Submitted:
17 December 2025
Posted:
18 December 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background: This study analyzed the epidemiological profile of patients with non-melanoma skin cancer, female breast cancer, prostate cancer, colon and rectum cancer, lung cancer, and stomach cancer in southeastern Brazil (Espírito Santo, São Paulo, Minas Gerais, and Rio de Janeiro), covering the pre-pandemic period (2017 to 2019) and the pandemic period (2020 to 2022). Methods: The DATASUS database was used to assess possible impacts of percentage differences between these periods through point regression analysis and comparisons between the pre-pandemic and pandemic periods, as well as between the sexes using the Student's t-test. Results: The results suggest that sex-specific characteristics impose varying impacts and incidences on each gender. In Espírito Santo, there was a growing trend in stomach and non-melanoma skin cancers, while in São Paulo, only stomach cancer showed a statistically significant upward trend. Regarding staging, it was observed that during the pandemic period, the highest incidence was in stage IV, whereas in the pre-pandemic period, the highest incidences were in stages 0 and I, with medium and small effect sizes. Furthermore, the loss of pre-pandemic data was 11.46% (54,080 cases), while during the pandemic, the loss was 27.52% (129,869 cases), both statistically significant values of considerable magnitude. Conclusion: It can be concluded that there was a significant increase in the temporal trend only for stomach cancer in the states of São Paulo and Espírito Santo; for the other cancers and states, the trends were stationary. The high rate of missing data during the pandemic suggests a considerable impact on the results, highlighting the importance of additional prospective studies to better understand the effects of COVID-19 on oncology.
Keywords:
cancers
; pandemic
; SARS-COV-2
; COVID-19
1. Introduction
The José Alencar Gomes da Silva National Cancer Institute (INCA) declares that cancer is the second leading cause of death in Brazil, second only to deaths caused by heart problems [1]. Cancer is a disease that encompasses more than 100 different types of malignant diseases whose mechanism of action is the disorderly growth of cells, which can invade tissues and/or organs.
Among all types of malignant neoplasms, the most common in Brazil are: non-melanoma skin (31.3%), female breast (10.5%), prostate (10.2%), colon and rectum (6.5%), lung (4.6%) and stomach (3.1%) (Brazil, 2020; Brazil 2022). INCA estimates that 704 thousand new cases of cancer in Brazil for each year of the three-year period 2023-2025, especially in the South and Southeast regions, which concentrate around 70% of all statistical incidence [1,2].
On December 31, 2019, several cases of pneumonia in Wuhan City, Hubei Province, People’s Republic of China were reported to WHO. It was a new strain of corona virus that had not yet been identified contaminating humans [3]. At the end of January 2020, more precisely on the 30th, the WHO declared that the outbreak of the new corona virus was considered a Public Health Emergency of International Concern (PHEIC) – the highest alert level of the Organization, as provided for in the Regulation International Sanitary. This decision aimed to improve the organization, prevention and control/stopping of the spread of the virus. Considering that these measures listed actions such as social isolation policies, school closures, restrictions on movement, work in addition to the demand for more hospital beds, hypothesizes impacts on the diagnosis and treatment of all neoplasms in Brazil in other countries of the world [4,5].
In view of the above, the objective of the present study is to analyze the epidemiological profile, staging, diagnosis, temporal trend and compare the referred values in the years that preceded the pandemic (2017, 2018 and 2019) and in the years of the pandemic (2020, 2021 and 2022) in relation to non-melanoma skin, female breast, prostate, colon and rectal, lung and stomach cancers in the Southeast region of Brazil, using public data available on DATASUS [6]. The importance of this work is justified by the fact that it elucidates part of the numerous repercussions that the pandemic period has had on the rates of diagnoses and deaths due to the root cause of the neoplasms in question in the Southeast region, analyzing the so-called pre-pandemic (2017 to 2019) and pandemic periods (2020 to 2022).
2. Materials and Methods
This was a cross-sectional, retrospective study that analyzed public data from the DATASUS portal for the period from 2017 to 2022. Since it involved secondary and public data, it was exempt from review and approval by an Ethics Committee in Research with Human Beings according to resolution nº. 510/2016 of the National Health Council [7]. After selecting the cases, descriptive statistics and incidence rates (per 100,000 inhabitants) were calculated, considering the population estimates for each year obtained from the IBGE cities page [8]. This incidence rate was used to conduct the analysis of temporal trends, annual percentage change (APC), and confidence intervals (CI 95%) of the sample using the Joinpoint Regression Program, version 4.9.1.0 [9].
In this study, due to the examination of only six years of data, no inflection points were included (at least seven years of data are needed to test for an inflection point). The analysis focused solely on whether the incidence rates of the studied malignancies exhibited a stationary, increasing, or decreasing trend from a statistical perspective, and this was conducted for both sexes and overall (both sexes) [10].
The next analysis was the comparison of the mean time intervals (in days) between cancer diagnosis and the start of treatment, between the pre-pandemic periods (2017 to 2019) and the pandemic period (2020 to 2022). For this analysis, a normality test (Shapiro-Wilk) was conducted beforehand, followed by a Student’s t-test using bootstrap techniques with 10,000 re-samplings and Welch’s correction for unequal variances [11]. In addition, for this comparison, effect size was calculated using Cohen’s “d” to determine the magnitude of significant differences, if detected [12].
Subsequently, analyses were conducted to verify whether there were significant differences in the staging grades (ranging from 0 to IV) of each neoplasia between the pre-pandemic and pandemic periods, as well as the amount of missing or unreported data for each neoplasia during those periods. Both calculations were performed for the Southeast region. The Chi-square test was used to determine whether the distribution of cases across periods showed significant differences [13].
To measure the magnitude of the differences (if found), Cramer’s “V” was calculated12. Both analyses were executed in RStudio version 3.5.3 [14].
The significance level for this study was set at p < 0.05.
3. Results
Information on the seven most common types of malignant neoplasms in both sexes, as well as those most prevalent among men and women in the southeastern states, was analyzed, totaling seven pathologies and a combined total of 471,864 cancer cases distributed across the four states of the Southeast region. In comparing the distribution of cancer cases between men and women in each state, it was observed that cancers of the colon, rectum, non-melanoma skin, and breast significantly affect women more than men, while malignant neoplasms of the stomach, lung, and prostate have significantly higher incidence rates. Significant differences were found in both women and men, with small effect sizes, indicating that while these differences are statistically significant, they are of low magnitude clinically (p = 0.00; Cramer’s V < 0.09) (see Table 1).
