
Submitted:
24 December 2025
Posted:
24 December 2025
You are already at the latest version
Abstract
Objectives: To summarize the best evidence regarding folic acid supplementation for preventing neural tube defects (NTDs) in women of childbearing age and to develop a structured evidence summary for guiding clinical practice. Methods: We systematically searched multiple databases and professional websites from January 1, 2013, to September 18, 2025. Sources included 7 databases (PubMed, Embase, CINAHL, Web of Science, CNKI, Wanfang, VIP) and 20 professional websites (e.g., Medlive, GIN, NICE, ACOG, UpToDate, Chinese Medical Knowledge Database, etc.). The search targeted clinical guidelines, expert consensuses, and recommended practices on folic acid supplementation for NTD prevention in women of childbearing age. The retrieved literature underwent quality assessment, evidence extraction, and summarization. Results: The review included 17 publications: 8 guidelines, 4 expert consensuses, and 5 recommended practices. From these, we synthesized 14 distinct evidence statements, organized into five thematic dimensions: risks of neural tube defects and the role of folic acid, time window of neural tube closure, timing and dosage of folic acid supplementation, relationship between dietary folic acid and folic acid tablets, and folic acid-related testing. Conclusions: his study synthesized the best available evidence regarding folic acid supplementation for preventing NTDs in women of childbearing age, providing an evidence-based foundation to inform clinical practice. Future implementation efforts should focus on integrating recommendations into electronic health systems, developing precision public health interventions, and employing visual aids for health education.
Keywords:
folic acid supplementation
; neural tube defects
; periconceptional care
; evidence-based medicine
; best evidence
1. Introduction
Neural tube defects (NTDs) constitute a major global public health issue, with an incidence rate of 18.6 per 10,000 live births worldwide. Approximately 260,100 new cases occur annually, and 75% of individuals born with an NTD die before reaching the age of five [1]. Beyond the profound impact on individual health, NTDs impose substantial economic and psychological burdens on families and place a heavy strain on healthcare system for long-term treatment and management [2]. The prevalence of NTDs demonstrates significant geographical and socioeconomic variation, with low- and middle-income countries bearing a disproportionately heavy burden [3]. Notably, adequate folic acid supplementation during the periconceptional period has been proven to significantly reduce the risk of NTDs [4], underscoring its central role as a primary prevention strategy.
However, a significant gap exists globally between folic acid supplementation practices and scientific evidence. A meta-analysis revealed that preconception supplementation rates are suboptimal, remaining below 50% in developed countries and consistently falling below 25% in low- and middle-income countries [5]. A study in China found that only 16.1% of pregnant women took folic acid at the correct time [6]. This low compliance rate is closely linked to low awareness levels among women of childbearing age regarding folic acid. International studies confirm this widespread knowledge gap: in South Korea, only 23.7% of women clearly understood folic acid’s role in preventing NTDs and the correct timing for its supplementation [7]; while a study in Saudi Arabia found that merely 55.7% of female university students were aware of the appropriate intake timing [8]; furthermore, research across six economically underdeveloped provinces in China revealed that only 15% of women mastered core knowledge including folic acid’s preventive effect, optimal intake timing, methods, and dosage [9].
At its root, the low awareness of folic acid knowledge among women of childbearing age stems from the combined effects of health determinants and contemporary information environment characteristics. Research consistently indicates that structural factors such as low educational attainment, low income, and limited healthcare accessibility are core barriers constraining the acquisition and understanding of folic acid supplementation knowledge [5,6,7,8]. However, in the digital age, this issue presents new characteristics: the internet has become the primary channels for women of childbearing age to obtain health information [7,8]. While these channels have broken down some geographical and economic barriers, they have introduced new challenges such as information overload, inconsistent quality, and the proliferation of misleading content. Although scientifically rigorous clinical practice guidelines exist, their comprehensive and highly specialized content—often embedding core recommendations within complex diagnostic and therapeutic contexts—makes them lengthy and impractical for public health advocacy, health education materials, and rapid consultation by primary healthcare workers.
Therefore, overcoming this challenge hinges on systematically extracting, synthesizing, and translating the core evidence scattered across high-quality guidelines. Currently, there is a lack of a comprehensive, authoritative, clear, and widely accessible evidence knowledge base and personalized support tools for folic acid supplementation [10]. Given this, there is an urgent need to synthesize the best available evidence on folic acid for preventing fetal neural tube defects, establish a standardized knowledge base, and develop new health education approaches to effectively enhance their folic acid-related knowledge and ultimately improve intake behaviors.
This study aimed to systematically retrieve, screen, and evaluate literature, then extract and synthesize evidence, thereby developing a structured, easily accessible and applicable knowledge base for guiding folate acid intake among women of childbearing age. This knowledge base will provide direct, reliable core knowledge support for developing evidence-based health education materials and clarifying key points for clinical counseling. Ultimately, it will serve clinical practice and public health interventions, helping to bridge the gap between knowledge, belief, and action.
2. Materials and Methods
2.1. Literature Inclusion and Exclusion Criteria
Studies were included if they met the following criteria: (1) focused on folic acid supplementation for the prevention of neural tube defects; (2) were guideline documents, expert consensuses, best practices, or recommended practices; (3) were developed using evidence-based or formal consensus methodologies (guidelines without evidence grading or recommendation strength were defined as “non-evidence-based” [11]); (4) were the latest version available; and (5) were published in Chinese or English.
Studies were excluded if they were: (1) direct translations, duplicates, or interpretations of existing guidelines; or (2) unavailable in full text.
2.2. Literature Search Strategy
A systematic search was performed following standard methodology for evidence synthesis. We employed a combination of subject headings and free-text terms in both English and Chinese. English terms included, but were not limited to: “Folic Acid,” “folate,” “Preconception Care,” “Neural Tube Defects,” “anencephaly,” and “spina bifida.” Corresponding Chinese terms were used in Chinese databases.
Comprehensive searches were conducted in electronic databases (e.g., PubMed, Embase, CINAHL, Web of Science, CNKI, Wanfang, VIP) and the websites of major professional organizations (e.g., UpToDate, NICE, SIGN, ACOG, SOGC, Chinese Medical Association). The detailed search strategies for all sources are provided in Appendix A.
The initial search covered the period from January 1, 2013, to December 31, 2024. An updated search was performed on September 18, 2025, to identify any newly published guidelines. Although 28 new records were identified, only one recent guideline [12] was deemed relevant. Upon full-text review, its recommendations were found to be derived from evidence already captured in our initial search; consequently, no additional publications were included from the update.
2.3. Literature Screening and Data Extraction
Two reviewers, who had received training in JBI evidence-based methodology and had experience in conducting systematic reviews, independently performed the study selection and data extraction. Any discrepancies were resolved through consensus or, when necessary, by consulting a third reviewer.
The selection process was managed using EndNote 20 software. After removing duplicates, the reviewers screened titles and abstracts against the inclusion criteria. The full texts of potentially relevant records were then retrieved and assessed for eligibility. Additionally, the reference lists of all included publications were manually searched to identify any additional relevant studies.
A standardized data extraction form was developed and used to extract key information from the included documents, including the title, publication/update year, author(s)/issuing body, source of publication, journal of publication, country/region, and recommendations related to folic acid and NTD prevention.
2.4. Literature Quality Assessment
The quality of the included evidence was critically appraised using standardized tools by two independent reviewers. Any discrepancies were resolved through discussion or with input from a third researcher.
