
Submitted:
30 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
Background: Arterial hypertension and increased blood pressure variability (BPV) are major prognostic determinants in patients with ischemic heart disease (IHD). While exercise training is known to improve blood pressure (BP) control, the effects of different combined exercise modalities on BPV in IHD remain poorly defined. This randomized pilot study compared the effects of continuous combined training (CCT; moderate-intensity continuous aerobic exercise plus resistance training) and interval combined training (ICT; high-intensity interval aerobic exercise plus resistance training) on BPV and BP parameters in hypertensive patients with IHD. Methods: Thirty-six clinically stable patients with IHD and hypertension were randomized to CCT or ICT for 12 weeks. Outcomes included short-term BPV assessed by 24-hour ambulatory BP monitoring, resting and 24-hour BP, and exercise capacity. Results: Short-term systolic BPV significantly decreased in the CCT group but remained unchanged in the ICT group: [adjusted between-group difference −2.1 mmHg (95% CI: −4.1 to −0.1; p 0.029]. Resting systolic BP decreased similarly in both groups, whereas no significant changes were observed in 24-hour BP values. Peak oxygen uptake improved in both groups with a greater increase in the ICT group [adjusted between-groups difference +1.7 mL·kg⁻¹·min⁻¹ (95% CI: 0.7 to 2.8); p = 0.032). Conclusion: These findings suggest that, in patients with IHD, continuous combined training may be more effective than interval combined training in reducing short-term BPV, whereas interval training may confer greater improvements in aerobic capacity. Further adequately powered studies are warranted to confirm these results.
Keywords:
combined interval training
; hypertension
; blood pressure variability
; ischemic heart disease
1. Introduction
Arterial hypertension remains one of the leading modifiable determinants of cardiovascular morbidity and mortality, affecting over 1.3 billion adults worldwide and accounting for a substantial burden of ischemic and heart failure events [1,2]. In individuals with ischemic heart disease (IHD), hypertension is particularly frequent, representing both a precipitating factor and a prognostic amplifier of adverse outcomes [3,4,5]. Therefore, optimization of BP levels represents a cornerstone of secondary prevention in patients with established IHD [6]. Beyond mean BP levels, blood pressure variability (BPV), the oscillation of BP over time, has emerged as an independent predictor of cardiovascular events [7,8]. In particular, an elevated short-term BPV, assessed by 24/hour ambulatory BP monitoring, resulted as the most powerful predictor of cardiovascular events when compared to long-term ambulatory BPV [9] and average 24/h BP [10]. However, despite the growing evidence supporting the prognostic role of BPV, there is currently limited evidence regarding effective interventions capable of reducing BPV [11,12]. Exercise training is a well-established nonpharmacological intervention for preventing and treating both hypertension and IHD [13,14,15,16]. Aerobic moderate intensity continuous training (MICT) is considered the gold standard for treating IHD patients in the context of cardiac rehabilitation programs since it has been associated with reduced cardiovascular mortality, cardiac events, and hospitalizations [17]. In recent years, combined training protocols, which integrate aerobic and dynamic resistance components, have been proposed to maximize cardiovascular and musculoskeletal adaptations [18,19]. Combined training has also demonstrated to reduce short-term BPV in patients with IHD more efficiently than other exercise modalities, including MICT alone [20,21]. High-intensity interval training (HIIT), characterized by alternating bouts of high- and low-intensity exercise, may elicit physiological adaptations that are superior to those achieved with MICT in patients with IHD [22,23]. However, the available clinical evidence remains limited, largely due to the small sample sizes and short follow-up durations of the studies conducted to date. HIIT has demonstrated small reductions in systolic BP, with minimal impact on diastolic BP in comparison to MICT [24]; however, direct comparisons in patients with IHD are lacking. Moreover, to the best of the authors’ knowledge, no studies have specifically investigated the effects of HIIT on BPV in these patients. Nevertheless, evidence directly comparing continuous combined training versus interval combined training in hypertensive patients with IHD are lacking. The present study investigated whether replacing the MICT component of the combined training sessions with HIIT would produce comparable effects on BP and BPV in IHD patients. To this purpose, we conducted a prospective randomized pilot study whose primary objective was to estimate the effects of the two exercise interventions on short-term BPV. Other outcome parameters were: changes in short-term BPV, resting BP, 24/h mean BP, and peak oxygen uptake (VO2 peak).
2. Materials and Methods
2.1. Population
The study enrolled 36 patients, average age = 65±7,55, males/famales= 33/3. These subjects were evaluated at San Raffaele IRCCS of Rome before starting a cardiac rehabilitation program to which they were referred by their cardiologist or primary care physician. The recruitment period started in January 2024 and was concluded in March 2025. Inclusion criteria of the study were: age ≥ 45 years old; previous diagnosis of IHD; established diagnosis of hypertension; clinical stability (no cardiovascular events in the previous six months); left ventricular ejection fraction (LVEF) (assessed by echocardiography) above 40%; the ratio between E-wave velocity and the average of septal and lateral e’-wave velocities below 14 (also assessed by echocardiography). Diagnosis of IHD relied on the following information obtained from the clinical history: previous myocardial infarction; previous percutaneous coronary intervention or coronary artery bypass grafting. All patients had to be under optimal pharmacological therapy, with resting BP values under acceptable control (systolic BP < 150 mmHg; diastolic BP < 90mmHg) and no changes in medications in the previous three months. All classes of antihypertensive drugs were admitted, and there were no restrictions on the number of antihypertensive drugs taken by the patients. Antihypertensive drugs included beta-blockers, diuretics, angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, alpha-adrenergic blockers, and calcium antagonists, as reported by medical charts. The following exclusion criteria were adopted: secondary hypertension; significant heart valve diseases; hypertrophic obstructive cardiomyopathy; signs and/or symptoms of myocardial ischemia at rest and/or during the ergometric test, uncontrolled arrhythmia, neurological and or orthopedic conditions contraindicating or limiting exercise training; diagnosis of chronic obstructive pulmonary disease with GOLD stage III–IV; chronic anemia with blood hemoglobin levels below 10.5 g/dL; previous diagnosis of chronic heart failure; presence of signs and/or symptoms of heart failure during the evaluation; symptomatic peripheral arterial disease. Patients who needed further and more sustained pharmacological interventions for lowering BP were excluded from the study.
