
Submitted:
30 December 2025
Posted:
01 January 2026
You are already at the latest version
Abstract
Chronic Obstructive Pulmonary Disease (COPD) is a progressive respiratory condition commonly caused by prolonged exposure to harmful particles or gases. The literature on COPD patients is rich in reports of psychological symptoms such as anxiety and depression, which often co-occur with the physical manifestations of the disease. The primary aim of this study was to investigate the role of the sense of coherence and family support in depressive symptomatology among patients with COPD. A total of 143 patients (107 men and 32 women) participated, completing the Beck Depression Inventory (BDI), the Sense of Coherence-13 scale (SOC), and the Family Support Scale (FSS). Among the participants, 46.8% exhibited no depressive symptoms (BDI≤9), 29.5% had mild symptoms (BDI 10–15), 16.5% had moderate symptoms (BDI 16–23), and 7.2% had severe depressive symptoms (BDI≥24). Multiple regression analysis revealed that SOC accounted for 35.2% of the variance in BDI scores, with FSS contributing an additional 3.6%. Mediation analysis was conducted with BDI as the outcome variable, FSS as the mediator, and SOC as the predictor. The analysis confirmed the mediating role of family support in the SOC–BDI relationship, with the model explaining 10.3% of the variance in depressive symptoms. Based on these findings, future studies may benefit from exploring interventions that enhance perceived family support in COPD patients.
Keywords:
COPD
; family support
; sense of coherence
; depression
; mediation
1. Introduction
Chronic Obstructive Pulmonary Disease (COPD) is “a common, preventable condition characterized by persistent respiratory symptoms and airflow limitation due to airway and/or alveolar abnormalities, typically caused by significant exposure to noxious particles or gases, and influenced by host factors, including abnormal lung development” [Vogelmeier et al.,2017; Vestbo et al.,, 2013]. Prolonged exposure to harmful agents induces chronic inflammation associated with structural lung changes [Barnes, 2016; MacNee,2005; Jeffery,2000]. While smoking remains the primary cause, additional factors such as air pollution, occupational exposure, and genetic predisposition also contribute [Tahery et al., 2021; Postma et al., 2015; Ryu et al.,2024; Agustí et al., 2022]. Symptoms of COPD include dyspnea, chronic cough, and sputum production, with severity ranging from asymptomatic cases to respiratory failure [Miravitlles & Ribera, 2017; Patel, 2024]. According to the World Health Organization (WHO), COPD ranked as the fourth leading cause of death worldwide in 2021, accounting for 3.5 million deaths, or 5% of all global mortality that year [Global Initiative for Chronic Obstructive Lung Disease, 2024; WHO, 2024].
The existing literature has consistently reported high rates of psychological symptoms, including anxiety and depression, among patients with COPD [Rahi et al, 2023; Tselebis et al., 2016; Tselebis et al, 2014; Tselebis et al, 2011a; Yohannes & Alexopoulos, 2014]. However, few studies have investigated protective psychological factors that may support patient adaptation to COPD [Tselebis, et al., 2013; Keil, 2017]. Two key positive psychological constructs examined in this context are the sense of coherence and perceived family support [Tselebis et al., 2013, Keil et al., 2017].
According to Aaron Antonovsky, the sense of coherence refers to the individual’s ability to perceive life as comprehensible, manageable, and meaningful [Antonovsky, 1979; Antonovsky, 1987], and is considered a relatively stable personal trait [Eriksson & Mittelmark, 2016]. High levels of sense of coherence have been associated with better diabetes management [Ahola et al., 2010; Odajima, & Sumi, 2018; Merakou et al., 2013] and improved quality of life in patients with chronic diseases [Delgado, 207; Kristofferzon et al., 2018; Fok et al., 2005].
The second protective factor examined in this study is perceived family support among COPD patients. Evidence from other chronic diseases, such as diabetes, indicates that higher perceived family support is linked to better glycemic control [Ilias et al., 2004; Ilias et al., AlHaidar et l., 2020; Kim et al., 2007]. Supportive family relationships also appear to contribute positively to outcomes in patients with stroke [Palmer & Glass, 2003; Evans et al., 1987], chronic kidney disease [Daneker et al., 2001; Khaira et al., 2012], and heart failure [Fry et al., 2016; Dunbar et al., 2008]. Similar associations have been observed in patients with bronchial asthma [Wood et al., 2008; Pérez-Marín et al., 2024] and cancer [Arora et al., 2007; Charos et al., 2025]. However, few studies have examined the role of family support specifically in patients with COPD [Tselebis et al., 2013].
Depression is prevalent among individuals with COPD, with rates ranging from 10% to over 50% [Pumar, 2014; Maurer, 2008], significantly higher than its prevalence of 6–8% in the general population. Patients with COPD have a 1.69-fold increased risk of developing depression [Atlantis et al., 2013]. Studies from Greece report similarly high rates of depressive symptoms in COPD patients, exceeding 42% [Tselebis et al.,2013; Tselebis A et al., 2010]. When compared to other respiratory conditions such as tuberculosis or asthma, individuals with COPD exhibit higher levels of depression [Moussas et al., 2008]. Moreover, depression is more prevalent in COPD than in other chronic diseases [Solano et al., 2006].
A substantial body of research supports a negative association between sense of coherence and depression. This relationship has been demonstrated in adolescents [Moksnes et al., 2012], healthcare professionals [Pachi et al., 2022], and patients with chronic conditions such as chronic pain, heart failure [Aguilar-Latorre et al., 2023; Nahlén & Saboonchi, 2010], and stroke [Guo et al., 2018]. Studies have also confirmed this association in individuals with major depressive disorder [Skärsäter et al., 2009; Skärsäter et al., 2005; Kouvonen et al., 2010; Carstens & Spangenberg, 1997].
During the COVID-19 pandemic, the importance of family support increased due to lockdown-related restrictions [Gostin et al., 2020; Τselebis & Pachi, 2021; Adolph et al., 2021], which reduced access to other forms of social support [Zeng at al., 2022; Sikaras et al., 2023]. Recent studies suggest that enhanced family support served as a protective factor against depressive symptoms during the pandemic [Koutsimani & Montgomery, 2023]. Moreover, recent findings indicate that family support may be the most significant component of social support in mitigating the link between depression and suicidal ideation [Blessing et al., 2023]. Previous research in COPD patients has suggested an inverse relationship between family support and depression [Tselebis et al, 2013], but the mediating role of family support has not been thoroughly explored.
Thus, the primary objective of this study was to examine the protective roles of sense of coherence and family support in depressive symptomatology among COPD patients. The central hypothesis was that enhanced family support could strengthen the protective effect of sense of coherence against depression.
Based on this framework, the following hypotheses were formulated:
H1: The sense of coherence is negatively associated with and predicts depression.
H2: Family support is negatively associated with and predicts depression.
H3: Family support mediates the relationship between sense of coherence and depression.
