Introduction
Renal cell carcinoma (RCC) is a clinically heterogeneous and biologically complex malignancy, accounting for 3%–5% of all adult cancers and more than 80,000 new cases annually [
1]. Approximately one-quarter of patients present with metastatic disease at diagnosis, reflecting its often silent progression and aggressive behavior [
2]. Clear-cell RCC is the predominant histopathological subtype, comprising nearly 70% of cases, followed by papillary, chromophobe, and collecting duct variants [
3]. While advances in systemic therapy have significantly improved outcomes, survival remains highly variable, highlighting the continued need for accurate and clinically meaningful prognostic tools.
For more than a decade, the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) classification has served as the most widely implemented prognostic system in metastatic RCC (mRCC), incorporating readily available clinical and laboratory parameters [
4,
5]. Developed in the era of VEGF-targeted therapies [
6], the IMDC model has guided treatment selection and clinical trial stratification with considerable success. However, the rapid evolution of the therapeutic landscape—with the introduction of immune checkpoint inhibitors (ICIs), VEGF–TKI/ICI combinations, and dual immunotherapy—has revealed important limitations of the IMDC score. Notably, favorable-risk patients do not consistently derive an overall survival (OS) benefit from ICI-based combinations [
7] and the benefit of first-line nivolumab plus ipilimumab has been confirmed primarily in intermediate- and poor-risk groups [
8]. These findings underscore the need for complementary prognostic tools that more accurately reflect contemporary treatment biology.
Systemic inflammation is now recognized as a key determinant of cancer progression and therapeutic resistance across multiple tumor types [
9,
10]. Simple, inexpensive inflammatory markers derived from peripheral blood—such as neutrophil-to-lymphocyte ratio (NLR), platelet-based indices, and acute-phase reactants—have demonstrated prognostic value across diverse malignancies and therapeutic settings[
11,
12,
13,
14,
15].
Building upon the IMDC framework and acknowledging the prognostic relevance of systemic inflammation, the Meet-URO score was developed and validated in a cohort of 571 patients receiving second-line nivolumab [
16]. By incorporating baseline bone metastases and pretreatment NLR (≥3.2) into the IMDC criteria, the Meet-URO score demonstrated superior prognostic accuracy, both for patients treated with nivolumab and those receiving later-line cabozantinib [
16,
17].
Traditional molecular biomarkers such as microsatellite instability (MSI) [
18] and tumor mutational burden (TMB) [
19] have limited relevance in RCC [
20] , further emphasizing the need for alternative prognostic tools. Recent studies highlight the key role of systemic inflammation—particularly C-reactive protein (CRP)—in shaping outcomes in patients treated with ICIs [
21]. In this context, the CANLPH score has emerged as a promising, inflammation-based prognostic model. This composite index incorporates three systemic markers: the CRP-to-albumin ratio (CAR) [
22], neutrophil-to-lymphocyte ratio (NLR) and platelet-to-hemoglobin ratio (PHR) [
23,
24]. Collectively, these parameters reflect systemic inflammation, nutritional status, and hematologic physiology, offering a comprehensive assessment of host–tumor interaction.
Taken collectively, the limitations of traditional prognostic systems, the emergence of novel inflammation-based biomarkers, and the diversity of real-world treatment settings highlight the need for models that maintain prognostic performance across different therapeutic contexts. Notably, the distinct survival gradients observed in our cohort—across both Meet-URO categories and CANLPH inflammatory groups—suggest that integrating clinical and inflammatory markers may offer more robust and clinically actionable prognostic stratification.
Therefore, the present study was designed to comprehensively evaluate and compare the prognostic performance of the Meet-URO and CANLPH scoring systems in patients with metastatic RCC receiving systemic therapy. By assessing these models side-by-side in a real-world cohort, the study aims to determine whether they provide improved and clinically relevant risk discrimination beyond existing frameworks, particularly in settings where access to modern ICI-based combinations remains limited.
Materials and Methods
This retrospective, single-center observational study included 112 patients diagnosed with renal cell carcinoma (RCC) who received systemic therapy. Clinical, laboratory, and pathological data at the time of diagnosis were extracted from institutional electronic medical records. Among the full cohort, 56 patients had complete biochemical data required for calculation of the CANLPH score, while 112 patients had sufficient information for assessment of the MEET-URO score. Patients lacking one or more laboratory parameters necessary for CANLPH scoring—including C-reactive protein (CRP), albumin, neutrophil count, lymphocyte count, platelet count, and hemoglobin—were excluded from inflammation-based analyses.
