
Submitted:
19 December 2025
Posted:
22 December 2025
You are already at the latest version
Abstract
Background/Objectives: The accessory mandibular foramina (AMaFs) are small openings in the mandible that have been proposed to play a significant role in clinical practice. The objective of the present study was to examine the number, diameter, and distance of AMaFs to mandibular foramen in dry mandibles and to meta-analyze all available data after a systematic review, aiming to address gaps regarding the AMaFs potential clinical impact. Methods: We assessed the number, diameter, and spatial relationship of AMaFs to the mandibular foramen in human adult dry mandibles of unknown gender and age derived from our Laboratory. Stainless steel wire threads and digimatic caliper measurements were utilized by two separate raters. Cluster analysis was employed for the classification of foramina into distinct spatial groups. Furthermore, following the PRISMA guidelines, we conducted an unlimited literature search using the terms “accessory mandibular” and “foramen/foramina” across the PubMed, Scopus, SciELO, and Google Scholar databases to identify all published studies that reported on the prevalence and morphology of AMaFs in dry mandibles or cadaveric material. Radiological studies were excluded. The search was completed on July 13, 2025. Study quality was evaluated using the appropriate AQUA tool. Data synthesis was carried out using STATA 19. No external funding was received. Results: A total of 96 dry mandibles (50 dentate and 46 edentulous) were analyzed. AMaFs were detected in 8 / 96 mandibles (8.3 %). In these mandibles, a total of 25 accessory mandibular foramina, all superior to the mandibular foramen, were recognized (mean: 3.13 foramina / mandible) with a mean diameter 0.56 ± 0.10 mm, and a mean distance from the mandibular foramen 11.34 ± 1.29 mm (mean vertical distance: 10.32 ± 1.35 mm and mean absolute horizontal distance: 3.78 ± 0.49 mm). Of these foramina, 21 / 25 (84 %) had a diameter of ≥0.5 mm; their number, diameters, and distances from the mandibular foramen was comparable between left and right hemimandibles. Based on their positioning to the mandibular foramen, the AMaFs were classified into two distinct groups (clusters). Furthermore, a total of 36 studies were included in the meta-analysis. In most of the mandibles (65.1%; 95% CI: 57.7 – 72.2%; I2: 94.9%), no AMaF was detected. Unilateral presence of one or more AMaFs was observed in 20.9% of mandibles (95% CI: 16.3 – 25.9%; I2: 91.3%), while bilateral occurrence was identified in 10.6% (95% CI: 6.9 – 15.0%; I2: 93.0%). Additionally, 2.4% of mandibles (95% CI: 1.0 – 4.2%; I2: 86.3%) exhibited multiple AMaFs (≥2) on at least one side. On average, each hemimandible contained 0.253 AMaFs (95% CI: 0.198 – 0.312; I2: 96.9%). The overall mean diameter of AMaFs was estimated at 0.65 ± 0.33 mm. The substantial heterogeneity observed was not attributed to publication bias. Conclusions: AMaFs are detected in one third of the mandibles. The AMaFs are typically located superior to the mandibular foramen, on the anterior or posterior aspect of the mandible, and may provide additional entry routes for nerve fibers. Failure to recognize these anatomical variations usually lead to incomplete anesthesia or persistent pain in specific regions of the lower jaw during routine dental procedures. Clinicians should remain aware of these variations and adjust their surgical or anesthetic techniques accordingly to ensure effective and comprehensive anesthesia.
Keywords:
mandible
; mandibular foramen
; accessory mandibular foramen
; inferior alveolar nerve
; alveolar ridge
1. Introduction
The mandibular foramen is an irregularly shaped opening located slightly above the midpoint of the medial surface of the mandibular ramus. From this foramen, the mandibular canal descends and extends anteriorly beneath the alveolar sockets toward the body of the mandible. The inferior alveolar nerve (IAN) and accompanying vessels enter the mandible through the mandibular foramen and course within this canal, providing sensory innervation and vascular supply to the teeth, periodontium, and lower lip [1,2]. Variations in the configuration of the mandibular canal are common; in approximately 60% of individuals the entire IAN is enclosed within a single canal, whereas in the remaining 40% the fibers are distributed in multiple branches [3].
Accessory mandibular foramina (AMaFs) are small openings located near the main mandibular foramen, occasionally large enough to transmit a neurovascular bundle [4]. Histological studies have confirmed the presence of nerve fibers within these foramina [5], while anatomical dissections suggest that in most cases the contained structures originate from tributaries of the inferior alveolar nerve, and less frequently from branches of the maxillary artery [6]. The arterial supply to this region is further complicated by small ascending or nutrient branches derived from the inferior alveolar and maxillary arteries [7,8].
Clinically, accessory mandibular foramina (AMaFs) have important implications as potential additional routes for neurovascular entry into the mandible, possibly explaining inferior alveolar nerve block (IANB) failures, which occur in up to 20% of cases even among experienced clinicians [3]. These accessory canals may also predispose to intraoperative bleeding or postoperative neurosensory disturbances during procedures such as sagittal split osteotomy, mandibular angle resection, or implant placement [9]. Beyond anesthetic relevance, AMaFs may facilitate the spread of infection or malignant cells from the floor of the mouth into the mandibular bone, underscoring their surgical and oncological significance and the need for precise knowledge of their prevalence and location [10]. Radiologically, panoramic imaging often fails to reveal these foramina due to superimposition and limited resolution, whereas cone-beam computed tomography (CBCT) provides superior three-dimensional visualization but may still underestimate their frequency. Consequently, direct anatomical examination of dry mandibles remains the most reliable method for identifying AMaFs and characterizing their morphology [11,12].
Despite multiple reports, data regarding the prevalence, size, and distribution of AMaFs remain inconsistent, likely due to variations in methodology, sample type, and imaging technique. Moreover, few studies have combined morphometric observation with quantitative synthesis. Therefore, the present study aimed to examine the number, diameter, and spatial relationship of accessory mandibular foramina to the mandibular foramen in adult dry mandibles, and to perform a comprehensive meta-analysis of all available anatomical data. This dual approach seeks to provide updated and clinically relevant insight into the anatomical variability and potential clinical significance of AMaFs, particularly regarding anesthesia and surgical interventions involving the mandible.
2. Materials and Methods
2.1. Specimen Selection
The study aimed to assess the number, size (diameter), and anatomical location of the AMaFs in relation to the mandibular foramen.
This observational study analyzed a total of 96 dry mandibles (50 dentate and 46 edentulous) sourced from the Anatomy Laboratory of the Department of Medicine at Democritus University of Thrace, Greece. The specimens came from individuals of Greek descent, though specific information regarding age or sex was not available. Specimens displaying fractures, deformities, or signs of erosion were excluded.
Since the research involved cadaveric material, ethical committee approval was not required.
2.2. Measurements
The purpose of the study was to quantify the number and diameter of AMaFs, as well as the distance between these structures and the mandibular foramen. The number of AMaFs was established though meticulous visual inspection under direct lighting conditions. Foramen diameters were assessed using a flexible stainless-steel wire with diameters ranging from 0.2 mm to 1.2 mm (UA218893; Zhejiang, China), following previously established methods [13] (Figure 1). Foramina measuring less than 0.2 mm were excluded from documentation. In cases where the wire could not be inserted, the diameter (di) was assigned the value of the next smallest wire size available. This method introduced a maximum absolute measurement error (de) of 0.1 mm. The average relative error was calculated as the mean of the ratios de / (di + de) across all i-th foramina.
All measurements were taken using a digimatic caliper (Mitutoyo Co., Japan) with an accuracy of 0.01 mm (Figure 2).
Each distance was measured from the center of each mandibular foramen. The location of each AMaF was determined using two imaginary lines (horizontal and vertical), dividing the area into four quadrants: anterior superior, posterior superior, anterior inferior, and posterior inferior. In detail, to determine the position of each foramen, the following distances were measured: i) Height, namely the vertical distance between the AMaF and the mandibular foramen (x); ii) Length, namely the horizontal distance between the genial AMaF and the mandibular foramen (y); and iii) Radius, namely the distance between the AMaF and the mandibular foramen (represented by the square root of x2 + y2). Of note, accessory mandibular foramina were assigned positive distance values if they were located superior to the mandibular foramen in the vertical plane and/or anterior to it in the horizontal plane. (Figure 3). The measurement protocol used is in keeping with recent studies [14]
2.3. Statistics
Continuous variables were expressed as means and standard errors (SE) and compared using Student’s t-test in case equal variances could be assumed; else, the Welch’s t-test was alternatively preferred. The Wilcoxon Signed Ranks test was used in case of deviation from normality.
Discrete variables were expressed as percentages and compared using chi-square test; in case of expected frequencies <5 in ≥25% of cells, the Fisher’s exact test was alternatively applied.
Two-step cluster analysis was further used to discriminate lingual foramina according to their direction and distance from genial tubercle.
Both stainless steel wire threads and digimatic caliper measurements were utilized by two separate raters; the intraclass correlation coefficient (ICC) was used to assess relatedness of raters.
The level of statistical significance was set to 0.05. All tests were two-tailed and performed using SPSS 26.0.
2.4. Meta-Analysis
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed [15]. Two separate investigators conducted an unlimited literature search using the terms “accessory mandibular” and “foramen/foramina” across the PubMed, Scopus, SciELO, and Google Scholar databases to identify all published studies that reported on the prevalence and morphology of AMaFs in dry mandibles or cadaveric material. In detail, we used the search algorithm “(accessory mandibular) AND ((foramen) OR (foramina))” in PubMed search and the “(accessory AND mandibular AND (foramina OR foramen)” in Scopus. Radiological studies were excluded. The search was completed on July 13, 2025.
For each included study, two independent reviewers extracted the following data: the first authors’ name, year of publication, study origin, type of material examined (dry mandibles or cadaveric specimens), total number of mandibles analyzed, number of mandibles without AMaFs, number of mandibles with unilateral or bilateral AMaFs (one or more), number of mandibles presenting multiple AMaFs (regardless of side), total count of AMaFs, mean diameter of the AMaFs, and their mean distance from the mandibular foramen. All data were entered into an Excel file formatted for compatibility with STATA.
The studies’ methodological rigor and potential for bias in both procedure and result reporting was evaluated by two individual reviewers using the Anatomical Quality Assessment (AQUA) tool for the quality assessment of anatomical studies [16]. Each of the 5 domains were judged as having low, high, or unclear risk of bias. The study was characterized to have high risk of bias if more than two domains were rated as “unclear”, or if any single domain was rated as high risk [17]. The Critical Appraisal Tool for Anatomical Meta-Analysis (CATAM) was used to evaluate the strength and reliability of the present meta-analysis [18].
Data synthesis was carried out using a random-effects model (REML) following Freeman-Tucked double arcsine transformation, implemented in STATA version 19 (StataCorp. 2025. Stata Statistical Software: Release 19. College Station, TX: StataCorp LLC) metaprop package for meta-analysis of proportions. Heterogeneity was assessed using the Q-test and the I2 statistic. Of note, I2 >75% is interpreted as high heterogeneity; however, we rather regarded I2 as the proportion of the variance in observed effects that is attributed to variance in true effects [19]. Publication bias was evaluated using Egger’s test, Begg’s test, funnel plot with trim-and-fill analysis, and Doi plot with its corresponding LFK index. The latter has been noted to offer additional value in detecting bias in prevalence meta-analyses, particularly those involving unregistered studies that are susceptible to selective reporting [20].
No external funding was received. This review was not registered in PROSPERO due to the temporary suspension of registrations for prevalence meta-analyses.
3. Results
3.1. Prevalence, Size and Location of Accessory Mandibular Foramina
Accessory mandibular foramina were detected in 8 out of the 96 mandibles examined (8.3%) (Figure 4).
In these mandibles, a total of 25 accessory mandibular foramina, all superiorly to the mandibular foramen, were recognized (mean: 3.13 foramina / mandible) with a mean diameter 0.56 ± 0.02 mm, and a mean distance from the mandibular foramen 11.34 ± 1.29 mm (mean vertical distance: 10.32 ± 1.35 mm and mean absolute horizontal distance: 3.78 ± 0.49 mm). Paradigms of multiple AMaFs are provided in Figure 5 (two foramina), Figure 6 (three foramina), and Figure 7 (five foramina). As per the latter case, an AMaF could be found very close to the main mandibular foramen (Figure 8).
Of these foramina, 21 / 25 (84%) had a diameter of ≥0.5 mm, as determined using stainless-steel wires. Their number was comparable between the left (1.25 ± 0.53) and the right (1.38 ± 0.32) hemimandible (p = 0.915). Moreover, their diameters and distances (p = 0.349) from the mandibular foramen did not present a statistically significant difference (p = 0.756).