In the results obtained, all states showed significantly lower values during the pandemic period, with effect sizes ranging from negligible (lung cancer, state of Espírito Santo, p=0.00; Cohen’s d = 0.09) to moderate (prostate cancer in all states, p=0.00; Cohen’s d > 0.40), as shown in Figure 1. When analyzing the temporal trend of the incidence rates of the studied cancers (Figure 1), both in the Southeast region as a whole and in each state, despite the percentages of annual changes (APC) showing positive values, the analysis using the Joinpoint regression method indicates that significant trends were only detected in the states of Espírito Santo and São Paulo. In Espírito Santo, stomach cancer (p=0.00; CI = 11.20 – 19.10) and non-melanoma skin cancer (P=0.01; CI = 22.00 – 122.00) exhibited a tendency to increase, while in São Paulo, only stomach cancer (p=0.00: CI = 8.80 – 52.10) showed a significant upward trend (see Figure 1).
Regarding the comparison of the average time (in days) between diagnosis and initiation of cancer treatment during the pre-pandemic period (2017 to 2019) and pandemic period (2020 to 2022) analyzed at the state level, a total of 287,915 records were available for this information, with 158,366 cases in the pre-pandemic period and 129,549 cases in the pandemic period. Regarding the analysis of staging levels in cancer diagnoses between the periods of the present study, for each neoplasm in each state, the data analyzed are the same as in the analysis of the average time between diagnosis and treatment (287,915 records). The results (Table 2) indicate that in most cases of cancer, in each state, the proportion of cases diagnosed with stage IV occurred during the pandemic period, while cases with stages 0 and I were more common in the pre-pandemic period. Furthermore, the effect sizes calculated for these differences were mostly considered small (Cramer’s V <0.10) or moderate (Cramer’s V > 0.10), indicating that these differences are clinically insignificant (see Table 2).
Regarding the records of patients who did not have staging information due to being referred for surgical treatment (Figure 2), the frequency distribution analysis between the pre-pandemic and pandemic periods showed that, with the exception of breast cancers in the states of Rio de Janeiro and Espírito Santo and prostate cancer in Espírito Santo, the number of cases sent for surgical treatment was significantly higher than in the pre-pandemic period. The magnitude of these differences was mostly moderate, ranging from negligible (Cramer’s V = 0.01, breast cancer in the state of São Paulo) to strong (Cramer’s V = 0.25, non-melanoma skin cancer in Rio de Janeiro) (see Figure 2).
During both the pre-pandemic (2017 to 2019) and pandemic (2020 to 2022) periods, there was a notable loss of data concerning treatment and staging for cancer patients. Out of 471,864 cases reported, 39.00% did not provide this information. The pandemic period saw a significantly greater loss of data compared to the pre-pandemic period. Specifically, there was a 27.52% loss of data during the pandemic compared to 11.46% before it, a statistically significant finding. This trend was consistent across all states and for all types of neoplasms, except for non-melanoma skin cancer in Minas Gerais and São Paulo (see Figure 3 and Figure 4).
4. Discussion
Among the characteristics evaluated in the research, the predominance of some types of cancer in one of the sexes was observed. It was noted that neoplasms of the colon, rectum, non-melanoma skin, and breast affect significantly more women, while cancers of the stomach, lung, and prostate have a significantly higher incidence in men, which is corroborated by the current literature worldwide [15,16,17].
In women, breast cancer was confirmed as being the most recurrent in the female population, while in men, prostate cancer was the most prevalent [18,19,20]. Black men are the most affected by prostate cancer, usually with late diagnoses, thus presenting high mortality rates compared to white men [20,21]. Another factor related to this racial disparity is social, as black men have less access to healthcare means, as well as prevention, early diagnosis, and treatment [20,21].
It is noteworthy that in the present study, the occurrence of prostate cancer in women was observed: 14 cases in MG, 18 cases in RJ, and 35 cases in SP. These data may be justified because they are possibly cases of diagnoses in trans women, transvestites, and non-binary individuals or errors in data entry into the system.
The analysis using the joinpoint regression method informs that only in the states of Espírito Santo and São Paulo were significant trends detected: stomach cancer in ES and non-melanoma skin cancerin SP, stomach cancer. A brazilian study conducted in 2022 [22] identified a high risk of gastric cancer-related mortality in space-time association in various regions of Brazil, during the first years of the study period (2000 to 2009). The study concluded that from 2010 to 2019, clusters of gastric cancer were identified in the Northeast region. The increase in mortality throughout the country in this analysis of data for 20 years shows the persistence of the high burden of gastric cancer in Brazil, especially in disadvantaged regions from the socioeconomic point of view [17,22].
This finding shows us that stomach cancer has been showing an increasing incidence and mortality over time, not only in the Southeast region but also in several other regions of Brazil. The contrast of this study with the growing tendency of cases of stomach cancer verified is that ES and SP are states with HDI (Human Development Index) between medium and high; not qualifying it as a socially disadvantaged region, however, it shows significant progression in the number of cases [22].
A North American survey has shown that the incidence and prevalence rates of melanoma cancer and non-melanoma skin cancer show a growth profile from 1990 to 2019, while mortality rates have remained reasonably stable. Women had higher incidence, prevalence, and death rates from non-melanoma skin cancer every year since 1990 [23]. The incidence and prevalence of both types of skin cancers were relatively higher in the northern half of the US than in the southern half. This trend was observed and confirmed by statistics in the state of ES [23].
Regarding the comparison of the average time in days between the diagnosis of the disease and the beginning of treatment in the pre-pandemic and pandemic periods (2020 to 2022) analyzed at the state level, we obtained 287,915 available records, with 158,366 cases in the pre-pandemic period and 129,549 cases during the pandemic period.
The findings showed that the average time between diagnosis and initiation of treatment was shorter in the pandemic period. However, the study [24] brazilian shows a contrast to the data found. A retrospective cohort study was carried out with women undergoing breast exams and procedures in São Paulo, SP, Brazil, in the year 2020, compared with the same period in 2019. The number of exams, cancer detection rates, pathological findings, and risk factors. In total, 32,144 patients who underwent breast imaging examinations and procedures in 2020 were analyzed, and a reduction of 78.9% was observed in the first period and 2.7% in the second period of the year. At the end of 2020, six fewer patients were diagnosed with breast cancer than in 2019, although the number of patients undergoing mammography was 35% lower 30. Silva et al. (2022) [25], in their cross-sectional, exploratory, and descriptive study, studied male and female adult cancer patients undergoing treatment from September to December 2021. It was observed that 59.78% had greater difficulty scheduling appointments and exams, and 43.48% had difficulties with continuing treatment, compared to before the pandemic. It also observed that 46.74% avoided seeking care for fear of contamination, and 57.61% reported having received information to seek medical care only in emergency cases [31,32].
