
Submitted:
18 December 2025
Posted:
19 December 2025
You are already at the latest version
Abstract
Background: Epidemiological studies have established a positive association between water hardness, chlorine content, and the prevalence or severity of atopic dermatitis (AD). These environmental factors are known to exacerbate skin barrier dysfunction and increase discomfort in individuals with atopy-prone skin. Objectives: This research aimed to objectify the detrimental effects of hard and chlorinated water on atopic skin, both under controlled experimental conditions and in real-life settings. The studies assessed the efficacy of a daily dermocosmetic routine (comprising a cleanser and moisturizer adapted for atopy-prone skin) for reducing water-induced discomfort and improving the quality of life. Methods: Three clinical studies were conducted: one experimental comparative study of repeated washing or immersion with hard, chlorinated, and soft water, and two intra-individual 21-day studies on hard water and swimming pool water (chlorinated) exposure in real-life conditions. Results: Cumulative exposure to hard water (HW) and chlorinated water (CW) increased TEWL, while soft water (SW) had no significant effect on barrier function. The dermocosmetic routine significantly improved skin hydration and barrier function, with TEWL significantly decreasing by 25% (HW), 17% (CW), and 20% (SW) compared to untreated areas. In real-life studies, 21-day use of the products significantly reduced skin discomfort and improved quality of life. Conclusion: Repeated exposure to hard and chlorinated water can exacerbate skin discomfort and clinical symptoms of atopic dermatitis. An adapted daily dermocosmetic routine can significantly mitigate these effects, improving barrier function, skin comfort, and daily quality of life.
Keywords:
atopic dermatitis
; cosmetic routine
; hard water
; chlorinated water
; soft water
1. Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease marked by recurrent eczematous flares, intense pruritus, and xerosis, contributing to its burden [1]. It can cause physical discomfort, emotional distress, stigma, and daily activity limitations [2]. While genetic predisposition plays a key role in AD pathogenesis, environmental factors also influence disease onset and flares. Exposure to external stressors such as harsh cleansers, pollutants, climate changes, and water quality can impair the skin barrier and increase sensitivity to irritants and allergens [1]. Addressing these triggers is essential to optimize AD management and improve quality of life.
Epidemiological studies link high water hardness to increased AD prevalence, with evidence that early-life exposure may predispose children to eczema [3,4,5]. Hard water, rich in calcium carbonate (CaCO₃) and magnesium, may impair skin-barrier integrity via several mechanisms. By raising skin pH, it can enhance protease activity in the stratum corneum, accelerating the breakdown of corneodesmosomes and reducing lipid lamellae synthesis, ultimately leading to increased transepidermal water loss (TEWL) and skin dryness. It may also worsen eczema by increasing soap and detergent use, which can irritate dry skin. Soap reacts with calcium ions to form insoluble chalk-like particles, further aggravating eczematous skin [6]. Clinical studies have demonstrated that children, both with and without FLG mutations, exhibit greater TEWL when exposed to high CaCO₃ levels [7]. Large-scale population studies support this association, linking water hardness to barrier dysfunction [8,9]. An instrumental study comparing skin responses in AD patients and healthy controls found that hard water increased sodium lauryl sulfate deposition, aggravating TEWL and irritation, especially in FLG mutation carriers [10]. Chlorinated water, commonly used for disinfection, poses additional risks for AD patients. Sodium hypochlorite (NaClO) can induce oxidative stress and worsen epidermal barrier disruption. Its byproducts, especially nitrogen trichloride (trichloramine), are major irritants linked to skin inflammation, ocular discomfort, and respiratory irritation [11]. Exposure to chlorine in swimming pools has been linked to irritant or allergic contact dermatitis (“pool dermatitis” or “pool water dermatitis”) in sensitive individuals [12]. Despite these epidemiological findings, data on the direct biometrological impact of water hardness and chlorination on atopic skin remain limited.
European guidelines for AD management emphasize daily dermocosmetic care with gentle cleansers and regular emollient use to restore hydration and barrier integrity [13]. The dermocosmetic routine tested (NAOS, Laboratoire Bioderma, France) includes a pH-balanced cleansing oil and a soothing balm enriched with moisturizing and anti-inflammatory agents. Its benefits have been demonstrated in a 6-month clinical study used adjunctively or alternately with topical therapies [14]. Our studies aimed to experimentally assess the cumulative effects of repeated exposure to hard, chlorinated, and soft water on atopic skin, and evaluate the ability of this adapted dermocosmetic routine to mitigate these effects and improve comfort and quality of life.
2. Methods
2.1. Experimental Study: Repeated Immersion/Washing with Different Water Types (Hard, Chlorinated, Soft)
2.1.1. Study Design
This study was designed as an open, intra-individual controlled trial, in which each participant acted as their own control. Treated and non-treated forearm areas were randomly assigned, allowing for direct before/after comparisons as well as intra-subject assessments to evaluate the effects of water repeated exposure and dermocosmetic intervention.
2.1.2. Population
Subjects included in the study were adults over 18 years old with atopic skin but without an active eczema flare at the time of inclusion. Participants were excluded if they had cutaneous lesions on the study area or were receiving topical or systemic treatments that could potentially interfere with the study outcomes.
2.1.3. Interventions
Participants were divided into three groups, each exposed to a different type of water under standardised conditions. In the chlorinated water (CW) group, both forearms were immersed in chlorinated water at standard swimming pool concentrations for five successive 10-minute sessions per day over three consecutive days. After each immersion, the dermocosmetic routine was applied to one forearm, simulating two weeks of skincare application following repeated exposure to swimming pool water. In the hard water (HW) and soft water (SW) groups, both forearms underwent five consecutive 10-minute washing sessions per day for three days. The dermocosmetic routine was similarly applied to one forearm after each wash, mimicking two weeks of daily showering. In the HW group, water hardness was verified using Aquadur® 4–21 semi-quantitative test strips, confirming CaCO₃ levels >4.0 mol/m³.
