Submitted:
22 December 2025
Posted:
23 December 2025
You are already at the latest version
Abstract
Background: Ductoscopic resolution is insufficient to distinguish the flat lesions and microcalcifications that indicate malignancy in patients with pathologic nipple discharge (PND). This study evaluated the feasibility of imaging intraductal epithelial layers, premalignant, or malignant lesions using catheter-integrated optical coherence tomography (OCT) through the nipple orifices.
Methods: Mastectomy specimens were prospectively obtained from patients who had undergone simple or skin-sparing mastectomies for either malignancy (n = 14) or prophylaxis (n = 4). Ductoscopy was used to ensure that the OCT catheter was safely inserted through the nipple orifice of the ex vivo specimens. Cross-sectional OCT scanning of the ductal epithelial layers was performed to acquire high-resolution images of approximately one million pixels. The abnormal lesions identified on the OCT images were evaluated using correlating histopathologic analyses.
Results: Fourteen out of 18 mastectomy specimens could be cannulated and distended using ductoscopic instruments and saline. Only 4 out of 18 specimens had presented with clinical PND. To confirm that the ductoscopic trocars were located inside the ducts, 14 specimens were randomly selected and explored with ductoscopy. The OCT catheter was able to insert through the ductoscopic trocars in 10 specimens and revealed one in situ ductal cancer (DCIS) in a cancer-involved specimen and one florid ductal hyperplasia in a prophylactic specimen. Both lesions were confirmed by histopathological correlations. The OCT scanning did not detect malignant lesions in 80% of the specimens without PND; however, the OCT scanning did detect microcalcifications and undefined lesions.
Conclusion: This is the first published study to confirm the feasibility of intraductal breast OCT to show millimetric Florid Ductal Hyperplasia and a DCIS in a prophylactic and cancer involved specimen, respectively.
Keywords:
optical coherence tomography
; OCT
; ductoscopy
; breast cancer
; nipple discharge
; mastectomy
; near-infrared light
1. Introduction
Pathologic nipple discharge (PND) is defined as a unilateral, spontaneous discharge from a single mammary duct; this condition is associated with a malignancy incidence rate of 1 to 23%.[1,2] Traditional diagnostic methods, such as galactography and ultrasonography, are not optimal for the differential diagnosis of PND. Consequently, new diagnostic tools, such as ductoscopy, have been developed. Although there is no consensus regarding the diagnostic protocols for PND patients, surgeries involving selective duct excision (microductectomy), with or without ductoscopy, and more extensive tissue excision (lumpectomy) are considered standard procedures for obtaining a definitive histopathology.[3,4] Ductoscopy is capable of detecting a single PND-causing papilloma; however, it is an insufficient diagnostic tool for an in situ or invasive cancer that is located within the fluid-yielding ducts.[5,6,7]
Optical coherence tomography (OCT) is a high-speed technology that provides real-time cross-sectional images of tissue structure on the micron scale. OCT is analogous to ultrasound imaging, except that it uses near-infrared light instead of sound. The application of OCT in combination with catheters and endoscopes enables the high-resolution intraluminal imaging of organ systems. OCT has also been used as a noninvasive imaging tool that utilizes light waves to capture cross-sectional pictures of the retina or coronary arteries.[8] The current study investigated the feasibility of OCT imaging of the ductal epithelial layers to identify abnormal lesions through ductoscopic trocars in the ex vivo mammary ducts of mastectomy specimens. The primary aims of the study were to explore the feasibility of inserting an OCT catheter into the breast ducts and to determine whether real-time cross-sectional images could be obtained that would distinguish the usual epithelial layers from the premalignant or malignant lesions in the breast ducts.
2. Methods
This study complied with the principles of the Declaration of Helsinki regarding medical research involving human subjects and was approved by the Ethics Committee of the Acibadem University Medical Center (IRB #766). All the patients that were included in the study provided written informed consent. This feasibility study was conducted prospectively to obtain the initial outcomes of ductal space OCT scanning in ex vivo mastectomy specimens with an intact nipple. The specimens were obtained from patients who had undergone simple or skin-sparing mastectomies for either malignancy (n = 14) or prophylaxis (n = 4). Only 4 out of 18 specimens had presented with clinical PND. A flow diagram of the study participants is shown in Table 1.