The ICC was 1.000 for diameter, 0.999 for vertical distance, and 1.000 for horizontal distance. Based on their positioning to the mandibular foramen, the accessory mandibular foramina were classified into two distinct groups (clusters).
3.2. Clustering Accessory Mandibular Foramina Reveals Two Distinct Groups
Aiming to further analyze the special infrastructure of AMaFs, a grouped scattergram depicting vertical vs. horizontal distance of these foramina from mandibular foramen is provided as Figure 9. This scattergram visualizes the results of a two-step cluster analysis, showing two distinct groups of data points corresponding to the 21 AMaFs recorded with a diameter ≥0.5 mm: i) lower-proximal AMaFs and ii) upper-distal AMaFs.
3.3. Meta-Analysis of Prevalence of Accessory Mandibular Foramina
A total of 476 publications identified through databases searches: 211 from PubMed, 242 from Scopus, and 10 from SciELO. An additional 13 records were found via Google Scholar, and 3 more were obtained through citation tracking. Thirty-six studies were included in qualitative and quantitative assessment. The PRISMA flow diagram illustrating the complete selection process is shown in Figure 10.
All included studies and their characteristics are summarized in Table 1.
Using the Anatomical Quality Assessment (AQUA) tool, Domain 1 (Objective(s) and subject characteristics) the present observational study was rated as having a high risk of bias, primarily due to the absence of data on the cadavers’ sex, age, and medical background. In contrast, all remaining domains - Domain 2 (Study Design), Domain 3 (Methodology Characterization), Domain 4 (Descriptive Anatomy), and Domain 5 (Reporting of Results) – were judged to carry a low risk of bias. Similarly, all other included studies were qualitatively assessed (Table 2).
An AMaF was not detected in most of the mandibles (65.1%; 95% CI: 57.7 – 72.2%; I2: 94.9%) (Figure 11).
In 20.9% of mandibles (95% CI: 16.3 – 25.9%; I2: 91.3%), one or more AMaFs were observed unilaterally (Figure 12), while 10.6% (95% CI: 6.9 – 15.0%; I2: 93.0%) exhibited bilateral occurrence (Figure 13). Additionally, 2.4% of mandibles (95% CI: 1.0 – 4.2%; I2: 86.3%) presented multiple AMaFs (≥2) on at least one side (Figure 14).
On average, each hemimandible contained 0.253 AMaFs (95% CI: 0.198 – 0.312; I2: 96.9%). Subgroup analysis revealed a comparable prevalence of AMaFs between mandibles of Indian and non-Indian origin (Figure 15).
Table 3 presents a summary of all available data on the diameter of AMaFs. Based on the means and SD from the four studies with reported values, the overall mean diameter of AMaFs was estimated at 0.65 ± 0.33 mm.
The funnel plot revealed apparent asymmetry, while the trim-and-fill analysis imputed 7 additional studies on the right side of the funnel plot (Figure 16).
The Doi plot constructed suggested no asymmetry. The relevant LFK index was computed to -0.56. (Figure 17).
Egger’s and Begg’s tests yielded non-significant results (p=0.568 and p=0.913, respectively).
3.4. Critical Appraisal of the Present Meta-Analysis
Applying the Critical Appraisal Tool for Anatomical Meta-Analysis (CATAM), the present meta-analysis has been awarded 2 points for title, 4 points for Abstract, 6 points for Introduction, 14 points for Methods (4 points for Search strategy, 2 points for Selection criteria, 2 points for Data extraction, 4 points for Quality assessment, and 2 points for Statistical analysis), 12 points for Results (2 points for Search results, 2 points for the Characteristics of included studies, and 8 points for Outcomes), 6 points for Discussion, 4 points for Conclusion, and 2 points for References.
4. Discussion
4.1. Additive Value of the Present Study in Relation to the Established Knowledge
In the present observational study, all accessory mandibular foramina (AMaFs) with a diameter of ≥0.2 mm were systematically examined in dry human mandibles using stainless steel wires. To our knowledge, this represents the first application of this technique to cadaveric specimens. No AMaF was identified below the main mandibular foramen, which is consistent with previous large-scale observational studies in dry mandibles [40]. In all specimens exhibiting AMaFs, the accessory foramina were situated within 50 mm of the mandibular foramen and consistently measured less than 2 mm in diameter, in agreement with earlier findings [32].
Furthermore, the location of AMaFs was determined by measuring their distance from the mandibular foramen—a method considered reliable, as it is unaffected by whether the mandible is dentate or edentulous. Furthermore, age-related changes appear to have minimal influence on the mandibular foramen’s position [55]. In contrast, alternative reference points, such as the horizontal distance from the anterior border of the ramus or the vertical distance from the mandibular notch, may vary due to age-related alveolar ridge resorption [56]. This resorptive process is particularly evident in the posterior mandible, where edentulous areas exhibit reduced vertical height and buccolingual width compared with the dentate side [57].
The accompanying meta-analysis constitutes the first attempt to summarize worldwide available data and assess their heterogeneity. Most mandibles (65.1%), no accessory mandibular foramen (AMaF) was detected. Unilateral AMaFs were present in 20.9% of mandibles, while bilateral occurrence was observed in 10.6%. Multiple foramina (≥2) on at least one side appeared in 2.4% of cases. On average, each hemimandible contained 0.25 AMaFs, with a mean diameter of 0.65 ± 0.33 mm. The high heterogeneity among studies was not related to publication bias.
Differences in the reported prevalence of AMaFs across studies may partly reflect methodological variability. Cadaveric and dry-bone examinations generally identify a greater number of foramina than radiological studies, likely due to the limited spatial resolution of CBCT. For this reason, our study relied on direct examination of dry mandibles rather than imaging data. Two-dimensional radiographs, such as panoramic images, often fail to detect small accessory foramina due to overlapping structures and limited image resolution [58]. In contrast, CBCT and multi-detector CT allow three-dimensional visualization of the mandibular canal system, enabling detection of even narrow accessory canals [12,59,60]. Recent advancements in artificial intelligence (AI) further enhance segmentation accuracy and identification of accessory canal structures on CBCT images, thus improving diagnostic precision and treatment planning [61,62].
The presence of AMaFs poses significant challenges for achieving effective local anesthesia. These foramina, which may transmit accessory branches of the inferior alveolar nerve, can lead to incomplete anesthesia when the nerve fibers enter the mandible via alternate routes not reached by a standard inferior alveolar nerve block (IANB) [3]. Consequently, patients may experience persistent pain or inadequate numbness, particularly in the posterior teeth and gingival regions. Although the IANB is routinely used to anesthetize the inferior alveolar nerve as it enters the mandibular foramen, the presence of accessory foramina, often located anteriorly or posteriorly to the main foramen, can allow additional neural input to the mandible, thereby compromising anesthetic efficacy. Clinicians must therefore remain alert to such anatomical variations and modify their anesthetic techniques accordingly.
The reported failure rate of IANB approaches 20%, even among experienced practitioners. While inaccurate needle placement is a primary cause, anatomical factors such as retrognathic mandibles, high lingular position, and the presence of AMaFs are also significant contributors [3,63]. These variations may necessitate repeated or supplemental injections, thereby increasing the risk of nerve injury, hematoma, and patient discomfort. Moreover, as AMaFs may contain small arteries or veins, their inadvertent injury during surgical procedures such as third molar extraction, endodontic surgery, or implant placement can result in unexpected bleeding [7,47,64]. Inadequate preoperative assessment or misinterpretation of imaging may therefore lead to intraoperative complications or postoperative pain. Given that conventional panoramic radiographs frequently fail to depict such structures, CBCT imaging should be considered, particularly in cases with prior anesthesia failure or complex mandibular anatomy [12,65].
From a clinical perspective, the presence of AMaFs carries notable implications for oral and maxillofacial surgery. Procedures such as sagittal split osteotomies, mandibular angle resections, or bone harvesting may be complicated by these additional canals, as they increase the risk of damaging neurovascular bundles—potentially resulting in prolonged bleeding, neuroma formation, or postoperative sensory disturbances [5,66]. Surgical complications are particularly likely when AMaFs are located near the mandibular ramus or lingula, areas routinely manipulated during orthognathic and trauma surgeries. Therefore, precise knowledge of their prevalence and topographic distribution is essential for surgical planning and the prevention of inadvertent neurovascular injury.
Beyond anesthesia-related implications, AMaFs may also play a role in the spread of malignant tumors. Their number and distribution along the medial mandibular surface are of particular concern to oncologists and radiotherapists, as these foramina may offer direct access routes into cancellous bone, facilitating tumor invasion from the floor of the mouth [10]. In oncologic contexts, AMaFs can serve as potential pathways for perineural or vascular tumor dissemination from primary oral malignancies into deeper mandibular bone [67]. This perineural invasion is associated with poorer prognosis and higher recurrence rates. Failure to recognize such accessory pathways could therefore result in underestimation of tumor extent and inadequate surgical margins.
Preoperative imaging, particularly cone-beam computed tomography (CBCT), plays a critical role in identifying the position and size of both the mandibular foramen and any AMaFs, thus facilitating accurate and safe surgical planning. Although major complications are relatively rare, clinicians should be equipped to manage them when they arise. Numerous studies have confirmed the superior precision and reliability of CBCT compared to conventional radiographic techniques for detecting small anatomical structures [68]. This improved visualization underscores CBCT’s value as an indispensable tool for preoperative assessment, enhancing surgical accuracy and minimizing intraoperative complications.
4.2. Strengths and Limitations of the Present Study
A key strength of this study lies in the application of cluster analysis to identify subgroups of AMaFs and explore their specific characteristics. To our knowledge, this is the first study to employ such an approach, making it a novel contribution to the existing body of anatomical literature. Conversely, the use of stainless-steel wires, a method not commonly adopted for measuring foramen diameter, could be regarded as a potential limitation. Nevertheless, this technique has been thoroughly validated in prior research, and interrater agreement for foramina of comparable diameter to AMaFs has been shown to be nearly perfect [13]. Moreover, as AMaFs measuring < 0.2 mm were excluded from documentation, and the method introduced a maximum absolute measurement error of 0.1 mm, our approach is in keeping with that of Iwanaga et al, who considered AMaFs as “absent” when had a diameter smaller than 0.3 mm [6]. Additionally, findings related to the prevalence of rare anatomical variants, such as the presence of multiple AMaFs, may be susceptible to notable reporting bias [20]; however, the quantification of the maximum reporting bias, as performed in the present study, offers additive value.
Future studies are encouraged to further investigate the clinical relevance of the above-mentioned anatomical observations.
5. Conclusions
This study provides anatomical insights into the morphology and topography of accessory mandibular foramina. The findings support more accurate preoperative assessment and optimization of inferior alveolar nerve block anesthesia during mandibular surgical procedures. Greater awareness of these anatomical variations can reduce complications and improve surgical and anesthetic outcomes.
