
Submitted:
26 December 2025
Posted:
30 December 2025
You are already at the latest version
Abstract
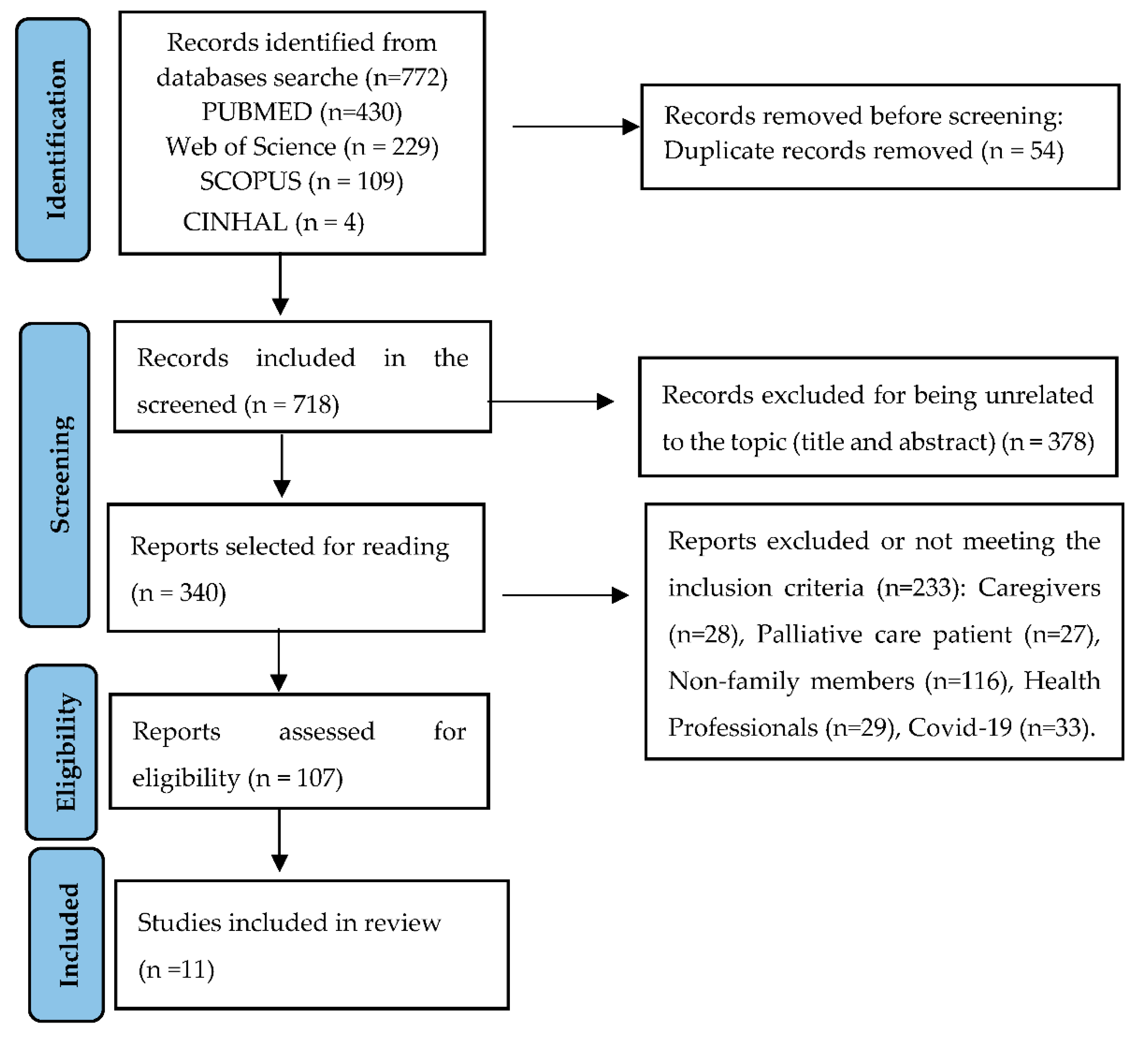
Background/Objectives: The aim of this study was to synthesise qualitative evidence from family members’ experiences of long-term home care for older adults provided by live-in migrant caregivers. Methods: We conducted a systematic literature review with meta-synthesis using four online databases. The search included articles published between January 2015 and November 2025 on the CINAHL, PubMed, SCOPUS and WOS databases. Thematic synthesis of qualitative data was conducted. Results: eleven papers from six different countries fulfilled the criteria and were included in the thematic synthesis. Four main themes were identified: 1. Not an easy decision. 2. A stranger at the heart of family life. 3. Two worlds that meet and need each other. 4. Improving the integration of migrant caregivers into family life. Hiring migrant caregivers to provide long-term home care to older adults can ease the burden on family caregivers, but it is an additional source of stress and worry. Conclusions: The family members of older adults call for greater financial and institutional support, as well as the involvement of social and health services in the training and education of families and migrant caregivers. Negotiation skills and the ability to reach consensus between older adults (OAs), family members and resident migrant caregivers are key to improving cohabitation and care for OAs. The primary goal is the well-being of the OAs, which involves overcoming cultural prejudices, learning together in response to the new situation, improving caregivers’ training, and ensuring continuity of care.
