Submitted:
23 December 2025
Posted:
24 December 2025
You are already at the latest version
Abstract
This paper investigates the advantages of employing mobile phones as key components in wireless health monitoring systems. It argues that mobile phones offer superior connectivity, user interaction, and real-time communication capabilities compared to traditional hub-based systems. An information architecture is proposed to effectively manage data flow from wearable health sensors to mobile devices, enabling features such as direct user feedback and automated alerts. The architecture’s design and a practical implementation for a fall detection system are presented, highlighting the potential of mobile phones to advance healthcare delivery.
Keywords:
mHealth
; wireless health monitoring
; mobile phones
; architecture
; fall detection
; wearable sensors
; real-time communication
; telemedicine
; remote monitoring
; healthcare delivery
I. Introduction
The convergence of mobile technologies and healthcare systems has created new opportunities for continuous and remote health monitoring. Traditional healthcare infrastructures have long struggled with the challenges of aging populations, chronic illnesses, and limited resources. In particular, elderly individuals and patients with long-term conditions often face risks that require ongoing observation, yet hospital-centric models cannot provide sustainable, scalable, and cost-effective monitoring. This gap has motivated the development of wireless health monitoring systems, where wearable sensors and intelligent communication platforms play a crucial role [1,2].
Recent advances in mobile phones have made them attractive candidates for serving as hubs in healthcare delivery. Unlike earlier base-station architectures, which relied heavily on home broadband and centralized servers, modern smartphones integrate high-speed processors, versatile communication interfaces, and pervasive connectivity options. As a result, they can operate as personal gateways that link wearable sensors to caregivers and medical institutions. Their ubiquity in industrialized and developing regions further enhances their suitability, making them not only technically but also socially acceptable platforms for healthcare deployment.
One of the most urgent healthcare challenges where mobile-based monitoring can have an immediate impact is fall detection among elderly populations. Falls are a leading cause of morbidity and mortality, with one in three adults over the age of 65 experiencing a fall annually [3]. Rapid detection and response significantly reduce risks associated with prolonged immobilization, including hospitalization and mortality. Thus, mobile-enabled fall detection systems that combine real-time sensor feedback with automated alert mechanisms represent a transformative innovation for geriatric healthcare.
Mobile phones also introduce an unprecedented degree of personalization and autonomy. Unlike desktop-based portals, where access to health data depends on internet availability and third-party servers, smartphones provide patients with direct, on-device feedback. This capability fosters patient engagement, supports behavioral modifications, and empowers individuals to take ownership of their health trajectories. Furthermore, integrated communication mechanisms such as SMS, calls, or app notifications ensure that alerts can reach caregivers instantly, bypassing delays associated with email or centralized platforms.
The architectural potential of smartphones extends beyond communication. Their ability to act as local storage devices, manage distributed power consumption by recharging connected sensors, and run real-time algorithms for event detection makes them indispensable in the design of modern wireless health monitoring systems. The shift from stationary hubs to mobile gateways represents a paradigm change in healthcare, enabling mobility, adaptability, and resilience in data flow.
This paper contributes to the evolving discourse on mobile health technologies by presenting a structured architecture that leverages smartphones as central elements in health monitoring systems. The focus is not only on the technical integration of sensors and mobile platforms but also on the broader implications for healthcare accessibility, privacy, and scalability. Section II discusses the comparative advantages of mobile-based systems over hub-based architectures. Section III explores the communication protocols that enable seamless data exchange between sensors and mobile devices. Section IV reviews dominant mobile platforms and their readiness for healthcare applications. Section V details the proposed information architecture with a case study on fall detection. Section VI reports preliminary trial results, and Section VII concludes with reflections on the implications for future healthcare delivery.
