
Submitted:
23 December 2025
Posted:
25 December 2025
You are already at the latest version
Abstract
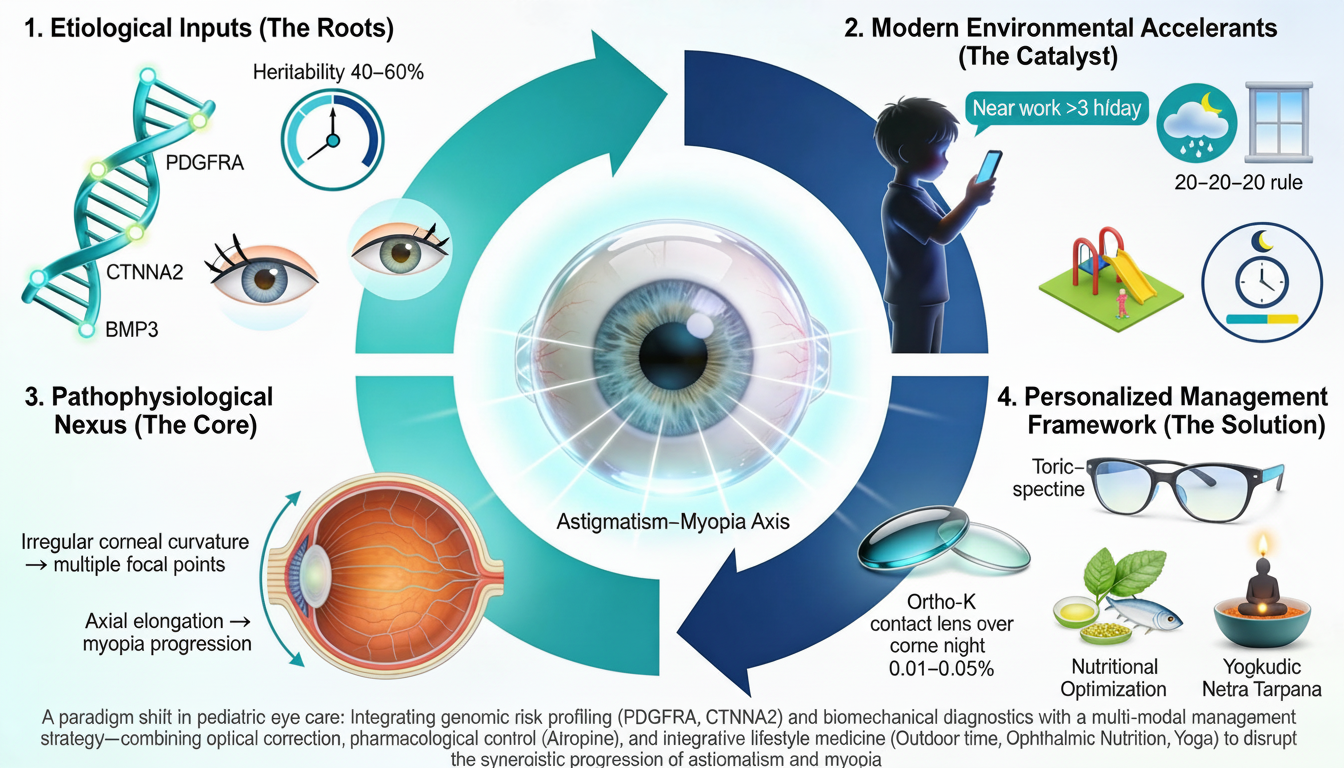
Astigmatism, a common refractive error characterized by an irregular corneal or lenticular curvature, represents a significant pediatric public health concern with profound implications for visual development and long-term ocular health. This review synthesizes contemporary evidence on the complex, multifactorial etiology of astigmatism, emphasizing its critical and synergistic relationship with myopia progression. We delineate the substantial genetic component, with heritability estimates of 40-60%, involving polygenic inheritance patterns and specific SNPs in loci such as PDGFRA and CTNNA2. The pathophysiology is further explored through physiological triggers, including extraocular muscle imbalance, dynamic eyelid pressure, and corneal biomechanical weakening. Modern environmental accelerants, notably prolonged near work and digital device usage, are examined for their role in disrupting emmetropization. The core thesis of this manuscript advocates for a paradigm shift towards early infantile screening and personalized, multi-modal intervention strategies. We critically evaluate conventional therapies (spectacles, toric contact lenses, orthokeratology), emerging pharmacological agents (low-dose atropine), and evidence-based lifestyle modifications (increased outdoor exposure, nutritional optimization). Furthermore, we explore the integration of advanced diagnostics (anterior-segment OCT, Scheimpflug tomography, genetic risk profiling) and complementary approaches like Nutritional optimization and traditional medicine systems, such as Ayurvedic Netra Tarpana and yogic eye exercises, within a holistic management framework. The convergence of genetic insights, advanced biometry, and personalized medicine heralds a new era in preventing astigmatism-related amblyopia and mitigating its role in axial elongation, ultimately preserving lifelong visual function.
Keywords:
1. Introduction
1.1. Background and Significance
1.2. Objectives of the Review
- Elucidate the complex, multifactorial etiology of pediatric astigmatism, integrating genetic, physiological, and environmental determinants.
- Critically analyze the pathophysiological link between astigmatism and accelerated myopia progression.
- Evaluate current and emerging diagnostic technologies for early detection and risk stratification.
- Synthesize evidence on conventional, pharmacological, and lifestyle-based management strategies.
- Explore the potential role of integrative and traditional medicine practices within a scientific framework.
- Propose a holistic, personalized management algorithm and identify future research directions to mitigate the lifelong impact of pediatric astigmatism.
2. Genetic Architecture and Heritability of Astigmatism
2.1. Polygenic Risk and Genome-Wide Association Studies (GWAS)
- PDGFRA (Platelet-Derived Growth Factor Receptor Alpha): Strongly associated with corneal curvature and astigmatism. This gene is crucial for neural crest cell migration and differentiation, which are fundamental to corneal and scleral development [Hideharu Fukasaku et al., 2023].
- ZC3H11B, BMP3, HERC2, PROX1-AS1: Other consistently identified genes involved in ocular development and connective tissue structure [ERICA SHING et al., 2025; Shing et al., 2024].
2.2. Heritability Estimates and Inheritance Patterns
2.3. Gene-Environment Interactions (GxE)
- High Genetic Risk + Adverse Environment: Children with high polygenic risk scores who engage in prolonged near work (>3 hours/day) demonstrate significantly faster astigmatism progression and axial elongation [Shah et al., 2025; Fan et al., 2016].
- Protective Environment Mitigates Genetic Risk: Sufficient daily outdoor exposure (≥2 hours) appears to exert a protective effect that can partially offset genetic susceptibility, likely mediated by dopamine release and regulation of ocular growth signals [Biswas et al., 2024].
- Epigenetic Modifications: Environmental exposures (e.g., nutrition, pollution, light exposure) can induce epigenetic changes (DNA methylation, histone modification) that alter the expression of genes involved in eye growth without changing the DNA sequence itself, providing a mechanistic link between lifestyle and astigmatism progression [An et al., 2023].
3. Physiological and Biomechanical Triggers
3.1. Extraocular Muscle Imbalance and Orbital Mechanics
3.2. Eyelid Pressure and Blink Dynamics
- Eyelid Morphology: Individuals with wider palpebral apertures, lower lid positions, or conditions like ptosis (droopy eyelid) exhibit characteristic corneal flattening in the meridian perpendicular to the lid axis, often worsening pre-existing astigmatism [Lieberman et al., 2000; Read, Scott, Collins, Michael, & Carney, Leo, 2007].
- Digital Device Use: Prolonged downward gaze during smartphone/tablet use increases the contact area and pressure of the upper eyelid, potentially driving the observed increase in astigmatism prevalence in the digital era [Kroczek Marta et al., 2025].
- Chronic Eye Rubbing: A significant risk factor for keratoconus, eye rubbing delivers high, irregular mechanical stress, degrading corneal collagen and destabilizing its architecture [Prasida Unni et al., 2023].
3.3. Corneal Biomechanics and Progressive Weakening
- Astigmatism Progression: In progressive astigmatism, often linked to subclinical keratoconus, localized biomechanical weakening occurs. This involves disruption of collagen cross-linking, altered proteoglycan composition, and enzymatic degradation (e.g., by matrix metalloproteinases), leading to reduced corneal hysteresis and increased deformability [David P. Piñero et al., 2011; Seyed-Farzad Mohammadi].