Clinical Practice Guidelines were assessed using the Appraisal of Guidelines for Research and Evaluation II (AGREE II) instrument. This tool comprises 23 items across 6 domains: Scope and Purpose, Stakeholder Involvement, Rigor of Development, Clarity of Presentation, Applicability, and Editorial Independence. Each of the 23 items is rated on a 7-point scale, where a score of 1 indicates an absence of relevant information or very poor reporting, and a score of 7 represents high-quality reporting that fulfills all criteria. Scores between 2 and 6 reflect varying levels of reporting completeness and quality. The score for each domain was calculated as the sum of the scores of all items within that domain. This raw score was then standardized using the AGREE II standard formula: Standardized Score (%) = (Obtained Score – Minimum Possible Score) / (Maximum Possible Score – Minimum Possible Score) × 100.
As the AGREE II User Manual does not define thresholds for standardized domain scores indicating high guideline quality, this study extensively referenced multiple guideline quality assessment studies [13,14,15]. Based on standardized domain scores, we defined the following criteria for recommendation: (1) Grade A (Recommended): Standardized scores ≥60% in all 6 domains; (2) Grade B (Recommended with modifications): Standardized scores are between 30% and 60% in most domains (≥3); (3) Grade C (Not recommended): ≥3 domains with standardized scores <30%. Only guidelines categorized as Grade A or B were included for evidence extraction.
To ensure consistency, inter-rater reliability was quantified using the Intraclass Correlation Coefficient (ICC). The ICC was interpreted as follows: < 0.40, poor; 0.40–0.75, moderate; and > 0.75, high agreement [16].
Expert Consensuses, Best Practices, and Recommended Practices were appraised using the corresponding JBI Critical Appraisal Checklist for Text and Opinion Papers [17]. This tool comprises six items that assess the credibility and logical development of the expert opinion. Two reviewers independently evaluated each document, rating the items as “Yes,” “No,” “Unclear,” or “Not Applicable.” A document was included only if it achieved a pre-established quality threshold, which required affirmative (“Yes”) responses to a majority of the items, with particular emphasis on the logical derivation of the conclusions.
2.5. Evidence Translation and Synthesis
Recommendations regarding folic acid intake for the prevention of neural tube defects were extracted from the included literature by two researchers working independently and concurrently. The extractions were then cross-checked. Any discrepancies identified were resolved through discussion between the two researchers, or by adjudication from a third researcher when consensus could not be reached. For recommendations published in English, both researchers independently translated them into Chinese. We compared these translations and discussed them to create a consensus version.
The synthesis of all recommendations (both translated and original) into the final evidence summary was guided by the following principles: (1) for identical recommendations, select the most clearly articulated version; (2) for conflicting recommendations, trace the evidence sources and prioritize the one based on the most recent and highest-quality evidence; (3) for complementary recommendations, merge their content into a comprehensive statement; and (4) for independent recommendations, retain the original statement. This methodology was adapted from established practices for evidence synthesis [18].
3. Results
3.1. Literature Search Results and Overview
The systematic search identified 840 records. After the removal of 261 duplicates, 509 records were excluded following title and abstract screening. A further 53 publications were excluded after full-text assessment, resulting in a final inclusion of 17 publications for evidence synthesis. The included literature comprised 10 clinical practice guidelines, 4 expert consensus statements, 2 recommended practice documents, and 1 best practice document. The study selection process is detailed in the PRISMA flow diagram (Figure 1), and the basic characteristics of the included publications are summarized in Table 1.
3.2. Included Guideline Quality Assessment Results
Among the included guidelines, three guidelines were rated as Grade A (recommended), five as Grade B (recommended with modifications), and two as Grade C (not recommended) which were excluded. The inter-rater reliability for the AGREE II assessments was high, with Intraclass Correlation Coefficient (ICC) values ranging from 0.773 to 0.908 across all evaluated guidelines, all exceeding the threshold of 0.75 for high agreement. The detailed scores for each domain are presented in Table 2.
3.3. Inclusion of Expert Consensus, Best Practice, and Recommended Practice Evaluation Results
All four expert consensus documents, two recommended practice documents, and one best practice document met the pre-specified quality threshold in the JBI critical appraisal and were therefore included for evidence extraction. The results of the quality evaluation for these documents are presented in Table 3.
3.4. Best Evidence Summary
By systematically synthesized evidence regarding folic acid intake for the prevention of neural tube defects in women of childbearing age, we integrated findings across five key thematic dimensions: (1) the harm of neural tube defects and the role of folic acid; (2) the time window of neural tube closure; (3) the timing and dosage of folic acid supplementation; (4) the relationship between dietary folate and folic acid supplements; and (5) folic acid-related testing. This synthesis yielded 14 distinct best practice evidence statements, which were graded using the JBI evidence pre-classification and evidence rank system (2014) [36], as shown in Table 4.
4. Discussion
4.1. Rigor and Scientific Soundness of the Evidence Summary Process
The development of this evidence summary adhered to a rigorous and systematic methodology to ensure its scientific soundness. The work was conducted by a team comprising two master’s degree candidates and one specialist in nursing education and research, all of whom have undergone formal training in evidence-based nursing and evidence translation methodology and have declared no conflicts of interest.
The process involved a comprehensive review of the literature on folic acid supplementation for preventing neural tube defects in women of childbearing age. Two researchers independently executed the systematic search, screening, quality appraisal, and data extraction from guidelines, expert consensuses, best practices, and recommended practices. The final evidence statements were derived through consensus meetings. The quality appraisal results affirm the reliability of the included evidence. Of the ten identified guidelines, seven met the quality threshold for inclusion: three [21,22,25] were rated as Level A (recommended) and five [19,20,23,24,26] as Level B (recommended with modifications), indicating that they were developed using rigorous and reliable methodologies. The two guidelines rated Level C (not recommended) [27,28] were excluded. Furthermore, all four [30,31,32,33] expert consensuses, one best practice [29], and two recommended practices [34,35] were assessed to be of high credibility and were retained.
This process culminated in a summary of 14 best evidence statements, organized across 5 domains. The entire process—from retrieval and screening to evaluation and extraction—was conducted according to strict principles of transparency and scientific rigor, under the supervision and final review of a senior nursing expert to ensure an objective and accurate synthesis of the current best evidence.
4.2. Knowledge Base on Folic Acid Intake for Preventing Neural Tube Defects in Women of Childbearing Age
4.2.1. The Risks of Neural Tube Defects and the Role of Folic Acid
Neural tube defects (NTDs), also known as neural tube malformations, represent a group of major congenital anomalies arising from the failure of normal neural tube closure during early embryogenesis. The primary clinical manifestations include anencephaly, spina bifida, and encephalocele. Anencephaly and severe encephalocele are conditions that most commonly lead to fetal death or stillbirth. In the rare instances where live birth occurs, affected newborns typically survive for only a very short period or present with severe neurological deficits. Children with spina bifida and mild encephalocele may survive but cannot be cured, often leading to lifelong disabilities such as lower limb paralysis, urinary and fecal incontinence, and intellectual impairment. Children with spina bifida are also prone to hydrocephalus, with many succumbing to premature death [19,34].
Folic acid, also known as vitamin B9, cannot be synthesized in the human body and must be obtained from external sources. Foods rich in natural folate include dark green vegetables, citrus fruits, legumes, nuts, and animal liver. Folic acid added to medications, supplements, and fortified foods is typically synthetic folic acid [19]. A substantial body of evidence confirms that additional folic acid intake and consumption of folate-rich diets effectively reduce the occurrence and recurrence of neural tube defects [19,20,23,29,34].