3. Study Protocol
Mastectomy specimens without nipple inversion or previous surgeries were selected for real-time intraductal OCT imaging. Initially, ductoscopy with saline infusion was used to confirm that the OCT catheter had been placed inside the duct. The ductoscopy was performed with a flexible ductoscope (Polydiagnost, Pfaffenhofen, Germany) that had three channels and a total diameter of 1.1 mm. The Solex (Polydiagnost GmbH, Pfaffenhofen, Germany) lumen expander system was used to dilate the ostium of the lactiferous ducts.[5,6,7] During the ductoscopic procedure, the non-fluid-yielding and pathologic ducts were recorded, and the shaft was marked with a pen to calculate the intended OCT scanning depth that correlated with the histopathologic findings. After nipple cannulation, the ductoscopy was inserted. Care was taken to confirm that the duct had not ruptured and that the trocar was located inside the duct. After safe cannulation, the OCT catheter was inserted through the ductoscopic shaft to launch the scanning. During the OCT, saline was continuously infused to distend the ductal space. All the normal and abnormal images acquired from the scanning were digitally stored for offline analyses to compare with the corresponding histopathologic analysis.
The OCT images were acquired using a commercially available OCT device (C7-Xrtm/Ilumien, Optis, St. Jude Medical, St. Paul, Minnesota, United States), as previously described.[9] Following a Z-offset adjustment, an OCT imaging catheter (St. Jude Medical, St. Paul, Minnesota, United States) was positioned so that its imaging lens was distal to the abnormal ductal epithelial abnormalities that had been identified and measured using the previous ductoscopy. All the OCT images were obtained using an automatic pullback device with an outer diameter of 0.9 mm, traveling at a rate of 20 mm/s, with a frame rate of 100 frames/s. To maintain duct distention, saline was infused directly through the OCT catheter at a rate of 2.5 to 4.5 mL/s using a syringe. The acquired cross-sectional OCT images were analyzed for the presence of abnormal lesions and measured for comparison with the histopathologic correlations. Since this study was the first to use OCT to endoscopically identify malignant images in mammary ducts, an OCT endoscopist with 15 years of ductoscopy experience performed the OCT procedure and analyzed the acquired snapshots by comparing them with the malignant OCT images that were obtained from the ex vivo lumpectomy specimens.[16] As described in Yemul et al.,[16] the differentiation between the pathologies was determined by considering the feature boundaries, interior appearance, posterior shadowing or enhancement, and the overall morphologic patterns.
The subject duct, which had been marked with a ductoscopic disposable shaft after the OCT scans, was carefully dissected to identify the millimetric lesions. The outer disposable shaft has a scale to understand how centimeter the normal ducts, bifurcations, or lesions are located in discharging or non-discharging ducts. To strength the location of lesions for histopathologic determination, a ductoscopic hook-wire was used to mark the suspected lesion after obtaining the exact location of lesions by OCT scanning. During the specimen dissection, representative 1 cm × 1 cm tissue regions were grossly identified, inked for orientation and image-matching purposes, and processed. The tissue sectioning was performed so that the captured histological images matched the plane orientation of the OCT image. The hematoxylin-and-eosin–stained histology slides that corresponded to the OCT image region were microscopically photographed. The interpretation and correlation of the paired image features were performed under the guidance of the pathologists.