- Advanced Diagnostics: Devices like the Corneal Visualization Scheimpflug Technology (Corvis ST) and the Ocular Response Analyzer (ORA) provide in-vivo metrics of corneal biomechanics (e.g., corneal hysteresis, corneal resistance factor). These are critical for early detection of ectatic disorders and monitoring progression [Wang, 2025; Wei P. et al., 2025].
- Corneal Cross-Linking (CXL): This evidence-based treatment uses ultraviolet-A light and riboflavin to create new covalent bonds between collagen fibrils, stiffening the cornea and halting the progression of ectatic diseases like keratoconus [Shinde et al., 2020].
3.4. Biomarkers for Early Detection of Progression of Astigmatism and Related Consequences
4. Environmental Modulators and Lifestyle Factors
4.1. The Digital Environment: Near Work and Screen Time
- Prolonged Accommodation and Ciliary Spasm: Sustained near focusing demands can lead to accommodative spasm and altered intraocular pressure dynamics, potentially influencing globe shape [Bui et al., 2023].
- Reduced Blink Rate and Dry Eye: Concentrated screen use reduces blink rate by up to 60%, destabilizing the tear film, causing ocular surface inflammation, and creating an irregular optical surface that may feedback to influence corneal remodeling [Gordon-Shaag et al., 2015; Kaur et al., 2022].
- Postural Effects: Sustained downgaze increases eyelid pressure as described in Section 3.2.
- Blue Light and Oxidative Stress: While the direct role of blue light in astigmatism is debated, it can generate reactive oxygen species on the ocular surface, contributing to inflammation and tissue damage over time [Passaro et al., 2025; Zhi-Chun Zhao et al., 2018].
4.2. The Protective Role of Outdoor Time and Natural Light
- Mechanism: Bright outdoor light (illuminance often >10,000 lux vs. <500 lux indoors) stimulates retinal dopamine release. Dopamine acts as a stop signal for excessive axial elongation, the hallmark of myopia [Thomas T. Norton et al., 2013; Higuchi,S, 2024].
- Dose-Response: Evidence shows a clear dose-response relationship. Each additional hour of outdoor time per week can reduce myopia risk by approximately 2%. Implementing 40+ minutes of daily outdoor time at school has been shown to reduce the incidence of new myopia cases [Biswas, Sayantan et al.; Rose KA., 2008].
- Spectral Quality and Visual Scene: The broader visual scenery outdoors, with ample opportunities for distance viewing and varying accommodative demands, may also play a role in healthy emmetropization.
4.3. Nutrition, Systemic Health, and Sleep
-
Nutrition: A diet rich in antioxidants and anti-inflammatory compounds supports corneal integrity.
- Lutein & Zeaxanthin: Found in leafy greens, eggs, and goji berries, these macular pigments filter blue light and protect retinal cells [Bucheli et al., 2011; Li et al., 2018].
- Omega-3 Fatty Acids: From fish and walnuts, they support tear film quality and have anti-inflammatory properties [CG Optical, n.d.].
- Vitamins A, C, E: Critical for photoreceptor function, collagen synthesis (corneal strength), and antioxidant defense [Jang et al., 2017; Neha & Sanwalka, 2012].
-
lifestyle factors:
- Sleep: Inadequate sleep is an emerging risk factor. A study in preschoolers found children with insufficient sleep had nearly triple the odds of having astigmatism [Xixuan Zhao et al., 2025]. Sleep disruption may affect hormonal regulation of ocular growth and repair.
- Obesity and Inflammation: Childhood obesity is independently associated with a higher prevalence and severity of astigmatism, likely mediated by chronic systemic inflammation that can affect scleral and corneal tissues [Wang et al., 2025].
4.4. Integrative Ocular Dietary Protocols for Structural and Retinal Support and Health Benefits
5. Personalized and Integrative Management Strategies
5.1. Precision Medicine: Integrating Genetic Insights
- Risk Stratification: Utilizing Polygenic Risk Scores (PRS) for astigmatism and myopia enables the identification of high-risk children before significant refractive shifts occur, allowing for early, aggressive monitoring.
- Treatment Response Prediction: Evidence suggests that genetic variants may dictate how a child responds to specific interventions, such as orthokeratology or low-dose atropine, allowing clinicians to bypass trial-and-error and select the most effective modality initially [Ruijing Xia et al., 2025; John G Lawrenson et al., 2023].
- Ethical Considerations: Integrating genetic data into pediatric care necessitates robust counseling to ensure parents understand the actionable nature of the results while avoiding unnecessary anxiety or genetic discrimination [Aideen M Moore, 2022; Kelly E. Ormond, 2023].
5.2. Conventional Optical and Pharmacological Therapies
-
Optical Correction: Timely prescription of spectacles or contact lenses is the first-line treatment to provide a clear retinal image, prevent amblyopia, and reduce astigmatic defocus that may drive myopia progression (Table 5).
- ○
- Spectacles: Modern digitally-surfaced, free-form lenses with precise cylinder and axis correction are highly effective.
- ○
- Toric Soft Contact Lenses: Provide stable vision and are excellent for active children and those with significant anisometropia.
- ○
- Orthokeratology (Ortho-K): Overnight wear of rigid gas-permeable lenses that temporarily reshape the cornea. Proven to slow axial elongation in myopic children by 30-60% and can correct moderate astigmatism [Vijaya Mallareddy et al., 2024].
-
Pharmacological Therapy:
- ○
- Low-Dose Atropine (0.01%, 0.05%): The gold-standard pharmaceutical for myopia control, shown to slow progression by 50-70%. Its mechanism involves acting on scleral fibroblasts and retinal signaling pathways. It is used concomitantly with optical correction [Fricke T, 2019; Zhang et al., 2025].
5.3. Lifestyle Prescription and Ergonomic Optimization
- Prescribed Outdoor Time: Recommend ≥ 90-120 minutes of cumulative outdoor activity daily.
- Structured Screen Hygiene: Enforce the 20-20-20 rule, ensure proper viewing distance (>30 cm for phones/tablets), and optimize ambient lighting to reduce glare.
- Sleep Hygiene: Advocate for age-appropriate, consistent sleep duration (9-11 hours for school-age children).
- Nutritional Guidance: Encourage a diet rich in the nutrients outlined in Table 4.
5.4. Evidence-Based Complementary Approaches
- Yogic Eye Exercises (Trataka, Palming): While not altering corneal shape, practices like Trataka (steady gazing) and palming can reduce accommodative fatigue, improve convergence ability, and mitigate symptoms of digital eye strain. Studies show improvements in visual acuity parameters and accommodation flexibility [Mehra et al., 2020; Soumya et al., 2017; Alagesan, 2011].(Table S3) (Figure S8.)
-
Ayurvedic Interventions:
- Netra Tarpana: This therapy, involving pooled medicated ghee over the eyes, is proposed to nourish ocular tissues, reduce dryness, and strengthen the drishti (vision). Triphala ghee is commonly used for its antioxidant and anti-inflammatory properties [Gupta et al., 2010; Peterson et al., 2017].
- Triphala: Used both internally and as an eyewash (kashaya), its constituents (gallic acid, ellagic acid) demonstrate potent antioxidant and anticataract activity in preclinical models. (Table S4)
- Medicinal herbs : The traditional medicine for ocular health, offering potential benefits through their bioactive compounds that modulate inflammation, intraocular pressure, circulation, and oxidative stress in conditions like glaucoma, cataracts, and retinal disorders (Table S5)
- Mindfulness and Stress Reduction: Psychological stress can manifest as visual dysfunction (e.g., Streff Syndrome). Techniques like guided meditation for vision, progressive muscle relaxation (PMR), and breathing exercises (Pranayama like Anulom Vilom and Bhramari (Table S6) can reduce overall sympathetic tone, potentially easing accommodative spasm and improving patient comfort [Yibo Li et al., 2022; Zulfikar S., 2022]. (Figure S9.)
6. Future Directions and Conclusions
6.1. Emerging Technologies and Research Frontiers
- Advanced Diagnostics & AI: Integration of AI and machine learning with multimodal data (genetics, corneal topography, biomechanics, axial length, lifestyle logs) will enable predictive algorithms for individual progression risk and optimized treatment pathways.
- Novel Therapeutics: Research into gene therapies targeting collagen regulation, scleral cross-linking agents, and novel dopamine agonists holds promise for more targeted interventions.