2.2. Study Design
The study design, which is summarized in Figure 1, complied with CONSORT guidelines [25]. The present research was conceived as a randomized pilot study that included two intervention arms: a continuous combined training (CCT) and an interval combined training (ICT). The protocol lasted 12 weeks for each group. Patients in both groups exercised three times a week, with each session lasting 90 minutes. Patient recruitment occurred after a screening visit during which eligibility was assessed according to the predefined inclusion and exclusion criteria. Eligible patients were then asked to participate in the study, and those who agreed signed an informed consent. The screening visit included medical and pharmacological history, collection of anthropometric measurements (weight and height), measurement of BP at rest, electrocardiography (ECG), and cardiopulmonary exercise testing (CPET). If the patient had not undergone a recent echocardiogram (within the previous 3 months), this examination was performed to assess LVEF. A second visit was scheduled within one week of screening. During this visit, participants performed a six-minute walk test (6MWT) and were familiarized with the device used during the training sessions. Within two days of the second visit, they underwent 24-hour ABPM. Once the training programs were completed, the patients performed a third visit and repeated the 24-hour ABPM, 6MWT, and CPET within the first week. This was an open-label trial. Patients were randomly assigned on a 1:1 basis to either the CCT or ICT group within a week from the screening visit. Randomization was performed using a computer-generated allocation sequence with allocation concealment ensured by sealed, opaque, sequentially numbered envelopes prepared by an investigator not involved in participant recruitment or assessment. All patients provided written informed consent to participate in the study, which was approved by the local Ethics Committee (N registration: SR 7/2024). The study has been registered on ClinicalTrials.gov (ID: NCT04282499).
Figure 1. Flowchart of the study, CCT, continuous combined training; ICT, interval combined training
2.3. Outcomes Measure
2.3.1. Resting Blood Pressure
Resting systolic and diastolic BP were measured using an automated oscillometric device (Omron HEM-7130™; Omron Healthcare Inc., Lake Forest, IL, USA). Measurements were obtained after at least 5 minutes of seated rest, with participants instructed to abstain from caffeine, exercise, and smoking for ≥60 minutes beforehand. The cuff was placed on the upper arm at heart level, and measurements were performed in a quiet environment without conversation. All assessments were conducted between 9:00 and 10:30 a.m.
2.3.2. Exercise Capacity
Maximal and submaximal exercise capacity were assessed through CPET and 6MWT, respectively. These examinations were performed at enrollment and at the end of the study. During CPET, patients were positioned on an electrically braked bicycle ergometer with monitoring of gas exchange (Quark CPET, COSMED, Frascati, Italy). Exercise started with 2 min of unloading pedaling, then there was a progressive increase of the load, at a rate of 10 W every minute until exhaustion, which was defined as the inability to keep the pedaling rate steady at 60 rpm. Peak VO2 was defined as the highest VO2 observed during the exercise, averaged for a 30-s recording during the last minute of the effort. Respiratory exchange ratio was calculated at the same time-point. A value >1.10 was considered representative of a maximal effort. The ventilation/carbon dioxide output (VE/VCO2) slope, which relates the rate of increase in ventilation/unit increase in carbon dioxide, was calculated for the whole exercise period. A 12-lead electrocardiogram was recorded continuously during the test, and BP was measured every 2 min by a sphygmomanometer. The 6MWT was performed in a 100 m long corridor, according to standardized procedures [26] and was supervised by a physical therapist.
2.3.3. 24–h Ambulatory Blood Pressure Monitoring
Twenty-four–hour ambulatory blood pressure monitoring (ABPM) was conducted using a validated oscillometric device (Cardioline Walk200B, Trento, Italy), with the cuff positioned on the non-dominant arm. Blood pressure was recorded every 15 minutes from 06:00 to 22:00 and every 20–30 minutes from 22:00 to 06:00. For analysis, only readings obtained between 08:00 and 20:00 (daytime) and between 00:00 and 06:00 (nighttime) were included to exclude transition periods. Participants were instructed to maintain usual daily activities and medication regimens during monitoring. All recordings were performed on working days and initiated between 09:00 and 10:30. ABPM data were considered valid if at least 75% of measurements were successfully obtained. The following parameters were analyzed: 24-hour, daytime, and nighttime systolic and diastolic BP, along with their corresponding time-related variability. BP variability was assessed using average real variability (ARV), calculated as previously described by Mena et al [27].: ARV = 1/(N−1) ∑|BPₖ₊₁−BPₖ|, where N represents the number of valid BP measurements.
2.3.4. Exercise Sessions
Each exercise session lasted 80 minutes and consisted of an aerobic phase (45 minutes) followed by a resistance training phase (35 minutes). All sessions were conducted in the morning, between 8:30 a.m. and 12:00 p.m. Aerobic exercise was performed on a stationary cycle ergometer (Technogym Wellness System, Technogym, Cesena, Italy). Participants assigned to the CCT group cycled at a constant heart rate (HR) corresponding to 60–70% of VO₂ peak as determined during CPET. HR was continuously monitored via the cycle ergometer display, which provided real-time feedback, including average and maximal HR. Participants in the ICT group performed aerobic exercise on the stationary cycle ergometer using an interval protocol consisting of alternating bouts of 5 minutes at 80–90% of VO₂ peak and 10 minutes at 50–60% of VO₂ peak. This sequence was repeated three times, resulting in a total aerobic exercise duration of 45 minutes. The resistance training component included the following exercises: leg press, leg extension, shoulder press, chest press, low row, and vertical traction (Technogym Wellness System, Technogym, Cesena, Italy). For each muscle group, a preliminary one-repetition maximum (1-RM) assessment was performed. The 1-RM was defined as the highest force achieved during three prior 5-second maximal voluntary contraction trials. Attention was paid to ensure that contractions were limited to the target muscle groups, minimizing the recruitment of accessory muscles. For each exercise, patients performed three sets, with each set consisting of 10 repetitions. A two-minute rest period was allowed between sets. The intensity of every exercise was set at 60% of 1-RM.
