Submitted:
18 December 2025
Posted:
19 December 2025
You are already at the latest version
Abstract
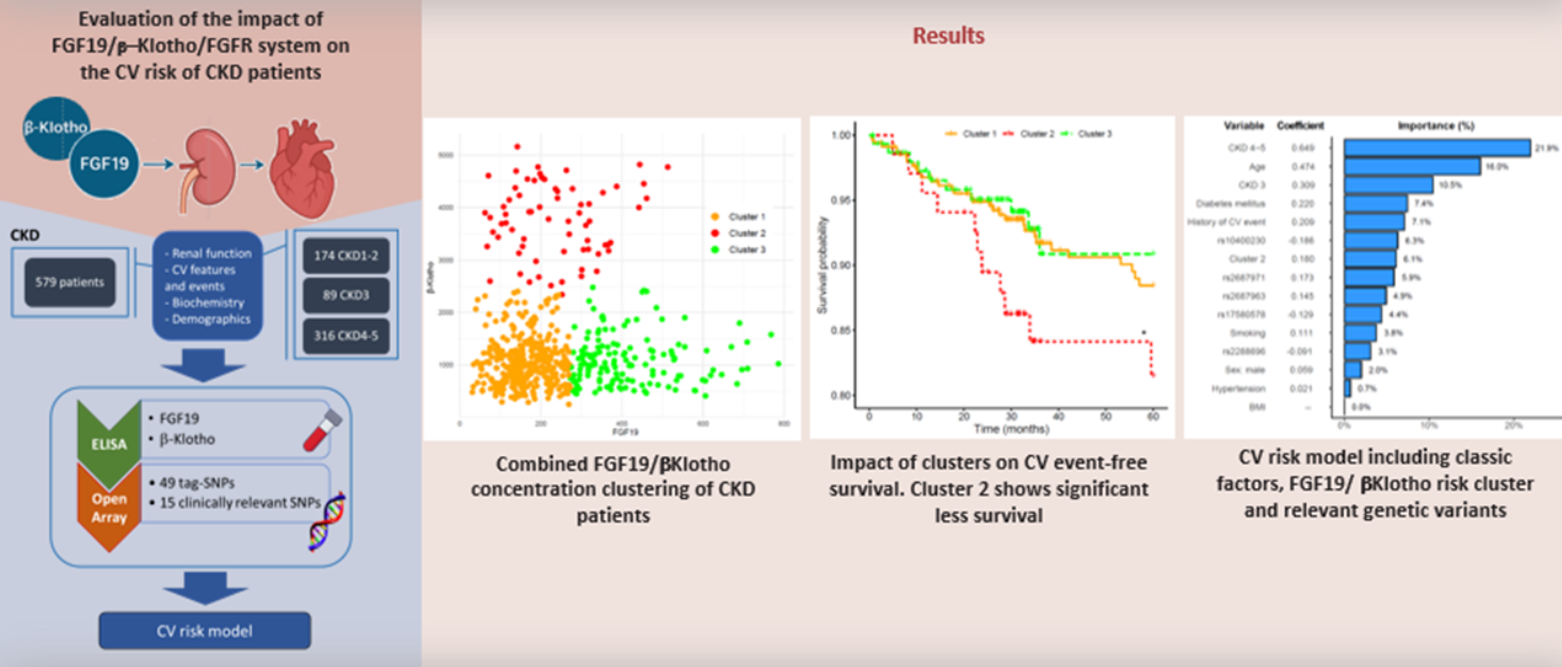
Chronic kidney disease (CKD) markedly increases the risk of cardiovascular events (CVE), yet conventional biomarkers often fail to capture this excess risk. We evaluated whether circulating levels and genetic variability within the FGF19/β-Klotho/FGFR axis contribute to CV risk stratification in CKD. In 579 CKD patients, plasma FGF19 and β-Klotho con-centrations were quantified, and 64 genetic variants across FGF19, KLB, FGFR1 and FGFR4 genes were analyzed. Cluster analysis identified three distinct biomarker profiles, with one cluster—characterized by low/intermediate FGF19 and markedly elevated β-Klotho—showing significantly reduced CV event-free survival. After adjustment for clinical covariates, this cluster was independently associated with higher CV risk [HR=2.97 (1.12–7.92), p=0.029]. Two genetic variants also showed independent associa-tions: FGFR1 rs2288696 (protective) [HR=0.51 (0.27–0.95), p=0.029] and KLB rs2687971 (risk-increasing) [HR=2.03 (0.97–4.27), p=0.046]. A combined CV risk model incorporating biomarker clusters, relevant SNPs and traditional risk factors achieved good discrimina-tive ability (C-index = 0.80), with the FGF19/β-Klotho cluster showing predictive im-portance comparable to diabetes and previous CV history. These findings suggest that in-tegrating FGF19-Klotho biomarkers with genetic information may enhance CV risk pre-diction in CKD.
Keywords:
chronic kidney disease
; cardiovascular risk
; FGF19
; β-Klotho
; risk prediction
1. Introduction
Chronic kidney disease (CKD) is becoming increasingly prevalent worldwide [1]. These patients have a significantly high risk of experiencing cardiovascular events (CVE) compared to the general population, despite adherence to evidence-based treatment guidelines [2]. In addition, because CKD progresses slowly and often without clear symptoms, early detection is crucial. Both lifestyle modifications and targeted drug therapies can help improve clinical outcomes in affected patients [3]. In consequence, there is a pressing need for discovering new biomarkers of the disease, as traditional CKD markers only stand out when the disease is well under way [4].
One of the most promising candidates in this regard is the endocrine Fibroblast Growth Factors (FGFs)-Klotho system. FGFs constitute a large family of signaling molecules that play pivotal roles in a wide array of cellular processes. Among these, FGF19, FGF21, and FGF23 operate as circulating hormones, regulating critical metabolic processes in distant tissues [5]. Interestingly, this FGF-Klotho system has been suggested to be related to the risk and clinical course of CKD [6]. However, whilst FGF21 and, especially, FGF23, have been extensively studied, significantly less data is available regarding the cardiorenal implications of FGF19.
The primary physiological role of FGF19 is the regulation of bile acid synthesis and subsequent cholesterol homeostasis [7], as well as being a modulator of insulin secretion and glycogen metabolism [8]. FGF19 requires β-Klotho to signal through two main receptors, FGFR1, which is primarily expressed in adipose tissue, and FGFR4, predominantly found in the liver [9,10]. Figure 1 shows the main biological functions of FGF19.
There are data linking FGF19 to conditions that are commonplace in CKD patients, such as diabetes, dyslipidemia or CV dysfunction [11,12,13,14]. However, only a few studies, with very limited sample size, have examined FGF19 levels in CKD, albeit with conflicting findings [11,15]. Additionally, to our knowledge, no clinical studies have evaluated the impact of genetic variants within these genes, namely KLB (encoding β-Klotho), FGF19, FGFR1 and FGFR4, which hold the potential to influence circulating FGF19/β-Klotho levels and/or their biological activity.
This study aims to investigate the relevance of the FGF19/β-Klotho/FGFR system in CKD, by evaluating the impact of both its circulating levels and genetic variants on these patients. In particular, we will focus on how these genetic and non-genetic markers may be linked to the CV complications that frequently occur in renal patients.
2. Results
Out of the 579 CKD patients, 61.8% were men and 38.2% were women, a distribution that did not change significantly among stage groups (p= 0.133). Median (IQR) age of patients was 67 (57-76) years, with age increasing significantly with CKD severity (p <0.001). Median eGFR in the CKD cohort was 25.0 (16.0-73.9) ml/min/1.73 m2. Regarding the incidence of CV risk factors, patients at CKD stage 1-2 showed less cases of hypertension, dyslipidemia, diabetes, and previous history of CV events (p<0.05 in all cases for the difference between the three study groups). Table 1 shows these and other clinical and demographic characteristics of the participants. The most frequent cause of CKD in our cohort was diabetic nephropathy (20.4%), followed by nephroangiosclerosis (18.0%) and interstitial nephropathy (13.5%). The cause could not be determined in 14.2% of cases.
2.1. Combined FGF19 and β-Klotho Concentrations in Chronic Kidney Disease
Median (IQR) of FGF19 and β-Klotho concentrations in the cohort were 210 (142-319) and 1083 (762-1552) pg/ml, respectively. Supplementary Table S2 displays values of the two biomarkers in the three stage groups. FGF19 was significantly increased in the patients with more severe CKD (p<0.001), while β-Klotho reached the highest values in the CKD 3 stage group, followed by CKD 4-5 and CKD 1-2 (p< 0.001).
We then performed cluster analyses to group our patients according to these biomarkers’ concentrations. Figure 2 depicts the three clusters obtained. Median (IQR) values of FGF19 and β-Klotho for each cluster were, respectively, cluster 1: 161 (121-211) and 1001 (692-1286) pg/mL; cluster 2: 219 (147-311) and 3811 (3,259-4358) pg/mL; and cluster 3: 379 (323-476) and 1007 (717-1324) pg/mL.
The distribution of the clusters among the three CKD stage groups studied is shown in Figure 3. The percentage of patients within Cluster 1, which contained subjects with low concentrations of both FGF19 and β-Klotho, was far less frequent in individuals at the higher stages of the disease (52.8%) compared with patients at stage 3 (68.5%) or stage 1-2 (71.5%). In contrast, cluster 3, i.e., patients with high concentrations of FGF19 but low β-Klotho levels, was more frequent among patients with stages 4-5 (35.9%) than in those with stage 1-2 (16.3%) or stage 3 (15.7%). Finally, Cluster 2, containing subjects that displayed high levels of β-Klotho but low/intermediate levels of FGF19, presented similar values across CKD stages (12.2%, 15.7% and 11.3% for stage 1-2, 3 and 4-5, respectively). The distribution of the three clusters across CKD stages was significantly different (p<0.001).