- Longitudinal Big Data: Large-scale, longitudinal cohort studies from infancy through adolescence are needed to refine understanding of critical periods for intervention and GxE interactions.
6.2. A Proposed Clinical Pathway for the 21st Century
- Universal Early Screening: Comprehensive eye exams starting at 6-12 months, including cycloplegic refraction and ocular health assessment.
- Risk Stratification: For children with astigmatism ≥1.5D, family history, or other risk factors, employ advanced diagnostics (biometry, topography) and consider genetic risk profiling where available.
-
Personalized Management Plan:
- ○
- Optical Correction: Immediate, precise prescription.
- ○
- Myopia Control: If myopia is present or imminent (based on risk), initiate evidence-based control (Ortho-K, low-dose atropine, specialty lenses).
- ○
- Lifestyle Prescription: Formal “prescription” for outdoor time, screen hygiene, and nutrition.
- ○
- Integrative Adjuncts: Consider evidence-based complementary therapies for symptom management and holistic care.
- Continuous Monitoring: Regular 6-12 month reviews with axial length measurement to monitor efficacy and adjust treatment.
6.3. Conclusion
Author ORCID ID
| Author Name | ORCID ID |
| Amrutha R Kenche | 0009-0008-1968-0372 |
| Deepthi Pilli | 0009-0008-1526-251X |
| Duhita Deshmane | 0009-0000-1053-1241 |
| Priyanka Bhore | 0009-0000-8777-6546 |
| Kailash Mehra | 0000-0003-3516-0373 |
| Deepshikha Satish | 0000-0002-1313-5495 |
Supplementary Materials
Author Contributions
Funding
Ethics Approval and Consent to Participate
Consent for Publication
Competing Interests
Data Availability
References
- Abu-Amero. Genetics of Keratoconus: Where Do We Stand? Journal of Ophthalmology 2014. [Google Scholar] [CrossRef]
- Moore, Aideen M. Genetic testing and screening in children. Paediatr Child Health. 2022, 27(4), 243–253. [Google Scholar] [CrossRef]
- Russo, Andrea. Myopia: Mechanisms and Strategies to Slow Down Its Progression. J Ophthalmol. 2022. [Google Scholar] [CrossRef]
- Biswas. The influence of the environment and lifestyle on myopia. J Physiol Anthropol 2024, *43*, 7. [Google Scholar] [CrossRef]
- Biswas, Sayantan. Interaction between indoor and outdoor lighting conditions and accommodation stimuli on ocular biometry. Ophthalmic and Physiological Optics. 2025. Available online: https://publications.aston.ac.uk/id/eprint/48358/.
- Kim, Bonghyun. Optimizing acupuncture treatment for dry eye syndrome: a systematic review. BMC Complement Altern Med 2018. [Google Scholar] [CrossRef]
- Bui. Keratoconus Diagnosis and Treatment: Recent Advances and Future Directions. Clinical ophthalmology 2023. [Google Scholar] [CrossRef]
- Chen. Association of nutritional intake with myopia and astigmatism. Sci Rep 2025. [Google Scholar] [CrossRef] [PubMed]
- Cho. Analysis of tear film spatial instability for pediatric myopia under treatment. Scientific Reports 2020, 10(1). [Google Scholar] [CrossRef] [PubMed]
- Das, S.; Roy, S. THE ROLE OF NUTRITION IN EYE HEALTH: A COMPREHENSIVE REVIEW. Journal of Population Therapeutics and Clinical Pharmacology 2024, 31(6), 1281–1286. [Google Scholar] [CrossRef]
- Piñero, David P. Vector Analysis of Evolutive Corneal Astigmatic Changes in Keratoconus. Investigative Ophthalmology & Visual Science 2011, 52, 4054–4062. [Google Scholar] [CrossRef]
- Davidson. The pathogenesis of keratoconus. Eye 2013, 28(2). [Google Scholar] [CrossRef]
- Pusti, Dibyendu. Disparity between central and peripheral refraction inheritance in twins. In Scientific Reports; 2021. [Google Scholar] [CrossRef]
- Dirani, M. Dominant genetic effects on corneal astigmatism: the genes in myopia (GEM) twin study. Invest Ophthalmol Vis Sci. 2008, 49(4), 1339–1344. [Google Scholar] [CrossRef]
- Dong. Impact of Astigmatism on Axial Elongation in School-Age Children: A Five-Year Population-Based Study in Tianjin, China. Investigative Ophthalmology & Visual Science 2024, Vol.65. [Google Scholar] [CrossRef]
- SHING, ERICA. Heritability and Genetic Factors of Astigmatism and Corneal Curvature: A Systematic Review and Meta-analysis. American Journal of Ophthalmology 2025, 269, 161–171. Available online: https://www.ajo.com/article/S0002-9394(24)00380-5/abstract. [CrossRef] [PubMed]
- Eye Yoga: Exercises to Reduce Eye Power, Relieve Stress, and Improve Vision Dr. Basu eye care center, Excellence in Ayurvedic Vision Care. 27 May 2024. Available online: https://drbasueyecarecentre.com/exercises-to-reduce-eye-power-and-improve-vision/.
- Fricke, T. Pharmacological interventions in myopia management. Community Eye Health 2019, 32(105), 21–22. [Google Scholar] [PubMed]
- Lingham, Gareth. Time spent outdoors in childhood is associated with reduced risk of myopia as an adult. Sci Rep 2021. [Google Scholar] [CrossRef] [PubMed]
- Gordon-Shaag. The Genetic and Environmental Factors for Keratoconus. In BioMed Research International; 2015. [Google Scholar] [CrossRef]
- Gupta. Childhood myopia: A lifestyle disease. Indian Journal of Ophthalmology 2025, 73((2):p), 307–308. [Google Scholar] [CrossRef]
- Han, Y. Association Between Maternal Pre-Pregnancy Body Mass Index and Astigmatism and Corneal Curvature in Offspring: A Cross-Sectional Study. Clin Ophthalmol 2025, 19, 3371–3380. [Google Scholar] [CrossRef]
- Fukasaku, Hideharu. Association of PDGFRA polymorphisms with the risk of corneal astigmatism in a Japanese population. Sci Rep 2023, 13. [Google Scholar] [CrossRef]
- Higuchi, S. Light at night and circadian rhythms: from the perspective of physiological anthropology research. J Physiol Anthropol 2024, 43. [Google Scholar] [CrossRef]
- Lihong, Huang. Global trends in refractive disorders from 1990 to 2021: insights from the global burden of disease study and predictive modeling. Frontiers in Public Health 2025, Volume 13. [Google Scholar] [CrossRef]
- Lin, Jian. Correlation between ocular residual astigmatism and anterior corneal astigmatism in children with low and moderate myopia. BMC Ophthalmology 2022. [Google Scholar] [CrossRef]
- Lawrenson, John G. Interventions for myopia control in children: a living systematic review and network meta-analysis. Cochrane Database Syst Rev 2023. [Google Scholar] [CrossRef]
- Kaur. Digital Eye Strain- A Comprehensive Review. Ophthalmology and Therapy n.d., 11(5). [Google Scholar] [CrossRef] [PubMed]
- Ormond, Kelly E. Ethical Aspects of Pediatric Genetic Care: Testing and Treatment. Pediatric Clinics of North America 2023, 70(5), 1029–1046. [Google Scholar] [CrossRef]
- Chen, Keyu. Association of nutritional intake with myopia and astigmatism. Sci Rep 2025. [Google Scholar] [CrossRef] [PubMed]
- Marta, Kroczek. The Impact of the Position of the Upper Eyelid on the Profile of Epithelial Thickness and the Topography of the Cornea. Journal of Clinical Medicine (JCM) 2025. [Google Scholar] [CrossRef]
- Łabuś. A Comprehensive Analysis of the Effects of Physical Activity, Rehabilitation Methods, Environmental and Behavioral Interventions on the Development and Progression of Myopia. Quality in Sport 2025. [Google Scholar] [CrossRef]
- Larouche, R. Determinants of Outdoor Time in Children and Youth: A Systematic Review of Longitudinal and Intervention Studies. Int J Environ Res Public Health 2023, 20(2). [Google Scholar] [CrossRef]
- Lieberman. The Lids Influence on Corneal Shape. Cornea 2000, 19, 336–342. [Google Scholar] [CrossRef]
- Lin. Correlation between ocular residual astigmatism and anterior corneal astigmatism in children with low and moderate myopia. BMC Ophthalmol 2022, 22, 374. [Google Scholar] [CrossRef]
- Liu. Clinical effect and multi-factor analysis of “Siming Acupoints “ massage in the treatment of myopia in children and adolescents. Research Square (Research Square) 2024. [Google Scholar] [CrossRef]
- Loukovitis. Genetic Aspects of Keratoconus: A Literature Review Exploring Potential Genetic Contributions and Possible Genetic Relationships with Comorbidities. Ophthalmology and Therapy 2018, 7(2). [Google Scholar] [CrossRef]
