Submitted:
17 December 2025
Posted:
19 December 2025
You are already at the latest version
Abstract
Eating disorders (ED) remain challenging to treat, with high dropout and low remission rates in cognitive-behavioral therapy for EDs (CBT-ED). Psilocybin treatment (PT) demonstrates therapeutic potential to enhance CBT-ED by exerting several neurobiological, psychological, and experiential effects (e.g., antidepressant, neuroplasticity, emotional openness) that are hypothesized to increase psychotherapeutic engagement, reduce dropout, and improve clinical outcomes. This article provides the first consolidation of existing theoretical evidence for PT/CBT-ED, proposes considerations for a con-current intervention protocol, and presents clinical and research considerations to empirically test its feasibility, safety, and efficacy. This line of inquiry is expected to advance the development of approaches that improve ED treatment outcomes and, more broadly, advance the study of psychedelics as tools to enhance evidence-based psychotherapy models.
Keywords:
psilocybin
; eating disorders
; psychotherapy
; psychedelic treatment
1. Introduction
Eating disorders (ED) are a group of severe psychiatric conditions that negatively impact quality of life and daily functioning in ~1-3% of the global population (Qian et al., 2022; Smink et al., 2012). Among the most frequently studied EDs, anorexia nervosa (AN), bulimia nervosa (BN), and binge eating disorder (BED) are characterized by maladaptive eating behaviors, neurocognitive dysfunction, and psychological distress, contributing to an increased risk of potentially fatal medical and psychiatric complications (Amianto et al., 2015; Castillo & Weiselberg, 2017; Harrington et al., 2015; van Eeden et al., 2021; van Hoeken & Hoek, 2020). The leading evidence-based treatment for EDs is cognitive-behavioral therapy (CBT-ED), developed to alter the cognitive and behavioral processes that maintain ED psychopathology (e.g., cognitive distortions about body shape and weight and dietary restraint) (Fairburn, 2008a; Fairburn et al., 2009; Murphy et al., 2010). However, sustained recovery following CBT-ED is only achieved in 40-50% of patients. Approximately 25-50% of patients dropout from CBT-ED prematurely, representing a major barrier to treatment success (Linardon, 2018; Linardon et al., 2018; Pinna et al., 2014).
The reason for suboptimal CBT-ED outcomes is not fully known and likely involves several neurobiological and psychological mechanisms associated with EDs and psychotherapeutic engagement (Coker et al., 1993; Fassino et al., 2009; Halmi, 2013; Steel et al., 2000; Vall & Wade, 2015). Dropout is associated with a lack of early symptom improvement, depressive symptoms, and experiential avoidance (Agras et al., 2000; Dixon et al., 2025; Fassino et al., 2002, 2009; Steel et al., 2000; Wagner et al., 2015). Pharmacotherapy can target mechanisms underlying suboptimal treatment response and premature dropout and has been shown to enhance outcomes when combined with psychotherapy for EDs (Grilo et al., 2024; Walsh et al., 1997). However, fluoxetine for BN and lisdexamfetamine for BED are the only pharmacological treatments approved for EDs, and, to our knowledge, no medications have demonstrated efficacy in significantly reducing dropout from CBT-ED (Crone et al., 2023, 1992; Rodan et al., 2023). There is a critical need to develop innovative approaches that enhance psychotherapeutic engagement and reduce dropout in ED clinical care.
Psilocybin treatment (PT) is emerging as a therapeutic approach in psychiatry, including robust antidepressant effects upon meta-analysis (Fang et al., 2024; Haikazian et al., 2023; Rosenblat et al., 2023) and reduced ED psychopathology in several small, open-label trials (Bevione et al., 2025; Gukasyan et al., 2022; Koning & Brietzke, 2023; Peck et al., 2023; Zhu et al., 2025). PT involves the administration of psilocybin—a plant alkaloid derived from the Psilocybe mushroom—in a medically supervised and psychologically supported context (Barber & Aaronson, 2022; Nichols, 2016). While PT most often occurs with general psychological support, there is growing scientific interest for its utility as a tool to enhance structured psychotherapies, supported by theoretical and empirical lines of evidence (Goodwin et al., 2024; Monson et al., n.d.; Sloshower et al., 2023; Wolff et al., 2025). For example, PT exerts several acute/subacute neurobiological (e.g., serotonergic, neuroplastic) and psychological (e.g., antidepressant, cognitive flexibility, experiential openness) effects that may be conducive to psychotherapeutic engagement and efficacy (Doss et al., 2021; MacLean et al., 2011; Mertens et al., 2020; Zhao et al., 2024). Therefore, leveraging PT to enhance evidence-based psychotherapy is considered a highly promising direction by both ED patients and experts in the psychedelic literature, but no study has investigated PT as a tool to enhance CBT-ED (Cuerva et al., 2024; Goodwin et al., 2024; Wolff et al., 2025).
The standard PT model is largely derived from historical research practices, involving non-specific, non-directive psychological support throughout preparation, dosing and integration sessions (Brennan & Belser, 2022; Cavarra et al., 2022; Kelly et al., 2021). However, transdiagnostic evidence and preliminary trials in EDs suggest that the addition of structured, evidence-based psychotherapy alongside PT may be necessary for improved and sustained behavioral changes (Johnson et al., 2017; Peck et al., 2023). Moreover, experts in the psychedelic literature call for the development of standardized psychotherapy protocols to improve reporting, measure fidelity, and promote replicability (Brennan & Belser, 2022; Cavarra et al., 2022; Chisamore et al., 2024; Hultgren et al., 2025). No publications have formally consolidated the theoretical rationale or developed a combined PT/CBT-ED protocol. Therefore, the current paper aims to do so by proposing PT/CBT-ED protocol considerations, specifically for non-underweight EDs (i.e., BED and BN), contextualized by its therapeutic rationale and implications for future research to test its feasibility, safety, and efficacy in ED treatment.
2. Methods
To characterize the theoretical rationale for PT/CBT-ED, a literature search was conducted to identify theoretical and empirical evidence for an effect of psilocybin treatment on CBT retention and outcomes in EDs. The online databases PubMed, PsycINFO, and Embase were searched for relevant publications from inception to September 2025 using a combination of the terms: psilocybin, psychotherapy, eating disorders, bulimia, anorexia, binge eating, body image, depressive symptoms, neuroplasticity, dropout, engagement, therapeutic alliance, cognitive/psychological flexibility, social function, and psychedelic experience. Additional sources were identified via bibliographic search inspection and targeted search. The articles included in this narrative review were not selected systematically and cannot be classified as all-inclusive.
To develop considerations for the development of the PT/CBT-ED protocol, the authors consulted established CBT-ED and psychedelic therapy manuals (e.g., MAPS Manual for MDMA-Assisted Psychotherapy, Yale Manual for Psilocybin-Assisted Therapy), and relevant scientific literature specific to ED psychotherapy (e.g., Russell et al., 2023). As extensive work has already been done to develop psychedelic psychotherapy frameworks, the focus of protocol considerations prioritized modifications of the traditional PT model that may be beneficial to participants with EDs, to reduce anticipated risks and enhance any therapeutic effects. The following questions guided the development of protocol considerations: 1) Who should conduct PT and CBT-ED sessions and what formal training should be required to do so?; 2) How many PT sessions (i.e., preparation, dosing, integration) should be conducted alongside CBT-ED and when should they be conducted?; 3) In the context of an ED, what content should be included in the preparation session(s)?; 4) What are important considerations for psychological and medical support during the dosing session?; 5) In the context of an ED, what should be included in the integration session(s), including linking session content to CBT-ED concepts?; and 6) Are there any other important considerations to address in the development of a PT/CBT-ED protocol?
3. Theoretical Rationale for PT/CBT-ED
The hypothesis that PT will augment the effects of CBT-ED (e.g., improve dropout rates and enhance clinical outcomes) represents a logically valid argument that is testable, falsifiable and clear (Thompson & Skau, 2023). Although never empirically tested, the potential additive therapeutic effect of PT and CBT-ED is supported by several converging empirical and theoretical findings (Fairburn et al., 2009; Öst et al., 2024; Evens et al., 2023; Majić et al., 2015; Sampedro et al., 2017). The specific neurobiological and psychological mechanisms underlying this rationale and supporting the primary hypothesis introduced herein are described in the following sections and summarized in Table 1.
3.1. Neurobiological Effects
3.1.1. Serotonergic Neurotransmission
Psilocybin exerts several neurobiological effects that are hypothesized to augment the effects of CBT-ED, demonstrated by several lines of preclinical and clinical research. Psilocybin is often referred to as a serotonergic psychedelic, a classification that reflects the similarities in chemical structure between psilocybin and the neurotransmitter serotonin (Adebo et al., 2025; Nichols, 2016). As such, the agonistic effects of psilocin—the active metabolite of psilocybin—at serotonin receptors is well-documented, indicating a mechanism for increased serotonergic neurotransmitter signaling following psilocybin administration (Adebo et al., 2025; Madsen et al., 2019; Wulff et al., 2023). Serotonin is crucially implicated in eating behavior, cognition and mood regulation (Bailer & Kaye, 2011; Steiger, 2004). A substantial body of evidence suggests dysfunctional serotonin signaling (i.e., altered post-synaptic receptor sensitivity, reduced serotonergic neurotransmission) is part of the body of observed neurobiological alterations contributing to ED symptoms (Becker et al., 2022; Madsen et al., 2019; Monteleone et al., 2000). Further, EDs are associated with clinical response to serotonergic medications, with selective serotonin reuptake inhibitors being a commonly prescribed pharmacotherapy for EDs and, in the case of fluoxetine, the only approved pharmacotherapy for BN (Davis & Attia, 2017, 1992; Rodan et al., 2023). It is therefore reasonable to deduce that the serotonergic effects of psilocybin may similarly be beneficial to ED clinical outcomes by normalizing neurotransmitter signaling in serotonergic pathways. Although no study has empirically assessed the relationship between psilocybin-induced serotonergic signaling and clinical outcomes in EDs, the serotonergic effects of psilocybin have been shown to correlate with greater acute psychoactive effects, the latter of which reliably predicts the magnitude of depressive symptom reduction (Levin et al., 2024; Madsen et al., 2019; Roseman et al., 2017; Stenbæk et al., 2021).