These contradictory results can be attributed to the fact that the present study deals with a macro view of the states and the Southeast region, and the aforementioned studies are studies of local scope (a hospital or specific health service) or municipality. However, they do not invalidate each other; in fact, they complement each other because both portray a state-of-the-art reality on the subject. The findings regarding the pre-pandemic and pandemic staging profiles showed differences: cases diagnosed with stage IV occurred in a greater proportion in the pandemic period, and cases with stages 0 and I in the pre-pandemic period.
According to Jesus et al. (2020) their results pointed to a worsening in the tumor staging of these patients, reaching a 115% increase in cases of metastasis. The main neoplasms found were breast, head and neck, prostate, and cervical cancer [26].
Among all the possible justifications for the fact that, in the pandemic period, the staging of cancer patients is diagnosed in a more compromised clinical profile is due to the low demand for hospital sectors [27,28,29]. This drop was due to the general fear instilled in the population in the face of COVID-19 contagion, difficulty in accessing the public and private health system (which, during the pandemic, concentrated its entire structure and investment on the treatment of people affected by this disease), a decrease in prevention policies and screening for early-stage cancers (such as mammography exams and Pap smears), public lockdown determinations in various areas of the country that restricted all activities in all segments (except hospitals), social isolation, and among other causes [17,29,30,31].
The relationship between the diagnosis of cancers in the pandemic being mostly in stage IV leads the patient to lose the prognosis of improvement or cure; since the discovery of any neoplasm in the early stages (0 and I in the vast majority) guarantees the patient greater therapeutic opportunities and great chances of life. On the other hand, late discoveries significantly reduce the chances of cure, consequently increasing the chances of death due to the disease [32,33,34].
Another important data that the study analyzed were the records of patients who did not have staging information because they were referred for surgical treatment. Frequency distribution analyzes between periods showed a decrease in the number of patients undergoing surgery in all regions and all cancers studied, except breast cancer in RJ and ES and prostate cancer in ES.
During the pandemic period [25], cases of neoplasms of the respiratory system, in men, there were significant reductions in therapy in general in all regions of Brazil. It was noticed a reduction of 68.22%, 19.58%, and 57.24% of cases treated surgically, with chemotherapy and radiotherapy in northeastern Brazil. For the neoplasms that affected women, there was an increase in the number of surgeries and a low level of radiotherapy throughout Brazil [35].
One aspect highlighted throughout the research was the amount of lost or uninformed data. This issue was present both in the pre-pandemic period and in the pandemic period. The pandemic period had higher percentages of loss, and this could be due to the chaotic moment the world was going through. However, several studies show that data loss or underreporting in the database is quite recurrent and does not only happen with neoplasm data; but also with notifiable diseases, births, and even deaths [25,36,37].
However, regarding the epidemiological study of neoplasms, this loss of data becomes very relevant and determinant for further research. Since this pandemic period, whenever understood in any analyzed period, the study will tend towards a statistical bias; because it is data that does not faithfully match the scenario. Furthermore, underreporting limits public measures that are based on statistical analyses of diagnosis, treatment, staging, deaths, among others, which will also have impacts when analyzing data with a large percentage of loss [37].
Thus, the study suggests that, as in many other segments and sectors of the world, the COVID-19 pandemic has also had an impact on the profile of patients affected by some form of neoplasia. This influence was confirmed through changes in public policies and incentives that, in that period, were directed only to control and remedy the situation of public calamity. Therefore, several services were impacted by the lack of structure, reduction of preventive exams, and reduced demand for health services.
5. Conclusions
In summary, the results indicate a significant increase in temporal trend only for stomach cancer in São Paulo and Espírito Santo, and for non-melanoma skin cancer in Espírito Santo. It was observed that men had slightly higher rates than women in cancers such as stomach, rectum, and lung, although these differences had a relatively modest impact.
During the pandemic, there was an increase in the number of cancer cases compared to the pre-pandemic period, but this difference was of reduced magnitude. Another relevant finding was the significant reduction in the time between diagnosis and initiation of treatment, as well as in the staging of cases, during the pandemic compared to the previous period. It is important to highlight the high rate of data loss regarding staging during the pandemic, suggesting that this loss of data may have affected the results overall, altering the profile of patients diagnosed with cancer.
In conclusion, while the data points to increase in certain cancers like stomach and non-melanoma skin cancers in specific regions, the overall impact of the pandemic on cancer trends seems moderate. The slight gender differences observed in specific cancers were not pronounced enough to suggest substantial disparities. The reduced time between diagnosis and treatment initiation is a positive outcome. However, the substantial loss of staging data during the pandemic could have influenced these results, potentially skewing the true impact of the pandemic on cancer diagnoses and treatment patterns. Future studies should aim to address this gap to ensure a more accurate understanding of cancer trends during crisis periods.
Author Contributions
A.C.F.S.T. and M.J.B.S. contributed equally to this project. M.J.B.S. is the corresponding author. The specific contributions of authors are as follows; Conceptualization, A.C.F.S.T. and M.J.B.S.; methodology, A.C.F.S.T. and M.J.B.S.; software, A.C.F.S.T. and M.J.B.S.; validation, A.C.F.S.T. and M.J.B.S.; formal analysis, A.C.F.S.T. and M.J.B.S.; investigation, A.C.F.S.T. and M.J.B.S.; resources, M.J.B.S.; data curation, A.C.F.S.T.; writing—original draft preparation, A.C.F.S.T.; writing—review and editing, M.J.B.S.; visualization, A.C.F.S.T. and M.J.B.S.; supervision, M.J.B.S.; project administration, M.J.B.S.; funding acquisition, M.J.B.S. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Publicly available datasets were analyzed in this study. This data was obtained from the Oncology Treatment Monitoring Panel (Painel-Oncologia), freely managed and provided by the Department of Informatics of the Unified Health System (DATASUS), Brazil. The panel integrates records from the Ambulatory Information System (SIA), Hospital Information System (SIH), and Cancer Information System (SISCAN) to monitor cancer treatment timelines in compliance with Law No. 12.732/2012. This data can be found here: http://tabnet.datasus.gov.br/cgi/painel_onco/doc/painel_oncologia.pdf.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| APC | Annual Percentage Change |
| Bootstrap | Bootstrap resampling technique |
| CI | Confidence Interval |
| COVID-19 | Coronavirus Disease 2019 |
| Chi-square | Chi-square test |
| DATASUS | Department of Informatics of the Brazilian Public Health System |
| ES | Espírito Santo |
| FU | Federated Unit |
| HDI | Human Development Index |
| IBGE | Brazilian Institute of Geography and Statistics |
| INCA | Brazilian National Cancer Institute |
| MG | Minas Gerais |
| PAP | Papanicolaou |
| PHEIC | Public Health Emergency of International Concern |
| RJ | Rio de Janeiro |
| SARS-COV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
| SE | Southeast |
| SP | São Paulo |
| TNM | Tumor, Node, Metastasis |
| FU | Federated Unit |
| WHO | World Health Organization |
| n | Number of cases |
| n.d. | Not reported/Not determined |
| P-value | Statistical significance level |
References
- Brasil; Ministério da Saúde; Secretaria de Vigilância em Saúde. Vigitel Brasil 2019: principais resultados. Boletim Epidemiológico 2020, 51, 16. Available online: https://antigo.saude.gov.br/images/pdf/2020/April/16/Boletim-epidemiologico-SVS-16.pdf (accessed on 30 August 2025).