- Huo, Lu. Refractive errors and risk factors for myopia in infants aged 1–18 months in Tianjin, China. BMC Ophthalmology 2021. [Google Scholar] [CrossRef]
- Lopes, Margarida C. Identification of a Candidate Gene for Astigmatism. Invest Ophthalmol Vis Sci 2013, 54(2), 1260–1267. [Google Scholar] [CrossRef]
- Pederzolli, Matteo. Keratoconus: The Local Manifestation of a Systemic Disease? Journal of Clinical Medicine 2025, 14(13), 4587. [Google Scholar] [CrossRef] [PubMed]
- Mehra. A pilot study on Effects of Eye Yogic Exercises & alternative Therapies on Eyesight Improvement. International Journal of Scientific and Research Publications 2020, 10(12). [Google Scholar] [CrossRef]
- Ba, Mengru; Li, Zhijie. The impact of lifestyle factors on myopia development: Insights and recommendations. AJO International 2024, 1(1). [Google Scholar] [CrossRef]
- Shah, Mutahir. Association of excessive screen time exposure with ocular changes leading to astigmatism in children. PLOS One 2025. [Google Scholar] [CrossRef]
- Namba. Age-Related Changes in Astigmatism and Potential Causes. Cornea 2020, 39(1). [Google Scholar] [CrossRef] [PubMed]
- Namba, et al. Age-Related Changes in Astigmatism and Potential Causes. Cornea 2020, 39(1), S34–S38. [Google Scholar] [CrossRef]
- Núñez, MX. Consensus on the management of astigmatism in cataract surgery. Clin Ophthalmol 2019, 13, 311–324. [Google Scholar] [CrossRef]
- Passaro. The oxidative-stress-senescence axis in keratoconus: new insights into corneal degeneration. Frontiers in Molecular Biosciences 2025, 12. [Google Scholar] [CrossRef] [PubMed]
- Unni, Prasida. Systemic Associations with Keratoconus. In Life (Basel); 2023. [Google Scholar] [CrossRef]
- Prousali, E. Efficacy and safety of interventions to control myopia progression in children: an overview of systematic reviews and meta-analyses. BMC Ophthalmol 2019. [Google Scholar] [CrossRef]
- R, J.; MH, H.; Amiri A, A.; S, H.; Charati F, G. The Prevalence of Astigmatism in 7 to 13 Years Old Children: A Cross-sectional Study. Journal of Pediatrics Review 2023, 11(4), 357–362. [Google Scholar] [CrossRef]
- Read. The Influence of Eyelid Morphology on Normal Corneal Shape. Investigative Ophthalmology and Visual Science 2007, 48(1), 112–119. Available online: https://eprints.qut.edu.au/10853/. [CrossRef]
- Jafari, Reza. The Prevalence of Astigmatism in 7 to 13 Years Old Children: A Cross-sectional Study. J. Pediatr. Rev 2023, 11(4), 357–362. Available online: http://jpr.mazums.ac.ir/article-1-553-en.html. [CrossRef]
- Hobday, Richard. Myopia and daylight-A combination of factors. Front Med (Lausanne) 2025. [Google Scholar] [CrossRef]
- Rose, KA. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology 2008, 115(8), 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Xia, Ruijing. Associations between RetNet gene polymorphisms and the efficacy of orthokeratology for myopia control: a retrospective clinical study. Eye and Vis 2025. [Google Scholar] [CrossRef]
- Russo. Myopia: Mechanisms and Strategies to Slow Down Its Progression. Journal of Ophthalmology 2022. [Google Scholar] [CrossRef] [PubMed]
- Reisner, Russ. 5 Vision Therapy Exercises To Reduce Astigmatism Symptoms. urban optique. 2022. Available online: https://urbanoptique.ca/5-vision-therapy-exercises-to-reduce-astigmatism-symptoms/.
- S, Y.; Y, J.; G, C.; Y, L. Age- and gender-related characteristics of astigmatism in a myopic population. Frontiers in Medicine n.d., 9, 1011743. [Google Scholar] [CrossRef]
- Mohammadi, Seyed-Farzad; Tahvildari, Maryam. Physiology of Astigmatism; EyeWiki, 2024; Available online: https://eyewiki.org/Physiology_of_Astigmatism.
- Shah, Guggenheim. Genome-wide association studies for corneal and refractive astigmatism in UK Biobank demonstrate a shared role for myopia susceptibility loci. Human Genetics 2018, 137, 881–896. [Google Scholar] [CrossRef]
- Shaw; Alyra, J. B. Eyelid pressure: Inferences from corneal topographic changes. Cornea 2009, 181–188. Available online: https://eprints.qut.edu.au/14508/. [CrossRef] [PubMed]
- Shinde. RNA sequencing of corneas from two keratoconus patient groups identifies potential biomarkers and decreased. Scientific Reports 2020, 10(1). [Google Scholar] [CrossRef]
- Shinde, I. Comparison of Surgically-induced Astigmatism using Topography and Keratometry in Patients undergoing Phacoemulsification and Small Incision Cataract Surgery: A Prospective Interventional Study. Journal of Clinical of Diagnostic Research 2024, 18(7), NC01–NC05. [Google Scholar] [CrossRef]
- Shing. Heritability and Genetic Factors of Astigmatism and Corneal Curvature: A Systematic Review and Meta-analysis. American Journal of Ophthalmology 2024, 269. [Google Scholar] [CrossRef]
- Takayama, Shin. Short-term effects of acupuncture on open-angle glaucoma in retrobulbar circulation: additional therapy to standard medication. Evid Based Complement Alternat Med 2012. [Google Scholar] [CrossRef]
- Sima. Evaluation of the efficiency and safety of TransPRK and FS-LASIK refractive procedures on patients with astigmatism and amblyopia. Rom J Ophthalmol. 2023, 67(3), 267–274. [Google Scholar] [CrossRef]
- Smita das; Roy, Sudeshna. THE ROLE OF NUTRITION IN EYE HEALTH: A COMPREHENSIVE REVIEW. Journal of Population Therapeutics and Clinical Pharmacology 2024, 31(6), 1281–1286. [Google Scholar] [CrossRef]
- Soumya. Assessment of Effectiveness of Trataka Exercise on Vision and Aesthenopia among Student Nurses with Refractive Error. International Journal of Health Sciences & Research 2017, 7(4). [Google Scholar]
- Norton, Thomas T. Light levels, refractive development, and myopia – A speculative review. Experimental Eye Research 2013, 144, 48–57. [Google Scholar] [CrossRef]
- Mallareddy, Vijaya. Innovations and Outcomes in Astigmatism Correction During Cataract Surgery: A Comprehensive Review. Cureus 2024, 16(8). [Google Scholar] [CrossRef]
- Wang. Astigmatism in school students of eastern China: prevalence, type, severity and associated risk factors. BMC Ophthalmol 2020. [Google Scholar] [CrossRef]
- Wang. Early diagnosis of keratoconus using corneal biomechanics and OCT derived technologies. Eye and Vision 2025, 12(1). [Google Scholar] [CrossRef] [PubMed]
- Wang, Z. Risk factors for astigmatic components and internal compensation:the Nanjing Eye Study. The Royal College of Ophthalmologists 2021, 35, 499–507. [Google Scholar] [CrossRef]
- Wang, et al. Prevalence and risk factors for astigmatism in 7 to 19-year-old students in Xinjiang, China: a cross-sectional study. BMC Ophthalmology 2024, 24, 116. [Google Scholar] [CrossRef] [PubMed]
- Wei, P. Biomechanics as a Causal Factor in Myopia and Astigmatism: Evidence from Mendelian Randomization. Ophthalmol Sci 2025. [Google Scholar] [CrossRef] [PubMed]
- Wong. Digital Screen Time During the COVID-19 Pandemic: Risk for a Further Myopia Boom? American Journal of Ophthalmology 2020, 223, 333–337. [Google Scholar] [CrossRef]
- Wong. High Prevalence of Astigmatism in Children after School Suspension during the COVID-19 Pandemic Is Associated with Axial Elongation. Children 2022, 9(6). [Google Scholar] [CrossRef]
- Zhang, Xiu Juan. Advances in myopia control strategies for children. British Journal of Ophthalmology 2025, 109(2), 165–176. Available online: https://bjo.bmj.com/content/109/2/165. [CrossRef]
- Zhao, Xixuan. Association between insufficient sleep and astigmatism in preschool children. Eur J Pediatr 2025. [Google Scholar] [CrossRef]
- Kim, Yangho; Lee. Association of blepharoptosis with refractive error in the Korean general population. Eye 2021, 35, 3141–3146. [Google Scholar] [CrossRef]
- Li, Yibo. Guided meditation for vision acuity training on adolescent myopia: study protocol for an open-label, prospective, multicenter, randomized controlled trial. Trials 2022. [Google Scholar] [CrossRef]
- Yoga for Your Eyes: Simple Asanas to Improve Your Vision. Yoga Journal. 14 January 2025. Available online: https://www.yogajournal.com/lifestyle/health/ayurveda/practices/insight-for-sore-eyes/.