Author Contributions
Conceptualization, Z-M.T., and V.P.; methodology, Z-M.T., and V.P.; software, V.P.; validation, Z-M.T., and V.P.; formal analysis, V.P.; investigation, Z-M.T., and V.P.; resources, Z-M.T., and V.P.; data curation, V.P.; writing—original draft preparation, V.P.; writing—review and editing, Z-M.T., and V.P.; visualization, Z-M.T., and V.P.; supervision, V.P.; project administration, V.P.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
An ethics committee approval was not applicable due to the cadaveric material studied.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data used can be provided upon reasonable request.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Gray’s Anatomy, 38th ed.; Gray, H., Williams, P.L., Bannister, L.H., Berry, M.M., Collins, P., Dyson, M., Dussek, J.E., Ferguson, M.W.J., Eds.; Churchill Livingstone: London, UK, 1995; pp. 576–577. [Google Scholar]
- Wolf, K.T.; Brokaw, E.J.; Bell, A.; Joy, A. Variant Inferior Alveolar Nerves and Implications for Local Anesthesia. Anesth Prog. 2016, 63, 84–90. [Google Scholar] [CrossRef]
- Das, S.; Suri, R.K. An anatomico-radiological study of an accessory mandibular foramen on the medial mandibular surface. Folia Morphol (Warsz) 2004, 63, 511–3. [Google Scholar] [PubMed]
- Haveman, C.W.; Tabo, H.G. Posterior accessory foramina of the human mandible. J Prosthet Dent. 1974, 35, 462–468. [Google Scholar] [CrossRef] [PubMed]
- Przystańska, A.; Bruska, M. Accessory mandibular foramina: histological and immunohistochemical studies of their contents. Arch Oral Biol. 2010, 55, 77–80. [Google Scholar] [CrossRef]
- Iwanaga, J.; Kikuta, S.; Ibaragi, S.; Watanabe, K.; Kusukawa, J.; Tubbs, R.S. Clinical anatomy of the accessory mandibular foramen: application to mandibular ramus osteotomy. Surg Radiol Anat. 2020, 42, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Olivetto, M.; Bettoni, J.; Duisit, J.; Chenin, L.; Bouaoud, J.; Dakpé, S.; Devauchelle, B.; Lengelé, B. Endosteal blood supply of the mandible: anatomical study of nutrient vessels in the condylar neck accessory foramina. Surg Radiol Anat. 2020, 42, 35–40. [Google Scholar] [CrossRef]
- Bruneder, S.; Schwaiger, M.; Kerner, A.; Steyer, G.; Toferer, A.; Zemann, W.; Hammer, N.; Brcic, L.; Avian, A.; Wallner, J. Expect the unexpected: The course of the inferior alveolar artery - Preliminary results and clinical implications. Ann Anat. 2022, 240, 151867. [Google Scholar] [CrossRef]
- Gupta, S.; Soni, A.; Singh, P. Morphological study of accessory foramina in mandible and its clinical implications. Indian Journal of Oral Sciences. 2017, 4, 12–15. [Google Scholar] [CrossRef]
- Fanibunda, K.; Matthews, J.N. The relationship between accessory foramina and tumour spread on the medial mandibular surface. J Anat. 2000, 196, 23–29. [Google Scholar] [CrossRef]
- Naitoh, M; Hiraiwa, Y; Aimiya, H; Ariji, E. Observation of bifid mandibular canal using cone-beam computerized tomography. Int J Oral Maxillofac Implants 2009, 24, 155–9. [Google Scholar]
- Orhan, K.; Aksoy, S.; Bilecenoglu, B.; Sakul, B.U.; Paksoy, C.S. Evaluation of bifid mandibular canals with cone-beam computed tomography in a Turkish adult population: a retrospective study. Surg Radiol Anat. 2011, 33, 501–7. [Google Scholar] [CrossRef] [PubMed]
- Thomaidi, Z.M.; Tsatsarelis, C.; Papadopoulos, V. Accessory Mental Foramina in Dry Mandibles: An Observational Study Along with Systematic Review and Meta-Analysis. Dent. J. 2025, 13, 94. [Google Scholar] [CrossRef]
- Le, L.N.; Do, T.T.; Truong, L.T.; Dang The, A.T.; Truong, M.H.; Huynh Ngoc, D.K.; Nguyen, L.M. Cone Beam CT Assessment of Mandibular Foramen and Mental Foramen Positions as Essential Anatomical Landmarks: A Retrospective Study in Vietnam. Cureus 2024, 16, e59337. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; Chou, R.; Glanville, J.; Grimshaw, J.M.; Hróbjartsson, A.; Lalu, M.M.; Li, T.; Loder, E.W.; Mayo-Wilson, E.; McDonald, S.; McGuinness, L.A.; Stewart, L.A.; Thomas, J.; Tricco, A.C.; Welch, V.A.; Whiting, P.; Moher, D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Henry, B.M.; Tomaszewski, K.A.; Ramakrishnan, P.K.; Roy, J.; Vikse, J.; Loukas, M.; Tubbs, R.S.; Walocha, J.A. Development of the anatomical quality assessment (AQUA) tool for the quality assessment of anatomical studies included in meta-analyses and systematic reviews. Clin Anat. 2017, 30, 6–13. [Google Scholar] [CrossRef]
- Malkidou, N.; Papadopoulos, V.; Fiska, A. Anatomical variations of the infrahyoid muscles and ansa cervicalis: a systematic review and an updated classification system for the omohyoid muscle. Anat Cell Biol. 2025. [Google Scholar] [CrossRef]
- D’Antoni, A.V.; Tubbs, R.S.; Patti, A.C.; Higgins, Q.M.; Tiburzi, H.; Battaglia, F. The Critical Appraisal Tool for Anatomical Meta-analysis: A framework for critically appraising anatomical meta-analyses. Clin Anat. 2022, 35, 323–331. [Google Scholar] [CrossRef]
- Borenstein, M. Research Note: In a meta-analysis, the I2 index does not tell us how much the effect size varies across studies. J Physiother. 2020, 66, 135–139. [Google Scholar] [CrossRef]
- Papadopoulos, V.; Filippou, D.; Fiska, A. Prevalence of rare anatomic variants - publication bias due to selective reporting in meta-analyses studies. Folia Med (Plovdiv) 2024, 66, 795–817. [Google Scholar] [CrossRef]
- Sutton, R.N. The practical significance of mandibular accessory foramina. Aust Dent J. 1974, 19, 167–73. [Google Scholar] [CrossRef]
- Suazo, G.I.; Zavando, M.D.A.; Smith, R.L. Is the conduct of Serres an anatomical variation? Int J Morphol. 2009, 27, 43–37. [Google Scholar]
- Murlimanju, B.V.; Prabhu, L.V.; Prameela, M.D.; Ashraf, C.M.; Krishnamurthy, A.; Kumar, C.G. Accessory Mandibular Foramina: Prevalence, embryological basis and surgical implications. Journal of Clinical and Diagnostic Research 2011, 5, 1137–1139. [Google Scholar]
- Freire, A.R.; Rossi, A.C.; Prado, F.B.; Caria, P.H.F.; Botacin, P.R. Incidence of the mandibular accessory foramina in Brazilian population. J Morphol Sci. 2012, 29, 171–173. [Google Scholar]
- Samanta, P.P.; Kharb, P. Morphometric analysis of mandibular foramen and incidence of accessory mandibular foramina in adult human mandibles of an Indian population. Rev Arg de Anat Clin. 2013, 5, 60–66. [Google Scholar] [CrossRef]
- Padmavathi, G.; Tiwari, S.; Varalakshmi, K.L.; Roopashree, R. An anatomical study of mandibular and accessory mandibular foramen in dry adult human mandibles of South Indian Origin. IOSR Journal of Dental and Medical Sciences 2014, 13, 83–88. [Google Scholar] [CrossRef]
- Patra, S.; Nayak, S.; Pradhan, S.; Bara, D.; Mohapatra, C. Incidence and localisation of accessory mandibular foramen in east Indian population-a single centre experience. Indian J Applied Res. 2015, 5, 664–66. [Google Scholar]
- Raghavendra, V.P.; Benjamin, W. Position of mandibular foramen and incidence of accessory mandibular foramen in dry mandibles. Int J Pharm Bio Sci. 2015, 6, 282–288. [Google Scholar]
- Gopalakrishna, K.; Deepalaxmi, S.; Somashekara, S.C.; Rathna, B.S. An anatomical study on the position of mandibular foramen in 100 dry mandibles. International Journal of Anatomy and Research 2016, 4, 1967–71. [Google Scholar] [CrossRef]
- Hoque, M.; Ara, S.; Begum, S.; Kamal, S.; Islam, S.A. Incidence of Accessory Mandibular Foramen in Dry Adult Human Mandible. Bangladesh Journal of Anatomy 2016, 14, 43–44. [Google Scholar] [CrossRef]
- Lima, F.J.C.; Oliveira Neto, O.B.; Barbosa, F.T.; Dantas, L.C.; Olave, E.; Sousa-Rodriguez, F.C. Occurrence of the accessory foramina of the mandibular ramus in Brazilian adults and its relation to important mandibular landmarks. Int J Morhpol 2016, 34, 33–334. [Google Scholar] [CrossRef]
- Shalini, R.; RaviVarman, C.; Manoranjitham, R.; Veeramuthu, M. Morphometric study on mandibular foramen and incidence of accessory mandibular foramen in mandibles of south Indian population and its clinical implications in inferior alveolar nerve block. Anat Cell Biol. 2016, 49, 241–248. [Google Scholar] [CrossRef]
- Sultana, Q.; Sharif, M.H.; Avadhani, R. Study of surgical landmarks of mandibular foramen for inferior alveolar nerve block: An osteological study. Indian Journal of Clinical Anatomy and Physiology 2016, 3, 37–40. [Google Scholar] [CrossRef]
- Goyal, N.; Sharma, M.; Miglani, R.; Garg, Al.; Gupta, P.K. Clinical significance of accessory foramina in adult human mandible. International Journal of Research in Medical Sciences. 2017, 5, 2449–2453. [Google Scholar] [CrossRef]