- Brasil; Instituto Nacional do Câncer. Estatísticas de câncer. Available online: https://www.gov.br/inca/pt-br/assuntos/cancer/numeros (accessed on 22 August 2025).
- Teixeira, C.F.D.S.; Soares, C.M.; Souza, E.A.; et al. A saúde dos profissionais de saúde no enfrentamento da pandemia de COVID-19. Ciência & Saúde Coletiva 2020, 25, 3465–3474. [Google Scholar] [CrossRef]
- Bharwani, A.; Li, D.; Vermund, S.H. A review of the effect of COVID-19-related lockdowns on global cancer screening. Cureus 2023, 15, e40268. [Google Scholar] [CrossRef] [PubMed]
- Patt, D.; Gordan, L.; Diaz, M.; et al. Impact of COVID-19 on cancer care: How the pandemic is delaying cancer diagnosis and treatment for American seniors. Journal of Clinical Oncology Clinical Cancer Informatics 2020, 4, 1059–1071. [Google Scholar] [CrossRef]
- Brasil; Ministério da Saúde. DATASUS TABNET. Available online: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sim/cnv/evitb10go.def (accessed on 30 August 2025).
- Brasil; Ministério da Saúde; Conselho Nacional de Saúde. RESOLUÇÃO no 510. Available online: https://bvsms.saude.gov.br/bvs/saudelegis/cns/2016/res0510_07_04_2016.html (accessed on 30 August 2025).
- Brasil. Brasil | Cidades e Estados | IBGE. Available online: https://ibge.gov.br/cidades-e-estados.html (accessed on 22 August 2025).
- Statistical Methodology and Applications Branch, Surveillance Research Program, National Cancer Institute. Joinpoint Regression Program, Version 5.0.2. Available online: https://surveillance.cancer.gov/help/joinpoint/tech-help/citation (accessed on 22 August 2025).
- Liu, B.; Kim, H.J.; Feuer, E.J.; Graubard, B.I. Joinpoint regression methods of aggregate outcomes for complex survey data. Journal of Survey Statistics and Methodology 2022, smac014. [Google Scholar] [CrossRef]
- Delacre, M.; Lakens, D.; Leys, C. Why psychologists should by default use Welch’s t-test instead of Student’s t-test. International Review of Social Psychology 2017, 30, 92–101. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; Serdar, M.A. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochemia Medica 2021, 31, 27–53. [Google Scholar] [CrossRef] [PubMed]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E. Análise Multivariada de Dados, 6ª ed.; Bookman: Porto Alegre, Brazil, 2009; pp. 1–688. [Google Scholar]
- RStudio Team. RStudio: Integrated Development for R; Version 4.3.2; Posit Support: Boston, MA, USA, 2024; Available online: https://www.rstudio.com/ (accessed on 30 August 2025).
- Wild, C.P.; Weiderpass, E.; Stewart, B.W. World Cancer Report: Cancer Research for Cancer Prevention, 3rd ed.; International Agency for Research on Cancer: Lyon, France, 2020; pp. 1–627. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Santos, M.D.O.; Lima, F.C.D.S.D.; Martins, L.F.L.; Oliveira, J.F.P.; Almeida, L.M.D.; Cancela, M.D.C. Estimativa de incidência de câncer no Brasil, 2023–2025. Revista Brasileira de Cancerologia 2023, 69, e3700. [Google Scholar] [CrossRef]
- Smetana, K., Jr.; Lacina, L.; Szabo, P.; Dvořánková, B.; Brož, P.; Šedo, A. Ageing as an important risk factor for cancer. Anticancer Research 2016, 36, 5009–5018. [Google Scholar] [CrossRef]
- Dunneram, Y.; Greenwood, D.C.; Cade, J.E. Diet, menopause and the risk of ovarian, endometrial and breast cancer. Proceedings of the Nutrition Society 2019, 78, 438–448. [Google Scholar] [CrossRef] [PubMed]
- Lillard, J.W.; Moses, K.A.; Mahal, B.A.; George, D.J. Racial disparities in Black men with prostate cancer: A literature review. Cancer 2022, 128, 3787–3795. [Google Scholar] [CrossRef] [PubMed]
- Yamoah, K.; Lee, K.M.; Awasthi, S.; et al. Racial and ethnic disparities in prostate cancer outcomes in the Veterans Affairs Health Care System. JAMA Network Open 2022, 5, e2144027. [Google Scholar] [CrossRef]
- Braga, L.L.B.C.; Ferreira, A.F.; Pinheiro, F.A.S.; et al. Temporal trends and spatial clusters of gastric cancer mortality in Brazil. Revista Panamericana de Salud Pública 2022, 46, 1. [Google Scholar] [CrossRef]