All laboratory tests were obtained prior to the initiation of first-line systemic therapy, ensuring that inflammatory markers reflected pretreatment baseline values. Using these measurements, the CAR, NLR, and PHR were calculated for each patient. These indices were used both for constructing the CANLPH score and for additional exploratory analyses. Specifically, Spearman’s rank correlation was applied to evaluate the association of each marker with overall survival (OS) and progression-free survival (PFS) in the available subsets (CAR: n = 58 for OS and n = 54 for PFS; NLR: n = 104 for OS and n = 96 for PFS; PHR: n = 104 for OS and n = 96 for PFS). One-tailed significance testing was employed based on the predefined hypothesis that elevated systemic inflammation would be associated with poorer clinical outcomes.
Demographic and clinical variables collected included age, sex, histologic subtype, disease stage at diagnosis, and sites of metastasis (bone, liver, lung, central nervous system, lymph nodes, or soft tissue). Treatment-related variables recorded included the number of systemic therapy lines received and the specific first-line regimen administered (sunitinib, pazopanib, cabozantinib, or nivolumab plus cabozantinib).
The CANLPH score was constructed in accordance with the methodology described by Komura et al. [
24]. Using cut-off values determined by the Youden Index [
25], each of the following was assigned one point: CAR ≥1.5, NLR ≥2.8, and sex-specific thresholds for PHR (≥2.1 for men and ≥2.3 for women). This yielded a composite inflammation score ranging from 0 to 3 for each patient.
The Meet-URO score incorporates the presence of bone metastases and baseline neutrophil-to-lymphocyte ratio (NLR) ≥3.2 into the IMDC score (a web calculator is available here:
https://proviso.shinyapps.io/ Meet-URO15_score/) [
16]. This scoring system stratifies patients from group 1 (most favorable prognosis) to group 5 (poorest prognosis), with lower- numbered groups associated with longer survival. Previous studies have demonstrated that the Meet-URO model outperforms the IMDC model in patients with mRCC treated with second-line nivolumab or cabozantinib, as well as in those receiving first-line nivolumab plus ipilimumab [
17,
26].
OS and PFS were calculated using standard time-to-event methodology. OS was defined as the interval from diagnosis of metastatic disease to death from any cause or last follow-up. PFS was defined exclusively for first-line systemic therapy as the time from treatment initiation to radiologic or clinical progression or death. Patients without documented progression were censored at their last available disease assessment.
All statistical analyses were performed using the IBM SPSS Statistics 27.0 (IBM Corp., Armonk, NY, USA) software package. Continuous variables were described as medians (interquartile range (IQR)) and categorical variables as percentages. Survival curves and rates were estimated using the Kaplan–Meier method. The log-rank test was used to compare the survival outcomes between the groups. All reported p-values were two-sided, and p-values <0.05 were regarded as statistically significant..
Results
A total of 112 patients were included in the analysis. Baseline demographic, pathological, and clinical characteristics are presented in table 1. The cohort comprised 37 females (33.0%) and 75 males (67.0%). Clear cell renal cell carcinoma was the predominant histologic subtype (89.3%), followed by papillary (6.3%), chromophobe (1.8%), and collecting duct carcinoma (1.8%). At diagnosis, the majority of patients presented with advanced disease, with 65.2% classified as Stage IV. The most common metastatic sites were the lung (59.8%) and lymph nodes or soft tissue (60.7%), followed by bone (43.8%), liver (22.3%), and the central nervous system (8.9%). Regarding treatment exposure, 62.5% of patients had received three or more lines of systemic therapy. Sunitinib (48.2%) and pazopanib (45.5%) were the most frequently used first-line regimens, whereas cabozantinib (4.5%) and the nivolumab plus cabozantinib combination (1.8%) were less common (
Table 1).
