
Submitted:
29 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Background and Clinical Significance: This case reports a severe pediatric presentation of cutaneous–visceral loxoscelism (CVL) following a suspected Loxosceles spider bite, highlighting rare systemic complications and the need for early intensive management; Case Presentation: A previously healthy 6-year-old girl developed acute hemolysis, respiratory failure, acute kidney injury requiring renal replacement therapy, coagulopathy, and diffuse alveolar hemorrhage, necessitating management in the intensive care unit; Conclusions: Pediatric CVL can rapidly progress to life-threatening multisystem involvement; early recognition and timely multidisciplinary supportive care are essential to achieve favorable outcomes.
Keywords:
spider bites
; cutaneous–visceral loxoscelism
; acute kidney injury
; diffuse alveolar hemorrhage
; case report
1. Introduction and Clinical Significance
Loxoscelism is the envenomation resulting from the bite of a spider of the genus Loxosceles, commonly known as the violin or recluse spider [1]. These species are distributed across various regions worldwide; in North America, most cases are attributed to Loxosceles reclusa, while in South America, L. laeta, L. intermedia, and L. gaucho are predominant [2].
Clinically, loxoscelism most often presents in its cutaneous form (LC), characterized by a progressive dermonecrotic lesion that can range from an erythematous plaque to a deep ulcer [3]. However, in up to 20% of cases, systemic dissemination of sphingomyelinase D (SMD), a phospholipase responsible for tissue and microvascular injury, leads to the development of cutaneous-visceral or systemic loxoscelism (CVL), an uncommon but potentially life-threatening presentation [4,5].
CVL may present with fever, gastrointestinal symptoms, hemoglobinuria, massive intravascular hemolysis, and consequently jaundice, acute kidney injury (AKI), pulmonary involvement, and coagulation disorders, with a reported mortality exceeding 15%, typically occurring within 4 to 24 hours after the bite [4,5,6].
Pediatric age is a recognized risk factor for the development of severe forms, and delayed initiation of specific management has been identified as a key determinant of mortality [7]. In this context, early recognition of systemic manifestations and timely therapeutic intervention are crucial to improving clinical outcomes. The aim of this report is to describe the clinical course, systemic complications, and therapeutic management of a pediatric patient with CVL, providing relevant clinical insights that may enhance diagnostic suspicion and optimize management of this condition.
2. Case Presentation
A 6-year-old female patient from Carhuaz, an Andean valley north of Lima, Peru, with no relevant medical history, suffered a venomous animal bite on the proximal third of the right arm. At the time of the incident, she experienced mild “stinging” pain without visible skin lesions; the area was cleaned with alcohol. Approximately four hours later, she developed an unquantified fever, and oral paracetamol 120 mg/5 mL (5 mL) was administered without resolution of the fever. Nine hours after the incident, disseminated purpuric lesions appeared on the thorax, prompting transfer to the local hospital; during transport, she exhibited generalized muscle weakness and jaundice.
At the local hospital, 5 mL of anti-Loxosceles serum was administered intravenously, oxygen therapy was initiated via nasal cannula at 3 L/min, and a Foley catheter was placed for strict urine output monitoring and early detection of hemoglobinuria. Despite these interventions, no clinical improvement was observed, and she was referred to a higher-level care center.
Upon arrival at the emergency department of the referral center, the patient was conscious and oriented, with oxygen support and a functional Foley catheter. Vital signs were as follows: blood pressure 94/59 mmHg, heart rate 116 bpm, respiratory rate 40 breaths per minute, temperature 36.9 °C, and oxygen saturation 96% on 3 L/min via nasal cannula.
Physical examination revealed a necrotic lesion with indurated edema and extensive perilesional ecchymosis (Figure 1), pallor, conjunctival jaundice, respiratory distress with accessory muscle use, decreased bilateral breath sounds with left-sided predominance, and hematuria. Laboratory investigations were requested, including complete blood count, coagulation profile, haptoglobin, lactate dehydrogenase, urea, creatinine, liver function tests, serum electrolytes, and arterial blood gases (Table 1).