2.3.5. Statistical Analysis
This study was designed as a pilot investigation; therefore, no formal a priori sample size calculation was performed; the sample size was determined based on feasibility and participant availability [28]. Continuous variables are presented as mean ± standard deviation (SD). Data normality was assessed using the Shapiro–Wilk test. Primary and secondary outcomes were analyzed using linear mixed-effects models to account for the repeated-measures design. In each model, time (baseline and 12 weeks), group (continuous combined training vs. interval combined training), and their interaction (group × time) were included as fixed effects, with participant included as a random intercept. The group × time interaction represented the primary test of between-group differences in intervention effects. Baseline values of the dependent variable were inherently accounted for within the model structure. When appropriate, models were additionally adjusted for clinically relevant covariates, including age and number of antihypertensive medications. All statistical analyses were conducted using IBM SPSS Statistics (version 26.0).
3. Results
From an initial number of 79 patients screened, fifteen did not accept the proposal to participate in the study; thirteen were excluded for having uncontrolled BP values at rest requiring changes in their anti-hypertensive therapy; nine patients had a history of heart failure, and six were excluded for presenting signs of ischemia during the exercise test. All participants completed the exercise protocol, and their data were included in the analysis. Baseline characteristics are reported in Table 1.
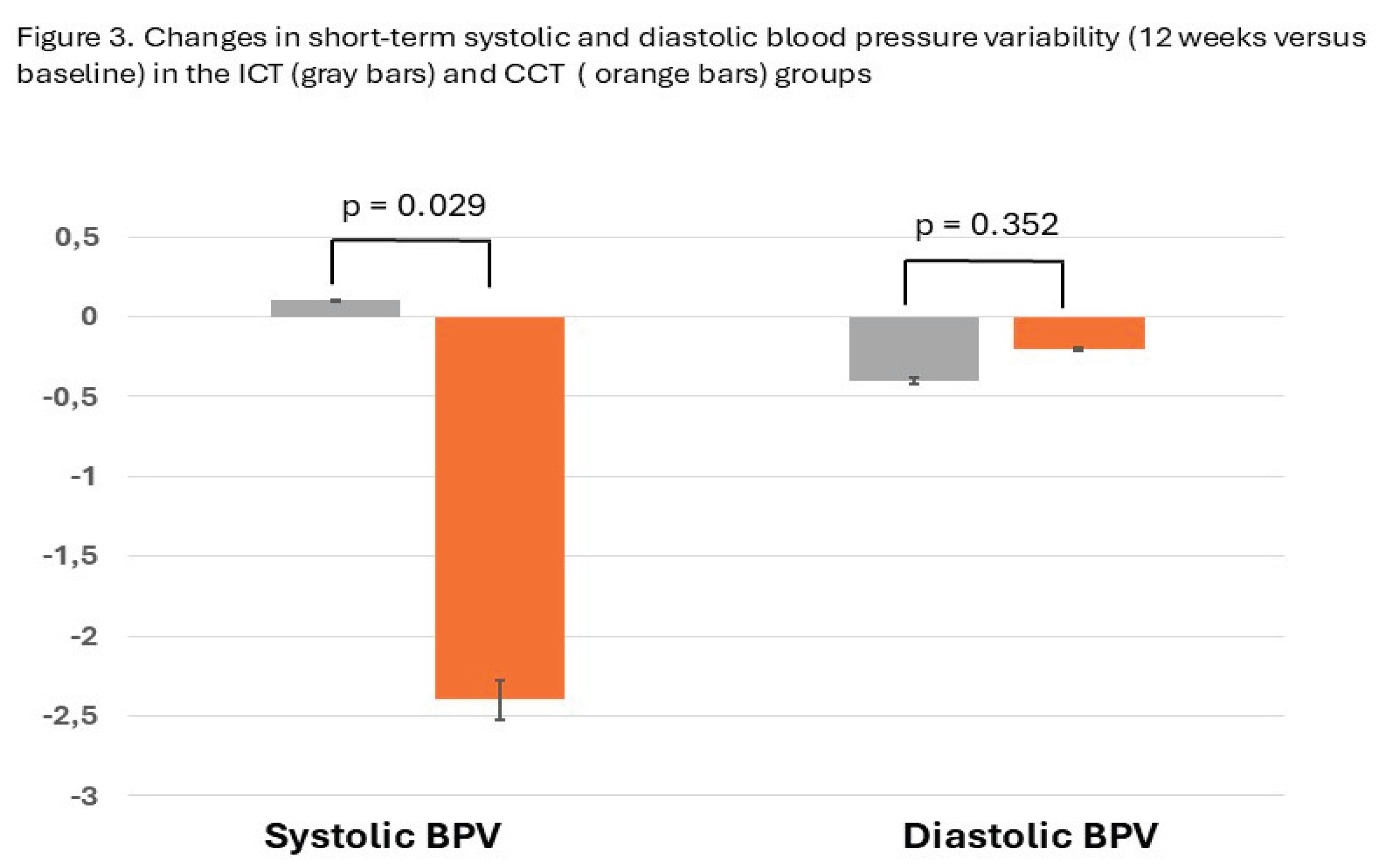
All patients had a BMI over 25, and seventeen out of 36 (47%) were obese. All patients were taking more than one medication to lower their BP, with an average number of 2.8± 1.4. The percentage of participants who took two, three, or four medications with anti-hypertensive effect was 47.2%, 30.5%, and 22.2%, respectively. All patients randomized completed the study, and their data were analysed. Both exercise protocols were well tolerated, and no clinical events occurred during the entire study. Patients of the CCT group attended 30 out of 36 planned exercise sessions (83.3%) while those of the ICT group attended 31 out of 36 (86.1). A significant group × time interaction was observed for peak oxygen uptake (VO₂ peak), indicating a greater improvement in aerobic capacity in the ICT group compared with the CCT group (adjusted between-group difference: +1.7 mL·kg⁻¹·min⁻¹; 95% CI: 0.7 to 2.8; p = 0.032) (figure 2). In contrast, no significant group × time interactions were detected for the VE/VCO₂ slope or for the six-minute walk test distance, indicating comparable training-related adaptations between groups for these outcomes. A significant group × time interaction was observed for short-term systolic BPV assessed by ARV (p = 0.029) (Figure 3). After 12 weeks of training, participants in the CCT group exhibited a greater reduction in systolic BPV compared with those in the ICT group, with an adjusted between-group difference of −2.1 mmHg (95% CI: −4.1 to −0.1). No significant group × time interactions were observed for diastolic BPV or for BP variability assessed using standard deviation metrics. No significant group × time interactions were observed for 24-hour, daytime, or nighttime systolic or diastolic BP values following the 12-week intervention period. Resting systolic BP decreased over time in both groups; however, the magnitude of change did not differ significantly between groups (Table 2).
