
Submitted:
18 December 2025
Posted:
18 December 2025
You are already at the latest version
Abstract
Background: Auricular carcinomas often require extensive surgical resection, resulting in complex three-dimensional defects,in some cases involving mastoid process exposure. Reconstruction aims to restore contour, protect underlying structures, and maintain patency of the external auditory canal (EAC). Case presentation and methods: We present a 45-year-old male patient, without comorbidities, who underwent subtotal auricular resection and wide retroauricular excision for basal cell carcinoma, resulting in mastoid bone exposure. Reconstruction was achieved using a temporal muscle flap covered by a skin graft, combined with a Z-plasty of the external auditory meatus to prevent postoperative stenosis. Recovery was uneventful, and 4 year follow-up demonstrated stable structural outcomes, preserved diameter of the meatus, without recurrence of the disease.The patient is prepared for autologous or prosthetic auricular reconstruction. Conclusion: A temporalis muscle flap with skin graft coverage offers a reliable, vascularized solution for large post-oncologic auricular defects while preserving the external auditory canal. Z-plasty remains a critical technique for preventing meatal stenosis.
Keywords:
reconstructive surgery of the ear
; temporalis muscle flap
; external ear carcinoma
; auricular reconstruction
1. Introduction
Cutaneous malignancies involving the auricle, such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), are common due to chronic sun exposure, sun burns, repeated trauma, immunosuppression and HPV infection. Skin neoplasms of the external ear often pose challenges because of the 3-dimensional anatomy and topographic peculiarities of the auricle. Auricular skin cancers are more common in man and the helix is one of the most frequently affected sub-unit. Moreover, auricle malignancies are classified in the high-risk group of the head and neck region, which necessitates a radical surgical approach [1,2,3]. Achieving oncologically safe margins often requires subtotal or total auricular resection, creating complex composite defects.
Advanced auricular carcinomas,involving the EAC and mastoid region can even require in some cases extensive resection in the retroauricular region. This surgical intervention often leaves severe exposure of the mastoid process, dead space around the EAC and in cases, in which chemo- or radiotherapy is included, the tissues remain poorly vascularized with higher risk for complications, such as infections, bone sequestration and delayed healing. The research background poses the question why exposure of the mastoid bone and its management matter in the overall treatment protocol. Recent literature data emphasizes on the covering of such defects with well-vascularized flaps to promote uneventful, faster healing and reduce the risk for infection and necrosis [4].
Reconstruction of such defects must provide stable coverage of exposed bone and cartilage, restore auricular contour and ensure preservation of EAC to prevent stenosis.
We describe a 45-year-old male patient who presented with a basal cell carcinoma, affecting the lobulus of the ear and the retroauricular and mastoid region. He underwent successful tumor resection with clear resection margins in an ENT department with a subsequent referral to our department for reconstruction. This report presents a successful reconstruction of a large post-excisional defect, 10x10 cm in diameter, with mastoid process exposure. Temporal muscle flip flap and skin graft, along with the preservation of the external auditory canal with Z-plasty, were incorporated for reconstruction after subtotal auricular amputation due to BCC. It highlights the importance of a diligent long-term follow-up, preservation of the canal, preventing meatal stenosis and the reconstructive potential of the muscle flap in patients with mastoid bone exposure in a single-stage.
A variety of techniques have been described, including local chondrocutaneous flaps, temporoparietal fascia flaps, temporalis muscle flap, free tissue transfer, and prosthetic reconstruction [1,2,3,4].
The temporalis muscle flap is regional, pedicled, option that can be rotated or flipped into the mastoid process and provide abundant vascularization and coverage, obliterate dead space and mitigate complications, such as infection, bone sequestrum and necrosis. A 2025 craniofacial review summarizes the temporal muscle flap’s advantages, such as dual vascular supply, volume thickness with low donor site morbidity [5].
One latest literature example described similar post-surgical defect, 8x7cm in diameter, involving the EAC and bone, utilizing the temporal muscle flap and skin graft to close the defect. In this case, silicone splint was used to preserve meatal patency [4].
However, to the best of our knowledge, there is insufficient data and reports describing the single-stage reconstructive combination of temporal muscle flip flap, skin graft and Z-plasty of the meatus, without silicone splint, to manage a very large defect. Moreover, hearing outcome and meatal patency results remain underreported in literature.