2.2. Effect of FGF19/β-Klotho Combined Concentrations on Cardiovascular Risk in CKD Patients
To assess CV risk in the cohort, the 579 participants were followed for a median of 34.9 (28.4-60.0) months to register the incidence of CVE, which were experienced by 52 (9.0%) patients. Table 2 shows demographic and clinical characteristics of patients who did or did not suffer a CVE. As expected, those who experienced CVE were older (p <0.001), had higher concentrations of glucose (p =0.001), cholesterol (total values, HDL and LDL, p <0.01), and albuminuria (p <0.001). Having a previous history of CVE (p <0.001) or diabetes (p <0.001). The association of the three FGF19/β-Klotho clusters with CV event-free survival is shown in Figure 4. Kaplan-Meier analysis revealed that patients within cluster 2 had a lower event-free survival (84.1%) than those in cluster 1 (91.0%) and 3 (93.3%). After adjusting a Cox regression model for age, sex, BMI, hypertension, diabetes, smoking, CKD stage and previous CV history, cluster 2 presented a significantly higher CV risk compared to cluster 3 [HR=2.97 (1.12-7.92), p =0.029].
2.3. Association of Genetic Variants in the FGF19-Klotho System with Cardiovascular Risk
Next, we assessed the impact of genetic variants in the participating genes (FGF19, KLB, FGFR1 and FGFR4) on the incidence of CVE in the cohort. Cox regression models adjusted by the aforementioned covariates revealed that rs2288696 in FGFR1 displayed a protective effect [HR=0.51 (0.27-0.95), p<0.029], whilst KLB rs2687971 increased CV risk [HR=2.03 (0.97-4.27), p=0.043] (Table 3). Figure 5 shows SNP-pair interactions between genetic variability in the four assayed genes with regard to their effect on CV events. Three pairs, namely FGF19 rs1192927-FGFR1 rs3758102 (p<0.001), FGFR1 rs17182127-KLB rs7674434 (p<0.001) and FGFR1 rs59778175-KLB rs77730696 (p<0.001) showed a marked impact on CV risk.
2.4. Combined Risk Model for Cardiovascular Risk in Chronic Kidney Disease
A combined CV risk model for the CKD patients was created that included the FGF19/β-Klotho concentration cluster, relevant genetic variants [the two SNPs with significant CV associations, rs2288696, rs2687971, and three more variants with suggestive p-values (<0.1), namely rs17580578, rs10400230 and rs2687963], as well as age, sex, BMI, hypertension, diabetes, smoking, CKD stage and previous CV history, as described in previous analyses. The model achieved a C-index of 0.80. Figure 6 shows that, as expected, CKD severity and age carried the largest weight in the model (importance ranging from 10.5 to 21.9%). Remarkably, the risk cluster showed a coefficient of 0.180 with a 6.1% importance in the model, figures that were similar to those shown by diabetes (0.220, 7.4%) or previous CV history (0.209, 7.1%), and far superior to other risk factors such as smoking (0.111, 3.8%), hypertension (0.021, 0.7%) or BMI (0%, left out of the model). The rs10400230 SNP was the variant displaying the highest coefficient (-0.186, 6.3% importance).
3. Discussion
CV diseases account for 40-50% of deaths in CKD patients [16,17]. This CV risk is disproportionately high compared to the general population and increases with the severity of the disease, so much so that renal patients with eGFR<45 ml/min/1.73 m2 or high proteinuria values are 6 times more likely to experience a CVE [18]. Multiple mechanisms have been suggested to underlie this excessive CV risk, amongst them, the FGF-Klotho system has lately been attracting a great deal of attention [6].
The implication of FGF23 and, to a lesser extent, of FGF21 in the CV complications of CKD has been widely studied [19,20]. However, it has only recently been hypothesized that alterations in circulating concentrations of FGF19 in CKD patients may also affect CV risk, due to its role in regulating crucial metabolic pathways, including glucose, lipid, and bile acid metabolism [14]. In this regard, we have just reported that a single score integrating plasma levels of all three endocrine FGFs (FGF19, FGF21 and FGF23) was an accurate biomarker of CV risk [21]. FGF19 carried the lower weight in this combined score, indicating that, by itself, its impact on CV risk was likely lower than that of FGF21 or, especially, FGF23. However, β-Klotho was not targeted in that study. Now, in the present article, by creating a cluster integrating the concentrations of both FGF19 and its necessary cofactor β-Klotho, we can obtain a clearer picture of the CV implications of dysregulation in the FGF19-β-Klotho partnership.
Our results show that patients with both low/intermediate levels of FGF19 and high levels of β-Klotho, were at significantly elevated CV risk, as compared with those with high FGF19 and low β-Klotho. It should be noted that patients within this risk cluster were uniformly distributed across all CKD stages and, therefore, the severity of the disease was not a confounding factor in their observed increased CV risk. To date, there are no studies that analyze the association of combined FGF19/β-Klotho concentrations with CV risk, and only a few analyze their individual impact, although none in the CKD setting. Regarding FGF19, and in line with the data presented herein, low FGF19 plasma levels have very recently been associated with diminished cardiac function [22] and worse prognosis in patients with acute ischemic stroke [23]. In contrast, Hu et al. showed that elevated FGF19 serum levels correlated with atherosclerosis severity in men with Type-2 Diabetes [24]. However, the reported mean values in this last study, even though they were considered elevated, were in fact lower than the mean concentration in our patients at high CV risk (171.2 pg/ml vs. 219.0 pg/ml). These findings underscore the complexity of the FGF19 implications in CV risk and the potential influence of the specific disease context, such as the presence or absence of diabetes or the existence of renal injury, as is the case in this study. In this respect, the severity of the renal disease correlated positively with plasma FGF19 levels in our patients, which is in agreement with three previous studies in CKD [15,25,26]. Conversely, Yamamoto et al. did not find an association with renal function in the general population, although only 73 subjects were analyzed [11]. The large number of patients included in our cohort supports the hypothesis that, indeed, there seems to be an inverse association between FGF19 concentrations and eGFR in CKD. It is possible that, similarly to FGF21, dysregulated concentrations of FGF19 in these patients result from metabolic changes, inflammation and probably even nutrition [15].
The other member of the combined biomarker was β-Klotho, which has been proposed as a promising drug target for metabolic and CV disease [27]. However, and unlike its alpha analogue [28], there is no information on the putative impact of its circulating concentrations, let alone in the CKD setting. Our findings show that subjects in cluster 2, with elevated plasma levels of β-Klotho, had a higher incidence of CVE. A hypothesis could be that, since these patients at-risk also had low FGF19 concentrations, the excess of β-Klotho would be free to interact and activate FGF21, hence triggering a signal that could end up increasing CV risk [29]. Indeed, high blood levels of FGF21 have been shown to be an independent risk factor for heart failure [30,31]. Moreover, cluster 1, also with low FGF19 concentrations but presenting low β-Klotho levels as well, did not show an increase of CV risk. Nevertheless, whether the CV impact is provoked by the β-Klotho interplay with FGFs or by independent mechanisms warrants further investigation.
A second aspect of the study dealt with the putative effect of genetic variability in the genes coding for all the players in this system: FGF19, β-Klotho, FGFR1 and FGFR4. Our findings revealed that rs2288696 in FGFR1 displayed a protective effect against CV risk. This is an intronic SNP that has not been evaluated before in the cardiorenal context, although, interestingly enough, it has also been attributed with a protective effect in ovarian cancer [32]. FGFRs are essential mediators of the biological effects of FGFs, and hence it is plausible that genetic variations in FGFRs may affect CV function. For instance, FGFR1 signaling has been implicated in the development of kidney injury associated with hypertension [33]. Furthermore, a very recent report points to FGFR1 as a novel locus and therapeutic target for cardiometabolic health [34]. The other variant with a significant impact on CV risk was rs2687971 in the KLB gene, which codes for β-Klotho and whose locus variability has recently been implicated in cardiometabolic complications [35] and the incidence of CVE [36]. KLB rs2687971 is located in the 3’-UTR region of the gene and could therefore be involved in mRNA stability or miRNA binding [37], although no clinical repercussions of this variant have been reported as yet. In any case, although the p-value for the association was significant, the lower limit of the confidence interval was 0.97, and therefore caution should be exerted when considering this result. In addition, our results also showed that variants present in the locus of different genes that need to work together to trigger biological functions (FGF19/FGFR1/KLB), may also interact to significantly affect these functions, in this case altering CV risk. In this regard, we have previously reported that interactions between SNPs in glucose homeostasis genes can also impact the susceptibility to CVE in patients with diabetic nephropathy [38].
Finally, we included both the FGF19/β-Klotho cluster and the relevant genetic variants in a CV risk model for CKD patients that showed a C-index of 0.80, which is considered good/excellent discriminative ability in other CV clinical studies [39,40]. The cluster and some of the variants carried a similar weight in the model as that shown by diabetes or previous CV history, while being superior to smoking, sex, hypertension or BMI. Traditional models often fall short in accurately predicting CV events in CKD. We have previously shown how CV risk models in CKD can be significantly enhanced by the addition of novel biomarkers, e.g. endothelin [41], genetic variants, e.g. those in the prostaglandin E2 pathway [42], or even nutritional information [43]. Taken together, these previous findings and our current data suggest that conventional markers still have considerable limitations and that risk models can and must be efficiently tuned up. There is a pressing need for novel CV biomarkers in renal disease, especially considering that CKD is projected to rank among the five leading causes of death globally by 2040, largely driven by its CV complications [44].