Figure 2.
Changes in cardiopulmonary parameters (12 weeks versus baseline) in the ICT (grey bars) and CCT (orange bars) groups.
Figure 2.
Changes in cardiopulmonary parameters (12 weeks versus baseline) in the ICT (grey bars) and CCT (orange bars) groups.
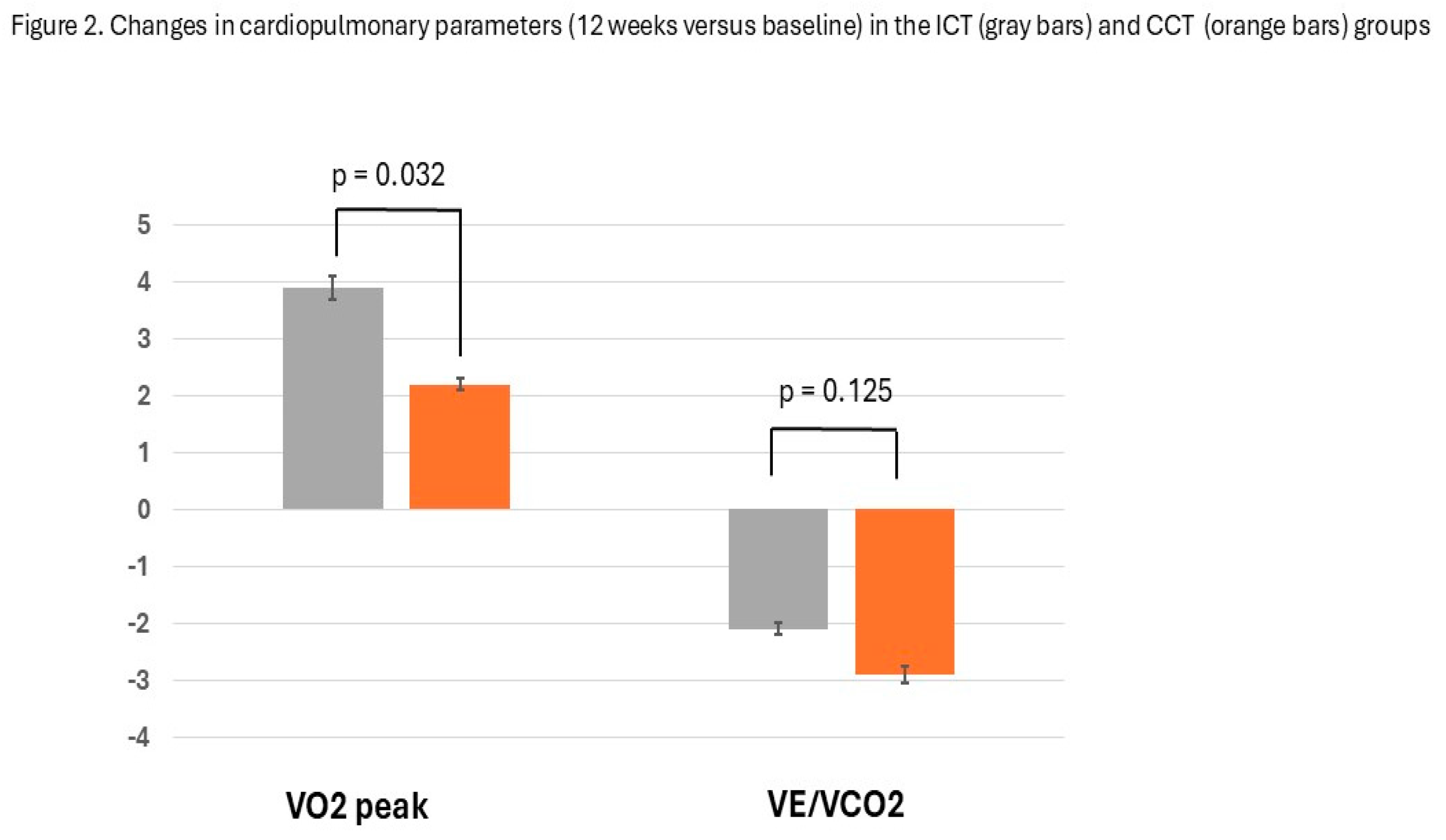
Figure 3.
Changes in short-term systolic and diastolic blood pressure variability (12 weeks versus baseline) in the ICT (grey bars) and CCT (orange bars) groups.
Figure 3.
Changes in short-term systolic and diastolic blood pressure variability (12 weeks versus baseline) in the ICT (grey bars) and CCT (orange bars) groups.