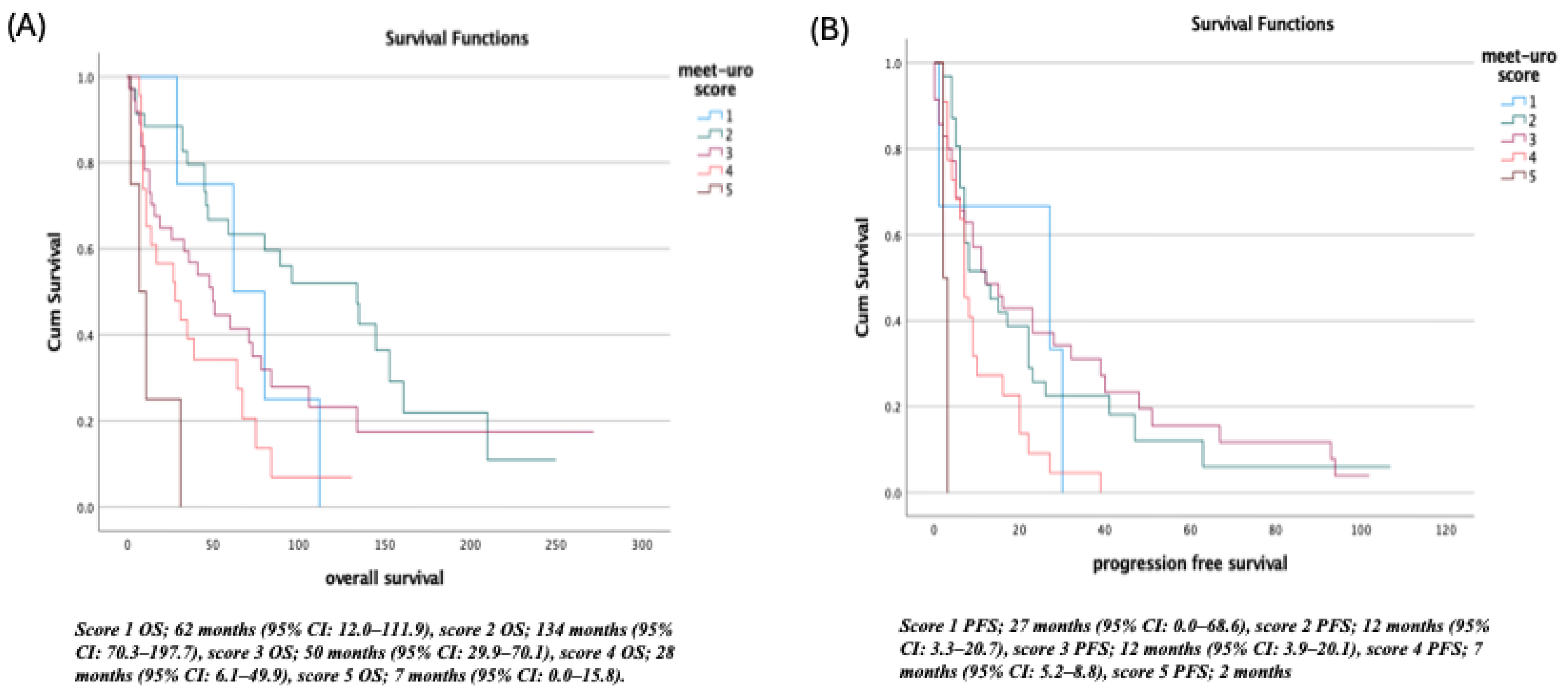
Survival Outcomes According to the MEET-URO Score
Survival analyses demonstrated a clear separation across MEET-URO risk categories. In the lowest-risk group (score 1), the median OS was 62 months (95% CI: 12.0–111.9), and PFS was 27 months (95% CI: 0.0–68.6). Patients with score 2 showed the most favorable OS at 134 months (95% CI: 70.3–197.7), while PFS was 12 months (95% CI: 3.3–20.7). In the intermediate-risk group (score 3), OS declined to 50 months (95% CI: 29.9–70.1) and PFS to 12 months (95% CI: 3.9–20.1). Higher-risk categories demonstrated progressively poorer outcomes: score 4 was associated with an OS of 28 months (95% CI: 6.1–49.9) and PFS of 7 months (95% CI: 5.2–8.8), while the highest-risk category (score 5) showed the shortest survival, with an OS of 7 months (95% CI: 0.0–15.8) and PFS of 2 months (
Figure 1).
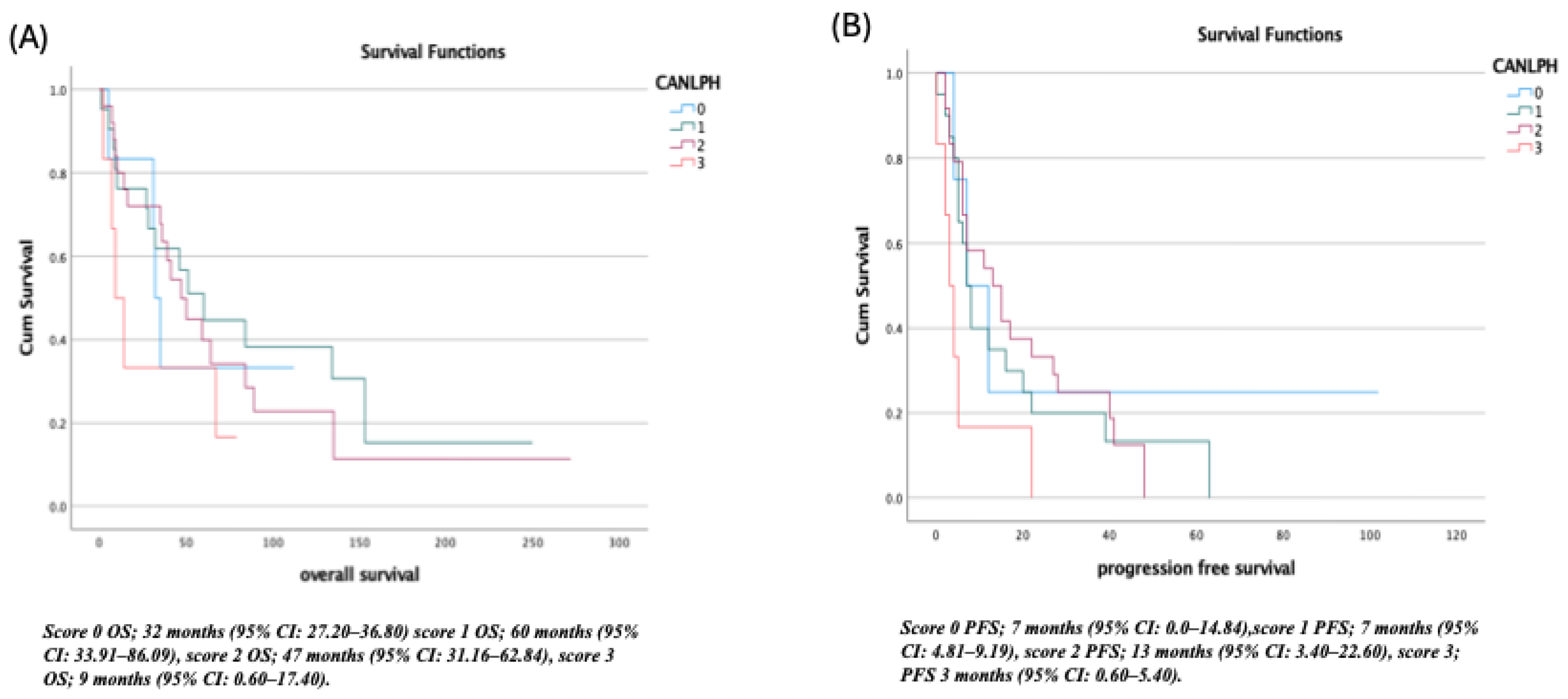
Survival Outcomes According to the CANLPH Score
Similar stratification was observed when patients were categorized according to the CANLPH score. Patients in the lowest-risk group (score 0) had a median OS of 32 months (95% CI: 27.20–36.80) and PFS 7 months (95% CI: 0.0–14.84). The score 1 group demonstrated the longest OS at 60 months (95% CI: 33.91–86.09), while PFS remained 7 months (95% CI: 4.81–9.19). For patients in the score 2 group, OS was 47 months (95% CI: 31.16–62.84) with the longest PFS observed at 13 months (95% CI: 3.40–22.60). The highest-risk group (score 3) exhibited markedly inferior outcomes, with OS falling to 9 (95% CI: 0.60–17.40) months and PFS to 3 months (95% CI: 0.60–5.40) (