This study has several strengths and limitations. To our knowledge, it is the first to examine the FGF19/β-Klotho system in renal patients as a means to assess CV risk. In addition, the parallel genetic analysis enabled the identification of relevant variants that can enhance the performance of CV risk models. Amongst the limitations, we did not measure the expression of FGF19/β-Klotho in the organs of interest, whose relationship with circulating levels would be most informative. Additionally, the genetic study design included the analysis of tag-SNPs, i.e., variants that represent genetic variability in a certain region but that usually lack a known functional impact, being most of them intronic. This means that, while we were able to capture the whole variability of each gene, connecting the observed genotype-phenotype association to a particular biochemical consequence of the SNP is challenging. Finally, the reported CV risk model should obviously undergo external validation before considering clinical use.
In summary, we have demonstrated how the FGF19/β-Klotho system plays a relevant role in CKD. Specifically, a concentration cluster integrating FGF19 and β-klotho concentrations could function as a biomarker of CV risk in the renal setting. Its inclusion in a CV risk model along with relevant genetic variants and traditional risk factors, holds the potential to improve the management of CV-related complications in CKD.
4. Patients and Methods
A total of 579 Spanish Caucasian CKD patients at different stages of the disease were recruited from the Badajoz University Hospital (Spain). Among them, 174 (30.1%) with CKD1-2, 89 (15.4%) with stage 3; and 316 (54.6%) with stage 4/5. Transplantation, pregnancy, breastfeeding, active infection, cancer, or acute kidney injury were all considered exclusion criteria. All patients were over 18 years of age and gave written consent for their participation in the study, which was approved by the Ethics Committees of the Badajoz University Hospital and was carried out in accordance with the Declaration of Helsinki and its subsequent revisions.
4.1. Clinical Variables
Diagnostic and prognostic stratification of patients was made using the KDIGO classification. Estimation of renal function was carried out by creatinine clearance (ml/min), glomerular filtration rate (GFR) estimated by the CKD-EPI formula with creatinine. Proteinuria was defined as a value greater than 500mg (or albuminuria >300mg) in 24h urine. Clinical records of the study participants were reviewed to retrieve data on renal function and CV events experienced during the follow-up, including death from CV cause, acute myocardial infarction, acute coronary syndrome, coronary catheterization requiring angioplasty, coronary bypass, typical angina with positive stress tests, sudden death, stroke, peripheral artery disease and lower limb ischemia.
4.2. Determination of Biomarkers Circulating Levels
Blood samples were collected and immediately subjected to plasma separation on the day of the participant’s visit to the hospital. The determination of FGF19 was carried out in an ELLATM equipment (Bio-Techne, Minneapolis, USA), which is an automated, low-volume, microfluidic ELISA platform. Thirty-two-well cartridges were used, allowing the simultaneous analysis of various analytes. Fifty μL of diluted plasma with equal volume of sample diluent were added to each well, followed by the addition of 1 mL of wash buffer to the corresponding buffer inlets. Automated immunoassay analyses were initiated via Simple Plex Runner software (v.3.9.0.28), and consisted of system start-up, microfluidic sample splitting, incubation within glass nano-reactor (GNR) channels containing immobilized capture antibody, biotinylated detection antibody and streptavidin dye conjugate, laser excitation of fluorophores and detection of fluorescence signals. Relative fluorescence units for each GNR were converted to FGFs concentrations by inverse fitting to a master calibration curve established by the manufacturer. Because each microfluidic channel has three GNRs, triplicate measurements were produced for each well/sample (average values are given).
β-Klotho determinations were conducted with commercially available ELISA kits (Bio-Techne, Minneapolis, USA), as described in detail elsewhere [45]. Quantification was performed spectrophotometrically using a Multiskan EX microplate reader (Thermo, Waltham, MA, USA). The coefficient of variability (%CV) was calculated using the following formula: %CV = standard deviation/mean. The limits for %CV were set at 5% and 10% for intra-assay and inter-assay measurements, respectively. All calculated %CV values were within these limits. Wavelengths were measured at 450 nm and 540 nm and calibration curves were between 31.3 and 2000 pg/ml.
4.3. Genetic Analyses
The DNA of the participants was purified from whole blood samples using a standard phenol-chloroform extraction method followed by ethanol precipitation. Four genes, namely FGF19, KLB, FGFR1, FGFR4, were studied using two different approaches. First, tag-SNPs, which define the variability of a specific area in a gene locus, were identified. For this, we obtained all the SNPs registered for Europeans for each gene (www.internationalgenome.org) and inserted this information into the Haploview software (https://www.broadinstitute.org/haploview) using the Ensembl's VCF to PED converter tool. Assuming a threshold of r2 = 0.8 and a minimum allele frequency (MAF) of 0.05, the Haploview tagger function generated 49 tag-SNPs by pairwise tagging. These variants capture 100% of the variability registered in the European population for these four genes. Second, we also included in the analyses 15 variants for which there are reports supporting a functional/clinical impact [46,47,48]. Genotyping analyses were performed using a customized panel containing the variants of interest on a QuantStudio™ 12K Flex Real-Time PCR System (Life Technologies, Carlsbad, California, USA) via TaqMan® OpenArray technology. Each run incorporated quality controls, consisting of sample trios sourced from the Coriell Institute Biorepository. These analyses were conducted at the Centro Nacional de Genotipado-Instituto de Salud Carlos III (CeGen-ISCIII; Madrid, Spain, www.cegen.org). Supplementary Tables S1 shows characteristics of the analyzed SNPs in our cohort.
4.4. Statistical Analysis
Categorical variables were presented as absolute counts and percentages, whereas continuous variables were described as medians and interquartile ranges (IQR, p25-p75). To evaluate the relationship between CKD stage and continuous variables, non-parametric Kruskal–Wallis tests were applied, given that clinical data did not follow a normal distribution. Associations between CKD stage and categorical variables were evaluated using the Likelihood Ratio Test (LRT). Cox proportional hazards regression models were applied to examine the relationship between clinical variables and genetic variants with CV event-free survival, assuming a dominant model of inheritance, as it produced more balanced groups for comparison.
Across the entire cohort, a cluster analysis was conducted to classify patients based on their FGF19 and β-Klotho concentrations. The two variables were standardized prior to the analysis, and 17 patients were excluded as outliers according to Density-based Spatial Clustering of Applications with Noise (DB-SCAN) algorithm. The Euclidean partitioning around medoids (PAM) algorithm then identified three distinct clusters, which were visualized in a scatter plot. These clusters were subsequently analyzed in relation to CKD severity and displayed in a bar plot. Associations between clusters and CV event free survival risk were assessed using Kaplan–Meier survival curves and Cox proportional hazards regression models adjusted for age, sex, BMI, hypertension, diabetes, smoking status, prior CV and CKD stage. These covariates were selected based on clinical relevance and/or results from univariate analyses. Results were expressed as hazard ratios (HR) with 95% confidence intervals (CI). The impact of SNP-pair interactions in the participating genes on CV risk was evaluated applying log-likelihood ratio tests and controlling for age, sex, BMI, hypertension, diabetes, smoking and previous CV history. In the charts illustrating these analyses, the upper triangle of the matrix displays the p-values for the interaction log-likelihood ratio test, whilst the lower triangle presents the p-values from the likelihood ratio test, which compares the additive likelihood of two variants to the best of the single-variant models. The diagonal line showcases the p-values derived from the likelihood ratio test for the crude effect of each variant.
An Elastic-Net regularized Cox proportional hazards model was fitted to estimate the risk of CVE. Predictors included concentration clusters, relevant SNP variants (rs10400230, rs2687971, rs2687963, rs17580578 and rs2288696), as well as adjustment covariates. All predictors were standardized before being entered into the model. A 10-fold cross-validation based on partial likelihood deviance was used to identify the regularization parameter (λ) that minimized the standard error. The Elastic-Net mixing parameter (α) was set to 0.5 to balance the LASSO and Ridge penalties, providing a compromise between variable selection and the retention of correlated predictors. Variable importance was assessed based on the absolute value of each coefficient in the model, scaled to 100%, and presented in a bar plot. Model discrimination was quantified using the concordance index (C-index) for right-censored data.
With the 579 individuals included in the study, a CVE incidence of 9.0% (52 patients), and a two-sided alpha of 0.05, the statistical power to detect a standardized effect size (Cohen´s d) of 0.45 between patients with and without CVE was 85.5%. Power calculations were based on the Wilcoxon-Mann-Whitney test (GPower v. 3.1.9.6, Kiel University, Germany).
All statistical procedures were carried out utilizing different R packages. Kaplan Meier-curves were generated with survminer. Cox proportional hazards regression models were fitted with survival. Cluster analysis was conducted with cluster and dbscan. Scatter and bar plots were produced using ggplot2. SNP-pair interactions were evaluated with SNPassoc. Elastic-Net regularized Cox proportional hazards model was obtained with glmnet. A p-value <0.05 was deemed statistically significant.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: P-values for the association of 16 tag-SNPs in OPRD1 with the risk of developing Anorexia Nervosa. All models of inheritance are shown; Table S2: P-values for the association of 16 tag-SNPs in OPRD1 with the risk of developing Bulimia Nervosa. All models of inheritance are shown.
Author Contributions
L G-R, data curation and writing of original draft; M M-A and V D-A, performed statistical and genetic analyses; S M-Z, data curation; CC, methodology; BC, R G-L, ZV, investigation; FB and NRR, supervision and conceptualization; GG, conceptualization, funding acquisition, supervision, writing (review and editing).