2. Subjects and Methods
2.1. Study Participants
From the outpatient registry of our hospital, which is the largest pulmonary disease center in the country, a total of 200 Greek patients with a confirmed diagnosis of COPD under the age of 80 were randomly selected. Patients were excluded if they had comorbid physical illnesses (e.g., cardiovascular disease), had been hospitalized for an exacerbation of COPD within the previous six months, or had a history of major psychiatric disorders. Based on these criteria, 29 patients were excluded. An additional 28 declined to participate, resulting in a final sample of 143 participants. Participation in the study was entirely voluntary. Researchers explained the aims of the study to each participant and assured them that all information would remain confidential. Written and verbal informed consent was obtained from all participants prior to data collection. Each participant completed a semi-structured form designed by the research team to collect demographic information and completed a series of self-report questionnaires assessing depression, perceived family support, and sense of coherence. All responses were collected anonymously.
2.2. Sample Size Power Calculation
A post hoc power analysis was conducted to assess the adequacy of the sample size for linear multiple regression. The analysis was performed using G*Power software [Kang, 2021; Faul et al., 2009]. A sample size of 143 with an effect size of f2 = 0.15, alpha = 0.05, and seven predictors yielded a statistical power of 0.933, which was deemed satisfactory. Furthermore, following the empirical rule proposed by Kline [Kline, 1998], a suitable sample size should be at least 10 times greater than the number of parameters examined (seven parameters were included in this study).
2.3. Ethical Considerations
This study was conducted in accordance with the ethical principles outlined in the General Data Protection Regulation of the European Union (GDPR-2016/679), the Declaration of Helsinki (1975, revised 2008), and the guidelines of the International Committee of Medical Journal Editors. The study protocol was approved by the Clinical Research Ethics Committee of the ‘Sotiria” General Hospital for Chest Diseases of Athens (Approval Number: 24252/27-09-21).
2.4. Measurement Instruments
Demographic and clinical data were collected from patient medical records, including sex, age, disease duration, and the most recent spirometric value for predicted FEV1% (Forced Expiratory Volume in 1 second).
i. Beck Depression Inventory (BDI)
Depressive symptomatology was assessed using the Beck Depression Inventory (BDI) [Beck et al., 1961]. This questionnaire captures the behavioral, emotional, and somatic symptoms experienced during the previous week. It consists of 21 items, each scored from 0 to 3 [Donias & Demertzis, 1983], with a total score ranging from 0 to 63. Scores ≥24 indicate severe depressive symptoms, scores ≤9 indicate the absence of depression, scores between 10–15 suggest mild symptoms, and scores between 16–23 indicate moderate symptoms [Donias& Demertzis, 1983]. The Greek version of the BDI has been validated and used in numerous clinical studies involving Greek populations [Tselebis et al.,2013; Sikaras et al., 2023]. The instrument has high internal consistency (Cronbach’s alpha = 0.83) and test-retest reliability ranging from 0.48–0.86 in clinical populations and 0.60–0.90 in non-clinical populations [Sikaras et al., 2023].
ii. Sense of Coherence (SOC)
Sense of coherence was assessed using the 13-item version of the Sense of Coherence scale (SOC-13), developed by Aaron Antonovsky. Each item is rated on a 0 to 7 scale, yielding a total score ranging from 13 to 91, with higher scores indicating a stronger sense of coherence [Antonovsky, 1993, Eriksson & Mittelmark, 2017]. The validated Greek version of the SOC-13 scale was used in this study [Anagnostopoulou & Kioseoglou, 2002; Pachi et al., 2022], and has demonstrated good reliability and validity in the Greek population, with a Cronbach’s alpha of 0.83.
iii. Family Support Scale (FSS)
Perceived family support was measured using the Family Support Scale (FSS) [Tselebis, A, et al., 2011,b]. This scale assesses the perceived support a person receives from cohabiting family members. It consists of 13 items, each rated from “strongly disagree” to “strongly agree” on a 5-point Likert scale. Total scores range from 13 to 65, with higher scores reflecting stronger perceived family support [Tselebis et al.,2011b; Pachi, et al., 2023]. The FSS has been employed in several Greek studies [[Tselebis et al., 2011, b; Pachi, et al., 2023] and has demonstrated good internal consistency (Cronbach’s alpha = 0.80).
2.5. Statistical Analysis
Statistical analyses were conducted using SPSS v.20 (IBM Corp., Armonk, NY, USA). For continuous variables, mean values and standard deviations were computed. The prevalence of depressive symptoms was also calculated in percentage terms. Normality of distribution for continuous variables was assessed using the Kolmogorov–Smirnov test (p > 0.05). Independent samples t-tests were used to identify gender differences in continuous variables, with Hedges’ g used to report effect sizes. Pearson correlation coefficients were computed to explore relationships between continuous variables. Assumptions for linear regression analysis were verified: the Durbin–Watson test was used to assess independence of residuals, variance inflation factor (VIF) values were examined for multicollinearity, and linearity was evaluated through visual inspection of partial plots (PPs). Multiple regression was performed to determine whether the identified predictors were significantly associated with depressive symptomatology. Mediation analysis was conducted using the Hayes PROCESS Macro for SPSS (v4.0, model 4) [Hayes, 2013; Hayes & Rockwood, 2020; Hayes, 2015] to evaluate whether family support mediated the relationship between sense of coherence and depression. A p-value < 0.05 (two-tailed) was considered to be statistically significant.
3. Results
The final sample included 107 men and 32 women (Table 1). Women demonstrated a statistically higher mean predicted FEV1% compared to men (52.2 ± 23.2 vs. 41.5 ± 20.2, independent t-test, p < 0.05). Conversely, male participants reported significantly higher family support scores (55.4 ± 11.3 vs. 51.4 ± 7.7, independent t-test, p < 0.05). No other significant gender differences were observed.
Table 2 presents the correlations between the continuous variables of the study. Depressive symptomatology was negatively correlated with both family support and sense of coherence (Pearson correlation, p < 0.01; Table 2). A positive correlation was observed between family support and sense of coherence (Pearson correlation, p < 0.01; Table 2).
To perform multiple regression analysis, we first assessed the linearity between the three variables (BDI, FSS, and SOC) through visual inspection of the predicted probability plots (PPs). Homoscedasticity was evaluated by visually inspecting the scatterplot of standardized residuals versus predicted values. The Durbin–Watson test was used to assess the independence of residuals, yielding a value of 1.87, which indicated no evidence of autocorrelation. The variance inflation factor (VIF) was 1.10, a value well below the threshold of 4, supporting the absence of multicollinearity (Table 3).
Using the stepwise method, we conducted multiple regression analysis in which depressive symptomatology (BDI) was designated as the dependent variable, while sex, sense of coherence, and family support were included as independent variables. The Sense of Coherence scale accounted for 35.2% of the variance in the Beck Depression Inventory scores, with the Family Support Scale contributing an additional 3.6% (Table 3).
To examine the hypothesis that the Family Support Scale mediates the relationship between sense of coherence and depressive symptomatology (BDI), we performed mediation analysis. In this model, BDI was set as the outcome variable, FSS as the mediator, and SOC as the predictor (Figure 1). Hayes’ SPSS Process Macro Model 4 was used, employing a bootstrap analysis based on 5000 samples [Hayes, 2015; Hayes & Rockwood , 2020].