4.2.2. Timing of Neural Tube Closure and the Significance of Preconception Folate Intake
Normally, the human embryonic neural tube closure begins on day 21 after conception (equivalent to day 35 after the last menstrual period) and completes closure by day 28 (equivalent to day 42 after the last menstrual period). If maternal folate levels are insufficient during this period, fetal neural tube closure may fail, consequently leading to NTDs [19,20,29].
4.2.3. Timing and Dosage of Folic Acid Supplementation
Overall, balanced diets, appropriate use of folic acid supplements, and food fortification are effective means to improve folate nutritional status [30]. Even when selecting folic acid supplements or fortified foods, a balanced diet should remain the foundation. Folate metabolism in the body is influenced by multiple factors. When developing a folic acid supplementation plan (including dosage, timing, type, etc.), it is necessary to consider factors such as genetics (MTHFR C677T genotype), physiological state (age, gender), disease, medication use, lifestyle (folate intake from diet, alcohol consumption), and the status of other related nutrients to achieve personalized supplementation [30].
Women without high-risk factors who are planning or may become pregnant should begin daily intake of folate-rich foods and supplementation with 0.4 mg of folic acid at least three months before anticipated conception and continue through the first trimester of pregnancy. For the second and third trimesters and during lactation, the recommended folic acid supplement dose is 0.4 mg/day [19,20,22,25,26,30,31,32,33,34,35]. Given that many pregnancies are unplanned, many individuals may be unaware of their pregnancy during the critical period. To fully benefit from supplementation, daily folic acid supplementation is recommended for all women of childbearing potential.
Women in the moderate-risk group require consumption of folate-rich foods and daily oral supplementation with a multivitamin containing 1.0 mg folic acid. This regimen should be initiated at least three months prior to conception and continued until the 12th week of pregnancy. For the second and third trimesters and during lactation, the recommended supplemental folic acid dose is 0.4 mg/day [19,26,30].
This group is defined by the following personal or comorbid conditions (1 to 5), or whose male partners have the following personal conditions (1 and 2): (1) Personal or family history of other folate-sensitive congenital malformations (limited to specific anomalies such as cardiac, limb, cleft palate, urinary tract, and congenital hydrocephalus); (2) Family history of NTDs in first- or second-degree relatives; (3) Pre-gestational diabetes (type 1 or 2) with associated fetal teratogenic risk. Measuring red blood cell folate levels may be part of preconception assessment to determine multivitamin and folic acid supplement dosing strategies (1.0 mg folic acid supplement when RBC folate < 906 ng/mL; 0.4 to 0.6 mg folic acid supplement when RBC folate > 906 ng/mL), in conjunction with a multivitamin; (4) Use of medications with antifolate and teratogenic effects. These include certain anticonvulsants (e.g., carbamazepine, valproic acid, phenytoin sodium, primidone, phenobarbital), metformin, methotrexate, sulfasalazine, trimethoprim (a component of co-trimoxazole), and cholestyramine; (5) Maternal gastrointestinal malabsorption secondary to specific medical or surgical conditions that are proven to cause reduced red blood cell folate levels (e.g., Crohn’s disease or active celiac disease, gastric bypass surgery, advanced liver disease, renal dialysis, excessive alcohol consumption).
High-risk groups, including women with a personal history of NTDs or a previous NTD-affected pregnancy and their male partners who have a personal history of an NTD, should consume folate-rich foods and begin taking a daily supplement of 4.0 mg of folic acid (or 5.0 mg, as 4 mg formulations are unavailable in China) at least one month before conception and continue until the 12th week of pregnancy. Additionally, from 12 weeks of pregnancy onwards, continue daily supplementation with a multivitamin containing 0.4 to 1.0 mg of folic acid throughout the entire pregnancy and for 4 to 6 weeks postpartum or until breastfeeding ceases [19,20,21,26,30,32,33].
Personalized supplementation may be considered for specific circumstances, such as residence in northern regions (especially rural northern areas), low dietary intake of fresh vegetables and fruits, low blood folate levels, the TT genotype at the DMTHFR 677 locus, or short preconception planning periods. In such cases, supplement dosage may be increased or preconception supplementation duration extended as appropriate [19,30]. For women with hyperhomocysteinemia, daily supplementation of at least 5 mg folic acid is recommended until blood homocysteine levels normalize before considering conception. This 5 mg daily supplementation should continue until the end of the third month of pregnancy. During the second and third trimesters and throughout lactation, the recommended folic acid supplementation dose is 0.4 mg/day.
Additionally, women should be advised against obtaining high-dose folic acid supplementation through multivitamin supplements, as this may lead to harmful levels of other vitamins, such as vitamin A, which is teratogenic. Prenatal vitamins taken once daily combined with 1mg folic acid tablets taken three times daily provide a total daily folic acid intake of 4 mg. Taking three 1mg folic acid tablets/capsules at once is more convenient [29]. Regarding folic acid safety, the tolerable upper intake level (UL) for adults is generally 1 mg. Preventive supplementation of 4 mg for women at high risk of NTD pregnancy is typically considered non-toxic in the short term. However, the dose should be reduced after early pregnancy, as it no longer serves to prevent NTDs at this stage. Furthermore, the possibility of adverse effects on the fetus from long-term high-dose exposure cannot be definitively ruled out [29].
4.2.4. The Relationship Between Dietary Folate and Folic Acid Supplements
Dietary intake alone cannot meet requirements, making folic acid tablet supplements necessary. The human body cannot synthesize folate and must obtain it from food, while the increased demands during pregnancy and fetal development further elevate requirements. Although folate in natural foods is relatively safe, its structure is unstable (easily destroyed during food processing) and its bioavailability is low, reaching only about 60% of synthetic folic acid. Absorption and utilization in the body are further affected by factors such as medications, alcohol, and deficiencies in other nutrients. Even for the general population, achieving adequate folate intake presents challenges. Particularly for high-risk groups prone to folate deficiency, such as populations in northern China, impoverished rural areas, winter/spring seasons, pregnant/lactating women, individuals on long-term folate-antagonistic medications, heavy drinkers, those with certain diseases, or those with folate metabolism gene variants, additional folic acid supplementation is recommended to address deficiency/insufficiency [26,30]. Dietary folate sources include asparagus, spinach, broccoli, soybeans, citrus fruits, dried fruits, beef liver, leafy greens, legumes, avocados, eggs, dairy products, barley, tofu skin, dried bean curd sticks, walnuts, garlic sprouts, peanuts, rapeseed, fennel, red amaranth, chrysanthemum greens, chicken eggs, and duck eggs [19,29,30].
4.2.5. Folate-Related Testing
Routine folate metabolism testing is generally not recommended, nor is MTHFR polymorphism testing, as daily supplementation with 0.4 mg of folic acid effectively increases folate concentrations in red blood cells regardless of test results [24,29]. Additionally, routine monitoring folate levels is unnecessary for reproductive-age women supplementing with folate [29]. However, if folate deficiency arises not from dietary insufficiency but from known comorbidities (e.g., inflammatory bowel disease or bariatric surgery), monthly serum folate monitoring is warranted to ensure adequate supplementation (serum folate levels of 28-30 nmol/L) [29].