Funding
This research was funded by grant PI22/00181 and RD21/0005/0031 from Instituto de Salud Carlos III, Madrid (Spain), cofinanced by the European Union – NextGeneration UE, Recovery and Resilience Mechanism; as well as by the Extremadura Research Chair in Cardiovascular Risk Reduction (CIRRCE). The work was also financed at 85% by the European Union, European Regional Development Fund, and the Regional Government of Extremadura, Managing Authority: Ministry of Finance (Grant GR24027). Funding sources did not have any involvement in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of Badajoz University Hospital (No PI22/00181, April 21 2022).”.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Source data for this study have been uploaded to the Figshare repository and are openly available at https://figshare.com/articles/dataset/FGF_betaKlotho_in_CKD/30720536?file=59866880 with DOI 10.6084/m9.figshare.30720536.
Acknowledgments
We would like to thank the auxiliary staff and nurses at the collaborating hospital, especially Sonia Martín, whose help was essential in completing this work. Also, we thank Sara Blas, lab technician, for her technical assistance and her support in managing the lab’s resources.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Abbreviations
The following abbreviations are used in this manuscript:
| CKD | Chronic Kidney Disease |
| CVE | Cardiovascular Event |
| SNP | Single-nucleotide polymorphism |
| eGFR | Estimated Glomerular Filtration Rate |
| HR | Hazard Ratio |
| ACR | Albumin to Creatinine Ratio |
| BMI | Body-mass Index |
References
- Ortiz, A. RICORS2040: the need for collaborative research in chronic kidney disease. Clin Kidney J 2022, 15, 372–387. [Google Scholar] [CrossRef]
- Schunk, S.J.; Zimmermann, P. Cardiovascular Risk and Its Presentation in Chronic Kidney Disease. J Clin Med 2025, 14. [Google Scholar] [CrossRef]
- Zhou, X.; Zhang, Y.; Wang, N. Regulation and Potential Biological Role of Fibroblast Growth Factor 21 in Chronic Kidney Disease. Front Physiol 2021, 12, 764503. [Google Scholar] [CrossRef]
- Alobaidi, S., Emerging Biomarkers and Advanced Diagnostics in Chronic Kidney Disease: Early Detection Through Multi-Omics and AI. Diagnostics (Basel) 2025, 15.
- Phan, P.; Ternier, G.; Edirisinghe, O.; Kumar, T.K.S. Exploring endocrine FGFs - structures, functions and biomedical applications. Int J Biochem Mol Biol 2024, 15, 68–99. [Google Scholar] [CrossRef]
- Kuro, O.M. Klotho and endocrine fibroblast growth factors: markers of chronic kidney disease progression and cardiovascular complications? Nephrol. Dial. Transplant. 2019, 34, 15–21. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, M.B.; Jorge, G.; Zanardo, L.W.; et al. The role of FGF19 in metabolic regulation: insights from preclinical models to clinical trials. Am J Physiol Endocrinol Metab 2024, 327, E279–E289. [Google Scholar] [CrossRef] [PubMed]
- Zeng, T.; Tang, X.; Bai, X.; Xiong, H. FGF19 Promotes the Proliferation and Insulin Secretion from Human Pancreatic beta Cells Via the IRS1/GLUT4 Pathway. Exp. Clin. Endocrinol. Diabetes 2024, 132, 152–161. [Google Scholar] [PubMed]
- Chen, L.; Fu, L.; Sun, J.; et al. Structural basis for FGF hormone signalling. Nature 2023, 618, 862–870. [Google Scholar] [CrossRef]
- Yang, C.; Jin, C.; Li, X.; Wang, F.; McKeehan, W.L.; Luo, Y. Differential specificity of endocrine FGF19 and FGF21 to FGFR1 and FGFR4 in complex with KLB. PLoS One 2012, 7, e33870. [Google Scholar] [CrossRef]
- Yamamoto, S.; Koyama, D.; Igarashi, R.; et al. Serum Endocrine Fibroblast Growth Factors as Potential Biomarkers for Chronic Kidney Disease and Various Metabolic Dysfunctions in Aged Patients. Intern. Med. 2020, 59, 345–355. [Google Scholar] [CrossRef]
- Dolegowska, K.; Marchelek-Mysliwiec, M.; Nowosiad-Magda, M.; Slawinski, M.; Dolegowska, B. FGF19 subfamily members: FGF19 and FGF21. J. Physiol. Biochem. 2019, 75, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Guo, J.; Tao, H.; et al. Circulating mediators linking cardiometabolic diseases to HFpEF: a mediation Mendelian randomization analysis. Cardiovasc Diabetol 2025, 24, 201. [Google Scholar] [CrossRef] [PubMed]
- Morita, H.; Hoshiga, M. Fibroblast Growth Factors in Cardiovascular Disease. J Atheroscler Thromb 2024, 31, 1496–1511. [Google Scholar] [CrossRef]
- Marchelek-Mysliwiec, M.; Dziedziejko, V.; Nowosiad-Magda, M.; et al. Chronic Kidney Disease Is Associated with Increased Plasma Levels of Fibroblast Growth Factors 19 and 21. Kidney Blood Press. Res. 2019, 44, 1207–1218. [Google Scholar] [CrossRef] [PubMed]
- Thompson, S.; James, M.; Wiebe, N.; et al. Cause of Death in Patients with Reduced Kidney Function. J. Am. Soc. Nephrol. 2015, 26, 2504–2511. [Google Scholar] [CrossRef]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Tarun, T.; Ghanta, S.N.; Ong, V.; et al. Updates on New Therapies for Patients with CKD. Kidney Int Rep 2024, 9, 16–28. [Google Scholar] [CrossRef]
- Freise, C.; Jernej, T.; Metzkow, S.; Schnorr, J.; Taupitz, M. Fibroblast growth factor-23 remodels vascular extracellular matrix via glycosaminoglycan induction: implications for calcification in chronic kidney disease. Ren. Fail. 2025, 47, 2567528. [Google Scholar] [CrossRef]
- Salgado, J.V.; Goes, M.A.; Salgado Filho, N. FGF21 and Chronic Kidney Disease. Metabolism 2021, 118, 154738. [Google Scholar] [CrossRef]
- González-Rodríguez, L.; Martí-Antonio, M.; Mota-Zamorano, S.; et al. Combined concentrations and genetic variability of Fibroblast Growth Factors predict cardiovascular risk in renal patients. iScience 2025, On line ahead of print. [CrossRef]
- Xu, W.; Wang, Y.; Guo, Y.; et al. Fibroblast growth factor 19 improves cardiac function and mitochondrial energy homoeostasis in the diabetic heart. Biochem. Biophys. Res. Commun. 2018, 505, 242–248. [Google Scholar] [CrossRef]
- Ren, X.; Yang, P.; Sun, L.; et al. High plasma fibroblast growth factor 19 is associated with improved prognosis in patients with acute ischemic stroke. Clin. Nutr. 2025, 48, 16–24. [Google Scholar] [CrossRef]
- Hu, J.; Liu, Z.; Tong, Y.; et al. Fibroblast Growth Factor 19 Levels Predict Subclinical Atherosclerosis in Men With Type 2 Diabetes. Front Endocrinol (Lausanne) 2020, 11, 282. [Google Scholar] [CrossRef] [PubMed]