4. Results
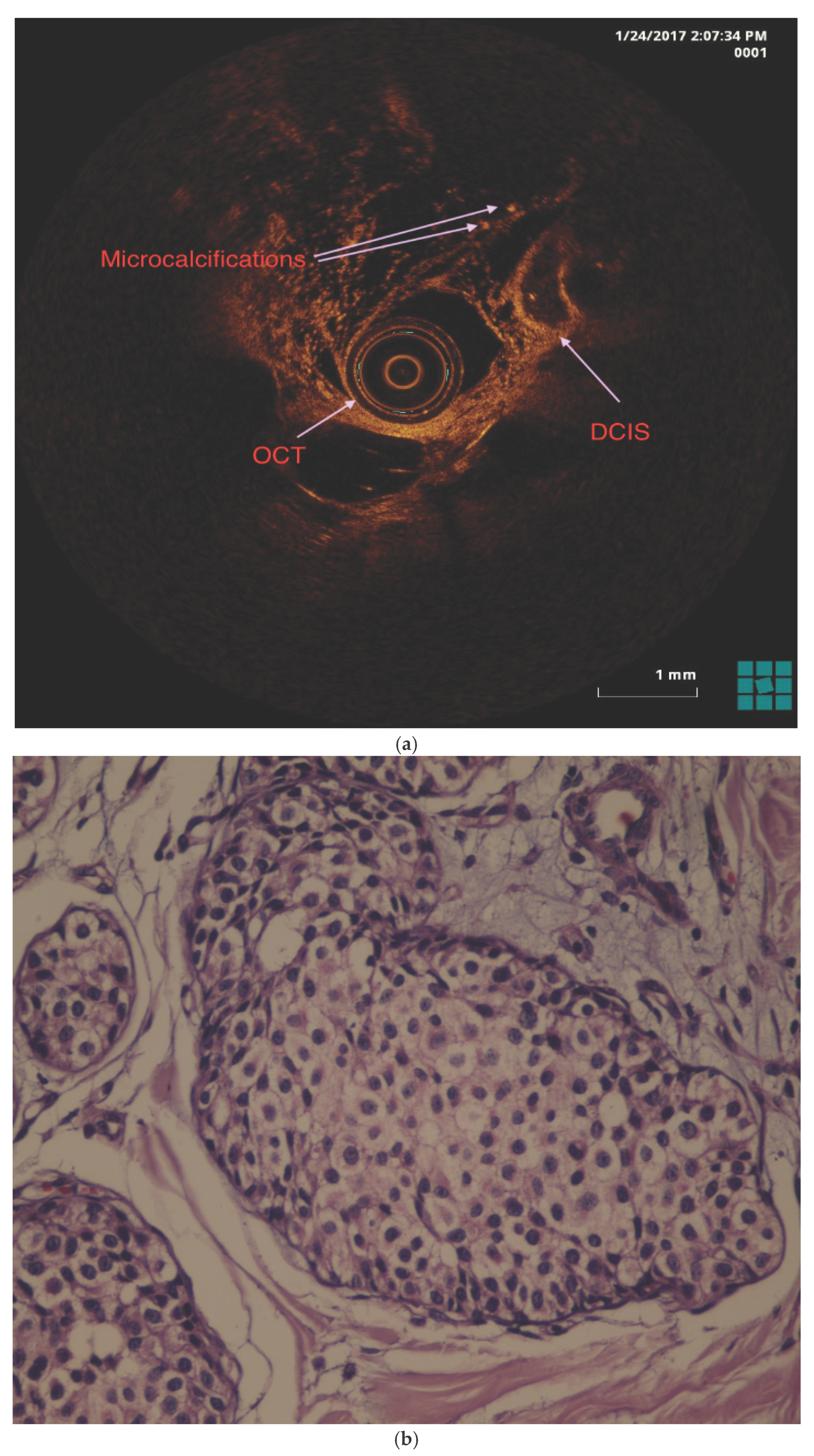
Fourteen out of 18 mastectomy specimens could be cannulated and distended using ductoscopic instruments and saline. Only 4 out of 18 specimens had clinically presented with PND. The insufficiency rate of the ductoscopic cannulation of the nipple orifice was higher (22.2%) than had been previously reported in the literature due to the contracted ducts in the ex vivo specimens without PND.[6,7] To ensure that the ductoscopic trocars were located inside the ducts, fourteen specimens were explored with ductoscopy. The OCT catheter was successfully advanced through the ductoscopic trocars and the associated ducts in only 10 specimens. The instances of OCT insertion or scanning failure were attributed to narrow ducts, kinked OCT catheters or ductal branches. The intraductal OCT scanning showed the usual ductal epithelium, layers, and cavities as cross-sectional images that were similar to standard hematoxylin and eosin slides (Figure 1a, Figure 1b and Figure 1c). The OCT scanning revealed one ductal carcinoma in situ (DCIS) in the duct of a cancer-related specimen (Figure 2a) and one florid ductal hyperplasia in a prophylactic specimen with the c.5265_5266insC (p.Gln1756ProfsTer74) BRCA1 mutation that was confirmed by histopathologic analysis (Figure 2b). The mean duration time ± standard deviation of the OCT procedures, including the ductoscopic guidance for an ex vivo ductal-lobular unit, was 25 min ± 7.2 min. The OCT catheter placement into the ductal space took 7 min ± 3.4 min, and the ductal scanning was completed in only 4 s. The OCT scanning did not detect malignant lesions in 80% of the specimens without PND; however, the OCT scanning did detect undefined microcalcifications and lesions that did not match with the corresponding histopathologic analysis.