Figure 2).
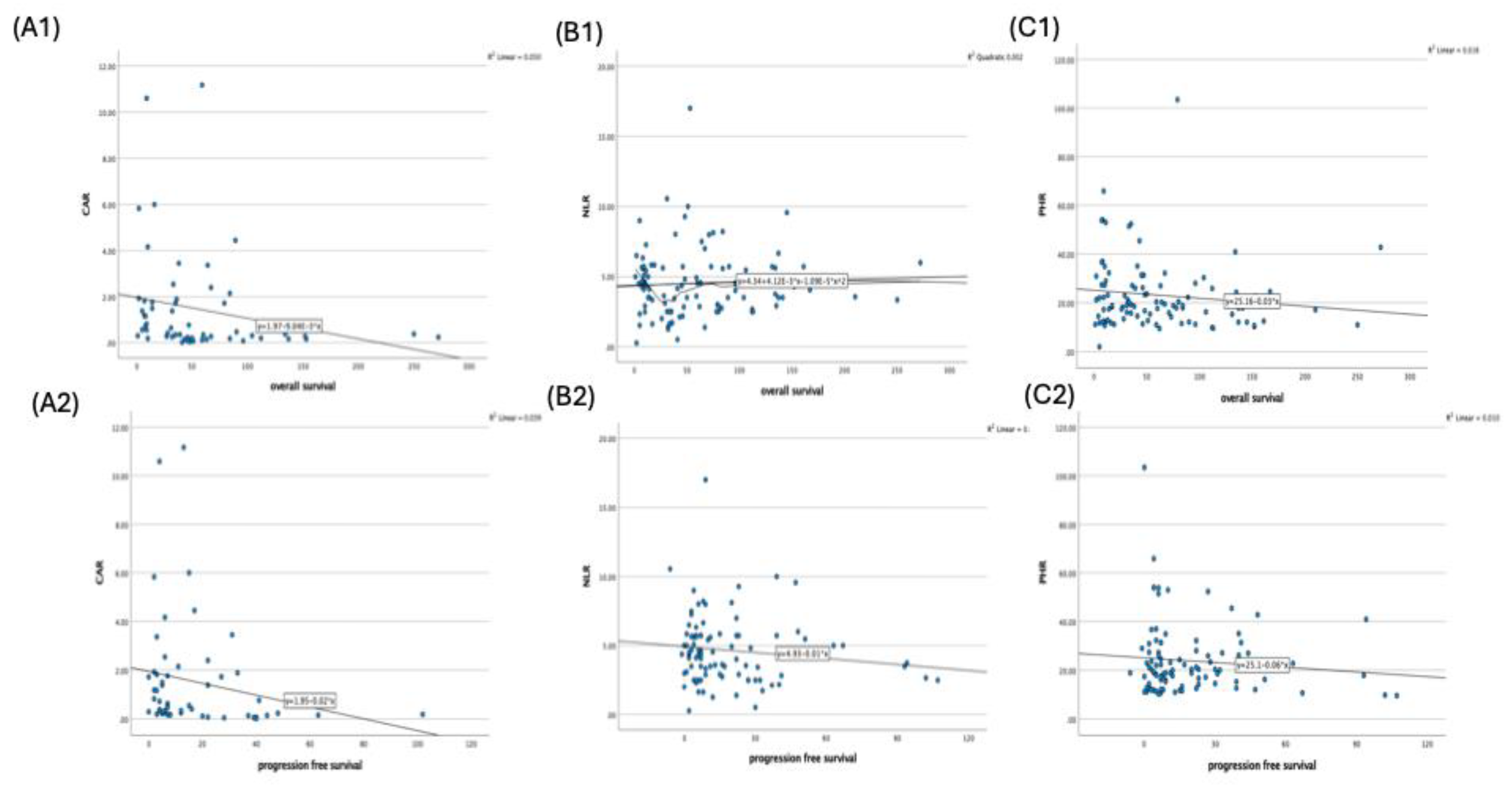
Correlation Between Inflammatory Markers and Survival Outcomes
Spearman’s correlation analysis revealed heterogeneous associations between the inflammatory biomarkers and survival endpoints (
Table 2). CAR demonstrated significant negative correlations with both OS (ρ = –0.380,
p = 0.002,
n = 58) and PFS (ρ = –0.376,
p = 0.003,
n = 54), indicating that higher baseline CAR values were associated with shorter survival. In contrast, NLR was not significantly correlated with OS (ρ = 0.041,
p = 0.341,
n = 104) or PFS (ρ = –0.149,
p = 0.074,
n = 96). PHR demonstrated a weak but statistically significant negative correlation with OS (ρ = –0.179,
p = 0.035,
n = 104), while its relationship with PFS did not reach significance (ρ = –0.047,
p = 0.324,
n = 96). These findings are illustrated in (
Figure 3).
The management of mRCC continues to evolve rapidly, driven by advances in systemic therapies and an improved understanding of tumor biology. Prognostic stratification remains essential for optimizing treatment selection, designing clinical trials, and counseling patients about expected outcomes. Historically, the IMDC score has served as the standard prognostic model for patients receiving VEGF-targeted therapies [
4,
5,