- Marchelek-Mysliwiec, M.; Dziedziejko, V.; Dolegowka, K.; et al. Association of FGF19, FGF21 and FGF23 with carbohydrate metabolism parameters and insulin resistance in patients with chronic kidney disease. J Appl Biomed 2020, 18, 61–69. [Google Scholar] [CrossRef]
- Reiche, M.; Bachmann, A.; Lossner, U.; Bluher, M.; Stumvoll, M.; Fasshauer, M. Fibroblast growth factor 19 serum levels: relation to renal function and metabolic parameters. Horm. Metab. Res. 2010, 42, 178–181. [Google Scholar] [CrossRef]
- Aaldijk, A.S.; Verzijl, C.R.C.; Jonker, J.W.; Struik, D. Biological and pharmacological functions of the FGF19- and FGF21-coreceptor beta klotho. Front Endocrinol (Lausanne) 2023, 14, 1150222. [Google Scholar] [CrossRef]
- Liu, Q.; Yu, L.; Yin, X.; Ye, J.; Li, S. Correlation Between Soluble Klotho and Vascular Calcification in Chronic Kidney Disease: A Meta-Analysis and Systematic Review. Front Physiol 2021, 12, 711904. [Google Scholar] [CrossRef]
- Shi, S.Y.; Lu, Y.W.; Richardson, J.; et al. A systematic dissection of sequence elements determining beta-Klotho and FGF interaction and signaling. Sci Rep 2018, 8, 11045. [Google Scholar] [CrossRef] [PubMed]
- Sunaga, H.; Yoshida, K.; Kagami, K.; et al. Prognostic Impact of Fibroblast Growth Factor 21 in Patients With Heart Failure. Circ Rep 2025, 7, 922–929. [Google Scholar] [CrossRef] [PubMed]
- Ianos, R.D.; Iancu, M.; Pop, C.; et al. Predictive Value of NT-proBNP, FGF21, Galectin-3 and Copeptin in Advanced Heart Failure in Patients with Preserved and Mildly Reduced Ejection Fraction and Type 2 Diabetes Mellitus. Medicina (Kaunas) 2024, 60 . [Google Scholar] [CrossRef]
- Meng, Q.H.; Xu, E.; Hildebrandt, M.A.; et al. Genetic variants in the fibroblast growth factor pathway as potential markers of ovarian cancer risk, therapeutic response, and clinical outcome. Clin. Chem. 2014, 60, 222–232. [Google Scholar] [CrossRef]
- Xu, Z.; Luo, W.; Chen, L.; et al. Ang II (Angiotensin II)-Induced FGFR1 (Fibroblast Growth Factor Receptor 1) Activation in Tubular Epithelial Cells Promotes Hypertensive Kidney Fibrosis and Injury. Hypertension 2022, 79, 2028–2041. [Google Scholar] [CrossRef]
- Ye, C.; Dou, C.; Liu, D.; et al. Multivariate genome-wide analyses of insulin resistance unravel novel loci and therapeutic targets for cardiometabolic health. Nat Commun 2025, 16, 10057. [Google Scholar] [CrossRef]
- Dai, M.; Li, Y.; Zhang, J.; et al. Genetic polymorphisms associated with metabolic dysfunction-associated steatotic liver disease and cardiometabolic risk susceptibility in the Chinese Han population. Hum Genomics 2025, 19, 125. [Google Scholar] [CrossRef]
- Antunez-Rodriguez, A.; Garcia-Rodriguez, S.; Pozo-Agundo, A.; et al. Targeted next-generation sequencing panel to investigate antiplatelet adverse reactions in acute coronary syndrome patients undergoing percutaneous coronary intervention with stenting. Thromb. Res. 2024, 240, 109060. [Google Scholar] [CrossRef]
- Kong, L.; Zhu, J.; Han, W.; et al. Significance of serum microRNAs in pre-diabetes and newly diagnosed type 2 diabetes: a clinical study. Acta Diabetol. 2011, 48, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Mota-Zamorano, S.; Gonzalez, L.M.; Robles, N.R.; et al. Polymorphisms in glucose homeostasis genes are associated with cardiovascular and renal parameters in patients with diabetic nephropathy. Ann. Med. 2022, 54, 3039–3051. [Google Scholar] [CrossRef] [PubMed]
- Erqou, S.; Shahab, A.; Fayad, F.H.; et al. Cardiovascular Risk Prediction Scores in Type 1 Diabetes: A Systematic Review and Meta-Analysis. JACC Adv 2025, 4, 101462. [Google Scholar] [CrossRef]
- Khan, S.S.; Matsushita, K.; Sang, Y.; et al. Development and Validation of the American Heart Association's PREVENT Equations. Circulation 2024, 149, 430–449. [Google Scholar] [CrossRef]
- Gonzalez-Rodriguez, L.; Marti-Antonio, M.; Mota-Zamorano, S.; et al. Endothelin-1 as dual marker for renal function decline and associated cardiovascular complications in patients with chronic kidney disease. Eur J Intern Med 2025, 106542. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, L.M.; Robles, N.R.; Mota-Zamorano, S.; et al. Influence of variability in the cyclooxygenase pathway on cardiovascular outcomes of nephrosclerosis patients. Sci Rep 2023, 13, 1253. [Google Scholar] [CrossRef] [PubMed]
- Gervasini, G.; Verde, Z.; Gonzalez, L.M.; et al. Prognostic Significance of Amino Acid and Biogenic Amines Profiling in Chronic Kidney Disease. Biomedicines 2023, 11. [Google Scholar] [CrossRef]
- Foreman, K.J.; Marquez, N.; Dolgert, A.; et al. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016-40 for 195 countries and territories. Lancet 2018, 392, 2052–2090. [Google Scholar] [CrossRef]
- Seiler, S.; Wen, M.; Roth, H.J.; et al. Plasma Klotho is not related to kidney function and does not predict adverse outcome in patients with chronic kidney disease. Kidney Int. 2013, 83, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Sellier, A.B.; Seiler-Mussler, S.; Emrich, I.E.; et al. FGFR4 and Klotho Polymorphisms Are Not Associated with Cardiovascular Outcomes in Chronic Kidney Disease. Am. J. Nephrol. 2021, 52, 808–816. [Google Scholar] [CrossRef]
- Gunawan, A.; Fajar, J.K.; Tamara, F.; et al. Nitride oxide synthase 3 and klotho gene polymorphisms in the pathogenesis of chronic kidney disease and age-related cognitive impairment: a systematic review and meta-analysis. F1000Res 2020, 9, 252. [Google Scholar] [CrossRef]
- Yu, W.; Zhu, H.; Chen, X.; et al. Genetic Variants Flanking the FGF21 Gene Were Associated with Renal Function in Chinese Patients with Type 2 Diabetes. J Diabetes Res 2019, 2019, 9387358. [Google Scholar] [CrossRef]
Figure 1.
Endocrine actions of FGF19 in different target organs. Abbreviations: FGF19, fibroblast growth factor 19; FGFR1, fibroblast growth factor receptor 1; FGFR4, fibroblast growth factor receptor 4; FXR, farnesoid X receptor; β-Klotho, beta Klotho protein.
Figure 1.
Endocrine actions of FGF19 in different target organs. Abbreviations: FGF19, fibroblast growth factor 19; FGFR1, fibroblast growth factor receptor 1; FGFR4, fibroblast growth factor receptor 4; FXR, farnesoid X receptor; β-Klotho, beta Klotho protein.
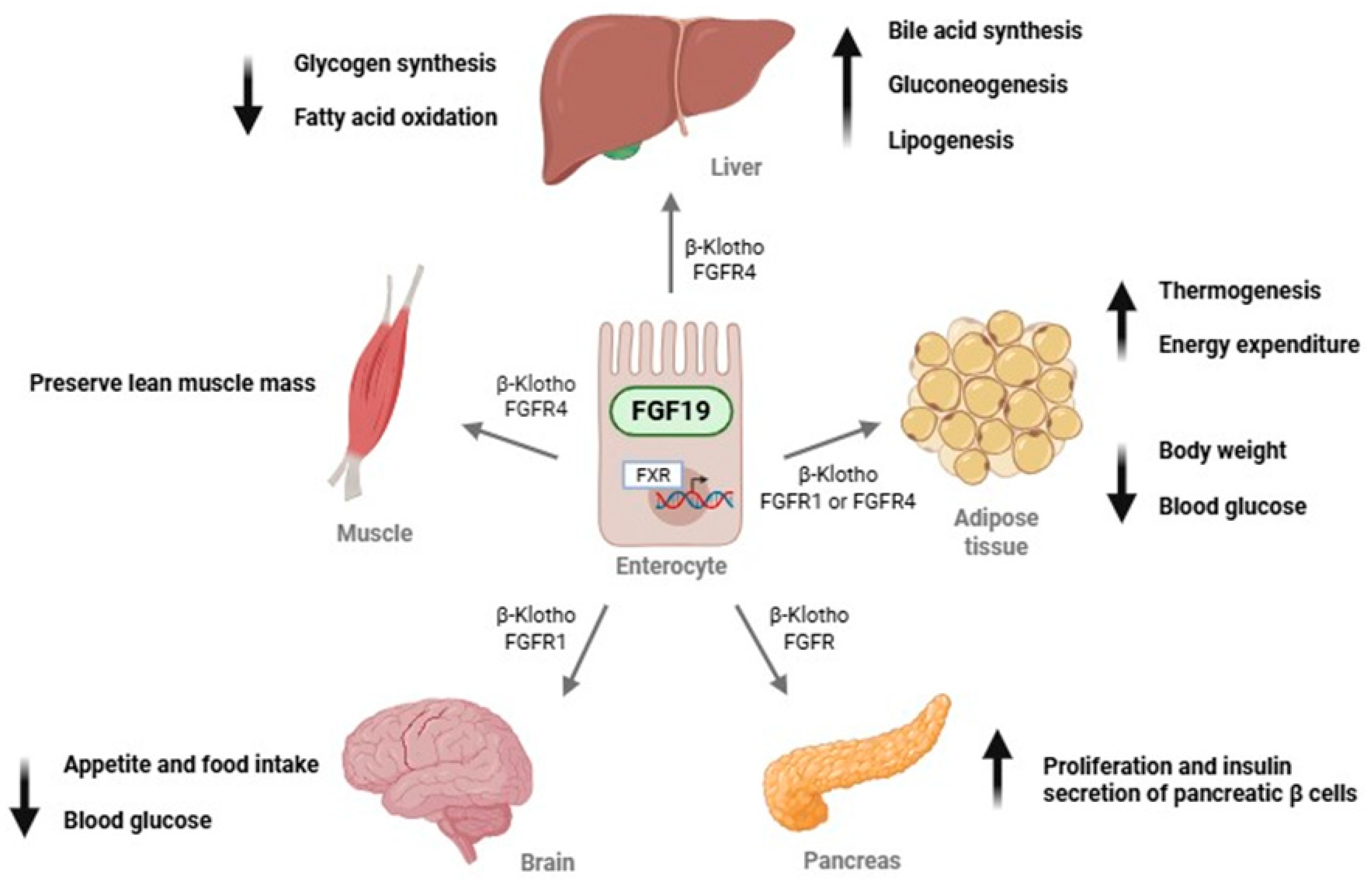
Figure 2.
Cluster analysis grouping both β-Klotho and FGF19 plasma concentrations in the cohort of renal patients.
Figure 2.
Cluster analysis grouping both β-Klotho and FGF19 plasma concentrations in the cohort of renal patients.