2.1.4. Outcome Measures
The study assessed multiple biometrological and subjective parameters to assess the impact of water exposure and the protective effect of the dermocosmetic routine. TEWL was measured using the Tewameter® TM 300, while skin hydration index (HI) was assessed with the MoistureMap MM 100® (Courage & Khazaka) [14]. All measurements were performed under controlled environmental conditions (22 ± 2 °C; 35–55% relative humidity), using water maintained at 30 ± 2 °C. Participants rated their global cutaneous discomfort, including sensations of skin dryness, irritation, itching, tightness, and burning, on a self-assessment scale ranging from 0 (none) to 15 (severe). Evaluations were conducted before the first immersion/washing, immediately after each five-immersion/washing session, and one hour after the final session over the three-day study period, for both treated and untreated forearms.
2.1.5. Statistical Analysis
Before comparing treated and untreated forearms, data distribution was assessed using the Shapiro-Wilk normality test. If normality was rejected, the Wilcoxon signed-rank test was applied; otherwise, a paired Student’s t-test was used. For between-group comparisons, data normality was similarly assessed. If the assumption was violated, the Mann-Whitney U test was used; otherwise, an unpaired Student’s t-test was performed.
2.2. Impact of Hard Water and Swimming Pool Water Repeated Exposure on Atopic Skin in Real-Life Conditions
2.2.1. Study Design
Two intra-individual open studies evaluating the effects of HW or swimming pool exposure (chlorinated water) on subjects with atopic skin. The subjects used the same daily dermocosmetic routine previously described (cleanser and soothing balm) for 21 days.
2.2.2. Population
Subject aged over 18 years with atopic dermatitis according to the UK Working Party’s Diagnostic Criteria for Atopic Dermatitis (defined by the presence of pruritus and at least three associated criteria: xerotic skin, personal history of eczema, history of asthma, rhinitis or allergic conjunctivitis, latent eczema, or onset of symptoms before the age of two) [15]. For the HW study, participants were additionally required to live in cities with hard water and to use it daily for bathing or showering. For the swimming pool study, participants were required to attend a swimming pool for 2 to 3 sessions of 1 hour per week during the study period.
2.2.3. Interventions
Subjects followed a 21-day dermocosmetic routine, with the cleanser applied once or twice daily in place of their usual cleansing product, and the balm applied twice daily under normal conditions of use. Both products were applied to the entire body.
2.2.4. Outcome Measures
The study assessed both subjective and objective parameters to evaluate skin discomfort, quality of life, product satisfaction, and cutaneous acceptability over the 21-day period. Subjects performed a self-assessment of five skin discomfort parameters: itching, irritation, burning sensation, tightness, and dry skin sensation, using a 4-point scale (0 = none, 3 = severe). A global skin discomfort score was calculated by summing individual scores, ranging from 0 (very high comfort) to 15 (very low comfort/high discomfort). Assessments were conducted at three time points: (i) after the first exposure (FE) to a calcareous bath/shower or swimming pool (D0FE), (ii) after the first application of the dermocosmetic routine (D0), (iii) after 21 days of daily application of the dermocosmetic routine (D21).
Subjects completed the Dermatology Life Quality Index (DLQI) [16], a validated self-administered questionnaire consisting of 10 questions scored from 0 to 3, with a global score ranging from 0 to 30. This assessment was conducted at D0 and D21 to evaluate the impact of atopic skin on different aspects of health-related quality of life over the previous week. Cutaneous acceptability was evaluated under dermatological control at D0 and D21, assessing clinical and functional signs, complemented by a self-assessment by participants at the same time points. Subjects provided feedback on the efficacy, and skin acceptability.
2.2.5. Statistical Analysis
To evaluate intra-individual changes between baseline and post-intervention conditions, paired statistical tests were performed. Depending on data distribution, either paired Student’s t-tests or Wilcoxon signed-rank tests were used to assess the significance of changes in clinical scores, subjective evaluations, and quality-of-life outcomes between Day 0 (baseline) and Day 21. Statistical significance was defined as p < 0.05.
3. Results
3.1. Experimental Study: Repeated Immersion/Washing to Water (Hard, Chlorinated, Soft)
3.1.1. Participants
A total of 66 adults were enrolled, equally distributed into three groups (hard water, chlorinated water, soft water; n = 22 each) (Table 1).
3.1.2. Effect of Repeated Exposure to Water (HW, CW, SW) on Untreated Forearms
The impact of HW, CW, and SW on skin barrier function was assessed by measuring TEWL and HI on untreated forearms over the course of repeated exposure. For the CW group, compared to baseline (D0t0), a significant increase in TEWL was observed after repeated immersion sessions on D1T1h (+6%; p = 0.0439) and D2T1h (+7%; p = 0.0488), indicating a measurable alteration in skin barrier function. Similarly, repeated washing with HW led to a significant increase in TEWL at D2T1h (+4% vs D0t0; p = 0.0011). In contrast, repeated washing with SW did not affect the skin barrier function, as no significant change in TEWL was observed at the different assessment time points compared to baseline (Figure 1). A significant increase in HI compared to baseline was noted one hour after each immersion/washing session across all three groups (p < 0.05). No statistically significant change in global discomfort sensation was observed between baseline values and measurements taken one hour after immersion/washing on D0, D1, and D2.