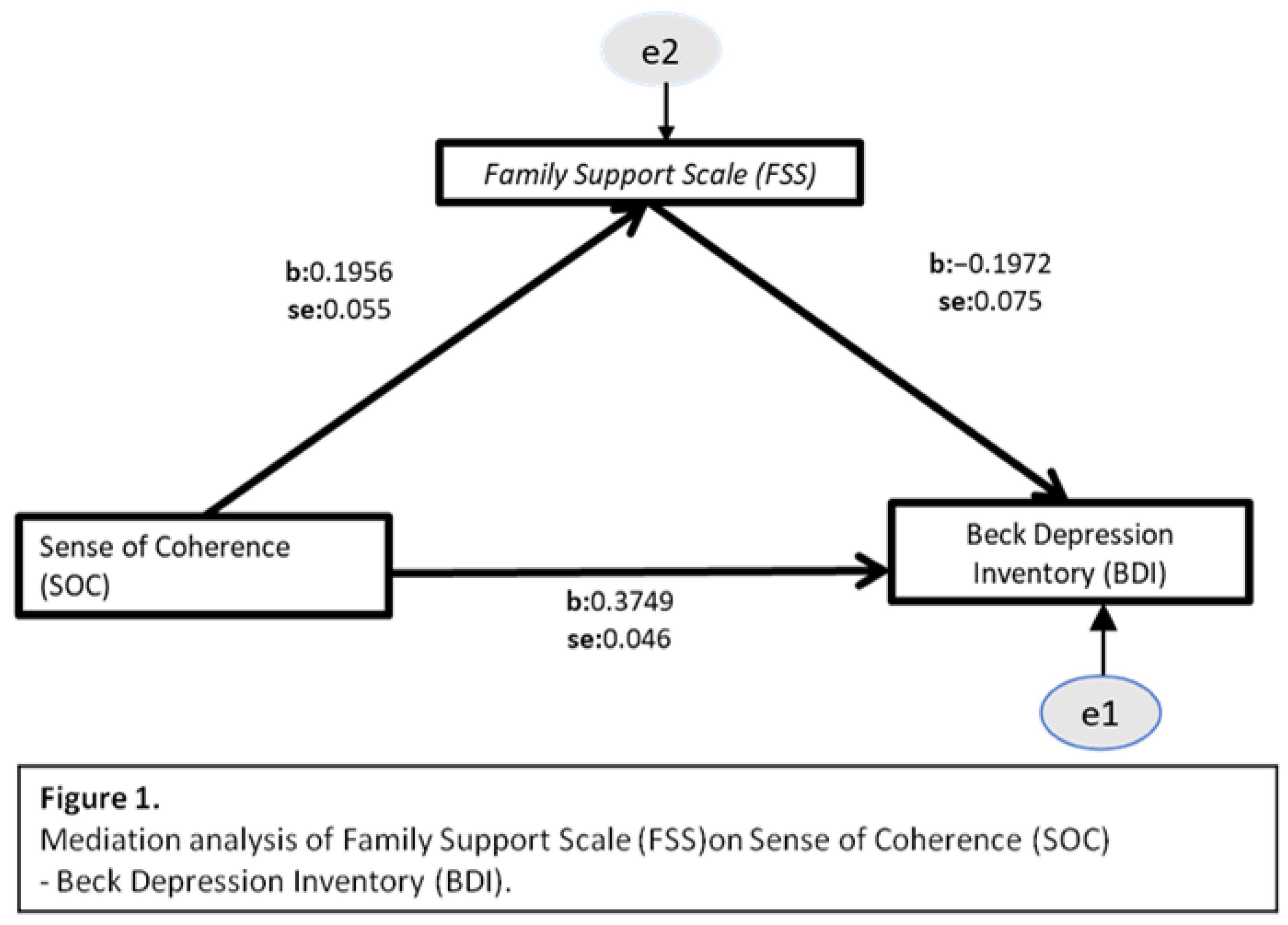
The analysis confirmed the mediation hypothesis, indicating that the Family Support Scale (FSS) mediates the relationship between sense of coherence (SOC) and depressive symptomatology (BDI). The indirect effect of FSS (Table 5) was statistically significant [b = -0.038, 95% CI (-0.0771, -0.0101), p ≤ 0.001]. The direct effect of SOC on BDI, in the presence of FSS as a mediator (Table 5), also remained statistically significant [b = -0.3364, 95% CI (-0.4306, -0.2421), p ≤ 0.001]. This model accounted for 10.3% of the variance in the outcome variable BDI.
4. Discussion
This study concurs with the findings of previous research reporting high rates of comorbid depressive symptomatology in patients with COPD [Xie et al., 2023; Zhang et al., 2011]. In the present sample, 27.7% of participants exhibited moderate to severe depressive symptoms. While the literature consistently indicates elevated rates of depression among individuals with COPD—particularly in comparison to the general population [Tselebis et al., 210; Moussas et al., 2008; Moretta et al.,2024 ]—the prevalence of depressive symptomatology varies significantly across studies [Moretta et al.,2024]. For instance, a Polish study reported prevalence rates of up to 50% [Homętowska et al., 2022], whereas other studies have found that 24–40% of patients with COPD experience depression [Wang et al., 2017; Maurer et al., 208; Sampaio et al., 2019]. Similarly high rates of depressive symptomatology have been documented in previous Greek studies [Tselebis et al., 2010; Moussas et al., 2008]. These discrepancies in prevalence may stem from differences in depression assessment tools, the characteristics of the study populations, and country-specific factors.
Comorbid depression in COPD patients can lead to poorer adherence to rehabilitation programs [Tselebis et al.,2014], worse clinical outcomes, more frequent exacerbations, diminished quality of life, increased mortality [Ng et al., 2007], and higher healthcare costs [Moretta et al.,2024]. Notably, the presence of depression in COPD patients is strongly associated with an elevated risk of suicidal ideation and suicidal behaviors [Roncero et al.,2022; Lin et al., 2020].
Biological theories have been proposed to explain the high prevalence of depression among individuals with COPD. Systemic inflammation and oxidative stress may represent common pathophysiological pathways linking the two conditions. Prolonged elevation of pro-inflammatory cytokines, frequently observed in COPD patients, may contribute to mood disturbances [Krishnadas et al., 2012; Young et al., 2014]. Likewise, oxidative stress, a hallmark of COPD, has been implicated in the pathogenesis of depression [Liu et al., 2015; Jiménez-Fernández et al., 2022]. Moreover, medications such as corticosteroids—particularly at high doses—have been associated with depressive disorders [Brown,209; Alturaymi et al,. 2023].
On the other hand, depression can also be viewed as a psychological response to the losses imposed by the illness, both at a practical and symbolic level [Tselebis et al., 2016]. The inability to continue occupational activities, shifts in familial and social roles, and disruptions to one’s physical appearance and functioning may be perceived as significant losses [Tselebis et al., 2016, Tselebis et al., 2011a]. Some authors also argue that patients with COPD may experience profound guilt stemming from the perception of COPD as a self-inflicted illness, largely due to its strong association with smoking habits [Halding et al., 2011, Lindqvist, G., & Hallberg, 2010].
Several approaches have been studied for the treatment of depression in COPD patients, including pharmacotherapy, cognitive behavioral therapy, and pulmonary rehabilitation programs [Cafarella et al., 2012; Smith et al., 2014; Gordon et al., 2019].
