
Submitted:
29 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Background: Achilles tendinopathy (AT) is a debilitating condition with limited therapeutic options in patients contraindicated for corticosteroids. Injective collagen has emerged as a promising alternative, yet evidence in fragile populations such as diabetics remains scarce. Objective: Aim of present work was to evaluate the clinical effectiveness of Porcine collagen injections in diabetic patients with chronic AT, looking for the pain reduction and increase of functionality. Methods: Twenty-two diabetic patients with degenerative Achilles tendinopathy unresponsive to treatment were included were splited in two groups, according the type of AT pathology: Insertional (I) and non-insertional (NI). Patients received five weekly peritendinous injections of porcine collagen. Outcome measures included VAS (baseline, post-2nd injection, 1 month, 6 months), VISA-A at 6 months, return-to-activity time and adverse events monitoring. Additional variables included BMI, HbA1c, symptom duration, and previous treatments. Analyses included descriptive statistics, paired t-tests, regression models, and ANOVA tests. Results: All patients completed the protocol with no adverse events. Mean VAS decreased significantly from baseline to 6 months in both AT-I and AT-NI patients (mean delta VAS: 5.1 and 4.4, respectively; p=0.001). Mean delta VISA-A scores were 32.78 and 38.97 in AT-I and AT-NI (p<0.0001) and median return to work (RTW) were 37 and 35 days in AT-I and AT-NI, respectively (p=ns). No significant differences were discovered comparing AT-I vs AT-NI, in terms both VAS and VISA-A variation per ml of injected product (p=ns). Conclusions: Porcine collagen is a safe, effective, and sustainable treatment for Achilles tendinopathy in diabetic patients with both AT-I and AT-NI conditions. This study supports its adoption as a first-line of conservative approach for pain reduction and functionality improvement.
Keywords:
diabetic patients
; Achilles tendinopathy
; pain
; VAS
; VISA-A
; collagen injection
; BMI
; return to work
1. Introduction
The Achilles tendon in medicine is also known as the “triceps surae”. It is the strongest and thickest tendon in the entire human body [1]. This tendon connects with the aponeuroses of the gastrocnemius, soleus, and plantaris muscles and joins them to the calcaneus bone [2]. The outer sheath of the tendon is a sheath-like structure made up of a single layer of cells; it is not a true synovial sheath, but rather a “false sheath” called the paratenon [2,3,4]. The paratenon significantly contributes to providing blood supply to the tendon [4]. The Achilles tendon is essential for allowing the calf muscles to exert force on the heel; this function becomes crucial for walking and running correctly [5,6,7]. The Achilles tendon can be affected by various pathological conditions such as insertional [2,8] and non-insertional tendinitis [9,10], paratenonitis [11,12] and tendon rupture [13,14]. Tendinopathy is one of the most common conditions affecting the Achilles tendon. The factors and causes triggering Achilles tendinopathy (AT) are divided into two main groups: intrinsic factors and extrinsic factors [5,6,7]:
- Intrinsic factors:
These include anatomic factors, age, sex, metabolic dysfunction [15] foot cavity, dysmetria, muscle weakness, imbalance, gastrocnemius dysfunction [16], anatomical variation of the plantaris muscle [17], tendon vascularization [18] and torsion of the Achilles tendons [19].
- Extrinsic factors:
These include mechanical overload, constant effort [20], diabetes and obesity [21,22,23,24,25,26] medications (corticosteroids, anabolic steroids, fluoroquinolones) [27,28,29,30], hard training surfaces and direct trauma to the lower leg [31].
The pathophysiology of AT, described the anatomical abnormality of the tendon is characterized by a reduction in parallel type I collagen fibers, associated with infiltration of adipose tissue and proliferation of vascular tissue. These changes manifest as a thickening of the tendon, visible through conventional imaging diagnostics [2,32]. Furthermore, the Achilles tendon histopathology showed its composition of 95% type I collagen fibers; these fibers provide strength and flexibility to the Achilles tendon. A decrease in this type of fiber can also occur with the normal aging process or as result of injuries. In tendinopathy, which includes both tendinosis and tendinitis, the amounts of proteoglycans, water content, and disorganized type III collagen, unlike type I, increase [32]. Notably, It has been shown that advanced glycation end-products (AGEs) increase in association with diabetes pathology impacted the functionality of the Achilles tendon [33]. The changes concerning the properties and the content of collagen fibers have been associated with diabetes [23,24,25]. These morphological changes observed in tendons can also be present in the early stages of type 2 diabetes (T2DM). Since the diagnosis of T2DM is often made when some patients already show evidence of chronic complications, this implies that the effects of hyperglycemia would have already been exerted for some time on tendon structures [34,35]. Alterations in the fibrillar organization of the Achilles tendon, the presence of hypoechoic areas found on ultrasound imaging, and calcific formations within the tendon are common degenerative abnormalities [35,36].
ATs can be categorized into two groups: insertional and non-insertional [5]. Insertional (AT-I) [22,24] and non-insertional (AT-NI) [6]. Achilles tendinopathies are pathological metabolic conditions frequently found in T2DM patients [22,33,37]. These pathologies are characterized by the onset of chronic pain, which leads to progressive motor disability both in normal daily activities and during sports activities. Therefore, therapeutic effectiveness in relieving pain and improving functionality is the desired goal for both patients and specialists in this field. The scenario concerning the management of AT is very broad and complex. Physic-kinesis-therapy (FKT) always constitutes an initial starting point for AT treatment [38]. However, clinicians, responsible for selecting the best clinical treatment for the patient, often must choose between an interventional approach (surgery) and a non-interventional approach (conservative therapy). The choice of a non-surgical approach is always preferred over a surgical one, which is generally considered only in cases of Achilles tendon rupture or in instances where conservative treatment has failed. Fortunately, beneficial effects have been reported for the treatment of AT and tendinopathies in general through various conservative approaches, including the use of platelet-rich plasm [39,40], shockwaves [41,42,43], and collagen. This type of treatment has been successfully tested in various pathological conditions of the musculoskeletal system [44], such as greater trochanteric pain syndrome (GTPS) [45,46], Knee Osteoarthritis (K-OA) [47,48,49], hip tendinitis [50,51,52] and tendinopathies of the rotator cuff of the shoulder [53]. Nonetheless, In addition, it has been shown that collagen injection collaborate with by tenocytes, demonstrating its relationship with mechanical stimuli [45,54].
Having said all that, the aim of this study is to evaluate the effectiveness of porcine collagen injections, thanks to its regenerative and reparative properties as an ECM matrix scaffold [55,56], in Achilles tendons in diabetic subjects for the realignment of collagen fibers, the improvement of pain symptoms and enhanced functionality.
2. Materials and Methods
2.1. General Aspects and Inclusion Criteria
Data were acquired from 2012 to 2023 by two authors (G.P. and M.B.) to build an database of clinical and anonymized personal data. First of all, an encrypted code was created, which made it possible not to identify the patients. The patients included in this study met the following inclusion criteria:
- Diabetic patients aged ≥18 years with ultrasound-confirmed degenerative Achilles tendinopathy unresponsive to conservative therapy for ≥6 months. Diagnosis of diabetis was assessed on the basis of glycated hemoglobin (Hb1C) > 6%.
- Sportive or athletic individuals.
- Both continuous pain and impairment of functionality.
- No previous conservative surgical treatments.