6]. However, with the emergence of ICIs, VEGF–TKI/ICI combinations, and dual checkpoint blockade, the limitations of the IMDC system have become increasingly pronounced. Multiple studies have demonstrated that patients classified as favorable-risk by IMDC may not derive a clear OS benefit from ICI-based combinations [
7]. Additionally, the confirmed benefit of nivolumab plus ipilimumab in the CheckMate-214 trial was predominantly restricted to intermediate- and poor-risk groups [
8], highlighting the need for refined prognostic tools capable of reflecting the biology and treatment response patterns of the modern therapeutic landscape.
The Meet-URO score was developed to address some of these gaps by integrating two additional variables—baseline bone metastases and pretreatment NLR—into the traditional IMDC framework [
16]. Both variables have strong biological rationale: bone metastases reflect aggressive disease biology and niche-mediated tumor support, while NLR represents systemic inflammation and dysregulated immunity, both of which are known to influence response to immunotherapy [
9,
10,
11,
12,
13,
14,
15]. Validation studies across multiple cohorts have demonstrated that Meet-URO outperforms the IMDC model in predicting OS and PFS in patients treated with second-line nivolumab, cabozantinib, and even first-line nivolumab plus ipilimumab in expanded-access programs [
16,
17,
26]. These results suggest that Meet-URO offers broader prognostic applicability across multiple treatment lines and therapeutic classes.