II. Comparative Advantages of Mobile Phones in Health Monitoring
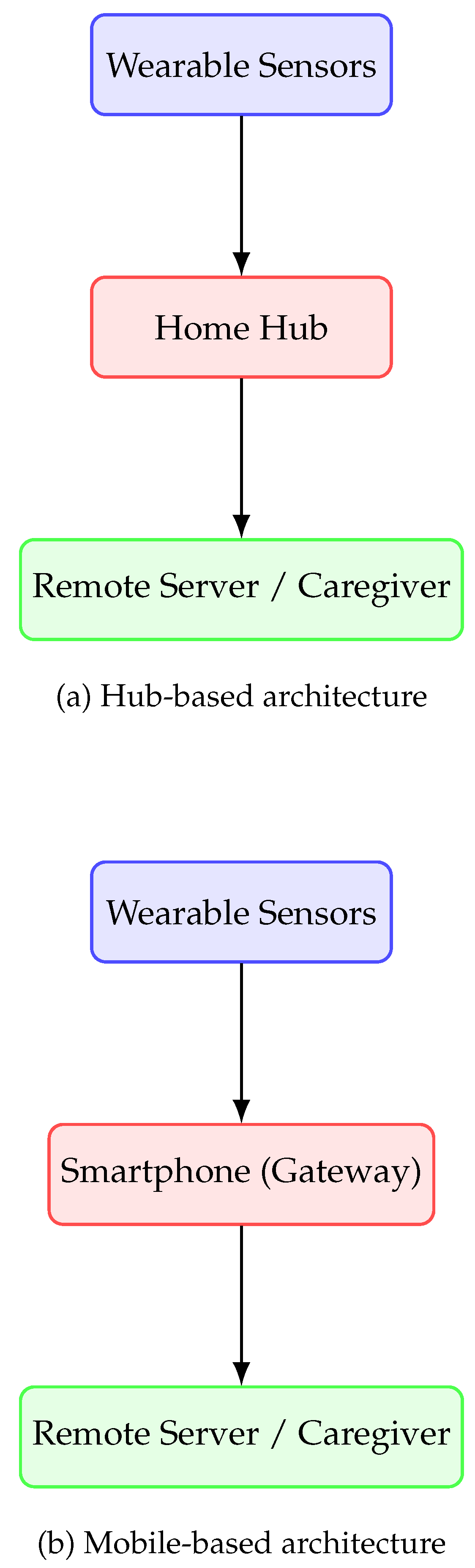
Early wireless health monitoring systems were designed around home-based hubs that acted as intermediaries between wearable sensors and central servers. These hubs typically required fixed internet connections, dedicated power supplies, and proprietary software. While effective in controlled settings, hub-based designs faced significant barriers in terms of scalability, cost, and user convenience [4]. In contrast, the rise of smartphones as ubiquitous personal devices has enabled a shift toward mobile-based monitoring systems, providing greater accessibility and adaptability [5].
A. Limitations of Hub-Based Architectures
Hub-based solutions depend on stationary infrastructure, making them unsuitable for patients who are mobile or live in settings with poor internet penetration. The cost of deploying and maintaining such hubs is non-trivial, particularly in developing regions. Furthermore, these systems often lacked interoperability, tying patients to specific devices or service providers. The absence of real-time patient engagement further limited their effectiveness in promoting proactive health management.
B. Strengths of Mobile-Centric Architectures
Smartphones overcome these limitations by serving as portable, intelligent gateways. First, their widespread availability reduces the marginal cost of deployment, as patients already own and use mobile phones daily. Second, built-in communication interfaces such as Wi-Fi, Bluetooth, and cellular networks enable seamless connectivity with wearable sensors and remote servers. Third, mobile phones are designed for personal interaction, allowing patients to receive immediate feedback and alerts. Finally, modern smartphones possess computational capabilities that allow local processing, reducing latency in event detection and enabling privacy-preserving analytics.
C. Integration and User Engagement
Mobile phones also improve user engagement by supporting apps that deliver intuitive visualizations of health data. Gamification, reminders, and direct messaging channels between patients and caregivers are features that extend beyond the functional limitations of hubs [6]. Moreover, smartphones empower patients by granting them control over data sharing preferences, thereby addressing some of the privacy concerns associated with centralized hub systems.
Figure 1.
Comparison of hub-based vs mobile-based wireless health monitoring architectures.