Keywords:
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Methods
2.3. Inclusion and Exclusion Criteria
2.4. Search Results
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Synthesis and Analysis
2.8. Rigor
3. Results
3.1. Not an Easy Decision
3.1.1. Hiring a Live-In Migrant Caregiver: When Choice Becomes a Necessity
I am the only child, I am working and have three children (…). I was ... overwhelmed, I went from home to work, from work to my mother’s home, (…) I stayed with her all night, returned to my home in the morning half asleep, then to work, and again run to cook something to eat.[19]
‘Home is incredibly important for us. When we built our house, we said “this is our senior apartment”. This is where we want to grow old’.[20]
Why do I hire migrant care workers? Because I work every day, and her (my mother’s) blood sugar is not well controlled.[46]
For example, my father had to go to bed at 7 p.m., because that was the time the nurse could be there. So, in fact, their whole life was arranged around the professional home care and not the other way around (Son).[20]
“I would say the main reason was that she wasn’t happy in the nursing homes. (…) she didn’t feel comfortable either” (daughter).[25]
We took turns, one months, two months, three months like that. Towards the end we were really tired and we started to point fingers at each other, like: Why do I have to take so much responsibility?[45]
‘So that the people can be taken care of at home and that the family can be at ease. The family can live in a different way. We were always anxious before: “I hope they didn’t fall; I hope nothing bad happened.’[20]
3.1.2. Demands of the Family Members
Of course they have to be able to deal well with older people with illnesses, have empathy, do a bit of housekeeping, be friendly to the older people, this is very important, and reassuring for the family’.[20]
She has her free days, but if anything arises, we need her to be available.[19]
One time my mother was not taken to the toilet in time, so she peed in the bed. That is a sign that [the live-in carer] does not really live up to the expectations... So I will continue to go there all the time to check up.[45]
Oh, that process was painful (…). My mother criticised the live-in carer, saying that she was ugly, that she had an ugly smile… So, it was difficult for her to take care of my mom, since my mom was criticising and insulting her all the time.[36]
My mother matters to her. She [the MCW] treats her like a person, not necessarily as someone for whom she works. [It is] more than that.[18]
3.1.3. Becoming an Employer
Therefore, in the morning, when (the live-in carer) wakes up, she will mop the floor and do the laundry. And, then, at seven o’clock, when he (the husband) wakes up, she will make milk for him, and give him milk and bread.[36]
She came to me and said that all her friends got higher salaries. . . I didn’t have a choice, did I? She would have left if I hadn’t given her more money.[31]
I see her as my family, she is like my sister and my friend. . . but what happens if she leaves? I don’t know.[45]
Am I, as her employer, supposed to purchase her cosmetics, such as body lotion and face lotion?[31]
She had to be available for 7 days, 24 hours to take care of my father. I thought it was almost slavery. But at the same time, it has been experienced by Linda (live-in carer) as an improvement in her situation (Son).[20]
3.2. A Stranger at the Heart of Family Life
“You don’t really know what kind of person is coming and how it will go and how they will react. (…) It’s a bit of an adventure” (daughter).[25]
3.2.1. Mixed Feelings: Between Doubt and Trust
They need to be watched closely because, at the first opportunity they get, they will care only for themselves.[31]
Of course, a lot of live-in carers are in families where they put up monitors or cameras and they are afraid that the live-in carers come only for money, and without any love... [I told the live-in carer] I trust that you will take good care of my sister, and you treat her as your own mother.[45]
We gave her money to buy groceries, and she said it cost 700 shekels per week, but we realized it was too much for two women, mainly as one of them hardly eats.[31]
“She (migrant home care worker) knows where the money is. I told her, ‘You don’t need to show me,’ I trust you 100%.” (Spouse)[47]
I feel that I can now be the master of my time management, because in the past, without the help of migrant care worker, the conditions of my parents were sometimes unstable, which made it difficult for me to engage in any activities.[46]