4. Discussion
Exercise training is widely adopted as a non-pharmacological intervention for blood pressure (BP) reduction in individuals with hypertension. In recent years, a growing body of evidence has also demonstrated that exercise training can effectively reduce blood pressure variability (BPV), particularly short-term systolic BPV [29,30]. However, uncertainty remains regarding the most effective exercise modality and training protocol for optimizing BPV reduction. In the present study, a combined exercise training program including moderate-intensity continuous training (MICT) plus dynamic resistance exercise was more effective than high-intensity interval training (HIIT) combined with dynamic resistance exercise in reducing short-term BPV in hypertensive patients with underlying ischemic heart disease (IHD). This finding is novel, as, to the best of our knowledge, no previous studies have directly compared these exercise modalities with respect to their effects on BPV. Importantly, this study focused on patients with IHD, a population at particularly high cardiovascular risk, in whom interventions leading to improved BP control may confer substantial prognostic benefits [31]. Several studies have shown that exercise training is effective in reducing short-term BPV in both healthy individuals and patients with hypertension. The largest meta-analysis to date, including 15 studies, reported a 10–20% exercise-mediated reduction in both systolic and diastolic short-term BPV compared with control conditions, with stronger evidence in favor of continuous aerobic training interventions [32]. Nevertheless, data on more complex patient populations, such as those with IHD—particularly within structured cardiac rehabilitation programs—remain limited. In this context, a previous study demonstrated that a combined aerobic continuous and resistance training program was more effective than aerobic training alone in reducing 24-hour systolic BP variability [21]. The absence of significant effects on BPV observed in the interval combined training (ICT) group appears to be consistent with previous findings. Specifically, 24-hour systolic and diastolic short-term BPV have been shown to increase following a single session of HIIT, while decreasing after a combined exercise session consisting of MICT plus dynamic resistance exercise [20]. Moreover, Zercher et al. [33] reported an increase in BP reactivity, assessed using beat-to-beat measurements, following eight weeks of HIIT. In contrast to the findings for BPV, the present study did not demonstrate significant reductions in 24-hour systolic or diastolic BP values. These results differ from those reported by Martínez-Aguirre-Betolaza et al. [34], who compared moderate-intensity continuous training with HIIT in obese hypertensive individuals and observed significant reductions in 24-hour systolic and diastolic BP in both groups, without changes in BPV indices. Several factors may account for these discrepancies. Differences in the BPV indices used (coefficient of variation versus average real variability), sample characteristics (including sex distribution, age, and body mass index), training duration (12 versus 16 weeks), and pharmacological treatment may all have contributed to the divergent results. In addition, patients enrolled in the present study were receiving multiple antihypertensive medications, which may have limited the magnitude of BP changes detectable in a relatively small sample. Regarding exercise capacity, a greater increase in peak oxygen uptake (VO₂ peak) was observed in the ICT group compared with the continuous combined training (CCT) group. This finding is consistent with previous research in both healthy individuals and patients with IHD, with most studies reporting superior improvements in VO₂ peak following HIIT [35]. However, the greater impact of HIIT may be partly attributable to its higher caloric expenditure. This interpretation is supported by studies showing that when isocaloric exercise protocols are compared, HIIT and continuous training produce similar improvements in VO₂ peak [36]. Further studies with larger sample sizes and longer follow-up periods are warranted to confirm and extend the findings of the present investigation.
Limitations
The main limitation of this study is the relatively small sample size; therefore, the findings should be confirmed in larger, adequately powered trials. Additionally, the results cannot be generalized to women, as the study population consisted predominantly of male participants. Another limitation is the absence of a non-exercising control group. However, within the context of this investigation, this represents more of a theoretical than a practical limitation, as it is unlikely that the observed improvements in functional capacity over a three-month period could occur in the absence of structured exercise or merely as a function of time. Moreover, the lack of a non-exercise control group was unavoidable, as all participants were formally referred to an exercise-based cardiac rehabilitation program by their cardiologist or primary care physician under the Italian National Health Service reimbursement system; allocating patients to a non-exercise arm was therefore considered unethical. Finally, caloric expenditure was not quantified, and comparing equal durations of interval and continuous aerobic exercise may represent a methodological limitation.
5. Conclusions
Our data suggest that continuous combined training was more effective than interval combined training in reducing short-term systolic BPV, whereas patients in the interval training group achieved greater improvements in aerobic capacity. These findings underscore the importance of individualized exercise prescription in patients with IHD, tailoring training modalities to specific clinical and physiological objectives.