Our findings strongly align with the existing literature and further validate the prognostic performance of the Meet-URO scoring system. A clear and clinically meaningful separation in survival outcomes was observed across all five Meet-URO categories. Patients in score group 2—representing the most favorable profile within the non–IMDC favorable-risk population—experienced the longest survival, whereas outcomes declined progressively toward the highest-risk group (score 5), which demonstrated markedly inferior OS and PFS. The preservation of this stratification effect in our patient population is particularly noteworthy, given the distinctive treatment patterns in our cohort.
A distinctive aspect of our study is the real-world therapeutic context in which these prognostic systems were evaluated. Unlike high-income countries where ICI–TKI combinations constitute the standard first-line therapy, the vast majority of our patients received single-agent VEGFR-TKIs (mainly sunitinib or pazopanib) in the first-line setting. Limited national access to immunotherapy, financial constraints, and reimbursement restrictions—all common features of developing healthcare systems—loom as major determinants of treatment choice. Despite these constraints, Meet-URO maintained its strong discriminatory performance, reinforcing the robustness and generalizability of this scoring system beyond immunotherapy-rich environments. This finding has meaningful implications for global oncology, as it supports the utility of Meet-URO in diverse socioeconomic and therapeutic settings.
Alongside the Meet-URO score, the CANLPH score also demonstrated significant prognostic relevance in our cohort. Inflammation and nutrition-related biomarkers have increasingly gained attention as prognostic tools in cancer due to their correlation with tumor progression, host immune response, and treatment resistance [
21,
22,
23,
24]. The CANLPH model incorporates three readily available laboratory measures—CAR, NLR, and PHR—that together capture systemic inflammation, nutritional status, and hematologic physiology. Consistent with previous findings by Komura et al. [
24], we observed that higher CANLPH scores were associated with progressively shorter OS and PFS. CANLPH 0–1 groups exhibited more favorable outcomes, whereas CANLPH 3—the highest inflammatory burden—was associated with a dramatically reduced survival.
Among the individual biomarkers, CAR emerged as the strongest predictor of both OS and PFS. Elevated CAR reflects increased CRP (a marker of cytokine-driven inflammation) combined with reduced albumin (a surrogate for malnutrition and systemic metabolic stress). This dual representation of inflammation and nutritional decline has been shown to predict poor outcomes in numerous malignancies and across treatment modalities [
21,
22]. Meanwhile, NLR and PHR showed weaker and more heterogeneous associations with survival, which may reflect their sensitivity to transient physiological changes or heterogeneous disease dynamics. Nonetheless, when integrated into the CANLPH model, these markers collectively produced a robust stratification pattern, supporting the clinical value of composite inflammatory scoring systems.
The complementary prognostic performance of Meet-URO and CANLPH in our study highlights the relevance of integrating clinical, metastatic, and inflammatory characteristics into contemporary prognostic assessment. While Meet-URO incorporates tumor burden and immune-inflammatory interactions through bone metastases and NLR, CANLPH focuses more specifically on systemic inflammation and nutritional physiology. The strong prognostic gradients observed with both models underscore the multidimensional nature of mRCC biology and the potential advantage of utilizing more than one scoring system to achieve precise prognostication.
Limitations
This study has several limitations that must be considered. First, the retrospective and single-center design increases the potential for selection and information bias. Second, although 112 patients were included overall, only 56 had complete biochemical data required for CANLPH scoring, limiting the power of inflammatory biomarker analyses. Third, treatment heterogeneity—including predominant first-line TKI monotherapy due to restricted access to ICI-based combinations—may affect survival outcomes and limit comparability with international cohorts.
Finally, the absence of external validation limits the generalizability of our findings.
Future Directions
Future research should incorporate multicenter prospective studies involving larger patient populations and including those treated with modern first-line ICI–TKI combinations or dual checkpoint inhibitor regimens. Evaluating dynamic changes in inflammation-related biomarkers during treatment could provide additional prognostic information and support adaptive therapeutic strategies. Integrating established clinical models such as IMDC and Meet-URO with inflammatory or nutritional indices like CANLPH, as well as emerging biomarkers—radiomics, circulating tumor DNA, cytokine signatures, and machine-learning–based risk calculators—may further refine prognostic precision. Given the global disparities in access to immunotherapy, additional real-world studies from low- and middle-income countries are essential to ensure broad applicability and equity in prognostic assessment.