Our findings support a negative association between depressive symptoms and sense of coherence (SOC), with SOC accounting for 35.2% of the variance in Beck Depression Inventory scores. This relationship has been corroborated in other chronic conditions, such as chronic pain, where SOC is considered to act as a significant determinant of depressive symptoms [Aguilar-Latorre et al.,2023; Nahlén &Saboonchi, 2010]. Our results also confirm the inverse association between family support and depression and suggest that family support mediates the relationship between SOC and depressive symptoms. In this mediating role, family support appears to further reduce depressive symptomatology among COPD patients.
Based on these findings, future research could benefit from evaluating techniques aimed at enhancing patients' sense of family support [Rosland, & Piette,2010; Gabriel et al.,2014 ]. Educating family members about the patient's diagnosis, prognosis, and treatment processes may strengthen their ability to provide appropriate and empathetic support. Including caregivers in care planning and clinical consultations, when appropriate, fosters a collaborative atmosphere and enhances the patient’s perception of being cared for. Furthermore, how patients interpret family interactions may shape their perceived support; thus, interventions that help patients reframe or reinterpret ambiguous family behaviors in a more positive light may reduce feelings of isolation or neglect. Meaningful shared activities can also foster emotional closeness and enhance the sense of support. Additionally, the role of technology-based support systems should be explored, such as telemedicine platforms and digital communication tools that can overcome geographic and logistical barriers to in-person support [Barton et al., 2014; Stellefson et al., 2018]. Scheduled video calls, coordinated digital care platforms, and mobile health applications involving both patients and their family members may promote sustained interaction and perceived support [Yohannes, 2021]. In sum, improving a patient’s sense of family support requires a multifaceted approach encompassing psychological, educational, relational, and technological strategies. By aligning clinical interventions with both individual cognitive factors and the broader family system, healthcare providers can foster a more supportive and resilient care environment.
Antonovsky’s theory posits that SOC stabilizes around the age of 30 [Eriksson & Mittelmark 2016]; however, more recent studies suggest that SOC may be enhanced even in older adults [Feldt et al., 2011; Nilsson et al., 2010]. Interventions designed to strengthen SOC often incorporate experiential learning components, defined as the process by which knowledge is created through the transformation of lived experience. In practice, physical activity programs—such as walking, dancing, or even Zumba—have been shown to improve SOC among older populations [Thompson et al., 2021]. Similar findings have been observed in COPD patients who participated in pulmonary rehabilitation programs, which include physical exercise and demonstrated increased SOC by the end of the program [Tselebis, 2012].
The objective of this study was to examine factors that positively influence individuals with COPD, reversing the typical question of "Why does a person with a chronic illness develop depressive symptoms?" to "Why does a person with a chronic illness not develop depressive symptoms?" Accordingly, we proposed two protective factors against depression. However, a limitation of this study is that it did not examine additional potential protective factors, such as psychological resilience or spirituality. Moreover, the gender imbalance in the study sample—with male patients being overrepresented, as is common in COPD—may limit the generalizability of the findings to other diseases. It should also be noted that the design of this study precludes definitive conclusions regarding causal relationships among the variables, which should be further investigated in future research using alternative methodologies.
5. Conclusions
The high prevalence of depressive symptomatology in COPD patients has been consistently highlighted in the literature and was also supported by the present study. However, what this study contributes is the emphasis on the need for future research to focus on protective factors that support patients' mental health. The roles of sense of coherence and family support were examined and found to be inversely associated with depressive symptoms. Furthermore, family support was shown to mediate the inverse relationship between sense of coherence and depression, amplifying the protective effect of coherence and further reducing depression.
There are various techniques and interventions that promote mental health by enhancing family support and sense of coherence, thereby mitigating the depressive symptoms associated with physical illness. Evaluating the effectiveness of these interventions—both in clinical practice and future studies—would be of significant value.
Author Contributions
Conceptualization, A.P., A.T.; methodology, A.P., A.T., I.I.; software, A.T., N.S., A.P.; validation, A.P., A.T., D.B.; formal analysis, A.P., A.T., D.B.; investigation, A.P., A.T.; resources, A.P., N.S., D.K., C.S.; data curation, A.P., D.K., C.S,; writing—original draft preparation, A.P., I.I.; writing—review and editing, A.P., I.I; supervision, A.P., A.T; project administration, A.P., A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of Sotiria General Hospital (Number 24252/27-9-21).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [A.T.], upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Adolph, C., Amano, K., Bang-Jensen, B., Fullman, N., & Wilkerson, J. (2021). Pandemic politics: Timing state-level social distancing responses to COVID-19. Journal of Health Politics, Policy and Law, 46(2), 211-233. [CrossRef]
- Aguilar-Latorre, A., Asensio-Martínez, Á., Oliván-Blázquez, B., Álvarez-Bueno, C., Cavero-Redondo, I., Lionis, C., ... &Magallón-Botaya, R. (2023). Association between sense of coherence and depression in patients with chronic pain: A systematic review and meta-analysis. Plosone, 18(1), e0279959.
- Agustí, A., Melén, E., DeMeo, D. L., Breyer-Kohansal, R., & Faner, R. (2022). Pathogenesis of chronic obstructive pulmonary disease: understanding the contributions of gene–environment interactions across the lifespan. The Lancet Respiratory Medicine, 10(5), 512-524. [CrossRef]
- Ahola AJ, Saraheimo M, Forsblom C, Hietala K, Groop PH; FinnDiane Study Group. The cross-sectional associations between sense of coherence and diabetic microvascular complications, glycaemic control, and patients' conceptions of type 1 diabetes. Health Qual Life Outcomes. 2010 Nov 29;8:142. PMID: 21110902; PMCID: PMC3009698. [CrossRef]
- AlHaidar, A. M., AlShehri, N. A., & AlHussaini, M. A. (2020). Family support and its association with glycemic control in adolescents with type 1 diabetes mellitus in Riyadh, Saudi Arabia. Journal of Diabetes Research, 2020(1), 5151604. [CrossRef]
- Alturaymi, M. A., Almadhi, O. F., Alageel, Y. S., Dayel, M. B., Alsubayyil, M. S., Alkhateeb, B. F. (2023). The Association Between Prolonged Use of Oral Corticosteroids and Mental Disorders: Do Steroids Have a Role in Developing Mental Disorders?. Cureus, 15(4). [CrossRef]
- Anagnostopoulou, T.; Kioseoglou, G. Sense of Coherence Scale. In Psychometric Tools in Greece; Stalikas, A., Triliva, S., Roussi, P., Eds.; EllinikaGrammata: Athens, Grece, 2002; pp. 291–292, (In Modern Greek).
- Antonovsky, A. The Structure and properties of the sense of coherence scale. Soc. Sci. Med. 1993 , 36 , 725-733. [CrossRef]
- Antonovsky, A. Health, Stress and Coping; Jossey Bass Inc.: San Francisco, CA, USA, 1979.
- Antonovsky, A. Unraveling the Mystery of Health. How People Manage Stress and Stay Well; Jossey Bass Inc.: San Francisco, CA, USA, 1987.