4.3. Strengths and Limitations of This Study
This study possesses several key strengths: (1) Comprehensive and systematic approach: Focusing on folic acid supplementation for preventing neural tube defects in women of childbearing age, this work systematically integrated clinical guidelines and expert consensus to construct a structured, actionable summary of the best available evidence. It comprehensively retrieved and synthesized guidelines, consensus statements, and recommended practices from multiple countries, including China, the United States, the United Kingdom, and Canada, ensuring broad and representative evidence sources. (2) Methodological rigor: The study employed internationally recognized quality assessment tools—AGREE II for guidelines and JBI criteria for expert consensus documents—with high inter-rater reliability (ICC > 0.75). Evidence extraction and synthesis were performed independently by two reviewers and reviewed by experts, ensuring methodological standardization and result reliability. (3) High-quality, and well-structured evidence output: A total of 17 high-quality publications were included, among which 10 were high-quality clinical guidelines. The 14 evidence statements were clearly graded using the JBI evidence grading system and organized into five thematic dimensions, facilitating efficient comprehension and application by clinicians and public health practitioners. (4) Strong clinical relevance and guidance value: The evidence summary not only distinguishes supplementation regimens for low-, medium-, and high-risk populations but also explicitly recommends against routine folate metabolism testing and serum monitoring, thereby helping to avoid unnecessary medical interventions and reflecting an evidence-based, patient-centered approach.
This study also has several limitations: (1) Language restriction: Only guidelines and consensus documents published in Chinese and English were included, which may have led to the omission of relevant high-quality evidence available in other languages. (2) Exclusion of primary research and systematic reviews: To maintain focus on consolidated recommendations and consensus, original studies and systematic reviews were not incorporated. While this strengthens the authority of the recommendations, it may not reflect the most recent research advances or region-specific evidence not yet captured in formal guidelines. (3) Subjective interpretation in quality appraisal: Although reviewers were trained and cross-checked, the evaluation of expert consensus documents relied on researchers’ interpretation of JBI criteria, which may introduce a degree of subjectivity. (4) Lack of implementation context analysis: The study primarily focused on synthesizing the “best evidence” content and did not systematically examine socioeconomic, cultural, or behavioral barriers that may affect adherence to folic acid supplementation. Future work should integrate implementation science approaches to better support the translation of evidence into practice.
5. Conclusions
This study has developed a comprehensive knowledge base regarding folic acid intake for the prevention of neural tube defects (NTDs) in women of childbearing age, providing a scientific foundation for clinical practice through systematic evidence synthesis. We systematically identified 17 high-quality documents, comprising 10 clinical guidelines and 4 expert consensuses. The final synthesis culminated in 14 key evidence statements, organized across five critical dimensions: the risks of NTDs and the role of folic acid; the time window of neural tube closure; the timing and dosage of folic acid supplementation; the relationship between dietary folate and folic acid supplements; and folate-related testing. These consolidated findings offer a robust, evidence-based resource to inform and guide future folic acid supplementation educations and related research initiatives.
Acknowledgments
During the preparation of this manuscript, the authors used DeepSeek for the purposes of language polishing and translation assistance to improve the clarity and readability of the English text. The authors have thoroughly reviewed, scientifically verified, and edited all AI-assisted content, and we take full responsibility for the accuracy and integrity of this publication.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A. Evidence Summary Retrieval Strategy

Table A1.
PubMed Search Strategy.
| No. | Search Expression | Results |
|---|---|---|
| #1 | “Folic Acid”[Mesh] OR “Prenatal Nutritional Physiological Phenomena”[Mesh] OR “Preconception Care”[Mesh] | 48400 |
| #2 | folate[Title/Abstract] OR “folic acid”[Title/Abstract] OR “tetrahydrofolate”[Title/Abstract] OR “vitamin B9”[Title/Abstract] OR “THF”[Title/Abstract] OR “Pregnancy Nutrition”[Title/Abstract] OR “Preconception Care”[Title/Abstract] | 67036 |
| #3 | #1 OR #2 | 87295 |
| #4 | “Neural Tube Defects”[Mesh] | 31855 |
| #5 | “neural tube defect*”[Title/Abstract] OR “congenital abnormality*”[Title/Abstract] OR anencephaly[Title/Abstract] OR encephalocele[Title/Abstract] OR “spina bifida”[Title/Abstract] OR meningocele[Title/Abstract] OR myelomeningocele[Title/Abstract] | 33847 |
| #6 | #4 OR #5 | 49355 |
| #7 | (((((guidelines as topic[MeSH]) OR guideline[Publication Type]) OR consensus[MeSH]) OR consensus development conferences as topic[MeSH]) OR consensus development conference[Publication Type]) OR standard of care[MeSH] | 255271 |
| #8 | (((((((((guideline*[Title]) OR guidance*[Title]) OR recommendation*[Title]) OR consensus*[Title]) OR “best practice*”[Title]) OR statement*[Title]) OR standard*[Title]) OR “practice parameter*”[Title]) OR “position paper”[Title]) OR “position stand”[Title] | 363818 |
| #9 | #7 OR #8 | 505414 |
| #10 | #3 AND #6 AND #9 | 163 |
| #11 | #10 Filters: from 2013 - 2025 | 54 |
Table A2.
Embase Search Strategy.
| No. | Search Expression | Results |
|---|---|---|
| #1 | (‘maternal nutrition’/exp OR ‘maternal nutrition’) AND [embase]/lim | 15034 |
| #2 | (‘prepregnancy care’/exp OR ‘prepregnancy care’) AND [embase]/lim | 3430 |
| #3 | (‘folic acid’/exp OR ‘folic acid’) AND [embase]/lim | 84215 |
| #4 | #1 OR #2 OR #3 | 100271 |
| #5 | (folate:ab,ti OR ‘folic acid’:ab,ti OR ‘tetrahydrofolate’:ab,ti OR ‘vitamin b9’:ab,ti OR ‘thf’:ab,ti OR ‘pregnancy nutrition’:ab,ti OR ‘preconception care’:ab,ti) AND [embase]/lim | 68114 |
| #6 | #4 OR #5 | 118093 |
| #7 | ‘neural tube defect’/exp | 46554 |
| #8 | (‘neural tube defect*’:ab,ti OR ‘congenital abnormality*’:ab,ti OR anencephaly:ab,ti OR encephalocele:ab,ti OR ‘spina bifida’:ab,ti OR meningocele:ab,ti OR myelomeningocele:ab,ti) AND [embase]/lim | 34767 |
| #9 | #7 OR #8 | 60082 |
| #10 | (‘guideline*’:ti OR ‘guidance*’:ti OR ‘recommendation*’:ti OR ‘consensus*’:ti OR ‘best practice*’:ti OR ‘statement*’:ti OR ‘standard*’:ti OR ‘practice parameter*’:ti OR ‘position paper’:ti OR ‘position stand’:ti) AND [embase]/lim | 352942 |
| #11 | (‘practice guideline’/exp OR ‘practice guideline’) AND [embase]/lim | 713415 |
| #12 | #10 OR #11 | 944239 |
| #13 | #6 AND #9 | 5754 |
| #14 | #12 AND #13 | 276 |
| #15 | #14 AND (2013:py OR 2014:py OR 2015:py OR 2016:py OR 2017:py OR 2018:py OR 2019:py OR 2020:py OR 2021:py OR 2022:py OR 2023:py OR 2024: py OR 2025:py) | 124 |
Table A3.