- No other concomitant pathologies concerning degenerative tendinopathy.
While, the exclusion criteria included the following tips
- Tendon rupture.
- Previous surgical treatments.
- Previous infiltrative or regenerative treatments.
- No corticosteroids use.
- Declaration of absence of allergy to collagen or similar derivatives.
2.2. Protocol and Adherence to Treatment
The treatment comprised five consecutive peritendinous injections of 2 ml collagen (GUNA MD-Tissue) weekly, administered around the insertion and proximal course of the Achilles tendon through ultrasound monitoring. All patients received the collagen injection in their tendon through ultrasound-guided injection with a 22G needle (23mm in length). Before the injection, the target area was disinfected with alcohol or another antiseptic solution. As whole, complete compliance with the treatment (100% adherence) consisted of receiving all 5 doses of collagen for a total of 10 ml of administered product. Adherence to treatment will be assessed for all subjects included in the study, and the minimum clinically effective dose will be evaluated.
2.3. End Points
The aims of this study were to analyze the changes in pain reduction and the increase in functionality six months after and treatment. Nonetheless, the purpose of this study was also to monitor possible adverse events (AEs) directly related to collagen injections. The list of undesirable AEs included: persistent pain after treatment, skin rash, excessive swelling or edema, and allergic reaction.
2.4. Scoring Assessments
The VAS (Visual Analogue Scale) is a widely used clinical tool for subjectively measuring pain intensity, represented by a 10 cm line (from 0 to 10), where 0 is "no pain" and 10 is "the worst possible pain," allowing the patient to mark the point that represents their experience and the clinician to measure the distance from 0 to obtain an accurate score, useful for monitoring the effectiveness of treatments.
The progresses of the clinical status of the diabetic patients was assessed through the Victorian Institute of Sport Assessment (VISA), Achilles (-A) questionnaire, which is a report clinical outcome measure used in patients with both insertional (I) and non-insertional (NI) Achilles Tendinopathies (AT). It consists of 10 questions that measure the domains of pain, function in daily life, and sporting activities. Question 8 and question 10 each contain three subcategories (A, B, C); the patient must choose only one, thus excluding the other two. Each question from 1 to 6 has a maximum score of 10. Questions 7 and 9 have a maximum score of 5, while questions 8 and 10 have a variable score depending on the option chosen among A, B, and C, which can reach up to 15. The maximum score is 100, corresponding to that of a healthy individual with no tendinopathy symptoms. This assessment was performed at baseline before the start of treatment (T0) and after six months after treatment. Clinical conditions were monitored by evaluation of biophysical parameters to evaluate the general condition for return to work (RTW).
2.5. Statistical Procedures
The continuous variables were summarized using the following descriptive statistics: n (number), mean, standard deviation, median, maximum, and minimum. The frequency and percentages (based on the non-missing sample size) were reported for all categorical measures. The data generated in this study were recorded in a dedicated file (e.g. excel) and the original rows of data can be made available on demand.
Demographic and clinical data of the following variables were aquired: age (years old), gender (male/female), weight, height, BMI calculation, pain evaluation (VAS), functionality (VISA-H score), and return to work (RTW) time.
2.6. Analytical Test Application (ATA)
GraphPad 10.0 version for Apple Computer was used for statistical analysis (PRISM, San Diego, CA, USA). The Shapiro–Wilk test was performed to determine whether the data were parametrically distributed. Both W- and p-values were calculated for all data distributions. Student’s Test (parametric and paired) was used to compare treatment results at the T0 and T1 visits. ANOVA tests were performed to evaluate doth delta VAS and VISA-A output in both AT-I and AT-NI patients after treatments. All the parameters measured in this study were evaluated using the classical descriptive statistics: mean, SD, minimum and maximum, and frequencies (for qualitative variables). The log-rank test was used to assess the time to return to work (RTW) outcomes (hazard ratio; (95% CI). For quantitative analyses, all statistical results were considered significant if the p-value was less than 0.05 (p < 0.05).
3. Results
3.1. Demographic and Clinical Data
The demographic and clinical data of the 22 patients included in the study were reported in Figure 1. No statistically significant differences were observed regarding the distribution of gender (12M vs 10F; Figure 1A) and age (64.1±5.1 M vs 58.0±7.2 F vs 61.3±6.7 All; Figure 1B) among the enrolled subjects. All subjects were classified as diabetic patients based on the distribution of glycated hemoglobin values (8.2±1.5 M vs 8.2±0.9 F vs 8.2±1.2 All; Figure 1C; p=0.9911) and Body Mass Index (BMI) values (29.1±3.7 M vs 28.1±2.1 F vs 28.6±3.1 All; Figure 1D; p=0.8004). From a clinical perspective, patients were divided based on the type of Achilles tendinopathy (ATs; Figure 1E) into two groups: Insertional (I; n=13) and Non-Insertional (NI; n=9). The duration of symptoms was recorded for each patient and no statistically significant differences were found between subjects with AT-I and those with AT-NI (13.3 vs 17.4; Figure 1F; p=0.1477). Porcine collagen treatment was applied equally to both groups, which were shown to have homogeneous characteristics.
3.2. VAS Results
The positive changes in VAS (Figure 2), was observed as early as two weeks and increases up to the twenty-fourth week (Figure 2A; p<0.0001). The pattern of VAS change follows a consistent hyperbolic trend, both for patients with AT-I and for those with AT-NI. The curves are parallel to each other, with a slight predominance in the AT-I patient group (Figure 2B). These differences remain consistent between the two curves throughout the treatment period and the differences at each step (2, 4, and 24 weeks) are statistically significant for both groups over time (Figure 2C; p<0.0001).
This is in agreement on the treatment revealing similar clinical results between the two groups regarding the return to work interval (RTW; Figure 1D), where no statistically significant differences were observed between AT-I and AT-NI groups. The average differences (measured in days for RTW) were respectively: 35 vs 37 days (p=0.2268; HR=1.057). The protocol provided the administration of 5 doses of collagen, each 2ml (A total of 10 ml). The compliance with the protocol was complete in 77% of cases (Complete Adherence (CA; 5 doses), while incomplete adherence (IA; 4 doses) was observed in 23% of cases. However, the change in VAS at six months was not statistically significant between the two groups (Figure 2E; p=ns). Even with 4 doses, the treatment's efficacy was demonstrated. Finally, the improvement in VAS in terms of score points per ml of collagen applied was a little better in patients with AT-I vs AT-NI (Figure 2F; p=0.0044), although the average infiltrated volumes were identical (9.38 vs 9.78).
