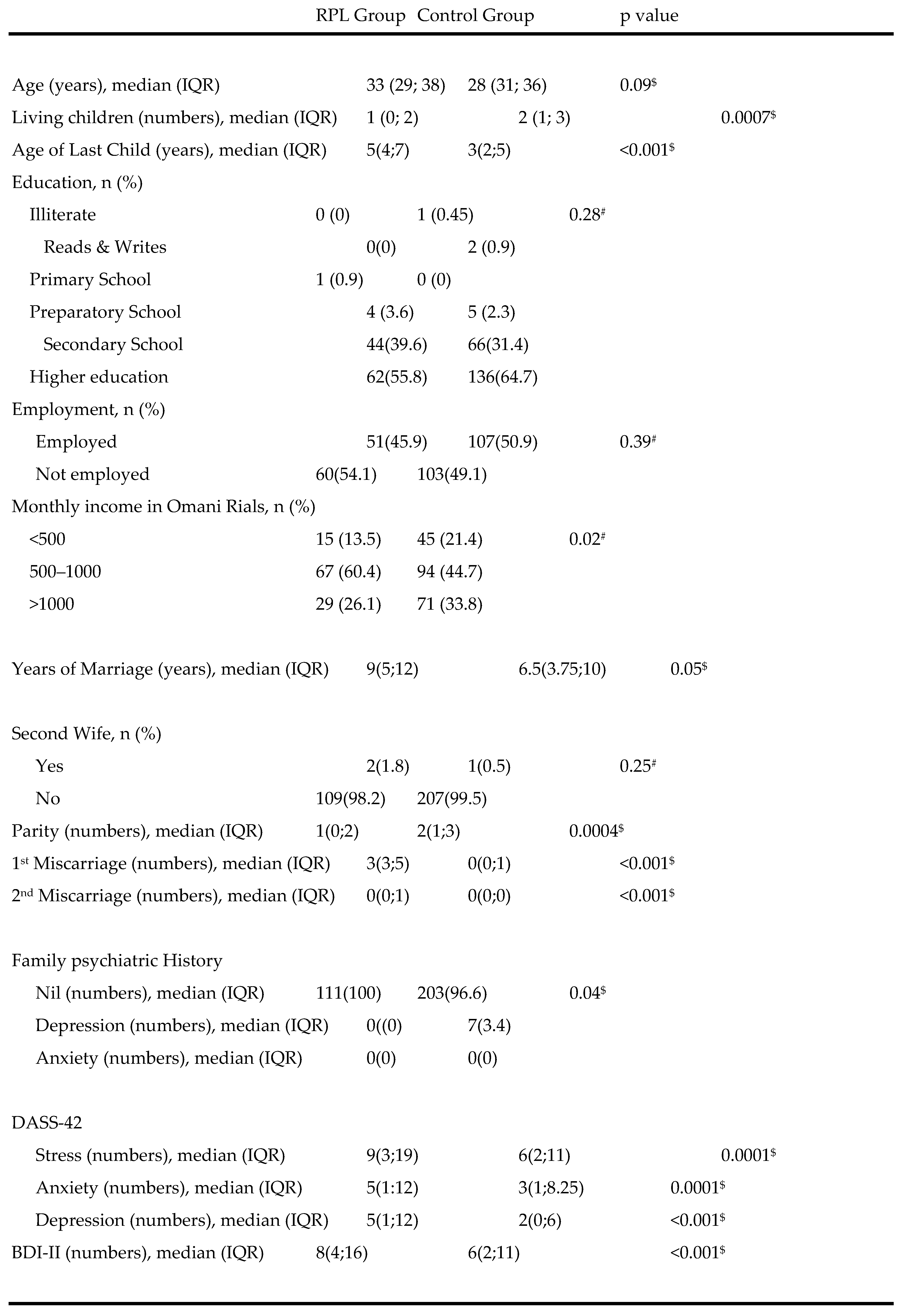
The study compared the demographic characteristics, psychological distress (DASS-42), and depressive symptoms (BDI-II) between recurrent pregnancy loss (RPL) patients (n=111) and a control group (n=210). The median age was slightly higher in the RPL group (33 years) compared to the control group (28 years), but this was not statistically significant (p=0.09). RPL patients had fewer living children (median: 1 vs. 2, p=0.0007) and older last children (median: 5 vs. 3 years, p<0.001). There were no significant differences in education or employment status. However, the RPL group had lower monthly income levels (p=0.02). They were also married for longer periods (median: 9 vs. 6.5 years, p=0.05) and reported higher rates of previous miscarriages (first miscarriage: p<0.001, second miscarriage: p<0.001). In terms of psychological distress, the RPL group scored significantly higher on stress, anxiety, and depression subscales of DASS-42, as well as on BDI-II (all p-values <0.001). Overall, the findings suggest that RPL patients experience greater psychological distress and depressive symptoms compared to the control group. (Table 1)

Table 1.