3.2.2. We Are All Interdependent: Grateful but Vigilant
It gives me a lot of comfort. So I don’t need to worry about what is happening at home...I think that the most important thing is that [live-in carer] takes good care of my mother, and then she will be in my family.[45]
This is a time for me to be alone with her, but there is someone (the migrant care worker) helping me. I feel an extreme need for this kind of service and assistance.[46]
I’m so dependent on her. She’s my oxygen, and therefore I’m very protective of her. I buy her presents and send gifts to her children. . . so she will stay with us.[45]
She is a good helper and now she is sick, then I have to be her caregiver right, I mean that’s only fair. So, I told her, ‘Ok, I will find a surgeon here in Singapore to do it and I will settle my mom’ […].[16]
Therefore, no matter what, honesty is crucial (…) truth, transparency, and regular updates.” (Son)[47]
It’s the same way as when I go to work, this is her job. She isn’t my friend and she isn’t my family.[18]
3.3. Two Worlds That Meet and Need Each Other
3.3.1. A Joint Effort
As she has a lot of experience already, in the beginning, I just observed a little bit on the side how she interacted with my mom, and then, after a couple of days, I just let her do her stuff. Also, I observed that the energy between the live-in carer and my mom was good.[36]
But my helper is good because she said that if your father knows that he has dementia, he will not behave in this manner. It’s because he doesn’t know, this is dementia she said. And she’s the one who taught us how to manage our temper.[16]
Transferring is a difficult thing because she’s (PWD) totally on us. Because she cannot control herself, and her neck and everything. Luckily my helper was very, very well trained that she can lift her onto the bed independently.[16]
Then for the rest of the week, the FDW has to do the day duty, and I do the night duty. We do rotation, otherwise it would be very difficult, very tiring.[44]
Originally, the migrant care worker was supposed to come to solve a problem, but there are also new adaptation issues that need to be addressed.[46]
3.3.2. When Problems Arise
(her mother)… was dissatisfied with her migrant care worker’s behavior, perceiving her as inattentive and wasteful, particularly critical of her use of a mobile phone and arguing back.[46]
It was quite challenging because my helper has the day-off, sometimes once a month or twice a month. So, when she is off, we don’t cook. Yah…otherwise, I would have to take leave or I would have to find respite care for my mum.[19]
We asked Ann to arrange a replacement for her weekends off. . . She told us how much it cost, and we paid her. But when we spoke with her replacement, we found out that Ann was charging us a commission. This hurt us.[31]
I don’t want to change caregivers. . . because then I would have to train another one and go through the process of adjusting all over again. . . It’s something that requires working through. . . I might consider a long-term care [facility] instead.[46]
3.3.3. Culture Shock
I don’t stop her practicing her religion. . .. we pray because we are Christians, and we pray for her, and when we come to pray [for my sister-in-law], we don’t force her to pray with us, but sometimes she comes to pray with us.[45]
[She should] learn the language better. She has been here for more than five years… She knows a lot of words in Hebrew and knows a little reading, but to construct a proper sentence—no![18]
I told my mother we have to get to know her and give her a chance because people cannot be judged by the color of their skin.[19]
3.4. Mejorando la Integración de Live-In Migrants Caregivers en la Vida Familiar
3.4.1. Llegar a Consensos
Yes, well, all of us siblings (...) got together. We had a meeting, and I had written down some important questions beforehand (...). And it was simply a question of what kind of help he needed (...). And my siblings then agreed because they saw that we (...) would organize it"[25]
“It was also important to try letting my aunt decide where she still has the ability to make decisions, like ‘What are we going to cook, what are we going to buy, where are we going to go now?’ (…) That we don’t just manage her. (…) That someone simply takes the reins and says: ‘Okay, I’m going to do it now.’ Or: ‘You will be cared for now.’”[25]
3.4.2. Superar Prejuicios Culturales