3.3. VISA-A Results
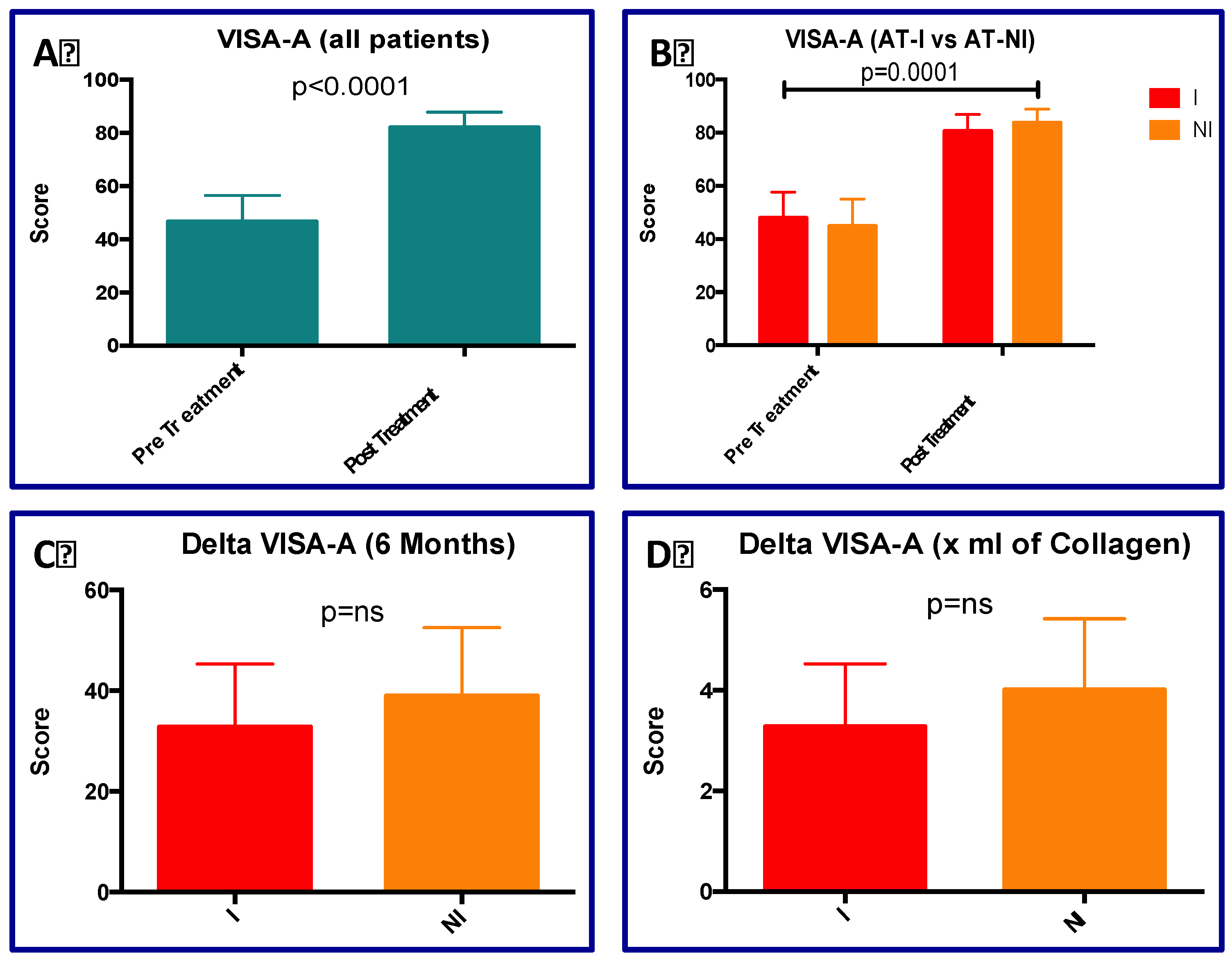
The statistical analysis concerning the VISA-A score (Figure 3) revealed a significant variation of mean values comparing pre- vs post-treatment in all patients (45.50 vs 82.70, p<0.00001; Figure 3A). Indeed, ANOVA analysis looking for the VISA-A variation in TA-I vs AT-NI pre- and post-treatment showed significant difference for the treatment (p<0.0001; Figure 3B), while no statistically significant differences were observed between the two types of tendinopathies (p=0.2222; Figure 3B). The delta VISA-A scores (at a 6-month follow-up) were equal to 32.78 vs 38.97 for AT-I and AT-NI, respectively (p=0.6523; Figure 3C). Numerical change of VISA-A per unit of collagen injected in the two types of ATs (I vs NI) were 3.28 vs 4.01, respectively (p=0.4961; Figure 3D). Although in this last analysis the differences are not statistically significant, AT-NI patients seem to benefit more from collagen treatment.
3.4. Adverse Events (AEs)
Throughout the duration of this study, no adverse events associated with Porcine collagen administration were reported, among those included and reported in the materials and methods section.
4. Discussion
Achilles tendinopathies are certainly associated with external factors such as prolonged activities, even under load stress, but systemic comorbidities can be a risk factor for tendon injuries, directly affecting their structure by changing the arrangement of collagen fibers in the tendon [57,58]. Intrinsic pathological factors such as quality, body mass index (BMI), diet, metabolic diseases, foot alterations like high arches, directly influence the health of tendons and their structure in different ways and have all been confirmed as risk factors for tendinopathies, including Achilles tendinopathies [59,60]. Diabetes is associated with tendinopathy by altering cellular metabolism [59], increasing intracellular water content leading to edema; decreasing the ability to tolerate ischemic stress; and increasing cross-links within collagen fibers due to advanced glycation end products, thus altering tissue structure [61]. Disorganization of collagen fibrils can also be a consequence of dyslipidemia, which leads to reduced tissue density, or hypercholesterolemia, where abnormal fat deposits can be macroscopically visible in tendons, forming xanthomas [58]. Long-term morbidity with unpredictable clinical outcomes is a clinical situation that can occur in diabetic patients with AT. Initial management is conservative, with many patients showing satisfactory results [58,60]. Physiotherapy and kinesitherapy are usually the first conservative approach, while surgical treatment is generally left as a last option [62,63,64]. A whole range of local conservative approaches are available for the treatment of tendinopathies. Among those shown to have a beneficial effect are: the use of platelet-rich plasm [39,40], shockwaves [41,42,43] and collagen [65,66,67,68]. Although collagen has been shown to have a positive effect in various tendinopathies, it is rarely used in both insertional and non-insertional AT thanks to its regenerative and reparative properties as an ECM matrix scaffold. In this study, the use of collagen seems to be justified and supported by the fact that diabetic patients have an altered collagen structure due to the side effects of excessive glycosylation [58,60,61]. The change in the type of collagen fibers in the tendon is indeed one of the reasons underlying tendinopathies in diabetic patients [69]. In the present study, the application of collagen improved functionality and reduced pain in diabetic patients affected by both insertional and non-insertional Achilles tendinopathy. In fact, improvement was observed in terms of changes in the VAS (Figure 2) and VISA-A (Figure 3). The clinical effect of collagen application can probably be explained by the fact that in vitro studies have shown the role of collagen as a modulator of the regenerative and morpho-functional activities of tenocytes [55,56]. Herein, the results of present analyses, concerning the improvements in VAS and VISA-A parameters, seem to be in line with those obtained with other conservative approaches such as platelet-rich-plasma [70] and extracorporeal shock waves [71]. These results seem to indicate a possible alternative for the treatment of Achilles tendinopathies in diabetic patients, where even pharmacological approaches also are challenging [60,72,73,74], as the treatment of Achilles tendinopathy with corticosteroids is strongly contraindicated, although literature reports positive results in this regard [75]. From a pharmacological standpoint, other substances, such as antibiotics, are also strongly contraindicated in the treatment of these conditions, even in non-diabetic patients [76,77].
As a whole, Looking at our results observed we found the following points of interest for improving the clinical condition of diabetic patients with Achilles tendon tendinopathy:
- The positive change in VAS is observable already after two weeks and increases up to week 24.