- Yu, M. Global risk factor analysis of myopia onset in children: A systematic review and meta-analysis. PLoS ONE 2023, 1. [Google Scholar] [CrossRef] [PubMed]
- Zhang. Epidemiology and Burden of Astigmatism: A Systematic Literature Review. Optometry and Vision Science 2023, 30(3), 218–231. [Google Scholar] [CrossRef]
- Zhang, S. Axial Elongation Trajectories in Chinese Children and Adults With High Myopia. JAMA Ophthalmol. 2024, 142(2), 87–94. [Google Scholar] [CrossRef]
- Zhao, Zhi-Chun. Research progress about the effect and prevention of blue light on eyes. Int J Ophthalmol 2018. [Google Scholar] [CrossRef]
- Zulfikar, S. The Effect of Stress on Visual Function amongst School-Going Children in Mumbai. Optometry & Visual Performance 2022, 10(2), 91–96. [Google Scholar]
- Adawi, H. H. H.; Alharbi, H. A. M.; Adam, A. M. S.; Aldosery, H. M. A.; Alzahrani, R. A. Y.; Albeladi, K. A. H. THE RELATIONSHIP BETWEEN APPARENT STRABISMUS AND TYPES OF REFRACTIVE ERRORS. Journal of Population and Therapeutics and Clinical Pharmacology 2023. [Google Scholar] [CrossRef]
- Alagesan, J. Effect of eye exercises on myopia: A randomized controlled study. Middle East African Journal of Ophthalmology 2011, 18(3), 225–228. [Google Scholar] [CrossRef]
- An, L.; Hu, Q.; Guan, J.; Zhu, Y.; Jiang, C.; Zhong, X.; Ma, S.; Yu, D.; Zhang, C.; Zhuo, Y.; Qin, P. A Longitudinal Analysis about the Effect of Air Pollution on Astigmatism for Children and Young Adults. No;arXiv 2023, arXiv:2310.08843. [Google Scholar] [CrossRef]
- Baratta, R. O.; Del Buono, B. J.; Schlumpf, E.; Ceresa, B. P.; Calkins, D. J. Collagen Mimetic Peptides Promote Corneal Epithelial Cell Regeneration. Frontiers in Pharmacology 2021, 12, 705623. [Google Scholar] [CrossRef]
- Birch, E. E.; Stager, D. R.; Wang, J.; O’Connor, A. Longitudinal changes in refractive error of children with infantile esotropia. Eye 2010, 24(12), 1814–1821. [Google Scholar] [CrossRef] [PubMed]
- Boopalan, D.; Prabu Kumar, A.; Vanamoorthy, M. K.; Vijayakumar, V.; Ravi, P.; Kasi, M.; Kuppusamy, M. Yoga therapy for eye health and disease: A scoping review. European Journal of Integrative Medicine 2025, 73, 102427. [Google Scholar] [CrossRef]
- Bucheli, P.; Vidal, K.; Shen, L.; Gu, Z.; Zhang, C.; Miller, L. E.; Wang, J. Goji Berry Effects on Macular Characteristics and Plasma Antioxidant Levels. Optometry and Vision Science 2011, 88(2), 257–262. [Google Scholar] [CrossRef]
- Çakır, B.; Aksoy, N. Ö.; Özmen, S.; Bursalı, Ö.; Çelik, E.; Horozoğlu, F. Corneal topography, anterior segment and high-order aberration assessments in children with ≥ 2 diopter astigmatism. International Ophthalmology 2020, 40(6), 1461–1467. [Google Scholar] [CrossRef]
- Optical, CG. How Walnuts Help Prevent Cataracts & Macular Degeneration. n.d. Available online: https://cgoptical.co.uk/walnuts-help-prevent-cataracts-macular-degeneration/.
- Chitra, J.; Aghav, V.; Gaonkar, A.; Rajapkar, A. Effect of Bates Method versus Tibetan Eye Chart Exercise on Digital Eye Strain among Students: A Randomized Clinical Trial. Indian Journal of Physical Therapy and Research 2024, 6(1), 53–59. [Google Scholar] [CrossRef]
- Fan, Q.; Guo, X.; Tideman, J. W. L.; Williams, K. M.; Yazar, S.; Hosseini, S. M.; Howe, L. D.; Pourcain, B. S.; Evans, D. M.; Timpson, N. J.; McMahon, G.; Hysi, P. G.; Krapohl, E.; Wang, Y. X.; Jonas, J. B.; Baird, P. N.; Wang, J. J.; Cheng, C.-Y.; Teo, Y.-Y.; Vatavuk, Z. Childhood gene-environment interactions and age-dependent effects of genetic variants associated with refractive error and myopia: The CREAM Consortium. Scientific Reports 2016, 6(1), 25853. [Google Scholar] [CrossRef]
- Gupta, S. K.; Kalaiselvan, V.; Srivastava, S.; Agrawal, S. S.; Saxena, R. Evaluation of anticataract potential of Triphala in selenite-induced cataract: In vitro and in vivo studies. Journal of Ayurveda and Integrative Medicine 2010, 1(4), 280–286. [Google Scholar] [CrossRef] [PubMed]
- Gwiazda, J.; Grice, K.; Held, R.; McLellan, J.; Thorn, F. Astigmatism and the development of myopia in children. Vision Research 2000, 40(8), 1019–1026. [Google Scholar] [CrossRef] [PubMed]
- Harvey, E. M.; Dobson, V.; Miller, J. M.; Sherrill, D. L. Treatment of astigmatism-related amblyopia in 3- to 5-year-old children. Vision Research 2004, 44(14), 1623–1634. [Google Scholar] [CrossRef]
- Jang, H.; Srichayet, P.; Park, W. J.; Heo, H. J.; Kim, D.-O.; Tongchitpakdee, S.; Kim, T.-J.; Jung, S. H.; Lee, C. Y. Phyllanthus emblica L. (Indian gooseberry) extracts protect against retinal degeneration in a mouse model of amyloid beta-induced Alzheimer’s disease. Journal of Functional Foods 2017, 37, 330–338. [Google Scholar] [CrossRef]
- Kowluru, R. A.; Kanwar, M. Effects of curcumin on retinal oxidative stress and inflammation in diabetes. Nutrition & Metabolism 2007, 4(1), 8. [Google Scholar] [CrossRef]
- Kulkarni, A.; Kamath, Y.; Shetty, L.; Kuzhuppilly, N. I. R. The Effect of Specific Techniques of Nasal Breathing [Pranayama] on Intra-Ocular Pressure in Normal Individuals, a Randomized Trial. In Clinical Ophthalmology; Auckland, N.Z., 2022; Volume 16, pp. 4047–4054. [Google Scholar] [CrossRef]
- Kumar, S. Yoga based Ocular Exercise (Trataka): The Scriptural and Scientific Review. Journal of Positive School Psychology 2022, 6, 6231–6240. [Google Scholar]
- Li, S.; Liu, N.; Lin, L.; Sun, E.-D.; Li, J.-D.; Li, P.-K. Macular pigment and serum zeaxanthin levels with Goji berry supplement in early age-related macular degeneration. International Journal of Ophthalmology 2018, 11(6), 970–975. [Google Scholar] [CrossRef]
- Little, J.-A.; Chan, V. F.; Saw, S.-M.; Tham, Y. C.; Chew, L.; Foo, L. L.; Collins, M.; Ebri, A. E.; Han, X.; Schultz, L.; Gleason, D.; Jacobs, L.; Prakash, W. D.; Morjaria, P.; Robler, S. K.; Emmett, S. D.; MacKenzie, G.; Wang, N.; Khanna, R. C.; Congdon, N. Current status of school vision screening—rationale, models, impact and challenges: A review. British Journal of Ophthalmology 2025, 109(11), 1207–1214. [Google Scholar] [CrossRef]
- Mahadik, S.; Khare, S.; Diwan, V. YOGA eye exercises and Refractive Errors. Central India Journal of Medical Research 2023, 2(02), 1–3. [Google Scholar] [CrossRef]
- Mehra, K.; Gaur, D. N.; Singh, P.; Kumar, G. A pilot study on Effects of Eye Yogic Exercises & alternative Therapies on Eyesight Improvement. International Journal of Scientific and Research Publications (IJSRP) 2020, 10(12), 495–504. [Google Scholar] [CrossRef]
- Moringa and Its Role in Supporting Eye Health Moringa Powder. n.d. Available online: https://moringapowder.com/blogs/benefits/moringa-and-its-role-in-supporting-eye-health.