The demographic data demonstrated no significant difference between the three groups in terms of age, gender and phototypes, so we performed a comparison between groups. Regarding the cumulative effect of repeated water exposure, no statistically significant overall degradation of the skin barrier was observed with HW and CW compared to SW in the context of this study. However, some significant differences were punctually shown between the groups, in particular in terms of TEWL and skin dryness self-assessment, with HW and CW showing a more pronounced negative impact compared to SW. At D1T1h, after ten washing cycles, a significant difference was observed between the HW and SW groups in terms of skin discomfort (-0.7% vs. +6%, respectively; p < 0.05) and skin dryness (-1.2% vs. +1.4%, respectively; p < 0.01). However, no statistical difference was detected between these groups at D0T1h and D2T1h. Similarly, at D0T1h, after five washing or immersion cycles, a significant difference was noted between the CW and SW groups in terms of skin dryness (-13% vs. +5%, respectively; p < 0.05). At D1T1h, after ten washing or immersion cycles, a significant increase in TEWL was observed in the CW group (+5%; p < 0.01), while no significant change was detected in the SW group (-0.5%; NS). A statistically significant difference was found in favor of the SW group (p < 0.01) (Figure 1; Supplementary data).
3.1.3. Effect of the Dermocosmetic Routine
An immediate and cumulative soothing effect of the dermocosmetic routine was observed, with significant decrease in cutaneous discomfort global score one hour after each cycle of five water immersions/washing, in each group (Figure 2). Compared to non-treated forearms, the dermocosmetic routine demonstrated significant higher improvements in skin hydration level and barrier function on the treated forearms in the three groups. After three days of repeated exposure, TEWL values decreased by -25% with HW, -17% with CW, and -20% with SW (p < 0.0001 vs. baseline D0T0), while HI values increased by 103% with HW, 122% with CW, and 101% with SW (significant difference of changes of HI and TEWL values) (Table 2; Figure 3).
No adverse reaction was observed during the experimental protocol on treated forearms.
3.2. Impact of Hard Water and Swimming Pool Water Repeated Exposure on Atopic Skin in Real-Life Conditions
3.2.1. Participants
A total of 33 adult subjects with atopic skin (history of atopic dermatitis without active lesions at the start of the study) were enrolled and completed each real-life study involving repeated exposure to hard or chlorinated water (Hard water study and Swimming pool water study). The demographic characteristics of the study population are summarized in Table 3.
3.2.2. Effect of the Dermocosmetic Routine
In both studies, the dermocosmetic routine demonstrated significant immediate and sustained soothing effects on atopic skin. Following the first application after a bath or shower with hard water, all discomfort parameters significantly decreased (p < 0.0001), with the global skin discomfort score improving by 56% (from 7.9 to 3.5; p < 0.0001). This effect was sustained over the 21 days, with continued use resulting in a 73% reduction (from 8.1 to 2.2; p < 0.0001), and all assessed skin discomfort parameters showed statistically significant decreases (p < 0.0001). In the Swimming pool water study, the first post-swimming application led to a 28% drop in discomfort (from 8.5 to 6.1; p < 0.0001). Over the 21-day period, cumulative application resulted in a 73% decrease in global discomfort (from 8.1 to 2.2; p < 0.0001), with all assessed parameters significantly reduced (p < 0.0001) (Table 3).
In both studies, the dermocosmetic routine significantly improved participants’ quality of life, as assessed by the DLQI. In the Hard water study, the mean DLQI score decreased by 81% (from 6.6 at D0 to 1.2 at D21; p < 0.0001), reflecting a shift from moderate to mild impact on daily life. In the Swimming pool water study, the mean DLQI score decreased by 82% (from 8.2 to 1.5) (Table 3). Notably, seven participants who initially reported a substantial impact (DLQI 11–20) showed minimal or no impact by D21 (mean score 0 to 1; p < 0.001). Higher score for “Over the last week how itchy, sore, painful or stinging has your skin been?” at D0 for both study group (1.36 to 0.18 in the hard water group) [17]. Before the study, 78% of subjects agreed or somewhat agreed that their atopic skin prevented them from going to the swimming pool. After 21 days of using the cosmetic routine, 94% of subjects agreed or somewhat agreed that the routine enabled them to go to the swimming pool despite their atopic skin.
No adverse reaction was observed after 21 days of products use in both studies.
4. Discussion
Epidemiological data suggest that hard water is linked to higher AD prevalence, with several mechanisms implicated in skin barrier impairment. Yet, few instrumental studies have directly assessed the effects of repeated water exposure on atopic skin. These studies aimed to evaluate the cumulative impact of hard, chlorinated, and soft water on skin barrier function and comfort, and to examine the protective role of a daily dermocosmetic routine.
Prior research has explored the effects of water on healthy skin with varying results. One study evaluating the impact of water exposure on experimentally irritated skin on the hands of healthy volunteers found no significant changes in barrier function after daily 30-minute immersion over two weeks [18]. However, a separate study demonstrated that TEWL significantly increased after just five minutes of water immersion, with cumulative effects observed within 10 minutes [19]. Additionally, a prospective observational study investigating the effects of water exposure and temperature on skin barrier function reported measurable damage, with hot water exposure leading to increased TEWL, elevated pH, and erythema [20]. These findings reinforce the concept that water exposure alone can affect skin homeostasis, and the extent of these effects is influenced by water composition and temperature.
Our primary objective was to design a controlled experimental protocol to assess biometrological changes in atopic skin following repeated exposure to hard and chlorinated water, compared with soft water. While repeated exposure to chlorinated and hard water did not yield consistently significant differences across all objective parameters, significant increases in TEWL were observed, suggesting a potential negative impact on skin barrier integrity. In contrast, repeated exposure to soft water did not significantly affect TEWL, reinforcing its neutrality regarding skin barrier function. Notably, at certain time points, significant differences were observed between hard and chlorinated water compared to soft water, supporting previous epidemiological findings suggesting that water quality can influence skin health. Several limitations must be acknowledged. The relatively small sample size may have limited statistical power, potentially underestimating subtle yet clinically relevant changes. The forearm, though methodologically appropriate and widely used for TEWL and hydration assessments, may not fully represent more reactive or affected AD sites such as the flexures, face, or hands. Still, its use ensured procedural consistency and comparability with prior studies. Additionally, flexural sites were avoided to minimize irritation risk from repeated washing, which could have biased results.