- The product acts positively on both diabetic patients with AT-I and those with AT-NI. The results seem to indicate a good efficacy of the product in terms of pain reduction already after 2 weeks looking for a hyperbolic increasement up to 24 weeks.
- The diabetic subjects treated with 4 doses of collagen show a sum of effects comparable to those treated with 5 doses. Four doses could already indicate an appropriate protocol for diabetic subjects with AT-I and AT-NI.
- Subjects with AT-I (typical of athletes) seem to benefit more in terms of pain improvement, but the functional evaluations of the VISA-A do not reveal statistically significant differences, although the VISA-A score is better in patients with AT-I.
This retrospective case series provides compelling evidence supporting the clinical benefit and safety of infiltrative collagen for Achilles tendinopathy in diabetic patients. The observed improvements in pain and function were rapid, sustained, and achieved without adverse events in compareson with other convervative approaches [70,71,78,79,80,81]. Comparison with existing literature indicates that collagen may offer a valid alternative to corticosteroids, particularly in fragile patients for whom steroids are contraindicated. The absence of complications further supports its safety profile. Nevertheless, it is necessary to mention the main limitations present in this study: 1) the number of subjects who underwent the treatment is still not high and a larger number of diabetic subjects affected by AT could provide greater statistical power. 2) The results obtained are based on an assessment conducted six months after the treatment. More extensive longitudinal analyses could provide more precise indications regarding the maintenance of the clinical outcome associated with collagen injection. 3) Instrumental analyses regarding the health status of the Achilles tendon could verify wheter the remodeling of the tendon might be associated with the action of collagen. However, methodological rigor, the quite complete protocol adherence by patients and the comprehensive outcome tracking, reinforce the validity of the findings rmentioned above.
5. Conclusions
Collagen injections are well tolerated and clinically effective in patients with diabetes. Improvement is noted both in terms of pain reduction and functional recovery. The treatment appears to be effective in both insertional and non-insertional Achilles tendinopathies. Diabetes seems to specifically affect the collagen fibers that make up tendons; consequently, the supply of new exogenous collagen appears to represent a direct approach against diabetes-associated tendinopathy. These results support the use of collagen injection as a first-line therapeutic alternative, thanks to its safety and effectiveness, in populations where corticosteroids are contraindicated. Future multicenter studies are needed to validate predictive models and stratified treatment strategies.
Author Contributions
Conceptualization, N.B. and V.S.; methodology, N.B.; software, M.A.M.; validation, N.B., G.P. and V.S.; formal analysis, N.B.; investigation, N.B.; resources, G.P.; data curation, M.A.M.; writing—original draft preparation, N.B.; writing—review and editing, G.P. and V.S.; visualization, M.A.M.; supervision, V.S.; project administration, G.P.; funding acquisition, V.S.
Funding
This research received no external funding.
Institutional Review Board Statement
Here, approval from the ethics committee was not necessary since it is a retrospective analysis on anonymized data. This aspect is regulated by law no. 675/1996 of the Guarantor of Privacy in Italy, in compliance with the use of personal data for scientific purposes. According to Italian national regulations (Ministerial Decree of 17 December 2004, and AIFA Guidelines for Observational Studies, 20 March 2008), as well as the European Regulation (EU) 2016/679 (GDPR) regarding data protection, and international ethical standards (Declaration of Helsinki, WMA 2013, art. 37), retrospective studies that do not involve identifiable data and do not alter the patient’s diagnostic–therapeutic path do not require prior approval by an ethics committee, provided that patient privacy and confidentiality are protected.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The raw data from the study will be made available upon request from the corresponding author of this study: Dr. Giacomo Placella.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- O’Brien, M. The Anatomy of the Achilles Tendon. Foot Ankle Clin 2005, 10, 225–238. [CrossRef]
- Chimenti, R.L.; Cychosz, C.C.; Hall, M.M.; Phisitkul, P. Current Concepts Review Update: Insertional Achilles Tendinopathy. Foot Ankle Int 2017, 38, 1160–1169. [CrossRef]
- Weinfeld, S.B. Achilles Tendon Disorders. Med Clin North Am 2014, 98, 331–338. [CrossRef]
- Ahmed, I.M.; Lagopoulos, M.; McConnell, P.; Soames, R.W.; Sefton, G.K. Blood Supply of the Achilles Tendon. J Orthop Res 1998, 16, 591–596. [CrossRef]
- Leiß, F.; Spörrer, J.-F.; Grifka, J.; Schwarz, T. Achillessehnenpathologien. Orthopädie 2023, 52, 857–866. [CrossRef]
- Medina Pabón, M.A.; Naqvi, U. Achilles Tendinopathy. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025.
- Tarantino, D.; Mottola, R.; Resta, G.; Gnasso, R.; Palermi, S.; Corrado, B.; Sirico, F.; Ruosi, C.; Aicale, R. Achilles Tendinopathy Pathogenesis and Management: A Narrative Review. IJERPH 2023, 20, 6681. [CrossRef]
- Chen, P.; Tzeng, I.; Yang, K.; Wang, C. Endoscopic versus Open Surgery for Insertional Achilles Tendinopathy: A Systematic Review and Meta-analysis of Comparative Outcomes. J. exp. orthop. 2025, 12, e70374. [CrossRef]
- Pearce, C.J.; Tan, A. Non-Insertional Achilles Tendinopathy. EFORT Open Reviews 2016, 1, 383–390. [CrossRef]