Author Contributions
M.V. (Matteo Vitarelli), M.A.P., F.I., and G.C. contributed to the conceptualization of the paper; C.C., A.A., D.M.G., and V.M. prepared the initial draft after acquisition, analysis, and interpretation of the results; G.M., B.R., E.P., and M.V. (Maurizio Volterrani) substantively revised the paper. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by funding from the Italian Ministry of Health [Ricerca corrente].
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Ethics Committee of San Raffaele IRCCS of Rome (protocol code SR 7/2024, approval date 21 September 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has also been obtained from the patients to publish this paper.
Data Availability Statement
The data presented in this study are available upon request from the corresponding authors.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BPV | Blood pressure variability |
| IHD | Ischemic heart disease |
| BP | Blood pressure |
| CCT | Continuous combined training |
| ICT | Interval combined training |
| MICT | Moderate intensity continuous training |
| HIIT | High-intensity interval training |
| LVEF | Left ventricular ejection fraction |
| ECG | Electrocardiography |
| CPET | Cardiopulmonary exercise testing |
| 6MWT | Six-minute walk test |
| ABPM | Ambulatory blood pressure monitoring |
| ARV | Average real variability |
| HR | Heart rate |
| 1-RM | One-repetition maximum |
| BMI | Body mass index |
References
- Wu, X.; Sha, J.; Yin, Q.; et al. Global burden of hypertensive heart disease and attributable risk factors, 1990–2021: insights from the global burden of disease study 2021. Sci Rep 2025, 15, 14594. [Google Scholar] [CrossRef] [PubMed]
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; et al. Global burden of hypertension and systolic blood pressure of at least 110 to 115 mmHg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef]
- Chen, Y.; Zhou, Z.F.; Han, J.M.; Jin, X.; Dong, Z.F.; Liu, L.; Wang, D.; Ye, T.B.; Yang, B.S.; Zhang, Y.P.; Shen, C.X. Patients with comorbid coronary artery disease and hypertension: a cross-sectional study with data from the NHANES. Ann Transl Med. 2022, 10, 745. [Google Scholar] [CrossRef] [PubMed]
- Weber, T.; Lang, I.; Zweiker, R.; Horn, S.; Wenzel, R.R.; Watschinger, B.; Slany, J.; Eber, B.; Roithinger, F.X.; Metzler, B. Hypertension and coronary artery disease: epidemiology, physiology, effects of treatment, and recommendations: A joint scientific statement from the Austrian Society of Cardiology and the Austrian Society of Hypertension. Wien Klin Wochenschr 2016, 128, 467–79. [Google Scholar] [CrossRef] [PubMed]
- Zang, J.; Liang, J.; Zhuang, X.; et al. Intensive blood pressure treatment in coronary artery disease: implications from the Systolic Blood Pressure Intervention Trial (SPRINT). J Hum Hypertens 2022, 36, 86–94. [Google Scholar] [CrossRef]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; Chieffo, A.; Christodorescu, R.M.; Deaton, C.; Doenst, T.; Jones, H.W.; Kunadian, V.; Mehilli, J.; Milojevic, M.; Piek, J.J.; Pugliese, F.; Rubboli, A.; Semb, A.G.; Senior, R.; Ten Berg, J.M.; Van Belle, E.; Van Craenenbroeck, E.M.; Vidal-Perez, R.; Winther, S.; ESC Scientific Document Group. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. Erratum in: Eur Heart J. 2025, 46, 1565. doi: 10.1093/eurheartj/ehaf079. 2024, 45, 3415–3537. [Google Scholar] [CrossRef]
- Parati, G.; Pomidossi, G.; Albini, F.; Malaspina, D.; Mancia, G. Relationship of 24-h blood pressure mean and variability to severity of target-organ damage in hypertension. J Hypertens 1987, 5, 93–98. [Google Scholar] [CrossRef]
- Cheng, X.; Song, C.; Ouyang, F.; Ma, T.; He, L.; Fang, F.; Zhang, G.; Huang, J.; Bai, Y. Systolic blood pressure variability: risk of cardiovascular events, chronic kidney disease, dementia, and death. Eur Heart J. 2025, 46, 2673–2687. [Google Scholar] [CrossRef]
- Saladini, F.; Fania, C.; Mos, L.; Vriz, O.; Mazzer, A.; Spinella, P.; Garavelli, G.; Ermolao, A.; Rattazzi, M.; Palatini, P. Short-Term but not Long-Term Blood Pressure Variability Is a Predictor of Adverse Cardiovascular Outcomes in Young Untreated Hypertensives. Am J Hypertens. 2020, 33, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Palatini, P.; Saladini, F.; Mos, L.; Fania, C.; Mazzer, A.; Cozzio, S.; Zanata, G.; Garavelli, G.; Biasion, T.; Spinella, P.; Vriz, O.; Casiglia, E.; Reboldi, G. Short-term blood pressure variability outweighs average 24-h blood pressure in the prediction of cardiovascular events in hypertension of the young. J Hypertens. 2019, 37, 1419–1426. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, S.; Parati, G.; Bangalore, S.; Bilo, G.; Kim, B.J.; Kario, K.; Messerli, F.; Stergiou, G.; Wang, J.; Whiteley, W.; Wilkinson, I.; Sever, P.S. Blood pressure variability: a review. J Hypertens. 2025, 43, 929–938. [Google Scholar] [CrossRef]
- Wang, J.G.; Yan, P.; Jeffers, B.W. Effects of amlodipine and other classes of antihypertensive drugs on long-term blood pressure variability: evidence from randomized controlled trials. J Am Soc Hypertens. 2014, 8, 340–9. [Google Scholar] [CrossRef]
- Toba, A. Effect of exercise and physical activity on blood pressure reduction. Hypertens Res 2025. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, J.W.; McCarthy, C.P.; Bruno, R.M.; Brouwers, S.; Canavan, M.D.; Ceconi, C.; Christodorescu, R.M.; Daskalopoulou, S.S.; Ferro, C.J.; Gerdts, E.; Hanssen, H.; Harris, J.; Lauder, L.; McManus, R.J.; Molloy, G.J.; Rahimi, K.; Regitz-Zagrosek, V.; Rossi, G.P.; Sandset, E.C.; Scheenaerts, B.; Staessen, J.A.; Uchmanowicz, I.; Volterrani, M.; Touyz, R.M.; ESC Scientific Document Group. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024, 45, 3912–4018. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Sharma, S.; Gati, S.; Bäck, M.; Börjesson, M.; Caselli, S.; Collet, J.P.; Corrado, D.; Drezner, J.A.; Halle, M.; et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021, 42, 17–96. [Google Scholar] [CrossRef] [PubMed]