3.1.2. Neuroplasticity
Psilocybin is included in the class of pharmacotherapies termed psychoplastogens, a group of therapeutics that rapidly promote structural and functional neuroplasticity (Olson, 2018). Neuroplasticity is a fundamental process for the adaptation and improvement of neural, psychological and behavioral processes, defined as the brain’s ability to change in response to internal and external stimuli. Psilocybin has been shown to stimulate neuroplasticity-related processes, including increased dendritic spine growth, synaptogenesis, and elevated levels of brain-derived neurotrophic factor (BDNF) in preclinical and human studies. Similar to many psychiatric conditions, neuroplasticity is reduced in EDs and considered a biomarker of treatment responsiveness (Keeler et al., 2022, 2024; Phillips et al., 2014; Shobeiri et al., 2022; Zhao et al., 2024). For example, individuals with AN have significantly lower levels of BDNF when compared to the general population (Keeler et al., 2022, 2023; Shobeiri et al., 2022). Regarding psychotherapeutic success, experts suggest psychoplastogens should be paired with structured therapy to not only channel neuroplastic changes toward desired outcomes, but also to avoid maladaptive outcomes (Jones, 2025). In a synergistic manner, the transient period (2-4 weeks) of heightened neuroplasticity induced by psilocybin, often termed the ‘psychedelic after-glow,’ is hypothesized to potentiate the cognitive and behavioral patterns introduced by CBT-ED, thereby supporting durable therapeutic change (Evens et al., 2023; Jones, 2025; Majić et al., 2015).
3.1.3. Neural Network Connectivity
Beyond receptor-level effects, psilocybin induces alterations in large-scale neural network connectivity, as consistently demonstrated by functional neuroimaging studies (Carhart-Harris et al., 2012; Gattuso et al., 2023; Siegel et al., 2024). Specifically, psilocybin is associated with disrupted functional connectivity in the default mode, salience and executive control networks—all of which are implicated in critical cognition- and emotion-related processes. In EDs, altered functional connectivity among the aforementioned neural networks is often observed and associated with cognitive inflexibility, a hypothesized mediator of poor psychotherapy engagement (Gattuso et al., 2023; Koning et al., 2024; Steward, 2024). For example, BN is associated with reduced neural signaling for prediction errors that are critical for reliably and flexibly updating beliefs and cognitions (Berner et al., 2023; Frank et al., 2011). By disrupting large-scale neural networks, psilocybin may create a state of cognitive flexibility that is conducive to psychological flexibility, behavioral modification and learning—changes that both counteract alterations observed in EDs and are beneficial for engagement in psychotherapy (Carhart-Harris et al., 2012; Carhart-Harris & Friston, 2019; Doss et al., 2021; Rutschmann et al., 2024). In depression, alterations in neural network connectivity have been shown to correlate with clinical outcomes (Daws et al., 2022).
Together, the aforementioned neurobiological effects have been implicated in the transdiagnostic therapeutic potential of PT and provide a constellation of potential mechanistic correlates for the psychological manifestations that will be beneficial for CBT-ED. For example, the serotonergic and antidepressant effects of psilocybin are expected to remove a critical barrier (i.e., mood symptoms) to engagement and CBT-ED, thereby reducing drop-out. Alterations to neuroplasticity and neural network connectivity are expected to promote enhanced CBT-ED outcomes by fostering learning and durable cognitive/behavioural change. See Koning et al., (2024) for a supplemental review of the potential neurobiological correlates of PT in EDs (Koning et al., 2024).
3.2. Psychological Effects
3.2.1. Body Image
Body image disturbances are considered key factors in the maintenance of EDs, including shape/weight-related concerns, fear of weight gain, and/or self-evaluation unduly influenced by body weight and shape in BN and AN (Fairburn, 2008b; Levinson et al., 2017). Although not considered a core criterion for BED, those who report body weight/shape overvaluation tend to have higher levels of overall ED psychopathology and distress when compared to individuals with BED without body weight/shape overvaluation (Grilo, 2013; Lydecker et al., 2017). As such, body image disturbance is considered a major psychological barrier to positive CBT-ED outcomes and often predicts symptom improvement (Calugi & Dalle Grave, 2019; Vall & Wade, 2015). PT is associated with rapid and sustained changes in maladaptive thoughts and cognitions, providing an opportunity to shift distorted and rigid high-level priors that uphold body image disturbances (Carhart-Harris & Friston, 2019; Ho et al., 2020). Calder et al. (2023) provide a more in-depth discussion of the proposed mechanisms in which PT may help overcome maladaptive cognitions related to body image in EDs via altered interoceptive awareness, reduced self-referential processing, and increased self-acceptance (Calder et al., 2023). The potential of PT to counteract body image disturbance is supported by previous PT trials in EDs, including the reorganization of values in AN and reduced body image preoccupation in body dysmorphic disorder (Peck et al., 2023; Zhu et al., 2025). For example, in a phase 1 trial of PT for AN, 60% of participants felt as though the importance they placed on their physical appearance had decreased posttreatment (Peck et al., 2023). These changes align with the established therapeutic goals of CBT-ED and may help accelerate therapeutic change in this domain (Askew et al., 2020; Fairburn, 2008a; Grilo et al., 2009).
3.2.2. Psychiatric Comorbidities
Emotional dysregulation, and depressive and anxiety symptoms represent common comorbidities in EDs and significant barriers to psychotherapy success. For example, EDs carry high lifetime rates of depression (76.3% for BN, 65.5% for BED, and 49.5% for AN) and approximately two-thirds of patients will meet the criteria for an anxiety disorder (Attia & Walsh, 2025; Godart et al., 2003; Kaye et al., 2004; Swinbourne et al., 2012). Depressive symptoms are a well-documented predictor of poor engagement and drop-out in CBT-ED (Coker et al., 1993; Schnicker et al., 2013; Steel et al., 2000). Similarly, anxiety (e.g., fear of weight gain) poses a barrier to psychotherapy retention and greater early reductions in anxiety predicts ED symptom improvement post-treatment (Gorrell et al., 2023; Velkoff et al., 2024). Several meta-analyses demonstrate that PT exerts robust antidepressant effects (Fang et al., 2024; Haikazian et al., 2023; Rosenblat et al., 2023) and reduces anxiety, albeit the strongest evidence for anxiolytic effects of PT is in the context of end-of-life distress (Feulner et al., 2023; Irizarry et al., 2022). It is therefore reasonable to hypothesize that PT may help overcome CBT-ED barriers (e.g., drop-out and poor engagement) and improve ED outcomes via antidepressant and anxiolytic effects. As reviewed by Calder et al. (2023), the mechanisms of PT also demonstrate potential to improve symptoms of other common comorbidities with EDs, including posttraumatic stress disorder, substance use disorder, and obsessive-compulsive disorder which further complicate and challenge CBT-ED (Calder et al., 2023).
3.2.3. Social Functioning
Social dysfunction is often observed in EDs and correlates with symptom onset, severity, and treatment response (Agras et al., 2000; Keller et al., 1992; Lie et al., 2019; Raykos et al., 2017). Difficulties in social functioning in EDs may manifest as interpersonal avoidance, impaired social reward processing, heightened sensitivity to social evaluation, and challenges building and maintaining relationships (Cardi et al., 2018). Such deficits are not only detrimental to overall quality of life and daily functioning in EDs but may also challenge CBT-ED engagement and success by compromising the therapeutic alliance which is among the strongest predictors of positive outcomes (Graves et al., 2017). Psychedelics have been shown to stimulate oxytocin release—a neuropeptide involved in prosocial behavior—and increase synaptic plasticity in neural circuits responsible for social reward learning (Holze, Avedisian, et al., 2021; Holze, Vizeli, et al., 2021). These changes may improve general social functioning and strengthen the therapeutic alliance, which is hypothesized to promote CBT-ED success (Accurso et al., 2015; Graves et al., 2017).
3.2.4. Social Functioning
Beyond improved relations with others, transdiagnostic empirical and theoretical evidence suggests that PT may help individuals improve their self-relationship and promote general well-being that may be conducive to positive CBT-ED outcomes. EDs frequently involve negative self-appraisals, shame, and experiential avoidance—factors that pose a significant challenge to the cognitive restructuring and self-acceptance goals of CBT-ED (Marques et al., 2021; Nechita et al., 2021; Scott et al., 2014; Waller & Beard, 2024). PT increases emotional processing, openness, and positive changes in subjective well-being in clinical and non-clinical populations (MacLean et al., 2011; Mertens et al., 2020; Wiepking et al., 2023). Participants commonly report sustained increases in self-acceptance, self-compassion, connectedness to values, and perceived insight into the root cause of one’s psychological issues (Crowe et al., 2023; Fauvel et al., 2023; Watts et al., 2017). These changes have been effectively communicated via qualitative analyses, including in a previous PT trial for AN (Breeksema et al., 2024; Crowe et al., 2023; Cuerva et al., 2024; Peck et al., 2025). A recent large-scale survey of prescription and non-prescription drug use in individuals with EDs (N=5123) found that psilocybin was among the highest self-rated drugs for, not only ED symptom improvement, but also overall mental health (Rodan et al., 2025). Together, these general salutary effects are hypothesized to target barriers to psychotherapeutic engagement and success in EDs, including experiential avoidance, self-criticism and shame (Erritzoe et al., 2019; Mertens et al., 2020; Nechita et al., 2021; Sønderland et al., 2024; Wiepking et al., 2023). Moreover, improvements in general well-being may support broader recovery trajectories, including fostering healthier lifestyle behaviors, self-efficacy and improved quality of life which may be protective against relapse (Heal-Cohen et al., 2025).