- Rajkumari, K.; Nongthombam, S.S.; Chongtham, R.S.; Huidrom, S.D.; Tharani, R.; Sanjenbam, S.D. A morphometric study of the mandibular foramen in dry adult human mandibles – a study in RIMS, Imphal. IOSR Journal of Dental and Medical Sciences 2017, 16, 39–45. [Google Scholar] [CrossRef]
- Asdullah, M.; Ansari, M.M.; Khan, M.M.; Salati, N.A.; Khawja, K.J.; Sachdev, A.S. Morphological variations of lingula and prevalence of accessory mandibular foramina in mandibles. Natl J Maxillofac Surg. 2018, 9, 129–33. [Google Scholar]
- Mathur, S.; Joshi, P. A study of incidence of accessory mandibular foramina in dry mandibles of Rajasthan State. International Journal of Research and Review 2018, 5, 1–6. [Google Scholar]
- Sarkar, A. A morphometric study of mandibular foramen and accessory mandibular foramina in adult human mandibles and its clinical implications. International Journal of Developmental Research 2013, 8, 23575–23578. [Google Scholar]
- Pal, A.; Mandal, T.; Ghosal, A.K. Mandibular and Accessory Mandibular Foramen – an anatomical study in dry adult human mandibles of eastern India. Indian Journal of Basic and Applied Medical Research 2018, 8, 7–12. [Google Scholar]
- Dave, U.H.; Gupta, S.; Astik, R.B. Cross sectional analysis of occurrence of accessory mandibular foramina and their positional variations in dry mandibles. International Journal of Anatomy and Research 2019, 7, 6035–39. [Google Scholar] [CrossRef]
- Kuperappa, V.; Khan, T.A. Study of distribution of various accessory foramina in 100 human mandibles of South India. International Journal of Anatomy and Research 2019, 7, 6423–36. [Google Scholar] [CrossRef]
- Mondal, M.; Mukhopadhyay, P. A morphometric study of mandibular foramen and incidence of accessory mandibular foramen in dry adult human mandible and its clinical significance. Indian Journal of Basic and Applied Medical Research 2019, 8, 338–345. [Google Scholar]
- Nayak, G.; Sahoo, N.; Panda, S. Accessory mandibular foramina and bifid mandibular canals – an anatomical study. Eur J Anat 2019, 23, 261–266. [Google Scholar]
- Chandan, C.B.; Akhtar, M.J.; Kumar, A.; Sinha, R.R.; Kumar, N.; Kumar, A. Morphological study of accessory foramina in dry mandible and its clinical significance. International Journal of Medical Research Professionals 2020, 6, 90–93. [Google Scholar]
- Singh, A.; Zaidi, S.H.H.; Gupta, R. A study of accessory mandibular foramina in north Indian mandibles. International Journal of Recent Trends in Science and Technology 2020, 10, 58–61. [Google Scholar]
- Thunyacharoen, S.; Lymkhanakhom, S.; Chantakhat, P.; Suwanin, S.; Sawanprom, S.; Iamaroon, A.; Janhom, A.; Mahakkanukrauh, P. An anatomical study on locations of the mandibular foramen and the accessory mandibular foramen in the mandible and their clinical implication in a Thai population. Anat Cell Biol. 2020, 53, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Mistry, P.N.; Rajguru, J.; Dave, M.R. Study of the accessory mandibular foramina in dry adult human mandibles and their clinical and surgical implications. International Journal of Anatomy, Radiology and Surgery 2021, 10, AO16–AO19. [Google Scholar] [CrossRef]
- Induja, M.P.; Chokkattu, J.J. Analysis of various accessory foramina in mandible. International Journal of Health Sciences 2022, 6, 11944–11949. [Google Scholar] [CrossRef]
- Shwetha, K.; Ravishankar, M.V.; Vidya, C.S.; Pushpalatha, K.; Dakshayani, K.R. A study of the morphology of retromolar, mandibular, and accessory mandibular foramen in dry mandibles belonging to the Southern part of Karnataka state and their clinical significance. Journal of Krishna Institute of Medical Sciences University 2022, 11, 36–45. [Google Scholar]
- Adalarasan, S.; Devi, L.; Ps, S. Morphometric Study on the Mandibular Foramen. Cureus 2024, 16, e70862. [Google Scholar] [CrossRef]
- Bandlamudi, S.; Pavithra, M.; Subramanian, M.; Mariappan, A.S.; Yoganandham, J. Location of mandibular foramen in dry mandibles in relation to various anatomical landmarks. IP International Journal of Maxillofacial Imaging 2024, 10, 14–19. [Google Scholar] [CrossRef]
- Sakalem, M.E.; Sestario, C.S.; Motta, A.L.; Quintihano, D.; Myszynski, S.L.; Sato, V.A.H. Anatomical variations of the human mandible and prevalence of duplicate mental and mandibular foramina in the collection of the State University of Londrina. Translational Research in Anatomy 2024, 37, 100357. [Google Scholar] [CrossRef]
- Sujatha, A.; Charitha, G.N.; Indira, T.; Nisha Parveen, C.B.; Rani, S.T. Positional variations and morphometry of mandibular foramen in adult dry human mandibles. Int J Med Pub Health 2024, 14, 765–769. [Google Scholar]
- Singh, Y.; Shakya, P.; Saba, N.U.; Singh, H.; Kumar, N. A Morphometric Study of the Mandibular Foramen, Lingula, and the Incidence of Accessory Mandibular Foramina in Dry Mandibles. Cureus 2025, 17, e81087. [Google Scholar] [CrossRef] [PubMed]
- Tshite, K.; Olaleye, O. Location of mandibular foramen in adult black South African population: A morphometric analysis and investigation into possible radiographic correlation. South African Dental Journal. 2024, 79, 191–198. [Google Scholar] [CrossRef]
- Charalampakis, A.; Kourkoumelis, G.; Psari, C.; Antoniou, V.; Piagkou, M.; Demesticha, T.; Kotsiomitis, E.; Troupis, T. The position of the mental foramen in dentate and edentulous mandibles: Clinical and surgical relevance. Folia Morphol. 2017, 76, 709–714. [Google Scholar] [CrossRef]
- Pramstraller, M.; Schincaglia, G.P.; Vecchiatini, R.; Farina, R.; Trombelli, L. Alveolar ridge dimensions in mandibular posterior regions: a retrospective comparative study of dentate and edentulous sites using computerized tomography data. Surg Radiol Anat. 2018, 40, 1419–1428. [Google Scholar] [CrossRef]
- Naitoh, M; Hiraiwa, Y; Aimiya, H; Ariji, E. Observation of bifid mandibular canal using cone-beam computerized tomography. Int J Oral Maxillofac Implants 2009, 24, 155–9. [Google Scholar]
- Wadu, S.G.; Penhall, B.; Townsend, G.C. Morphological variability of the human inferior alveolar nerve. Clin Anat. 1997, 10, 82–7. [Google Scholar] [CrossRef]
- Kuribayashi, A.; Watanabe, H.; Imaizumi, A.; Tantanapornkul, W.; Katakami, K.; Kurabayashi, T. Bifid mandibular canals: cone beam computed tomography evaluation. Dentomaxillofac Radiol. 2010, 39, 235–9. [Google Scholar] [CrossRef]
- Gumussoy, I.; Demirezer, K.; Duman, S.B.; Haylaz, E.; Bayrakdar, I.S.; Celik, O.; Syed, A.Z. AI-powered segmentation of bifid mandibular canals using CBCT. BMC Oral Health 2025, 25, 907. [Google Scholar] [CrossRef]
- Jindanil, T; Fontenele, RC; de-Azevedo-Vaz, SL; Lahoud, P; Neves, FS; Jacobs, R. Artificial intelligence-based incisive canal visualization for preventing and detecting post-implant injury, using cone beam computed tomography. Int J Oral Maxillofac Surg. 2025, 54, 769–776. [Google Scholar] [CrossRef]
- Skrzat, J.; Ryniewicz, W.; Goncerz, G.; Kozerska, M. Anatomical features of the mandibular foramen and their clinical significance – review of the literature. Folia Medica Cracoviensia 2023, 63, 157–170. [Google Scholar] [CrossRef]
- Yameen, M.; Modi, V. Morphometric variation of mandibular foramina with related accessory foramina in dry adult human mandibles and its possible clinical significance. International Journal of Research Publication and Reviews 2024, 5, 3094–3101. [Google Scholar]
- Varvara, G.; Feragalli, B.; Turkyilmaz, I.; D’Alonzo, A.; Rinaldi, F.; Bianchi, S.; Piattelli, M.; Macchiarelli, G.; Bernardi, S. Prevalence and Characteristics of Accessory Mandibular Canals: A Cone-Beam Computed Tomography Study in a European Adult Population. Diagnostics (Basel). 2022, 12, 1885. [Google Scholar] [CrossRef] [PubMed]
- Okiriamu, A.; Butt, F.; Opondo, F.; Onyango, F. Morphology and Variant Anatomy of the Mandibular Canal in a Kenyan Population: A Cone-Beam Computed Tomography Study. Craniomaxillofacial Research & Innovation 2023, 8. [Google Scholar] [CrossRef]
- Rajchel, J.; Ellis, E., 3rd; Fonseca, R.J. The anatomical location of the mandibular canal: its relationship to the sagittal ramus osteotomy. Int J Adult Orthodon Orthognath Surg. 1986, 1, 37–47. [Google Scholar]
- Patil, S.; Matsuda, Y.; Okano, T. Accessory mandibular foramina: a CT study of 300 cases. Surg Radiol Anat. 2013, 35, 323–30. [Google Scholar] [CrossRef]
Figure 1.
Wire used to determine the diameter of accessory mandibular foramina.
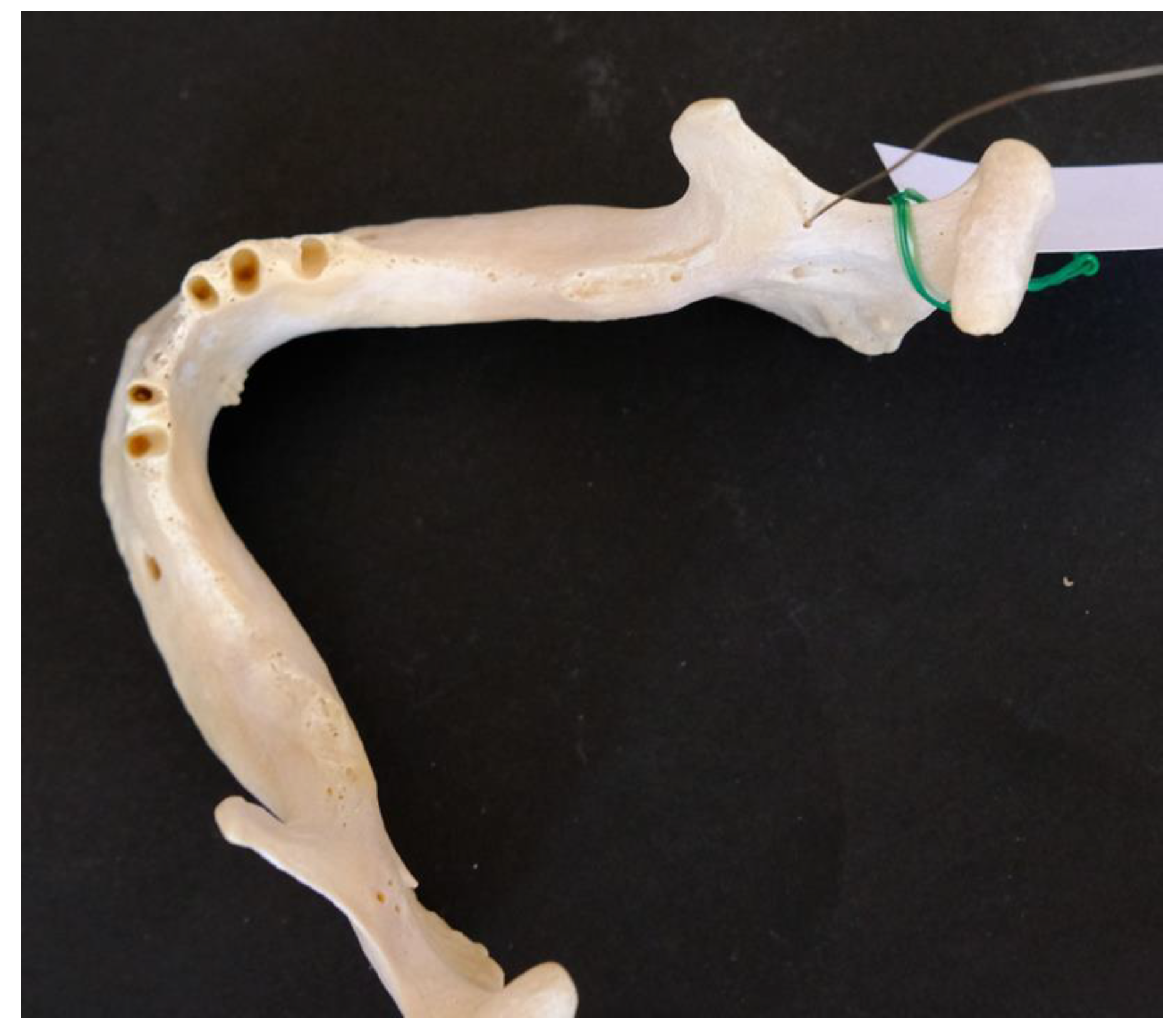
Figure 2.
Measurements were performed using a digimatic caliper.

Figure 3.
Measurements protocol.
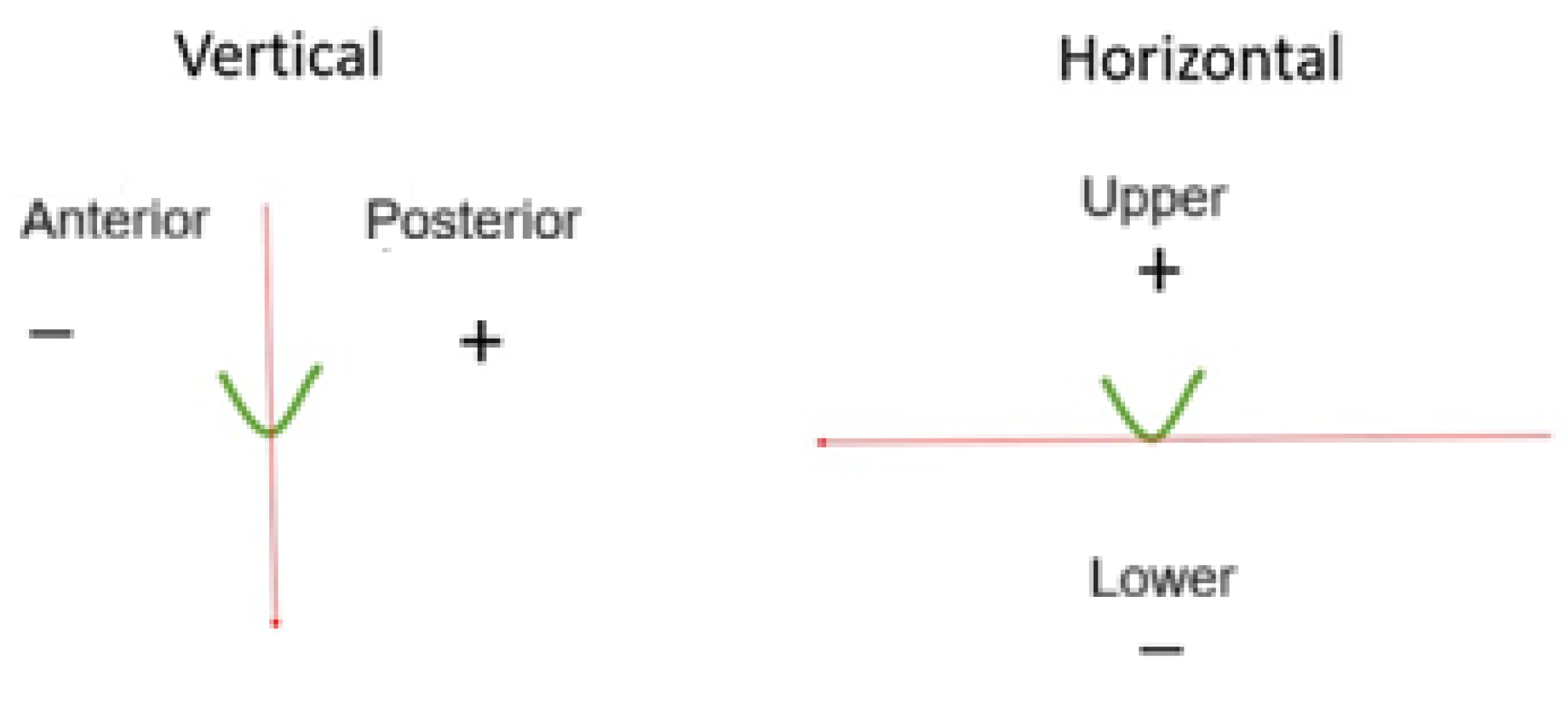
Figure 4.
A single accessory mandibular foramen indicated by red arrow.