5. Discussion
Using the study protocol, intraductal images were acquired after the safe insertion of the ductoscopy with its trocar inside the pathologic duct. Then, an OCT catheter was inserted beyond the susceptible area (e.g., the epithelial alterations) that had been previously measured using ductoscopy. Ducts that did not have epithelial abnormalities according to ductoscopy were also randomly chosen for the OCT protocol. The specimens included lesions that had been diagnosed with cancer; specimens where no cancer had been detected but the patient carried the BRCA mutation were also included. The diameter of a cardiological OCT catheter was considered suitable for entering the non-discharging ducts, but this catheter was difficult to insert through the ductoscopic trocar. The current OCT catheter was used to successfully identify two round oval-shaped premalignant lesions with diameters of approximately 1 mm (the imaging range and working distance of the OCT catheter was 10 mm and 6cm, respectively). Future studies should be designed to evaluate an OCT catheter with a thinner diameter that is also compatible with ductoscopic trocars. Ductoscopy was used prior to the OCT scanning due to the absence of an anterior view from the current OCT device during the insertion procedure. The integration of ductoscopy with an OCT catheter and the ability to generate OCT images with an anterior view will be critical for the practical use of OCT in the intraductal space.
Instead of a contrast solution, saline was used for both clearance and duct distention. In a coronary OCT, a contrast solution is automatically power-injected every 3 s to clear blood from the vessel so that the vessel layers can been seen using OCT. In coronary OCTs, contrast agents are preferred over saline because their viscosity is more effective for clearing blood from the vessels.[10] However, in the breast, contrast-facilitated clearance is not needed for intraductal OCT since the duct has no interior bloodstream. Even in specimens with a bloody discharge, images could be successfully obtained using intraductal OCT with saline. For future OCT scans in live patients, saline would be a safer alternative to contrast agents, which can cause allergic reactions in some patients. The distention of ex vivo mammary ducts with saline made the OCT procedure more efficient than if shrunken ex vivo ducts had been used. The distention did not upgrade the resolution; however, the images of the ductal epithelial layer, lumen, and lesions were clearer and more distinguishable than the images that had been acquired with shrunken ducts.
No published studies have reported on real-time cross-sectional imaging of mammary ducts using an OCT catheter that enters through the nipple orifices. Since the mammary ducts are narrow, only ductoscopy with a diameter of < 1.15 mm has been developed to acquire images of fluid-yielding ducts.[3] Currently, OCT studies related to breast images have only included the analysis of a handheld OCT camera to evaluate the surgical margins of lumpectomy specimens.[11,12] In breast cancer surgery, it is essential that the borders of the excised specimen do not contain any tumor cells, since these positive margins are associated with a higher risk of local recurrence by the primary tumor.[13] With a penetration depth at least of 2 mm in breast tissue, OCT is a suitable technology for intraoperative tumor margin assessment.[14] Nguyen et al. analyzed resection margins ex vivo using OCT in 37 breast cancer specimens.[15] That analysis showed a sensitivity and specificity of 100% and 82%, respectively, in tumor detection compared to histology. However, the OCT technique in those studies did not use a catheter to acquire the intraductal cross-sectional images. In contrast, the current study used a catheter-based OCT to enter the natural duct orifices to obtain direct images of the epithelium and the layers underneath. Intraductal OCT was able to show the ductal epithelium, layers, and cavities as cross-sectional images that were similar to standard hematoxylin and eosin slides. Since the ducts with PND may involve millimetric lesions such as intraductal papilloma or rarely DCIS, the intraductal OCT could enable to show those lesions, which are invisible in conventional imaging such as mammography and MRI. Besides, as a proposal, we may use the intraductal OCT in real-time to understand whether the malignant lesion invades the basal membrane confirming the cancer invasive or not.