- Kumar, V.; Ailawadhi, M.; Dutta, N.; et al. Trends in early mortality from multiple myeloma: A population-based analysis. Clinical Lymphoma, Myeloma and Leukemia 2021, 21, e449–e455. [Google Scholar] [CrossRef]
- Tachibana, B.M.T.; Ribeiro, R.L.D.M.; Federicci, É.E.F.; et al. The delay of breast cancer diagnosis during the COVID-19 pandemic in São Paulo, Brazil. Einstein 2021, 19, eAO6721. [Google Scholar] [CrossRef]
- Silva, T.A.; Camargo, G.; Estevão, R.; Lisboa Coda Dias, N.; Hattori, W.T. Perfil epidemiológico dos casos de neoplasias pulmonares durante a pandemia da COVID-19 no Brasil. Journal of Health & Biological Sciences 2022, 10, e4519. [Google Scholar] [CrossRef]
- Jesus, A.S.; Guedes, T.D.S.; Martins, G.B. Impacto da pandemia de COVID-19 no atendimento do serviço de radioterapia em um hospital público de Salvador/BA. Cambio 2021, 20, 369–374. [Google Scholar] [CrossRef]
- Nabuco, G.; Pires de Oliveira, M.H.P.; Afonso, M.P.D. O impacto da pandemia pela COVID-19 na saúde mental: qual é o papel da Atenção Primária à Saúde? Revista Brasileira de Medicina de Família e Comunidade 2020, 15, 2532. [Google Scholar] [CrossRef]
- Ornell, F.; Schuch, J.B.; Sordi, A.O.; Kessler, F.H.P. “Pandemic fear” and COVID-19: mental health burden and strategies. Brazilian Journal of Psychiatry 2020, 42, 232–235. [Google Scholar] [CrossRef]
- Xiang, Y.T.; Yang, Y.; Li, W.; et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. The Lancet Psychiatry 2020, 7, 228–229. [Google Scholar] [CrossRef] [PubMed]
- Araujo, L.H.; Baldotto, C.; Castro, G., Jr.; et al. Lung cancer in Brazil. Jornal Brasileiro de Pneumologia 2018, 44, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Shuja, K.H.; Aqeel, M.; Jaffar, A.; et al. COVID-19 pandemic and impending global mental health implications. Psychiatria Danubina 2020, 32, 32–35. [Google Scholar] [CrossRef] [PubMed]
- Eckhardt, B.L.; Francis, P.A.; Parker, B.S.; Anderson, R.L. Strategies for the discovery and development of therapies for metastatic breast cancer. Nature Reviews Drug Discovery 2012, 11, 479–497. [Google Scholar] [CrossRef]
- Medford, A.J.; Gillani, R.N.; Park, B.H. Detection of cancer DNA in early stage and metastatic breast cancer patients. In Digital PCR; Karlin-Neumann, G., Bizouarn, F., Eds.; Springer: New York, NY, USA, 2018; Volume 1768, pp. 209–227. [Google Scholar] [CrossRef]
- Morais, I.; Rêgo, J.; Reis, L.; Moura, T. A importância do exame preventivo na detecção precoce do câncer de colo uterino: uma revisão de literatura. Revista Eletrônica Acervo Enfermagem 2021, 10, e6472. [Google Scholar] [CrossRef]
- Silva, T.C.D.; Fortes, R.C.; Ferrão, P.D.A. Percepção de pacientes oncológicos quanto ao impacto da pandemia de COVID-19 frente ao diagnóstico e tratamento do câncer. Brazilian Journal of Development 2022, 8, 6508–6532. [Google Scholar] [CrossRef]
- Da Costa Bezerra, Í.; Cardoso da Rocha, R.; Lucas Pereira Guimarães, G.; Dos Santos Santana, S.; Cunha Silva, Q.G.; Costa Tavares, P.P. Datasus: possibilidade de contribuição no combate à violência contra a mulher no Rio de Janeiro. Saúde Coletiva 2020, 10, 4194–4203. [Google Scholar] [CrossRef]
- Santos, B.G.D.; Silva, I.O.S.D.; Silva, G.D.O.; Silva, B.D.O.; Guedes, L.S. Um panorama da esquistossomose na Bahia: a realidade de uma doença negligenciada. Revista de APS 2020, 23. Available online: https://periodicos.ufjf.br/index.php/aps/article/view/33837 (accessed on 30 August 2025).
Figure 1.
Time trend analysis of cancer incidence rates in each state of the Southeast region. The figure shows the temporal evolution of seven cancer types across four Brazilian states from 2017 to 2022, illustrating trends both in the pre-pandemic (2017-2019) and pandemic (2020-2022) periods.
Figure 1.
Time trend analysis of cancer incidence rates in each state of the Southeast region. The figure shows the temporal evolution of seven cancer types across four Brazilian states from 2017 to 2022, illustrating trends both in the pre-pandemic (2017-2019) and pandemic (2020-2022) periods.
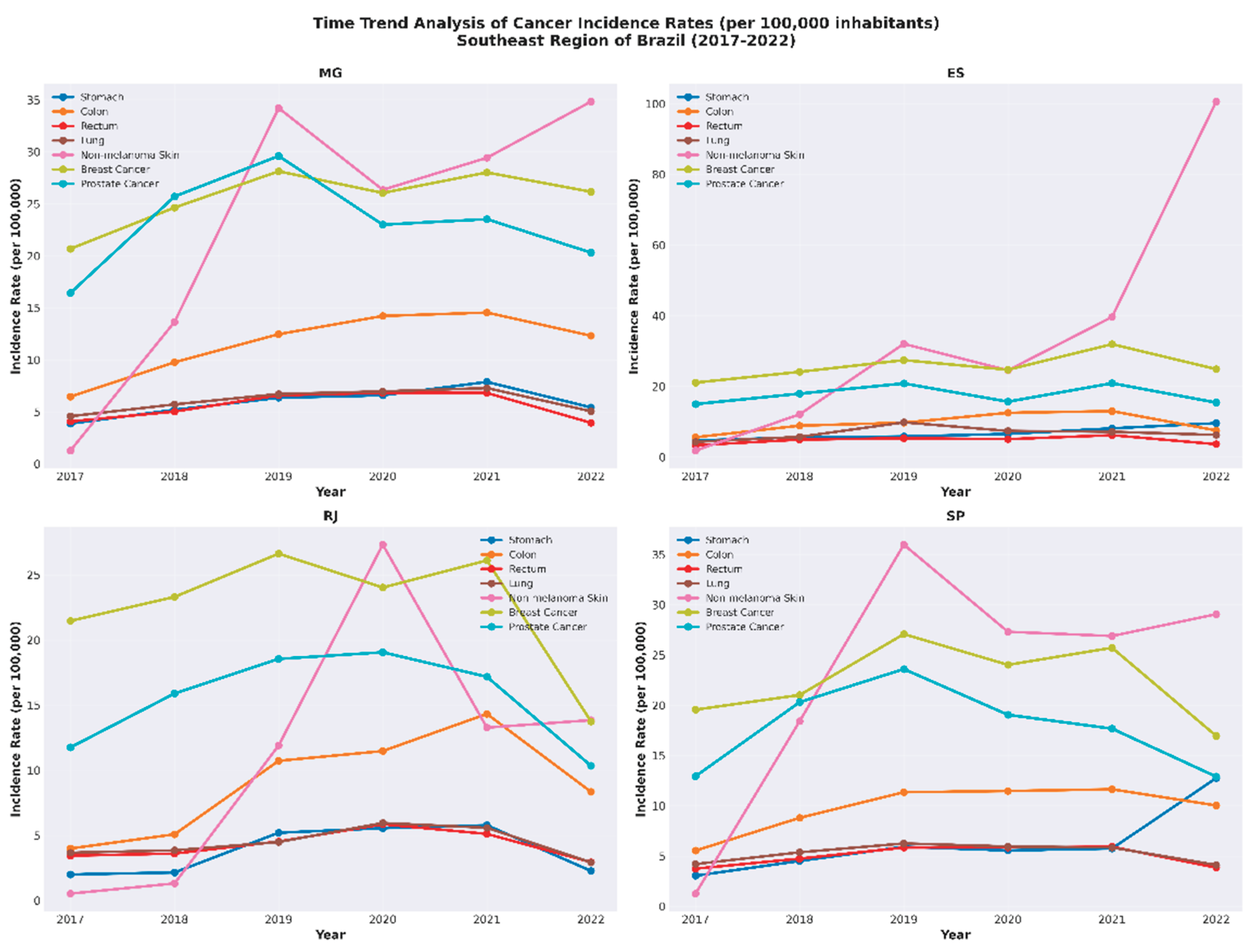
Figure 2.