Conclusion
In conclusion, our findings demonstrate that both the Meet-URO and CANLPH scoring systems provide strong and independent prognostic information in metastatic RCC, even in a real-world population in which most patients received TKI monotherapy rather than modern immunotherapy-based combinations. Meet-URO effectively stratified risk across all five categories, while CANLPH distinguished meaningful differences in survival based on systemic inflammation and nutritional status. These results highlight the complementary nature of clinical and inflammatory prognostic models and support their integration into routine risk assessment, particularly in resource-limited settings. Further prospective validation in diverse treatment landscapes is warranted to refine and extend their clinical utility.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by Ömer Faruk Kuzu, Nuri Karadurmuş, Nebi Batuhan Kanat, Dilruba İlayda Özel Bozbağ, Berkan Karadurmuş, Esmanur Kaplan Tüzün, Hüseyin Atacan, Nurlan Mammadzada, Gizem Yıldırım, Emre HAFIZOĞLU, Musa Barış Aykan, İsmail Ertürk. The first draft of the manuscript was written by Ömer Faruk Kuzu, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
This manuscript does not report data generation or analysis. Therefore, there are no datasets available for public access.
Conflicts of Interest
The authors report no conflict of interest. The datasets used and analyzed during the current study are available from the cor-responding author on reasonable request.
Ethics Approval
Approval for the study was obtained from the Gulhane Education and Research Hospital Ethics Committee on 04 December 2025; approved number: 2025/256. This study was conducted in accordance with the guideli-nes approved by the ethics committee.
Informed Consent Statement
Due to the retrospective nature of the study, the Gulhane Education and Research Hospital Ethics Committee waived the need for obta-ining informed consent.
References
- Siegel, RL; Miller, KD; Wagle, NS; Jemal, A. Cancer statistics, 2023. CA: A Cancer Journal for Clinicians 2023, 73(1), 17–48. [Google Scholar] [CrossRef]
- Cohen, HT; McGovern, FJ. Renal-cell carcinoma. N Engl J Med. 2005, 353(23), 2477–2490. [Google Scholar] [CrossRef]
- Vamesu, S; Ursica, OA; Milea, SE; et al. Same Organ, Two Cancers: Complete Analysis of Renal Cell Carcinomas and Upper Tract Urothelial Carcinomas. Medicina (Kaunas) 2024, 60(7), 1126. [Google Scholar] [CrossRef]
- Heng, DY; Xie, W; Regan, MM; et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. The Lancet Oncology 2013, 14(2), 141–148. [Google Scholar] [CrossRef]
- Heng, DYC; Xie, W; Regan, MM; et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol. 2009, 27(34), 5794–5799. [Google Scholar] [CrossRef]
- Comparative Effectiveness of First-Line Immune Checkpoint Inhibitors Plus Tyrosine Kinase Inhibitors According to IMDC Risk Groups in Metastatic Renal Cell Carcinoma: A Meta-Analysis: Immunotherapy. No 9 - Get Access. Accessed November 20, 2025. https://www.tandfonline.com/doi/full/10.2217/imt-2021-0005. Vol 13. (accessed on 20 November 2025).
- Ciccarese, C; Iacovelli, R; Porta, C; et al. Efficacy of VEGFR-TKIs plus immune checkpoint inhibitors in metastatic renal cell carcinoma patients with favorable IMDC prognosis. Cancer Treatment Reviews 2021, 100, 102295. [Google Scholar] [CrossRef]
- Escudier, B; Motzer, RJ; Tannir, NM; et al. Efficacy of Nivolumab plus Ipilimumab According to Number of IMDC Risk Factors in CheckMate 214. European Urology 2020, 77(4), 449–453. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D; Weinberg, RA. Hallmarks of cancer: the next generation. Cell. 2011, 144(5), 646–674. [Google Scholar] [CrossRef]
- Bersanelli, M; Cortellini, A; Buti, S. The interplay between cholesterol (and other metabolic conditions) and immune-checkpoint immunotherapy: shifting the concept from the inflamed tumor to the inflamed patient. Hum Vaccin Immunother. 2021, 17(7), 1930–1934. [Google Scholar] [CrossRef] [PubMed]
- Templeton, AJ; McNamara, MG; Šeruga, B; et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014, 106(6), dju124. [Google Scholar] [CrossRef]
- Templeton, AJ; Ace, O; McNamara, MG; et al. Prognostic role of platelet to lymphocyte ratio in solid tumors: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2014, 23(7), 1204–1212. [Google Scholar] [CrossRef]