Several studies have used OCT to visualize invasive ductal carcinomas and infiltrating tumor cells moving into the surrounding tissue and fibrous stroma.[11,12] Recently, Yemul et al. assessed the mastectomy and breast-conserving surgery specimens from 26 women that were imaged with a handheld OCT probe.[16] Histology slides corresponding to the OCT image regions were digitally photographed. The OCT and histology images from the same region were paired by selecting the best structural matches. In total, 2,880 OCT images were acquired from the 26 breast specimens, and 48 matching OCT–histology image pairs were identified. The results indicated that OCT could be used to identify and distinguish benign and malignant features in human breast tissue. In the present study, a round lesion with an approximately 1 mm border was identified. This lesion completely obstructed the duct, as shown by the hyporeflective interiors and the distinct edges of the well-circumscribed boundary architecture. The architectural findings of florid ductal hyperplasia in our study were similar to the findings of Yemul et al.,[16] who reported images of a moderately hyporeflective interior and less distinct boundaries of the hyperplastic ducts. The OCT evaluation of another oval-shaped lesion, which was confirmed to be a DCIS focal point by histopathologic analysis, also had a hyporeflective interior and distinct edges with well-circumscribed boundary architecture, similar to the OCT findings in Yemul et al.[16]
Study Limitations
First, the present study was a feasibility study and only used ex vivo mastectomy specimens with or without clinically presenting PND. Future studies in live patients are needed to analyze the specificity and sensitivity of OCT in patients with PND. Future studies should also be conducted to compare the efficacy and safety of intraductal OCT versus ductoscopy in patients with PND.
Second, the diameter of the nipple orifice in the ex vivo specimens with non-fluid-yielding and shrunken ducts was narrower than the orifice in live patients with fluid-yielding ducts. Consequently, the cannulation success rate was lower than had been previously reported in the literature. This drawback also explains the identification of lower numbers of OCT lesions than expected. An intraductal OCT study, conducted on live patients with naturally distended ducts that include pathological lesions, would provide improved identification of ductal malignancies.
Future Directions
Susceptible genes such as BRCA 1 and 2 have been widely used to determine whether a high-risk patient should undergo a prophylactic mastectomy. However, there are no precise data analyzing whether the patients who have undergone prophylactic mastectomy actually needed the procedure. OCT images may be used as an additional screening tool to predict breast cancer in high-risk patients through the high-speed, high-resolution scanning of the intraductal space without the need for invasive tissue sampling for histopathologic evaluation.
Currently, there is no protocol for assessing malignant lesions using intraductal OCT, and it took several days of offline analyses at our institution to confirm that the lesion seen on the OCT image was malignant and not an artifact of histopathology processing. Automated image analysis has the potential to improve diagnostic accuracy with lower inter-observer variability and faster speed. These features would enhance the clinical impact of intraductal OCT and improve its suitability for PND diagnosis during microductectomy operations. Additional research might enable the automatic analysis of OCT images, reducing image interpretation time.
In conclusion, this is the first published study to confirm the feasibility of intraductal OCT diagnosis of millimetric malignancies in patients with or without PND. The innovative use of OCT in breast ducts should be further investigated by the development of a catheter that has a thinner diameter and an anterior view, in addition to cross-sectional imaging ability. In the current study, a ductoscopy facilitated the insertion of the OCT catheter with its anterior view; however, it is not certain that the OCT catheter reached the same peripheral branches as those reached by the ductoscopy. Thus, integration of ductoscopy with OCT is needed for more efficient and safe diagnosis of malignancy in patients with PND. An intraductal OCT would also be more efficient if the OCT images could be created using an OCT catheter that is integrated with artificial intelligence.
Funding
The proposed study or innovative idea honored or awarded at Dr. Susan Love Research Foundation’s 8th International Symposium on the Breast, February 19-21, 2015 (Award contributed by the Susan G. Komen Breast Cancer Organization; Grant number: Not Available).
Acknowledgement
Fatih Levent Balci, MD, reserved all rights of innovative use of real-time optical coherence tomography via intraductal route in breast tissue.