Demography, DASS-42 & BDI-II in recurrent pregnancy loss (RPL) patients [n=111] versus control group [n=210].
Table 1.
Demography, DASS-42 & BDI-II in recurrent pregnancy loss (RPL) patients [n=111] versus control group [n=210].
 |
|---|
Key: DASS-42 - Depression Anxiety Stress Scale; BDI-II - Beck Depression Inventory-II; IQR-Interquartile range; p-value -# Chi Square test; $ Students t test.
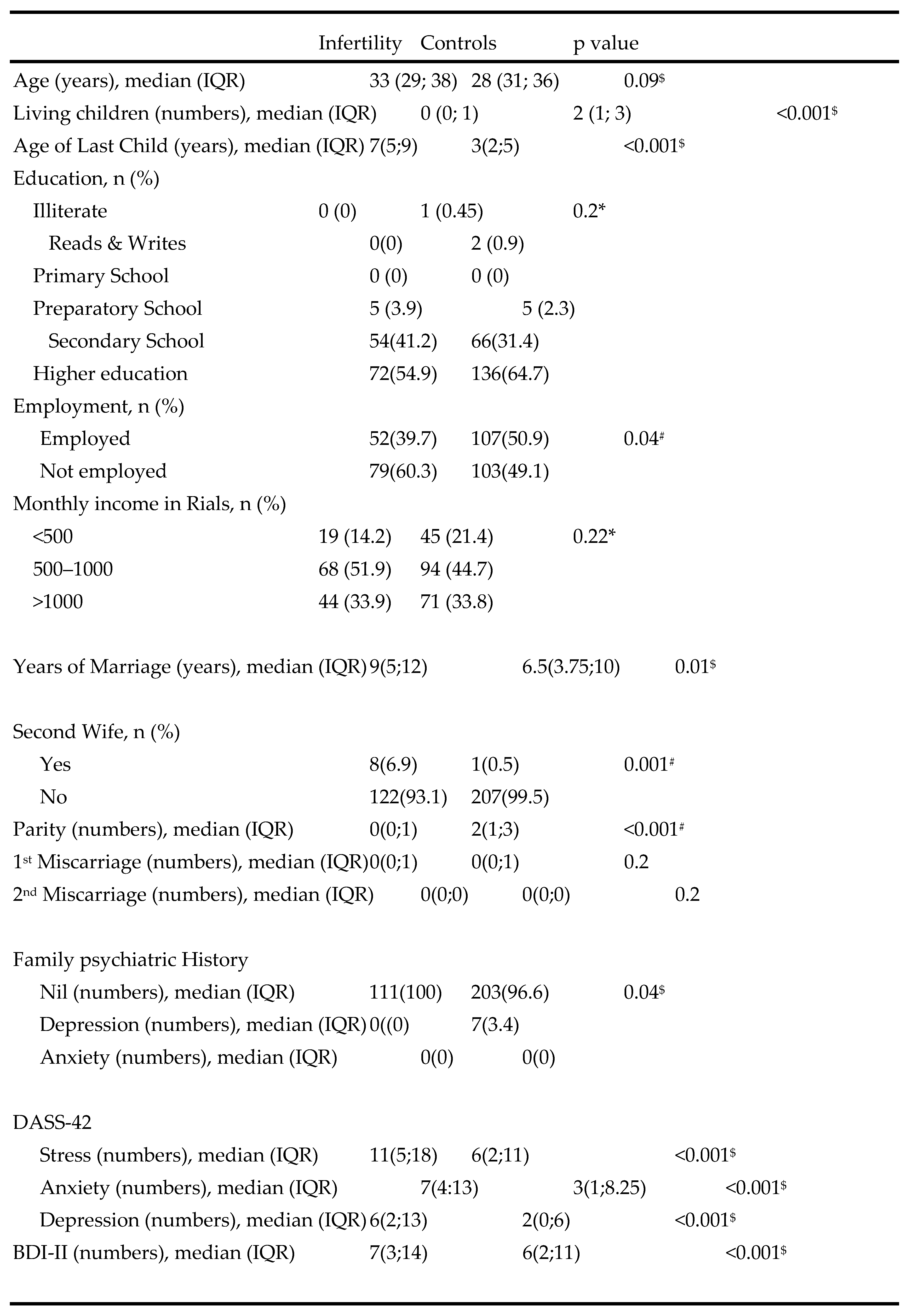
The study compared demographic characteristics, psychological distress (DASS-42), and depressive symptoms (BDI-II) between infertility patients (n=131) and a control group (n=210). The median age was similar between the groups (33 vs. 28 years, p=0.09). Infertility patients had significantly fewer living children (median: 0 vs. 2, p<0.001) and older last children (median: 7 vs. 3 years, p<0.001). There were no significant differences in education levels. However, infertility patients were less likely to be employed (39.7% vs. 50.9%, p=0.04). No significant differences were observed in monthly income. Infertility patients were married for longer (median: 9 vs. 6.5 years, p=0.01) and were more likely to be in polygamous marriages (6.9% vs. 0.5%, p=0.001). They also reported lower parity (median: 0 vs. 2, p<0.001). In terms of psychological distress, infertility patients scored significantly higher on stress, anxiety, and depression subscales of DASS-42, as well as on BDI-II (all p-values <0.001). These findings indicate that infertility patients experience greater psychological distress and depressive symptoms compared to the control group. (Table 2)
Table 2.
Demography, DASS-42 & BDI-II in Infertility patients[n=131] versus controls [n=210].
 |
|---|
Key: DASS-42 - Depression Anxiety Stress Scale; BDI-II - Beck Depression Inventory-II; IQR-Interquartile range; p-value -# Chi Square test; $ Students t test.
3.2. Prevalence of Stress, Anxiety, and Depression
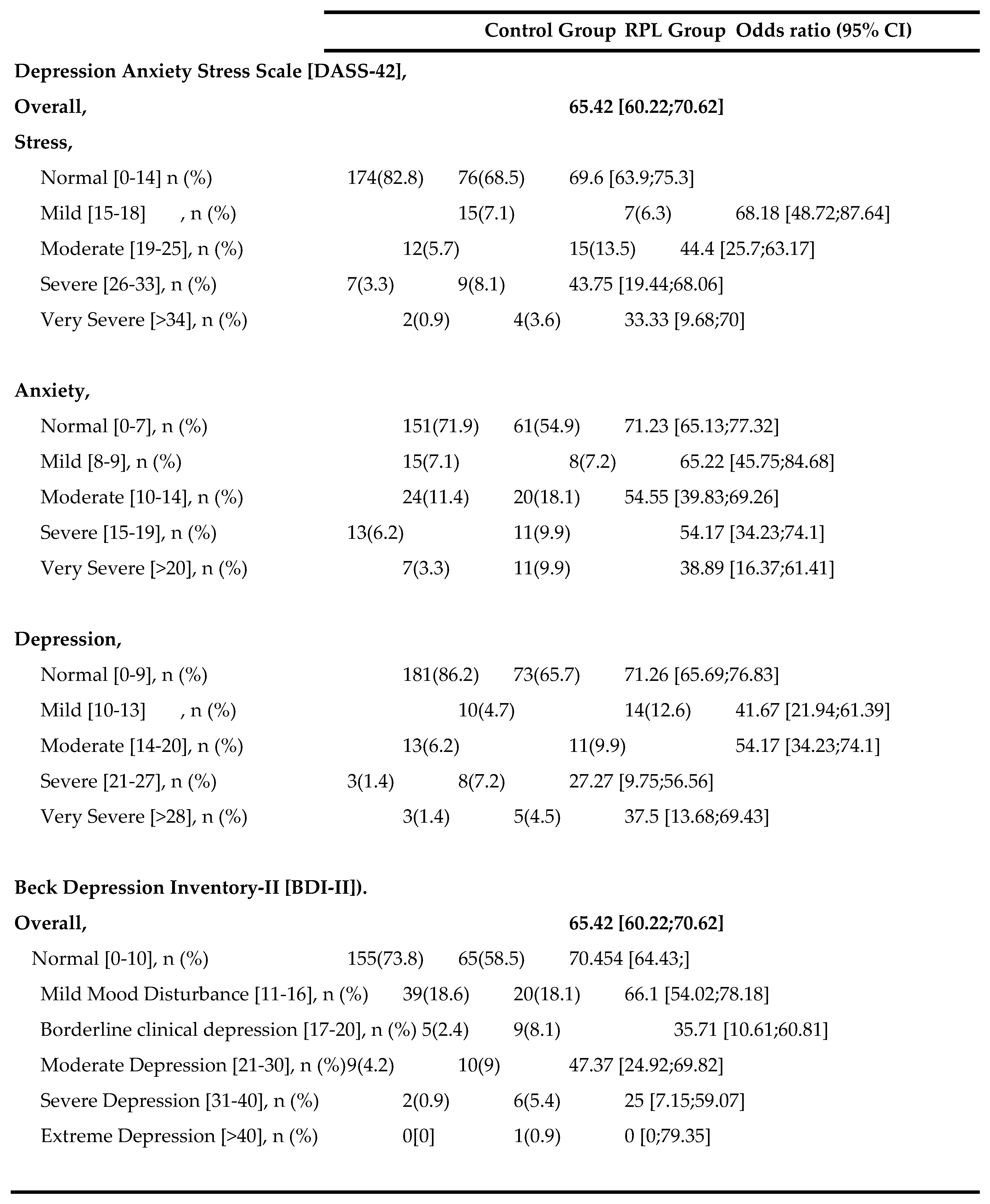
The correlation of psychological distress (DASS-42) and depressive symptoms (BDI-II) was analyzed among recurrent pregnancy loss (RPL) patients (n=111) and a control group (n=210). Overall, RPL patients showed higher scores on DASS-42, indicating greater psychological distress.