- Kumarasamy, C; Sabarimurugan, S; Madurantakam, RM; et al. Prognostic significance of blood inflammatory biomarkers NLR, PLR, and LMR in cancer-A protocol for systematic review and meta-analysis. Medicine (Baltimore) 2019, 98(24), e14834. [Google Scholar] [CrossRef]
- Shao, Y; Wu, B; Jia, W; Zhang, Z; Chen, Q; Wang, D. Prognostic value of pretreatment neutrophil-to-lymphocyte ratio in renal cell carcinoma: a systematic review and meta-analysis. BMC Urol. 2020, 20(1), 90. [Google Scholar] [CrossRef]
- Brighi, N; Farolfi, A; Conteduca, V; et al. The Interplay between Inflammation, Anti-Angiogenic Agents, and Immune Checkpoint Inhibitors: Perspectives for Renal Cell Cancer Treatment. Cancers (Basel) 2019, 11(12), 1935. [Google Scholar] [CrossRef] [PubMed]
- Inflammatory indices and clinical factors in metastatic renal cell carcinoma patients treated with nivolumab: the development of a novel prognostic score (Meet-URO 15 study) - Sara Elena Rebuzzi, Alessio Signori, Giuseppe Luigi Banna, Marco Maruzzo, Ugo De Giorgi, Paolo Pedrazzoli, Andrea Sbrana, Paolo Andrea Zucali, Cristina Masini, Emanuele Naglieri, Giuseppe Procopio, Sara Merler, Laura Tomasello, Lucia Fratino, Cinzia Baldessari, Riccardo Ricotta, Stefano Panni, Veronica Mollica, Mariella Sorarù, Matteo Santoni, Alessio Cortellini, Veronica Prati, Hector Josè Soto Parra, Marco Stellato, Francesco Atzori, Sandro Pignata, Carlo Messina, Marco Messina, Franco Morelli, Giuseppe Prati, Franco Nolè, Francesca Vignani, Alessia Cavo, Giandomenico Roviello, Francesco Pierantoni, Chiara Casadei, Melissa Bersanelli, Silvia Chiellino, Federico Paolieri, Matteo Perrino, Matteo Brunelli, Roberto Iacovelli, Camillo Porta, Sebastiano Buti, Giuseppe Fornarini, 2021. Accessed November 20, 2025. https://journals.sagepub.com/doi/full/10.1177/17588359211019642.
- Rebuzzi, SE; Cerbone, L; Signori, A; et al. Application of the Meet-URO score to metastatic renal cell carcinoma patients treated with second- and third-line cabozantinib. Ther Adv Med Oncol. 2022, 14, 17588359221079580. [Google Scholar] [CrossRef] [PubMed]
- Wilbur, HC; Le, DT; Agarwal, P. Immunotherapy of MSI Cancer: Facts and Hopes. Clin Cancer Res. 2024, 30(8), 1438–1447. [Google Scholar] [CrossRef]
- Turajlic, S; Litchfield, K; Xu, H; et al. Insertion-and-deletion-derived tumour-specific neoantigens and the immunogenic phenotype: a pan-cancer analysis. Lancet Oncol. 2017, 18(8), 1009–1021. [Google Scholar] [CrossRef]
- Motzer, RJ; Choueiri, TK; McDermott, DF; et al. Biomarker analysis from CheckMate 214: nivolumab plus ipilimumab versus sunitinib in renal cell carcinoma. J Immunother Cancer 2022, 10(3), e004316. [Google Scholar] [CrossRef] [PubMed]
- Barth, DA; Moik, F; Steinlechner, S; et al. Early kinetics of C reactive protein for cancer-agnostic prediction of therapy response and mortality in patients treated with immune checkpoint inhibitors: a multicenter cohort study. J Immunother Cancer 2023, 11(12), e007765. [Google Scholar] [CrossRef]
- Tsujino, T; Komura, K; Hashimoto, T; et al. C-reactive protein-albumin ratio as a prognostic factor in renal cell carcinoma - A data from multi-institutional study in Japan. Urol Oncol. 2019, 37(11), 812.e1–812.e8. [Google Scholar] [CrossRef]
- Ko, JJ; Xie, W; Kroeger, N; et al. The International Metastatic Renal Cell Carcinoma Database Consortium model as a prognostic tool in patients with metastatic renal cell carcinoma previously treated with first-line targeted therapy: a population-based study. Lancet Oncol. 2015, 16(3), 293–300. [Google Scholar] [CrossRef]
- Komura, K; Hashimoto, T; Tsujino, T; et al. The CANLPH Score, an Integrative Model of Systemic Inflammation and Nutrition Status (SINS), Predicts Clinical Outcomes After Surgery in Renal Cell Carcinoma: Data From a Multicenter Cohort in Japan. Ann Surg Oncol. 2019, 26(9), 2994–3004. [Google Scholar] [CrossRef]
- Youden, WJ. Index for rating diagnostic tests. Cancer 1950, 3(1), 32–35. [Google Scholar] [CrossRef] [PubMed]
- Rebuzzi, SE; Signori, A; Buti, S; et al. Validation of the Meet-URO score in patients with metastatic renal cell carcinoma receiving first-line nivolumab and ipilimumab in the Italian Expanded Access Program. ESMO Open. 2022, 7(6), 100634. [Google Scholar] [CrossRef] [PubMed]
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).