The openness and willingness to learn of the care migrant also play an important role, as a niece and her aunt explained[25]
Whenever we went to the hospital for the list, they recommended, ’no Colombians’, because, in the end, we all know each other.[19]
“She (migrant home care worker) is in a different place culturally. She doesn’t feel the connection that I do, she doesn’t have the love that I do, she doesn’t provide the care that I do (…) when we bring a human being and expect them to adapt to us, it doesn’t work that way. They come with their ‘bag’, with their life, with their culture, with their character, and they act here according to that, not according to the situation of our parents. Definitely not.” (Daughter)[47]
3.4.3. Learning Together
“… almost like family members” (son), “almost like a sister to me” (niece), or even “like a daughter” (husband receiving care).[25]
‘He has no medical knowledge. That in itself is the problem. I have trained him as far as I could. But the initiative has to come from him and there’s not much there’“[20]
“My mother gradually became reliant. . .[then later] too reliant, which led to a regression in her habits and abilities.”[46]
“We can relieve her so she can get some fresh air, go out to recharge her batteries. I try to come once a week. My sister also tries to visit. We really make an effort and tell her: ‘Go out, take some time for yourself.’ We are interested in her well-being, (…) we need to give her a good feeling, show her that she is important, that we appreciate her work.(Daughter [47]
3.4.4. Ensuring Continuity of Care
“Right now, it’s going very well because it’s always the same two women who come. They’ve been alternating for two years. It’s working really well now; when one arrives and the other leaves, we hardly notice it anymore”[25]
The elderly may exhibit resistance due to this unfamiliarity.[46]
3.4.5. Que OAs Estén Contentos
Yesterday, I took my mother out, and the migrant care worker accompanied us to the clinic to pick up medication. I even saw my mother in the examination room telling the caregiver, 'I am very grateful that you are here to take care of me.’ Witnessing this moment was quite comforting for me.[46]
4. Discussion
Limitations
5. Conclusions
6. Relevance to Clinical Practice
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations (UN). World Population Prospects 2022: Summary of Results. 2022. Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/wpp2022_summary_of_results.pdf (accessed on 26 March 2025).
- Dericioglu, D.; Methven, L.; Clegg, M.E. Understanding age-related changes: Exploring the interplay of protein intake, physical activity and appetite in the ageing population. Proc Nutr Soc. 2024, 1, 1–13. [Google Scholar] [CrossRef]
- INE (Instituto Nacional de Estadística). (2023). Indicadores de estructura de la población (Population Structure Indicators). 2022. Available online: https://www.ine.es/jaxi/Datos.htm?tpx=58505 (accessed on 6 April 2025).
- Ofori-Asenso, R.; Chin, K.L.; Curtis, A.J.; Zomer, E.; Zoungas, S.; Liew, D. Recent patterns of multimorbidity among older adults in high-income countries. Popul Health Manag. 2019, 22, 127–137. [Google Scholar] [CrossRef]
- Vetrano, D.L.; Palmer, K.; Marengoni, A.; Marzetti, E.; Lattanzio, F.; Roller-Wirnsberger, R.; Samaniego, L.L.; Rodríguez-Mañas, L.; Bernabei, R.; Onder, G. Frailty and multimorbidity: A systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci. 2019, 74, 659–666. [Google Scholar] [CrossRef]
- Kadambi, S.; Abdallah, M.; Loh, K.P. Multimorbidity, function, and cognition in aging. Clin Geriatr Med. 2020, 36, 569–584. [Google Scholar] [CrossRef]
- Dobarrio-Sanz, I.; Ruiz-González, C.; Fernández-Sola, C.; Roman, P.; Granero-Molina, J.; Hernández-Padilla, J.M. Healthcare professionals' perceptions of loneliness amongst older adults: A qualitative study. Int J Environ Res Public Health 2021, 18, 12071. [Google Scholar] [CrossRef]
- Knapp, S.J.; Wurm, G. Theorizing family change: A review and reconceptualization. J Fam Theory Rev 2019, 11, 212–229. [Google Scholar] [CrossRef]
- Kokorelias, K.M.; Gignac, M.A.M.; Naglie, G.; Cameron, J.I. Towards a universal model of family centered care: A scoping review. BMC Health Serv Res. 2019, 19, 1–11. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Framework for countries to achieve an integrated continuum of long-term care. 2021. Available online: https://apps.who.int/iris/bitstream/handle/10665/349911/9789240038844-eng.pdf?sequence=1 (accessed on 14 June 2025).