- Thermann, H.; Fischer, R.; Gougoulias, N.; Cipollaro, L.; Maffulli, N. Endoscopic Debridement for Non-Insertional Achilles Tendinopathy with and without Platelet-Rich Plasma. Journal of Sport and Health Science 2023, 12, 275–280. [CrossRef]
- Yan, X.; Yue, J.; Zeng, X.; Xu, T.; Zhang, Y.; Wang, W.; Zhao, G.; Mi, J.; Rui, Y.; Liu, S.; et al. Minimum 24-Month Outcomes of Minimally Invasive Paratenon Protection Repair vs Open Giftbox Repair of Ruptured Achilles Tendon. Foot Ankle Int. 2025, 46, 200–209. [CrossRef]
- Micheroli, R.; Ricci, V.; Naňka, O.; Tamborrini, G. Paratenon Effusion of the Achilles Tendon: A Rare Finding. Reumatismo 2025. [CrossRef]
- Lee, J.H.; Ku, K.; Kang, C.M.; D’Lima, D.D.; Baek, J.H. Safety of One-Stage Reconstruction of Achilles Tendon and Soft Tissue Defects Resulting from Infection After Achilles Tendon Repair using Flexor Hallucis Longus Tendon Transfer and Reverse Sural Artery Flap. Handchir Mikrochir Plast Chir 2025, a-2681-8656. [CrossRef]
- Buddecke, D. Acute Achilles Tendon Ruptures. Clinics in Podiatric Medicine and Surgery 2021, 38, 201–226. [CrossRef]
- Abate, M.; Salini, V. Mid-Portion Achilles Tendinopathy in Runners with Metabolic Disorders. Eur J Orthop Surg Traumatol 2019, 29, 697–703. [CrossRef]
- Zhao, H.; Ren, Y.; Roth, E.J.; Harvey, R.L.; Zhang, L.-Q. Concurrent Deficits of Soleus and Gastrocnemius Muscle Fascicles and Achilles Tendon Post Stroke. J Appl Physiol (1985) 2015, 118, 863–871. [CrossRef]
- Olewnik, Ł.; Wysiadecki, G.; Podgórski, M.; Polguj, M.; Topol, M. The Plantaris Muscle Tendon and Its Relationship with the Achilles Tendinopathy. BioMed Research International 2018, 2018, 1–9. [CrossRef]
- Yang, X.; Coleman, D.P.; Pugh, N.D.; Nokes, L.D.M. The Volume of the Neovascularity and Its Clinical Implications in Achilles Tendinopathy. Ultrasound Med Biol 2012, 38, 1887–1895. [CrossRef]
- Slane, L.C.; Dandois, F.; Bogaerts, S.; Vandenneucker, H.; Scheys, L. Non-Uniformity in the Healthy Patellar Tendon Is Greater in Males and Similar in Different Age Groups. Journal of Biomechanics 2018, 80, 16–22. [CrossRef]
- Federer, A.E.; Steele, J.R.; Dekker, T.J.; Liles, J.L.; Adams, S.B. Tendonitis and Tendinopathy. Foot and Ankle Clinics 2017, 22, 665–676. [CrossRef]
- Moon, J.L.; Moon, K.M.; Carlisle, D.M. Obesity-Related Foot Pain. Clinics in Podiatric Medicine and Surgery 2019, 36, 141–151. [CrossRef]
- Abate, M.; Salini, V.; Schiavone, C. Achilles Tendinopathy in Elderly Subjects with Type II Diabetes: The Role of Sport Activities. Aging Clin Exp Res 2016, 28, 355–358. [CrossRef]
- Department of Radiology, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Osun State, Nigeria; Afolabi, B.I.; Idowu, B.M.; Department of Radiology, Union Diagnostics and Clinic Services Plc, Yaba, Lagos, Nigeria; Onigbinde, S.O.; School of Medicine, St George’s University, Grenada Achilles Tendon Degeneration on Ultrasound in Type 2 Diabetic Patients. J Ultrason 2020, 20, 291–299. [CrossRef]
- Huang, X.; Chen, X.; Chen, X.; Chi, P.; Wang, P.; Zhan, X.; Zou, C.; Wang, L.; Dong, Y. Sound Touch Elastography of Achilles Tendons in Patients with Type 2 Diabetes Mellitus versus Healthy Adults. Diabetol Metab Syndr 2023, 15. [CrossRef]
- Łazarz, D.P.; Jasińska, M.; Dubrowski, A.; Moskała, A.; Możdżeń, K.; Malinowski, K.; Zamojska, I.; Walocha, J.A.; Lis, G.J.; Pękala, P.A. Histological Study of the Achilles Tendon in Diabetic and Non-Diabetic Individuals: Comprehensive Comparison. Folia Morphologica 2025, VM/OJS/J/107641. [CrossRef]
- Lui, P.P.Y. Tendinopathy in Diabetes Mellitus Patients—Epidemiology, Pathogenesis, and Management. Scandinavian Med Sci Sports 2017, 27, 776–787. [CrossRef]
- Ileri, S. Levofloxacin-Induced Gastrocnemius Tendon Rupture: A Case Report. J Med Case Reports 2025, 19, 228. [CrossRef]
- Bolon, B. Mini-Review: Toxic Tendinopathy. Toxicol Pathol 2017, 45, 834–837. [CrossRef]
- Alušík, Š.; Paluch, Z. [Drug induced tendon injury]. Vnitr Lek 2018, 63, 967–971.
- Godoy-Santos, A.L.; Bruschini, H.; Cury, J.; Srougi, M.; De Cesar-Netto, C.; Fonseca, L.F.; Maffulli, N. Fluoroquinolones and the Risk of Achilles Tendon Disorders: Update on a Neglected Complication. Urology 2018, 113, 20–25. [CrossRef]
- Almekinders, L.C.; Engle, C.R. Common and Uncommon Injuries in Ultra-Endurance Sports. Sports Medicine and Arthroscopy Review 2019, 27, 25–30. [CrossRef]
- Pirozzi, K.M. Histophysiology of Fibrocartilage. Clinics in Podiatric Medicine and Surgery 2022, 39, 363–370. [CrossRef]
- Zellers, J.A.; Eekhoff, J.D.; Walk, R.E.; Hastings, M.K.; Tang, S.Y.; Lake, S.P. Human Achilles Tendon Mechanical Behavior Is More Strongly Related to Collagen Disorganization than Advanced Glycation End-Products Content. Sci Rep 2021, 11, 24147. [CrossRef]
- Łazarz, D.P.; Jasińska, M.; Dubrowski, A.; Moskała, A.; Możdżeń, K.; Malinowski, K.; Zamojska, I.; Walocha, J.A.; Lis, G.J.; Pękala, P.A. Histological Study of the Achilles Tendon in Diabetic and Non-Diabetic Individuals: Comprehensive Comparison. Folia Morphologica 2025, VM/OJS/J/107641. [CrossRef]
- Department of Radiology, Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Osun State, Nigeria; Afolabi, B.I.; Idowu, B.M.; Department of Radiology, Union Diagnostics and Clinic Services Plc, Yaba, Lagos, Nigeria; Onigbinde, S.O.; School of Medicine, St George’s University, Grenada Achilles Tendon Degeneration on Ultrasound in Type 2 Diabetic Patients. J Ultrason 2020, 20, 291–299. [CrossRef]
- Klatte-Schulz, F.; Minkwitz, S.; Schmock, A.; Bormann, N.; Kurtoglu, A.; Tsitsilonis, S.; Manegold, S.; Wildemann, B. Different Achilles Tendon Pathologies Show Distinct Histological and Molecular Characteristics. IJMS 2018, 19, 404. [CrossRef]