- Arora, N. K., Finney Rutten, L. J., Gustafson, D. H., Moser, R., & Hawkins, R. P. (2007). Perceived helpfulness and impact of social support provided by family, friends, and health care providers to women newly diagnosed with breast cancer. Psycho-Oncology, 16(5), 474-486. [CrossRef]
- Atlantis, E., Fahey, P., Cochrane, B., & Smith, S. (2013). Bidirectional associations between clinically relevant depression or anxiety and COPD: a systematic review and meta-analysis. Chest, 144(3), 766-777.
- Barnes, P. J. (2016). Inflammatory mechanisms in patients with chronic obstructive pulmonary disease. Journal of Allergy and ClinicalImmunology, 138(1), 16-27.
- Barton, C., Effing, T. W., & Cafarella, P. (2015). Social support and social networks in COPD: a scoping review. COPD: Journal of Chronic Obstructive Pulmonary Disease, 12(6), 690-702. [CrossRef]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbauch, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571.
- Blessing, A., Russell, P., DeBeer, B. B., & Morissette, S. B. (2023). Perceived family support buffers the impact of PTSD-depression symptoms on suicidal ideation in college students. Psychologicalreports, 00332941231175358. [CrossRef]
- Brown, E. S. (2009). Effects of glucocorticoids on mood, memory, and the hippocampus: treatment and preventive therapy. Annals of the New York Academy of Sciences, 1179(1), 41-55.
- Cafarella, P. A., Effing, T. W., USMANI, Z. A., & Frith, P. A. (2012). Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: a literature review. Respirology, 17(4), 627-638. [CrossRef]
- Carstens, J. A., & Spangenberg, J. J. (1997). Major depression: a breakdown in sense of coherence?. Psychologicalreports, 80(3_suppl), 1211-1220. [CrossRef]
- Charos, D.; Andriopoulou, M.; Kyrkou, G.; Kolliopoulou, M.; Deltsidou, A.; Bothou, A.; Vivilaki, V. Family Resilience, Support, and Functionality in Breast Cancer Patients: A Longitudinal Pre- and Post-Operative Study. Behav. Sci. 2025, 15, 880. [CrossRef]
- Chronic obstructive pulmonary disease (COPD),WHO, 6 November 2024, https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) Accessed December 2024.
- Daneker, B., Kimmel, P. L., Ranich, T., & Peterson, R. A. (2001). Depression and marital dissatisfaction in patients with end-stage renal disease and in their spouses. American journal of kidneydiseases, 38(4), 839-846. [CrossRef]
- Delgado C. Sense of coherence, spirituality, stress and quality of life in chronic illness. J NursScholarsh. 2007;39(3):229-34. PMID: 17760795. [CrossRef]
- Donias, S.; Demertzis, I. Validation of the Beck depression inventory. In 10th Hellenic Congress of Neurology and Psychiatry; Varfis, G., Ed.; University Studio Press: Thessaloniki, Greece, 1983; pp. 486–492. (In Greek).
- Dunbar, S. B., Clark, P. C., Quinn, C., Gary, R. A., & Kaslow, N. J. (2008). Family influences on heart failure self-care and outcomes. Journal of Cardiovascular Nursing, 23(3), 258-265. [CrossRef]
- Eriksson, M.; Mittelmark, M. The sense of coherence and its measurement. In The Handbook of Salutogenesis; Mittelmark, M.B., Sagy, S., Eriksson, M., Bauer, G.F., Pelikan, J.M., Lindström, B., Espnes, G.A., Eds.; Springer: Berlin/Heidelberg, Germany, 2017; pp. 97–106.
- Eriksson, M.; Mittelmark, M.B. The Sense of Coherence and Its Measurement. In The Handbook of Salutogenesis; Springer International Publishing: Cham, Switzerland, 2016.
- Evans, R. L., Bishop, D. S., Matlock, A. L., Stranahan, S., Halar, E. M., & Noonan, W. C. (1987). Prestroke family interaction as a predictor of stroke outcome. Archives of Physical Medicine and Rehabilitation, 68(8), 508-512.
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149. [CrossRef]
- Feldt, T., Leskinen, E., Koskenvuo, M., Suominen, S., Vahtera, J., & Kivimäki, M. (2011). Development of sense of coherence in adulthood: a person-centered approach. The population-based HeSSup cohort study. Quality of Life Research, 20(1), 69-79. [CrossRef]
- Fok, S. K., Chair, S. Y., & Lopez, V. (2005). Sense of coherence, coping and quality of life following a critical illness. Journal of advanced nursing, 49(2), 173-181. [CrossRef]
- Fry, M., McLachlan, S., Purdy, S., Sanders, T., Kadam, U. T., & Chew-Graham, C. A. (2016). The implications of living with heart failure; the impact on everyday life, family support, co-morbidities and access to healthcare: a secondary qualitative analysis. BMC familypractice, 17, 1-8. [CrossRef]
- Gabriel, R., Figueiredo, D., Jácome, C., Cruz, J., & Marques, A. (2014). Day-to-day living with severe chronic obstructive pulmonary disease: towards a family-based approach to the illness impacts. Psychology & Health, 29(8), 967-983. [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2024 Report). https://goldcopd.org/2024-gold-report/. Accessed December 2024.
- Gordon, C. S., Waller, J. W., Cook, R. M., Cavalera, S. L., Lim, W. T., &Osadnik, C. R. (2019). Effect of pulmonary rehabilitation on symptoms of anxiety and depression in COPD: a systematic review and meta-analysis. Chest, 156(1), 80-91.
- Gostin, L. O., & Wiley, L. F. (2020). Governmental public health powers during the COVID-19 pandemic: stay-at-home orders, business closures, and travel restrictions. Jama, 323(21), 2137-2138.
- Guo, L. N., Liu, Y. J., McCallum, J., Söderhamn, U., Ding, X. F., Yv, S. Y., ... & Guo, Y. R. (2018). Perceived stress and depression amongst older stroke patients: Sense of coherence as a mediator?. Archives of Gerontology and Geriatrics, 79, 164-170. [CrossRef]
- Halding, A. G., Heggdal, K., & Wahl, A. (2011). Experiences of selfblame and stigmatisation for selfinfliction among individuals living with COPD. Scandinavian journal of caring sciences, 25(1), 100-107. [CrossRef]
- Hayes, A. F. (2015). An index and test of linear moderated mediation. Multivariate behavioral research, 50(1), 1-22. [CrossRef]
- Hayes, A. F., & Rockwood, N. J. (2020). Conditional process analysis: Concepts, computation, and advances in the modeling of the contingencies of mechanisms. American Behavioral Scientist, 64(1), 19-54. [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; The Guilford Press: New York, NY, USA, 2013; Available online: http://www.afhayes.com (accessed on 25 March 2025).
- Homętowska H, Klekowski J, Świątoniowska-Lonc N, Jankowska-Polańska B, Chabowski M. Fatigue, Depression, and Anxiety in Patients with COPD, Asthma and Asthma-COPD Overlap. Journal of Clinical Medicine. 2022; 11(24):7466. [CrossRef]
- Ilias I, Tselebis A, Theotoka I, Hatzimichelakis E. Association of perceived family support through glycemic control in native Greek patients managing diabetes with diet alone. Ethn Dis. 2004 Winter;14(1):2. PMID: 15002916.