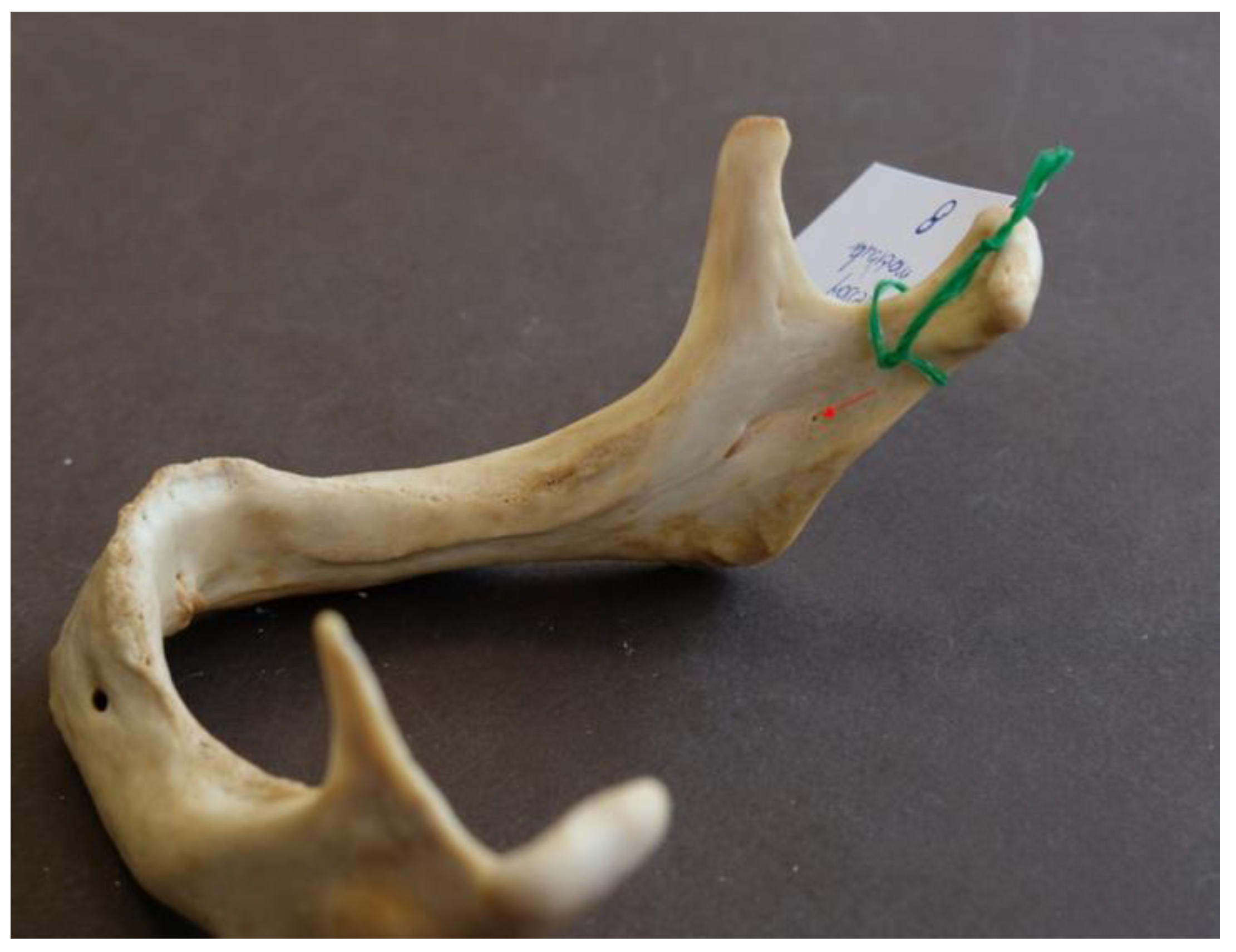
Figure 5.
Two accessory mandibular foramina indicated by red arrow.

Figure 6.
Three accessory mandibular foramina indicated by red arrow.

Figure 7.
Five accessory mandibular foramina indicated by red arrow.
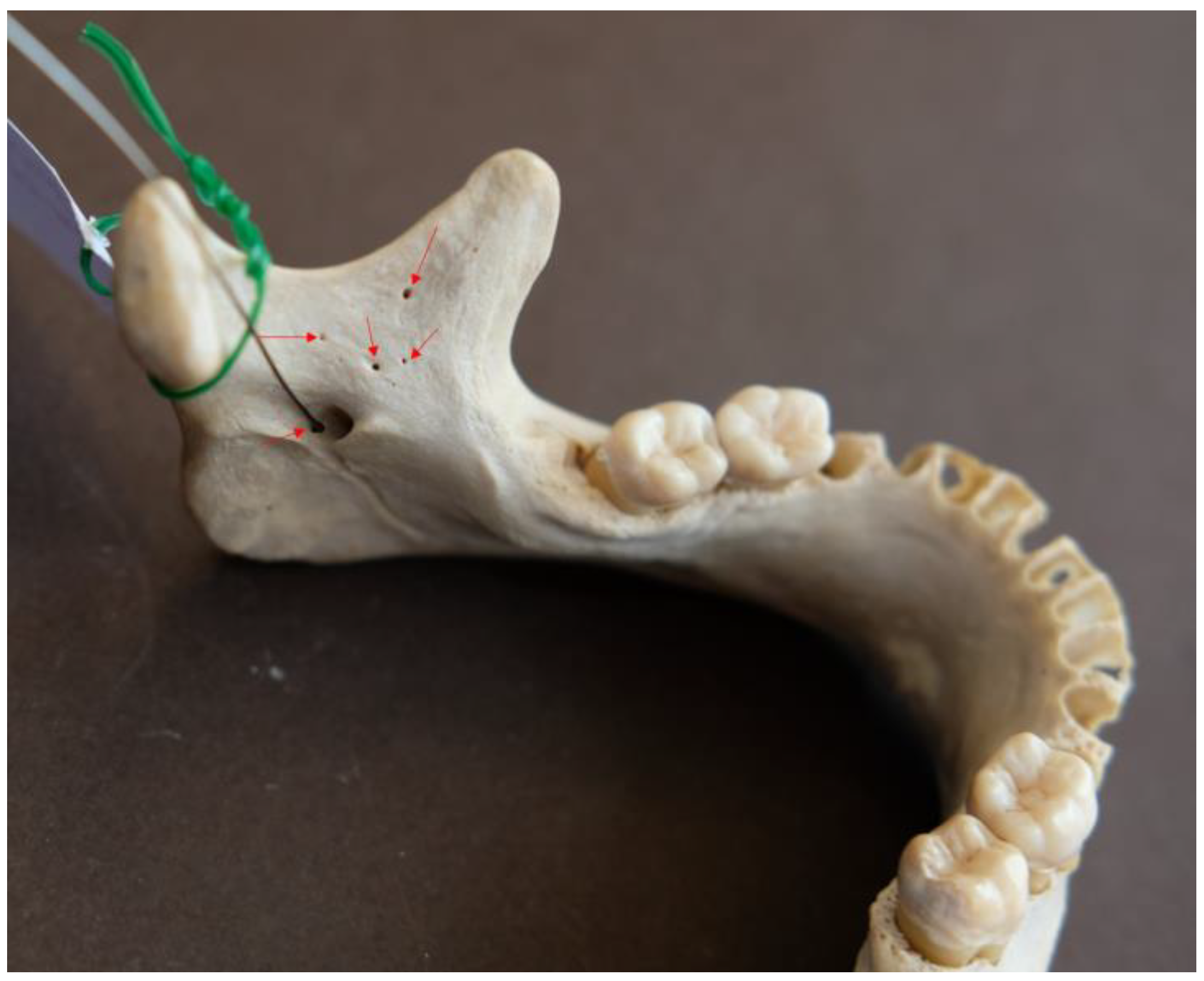
Figure 8.
Accessory mandibular foramen very close to the main foramen indicated by red arrow.

Figure 9.
Grouped scattergram depicting vertical vs horizontal distance of AMaFs from mandibular foramen after two step cluster analysis: two discrete clusters (lower-proximal AMaFs: green circle; upper-distal AMaFs: red circle) determine the direction and radius of IAN anesthesia.
Figure 9.
Grouped scattergram depicting vertical vs horizontal distance of AMaFs from mandibular foramen after two step cluster analysis: two discrete clusters (lower-proximal AMaFs: green circle; upper-distal AMaFs: red circle) determine the direction and radius of IAN anesthesia.
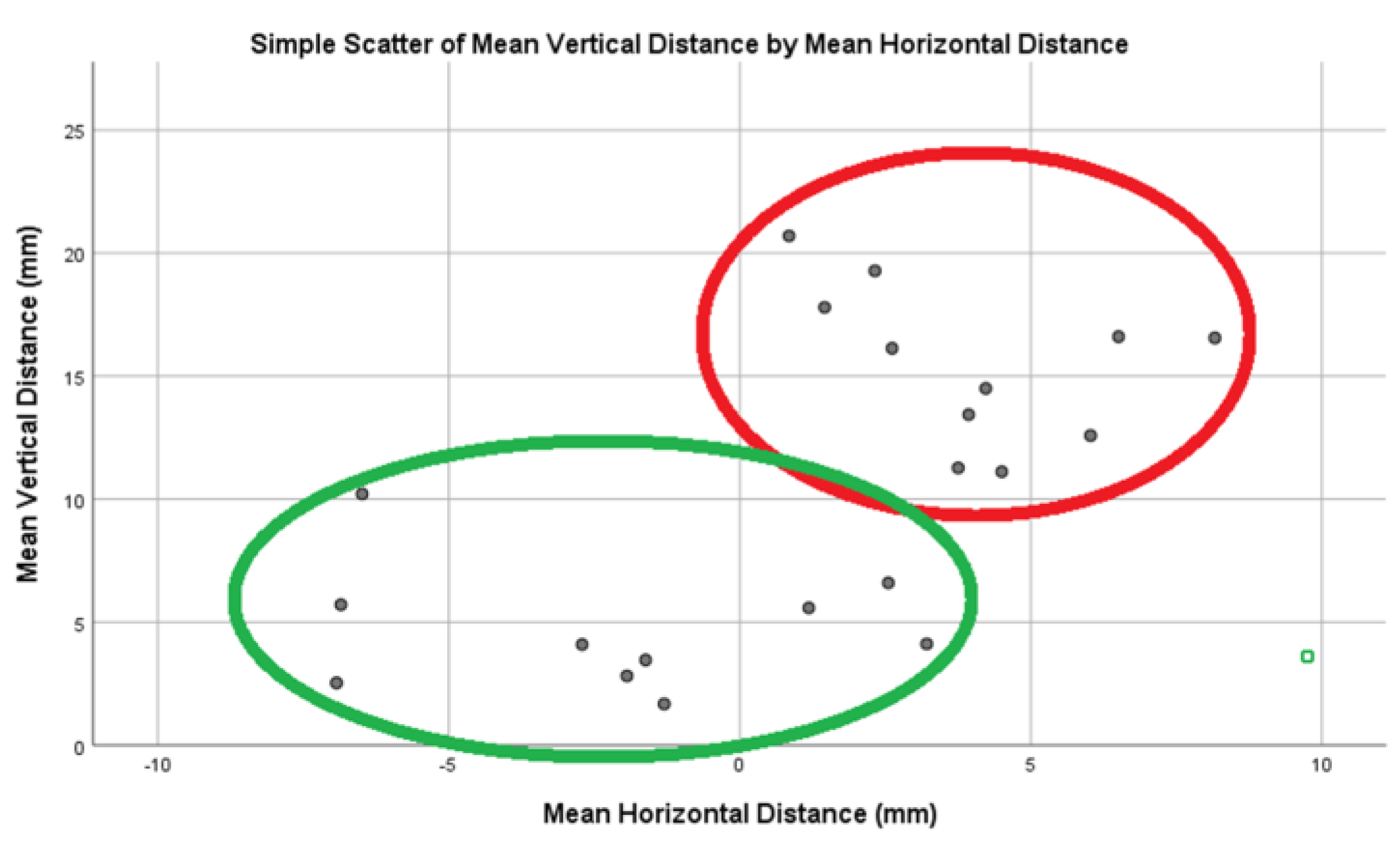
Figure 10.
PRISMA flow diagram of the present meta-analysis.