- Zerbib, S.; Vallet, L.; Muggeo, A.; de Champs, C.; Lefebvre, A.; Jolly, D.; Kanagaratnam, L. Copper for the prevention of outbreaks of health care–associated infections in a long-term care facility for older adults. J Am Med Dir Assoc. 2020, 21, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Kanda, K.; Sakurazawa, H.; Yoshida, T. International comparison of social support policies on long-term care in workplaces in aging societies. Int J Environ Res Public Health 2022, 19, 3284. [Google Scholar] [CrossRef]
- Aburto, J.M.; Villavicencio, F.; Basellini, U.; Kjærgaard, S.; Vaupel, J.W. Dynamics of life expectancy and life span equality. Proc Natl Acad Sci USA 2020, 117, 5250–5259. [Google Scholar] [CrossRef]
- Grete, B.; Dølvik, J.E. Long-term care. In Routledge handbook of the welfare state, 2nd ed.; Greve, B., Ed.; Routledge: Abingdon, 2018; pp. 498–507. [Google Scholar]
- Oh, E.; Moon, S.H.; Chung, D.; Choi, R.; Hong, G.R.S. The moderating effect of care time on care-related characteristics and caregiver burden: Differences between formal and informal caregivers of dependent older adults. Front Public Health 2024, 12. [Google Scholar] [CrossRef]
- Yuan, Q.; Zhang, Y.; Samari, E.; Jeyagurunathan, A.; Tan, G.T.H.; Devi, F.; Wang, P.; Magadi, H.; Goveas, R.; Ng, L.L.; et al. The impact of having foreign domestic workers on informal caregivers of persons with dementia – findings from a multi-method research in Singapore. BMC Geriatr. 2022, 22. [Google Scholar] [CrossRef]
- Liem, A.; Anggraini, L.; Bariyah, Nasrikah; Lestari, E. A long overdue recognition: Domestic workers as caregivers for older people in Asia. Lancet Healthy Longev. 2023, 4, e129–e130. [Google Scholar] [CrossRef]
- Cohen-Mansfield, J.; Golander, H. Bound in an imbalanced relationship: Family caregivers and migrant live-in care-workers of frail older persons in Israel. Qual Health Res. 2023, 33, 1116–1130. [Google Scholar] [CrossRef] [PubMed]
- Morales-Gázquez, M.J.; Medina-Artiles, E.N.; López-Liria, R.; Aguilar-Parra, J.M.; Trigueros-Ramos, R.; González-Bernal, J.J.; Rocamora-Pérez, P. Migrant caregivers of older people in spain: Qualitative insights into relatives’ experiences. Int J Environ Res Public Health 2020, 17, 2953. [Google Scholar] [CrossRef]
- Hoens, S.; Smetcoren, A.S. Hiring live-in migrant care workers: Motivations and experiences of older people and their families. J Popul Ageing 2023, 16, 497–518. [Google Scholar] [CrossRef]
- Casanova, G.; Martarelli, R.; Belletti, F.; Moreno-Castro, C.; Lamura, G. The impact of long-term care needs on the socioeconomic deprivation of older people and their families: Results from mixed-methods scoping review. Healthcare 2023, 11, 2593. [Google Scholar] [CrossRef]
- Heger, D.; Korfhage, T. Short- and medium-term effects of informal eldercare on labor market outcomes. Fem Econom 2020, 26, 205–227. Available online: https://www.tandfonline.com/doi/epdf/10.1080/13545701.2020.1786594?needAccess=true. [CrossRef]
- Ho, K.H.M.; Chiang, V.C.L.; Leung, D.; Ku, B.H.B. When foreign domestic helpers care for and about older people in their homes: I am a maid or a friend. Glob Qual Nurs Res. 2018, 29, 5. [Google Scholar] [CrossRef]
- Horn, V.; Schweppe, C.; Böcker, A.; Bruquetas-Callejo, M. Live-in migrant care worker arrangements in Germany and the Netherlands: Motivations and justifications in family decisionmaking. Int J Ageing Later Life 2019, 13. [Google Scholar] [CrossRef]
- Petry, H; Naef, R.; Rüesch, P.; Mahrer-Imhof, R.; Dreizler, J. Older persons’ and their families’ experience with live-in foreign home care workers. A grounded theory study. Pflege 2016, 29, 301–314. [Google Scholar] [CrossRef]
- European Migration Network (EMN). Annual report on migration and asylum, 2022. 2023. Available online: https://home-affairs.ec.europa.eu/system/files/2023-07/00_eu_arm2022_report.pdf (accessed on 12 May 2025).
- ILO (International Labour Organization). International Labour Organization ILO global estimates on international migrant workers. 2023. Available online: https://www.ilo.org/publications/major-publications/ilo-global-estimates-international-migrants-labour-force (accessed on 13 June 2025).
- Monguí, M.; Cáceres, P.; Ezquiaga, A. Libro Blanco sobre la situación de las mujeres inmigrantes en el sector del trabajo del hogar y los cuidados en España. 2022. Available online: https://www.inmujeres.gob.es/publicacioneselectronicas/documentacion/Documentos/DE1924.pdf (accessed on 10 June 2025).