Results indicated acute hemolytic anemia, AKI, coagulopathy, and respiratory compromise, prompting transfer to the intensive care unit (ICU). In the ICU, the patient received assisted mechanical ventilation via endotracheal intubation, vancomycin 15 mg/kg intravenous, intermittent hemodialysis, and fluid and electrolyte management. Forty-eight hours after the incident, the cutaneous lesion developed blisters, necrosis, and eschar formation, leading to surgical debridement performed by the pediatric surgery team (Figure 2).
On the seventh day of hospitalization, the patient developed nosocomial pneumonia; antibiotic therapy was changed to piperacillin/tazobactam 80 mg/kg every 12 hours for 14 days. During a hemodialysis session, she experienced hemoptysis with a drop in hemoglobin to 6.5 g/dL and new bilateral alveolar infiltrates on chest radiography, consistent with diffuse alveolar hemorrhage (DAH) (Figure 3).
Renal function was monitored via serum urea and creatinine levels: on admission, values were 162 mg/dL and 3.18 mg/dL, respectively; on day 26, 117 mg/dL and 2.0 mg/dL; and on day 36, 31 mg/dL and 0.68 mg/dL. Urine output progressed from oliguria/anuria (<0.5 mL/kg/h) to normal ranges (>0.5–1 mL/kg/h), allowing discontinuation of hemodialysis and removal of the central venous catheter.
Following surgical debridement, the wound demonstrated viable granulation tissue. Porcine skin was applied to optimize the wound bed prior to autologous skin grafting, which was obtained from the scalp approximately one week after debridement. After two weeks of postoperative monitoring, the patient was discharged with scheduled outpatient follow-up. At one- and two-month follow-up visits, the wound exhibited a keloid scar with mildly erythematous borders and slight pruritus (Figure 4), with no evidence of pulmonary or renal sequelae or other long-term complications related to the clinical course.
3. Discussion
The violin or recluse spider (Loxosceles spp.) is distributed across various regions of the world. In North America, most cases are attributed to L. reclusa, whereas in South America, L. laeta, L. intermedia, and L. gaucho predominate [2]. This geographic distribution influences both the risk of envenomation and the most frequent clinical manifestations in each region [8,9]. It is important to note that the actual incidence of loxoscelism is uncertain due to the infrequent identification of the causative spider [8]. Nevertheless, CVL accounts for approximately 20% of envenomation cases caused by spiders of the genus Loxosceles and represents the most severe form of this condition [1,2,8].
The pathophysiology of CVL has been primarily linked to SMD present in the venom, a highly active type of enzyme responsible for both local and systemic damage [10]. These enzymes can induce microvascular and tissue injury, complement activation, and intravascular hemolysis, mechanisms that explain the characteristic triad of the visceral syndrome: hemolysis, AKI, and coagulopathy [5,6,8,10]. These findings were clearly evidenced in our patient, accounting for both the extent of cutaneous necrosis and the severity of systemic complications.
Regarding the progression of the cutaneous lesion, the literature describes that, following the initial bite, an erythematous macule or painful papule usually appears, which progresses within hours to the “red--white--blue” pattern, characterized by a pale center, an erythematous halo, and peripheral ecchymosis, and may evolve over several days into a livedoid plaque or necrotic ulcer [11,12]. In our case, the patient presented a necrotic lesion in the proximal third of the right arm, accompanied by extensive perilesional ecchymosis, findings that are consistent with the literature and reinforce the diagnosis (Figure 1). Furthermore, the proximal location of the bite and the patient’s pediatric age (6 years) are recognized risk factors for progression to severe systemic manifestations [2,7,13,14]. In this context, available evidence indicates that systemic loxoscelism can present with severe intravascular hemolysis, coagulopathies, thrombocytopenia, renal dysfunction, and even fatal outcomes [1,2,4,5,6,7,13,14,15]. However, the DAH observed in our patient represents an uncommon finding, highlighting clinical variability.