CINAHL Search Strategy.
| No. | Search Expression | Results |
|---|---|---|
| #1 | MH “Prepregnancy Care” OR MH “Prenatal Nutritional Physiology” OR MH “Folic Acid” | 10646 |
| #2 | Title (folate OR folic acid OR tetrahydrofolate OR vitamin B9 OR THF OR Pregnancy Nutrition OR Preconception Care) OR Abstract (folate OR folic acid OR tetrahydrofolate OR vitamin B9 OR THF OR Pregnancy Nutrition OR Preconception Care) | 12508 |
| #3 | #1 OR #2 | 16525 |
| #4 | MH “Neural Tube Defects” | 2938 |
| #5 | TI (neural tube defect OR congenital abnormalities OR anencephaly OR encephalocele OR spina bifida OR meningocele OR myelomeningocele) OR AB (neural tube defect OR congenital abnormalities OR anencephaly OR encephalocele OR spina bifida OR meningocele OR myelomeningocele) | 7496 |
| #6 | #4 OR #5 | 9030 |
| #7 | MH “Practice Guidelines” OR MH “Consensus” OR PT practice guidelines | 107901 |
| #8 | TI (guideline* OR guidance OR recommendation* OR consensus* OR best practice* OR statement* OR standard* OR practice parameter* OR position paper OR position stand) | 166501 |
| #9 | #7 OR #8 | 231224 |
| #10 | #3 OR #6 | 24175 |
| #11 | #9 AND #10 | 659 |
| #12 | #9 AND #10 (Limiters - Publication Date: 20130101-20250918) | 422 |
Table A4.
Web of Science Search Strategy.
| No. | Search Expression | Results |
|---|---|---|
| #1 | (TI=(“Folic Acid” OR folate OR “tetrahydrofolate” OR “vitamin B9” OR “THF”)) OR AB=(“Folic Acid” OR folate OR “tetrahydrofolate” OR “vitamin B9” OR “THF”) | 128589 |
| #2 | (TI=(“neural tube defect*” OR “congenital abnormality*” OR anencephaly OR encephalocele OR “spina bifida” OR meningocele OR myelomeningocele)) OR AB=(“neural tube defect*” OR “congenital abnormality*” OR anencephaly OR encephalocele OR “spina bifida” OR meningocele OR myelomeningocele) | 41809 |
| #3 | TI=(guideline* OR guidance* OR recommendation* OR consensus* OR “best practice*” OR statement* OR standard* OR “practice parameter*” OR “position paper” OR “position stand”) | 793798 |
| #4 | #1 AND #2 | 4436 |
| #5 | #3 AND #4 | 97 |
| #6 | #3 AND #4 and 2025 or 2024 or 2023 or 2022 or 2021 or 2019 or 2018 or 2017 or 2016 or 2015 or 2014 or 2013 (Publication Years) | 36 |
Table A5.
CNKI Search Strategy.
| No. | Search Expression | Results |
|---|---|---|
| #1 | (Title: “Prenatal Nutrition” + “Prenatal Care” + “Folic Acid” + “Vitamin B9” (exact)) OR (Abstract: “Prenatal Nutrition” + “Prenatal Care” + “Folic Acid” + “Vitamin B9” (exact)) | 29792 |
| #2 | (Title: “Birth Defects” + “Neural Tube Defects” + “Neural Tube Malformations” + “Neural Tube Defect Syndrome” (exact)) OR (Abstract: “Birth Defects” + “Neural Tube Defects” + “Neural Tube Malformations” + “Neural Tube Defect Syndrome” (exact)) | 15784 |
| #3 | (Title: “Guidelines” + “Consensus” + “Evidence” + “Standards” + “Recommendations” + “Draft” + “Norms” + “Statements” (exact)) | 1249959 |
| #4 | #1 AND #2 AND #3 | 11 |
Note: Timeframe limited to January 1, 2013 – September 18, 2025.
Table A6.
Wanfang Search Strategy.
| No. | Search Expression | Results |
|---|---|---|
| #1 | ((Title or Keywords: (“Birth Defects” or “Neural Tube Defects” or “Neural Tube Malformations” or “Neural Tube Defect Syndrome”) or Abstract: (“ birth defects” or “neural tube defects” or “neural tube malformations” or “neural tube defect syndrome”)) AND (Title or Keywords: (“preconception nutrition” or “preconception care” or “folic acid” or “vitamin B9”) or Abstract: (“ Prenatal Nutrition” or “Prenatal Care” or “Folic Acid” or “Vitamin B9”)) AND (Title:(“Guidelines” or “Consensus” or “Evidence” or “Standards” or “Recommendations” or “Draft”+”Specifications” or “Statements”))) and Publication Date:2013-2025 | 18 |
Table A7.
VIP Search Strategy.
| No. | Search Expression | Results |
|---|---|---|
| #1 | (M=(“birth defects” or “neural tube defects” or “neural tube malformations” or “neural tube defect syndrome”) OR R=(“birth defects” or “neural tube defects” or “neural tube malformations” or “neural tube defect syndrome”)) AND (M=(“Prenatal Nutrition” or “Prenatal Care” or “Folic Acid” or “Vitamin B9”) OR R=(“prenatal nutrition” or “prenatal care” or “folic acid” or “vitamin B9”)) AND (T=(“guidelines” or “consensus” or “evidence” or “standards” or “recommendations” or “draft”+”specifications” or “statements”)) | 18 |
Note: Time period limited to January 1, 2013 – September 18, 2025.
Table A8.
Search Strategy for Guidelines, Expert Consensus, Recommended Practices, and Best Practices.
Table A8.
Search Strategy for Guidelines, Expert Consensus, Recommended Practices, and Best Practices.
| Search Terms | Database | Results |
|---|---|---|
| “Folic Acid”/folate/”tetrahydrofolate”/”vitamin B9”/folacin/”Preconception Care”/”Pregnancy Nutrition”, “neural tube defect”/anencephaly/encephalocele/”spina bifida”/meningocele/myelomeningocele | GIN (Guidelines Network) | 19 |
| NICE* (Guidelines Network) | 61 | |
| SIGN (Guidelines Network) | 23 | |
| CMA (Guidelines Network) | 5 | |
| NZGG** (Guide Network) | 2 | |
| ACOG | 23 | |
| ACMG | 2 | |
| FIGO | 7 | |
| SOGC | 13 | |
| UpToDate | 1 | |
| “Folic Acid”/”Vitamin B9”/”Preconception Care”/”Preconception Nutrition”/”Neural Tube Defects”/”Neural Tube Malformations”/”Anencephaly” | Medlive (Guidelines Network) | 1 |
*Check “guidance” “NICE advice”. **Take the results under “Guides and standards”.