Comparison of the frequencies of missing staging data for malignant neoplasms between the pre-pandemic and pandemic periods in the Southeast region using the chi-square test. The pandemic period shows substantially higher rates of missing staging information across all cancer types and states, indicating data quality issues during the health crisis.
Figure 2.
Comparison of the frequencies of missing staging data for malignant neoplasms between the pre-pandemic and pandemic periods in the Southeast region using the chi-square test. The pandemic period shows substantially higher rates of missing staging information across all cancer types and states, indicating data quality issues during the health crisis.
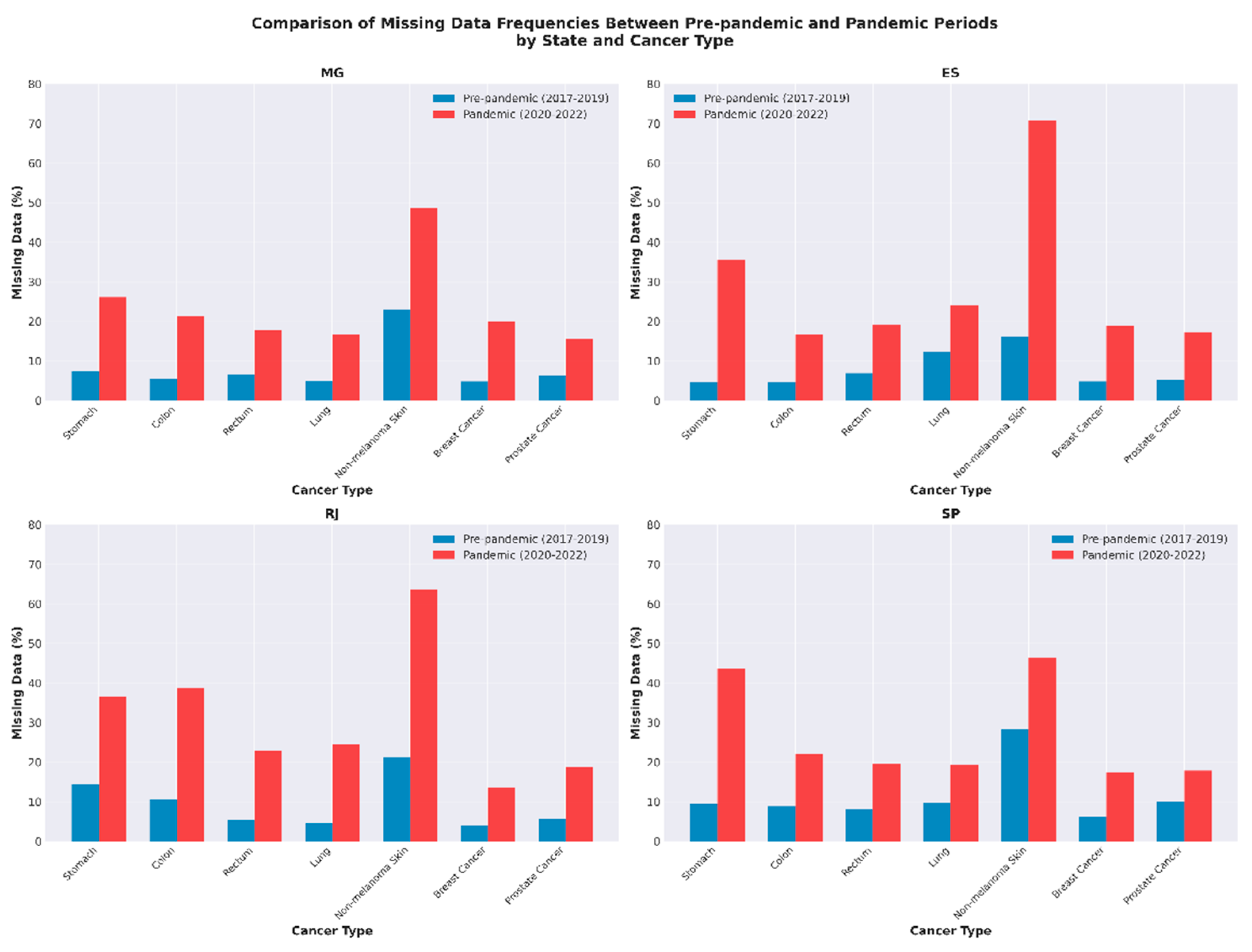
Figure 3.
Comparison of the frequencies of neoplasm staging between the pre-pandemic periods of each state by the chi-square test. Early-stage (stages 0 and I) cancer distribution: comparative analysis between Minas Gerais and São Paulo. Both states show reduced early-stage diagnoses during the pandemic period, though the magnitude varies by cancer type. This regional comparison suggests widespread but variable impacts of COVID-19 on cancer screening and early detection programs across the Southeast region.
Figure 3.
Comparison of the frequencies of neoplasm staging between the pre-pandemic periods of each state by the chi-square test. Early-stage (stages 0 and I) cancer distribution: comparative analysis between Minas Gerais and São Paulo. Both states show reduced early-stage diagnoses during the pandemic period, though the magnitude varies by cancer type. This regional comparison suggests widespread but variable impacts of COVID-19 on cancer screening and early detection programs across the Southeast region.