Regarding therapeutic management, CVL requires the timely administration of antivenom, ideally within the first 12 to 24 hours [16]. Previous studies have shown that the antivenom is effective in cutaneous forms when administered early, preventing or reducing progression to systemic manifestations [17,18,19]. Nevertheless, in our patient, no discernible clinical improvement was observed despite administration 15 hours post-bite, suggesting that therapeutic efficacy depends not only on the timing of administration but also on the specific characteristics of the venom and the identification of the species involved. This limitation reflects the ongoing controversy regarding the relative efficacy of Brazilian polyvalent antivenoms versus Peruvian species-specific preparations, a matter relevant for public health policy and hospital stock management [20].
Given the rapid progression and severity of complications, ventilatory support, hemodialysis, fluid and electrolyte correction, antibiotic therapy, surgical debridement, and subsequent skin grafting was implemented. These interventions resulted in a favorable outcome, with resolution of renal failure, normalization of urinary output, withdrawal of dialytic support, and adequate reconstruction of the affected tissue.
4. Conclusions
As previously stated, LC can rapidly progress to severe and potentially life-threatening systemic involvement in pediatric patients. Early recognition of systemic manifestations and the timely initiation of individualized and comprehensive management were critical in achieving a favorable outcome. The absence of a clear clinical response to antivenom, despite its administration within the recommended time frame, reflects the variability in its efficacy and the persistent uncertainty reported in the literature regarding its impact on systemic forms. In this context, comprehensive supportive care remains the cornerstone of treatment. This report emphasizes the importance of maintaining a high index of clinical suspicion, optimizing early intervention, and strengthening the available evidence to improve the management and prognosis of severe loxoscelism in the pediatric population.
Author Contributions
Conceptualization, M.R. and C.Y.; methodology, M.R; validation, M.R., C.Y. and V.A.; investigation, M.R., C.Y. and IR.; resources, M.R., C.Y., V.A., I.R., K.D. and J.B.; writing—original draft preparation, M.R., C.Y., V.A., I.R., K.D. and J.B; writing—review and editing, C.Y., M.R. and V.A.; visualization, C.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study because it is a retrospective case report describing routine clinical care. Written informed consent was obtained from the patient’s legal guardians for publication.
Informed Consent Statement