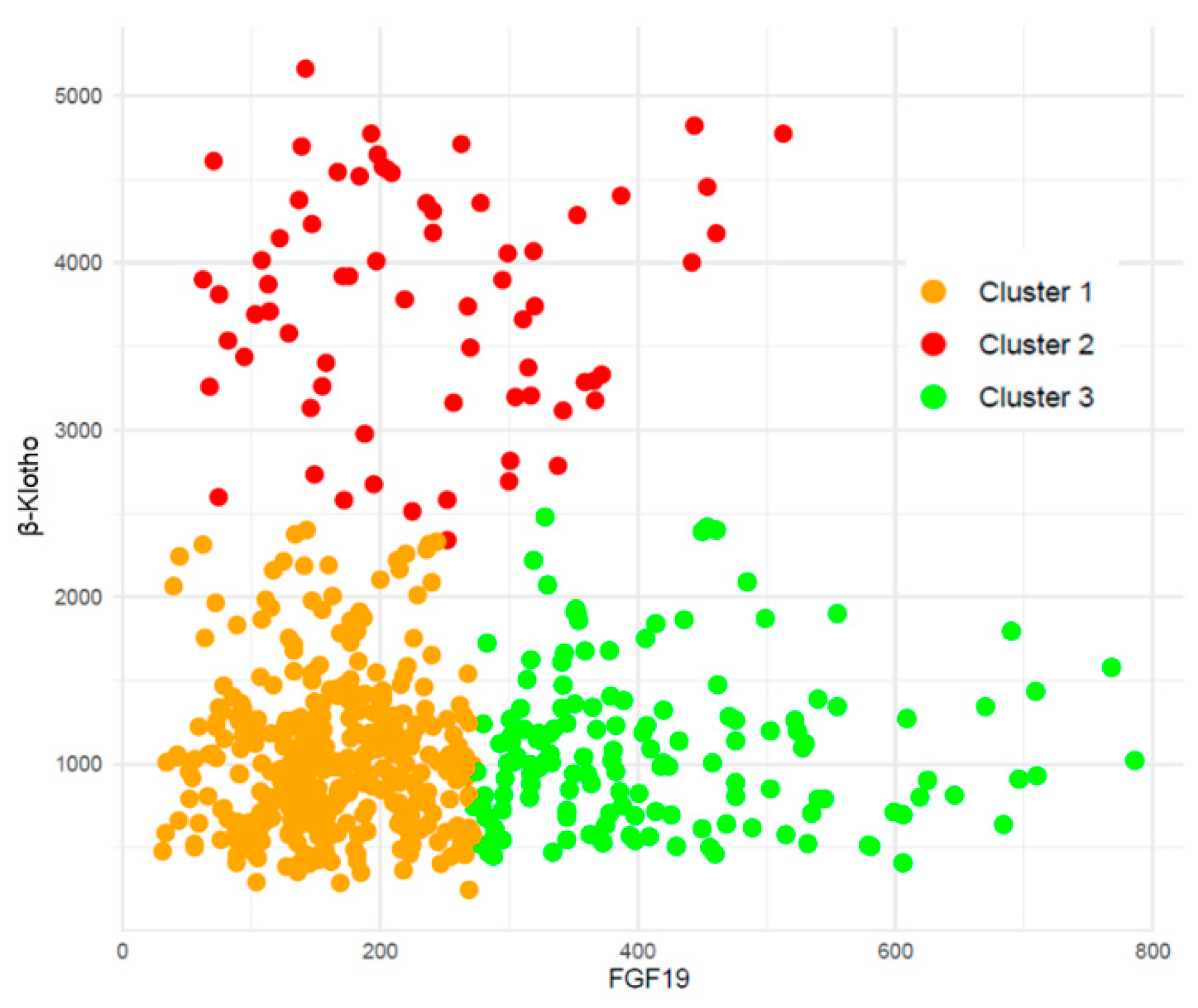
Figure 3.
Distribution of the FGF19/β-Klotho cluster groups across stages of chronic kidney disease (CKD).
Figure 3.
Distribution of the FGF19/β-Klotho cluster groups across stages of chronic kidney disease (CKD).
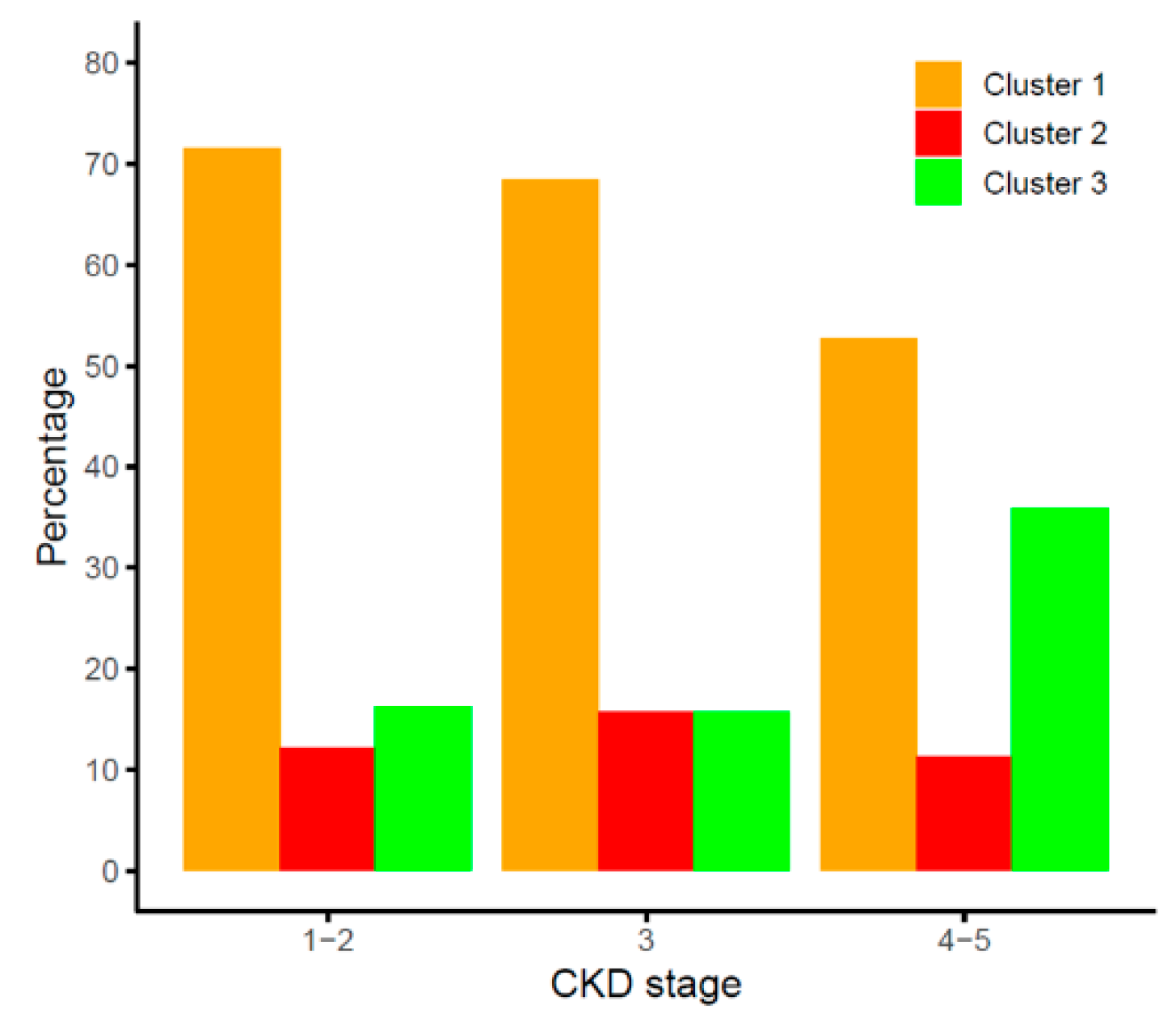
Figure 4.
Kaplan Meier curves for the association of FGF19/β-Klotho cluster groups with cardiovascular event-free survival in chronic kidney disease patients. *Cox-adjusted p<0.05 vs. cluster 3.
Figure 4.
Kaplan Meier curves for the association of FGF19/β-Klotho cluster groups with cardiovascular event-free survival in chronic kidney disease patients. *Cox-adjusted p<0.05 vs. cluster 3.