- de Koning, I.A.; Heutinck, J.M.; Vromen, T.; Bakker, E.A.; Maessen, M.F.H.; Smolders, J.; Eijsvogels, T.M.H.; Grutters, J.P.C.; van Geuns, R.-J.M.; Kemps, H.M.C.; et al. Cardiac rehabilitation vs. percutaneous coronary intervention for stable angina pectoris: A retrospective study of effects on major adverse cardiovascular events and associated healthcare costs. Eur. J. Prev. Cardiol. 2024, 31, 1987–1990. [Google Scholar] [CrossRef]
- Ambrosetti, M.; Abreu, A.; Corrà, U.; Davos, C.H.; Hansen, D.; Frederix, I.; et al. Secondary prevention through comprehensive cardiovascular rehabilitation: from knowledge to implementation. 2020 update. A position paper from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology. Eur J Prev Cardiol. 2021, 28, 460–95. [Google Scholar] [CrossRef]
- Dibben, G.O.; Faulkner, J.; Oldridge, N.; Rees, K.; Thompson, D.R.; Zwisler, A.D.; Taylor, R.S. Exercise-based cardiac rehabilitation for coronary heart disease: a meta-analysis. Eur Heart J. 2023, 44, 452–469. [Google Scholar] [CrossRef]
- Kambic, T.; Šarabon, N.; Lainscak, M.; Hadžić, V. Combined resistance training with aerobic training improves physical performance in patients with coronary artery disease: A secondary analysis of a randomized controlled clinical trial. Front Cardiovasc Med. 2022, 9, 909385. [Google Scholar] [CrossRef]
- Caminiti, G.; Mancuso, A.; Raposo, A.F.; Fossati, C.; Selli, S.; Volterrani, M. Different exercise modalities exert opposite acute effects on short-term blood pressure variability in male patients with hypertension. Eur J Prev Cardiol. 2019, 26, 1028–1031. [Google Scholar] [CrossRef]
- Caminiti, G.; Iellamo, F.; Mancuso, A.; Cerrito, A.; Montano, M.; Manzi, V.; Volterrani, M. Effects of 12 weeks of aerobic versus combined aerobic plus resistance exercise training on short-term blood pressure variability in patients with hypertension. J Appl Physiol (1985) 2021, 130, 1085–1092. [Google Scholar] [CrossRef]
- Li, S.; Chen, X.; Jiao, H.; Li, Y.; Pan, G.; Yitao, X. The Effect of High-Intensity Interval Training on Exercise Capacity in Patients with Coronary Artery Disease: A Systematic Review and Meta-Analysis. Cardiol Res Pract. 2023, 2023, 7630594. [Google Scholar] [CrossRef]
- Li, L.; Liu, X.; Shen, F.; Xu, N.; Li, Y.; Xu, K.; Li, J.; Liu, Y. Effects of high-intensity interval training versus moderate-intensity continuous training on blood pressure in patients with hypertension: A meta-analysis. Medicine (Baltimore) 2022, 101, e32246. [Google Scholar] [CrossRef] [PubMed]
- Romero-Vera, L.; Ulloa-Díaz, D.; Araya-Sierralta, S.; Guede-Rojas, F.; Andrades-Ramírez, O.; Carvajal-Parodi, C.; Muñoz-Bustos, G.; Matamala-Aguilera, M.; Martínez-García, D. Effects of High-Intensity Interval Training on Blood Pressure Levels in Hypertensive Patients: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Life (Basel) 2024, 14, 1661. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. PAFS consensus group. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef]
- Kammin, E.J. The 6-Minute Walk Test: Indications and Guidelines for Use in Outpatient Practices. J Nurse Pract. 2022, 18, 608–610. [Google Scholar] [CrossRef] [PubMed]
- Mena, L.; Pintos, S.; Queipo, N.V.; Aizpurua, J.A.; Maestre, G.; Sulbaran, T. A reliable index for the prognostic significance of blood pressure variability. J Hypertens 2005, 23, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Flight, L.; Julious, S.A. Practical guide to sample size calculations: An introduction. Pharm. Stat. 2016, 15, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Lin, M; Lin, Y; Li, Y; Lin, X. Effect of exercise training on blood pressure variability in adults: A systematic review and meta-analysis. PLoS One 2023, 18, e0292020. [Google Scholar] [CrossRef]
- Lopes, S.; Mesquita-Bastos, J.; Garcia, C.; Leitão, C.; Ribau, V.; Teixeira, M.; Bertoquini, S.; Ribeiro, I.P.; de Melo, J.B.; Oliveira, J.; et al. Aerobic exercise improves central blood pressure and blood pressure variability among patients with resistant hypertension: Results of the EnRicH trial. Hypertens. Res. Off. J. Jpn. Soc. Hypertens. 2023, 46, 1547–1557. [Google Scholar] [CrossRef] [PubMed]
- Hao, Z.; Tran, J.; Lam, A.; Yiu, K.; Tsoi, K. Aerobic, Resistance, and Isometric Exercise to Reduce Blood Pressure Variability: A Network Meta-Analysis of 15 Clinical Trials. J Clin Hypertens (Greenwich) 2025, 27, e70050. [Google Scholar] [CrossRef] [PubMed]
- Zercher, S.; Muth, B.; Stock, J.; Edwards, D.G. The Effects of High-Intensity Interval Training and Moderate-Intensity Continuous Training in Sedentary Individuals on Blood Pressure Reactivity. Physiology 2025, 40, S1. [Google Scholar] [CrossRef]
- MartinezAguirre-Betolaza, A.; Mujika, I.; Fryer, S.M.; Corres, P.; Gorostegi-Anduaga, I.; Arratibel-Imaz, I.; Pérez-Asenjo, J.; Maldonado-Martín, S. Effects of different aerobic exercise programs on cardiac autonomic modulation and hemodynamics in hypertension: data from EXERDIET-HTA randomized trial. J Hum Hypertens. 2020, 34, 709–718. [Google Scholar] [CrossRef]
- Gomes-Neto, M.; Durães, A.R.; Conceição, L.S.R.; Silva, C.M.; Martinez, B.P.; Carvalho, V.O. High-intensity interval training versus moderate-intensity continuous training on exercise capacity and health-related quality of life in patients with coronary artery disease: An updated systematic review and meta-analysis. Braz J Phys Ther. 2025, 29, 101137. [Google Scholar] [CrossRef] [PubMed]
- Hannan, A.L.; Hing, W.; Simas, V.; et al. High-intensity interval training versus moderate-intensity continuous training within cardiac rehabilitation: a systematic review and meta-analysis. Open Access J Sports Med. 2018, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Study flow-chart.
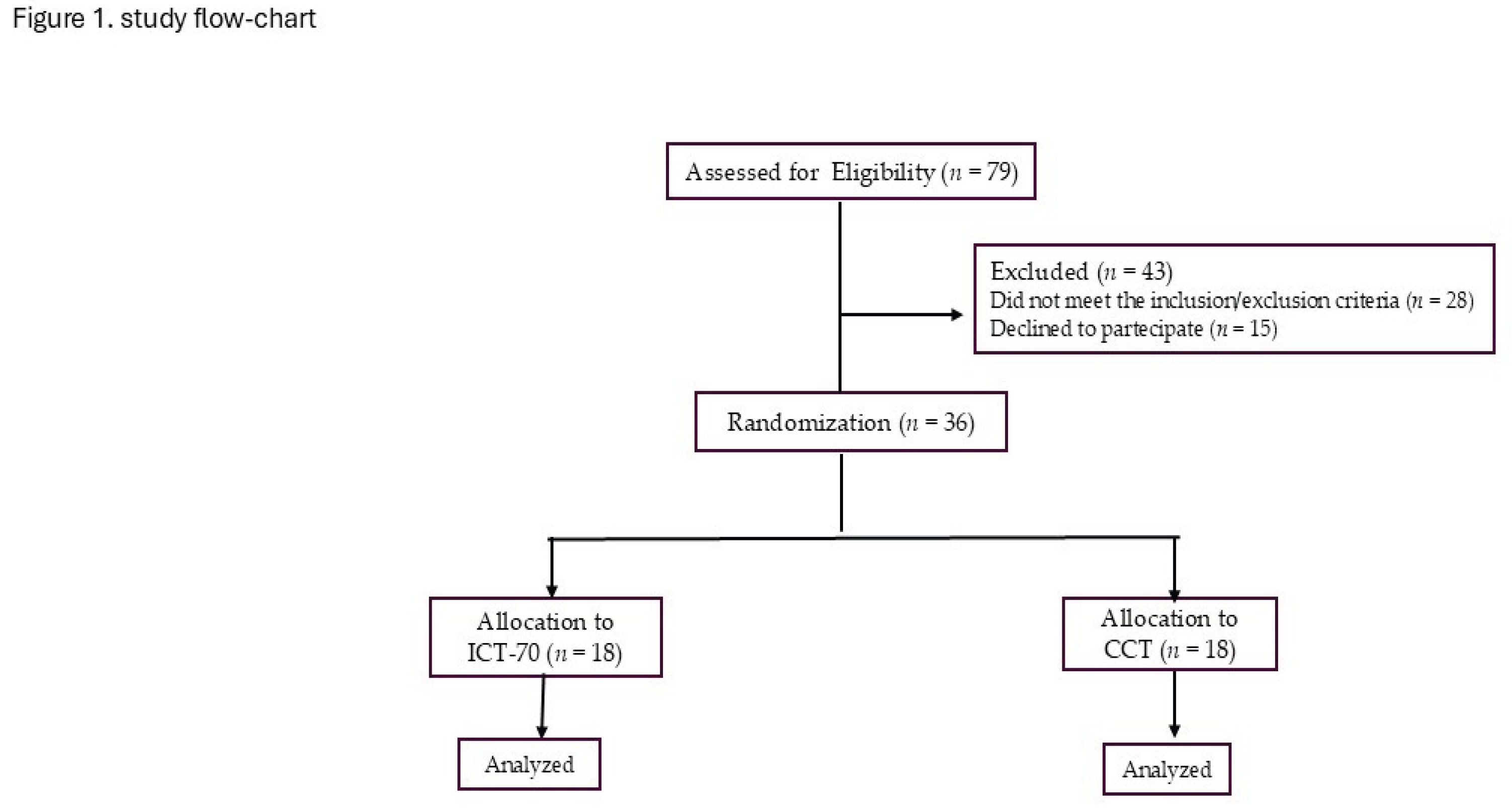

Table 1.