Unequivocally, the flap is a solid vascularized bed and foundation for skin grafts and future autologous or prosthetic ear choices. Furthermore, the preservation of the EAC and hearing diversifies the subsequent pinna reconstruction methods.
2. Case Presentation
A 45-year-old man, without any comorbidities, presented with a history of a progressively enlarging ulcerated lesion of the left auricle and mastoid area. (Figure 1A)
Biopsy confirmed BCC. Preoperative CT scan showed no spread to other organs. The staging of the disease is T3 N0 M0. Following multidisciplinary oncologic board discussion, the patient was referred for surgical management in the ENT department. A subtotal auricular resection was performed, along with partial (5 mm) excision of the EAC, and wide retroauricular resection, exposing the mastoid process, leaving a large defect, 10x10cm in diameter, as shown in Figure 1B.
After histopathological verification of clear resection margins, the patient was referred to our department for reconstruction of the large post-excisional defect. Surgical options were evaluated and the temporalis muscle flap with skin graft from the inguinal area were utilized. Other possibilities included free flaps, such as the ALT flap. However, the chosen surgical approach has significant advantages compared to free flaps, such as: shortened duration of surgery, lower risk for ICU admission, lower burden of care.
A temporal muscle flap was designed, as dissection and elevation of the flap was done through a classical open temporal approach. Then, the flap was mobilized and flipped to provide vascularized coverage of the exposed bone. Figure 2.
A manually perforated skin graft from the inguinal area was used as an external layer. Simultaneously, a Z-plasty of the EAC was performed to preserve canal patency and prevent postoperative stenosis. Figure 3.
The postoperative course was uneventful. The flap demonstrated good perfusion, and at one-month follow-up, there was complete healing and full graft integration over the temporalis muscle flap.
The patient was subsequently referred for targeted therapy with vismodegib (Erivedge) based on tumor molecular profile and characteristics. No adjuvant chemo- or radiotherapy was included in the treatment protocol Regular postoperative imaging showed only fibrotic changes consistent with healing. The most recent MRI examination, four years after surgery, demonstrated no recurrence and a stable disease.
Clinically, 4 years postoperatively, the patient exhibited a well-vascularized, stable reconstruction without meatal stenosis, suitable for future autologous cartilage or implant-based auricular reconstruction. Figure 4.
Moreover, novel technologies such as 3D bioprinting are widely used in creating biocompatible implants, especially when the external ear is involved.
4. Discussion
Surgical management of complex oncological post-resection defects of the external ear and external acoustic meatus requires detailed understanding not only of the anatomical elements, but also vascularity and innervation of local tissues. In our case, a subtotal ear amputation with exposure of the mastoid bone and disruption of the posterior wall of EAC, created a composite, multi-dimensional problem, involving skin, missing cartilage framework and possible bone necrosis. Well-vascularized and thick coverage is required to reconstruct the area and prepare it for future outer ear reconstruction possibilities, including autologous cartilage, Medpor etc.
Anatomical considerations and reconstructive implications
The auricle is an elastic cartilaginous framework, covered by thin skin and composed of the following subunits: helix, antihelix, concha, tragus, antitragus and fibrofatty subunit, called lobulus. The elastic cartilage of the auricle is covered by perichondrium, which is firmly attached to anterior side and loosely to the posterior side. The auricle serves both functional and aesthetic purpose, contributing to the hearing aspect and facial symmetry. Loss of the 3-dimensional organ not only impairs the collection and directing of sound waves, but also causes severe cosmetic deformity. The EAC is critical for sound conduction and represent a surgically sensitive region due to its layered structural composition. From a reconstructive standpoint, the anatomical constraints of the EAC and the importance of maintaining physiological diameter highlights the need for early, timely and proactive stenosis prevention measures, especially following oncologic resections [1,5,6,7].
When the mastoid or temporal bone is exposed, a vascularized flap is mandatory to ensure durable coverage and minimize infection, necrosis or sequestrum of the bone.
The temporal muscle flap offers several advantages: robust and reliable vascularization, proximity to the defect, ability to cover exposed bone, and formation of a stable bed for secondary procedures such as cartilage framework placement or prosthetic fitting. It is an excellent regional flap for head defects’ reconstruction and it is widely recognized as a reliable and safe option for reconstruction after orbital exenteration, large midface defects or facial palsy. It is classified under Mathes-Nahai type III flap with two dominant vascular pedicles- the deep temporal arteries (branches of the maxillary artery) and the middle temporal artery (branch of the superficial temporal artery) [5,8,9].