For stress, a lower percentage of RPL patients were in the normal range (68.5% vs. 82.8% in controls), while higher proportions experienced moderate (13.5% vs. 5.7%), severe (8.1% vs. 3.3%), and very severe stress (3.6% vs. 0.9%). The odds of severe and very severe stress were notably higher in the RPL group (Odds Ratios: 43.75 and 33.33, respectively).
For anxiety, 54.9% of RPL patients were in the normal range compared to 71.9% of controls. RPL patients also showed higher rates of moderate (18.1% vs. 11.4%), severe (9.9% vs. 6.2%), and very severe anxiety (9.9% vs. 3.3%). The odds of very severe anxiety were significantly increased (OR: 38.89).
Regarding depression, fewer RPL patients were in the normal range (65.7% vs. 86.2%). They also had higher rates of mild (12.6% vs. 4.7%), severe (7.2% vs. 1.4%), and very severe depression (4.5% vs. 1.4%). The odds of severe and very severe depression were considerably elevated (ORs: 27.27 and 37.5, respectively).
For BDI-II, RPL patients had a lower percentage in the normal range (58.5% vs. 73.8%) and higher rates of borderline clinical depression (8.1% vs. 2.4%), moderate depression (9% vs. 4.2%), and severe depression (5.4% vs. 0.9%). Notably, the odds for severe depression were significantly higher in the RPL group (OR: 25).