References
- Blencowe, H.; Kancherla, V.; Moorthie, S.; Darlison, M.W.; Modell, B. Estimates of global and regional prevalence of neural tube defects for 2015: a systematic analysis. Ann N Y Acad Sci 2018, 1414, 31-46. [CrossRef]
- Zhang ZP, L.J. Research progress on the relationship between miRNA and MAPKs signaling pathways and neural tube defects [miRNA和MAPKs信号传导通路与神经管缺陷关系的研究进展]. Journal of Shanxi Medical University 2014, 45, 776-780. [CrossRef]
- Kancherla, V.; Black, R.E. Historical perspective on folic acid and challenges in estimating global prevalence of neural tube defects. Annals of the New York Academy of Sciences 2018, 1414, 20-30. [CrossRef]
- De-Regil, L.M.; Peña-Rosas, J.P.; Fernández-Gaxiola, A.C.; Rayco-Solon, P. Effects and safety of periconceptional oral folate supplementation for preventing birth defects. Cochrane Database Syst Rev 2015, 2015, Cd007950. [CrossRef]
- Toivonen, K.I.; Lacroix, E.; Flynn, M.; Ronksley, P.E.; Oinonen, K.A.; Metcalfe, A.; Campbell, T.S. Folic acid supplementation during the preconception period: A systematic review and meta-analysis. Prev Med 2018, 114, 1-17. [CrossRef]
- Xing, X.Y.; Tao, F.B.; Hao, J.H.; Huang, K.; Huang, Z.H.; Zhu, X.M.; Xiao, L.M.; Cheng, D.J.; Su, P.Y.; Zhu, P., et al. Periconceptional folic acid supplementation among women attending antenatal clinic in Anhui, China: data from a population-based cohort study. Midwifery 2012, 28, 291-297. [CrossRef]
- Kim, M.J.; Kim, J.; Hwang, E.J.; Song, Y.; Kim, H.; Hyun, T. Awareness, knowledge, and use of folic acid among non-pregnant Korean women of childbearing age. Nutr Res Pract 2018, 12, 78-84. [CrossRef]
- Sabi, E.M.; Mujamammi, A.H.; Alturki, N.; Alzaid, T.; Almutairi, A.; Algarni, R.; Almaziad, D.; Alhumaidhi, N.; Kurdee, Z.; Sumaily, K.M. Level of Knowledge and Awareness of Female Undergraduate Students and Determinants of Knowledge of Folic Acid and Supplementation. Medicina (Kaunas) 2022, 58. [CrossRef]
- Zeng, Z.; Yuan, P.; Wang, Y.; Ma, X.; Zhu, J. Folic acid awareness and intake among women in areas with high prevalence of neural tube defects in China: a cross-sectional study. Public Health Nutr 2011, 14, 1142-1147. [CrossRef]
- Wei, H. Research on the Integration of Infection Control and Health Education within Healthcare Institutions. MEDS Public Health and Preventive Medicine 2023, 3. [CrossRef]
- MA H P, H.Z.Y., CHANG Z,et al. Quality assessment of guidelines forvascular cognitive impairment using the AGREE Ⅱ [血管性认知障碍指南质量评价]. Chinese General Practice 2022, 25, 1039-1046. [CrossRef]
- Neurogenetic and Developmental Disorders Section of the China Chapter of the International Neurorestoration Society; Wang LL; Fan YJ; Wang XQ; Li SL; Yu YG, B.D.P.a.M.G.B.o.t.C.M.a.C.H.A.P.G.G.o.t.M.G.P.B.o.t.C.M.D.A. Multidisciplinary expert consensus on the prevention,screening,diagnosis,counseling and intervention of neural tube defects [神经管缺陷预防、筛查、诊断、咨询及干预多学科专家共识]. Journal of Clinical Pediatrics 2025, 43.
- Jing F, H.M., Hu Y. Quality evaluation of children′s medication safety guidelines based on AGREE Ⅱ [基于AGREE Ⅱ的儿童用药安全指南质量评价]. Evidence-Based Nursing 2022, 8, 718-725.
- Zhao C, W.X., Han CY, et al. Quality Evaluation of Evidence-based Guidelines for Pain Assessment in Patients with Total Hip Arthroplasty [全髋关节置换患者疼痛评估循证指南质量评价]. Journal of Nursing 2020, 27, 31-37. [CrossRef]
- Shang MH, C.P., Feng D, et al. Quality evaluation and content analysis of fatigue-related management guidelines for cancer patients [癌症患者疲乏相关性管理指南的质量评价及内容分析]. Chongqing Medical Journal 2023, 52, 913-918.
- Yang QM, L.J. Intraclass correlation coefficient: definitions, estimation and applications [组内相关系数:定义辨析、估计方法与实际应用]. Journal of Zhejiang University(Science Edition) 2013, 40, 509-515. [CrossRef]
- JBI. Chapter 4: Systematic reviews of text and opinion. Availabe online: https://jbi-global-wiki.refined.site/space/MANUAL/3283911274/Appendix+4.2%3A+Explanation+of+Text+and+Expert+Opinion+critical+appraisal+tool (accessed on.
- Yan LJ, Q.C., Li XJ, et al. The exploration of evidence synthesis methodology in development of evidence-based clinical protocol [临床实践方案制定中不同级别证据综合的方法学探讨]. Chinese Journal of Evidence-Bases Cardiovascular Medicine 2020, 12, 1039-1042. [CrossRef]
- Ren AG, Z.X., Liu HS, et al. Guideline for prevention of neural tube defects by periconceptional folic acid.
- supplementation (2017) [围受孕期增补叶酸预防神经管缺陷指南(2017)]. In Proceedings of Inaugural Conference of the Southwest China & Sichuan Provincial TCM Gynecology (Obstetrics) Specialty Alliance, 成都; pp. 311-318.
- Practice Bulletin No. 187: Neural Tube Defects. Obstet Gynecol 2017, 130, e279-e290. [CrossRef]
- Scottish Intercollegiate Guidelines, N. Diagnosis and management of epilepsy in adults: A national clinical guideline; SIGN: Edinburgh, Scotland, 2015.
- National Collaborating Centre for, W.s.; Children’s, H. National Institute for Health and Clinical Excellence: Guidance. In Fertility: Assessment and Treatment for People with Fertility Problems, Royal College of Obstetricians & Gynaecologists, National Collaborating Centre for Women’s and Children’s Health.: London, 2013.
- Douglas Wilson, R.; Van Mieghem, T.; Langlois, S.; Church, P. Guideline No. 410: Prevention, Screening, Diagnosis, and Pregnancy Management for Fetal Neural Tube Defects. J Obstet Gynaecol Can 2021, 43, 124-139.e128. [CrossRef]
- Wilson, R.D.; O’Connor, D.L. Guideline No. 427: Folic Acid and Multivitamin Supplementation for Prevention of Folic Acid-Sensitive Congenital Anomalies. J Obstet Gynaecol Can 2022, 44, 707-719.e701. [CrossRef]
- National Institute for, H.; Care, E. Maternal and child nutrition. 2014.
- Wilson, R.D.; Wilson, R.D.; Audibert, F.; Brock, J.A.; Carroll, J.; Cartier, L.; Gagnon, A.; Johnson, J.A.; Langlois, S.; Murphy-Kaulbeck, L., et al. Pre-conception Folic Acid and Multivitamin Supplementation for the Primary and Secondary Prevention of Neural Tube Defects and Other Folic Acid-Sensitive Congenital Anomalies. J Obstet Gynaecol Can 2015, 37, 534-552. [CrossRef]
- Obstetrics Subgroup, C.S.o.O.a.G., Chinese Medical Association. Guideline of preconception and prenatal care(2018) [孕前和孕期保健指南(2018)]. Chinese Journal of Obstetrics and Gynecology 2018, 53, 7-13. [CrossRef]
- Wilkes, J. AAFP Releases Position Paper on Preconception care. Am Fam Physician 2016, 94, 508-510.
- Goetzl, L.M.; Wilkins-Haug, L.; Barss, V.A. Preconception and prenatal folic acid supplementation. UpToDate 2024.
- Group, C.M.E.C.W. Chinese multidisciplinary expert consensus on rational.
- clinical folic acid supplementation [中国临床合理补充叶酸多学科专家共识]. Herald of Medicine 2021, 40, 1-19.