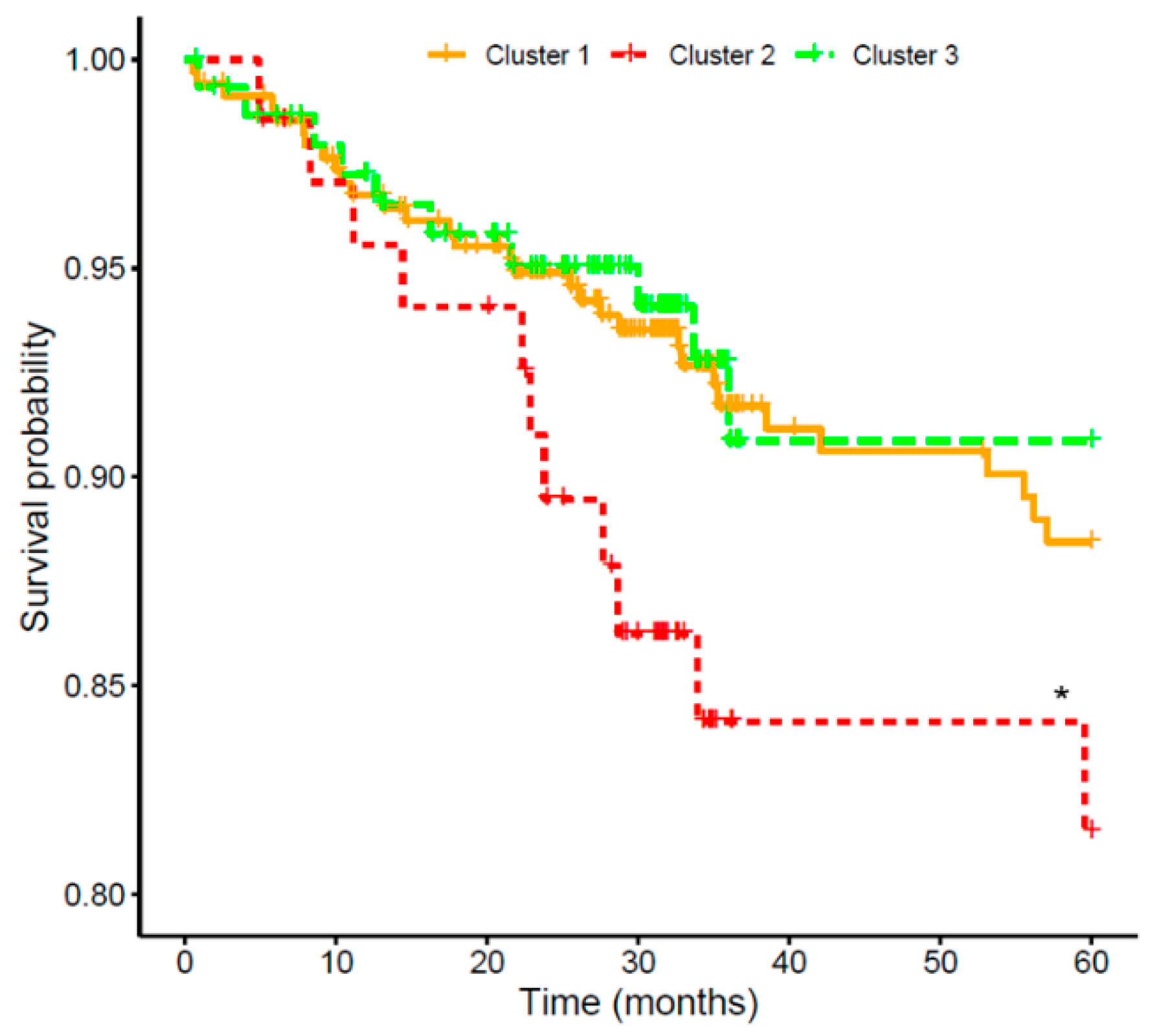
Figure 5.
Effect of SNP-pair interactions in the FGF19, KLB, FGFR1 and FGFR4 genes on the cardiovascular risk of patients with chronic kidney disease. The diagonal line contains the p-values from likelihood ratio test for the crude effect of each SNP. The upper triangle in the matrix contains the p-values for the interaction (epistasis) log-likelihood ratio test. The lower triangle contains the p-values from likelihood ratio test comparing the two-SNP additive likelihood to the best of the single-SNP models.
Figure 5.
Effect of SNP-pair interactions in the FGF19, KLB, FGFR1 and FGFR4 genes on the cardiovascular risk of patients with chronic kidney disease. The diagonal line contains the p-values from likelihood ratio test for the crude effect of each SNP. The upper triangle in the matrix contains the p-values for the interaction (epistasis) log-likelihood ratio test. The lower triangle contains the p-values from likelihood ratio test comparing the two-SNP additive likelihood to the best of the single-SNP models.
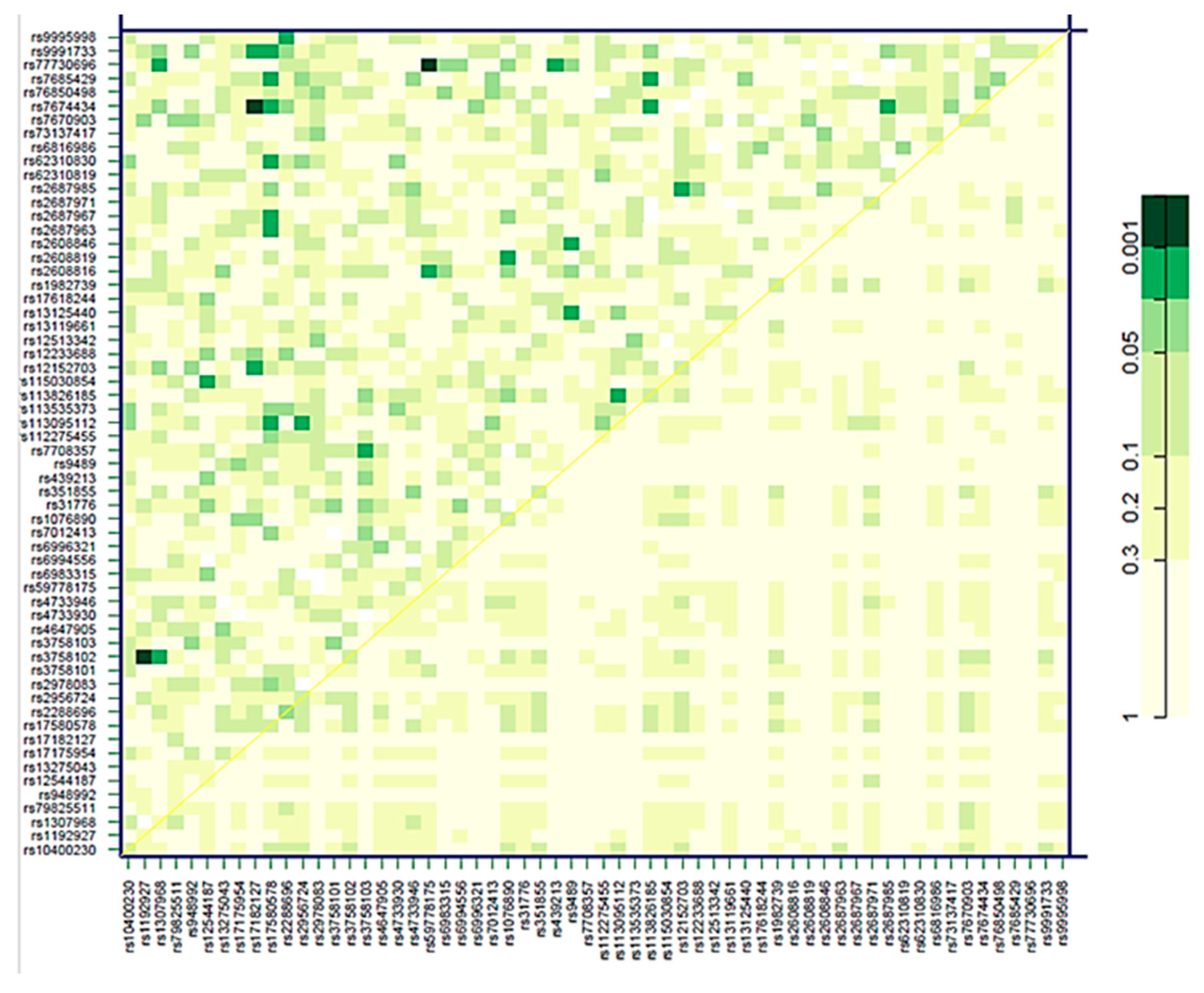
Figure 6.
Elastic-Net regularized Cox proportional hazards model to estimate the risk of cardiovascular events. Coefficients and relative importance of each variable in the model are shown.
Figure 6.
Elastic-Net regularized Cox proportional hazards model to estimate the risk of cardiovascular events. Coefficients and relative importance of each variable in the model are shown.
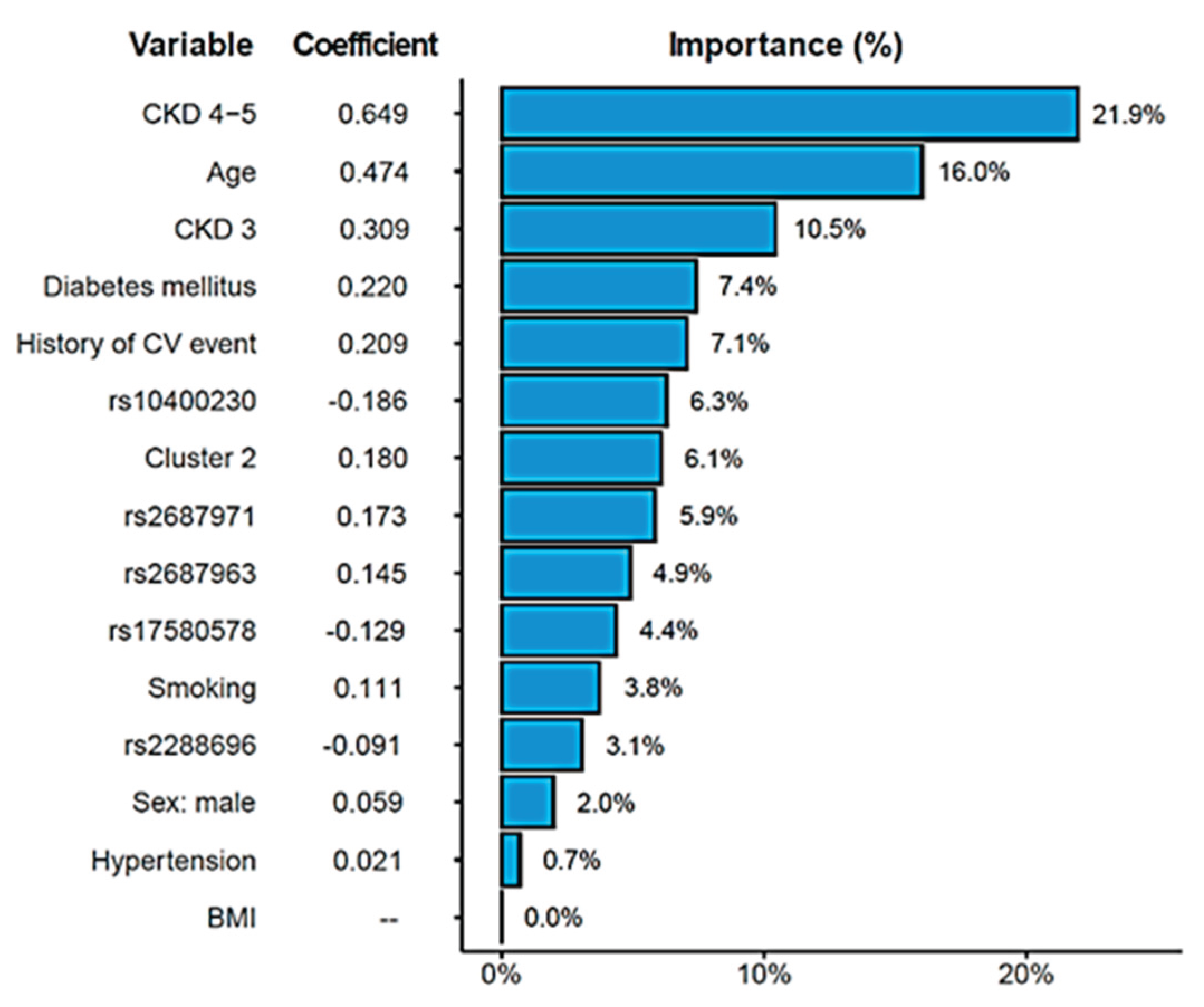

Table 1.