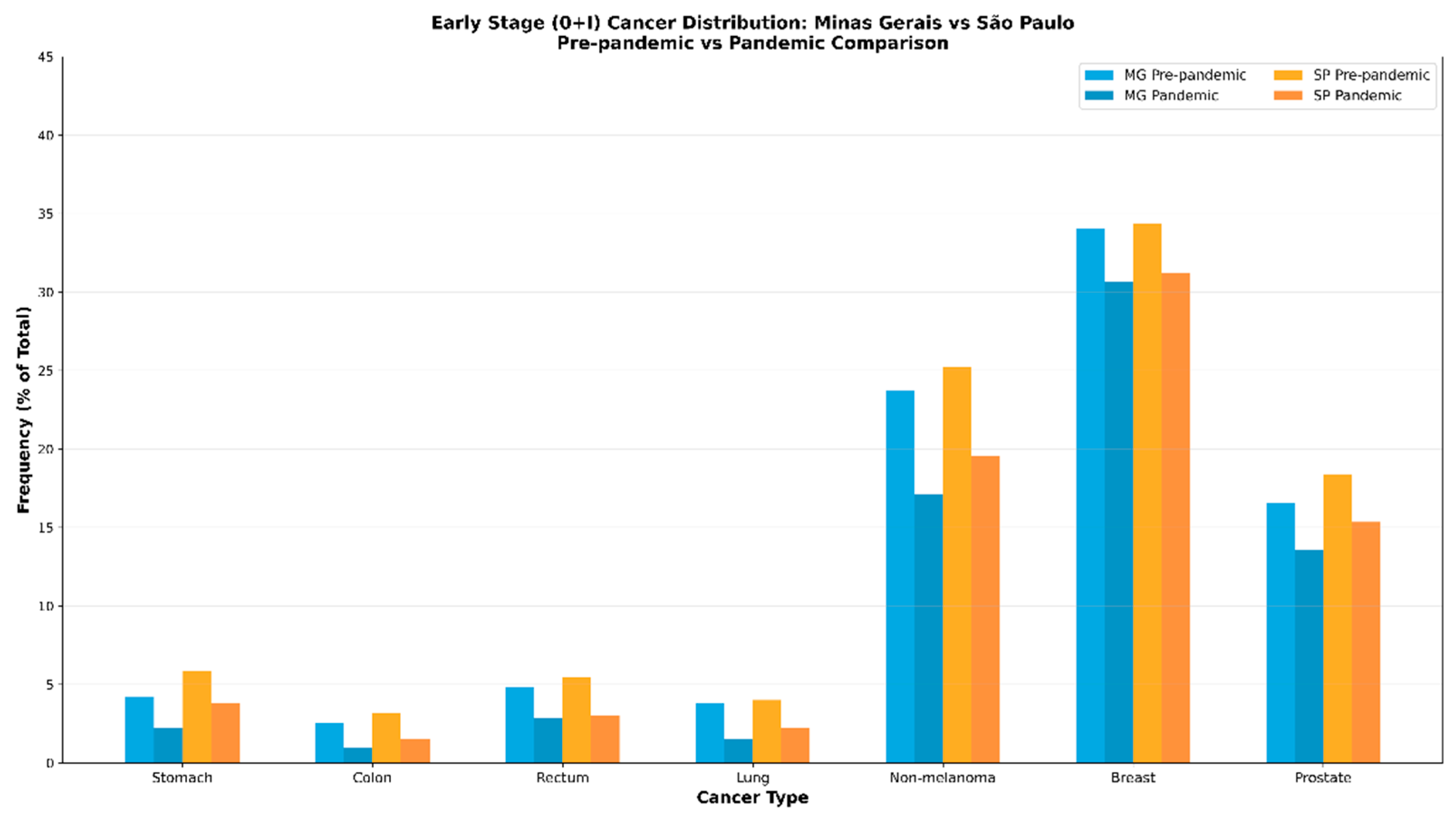
Figure 4.
Comparison of the frequencies of neoplasm staging between the pre-pandemic periods of each state by the chi-square test. Advanced-stage (stage IV) cancer distribution: comparative analysis between Minas Gerais and São Paulo. While both states show stage IV diagnoses representing similar proportions across cancer types, the pandemic period demonstrates region-specific variations in the relative frequency of advanced cases, reflecting potential differences in healthcare access and disruption patterns.
Figure 4.
Comparison of the frequencies of neoplasm staging between the pre-pandemic periods of each state by the chi-square test. Advanced-stage (stage IV) cancer distribution: comparative analysis between Minas Gerais and São Paulo. While both states show stage IV diagnoses representing similar proportions across cancer types, the pandemic period demonstrates region-specific variations in the relative frequency of advanced cases, reflecting potential differences in healthcare access and disruption patterns.
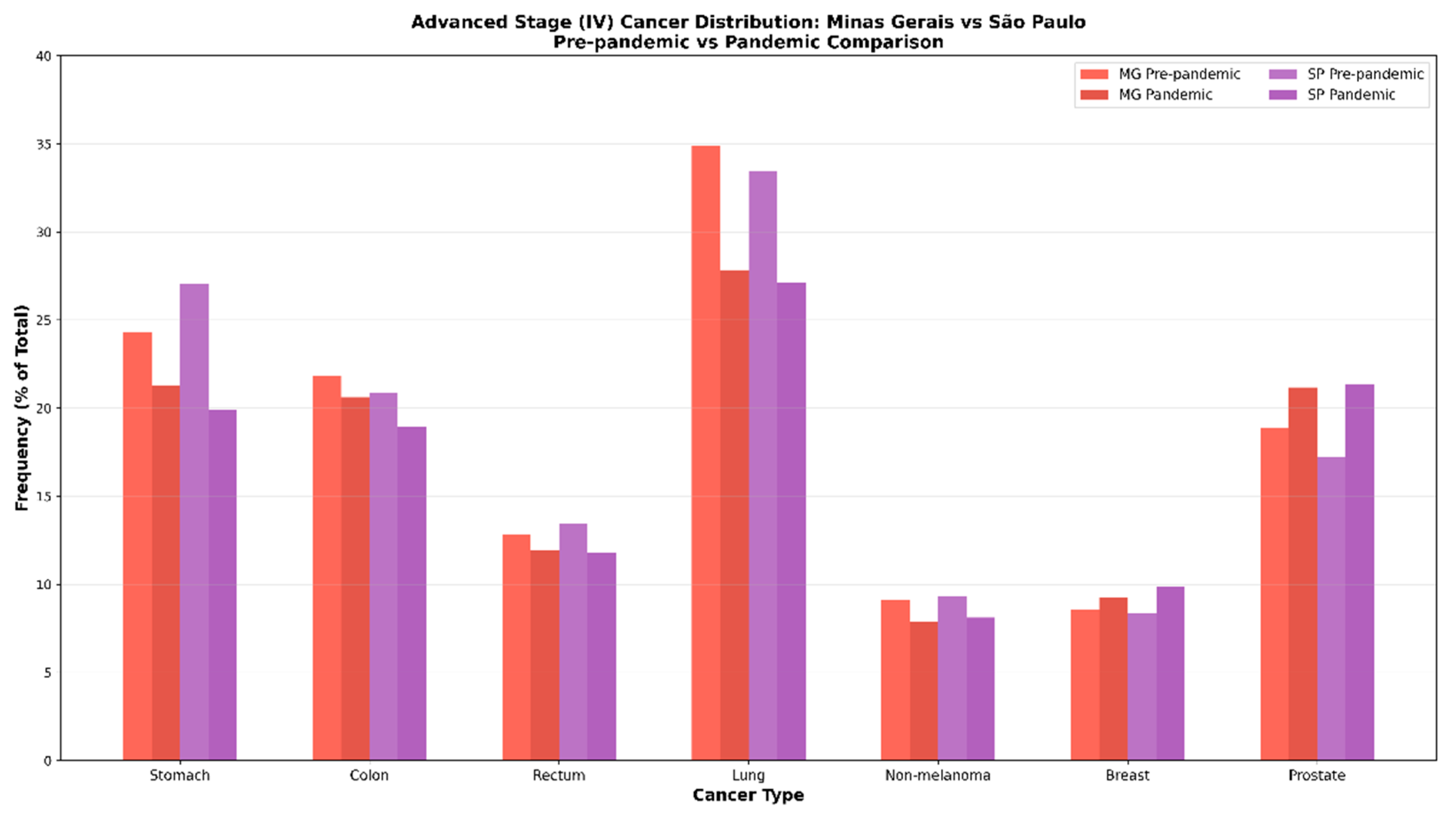

Table 1.