These findings highlight a substantial increase in psychological distress and depressive symptoms among RPL patients compared to controls, emphasizing the need for targeted mental health interventions in this population. (Table 3)
Table 3.
Correlation of DASS-42 and [BDI-II] among RPL patients (n = 111) and control group (n = 210).
Table 3.
Correlation of DASS-42 and [BDI-II] among RPL patients (n = 111) and control group (n = 210).
 |
|---|
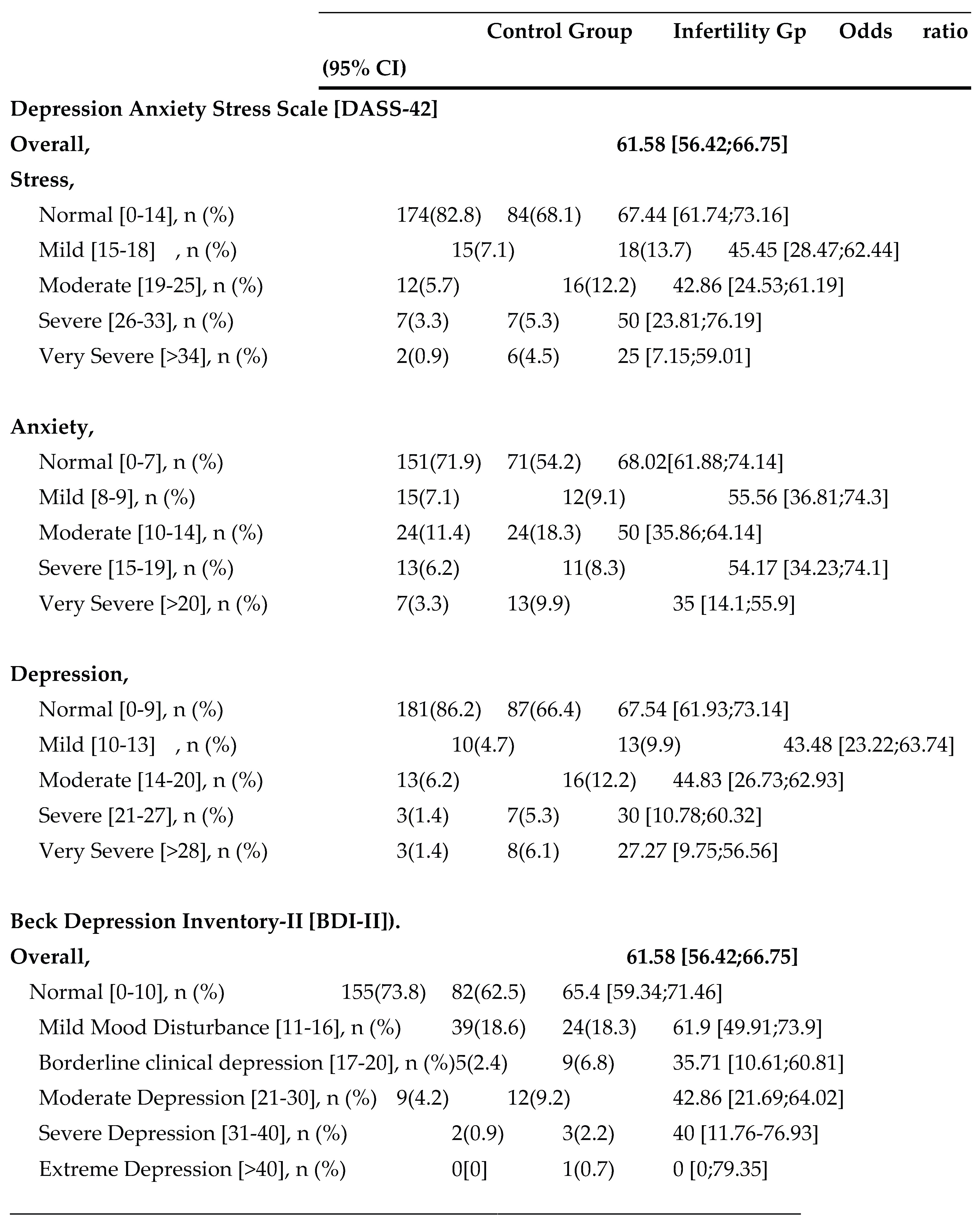
The correlation of psychological distress (DASS-42) and depressive symptoms (BDI-II) was evaluated among infertility patients (n=131) and a control group (n=210). Overall, infertility patients exhibited higher scores on DASS-42, indicating greater psychological distress.