The role of an adapted dermocosmetic routine in maintaining skin hydration and improving comfort and quality of life in AD is well established. In a pilot study of 43 subjects with dry skin exposed to hard water, a 28-day dermocosmetic regimen significantly improved corneometry-measured hydration and reduced xerosis-related discomfort (unpublished data). These findings align with the present results, confirming the value of structured skincare in supporting barrier function and cutaneous comfort, even under harsh water conditions. Beyond instrumental outcomes, the observed DLQI improvements highlight the positive impact of dermocosmetic care on patients’ quality of life. These results reinforce the importance of integrating environmental considerations, such as water quality, into holistic AD management.
Larger studies with longer follow-up are needed to better understand the long-term effects of repeated water exposure and to explore the interplay between water composition, genetic predisposition, and skincare strategies to inform personalized recommendations in AD.
5. Conclusions
The studies conducted across different water types demonstrate that regular exposure can exacerbate skin discomfort and symptoms of atopic dermatitis. An adapted daily dermocosmetic routine, including a gentle cleanser and a hydrating moisturizer, can significantly mitigate these effects, improving skin comfort and barrier function. Beyond skin health, these results highlight the role of skincare in enhancing quality of life, allowing individuals with AD to maintain an active lifestyle and access leisure activities without restriction.
References
- Guttman-Yassky, E.; Renert-Yuval, Y.; Brunner, P.M. Atopic dermatitis. The Lancet 2025, 405, 583–596. [Google Scholar] [CrossRef] [PubMed]
- Gochnauer, H.; Valdes-Rodriguez, R.; Cardwell, L.; Anolik, R.B. The Psychosocial Impact of Atopic Dermatitis. In Management of Atopic Dermatitis;Advances in Experimental Medicine and Biology; Feldman, SR, Strowd, LC, Lovell, KK, Eds.; Springer International Publishing, 2024; Vol 1447, pp. 69–81. [Google Scholar] [CrossRef]
- Miyake, Y.; Yokoyama, T.; Yura, A.; Iki, M.; Shimizu, T. Ecological association of water hardness with prevalence of childhood atopic dermatitis in a Japanese urban area. Environ Res. 2004, 94, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Arnedo-Pena, A.; Bellido-Blasco, J.; Puig-Barbera, J.; et al. Dureza del agua de consumo doméstico y prevalencia de eczema atópico en escolares de Castellón, España. Salud Pública México 2007, 49, 295–301. [Google Scholar] [CrossRef] [PubMed]
- McNally, N.; Williams, H.; Phillips, D.; et al. Atopic eczema and domestic water hardness. The Lancet 1998, 352, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.S.; Dean, T.; O’Leary, C.; et al. A Randomised Controlled Trial of Ion-Exchange Water Softeners for the Treatment of Eczema in Children. In PLoS Med.; Sheikh, A, Ed.; 2011; Volume 8. [Google Scholar] [CrossRef]
- Perkin, M.R.; Craven, J.; Logan, K.; et al. Association between domestic water hardness, chlorine, and atopic dermatitis risk in early life: A population-based cross-sectional study. J Allergy Clin Immunol. 2016, 138, 509–516. [Google Scholar] [CrossRef] [PubMed]
- Engebretsen, K.A.; Bager, P.; Wohlfahrt, J.; et al. Prevalence of atopic dermatitis in infants by domestic water hardness and season of birth: Cohort study. J Allergy Clin Immunol. 2017, 139, 1568–1574.e1. [Google Scholar] [CrossRef]
- Jabbar-Lopez, Z.K.; Ung, C.Y.; Alexander, H.; et al. The effect of water hardness on atopic eczema, skin barrier function: A systematic review, meta-analysis. Clin Exp Allergy 2021, 51, 430–451. [Google Scholar] [CrossRef]
- Danby, S.G.; Brown, K.; Wigley, A.M.; et al. The Effect of Water Hardness on Surfactant Deposition after Washing and Subsequent Skin Irritation in Atopic Dermatitis Patients and Healthy Control Subjects. J Invest Dermatol 2018, 138, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Gomà, A.; De Lluis, R.; Roca-Ferrer, J.; Lafuente, J.; Picado, C. Respiratory, ocular and skin health in recreational and competitive swimmers: Beneficial effect of a new method to reduce chlorine oxidant derivatives. Environ Res. 2017, 152, 315–321. [Google Scholar] [CrossRef]
- Tlougan, B.E.; Podjasek, J.O.; Adams, B.B. Aquatic sports dermatoses: Part 1. In the Water: Freshwater Dermatoses. Int J Dermatol 2010, 49, 874–885. [Google Scholar] [CrossRef]
- Wollenberg, A.; Kinberger, M.; Arents, B.; et al. European guideline ( EuroGuiDerm ) on atopic eczema – part II: non-systemic treatments and treatment recommendations for special AE patient populations. J Eur Acad Dermatol Venereol. 2022, 36, 1904–1926. [Google Scholar] [CrossRef]
- Akdeniz, M.; Gabriel, S.; Lichterfeld-Kottner, A.; Blume-Peytavi, U.; Kottner, J. Transepidermal water loss in healthy adults: a systematic review and meta-analysis update. British Journal of Dermatology 2018, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.C.; Jburney, P.G.; Pembroke, A.C.; Hay, R.J. Atopic Dermatitis Diagnostic Criteria Working Party The, U.K. Working Party’s Diagnostic Criteria for Atopic Dermatitis. III. Independent hospital validation. Br J Dermatol 1994, 131, 406–416. [Google Scholar] [CrossRef] [PubMed]
- Finlay, A.Y.; Khan, G.K. Dermatology Life Quality Index (DLQI)-a simple practical measure for routine clinical use. Clin Exp Dermatol 1994, 19, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Hongbo, Y.; Thomas, C.L.; Harrison, M.A.; Sam Salek, M.; Finlay, A.Y. Translating the Science of Quality of Life into Practice: What Do Dermatology Life Quality Index Scores Mean? J Invest Dermatol 2005, 125, 659–664. [Google Scholar] [CrossRef] [PubMed]
- Ramsing, D.; Agner, T. Effect of water on experimentally irritated human skin. British Journal of Dermatology 1997, 364–367. [Google Scholar] [CrossRef]
- Nitiyarom, R.; Siriwat, N.; Wisuthsarewong, W. Transepidermal Water Loss after Water Immersion. Siriraj Med J. 2021, 73, 386–390. [Google Scholar] [CrossRef]
- Herrero-Fernandez, M.; Montero-Vilchez, T.; Diaz-Calvillo, P.; Romera-Vilchez, M.; Buendia-Eisman, A.; Arias-Santiago, S. Impact of Water Exposure and Temperature Changes on Skin Barrier Function. J Clin Med. 2022, 11, 298. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Change over time of TEWL (g/m2/h) on untreated forearms after repeated water exposure (* p < 0.05 versus D0T0; ¥ p < 0.01 for D1T1h-D1T0 chlorinated water versus soft water).