- Giai Via, A.; Oliva, F.; Padulo, J.; Oliva, G.; Maffulli, N. Insertional Calcific Tendinopathy of the Achilles Tendon and Dysmetabolic Diseases: An Epidemiological Survey. Clinical Journal of Sport Medicine 2022, 32, e68–e73. [CrossRef]
- Karapınar, M.; Smitheman, H.P.; Cone, S.G.; Silbernagel, K.G. Effects of an Exercise Program on Calf Muscle Characteristics in Patients with Achilles Tendinopathy. Physical Therapy in Sport 2025, 76, 127–133. [CrossRef]
- Abate, M.; Paganelli, R.; Pellegrino, R.; Di Iorio, A.; Salini, V. Platelet Rich Plasma Therapy in Achilles and Patellar Tendinopathies: Outcomes in Subjects with Diabetes (A Retrospective Case-Control Study). JCM 2024, 13, 5443. [CrossRef]
- Pallikkara Kuttyadan, N.; Samad, S.; Shahzad, M.; Sanaullah, K.; Gillani, S.H.M.; Mushtaq, H.; Butt, S.B.; Hayat, S.K.; Raif, M.; Ali, S.M.; et al. Effectiveness of Platelet-Rich Plasma Injection for Chronic Achilles Tendinopathy: An Umbrella Systematic Review. Cureus 2025. [CrossRef]
- Charles, R.; Fang, L.; Zhu, R.; Wang, J. The Effectiveness of Shockwave Therapy on Patellar Tendinopathy, Achilles Tendinopathy, and Plantar Fasciitis: A Systematic Review and Meta-Analysis. Front. Immunol. 2023, 14, 1193835. [CrossRef]
- Saxena, A.; Bondi, E.; Gerdesmeyer, L.; Tenforde, A.S. Extracorporeal Shock Wave Therapy (ESWT) and Radial Pressure Waves (RPW) May Improve Post-Operative Recovery Following Insertional Achilles Tendon Surgeries: A Case-Control Pilot Study. J Orthop Surg Res 2025, 20, 751. [CrossRef]
- Stania, M.; Juras, G.; Chmielewska, D.; Polak, A.; Kucio, C.; Król, P. Extracorporeal Shock Wave Therapy for Achilles Tendinopathy. BioMed Research International 2019, 2019, 1–13. [CrossRef]
- De Lucia, O.; Giarda, F.; Bernetti, A.; Ceccarelli, C.; Mauro, G.L.; Gervasoni, F.; Berti, L.; Robecchi Majnardi, A. Injectable Porcine Collagen in Musculoskeletal Disorders: A Delphi Consensus. JCM 2025, 14, 6058. [CrossRef]
- Randelli, F.; Fioruzzi, A.; Mazzoleni, M.G.; Radaelli, A.; Rahali, L.; Verga, L.; Menon, A. Efficacy of Ultrasound-Guided Injections of Type I Collagen-Based Medical Device for Greater Trochanteric Pain Syndrome: A Pilot Study. Life 2025, 15, 366. [CrossRef]
- Koszela, K.; Woldańska-Okońska, M.; Słupiński, M.; Gasik, R. The Role of Injection Collagen Therapy in Greater Trochanter Pain Syndrome. A New Therapeutic Approach? Reumatologia 2025. [CrossRef]
- Tarantino, D.; Mottola, R.; Palermi, S.; Sirico, F.; Corrado, B.; Gnasso, R. Intra-Articular Collagen Injections for Osteoarthritis: A Narrative Review. IJERPH 2023, 20, 4390. [CrossRef]
- Borja-Flores, A.; Macías-Hernández, S.I.; Hernández-Molina, G.; Perez-Ortiz, A.; Reyes-Martínez, E.; Belzazar-Castillo De La Torre, J.; Ávila-Jiménez, L.; Vázquez-Bello, M.C.; León-Mazón, M.A.; Furuzawa-Carballeda, J.; et al. Long-Term Effectiveness of Polymerized-Type I Collagen Intra-Articular Injections in Patients with Symptomatic Knee Osteoarthritis: Clinical and Radiographic Evaluation in a Cohort Study. Advances in Orthopedics 2020, 2020, 1–9. [CrossRef]
- Lee, H.S.; Oh, K.J.; Moon, Y.W.; In, Y.; Lee, H.J.; Kwon, S.Y. Intra-Articular Injection of Type I Atelocollagen to Alleviate Knee Pain: A Double-Blind, Randomized Controlled Trial. CARTILAGE 2021, 13, 342S-350S. [CrossRef]
- Aicale, R.; Savarese, E.; Mottola, R.; Corrado, B.; Sirico, F.; Pellegrino, R.; Donati, D.; Tedeschi, R.; Ruosi, L.; Tarantino, D. Collagen Injections for Rotator Cuff Diseases: A Systematic Review. Clinics and Practice 2025, 15, 28. [CrossRef]
- Corrado, B.; Bonini, I.; Chirico, V.A.; Filippini, E.; Liguori, L.; Magliulo, G.; Mazzuoccolo, G.; Rosano, N.; Gisonni, P. Ultrasound-Guided Collagen Injections in the Treatment of Supraspinatus Tendinopathy: A Case Series Pilot Study. J Biol Regul Homeost Agents 2020, 34, 33-39. ADVANCES IN MUSCULOSKELETAL DISEASES AND INFECTIONS-SOTIMI 2019.
- Corrado, B.; Bonini, I.; Alessio Chirico, V.; Rosano, N.; Gisonni, P. Use of Injectable Collagen in Partial-Thickness Tears of the Supraspinatus Tendon: A Case Report. Oxford Medical Case Reports 2020, 2020, omaa103. [CrossRef]
- Aicale, R.; Savarese, E.; Mottola, R.; Corrado, B.; Sirico, F.; Pellegrino, R.; Donati, D.; Tedeschi, R.; Ruosi, L.; Tarantino, D. Collagen Injections for Rotator Cuff Diseases: A Systematic Review. Clinics and Practice 2025, 15, 28. [CrossRef]
- Koszela, K.; Woldańska-Okońska, M.; Słupiński, M.; Gasik, R. The Role of Injection Collagen Therapy in Greater Trochanter Pain Syndrome. A New Therapeutic Approach? Reumatologia 2025. [CrossRef]
- Randelli, F.; Menon, A.; Giai Via, A.; Mazzoleni, M.; Sciancalepore, F.; Brioschi, M.; Gagliano, N. Effect of a Collagen-Based Compound on Morpho-Functional Properties of Cultured Human Tenocytes. Cells 2018, 7, 246. [CrossRef]
- Randelli, F.; Sartori, P.; Carlomagno, C.; Bedoni, M.; Menon, A.; Vezzoli, E.; Sommariva, M.; Gagliano, N. The Collagen-Based Medical Device MD-Tissue Acts as a Mechanical Scaffold Influencing Morpho-Functional Properties of Cultured Human Tenocytes. Cells 2020, 9, 2641. [CrossRef]
- Uhthoff, H.K. Calcifying Tendinitis, an Active Cell-Mediated Calcification. Virchows Arch. A Path. Anat. and Histol. 1975, 366, 51–58. [CrossRef]
- Tarantino, D.; Mottola, R.; Resta, G.; Gnasso, R.; Palermi, S.; Corrado, B.; Sirico, F.; Ruosi, C.; Aicale, R. Achilles Tendinopathy Pathogenesis and Management: A Narrative Review. IJERPH 2023, 20, 6681. [CrossRef]
- De Luca, P.; Grieco, G.; Bargeri, S.; Colombo, C.; Guida, S.; Taiana, M.M.; De Girolamo, L. The Interplay between Metabolic Disorders and Tendinopathies: Systematic Review and Meta-analysis. J. exp. orthop. 2025, 12, e70429. [CrossRef]
- Medina Pabón, M.A.; Naqvi, U. Achilles Tendinopathy. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025.