In most cases, PT elicits the changes described above in 1-2 dosing sessions, suggesting an opportunity to accelerate therapeutic progress and strengthen engagement with the addition of PT to the CBT-ED protocol. This may be especially beneficial considering that early improvement is the strongest predictor of positive CBT-ED outcomes (Dixon et al., 2025; MacDonald & Trottier, 2019).
4. Considerations for PT/CBT-ED Protocol Development
The proposed protocol for a combined PT and CBT-ED intervention has been developed based on the hypothetical premise that it will have synergistic therapeutic effects for individuals with EDs. While the intervention primarily focuses on CBT-ED for non-underweight EDs, potential applications to CBT for anorexia nervosa (CBT-AN) are mentioned in the discussion section. This intervention is not intended for current clinical use but is designed to investigate its therapeutic efficacy in future clinical studies.
The CBT-ED component consists of a structured, time-limited adaptation specifically designed to address core ED symptoms, including binge eating, purging, and associated cognitive distortions. Brief CBT-ED, also known as CBT-Ten or CBT-T, is an evidence-based psychotherapy model for non-underweight EDs, comprising ten sessions followed by follow-up at one and three months (Keegan et al., 2022; Paphiti & Newman, 2023). The proposed intervention involves a standard course of CBT-T augmented by two adjunctive PT sessions, scheduled after the first and fifth CBT-T sessions (see Figure 1). These time points are critical, as outcome data indicate high dropout risks after session one—when rapid, anxiety-provoking behavioral changes are introduced—and after session five, when challenging body image work begins (Dixon et al., 2025).
The PT sessions follow traditional psychedelic therapy practices, structured as a three-step model involving preparation, dosing, and integration. The preparation session is a 90-minute session in a private therapy room the day before dosing, involving the CBT-T therapist and one PT therapist who will attend the dosing session. Its aims include building rapport, setting therapeutic intentions, establishing boundaries for nondirective emotional support, gathering participant history, assessing readiness, providing education on psilocybin's psychoactive effects (including potential adverse physical and psychological impacts), and explaining dosing logistics and safety measures.
The dosing session occurs in a controlled setting with the CBT-T therapist and PT therapist present, lasting up to eight hours, during which participants listen to ambient instrumental music (with input on the playlist) and are monitored for safety before discharge. The environment is private and quiet, free from interruptions, with comfortable seating or lying areas, optional eye masks and headphones, blankets, temperature control, aesthetic appeal, access to food, drink, and bathrooms, locked windows, stereo equipment, video-recording tools, medical supplies, and secure storage for records and investigational products. Aims for this session focus on cultivating an optimal "set" (i.e., mindset, intentions, expectations) and "setting" (i.e., physical space, therapists, music), offering nondirective support with a "beginner's mind" (i.e., approaching internal experience with openness, curiosity, and nonjudgment; allowing thoughts, emotions, and sensations to arise without preconceived expectations or attempts to control the experience), addressing any resistance through processing rather than avoidance, and ensuring safety and tolerability.
The integration session is a 90-minute follow-up the day after dosing, held in a private therapy room with the CBT-T therapist and PT therapist. Its aims involve assessing the participant's tolerance of PT and linking therapeutic insights to CBT-T concepts, reviewing and processing the dosing experience, including emotional distress, cognitive dilemmas, and affirming insights, and anchoring lessons into daily life to actualize behavioral changes for ED recovery. This includes recognizing the evolving nature of insights, encouraging ongoing support connections, and acknowledging that others (e.g., family members) may not fully grasp the experience's depth.
For a session-by-session summary of the CBT-T protocol, including integration considerations with PT, refer to Table 2.
5. Discussion
5.1. Implications
The present article consolidates the theoretical and empirical foundations supporting PT as an adjunct to CBT-ED, and proposes considerations for protocol development. The hypothesis that the neurobiological and psychological mechanisms of PT will improve CBT-ED outcomes should be tested in future interventional trials of feasibility, acceptability, tolerability, and preliminary efficacy (e.g., improved ED symptoms and reduced CBT-ED drop-out). Our research group plans to do this, although broader use of the protocol considerations in the development of population-specific PT protocols is encouraged. For example, although the protocol outlined above is specific to CBT for non-underweight EDs, a similar approach could be applied to CBT for AN with adaptations to address the unique needs of this population (e.g., ego-syntonic features, weight regain, extended treatment duration). If empirically supported, PT/CBT-ED could address the critical challenge of drop-out and poor outcomes that limit therapeutic success from first-line psychotherapies for EDs.
More broadly, the proposed intervention contributes to the advancement of conventional psychedelic therapy models which are largely based on traditional approaches that include non-directive, non-specific psychological support; these psychotherapy components are often inadequately defined and emphasize concepts of the “inner-healer.” The present framework departs from this historical model by embedding a structured, evidence-based psychotherapy (i.e., CBT-ED) both as concurrent sessions and throughout PT integration. Upon further development of the treatment manual, this shift towards protocol-based psychotherapy may help address longstanding methodological criticisms of psychedelic treatments such as poor fidelity and replicability, and difficulty isolating drug effects from psychotherapy effects. From a clinical perspective, the incorporation of structured psychotherapy may promote more durable behavioural change, as described by the rationale presented above.
5.2. Limitations
The major limitation of the interventional framework presented herein is the lack of empirical evidence testing PT-assisted psychotherapies in EDs and the regulatory barriers that continue to hinder this line of inquiry (e.g., psilocybin is a Schedule III controlled substance in Canada). Currently, there are no placebo-controlled trials of PT combined with CBT-ED, and only a handful of small, open-label studies have examined PT in ED populations. Another criticism of PT is the resource-intensive nature of the intervention, including specialized provider training, medical supervision, and drug costs. However, recent economic modelling suggests potential long-term cost savings via improved patient outcomes; for example, Avanceña et al. (2025) found that PT had a 75% probability of being more cost-effective than standard of care for treatment-resistant depression (Avanceña et al., 2025).
5.3. Safety & Tolerability Considerations
Psilocybin exhibits a favorable acute safety profile when administered at standard doses (up to 30mg) in medically-supervised settings (Fang et al., 2024; Freitas et al., 2025; Hinkle et al., 2024). The most common (17-40% of cases) side effects are typically mild and transient including nausea, dizziness, fatigue, anxiety, sympathomimetic effects and headache (Hinkle et al., 2024). However, patients with EDs may present unique medical and psychological vulnerabilities such as electrolyte imbalances, cardiovascular abnormalities (e.g., bradycardia, arrhythmias), and possible distress from vomiting/nausea or body image distortions during the dosing session (Downey et al., 2024; Lacroix et al., 2024). These risks warrant careful screening prior to participation in PT, as well as medical monitoring during dosing to manage adverse reactions and provide psychological support throughout challenging experiences. In a PT trial in AN, no serious adverse events or significant changes in vital signs occurred and the intervention was deemed safe and tolerable (Peck et al., 2023).
5.4. Research Recommendations
Moving forward, several publications call for increased funding for psychedelic studies in EDs (Bevione et al., 2025; Otterman, 2023; Xi et al., 2023) and studies which examine PT as an add-on to evidence-based psychotherapy (Cuerva et al., 2024; Goodwin et al., 2024; Wolff et al., 2025). Pilot trials are needed to establish feasibility, optimal dosing, acceptability, and preliminary efficacy of PT/CBT-ED. Subsequent phase II randomized, double-blind, placebo-controlled trials should incorporate active comparator arms to address functional unblinding and expectancy bias which remain major methodological limitations in psychedelic research (van Elk & Fried, 2023). The mechanisms proposed above may be investigated via neurobiological (e.g., neuroimaging, plasma neurotrophin analysis) and phenomenological approaches in order to extract insights about precise therapeutic actions (Koning et al., 2025). If there is sufficient evidence of therapeutic efficacy, larger trials should examine durability of intervention outcomes, long-term safety, and cost-effectiveness as appropriate. Increased public and private funding, expanded investigator training programs, and regulatory facilitation will be critical to realizing this research agenda.
6. Conclusion
Together, this article presents existing evidence to support the therapeutic potential of a combined PT/CBT-ED intervention—a potential solution to the critical problem of poor psychotherapy outcomes and high drop-out in EDs. Considerations for a concurrent intervention framework are also provided to facilitate future research initiatives evaluating the utility of PT to enhance evidence-based psychotherapy models. This line of inquiry is expected to contribute to the development of innovative approaches that improve ED treatment and, more broadly, advance the study of psychedelics as tools to enhance evidence-based psychotherapy models.
Author Contributions
Conceptualization, E.K. and A.K.; writing—original draft preparation, E.K., A.K. and S.G.; writing—review and editing, E.K., A.K. and S.G. All authors have read and agreed to the published version of the manuscript.
Funding
E.K. is funded by the Killam Postdoctoral Fellowship.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
E.K. has received payment from CAN-BIND Solutions for contract work for the Centre for Psychedelics Health & Research at Queen’s University.