- Li L, L.X., Cheng WW, et al. Expert consensus on preconception care(2023) [备孕保健专家共识 (2023)]. Chinese Journal of Birth Health & Heredity 2023, 31, 1737-1743. [CrossRef]
- Ogunwole, S.M.; Chen, X.; Mitta, S.; Minhas, A.; Sharma, G.; Zakaria, S.; Vaught, A.J.; Toth-Manikowski, S.M.; Smith, G. Interconception Care for Primary Care Providers: Consensus Recommendations on Preconception and Postpartum Management of Reproductive-Age Patients With Medical Comorbidities. Mayo Clin Proc Innov Qual Outcomes 2021, 5, 872-890. [CrossRef]
- ACOG Committee Opinion No. 762: Prepregnancy Counseling. Obstet Gynecol 2019, 133, e78-e89. [CrossRef]
- Barry, M.J.; Nicholson, W.K.; Silverstein, M.; Chelmow, D.; Coker, T.R.; Davis, E.M.; Donahue, K.E.; Jaén, C.R.; Li, L.; Ogedegbe, G., et al. Folic Acid Supplementation to Prevent Neural Tube Defects: US Preventive Services Task Force Reaffirmation Recommendation Statement. Jama 2023, 330, 454-459. [CrossRef]
- Good clinical practice advice: Micronutrients in the periconceptional period and pregnancy. Int J Gynaecol Obstet 2019, 144, 317-321. [CrossRef]
- Wang CQ, H.Y. JBI evidence pre-classification and evidence rank system (2014 Edition) [JBI证据预分级及证据推荐级别系统(2014版)]. Journal of Nurses Training 2015, 30, 964-967. [CrossRef]
Figure 1.
The literature searching flowchart.
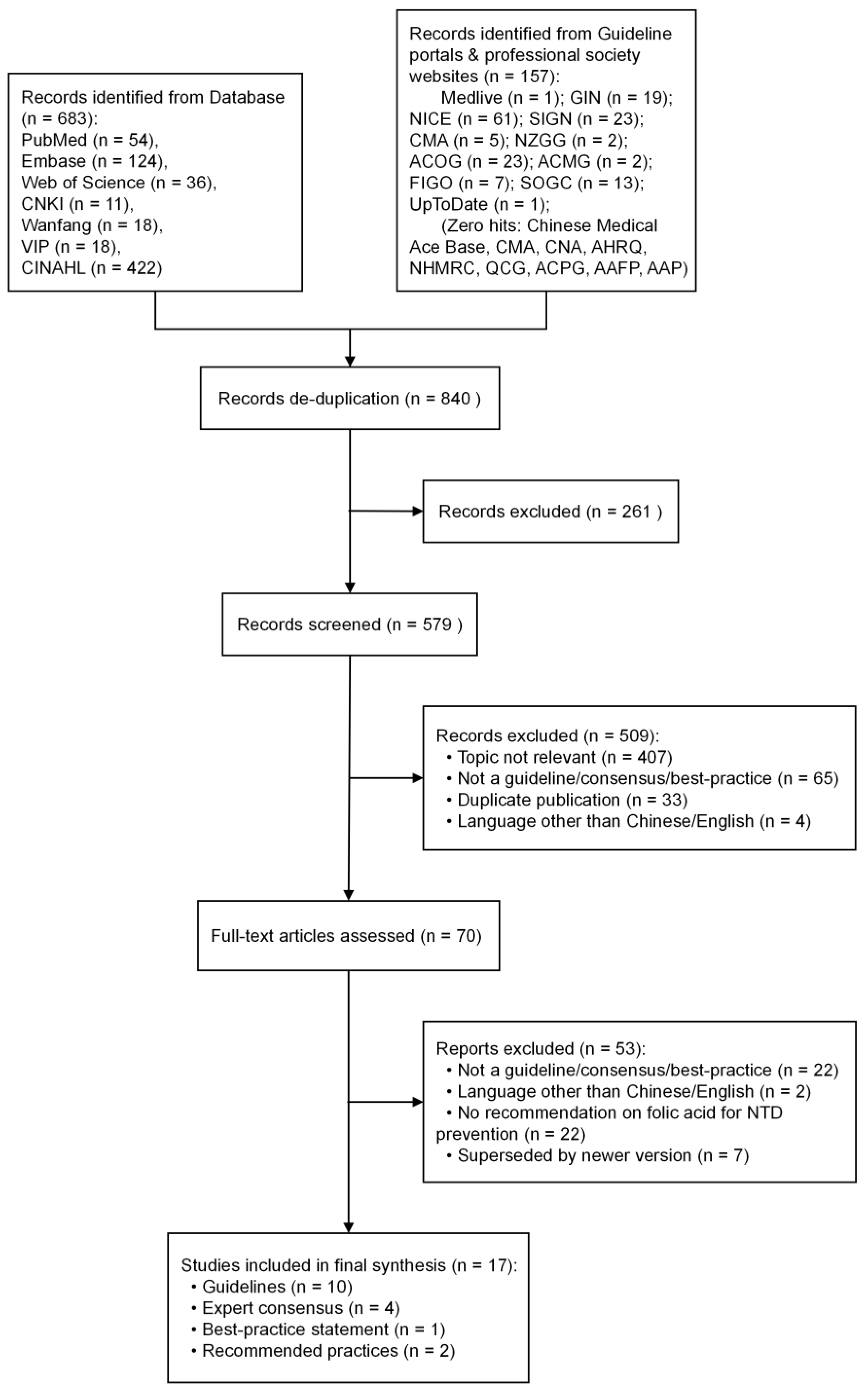
Table 1.
Basic characteristics of the included literature (n = 14).
| No. | Literature Title | Publication/Update Year | Author/ Publishing Organization | Literature Type | Country |
|---|---|---|---|---|---|
| 1 | Guideline for the Prevention of Neural Tube Defects by Periconceptional Folic Acid Supplementation (2017) [19] | 2017 | Periconceptional Folic Acid Supplementation to Prevent NTDs Guideline Working Group | Guideline | China |
| 2 | Neural Tube Defects [20] | 2017 | ACOG | Guideline | USA |
| 3 | Diagnosis and management of epilepsy in adults [21] | 2015 | SIGN | Guideline | UK |
| 4 | Fertility: assessment and treatment for people with fertility problems [22] | 2013 | NICE | Guideline | UK |
| 5 | Guideline No. 410: Prevention, Screening, Diagnosis, and Pregnancy Management for Fetal Neural Tube Defects [23] | 2021 | SOGC | Guideline | Canada |
| 6 | Guideline No. 427: Folic Acid and Multivitamin Supplementation for Prevention of Folic Acid Sensitive Congenital Anomalies [24] | 2022 | SOGC | Guideline | Canada |
| 7 | Maternal and child nutrition [25] | 2014 | NICE | Guideline | UK |
| 8 | Pre-conception Folic Acid and Multivitamin Supplementation for the Primary and Secondary Prevention of Neural Tube Defects and Other Folic Acid-Sensitive Congenital Anomalies [26] | 2015 | SOGC | Guideline | Canada |
| 9 | Guideline of preconception and prenatal care(2018) [27] | 2018 | Obstetrics Subgroup, Chinese Society of Obstetrics and Gynecology, Chinese Medical Association | Guideline | China |
| 10 | AAFP Releases Position Paper on Preconception Care [28] | 2016 | AAFP | Guideline | USA |
| 11 | Preconception and prenatal folic acid supplementation [29] | 2024 | Laura M Goetzl, et al. | Best Practice | USA |
| 12 | Chinese Multidisciplinary Expert Consensus on Rational Clinical Folic Acid Supplementation [30] | 2021 | Chinese Multidisciplinary Expert Consensus Writing Group on Folic Acid | Expert Consensus | China |
| 13 | Expert consensus on preconception care(2023) [31] | 2023 | Li, Li, et al. | Expert Consensus | China |
| 14 | Interconception Care for Primary Care Providers: Consensus Recommendations on Preconception and Postpartum Management of Reproductive-Age Patients with Medical Comorbidities [32] | 2021 | S. Michelle Ogunwole, et al. | Expert Consensus | USA |
| 15 | Prepregnancy Counseling [33] | 2019 | ACOG | Expert Consensus | USA |
| 16 | Folic Acid Supplementation to Prevent Neural Tube Defects US Preventive Services Task Force Reaffirmation Recommendation Statement [34] | 2023 | US Preventive Services Task Force | Recommended Practice | USA |
| 17 | Good clinical practice advice: Micronutrients in the periconceptional period and pregnancy [35] | 2019 | FIGO | Recommended Practice | Global |
Table 2.