Baseline features of participants according to their allocation group.
| ICT (n=18) | CTT (n=18) | p | |
|---|---|---|---|
| Age, y | 66.1±11.2 | 65.4±12.7 | 0.682 |
| BMI, kg/m2 | 29.3±6.8 | 29.1±8.0 | 0.473 |
| Males, n (%) | 17 (94.4) | 16 (88.8) | 0.457 |
| Previous STEMI/NSTEMI-UA, n (%) | 13 (72.2)/ 5 (27.7) | 14 (77.7) / 4 (22.2) | 0.542 |
| Previous CABG/PCI, n (%) | 10 (55.5) / 14 (77.7) | 11 (61.1) / 14 (77.7) | 0.846 |
| Multivessel disease, n (%) | 13 (72.2) | 15 (83.3) | 0.439 |
| Carotid artery disease, n (%) | 9 (50.0) | 10 (55.5) | 0.598 |
| Diabetes, n (%) | 4 (22.2) | 5 (27.7) | 0.362 |
| Hypercholesterolemia, n (%) | 16 (88.8) | 17 (94.4) | 0.248 |
| Previous/active smoker, n (%) | 13 (72.2) / 3 (16.6) | 11( 61.1) / 2 (11.1) | 0.623 |
| eGFR, mL/min/1.73 m2 | 74.8±10.3 | 72.5±13.6 | 0.528 |
| LVEF, % | 54.2±7.2 | 53.8±8.2 | 0.344 |
| E/e’ ratio | 7.2±2.2 | 7.8±1.6 | 0.597 |
| Treatment | |||
| ACE-i/ARBs, n (%) | 18 (100.0) | 18 (100.0) | 0.784 |
| Betablockers, n (%) | 18 (100.0) | 18 (100.0) | 0.572 |
| MRAs, n (%) | 5 (27.7) | 4 (22.2) | 0.211 |
| Thiazide diuretic, n (%) | 9 (50.0) | 11 ( 61.1) | 0.668 |
| Ivabradine, n (%) | 2 (11.1) | 3 (16.6) | 0.395 |
| Statins, n (%) | 18 (100.0) | 18 (100.0) | 0.714 |
| CCAs, n (%) | 10 (55.5) | 11 (61.1) | 0.848 |
| Acetylsalicylic acid | 16 (88.8) | 16 (88.8) | 0.652 |
| Clopidogrel, | 3 (16.6) | 2 (11.1) | 0.283 |
| GLT-2 |
Table 2.
comparison.
| ICT | CCT | Adjusted between-group p | |||
| Baseline | 12-weeks | Baseline | 12-weeks | ||
| CPET | |||||
| VO2, ml/ kg/min | 25.5±3.9 | 29.4±3,6 | 24.9±4.3 | 27.1±38 | 0.032 |
| VE/VCO2 | 31.3±6.9 | 29.2±7.8 | 32.4±8.1 | 29.5±6.4 | 0.095 |
| Exercise time, sec | 498±66.2 | 567.3±73.1 | 512.6±78.8 | 581.2±84.1 | 0.368 |
| 6MWT distance, m | 351.7±88.4 | 426.3±92.1 | 349.4±84.8 | 413.3± 98.2 | 0.185 |
| SBP at rest , mmHg | 116.5±12.7 | 112.1±7.9 | 117.2±10.3 | 114.6±8.4 | 0.174 |
| DBP at rest, mmHg | 78.1 ± 6.8 | 75.7±7.6 | 77.7 ± 6.8 | 77.3 ± 5.4 | 0.511 |
| 24/h BP monitoring, mmHg | |||||
| BP averages | |||||
| 24/h SBP | 117.6±6.6 | 117.4±8.1 | 119.1±10.8 | 118.2±9.6 | 0.476 |
| Daytime SBP | 119±17.4 | 121.1±16.9 | 121.9±22.3 | 120.4±18.4 | 0.251 |
| Nighttime SBP | 111.5±13.2 | 112.1±16.8 | 112.7±13.5 | 112.1±15.0 | 0.063 |
| 24/h DBP | 76.6±4.4 | 75.1±5.7 | 72.9±6.9 | 72.8±8.0 | 0.683 |
| Daytime DBP | 78.2±8.4 | 77.8±9.1 | 75.3±6.6 | 75.4±9-4 | 0.372 |
| Nighttime DBP | 69.0±5.7 | 68.3±8.8 | 66.7±7.3 | 67.0±8.7 | 0.239 |
| BP variabiliy | |||||
| PAS – AVR | 9.4±2.1 | 9.5±2.7 | 10.7 ±2.6 | 8.3±1.8* | 0.029 |
| PAD- AVR | 7.6±1.4 | 7.2±1.0 | 8.1±2.6 | 7.9±2.8 | 0.352 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