Abbreviations
The following abbreviations are used in this manuscript:
| ED | Eating Disorders |
| AN | Anorexia Nervosa |
| BN | Bulimia Nervosa |
| BED | Binge eating disorder |
| CBT | Cognitive-behavioral therapy |
| PT | Psilocybin treatment |
| MAPS | Multidisciplinary Association for Psychedelic Studies |
| MDMA | 3,4-methylenedioxymethamphetamine |
| BDNF | Brain-derived neurotrophic factor |
References
- Accurso, E. C.; Fitzsimmons-Craft, E. E.; Ciao, A.; Cao, L.; Crosby, R. D.; Smith, T. L.; Klein, M. H.; Mitchell, J. E.; Crow, S. J.; Wonderlich, S. A.; Peterson, C. B. Therapeutic alliance in a randomized clinical trial for bulimia nervosa. Journal of Consulting and Clinical Psychology 2015, 83, 637–642. [Google Scholar] [CrossRef]
- Adebo, M.; Bonnet, M.; Laouej, O.; Defaix, C.; McGowan, J. C.; Butlen-Ducuing, F.; David, D. J.; Poupon, E.; Tritschler, L.; Gardier, A. M. Psilocybin as Transformative Fast-Acting Antidepressant: Pharmacological Properties and Molecular Mechanisms. Fundamental & Clinical Pharmacology 2025, 39, e70038. [Google Scholar] [CrossRef]
- Agras, W. S.; Crow, S. J.; Halmi, K. A.; Mitchell, J. E.; Wilson, G. T.; Kraemer, H. C. Outcome predictors for the cognitive behavior treatment of bulimia nervosa: Data from a multisite study. The American Journal of Psychiatry 2000, 157, 1302–1308. [Google Scholar] [CrossRef]
- Amianto, F.; Ottone, L.; Abbate Daga, G.; Fassino, S. Binge-eating disorder diagnosis and treatment: A recap in front of DSM-5. BMC Psychiatry 2015, 15, 70. [Google Scholar] [CrossRef]
- Askew, A. J.; Peterson, C. B.; Crow, S. J.; Mitchell, J. E.; Halmi, K. A.; Agras, W. S.; Haynos, A. F. Not all body image constructs are created equal: Predicting eating disorder outcomes from preoccupation, dissatisfaction, and overvaluation. The International Journal of Eating Disorders 2020, 53, 954–963. [Google Scholar] [CrossRef] [PubMed]
- Attia, E.; Walsh, B. T. Eating Disorders: A Review. JAMA 2025, 333, 1242–1252. [Google Scholar] [CrossRef]
- Avanceña, A. L. V.; Vuong, L.; Kahn, J. G.; Marseille, E. Psilocybin-assisted therapy for treatment-resistant depression in the US: A model-based cost-effectiveness analysis. Translational Psychiatry 2025, 15, 330. [Google Scholar] [CrossRef] [PubMed]
- Bailer, U. F.; Kaye, W. H. Serotonin: Imaging Findings in Eating Disorders. Current Topics in Behavioral Neurosciences 2011, 6, 59–79. [Google Scholar] [CrossRef]
- Barber, G. S.; Aaronson, S. T. The Emerging Field of Psychedelic Psychotherapy. Current Psychiatry Reports 2022, 24, 583–590. [Google Scholar] [CrossRef]
- Becker, A. M.; Holze, F.; Grandinetti, T.; Klaiber, A.; Toedtli, V. E.; Kolaczynska, K. E.; Duthaler, U.; Varghese, N.; Eckert, A.; Grünblatt, E.; Liechti, M. E. Acute Effects of Psilocybin After Escitalopram or Placebo Pretreatment in a Randomized, Double-Blind, Placebo-Controlled, Crossover Study in Healthy Subjects. Clinical Pharmacology & Therapeutics 2022, 111, 886–895. [Google Scholar] [CrossRef]
- Berner, L. A.; Fiore, V. G.; Chen, J. Y.; Krueger, A.; Kaye, W. H.; Viranda, T.; de Wit, S. Impaired belief updating and devaluation in adult women with bulimia nervosa. Translational Psychiatry 2023, 13, 2. [Google Scholar] [CrossRef]
- Bevione, F.; Lacidogna, M. C.; Lavalle, R.; Abbate Daga, G.; Preti, A. Psilocybin in the treatment of eating disorders: A systematic review of the literature and registered clinical trials. Eating and Weight Disorders 2025, 30, 58. [Google Scholar] [CrossRef] [PubMed]
- Breeksema, J. J.; Niemeijer, A.; Krediet, E.; Karsten, T.; Kamphuis, J.; Vermetten, E.; van den Brink, W.; Schoevers, R. Patient perspectives and experiences with psilocybin treatment for treatment-resistant depression: A qualitative study. Scientific Reports 2024, 14, 2929. [Google Scholar] [CrossRef]
- Brennan, W.; Belser, A. B. Models of Psychedelic-Assisted Psychotherapy: A Contemporary Assessment and an Introduction to EMBARK, a Transdiagnostic, Trans-Drug Model. Frontiers in Psychology 2022, 13. [Google Scholar] [CrossRef]
- Calder, A.; Mock, S.; Friedli, N.; Pasi, P.; Hasler, G. Psychedelics in the treatment of eating disorders: Rationale and potential mechanisms. European Neuropsychopharmacology: The Journal of the European College of Neuropsychopharmacology 2023, 75, 1–14. [Google Scholar] [CrossRef]
- Calugi, S.; Dalle Grave, R. Body image concern and treatment outcomes in adolescents with anorexia nervosa. The International Journal of Eating Disorders 2019, 52, 582–585. [Google Scholar] [CrossRef]
- Cardi, V.; Tchanturia, K.; Treasure, J. Premorbid and Illness-related Social Difficulties in Eating Disorders: An Overview of the Literature and Treatment Developments. Current Neuropharmacology 2018, 16, 1122–1130. [Google Scholar] [CrossRef]
- Carhart-Harris, R. L.; Erritzoe, D.; Williams, T.; Stone, J. M.; Reed, L. J.; Colasanti, A.; Tyacke, R. J.; Leech, R.; Malizia, A. L.; Murphy, K.; Hobden, P.; Evans, J.; Feilding, A.; Wise, R. G.; Nutt, D. J. Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proceedings of the National Academy of Sciences 2012, 109, 2138–2143. [Google Scholar] [CrossRef] [PubMed]
- Carhart-Harris, R. L.; Friston, K. J. REBUS and the Anarchic Brain: Toward a Unified Model of the Brain Action of Psychedelics. Pharmacological Reviews 2019, 71, 316–344. [Google Scholar] [CrossRef]
- Castillo, M.; Weiselberg, E. Bulimia Nervosa/Purging Disorder. Current Problems in Pediatric and Adolescent Health Care 2017, 47, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Cavarra, M.; Falzone, A.; Ramaekers, J. G.; Kuypers, K. P. C.; Mento, C. Psychedelic-Assisted Psychotherapy—A Systematic Review of Associated Psychological Interventions. Frontiers in Psychology 2022, 13. [Google Scholar] [CrossRef]
- Chisamore, N.; Johnson, D.; Chen, M. J. Q.; Offman, H.; Chen-Li, D.; Kaczmarek, E. S.; Doyle, Z.; McIntyre, R. S.; Rosenblat, J. D. Protocols and practices in psilocybin assisted psychotherapy for depression: A systematic review. Journal of Psychiatric Research 2024, 176, 77–84. [Google Scholar] [CrossRef]
- Coker, S.; Vize, C.; Wade, T.; Cooper, P. J. Patients with bulimia nervosa who fail to engage in cognitive behavior therapy. The International Journal of Eating Disorders 1993, 13, 35–40. [Google Scholar] [CrossRef]
- Crone, C.; Fochtmann, L. J.; Attia, E.; Boland, R.; Escobar, J.; Fornari, V.; Golden, N.; Guarda, A.; Jackson-Triche, M.; Manzo, L.; Mascolo, M.; Pierce, K.; Riddle, M.; Seritan, A.; Uniacke, B.; Zucker, N.; Yager, J.; Craig, T. J.; Hong, S.-H.; Medicus, J. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders. American Journal of Psychiatry 2023, 180, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Crowe, M.; Manuel, J.; Carlyle, D.; Lacey, C. Experiences of psilocybin treatment for clinical conditions: A qualitative meta-synthesis. International Journal of Mental Health Nursing 2023, 32, 1025–1037. [Google Scholar] [CrossRef]
- Cuerva, K.; Spirou, D.; Cuerva, A.; Delaquis, C.; Raman, J. Perspectives and preliminary experiences of psychedelics for the treatment of eating disorders: A systematic scoping review. European Eating Disorders Review 2024, 32, 980–1001. [Google Scholar] [CrossRef]
- Davis, H.; Attia, E. Pharmacotherapy of Eating Disorders. Current Opinion in Psychiatry 2017, 30, 452–457. [Google Scholar] [CrossRef]
- Daws, R. E.; Timmermann, C.; Giribaldi, B.; Sexton, J. D.; Wall, M. B.; Erritzoe, D.; Roseman, L.; Nutt, D.; Carhart-Harris, R. Increased global integration in the brain after psilocybin therapy for depression. Nature Medicine 2022, 28, 844–851. [Google Scholar] [CrossRef]
- Dixon, L.; Price, C.; Bartel, S.; Harris, A.; Schenkels, M.; Spinella, T.; Nunes, A.; Ali, S. I.; Waller, G.; Wournell, J.; Gamberg, S.; Keshen, A. Delivering Brief Cognitive Behavioral Therapy (CBT-T) for Eating Disorders: Examining Real-World Outcomes of a Large-Scale Training Program. The International Journal of Eating Disorders 2025. [Google Scholar] [CrossRef] [PubMed]