- Morya, A. K.; Shrivastava, A. K.; Janti, S. S.; Tejaswini, A.; Gupta, R.; Gurnani, B.; Venkatesh, D.; Prasad, R. Effect of Asanas in Yoga on Intraocular Pressure of Practicing Healthy Individuals: A Prospective Observational Study. Maedica 2023, 18(2), 238–245. [Google Scholar] [CrossRef] [PubMed]
- Mutti, D. O.; Hayes, J. R.; Mitchell, G. L.; Jones, L. A.; Moeschberger, M. L.; Cotter, S. A.; Kleinstein, R. N.; Manny, R. E.; Twelker, J. D.; Zadnik, K. Refractive Error, Axial Length, and Relative Peripheral Refractive Error before and after the Onset of Myopia. Investigative Ophthalmology & Visual Science 2007, 48(6), 2510. [Google Scholar] [CrossRef] [PubMed]
- Neha, J.; Sanwalka. Role of nutrition in the prevention of age-related macular degeneration [University of Manitoba]. 2012. Available online: https://mspace.lib.umanitoba.ca/handle/1993/23870.
- Niroula, A.; Khatri, S.; Timilsina, R.; Khadka, D.; Khadka, A.; Ojha, P. Profile of chlorophylls and carotenoids of wheat (Triticum aestivum L.) and barley (Hordeum vulgare L.) microgreens. Journal of Food Science and Technology 2019, 56(5), 2758–2763. [Google Scholar] [CrossRef] [PubMed]
- Peterson, C. T.; Denniston, K.; Chopra, D. Therapeutic Uses of Triphala in Ayurvedic Medicine. The Journal of Alternative and Complementary Medicine 2017, 23(8), 607–614. [Google Scholar] [CrossRef]
- Radomska-Leśniewska, D. M.; Osiecka-Iwan, A.; Hyc, A.; Góźdź, A.; Dąbrowska, A. M.; Skopiński, P. Therapeutic potential of curcumin in eye diseases. Central European Journal of Immunology 2019, 44(2), 181–189. [Google Scholar] [CrossRef]
- Ramakrishna, B. R. Ayurveda, Yoga, and the Conscious Self: An Integrated Approach to Health. Journal of Applied Consciousness Studies 2025, 13(2), 59–60. [Google Scholar] [CrossRef]
- Retina Specialty Hospital. Best Dry Fruits for Eye Health. n.d. Available online: https://retinaspecialityhospital.com/best-dry-fruits-for-eye-health/.
- Román-López, T. V.; García-Vilchis, B.; Murillo-Lechuga, V.; Chiu-Han, E.; López-Camaño, X.; Aldana-Assad, O.; Diaz-Torres, S.; Caballero-Sánchez, U.; Ortega-Mora, I.; Ramírez-González, D.; Zenteno, D.; Espinosa-Valdés, Z.; Tapia-Atilano, A.; Pradel-Jiménez, S.; Rentería, M. E.; Medina-Rivera, A.; Ruiz-Contreras, A. E.; Alcauter, S. Estimating the Genetic Contribution to Astigmatism and Myopia in the Mexican Population. Twin Research and Human Genetics 2023, 26(4–5), 290–298. [Google Scholar] [CrossRef] [PubMed]
- Safir, M.; Nitzan, I.; Hanina, Y.; Heller, D.; Mimouni, M.; Sorkin, N. Keratoconus prevalence in astigmatic adolescents: Findings from a nationwide screening setting. Eye 2025, 39(16), 2958–2962. [Google Scholar] [CrossRef]
- Sarla, G. S. Saunf: Do we really need fennel seeds after a meal? 2019. [Google Scholar] [CrossRef]
- Saunders, K. J. Emmetropisation following preterm birth. British Journal of Ophthalmology 2002, 86(9), 1035–1040. [Google Scholar] [CrossRef]
- Shah, M.; Natarajan, S. B.; Ahmad, N. Association of excessive screen time exposure with ocular changes leading to astigmatism in children. PLOS ONE 2025, 20(4), e0317961. [Google Scholar] [CrossRef]
- Sharma, A.; Yadav, M.; Tiwari, V.; Chaudhary, E.; Sheoran, B.; Krishania, M.; Navik, U.; Garg, M. Wheatgrass pigments: Germination, extraction, stability, and its therapeutic potential in health and diseases. International Journal of Advances in Engineering Sciences and Applied Mathematics 2025, 17(3), 279–292. [Google Scholar] [CrossRef]
- Shen, L.; Cui, Y.; Zhao, N.; Yang, F.; Zhou, Q.; Wang, X.; Qin, S. Prevalence and patterns of subnormal visual acuity and refractive errors among preschool children in Sucheng district: A cross-sectional study. BMC Ophthalmology 2025, 25(1), 420. [Google Scholar] [CrossRef]
- Shing, E.; Kam, K. W.; Zaabaar, E.; Zhang, X. J.; Young, A. L.; Pang, C. P.; Tham, C. C.; Yam, J. C.; Chen, L. J. Heritability and Genetic Factors of Astigmatism and Corneal Curvature: A Systematic Review and Meta-analysis. American Journal of Ophthalmology 2025, 269, 161–171. [Google Scholar] [CrossRef]
- Syed, F. Q.; Mirza, M. B.; Elkady, A. I.; Hakeem, K. R.; Alkarim, S. An Insight of Multitudinous and Inveterate Pharmacological Applications of Foeniculum vulgare (Fennel). In Plant and Human Health, Volume; Ozturk, M., Hakeem, K. R., Eds.; Springer International Publishing, 2019; Volume 3, pp. 231–254. [Google Scholar] [CrossRef]
- Tavazo. The Science Behind Almonds and Their Impact on Optimal Eye Function. n.d. Available online: https://tavazo.us/blogs/news/the-science-behind-almonds-and-their-impact-on-optimal-eye-function.
- Li, Q.; Wojciechowski, R.; Simpson, C. L.; Hysi, P. G.; Verhoeven, V. J. M.; Ikram, M. K.; Höhn, R.; Vitart, V.; Hewitt, A. W.; Oexle, K.; Mäkelä, K.-M.; MacGregor, S.; Pirastu, M.; Fan, Q.; Cheng, C.-Y.; St Pourcain, B.; McMahon, G.; Kemp, J. P.; Guggenheim, J. A.; The CREAM Consortium. Genome-wide association study for refractive astigmatism reveals genetic co-determination with spherical equivalent refractive error: The CREAM consortium. Human Genetics 2015, 134(2), 131–146. [Google Scholar] [CrossRef] [PubMed]
- Tóth, Gergő. The role of nutrition and supplements in the prevention and therapy of ophthalmological diseases [University of Debrecen]. 2023. Available online: https://dea.lib.unideb.hu/handle/123456789/37540.