Figure 1.
Change over time of TEWL (g/m2/h) on untreated forearms after repeated water exposure (* p < 0.05 versus D0T0; ¥ p < 0.01 for D1T1h-D1T0 chlorinated water versus soft water).
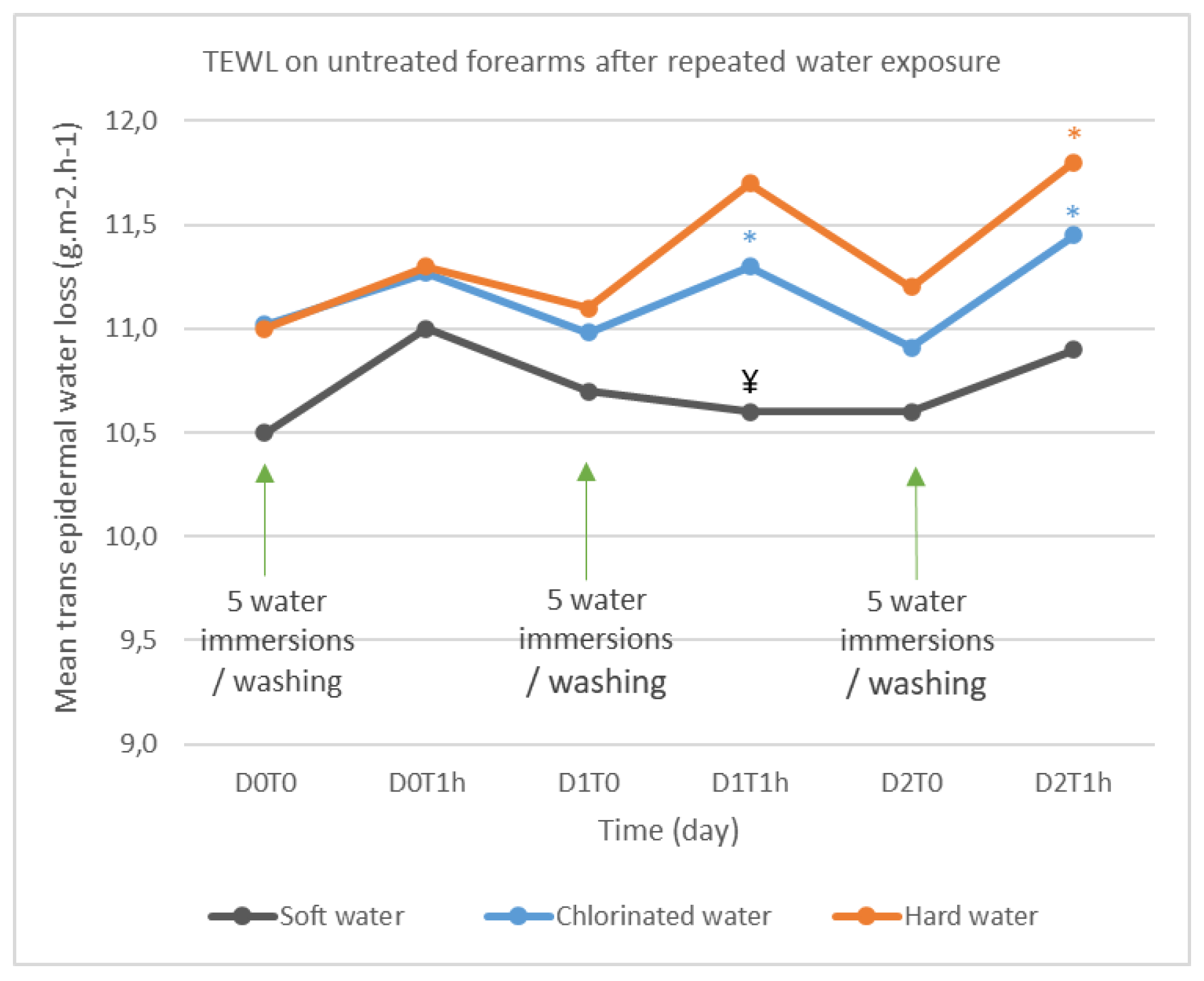
Figure 2.