For stress, a smaller proportion of infertility patients were in the normal range (68.1% vs. 82.8% in controls), while more experienced mild (13.7% vs. 7.1%), moderate (12.2% vs. 5.7%), severe (5.3% vs. 3.3%), and very severe stress (4.5% vs. 0.9%). The odds of very severe stress were significantly higher in the infertility group (OR: 25).
For anxiety, 54.2% of infertility patients were in the normal range compared to 71.9% of controls. There were also higher rates of moderate (18.3% vs. 11.4%), severe (8.3% vs. 6.2%), and very severe anxiety (9.9% vs. 3.3%) among infertility patients. The odds of very severe anxiety were considerably increased (OR: 35).
Regarding depression, fewer infertility patients were in the normal range (66.4% vs. 86.2%). They also had elevated rates of mild (9.9% vs. 4.7%), moderate (12.2% vs. 6.2%), severe (5.3% vs. 1.4%), and very severe depression (6.1% vs. 1.4%). The odds of severe and very severe depression were markedly higher in the infertility group (ORs: 30 and 27.27, respectively).
For BDI-II, infertility patients showed a lower percentage in the normal range (62.5% vs. 73.8%) and increased rates of borderline clinical depression (6.8% vs. 2.4%), moderate depression (9.2% vs. 4.2%), and severe depression (2.2% vs. 0.9%). The odds for severe depression were notably elevated (OR: 40).
These results demonstrate significantly higher psychological distress and depressive symptoms among infertility patients compared to controls, underscoring the importance of mental health support in this population. (Table 4)
Table 4.
Correlation of DASS-42 and [BDI-II] among Infertility patients (n = 131) and control group (n = 210).
Table 4.
Correlation of DASS-42 and [BDI-II] among Infertility patients (n = 131) and control group (n = 210).
 |
|---|
4. Discussion
Principal Findings: This study assessed the prevalence of stress, anxiety, and depression among Omani women with recurrent pregnancy loss (RPL), infertility, and antenatal controls without fertility concerns. The prevalence of psychological distress was significantly higher in the RPL and infertility groups compared to controls. Among RPL patients, 31.5% experienced stress, 45.0% anxiety, and 34.2% depression (DASS-42), while the infertility group reported stress (35.9%), anxiety (45.5%), and depression (33.6%). The control group demonstrated lower rates of psychological morbidity: stress (17.1%), anxiety (28.1%), and depression (13.8%).
Results in the Context of Existing Literature: The prevalence of stress in RPL patients (31.5%) was lower than Kolte et al.’s findings (41.2%) [6] , whereas anxiety (45.0%) and depression (34.2%) exceeded rates reported by He et al. (7% anxiety) and Wang et al. (28.7% anxiety; 10.8% depression) [11,12]. Among infertility patients, psychological morbidity rates were lower compared to findings by Yusuf et al. (69–79%), Patel et al. (80% infertility-specific stress), Maroufizadeh et al. (49.6% anxiety, 33.0% depression), Omani-Samani et al. (57% depression), and Haririan et al. (58% depression) [13,14,15,16,17] . The observed variations may reflect differences in study populations, diagnostic tools, and cultural or social contexts [16]. In the control group, prevalence rates of stress, anxiety, and depression were comparable to or slightly lower than regional studies, such as those by Alqahtani et al. and Al-Azri et al [18,19].