Written informed consent has been obtained from the patient’s legal guardians for publication of this case report and any accompanying images.
Data Availability Statement
All relevant data are included in this article. For any further inquiries, please contact the corresponding author.
Acknowledgments
During the preparation of this manuscript, the authors utilized ChatGPT (OpenAI, GPT-5 mini model, 2025 version) to assist with English translation and stylistic and linguistic refinement of selected paragraphs. All content was thoroughly reviewed and edited by the authors, who assume full responsibility for the scientific accuracy and integrity of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| LC | Cutaneous loxoscelism |
| SMD | Sphingomyelinase D |
| CVL | Cutaneous-visceral loxoscelism |
| AKI | Acute Kidney Injury |
| Hb | Hemoglobin |
| Hct | Hematocrit |
| WBC | White Blood Cells |
| Plt | Platelets |
| PT | Prothrombin Time |
| INR | International Normalized Ratio |
| TT | Thrombin Time |
| LDH | Lactate Dehydrogenase |
| AST(TGO) | Aspartate Aminotransferase |
| ALT (TGP) | Alanine Aminotransferase |
| Na | Sodium |
| K | Potassium |
| Cl | Chloride |
| pCO₂ | Partial pressure of carbon dioxide |
| HCO3 | Bicarbonate |
| ICU | Intensive Care Unit |
| DAH | Diffuse Alveolar Hemorrhage |
References
- Sánchez-Olivas, MA; Valencia-Zavala, MP; Sánchez-Olivas, JA; Sepulveda-Velázquez, G; Vega-Robledo, G. Loxoscelismo cutáneo necrótico. Informe de un caso. Rev Alerg México 2011, 58(3), 171–176. [Google Scholar]
- Droppelmann, K.; Majluf-Cáceres, P.; Sabatini-Ugarte, N.; Valle, E.; Herrera, H.; Acuña, D. Caracterización clínica y epidemiológica de 200 pacientes con loxoscelismo cutáneo y cutáneo visceral. Rev. Medica De Chile 2021, 149, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Lopes, P.H.; Squaiella-Baptistão, C.C.; Marques, M.O.T.; Tambourgi, D.V. Clinical aspects, diagnosis and management of Loxosceles spider envenomation: literature and case review. Arch. Toxicol. 2020, 94, 1461–1477. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, P.L.M.M.; Tessarolo, L.D.; Menezes, F.H.; de Lima, T.B.; Paiva, J.H.H.G.L.; Júnior, G.B.d.S.; Martins, A.M.C.; Daher, E.d.F. Acute kidney injury due to systemic Loxoscelism: a cross-sectional study in Northeast Brazil. Rev. da Soc. Bras. de Med. Trop. 2018, 51, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Severino, F.B.; Vivanco, P.; Mix, A. Loxoscelismo: revisión de la literatura a propósito de un caso. 2022, 47, 29–35. [Google Scholar] [CrossRef]
- Rodríguez, C.A.; Martínez, N.M.H. Complicaciones de la picadura de araña Loxosceles fugescens. Med. Gen. y de Fam. 2024, 13, 175–178. [Google Scholar] [CrossRef]
- R.J., S.; H.H., I.; A.V., P. Loxoscelismo cutáneo-visceral por mordedura de araña Loxosceles laeta en niños: factores asociados. Rev. De Investig. Veter- Del Peru 2023, 34, e24949–e24949. [Google Scholar] [CrossRef]