References
- Simpson, JS; Connolly, EM; Leong, WL; et al. Mammary ductoscopy in the evaluation and treatment of pathologic nipple discharge: a Canadian experience. Can J Surg. 2009, 52(6), 245–248. [Google Scholar]
- Shen, K; Wu, J; Lu, JS; et al. Fiberopticductoscopy for breast cancer patients with nipple discharge. Surg Endosc. 2001, 15(11), 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Waaijer, L; Simons, JM; Borel Rinkes, IH; et al. Systematic review and meta-analysis of the diagnostic accuracy of ductoscopy in patients with pathological nipple discharge. Br J Surg. 2016, 103(6), 632–643. [Google Scholar] [CrossRef] [PubMed]
- Simmons, R; Adamovich, T; Brennan, M; et al. Nonsurgical evaluation of pathologic nipple discharge. Ann Surg Oncol. 2003, 10(2), 113–116. [Google Scholar] [CrossRef] [PubMed]
- Balci, FL; Feldman, SM. Exploring breast with therapeutic ductoscopy. Gland Surg. 2014, 3(2), 136–141. [Google Scholar] [PubMed]
- Balci, FL; Feldman, SM. Interventional ductoscopy for pathological nipple discharge. Ann Surg Oncol. 2013, 20(10), 3352–3354. [Google Scholar] [CrossRef]
- Bender, O; Balci, FL; Yüney, E; Akbulut, H. Scarless endoscopic papillomectomy of the breast. Onkologie 2009, 32(3), 94–98. [Google Scholar] [CrossRef]
- Fujimoto, JG; Pitris, C; Boppart, SA; Brezinski, ME. Optical Coherence Tomography: An Emerging Technology for Biomedical Imaging and Optical Biopsy. Neoplasia 2000, 2(1-2), 9–25. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, Y; Tanaka, A; Nishiguchi, T; et al. High-density lipoprotein cholesterol as a therapeutic target for residual risk in patients with acute coronary syndrome. PLoS One 2018, 13(7), e0200383. [Google Scholar] [CrossRef] [PubMed]
- Takarada, S; Imanishi, T; Liu, Y; et al. Advantage of next-generation frequency-domain optical coherence tomography compared with conventional time-domain system in the assessment of coronary lesion. Catheter Cardiovasc Interv. 2010, 75(2), 202–206. [Google Scholar] [CrossRef] [PubMed]
- Yao, X; Gan, Y; Chang, E; Hibshoosh, H; Feldman, S; Hendon, C. Visualization and tissue classification of human breast cancer images using ultrahigh-resolution OCT. Lasers Surg Med. 2017, 49(3), 258–269. [Google Scholar] [CrossRef] [PubMed]
- Assayag, O; Antoine, M; Sigal-Zafrani, B; et al. Large field, high resolution full-field optical coherence tomography: a pre-clinical study of human breast tissue and cancer assessment. Technol Cancer Res Treat. 2014, 13(5), 455–468. [Google Scholar] [CrossRef] [PubMed]
- Pleijhuis, RG; Graafland, M; de Vries, J; Bart, J; de Jong, JS; van Dam, GM. Obtaining adequate surgical margins in breast-conserving therapy for patients with early-stage breast cancer: current modalities and future directions. Ann Surg Oncol. 2009, 16(10), 2717–2730. [Google Scholar] [CrossRef] [PubMed]
- Wang, J; Xu, Y; Boppart, SA. Review of optical coherence tomography in oncology. J Biomed Opt. 2017, 22(12), 1–23. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, FT; Zysk, AM; Chaney, EJ; et al. Intraoperative evaluation of breast tumor margins with optical coherence tomography. Cancer Res. 2009, 69(22), 8790–8796. [Google Scholar] [CrossRef] [PubMed]
- Yemul, KS; Zysk, AM; Richardson, AL; Tangella, KV; Jacobs, LK. Interpretation of optical coherence tomography images for breast tissue assessment. Surg Innov. 2019, 26(1), 50–56. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(a) Intraductal OCT showing usual ductal epithelial layers; (b) Florid ductal hyperplasia detected using intraductal OCT in a patient with a BRCA mutation and *histopathologic correlation ; (c) *Histopathologic (Hematoxylin and eosin staining, 30x) images of a florid ductal hyperplasia showing a round lesion with well-circumscribed boundary. OCT, optical coherence tomography.
Figure 1.
(a) Intraductal OCT showing usual ductal epithelial layers; (b) Florid ductal hyperplasia detected using intraductal OCT in a patient with a BRCA mutation and *histopathologic correlation ; (c) *Histopathologic (Hematoxylin and eosin staining, 30x) images of a florid ductal hyperplasia showing a round lesion with well-circumscribed boundary. OCT, optical coherence tomography.