Absolute and relative frequencies of malignant neoplasms studied from 2017 to 2022.
| Cancer site | Gender* | Minas Gerais | Espírito Santo | Rio de Janeiro | São Paulo | P value |
Cramér’s V | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||||
| M | 4773,00 | 63,67 | 978,00 | 59,49 | 2099,00 | 53,26 | 9343,00 | 53,73 | 0,00 | 0,08 | |
| Stomach | F | 2724,00 | 36,33 | 666,00 | 40,51 | 1842,00 | 46,74 | 8047,00 | 46,27 | ||
| Total | 7497,00 | 100,00 | 1644,00 | 100,00 | 3941,00 | 100,00 | 17390,00 | 100,00 | |||
| M | 6819,00 | 46,06 | 1086,00 | 46,69 | 4301,00 | 46,77 | 13393,00 | 49,29 | 0,00 | 0,03 | |
| Colon | F | 7987,00 | 53,94 | 1240,00 | 53,31 | 4896,00 | 53,23 | 13781,00 | 50,71 | ||
| Total | 14806,00 | 100,00 | 2326,00 | 100,00 | 9197,00 | 100,00 | 27174,00 | 100,00 | |||
| M | 3689,00 | 52,23 | 586,00 | 50,60 | 2015,00 | 48,14 | 7586,00 | 54,94 | 0,00 | 0,05 | |
| Rectum | F | 3374,00 | 47,77 | 572,00 | 49,40 | 2171,00 | 51,86 | 6221,00 | 45,06 | ||
| Total | 7063,00 | 100,00 | 1158,00 | 100,00 | 4186,00 | 100,00 | 13807,00 | 100,00 | |||
| M | 4478,00 | 58,13 | 856,00 | 51,85 | 2256,00 | 51,32 | 7867,00 | 53,79 | 0,00 | 0,04 | |
| Lung | F | 3226,00 | 41,87 | 795,00 | 48,15 | 2140,00 | 48,68 | 6759,00 | 46,21 | ||
| Total | 7704,00 | 100,00 | 1651,00 | 100,00 | 4396,00 | 100,00 | 14626,00 | 100,00 | |||
| M | 13506,00 | 45,48 | 3699,00 | 42,77 | 4235,00 | 49,07 | 30526,00 | 47,46 | 0,00 | 0,03 | |
| Non-melanoma Skin | F | 16191,00 | 54,52 | 4949,00 | 57,23 | 4396,00 | 50,93 | 33794,00 | 52,54 | ||
| Total | 29697,00 | 100,00 | 8648,00 | 100,00 | 8631,00 | 100,00 | 64320,00 | 100,00 | 0,04 | ||
| M | 326,00 | 1,00 | 147,00 | 2,36 | 226,00 | 0,97 | 1388,00 | 2,24 | 0,00 | ||
| Breast | F | 32242,00 | 99,00 | 6095,00 | 97,64 | 23099,00 | 99,03 | 60529,00 | 97,76 | ||
| Total | 32568,00 | 100,00 | 6242,00 | 100,00 | 23325,00 | 100,00 | 61917,00 | 100,00 | |||
| M | 29351,00 | 99,95 | 4279,00 | 100,00 | 15229,00 | 99,88 | 49024,00 | 99,93 | 0,01 | 0,01 | |
| Prostate | F | 14,00 | 0,05 | 0,00 | 0,00 | 18,00 | 0,12 | 35,00 | 0,07 | ||
| Total | 29365,00 | 100,00 | 2099,00 | 53,26 | 15247,00 | 100,00 | 49059,00 | 100,00 | |||
Source: The author. Caption: *Gender: M= male, F= female.
Table 2.
Comparison of the frequencies of staging of neoplasms between the pre-pandemic and pandemic periods in the southeast region using the chi-square test.
Table 2.
Comparison of the frequencies of staging of neoplasms between the pre-pandemic and pandemic periods in the southeast region using the chi-square test.
| Cancer Location | Period | Number of cases | Staging | P value | Effect Size* | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | ||||||
| Stomach | Pre | 6379,00 | 315,00 | 203,00 | 818,00 | 2209,00 | 2834,00 | 0,00 | 0,03 | |
| Pan | 4846,00 | 166,00 | 153,00 | 640,00 | 1667,00 | 2220,00 | ||||
| Colon | Pre | 10315,00 | 398,00 | 145,00 | 1681,00 | 3732,00 | 4359,00 | 0,00 | 0,05 | |
| Pan | 8042,00 | 177,00 | 92,00 | 1325,00 | 2905,00 | 3543,00 | ||||
| Rectum | Pre | 9035,00 | 517,00 | 335,00 | 2109,00 | 3834,00 | 2240,00 | 0,00 | 0,05 | |
| Pan | 6724,00 | 283,00 | 325,00 | 1370,00 | 3076,00 | 1670,00 | ||||
| Lung | Pre | 9735,00 | 516,00 | 234,00 | 554,00 | 2480,00 | 5951,00 | 0,00 | 0,05 | |
| Pan | 6592,00 | 223,00 | 175,00 | 316,00 | 1617,00 | 4261,00 | ||||
| Non-melanoma Skin | Pre | 2532,00 | 213,00 | 813,00 | 720,00 | 420,00 | 366,00 | 0,00 | 0,06 | |
| Pan | 1595,00 | 153,00 | 468,00 | 417,00 | 342,00 | 215,00 | ||||
| Breast Cancer | Pre | 42778,00 | 1962,00 | 7822,00 | 12110,00 | 15919,00 | 4965,00 | 0,00 | 0,06 | |
| Pan | 31476,00 | 1227,00 | 4602,00 | 8729,00 | 12465,00 | 4453,00 | ||||
| Prostate Cancer | Pre | 31807,00 | 2816,00 | 3650,00 | 11537,00 | 6173,00 | 7631,00 | 0,00 | 0,06 | |
| Pan | 17432,00 | 1193,00 | 1871,00 | 5716,00 | 3690,00 | 4962,00 | ||||
Source: The author. Legend: *Obtained by Cramér’s V calculation; Pre = pre-pandemic period; Pan = pandemic period.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