Alternative Reconstruction options
Alternatives to the temporalis muscle flap include:
Free flap transfer- microvascular reconstructive surgery with radial forearm free flap or anterolateral (ALT) flap. These flaps provide sufficient coverage and vascularity. However, donor site morbidity is higher compared to the usage of temporalis muscle flap. Secondly, survival of the free flaps is of greater risk than to regional flaps. Thirdly, the implication of free flaps significantly increases the duration of the surgery and it is associated with higher rate of ICU admission. Recovery period and burden of care is significantly lower with the employment of regional head flaps instead of free flaps. Cervicofacial advancement flap might be insufficient in widely exposed bone and scalp rotational flaps are more suitable for superiorly located defects. Other local transposition flaps, such as the bilobed flap could be a possible option. However, for extensive defects with bone exposure, more robust vascularization and tissue volume is required to cover the defect [10,11,12,13] Another alternative to the temporal flap is the supraclavicular island flap, which has a long pedicle and vast application in various head and neck defects, providing sufficient coverage and relatively close texture and color match of the surrounding tissues [14].
EAC stenosis prevention
The Z-plasty is a key technique to prevent cicatricial EAC stenosis, a frequent complication after oncologic surgery in this region. Other described techniques include M-plasty, skin-grafted stents, rotational or transpositional flaps, or temporoparietal fascia flaps [11,12,13].
Oncologic considerations
Adjuvant therapy with vismodegib is consistent with current recommendations for high-risk, locally advanced, or recurrent BCC [15,16,17]. At four-year follow-up, the patient demonstrated stable reconstruction and no recurrence, supporting the durability and oncologic safety of this approach.
Failure to address all anatomical implications and local status may result in conductive hearing loss, recurrent infection, keratin debris accumulation, chronic ottorhea and significantly low postoperative quality of life and functional outcome.
At long-term follow-up, the patient maintained a stable reconstruction with no evidence of recurrence, confirming the durability and oncologic safety of this approach. Further reconstruction of the auricle with autologous tissues or implant is considered on the next stage of treatment.
5. Conclusions
Temporal muscle flip flap reconstruction, skin grafting and meatal Z-plasty offers a safe, single-stage, and effective technique for coverage of large post-oncologic defects involving the mastoid region. It ensures durable vascularized tissue, prevents meatal stenosis, and provides a solid foundation for secondary auricular reconstruction, if desired. Additionally, the temporal flap pertains several advantages over free or other regional flaps, concerning duration of surgery, rate of complications and hospital stay. Furthermore, had the temporalis flap been unsuccessful, we would still have the opportunity to address the issue with the previously mentioned options.Long-term follow-up in this case confirms both oncologic control and functional success.
Author Contributions
Conceptualization, K.G. and I.G.; methodology, K.G.; software, I.G.M.B.; validation, K.G.; formal analysis, P.K.; investigation, P.K.; resources, K.G.; data curation, I.G.; writing—original draft preparation, K.G.; writing—review and editing, K.G.; visualization, I.G.; supervision, K.G, M.B..; project administration, P.K.; funding acquisition, I.G.
Funding
This research received no external funding
Institutional Review Board Statement
Ethical review board statement was waived for this study due to its case report nature.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data are contained within the article.
Conflicts of Interest
The authors declare no conflicts of interest..