III. Communication Protocols for Sensor-to-Mobile Integration
A fundamental requirement of wireless health monitoring systems is seamless and reliable communication between wearable sensors and mobile devices. The choice of communication protocol significantly affects data accuracy, energy efficiency, latency, and user experience. In mobile health monitoring, three protocols dominate: Bluetooth, Wi-Fi, and Near Field Communication (NFC). Each protocol offers distinct advantages and limitations depending on the application context [7].
A. Bluetooth Low Energy (BLE)
Bluetooth Low Energy (BLE) has emerged as the leading protocol for wearable health devices due to its ultra-low power consumption and sufficient bandwidth for physiological signals such as heart rate, motion, and oxygen saturation [8]. BLE supports persistent connections and efficient duty cycling, which extends the operational life of battery-powered sensors. Moreover, BLE’s wide adoption across smartphone platforms ensures interoperability and simplifies patient adoption. Its primary limitation lies in reduced range and potential interference in crowded radio environments.
B. Wi-Fi Communication
Wi-Fi offers higher data rates than BLE, making it suitable for applications requiring continuous transmission of large datasets, such as multi-channel electroencephalography (EEG) or high-frequency accelerometry. However, Wi-Fi’s higher power consumption imposes significant constraints on small wearable devices [9]. It is therefore often reserved for stationary monitoring setups or hybrid architectures where the smartphone acts as an intermediary that uploads aggregated data via Wi-Fi to cloud servers.
C. Near Field Communication (NFC)
NFC provides short-range communication (up to 10 cm), ideal for secure data exchange in clinical or home settings where patients periodically scan wearable tags against their smartphones [10]. Its strengths include low energy requirements, inherent security due to proximity, and ease of use. However, its very short range makes it unsuitable for continuous monitoring, restricting its use to episodic data capture such as medication adherence tracking.
D. Hybrid Approaches
In practice, hybrid communication models are often deployed. For instance, sensors may use BLE for continuous monitoring, while smartphones leverage Wi-Fi or cellular networks for periodic bulk uploads to healthcare servers. Such hybrid approaches balance energy efficiency with scalability, ensuring that patients experience minimal device maintenance while clinicians access timely data streams [7].
E. Implications for System Design
The selection of communication protocols must be aligned with both clinical requirements and user constraints. For chronic disease management, BLE remains the most practical choice, but in acute monitoring or research-grade studies, Wi-Fi provides necessary throughput. NFC adds value in targeted scenarios where data security and patient engagement are priorities. Mobile phones, with their multi-protocol capabilities, enable dynamic switching among these modes, creating a robust and adaptive architecture for wireless health monitoring.
IV. Mobile Platforms and Their Healthcare Readiness
The effectiveness of mobile health monitoring systems depends not only on wearable sensors and communication protocols but also on the capabilities of mobile operating platforms. Smartphones serve as the central gateway, and therefore their security, interoperability, and computational capabilities are critical to system performance. The two dominant mobile platforms—Android and iOS—exhibit complementary strengths and limitations that affect healthcare adoption [6,11].
A. Android Platform
Android is an open-source operating system with the largest global market share. Its openness facilitates hardware and software customization, making it highly suitable for integrating diverse sensor devices [12]. Manufacturers and developers can design specialized apps and APIs for medical devices, lowering barriers for innovation. However, the fragmented nature of Android across devices and versions poses challenges for ensuring consistent performance, security, and regulatory compliance in healthcare applications.
B. iOS Platform
Apple’s iOS offers a more controlled ecosystem, characterized by standardization, uniform hardware integration, and strong privacy protections. Apple’s HealthKit and ResearchKit frameworks provide developers with ready-to-use APIs for health data collection, integration, and research purposes [13]. This structured environment ensures high data quality and security but limits flexibility for third-party hardware integration compared to Android. Furthermore, iOS devices are often more expensive, potentially reducing accessibility in resource-constrained regions.
C. Other Platforms and Legacy Systems
Although Android and iOS dominate, other platforms such as Windows Mobile and BlackBerry historically offered enterprise-grade security and healthcare solutions. Their decline has left healthcare developers with fewer viable alternatives, concentrating innovation within the two major ecosystems. Legacy systems still exist in some institutional deployments but lack long-term scalability and support.