- Isbister, G.K.; Fan, H.W. Spider bite. Lancet 2011, 378, 2039–2047. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, V.S.; Gomes, A.A.; Silva, I.M.; Sachett, J.; Ferreira, L.C.L.; Oliveira, S.; Sabidò, M.; Chalkidis, H.; Guerra, M.G.V.B.; Salinas, J.L.; et al. Low Health System Performance, Indigenous Status and Antivenom Underdosage Correlate with Spider Envenoming Severity in the Remote Brazilian Amazon. PLOS ONE 2016, 11, e0156386–e0156386. [Google Scholar] [CrossRef] [PubMed]
- Gremski, L.H.; da Justa, H.C.; Polli, N.L.C.; Schluga, P.H.d.C.; Theodoro, J.L.; Wille, A.C.M.; Senff-Ribeiro, A.; Veiga, S.S. Systemic Loxoscelism, Less Frequent but More Deadly: The Involvement of Phospholipases D in the Pathophysiology of Envenomation. Toxins 2022, 15, 17. [Google Scholar] [CrossRef] [PubMed]
- Suárez-Ospino, N.I.; Díaz-Anaya, E.; Ochoa-Díaz, A.F. Dermatological Features as a Diagnostic Clue in Systemic Loxocelism Caused by Brown Recluse Spider Bite. Am. J. Trop. Med. Hyg. 2023, 109, 1207–1208. [Google Scholar] [CrossRef] [PubMed]
- Mani, S.; Katzman, C.; Liu, V. Histopathology aiding diagnosis of viscerocutaneous loxoscelism in a nonendemic region. JAAD Case Rep. 2024, 45, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.; Pandey, M. Loxoscelism: Cutaneous and Hematologic Manifestations. Adv. Hematol. 2019, 2019, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Harry, S.; Brugioni, E.; Madhusudhana, S. Acute Hemolytic Anemia Caused by Loxoscelism Treated With Plasmapheresis: A Case Report. J. Med Cases 2022, 13, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Mondal, S.; Nag, A.; Datta, J.; Das, A.; Agarwal, A.; Sinha, D.; Ete, T.; Chakraborty, A.; Ghosh, S. Acute kidney injury and dermonecrosis after Loxosceles reclusa envenomation. Indian J. Nephrol. 2014, 24, 246–8. [Google Scholar] [CrossRef] [PubMed]
- Vargas, C.M.; Vásquez, V.F.; Ugarte, R.P. Actualización sobre manejo de araneismo en Perú. Rev. Medica Hered. 2017, 28, 200. [Google Scholar] [CrossRef]
- Pauli, I.; Puka, J.; Gubert, I.C.; Minozzo, J.C. The efficacy of antivenom in loxoscelism treatment. Toxicon 2006, 48, 123–137. [Google Scholar] [CrossRef] [PubMed]
- Malaque, C.M.S.; Novaes, C.T.G.; Piorelli, R.O.; Risk, J.Y.; Murad, J.C.; Lara, A.N.; Virgulino, C.C.; Miyaji, K.T.; Santoro, M.L. Impact of antivenom administration on the evolution of cutaneous lesions in loxoscelism: A prospective observational study. PLOS Neglected Trop. Dis. 2022, 16, e0010842. [Google Scholar] [CrossRef]
- Azuara-Antonio, O.; Ortiz, M.I.; Jimenez-Oliver, K.D.; Hernandez-Cruz, L.E.; Rivero-Veras, G.; Hernandez-Ramirez, L. Clinical Evolution After Administering Antivenom in Patients With Loxoscelism. J. Med Cases 2023, 14, 378–386. [Google Scholar] [CrossRef] [PubMed]