- Zellers, J.A.; Eekhoff, J.D.; Walk, R.E.; Hastings, M.K.; Tang, S.Y.; Lake, S.P. Human Achilles Tendon Mechanical Behavior Is More Strongly Related to Collagen Disorganization than Advanced Glycation End-Products Content. Sci Rep 2021, 11, 24147. [CrossRef]
- Kipp, J.A.; Blazek, C.D. Current Concepts in the Nonoperative Management of Achilles Tendon Pathologies: A Scoping Review. JCM 2025, 14, 4736. [CrossRef]
- Lee, W.; Jagasia, A. Comparison of Early Postoperative Outcomes and Reimbursement Metrics in Obese Versus Nonobese Patients Undergoing Secondary Reconstruction for Achilles Tendinopathy. J Am Acad Orthop Surg 2025. [CrossRef]
- Chen, P.; Tzeng, I.; Yang, K.; Wang, C. Endoscopic versus Open Surgery for Insertional Achilles Tendinopathy: A Systematic Review and Meta-analysis of Comparative Outcomes. J. exp. orthop. 2025, 12, e70374. [CrossRef]
- De Lucia, O.; Giarda, F.; Bernetti, A.; Ceccarelli, C.; Mauro, G.L.; Gervasoni, F.; Berti, L.; Robecchi Majnardi, A. Injectable Porcine Collagen in Musculoskeletal Disorders: A Delphi Consensus. JCM 2025, 14, 6058. [CrossRef]
- Corrado, B.; Mazzuoccolo, G.; Liguori, L.; Chirico, V.A.; Costanzo, M.; Bonini, I.; Bove, G.; Curci, L. Treatment of Lateral Epicondylitis with Collagen Injections: A Pilot Study. Muscle Ligaments and Tendons J 2019, 09, 584. [CrossRef]
- Corrado, B.; Bonini, I.; Chirico, V.A.; Filippini, E.; Liguori, L.; Magliulo, G.; Mazzuoccolo, G.; Rosano, N.; Gisonni, P. Ultrasound-Guided Collagen Injections in the Treatment of Supraspinatus Tendinopathy: A Case Series Pilot Study. J Biol Regul Homeost Agents 2020, 34, 33-39. ADVANCES IN MUSCULOSKELETAL DISEASES AND INFECTIONS-SOTIMI 2019.
- Corrado, B.; Bonini, I.; Alessio Chirico, V.; Rosano, N.; Gisonni, P. Use of Injectable Collagen in Partial-Thickness Tears of the Supraspinatus Tendon: A Case Report. Oxford Medical Case Reports 2020, 2020, omaa103. [CrossRef]
- Connizzo, B.K.; Bhatt, P.R.; Liechty, K.W.; Soslowsky, L.J. Diabetes Alters Mechanical Properties and Collagen Fiber Re-Alignment in Multiple Mouse Tendons. Ann Biomed Eng 2014, 42, 1880–1888. [CrossRef]
- Abate, M.; Paganelli, R.; Pellegrino, R.; Di Iorio, A.; Salini, V. Platelet Rich Plasma Therapy in Achilles and Patellar Tendinopathies: Outcomes in Subjects with Diabetes (A Retrospective Case-Control Study). JCM 2024, 13, 5443. [CrossRef]
- Stania, M.; Juras, G.; Chmielewska, D.; Polak, A.; Kucio, C.; Król, P. Extracorporeal Shock Wave Therapy for Achilles Tendinopathy. BioMed Research International 2019, 2019, 1–13. [CrossRef]
- Alušík, Š.; Paluch, Z. [Drug induced tendon injury]. Vnitr Lek 2018, 63, 967–971.
- Bolon, B. Mini-Review: Toxic Tendinopathy. Toxicol Pathol 2017, 45, 834–837. [CrossRef]
- Barboni, B.; Russo, V.; Gatta, V.; Bernabò, N.; Berardinelli, P.; Mauro, A.; Martelli, A.; Valbonetti, L.; Muttini, A.; Di Giacinto, O.; et al. Therapeutic Potential of hAECs for Early Achilles Tendon Defect Repair through Regeneration. J Tissue Eng Regen Med 2018, 12. [CrossRef]
- Huang, J.; Chen, Q. Bilateral Achilles Tendinopathy of Unknown Origin Responsive to Corticosteroids: Case Report. Medicine 2025, 104, e45436. [CrossRef]
- Ileri, S. Levofloxacin-Induced Gastrocnemius Tendon Rupture: A Case Report. J Med Case Reports 2025, 19, 228. [CrossRef]
- Godoy-Santos, A.L.; Bruschini, H.; Cury, J.; Srougi, M.; De Cesar-Netto, C.; Fonseca, L.F.; Maffulli, N. Fluoroquinolones and the Risk of Achilles Tendon Disorders: Update on a Neglected Complication. Urology 2018, 113, 20–25. [CrossRef]
- Caravaggio, F.; Depalmi, F.; Antonelli, M. Treatment of Achilles Tendon Partial Injuries with Injection of Peripheral Blood Mononuclear Cells (PB-MNCs): A Case Series. Eur J Transl Myol 2022. [CrossRef]
- Gervasi, M.; Barbieri, E.; Capparucci, I.; Annibalini, G.; Sisti, D.; Amatori, S.; Carrabs, V.; Valli, G.; Donati Zeppa, S.; Rocchi, M.B.L.; et al. Treatment of Achilles Tendinopathy in Recreational Runners with Peritendinous Hyaluronic Acid Injections: A Viscoelastometric, Functional, and Biochemical Pilot Study. JCM 2021, 10, 1397. [CrossRef]
- Pallikkara Kuttyadan, N.; Samad, S.; Shahzad, M.; Sanaullah, K.; Gillani, S.H.M.; Mushtaq, H.; Butt, S.B.; Hayat, S.K.; Raif, M.; Ali, S.M.; et al. Effectiveness of Platelet-Rich Plasma Injection for Chronic Achilles Tendinopathy: An Umbrella Systematic Review. Cureus 2025. [CrossRef]
- Thermann, H.; Fischer, R.; Gougoulias, N.; Cipollaro, L.; Maffulli, N. Endoscopic Debridement for Non-Insertional Achilles Tendinopathy with and without Platelet-Rich Plasma. Journal of Sport and Health Science 2023, 12, 275–280. [CrossRef]
Figure 1.
Demographic and Clinical data. No statistical different distributions were observed according the following sets: A) Gender; B) Age; C) HbC1; D) BMI; E) Type of tendinopathy: Insertional (I) and Non-Insertional (NI) F) Symptoms duration (months).
Figure 1.
Demographic and Clinical data. No statistical different distributions were observed according the following sets: A) Gender; B) Age; C) HbC1; D) BMI; E) Type of tendinopathy: Insertional (I) and Non-Insertional (NI) F) Symptoms duration (months).