Clinical Implications: This study highlights the need for targeted mental health support for Omani women with RPL and infertility. Understanding protective factors such as higher education, employment, and having a living child can guide clinicians in identifying women at lower risk. Additionally, tailored interventions for high-risk groups, such as those with recent miscarriages or without fertility treatments, are essential for improving psychological outcomes.
Research Implications: Future studies should explore culturally specific factors that influence psychological resilience and distress in Omani women. Social stability and strong relationships are protective factors against depression and may vary significantly across cultures [20]. Understanding how women in Oman regulate their emotions and cope with stress can help develop mental health programs that align with their cultural values [21]. Additionally, the way depression is expressed differs among cultures, with non-Western populations often emphasizing physical symptoms like fatigue or body pain over emotional ones. Recognizing these unique expressions is essential for accurate diagnosis and effective treatment in the Omani context [22]. Research should also address stigma surrounding mental health in this population, which may prevent women from seeking support, and examine strategies to reduce its impact. These insights can guide the development of culturally sensitive psychological interventions and support systems tailored to the needs of women with RPL and infertility.
Conclusions: Women with RPL and infertility in Oman experience significantly higher levels of stress, anxiety, and depression compared to antenatal controls, underscoring the need for psychological support tailored to cultural contexts. Addressing stigma and understanding cultural expressions of distress are critical for developing effective mental health interventions.
Author Contributions
MA-B, contributed to study design, data collection, data analysis, and wrote the initial manuscript draft. A-G conceptualized the study, supervised the project, contributed to participant recruitment and manuscript review. MA-S contributed to participant recruitment, and manuscript review. HA-S advised on psychological scales and contributed to the interpretation of results. RA-G contributes to participant recruitment. VG contributed to participant recruitment and data analysis. All authors read and approved the final manuscript.
Funding
this research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Institutional Review Board Statement
MREC approval#1852.
Informed Consent Statement
Obtained.
Data Availability Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Nil.
Conflicts of interest
All authors declare that they have no conflict of interest to disclose and have received no financial support or funding related to the content of this manuscript.
References
- Ewington, LJ; Tewary, S; Brosens, JJ. New insights into the mechanisms underlying recurrent pregnancy loss. J Obstet Gynaecol Res. 2019, 45, 258–265. [Google Scholar] [CrossRef]
- El Hachem, H; Crepaux, V; May-Panloup, P; Descamps, P; Legendre, G; Bouet, PE. Recurrent pregnancy loss: current perspectives. Int J Womens Health. 2017, 9, 331–345. [Google Scholar] [CrossRef]
- Eltayeb, SM; Ambusaidi, SK; Gowri, V; Alghafri, WM. Etiological profile of Omani women with recurrent pregnancy loss. Oman Med J. 2021, 36, 249–253. [Google Scholar] [CrossRef]
- Morley, L; Shillito, J; Tang, T. Preventing recurrent miscarriage of unknown aetiology. Obstet Gynaecol. 2013, 15, 99–105. [Google Scholar] [CrossRef]
- Lok, IH; Neugebauer, R. Psychological morbidity following miscarriage. Best Pract Res Clin Obstet Gynaecol. 2007, 21, 229–247. [Google Scholar] [CrossRef]
- Kolte, AM; Olsen, LR; Mikkelsen, EM; Christiansen, OB; Nielsen, HS. Depression and emotional stress is highly prevalent among women with recurrent pregnancy loss. Hum Reprod. 2015, 30, 777–782. [Google Scholar] [CrossRef]