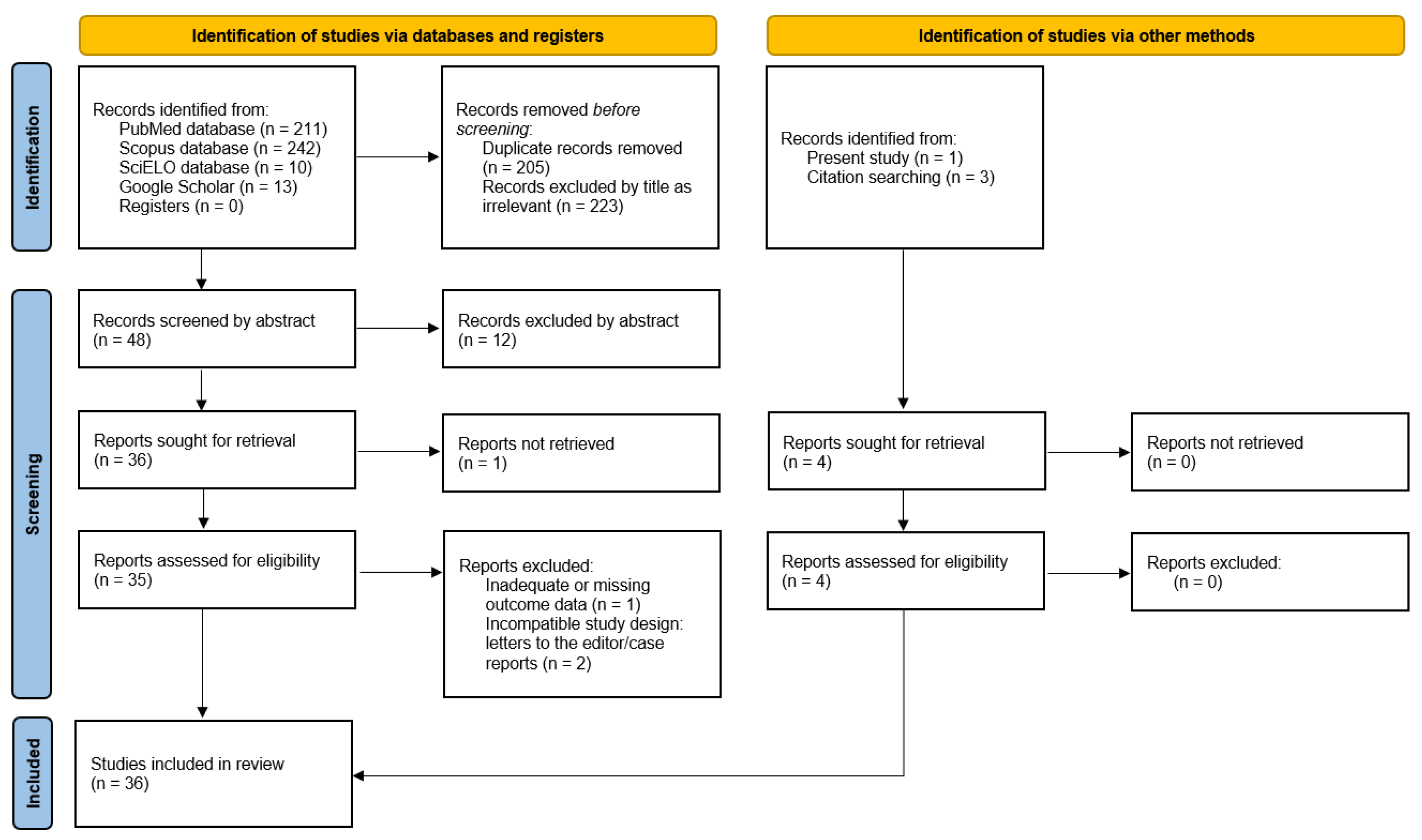
Figure 11.
Absence of AMaFs in mandibles; forest plot.
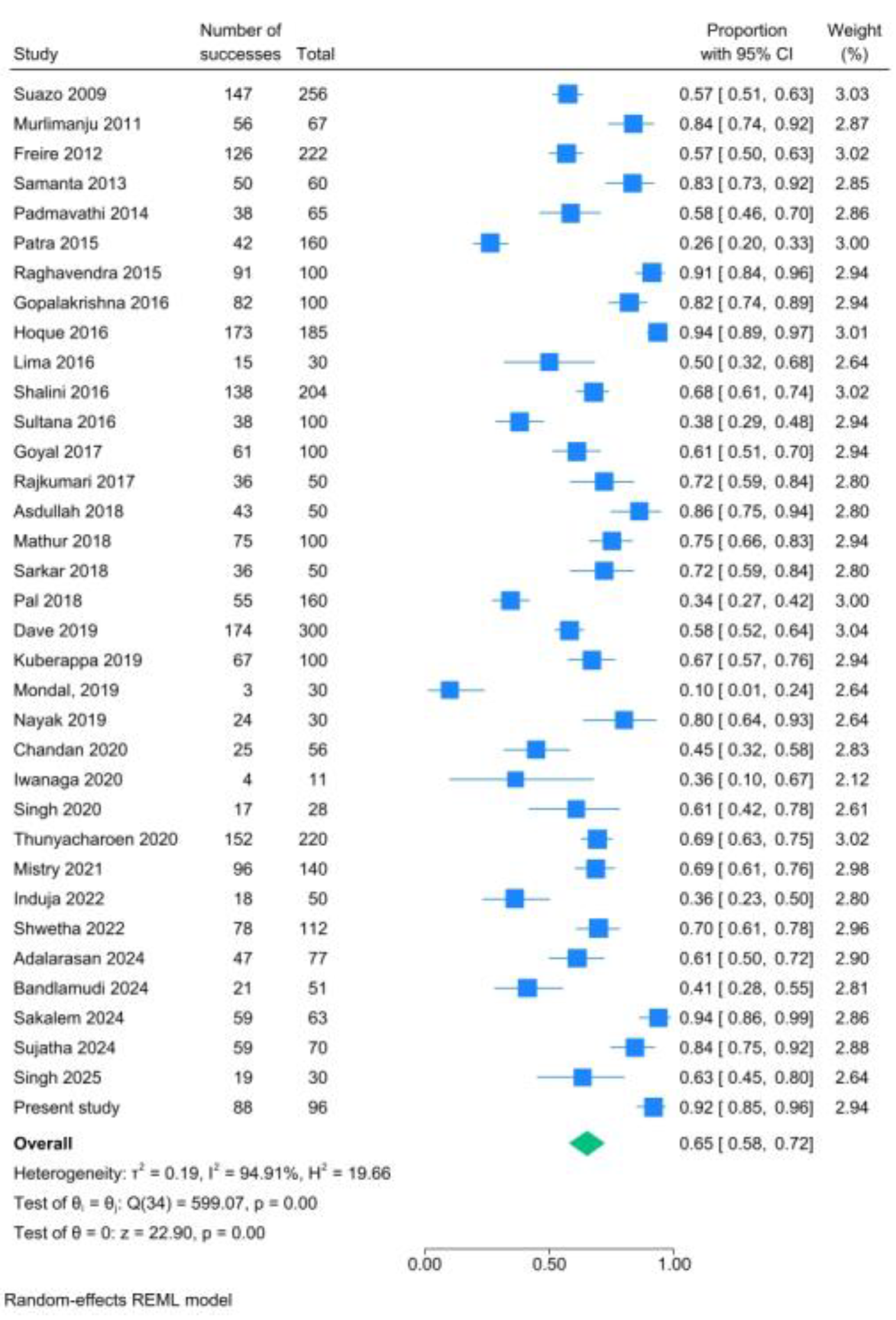
Figure 12.
Unilateral presence of AMaFs in mandibles; forest plot.
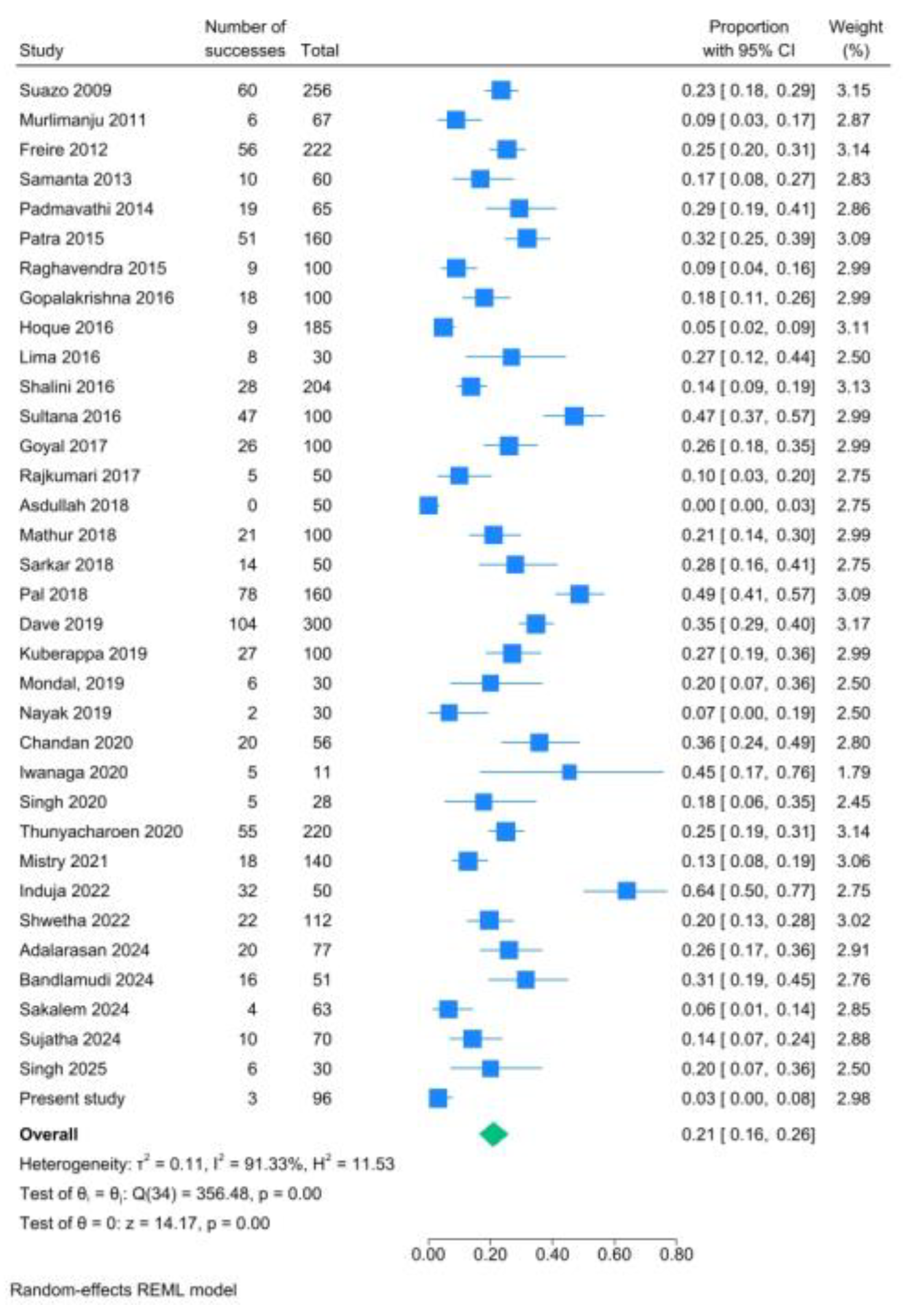
Figure 13.
Bilateral presence of AMaFs in mandibles; forest plot.