Abbreviations
The following abbreviations are used in this manuscript:
| BCC | Basal Cell Carcinoma HPV- Human Papilloma Virus ENT-Ear,Nose and Throat. |
| EAC | External auditory canal |
| EAM | External auditory meatus |
| SCC | Squamous cell carcinoma |
References
- Özgür, E; Kamiloğlu, U; Temiz, P; Eskiizmir, G. Skin Cancers of the Auricle: A Retrospective Analysis of 41 Patients. Turk Arch Otorhinolaryngol 2020, 58(3), 169–173. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gigov, K.; Ginev, I.; Minev, I.; Kavradzhieva, P. Three-Layer Reconstruction of a Full-Thickness Nasal Alar Defect after Basal-Cell Carcinoma Removal. Reports 2024, 7, 75. [Google Scholar] [CrossRef] [PubMed]
- Prendergast, Peter. Anatomy of the External Ear. 2013. [Google Scholar] [CrossRef]
- Pignatti, M.; Sorbi, G.; Pinto, V.; et al. Use of the Spare-Part Strategy to Reconstruct the External Auditory Canal After Subtotal Auriculectomy for Basal Cell Carcinoma. Indian J. Otolaryngol. Head Neck Surg. 2022, 74 Suppl. 3, 5974–5977. [Google Scholar] [CrossRef] [PubMed]
- Landfald, I.C.; Vazquez, T.; Okoń, A.; Olewnik, Ł. Temporalis Muscle Flap in Craniofacial Reconstruction: Anatomy, Techniques, Outcomes, and Innovations. Front. Surg. 2025, 12, 1678935. [Google Scholar] [CrossRef] [PubMed]
- Mozaffari, M; Nash, R; Tucker, AS. Anatomy and Development of the Mammalian External Auditory Canal: Implications for Understanding Canal Disease and Deformity. Frontiers in Cell and Developmental Biology. 2021, 8, 617354. [Google Scholar] [CrossRef] [PubMed]
- Sundar, P. S.; Chowdhury, C.; Kamarthi, S. Evaluation of Human Ear Anatomy and Functionality by Axiomatic Design. Biomimetics 2021, 6(2), 31. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, S; Govindasamy, G; Hussain, SA; Maheswaran, S. Temporalis Muscle Flap in Head and Neck Reconstructions Is That Forgotten or Forbidden? Our Case Series and Review of Literature. Indian J Surg Oncol 2017, 8(3), 321–325. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ein, L.; Daniyan, O.; Nicolli, E. Temporalis muscle flap. Oper. Tech. Otolaryngol. Head Neck Surg. 2019, 30(2), 120–126. [Google Scholar] [CrossRef]
- Lam, D.; Carlson, E.R. The temporalis muscle flap and temporoparietal fascial flap. Oral Maxillofac. Surg. Clin. North Am. 2014, 26(3), 359–369. [Google Scholar] [CrossRef] [PubMed]
- Hossan, A; Nafis, A; Khan, D; Alam, M. Regional vs. Free Flap Reconstruction in Orofacial Surgery: A Comparative Analysis. IOSR Journal of Dental and Medical Sciences. 2025, 24(6), 55–61. [Google Scholar] [CrossRef]
- Gigov, K.; Ginev, I.; Shopova, D. Removal of a Recurrent Calvarial Hemangioma Followed by Autologous Iliac Crest Bone Reconstruction: A Case-Based Experience. Curr. Oncol. 2025, 32, 551. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.C.; Speed, O.; Boyette, J.R.; Saadi, R. A Systematic Review of Local Flaps Utilized for External Auditory Canal Defects. Craniomaxillofac. Trauma Reconstr. 2024, 17, 59. [Google Scholar] [CrossRef] [PubMed]
- Kokot, N.; Mazhar, K.; Reder, L.S.; Peng, G.L.; Sinha, U.K. The Supraclavicular Artery Island Flap in Head and Neck Reconstruction: Applications and Limitations. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Ulaganathan, P; Subramanian, S. Bilobed flap cover for ear resection defect: A case report and literature review. International Journal of Case Reports in Surgery 2025, 7(1), 96–100. [Google Scholar] [CrossRef]
- Gökmen, İ; Şen, E. Vismodegib treatment in locally advanced basal cell carcinoma limited to the facial region: a single-center experience. BMC Cancer 2025, 25(1), 1514. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jabbehdari, S.; Veluvolu, M.; Kornhauser, T.; Jennings, T.A.; Pemberton, J.D. Vismodegib as an adjuvant treatment for periorbital basal cell carcinoma: a case report and review of literature. Ann. Transl. Med. 2024, 12(3), 54. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A) Initial tumor lesion. (B) After radical excision with histologically verified clear resection margins. Temporalis muscle flip flap was designed to cover the large defect including exposed mastoid bone.
Figure 1.
(A) Initial tumor lesion. (B) After radical excision with histologically verified clear resection margins. Temporalis muscle flip flap was designed to cover the large defect including exposed mastoid bone.

Figure 2.
(A,B) Temporalis muscle flip flap covering the exposed bone.

Figure 3.
(A) Temporalis muscle flip flap covering the defect and Z-plasty of the external acoustic meatus; (B) Skin graft to cover the muscle.