- Vani, T.; Rajani, M.; Sarkar, S.; Shishoo, C. J. ANTIOXIDANT PROPERTIES OF THE AYURVEDIC FORMULATION T RIPHALA AND ITS CONSTITUENTS. International Journal of Pharmacognosy 1997, 35(5), 313–317. [Google Scholar] [CrossRef]
- Wang, M.; Zhou, Y.; Chen, X.; Zhu, Y.; Huang, X.; Li, L.; Xiong, Y.; Gong, Y.; Wang, Y.; Sun, Z. Obesity Increases the Prevalence of Astigmatism in Children and Adolescents. The Open Ophthalmology Journal 2025, 19(1), e18743641375929. [Google Scholar] [CrossRef]
- Wei, P.; Han, G.; Su, Q.; Jia, L.; Xue, C.; Wang, Y. Corneal Biomechanics as a Causal Factor in Myopia and Astigmatism: Evidence from Mendelian Randomization. Ophthalmology Science 2025, 5(5), 100738. [Google Scholar] [CrossRef] [PubMed]
- Weise, K. K.; Repka, M. X.; Zhu, Y.; Manny, R. E.; Raghuram, A.; Chandler, D. L.; Summers, A. I.; Lee, K. A.; Kehler, L. A. F.; Pang, Y.; Allen, M. S.; Anderson, H. A.; Erzurum, S. A.; Golden, R. P.; Koutnik, C. A.; Kuo, A. F.; Lenhart, P. D.; Mokka, P. L.; Petersen, D. B. on behalf of the Pediatric Eye Disease Investigator Group Baseline factors associated with myopia progression and axial elongation over 30 months in children 5 to 12 years of age. Optometry and Vision Science 2024, 101(10), 619–626. [Google Scholar] [CrossRef]
- Yaghoobi, R.; Kazerouni, A.; Kazerouni, O. Evidence for Clinical Use of Honey in Wound Healing as an Anti-bacterial, Anti-inflammatory Anti-oxidant and Anti-viral Agent: A Review. Jundishapur Journal of Natural Pharmaceutical Products 2013, 8(3), 100–104. [Google Scholar] [CrossRef]
- Barcelo-Canton, R. H.; Ting, D. S. J.; Mehta, J. S. Genetics of Keratoconus: Comprehensive Review. Genes 2025, 16(10), 1147. [Google Scholar] [CrossRef]

| Gene Locus | Associated Trait | Proposed Biological Function |
|---|---|---|
| PDGFRA | Corneal Curvature, Astigmatism | Neural crest cell development, corneal stroma formation |
| ZC3H11B | Refractive Astigmatism | Gene regulation, RNA metabolism |
| BMP3 | Corneal Astigmatism | Bone morphogenetic protein signaling, tissue differentiation |
| CTNNA2 | Corneal Curvature | Cell-cell adhesion, structural integrity of tissues |
| HERC2 | Pigmentation & Refractive Error | Protein ubiquitination, pigmentation pathway (influences axial length) |
| SNP | Associated Gene/Locus | Chromosome | Associated Trait | Key Finding / Role | Reference | |
|---|---|---|---|---|---|---|
| 1. Astigmatism SNPs (Corneal Astigmatism) | rs7677751 | PDGFRA (Platelet-Derived Growth Factor Receptor Alpha) | 4 | Corneal Astigmatism (CA), Corneal Curvature | One of the most consistently reported SNPs, particularly in Asian populations. PDGFRA variants are linked to eye size and corneal shape. | Fan et al. (2011) PLoS Genet. DOI: 10.1371/journal.pgen.1002402 |
| rs17084051 | PDGFRA | 4 | Corneal Curvature, Astigmatism | Located in the same critical gene region as rs7677751, involved in eye structure development. | Fan et al. (2011) PLoS Genet. DOI: 10.1371/journal.pgen.1002402 | |
| rs3771395 | VAX2 (Ventricular homeobox 2) | 2p13.3 | Refractive Astigmatism (RA) | VAX2 plays a vital role in the development of the dorsoventral axis of the eye (top-bottom structure). | Lopes et al. (2013) Invest Ophthalmol Vis Sci. DOI: 10.1167/iovs.12-10463 | |
| rs1579050 | FMNL2 (Formin-Like 2) | 2 | Corneal Astigmatism (CA) | Associated with both corneal curvature and astigmatism, with significant associations reported in children. | Lopes et al. (2013) Invest Ophthalmol Vis Sci. DOI: 10.1167/iovs.12-10463 | |
| rs1401327 | NRXN1 (Neurexin 1) | 2p12 | Refractive Astigmatism | Identified in a large GWAS by the CREAM Consortium for Refractive Astigmatism. | MacGregor et al. (2015) Hum Genet. DOI: 10.1007/s00439-014-1500-y | |
| 2. Myopia / Early Onset Myopia SNPs | rs524952 | GJD2 (Gap Junction Protein Delta 2) | 1q41 | Myopia, Spherical Equivalent Refraction (SE) | Highly replicated myopia locus. Studies suggest its effect on myopia is intensified by higher levels of education/near work (gene-environment interaction). | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 |
| rs7744813 | KCNQ5 (Potassium Voltage-Gated Channel Subfamily Q Member 5) | 6q14.1 | Myopia, Axial Length | A significant genetic factor for refractive error, often studied in relation to myopia severity in children. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| rs4373767 | ZC3H11B (Zinc Finger CCCH Type Containing 11B) | 17 | High Myopia, Axial Length | Confers a higher risk for high myopia. Research supports its role as a genetic factor for refractive error in children. | Fan et al. (2012) PLoS Genet. DOI: 10.1371/journal.pgen.1002753 | |
| rs7829127 | ZMAT4 (Zinc Finger, Matrin Type 4) | 16 | Myopia, Axial Length, SE | Associated with baseline measurements and longitudinal changes in ocular length and refractive error in children. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| rs2969180 | SHISA6-DNAH9 Locus | 17q25.3 | Myopia, Refractive Error | Exhibits a strong association with myopia, particularly in individuals with higher education/near work exposure. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| rs11601239 | GRIA4 (Glutamate Ionotropic Receptor AMPA Type Subunit 4) | 11q22.2 | Myopia, SE, Axial Length | Linked to myopia and axial length in children, suggesting a role in signaling pathways involved in eye growth. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| 3. Axial Length (AL) & Myopia SNPs (Eye Elongation) | rs524952 | GJD2 (Gap Junction Protein Delta 2) | 15q14 | Myopia, AL, Refractive Error (SE) | One of the most significant and highly replicated myopia loci. Encodes connexin 36, critical for retinal signal transmission and control of eye growth. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 |
| rs7744813 | KCNQ5 (Potassium Voltage-Gated Channel Subfamily Q Member 5) | 6q14.1 | Myopia, AL | Involved in cell excitability and volume regulation, potentially impacting the regulation of eye size. Highly replicated in multiple populations. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| rs4778879 | RASGRF1 (Ras-Guanine Nucleotide Releasing Factor 1) | 15q25 | Myopia, AL | Located near a transcription site expressed in the retina. Involved in synaptic transmission and memory consolidation, suggesting a link to the visual processing feedback loop. | - | |
| rs4373767 | ZC3H11B (Zinc Finger CCCH Type Containing 11B) | 17 | AL, High Myopia | Associated with increased axial length, suggesting a role in cellular regulation that contributes to excessive eye growth. | Fan et al. (2012) PLoS Genet. DOI: 10.1371/journal.pgen.1002753 | |
| rs11601239 | GRIA4 (Glutamate Receptor, Ionotropic, AMPA 4) | 11q22.2 | AL, Refractive Error | Implicated in glutamate signaling, which is essential for the retina’s ability to communicate with the sclera (the outer wall) to control growth. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| rs13382811 | ZEB2 (Zinc Finger E-Box Binding Homeobox 2) | 2q22.3 | High Myopia | A gene often associated with syndromic forms of myopia (like Mowat-Wilson syndrome) but also shows strong association with common and high myopia severity. | Fan et al. (2016) Nat Genet. DOI: 10.1038/ng.3738 | |
| rs10034228 | Gene Desert (MYP11 Locus) | 4q25 | Myopia, Refractive Error | A highly significant locus in a gene-poor region, possibly containing a long-range enhancer for a distant gene. | Hysi et al. (2012) Hum Genet. DOI: 10.1007/s00439-012-1175-0 | |
| rs10824518 | KCNMA1 (Potassium Large Conductance Calcium-Activated Channel Subfamily M Alpha 1) | 10 | Myopia | Linked to myopic macular degeneration, suggesting a role in the health and structure of the high-myopic eye. | Cui et al. (2019) Nat Commun. DOI: 10.1038/s41467-019-10629-9 | |