- Doss, M. K.; Považan, M.; Rosenberg, M. D.; Sepeda, N. D.; Davis, A. K.; Finan, P. H.; Smith, G. S.; Pekar, J. J.; Barker, P. B.; Griffiths, R. R.; Barrett, F. S. Psilocybin therapy increases cognitive and neural flexibility in patients with major depressive disorder. Translational Psychiatry 2021, 11, 574. [Google Scholar] [CrossRef] [PubMed]
- Downey, A. E.; Chaphekar, A. V.; Woolley, J.; Raymond-Flesch, M. Psilocybin therapy and anorexia nervosa: A narrative review of safety considerations for researchers and clinicians. Journal of Eating Disorders 2024, 12, 49. [Google Scholar] [CrossRef]
- Erritzoe, D.; Smith, J.; Fisher, P. M.; Carhart-Harris, R.; Frokjaer, V. G.; Knudsen, G. M. Recreational use of psychedelics is associated with elevated personality trait openness: Exploration of associations with brain serotonin markers. Journal of Psychopharmacology (Oxford, England) 2019, 33, 1068–1075. [Google Scholar] [CrossRef]
- Evens, R.; Schmidt, M. E.; Majić, T.; Schmidt, T. T. The psychedelic afterglow phenomenon: A systematic review of subacute effects of classic serotonergic psychedelics. Therapeutic Advances in Psychopharmacology 2023, 13, 20451253231172254. [Google Scholar] [CrossRef] [PubMed]
- Fairburn, C. G. Cognitive Behavior Therapy and Eating Disorders; Guilford Press, 2008a. [Google Scholar]
- Fairburn, C. G. Eating disorders: The transdiagnostic view and the cognitive behavioral theory. In Cognitive behavior therapy and eating disorders; Guilford Press, 2008b; pp. 7–22. [Google Scholar]
- Fairburn, C. G.; Cooper, Z.; Doll, H. A.; O’Connor, M. E.; Bohn, K.; Hawker, D. M.; Wales, J. A.; Palmer, R. L. Transdiagnostic cognitive-behavioral therapy for patients with eating disorders: A two-site trial with 60-week follow-up. The American Journal of Psychiatry 2009, 166, 311–319. [Google Scholar] [CrossRef]
- Fang, Q.; Chan, V. K. Y.; Chan, S. S. M.; Jiao, Y.; Wang, J.; Li, X. Efficacy and safety of psilocybin on treatment-resistant depression: A systematic review and meta-analysis. Psychiatry Research 2024, 337, 115960. [Google Scholar] [CrossRef]
- Fassino, S.; Daga, G. A.; Pierò, A.; Rovera, G. G. Dropout from brief psychotherapy in anorexia nervosa. Psychotherapy and Psychosomatics 2002, 71, 200–206. [Google Scholar] [CrossRef]
- Fassino, S.; Pierò, A.; Tomba, E.; Abbate-Daga, G. Factors associated with dropout from treatment for eating disorders: A comprehensive literature review. BMC Psychiatry 2009, 9, 67. [Google Scholar] [CrossRef]
- Fauvel, B.; Strika-Bruneau, L.; Piolino, P. Changes in self-rumination and self-compassion mediate the effect of psychedelic experiences on decreases in depression, anxiety, and stress. Psychology of Consciousness: Theory, Research, and Practice 2023, 10, 88–102. [Google Scholar] [CrossRef]
- Feulner, L.; Sermchaiwong, T.; Rodland, N.; Galarneau, D. Efficacy and Safety of Psychedelics in Treating Anxiety Disorders. Ochsner Journal 2023, 23, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Fluoxetine Bulimia Nervosa Collaborative Study Group. Fluoxetine in the Treatment of Bulimia Nervosa: A Multicenter, Placebo-Controlled, Double-blind Trial. Archives of General Psychiatry 1992, 49, 139–147. [CrossRef]
- Frank, G. K. W.; Reynolds, J. R.; Shott, M. E.; O’Reilly, R. C. Altered temporal difference learning in bulimia nervosa. Biological Psychiatry 2011, 70, 728–735. [Google Scholar] [CrossRef]
- Freitas, R. R.; Gotsis, E. S.; Gallo, A. T.; Fitzgibbon, B. M.; Bailey, N. W.; Fitzgerald, P. B. The safety of psilocybin-assisted psychotherapy: A systematic review. The Australian and New Zealand Journal of Psychiatry 2025, 59, 128–151. [Google Scholar] [CrossRef] [PubMed]
- Gattuso, J. J.; Perkins, D.; Ruffell, S.; Lawrence, A. J.; Hoyer, D.; Jacobson, L. H.; Timmermann, C.; Castle, D.; Rossell, S. L.; Downey, L. A.; Pagni, B. A.; Galvão-Coelho, N. L.; Nutt, D.; Sarris, J. Default Mode Network Modulation by Psychedelics: A Systematic Review. The International Journal of Neuropsychopharmacology 2023, 26, 155–188. [Google Scholar] [CrossRef]
- Godart, N. T.; Flament, M. F.; Curt, F.; Perdereau, F.; Lang, F.; Venisse, J. L.; Halfon, O.; Bizouard, P.; Loas, G.; Corcos, M.; Jeammet, P.; Fermanian, J. Anxiety disorders in subjects seeking treatment for eating disorders: A DSM-IV controlled study. Psychiatry Research 2003, 117, 245–258. [Google Scholar] [CrossRef]
- Goodwin, G. M.; Malievskaia, E.; Fonzo, G. A.; Nemeroff, C. B. Must Psilocybin Always “Assist Psychotherapy”? American Journal of Psychiatry 2024, 181, 20–25. [Google Scholar] [CrossRef]
- Gorrell, S.; Hail, L.; Reilly, E. E. Predictors of Treatment Outcome in Eating Disorders: A Roadmap to Inform Future Research Efforts. Current Psychiatry Reports 2023, 25, 213–222. [Google Scholar] [CrossRef]
- Graves, T. A.; Tabri, N.; Thompson-Brenner, H.; Franko, D. L.; Eddy, K. T.; Bourion-Bedes, S.; Brown, A.; Constantino, M. J.; Flückiger, C.; Forsberg, S.; Isserlin, L.; Couturier, J.; Paulson Karlsson, G.; Mander, J.; Teufel, M.; Mitchell, J. E.; Crosby, R. D.; Prestano, C.; Satir, D. A.; Thomas, J. J. A meta-analysis of the relation between therapeutic alliance and treatment outcome in eating disorders. The International Journal of Eating Disorders 2017, 50, 323–340. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C. M. Why no cognitive body image feature such as overvaluation of shape/weight in the binge eating disorder diagnosis? The International Journal of Eating Disorders 2013, 46, 208–211. [Google Scholar] [CrossRef]
- Grilo, C. M.; Crosby, R. D.; Masheb, R. M.; White, M. A.; Peterson, C. B.; Wonderlich, S. A.; Engel, S. G.; Crow, S. J.; Mitchell, J. E. Overvaluation of shape and weight in binge eating disorder, bulimia nervosa, and sub-threshold bulimia nervosa. Behaviour Research and Therapy 2009, 47, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Grilo, C. M.; Ivezaj, V.; Tek, C.; Yurkow, S.; Wiedemann, A. A.; Gueorguieva, R. Cognitive Behavioral Therapy and Lisdexamfetamine, Alone and Combined, for Binge-Eating Disorder With Obesity: A Randomized Controlled Trial. The American Journal of Psychiatry 2024. [Google Scholar] [CrossRef]
- Gukasyan, N.; Schreyer, C. C.; Griffiths, R. R.; Guarda, A. S. Psychedelic-Assisted Therapy for People with Eating Disorders. Current Psychiatry Reports 2022, 24, 767–775. [Google Scholar] [CrossRef]
- Haikazian, S.; Chen-Li, D. C. J.; Johnson, D. E.; Fancy, F.; Levinta, A.; Husain, M. I.; Mansur, R. B.; McIntyre, R. S.; Rosenblat, J. D. Psilocybin-assisted therapy for depression: A systematic review and meta-analysis. Psychiatry Research 2023, 329, 115531. [Google Scholar] [CrossRef]
- Halmi, K. A. Perplexities of treatment resistance in eating disorders. BMC Psychiatry 2013, 13, 292. [Google Scholar] [CrossRef]
- Harrington, B. C.; Jimerson, M.; Haxton, C.; Jimerson, D. C. Initial Evaluation, Diagnosis, and Treatment of Anorexia Nervosa and Bulimia Nervosa. American Family Physician 2015, 91, 46–52. [Google Scholar]
- Heal-Cohen, N.; Allan, S. M.; Gauvain, N.; Nabirinde, R.; Burgess, A. Relapse in Eating Disorders: A Systematic Review and Thematic Synthesis of Individuals’ Experiences. Clinical Psychology & Psychotherapy 2025, 32, e70101. [Google Scholar] [CrossRef] [PubMed]
- Hinkle, J. T.; Graziosi, M.; Nayak, S. M.; Yaden, D. B. Adverse Events in Studies of Classic Psychedelics: A Systematic Review and Meta-Analysis. JAMA Psychiatry 2024, 81, 1225–1235. [Google Scholar] [CrossRef]
- Ho, J. T.; Preller, K. H.; Lenggenhager, B. Neuropharmacological modulation of the aberrant bodily self through psychedelics. Neuroscience and Biobehavioral Reviews 2020, 108, 526–541. [Google Scholar] [CrossRef] [PubMed]