Biophysical measurements of the skin barrier. Change over time of TEWL (g/m2/h) and HI (A.U.) on treated and untreated forearms after repeated water exposure (* p < 0.05; ** p < 0.001 versus untreated forearm).
Figure 2.
Biophysical measurements of the skin barrier. Change over time of TEWL (g/m2/h) and HI (A.U.) on treated and untreated forearms after repeated water exposure (* p < 0.05; ** p < 0.001 versus untreated forearm).
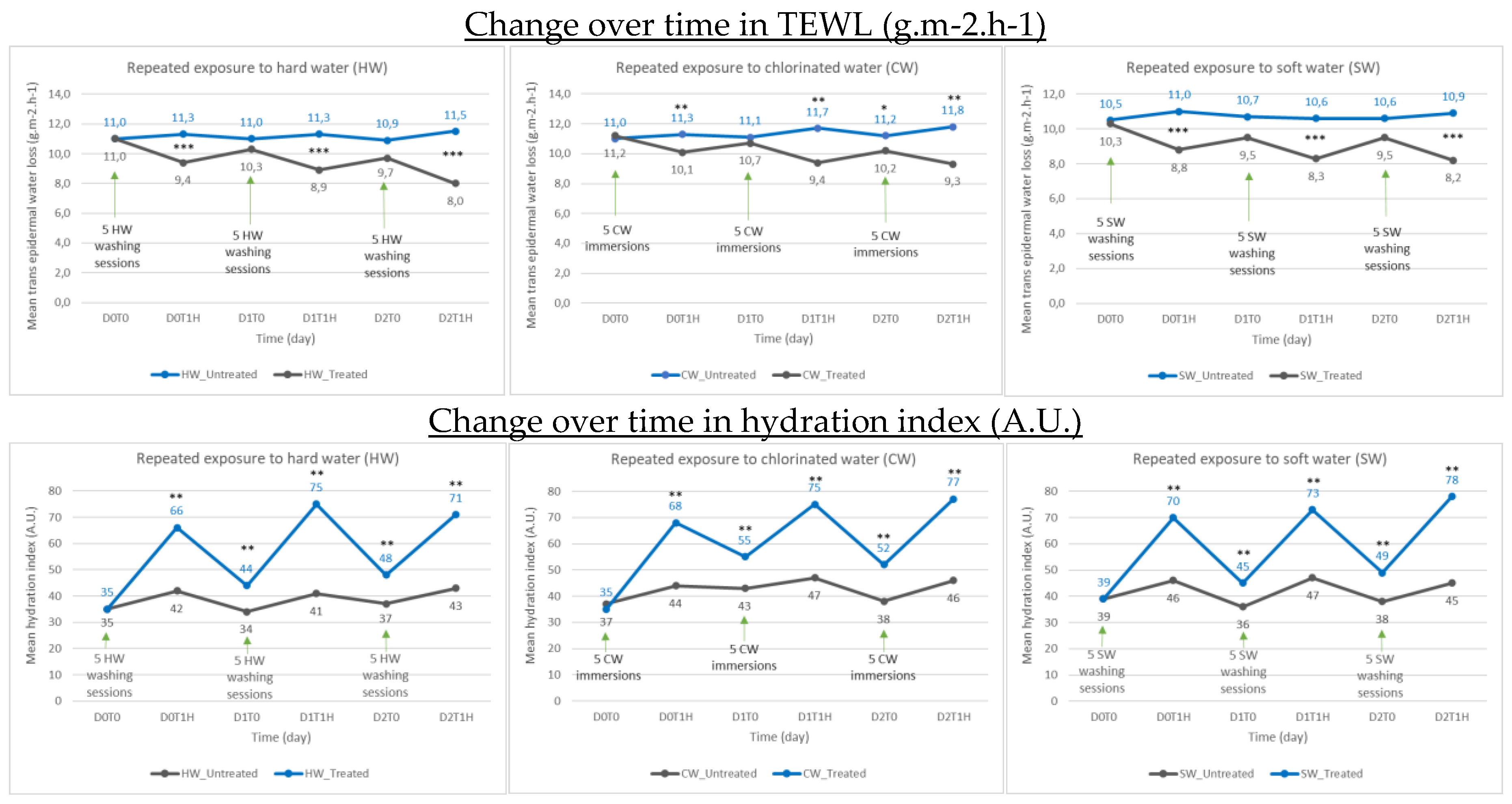
Figure 3.
Change in global cutaneous discomfort score on treated and untreated forearms after repeated water exposure (** p < 0.001 versus untreated forearm).
Figure 3.
Change in global cutaneous discomfort score on treated and untreated forearms after repeated water exposure (** p < 0.001 versus untreated forearm).
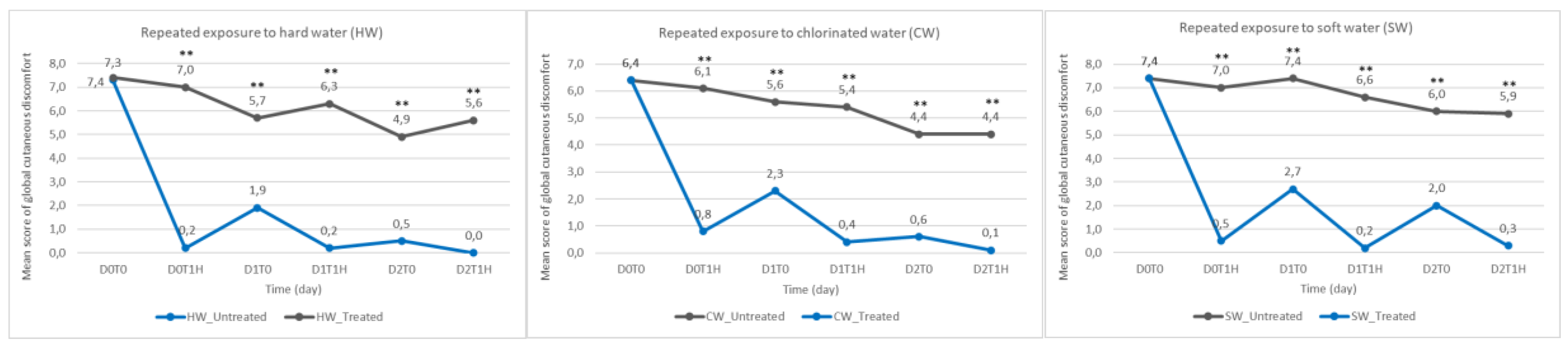

Table 1.