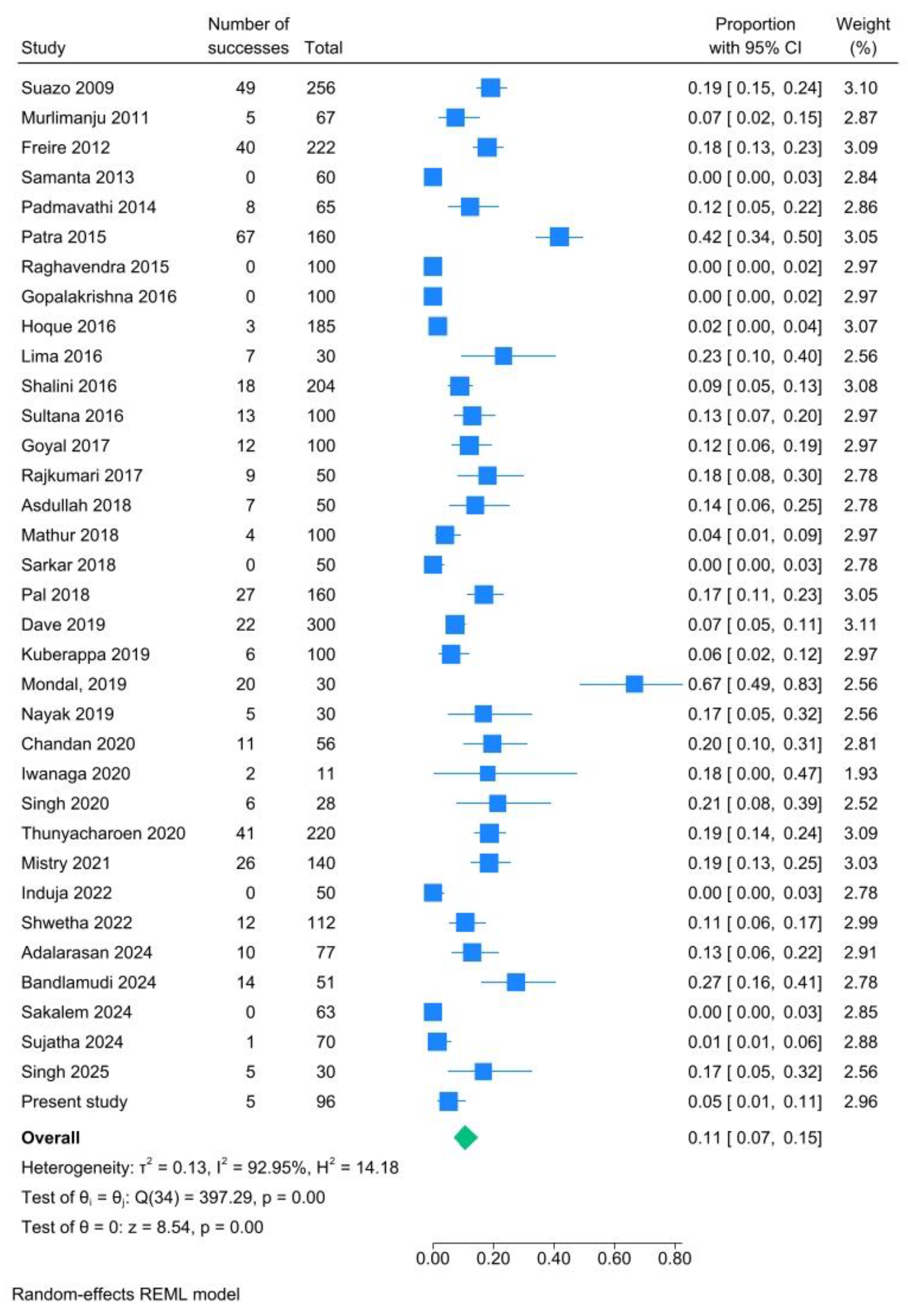
Figure 14.
Presence of multiple AMaFs in mandibles; forest plot.
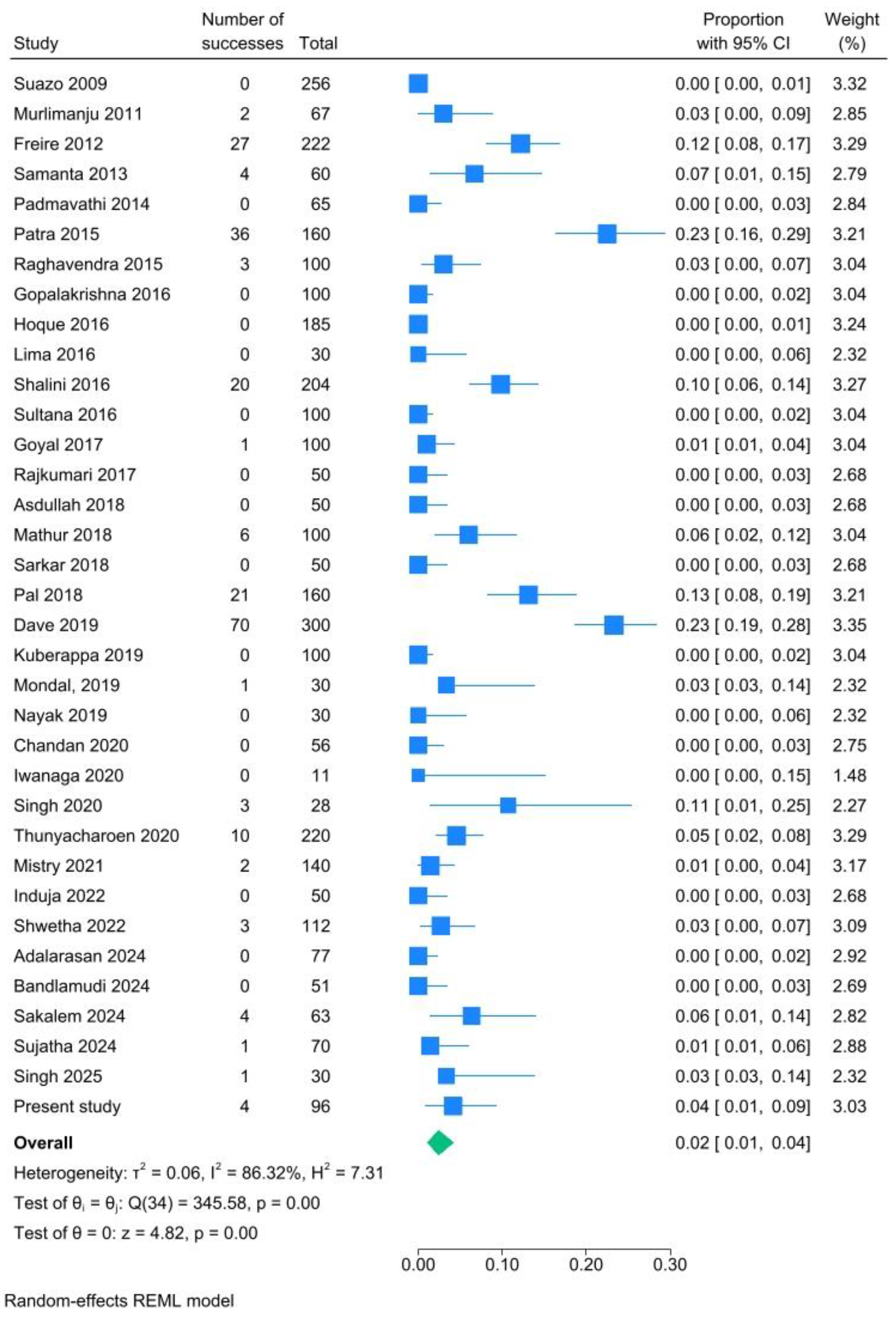
Figure 15.
Prevalence of AMaFs per hemimandibles; subgroup analysis (Indian vs non-Indian descent) forest plot.
Figure 15.
Prevalence of AMaFs per hemimandibles; subgroup analysis (Indian vs non-Indian descent) forest plot.
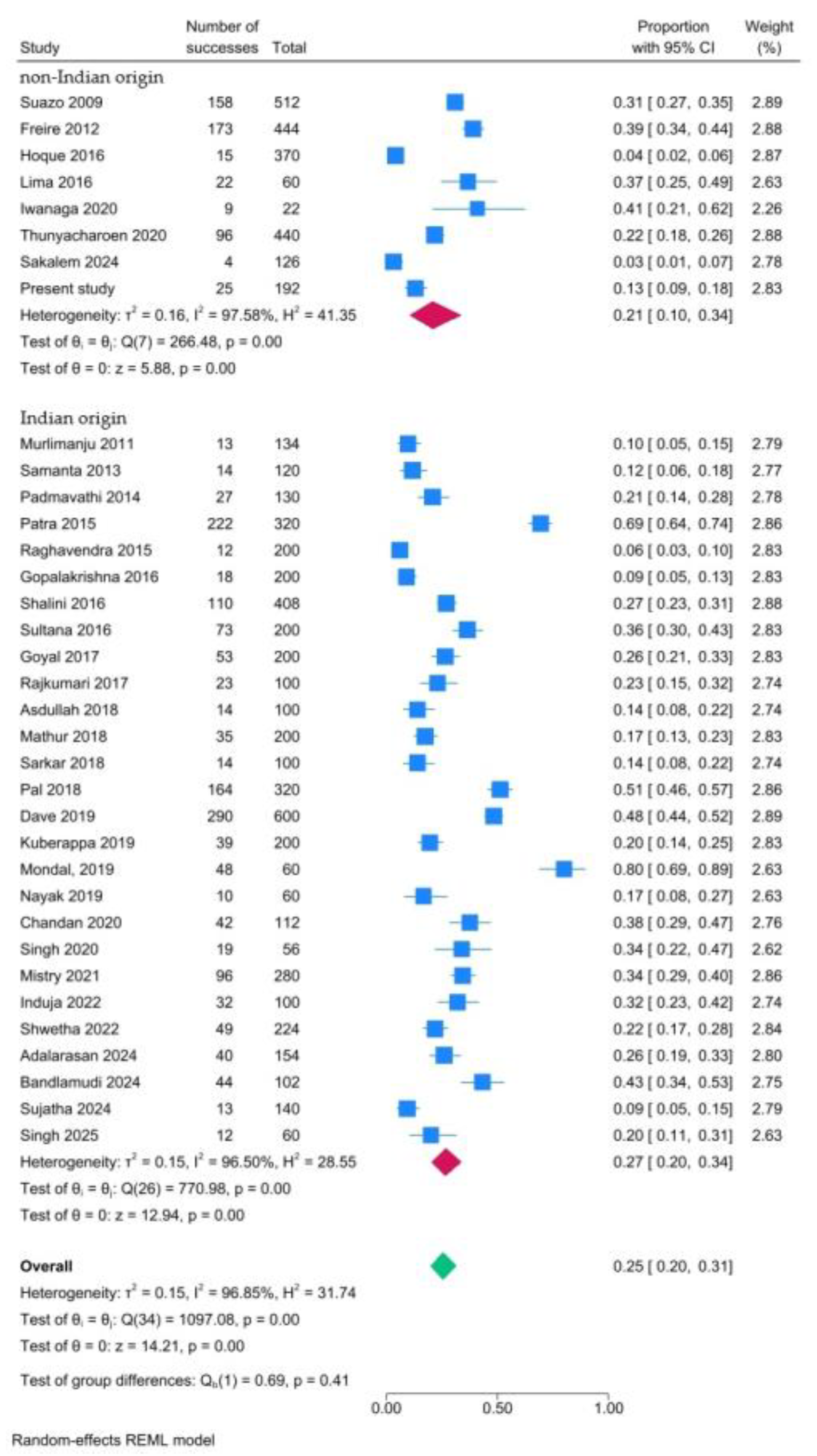
Figure 16.
Funnel plot.
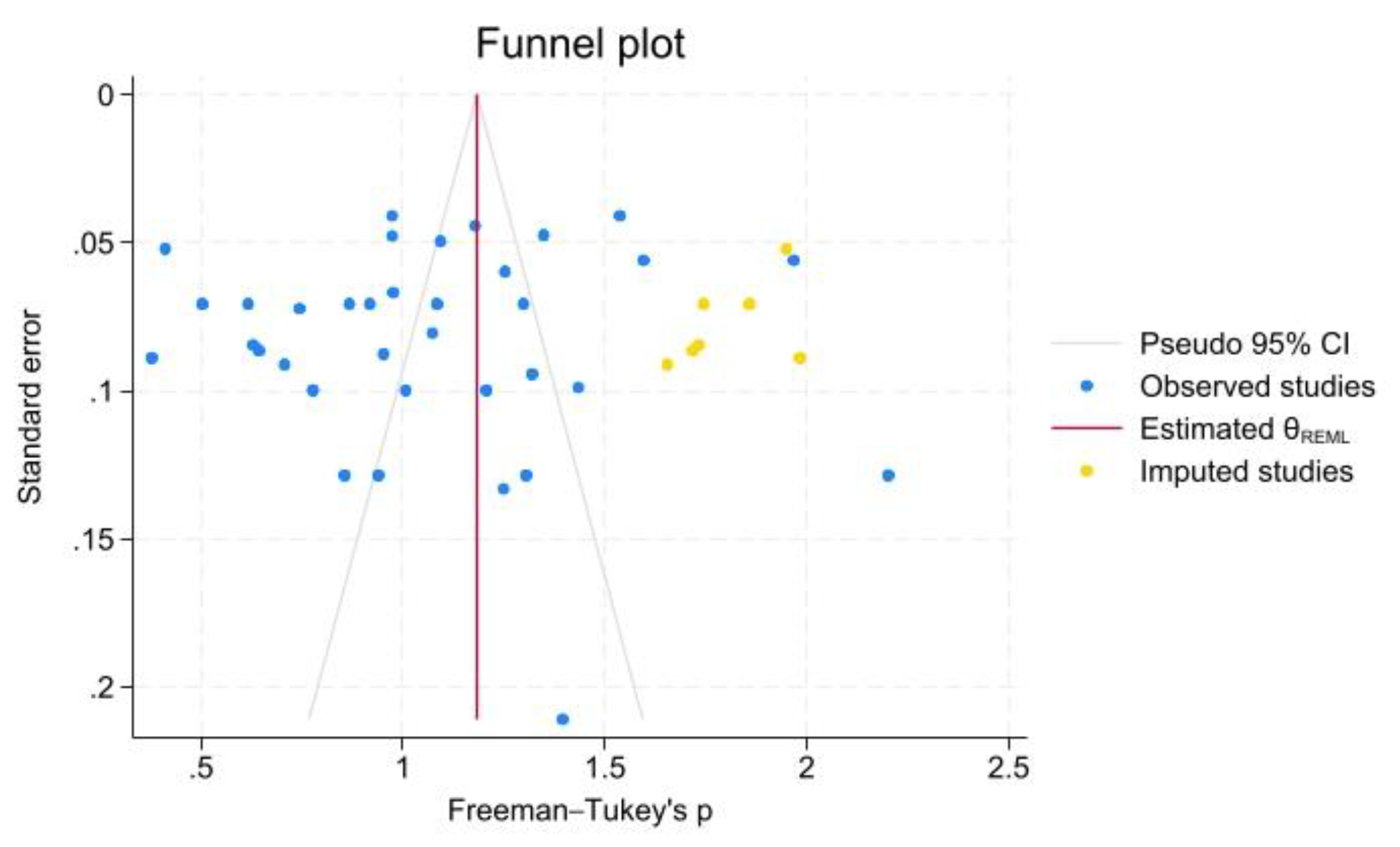
Figure 17.