- Ayalon, L. Fears come true: The experiences of older care recipients and their family members of live-in foreign home care workers. Int Psychogeriatr. 2009, 21, 779–786. [Google Scholar] [CrossRef]
- Díaz-Gorfinkiel, M.; Martínez-Buján, R. Mujeres migrantes y trabajos de cuidados: Transformaciones del sector doméstico en España. Panorama Social. 2018, 27, 105–118. Available online: https://www.funcas.es/wp-content/uploads/migracion/articulos/funcas_ps/027art08.pdf.
- Arieli, D.; Halevi, I. Family caregivers as employers of migrant live-in care workers: Experiences and policy implications. J Aging Soc Policy 2023, 36, 639–657. [Google Scholar] [CrossRef]
- Salami, B.; Duggleby, W.; Rajani, F. The perspective of employers/families and care recipients of migrant live-in caregivers: A scoping review. Health Soc Care Community 2017, 25, 1667–1678. [Google Scholar] [CrossRef] [PubMed]
- de São José, J.; Barros, R.; Samitca, S.; Teixeira, A. Older persons’ experiences and perspectives of receiving social care: A systematic review of the qualitative literature. Health Soc Care Community 2016, 24, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Teshuva, K.; Cohen-Mansfield, J.; Iecovich, E.; Golander, H. Like one of the family? Understanding relationships between migrant live-in care workers and older care recipients in Israel. Ageing Soc. 2019, 39, 1387–1408. [Google Scholar] [CrossRef]
- Kramar, M.J.F.; García-Caro, M.P.; Ternero, A.M.; Martí-García, C. Migrant women caregivers’ experiences in end-of-life formal care. Rev Esc Enferm USP 2023, 57, e20230031. [Google Scholar] [CrossRef]
- Munkejord, M.C.; Ness, T.M.; Gao, I.W.S. “This Life is Normal for Me”: A Study of Everyday Life Experiences and Coping Strategies of Live-in Carers in Taiwan. J Gerontol Soc Work. 2021, 64, 533–546. [Google Scholar] [CrossRef]
- Vahabi, M.; Wong, J.P.H. Caught between a rock and a hard place: Mental health of migrant live-in caregivers in Canada. BMC Public Health 2017, 17, 498. [Google Scholar] [CrossRef]
- Corbally, M.; Ffrench, O.; Rodger, D.; Ricci, R.; Phelan, A. A narrative exploration of family members' perspectives of life story phases following transition of an older family relative into Long-Term Care. Int J Older People Nurs. 2025, 20, e70001. [Google Scholar] [CrossRef]
- Sandelowski, M.; Barroso, J. Handbook for synthesizing qualitative research; Springer: New York, 2007. [Google Scholar]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med Res Methodol. 2012, 12, 181. [Google Scholar] [CrossRef]
- Aromataris, E.; Lockwood, C.; Porritt, K.; Pilla, B.; Jordan, Z. (Eds.) JBI Manual for Evidence Synthesis; JBI, 2024; Available online: https://synthesismanual.jbi.global (accessed on 30 October 2025). [CrossRef]
- Joanna Briggs Institute (JBI). Checklist for qualitative research. 2020. Available online: https://jbi.global/critical-appraisal-tools (accessed on 1 April 2024).