Characteristics of the studied patients with chronic kidney disease stratified by disease stage.
Table 1.
Characteristics of the studied patients with chronic kidney disease stratified by disease stage.
| CKD 1-2 (N=174) | CKD 3 (N=89) | CKD 4-5 (N=316) | *p | |
|---|---|---|---|---|
| Males (%) | 97 (55.7%) | 59 (66.3%) | 202 (63.9%) | 0.133 |
| Age (Years) | 58.0 (49.0-67.0) | 66.0 (60.0-75.0) | 71.0 (60.0-79.3) | <0.0001 |
| Weight (Kg) | 81.0 (66.3-91.4) | 79.7 (73.0-90.5) | 78.1 (67.1-89.1) | 0.108 |
| BMI | 28.3 (25.1-31.1) | 29.5 (26.8-32.4) | 28.8 (25.5-32.7) | 0.099 |
| Glucose (mg/dL) | 100.5 (93.0-112.0) | 111.0 (97.0-145.0) | 101.0 (90.0-119.3) | <0.0001 |
| Total cholesterol (mg/dL) | 173.0 (154.3-196.8) | 158.0 (138.0-199.0) | 144.0 (122.8-171.3) | <0.0001 |
| HDL cholesterol (mg/dL) | 54.0 (44.0-64.0) | 46.0 (37.0-54.0) | 45.0 (37.0-57.0) | <0.0001 |
| LDL cholesterol (mg/dL) | 96.0 (79.0-114.0) | 83.0 (62.0-109.5) | 68.7 (51.0-92.0) | <0.0001 |
| Total calcium (mg/dL) | 9.4 (9.3-9.7) | 9.6 (9.2-9.8) | 9.3 (8.9-9.6) | <0.0001 |
| Potassium (mEq/L) | 4.3 (4.1-4.6) | 4.7 (4.4-5.1) | 5.0 (4.5-5.3) | <0.0001 |
| Sodium (mEq/L) | 141.0 (140.0-143.0) | 142.0 (140.0-143.0) | 141.0 (139.0-142.0) | 0.0001 |
| ACR (mg/g) in urine 24h | 8.4 (4.2-31.3) | 97.7 (12.4-281.9) | 410.0 (139.4-1180.0) | <0.0001 |
| eGFR (mL/min/1.73 m2) | 98.9 (83.3-106.8) | 40.9 (33.7-49.0) | 16.4 (13.0-20.0) | <0.0001 |
| Systolic blood pressure (mmHg) | 132.0 (123.0-147.0) | 147.0 (129.5-164.0) | 144.0 (127.0-163.3) | <0.0001 |
| Diastolic blood pressure (mmHg) | 80.0 (74.0-89.0) | 80.0 (67.5-87.5) | 74.0 (66.0-85.0) | <0.0001 |
| Pulse pressure (mmHg) | 51.0 (43.0-64.0) | 67.0 (53.5-83.0) | 69.0 (51.0-86.3) | <0.0001 |
| Hypertension (%) | 0.042 | |||
| No | 40 (23.0%) | 16 (18.0%) | 44 (13.9%) | |
| Yes | 134 (77.0%) | 73 (82.0%) | 272 (86.1%) | |
| Diabetes (%) | <0.0001 | |||
| No | 143 (82.2%) | 40 (44.9%) | 167 (52.8%) | |
| Yes | 31 (17.8%) | 49 (55.1%) | 149 (47.2%) | |
| Smoking (%) | 0.304 | |||
| Nonsmoker | 84 (48.8%) | 33 (38.8%) | 140 (44.4%) | |
| Ever smoker | 88 (51.2%) | 52 (61.2%) | 175 (55.6%) | |
| Hyperlipidemia (%) | <0.0001 | |||
| No | 120 (69.0%) | 40 (44.9%) | 90 (28.6%) | |
| Yes | 54 (31.0%) | 49 (55.1%) | 224 (71.1%) |
ACR, albumin to creatinine ratio; BMI, body mass index; CKD, Chronic Kidney Disease; eGFR, estimated glomerular filtration rate. *p-value for the difference between the three groups.
Table 2.
Demographic and clinical variables of participants according to the presence or absence of cardiovascular events during the study.
Table 2.
Demographic and clinical variables of participants according to the presence or absence of cardiovascular events during the study.
| No CVE (N=527) | CVE (N=52) | p-value | |
|---|---|---|---|
| Males (%) | 322 (61.1%) | 36 (69.2%) | 0.214 |
| Age (Years) | 66 (56-75) | 72 (66-78) | <0.0001 |
| Weight (Kg) | 79 (68-90) | 79 (69-90) | 0.417 |
| BMI | 28.7 (25.5-32.5) | 28.9 (25.6-31.8) | 0.751 |
| Glucose (mg/dL) | 101.0 (91.0-117.0) | 123.0 (96.5-150.5) | 0.001 |
| Total cholesterol (mg/dL) | 158 (136-184) | 129 (117-175) | <0.0001 |
| HDL cholesterol (mg/dL) | 48 (39-60) | 43 (36-52) | 0.001 |
| LDL cholesterol (mg/dL) | 82 (61-104) | 60 (51-93) | 0.005 |
| Total calcium (mg/dL) | 9.4 (9.1-9.7) | 9.3 (8.9-9.6) | 0.116 |
| Potassium (mEq/L) | 4.7 (4.3-5.1) | 4.8 (4.4-5.3) | 0.613 |
| Sodium (mEq/L) | 141 (139-143) | 141 (139-142) | 0.990 |
| ACR (mg/g) in urine 24h | 156.5 (14.2-594.1) | 377.9 (73.3-1056.7) | <0.0001 |
| Troponin | 33.3 (21.5-51.6) | 49.3 (34.8-68.5) | 0.045 |
| NT_proBNP | 796 (307-2092) | 2923 (698-6538) | 0.007 |
| eGFR (ml/min/1.73 m2) | 26.0 (16.0-81.5) | 20.0 (15.0-42.3) | <0.0001 |
| Systolic blood pressure (mmHg) | 140 (125-159) | 149 (132-167) | 0.082 |
| Diastolic blood pressure (mmHg) | 77 (69-87) | 74 (66-84) | 0.025 |
| Pulse pressure (mmHg) | 61 (47-78) | 73 (60-86) | 0.001 |
| Hypertension (%) | 0.128 | ||
| No | 94 (17.8%) | 6 (11.5%) | |
| Yes | 433 (82.2%) | 46 (88.5%) | |
| History of CV event (%) | <0.0001 | ||
| No | 395 (75.4%) | 28 (54.9%) | |
| Yes | 129 (24.6%) | 23 (45.1%) | |
| Diabetes (%) | <0.0001 | ||
| No | 330 (62.6%) | 20 (38.5%) | |
| Yes | 197 (37.4%) | 32 (61.5%) | |
| CKD stages | <0.0001 | ||
| CKD 1-2 | 170 (32.3%) | 4 (7.7%) | |
| CKD 3 | 75 (14.2%) | 14 (26.9%) | |
| CKD 4-5 | 282 (53.5%) | 34 (65.4%) | |
| Smoking (%) | 0.308 | ||
| Non smoker | 238 (45.6%) | 19 (38.0%) | |
| Ever smoker | 284 (54.4%) | 31 (62.0%) | |
| Hyperlipidemia (%) | 0.032 | ||
| No | 234 (44.5%) | 16 (30.8%) | |
| Yes | 291 (55.3%) | 36 (69.2%) |
BMI, body-mass index; ACR, albumin to creatinine ratio; CV, cardiovascular; CKD, chronic kidney disease.
Table 3.
Significant associations of genetic variants with cardiovascular event-free survival. HR, hazard ratio.
Table 3.
Significant associations of genetic variants with cardiovascular event-free survival. HR, hazard ratio.
| SNP | Genotype | No CVE | CVE | HR (95% CI) | p-value |
|---|---|---|---|---|---|
| FGFR1 rs2288696 | G/G | 87.6% | 12.4% | Reference | |
| A/G, A/A | 91.5% | 8.5% | 0.51 (0.27,0.95) | 0.029 | |
| KLB rs2687971 | C/C | 91.9% | 8.1% | Reference | |
| CG, GG | 88.1% | 11.9% | 2.03 (0.97,4.27) | 0.046 |
CVE, cardiovascular events; HR (95% CI), hazard ratio with 95% confidence intervals.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