- Holze, F.; Avedisian, I.; Varghese, N.; Eckert, A.; Liechti, M. E. Role of the 5-HT2A Receptor in Acute Effects of LSD on Empathy and Circulating Oxytocin. Frontiers in Pharmacology 2021, 12, 711255. [Google Scholar] [CrossRef] [PubMed]
- Holze, F.; Vizeli, P.; Ley, L.; Müller, F.; Dolder, P.; Stocker, M.; Duthaler, U.; Varghese, N.; Eckert, A.; Borgwardt, S.; Liechti, M. E. Acute dose-dependent effects of lysergic acid diethylamide in a double-blind placebo-controlled study in healthy subjects. Neuropsychopharmacology 2021, 46, 537–544. [Google Scholar] [CrossRef]
- Hultgren, J.; Hafsteinsson, M. H.; Brulin, J. G. A dose of therapy with psilocybin—A meta-analysis of the relationship between the amount of therapy hours and treatment outcomes in psychedelic-assisted therapy. General Hospital Psychiatry 2025, 96, 234–243. [Google Scholar] [CrossRef]
- Irizarry, R.; Winczura, A.; Dimassi, O.; Dhillon, N.; Minhas, A.; Larice, J. Psilocybin as a Treatment for Psychiatric Illness: A Meta-Analysis. Cureus 2022, 14, e31796. [Google Scholar] [CrossRef]
- Johnson, M. W.; Garcia-Romeu, A.; Griffiths, R. R. Long-term follow-up of psilocybin-facilitated smoking cessation. The American Journal of Drug and Alcohol Abuse 2017, 43, 55–60. [Google Scholar] [CrossRef]
- Jones, J. L. Harnessing neuroplasticity with psychoplastogens: The essential role of psychotherapy in psychedelic treatment optimization. Frontiers in Psychiatry 2025, 16. [Google Scholar] [CrossRef]
- Kaye, W. H.; Bulik, C. M.; Thornton, L.; Barbarich, N.; Masters, K. Comorbidity of anxiety disorders with anorexia and bulimia nervosa. The American Journal of Psychiatry 2004, 161, 2215–2221. [Google Scholar] [CrossRef]
- Keegan, E.; Waller, G.; Wade, T. D. A systematic review and meta-analysis of a 10-session cognitive behavioural therapy for non-underweight eating disorders. Clinical Psychologist 2022, 26, 241–254. [Google Scholar] [CrossRef]
- Keeler, J. L.; Bahnsen, K.; Wronski, M. L.; Bernardoni, F.; Tam, F.; Arold, D.; King, J. A.; Kolb, T.; Poitz, D. M.; Roessner, V.; Treasure, J.; Himmerich, H.; Ehrlich, S. Longitudinal changes in brain-derived neurotrophic factor (BDNF) but not cytokines contribute to hippocampal recovery in anorexia nervosa above increases in body mass index. In Psychol Med; Publisher, 2024; pp. 1–12. [Google Scholar] [CrossRef]
- Keeler, J. L.; Kan, C.; Treasure, J.; Himmerich, H. Novel treatments for anorexia nervosa: Insights from neuroplasticity research. Eur Eat Disord Rev 2023. [Google Scholar] [CrossRef] [PubMed]
- Keeler, J. L.; Robinson, L.; Keeler-Schaffeler, R.; Dalton, B.; Treasure, J.; Himmerich, H. Growth factors in anorexia nervosa: A systematic review and meta-analysis of cross-sectional and longitudinal data. In World J Biol Psychiatry; Medline, 2022; Volume 23, pp. 582–600. [Google Scholar] [CrossRef]
- Keller, M. B.; Herzog, D. B.; Lavori, P. W.; Bradburn, I. S.; Mahoney, E. S. The naturalistic history of bulimia nervosa: Extraordinarily high rates of chronicity, relapse, recurrence, and psychosocial morbidity. International Journal of Eating Disorders 1992, 12, 1–9. [Google Scholar] [CrossRef]
- Kelly, J. R.; Gillan, C. M.; Prenderville, J.; Kelly, C.; Harkin, A.; Clarke, G.; O’Keane, V. Psychedelic Therapy’s Transdiagnostic Effects: A Research Domain Criteria (RDoC) Perspective. Frontiers in Psychiatry 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Koning, E.; Brietzke, E. Psilocybin-Assisted Psychotherapy as a Potential Treatment for Eating Disorders: A Narrative Review of Preliminary Evidence. Trends in Psychiatry and Psychotherapy 2023. [Google Scholar] [CrossRef]
- Koning, E.; Chaves, C.; Kirkpatrick, R. H.; Brietzke, E. Exploring the neurobiological correlates of psilocybin-assisted psychotherapy in eating disorders: A review of potential methodologies and implications for the psychedelic study design. Journal of Eating Disorders 2024, 12, 214. [Google Scholar] [CrossRef]
- Koning, E.; McMillan, R. M.; Keshen, A.; Hay, P.; Fernandez, A. V.; Reynolds, J.; Touyz, S. Why psychedelic-assisted therapy studies in eating disorders risk missing the mark on outcomes: A phenomenological psychopathology perspective. Journal of Eating Disorders 2025, 13, 1–7. [Google Scholar] [CrossRef]
- Lacroix, E.; Fatur, K.; Hay, P.; Touyz, S.; Keshen, A. Psychedelics and the treatment of eating disorders: Considerations for future research and practice. Journal of Eating Disorders 2024, 12, 165. [Google Scholar] [CrossRef]
- Levin, A. W.; Lancelotta, R.; Sepeda, N. D.; Gukasyan, N.; Nayak, S.; Wagener, T. L.; Barrett, F. S.; Griffiths, R. R.; Davis, A. K. The therapeutic alliance between study participants and intervention facilitators is associated with acute effects and clinical outcomes in a psilocybin-assisted therapy trial for major depressive disorder. PloS One 2024, 19, e0300501. [Google Scholar] [CrossRef] [PubMed]
- Levinson, C. A.; Zerwas, S.; Calebs, B.; Forbush, K.; Kordy, H.; Watson, H.; Hofmeier, S.; Levine, M.; Crosby, R. D.; Peat, C.; Runfola, C. D.; Zimmer, B.; Moesner, M.; Marcus, M. D.; Bulik, C. M. The Core Symptoms of Bulimia Nervosa, Anxiety, and Depression: A Network Analysis. Journal of Abnormal Psychology 2017, 126, 340–354. [Google Scholar] [CrossRef] [PubMed]
- Lie, S. Ø.; Rø, Ø.; Bang, L. Is bullying and teasing associated with eating disorders? A systematic review and meta-analysis. The International Journal of Eating Disorders 2019, 52, 497–514. [Google Scholar] [CrossRef]
- Linardon, J. Meta-analysis of the effects of cognitive-behavioral therapy on the core eating disorder maintaining mechanisms: Implications for mechanisms of therapeutic change. Cognitive Behaviour Therapy 2018, 47, 107–125. [Google Scholar] [CrossRef]
- Linardon, J.; Hindle, A.; Brennan, L. Dropout from cognitive-behavioral therapy for eating disorders: A meta-analysis of randomized, controlled trials. The International Journal of Eating Disorders 2018, 51, 381–391. [Google Scholar] [CrossRef] [PubMed]
- Lydecker, J. A.; White, M. A.; Grilo, C. M. Form and Formulation: Examining the Distinctiveness of Body Image Constructs in Treatment- Seeking Patients with Binge-Eating Disorder. Journal of Consulting and Clinical Psychology 2017, 85, 1095–1103. [Google Scholar] [CrossRef]
- MacDonald, D. E.; Trottier, K. Rapid improvements in emotion regulation predict eating disorder psychopathology and functional impairment at 6-month follow-up in individuals with bulimia nervosa and purging disorder. The International Journal of Eating Disorders 2019, 52, 962–967. [Google Scholar] [CrossRef]
- MacLean, K. A.; Johnson, M. W.; Griffiths, R. R. Mystical Experiences Occasioned by the Hallucinogen Psilocybin Lead to Increases in the Personality Domain of Openness. Journal of Psychopharmacology (Oxford, England) 2011, 25, 1453–1461. [Google Scholar] [CrossRef]
- Madsen, M. K.; Fisher, P. M.; Burmester, D.; Dyssegaard, A.; Stenbæk, D. S.; Kristiansen, S.; Johansen, S. S.; Lehel, S.; Linnet, K.; Svarer, C.; Erritzoe, D.; Ozenne, B.; Knudsen, G. M. Psychedelic effects of psilocybin correlate with serotonin 2A receptor occupancy and plasma psilocin levels. Neuropsychopharmacology: Official Publication of the American College of Neuropsychopharmacology 2019, 44, 1328–1334. [Google Scholar] [CrossRef]
- Majić, T.; Schmidt, T. T.; Gallinat, J. Peak experiences and the afterglow phenomenon: When and how do therapeutic effects of hallucinogens depend on psychedelic experiences? Journal of Psychopharmacology 2015, 29, 241–253. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.; Simão, M.; Guiomar, R.; Castilho, P. Self-disgust and urge to be thin in eating disorders: How can self-compassion help? Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity 2021, 26, 2317–2324. [Google Scholar] [CrossRef]