Demographic data.
| Experimental repeated immersion/washing study | Real-life conditions | |||||
| Hard water | Chlorinated water | Soft water | Hard water | Swimming pool water | ||
| Population | N | 22 | 22 | 22 | 33 | 33 |
| Age, years | Mean (S.D.) Range |
43.0 (12.8) 24-64 |
39.5 (12.4) 18-62 |
38.9 (13.6) 18-66 |
42.2 (16.1) 20-78 |
34.9 (12.9) 19-71 |
| Gender, n (%) |
Female Male |
20 (91) 2 (9) |
18 (81) 4 (18) |
22 (100) 0 (0) |
17 (52) 16 (48) |
14 (42) 19 (58) |
| Phototype, n (%) |
I II III |
0 (0) 33 (100) 0 (0) |
1 (5) 17 (77) 4 (18) |
0 (0) 15 (68) 7 (32) |
0 (0) 33 (100) 0 (0) |
0 (0) 33 (100) 0 (0) |
| Skin type, n (%) |
Dry skin Very dry skin |
12 (55) 10 (45) |
15 (68) 7 (32) |
12 (55) 10 (45) |
15 (45) 18 (55) |
5 (15) 28 (85) |
Table 2.
Comparison between treated (T) forearms with the dermocosmetic routine and non-treated (NT) forearms vs baseline (D0t0). AU, arbitrary units; ns, not significant.
Table 2.
Comparison between treated (T) forearms with the dermocosmetic routine and non-treated (NT) forearms vs baseline (D0t0). AU, arbitrary units; ns, not significant.
| Comparison | Mean difference ± S.D. | 95% Confidence Interval | p-value | Change (%) |
|---|---|---|---|---|
| TEWL (g/m2/h) | ||||
| Hard water T vs NT | ||||
| D0T1h – D0T0 | -2.00 ± 1.32 | -2.61; -1.39 | <0.0001 | -16.8 |
| D1T0 – D0T0 | -0.72 ± 0.74 | -1.06; -0.39 | 0.0002 | -6.5 |
| D1T1h – D0T0 | -2.49 ± 1.18 | -3.02; -1.96 | <0.0001 | -22.5 |
| D2T0 – D0T0 | -1.25 ± 1.09 | -1.73; -0.77 | <0.0001 | -11.3 |
| D2T1h – D0T0 | -3.22 ± 1.27 | -3.78; -2.66 | <0.0001 | -29.1 |
| Chlorinated water T vs NT | ||||
| D0T1h – D0T0 | -1.31 ± 1.56 | -2.02; -0.60 | 0.0010 | -11.7 |
| D1T0 – D0T0 | -0.53 ± 1.33 | -1.13; 0.08 | 0.0845 (ns) | -4.7 |
| D1T1h – D0T0 | -2.42 ± 1.52 | -3.11; -1.72 | <0.0001 | -21.7 |
| D2T0 – D0T0 | -1.17 ± 2.10 | -2.13; -0.22 | 0.0186 | -10.5 |
| D2T1h – D0T0 | -2.67 ± 2.34 | -3.73; -1.60 | <0.0001 | -23.9 |
| Soft water T vs NT | ||||
| D0T1h – D0T0 | -1.99 ± 1.43 | -2.63; -1.36 | <0.0001 | -19.3 |
| D1T0 – D0T0 | -0.96 ± 0.89 | -1.35; -0.56 | <0.0001 | -9.3 |
| D1T1h – D0T0 | -2.11 ± 0.78 | -2.45; -1.76 | <0.0001 | -20.5 |
| D2T0 – D0T0 | -0.97 ± 1.15 | -1.48; -0.46 | 0.0007 | -9.4 |
| D2T1h – D0T0 | -2.60 ± 1.28 | -3.18; -2.02 | <0.0001 | -24.8 |
| HI (A.U.) | ||||
| Hard water T vs NT | ||||
| D0T1h – D0T0 | 24.53 ± 10.32 | 19.95; 29.10 | <0.0001 | 69.8 |
| D1T0 – D0T0 | 9.79 ± 10.77 | 4.75; 14.83 | 0.0001 | 29.9 |
| D1T1h – D0T0 | 34.33 ± 11.29 | 29.33; 39.34 | <0.0001 | 97.6 |
| D2T0 – D0T0 | 11.25 ± 12.27 | 5.81; 16.69 | 0.0003 | 32.0 |
| D2T1h – D0T0 | 28.57 ± 15.93 | 21.32; 35.82 | <0.0001 | 81.7 |
| Chlorinated water T vs NT | ||||
| D0T1h – D0T0 | 26.12 ± 8.12 | 22.43; 29.82 | <0.0001 | 76.1 |
| D1T0 – D0T0 | 14.05 ± 9.16 | 9.34; 18.76 | <0.0001 | 41.3 |
| D1T1h – D0T0 | 29.70 ± 13.95 | 23.35; 36.05 | <0.0001 | 86.9 |
| D2T0 – D0T0 | 15.37 ± 11.05 | 10.34; 20.40 | <0.0001 | 44.4 |
| D2T1h – D0T0 | 32.93 ± 12.02 | 27.46; 38.40 | <0.0001 | 96.0 |
| Soft water T vs NT | ||||
| D0T1h – D0T0 | 25.36 ± 16.14 | 18.21; 32.52 | <0.0001 | 66.2 |
| D1T0 – D0T0 | 10.43 ± 10.89 | 5.02; 15.85 | 0.0008 | 26.2 |
| D1T1h – D0T0 | 26.62 ± 15.32 | 19.82; 33.41 | <0.0001 | 69.6 |