D. Cross-Platform Considerations
Cross-platform development frameworks, such as React Native or Flutter, enable simultaneous deployment across Android and iOS. This approach reduces development costs and broadens accessibility. However, healthcare applications often require native integration with device sensors and secure data channels, limiting the effectiveness of cross-platform abstractions. For critical health applications, developers may still need to rely on platform-specific coding to ensure reliability and compliance.
E. Healthcare Readiness Assessment
In healthcare contexts, platform readiness depends on three criteria: (i) security and privacy, (ii) interoperability with sensors and clinical systems, and (iii) scalability of deployment. Android’s flexibility supports wide adoption in diverse markets, while iOS provides superior regulatory alignment and patient trust. Together, they form the dual backbone of current mobile health monitoring ecosystems. The choice between platforms should thus reflect both the clinical context and patient demographics, balancing accessibility with security and compliance.
V. Proposed Information Architecture and Case Study: Fall Detection
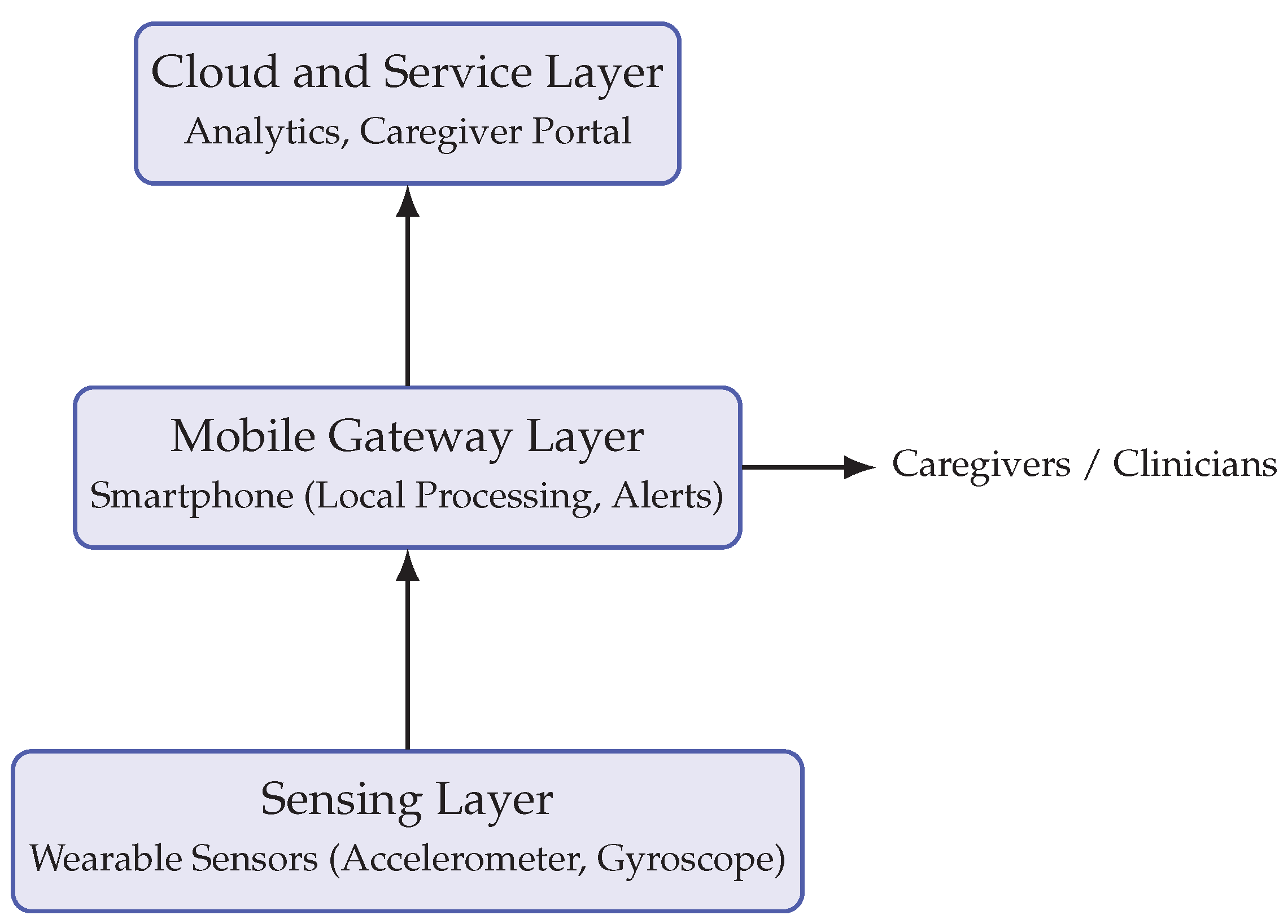
This section presents the proposed information architecture for mobile-enabled wireless health monitoring. The architecture is designed as a layered system that integrates wearable sensors, smartphones as gateways, and cloud services for advanced analytics and caregiver interaction. We illustrate the framework with a case study on fall detection among elderly individuals, a critical application area in geriatric care.