- Mertens, L. J.; Wall, M. B.; Roseman, L.; Demetriou, L.; Nutt, D. J.; Carhart-Harris, R. L. Therapeutic mechanisms of psilocybin: Changes in amygdala and prefrontal functional connectivity during emotional processing after psilocybin for treatment-resistant depression. Journal of Psychopharmacology 2020, 34, 167–180. [Google Scholar] [CrossRef]
- Monson, C. M.; Wagner, A. C.; Mithoefer, A. T.; Liebman, R. E.; Feduccia, A. A.; Jerome, L.; Yazar-Klosinski, B.; Emerson, A.; Doblin, R.; Mithoefer, M. C. MDMA-facilitated cognitive-behavioural conjoint therapy for posttraumatic stress disorder: An uncontrolled trial. European Journal of Psychotraumatology n.d., 11, 1840123. [Google Scholar] [CrossRef]
- Monteleone, P.; Brambilla, F.; Bortolotti, F.; Maj, M. Serotonergic dysfunction across the eating disorders: Relationship to eating behaviour, purging behaviour, nutritional status and general psychopathology. Psychological Medicine 2000, 30, 1099–1110. [Google Scholar] [CrossRef]
- Murphy, R.; Straebler, S.; Cooper, Z.; Fairburn, C. G. Cognitive behavioral therapy for eating disorders. The Psychiatric Clinics of North America 2010, 33, 611–627. [Google Scholar] [CrossRef]
- Nechita, D.-M.; Bud, S.; David, D. Shame and eating disorders symptoms: A meta-analysis. The International Journal of Eating Disorders 2021, 54, 1899–1945. [Google Scholar] [CrossRef]
- Nichols, D. E. Psychedelics. Pharmacological Reviews 2016, 68, 264–355. [Google Scholar] [CrossRef] [PubMed]
- Olson, D. E. Psychoplastogens: A Promising Class of Plasticity-Promoting Neurotherapeutics. Journal of Experimental Neuroscience 2018, 12. [Google Scholar] [CrossRef] [PubMed]
- Öst, L.-G.; Brattmyr, M.; Finnes, A.; Ghaderi, A.; Havnen, A.; Hedman-Lagerlöf, M.; Parling, T.; Welch, E.; Wergeland, G. J. Cognitive behavior therapy for adult eating disorders in routine clinical care: A systematic review and meta-analysis. The International Journal of Eating Disorders 2024, 57, 249–264. [Google Scholar] [CrossRef]
- Otterman, L. S. Research into Psychedelic-Assisted Psychotherapy for Anorexia Nervosa Should be Funded. Journal of Bioethical Inquiry 2023, 20, 31–39. [Google Scholar] [CrossRef]
- Paphiti, A.; Newman, E. 10-session Cognitive Behavioural Therapy (CBT-T) for Eating Disorders: A Systematic Review and Narrative Synthesis. International Journal of Cognitive Therapy 2023, 16, 646–681. [Google Scholar] [CrossRef]
- Peck, S. K.; Brewerton, T. D.; Fisher, H.; Trim, J.; Shao, S.; Modlin, N. L.; Kim, J.; Finn, D. M.; Kaye, W. H. Therapeutic emergence of dissociated traumatic memories during psilocybin treatment for anorexia nervosa. Journal of Eating Disorders 2025, 13, 1–10. [Google Scholar] [CrossRef]
- Peck, S. K.; Shao, S.; Gruen, T.; Yang, K.; Babakanian, A.; Trim, J.; Finn, D. M.; Kaye, W. H. Psilocybin therapy for females with anorexia nervosa: A phase 1, open-label feasibility study. Nature Medicine 2023, 29, 1947–1953. [Google Scholar] [CrossRef] [PubMed]
- Phillips, K.; Keane, K.; Wolfe, B. E. Peripheral Brain Derived Neurotrophic Factor (BDNF) in Bulimia Nervosa: A Systematic Review. Archives of Psychiatric Nursing 2014, 28, 108–113. [Google Scholar] [CrossRef]
- Pinna, F.; Sanna, L.; Carpiniello, B. Alexithymia in eating disorders: Therapeutic implications. Psychology Research and Behavior Management 2014, 8, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Wu, Y.; Liu, F.; Zhu, Y.; Jin, H.; Zhang, H.; Wan, Y.; Li, C.; Yu, D. An update on the prevalence of eating disorders in the general population: A systematic review and meta-analysis. Eating and Weight Disorders 2022, 27, 415–428. [Google Scholar] [CrossRef] [PubMed]
- Raykos, B. C.; McEvoy, P. M.; Fursland, A. Socializing problems and low self-esteem enhance interpersonal models of eating disorders: Evidence from a clinical sample. The International Journal of Eating Disorders 2017, 50, 1075–1083. [Google Scholar] [CrossRef]
- Rodan, S.-C.; Bryant, E.; Le, A.; Maloney, D.; Touyz, S.; McGregor, I. S.; Maguire, S. Pharmacotherapy, alternative and adjunctive therapies for eating disorders: Findings from a rapid review. Journal of Eating Disorders 2023, 11, 1–23. [Google Scholar] [CrossRef]
- Rodan, S.-C.; Maguire, S.; Meez, N.; Greenstien, K.; Zartarian, G.; Mills, K. L.; Suraev, A.; Bedoya-Pérez, M. A.; McGregor, I. S. Prescription and Nonprescription Drug Use Among People With Eating Disorders. JAMA Network Open 2025, 8, e2522406. [Google Scholar] [CrossRef]
- Roseman, L.; Nutt, D. J.; Carhart-Harris, R. L. Quality of Acute Psychedelic Experience Predicts Therapeutic Efficacy of Psilocybin for Treatment-Resistant Depression. Frontiers in Pharmacology 2017, 8, 974. [Google Scholar] [CrossRef] [PubMed]
- Rosenblat, J. D.; Husain, M. I.; Lee, Y.; McIntyre, R. S.; Mansur, R. B.; Castle, D.; Offman, H.; Parikh, S. V.; Frey, B. N.; Schaffer, A.; Greenway, K. T.; Garel, N.; Beaulieu, S.; Kennedy, S. H.; Lam, R. W.; Milev, R.; Ravindran, A. V.; Tourjman, V.; Ameringen, M. V.; Taylor, V. The Canadian Network for Mood and Anxiety Treatments (CANMAT) Task Force Report: Serotonergic Psychedelic Treatments for Major Depressive Disorder. Canadian Journal of Psychiatry. Revue Canadienne De Psychiatrie 2023, 68, 5–21. [Google Scholar] [CrossRef]
- Russell, H.; Aouad, P.; Le, A.; Marks, P.; Maloney, D.; Touyz, S.; Maguire, S. Psychotherapies for eating disorders: Findings from a rapid review. Journal of Eating Disorders 2023, 11, 175. [Google Scholar] [CrossRef] [PubMed]
- Rutschmann, R.; Romanczuk-Seiferth, N.; Gloster, A.; Richter, C. Increasing psychological flexibility is associated with positive therapy outcomes following a transdiagnostic ACT treatment. Frontiers in Psychiatry 2024, 15, 1403718. [Google Scholar] [CrossRef]
- Sampedro, F.; de la Fuente Revenga, M.; Valle, M.; Roberto, N.; Domínguez-Clavé, E.; Elices, M.; Luna, L. E.; Crippa, J. A. S.; Hallak, J. E. C.; de Araujo, D. B.; Friedlander, P.; Barker, S. A.; Álvarez, E.; Soler, J.; Pascual, J. C.; Feilding, A.; Riba, J. Assessing the Psychedelic “After-Glow” in Ayahuasca Users: Post-Acute Neurometabolic and Functional Connectivity Changes Are Associated with Enhanced Mindfulness Capacities. International Journal of Neuropsychopharmacology 2017, 20, 698–711. [Google Scholar] [CrossRef]
- Schnicker, K.; Hiller, W.; Legenbauer, T. Drop-out and treatment outcome of outpatient cognitive-behavioral therapy for anorexia nervosa and bulimia nervosa. Comprehensive Psychiatry 2013, 54, 812–823. [Google Scholar] [CrossRef]
- Scott, N.; Hanstock, T. L.; Thornton, C. Dysfunctional self-talk associated with eating disorder severity and symptomatology. Journal of Eating Disorders 2014, 2, 14. [Google Scholar] [CrossRef] [PubMed]
- Shobeiri, P.; Bagherieh, S.; Mirzayi, P.; Kalantari, A.; Mirmosayyeb, O.; Teixeira, A. L.; Rezaei, N. Serum and plasma levels of brain-derived neurotrophic factor in individuals with eating disorders (EDs): A systematic review and meta-analysis. In J Eat Disord; PubMed-not-MEDLINE, 2022; Volume 10, p. 105. [Google Scholar] [CrossRef]
- Siegel, J. S.; Subramanian, S.; Perry, D.; Kay, B. P.; Gordon, E. M.; Laumann, T. O.; Reneau, T. R.; Metcalf, N. V.; Chacko, R. V.; Gratton, C.; Horan, C.; Krimmel, S. R.; Shimony, J. S.; Schweiger, J. A.; Wong, D. F.; Bender, D. A.; Scheidter, K. M.; Whiting, F. I.; Padawer-Curry, J. A.; Dosenbach, N. U. F. Psilocybin desynchronizes the human brain. Nature 2024, 1–8. [Google Scholar] [CrossRef]
- Sloshower, J.; Skosnik, P. D.; Safi-Aghdam, H.; Pathania, S.; Syed, S.; Pittman, B.; D’Souza, D. C. Psilocybin-assisted therapy for major depressive disorder: An exploratory placebo-controlled, fixed-order trial. Journal of Psychopharmacology (Oxford, England) 2023, 37, 698–706. [Google Scholar] [CrossRef]