- Lockwood, C.; Munn, Z.; Porritt, K. Qualitative research synthesis: Methodological guidance for systematic reviewers utilizing meta-aggregation. Int J Evid Based Healthc. 2015, 13, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Mehta, K.K.; Leng, T.L. Experiences of formal and informal caregivers of older persons in Singapore. J Cross-Cult Gerontol. 2017, 32, 373–385. [Google Scholar] [CrossRef] [PubMed]
- Ness, T.M.; Silan, W. We tried to take care of her, but it got too exhausting": A study of the transition from family carer to employer. Glob Qual Nurs Res. 2023, 16. [Google Scholar] [CrossRef]
- Yen, C.M. Understanding family caregivers' experiences with live-in migrant care workers in dementia care: Challenges and perspectives from a qualitative study in Taiwan. Inquiry. 2025, 62, 469580251355826. [Google Scholar] [CrossRef] [PubMed]
- Ayalon, L.; Ulitsa, N.; Nebowsky, A.E.; Schweda, M.; von Kutzleben, M. Caring for an older person with dementia: Behavioral problems in the eyes of family caregivers and migrant home care workers. Dementia 2025, 24, 884–901. [Google Scholar] [CrossRef]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 2008, 8, 45. [Google Scholar] [CrossRef]
- Lee, C.S.; Tan, J.S.Y.; Goh, S.Y.; Ho, K.H.M.; Chung, R.Y.; Chan, E.Y.; Liaw, S.Y.; Seah, B. Experiences of live-in migrant caregivers providing long-term care for older adults at home: A qualitative systematic review and meta-ethnography. Int J Nurs Stud. 2025, 164, 105019. [Google Scholar] [CrossRef]
- Septi, Y.; Yeni, C.; Fields, B.E.; Chang, F.H. A descriptive qualitative study of foreign caregivers of older adult stroke survivors. Gerontologist 2023, 63, 82–95. [Google Scholar] [CrossRef]
- Cea, M.A. Percepción social de las migraciones en España. Panorama Social 2016, 24, 129–144. [Google Scholar]
- Walsh, K.; Shutes, I. Care relationships, quality of care and migrant workers caring for older people. Ageing & Society 2013, 393–420. [Google Scholar]
- Iecovich, E. Client satisfaction with live-in and live-out home care workers in Israel. J Aging Soc Policy 2007, 19, 105–122. [Google Scholar] [CrossRef]
- Phua, G.L.G.; Poh, Y.K.; Ong, B.S.; Tan, J.Y.T.; Koh, A.R.X.; Yang, G.M. Experiences of migrant live-in caregivers in caring for patients with advanced cancer - a qualitative study. Am J Hosp Palliat Care 2025, 42, 989–996. [Google Scholar] [CrossRef]
- McArthur, C.; Bai, Y.; Hewston, P.; Giangregorio, L.; Straus, S.; Papaioannou, A. Barriers and facilitators to implementing evidence-based guidelines in long-term care: A qualitative evidence synthesis. Implement Sci. 2021, 16, 70. [Google Scholar] [CrossRef]
- Nurunnaher; Xiao, L.; Gordon, S.; Ahmad, M. Experiences of family caregivers of people with dementia from a Muslim migrant background in high-income countries: A systematic review and meta-synthesis. Aging Ment Health 2023, 27, 2319–2328. [Google Scholar] [CrossRef] [PubMed]
- Tawodzera, O. Unravelling the tensions: Exploring the interplay of paid care work, family obligations, and transnational care among Zimbabwean migrant care workers in the UK. J Fam Stud. 2024, 30, 739–758. [Google Scholar] [CrossRef]

| Databases | Search Strategy | Results |
|---|---|---|
| CINAHL | XB (famil' or relatives) AND TI (qualitative) AND XB (migrant care) | 4 |
| PubMed | ((("migrant care worker"[Title/Abstract]) AND ("family" [Title])) OR ("relatives"[Title])) AND ("qualitative"[Title) | 430 |
| SCOPUS | TITLE-ABS-KEY (famil* OR relatives OR employer) AND TITLE-ABS-KEY (experiences OR perception) AND TITLE-ABS-KEY (migrant AND care AND worker) AND TITLE-ABS-KEY (qualitative AND research) | 109 |
| Web of Science | (((((((TS=(famil*)) OR TS=(relatives)) OR TS=(employer)) AND TS=(experiences)) OR TS=(perception)) AND TS=(migrant care worker)) AND TS=(qualitative research)) | 229 |
| TOTAL | 772 | |
| Article | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Petry et al. (2016) [25] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Mehta & Leng, (2017) [44] | ✔ | ✔ | ↔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ | ✔ |
| Morales-Gázquez et al. (2020) [19] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ |
| Munkejord et al. (2021) [36] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Yuan et al. (2022) [16] | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ | ✔ |
| Cohen-Mansfield & Golander (2023) [18] | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ | ✔ |
| Ness & Silan (2023) [45] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Hoens & Smetcoren (2023) [20] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ↔ | ✔ |
| Arieli & Halevi, 2024 [31] | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ | ✔ |
| Yen (2025) [46] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Ayalon et al. (2025) [47] | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ |
| Stage | Description | Steps |
|---|---|---|
| STAGE 1 | Text coding | Recall review question Read/re-read findings of the studies Line-by-line inductive coding Review of codes in relation to the text |