Doi plot and Luis Furuja-Kanamori (LFK) index.
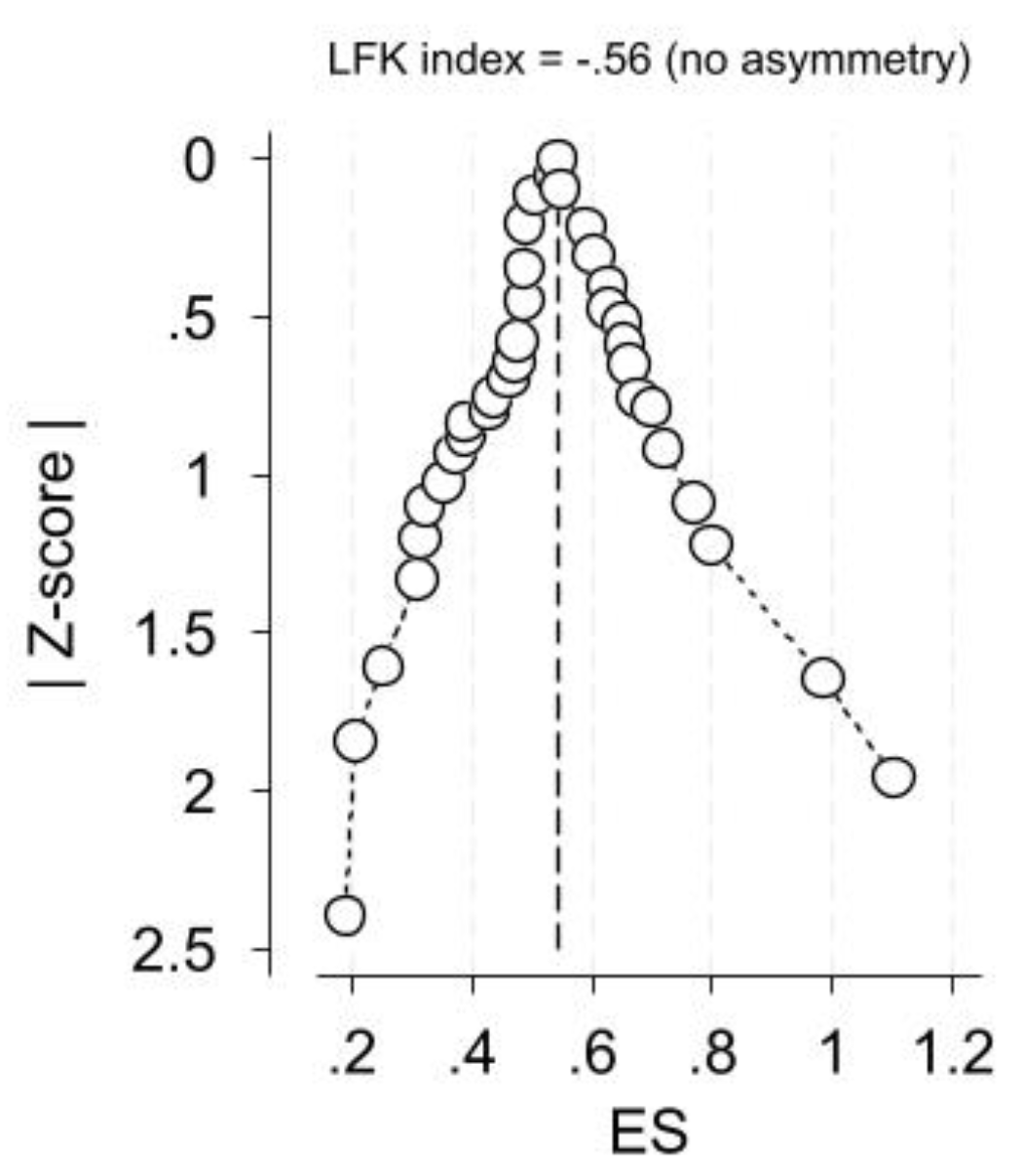

Table 1.
Included studies.
| Study | Origin | Material | Sample (No of mandibles) | Mandibles without AMaF | Mandibles with unilateral AMaF | Mandibles with bilateral AMaF | Mandibles with multiple AMaFs | Total number of AMaFs |
| Sutton 1974 [21] | Australia | DM | 300 | 131 | ||||
| Suazo 2009 [22] | Brazil | DM | 256 | 147 | 60 | 49 | 0 | 158 |
| Murlimanju 2011 [23] | India | DM | 67 | 56 | 6 | 5 | 2 | 13 |
| Freire 2012 [24] | Brazil | DM | 222 | 126 | 56 | 40 | 27 | 173 |
| Samanta 2013 [25] | India | DM | 60 | 50 | 10 | 0 | 4 | 14 |
| Padmavathi 2014 [26] | India | DM | 65 | 38 | 19 | 8 | 0 | 27 222 12 18 |
| Patra 2015 [27] | India | DM | 160 | 42 | 51 | 67 | 36 | |
| Raghavendra 2015 [28] | India | DM | 100 | 91 | 9 | 0 | 3 | |
| Gopalakrishna 2016 [29] | India | DM | 100 | 82 | 18 | 0 | 0 | |
| Hoque 2016 [30] | Bangladesh | DM | 185 | 173 | 9 | 3 | 0 | 15 |
| Lima 2016 [31] | Brazil | DM | 30 | 15 | 8 | 7 | 0 | 22 |
| Shalini 2016 [32] | India | DM | 204 | 138 | 28 | 18 | 20 | 110 |
| Sultana 2016 [33] | India | DM | 100 | 38 | 47 | 13 | 0 | 73 |
| Goyal 2017 [34] | India | DM | 100 | 61 | 26 | 12 | 1 | 53 |
| Rajkumari 2017 [35] | India | DM | 50 | 36 | 5 | 9 | 0 | 23 |
| Asdullah 2018 [36] | India | DM | 50 | 43 | 0 | 7 | 0 | 14 |
| Mathur 2018 [37] | India | DM | 100 | 75 | 21 | 4 | 6 | 35 |
| Sarkar 2018 [38] | India | DM | 50 | 36 | 14 | 0 | 0 | 14 |
| Pal 2018 [39] | India | DM | 160 | 55 | 78 | 27 | 21 | 164 |
| Dave 2019 [40] | India | DM | 300 | 174 | 104 | 22 | 70 | 290 |
| Kuberappa 2019 [41] | India | DM | 100 | 67 | 27 | 6 | 0 | 39 |
| Mondal, 2019 [42] | India | DM | 30 | 3 | 6 | 20 | 1 | 48 |
| Nayak 2019 [43] | India | DM | 30 | 24 | 2 | 5 | 0 | 10 |
| Chandan 2020 [44] | India | DM | 56 | 25 | 20 | 11 | 0 | 42 |
| Iwanaga 2020 [6] | Japan | FFC | 11 | 4 | 5 | 2 | 0 | 9 |
| Singh 2020 [45] | India | DM | 28 | 17 | 5 | 6 | 3 | 19 |
| Thunyacharoen 2020 [46] | Thailand | DM | 220 | 152 | 55 | 41 | 10 | 96 |
| Mistry 2021 [47] | India | DM | 140 | 96 | 18 | 26 | 2 | 96 |
| Induja 2022 [48] | India | DM | 50 | 18 | 32 | 0 | 0 | 32 |
| Shwetha 2022 [49] | India | DM | 112 | 78 | 22 | 12 | 3 | 49 |
| Adalarasan 2024 [50] | India | DM | 77 | 124 | 20 | 10 | 0 | 40 |
| Bandlamudi 2024 [51] | India | DM | 51 | 21 | 16 | 14 | 0 | 44 |
| Sakalem 2024 [52] | Brazil | DM | 63 | 59 | 4 | 0 | 4 | 4 |
| Sujatha 2024 [53] | India | DM | 70 | 59 | 10 | 1 | 1 | 13 |
| Singh 2025 [54] | India | DM | 30 | 19 | 6 | 5 | 1 | 12 |
| Present study | Greece | DM | 96 | 88 | 3 | 5 | 4 | 25 |
DM: Dry Mandibles; FFC: Fresh Frozen Cadavers.
Table 2.
Quality assessment of the included studies using the AQUA tool.
| Study | Domain 1: Objectives and study characteristics | Domain 2: Study design | Domain 3: Methodology characterization | Domain 4: Descriptive anatomy | Domain 5: Reporting of results | Quality assessment |
| Sutton 1974 [21] | Unclear | Low | Low | Unclear | Low | Medium |
| Suazo 2009 [22] | Low | Low | Low | Low | Low | High |
| Murlimanju 2011 [23] | Low | Low | Low | Low | Low | High |
| Freire 2012 [24] | Unclear | Low | Low | Low | Low | High |
| Samanta 2013 [25] | Unclear | Low | Unclear | Low | Low | Medium |
| Padmavathi 2014 [26] | Unclear | Low | Low | Low | Low | High |
| Patra 2015 [27] | Unclear | Low | Unclear | Low | Low | Medium |
| Raghavendra 2015 [28] | Unclear | Low | Unclear | Low | Low | Medium |
| Gopalakrishna 2016 [29] | Unclear | Low | Unclear | Low | Low | Medium |
| Hoque 2016 [30] | Unclear | Low | Unclear | Low | Low | Medium |
| Lima 2016 [31] | Unclear | Low | Low | Low | Low | High |
| Shalini 2016 [32] | Unclear | Low | Low | Low | Low | High |
| Sultana 2016 [33] | Unclear | Low | Low | Low | Low | High |
| Goyal 2017 [34] | Unclear | Low | Unclear | Low | Low | Medium |
| Rajkumari 2017 [35] | Unclear | Low | Low | Low | Low | High |
| Asdullah 2018 [36] | Unclear | Low | Unclear | Low | Low | Medium |
| Mathur 2018 [37] | Unclear | Low | Unclear | Low | Low | Medium |
| Sarkar 2018 [38] | Unclear | Low | Low | Low | Low | High |
| Pal 2018 [39] | Unclear | Low | Unclear | Low | Low | Medium |
| Dave 2019 [40] | Unclear | Low | Unclear | Low | Low | Medium |
| Kuberappa 2019 [41] | Unclear | Low | Unclear | Low | Low | Medium |
| Mondal, 2019 [42] | Unclear | Low | Unclear | Low | Low | Medium |
| Nayak 2019 [43] | Low | Low | Unclear | Low | Low | High |
| Chandan 2020 [44] | Unclear | Low | Unclear | Low | Low | Medium |
| Iwanaga 2020 [6] | Low | Low | Low | Low | Low | High |
| Singh 2020 [45] | Unclear | Low | Unclear | Low | Low | Medium |
| Thunyacharoen 2020 [46] | Low | Low | Low | Low | Low | High |
| Mistry 2021 [47] | Unclear | Low | Unclear | Low | Low | Medium |
| Induja 2022 [48] | Unclear | Low | Low | Low | Unclear | Medium |
| Shwetha 2022 [49] | Unclear | Low | Low | Low | Low | High |
| Adalarasan 2024 [50] | Unclear | Low | Low | Low | Low | High |
| Bandlamudi 2024 [51] | Unclear | Low | Low | Low | Low | High |
| Sakalem 2024 [52] | Unclear | Low | Low | Low | Low | High |
| Sujatha 2024 [53] | Unclear | Low | Low | Low | Low | High |
| Singh 2025 [54] | Unclear | Low | Low | Low | Low | High |
| Present study | Unclear | Low | Low | Low | Low | High |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