Figure 3.
(A) Temporalis muscle flip flap covering the defect and Z-plasty of the external acoustic meatus; (B) Skin graft to cover the muscle.
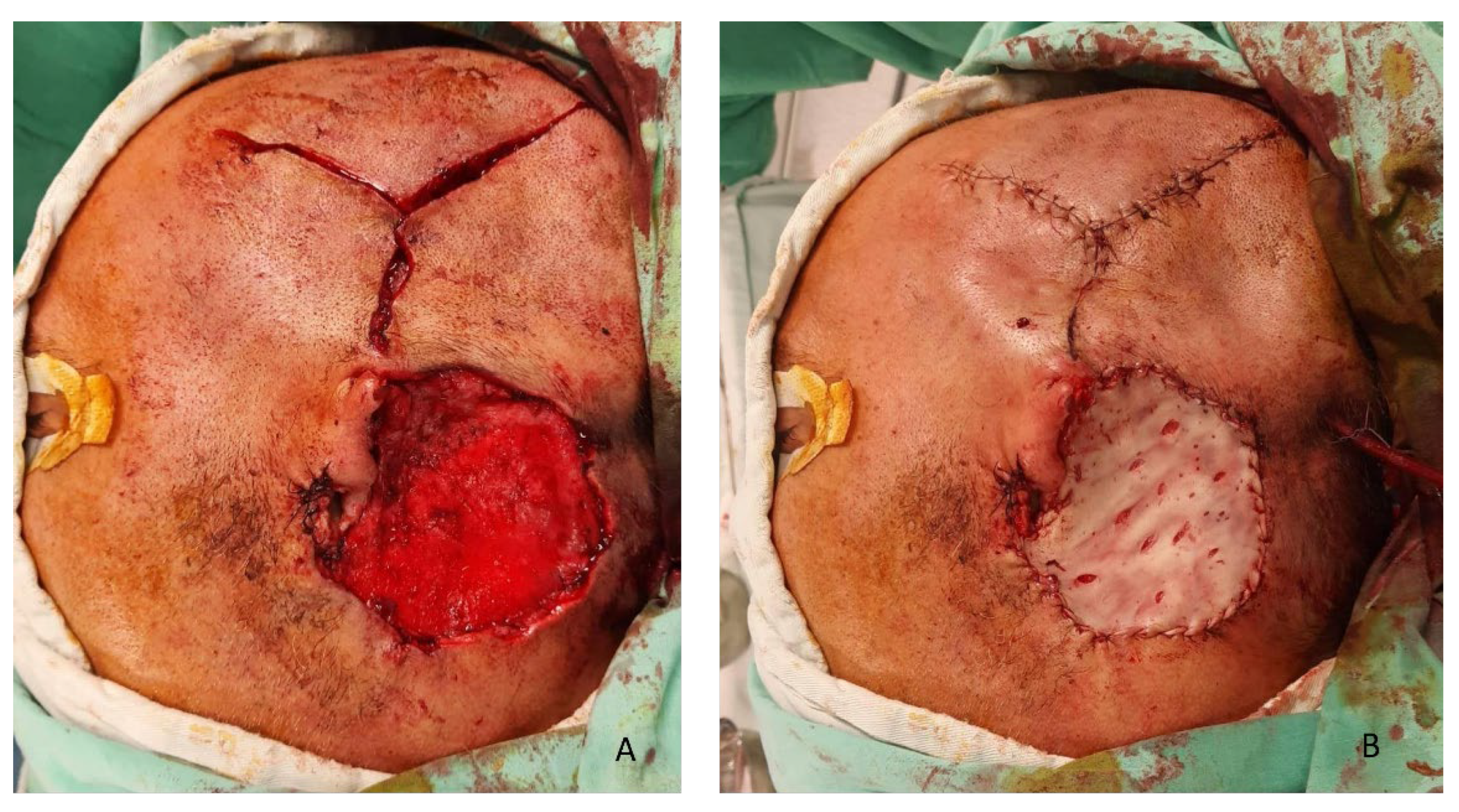
Figure 4.
Results 4 years after surgery. No stenosis of the external meatus can be observed. Now the patient can be planned for ear reconstruction.
Figure 4.
Results 4 years after surgery. No stenosis of the external meatus can be observed. Now the patient can be planned for ear reconstruction.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