| D2T0 – D0T0 | 13.86 ± 13.34 | 7.79; 19.93 | 0.0001 | 32.3 |
| D2T1h – D0T0 | 32.56 ± 13.31 | 26.50; 38.61 | <0.0001 | 86.6 |
| Global cutaneous discomfort | ||||
| Hard water T vs NT | ||||
| D0T1h – D0T0 | -6.73 ± 1.84 | -7.54; -5.91 | <0.0001 | -91.7% |
| D1T0 – D0T0 | -3.72 ± 3.58 | -5.31; -2.13 | <0.0001 | -50.8% |
| D1T1h – D0T0 | -6.02 ± 2.97 | -7.34; -4.70 | <0.0001 | -82.1% |
| D2T0 – D0T0 | -4.36 ± 1.71 | -5.12; -3.61 | <0.0001 | -59.6% |
| D2T1h – D0T0 | -5.55 ± 1.53 | -6.22; -4.87 | <0.0001 | -75.7% |
| Chlorinated water T vs NT | ||||
| D0T1h – D0T0 | -5.29 ± 2.21 | -6.29; -4.28 | <0.0001 | -83.1% |
| D1T0 – D0T0 | -3.30 ± 2.72 | -4.53; -2.06 | <0.0001 | -51.8% |
| D1T1h – D0T0 | -4.92 ± 3.18 | -6.37; -3.47 | <0.0001 | -77.4% |
| D2T0 – D0T0 | -3.77 ± 3.33 | -5.29; -2.26 | <0.0001 | -59.2% |
| D2T1h – D0T0 | -4.33 ± 2.99 | -5.70; -2.97 | <0.0001 | -68.1% |
| Soft water T vs NT | ||||
| D0T1h – D0T0 | -6.43 ± 2.62 | -7.59; -5.27 | <0.0001 | -87.0% |
| D1T0 – D0T0 | -4.66 ± 3.46 | -6.20; -3.13 | <0.0001 | -63.1% |
| D1T1h – D0T0 | -6.35 ± 2.66 | -7.53; -5.18 | <0.0001 | -86.0% |
| D2T0 – D0T0 | -3.97 ± 3.17 | -5.38; -2.57 | <0.0001 | -53.8% |
| D2T1h – D0T0 | -5.63 ± 2.60 | -6.78; -4.47 | <0.0001 | -76.2% |
Table 3.
FE: after first exposure to hard or chlorinated water; FA: after first application of the dermocosmetic routine.
Table 3.
FE: after first exposure to hard or chlorinated water; FA: after first application of the dermocosmetic routine.
| Outcomes | ||||||
| Hard water study | ||||||
| Skin discomfort parameters | D0FA - D0FE (Mean ± SD) |
Change (%) | p-value | D21 - D0FE (Mean± SEM) |
Change (%) | p-value |
| Global score (0 to 15) | -2.4 ± 1.8 | -28% | <0.0001 | -5.9 ± 0.4 | -73% | <0.0001 |
| Itching (0 to 3) | -0.7 ± 0.5 | -35% | <0.0001 | -1.2 ± 0.1 | -69% | <0.0001 |
| Irritation sensation (0 to 3) | -0.5 ± 0.5 | -27% | <0.0001 | -1.1 ± 0.1 | -77% | <0.0001 |
| Burning sensation (0 to 3) | -0.4 ± 0.5 | -26% | 0.0001 | -1.0 ± 0.1 | -72% | <0.0001 |
| Tightness sensation (0 to 3) | -0.5 ± 0.5 | -28% | <0.0001 | -1.1 ± 0.1 | -78% | <0.0001 |
| Dry skin sensation (0 to 3) | -0.4 ± 0.5 | -21% | 0.0005 | -1.5 ± 0.1 | -73% | <0.0001 |
| DLQI | D21 - D0FE (Mean± SEM) |
Change (%) | p-value | |||
| Global score (0 to 30) | -5.4 ± 4.5 | -81% | <0.0001 | |||
| Swimming pool water study | ||||||
| Skin discomfort parameters | D0FA - D0FE (Mean ± SD) |
Change (%) | p-value | D21 - D0FE (Mean± SEM) |
Change (%) | p-value |
| Global score (0 to 15) | -4.4 ± 2.9 | -56% | <0.0001 | -8.7 ± 0.3 | -92% | <0.0001 |
| Itching (0 to 3) | -0.8 ± 0.7 | -51% | <0.0001 | -1.7 ± 0.1 | -86% | <0.0001 |
| Irritation sensation (0 to 3) | -0.9 ± 0.7 | -56% | <0.0001 | -1.8 ± 0.1 | -97% | <0.0001 |
| Burning sensation (0 to 3) | -0.8 ± 0.6 | -55% | <0.0001 | -1.6 ± 0.1 | -91% | <0.0001 |
| Tightness sensation (0 to 3) | -0.9 ± 0.7 | -60% | <0.0001 | -1.8 ± 0.1 | -97% | <0.0001 |
| Dry skin sensation (0 to 3) | -0.9 ± 0.7 | -56% | <0.0001 | -1.8 ± 0.1 | -91% | <0.0001 |
| DLQI | D21 - D0FE (Mean± SD) |
Change (%) | p-value | |||
| Global score (0 to 30) | -6.7 ± 5.3 | -82% | <0.0001 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