| rs7829127 | ZMAT4 (Zinc Finger, Matrin Type 4) | 16 | AL, Spherical Equivalent (SE) | Associated with the elongation of the eye (increased AL) and is often investigated for interaction with environmental factors like near work. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| Novel Loci | ADAMTS16, PIGZ | High Myopia AL ($\geq 26$ mm) | Identified in GWAS focusing specifically on patients with high myopia. ADAMTS16 is linked to extracellular matrix (ECM) remodeling (scleral structure). | - | ||
| 4. Corneal Curvature (CR) & Astigmatism SNPs | rs7677751 | PDGFRA (Platelet-Derived Growth Factor Receptor Alpha) | 4q12 | Corneal Astigmatism (CA), CR | One of the most widely replicated SNPs for corneal traits. PDGFRA is a receptor for a growth factor that regulates cell proliferation and migration during development. | Fan et al. (2011) PLoS Genet. DOI: 10.1371/journal.pgen.1002402 |
| rs3771395 | VAX2 (Ventricular homeobox 2) | 2p13.3 | Refractive Astigmatism (RA) | Involved in the development of the top-to-bottom axis of the eye, directly influencing corneal shape. | Lopes et al. (2013) Invest Ophthalmol Vis Sci. DOI: 10.1167/iovs.12-10463 | |
| rs1579050 | FMNL2 (Formin-Like 2) | 2 | CA, CR | Linked to both the degree of astigmatism and overall curvature. FMNL2 is involved in actin cytoskeleton organization, affecting cell shape and tissue integrity. | Lopes et al. (2013) Invest Ophthalmol Vis Sci. DOI: 10.1167/iovs.12-10463 | |
| rs60078183 | CMPK1 (Cytidine/Uridine Monophosphate Kinase 1) | 14q32.33 | CR | A novel locus associated with increased radius of corneal curvature (flatter cornea). | Chen et al. (2020) Cell Rep. DOI: 10.1016/j.celrep.2020.108250 | |
| rs11204213 | RBP3 (Retinol-Binding Protein 3) | 15q24 | CR, AL | Associated with both CR and AL, suggesting a pleiotropic effect on general eye growth and shape. RBP3 is involved in retinoid transport. | Verhoeven et al. (2013) Nat Genet. DOI: 10.1038/ng.2554 | |
| rs1353386 | BMP3 (Bone Morphogenetic Protein 3) | 4q21.21 | CR, Astigmatism | BMP3 is a growth factor involved in tissue morphogenesis and differentiation, which plays a role in establishing the final corneal shape. | Sim et al. (2018) Am J Hum Genet. DOI: 10.1016/j.ajhg.2018.06.002 | |
| rs17084051 | PDGFRA | 4 | CR, Corneal Astigmatism | Located near the same PDGFRA gene, reinforcing the role of this signaling pathway in determining corneal geometry. | Fan et al. (2011) PLoS Genet. DOI: 10.1371/journal.pgen.1002402 | |
| rs4896367 | NHSL1 (NHS-Like 1) | 6 | Internal Astigmatism (IA), CR | While strongly associated with Internal Astigmatism (lens-related), it is also linked to CR, highlighting its role in general eye structure. | MacGregor et al. (2015) Hum Genet. DOI: 10.1007/s00439-014-1500-y | |
| rs12144639 | RPS6KC1 (Ribosomal Protein S6 Kinase C1) | 16 | CR, Astigmatism | Identified in large meta-analyses for its influence on the mean radius of corneal curvature. | - |
| Gene | Associated trait | Proposed biological function |
|---|---|---|
| LOX | Corneal thinning and keratoconus; severity correlates with reduced LOX expression and activity. | Copper-dependent lysyl oxidase that crosslinks collagen and elastin, stabilizing corneal stromal ECM and maintaining biomechanical strength. |
| COL5A1 | Central corneal thickness variation and keratoconus-related thinning. | Fibrillar collagen V alpha chain that nucleates and regulates collagen I fibrillogenesis, controlling stromal fibril diameter, spacing, and thus corneal thickness and transparency. |
| COL1A1 | Reduced expression and rare variants reported in keratoconus and other ectasias. | Major fibrillar collagen of corneal stroma provides tensile strength; works with collagen V to form properly packed fibrils. |
| COL5A2 | Rare variants associated with keratoconus in familial cohorts. | Collagen V alpha-2 chain partnering with COL5A1 in heterotrimeric collagen V, modulating fibril assembly and stromal architecture. |
| COL4A1 | Novel variants linked to keratoconus pedigrees. | Basement-membrane collagen IV component contributing to Bowman’s layer and epithelial–stromal interface integrity, influencing corneal curvature and thickness. |
| PLOD1 | Familial keratoconus with ECM abnormalities. | Lysyl hydroxylase that post-translationally modifies collagen, enabling proper crosslinking and stabilizing stromal collagen networks. |
| TGFBI (BIGH3) | Variants reported in keratoconus and corneal dystrophies with altered corneal thickness and ECM composition. | Extracellular matrix protein induced by TGF-β that binds collagens and integrins, modulating stromal remodeling, cell adhesion, and ECM organization. |
| ZNF469 | Strongly associated with extreme thinning (e.g., brittle cornea), CCT variation, and keratoconus in GWAS and rare variant studies. | Putative transcription factor regulating expression of collagens and other ECM components, influencing overall stromal collagen content and corneal thickness. |
| FOXO1 | Locus associated with central corneal thickness; expressed in cornea and downstream of FOXC1. | Forkhead transcription factor implicated in stromal cell survival and metabolism, potentially regulating ECM gene expression and anterior segment development, thereby affecting corneal thickness. |
| COL12A1 | Implicated in corneal stromal structural organization; disruption alters fibril morphology. | FACIT collagen XII that decorates collagen I fibrils and modulates TGF-β activity, organizing fibril packing and hierarchical stromal structure important for thickness and transparency. |
| Nutrient | Primary Dietary Sources | Proposed Ocular Mechanism |
|---|---|---|
| Lutein/Zeaxanthin | Spinach, kale, corn, eggs, goji berries | Filters high-energy blue light; protects retinal pigment epithelium; antioxidant. |
| Omega-3 (DHA/EPA) | Fatty fish (salmon, mackerel), flaxseeds, walnuts | Anti-inflammatory; component of photoreceptor membranes; supports tear film. |
| Vitamin A (Retinol/Beta-Carotene) | Liver, carrots, sweet potatoes, spinach | Essential for rhodopsin synthesis (night vision); maintains conjunctival/corneal epithelium. |
| Vitamin C | Amla (Indian gooseberry), citrus fruits, bell peppers | Critical for collagen synthesis (cornea, sclera); potent aqueous humor antioxidant. |
| Vitamin E | Almonds, sunflower seeds, wheat germ oil | Protects cell membranes from lipid peroxidation; works synergistically with Vitamin C. |
| Zinc | Oysters, beef, pumpkin seeds | Cofactor for antioxidant enzymes; involved in vitamin A metabolism in the retina |
| Domain | Specific Intervention | Primary Goal | Level of Evidence |
|---|---|---|---|
| Optical | Spectacles / Toric Contact Lenses | Correct refractive error, prevent amblyopia | Strong (Standard of Care) |
| Optical (Myopia Control) | Orthokeratology, Multifocal Soft Lense | Slow axial elongation, control myopia progression | Strong |
| Pharmacological | Low-Dose Atropine (0.01%, 0.05%) | Slow axial elongation, control myopia progression | Strong |
| Lifestyle | ≥90 min Daily Outdoor Time | Protective against onset/progression of myopia/astigmatism | Strong |
| Lifestyle | 20-20-20 Rule, Screen Hygiene | Reduce accommodative strain, digital eye fatigue | Moderate-Strong |
| Nutritional | Diet rich in Lutein, Zeaxanthin, Omega-3, Vitamins | Support ocular tissue integrity, reduce oxidative stress | Moderate (for general eye health) |
| Complementary | Yogic Exercises (Trataka, Palming) | Reduce eye strain, improve accommodative facility | Moderate (for symptom relief) |
| Complementary | Ayurvedic Netra Tarpana / Triphala | Nourishment, antioxidant support (traditional use) | Emerging / Preclinical |
| Behavioral | Mindfulness, Stress Reduction Techniques | Manage stress-related visual symptoms | Moderate (for functional symptoms) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