- Ilias, I.,Hatzimichelakis, E., Souvatzoglou, A., Anagnostopoulou, T., &Tselebis, A. (2001). Perception of Family Support is Correlated with Glycemic Control in Greeks with Diabetes Mellitus. Psychological Reports, 88(3), 929-930. [CrossRef]
- Jeffery, P. K. (2000). Comparison of the structural and inflammatory features of COPD and asthma Giles F. Filley Lecture. Chest, 117(5), 251S-260S.
- Jiménez-Fernández, S., Gurpegui, M., Garrote-Rojas, D., Gutiérrez-Rojas, L., Carretero, M. D., & Correll, C. U. (2022). Oxidative stress parameters and antioxidants in adults with unipolar or bipolar depression versus healthy controls: Systematic review and meta-analysis. Journal of affective disorders, 314, 211-221. [CrossRef]
- Kang, H. (2021). Sample size determination and power analysis using the G* Power software. Journal of educational evaluation for health professions, 18. [CrossRef]
- Keil, D. C., Vaske, I., Kenn, K., Rief, W., & Stenzel, N. M. (2017). With the strength to carry on: the role of sense of coherence and resilience for anxiety, depression and disability in chronic obstructive pulmonary disease. Chronic respiratory disease, 14(1), 11-21.
- Khaira, A., Mahajan, S., Khatri, P., Bhowmik, D., Gupta, S., & Agarwal, S. K. (2012). Depression and marital dissatisfaction among Indian hemodialysis patients and their spouses: a cross-sectional Study. Renalfailure, 34(3), 316-322. [CrossRef]
- Kim, E. S., Lee, S. J., Ryu, O. H., Lee, J. Y., Yun, H. S., & Choi, M. G. (2007). The relationship of family support with blood glucose control in elderly type 2 diabetic patients. The Journal of KoreanDiabetes Association, 31(5), 435-443.
- Kline, R.B. Methodology in the Social Sciences. Principles and Practice of Structural Equationmodeling; Guilford Press: New York, NY, USA, 1998.
- Koutsimani, P., & Montgomery, A. (2023). A two-wave study on the associations of burnout with depression and anxiety: The mediating and moderating role of perceived family support. Psychological Reports, 126(1), 220-245. [CrossRef]
- Kouvonen, A. M., Väänänen, A., Vahtera, J., Heponiemi, T., Koskinen, A., Cox, S. J., & Kivimäki, M. (2010). Sense of coherence and psychiatric morbidity: a 19-year register-based prospective study. Journal of epidemiology&communityhealth, 64(3), 255-261. [CrossRef]
- Krishnadas, Rajeev, and Jonathan Cavanagh. "Depression: an inflammatory illness?." Journal of Neurology, Neurosurgery & Psychiatry 83.5 (2012): 495-502.
- Kristofferzon, M. L., Engström, M., & Nilsson, A. (2018). Coping mediates the relationship between sense of coherence and mental quality of life in patients with chronic illness: a cross-sectional study. Quality of liferesearch, 27, 1855-1863. [CrossRef]
- Lin, C. Y., Harnod, T., Lin, C. L., & Kao, C. H. (2020). Suicide attempt and suicidal drug overdose in chronic obstructive pulmonary disease patients with or without depression. Frontiers in psychiatry, 11, 270.
- Lindqvist, G., & Hallberg, L. R. (2010). ‘Feelings of Guilt due to Self-inflicted Disease’ A Grounded Theory of Suffering from Chronic Obstructive Pulmonary Disease (COPD). Journal of Health Psychology, 15(3), 456-466.
- Liu, T., Zhong, S., Liao, X., Chen, J., He, T., Lai, S., & Jia, Y. (2015). A meta-analysis of oxidative stress markers in depression. PloS one, 10(10), e0138904. [CrossRef]
- MacNee, W. (2005). Pathogenesis of chronic obstructive pulmonary disease. Proceedings of the American thoracicsociety, 2(4), 258-266.
- Maurer J, Rebbapragada V, Borson S, Goldstein R, Kunik M, Yohannes AM et al. Anxiety and Depression in COPD. Chest 2008, 134:43S–56S. [CrossRef]
- Maurer, J.; Rebbapragada, V.; Borson, S.; Goldstein, R.; Kunik, M.E.; Yohannes, A.M.; Hanania, N.A. Anxiety and Depression in COPD. Chest 2008, 134, 43S–56S. [CrossRef]
- Merakou, K., Koutsouri, A., Antoniadou, E., Barbouni, A., Bertsias, A., Karageorgos, G., &Lionis, C. (2013). Sense of coherence in people with and without type 2 diabetes mellitus: an observational study from Greece. Mentalhealth in familymedicine, 10(1), 3.
- Miravitlles, M., & Ribera, A. (2017). Understanding the impact of symptoms on the burden of COPD. Respiratory research, 18(1), 67. [CrossRef]
- Moksnes, U. K., Espnes, G. A., &Lillefjell, M. (2012). Sense of coherence and emotional health in adolescents. Journal of adolescence, 35(2), 433-441.
- Moretta, P.; Cavallo, N.D.; Candia, C.; Lanzillo, A.; Marcuccio, G.; Santangelo, G.; Marcuccio, L.; Ambrosino, P.; Maniscalco, M. Psychiatric Disorders in Patients with Chronic Obstructive Pulmonary Disease: Clinical Significance and Treatment Strategies. J. Clin. Med. 2024, 13, 6418. [CrossRef]
- Moussas G, Tselebis A, Karkanias A, Stamouli D, Ilias I, Bratis D, Vassila-Demi K. A comparative study of anxiety and depression in patients with bronchial asthma, chronic obstructive pulmonary disease and tuberculosis in a general hospital of chest diseases. Ann Gen Psychiatry. 2008 May 21;7:7. PMID: 18495038; PMCID: PMC2430563. [CrossRef]
- Nahlén, C., &Saboonchi, F. (2010). Coping, sense of coherence and the dimensions of affect in patients with chronic heart failure. European Journal of CardiovascularNursing, 9(2), 118-125..
- Ng, T. P., Niti, M., Tan, W. C., Cao, Z., Ong, K. C., & Eng, P. (2007). Depressive symptoms and chronic obstructive pulmonary disease: effect on mortality, hospital readmission, symptom burden, functional status, and quality of life. Archives of internal medicine, 167(1), 60-67.
- Nilsson, K. W., Leppert, J., Simonsson, B., & Starrin, B. (2010). Sense of coherence and psychological well-being: improvement with age. Journal of Epidemiology & Community Health, 64(4), 347-352. [CrossRef]
- Odajima, Y., & Sumi, N. (2018). Factors related to sense of coherence in adult patients with Type 2 diabetes. Nagoyajournal of medicalscience, 80(1), 61. [CrossRef]
- Pachi, A., Anagnostopoulou, M., Antoniou, A., Papageorgiou, S. M., Tsomaka, E., Sikaras, C., ... &Tselebis, A. (2023). Family support, anger and aggression in health workers during the first wave of the pandemic. AIMS Public Health, 10(3), 524.