- Bushnik, T; Cook, JL; Yuzpe, AA; Tough, S; Collins, J. Estimating the prevalence of infertility in Canada. Hum Reprod. 2012, 27, 738–746. [Google Scholar] [CrossRef] [PubMed]
- Simionescu, G.; Doroftei, B.; Maftei, R.; Obreja, B.E.; Anton, E.; Grab, D.; Ilea, C.; Anton, C. The complex relationship between infertility and psychological distress (Review). Exp. Ther. Med. 2021, 21, 306. [Google Scholar] [CrossRef] [PubMed]
- Deka, PK; Sarma, S. Psychological aspects of infertility. Indian J Psychol Med. 2010, 32, 3–7. [Google Scholar]
- Luo, D.; Zhouchen, Y.-B.; Li, L.; Jiang, Y.-L.; Liu, Y.; Redding, S. R.; Wang, R.; Ouyang, Y.-Q. The Stigma and Infertility-Related Stress of Chinese Infertile Women: A Cross-Sectional Study. Healthcare 2024, 12, 1053. [Google Scholar] [CrossRef] [PubMed]
- He, L; Wang, T; Xu, H; Chen, C; Liu, Z; Kang, X; et al. Prevalence of depression and anxiety in women with recurrent pregnancy loss and the associated risk factors. Arch Gynecol Obstet. 2019, 300, 1061–1066. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y; Meng, Z; Pei, J; Qian, L; Mao, B; Li, Y; et al. Anxiety and depression are risk factors for recurrent pregnancy loss: a nested case-control study. Health Qual Life Outcomes. 2021, 19, 78. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, L. Depression, anxiety and stress among female patients of infertility; A case-control study. Pak J Med Sci. 2016, 32, 1340–1343. [Google Scholar] [CrossRef] [PubMed]
- Patel, A; Sharma, PSVN; Narayan, P; Binu, VS; Dinesh, N; Pai, PJ. Prevalence and predictors of infertility-specific stress in women diagnosed with primary infertility: A clinic-based study. J Hum Reprod Sci. 2016, 9, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Maroufizadeh, S; Ghaheri, A; Almasi-Hashiani, A; Mohammadi, M; Navid, B; Ezabadi, Z; et al. The prevalence of anxiety and depression among people with infertility referring to Royan Institute in Tehran, Iran: A cross-sectional questionnaire study. Middle East Fertil Soc J. 2018, 23, 103–106. [Google Scholar] [CrossRef]
- Omani-Samani, R; Maroufizadeh, S; Almasi-Hashiani, A; Amini, P. Prevalence of depression and its determinant factors among infertile patients in Iran based on the PHQ-9. Middle East Fertil Soc J. 2018, 23, 460–463. [Google Scholar] [CrossRef]
- Haririan, HR; Mohammadpour, Y; Aghajanloo, A. Prevalence of depression and contributing factors of depression in the infertile women referred to Kosar infertility center, 2009. Iran J Obstet Gynecol Infertil. 2010, 13, 45–49. [Google Scholar] [PubMed]
- Alqahtani, A; Al-Khedair, K; Al-Jeheiman, R; Al-Turki, H; Al Qahtani, N. Anxiety and depression during pregnancy in women attending clinics in a University Hospital in Eastern province of Saudi Arabia: prevalence and associated factors. Int J Womens Health. 2018, 10, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Al-Azri, M; Al-Lawati, I; Al-Kamyani, R; Al-Kiyumi, M; Al-Rawahi, A; Davidson, R; et al. Prevalence and Risk Factors of Antenatal Depression among Omani Women in a Primary Care Setting. Sultan Qaboos Univ Med J. 2016, 16, e35–e41. [Google Scholar] [CrossRef] [PubMed]
- How Culture Affects Depression. Psychology Today. Available online: https://www.psychologytoday.com/intl/blog/between-cultures/201712/how-culture-affects-depression (accessed on 11 October 2024).
- General (US) Office of the Surgeon; Services (US) Center for Mental Health; Health (US) National Institutes of Mental Health. Chapter 2 Culture Counts: The Influence of Culture and Society on Mental Health. In: Mental Health: Culture, Race, and Ethnicity: A Supplement to Mental Health: A Report of the Surgeon General. Substance Abuse and Mental Health Services Administration (US). 2001. Available online: https://www.ncbi.nlm.nih.gov/books/NBK44249/ (accessed on 11 October 2024).
- Gotlib, IH; Hammen, CL (Eds.) Handbook of Depression, 2nd ed.; Guilford Press: New York, 2010. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