| STAGE 2 | Development of descriptive themes | Search for similarities/differences between codes Inductive generation of new codes Write preliminary and final report |
| STAGE 3 | Development of analytical themes | Inductive analysis of sub-themes Individual/independent analysis Pooling and group review |
| Author and year | Country | Sample | Design | Data collection |
Data analisys |
Main Theme |
|---|---|---|---|---|---|---|
| Petry et al. (2016) [25] | Swiss | 15 family members | Mixed methods study. Grounded Theory | Semi-structured interviews | Grounded Theory techniques | A successful care system includes relationships and negotiated coexistence within the family network. |
| Mehta & Leng (2017) [44] | Singapore | 30 family members and 15 migrant caregivers | Descriptive qualitative study | Semi-structured in-depth interview | Strauss thematic analysis | Experiences and impact of caregiving on migrant family members and caregivers. |
| Morales-Gázquez et al. (2020) [19] | Spain | 9 family members | Descriptive phenomenological study | In-depth interviews and a focus group | Braun & Clarke thematic analysis | Reasons for hiring a migrant caregiver and adaptation of family members during the process |
| Munkejord et al. (2021) [36] | Taiwan | 10 family members and 10 caregivers | Descriptive qualitative study | Semi-structured conversations |
Braun & Clarke thematic analysis | Interrelationships and collaboration between family members and caregivers |
| Yuan et al. (2022) [16] |
Singapore | 15 family members | Mixed methods study | Semi-structured interviews | Braun & Clarke thematic analysis | Support and challenges for family members of people with dementia in hiring a migrant caregiver. |
| Cohen-Mansfield & Golander (2023) [18] | Israel | 92 caregiver-family dyads | Mixed methods study | One-on-One interview | Braun & Clark thematic analysis, theory founded on Strauss & Corbin | Family members’ experiences of the relationship with caregivers and development of interdependence. |
| Ness & Silan, (2023) [45] | Taiwan | 6 family members and 10 caregivers | Descriptive qualitative study | Semi-structured conversations |
Narrative hermeneutic analysis | Experiences of transition from family caregiver to employer |
| Hoens & Smetcoren (2023) [20] | Belgium | 8 family members, 8 OAs and 11 healthcare providers | Descriptive qualitative study | Semi-structured interviews and a focus group | Braun & Clark thematic analysis | Experiences of hiring and living with a migrant caregiver. |
| Arieli & Halevi (2023) [31] | Israel | 35 family members | Descriptive phenomenology | Semi-structured in-depth interview | Thematic analysis according to Graneheim and Lundman | Experiences of family employers of migrant caregivers |
| Yen (2025) [46] | Taiwan | 4 family caregivers | Descriptive qualitative study | Semi-structured in-depth interview | Braun & Clark thematic analysis | The need to strengthen the knowledge of migrant caregivers. |
| Ayalon et al. (2025) [47] | Israel | 17 family members and 21 migrants caregivers | Descriptive qualitative study | Semi-structured in-depth interview | Braun & Clark thematic analysis | Families as guarantors of labor relations with migrant caregivers. |
| Theme | Subtheme | Units of meaning |
|---|---|---|
| 3.1 Not an easy decision. | 3.1.1 Hiring a migrant domestic caregiver: when choice becomes a necessity | Deteriorating health, only child, working woman, difficulty adapting to a nursing home, lack of social assistance, need to reduce the workload of the informal caregiver |
| 3.1.2 Demands of the family members | Household chores, affection, respect, conditions, lack of training, initiative, keen to learn | |
| 3.1.3 Becoming an employer | Financial problems, salary increase, caregiver needs, caregiver overload, mediation | |
| 3. 2. A stranger at the heart of family life | 3.2.1 Mixed feelings: between doubt and trust | Increased responsibilities, support, insecurity, supervision, financial control |
| 3.2.2 We are all interdependent: grateful but vigilant | Balancing personal life with caregiving, gratitude, caring for the caregiver, mutual help, part of the family, working relationship, care recipient | |
| 3.3 Two worlds that meet and need each other | 3.3.1 A joint effort | Emotional support, physical support, training, household organisation |
| 3.3.2 When problems arise | Manipulation, deception, departure, financial gain, extortion | |
| 3.3.3 Culture shock | Adaptation, language barrier, customs, respect, rejection | |
| 3.4 Improving the integration of live-in migrant caregivers into family life | 3.4.1 Reaching consensus. | Family consensus, consensus with migrant caregiver, negotiation |
| 3.4.2 Overcoming cultural prejudices | Lack of local caregivers, recommendations, prejudices | |
| 3.4.3 Learning together | Language barriers, caring for the caregiver, training the caregiver, integration into family and social life | |
| 3.4.4 Ensuring continuity of care | Building relationships, safety of OAs, family’s peace of mind | |
| 3.4.5 The well-being of OAs | Staying at home, feeling cared for, joining the caregiver |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