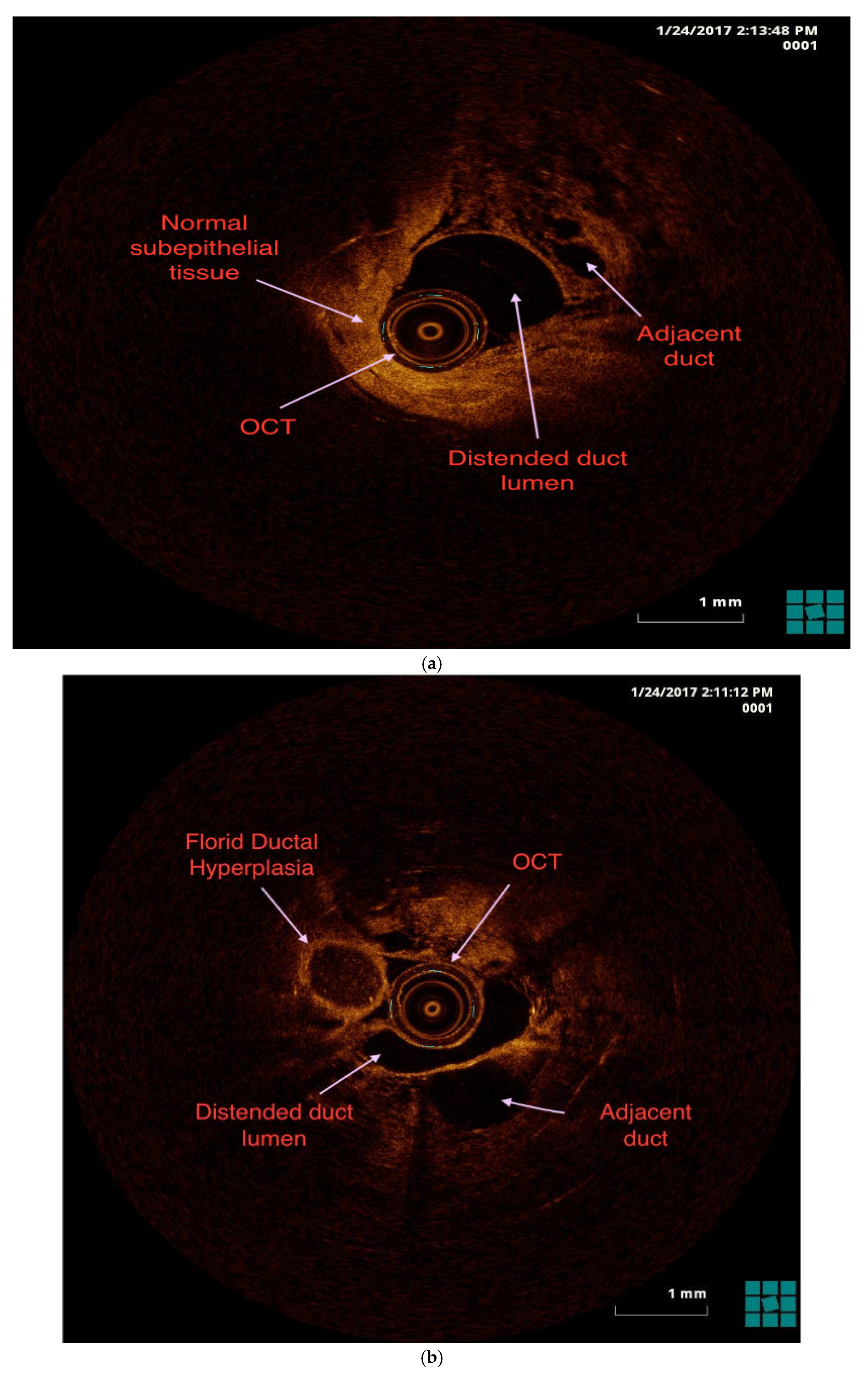
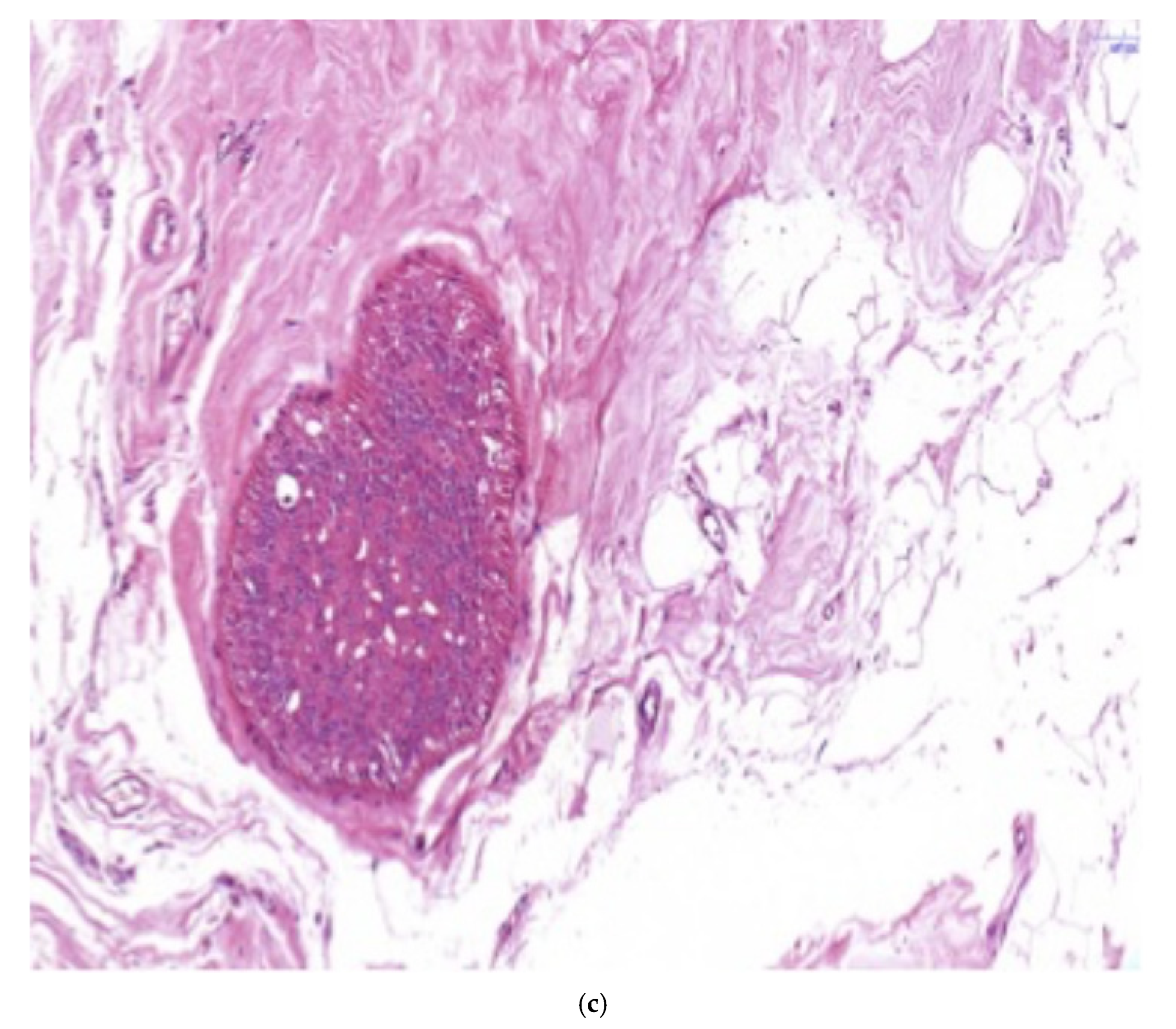
Figure 2.
a) The first reported DCIS detected using intraductal OCT and *histopathologic correlation; b)*Solid type DCIS. Ductal lumina completely filled with low-grade ductal cinoma cells. Ductal basal membrane is intact. Hematoxylin and eosin staining, 400x. DCIS, Ductal carcinoma in situ; OCT, Optical coherence tomography.
Figure 2.
a) The first reported DCIS detected using intraductal OCT and *histopathologic correlation; b)*Solid type DCIS. Ductal lumina completely filled with low-grade ductal cinoma cells. Ductal basal membrane is intact. Hematoxylin and eosin staining, 400x. DCIS, Ductal carcinoma in situ; OCT, Optical coherence tomography.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license.
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