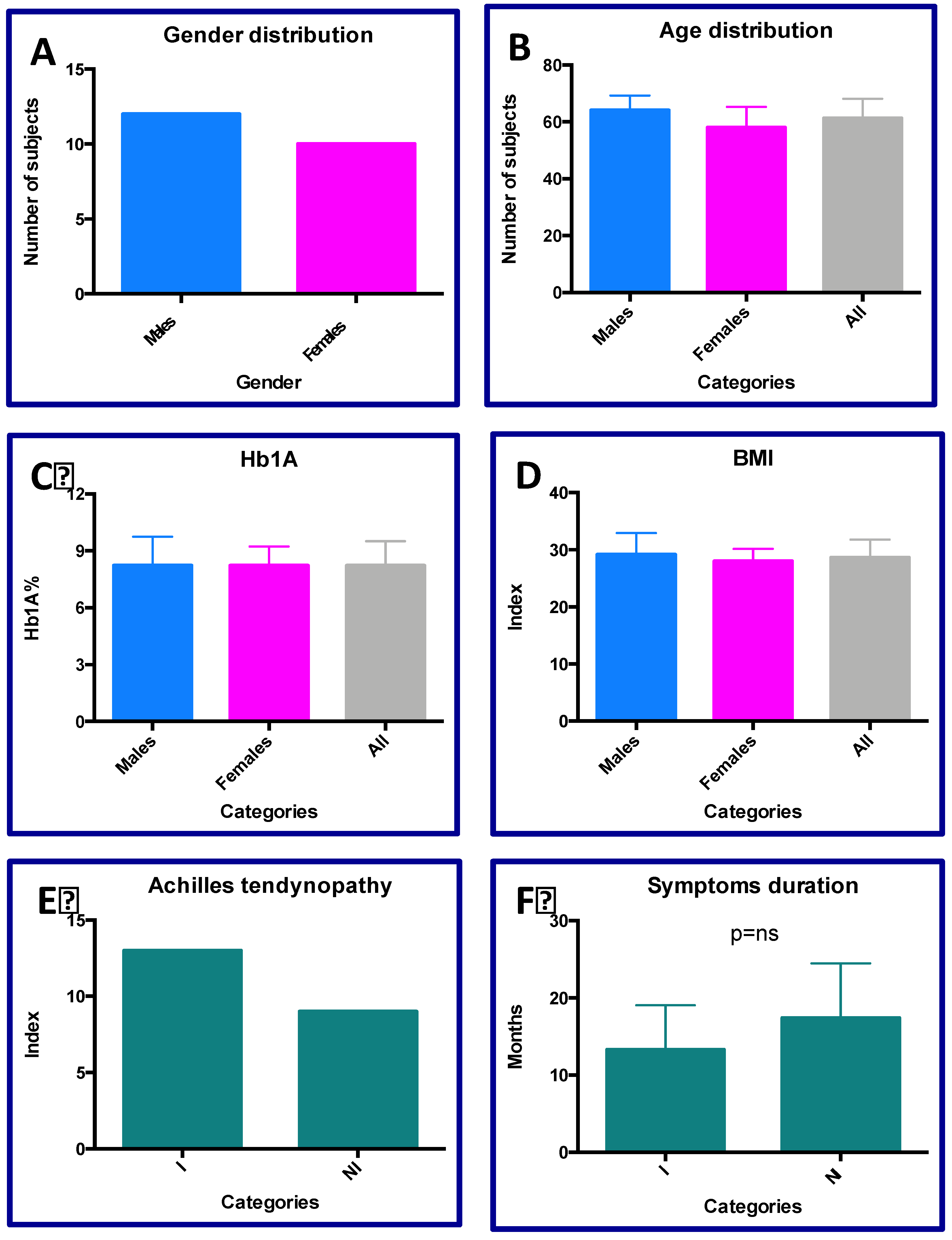
Figure 2.
VAS analyses. A) Mean VASvalues including all patients during the time; B) VAS linear regression according the type of AT: Insertional (I) and Non-Insertional (NI); C) ANOVA test concerning the VAS variation in AT-I and AT-NI groups; D) Log-rank test for the RTW time calculation; E) Delta VAS according the compliance of protocol; F) Delta VAS variation associated for ml of collagen injected.
Figure 2.
VAS analyses. A) Mean VASvalues including all patients during the time; B) VAS linear regression according the type of AT: Insertional (I) and Non-Insertional (NI); C) ANOVA test concerning the VAS variation in AT-I and AT-NI groups; D) Log-rank test for the RTW time calculation; E) Delta VAS according the compliance of protocol; F) Delta VAS variation associated for ml of collagen injected.
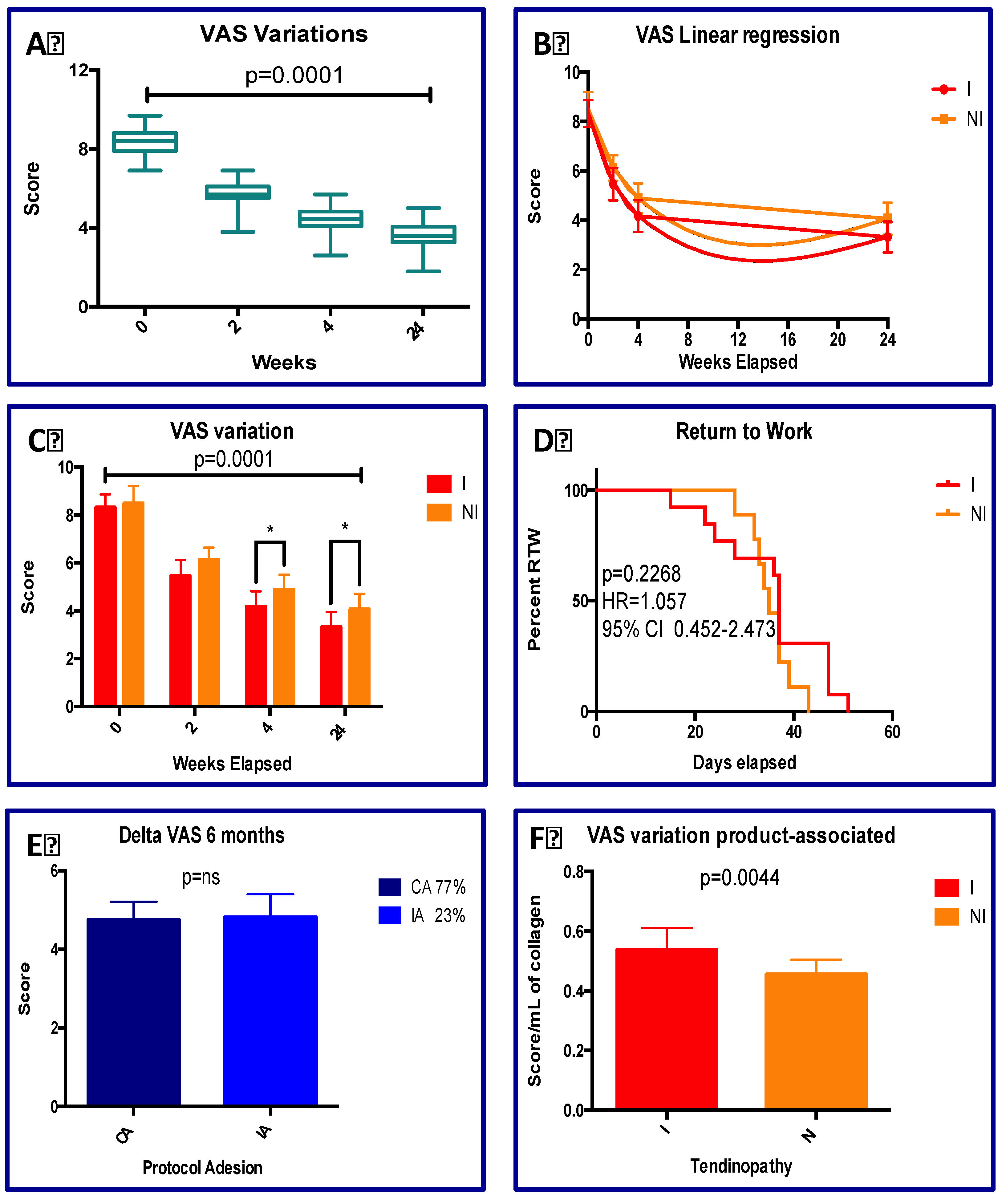
Figure 3.
VISA-A analyses. A) VISA_A mean scores in all AT patients in pre and post treatment; B) VISA-A variation in the AT-I and AT-NI; C) Delta VISA-A variation after six months; D) Delta VISA-A variation for ml of collagen administered.
Figure 3.
VISA-A analyses. A) VISA_A mean scores in all AT patients in pre and post treatment; B) VISA-A variation in the AT-I and AT-NI; C) Delta VISA-A variation after six months; D) Delta VISA-A variation for ml of collagen administered.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