- Pachi, A.; Sikaras, C.; Ilias, I.; Panagiotou, A.; Zyga, S.; Tsironi, M.; Baras, S.; Tsitrouli, L.A.; Tselebis, A. Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis. Healthcare 2022, 10, 134. [CrossRef]
- Pachi, A.; Tselebis, A.; Ilias, I.; Tsomaka, E.; Papageorgiou, S.M.; Baras, S.; Kavouria, E.; Giotakis, K. Aggression, (2022) Alexithymia and Sense of Coherence in a Sample of Schizophrenic Outpatients. Healthcare 2022, 10, 1078. [CrossRef]
- Palmer, S., & Glass, T. A. (2003). Family function and stroke recovery: a review. Rehabilitationpsychology, 48(4), 255. [CrossRef]
- Patel, N. (2024). An update on COPD prevention, diagnosis, and management: The 2024 GOLD Report. The Nurse Practitioner, 49(6), 29-36.
- Pérez-Marín, M., Schoeps, K., Postigo-Zegarra, S., Montoya-Castilla, I., & Valero-Moreno, S. (2024). The Psychological Impact of Bronchial Asthma in Childhood and Adolescence. In Handbook of the Behavior and Psychology of Disease (pp. 1-24). Cham: Springer International Publishing.
- Postma, D. S., Bush, A., & van den Berge, M. (2015). Risk factors and early origins of chronic obstructive pulmonary disease. The Lancet, 385(9971), 899-909.
- Pumar, M. I., Gray, C. R., Walsh, J. R., Yang, I. A., Rolls, T. A., & Ward, D. L. (2014). Anxiety and depression—Important psychological comorbidities of COPD. Journal of thoracic disease, 6(11), 1615. [CrossRef]
- Rahi, M. S., Thilagar, B., Balaji, S., Prabhakaran, S. Y., Mudgal, M., Rajoo, S., ... & Gunasekaran, K. (2023). The impact of anxiety and depression in chronic obstructive pulmonary disease. Advances in RespiratoryMedicine, 91(2), 123-134. [CrossRef]
- Roncero, C.; Pérez, J.; Molina, J.; Quintano, J.A.; Campuzano, A.I.; Pérez, J.; Miravitlles, M. Frequency and Associated Factors of Suicidal Ideation in Patients with Chronic Obstructive Pulmonary Disease. J. Clin. Med. 2022, 11, 2558. [CrossRef]
- Rosland, A. M., & Piette, J. D. (2010). Emerging models for mobilizing family support for chronic disease management: a structured review. Chronic illness, 6(1), 7-21. [CrossRef]
- Ryu, M. H., Murphy, S., Hinkley, M., & Carlsten, C. (2024). COPD exposed to air pollution: a path to understand and protect a susceptible population. Chest, 165(4), 836-846.
- Sampaio, M.S.; Vieira, W.D.A.; Bernardino, Í.D.M.; Herval, Á.M.; Flores-Mir, C.; Paranhos, L.R. Chronic Obstructive Pulmonary Disease as a Risk Factor for Suicide: A Systematic Review and Meta-Analysis. Respir. Med. 2019, 151, 11–18. [CrossRef]
- Sikaras, C., Tsironi, M., Zyga, S., & Panagiotou, A. (2023). Anxiety, insomnia and family support in nurses, two years after the onset of the pandemic crisis. AIMS publichealth, 10(2), 252. [CrossRef]
- Sikaras, C.;Zyga, S.; Tsironi, M.; Tselebis, A.; Pachi, A.; Ilias, I.; Panagiotou, A. The Mediating Role of Depression and of State Anxiety οn the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis. Healthcare 2023, 11, 367. [CrossRef]
- Skärsäter, I., Langius, A., Ågren, H., Häggström, L., & Dencker, K. (2005). Sense of coherence and social support in relation to recovery in first-episode patients with major depression: A one-year prospective study. International Journal of Mental Health Nursing, 14(4), 258-264. [CrossRef]
- Skärsäter, I., Rayens, M. K., Peden, A., Hall, L., Zhang, M., Ågren, H., & Prochazka, H. (2009). Sense of coherence and recovery from major depression: a 4-year follow-up. Archives of PsychiatricNursing, 23(2), 119-127. [CrossRef]
- Smith, S. M., Sonego, S., Ketcheson, L., & Larson, J. L. (2014). A review of the effectiveness of psychological interventions used for anxiety and depression in chronic obstructive pulmonary disease. BMJ open respiratory research, 1(1). [CrossRef]
- Solano, J. P., Gomes, B., & Higginson, I. J. (2006). A comparison of symptom prevalence in far advanced cancer, AIDS, heart disease, chronic obstructive pulmonary disease and renal disease. Journal of pain and symptommanagement, 31(1), 58-69. [CrossRef]
- Stellefson M, Paige SR, Alber JM, Stewart M. COPD360social Online Community: A Social Media Review. Health Promotion Practice. 2018;19(4):489-491. [CrossRef]
- Tahery, N., Zarea, K., Cheraghi, M., Hatamzadeh, N., Farhadi, M., Dobaradarn, S., & Mohammadi, M. J. (2021). Chronic obstructive pulmonary disease (COPD) and air pollution: a review. Jundishapur Journal of ChronicDiseaseCare, 10(1).
- Thompson, K., Herens, M., van Ophem, J., &Wagemakers, A. (2021). Strengthening sense of coherence: Evidence from a physical activity intervention targeting vulnerable adults. Preventive medicine reports, 24, 101554. [CrossRef]
- Tselebis A, Kosmas E, Bratis D, Moussas G, Karkanias A, Ilias I, Siafakas N, Vgontzas A, Tzanakis N. Prevalence of alexithymia and its association with anxiety and depression in a sample of Greek chronic obstructive pulmonary disease (COPD) outpatients. Ann Gen Psychiatry. 2010 Apr 14;9:16. PMID: 20398249; PMCID: PMC2873300. [CrossRef]
- Tselebis, A., Bratis, D., Kosmas, E., Harikiopoulou, M., Theodorakopoulou, E., Dumitru, S., ... &Tzanakis, N. (2011a). Psychological symptom patterns and vital exhaustion in outpatients with chronic obstructive pulmonary disease. Annals of General Psychiatry, 10, 1-6.
- Tselebis, A., Anagnostopoulou, T., Bratis, D., Moulou, A., Maria, A., Sikaras, C., ... &Tzanakis, N. (2011 b). The 13 item Family Support Scale: Reliability and validity of the Greek translation in a sample of Greek health care professionals. Asia Pacific family medicine, 10, 1-4.
- Tselebis, A., Bratis, D., Pachi, A., Moussas, G., Karkanias, A., Harikiopoulou, M., ... &Tzanakis, N. (2013). Chronic obstructive pulmonary disease: sense of coherence and family support versus anxiety and depression. Psychiatrike= Psychiatriki, 24(2), 109-116.
- Tselebis, A., Kosmas, E., Bratis, D., Pachi, A., Ilias, I., Harikiopoulou, M., ... &Tzanakis, N. (2014). Contribution of psychological factors in dropping out from chronic obstructive pulmonary disease rehabilitation programs. BioMed Research International, 2014(1), 401326.
- Tselebis, A., Pachi, A., Ilias, I., Kosmas, E., Bratis, D., Moussas, G., &Tzanakis, N. (2016). Strategies to improve anxiety and depression in patients with COPD: a mental health perspective. Neuropsychiatricdisease and treatment, 297-328.