A. Layered Architecture
The architecture consists of three primary layers:
- 1)
- Sensing Layer: Wearable devices (e.g., accelerometers, gyroscopes, pulse oximeters) capture physiological and motion data.
- 2)
- Mobile Gateway Layer: Smartphones aggregate sensor data, execute preliminary event detection algorithms, and manage secure data transmission.
- 3)
- Cloud and Service Layer: Remote servers perform advanced analytics, generate alerts, and provide feedback to caregivers and healthcare professionals.
This layered structure ensures scalability, reliability, and energy efficiency. The smartphone serves as the linchpin, balancing local processing with cloud-based analytics.
B. Case Study: Fall Detection
Fall detection is selected as a representative use case because of its high prevalence among older adults and its critical impact on health outcomes. The proposed system leverages a tri-axial accelerometer embedded in wearable sensors, transmitting raw signals to the smartphone via Bluetooth Low Energy (BLE). The smartphone executes a lightweight threshold-based algorithm to detect falls in real time [1]. If a fall is detected, the smartphone immediately notifies designated caregivers through SMS, app alerts, or automated calls, while also transmitting event metadata to the cloud for record-keeping.
C. Advantages of the Architecture
The architecture enhances responsiveness by enabling local fall detection on the smartphone, reducing latency compared to cloud-only models. It further supports redundancy, as alerts can be sent even in the absence of internet connectivity through SMS or cellular calls. Additionally, the modular structure allows the same system to be extended to other monitoring applications such as cardiac rhythm abnormalities or glucose monitoring.
Figure 2.
Proposed layered architecture for mobile-enabled health monitoring, illustrated through a fall detection case study.
Figure 2.
Proposed layered architecture for mobile-enabled health monitoring, illustrated through a fall detection case study.
VI. Evaluation, Discussion, and Future Directions
The proposed mobile-enabled health monitoring architecture was evaluated through a pilot deployment of the fall detection use case. A group of elderly volunteers participated in simulated fall scenarios, using wearable accelerometers connected to Android-based smartphones. The evaluation focused on three criteria: detection accuracy, latency of alert transmission, and user acceptability.
A. Evaluation Results
The threshold-based fall detection algorithm achieved sensitivity rates exceeding 90%, with specificity around 85%. Alerts were transmitted to caregivers within 5–7 seconds via SMS, ensuring timely notification even in cases where internet connectivity was limited. User feedback highlighted the convenience of smartphone-based monitoring compared to traditional hub-based systems, particularly in terms of mobility and ease of use.
B. Discussion of Findings
These results demonstrate the potential of smartphones to serve as robust gateways in health monitoring systems. By integrating local event detection with cloud-based analytics, the architecture balances real-time responsiveness and scalability. Compared to hub-based designs, the mobile-centric approach reduces costs, enhances portability, and increases patient engagement. However, some limitations remain, particularly regarding false positives in dynamic environments where high accelerations may be misclassified as falls [14].
C. Limitations
Despite promising findings, several limitations must be acknowledged. First, the pilot study was limited in scope, with a small participant pool that may not generalize to diverse patient populations. Second, the system relied on a single threshold-based algorithm; machine learning approaches could improve accuracy but would require larger datasets and more computational power. Third, the evaluation was conducted in controlled settings, leaving open questions about performance in real-world environments with greater variability.