- Salud (ETESA) CM de SD de P y PD de C de PU de E de T de. Efectividad del suero anti-loxosceles: síntesis de evidencia. Published online 2004:20-20.
Figure 1.
Approximately 24 hours after the incident, a necrotic lesion was observed on the proximal third of the lateral aspect of the right arm, showing extensive perilesional ecchymosis at the time of admission.
Figure 1.
Approximately 24 hours after the incident, a necrotic lesion was observed on the proximal third of the lateral aspect of the right arm, showing extensive perilesional ecchymosis at the time of admission.

Figure 2.
Dermonecrotic lesion after surgical debridement.

Figure 3.
(a) Chest X-ray obtained at the time of admission; (b) Chest X-ray showing diffuse bilateral alveolar infiltrates.
Figure 3.
(a) Chest X-ray obtained at the time of admission; (b) Chest X-ray showing diffuse bilateral alveolar infiltrates.
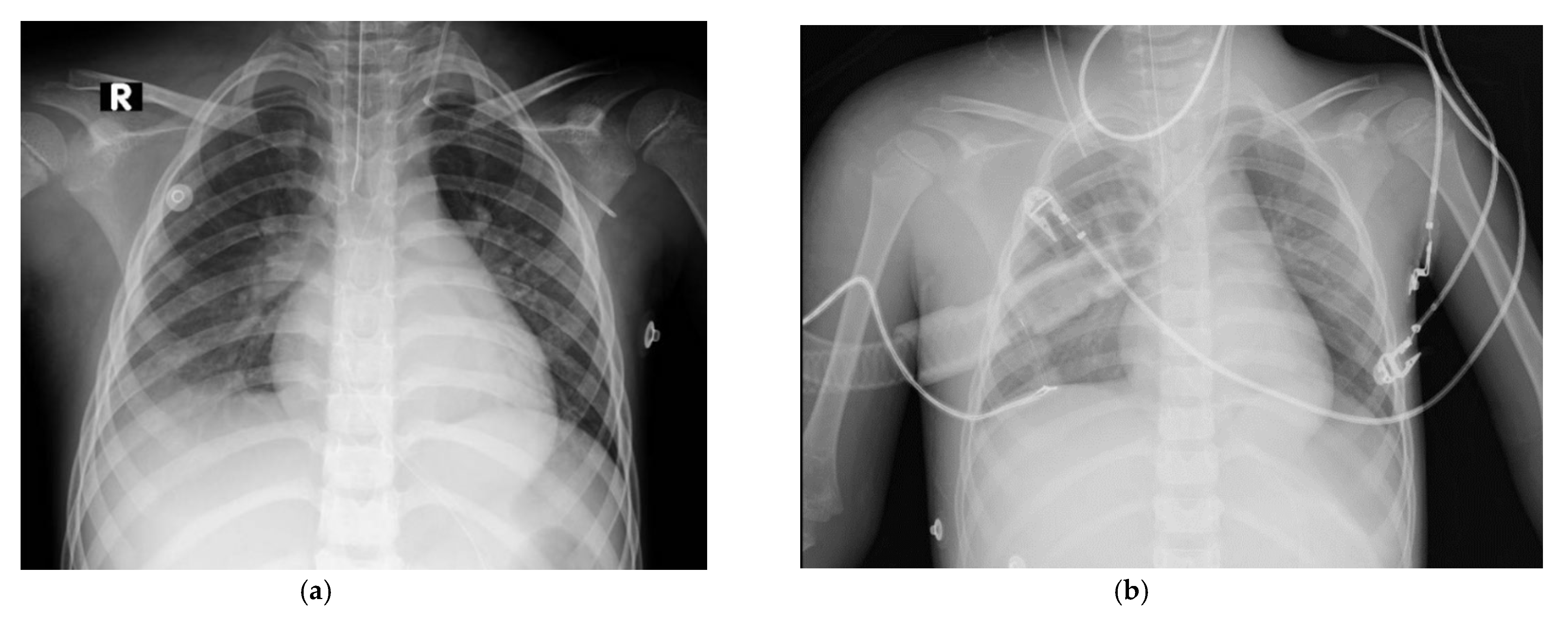
Figure 4.
Postoperative wound at two months, located on the right shoulder and arm, showing a keloid scar with erythematous borders.
Figure 4.
Postoperative wound at two months, located on the right shoulder and arm, showing a keloid scar with erythematous borders.


Table 1.
Laboratory tests conducted at admission.
| Laboratory Test | Result |
| Hematology | |
| Hb | 8.0 g/dL |
| Hct | 19.8% |
| WBC | 27,970 /mm³ |
| Segmented neutrophils | 84% |
| Lymphocytes | 14% |
| Plt | 200,000 /mm³ |
| Direct/indirect Coombs test | Negative |
| Coagulation Profile | |
| PT | 18.6 sec |
| INR | 1.55 |
| TT | 18.3 sec |
| D-dimer | 34,651 mg/L |
| Haptoglobin | 24 mg/dL |
| LDH | 185,600 U/L |
| Renal Function | |
| Creatinine | 3.18 mg/dL |
| Urea | 162 mg/dL |
| Liver Function Tests | |
| Albumin | 1.9 g/dL |
| Globulin | 7.5 g/dL |
| AST (TGO) | 73 U/L |
| ALT (TGP) | 32 U/L |
| Total bilirubin | 8.42 mg/dL |
| Indirect bilirubin | 7.94 mg/dL |
| Direct bilirubin | 0.48 mg/dL |
| Electrolytes | |
| Na | 137 mmol/L |
| K | 6.2 mmol/L |
| Cl | 107 mmol/L |
| Arterial Blood Gases | |
| pH | 7.31 |
| pCO2 | 18.1 mmHg |
| HCO3 | 9.2 mmol/L |
| Lactate | 3.7 mmol/L |
1 Severe anemia (Hb < 10 g/dL), leukocytosis, markedly elevated D-dimer and LDH, acute kidney injury (elevated creatinine and urea), hypoalbuminemia, hyperbilirubinemia (predominantly indirect), hyperkalemia, metabolic acidosis (low HCO₃⁻ and pH), and elevated lactate were observed. Hb: Hemoglobin; Hct: Hematocrit; WBC: White Blood Cells; Plt: Platelets; PT: Prothrombin Time; INR: International Normalized Ratio; TT: Thrombin Time; LDH: Lactate Dehydrogenase; AST (TGO): Aspartate Aminotransferase; ALT (TGP): Alanine Aminotransferase; Na: Sodium; K: Potassium; Cl: Chloride; pCO₂: Partial Pressure of Carbon Dioxide; HCO3: Bicarbonate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