- Smink, F. R. E.; van Hoeken, D.; Hoek, H. W. Epidemiology of eating disorders: Incidence, prevalence and mortality rates. Current Psychiatry Reports 2012, 14, 406–414. [Google Scholar] [CrossRef]
- Sønderland, N. M.; Solbakken, O. A.; Eilertsen, D. E.; Nordmo, M.; Monsen, J. T. Emotional changes and outcomes in psychotherapy: A systematic review and meta-analysis. Journal of Consulting and Clinical Psychology 2024, 92, 654–670. [Google Scholar] [CrossRef]
- Steel, Z.; Jones, J.; Adcock, S.; Clancy, R.; Bridgford-West, L.; Austin, J. Why the high rate of dropout from individualized cognitive-behavior therapy for bulimia nervosa? The International Journal of Eating Disorders 2000, 28, 209–214. [Google Scholar] [CrossRef]
- Steiger, H. Eating disorders and the serotonin connection: State, trait and developmental effects. Journal of Psychiatry and Neuroscience 2004, 29, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Stenbæk, D. S.; Madsen, M. K.; Ozenne, B.; Kristiansen, S.; Burmester, D.; Erritzoe, D.; Knudsen, G. M.; Fisher, P. M. Brain serotonin 2A receptor binding predicts subjective temporal and mystical effects of psilocybin in healthy humans. Journal of Psychopharmacology (Oxford, England) 2021, 35, 459–468. [Google Scholar] [CrossRef]
- Steward, T. Endocrinology-informed neuroimaging in eating disorders: GLP1, orexins, and psilocybin. Trends in Molecular Medicine 2024, 30, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Swinbourne, J.; Hunt, C.; Abbott, M.; Russell, J.; St Clare, T.; Touyz, S. The comorbidity between eating disorders and anxiety disorders: Prevalence in an eating disorder sample and anxiety disorder sample. The Australian and New Zealand Journal of Psychiatry 2012, 46, 118–131. [Google Scholar] [CrossRef]
- Thompson, W. H.; Skau, S. On the scope of scientific hypotheses. Royal Society Open Science 2023, 10, 230607. [Google Scholar] [CrossRef] [PubMed]
- Vall, E.; Wade, T. D. Predictors of treatment outcome in individuals with eating disorders: A systematic review and meta-analysis. International Journal of Eating Disorders 2015, 48, 946–971. [Google Scholar] [CrossRef]
- van Eeden, A. E.; van Hoeken, D.; Hoek, H. W. Incidence, prevalence and mortality of anorexia nervosa and bulimia nervosa. Current Opinion in Psychiatry 2021, 34, 515–524. [Google Scholar] [CrossRef]
- van Elk, M.; Fried, E. I. History repeating: Guidelines to address common problems in psychedelic science. Therapeutic Advances in Psychopharmacology 2023, 13, 20451253231198466. [Google Scholar] [CrossRef]
- van Hoeken, D.; Hoek, H. W. Review of the burden of eating disorders: Mortality, disability, costs, quality of life, and family burden. Current Opinion in Psychiatry 2020, 33, 521. [Google Scholar] [CrossRef]
- Velkoff, E. A.; Rubino, L. G.; Liu, J.; Manasse, S. M.; Juarascio, A. S. Early reduction in anxiety sensitivity predicts greater reduction in disordered eating and trait anxiety during treatment for bulimia nervosa. The International Journal of Eating Disorders 2024, 57, 1791–1796. [Google Scholar] [CrossRef] [PubMed]
- Wagner, G.; Penelo, E.; Nobis, G.; Mayrhofer, A.; Wanner, C.; Schau, J.; Spitzer, M.; Gwinner, P.; Trofaier, M.-L.; Imgart, H.; Fernandez-Aranda, F.; Karwautz, A. Predictors for good therapeutic outcome and drop-out in technology assisted guided self-help in the treatment of bulimia nervosa and bulimia like phenotype. European Eating Disorders Review: The Journal of the Eating Disorders Association 2015, 23, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Waller, G.; Beard, J. Recent Advances in Cognitive-Behavioural Therapy for Eating Disorders (CBT-ED). Current Psychiatry Reports 2024, 26, 351–358. [Google Scholar] [CrossRef]
- Walsh, B. T.; Wilson, G. T.; Loeb, K. L.; Devlin, M. J.; Pike, K. M.; Roose, S. P.; Fleiss, J.; Waternaux, C. Medication and psychotherapy in the treatment of bulimia nervosa. The American Journal of Psychiatry 1997, 154, 523–531. [Google Scholar] [CrossRef]
- Watts, R.; Day, C.; Krzanowski, J.; Nutt, D.; Carhart-Harris, R. Patients’ Accounts of Increased “Connectedness” and “Acceptance” After Psilocybin for Treatment-Resistant Depression. Journal of Humanistic Psychology 2017, 57, 520–564. [Google Scholar] [CrossRef]
- Wiepking, L.; de Bruin, E.; Ghiţă, A. The potential of psilocybin use to enhance well-being in healthy individuals – A scoping review 2023. [CrossRef]
- Wolff, M.; Gukasyan, N.; Roseman, L.; Liknaitzky, P. Reframing psychedelic regulation: Tools, not treatments. Drug Science, Policy and Law 2025, 11, 20503245251348272. [Google Scholar] [CrossRef]
- Wulff, A. B.; Nichols, C. D.; Thompson, S. M. Preclinical perspectives on the mechanisms underlying the therapeutic actions of psilocybin in psychiatric disorders. Neuropharmacology 2023, 231, 109504. [Google Scholar] [CrossRef] [PubMed]
- Xi, D.; Berger, A.; Shurtleff, D.; Zia, F. Z.; Belouin, S. National Institutes of Health psilocybin research speaker series: State of the science, regulatory and policy landscape, research gaps, and opportunities. Neuropharmacology 2023, 230, 109467. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Du, Y.; Yao, Y.; Dai, W.; Yin, Y.; Wang, G.; Li, Y.; Zhang, L. Psilocybin promotes neuroplasticity and induces rapid and sustained antidepressant-like effects in mice. Journal of Psychopharmacology 2024, 02698811241249436. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zhang, C.; Hellerstein, D.; Feusner, J. D.; Wheaton, M. G.; Gomez, G. J.; Schneier, F. Single-dose psilocybin alters resting state functional networks in patients with body dysmorphic disorder. Psychedelics 2025, 1, 25–31. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Overview of the timeline for psilocybin treatment as an adjunct to cognitive-behavioral therapy for eating disorders.
Figure 1.
Overview of the timeline for psilocybin treatment as an adjunct to cognitive-behavioral therapy for eating disorders.
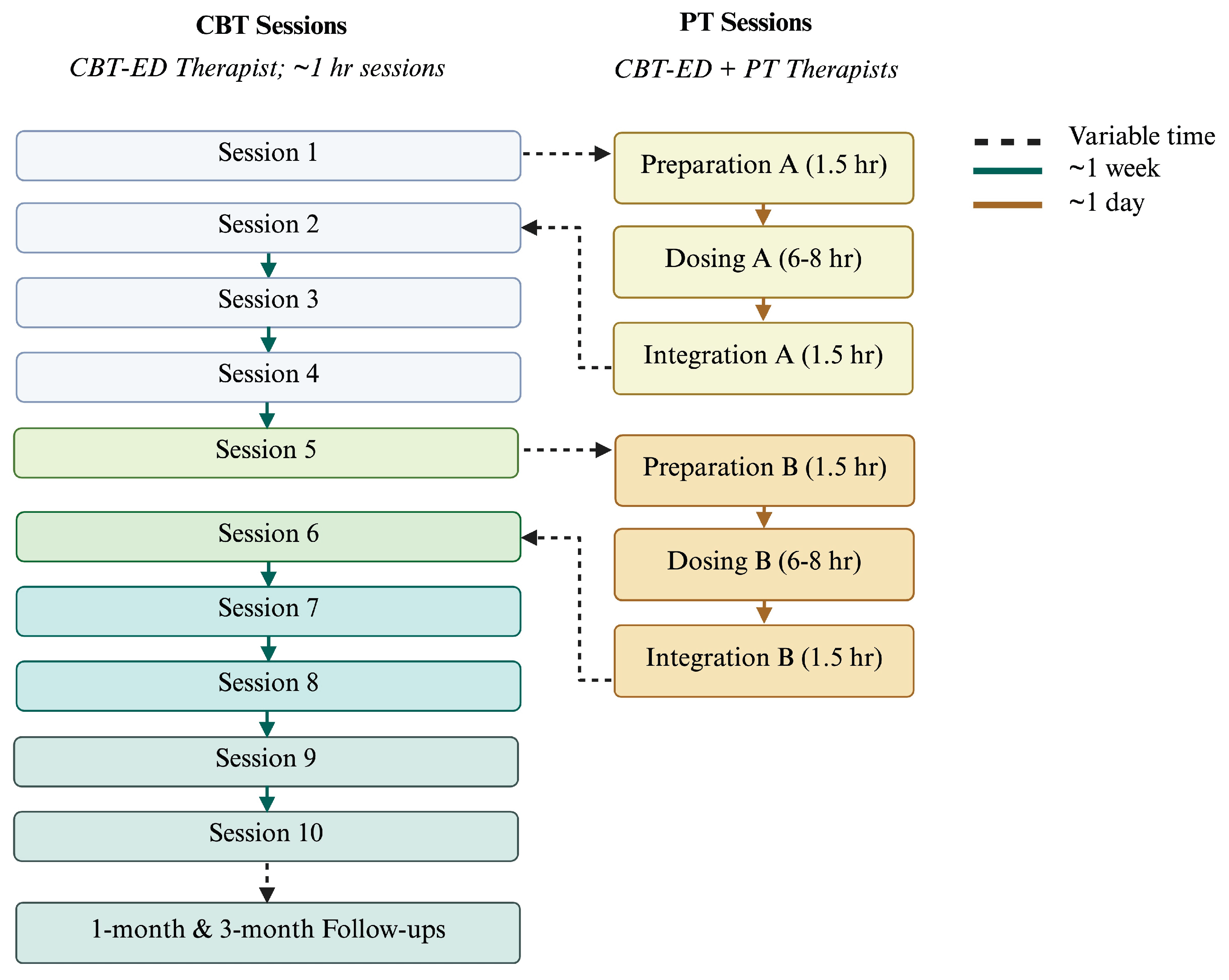

Table 1.
A summary of the hypothesized mechanisms in which psilocybin treatment may augment cognitive-behavioral therapy for eating disorders.
Table 1.
A summary of the hypothesized mechanisms in which psilocybin treatment may augment cognitive-behavioral therapy for eating disorders.
| Mechanism | ED Psychopathology and CBT-ED Barriers | Psilocybin Treatment | ||
| Neurobiological | ||||
| Serotonergic neurotransmission |
Dysregulated serotonin signaling; clinical response from serotonergic medications | ↑ serotonin signaling | ||
| Neuroplasticity | ↓ markers of neuroplasticity | ↑ markers of neuroplasticity | ||
| Neural network connectivity | Maladaptive neural network connectivity; ↓ cognitive flexibility | Disrupted functional connectivity; ↑ cognitive flexibility | ||
| Psychological | ||||
| Body image | ↑ body image overvaluation | ↓ body image overvaluation | ||
| Mood | ↑ depressive and anxiety symptoms | ↓ depressive and anxiety symptoms | ||
| Social function | Social dysfunction; challenges to therapeutic alliance | Prosocial effects; strengthened therapeutic alliance | ||
| General well-being | Experiential avoidance, shame, self-criticism, low self-esteem | Self-acceptance/compassion, sense of connectedness and insight | ||
Table 2.
Session-by-session CBT-T program with considerations for psilocybin treatment integration.
| Phase | Session | Key Activities & Topics | PT Considerations / Facilitator Guidance |
|---|---|---|---|
| Phase 1: Early engagement & eating structure | 1 |
|
|
| 2 |
|
||
| 3 |
|
||
| 4 |
|
||
| Phase 2: Behavioural Experiments | 5 |
|
|
|
Phase 3: Emotional Triggers (Behavioural Experiments if needed) |
6 |
|
|
|
Phase 4: Body Image (Behavioural Experiments and/or Emotional Triggers if needed) |
7 |
|
|
| 8 |
|
||
|
Phase 5: Relapse Prevention (Body image if needed) |
9 |
|
|
| 10 |
|
||
| Follow-up Phase | 11 12 |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