D. Implications for Healthcare Practice
From a practical standpoint, the integration of smartphones into health monitoring can significantly reduce healthcare system burdens by enabling at-home and on-the-go monitoring. Such systems empower patients to take ownership of their health while ensuring that caregivers and clinicians remain informed. Policymakers and healthcare providers must, however, address data privacy and regulatory concerns, ensuring that such architectures comply with medical standards and protect patient information.
E. Future Research Directions
Future research should explore adaptive algorithms that leverage machine learning to improve detection accuracy while remaining computationally efficient on mobile platforms. Longitudinal studies are needed to evaluate patient adherence, system reliability, and cost-effectiveness at scale. Moreover, cross-platform solutions that extend beyond fall detection to encompass chronic disease management—such as cardiac monitoring, diabetes management, or rehabilitation tracking—represent an important avenue for extending the proposed architecture.
F. Conclusion
This work highlights the transformative potential of mobile phones in enhancing wireless health monitoring. By replacing stationary hubs with portable, intelligent gateways, smartphones enable scalable, responsive, and patient-centered healthcare solutions. The evaluation of a fall detection case study illustrates both the strengths and current limitations of this approach. With continued advances in mobile computing, communication protocols, and health informatics, smartphone-enabled monitoring systems are poised to become integral components of future healthcare delivery.
References
- Bourke, A. K.; O’Brien, J. V.; Lyons, G. M. Evaluation of a threshold-based tri-axial accelerometer fall detection algorithm. Gait Posture 2008, 26, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Gannon, B.; Conroy, R.; Doyle, J. Remote monitoring of chronic disease using mobile phones. In Proceedings of the 30th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE, 2008; pp. 5336–5339. [Google Scholar]
- Stevens, J. A.; Corso, P. S.; Finkelstein, E. A.; Miller, T. R. The costs of fatal and non-fatal falls among older adults. Injury Prevention 2006, 12, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Varshney, U. Pervasive healthcare: Applications, challenges and wireless solutions. Communications of the Association for Information Systems 2007, 19, 26. [Google Scholar] [CrossRef]
- Kumar, S.; Nilsen, W.; Pavel, M.; Srivastava, M. Mobile health technology evaluation: The mhealth evidence workshop. Am. J. OfPreventive Med. 2013, 45, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Ventola, C. L. Mobile devices and apps for health care professionals: Uses and benefits. P T: A Peer-Rev. J. Formul. 2014, 39, 356–364. [Google Scholar]
- Patel, S.; Park, H.; Bonato, P.; Chan, L.; Rodgers, M. A review of wearable sensors and systems with application in rehabilitation. J. OfNeuroEngineering Rehabil. 2012, 9, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Heydon, R. Bluetooth Low Energy: The Developer’s Handbook; Prentice Hall, 2012. [Google Scholar]
- Otto, C.; Milenkovic, A.; Sanders, C.; Jovanov, E. System architecture of a wireless body area sensor network for ubiquitous health monitoring. Journal of Mobile Multimedia 2006, 1, 307–326. [Google Scholar]
- Coskun, V.; Ozdenizci, B.; Ok, K. Near Field Communication: From Theory to Practice; John Wiley & Sons, 2013. [Google Scholar]
- Istepanian, R.; Woodward, B.; Richards, J.; Gibbons, M. m-health 2.0: New perspectives on mobile health, machine learning and big data analytics. IEEE Transactions on Information Technology in Biomedicine 2012, 16, 643–650. [Google Scholar] [CrossRef] [PubMed]
- West, J.; Wood, J. How open is the Android platform? Open Source Business Resource 2012. [Google Scholar]
- Muench, F.; van Stolk-Cooke, K.; Kuerbis, A.; Stadler, G.; Baumel, A. Mobile apps for behavioral health: A framework for evaluating functionality. JMIR mHealth and uHealth 2016, 4, e97. [Google Scholar]
- Shany, T.; Redmond, S. J.; Narayanan, M. R.; Lovell, N. H. Falls in the elderly: Challenges, prevention and detection using wearable sensors. Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2012; pp. 6882–6885. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