- Tselebis, A.; Pachi, A. (2022)Primary Mental Health Care in a New Era. Healthcare 2022, 10, 2025. [CrossRef]
- Tselebis. (2014). Psychological characteristics of patients with chronic obstructive pulmonary disease and the change in the pulmonary rehabilitation program (Doctoral dissertation, Social Medicine, Laboratory of Epidemiology, University of Crete Medical School, Heraklion). https://www.didaktorika.gr/eadd/handle/10442/42288. [CrossRef]
- Vestbo, J., Hurd, S. S., Agustí, A. G., Jones, P. W., Vogelmeier, C., Anzueto, A., ... & Rodriguez-Roisin, R. (2013). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. American journal of respiratory and critical care medicine, 187(4), 347-365.
- Vogelmeier, C. F., Criner, G. J., Martinez, F. J., Anzueto, A., Barnes, P. J., Bourbeau, J., ... & Agusti, A. (2017). Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report. GOLD executive summary. American journal of respiratory and critical care medicine, 195(5), 557-582.
- Wang, J.; Wu, X.; Lai, W.; Long, E.; Zhang, X.; Li, W.; Zhu, Y.; Chen, C.; Zhong, X.; Liu, Z.; et al. Prevalence of Depression and Depressive Symptoms among Outpatients: A Systematic Review and Meta-Analysis. BMJ Open 2017, 7, e017173. [CrossRef]
- Wood, B. L., Lim, J., Miller, B. D., Cheah, P., Zwetsch, T., Ramesh, S., & Simmens, S. (2008). Testing the biobehavioral family model in pediatric asthma: Pathways of effect. Familyprocess, 47(1), 21-40. [CrossRef]
- Xie, H., Jiang, Y., Liu, L., Peng, H., Li, J., & Chen, Z. (2023). Global prevalence and risk factors of depression in patients with chronic obstructive pulmonary disease: A systematic review and meta-analysis from 2000 to 2022. Journal of Psychosomatic Research, 175, 111537. [CrossRef]
- Yohannes, A. M. (2021). COPD patients in a COVID-19 society: depression and anxiety. Expert Review of Respiratory Medicine, 15(1), 5-7. [CrossRef]
- Yohannes, A. M., & Alexopoulos, G. S. (2014). Depression and anxiety in patients with COPD. European respiratoryreview, 23(133), 345-349.
- Young, Juan Joseph, Davide Bruno, and Nunzio Pomara. "A review of the relationship between proinflammatory cytokines and major depressive disorder." Journal of affective disorders 169 (2014): 15-20. [CrossRef]
- Zeng, W., Fang, Q., Wang, C., Tong, B., Li, D., Zou, Z. ... & Shang, S. (2022). Perceived family function and associated predictors in nurses: A cross-sectional study. Frontiers in psychiatry, 13, 904581. [CrossRef]
- Zhang, M. W., Ho, R. C., Cheung, M. W., Fu, E., & Mak, A. (2011). Prevalence of depressive symptoms in patients with chronic obstructive pulmonary disease: a systematic review, meta-analysis and meta-regression. General hospital psychiatry, 33(3), 217-223. [CrossRef]

Table 1.
Descriptive statistics of participants.
| Age | Years of disease | Fev1% | Beck Depression Inventory (BDI) | Family Support Scale (FSS) | Sense of Coherence (SOC) | ||
|
Male N=107 |
Mean | 64.916 | 8.965 | 41.454* | 11.112 | 55.418* | 64.178 |
| Std. Deviation | 8.158 | 6.276 | 20.238 | 7.150 | 7.152 | 11.347 | |
|
Female N=32 |
Mean | 63.656 | 8.059 | 52.177* | 13.719 | 51.375* | 65.344 |
| Std. Deviation | 7.740 | 9.284 | 23.264 | 8.053 | 7.694 | 12.8323 | |
| Hedges' g | 0.511 | 0,555 | |||||
|
Total N=139 |
Mean | 64.626 | 8.630 | 43.483 | 11.712 | 54.623 | 64.446 |
| Std. Deviation | 8.054 | 7.440 | 21.156 | 7.419 | 7.407 | 11,668 | |
| *t test p<0.05 | |||||||
Table 2.
Correlations among age, Years of disease, Fev1%, BDI, FSS, and SOC.
| N=139 | Age | Years of disease | Fev1% | BDI | FSS | |
| Years of disease | Pearson Correlation | 0.102 | ||||
| Sig. (2-tailed) | 0.499 | |||||
| Fev1% | Pearson Correlation | 0.033 | -0.140 | |||
| Sig. (2-tailed) | 0.730 | 0.503 | ||||
| Beck Depression Inventory (BDI) | Pearson Correlation | -0.016 | -0.202 | 0.045 | ||
| Sig. (2-tailed) | 0.856 | 0.177 | 0.640 | |||
| Family Support Scale (FSS) | Pearson Correlation | 0.144 | 0.199 | -0.188 | -0.362* | |
| Sig. (2-tailed) | 0.114 | 0.225 | 0.064 | 0.001 | ||
| Sense of Coherence (SOC) | Pearson Correlation | 0.030 | -0.057 | 0.049 | -0.609* | 0.307* |
| Sig. (2-tailed) | 0.725 | 0.708 | 0.607 | 0.001 | 0.001 | |
| N | 139 | 139 | 139 | 139 | 122 | |
| * Pearson correlations p < 0.01, (r: 0.1–03 weak correlation, 0.31–0.7 moderate correlation, 0.71–1 strong correlation.) | ||||||
Table 3.
Stepwise multiple regression
| Dependent Variable: Beck Depression Inventory (BDI) |
R Square |
R Square Change |
Beta | t | p | VIF | Durbin–Watson |
| Sense of Coherence (SOC) | 0.352 | 0.352 | -0.532 | -7.065 | 0.001 * | 1.104 | 1.869 |
| Family Support Scale (FSS) | 0.388 | 0.036 | -0.199 | -2.638 | 0.001 * | 1.104 | |
| Notes: only statistically significant variables are included; Beta = standardised regression coefficient; * correlations are statistically significant at the p < 0.001 level. | |||||||
Table 5.
Mediation analysis of Family Support Scale (FSS) on Sense of Coherence (SOC)- Beck Depression Inventory (BDI) relationship.
Table 5.
Mediation analysis of Family Support Scale (FSS) on Sense of Coherence (SOC)- Beck Depression Inventory (BDI) relationship.
| Variable | b | SE | t | p | 95% ConfidenceInterval | |
| LLCI | ULCI | |||||
| SOC→FSS | 0. 1956 | 0.0553 | 3.5356 | 0.001 | 0. 0861 | 0.3052 |
| SOC→BDI | -0.3749 | 0.0464 | -8.0768 | 0.001 | -0.4669 | -0.2830 |
| SOC→FSS → BDI | −0.1972 | 0.0748 | −2.6379 | 0.009 | −0.3453 | −0.0492 |
| Effects | ||||||
| Direct | -0.3364 | 0.0476 | -7.0646 | 0.001 | -0.4306 | -0.2421 |
| Indirect* | -0.0386 | 0.0175 | -0.0771 | -0.0101 | ||
| Total | -0.3749 | 0.0464 | -8.0768 | 0.001 | -0.4669 | -0.2830 |
| *Based on 5000 bootstrapsamples | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