Results of quality evaluation of included guidelines.
| No. | Percentage of Standardized Domains (%) | Domains with > 60% (number) | Domains with < 30% (number) |
ICC | Level | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Scope and Purpose | Stakeholder Involvement | Rigor | Clarity | Applicability | Independence | |||||
| 1 [19] | 69.44 | 66.67 | 30.21 | 94.44 | 37.50 | 8.33 | 3 | 2 | 0.908 | B |
| 2 [20] | 72.22 | 33.33 | 45.83 | 86.11 | 39.58 | 8.33 | 2 | 1 | 0.880 | B |
| 3 [21] | 80.56 | 75.00 | 76.04 | 91.67 | 95.83 | 100.00 | 6 | 0 | 0.879 | A |
| 4 [22] | 88.89 | 83.33 | 94.79 | 100.00 | 95.83 | 100.00 | 6 | 0 | 0.773 | A |
| 5 [23] | 94.44 | 66.67 | 56.25 | 94.44 | 54.17 | 83.33 | 4 | 0 | 0.973 | B |
| 6 [24] | 94.44 | 69.44 | 55.21 | 94.44 | 54.17 | 83.33 | 4 | 0 | 0.775 | B |
| 7 [25] | 88.89 | 86.11 | 96.88 | 100.00 | 95.83 | 100.00 | 6 | 0 | 0.815 | A |
| 8 [26] | 94.44 | 66.67 | 56.25 | 94.44 | 54.17 | 83.33 | 4 | 0 | 0.832 | B |
| 9 [27] | 80.56 | 61.11 | 10.42 | 66.67 | 27.08 | 8.33 | 3 | 3 | 0.798 | C |
| 10 [28] | 58.33 | 25.00 | 0.00 | 69.44 | 35.42 | 8.33 | 1 | 3 | 0.845 | C |
Table 3.
Results of quality evaluation of expert consensus, best practices, and recommended practices.
Table 3.
Results of quality evaluation of expert consensus, best practices, and recommended practices.
| No. | Item 1 1 | Item 2 2 | Item 3 3 | Item 4 4 | Item 5 5 | Item 6 6 | Inclusion |
|---|---|---|---|---|---|---|---|
| 11 [29] | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 12 [30] | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 13 [31] | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 14 [32] | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 15 [33] | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 16 [34] | Yes | Yes | Yes | Yes | Yes | No | Yes |
| 17 [35] | Yes | Yes | Yes | Yes | Yes | No | Yes |
1 Item 1: Is the source of the viewpoint clearly indicated? 2 Item 2: Does the viewpoint originate from influential experts in the field? 3 Item 3: Is the proposed viewpoint centered on the interests of the relevant population? 4 Item 4: Is the stated conclusion based on the results of the analysis? Is the expression of the viewpoint logical? 5 Item 5: Are other existing literature references consulted? 6 Item 6: Are there inconsistencies between the proposed viewpoint and previous literature?
Table 4.
Summary of the best evidence of folic acid supplementation for prevention of neural tube defects in women of childbearing age.
Table 4.
Summary of the best evidence of folic acid supplementation for prevention of neural tube defects in women of childbearing age.
| Category | Evidence Content | Evidence Level (Grade) |
|---|---|---|
| 1. Risks of Neural Tube Defects and the Role of Folic Acid | 1.1 Risks of Neural Tube Defects [19,34] | 5 |
| 1.2 The Role of Folic Acid in Preventing Neural Tube Defects [19,20,29] | 1 | |
| 2. Timing Window for Neural Tube Closure | 2.1 Timing of Neural Tube Closure and Significance of Preconception Folic Acid Intake [19,20,23,29,34] | 5 |
| 3. Timing and Dosage of Folic Acid Supplementation | 3.1 Balanced Diet, Rational Use of Folic Acid Supplements, and Food Fortification Are Effective Means to Improve Folic Acid Nutritional Status [30] | 5 |
| 3.2 Women without high-risk factors who are planning pregnancy or may become pregnant should begin daily intake of folate-rich foods and supplements containing 0.4 mg of folic acid at least three months before anticipated conception. This should continue until the end of the first trimester. For the second and third trimesters and during lactation, the recommended supplemental folate dose is 0.4 mg/day [19,20,22,25,26,30,31,32,33,34,35]. | 1 | |
| 3.3 Women in the moderate-risk group should consume folate-rich foods and take a daily multivitamin supplement containing 1.0 mg of folic acid, starting at least three months before conception. This regimen should be continued until 12 weeks of pregnancy. For the second and third trimesters and during lactation, the recommended supplemental folic acid dose is 0.4 mg/day [19,26,30]. | 1 | |
| 3.4 High-risk groups should consume folate-rich foods and begin daily supplementation with 4.0 mg of folic acid at least one month before conception, continuing through the 12th week of pregnancy. Since 4 mg formulations are unavailable domestically but 5 mg formulations exist, daily supplementation with 5 mg of folic acid is also acceptable. From 12 weeks of pregnancy onwards, continue daily supplementation with a multivitamin containing 0.4 to 1.0 mg of folic acid throughout the entire pregnancy and for 4 to 6 weeks postpartum or until breastfeeding ceases [19,20,21,26,30,32,33]. | 1 | |
| 3.5 Personalized supplementation: In special circumstances, supplement dosage may be increased or preconception supplementation duration extended as appropriate [19,30]. | 3 | |
| 3.6 Do not obtain high-dose folic acid supplementation through multivitamin intake [29]. | 5 | |
| 3.7 The tolerable upper intake level for folic acid in adults is generally 1 mg. A 4 mg prophylactic dose for women at high risk of NTD pregnancies is typically considered non-toxic in the short term [29]. | 5 | |
| 4. Relationship between dietary folate and folic acid tablets | 4.1 Dietary folate sources include asparagus, spinach, broccoli, soybeans, citrus fruits, dried fruits, beef liver, leafy greens, legumes, avocados, eggs, dairy products, barley, tofu skin, dried bean curd sticks, walnuts, garlic sprouts, peanuts, rapeseed, fennel, red amaranth, chrysanthemum greens, chicken eggs, and duck eggs [19,29,30]. | 1 |
| 4.2 Dietary intake alone is insufficient; folic acid supplementation is necessary [26,30]. | 2 | |
| 5. Folate-Related Testing | 5.1 Folic acid metabolism testing is generally not recommended [24,29]. | 1 |
| 5.2 Women of childbearing age taking folic acid supplements do not require monitoring of folate levels [29]. | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



